Embed Size (px)
Citation preview

Transoral IncisionlessIs It as Safe and Efficacious as a Nissenor Toupet Fundoplication?PAUL TOOMEY, M.D., ANTHONY TETA, B.S., KRLSHEN PATEL, B.S., SHARONA ROSS, M.D., PRASHANT SUKHARAMWALA, M.D., ALEXANDER S. ROSEMURGY, M.D.
From Florida Hospital Tampa, Tampa, Florida
Transoral incisionless fundoplication (TIF) was U.S. Food and Drug Administration-approved in 2007 to treat gastroesophageal reflux disease (GERD), but comparative data are lacking. This study was undertaken to compare outcomes for patients with GERD undergoing TIF versus laparoscopic Nissen or Toupet fundoplications. We undertook a case-controlled study of three cohorts of 20 patients undergoing TIF or laparoscopic Nissen or Toupet fundoplications from 2010 to 2013 controlling for age, body mass index, and preoperative DeMeester scores. All patients were pro spectively followed. Median data are reported. Patients undergoing TIF had significantly shorter operative times (in minutes: 71 vs 119 and 85, respectively, P < 0.001) and length of stay (in days: 1, 2, and 1, respectively, P < 0.001). No matter the approach, patients reported dramatic and similar reduction in symptom frequency and severity (e.g., heartburn 8 to 0, P < 0.05). At follow-up, 83 per cent of patients after TIF, 80 per cent after Nissen, or 92 per cent after Toupet fundoplications had symptoms less than once per month (P = 0.12). TIF leads to dramatic symptom resolution, similar when compared with Nissen or Toupet fundoplications. TIF promotes shorter operative times and lengths of stay. Patient satisfaction and effective palliation of symptoms show that TIF is safe and efficacious in comparison to Nissen and Toupet fundoplications and support its continued ap plication and evaluation.
L a pa r o s c o pic f u n d o pl ic a t io n is the gold standard approach in definitive treatment for patients with
gastroesophageal reflux disease (GERD). One of five Americans experience GERD-related symptoms weekly, and millions of medical office visits per year in the United States are the result of GERD.1-4 The rising incidence of GERD has been the driving force behind the search for a definitive treatment for reflux outside of medical therapy and in that, the rise of endoluminal therapy in treatment.5-10 In 2007, the U.S. Food and Drug Administration approved EsophyX® for transoral incisionless fundoplication (TIF) to treat GERD, but comparative data are lacking.
This novel approach to fundoplication warrants further evaluation in the safety, feasibility, and efficacy in operative therapy for GERD. The salutary benefits of minimally invasive surgery (MIS) are well estab lished in the literature. Those benefits of MIS are
Presented at the Annual Scientific Meeting and Postgraduate Course Program, Southeastern Surgical Congress, Savannah, GA, February 22-25, 2014.
Address correspondence and reprint requests to Alexander S. Rosemurgy M.D., Florida Hospital Tampa, 3000 Medical Park Drive, Suite 310, Tampa, FL 33613. E-mail: [email protected].
evident and further improved when used by TIF given the advantages of no surgical scar and avoiding a transperitoneal approach.11-16 In the early stages of endoluminal therapy using TIF and with short-term postoperative follow-up, patients report similar symp tom resolution and significant improvement in their GERD after TIF when compared with patients un dergoing laparoscopic fundoplication.17-19
This study was undertaken to compare outcomes for patients with GERD undergoing TIF versus laparo- endoscopic single-site (LESS) Nissen or Toupet fun doplications. The specific purpose of our study was to illustrate the postoperative outcomes including symp tom resolution for each operative approach. Our hy pothesis undertaking this study was that there would be dramatic improvement in and no significant differ ences in postoperative outcomes for frequency and severity of symptoms in patients who underwent TIF versus LESS Nissen or Toupet fundoplications.
Methods
The study design and patient data collection were conducted at Florida Hospital Tampa. With Institu tional Review Board approval and informed consent,
860
No. 9 TRANSORAL INCISIONLESS FUNDOPLICATION Toomey et al. 861
we undertook a case-controlled study of three cohorts of 20 patients undergoing TIF or LESS Nissen or Toupet fundoplications from 2010 to 2013 controlling for age, body mass index, and preoperative DeMeester scores. Patients with a hiatal hernia 2 cm or less were eligible to undergo TIF. All patients with giant hiatal hernias were excluded from this study. We eliminated patients undergoing LESS Nissen or Toupet fundo plications before 2010 to control for the known learning curve for optimal results associated with LESS Nissen or Toupet fundoplications.12 Since 2007, we have implemented the LESS approach for all of our laparoscopic fundoplications.
Demographic data were collected preoperatively
prospectively followed to determine the efficacy and functional outcomes of their operations. On each postoperative follow-up, patients scored frequency and severity of their symptoms before and after their re spective TIF, Nissen, or Toupet fundoplication by us ing a Likert scale (0 = never/not bothersome to 10 = always/very bothersome). Frequency and severity of symptoms, including heartburn, dysphagia, regur gitation, coughing, and chest pain, were recorded for each cohort. Data from last follow-up were an alyzed. Data were maintained on a spreadsheet (Excel; M icrosoft‘ , Redmond, WA) and analyzed using GraphPad InStat, Version 3.06 (GraphPad InStat®; GraphPad Software, Inc., San Diego, CA).
for all patients (Table 1) and
Ta b l e 1. Patient Demographic Data
these patients were Where appropriate, data are presented as median
TIF Toupet Nissen P ValueDemographic data
Number of patients 20 20 20 NSGender (men) 7 11 10 NSAge (years) 68 (61 ± 14.7) 67 (64 ± 14.1) 60 (54 ± 14.5) NSBMI (kg/m2) 25 (25 ± 2.3) 26 (26 ± 2.8) 26 (26.2 ± 1.0) NSDuration of symptoms (years) 11 (13 ± 14.0) 13 (16 ± 14) 10 (14 ± 12.9) NSDeMeester score 35 (63 ± 60.6) 35 (36 ± 13.4) 36 (35 ± 12.6) NSHiatal hernia 15% (3/20) 65% (13/20) 55% (11/20) NSReoperative fundoplication 25% (5/20) 5% (1/20) 5% (1/20) NS
Intraoperative courseAdditional incision 0% (0/20) 0% (0/20) 0% (0/20) NSConversion to open 0% (0/20) 0% (0/20) 0% (0/20) NSOperative time (minutes) 71 (71 ± 18.4) 119 (129 ± 29.0) 85 (90 ± 20.0) 0.002Blood loss (cc) 50 (39 ± 26.6) 25 (49 ± 58.8) 50 (160.9 ± 200.6) NS
Postoperative courseComplications 0% (0/20) 10% (2/20) 5% (1/20) NSLength of stay (days) 1 (1 ± 1.1) 2 (3 ± 3.7) 1 (2 ± 1.3) 0.006
TIF, transoral incisionless fundoplication; BMI, body mass index; NS, nonsignificant.
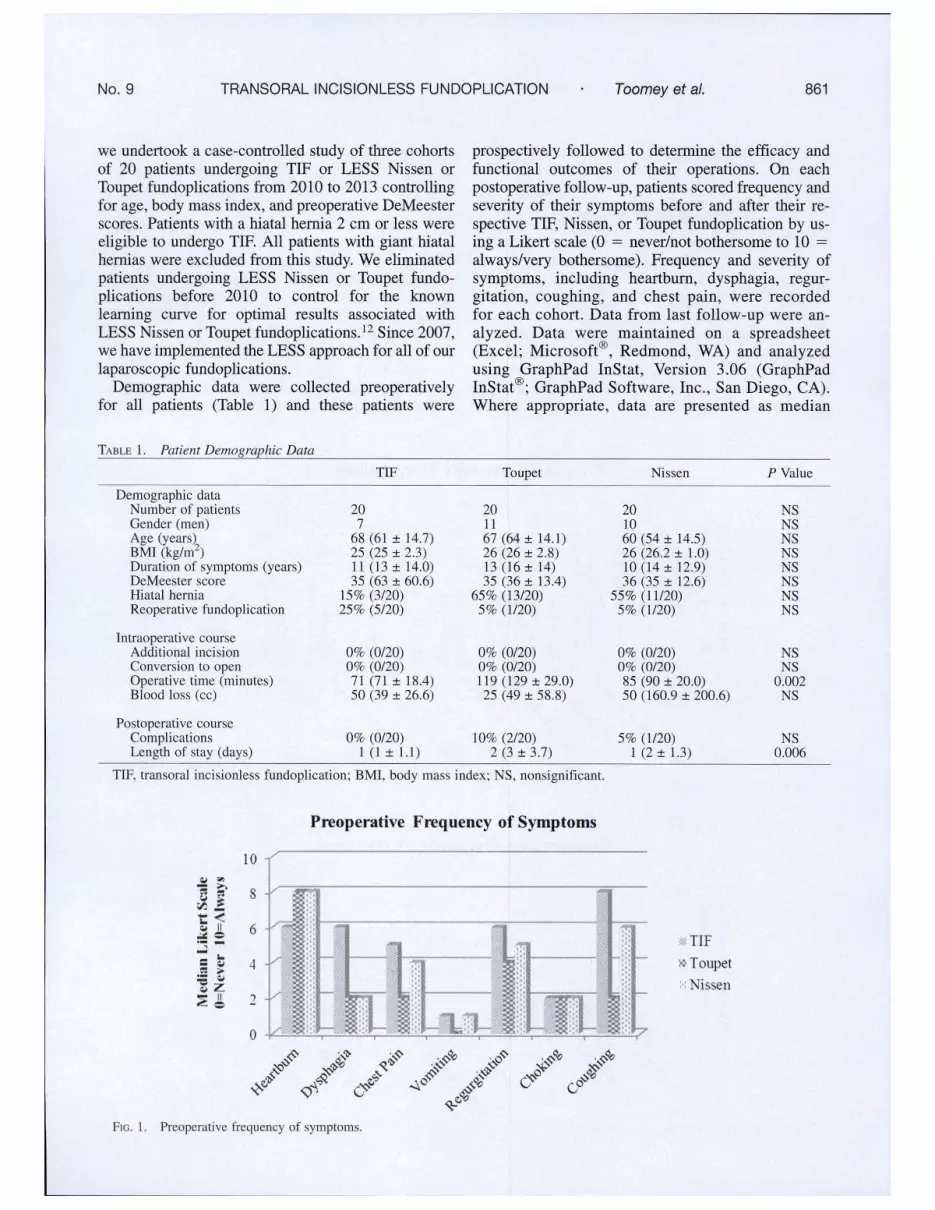
Preoperative Frequency of Symptoms
Fig . 1. Preoperative frequency of symptoms.

862 THE AMERICAN SURGEON Septem ber 2014 Vol. 80
(mean ± standard deviation). Significance was ac cepted with 95 per cent confidence.
Preoperative Evaluation
All patients who are referred for treatment of GERD refractory to or requiring open-ended medical therapy undergo evaluation with an upper gastrointestinal se ries in 15° head down position using a barium-laden bagel and a marshmallow to mimic a normal bolus of food.20 If the patients have more than two stripping motions of the esophagus to clear the bolus of food, then they have esophageal dysmotility. All patients who have esophageal dysmotility undergo a LESS Toupet fundoplication and all patients who have normal
esophageal motility undergo a LESS Nissen fundopli cation. All patients after 2010 were also offered a TIF if they did not have a hiatal hernia greater than 2 cm.
Results
All patients undergoing TIF, Nissen fundoplication, or Toupet fundoplication did not significantly differ regarding age, body mass index, or DeMeester score by design (Table 1). However, patients undergoing TIF were more likely to have undergone prior fun doplication (25, 5, and 5%, respectively; P < 0.01). Preoperatively across all cohorts, patients recorded similar frequency and severity of symptoms (Figs. 1 and 2). Postoperatively across all cohorts, there was
Preoperative Severity of Symptoms
Postoperative Frequency of Symptoms
ssTIF
* T oupet Nissen
Fig . 3. Postoperative frequency of symptoms.
No. 9 TRANSORAL INCISIONLESS FUNDOPLICATION Toom ey e t al. 863
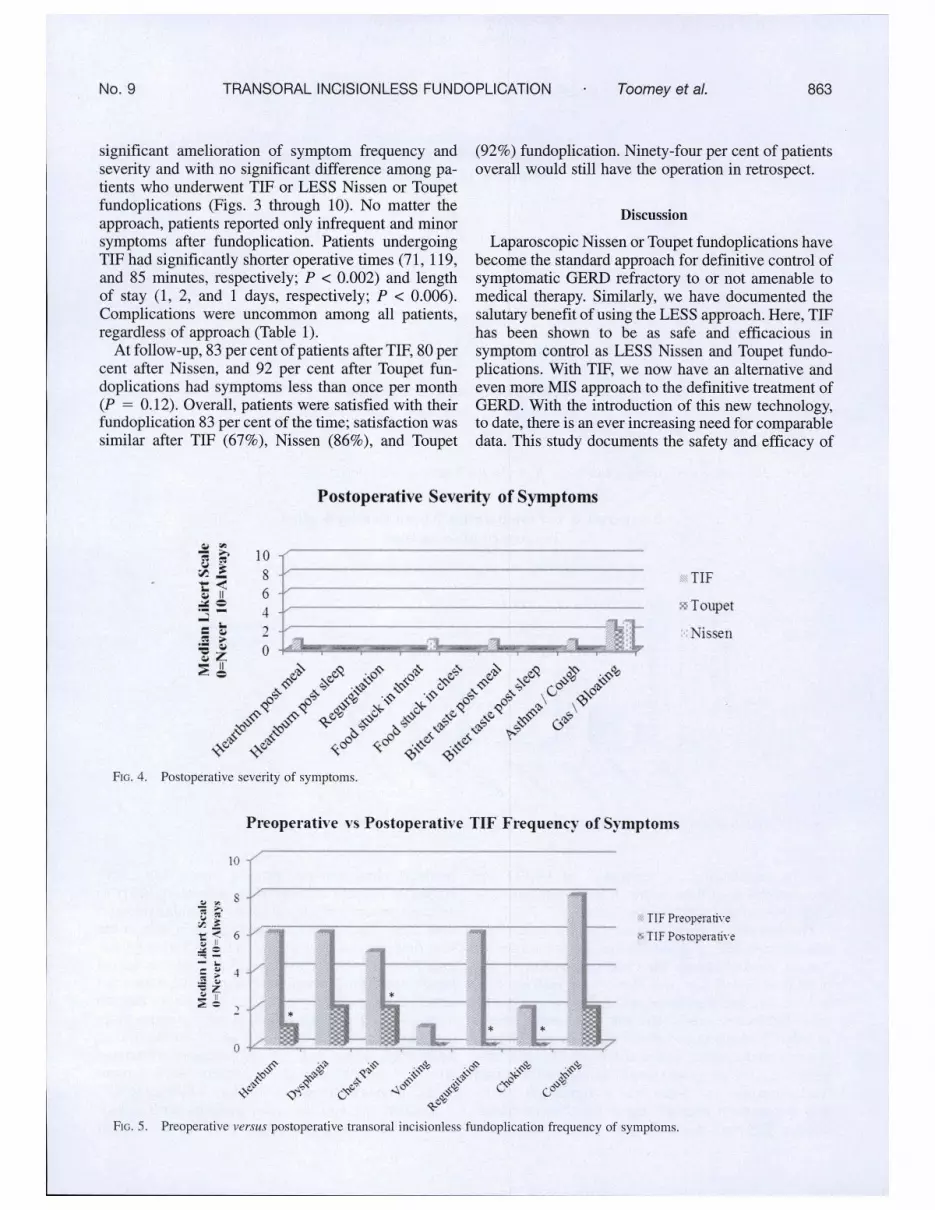
significant amelioration of symptom frequency and severity and with no significant difference among pa tients who underwent TIF or LESS Nissen or Toupet fundoplications (Figs. 3 through 10). No matter the approach, patients reported only infrequent and minor symptoms after fundoplication. Patients undergoing TIF had significantly shorter operative times (71, 119, and 85 minutes, respectively; P < 0.002) and length of stay (1, 2, and 1 days, respectively; P < 0.006). Complications were uncommon among all patients, regardless of approach (Table 1).
At follow-up, 83 per cent of patients after TIF, 80 per cent after Nissen, and 92 per cent after Toupet fun doplications had symptoms less than once per month (P = 0.12). Overall, patients were satisfied with their fundoplication 83 per cent of the time; satisfaction was similar after TIF (67%), Nissen (86%), and Toupet
(92%) fundoplication. Ninety-four per cent of patients overall would still have the operation in retrospect.
Discussion
Laparoscopic Nissen or Toupet fundoplications have become the standard approach for definitive control of symptomatic GERD refractory to or not amenable to medical therapy. Similarly, we have documented the salutary benefit of using the LESS approach. Here, TIF has been shown to be as safe and efficacious in symptom control as LESS Nissen and Toupet fundo plications. With TIF, we now have an alternative and even more MIS approach to the definitive treatment of GERD. With the introduction of this new technology, to date, there is an ever increasing need for comparable data. This study documents the safety and efficacy of
Postoperative Severity of Symptoms
Fig . 4. Postoperative severity of symptoms.
TIF
» Toupet
Nissen
Preoperative vs Postoperative TIF Frequency of Symptoms
Fig . 5.
TIF Preopera rive TIF Postoperative
Preoperative versus postoperative transoral incisionless fundoplication frequency of symptoms.

864 THE AMERICAN SURGEON September 2014 Vol. 80
Preoperative vs Postoperative Toupet Fundoplication Frequency of Symptoms
Fig . 6. Preoperative versus postoperative Toupet fundoplication frequency o f symptoms.
Toupet Preoperative
Sf T oupet Postoperative
Preoperative vs Postoperative Nissen Fundoplication Frequency of Symptoms
F ig . 7. Preoperative versus postoperative Nissen fundoplication frequency o f symptoms.
Nissen Preoperative
a Nissen Postoperative
TIF in ameliorating the symptoms of GERD and documents that in these terms, it is the equivalent of LESS Nissen or Toupet fundoplications.
This is a series of patients undergoing a fundoplica tion through TIF or LESS Nissen fundoplication or Toupet fundoplication. Our patient population was older than middle age, was evenly split between men and women, had significant acid reflux (i.e., very ele vated DeMeester scores), and was of moderate fitness, as judged by body mass index. Patients, independent of therapy undertaken, had similar preoperative fre quency and severity of symptoms of GERD before fundoplications and there was a significant reduc tion in symptoms after all approaches. Patients under going a TIF were more likely to have a prior failed
fundoplication, whereas patients undergoing LESS Nissen or Toupet fundoplications were more likely to have the presence of a hiatal hernia particularly greater than 2 cm. Each of these factors plays a role in the selection process; patients with a hiatal hernia greater than 2 cm are not eligible for TIF and patients failing laparoscopic fundoplication without hiatal hernia are rather ideal candidates for TIF. Not surprisingly, patients undergoing TIF had significantly shorter operative times and length of stay. Blood loss was not notable for all approaches. There were no complications associated with TIF and there were no conversions to laparo scopic or open approaches for patients undergoing TIF.
Medical therapy for most patients with symp toms of GERD is presumptive. With improvement in

No. 9 TRANSORAL INCISIONLESS FUNDOPLICATION Toomey et al. 865
Preoperative vs Postoperative TIF Severity of Symptoms
TIF Preoperative * TIF Postoperative
Fig . 8. Preoperative versus postoperative transoral incisionless fundoplication severity of symptoms.
Preoperative vs Postoperative Toupet Fundoplication Severity of Symptoms
Toupet Preoperative x T oupet Postoperative
Fig . 9. Preoperative versus postoperative Toupet fundoplication severity of symptoms.
symptoms, whether frequency or severity, medical therapy is continued, often “open-ended.” Although there is considerable evidence that this is shortsighted (e.g., cost, osteoporosis, and alkaline reflux), pre sumptive therapy is the backbone of medical therapy, bordering on indiscriminant application. Nonsurgeons have no hesitation in judging the success of medical therapy on the amelioration of symptoms, i.e., symp tom control. Using their yardstick here, we document very impressive symptom control with the three cho sen morbidities, none being better than the other. Furthermore, the achieved symptom control here is not complicated by ongoing cost, osteoporosis, alkaline reflux, and other “side effects” of open-ended medical therapy. As surgeons, we seek objective measures for cessation of reflux such as ambulatory pH monitoring,
but patients after successful control of symptoms through fundoplication are nearly universally non- compliant about follow-up pH monitoring and, in our experience, cannot be convinced, cajoled, or bribed into undergoing such follow-up studies. The follow up pH monitoring we do have is supportive, very supportive.
LESS fundoplication seems to be the best measure to compare TIF because it is the least invasive of the minimally invasive laparoscopic techniques. Our ex perience with LESS fundoplication is notable and supports this contention. Here, it is a testament to the LESS approach that patients of this description (e.g., median DeMeester score of 35 and median duration of symptoms 12 years) noted such remarkable and pro found resolution of symptoms.

866 THE AMERICAN SURGEON September 2014 Vol. 80
Preoperative vs Postoperative Nissen Fundoplication Severityof Symptoms
Fig . 10. Preoperative versus postoperative Nissen fundoplication severity of symptoms.
Nissen Preoperative
« Nissen Postoperative
TIF is a safe and efficacious means of controlling symptoms of GERD.21 TIF may represent a paradigm shift in treatment of GERD, because it leads to similar dramatic symptom resolution when compared with Nissen or Toupet fundoplications with significantly shorter operative times and length of stay. With the introduction of TIF for patients with prior failed lap aroscopic or “open” fundoplications without notable hiatal hernias (i.e., less than 2 cm), we can avoid a reoperative field with this endoluminal approach. Also, patients with a history of gastric or upper abdominal surgery are particularly attractive patients for TIF, again because it avoids a reoperative field. Further more, the very minimally invasive attributes of TIF promise hope for faster recoveries and resumption of normal activities.
Here, we document that the cosmetic and salutary benefits of TIF are applicable for treatment of GERD. Patient satisfaction and effective palliation of symptoms prove that TIF is safe and efficacious in comparison to LESS Nissen and Toupet fundoplications, and we offer strong support for its continued application and evaluation.
REFERENCES1. Sandler RS, Everhart JE, Donowitz M, et al. The burden of
selected digestive diseases in the United States. Gastroenterology 2002;122:1500-11.
2. Dent J, El-Serag HB, Wallander MA, Johansson S. Epide miology of gastro-oesophageal reflux disease; a systematic review. Gut 2005;54:710-7.
3. Peters JH. Laparoscopic treatment of gastroesophageal reflux disease and hiatal hernia. The SAGES Manual. Fundamentals of Laparoscopy, Thoracoscopy, and G1 Endoscopy 2006;2:208-24.
4. Vesper BJ, Altman KW, Elseth KM, et al. Gastroesophageal reflux disease (GERD): is there more to the story? Chem Med Chem 2008;3:552-9.
5. Elakkary E, Duffy A, Roberts K, et al. Recent advances in the surgical treatment of achalasia and gastroesophageal reflux dis ease. J Clin Gastroenterol 2008;42:603-9.
6. Hinder R, Filipi C, Wetscher G, et al. Laparoscopic Nissen fundoplication is an effective treatment for gastroesophageal reflux disease. Ann Surg 1994;220:472-81.
7. Voitk A, Joffe J, Alvarez C, et al. Factors contributing to laparoscopic failure during the learning curve for laparoscopic Nissen fundoplication in a community hospital. Laparoendosc Adv Surg Tech A 1999;9:243-9.
8. Ross SB, Villadolid D, Paul H, et al. Laparoscopic Nissen fundoplication ameliorates symptoms of reflux, especially for pa tients with very abnormal DeMeester scores. Am Surg 2008;74: 635-42.
9. Stroup SP, Bazzi W, Derweesh IH. Training for laparoendo- scopic single-site surgery and natural orifice transluminal endo scopic surgery. BJU Int 2010;106:934-40.
10. Rosemurgy AS, Donn N, Paul H, et al. Gastroesophageal reflux disease. Surg Clin North Am 2011 ;91:1015—29.
11. Ross SB, Gal S, Teta AF, et al. Late results after laparo scopic fundoplication denote durable symptomatic relief of gas troesophageal reflux disease. Am J Surg 2013;206:47-51.
12. Ross SB, Choung E, Teta AF, et al. The learning curve of laparo-endoscopic single site (LESS) fundoplication: definable, short, and safe. JSLS 2013;17:376-84.
13. Rosemurgy A, Villadolid D, Paul H, et al. A single in stitution’s experience and journey with over 1000 laparoscopic fundoplications for GERD. Am Surg 2012;78:917-25.
14. Ross S, Roddenbery A, Luberice K, et al. Laparoendoscopic single site (LESS) vs. conventional laparoscopic fundoplication for GERD: is there a difference. Surg Endosc 2013;27:538- 47.
15. Rakita S, Villadolid D, Thomas A, et al. Laparoscopic Nissen fundoplication offers high patient satisfaction with relief

No. 9 TRANSORAL INCISIONLESS FUNDOPLICATION Toomey et al. 867
of extra-esophageal symptoms of GERD. Am Surg 2006;72: 207-12.
16. Cowgill S, Gillman R, Kraemer E, et al. Ten-year follow-up after laparoscopic Nissen fundoplication for gastroesophageal reflux disease. Am Surg 2007;73:748-52.
17. Cadiere GB, Buset M, Muls V, et al. Antireflux transoral incisionless fundoplication using EsophyX: 12-month results of a prospective multicenter study. World J Surg 2008;32:1676-88.
18. Barnes WE, Hoddinott KM, Mundy S, et al. Transoral incisionless fundoplication offers high patient satisfaction and relief of therapy-resistant typical and atypical symptoms of GERD in community practice. Surg Innov 2001;18:119-29.
19. Demyttenaere SV, Bergman S, Pham T, et al. Transoral incisionless fundoplication for gastroesophageal reflux disease in an unselected patient population. Surg Endosc 2010;24: 854-8.
20. D’Alessio MJ, Rakita S, Bloomston M, et al. Esophagog- raphy predicts favorable outcomes after laparoscopic Nissen fun doplication for patients with esophageal dysmotility. J Am Coll Surg 2005;201:335-42.
21. Wilson EB, Barnes WE, Mavrelis PG, et al. The effects of transoral incisionless fundoplication on chronic GERD patients: 12-month prospective multicenter experience. Surg Laparosc Endosc Percutan Tech 2014;24:26-36.

Copyright of American Surgeon is the property of Southeastern Surgical Congress and itscontent may not be copied or emailed to multiple sites or posted to a listserv without thecopyright holder's express written permission. However, users may print, download, or emailarticles for individual use.






![The Enemy in Assyrian Royal Inscriptions: The 'Moral Judgement'. In: H.J. Nissen, J. Renger (Hrsgg.), Mesopotamien und seine Nachbarn [=XXV Rencontre Assyriologique Internationale,],](https://img.pdfslide.net/doc/110x75/631993d8d4191f2f9307ab63/the-enemy-in-assyrian-royal-inscriptions-the-moral-judgement-in-hj-nissen.jpg)

![[Laparoscopic total fundoplication is not an obstacle to oesophageal emptying after oesophago-gastric myotomy for the surgical treatment of achalasia]](https://img.pdfslide.net/doc/110x75/634a7ed7913672970c089057/laparoscopic-total-fundoplication-is-not-an-obstacle-to-oesophageal-emptying-after.jpg)









