Embed Size (px)
Citation preview

The Psychological Adaptation ofPsychologists in Clinical Training:The Role of Cognition, Coping andSocial Support
Willem Kuyken1*, Emmanuelle Peters2, Mick Power3
and Tony Lavender4
1Centre for Cognitive Therapy, Department of Psychiatry, University ofPennsylvania, PA 19104, USA2Sub-Department of Clinical Health Psychology, University College London,1±19 Torrington Place, London WC1E 6BT, UK3Department of Psychiatry, University of Edinburgh, Kennedy Tower,Royal Edinburgh Hospital, Edinburgh EG10 5HF, UK4South Thames (Salomons) Clinical Psychology Training Scheme, SalomonsCentre, Broomhill Road, Southborough, Kent TN3 0TG, UK
The current study sought to profile the psychological adaptation ofpsychologists in clinical training and examine the extent to whichappraisal, coping and social support were related to psychologicaladaptation. A cross-sectional survey questionnaire design was used. Asample of 183 psychologists in clinical training (60.2% response rate)from 15 British clinical psychology training courses participated. Theycompleted measures of cognition (appraisals of threat and control overcourse-related stressors), coping and social support. A multidimen-sional assessment of psychological adaptation included measures ofperceived stress, self-esteem, anxiety and depression. Trainee clinicalpsychologists reported high levels of stress, but did not experienceextensive problems of psychological adaptation in terms of anxiety,depression, self-esteem problems, marital problems, family problems,external stressors, interpersonal conflict, work adjustment or substanceabuse. However, a significant subgroup reported self-esteem problems,work adjustment problems, depression and anxiety. Gender, age,current clinical placement and training course were related to psycho-logical adaptation. Appraisal processes, coping and social supportpredicted a significant amount of variation in psychological adaptation.Appraisals of threat, avoidance coping, emotional support from clinicalsupervisors, emotional support from courses and emotional supportfrom a confidante at home all predicted the variance in psychologicaladaptation. The findings were discussed in terms of a cognitive theoryof stress and adaptation and implications for clinical psychologytraining were considered. # 1998 John Wiley & Sons, Ltd.
CCC 1063±3995/98/040238±15$17.50# 1998 John Wiley & Sons, Ltd.
Clinical Psychology and PsychotherapyClin. Psychol. Psychother. 5, 238±252 (1998)
*Correspondence to: Willem Kuyken, Centre for Cognitive Therapy, Department of Psychiatry, University of Pennsylvania,PA 19104, USA.
Contract grant sponsor: Nuffield Foundation.

THE PSYCHOLOGICAL ADAPTATIONOF PSYCHOLOGISTSIn their day-to-day work clinical psychologistscome into direct contact with other people's distressand the individual, familial and environmentalconflicts and meanings that underlie this distress.In any week clinical psychologists might span theroles of individual, family and group therapist,researcher, advocate, teacher, manager, supervisorand team member. Each of these roles is challen-ging both personally and professionally; it is easy tounderstand how clinical psychologists mightexperience difficulties adapting to these stressors.Although there have been several rich autobiogra-phical accounts of mental health professionalsin distress (e.g. Rippere and Williams, 1985;Chadwick, 1993), the `existing data on the prevalenceof impairment in psychology are sparse and imprecise'(Sherman, 1996, p. 302). As Sherman (1996) hasargued, an understanding of the psychologicaladaptation of psychologists is important for severalreasons. First, psychologists and psychiatrists haveused their personal experiences to inform theirclinical models of work (Rogers, 1961; Frankl, 1963;Freud, 1964; Epstein, 1995; Cohen, 1996). Second,psychologists experiencing significant personal dis-tress may find that their work is adversely affected(Garfield and Bergin, 1971; Guy et al., 1989). Third,an understanding of the difficulties that psycholo-gists experience enables the systems in which theywork to adapt themselves to promote optimalworking environments (Lamb et al., 1991; Schwebelet al., 1994). Finally, an understanding of thepsychological adaptation of psychologists and aresponse to their identified needs is likely to shapethe profession as a whole in a positive way(Sherman, 1996).
While by no means conclusive, a theme emergingfrom the literature is that significant numbers ofmental health professionals experience significantmental health problems (Sherman, 1996). Forexample, in one study of psychiatrists in theirearly years of practice, over half reported moderateto incapacitating depression and anxiety (Looneyet al., 1980). The range of problems reported amongmental health professionals has included depres-sion, anxiety, somatic problems, relationship pro-blems, substance abuse, suicidal thoughts andattempts, job stress, marital problems and financialproblems (Prochaska and Norcross, 1983; Thoresonet al., 1989; Guy et al., 1989; Pope and Tabachnick,1994; Cushway et al., 1996).
At least two studies have looked specifically atpsychologists in clinical training (Cushway, 1992;Lamb et al., 1987). Cushway (1992), using aquestionnaire measure of `psychiatric caseness'(General Health Questionnaire, Goldberg, 1978),found high levels of psychological distress amongBritish trainee clinical psychologists (59%). Rates ofdistress were higher in the second and third year oftraining than in the first year of training. Neitherstudy considered the influence of the trainingprogramme or trainees' clinical placement on thepsychological adaptation of trainee clinical psychol-ogists. The high rates of distress found in thesestudies might be explained by the particulardemands and experiences of training as a clinicalpsychologist. Psychologists in training experiencemany life events (e.g. moving house, examinations),are often required to travel long distances, haveacademic workloads in addition to their clinicalwork, sometimes have to manage difficulties insupervision, may experience financial strains andare required to begin and end clinical placementsregularly throughout training. These stressors canplace demands on relationships and responsibilitiesboth at work and home. Moreover, trainingcan involve learning many and diverse ways ofworking (behavioural, cognitive, psychodynamicand systemic work), and learning a range of roles(e.g. therapist, researcher, team member). Further-more, the psychologist in training is continuallybeing evaluated, which can lead to a `crisis ofconfidence' (Cherniss, 1980) and a sense of alwaysworking on the edge of one's competence.
Studies on the psychological adaptation ofpsychologists have been marred by problems ofmethodology. Several studies report difficulties inrecruiting participants (e.g. Looney et al., 1980; Guyet al., 1989), raising doubts about the general-izability of these findings. Psychologists may beloathe to participate because of concerns aboutanonymity and if they do participate may givesocially desirable responses (Sherman, 1996). Thechoice of assessment of psychological adaptationhas tended to be unidimensional and psychiatric infocus. For example, several studies have relied onassessments that are screening devices for psychi-atric caseness (e.g. Cushway, 1992; Good et al.,1995), and do not enable a more comprehensivemapping of individuals along a continuum ofpsychological adaptation. Finally, much of thework has lacked a conceptual framework onwhich to hang its findings.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 239

A POSSIBLE CONCEPTUALFRAMEWORK: COGNITION, COPINGAND SOCIAL SUPPORTOne area of theoretical and empirical enquiry thatcan provide a helpful framework to understand andstudy psychological adaptation is the work ofLazarus and his colleagues on stress, appraisal andcoping: sometimes called the transactional theory ofcoping (see Lazarus and Folkman, 1984; Lazarus,1993). Transactional theory proposes that there aretwo processes in coping, appraisal and coping per se.Appraisal involves first assessing the stressfulsituation (e.g. the extent to which it is threateningor controllable) and second using the personal andcoping resources available to deal with the stress(e.g. social support, financial resources). Thus, aperson who perceives a situation as threatening, andhis or her own coping resources as inadequate, mayexperience stress (Lazarus and Folkman, 1984). It isargued that the person's appraisal determines whichcoping strategies are employed (e.g. planful problemsolving, avoidance or positive reappraisal). Appro-priate appraisals, it is suggested, lead to appropriatecoping and better psychological adaptation.
What is the evidence for this theory? The way inwhich stressful events are appraised and theavailable coping resources have each been shownto significantly mediate and/or moderate the effectsof stressors on longer-term adaptations, in cross-sectional and longitudinal studies (Folkman et al.,1986a, b; Scheier et al., 1986; Lazarus and Folkman,1987; Bolger, 1990; Valentiner et al., 1994). Theperceived controllability of the stressor appearscrucial (Folkman, 1984). A range of studies hasshown that a sense of control mediates the `stressor±psychological adaptation relationship' (see Thoits,1995). The theory predicts that appraisals of controllead to more effective coping, and there is evidencefor this hypothesis (Folkman Lazarus, 1980; Scheieret al., 1986; Lazarus and Folkman, 1987). However,not all studies have produced this effect (see Sulsand Fletcher, 1985). This has led to the suggestionthat appraisals of control must match the reality ofhow controllable the stressor is, sometimes called the`goodness-of-fit theory' (Aldwin, 1994). Within thistheory, the appropriateness of approach or avoid-ance coping will depend on the controllability of thestressor. Roth and Cohen (1986) have argued thatavoidance coping can be a useful short-term copingstrategy in reducing stress and increasing hope andcourage, particularly with short-term and unchange-able stressors. However, in the longer term it mayinterfere with appropriate action and inhibitemotional processing, and is therefore generally
associated with poorer psychological adaptation. Ingeneral, people who rely more on approach copingreport better psychological adaptation. In contrast,people who cope with stressors through avoidancecoping, beyond the initial crisis, tend to reportpoorer psychological adaptation. There is evidenceto support this broad, but qualified generalizationwith different populations, different stressors, anddifferent dimensions of psychological adaptation, inboth cross-sectional and longitudinal designs (Sulsand Fletcher, 1985).
Psychological research into occupational stresshas demonstrated a relationship between stressorsat work and poor psychological adaptation (Osi-pow and Davis, 1988; Decker and Borgen, 1993). Intwo cross-sectional studies of public sector andhealth workers, avoidance coping was associatedwith poorer psychological adaptation in the work-place, and this was mediated by appraisals ofcontrol (Bowman and Stern, 1995; Terry, Tonge andCallan, 1995). Among emergency services workers,perceived threat, avoidance coping and self-control-ling were associated with poorer psychologicaladaptation, particularly dissociative responses(Marmar et al., 1996).
As for social support at work, a review of theliterature suggests a main effect for social supporton psychological adaptation (20 of the 22 studiesreviewed) (Kahn and Byosiere, 1992). Several studiesof public sector and health care workers suggest thatpractical and emotional support from supervisorsand co-workers moderate the `stressor±psycho-logical adaptation relationship' (Ross et al., 1989;Baker et al., 1996). One study of work stress, supportand psychological adaptation among mental healthworkers found that social support from co-workers(particularly practical support) was related tolevels of emotional exhaustion, depersonalizationand a sense of personal accomplishment at work(Bowden, 1994). Interestingly, support outside workwas not related to these dimensions of psychologicaladaptation. Another study showed that supportfrom supervisors and co-workers was associatedmore strongly with psychological adaptation atwork than support from family or friends (Green-glass et al., 1996). This tentatively suggests thatdifferent types of support have different functionalvalues in work-related psychological adaptation.
THE CURRENT STUDY
The aim of the current study was to profile thepsychological adaptation of psychologists in clinical
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
240 W. Kuyken et al.

training, and examine to what extent appraisal,coping and social support could predict thevariance in psychological adaptation. Our firstresearch question was `What is the profile of stressand psychological adaptation in trainee clinicalpsychologists?' By including a standardized multi-dimensional measure of psychological adaptation,recruiting a representative sample, and including ameasure of problem minimization to address anysocial desirability effects we hoped to overcomesome of the difficulties of earlier studies.
The literature suggested several research hypo-theses about the role of appraisal, coping and socialsupport in psychological adaptation.
H1 Appraisals of less threat and greater controlover course stresses will be associated withmore approach coping and less avoidancecoping.
H2 More approach and less avoidance coping willpredict better psychological adaptation.
H3 Perceptions of course-based social supportwill have a greater function in predictingpsychological adaptation than home-basedsocial support.
METHOD
The Sample
One hundred and eighty-three first and second yeartrainee clinical psychologists from 15 3-year Britishclinical psychology training courses participated(total available sample 304, 60.2% response rate).One hundred and fifty participants were women(82%) and 33 were men (18%). Participants' meanage was 27.2 years (SD 4.05), ranging from 23 to43 years. The marital status of the participants wasas follows: single 87 (48%), cohabiting 58 (32%),married 36 (20%) and divorced 1 (0.5%). Onerespondent did not indicate his or her maritalstatus. The sample's profile of demographic featuresis broadly consistent with trainee clinical psych-ologists nationally (Clearing House for Post-graduate Courses in Clinical Psychology EqualOpportunities 1994, 1995).
The measures
AppraisalAs no validated measure of appraisal has been
published that is consistent with Lazarus andFolkman's (1984) theory, a measure of appraisal
was developed for this study. On conceptualgrounds questions addressing appraisals of(1) threat, (2) harm±loss and (3) control wereincluded. Questions were selected from severalkey papers suggested by Lazarus (Lazarus,personal communication, 1995) (Folkman andLazarus, 1985; Folkman et al., 1986a,b; Valentineret al., 1994; Florian et al., 1995). Appraisal questionswere matched with 5-point Likert scales rangingfrom `not at all/does not apply to me' (1) to `verymuch' (5).
Appraisals of threat, particularly to self-esteem,were assessed with six conceptually derived ques-tions, that have subsequently been confirmedthrough factor analyses (Folkman and Lazarus,1985; Folkman et al., 1986a,b). This suggests someface and construct validity. In this sample accep-table item intercorrelations (0.30 to 0.64), item±totalcorrelations (0.48 to 0.71) and substantial internalconsistency (Cronbach alpha 0.83) were found(N� 179). The questions selected for the appraisalsof threat scale asked about the extent to whichrespondents: `thought you might lose the approvalor respect of someone important to you because ofthe stresses of the course?'; `thought you might loseyour self-respect because of the stresses of thecourse?'; `thought you might appear incompetentbecause of the stresses of the course?'; `thought youmight lose the affection of someone important toyou because of the stresses of the course?'; `thoughtthe stresses of the course might make you appear tobe an uncaring person?'; and `thought you mightappear unethical because of the stresses of thecourse?' The threat appraisal scale was scoredthrough summative scaling, so that a higher scoreindicated greater appraisals of threat (range 6±30).
Appraisals of harm±loss were addressed throughfour questions. However these showed little vari-ance, low item±total correlations, and low internalconsistency and were therefore not used in furtheranalyses.
Appraisals of control over the demands andstresses of the course were measured with threequestions (one reverse scored). These questionswere derived from a theoretical theory (Lazarusand Launier, 1978), and have been subjected to testsof test±retest reliability, construct validity, predic-tive validity and criterion validity (Folkman andLazarus, 1980; Folkman et al., 1986a,b; Florian et al.,1995). Item intercorrelations (0.41 to 0.51), item±total correlations (0.48 to 0.56) and internal consist-ency (Cronbach alpha 0.71) were acceptable. Thethree questions included in this scale asked aboutthe extent to which `you have felt you had control
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 241

over the stresses of the course?'; `the stresses ofthe course were something you could change ordo something about?'; and `the stresses of thecourse were something you had to accept?' Thecontrol scale was scored through summativescaling (one question reverse scored), so that higherscores suggested appraisals of greater control (range3±15).
CopingThe Ways of Coping Questionnaire (WCQ) is a
well-established 50-question measure, addressing abroad range of emotional and behavioural copingstrategies. Folkman and Lazarus describe eightscales that can be derived from the WCQ. Theseare confrontative coping (six questions, e.g. `I stoodmy ground and fought for what I wanted', range0±18); distancing (six questions, e.g. `I went on as ifnothing had happened', range 0±18); self-controlling(seven questions, e.g. `I tried to keep my feelings tomyself', range 0±21); accepting responsibility (fourquestions, e.g. `I criticized or lectured myself', range0±12); escape±avoidance (eight questions, e.g. `Iavoided being with people in general', range 0±24);seeking social support (six questions, e.g. `I asked afriend or relative for advice', range 0±18); planfulproblem solving (six questions, e.g. `I just concen-trated on what I had to do next', range 0±18); andpositive reappraisal (seven questions, e.g. `I changedor grew as a person in a good way', range 0±21).Respondents were required to indicate the extent towhich they used each of the coping responses on4-point Likert scales, ranging from `does not applyor not used' (0), to `used somewhat' (1), to `usedquite a bit' (2), to `used a great deal' (3). Although,operationally it can be difficult to conceptualizecoping scales in terms of approach and avoidancecoping, the following distinctions were drawn:approach coping: seeking social support, planfulproblem solving and positive reappraisal; avoidancecoping: distancing and escape±avoidance. The fol-lowing scales included items addressing copingstrategies that were both approach and avoidance:confrontative coping, self-controlling and acceptingresponsibility.
The WCQ has been shown to have acceptablereliability and validity and responsiveness (Aldwinand Revenson, 1987; Folkman and Lazarus, 1988).In the current sample (N� 183), Cronbach alphasranged from 0.48 (accepting responsibility) to 0.68(positive reappraisal and escape±avoidance),suggesting adequate to moderate internal consist-encies.
Social SupportSocial support was assessed with the Significant
Others Scale (SOS) (Power et al., 1992). The SOS wasdeveloped to assess a person's self-ratings of actualand ideal emotional and practical support, and thediscrepancy between ideal and actual support. Thediscrepancy between actual and ideal supportprovides an index of likely satisfaction withavailable support in each area, and was the measureof social support used in this work. Higher scoressuggest greater dissatisfaction with support.
Power et al. (1992) report satisfactory reliabilityand validity. The following four named sources ofsocial support were included: the supervisor onclinical placement; the clinical psychology trainingcourse (i.e. the formal support structure providedby the training course); other trainees on the course;a confidante outside work (e.g. spouse, partner, aclose friend or relative). The scale was self-adminis-tered. Respondents rated each individual named foreach of the four types of support. Seven-pointLikert scales of the frequency that actual/ideal andemotional/practical support were felt were used,ranging from `never' (1) to `always' (7).
Perceived StressPerceived stress was assessed using the Perceived
Stress Scale (Cohen et al., 1983). This scale aims tomeasure the degree to which situations over theprevious month are appraised as stressful, andincludes questions about the unexpectedness, con-trollability and amount of stressors.
The 10-question scale was used because of itsestablished internal reliability, construct and pre-dictive validity (Cohen et al., 1983; Cohen andWilliamson, 1988). Questions are scored on 5-pointscales from `never' (0) to `very often' (4) (fourquestions reverse scored). Higher scores suggestgreater perceived stress (range 0-40).
Psychological AdaptationTo assess psychological adaptation the Employee
Assistance Program Inventory (EAPI) (Anton andReed, 1994) was used. The EAPI is a 120-questionmeasure designed as an assessment or screeningmeasure for working adults. It enables the identi-fication and profiling of psychological problems.Consistent with a conceptualization of adaptationas a multidimensional profile, the EAPI measures10 domains of psychological adaptation. These areanxiety, depression, self-esteem problems (tapsnegative self-evaluations and satisfaction withpersonal achievement), marital problems, familyproblems, external stressors (stressful events
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
242 W. Kuyken et al.

external to the work situation, including legal,financial, and health-related stressors), inter-personal conflict (conflicts with others at work),work adjustment (person's satisfaction with variousfeatures of work, including pay, opportunity foradvancement and working conditions), problemminimization (extent to which the person under-states the extent or severity of problems) andsubstance abuse (degree of disruption in interper-sonal, social and vocational functioning resultingfrom drug and/or alcohol use and abuse).
Scales are scored through summative scaling(with some questions reverse scored), such thatscale scores suggest greater problems in each of the10 domains of adaptation; the range of possiblescores for each scale is 10±40. Anton and Reed(1994) describe guidelines for calculating T scores(i.e. 0±100, mean 50, standard deviation 10) basedon large normative data sets (1266 employedadults). In addition, a screening cut-off for sub-stance abuse problems is suggested, for whichacceptable discriminant and convergent validity isreported. Anton and Reed (1994) report extensivedata attesting to the reliability and validity of themeasure. The influence of demographic variableson T scores is minimal (Anton and Reed, 1994).
Positive FeelingsTo assess positive aspects of psychological
adaptation a 4-item scale that comprises part of theWorld Health Organization Quality of Life Assess-ment (WHOQOL) was used (WHOQOL Group,1994, 1995, in press). The positive feelings scalemeasures how much a person experiences positivefeelings of contentment, balance, peace, happiness,hopefulness, joy and enjoyment. The scale is scoredthrough summative scaling, with higher scoressuggesting greater positive feelings (range 4±20).
The WHOQOL is still under development, butpreliminary data attest to its face, content anddiscriminant validity (WHOQOL Group, in press).In the current sample good internal consistency wasfound for the positive feelings scale (Cronbachalpha 0.79).
Procedure
Permission to carry out the study was requestedfrom clinical psychology training course directorsnationally. To maximize the response rate thesuggestions of Dillman (1978) and Streiner andNorman (1989) were followed. Their suggestionsinclude advance warning that the survey is coming,careful attention to the cover letter, ensuring
anonymity, personalization, enclosing a stampedaddressed envelope, reasonable questionnairelength and follow-up. The confidentiality of partici-pants was assured, and informed consent obtained.The questionnaires were distributed to individualtrainee clinical psychologists in the first and secondyears of training with prepaid addressed envelopesin November 1995, and were returned up to March1996.
RESULTS
The research question and hypotheses were ad-dressed in turn.1 However, before considering theresearch question and hypotheses, any influence ofthe demographic variables was examined.2 Thefollowing significant relationships were observed:older trainee clinical psychologists reported lesscontrol over the stresses of the course (rho�ÿ0.21,N� 182, p5 0.01) and reported more externalstressors than younger trainee clinical psychologists(rho� 0.23, N� 182, p5 0.001).
One-way ANOVAs were computed to comparemales and females across variables, co-varying agefor appraisals of control and external stressors.These suggested significant differences betweenmale and female trainees in: (1) distancing: maleM� 6.21, SD 2.71, 95% confidence interval 5.00±7.43; female M� 4.41, SD 2.42, 95% confidenceinterval 4.02±4.80; F(1, 182)� 12.79, p5 0.01; (2)seeking social support: male M� 8.67, SD 3.54,95% confidence interval 7.41±9.92; femaleM� 10.44, SD 3.11, 95% confidence interval 9.93±10.94; F(1, 182)� 8.32, p5 0.01; (3) substanceabuse problems: 13% of female trainees abovescale cut-off (416); 42% of male trainees abovescale cut-off (416); chi-square� 16.20, p5 0.001,N� 183.
In sum, male trainees were significantly morelikely to cope through distancing and less likely tocope through seeking social support than femaletrainees. They were also more likely to reportsubstance abuse problems than female trainees.
1To protect against the risk of Type I errors, a probability levelof p5 0.01 was set for all exploratory analyses, and aprobability level of p5 0.05 was set for hypothesis testing.2Several scales did not meet criteria for parametric statistics.Therefore, generally both parametric and non-parametricstatistics were computed throughout. When results observedusing Pearson and Spearman correlations were different, two-tailed Spearman correlations were reported.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 243

What is the profile of stress and psychologicaladaptation in trainee clinical psychologists?
To address this question descriptive statistics on thepsychological adaptation scales were examined(Table 1). The transformed T score on the problemminimization scale (mean 38.71, standard deviation8.84, 95% confidence intervals 37.36±40.01)suggested that the extent or severity of problemswere not being underreported.
Visual inspection of the stem and leaf plots anddescriptive statistics suggested that all EAPIpsychological adaptation scale scores were withinone standard deviation of the standardizationsample's descriptive statistics. However, significantnumbers of individuals in this sample reportedpoorer psychological adaptation than the standard-ization sample (positive skew, elevated means),particularly in terms of self-esteem problems, workadjustment problems, anxiety and depression(Table 1).3
The three EAPI questions concerned with hope-lessness (thought to be predictive of suicidalideation) were examined (e.g. `I feel hopelessabout my life'). Most respondents (480%) reportedno hopelessness, a significant minority reported
slight hopelessness (approximately 10%) and asmall number reported significant hopelessness(approximately 1%). The WHOQOL positive feel-ings scale suggested that most trainees reportedpositive feelings. Again, a significant number oftrainees reported the absence of positive feelings.
To examine the psychological adaptation ofpsychologists in clinical training further, the extentto which cognition, coping, social support andpsychological adaptation differed across courseswas examined. Differences were observed acrosscourses in: appraisals of threat (F(14, 178)� 2.54,p5 0.01); work adjustment problems (F(14, 182)�2.38, p5 0.01); and depression (F(14, 182)� 3.11,p5 0.001). Post-hoc Scheffe tests suggested nospecific differences between particular courses(p5 0.05). The significant differences across coursesin appraisals of threat and psychological adaptationraise the question of what features of courses accountfor these differences. One obvious difference is thenumber of people on each course. No significantassociation was found between course size and anyof the variables (no Pearson r significant at p5 0.01,N� 183).
Finally, the extent to which cognition, coping,social support and psychological adaptationdiffered across clinical placements (Adult MentalHealth N� 92, Children and Families N� 37,Learning Disabilities N� 41 and Older AdultsN� 13) was examined. Trainees on the AdultMental Health Placement reported greater control
Table 1. The psychological adaptation of trainee clinical psychologists (N� 183)
Mean (standarddeviation)
95% confidenceintervals
Percentage of trainees scoring1 and 2 standard deviations
above the mean
Distribution
1SD 2SD
Stress 17.37 (6.08) 16.48±18.26 ± ± Bi-modal
EAPI scalesSelf-esteem problems 56.73 (10.12) 55.24±58.23 35 15 Positive skewWork adjustment problems 53.53 (8.84) 52.23±54.84 26 5 Positive skewDepression 54.50 (11.07) 52.88±56.12 26 14 Positive skewExternal stressors 51.25 (9.78) 49.82±52.69 23 6 Positive skewFamily problems 51.81 (10.35) 50.28±53.33 19 8 Positive skewAnxiety 54.59 (10.17) 53.09±56.09 28 9 Bi-modalInterpersonal conflict 49.60 (8.67) 48.33±50.88 12 4 Positive skewMarital problems 47.99 (8.36) 46.76±49.22 9 3 Bi-modal
WHOQOL positive feelings 14.32 (2.25) 13.99±14.64 ± ± Negative skew
Scores on the EAPI psychological adaptation scales are transformed T scores (i.e. 0±100 from normative data). Scores on the perceivedstress scale (0±34) and WHOQOL positive feelings scale (4±20) are raw scores; normative data from which to calculate T scores are notavailable.
3`Significant numbers of trainees experiencing problems' wasdefined as 25% of trainees scoring at least one standarddeviation above the standardization sample mean providedby Anton and Reed (1994), namely a T score4 60.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
244 W. Kuyken et al.

than trainees on the Children and Families andLearning Disabilities placements {F(age co-varied)3, 180� 15.24, p5 0.001 post-hoc ScheffeÂ, p5 0.05};trainees on their Learning Disabilities Placementwere experiencing more work adjustment pro-blems than trainees on their Adult Mental HealthPlacement (F(3, 179)� 13.04, p5 0.001, post-hocScheffeÂ, p5 0.05); and trainees on their
Learning Disabilities and Older Adults Placementsreported more interpersonal conflict than traineeson their Adult Mental Health Placement(F(3, 179)� 7.45, p5 0.001, post-hoc ScheffeÂ,p5 0.05.
A series of correlational analyses and multipleregression analyses were computed to address theresearch hypotheses (Table 2, 3 and 4).
Table 3. Correlations between appraisal, coping, social support and psychological adaptation variables (Pearson r,two-tailed, N� 183)
EAPI Psychological Well-being Scales
Self-esteemproblems
Work adjustmentproblems
Depression Anxiety
AppraisalThreat 0.461 0.611 0.561 0.561
Control ÿ0.16 ÿ0.471 ÿ0.341 ÿ0.291
CopingConfrontative coping ÿ0.12 0.12 0.07 0.09Distancing 0.08 0.11 0.10 0.09Self-controlling 0.202 0.15 0.222 0.202
Seeking social support ÿ0.01 0.14 0.01 0.212
Accepting responsibility 0.411 0.311 0.361 0.491
Escape±avoidance 0.431 0.471 0.611 0.611
Planful problem solving 0.01 0.07 0.06 0.15Positive reappraisal 0.09 0.02 0.10 0.13
Social supportPractical support from supervisor 0.11 0.16 0.08 0.04Emotional support from supervisor 0.212 0.281 0.14 0.13Practical support from course 0.01 0.232 0.15 0.02Emotional support from course 0.212 0.331 0.16 0.07Practical support from other trainees 0.07 0.12 0.202 0.11Emotional support from other trainees 0.02 0.09 0.12 0.05Practical support from home confidante 0.11 ÿ0.02 0.18 0.07Emotional support from home confidante 0.261 0.01 0.212 0.12
1p5 0.05. 2p5 0.01. 3p5 0.001.
Table 2. Correlations between appraisals of threat and control and ways ofcoping (Pearson r, one-tailed, N� 183)
Coping Appraisals of threat Appraisals of control(N� 179) (N� 175)
Confrontative coping r� 0.10 rp(age)� 0Distancing r� 0.131 rp(age)�ÿ0.06Self-controlling r� 0.283 rp(age)�ÿ0.02Seeking social support r� 0.172 rp(age)� 0Accepting responsibility r� 0.443 rp(age)�ÿ0.131
Escape±avoidance r� 0.493 rp(age)�ÿ0.343
Planful problem solving r� 0.293 rp(age)� 0.05Positive reappraisal r� 0.172 rp(age)� 0.12
1p5 0.05. 2p5 0.01. 3p5 0.001.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 245
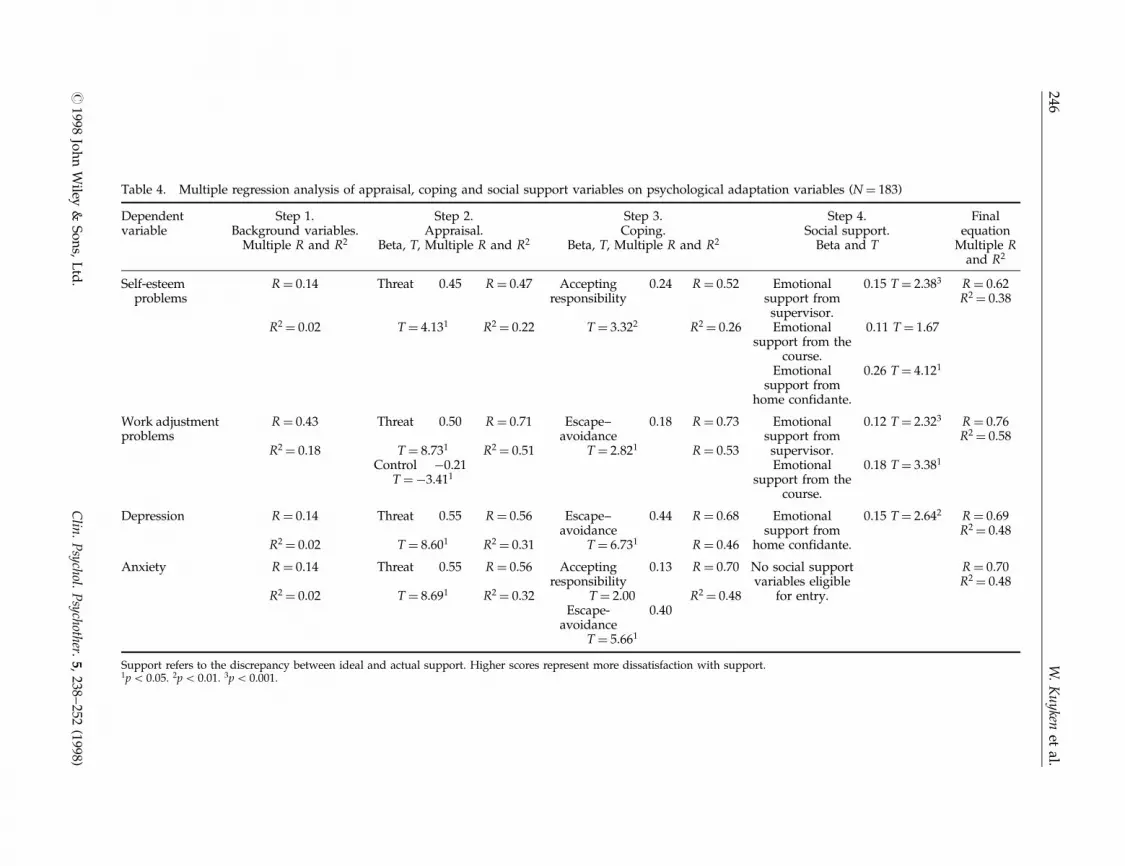
Table 4. Multiple regression analysis of appraisal, coping and social support variables on psychological adaptation variables (N� 183)
Dependentvariable
Step 1.Background variables.
Multiple R and R2
Step 2.Appraisal.
Beta, T, Multiple R and R2
Step 3.Coping.
Beta, T, Multiple R and R2
Step 4.Social support.
Beta and T
Finalequation
Multiple Rand R2
Self-esteemproblems
R� 0.14 Threat 0.45 R� 0.47 Acceptingresponsibility
0.24 R� 0.52 Emotionalsupport fromsupervisor.
0.15 T� 2.383 R� 0.62R2� 0.38
R2� 0.02 T� 4.131 R2� 0.22 T� 3.322 R2� 0.26 Emotionalsupport from the
course.
0.11 T� 1.67
Emotionalsupport from
home confidante.
0.26 T� 4.121
Work adjustmentproblems
R� 0.43 Threat 0.50 R� 0.71 Escape±avoidance
0.18 R� 0.73 Emotionalsupport fromsupervisor.
0.12 T� 2.323 R� 0.76R2� 0.58
R2� 0.18 T� 8.731 R2� 0.51 T� 2.821 R� 0.53Control ÿ0.21 Emotional
support from thecourse.
0.18 T� 3.381
T�ÿ3.411
Depression R� 0.14 Threat 0.55 R� 0.56 Escape±avoidance
0.44 R� 0.68 Emotionalsupport from
home confidante.
0.15 T� 2.642 R� 0.69R2� 0.48
R2� 0.02 T� 8.601 R2� 0.31 T� 6.731 R� 0.46
Anxiety R� 0.14 Threat 0.55 R� 0.56 Acceptingresponsibility
0.13 R� 0.70 No social supportvariables eligible
for entry.
R� 0.70R2� 0.48
R2� 0.02 T� 8.691 R2� 0.32 T� 2.00 R2� 0.48Escape-
avoidance0.40
T� 5.661
Support refers to the discrepancy between ideal and actual support. Higher scores represent more dissatisfaction with support.1p5 0.05. 2p5 0.01. 3p5 0.001.
#1998
Joh
nW
iley&
So
ns,
Ltd
.C
lin.
Psychol.
Psychother.
5,238
±252
(1998)
246W
.K
uyken
etal.

H1 Appraisals of less threat and greater controlover course stresses will be associated with moreapproach coping and less avoidance coping
Support for this hypothesis was mixed (Table 2).Appraisals of threat were associated with both moreapproach (seeking social support, planful problemsolving and positive reappraisal) and more avoid-ance coping (distancing and escape±avoidance).Appraisals of control were not associated withmore approach coping but were associated with lessavoidance coping (escape±avoidance).
Following Tabachnick and Fidell (1989), a mixedconceptual and statistical multiple regressionanalysis strategy was used to address the finaltwo hypotheses (Tables 3 and 4). Four hierarchicalregressions were computed to determine if back-ground variables (age, gender and year of train-ing),4 then appraisal variables, then copingvariables and then social support variables pre-dicted the variance in psychological adaptation.Four psychological adaptation variables, which hadbeen found to be important in this sample, wereselected as the dependent variable in eachregression analysis (self-esteem problems, workadjustment, depression and anxiety). Predictorvariables were selected on conceptual and statisticalgrounds. Background variables were added as thefirst step, as these had been found to be associatedwith psychological adaptation, to control anyconfounding effects. The order of entry for theindependent variables followed the order of influ-ence predicted by transactional theory. Therefore,appraisal variables were added in a second step,coping variables were added as a third step andsocial support variables were added as a fourthstep. Only those cognition, coping and socialsupport variables that correlated significantly(p5 0.01) were considered for entry into theequation (Table 3). At each step of the equation,variables not contributing significantly to theequation were dropped. The final regression equa-tions are shown in Table 4. Only variables thatremained significant for the final equation, when allrelevant variables had been added, are reported ateach step. Reported beta values were final equationvalues, not beta values at each step.
H2 More approach and less avoidance copingwill predict better psychological adaptation
Approach coping (i.e. seeking social support,planful problem solving and positive reappraisal)was not related to psychological adaptation(Tables 3 and 4). However, avoidance coping wasrelated to poorer psychological adaptation in termsof work adjustment problems, depression andanxiety. Coping through accepting responsibilitywas associated with self-esteem problems andanxiety.
H3 Perceptions of course-based social supportwill have a greater function in predictingpsychological adaptation than home-basedsocial support
As hypothesized, different types of social supportwere associated with psychological adaptation indifferent ways (Tables 3 and 4). On placement,dissatisfaction with emotional support from clinicalsupervisors predicted variance in both self-esteemand work adjustment problems. Support from thetraining course appeared to predict variance in theself-esteem and work adjustment of trainee clinicalpsychologists, but no other aspects of psychologicaladaptation. Support from a confidante at home wasassociated with psychological adaptation, in termsof self-esteem and depression.
DISCUSSION
What is the profile of stress and psychologicaladaptation in trainee clinical psychologists? Acomparison of our data with normative data setssuggest that while trainee clinical psychologistsreport relatively high levels of perceived stress(compared with a large stratified sample, Cohenand Williamson, 1988), as a group they do notreport extensive problems of psychological adapta-tion (Anton and Reed, 1994). Trainees' psycho-logical and social functioning at work and home(Anton and Reed, 1994) were in the normal range.Although an overall picture of psychologicaladaptation emerged, the findings suggested thatmore than 25% of trainees were experiencingdifficulties, particularly in terms of self-esteem,work adjustment, depression and anxiety.Although this work does not enable any definitivestatements about rates of global distress amongtrainee clinical psychologists, the findings contrastwith those of earlier studies suggesting high rates of
4Year of training served as proxy measure for clinicalplacement, thereby avoiding the need for four dummyplacement variables.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 247

global distress among mental health professionals(e.g. Looney et al., 1980; Guy et al., 1989; Cushway,1992). Possibly breaking down concepts such as`psychiatric caseness' into dimensions of psycho-logical adaptation enabled a more holistic assess-ment.
It is instructive to consider the subgroups ofindividuals who were experiencing difficulties. Ofthe men, 42% reported substance abuse problemsand tended to use less approach (specifically socialsupport seeking) and more avoidance coping(specifically distancing) than women. This findingreplicated Freudenberger's (1987) work with maletherapists. He argued that male therapists strugglewith particular personal issues that may manifestthemselves in mental health problems and sub-stance abuse (Freudenberger, 1990). Men are in aminority in British clinical psychology, and it ispossible that the avenues of available coping andsupport are experienced as less accessible to malethan female trainees.
Older trainees appeared to feel less control overthe stresses of the course, and reported greaterexternal stressors (e.g. legal, financial and health-related stressors). Older trainees have often hadexperiences of previous careers that can exacerbatethe difficulties of returning to study and mean thatthey have to cope concurrently with more externaldemands such as families and financial commit-ments. The fact that older trainees did not differfrom younger trainees in terms of stress or psycho-logical adaptation attests to their coping resourcesand/or support networks. Interestingly, traineeclinical psychologists on placements where multipleroles and systemic work are commonplace (i.e.Learning Disabilities and Children and Familiesplacements) experienced more difficulties (e.g.conflict with colleagues) than trainees on place-ments where individual clinical work is morecommonplace (Adult Mental Health placements).However, this may be confounded by year oftraining, as Adult Mental Health placements tendto occur in earlier stages of training. Furthermore,the study sampled only first and second yeartrainees, and findings cannot therefore be extendedto final year trainees.
Significant differences were found across trainingcourses in trainee clinical psychologists' workadjustment and depression. The data could notsuggest any firm explanation, although the explora-tory analyses suggested that the size of the course(defined as the number of trainees on a course) wasnot associated with psychological adaptation.Possible alternative explanations include courses'
selection criteria, staff±trainee ratios, support struc-tures, examination procedures and training models.The response rate, the sizes of the differences andthe fact that the pattern of differences was stableacross courses suggested that these differences werereal and warrant further enquiry.
The role of cognition, copingand social support
The hypothesized relationships between appraisal,coping and psychological adaptation were for themost part observed. Appraisals of threat werestrongly related to more avoidance coping, but wedid not predict that threat would also be related tomore approach coping. Appraisal processes, part-icularly threat appraisals, and avoidance copingappear to predict much of the variance in psycho-logical adaptation. Salkovskis (1996) has suggesteda cognitive formulation by which threat beliefs andavoidance behaviour maintain one another, leadingto hypervigilance to threat and disabling opportu-nities for disconfirmation, thus maintaining anxiety.Our findings provide only partial support forLazarus' theory, as threat appraisals appeared tomobilize trainees to use not only more avoidancecoping, but also more approach coping. Threat,therefore, may function as an alarm function tomobilize coping. Whilst this may explain thefindings, many alternative causal pathways arealso possible. For example, self-esteem is thoughtto mediate between cognition and psychologicaladaptation (Higgins, 1987).
The buffering effectiveness of support againstconsiderable levels of perceived stress, both fromthe course and a confidante at home, wassuggested. Specifically emotional support fromclinical supervisors, emotional support from thecourse and emotional support from a mainconfidante at home predicted much of the variancein psychological adaptation, particularly in termsof self-esteem. This is consistent with findingsthat approval or acceptance from a `generalizedother' (the training course) is predictive of self-esteem, perhaps because it is perceived as supportfrom an objective and credible source (see Harter,1996). Emotional support from a confidante outsidework might serve the function of `a secure psycho-logical base from which the individual can reemerge tomeet the . . . challenges' to their self-esteem (Harter,1996, p. 19). It is noteworthy that, as predicted,emotional support from clinical supervisors and thecourse contributed to prediction of work adjust-ment.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
248 W. Kuyken et al.

Possible explanations and implications
From the perspectives of trainee clinical psycholo-gists, the demands and challenges of training aregreat. These include a transformation in identity,learning to manage a variety of professional roles,coping with the demands of clinical and academicwork, professionally and personally challengingclinical work, changing clinical placements regul-arly and the demands that all these can place onrelationships and responsibilities both at work andat home. For the individual this can lead to sadnessover losses, fears about being overwhelmed, con-fusion over identity and concerns about self-worth(Stovholt and Ronnestad,1995). Yet, as one partici-pant remarked `There is a great pressure to be seen tobe coping and doing well'. A fear of admittingvulnerabilities or distress because of loss of status,poor evaluations, possible course failure and notwanting to become the `patient' may explain ourfindings that external demands and home and workrelationships are generally managed well. However,for some trainee clinical psychologists there is anemotional cost to self-esteem, anxiety and depres-sion. In male trainees this may be managed throughdistancing and manifest in substance abuse. Ourfindings tentatively suggest that acknowledging andchallenging appraisals of threat and low control,where appropriate, reducing avoidance coping andusing available support from clinical supervisors,the course and emotional support at home wouldpredict better psychological adaptation.
From the perspective of clinical psychologytraining courses, the responsibilities, demands andchallenges are also considerable. This study raisessome fundamental questions about how best toprovide support to trainees during a training that islikely to require them to develop significantly at apersonal and professional level. Although at anygiven time most trainees appear to cope well withexternal demands, a significant minority do so atsome expense to their psychological adaptation. Asthe number of funded places increases, it is likelythat this minority will also grow, and unless coursesfind ways to help such trainees develop moreadaptive coping strategies, the high pass andservice retention rates (Lavender et al., in press)are likely to fall. Indeed, it seems self-evident that iftrainees are unable to adopt adaptive coping styles,then they may be in a position of some difficultyassisting the people who come to them for help inadopting such strategies. Even those trainees whoappear to be coping well, nevertheless, faceconsiderable demands and will need assistance in
maintaining and developing their coping if theyare to both learn from and enjoy the training.Courses have made significant efforts in this regardalthough the extent to which they assess trainees'ability to cope at selection, integrate support intoclinical supervision, include such issues in teachingprogrammes and provide formal systems for sup-port remains variable. This is not to pretend thatstress can be taken out of training. Perhaps it is evennecessary to facilitate development, but care needsto be taken to ensure that it stays within manage-able proportions.
The findings relating to self-esteem are particu-larly interesting when considered with findings thatprofessional self-doubt is also an important issuefor qualified clinical psychologists (Cushway et al.,1996). There are at least three explanations. First,people with self-esteem problems may be attractedto the profession to resolve their problems throughtheir professional practice (Sherman, 1996). Second,the profession as a whole is young and smallcompared with more established health professions.In a health service climate of continual change andservice evaluation, the profession is in the vulner-able position of continually asserting and provingits worth both to allied health professionals andcommissioners of clinical psychology services. Thisrepresents a threat to the profession as a whole,which may be reflected in the self-esteem ofindividual clinical psychologists. Third, there maybe aspects of the work of clinical psychologists thatare intrinsically threatening to self-esteem, such asmultidisciplinary work in a model evolved by andfor other professions.
Methodological limitations
Several methodological limitations limit theinterpretation of the findings. First, the cross-sectional design does not enable a causal relation-ship between appraisal, coping, social support andpsychological adaptation to be established. Further-more, it is possible that at different times, differentindividuals experience difficulties of self-esteemproblems, anxiety and depression. Second, severalmeasures used in this research have not beenwidely used (social support and psychologicaladaptation measures). This limits comparisonswith earlier studies using different measures.Third, the correlational and regression analysesmay have been confounded by common methodvariance. However, appraisal, coping and psycho-logical adaptation are subjective concepts. There-fore, arguably, subjective self-report ratings are the
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 249

most valid and reliable way of collecting thisinformation, albeit at some cost to common methodvariance. Nonetheless, it is important to interpretfindings and the degree of relationships with respect tocommon method variance. Finally, our use ofsurvey methodology enabled a larger and morerepresentative sample to be studied, but at somecost to depth of information. More in-depth andlongitudinal studies are required to address issuesof generalizability and causality.
ACKNOWLEDGEMENTS
We are indebted to the psychologists in clinicaltraining who chose to share their experience ofclinical psychology training. We are grateful toGillian Bowden, Margie Callanan, Steve Joseph andSophia Rabe-Hesketh for their comments andsupport in the planning, carrying out, analysisand writing up of this project, to Jane Henry for thedata entry and to Halley Cohen for proofreading.Finally we are grateful to Delia Cushway and twoanonymous reviewers for their helpful commentson an earlier draft of this paper. This work wassupported by the South Thames (Salomons), Uni-versity College London and Edinburgh ClinicalPsychology Training Courses and by a grant fromthe Nuffield Foundation awarded to the secondauthor.
REFERENCES
Aldwin, C. M. (1994). Stress, Coping and Development: AnIntegrative Perspective. New York: Guilford.
Aldwin, C. M. and Revenson, T. A. (1987). Does copinghelp? A re-examination of the relation between copingand mental health. Journal of Personality and SocialPsychology, 53, 337±348.
Anton, W. D. and Reed, J. R. (1994). Employee AssistanceProgram Inventory: Professional Manual. PsychologicalAssessment Resources, Inc.
Baker, E., Israel, B. and Schurman, S. (1996). Role ofcontrol and support in occupational stress: An inte-grated model. Social Science and Medicine, 43, 1145-1159.
Bolger, N. (1990). Coping as a personality process:A prospective study. Journal of Personality and SocialPsychology, 59, 525±537.
Bowden, G. (1994). Work stress, burnout and coping:A review and an empirical study of staff in supportedhousing. Clinical Psychology and Psychotherapy, 1,219±232.
Bowman, G. D. and Stern, M. (1995). Adjustment tooccupational stress: The relationship of perceivedcontrol to effectiveness of coping strategies. Journal ofCounselling Psychology, 42, 294±303.
Chadwick, P. K. (1993). The stepladder to the impossible:A first hand phenomenological account of a schizoaf-fective psychotic crisis. Journal of Mental Health, 2,239±250.
Cherniss, C. (1980). Staff Burnout: Job Stress in the HumanServices. Beverly Hills, CA: Sage.
Cohen, I. (1996). Lessons from an Ever-evolving Therapist.Sarasota, FL: Professional Resource Press.
Cohen, S. and Williamson, G. M. (1988). Perceived stressin a probability sample in the United States. In:A Spacapan and A. Oskamp (Eds), The Social Psychologyof Health. California: Sage.
Cohen, S., Kamarck, T. and Mermelstein, R. (1983).A global measure of perceived stress. Journal of Healthand Social Behaviour, 24, 385±396.
Cushway, D. 1992). Stress in clinical psychology trainees.British Journal of Clinical Psychology, 31, 169±179.
Cushway, D., Tyler, P. A. and Nolan, P. (1996). Develop-ment of a stress scale for mental health professionals.British Journal of Clinical Psychology, 35, 279±296.
Decker, P. J. and Borgen, F. H. (1993). Dimensions of workappraisal: Stress, strain, coping, job satisfaction andnegative affectivity. Journal of Counselling Psychology, 40,470±478.
Dillman, D. A. (1978). Mail and Telephone Surveys: The TotalDesign Method. New York: Wiley.
Epstein, M. (1995). Thoughts Without a Thinker: Psycho-therapy from a Buddhist Perspective. New York: BasicBooks.
Florian, V., Mikulincer, M. and Taubman, O. (1995).Does hardiness contribute to mental health during astressful real-life situation? The roles of appraisal andcoping. Journal of Personality and Social Psychology, 68,687±695.
Folkman, S. (1984). Personal control and stress and copingprocesses: A theoretical analysis. Journal of Personalityand Social Psychology, 46, 839±852.
Folkman, S. and Lazarus, R. S. (1980). An analysis ofcoping in a middle-aged community sample. Journal ofHealth and Social Behaviour, 21, 219±239.
Folkman, S. and Lazarus, R. S. (1985). If it changes it mustbe a process: A study of the emotion and coping duringthree stages of college examination. Journal of Personalityand Social Psychology, 48, 150±170.
Folkman, S. and Lazarus, R. S. (1988). Manual for the Waysof Coping Questionnaire. Palo Alto, CA: ConsultingPsychologists Press.
Folkman, S., Lazarus, R. S., Dunkel-Schetter, C., DeLon-gis, A. and Gruen, R. J. (1986a). Dynamics of a stressfulencounter: cognitive appraisal, coping and encounteroutcomes. Journal of Personality and Social Psychology, 50,992±1003.
Folkman, S., Lazarus, R. S., Gruen, R. and DeLongis, A.(1986b). Appraisal, coping and health status andpsychological symptoms. Journal of Personality and SocialPsychology, 50, 571±579.
Frankl, V. E. (1963). Man's Search for Meaning. New York:Pocket Books.
Freud, S. (1964). Analysis terminable and interminable. In:J. Strachey (Ed and Translator), The Standard Edition ofthe Complete Psychological Works of Sigmund Freud,Vol. 23. London: Hogarth Press.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
250 W. Kuyken et al.

Freudenberger, H. J. (1987). Chemical abuse amongpsychologists: Symptoms, causes and treatment issues.In: R. R. Kilburg, P. E. Nathan and R. W. Thoresun(Eds), Professionals in Distress. Washington DC: Amer-ican Psychological Association.
Freudenberger, H. J. (1990). Therapists as men and men astherapists. Psychotherapy, 27, 340±343.
Garfield, S. and Bergin, A. (1971). Personal therapy,outcome and some therapist variables. Psychotherapy:Theory, Research and Practice, 8, 251±253.
Greenglass, E., Fiksenbaum, L. and Burke, R. J. (1996).Components of social support, buffering effects andburnout: Implications for psychological functioning.Anxiety, Stress and Coping, 9, 185±197.
Goldberg, D. (1978). Manual of the General Health Ques-tionnaire. Windsor: NFER-Nelson.
Good, G. E., Thoreson, R. W. and Shaughnessy, P. (1995).Substance use, confrontation of impaired colleagues,and psychological functions among counselling psy-chologists: A national survey. The Counselling Psych-ologist, 23, 703±721.
Guy, J. D., Poelstra, P. L. and Stark, M. J. (1989). Personaldistress and therapeutic effectiveness: National surveyof psychologists practising psychotherapy. ProfessionalPsychology: Research and Practice, 20, 48±50.
Harter, S. (1996). Historical roots of contemporary issuesinvolving self-concept. In: B. A. Bracken (Ed), Handbookof Self-concept: Developmental, Social and Clinical Con-siderations. New York: Wiley.
Higgins, E. (1987). Self-discrepancy: Theory relating selfand affect. Psychological Review, 94, 319±340.
Kahn, R. L. and Byosiere, P. (1992). Stress in organiz-ations. In: M. D. Dunnette and L. M. Hough (Eds),Handbook of Industrial and Organizational Psychology, 2ndedn. Palo Alto, CA: Consulting Psychologists Press.
Lamb, D. H., Cochran, D. J. and Jackson, V. R. (1991).Training and organizational issues associated withidentifying and responding to intern impairment.Professional Psychology: Research and Practice, 22, 291±296.
Lamb, D. H., Presser, N. R., Pfost, K. S., Baum, M. C.,Jackson, V. R. and Jarvis, P. A. (1987). Confrontingprofessional impairment during the internship: Identi-fication, due process and remediation. Professionalpsychology: Research and Practice, 18, 597±603.
Lavender, A., Rolleston, M. and Thompson, L. (in press).Training and staff retention: National issues andfindings from the South Thames (Salomons) ClinicalPsychology Training Scheme. Clinical Psychology Forum.
Lazarus, R. S. (1993). Coping theory and research: past,present, and future. Psychosomatic Medicine, 55,234±247.
Lazarus, R. S. and Folkman, S. (1984). Stress, Appraisal andCoping. New York: Springer Publishing Company.
Lazarus, R. S. and Folkman, S. (1987). Transactionaltheory and research on emotions and coping. EuropeanJournal of Personality, 1, 141±169.
Lazarus, R. S. and Launier, R. (1978). Stress relatedtransactions between person and environment. In: L. A.Pervin and M. Lewis (Eds), Perspectives in InteractionalPsychology. New York: Plenum Press.
Looney, J. G., Harding, R. K., Blotcky, M. J. and Barnhart,F. D. (1980). Psychiatrists' transition from training
to careers: Stress and mastery. American Journal ofPsychiatry, 137, 32±36.
Marmar, C. R., Weiss, D. S., Metzler, T. J. and Delucchi, K.(1996). Characteristics of emergency services personnelrelated to peritraumatic dissociation during criticalincident exposure. American Journal of Psychiatry, 152,94±102.
Osipow, S. H. and Davis, A. S. (1988). The relationship ofcoping resources to occupational stress and strain.Journal of Vocational Behaviour, 27, 98±108.
Pope, K. S. and Tabachnick, B. G. (1994). Therapists aspatients: A national survey of psychologists' experi-ences, problems and beliefs. Professional Psychology:Research and Practice, 25, 247±258.
Power, M. J., Champion, L. A. and Aris, S. J. (1992). Thedevelopment of a measure of social support: TheSignificant Others Scale (SOS). British Journal of ClinicalPsychology, 27, 349±358.
Prochaska, J. O. and Norcross, J. C. (1983). Psychothera-pists' perspectives on treating themselves and theirclients for psychic distress. Professional Psychology:Research and Practice, 14, 642±655.
Rippere, V. and Williams, R. (1985). Wounded Healers:Mental Health Workers' Experiences of Depression.New York: Wiley.
Rogers, C. R. (1961). On Becoming a Person: A Therapist'sView of Psychotherapy. London: Constable.
Ross, R. R., Altmaier, E. M. and Russell, D. W. (1989).Job stress, social support, and burnout among counsel-ling center staff. Journal of Counselling Psychology, 36,464±470.
Roth, S. and Cohen, L. J. (1986). Approach, avoidance,and coping with stress. American Psychologist, 41,813±819.
Salkovskis, P. M. (1996). Avoidance behaviour is motiv-ated by threat beliefs: A possible resolution of thecognitive-behaviour debate. In: P. M. Salkovskis (Ed),Trends in Cognitive and Behavioural Therapies. Chichester:Wiley.
Scheier, M., Weintraub, J. and Carver, C. (1986). Copingwith stress: Divergent strategies for optimists andpessimists. Journal of Personality and Social Psychology,51, 1257±1264.
Schwebel, M., Skorina, J. K. and Schoener, G. (1994).Assisting Impaired Psychologists, revised edn. Washing-ton DC: American Psychological Association.
Sherman, M. D. (1996). Distress and professionalimpairment due to mental health problems amongpsychotherapists. Clinical Psychology Review, 16,299±315.
Stovholt, T. M. and Ronnestad, M. H. (1995). The EvolvingProfessional Self: Stages and Themes in Therapist andCounselling Development. Chichester: Wiley.
Streiner, D. L. and Norman, G. R. (1989). HealthMeasurement Scales: A Practical Guide to Their Develop-ment and Use. Oxford: Oxford University Press.
Suls, J. and Fletcher, B. (1985). The relative efficacy ofavoidant and non-avoidant coping strategies: A meta-analysis. Health Psychology, 4, 249±288.
Tabachnick, B. G. and Fidell, L. S. (1989). UsingMultivariate Statistics, 2nd edn. New York: Harper andRow.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
Psychologists in Clinical Training 251

Terry, D. J., Tonge, L. and Callan, V. J. (1995). Employeeadjustment to stress: The role of coping resources,situational factors, and coping responses. Anxiety, Stressand Coping, 8, 1±24.
Thoits, P. A. (1995). Stress, coping and social supportprocesses. Where are we? What next? Journal of Healthand Social Behaviour, Suppl., 53±79.
Thoreson, R. W., Miller, M. and Krauskopf, C. J. (1989).The distressed psychologist: prevalence and treatmentconsiderations. Professional Psychology: Research andPractice, 20, 153±158.
Valentiner, D. P., Holahan, C. J. and Moos, R. H. (1994).Social support, appraisals of event controllability and
coping: An integrative model. Journal of Personality andSocial Psychology, 66, 1094±1102.
WHOQOL Group (1994). Development of the WHOQOL:Rationale and current status. International Journal ofMental Health, 23, 5±27.
WHOQOL Group (1995). The World Health OrganizationQuality of Life assessment (WHOQOL): Position paperfrom the World Health Organization. Social Science andMedicine, 41, 1403±1409.
WHOQOL Group (in press). The World Health Organiza-tion Quality of Life assessment (WHOQOL): Develop-ment and general psychometric properties. SocialScience and Medicine.
# 1998 John Wiley & Sons, Ltd. Clin. Psychol. Psychother. 5, 238±252 (1998)
252 W. Kuyken et al.





























