Embed Size (px)
Citation preview

PHOTOBIOLOGY DOI 10.1111/j .1365-2133.2006.07484.x
Topical application of 5-aminolaevulinic acid, methyl5-aminolaevulinate and hexyl 5-aminolaevulinate onnormal human skinA. Juzeniene,* P. Juzenas,* L-W. Ma,* V. Iani* and J. Moan*�
*Department of Radiation Biology, Institute for Cancer Research, The Norwegian Radium Hospital, 0310 Montebello, Oslo, Norway
�Department of Physics, Oslo University, 0316 Blindern, Oslo, Norway
CorrespondenceAsta Juzeniene.
E-mail: [email protected]
Accepted for publication22 May 2006
Key words5-aminolaevulinic acid, hexyl 5-aminolaevulinate,
methyl 5-aminolaevulinate, photodynamic therapy,
protoporphyrin IX
Conflicts of interestNone declared.
Summary
Background 5-Aminolaevulinic acid (ALA) and its ester derivatives are used in photo-dynamic therapy. Despite extensive investigations, the differences in biodistribu-tion and pharmacokinetics of protoporphyrin IX (PpIX) induced by ALA and itsderivatives are still not well understood, notably for humans.Objectives To study porphyrin accumulation after topical application of ALA andtwo of its ester derivatives in normal human skin.Methods Creams containing 0Æ2%, 2% and 20% (w/w) of ALA, methyl 5-amino-laevulinate (MAL) and hexyl 5-aminolaevulinate (HAL) were applied on normalhuman skin of six volunteers. The amount and distribution of porphyrins formedin the skin was investigated noninvasively by means of fluorescencespectroscopy.Results Fluorescence emission and excitation spectra exhibited similar spectralshapes for the all drugs, indicating that mainly PpIX was formed. Low concentra-tions (0Æ2% and 2%) of MAL induced considerably less PpIX in normal humanskin than similar concentrations of ALA and HAL. A high concentration (20%) ofALA gave higher PpIX fluorescence in normal human skin than was found forMAL and HAL.Conclusions The concentrations inducing half of the maximal PpIX fluorescence arearound 2% for ALA, 8% for MAL and 1% for HAL.
Photodynamic therapy (PDT) combines the administration of
a photosensitizer and light exposure. In many cases photosen-
sitizers are preferentially localized in neoplastic tissue.1 Light
exposure initiates photosensitizing reactions, resulting in pho-
todamage and elimination of the tumour. Porphyrin-type dyes
are commonly used as photosensitizers in PDT.2 Under excita-
tion with visible light porphyrins fluoresce, and their charac-
teristic red emission has been suggested for use in
fluorescence diagnosis of neoplastic tissues.3 Most importantly,
fluorescence spectroscopy enables noninvasive investigation of
neoplastic and normal tissues labelled with porphyrins.2 Dur-
ing the last two decades tissue imaging using fluorescence has
been extensively exploited in vivo.4,5
A new approach in PDT, namely to use the endogenous
photosensitizer protoporphyrin IX (PpIX), has been introduced
during the past decade. Accumulation of PpIX in tissues is
achieved by exogenous administration of its natural precursor
5-aminolaevulinic acid (ALA). Normally, every living cell syn-
thesizes PpIX from endogenous ALA. The haem biosynthesis
cycle tightly regulates the endogenous levels of ALA, and con-
centrations of PpIX high enough to induce tissue photosensiti-
zation normally do not accumulate. ALA administered
exogenously bypasses this feedback control and consequently
free PpIX accumulates in the cells. Destruction of cells by
endogenous porphyrins was suggested by Malik and Lugaci.6
PpIX formation in animal tumours was studied by Qian et al.7
Kennedy et al. applied ALA in the clinics, and so-called ALA-
PDT was proposed for clinical practice by several investiga-
tors.8–11 ALA-induced PpIX is also intended for use in fluores-
cence diagnosis.12 ALA can be administered either systemically
(intravenously or orally) or topically in an ointment applied
directly on lesions.10,11,13 Basically, topical application is
advantageous over systemic administration in ALA-PDT as sys-
temic photosensitization is avoided.
Ester derivatives of ALA have been proposed for use in
PDT.14–16 These derivatives are more lipophilic17 and were
expected to penetrate deeper than ALA.18 However, it appears
that ALA goes more readily into circulation than ALA esters,19
which is an opposing argument. Despite extensive investiga-
tions, the differences in biodistribution and pharmacokinetics
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799 791

of ALA and its derivatives are still not well understood, especi-
ally in humans. Therefore, the aim of the present work was to
study the accumulation of porphyrin after topical application
of ALA and two of its ester derivatives in normal human skin.
The amount and distribution of PpIX formed in the skin was
investigated noninvasively by means of fluorescence spectros-
copy. Considerations for dosimetry (drug concentration, appli-
cation time) are discussed on the basis of the experimental
results.
Materials and methods
Chemicals
ALA and methyl 5-aminolaevulinate (MAL) were purchased
from Sigma Chemical Co. (St Louis, MO, U.S.A.). Hexyl 5-
aminolaevulinate (HAL) was kindly supplied by PhotoCure
ASA (Oslo, Norway).
Human volunteers
Fluorescence measurements were carried out in six healthy
white-skinned volunteers (age range 29–57 years) with skin
types II or III. The study was approved by the local ethical
committee (Regional Komite for Medisinsk Forskningsetikk
Sør-Norge, ref. S-05112). Three volunteers had visually lighter
skin and three volunteers had visually darker skin.
Topical application of 5-aminolaevulinic acid, methyl
5-aminolaevulinate and hexyl 5-aminolaevulinate
For the experiments intended to study fluorescence kinetics,
creams were prepared using 0Æ2%, 2% and 20% (w/w) of
ALA, MAL and HAL in a standard ointment (Unguentum;
Merck, Darmstadt, Germany). Transparent adhesive dressings
(OpSite Flexifix; Smith & Nephew Medical Ltd, Hull, U.K.)
with defined cut areas of 1 cm2 were applied on the upper
right arm of six volunteers with a distance of approximately
1 cm between adjacent application spots. Approximately
75 ± 10 mg cm)2 of the freshly prepared cream formulations
were applied topically on a single spot of defined area 1 cm2
(Fig. 1a). After cream application, the whole area was covered
with another dressing of the same type. The creams were
maintained continuously on the test spots for the duration of
the experiment (24 h).
Fluorescence excitation spectroscopy was performed on
three volunteers. Twenty per cent ALA (1Æ2 mmol g)1), 20%
MAL (1Æ1 mmol g)1), 20% HAL (0Æ8 mmol g)1) creams and
(a) (b)
Fig 1. Set of application areas on the upper arm of the volunteers used for fluorescence kinetics (a) and fluorescence excitation spectroscopy
(b). Numbers denote percentage of 5-aminolaevulinic acid (A), methyl 5-aminolaevulinate (M) and hexyl 5-aminolaevulinate (H) in the cream
and C is the control (ointment only).
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
792 Topical ALA and its esters on human skin, A. Juzeniene et al.

ointment only were applied topically on defined application
areas (Fig. 1b) on the upper left arm. The dressings were
removed and the creams were gently wiped off after 6 h of
application. The fluorescence excitation spectra were measured
on the application areas immediately after cream removal
(corresponding to 6 h after application) and at 9, 12 and
24 h after application.
Fluorescence measurements
The fluorescence of porphyrins was measured noninvasively
with a fibre-optic probe coupled to a luminescence spectro-
meter (LS50B; Perkin Elmer, Norwalk, CT, U.S.A.). The probe
is a commercially available fibre accessory (Perkin-Elmer, two
1-m fused silica fibre bundles joined in parallel at the measur-
ing tip) fitted with a cylinder-shaped aluminium spacer
(6Æ5 mm diameter), which provides a constant fixed distance
of 10 mm between the fibre ends and the sample surface. This
assures a relatively uniform distribution of the excitation light
over the area to be measured and provides the maximum
fluorescence signal for a given set-up.
For kinetic measurements, fluorescence emission was meas-
ured at 635 nm, following application of 407-nm excitation
light from the luminescence spectrometer. This light had a
low intensity (< 1 mW cm)2) and did not induce any signifi-
cant photobleaching of PpIX. A 515-nm cut-off filter built in
the luminescence spectrometer was used on the emission side
of the spectrometer. In addition, complete emission spectra in
the range of 550–800 nm were measured. The fluorescence
measurements were carried out through the transparent occlu-
sive dressing, which did not alter the fluorescence signal.
For fluorescence excitation spectroscopy, the emission
wavelength was set at 705 nm, corresponding to the second
emission maximum of PpIX. The complete excitation spectra
were recorded in the range of 300–685 nm. An interference
filter (Ealing Electro-Optics, Inc., Holliston, MA, U.S.A.) with
a narrow bandpass (700–720 nm) was used on the emission
side of the luminescence spectrometer.
The autofluorescence background, i.e. the fluorescence of
the skin measured before the application of the drugs, was
subtracted from the fluorescence data. Individual fluorescence
data were calculated as means of three recordings and the pre-
sented data are means from all volunteers within the groups.
Error bars represent SEM.
Light transmission through human skin
A specimen of healthy human skin, excised from the abdom-
inal region of a patient, was kindly supplied by Dr J. Evensen
(Oncology Department of the Norwegian Radium Hospital,
Oslo). Light emitted from a 10-W halogen lamp was guided
on to the skin surface and the light transmitted through the
skin was collected with a quartz fibre (diameter 1 mm)
attached to the other side of the skin. The distance between
the skin surface and the fibre, i.e. the thickness of the skin,
was set by a micrometric screw.20 The fibre was connected to
the luminescence spectrometer and emission spectra of the
transmitted light were recorded in the range of 300–900 nm
for different skin thicknesses. The light fluence followed an
exponential decay with increasing skin thickness and the light
penetration depth d was determined as described earlier.20
Kinetics analysis and statistics
The kinetics of PpIX fluorescence were plotted as a function of
application time. The significance (P < 0Æ05) of differences in
kinetics was tested with Student’s t-test. Concentration
dependence curves were fitted (P < 0Æ01) with the equation
describing a saturating process:
F ¼ FmaxC
C1=2 þ Cð1Þ
where F is measured fluorescence intensity of PpIX, C is con-
centration (%) of ALA or its derivatives in the applied cream,
Fmax is the maximal intensity of PpIX fluorescence that can be
achieved after application of the cream, and C1/2 is the con-
stant for the process showing the concentration of the drug in
the applied cream that will induce 50% of the maximal
amount of a fluorophore (in our case, that will induce half of
the maximal fluorescence, F ¼ ½Fmax).
Spectroscopic determination of the penetration depth
Comparison of the spectral shape of the excitation spectra, by
normalizing their intensity to 1 at 633 nm, can be used for
estimation of PpIX fluorescence depth:21
FðkexÞ ¼ F0ðkexÞs�1ð1� e�dsÞ ð2Þ
in which s ¼ 1dðkexÞ þ
1dðkemÞ and F0 is the excitation spectrum
recorded in cells in vitro under dilute conditions, taken from
our previous work,21 F is the excitation spectrum measured
with the fibre probe on the surface of the skin, kex ¼ 300–
685 nm, kem ¼ 705 nm and d(k) is the light penetration
depth measured in the human skin for a certain wavelength k.The depth d of PpIX fluorescence is then varied to obtain the
best fit. The depth d is expressed in comparative units (comp.
u.) as the excitation spectra compare relative penetration of
the drugs, and not the actual penetration depth.
Results
Protoporphyrin IX accumulation in normal human skin
Typical fluorescence emission and excitation spectra of PpIX
were observed in normal human skin after topical application
of the creams containing ALA or its derivatives (Fig. 2). Top-
ical application of ALA, MAL and HAL resulted in gradual
increase of PpIX fluorescence, which depended on the concen-
tration (Fig. 2). Low concentration (0Æ2%) induced negligible
amounts of PpIX in the case of MAL, whereas ALA and HAL
gave significantly higher fluorescence (Fig. 2a). An intermedi-
ate concentration (2%) of MAL induced PpIX but significantly
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
Topical ALA and its esters on human skin, A. Juzeniene et al. 793

less compared with ALA and HAL (Fig. 2b). The difference
was not statistically significant between 2% ALA and 2% HAL.
The highest PpIX fluorescence was achieved using 20% of
the drugs in the cream. ALA at 20% gave more PpIX in nor-
mal skin than 20% MAL and 20% HAL (Fig. 2c), but differ-
ences were not statistically significant. The variations of PpIX
fluorescence between volunteers are reflected in large error
bars (Fig. 2).
Fluorescence images taken in one of the volunteers showed
a strong fluorescence in normal skin after a 12-h topical appli-
cation of 20% ALA, 20% MAL and 20% HAL cream (Fig. 3b).
In this case the strongest fluorescence was observed with ALA
and MAL cream. HAL (20%) cream had lower viscosity and
was distributed over a larger area than ALA or MAL (Fig. 3b).
Fluorescence measurements of PpIX from the same patch
showed that after a 12-h cream application ALA gave the
strongest fluorescence, while for MAL and HAL the fluores-
cence was 10% and 25% weaker, respectively, compared with
ALA (Fig. 3b). Fluorescence images of the same area at 24 h
after cream removal showed the strongest fluorescence for
ALA cream and weaker for MAL and HAL (Fig. 3c). At 24 h
after the cream removal the fluorescence had decreased by
30% for ALA, by 85% for MAL and by 30% for HAL
(Fig. 3c). No visible skin reactions were found after vehicle
cream application.
Influence of drug concentration on protoporphyrin IX
accumulation
We suppose that measured fluorescence is proportional to
PpIX concentration in the upper layers of skin. This fluores-
cence increased with time (1–14 h) for all drugs studied
(Fig. 4), and at prolonged application times (14–24 h) the
PpIX fluorescence had similar profiles (Fig. 4).
The accumulation of PpIX after topical application of ALA
and HAL showed saturation kinetics (Fig. 4a,c). The accumu-
lation of PpIX by MAL was delayed at low concentrations
(Fig. 4b) and seemed to reach saturation at higher concentra-
tions than those of ALA and HAL. Higher concentrations than
20% were not studied, because they increased the fluidity of
the cream.
The fit parameter (C1/2) was calculated using Equation 1.
Half of the maximal PpIX fluorescence was achieved at much
lower concentrations using ALA and HAL than MAL (Fig. 5a).
Concentrations inducing half of the maximal PpIX fluorescence
were around 1Æ5 ± 0Æ2% for ALA (0Æ09 ± 0Æ02 mmol g)1)
(a)
(b)
(c)
Fig 2. Kinetics of protoporphyrin IX (PpIX) fluorescence at 636 nm
during topical application of 5-aminolaevulinic acid (ALA), methyl 5-
aminolaevulinate (MAL) and hexyl 5-aminolaevulinate (HAL) at
different concentrations: (a) 0Æ2%, (b) 2% and (c) 20%. Results are
shown as mean ± SEM; rel. u., relative units. Inset: the fluorescence
emission spectrum (corrected for the spectral sensitivity of the
luminescence spectrometer) of PpIX recorded in human skin. Only
one fluorescence spectrum is shown because the spectral shape was
identical in all cases.
(a)
(b)
(c)
Fig 3. Set of application areas on the upper arm of a volunteer used
for 20% hexyl 5-aminolaevulinate (HAL), 20% methyl 5-
aminolaevulinate (MAL), 20% 5-aminolaevulinic acid (ALA) and
vehicle cream only (a). Fluorescence images of the same patch area
after 12 h topical application (b) and after 24 h following cream
removal (c).
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
794 Topical ALA and its esters on human skin, A. Juzeniene et al.
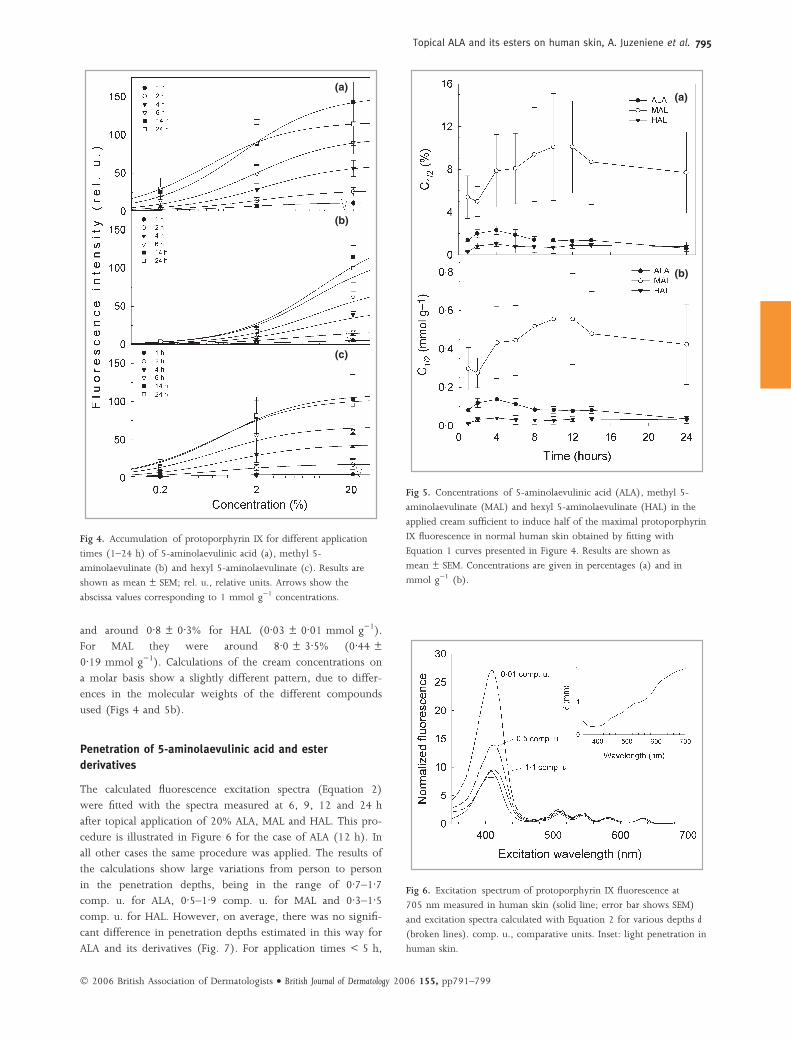
and around 0Æ8 ± 0Æ3% for HAL (0Æ03 ± 0Æ01 mmol g)1).
For MAL they were around 8Æ0 ± 3Æ5% (0Æ44 ±
0Æ19 mmol g)1). Calculations of the cream concentrations on
a molar basis show a slightly different pattern, due to differ-
ences in the molecular weights of the different compounds
used (Figs 4 and 5b).
Penetration of 5-aminolaevulinic acid and ester
derivatives
The calculated fluorescence excitation spectra (Equation 2)
were fitted with the spectra measured at 6, 9, 12 and 24 h
after topical application of 20% ALA, MAL and HAL. This pro-
cedure is illustrated in Figure 6 for the case of ALA (12 h). In
all other cases the same procedure was applied. The results of
the calculations show large variations from person to person
in the penetration depths, being in the range of 0Æ7–1Æ7comp. u. for ALA, 0Æ5–1Æ9 comp. u. for MAL and 0Æ3–1Æ5comp. u. for HAL. However, on average, there was no signifi-
cant difference in penetration depths estimated in this way for
ALA and its derivatives (Fig. 7). For application times < 5 h,
(a)
(b)
(c)
Fig 4. Accumulation of protoporphyrin IX for different application
times (1–24 h) of 5-aminolaevulinic acid (a), methyl 5-
aminolaevulinate (b) and hexyl 5-aminolaevulinate (c). Results are
shown as mean ± SEM; rel. u., relative units. Arrows show the
abscissa values corresponding to 1 mmol g)1 concentrations.
(a)
(b)
Fig 5. Concentrations of 5-aminolaevulinic acid (ALA), methyl 5-
aminolaevulinate (MAL) and hexyl 5-aminolaevulinate (HAL) in the
applied cream sufficient to induce half of the maximal protoporphyrin
IX fluorescence in normal human skin obtained by fitting with
Equation 1 curves presented in Figure 4. Results are shown as
mean ± SEM. Concentrations are given in percentages (a) and in
mmol g)1 (b).
Fig 6. Excitation spectrum of protoporphyrin IX fluorescence at
705 nm measured in human skin (solid line; error bar shows SEM)
and excitation spectra calculated with Equation 2 for various depths d
(broken lines). comp. u., comparative units. Inset: light penetration in
human skin.
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
Topical ALA and its esters on human skin, A. Juzeniene et al. 795

the fluorescence intensity at 705 nm was low and the excita-
tion spectra were noisy, with only the Soret band distinct.
According to Equation 2, this leads to high values of the ratio
F408/F633, and, in turn, low penetration values (d < 0Æ5 comp.
u.) are estimated for t < 5 h.
The spectral shape of the calculated spectrum differs slightly
from the measured spectrum (Fig. 6); the difference may be
due to different environments in cells in vitro and in human
skin in vivo, to different conditions (cuvette vs. fibre probe)
used to record these spectra and to differences in PpIX aggre-
gation. The fit is mainly weighted by the ratio of the Soret
peak (408 nm) to the long wavelength peak (633 nm), which
is practically independent of the spectral shape in this case.
Discussion
Topical ALA-PDT has been used to treat different skin
neoplasms.22–36 However, the limited penetration depth of
topically applied ALA is a major problem16,37,38 resulting in
low cure rates, particularly for nodular and thick tumours.10,11
The distribution of ALA in skin is dependent on many param-
eters such as drug penetration through the stratum corneum,
diffusion through the epidermis and dermis, drug clearance
rate and conversion of ALA into PpIX.39
ALA derivatives, which are more lipophilic than ALA,17
have been proposed as new PDT drugs under the assumption
that they should penetrate deeper than ALA.18,40 ALA deriva-
tives were found to induce PpIX up to 100-fold more effi-
ciently than ALA in cell cultures in vitro.14,16 So the assumption
is certainly fulfilled for layers as thin as a cell membrane.
However, in animal models ALA derivatives do not induce
widely different amounts of PpIX.41,42 In most cases ALA
esters induced similar or slightly higher PpIX levels compared
with ALA18 in normal mouse skin,42–44 while in humans the
opposite result was found.45,46 The structures of the hair folli-
cles and of the stratum corneum in mouse skin differ from
those in human skin.47,48 These differences may influence
drug penetration route and ability to penetrate the stratum
corneum and produce endogenous porphyrins. Therefore, the
permeation of ALA and its ester across the stratum corneum
and following porphyrin production in the mouse model will
not always be the same as in human skin.
ALA was the most efficient at inducing PpIX in normal
human skin (Fig. 2). This is in agreement with the data of
Fritsch et al.45 and Wiegell et al.46 Considerably higher doses of
MAL must be applied to achieve the same effect (Figs 2, 4
and 5). HAL at 20% gave lower PpIX fluorescence than ALA
and MAL because it had a lower viscosity and was distributed
over a larger area compared with ALA and MAL (Fig. 3b).
Accumulation of PpIX after topical application of ALA and
HAL followed saturation kinetics (Fig. 2). However, higher
concentrations of MAL (> 20%) were not tested. It seems that
MAL has to overcome a concentration threshold before it can
induce significant amounts of PpIX in normal human skin
(Fig. 4). Some ALA derivatives were found to induce higher
amounts of PpIX than ALA in human cancers in vivo.49,50 Expo-
sure of rat skin explants to ALA, MAL and HAL41 led to almost
similar PpIX levels, as we found in human skin (Fig. 4). The
use of MAL, rather than that of ALA, preferentially enriched
solar keratoses with porphyrins, although lower porphyrin
levels were found after application of MAL as compared with
ALA.45 Topical application of ALA or its esters on human skin
probably does not induce any systemic action in contrast to
what was observed for ALA in mice,19,42 as the fluorescence
was located in the areas of cream application. This is most
likely to be because a large area relative to the body mass was
used in the case of mice, whereas a very small area relative to
the body mass was employed in the human situation.
The stratum corneum is three to five orders of magnitude
less permeable than the dermis.51 The thickness of the stratum
corneum (10–50 lm), epidermis (50–100 lm) and the entire
dermis (2000 lm) varies greatly from person to person and
from one location to another in the same person.51 There are
large differences in the rates of penetration of different
Fig 7. Apparent penetration depths, as determined by fluorescence
excitation spectroscopy. Error bars show SEM; comp. u., comparative
units. ALA, 5-aminolaevulinic acid; MAL, methyl 5-aminolaevulinate;
HAL, hexyl 5-aminolaevulinate.
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
796 Topical ALA and its esters on human skin, A. Juzeniene et al.

substances.52 From such facts and from our experimental data
it is clear that the stratum corneum of normal human skin is
the main barrier for topically applied ALA and its derivatives,
especially for low concentrations (0Æ2%) of MAL (Figs 2 and
4). Fluorescence excitation spectroscopy indicates that ALA
and its derivatives penetrate down to similar depths after 6 h
of topical application (Fig. 7). The depth remains nearly con-
stant up to 12 h. The constant presence of PpIX after cream
removal (Fig. 7) indicates bioavailability of ALA and its deriv-
atives in the skin. This ‘reservoir effect’ has been observed
after topical application, and the drug reservoirs seem to be
located mainly in the stratum corneum.52 Spectroscopic deter-
minations of the penetration are in reasonable agreement with
data obtained by other methods. ALA, being a small hydrophi-
lic molecule, might be expected to penetrate about 3 mm after
3–15 h of topical application.53 Application times of more
than 4 h seem to be necessary for penetration down into thick
tumours.37 Martin et al.38 found that after topical application
of ALA on nodular basal cell carcinomas the fluorescence of
PpIX was distributed through the whole thickness in thinner
tumours (0Æ42 mm), while in thicker tumours (1Æ25 mm)
fluorescence was seen only in upper layers. Fluorescence micro-
scopy shows that the penetration depth of ALA in basal cell
carcinoma is around 1–2 mm.54 The application of 16% MAL
for 3 h can induce porphyrin formation throughout the depth
of thick basal cell carcinoma lesions up to 2 mm with high
selectivity.55 The number of publications related to ALA and
its esters has steadily been increasing during the last decade.
However, hardly any attempts have been made to compare
these compounds systematically in vivo.
ALA and MAL induced more homogeneous PpIX distribu-
tion after 12 h application compared with HAL (Fig. 3b). Fur-
thermore, at the same time we found higher fluorescence of
PpIX by fluorescence measurements after ALA and MAL appli-
cation than after HAL. Small spots with enhanced PpIX fluores-
cence (probably from hair follicles56 or sebaceous glands57)
were seen after HAL application. After topical application of
ALA on human skin, high levels of PpIX fluorescence were
found in the epidermis, with little PpIX in the dermis, cutane-
ous musculature and vasculature.38 The hair follicles and seba-
ceous glands are localized relatively deep in human skin.
Therefore, the fraction of the PpIX fluorescence around the
hair follicles and sebaceous glands measured at the skin sur-
face is considerably less than the fraction of the fluorescence
measured from the epidermis.
The esters have generally been reported to give a more
homogeneous PpIX distribution than ALA.58 Gerscher et al.59
found more homogeneous tissue distribution of PpIX with
ALA-n-pentyl ester than with ALA in healthy human skin. At
the same time they found greater phototoxicity with ALA-n-
pentyl ester than with ALA but no difference in surface-detec-
ted PpIX levels and no difference in depth of PpIX production
induced by these compounds. This implies that the distribu-
tion of PpIX in skin is important.
ALA-, MAL- and HAL-induced PpIX fluorescence shows
large variability among different volunteers (Fig. 2). This may
be related to different skin thickness of different volunteers.
Human skin exposed frequently to solar radiation produces
less PpIX than skin exposed more rarely to the sun.60 Ultravi-
olet radiation introduces persistent changes in the skin, cer-
tainly relevant in view of its capability to produce PpIX from
ALA. Thickening of the stratum corneum and the viable epi-
dermis after sun exposure61 may be one of the reasons for
this. Experiments show that the stratum corneum acts as a bar-
rier for ALA and its esters: use of penetration enhancer or tape
stripping enhanced PpIX production after ALA and HAL appli-
cation in normal mouse skin.62 Higher fluorescence of PpIX
from ALA, MAL and HAL was recorded for volunteers with
light skin than for those with visually darker skin.
In conclusion, topical application to normal human skin of
creams containing ALA, MAL and HAL induced production of
PpIX with some pharmacokinetic differences. Detectable PpIX
fluorescence appears 1–2 h after application. From the present
data the following practical conclusions can be drawn, relevant
for dosimetry in normal human skin: half of the maximal
amount of PpIX is achieved already at concentrations of the
order of 2% (0Æ12 mmol g)1) for ALA, 8% (0Æ44 mmol g)1)
for MAL and 1% (0Æ04 mmol g)1) for HAL. On average, as
estimated by fluorescence excitation spectroscopy, there is no
significant difference in the penetration depths of ALA and its
derivatives in normal skin.
Acknowledgments
The present work was supported by the Research Foundation
of the Norwegian Radium Hospital and by the Norwegian
Cancer Society (Kreftforeningen).
References
1 Dougherty TJ, Gomer CJ, Henderson BW et al. Photodynamic ther-apy. J Natl Cancer Inst 1998; 90:889–905.
2 Pottier R, Truscott TG. The photochemistry of haematoporphyrinand related systems. Int J Radiat Biol Relat Stud Phys Chem Med 1986;
50:421–52.3 Sanderson DR, Fontana RS, Lipson RL et al. Hematoporphyrin as a
diagnostic tool. A preliminary report of new techniques. Cancer1972; 30:1368–72.
4 Andersson PS, Montan S, Persson T et al. Fluorescence endoscopyinstrumentation for improved tissue characterization. Med Phys
1987; 14:633–6.5 Svanberg K, af Klinteberg C, Nilsson A et al. Laser-based spectro-
scopic methods in tissue characterization. Ann NY Acad Sci 1998;838:123–9.
6 Malik Z, Lugaci H. Destruction of erythroleukaemic cells by photo-activation of endogenous porphyrins. Br J Cancer 1987; 56:589–95.
7 Qian P, Evensen JF, Rimington C, Moan J. A comparison of differ-ent photosensitizing dyes with respect to uptake C3H-tumors and
tissues of mice. Cancer Lett 1987; 36:1–10.8 Kennedy JC, Pottier RH, Pross DC. Photodynamic therapy with
endogenous protoporphyrin IX: basic principles and present clin-ical experience. J Photochem Photobiol B 1990; 6:143–8.
9 Charlesworth P, Truscott TG. The use of 5-aminolevulinic acid(ALA) in photodynamic therapy (PDT). J Photochem Photobiol B 1993;
18:99–100.
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
Topical ALA and its esters on human skin, A. Juzeniene et al. 797

10 Peng Q, Berg K, Moan J et al. 5-Aminolevulinic acid-based photo-dynamic therapy: principles and experimental research. Photochem
Photobiol 1997; 65:235–51.11 Peng Q, Warloe T, Berg K et al. 5-Aminolevulinic acid-based photo-
dynamic therapy. Clinical research and future challenges. Cancer1997; 79:2282–308.
12 Kennedy JC, Marcus SL, Pottier RH. Photodynamic therapy (PDT)and photodiagnosis (PD) using endogenous photosensitization
induced by 5-aminolevulinic acid (ALA): mechanisms and clinicalresults. J Clin Laser Med Surg 1996; 14:289–304.
13 Wolf P, Rieger E, Kerl H. Topical photodynamic therapy with
endogenous porphyrins after application of 5-aminolevulinic acid.An alternative treatment modality for solar keratoses, superficial
squamous cell carcinomas, and basal cell carcinomas? J Am Acad Der-matol 1993; 28:17–21.
14 Gaullier JM, Berg K, Peng Q et al. Use of 5-aminolevulinic acidesters to improve photodynamic therapy on cells in culture. Cancer
Res 1997; 57:1481–6.15 Washbrook R, Riley PA. Comparison of delta-aminolaevulinic acid
and its methyl ester as an inducer of porphyrin synthesis in cul-tured cells. Br J Cancer 1997; 75:1417–20.
16 Kloek J, Akkermans W, Beijersbergen van Henegouwen GM. Deriva-tives of 5-aminolevulinic acid for photodynamic therapy: enzymatic
conversion into protoporphyrin. Photochem Photobiol 1998; 67:150–4.17 Uehlinger P, Zellweger M, Wagnieres G et al. 5-Aminolevulinic
acid and its derivatives: physical chemical properties and proto-porphyrin IX formation in cultured cells. J Photochem Photobiol B
2000; 54:72–80.18 Peng Q, Moan J, Warloe T et al. Build-up of esterified aminolevuli-
nic-acid-derivative-induced porphyrin fluorescence in normalmouse skin. J Photochem Photobiol B 1996; 34:95–6.
19 Moan J, Ma LW, Iani V. On the pharmacokinetics of topicallyapplied 5-aminolevulinic acid and two of its esters. Int J Cancer
2001; 92:139–43.20 Moan J, Peng Q, Sorensen R et al. The biophysical foundations of
photodynamic therapy. Endoscopy 1998; 30:387–91.21 Juzenas P, Juzeniene A, Kaalhus O et al. Noninvasive fluorescence
excitation spectroscopy during application of 5-aminolevulinic acidin vivo. Photochem Photobiol Sci 2002; 1:745–8.
22 Cairnduff F, Stringer MR, Hudson EJ et al. Superficial photodynamictherapy with topical 5-aminolaevulinic acid for superficial primary
and secondary skin cancer. Br J Cancer 1994; 69:605–8.23 Wolf P, Kerl H. Photodynamic therapy with 5-aminolevulinic acid:
a promising concept for the treatment of cutaneous tumors. Derma-
tology 1995; 190:183–5.24 Szeimies RM, Karrer S, Sauerwald A et al. Photodynamic therapy
with topical application of 5-aminolevulinic acid in the treatmentof actinic keratoses: an initial clinical study. Dermatology 1996;
192:246–51.25 Hurlimann AF, Hanggi G, Panizzon RG. Photodynamic therapy of
superficial basal cell carcinomas using topical 5-aminolevulinic acidin a nanocolloid lotion. Dermatology 1998; 197:248–54.
26 Hongcharu W, Taylor CR, Chang Y et al. Topical ALA-photodynam-ic therapy for the treatment of acne vulgaris. J Invest Dermatol 2000;
115:183–92.27 Lang K, Lehmann P, Bolsen K et al. Aminolevulinic acid: pharmaco-
logical profile and clinical indication. Expert Opin Investig Drugs 2001;10:1139–56.
28 Kelty CJ, Brown NJ, Reed MW et al. The use of 5-aminolaevulinicacid as a photosensitiser in photodynamic therapy and photodiag-
nosis. Photochem Photobiol Sci 2002; 1:158–68.29 Szeimies RM, Landthaler M, Karrer S. Non-oncologic indications
for ALA-PDT. J Dermatolog Treat 2002; 13(Suppl. 1):S13–18.
30 Szeimies RM, Landthaler M. Photodynamic therapy and fluores-cence diagnosis of skin cancers. Recent Results Cancer Res 2002;
160:240–5.31 Morton CA. The emerging role of 5-ALA-PDT in dermatology: is
PDT superior to standard treatments? J Dermatolog Treat 2002; 13(Suppl. 1):S25–9.
32 Jeffes EW. Levulan: the first approved topical photosensitizer forthe treatment of actinic keratosis. J Dermatolog Treat 2002; 13 (Suppl.
1):S19–23.33 Taylor EL, Brown SB. The advantages of aminolevulinic acid photo-
dynamic therapy in dermatology. J Dermatolog Treat 2002; 13 (Suppl.
1):S3–11.34 Ibbotson SH. Topical 5-aminolaevulinic acid photodynamic therapy
for the treatment of skin conditions other than non-melanoma skincancer. Br J Dermatol 2002; 146:178–88.
35 Zeitouni NC, Oseroff AR, Shieh S. Photodynamic therapy for non-melanoma skin cancers. Current review and update. Mol Immunol
2003; 39:1133–6.36 Lopez RF, Lange N, Guy R et al. Photodynamic therapy of skin can-
cer: controlled drug delivery of 5-ALA and its esters. Adv Drug DelivRev 2004; 56:77–94.
37 Szeimies RM, Sassy T, Landthaler M. Penetration potency of topicalapplied delta-aminolevulinic acid for photodynamic therapy of
basal cell carcinoma. Photochem Photobiol 1994; 59:73–6.38 Martin A, Tope WD, Grevelink JM et al. Lack of selectivity of proto-
porphyrin IX fluorescence for basal cell carcinoma after topicalapplication of 5-aminolevulinic acid: implications for photodynam-
ic treatment. Arch Dermatol Res 1995; 287:665–74.39 Svaasand LO, Wyss P, Wyss MT et al. Dosimetry model for photo-
dynamic therapy with topically administered photosensitizers. LasersSurg Med 1996; 18:139–49.
40 Kloek J, Beijersbergen van Henegouwen GM. Prodrugs of 5-amino-levulinic acid for photodynamic therapy. Photochem Photobiol 1996;
64:994–1000.41 Casas A, Batlle AM, Butler AR et al. Comparative effect of ALA
derivatives on protoporphyrin IX production in human and rat skinorgan cultures. Br J Cancer 1999; 80:1525–32.
42 Juzeniene A, Juzenas P, Iani V et al. Topical application of 5-amino-levulinic acid and its methylester, hexylester and octylester deriva-
tives: considerations for dosimetry in mouse skin model. PhotochemPhotobiol 2002; 76:329–34.
43 Moan J, Ma LW, Juzeniene A et al. Pharmacology of protoporphy-rin IX in nude mice after application of ALA and ALA esters. Int J
Cancer 2003; 103:132–5.
44 De Rosa FS, Lopez RF, Thomazine JA et al. In vitro metabolismof 5-ALA esters derivatives in hairless mice skin homogenate
and in vivo PpIX accumulation studies. Pharm Res 2004; 21:2247–52.
45 Fritsch C, Homey B, Stahl W et al. Preferential relative porphyrinenrichment in solar keratoses upon topical application of delta-
aminolevulinic acid methylester. Photochem Photobiol 1998; 68:218–21.
46 Wiegell SR, Stender IM, Na R et al. Pain associated with photody-namic therapy using 5-aminolevulinic acid or 5-aminolevulinic
acid methylester on tape-stripped normal skin. Arch Dermatol 2003;139:1173–7.
47 Sato K, Sugibayashi K, Morimoto Y. Species differences inpercutaneous absorption of nicorandil. J Pharm Sci 1991; 80:104–7.
48 Panchagnula R, Stemmer K, Ritschel WA. Animal models for trans-dermal drug delivery. Methods Find Exp Clin Pharmacol 1997; 19:335–
41.49 Lange N, Jichlinski P, Zellweger M et al. Photodetection of early
human bladder cancer based on the fluorescence of 5-amino-
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
798 Topical ALA and its esters on human skin, A. Juzeniene et al.

laevulinic acid hexylester-induced protoporphyrin IX: a pilot study.Br J Cancer 1999; 80:185–93.
50 Marti A, Jichlinski P, Lange N et al. Comparison of aminolevulinicacid and hexylester aminolevulinate induced protoporphyrin IX
distribution in human bladder cancer. J Urol 2003; 170:428–32.51 Shaw JE, Prevo M, Gale R et al. Percutaneous absorption. In: Physiol-
ogy, Biochemistry, and Molecular Biology of the Skin (Goldsmith LA, ed.).New York: Oxford University Press, 1991; 1447–79.
52 Scheuplein RJ, Blank IH. Permeability of the skin. Physiol Rev 1971;51:702–47.
53 Svaasand LO, Tromberg BJ, Wyss P et al. Light and drug distribu-
tion with topically administered photosensitizers. Lasers Med Sci1996; 11:261–5.
54 Peng Q, Warloe T, Moan J et al. Distribution of 5-aminolevulinicacid-induced porphyrins in noduloulcerative basal cell carcinoma.
Photochem Photobiol 1995; 62:906–13.55 Peng Q, Soler AM, Warloe T et al. Selective distribution of porphy-
rins in skin thick basal cell carcinoma after topical application ofmethyl 5-aminolevulinate. J Photochem Photobiol B 2001; 62:140–5.
56 Meijnders PJN, Star WM, de Bruijn HS et al. Clinical results ofphotodynamic therapy for superficial skin malignancies or actinic
keratosis using topical 5-aminolevulinic acid. Lasers Med Sci 1996;11:123–31.
57 Bissonnette R, Shapiro J, Zeng H et al. Topical photodynamic ther-apy with 5-aminolaevulinic acid does not induce hair regrowth in
patients with extensive alopecia areata. Br J Dermatol 2000;143:1032–5.
58 Gerscher S, Connelly JP, Beijersbergen van Henegouwen GM et al.A quantitative assessment of protoporphyrin IX metabolism and
phototoxicity in human skin following dose-controlled delivery ofthe prodrugs 5-aminolaevulinic acid and 5-aminolaevulinic acid-n-
pentylester. Br J Dermatol 2001; 144:983–90.59 Gerscher S, Connelly JP, Griffiths J et al. Comparison of the phar-
macokinetics and phototoxicity of protoporphyrin IX metabolized
from 5-aminolevulinic acid and two derivatives in human skin invivo. Photochem Photobiol 2000; 72:569–74.
60 von Beckerath M, Juzenas P, Ma LW et al. The influence of UVexposure on 5-aminolevulinic acid-induced protoporphyrin IX pro-
duction in skin. Photochem Photobiol 2001; 74:825–8.61 Honigsmann H. Erythema and pigmentation. Photodermatol Photoimmu-
nol Photomed 2002; 18:75–81.62 van den Akker JT, Iani V, Star WM et al. Topical application of
5-aminolevulinic acid hexyl ester and 5-aminolevulinic acid tonormal nude mouse skin: differences in protoporphyrin IX fluores-
cence kinetics and the role of the stratum corneum. Photochem Photo-biol 2000; 72:681–9.
� 2006 British Association of Dermatologists • British Journal of Dermatology 2006 155, pp791–799
Topical ALA and its esters on human skin, A. Juzeniene et al. 799


![Crystal structures of N-tert-butyl-3-(4-fluoro-phenyl)-5-oxo-4-[2-(tri-fluoro-meth-oxy)phen-yl]-2,5-di-hydro-furan-2-carboxamide and 4-(2H-1,3-benzodioxol-5-yl)-N-cyclo-hexyl-5-oxo-3-[4-(tri-fluoro-meth-yl)phen-yl]-2,5-di-hydro-furan-2-carboxamide](https://img.pdfslide.net/doc/110x75/6358cb51a90bb46f52088ee9/crystal-structures-of-n-tert-butyl-3-4-fluoro-phenyl-5-oxo-4-2-tri-fluoro-meth-oxyphen-yl-25-di-hydro-furan-2-carboxamide.jpg)


























![[Untitled] (5)](https://img.pdfslide.net/doc/110x75/6344b58638eecfb33a063664/untitled-5.jpg)