Embed Size (px)
Citation preview
tumor nests appear more mature and have more abun-dant eosinophilic cytoplasm in comparison to cells inthe periphery. The cell-to-cell attachments (intercellu-lar bridges) are well-defined. Keratin pearls (extracel-lular keratin arranged in whorls) are frequent. There isa paucity of compact basaloid cells.
• Grade 2, moderately differentiated squamous cellcarcinoma. A moderately differentiated tumor hasirregular nests and a higher proportion of primitivebasal cells than that in well-differentiated tumors. Thetumor cells, still recognizable as squamous, have lesscytoplasm and form less keratin than those in well-differentiated tumors. Intercellular bridges areretained.
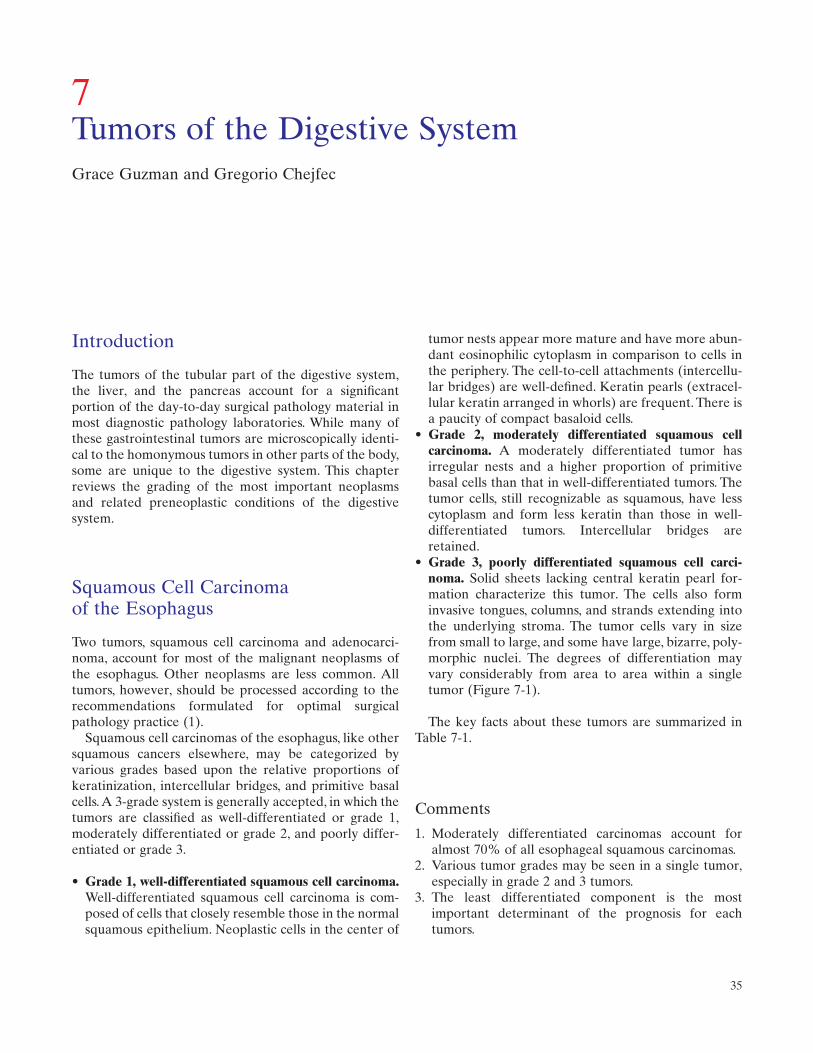
• Grade 3, poorly differentiated squamous cell carci-noma. Solid sheets lacking central keratin pearl for-mation characterize this tumor. The cells also forminvasive tongues, columns, and strands extending intothe underlying stroma. The tumor cells vary in sizefrom small to large, and some have large, bizarre, poly-morphic nuclei. The degrees of differentiation mayvary considerably from area to area within a singletumor (Figure 7-1).
The key facts about these tumors are summarized inTable 7-1.
Comments
1. Moderately differentiated carcinomas account foralmost 70% of all esophageal squamous carcinomas.
2. Various tumor grades may be seen in a single tumor,especially in grade 2 and 3 tumors.
3. The least differentiated component is the most important determinant of the prognosis for eachtumors.
Introduction
The tumors of the tubular part of the digestive system,the liver, and the pancreas account for a significantportion of the day-to-day surgical pathology material inmost diagnostic pathology laboratories. While many ofthese gastrointestinal tumors are microscopically identi-cal to the homonymous tumors in other parts of the body,some are unique to the digestive system. This chapterreviews the grading of the most important neoplasms and related preneoplastic conditions of the digestivesystem.
Squamous Cell Carcinoma of the Esophagus
Two tumors, squamous cell carcinoma and adenocarci-noma, account for most of the malignant neoplasms ofthe esophagus. Other neoplasms are less common. Alltumors, however, should be processed according to therecommendations formulated for optimal surgicalpathology practice (1).
Squamous cell carcinomas of the esophagus, like othersquamous cancers elsewhere, may be categorized byvarious grades based upon the relative proportions ofkeratinization, intercellular bridges, and primitive basalcells.A 3-grade system is generally accepted, in which thetumors are classified as well-differentiated or grade 1,moderately differentiated or grade 2, and poorly differ-entiated or grade 3.
• Grade 1, well-differentiated squamous cell carcinoma.Well-differentiated squamous cell carcinoma is com-posed of cells that closely resemble those in the normalsquamous epithelium. Neoplastic cells in the center of
7Tumors of the Digestive SystemGrace Guzman and Gregorio Chejfec
35
36 G. Guzman and G. Chejfec
Esophageal Adenocarcinoma and Its Precursors
Most adenocarcinomas of the esophagus develop fromthe intestinal epithelium forming the foci of metaplasiain Barrett esophagus. The sequence of events leading tothe progression from normal intestinal epithelium to mildand severe dysplasia and intraepithelial carcinoma can berecognized in biopsy material. As summarized byIacobuzio-Donahue and Montgomery (2005), the diag-nosis is made by analyzing the following 4 aspects ofthese lesions: surface maturation, architecture, cytologicfeatures, and inflammation and erosion of the epithelium(Figure 7-2).
• Surface maturation. In nondysplastic lesions, the basalglands of Barrett esophagus have larger nuclei thanthat in the surface epithelium.The nuclei on the surfacetend to appear elongated and slim, and are located inthe basal portion of the cytoplasm positioned perpen-dicularly to the basement membrane.
• Architecture. The nondysplastic lesions contain well-developed stroma surrounding the glands, which are of
uniform shape and regularly distributed. Architecturalabnormalities include crowding, back-to-back arrange-ment, cribriform glands, cystic dilatation, and necroticdebris.
• Cytologic features. Minor nuclear changes, such asnuclear enlargement and atypia, are part of intestinalmetaplasia and are to be expected in the basal glandsof Barrett esophagus. Significant dysplasia is charac-terized by an obvious enlargement of the nuclei, whichbecome hyperchromatic, lose their polarity, and arearranged at random.
• Inflammation and erosion. Barrett esophagus is proneto inflammation that is often associated with surfaceerosions. Inflammation and regeneration of the epithe-lium may mask the neoplastic changes, but also maycause architectural distortion and nuclear changes thatshould not be confused with neoplastic atypia.
According to a consensus of gastrointestinal patholo-gists (see Iacobuzio-Donahue and Montgomery, 2005),esophageal biopsies containing the typical features ofBarrett esophagus should be reported under 4 headings,as follows:
• Barrett esophagus, negative for dysplasia. In thislesion, there is appropriate surface maturation, and theglands are of uniform shape and enclosed in well-developed stroma. The nuclei have smooth contoursand are polarized and located in the basal part of thewell-developed cytoplasm. Nucleoli are not prominent.The cells contain and/or secrete mucin, albeit somemucin loss may be evident focally. Inflammation couldinduce reactive changes.
• Barrett esophagus, indefinite for dysplasia. The epithe-lium of this lesion shows good surface maturation,and there are only minor architectural abnormalities,such as the focal crowding of glands. The nuclei of basal glands show some hyperchromasia and slightirregularity of contour. Loss of nuclear polarity is notevident. Mitoses may be increased in the basal glands.
• Barrett esophagus, low-grade dysplasia. The surfaceepithelium of this lesion resembles the basal glandsand shows only slight maturation. The glands arecrowded, but still separated by connective tissue
Figure 7-1. Squamous cell carcinoma of the esophagus. Poorlydifferentiated squamous cells show signs of focal keratinization.
Table 7-1. Microscopic grading of esophageal squamous cell carcinoma.
Degree of differentiation
Features Well differentiated Moderately differentiated Poorly differentiated
Resemblance to normal epithelium High resemblance Still recognizable as squamous Hardly recognizable as squamousKeratin pearl formation Frequent Rare to none NonePredominant cell population Mature squamous More basaloid, some squamous UndifferentiatedIntercellular bridges Distinct Focally retained Rare or none
7. Tumors of the Digestive System 37
A
C
B
D
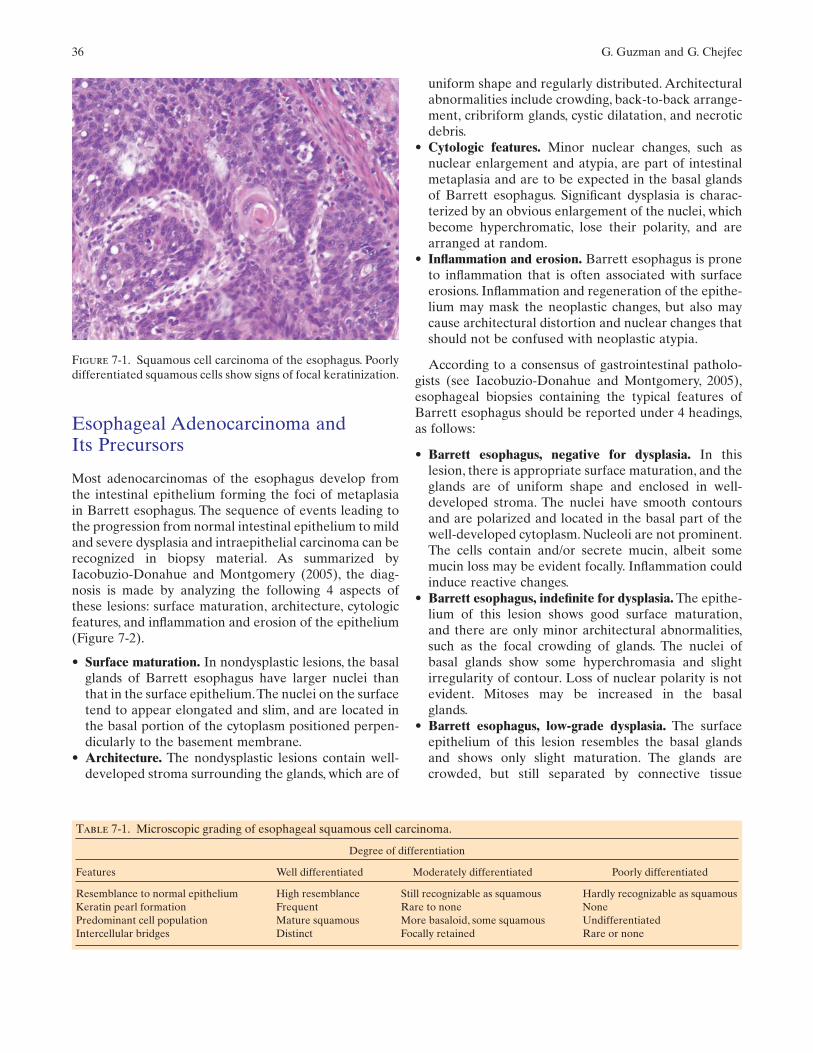
Figure 7-2. Barrett esophagus, with and without dysplasia. A.Barrett esophagus, indefinite for dysplasia. The surface epithe-lium reveals mild stratification of the nuclei and a depletion ofmucus. There is no evidence of nuclear atypia. B. Barrett esoph-agus, low-grade dysplasia. At low magnification, it is possible toappreciate the complex branching pattern of the glands thatappear crowded and irregular. However, the surface epitheliumstill shows regular stratification of the nuclei, which do not
appear hyperchromatic and do not show severe atypia. C.Barrett esophagus, low-grade dysplasia. At higher magnifica-tion, the surface epithelium is lined by cells that have stratifiednuclei with only mild atypia and hyperchromasia. D. Barrettesophagus, high-grade dysplasia. There is marked architecturaldisarray, and the glands are arranged back to back. The surfaceepithelium shows loss of nuclear polarity and hyperchromasiaof vesicular and irregularly shaped nuclei.
stroma. The nuclei show hyperchromasia with chro-matin clumping. The nuclei are still elongated, andeven though they may have slightly irregular contours,they are still polarized. Nuclear stratification resem-bling the changes in tubular adenomas of the colonmay extend all the way to the surface of the lesions.Nucleoli may be seen, but are not prominent.
• Barrett esophagus, high-grade dysplasia. Loss ofsurface maturation is the most important feature of thislesion. The glands appear crowded in the surface andbasal parts of the epithelium, and the stroma is barelyevident. The nuclei are often markedly enlarged andhyperchromatic. The chromatin is often clumped, andthe nucleoli may be prominent. Nuclei have irregular
38 G. Guzman and G. Chejfec
contours, and there is obvious loss of nuclear polarity,which characteristically extends all the way to thesurface of the lesions. Mitoses are prominent and maybe seen in any part of the lesion. Typically, there is noor only minimal inflammation.
For intramucosal adenocarcinoma, the transition fromdysplasia to carcinoma is gradual and is marked by subtlemicroscopic changes. Accordingly, Barrett esophaguswith high-grade dysplasia may be difficult to separatefrom intramucosal carcinoma. These changes includeextensive back-to-back growth of glands with a completeloss of intervening stroma, a syncytial growth pattern, andthe separation of single cells lying freely in the stroma.Desmoplastic reaction is seen only after the intramucosalcarcinoma invades the submucosa (Iacobuzio-Donahueand Montgomery, 2005).
Invasive esophageal adenocarcinomas are best gradedusing the guidelines of the American Joint Committee onCancer (AJCC).According to this system, the tumors aregraded by the proportion of fully formed glands seen inmicroscopic slides and classified as well-differentiated,moderately differentiated, and poorly differentiated
(Figure 7-3). The key facts about these tumors are sum-marized in Table 7-2.
• Well-differentiated carcinoma. This tumor containsglands with open lumina in more than 95% of the totalmass. The glands maybe regularly shaped, cystic, ortubular. The tumor cells are cuboidal or columnar. Thenuclei are vesicular, with a coarse chromatin patternand variable amount of eosinophilic or clear cytoplasm.
• Moderately differentiated carcinoma. This tumorforms glands in 50% to 95% of its mass.The tumor cellsin nonglandular areas maybe arranged in irregularclusters or solid nests. The glandular regions show crib-riform formation and extensive nuclear stratification.
• Poorly differentiated carcinoma. This tumor formsglands in 5% to 50% of its mass. Most of the cells arearranged into solid nests and invasive cords and sheets.Single cells invading the adjacent tissue also are found.The glands, if present, range from poorly formed to infiltrating the normal tissue and evoking an exten-sive desmoplastic fibrosis. The cells show considerablepleomorphisms and may assume signet ring-like features.
Comments
1. Various grades may be observed within a single tumor.If there is variation of histologic grade in the sametumor, the highest grade is designated to the tumor.
2. The majority of the tumors are moderately differenti-ated.
3. In early esophageal carcinoma, the histopathologictype (adenocarcinoma vs. squamous cell carcinoma) isan important independent prognostic factor.
4. Patients with early squamous cell carcinoma have ahigher recurrence rate and are more often found tohave a second primary tumor (2).
5. The depth of invasion in the esophageal wall andregional lymph node involvement were independentprognostic factors in the prognosis of patients withadenocarcinoma arising in Barrett esophagus (3,4).
6. The gross appearance and histologic differentiationwere not found to impact prognosis.
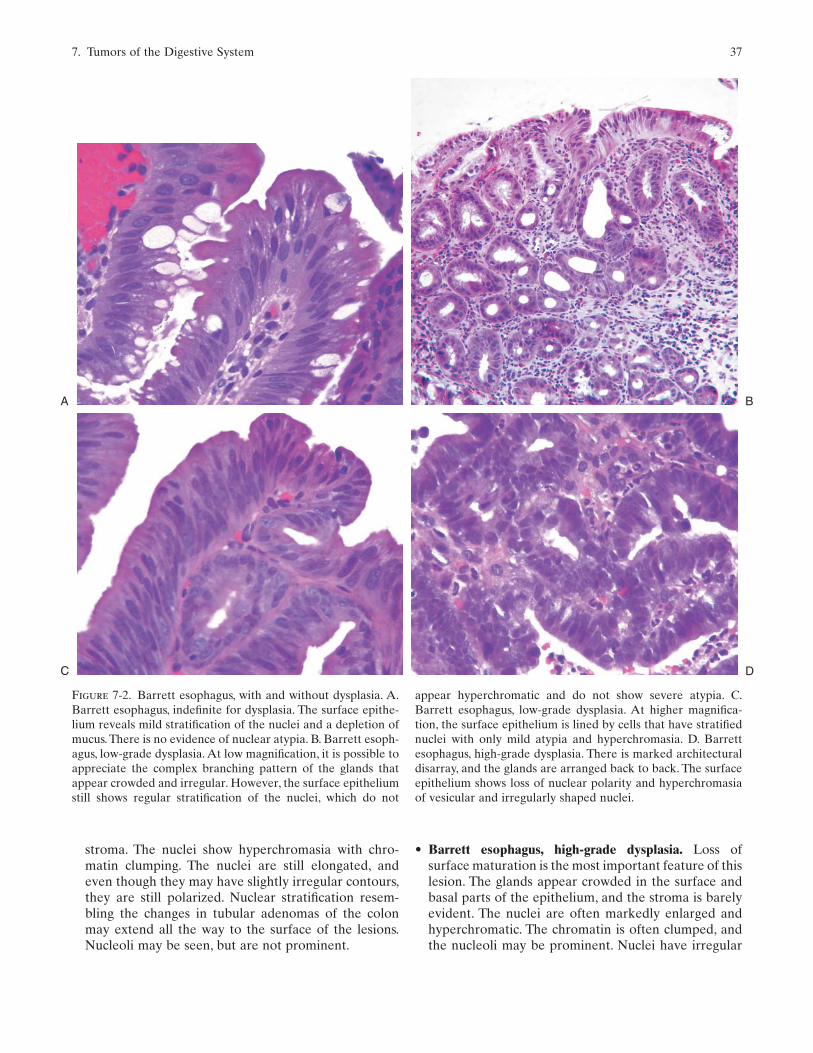
Figure 7-3. Adenocarcinoma of the esophagus.Atypical hyper-chromatic cells form gland-like structures embedded in the con-nective tissue stroma.
Table 7-2. Features of adenocarcinoma of the esophagus.
Degree of differentiation Extent of glandular Appearance of glandular areas Nonglandular differentiation areas
Well-differentiated 95 Cystic Minimal to none Tubular
Moderately differentiated 50–95 Irregular glands Solid or cribriformPoorly differentiated 5–50 Narrow or cords Solid sheets
Signet-ring cell Desmoplasia
7. Tumors of the Digestive System 39
Gastric Adenocarcinoma
Adenocarcinoma is the most common malignant tumorof the stomach (Lewin and Appelman, 1996). Severalsystems have been proposed for classifying and gradingthese tumors. These classifications are known epony-mously as the Ming (5), Lauren (6), and Goseki (7) classifications.
The Ming classification of gastric carcinomas is basedon the pattern of tumor growth and infiltration (5).This 2-tiered classification divides gastric tumors into those thatshow an expansile pattern of growth, and those with aninfiltrative growth pattern. The expansile growth patterncomprises about three-quarters of gastric carcinomas.These are well-differentiated intestinal-type adenocarci-nomas with good prognosis. They are characterized bywell-formed tubular glands with a clear-cut demarcationof infiltration between the tumor and the surroundinguninvolved stroma. On the other hand, the infiltrativetype of carcinoma is more aggressive, characterized bytumor cells growing individually or in small clusters.
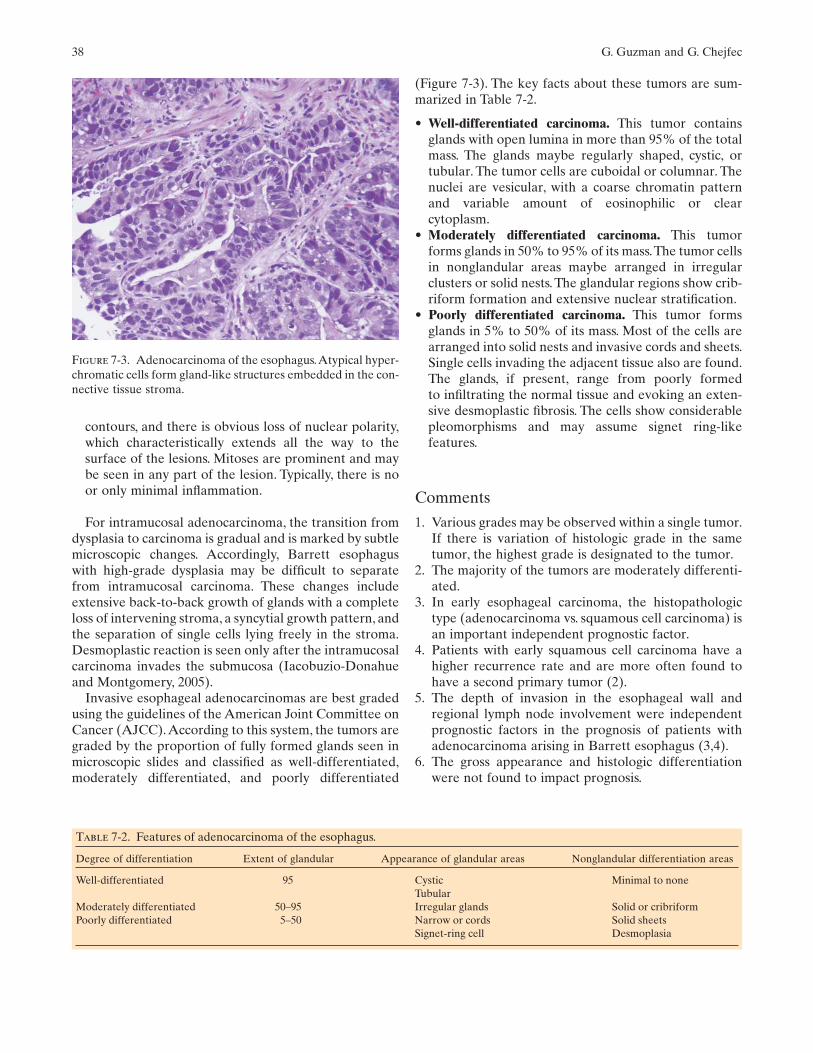
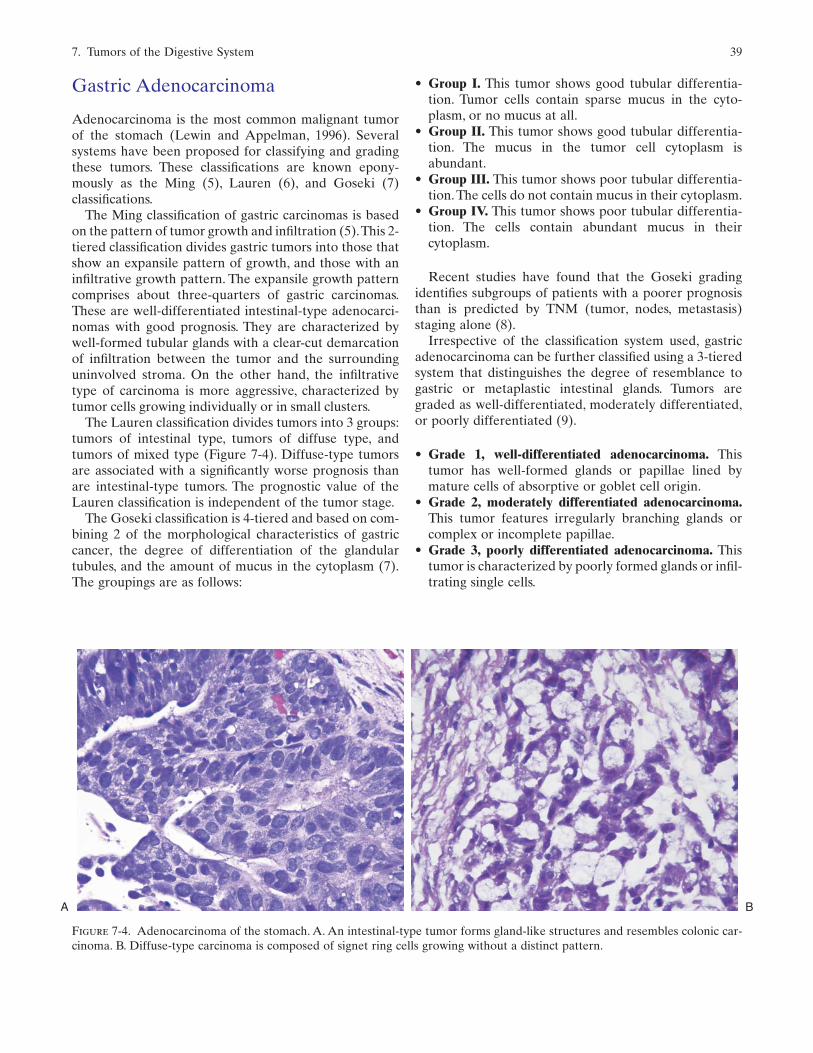
The Lauren classification divides tumors into 3 groups:tumors of intestinal type, tumors of diffuse type, andtumors of mixed type (Figure 7-4). Diffuse-type tumorsare associated with a significantly worse prognosis thanare intestinal-type tumors. The prognostic value of theLauren classification is independent of the tumor stage.
The Goseki classification is 4-tiered and based on com-bining 2 of the morphological characteristics of gastriccancer, the degree of differentiation of the glandulartubules, and the amount of mucus in the cytoplasm (7).The groupings are as follows:
• Group I. This tumor shows good tubular differentia-tion. Tumor cells contain sparse mucus in the cyto-plasm, or no mucus at all.
• Group II. This tumor shows good tubular differentia-tion. The mucus in the tumor cell cytoplasm is abundant.
• Group III. This tumor shows poor tubular differentia-tion.The cells do not contain mucus in their cytoplasm.
• Group IV. This tumor shows poor tubular differentia-tion. The cells contain abundant mucus in their cytoplasm.
Recent studies have found that the Goseki gradingidentifies subgroups of patients with a poorer prognosisthan is predicted by TNM (tumor, nodes, metastasis)staging alone (8).
Irrespective of the classification system used, gastricadenocarcinoma can be further classified using a 3-tieredsystem that distinguishes the degree of resemblance togastric or metaplastic intestinal glands. Tumors aregraded as well-differentiated, moderately differentiated,or poorly differentiated (9).
• Grade 1, well-differentiated adenocarcinoma. Thistumor has well-formed glands or papillae lined bymature cells of absorptive or goblet cell origin.
• Grade 2, moderately differentiated adenocarcinoma.This tumor features irregularly branching glands orcomplex or incomplete papillae.
• Grade 3, poorly differentiated adenocarcinoma. Thistumor is characterized by poorly formed glands or infil-trating single cells.
A B
Figure 7-4. Adenocarcinoma of the stomach. A. An intestinal-type tumor forms gland-like structures and resembles colonic car-cinoma. B. Diffuse-type carcinoma is composed of signet ring cells growing without a distinct pattern.
40 G. Guzman and G. Chejfec
Comments
1. Undifferentiated carcinomas do not display any dif-ferentiating features and may resemble other tumorssuch as lymphoma, poorly differentiated squamous car-cinoma, or sarcomas. Immunohistochemical positivity forcytokeratins may be necessary to identify the epithelialnature of these tumors (10).
2. The Lauren classification provides prognostic indi-cators that are independent of the tumor grade and otherdata gathered about gastric adenocarcinoma.
Gastrointestinal Stromal Tumors
Mesenchymal tumors of the stomach are divided into 2major groups. The first comprises the tumors that origi-nate and/or are composed of cells that are ubiquitous,such as fibroblasts, fat cells, or endothelial cells. Tumorsof this group, such as lipomas, schwannomas, and others,as well as their malignant counterparts do not differ fromhomonymous tumors in other parts of the body. Thesecond group includes gastrointestinal stromal tumors(GIST), a type of neoplasia that predominantly occurs inthe gastrointestinal tract and the abdominal cavity.
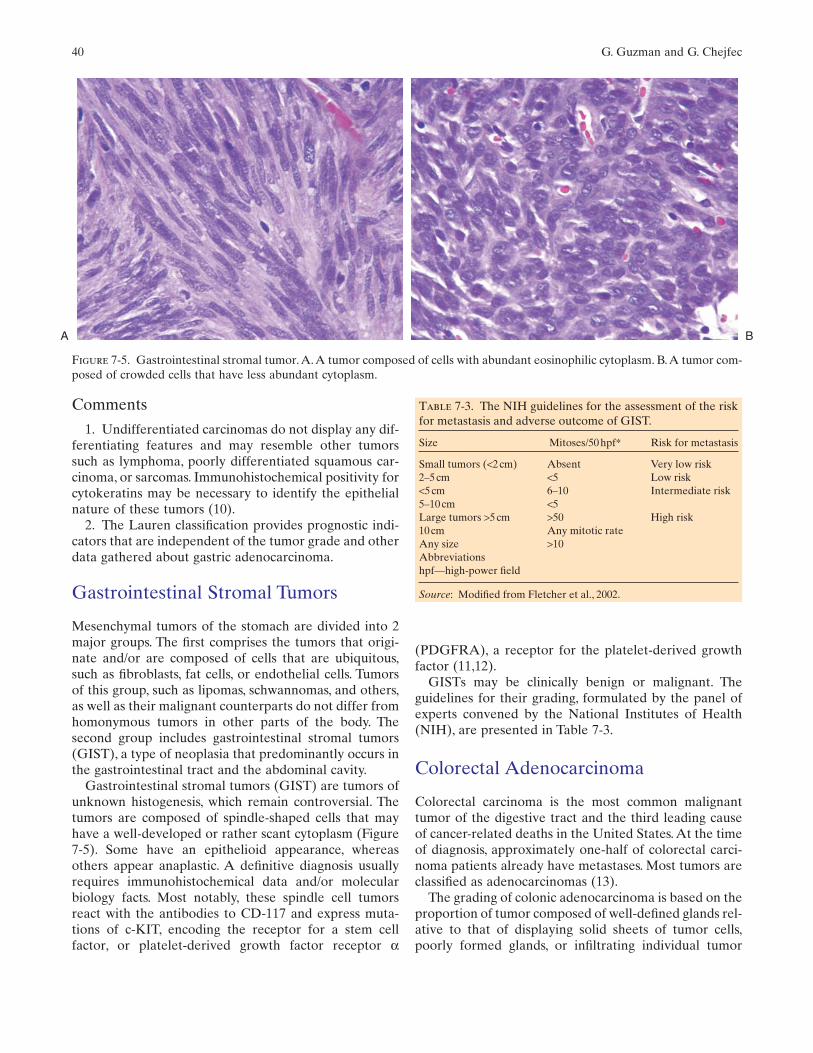
Gastrointestinal stromal tumors (GIST) are tumors ofunknown histogenesis, which remain controversial. Thetumors are composed of spindle-shaped cells that mayhave a well-developed or rather scant cytoplasm (Figure7-5). Some have an epithelioid appearance, whereasothers appear anaplastic. A definitive diagnosis usuallyrequires immunohistochemical data and/or molecularbiology facts. Most notably, these spindle cell tumorsreact with the antibodies to CD-117 and express muta-tions of c-KIT, encoding the receptor for a stem cellfactor, or platelet-derived growth factor receptor α
(PDGFRA), a receptor for the platelet-derived growthfactor (11,12).
GISTs may be clinically benign or malignant. Theguidelines for their grading, formulated by the panel ofexperts convened by the National Institutes of Health(NIH), are presented in Table 7-3.
Colorectal Adenocarcinoma
Colorectal carcinoma is the most common malignanttumor of the digestive tract and the third leading causeof cancer-related deaths in the United States. At the timeof diagnosis, approximately one-half of colorectal carci-noma patients already have metastases. Most tumors areclassified as adenocarcinomas (13).
The grading of colonic adenocarcinoma is based on theproportion of tumor composed of well-defined glands rel-ative to that of displaying solid sheets of tumor cells,poorly formed glands, or infiltrating individual tumor
A B
Figure 7-5. Gastrointestinal stromal tumor.A.A tumor composed of cells with abundant eosinophilic cytoplasm. B.A tumor com-posed of crowded cells that have less abundant cytoplasm.
Table 7-3. The NIH guidelines for the assessment of the riskfor metastasis and adverse outcome of GIST.
Size Mitoses/50hpf* Risk for metastasis
Small tumors (<2cm) Absent Very low risk2–5cm <5 Low risk<5cm 6–10 Intermediate risk5–10cm <5Large tumors >5cm >50 High risk10cm Any mitotic rateAny size >10Abbreviationshpf—high-power field
Source: Modified from Fletcher et al., 2002.
7. Tumors of the Digestive System 41
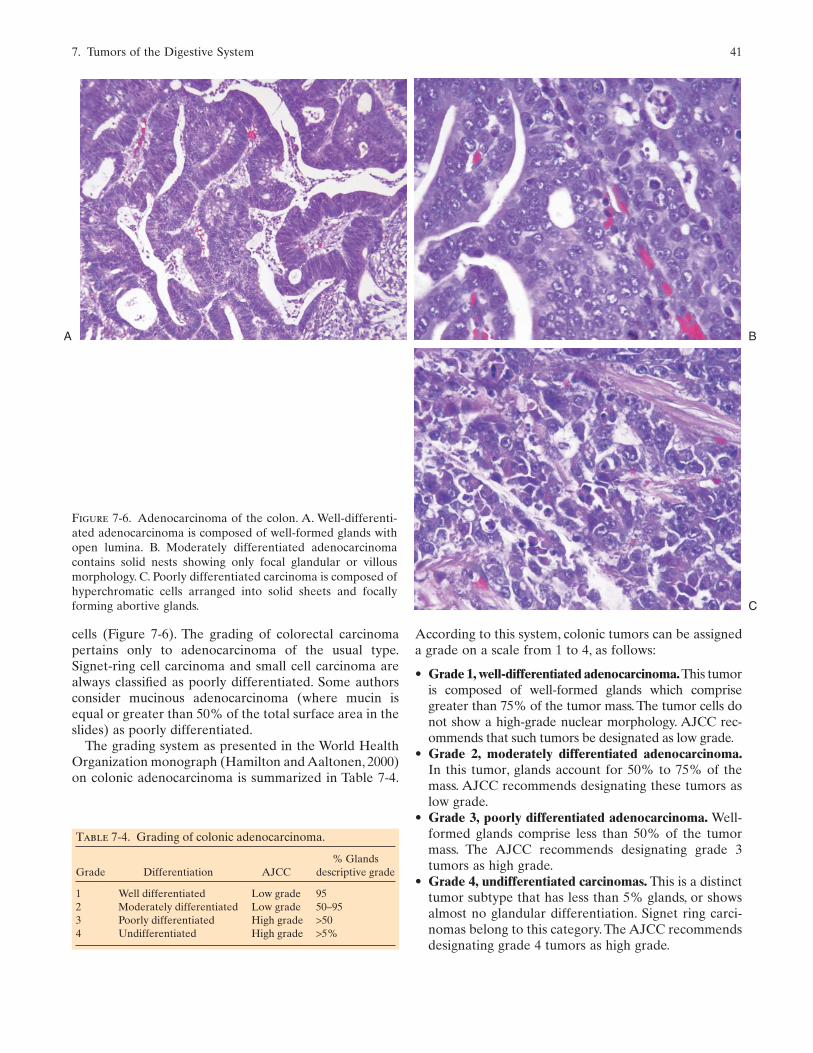
cells (Figure 7-6). The grading of colorectal carcinomapertains only to adenocarcinoma of the usual type.Signet-ring cell carcinoma and small cell carcinoma arealways classified as poorly differentiated. Some authorsconsider mucinous adenocarcinoma (where mucin isequal or greater than 50% of the total surface area in theslides) as poorly differentiated.
The grading system as presented in the World HealthOrganization monograph (Hamilton and Aaltonen, 2000)on colonic adenocarcinoma is summarized in Table 7-4.
According to this system, colonic tumors can be assigneda grade on a scale from 1 to 4, as follows:
• Grade 1, well-differentiated adenocarcinoma.This tumoris composed of well-formed glands which comprisegreater than 75% of the tumor mass. The tumor cells donot show a high-grade nuclear morphology. AJCC rec-ommends that such tumors be designated as low grade.
• Grade 2, moderately differentiated adenocarcinoma.In this tumor, glands account for 50% to 75% of themass. AJCC recommends designating these tumors aslow grade.
• Grade 3, poorly differentiated adenocarcinoma. Well-formed glands comprise less than 50% of the tumormass. The AJCC recommends designating grade 3tumors as high grade.
• Grade 4, undifferentiated carcinomas. This is a distincttumor subtype that has less than 5% glands, or showsalmost no glandular differentiation. Signet ring carci-nomas belong to this category. The AJCC recommendsdesignating grade 4 tumors as high grade.
A
C
B
Figure 7-6. Adenocarcinoma of the colon. A. Well-differenti-ated adenocarcinoma is composed of well-formed glands withopen lumina. B. Moderately differentiated adenocarcinomacontains solid nests showing only focal glandular or villousmorphology. C. Poorly differentiated carcinoma is composed ofhyperchromatic cells arranged into solid sheets and focallyforming abortive glands.
Table 7-4. Grading of colonic adenocarcinoma.
% GlandsGrade Differentiation AJCC descriptive grade
1 Well differentiated Low grade 952 Moderately differentiated Low grade 50–953 Poorly differentiated High grade >504 Undifferentiated High grade >5%
42 G. Guzman and G. Chejfec
Using this classification, most colonic adenocarcinomasare designated as moderately differentiated, whichaccount for 70% of all colonic tumors. Those classified aswell-differentiated or poorly differentiated adenocarci-nomas account for the remaining 30%.
Comments
1. Epidermal growth factor receptor (EGFR) isexpressed in up to 75% of colorectal cancer tumors (14).In the near future, identification of EGFR should becommon practice in the pathology work-up of colorectalcarcinomas.
2. The term adenocarcinoma is used only for neoplasticlesions that invade through the muscularis mucosae andshould not be applied to intramucosal lesions seen in ade-nomatous polyps (Odze et al., 2004). “Severe dysplasia” isthe preferred term for the lesions that were previous calledintraepithelial adenocarcinoma or carcinoma in situ.
3. Dysplasia is a precursor of adenocarcinomas thatdevelop in ulcerative colitis and Crohn disease. Dysplas-tic changes may be reliably identified with the micro-scopic examination of colorectal biopsies (15), which areperiodically performed on these patients.The biopsy find-ings in patients with chronic inflammatory bowel diseaseare reported as follows:
• Negative for dysplasia. Special attention should bepaid to the surface epithelium, which in these casesshows normal maturation. One should ignore theregeneration-related changes in the basal parts of thecrypts, which may resemble adenomatous epithelium.
• Indefinite for dysplasia. This category is reserved forinstances when reactive changes cannot be differen-tiated from neoplastic changes with certainty. Insuch cases, the nuclei of regenerating cells appearslightly hyperchromatic and may acquire enlargednucleoli. Yet they remain elongated, and there issurface maturation, which may not always beevident in a small biopsy.
• Positive for dysplasia, low grade. This diagnosis ismade in biopsies that show minimal distortion of thenormal architecture of the colonic mucosa, whichmay even appear normal. The cell nuclei appearhypochromatic, overlapping each other, and pseu-dostratified, thus resembling those in tubular ade-nomas.The surface epithelium is usually flattened orprotruding, with a reduced number of goblet cells.Generally, mitoses are easily found and are notlimited to the basal part of the crypts.
• Positive for dysplasia, high grade. This lesion is char-acterized by a loss of normal mucosal architectureand more pronounced nuclear changes than thatseen in low-grade dysplasia. The normal mucosa isreplaced by irregular glands in a back-to-back orcribriform arrangement. The nuclei vary in size and
shape, appear irregularly hyperchromatic, and showa loss of polarity. Mitoses are more numerous thanthat in mild dysplasia, and they may be atypical.These changes extend all the way to the surface ofthe epithelium.
It is worth noting that invasive adenocarcinomas maydevelop in the course of chronic inflammatory boweldisease, showing either low-grade or high-grade dyspla-sia, but more often occurring in the context of high-gradedysplasia.
Hepatocellular Carcinoma
Hepatocellular carcinoma (HCC) is not a common tumorin the United States, but worldwide it has a high preva-lence, especially in parts of Africa and Asia. All cirrhoticpatients of any etiology are at risk for the developmentof HCC, making it the fifth most common malignancyworldwide (Hamilton and Aaltonen, 2000).
HCC is most often of the classical type, in which thecells retain some resemblance to normal liver cells.Several other microscopic subtypes have been recog-nized, including the following:
• Clear cell• Small cell• Spindle cell• Sclerosing• Fibrolamellar• Mixed hepatocellular-cholangiocellular carcinoma
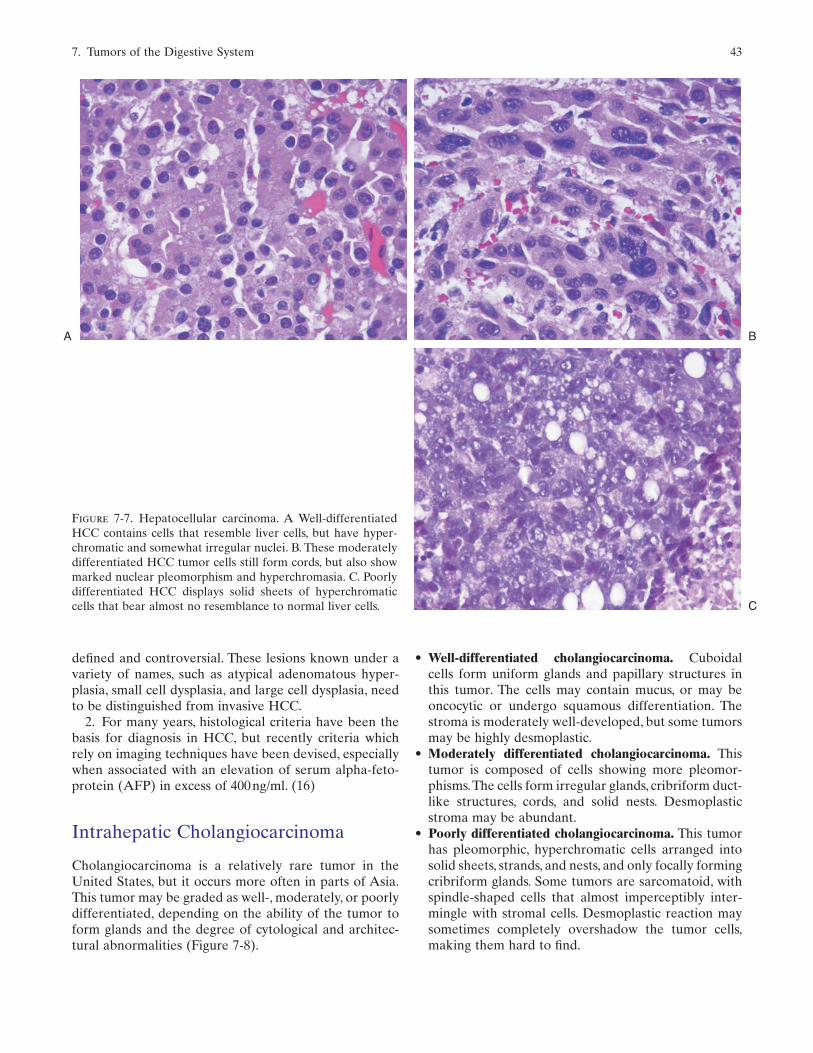
The classical type of HCC may be classified as well-differentiated, moderately differentiated, or poorly differentiated (Figure 7-7).
• Well-differentiated hepatocellular carcinoma. Thistumor measures less than 2cm. There is minimal cyto-logic atypia and an increased nuclear-cytoplasmic ratio.The pattern is usually trabecular or pseudoglandular.
• Moderately differentiated hepatocellular carcinoma.This is the most common grade of HCC, usually seen inlesions greater than 3cm. Pseudoglandular and trabecu-lar patterns characterize this tumor.The nuclei are vesic-ular, hyperchromatic, and contain well-defined nucleoli.
• Poorly differentiated hepatocellular carcinoma. Thisform of HCC is composed of pleomorphic and evengiant cells, usually arranged in solid nests. In poorly dif-ferentiated tumors, the blood vessels may be slit-likeand the sinusoidal pattern is lost.
Comment
1. Most HCC develop in the background of cirrhosis.Invasive carcinoma is often associated and most likely preceded by premalignant changes that are poorly
7. Tumors of the Digestive System 43
defined and controversial. These lesions known under avariety of names, such as atypical adenomatous hyper-plasia, small cell dysplasia, and large cell dysplasia, needto be distinguished from invasive HCC.
2. For many years, histological criteria have been thebasis for diagnosis in HCC, but recently criteria whichrely on imaging techniques have been devised, especiallywhen associated with an elevation of serum alpha-feto-protein (AFP) in excess of 400ng/ml. (16)
Intrahepatic Cholangiocarcinoma
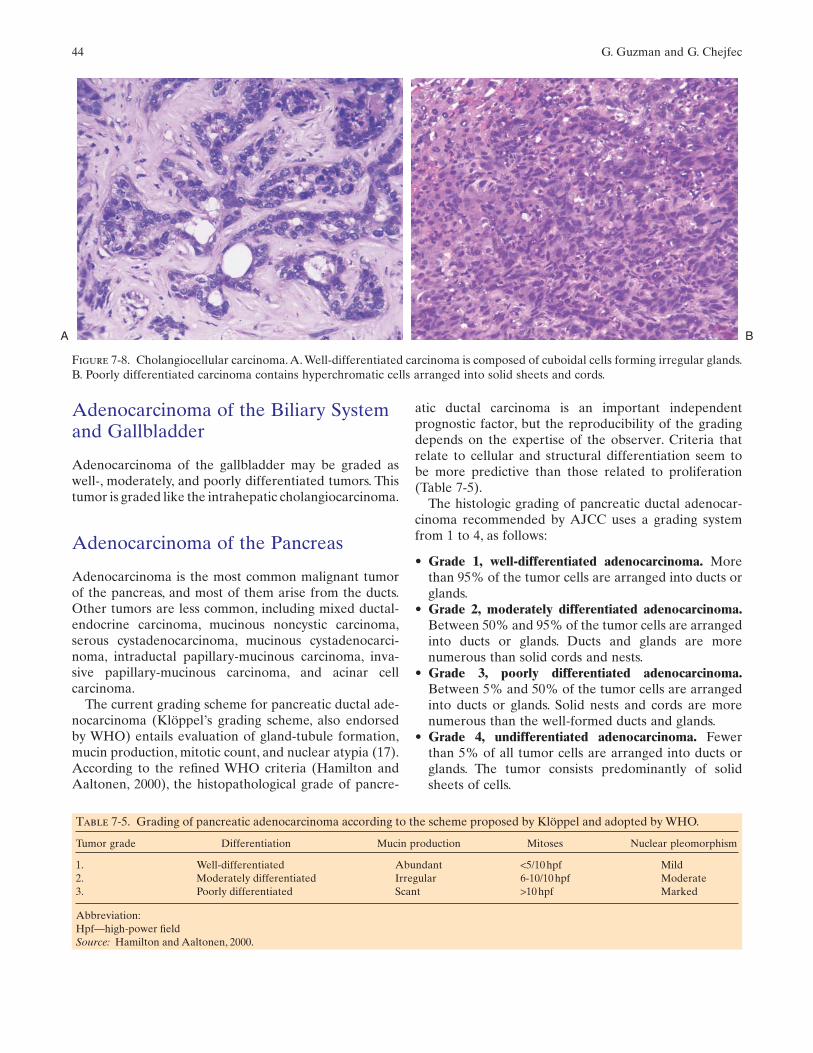
Cholangiocarcinoma is a relatively rare tumor in theUnited States, but it occurs more often in parts of Asia.This tumor may be graded as well-, moderately, or poorlydifferentiated, depending on the ability of the tumor toform glands and the degree of cytological and architec-tural abnormalities (Figure 7-8).
• Well-differentiated cholangiocarcinoma. Cuboidalcells form uniform glands and papillary structures inthis tumor. The cells may contain mucus, or may beoncocytic or undergo squamous differentiation. Thestroma is moderately well-developed, but some tumorsmay be highly desmoplastic.
• Moderately differentiated cholangiocarcinoma. Thistumor is composed of cells showing more pleomor-phisms.The cells form irregular glands, cribriform duct-like structures, cords, and solid nests. Desmoplasticstroma may be abundant.
• Poorly differentiated cholangiocarcinoma. This tumorhas pleomorphic, hyperchromatic cells arranged intosolid sheets, strands, and nests, and only focally formingcribriform glands. Some tumors are sarcomatoid, withspindle-shaped cells that almost imperceptibly inter-mingle with stromal cells. Desmoplastic reaction maysometimes completely overshadow the tumor cells,making them hard to find.
A
C
B
Figure 7-7. Hepatocellular carcinoma. A Well-differentiatedHCC contains cells that resemble liver cells, but have hyper-chromatic and somewhat irregular nuclei. B. These moderatelydifferentiated HCC tumor cells still form cords, but also showmarked nuclear pleomorphism and hyperchromasia. C. Poorlydifferentiated HCC displays solid sheets of hyperchromaticcells that bear almost no resemblance to normal liver cells.
44 G. Guzman and G. Chejfec
Adenocarcinoma of the Biliary Systemand Gallbladder
Adenocarcinoma of the gallbladder may be graded aswell-, moderately, and poorly differentiated tumors. Thistumor is graded like the intrahepatic cholangiocarcinoma.
Adenocarcinoma of the Pancreas
Adenocarcinoma is the most common malignant tumorof the pancreas, and most of them arise from the ducts.Other tumors are less common, including mixed ductal-endocrine carcinoma, mucinous noncystic carcinoma,serous cystadenocarcinoma, mucinous cystadenocarci-noma, intraductal papillary-mucinous carcinoma, inva-sive papillary-mucinous carcinoma, and acinar cellcarcinoma.
The current grading scheme for pancreatic ductal ade-nocarcinoma (Klöppel’s grading scheme, also endorsedby WHO) entails evaluation of gland-tubule formation,mucin production, mitotic count, and nuclear atypia (17).According to the refined WHO criteria (Hamilton andAaltonen, 2000), the histopathological grade of pancre-
atic ductal carcinoma is an important independent prognostic factor, but the reproducibility of the gradingdepends on the expertise of the observer. Criteria thatrelate to cellular and structural differentiation seem to be more predictive than those related to proliferation (Table 7-5).
The histologic grading of pancreatic ductal adenocar-cinoma recommended by AJCC uses a grading systemfrom 1 to 4, as follows:
• Grade 1, well-differentiated adenocarcinoma. Morethan 95% of the tumor cells are arranged into ducts orglands.
• Grade 2, moderately differentiated adenocarcinoma.Between 50% and 95% of the tumor cells are arrangedinto ducts or glands. Ducts and glands are morenumerous than solid cords and nests.
• Grade 3, poorly differentiated adenocarcinoma.Between 5% and 50% of the tumor cells are arrangedinto ducts or glands. Solid nests and cords are morenumerous than the well-formed ducts and glands.
• Grade 4, undifferentiated adenocarcinoma. Fewerthan 5% of all tumor cells are arranged into ducts orglands. The tumor consists predominantly of solidsheets of cells.
A B
Figure 7-8. Cholangiocellular carcinoma.A.Well-differentiated carcinoma is composed of cuboidal cells forming irregular glands.B. Poorly differentiated carcinoma contains hyperchromatic cells arranged into solid sheets and cords.
Table 7-5. Grading of pancreatic adenocarcinoma according to the scheme proposed by Klöppel and adopted by WHO.
Tumor grade Differentiation Mucin production Mitoses Nuclear pleomorphism
1. Well-differentiated Abundant <5/10hpf Mild2. Moderately differentiated Irregular 6-10/10hpf Moderate3. Poorly differentiated Scant >10hpf Marked
Abbreviation:Hpf—high-power fieldSource: Hamilton and Aaltonen, 2000.
7. Tumors of the Digestive System 45
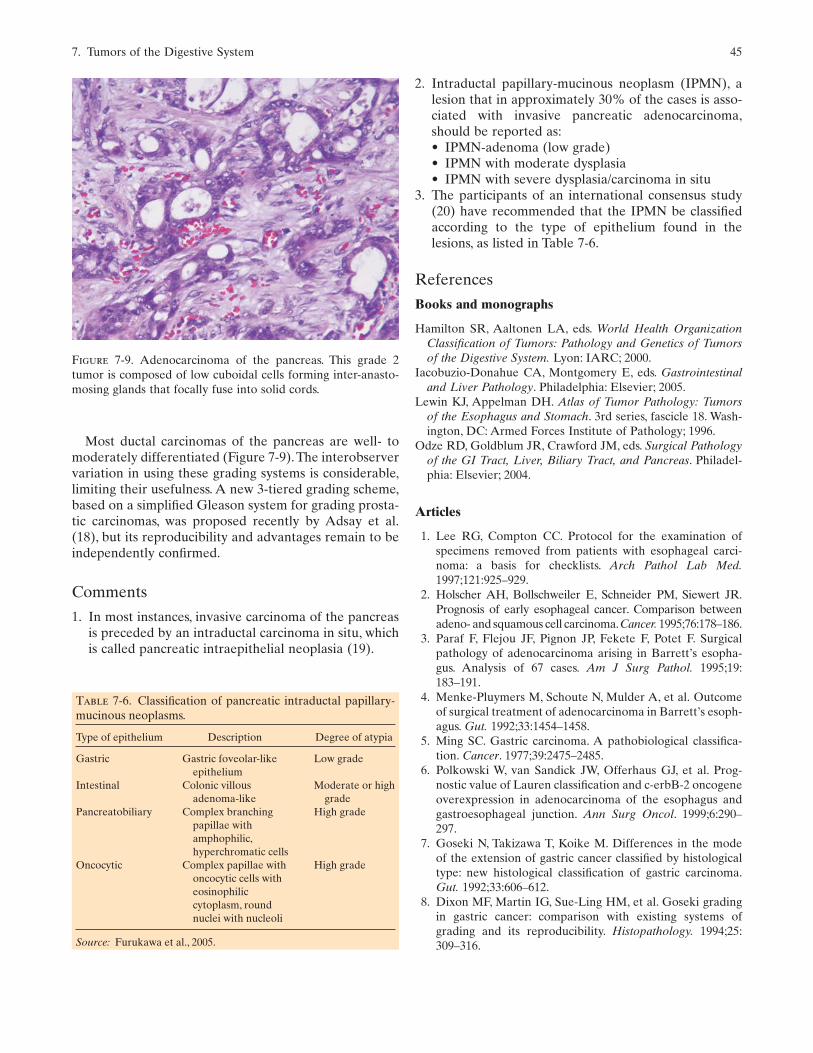
Most ductal carcinomas of the pancreas are well- tomoderately differentiated (Figure 7-9).The interobservervariation in using these grading systems is considerable,limiting their usefulness. A new 3-tiered grading scheme,based on a simplified Gleason system for grading prosta-tic carcinomas, was proposed recently by Adsay et al.(18), but its reproducibility and advantages remain to beindependently confirmed.
Comments
1. In most instances, invasive carcinoma of the pancreasis preceded by an intraductal carcinoma in situ, whichis called pancreatic intraepithelial neoplasia (19).
2. Intraductal papillary-mucinous neoplasm (IPMN), alesion that in approximately 30% of the cases is asso-ciated with invasive pancreatic adenocarcinoma,should be reported as:• IPMN-adenoma (low grade)• IPMN with moderate dysplasia• IPMN with severe dysplasia/carcinoma in situ
3. The participants of an international consensus study(20) have recommended that the IPMN be classifiedaccording to the type of epithelium found in thelesions, as listed in Table 7-6.
References
Books and monographs
Hamilton SR, Aaltonen LA, eds. World Health OrganizationClassification of Tumors: Pathology and Genetics of Tumorsof the Digestive System. Lyon: IARC; 2000.
Iacobuzio-Donahue CA, Montgomery E, eds. Gastrointestinaland Liver Pathology. Philadelphia: Elsevier; 2005.
Lewin KJ, Appelman DH. Atlas of Tumor Pathology: Tumorsof the Esophagus and Stomach. 3rd series, fascicle 18. Wash-ington, DC: Armed Forces Institute of Pathology; 1996.
Odze RD, Goldblum JR, Crawford JM, eds. Surgical Pathologyof the GI Tract, Liver, Biliary Tract, and Pancreas. Philadel-phia: Elsevier; 2004.
Articles
1. Lee RG, Compton CC. Protocol for the examination ofspecimens removed from patients with esophageal carci-noma: a basis for checklists. Arch Pathol Lab Med.1997;121:925–929.
2. Holscher AH, Bollschweiler E, Schneider PM, Siewert JR.Prognosis of early esophageal cancer. Comparison betweenadeno- and squamous cell carcinoma.Cancer. 1995;76:178–186.
3. Paraf F, Flejou JF, Pignon JP, Fekete F, Potet F. Surgicalpathology of adenocarcinoma arising in Barrett’s esopha-gus. Analysis of 67 cases. Am J Surg Pathol. 1995;19:183–191.
4. Menke-Pluymers M, Schoute N, Mulder A, et al. Outcomeof surgical treatment of adenocarcinoma in Barrett’s esoph-agus. Gut. 1992;33:1454–1458.
5. Ming SC. Gastric carcinoma. A pathobiological classifica-tion. Cancer. 1977;39:2475–2485.
6. Polkowski W, van Sandick JW, Offerhaus GJ, et al. Prog-nostic value of Lauren classification and c-erbB-2 oncogeneoverexpression in adenocarcinoma of the esophagus andgastroesophageal junction. Ann Surg Oncol. 1999;6:290–297.
7. Goseki N, Takizawa T, Koike M. Differences in the mode of the extension of gastric cancer classified by histologicaltype: new histological classification of gastric carcinoma.Gut. 1992;33:606–612.
8. Dixon MF, Martin IG, Sue-Ling HM, et al. Goseki gradingin gastric cancer: comparison with existing systems ofgrading and its reproducibility. Histopathology. 1994;25:309–316.
Figure 7-9. Adenocarcinoma of the pancreas. This grade 2tumor is composed of low cuboidal cells forming inter-anasto-mosing glands that focally fuse into solid cords.
Table 7-6. Classification of pancreatic intraductal papillary-mucinous neoplasms.
Type of epithelium Description Degree of atypia
Gastric Gastric foveolar-like Low gradeepithelium
Intestinal Colonic villous Moderate or high adenoma-like grade
Pancreatobiliary Complex branching High gradepapillae withamphophilic,hyperchromatic cells
Oncocytic Complex papillae with High gradeoncocytic cells with eosinophiliccytoplasm, round nuclei with nucleoli
Source: Furukawa et al., 2005.

46 G. Guzman and G. Chejfec
9. Fenoglio-Preiser CM, Noffsinger AE, Belli J, StemmermannGN. Pathologic and phenotypic features of gastric cancer.Semin Oncol. 1996;23:292–306.
10. Murayama H, Imai T, Kikuchi M. Solid carcinomas of thestomach. A combined histochemical, light and electronmicroscopic study. Cancer. 1983;51:1673–1681.
11. Miettinen M, Sobin LH, Lasota J. Gastrointestinal stromaltumors of the stomach: a clinicopathologic, immuno-histochemical, and molecular genetic study of 1765 caseswith long-term follow-up. Am J Surg Pathol. 2005;29:52–68.
12. Fletcher CD, Berman JJ, Corless C, et al. Diagnosis of gas-trointestinal stromal tumors: a consensus approach. HumPathol. 2002;33:459–465.
13. Compton C, Fenoglio-Preiser CM, Pettigrew N, Fielding LP.American Joint Committee on Cancer Prognostic FactorsConsensus Conference: Colorectal Working Group. Cancer.2000;88:1739–1757.
14. Layfield LJ, Bernard PS, Goldstein NS. Color multiplexpolymerase chain reaction for quantitative analysis of epi-
dermal growth factor receptor genes in colorectal adeno-carcinoma. J Surg Oncol. 2003;83:227–231.
15. Greenson JK. Dysplasia in inflammatory bowel disease.Semin Diagn Pathol. 2002;19:31–37.
16. Llovet J, Beaugrand M. Hepatocellular carcinoma: presentstatus and future prospects. J Hepatol. 2003;38:136–149.
17. Luttges J, Schemm S, Vogel I, et al. The grade of pancreaticductal carcinoma is an independent prognostic factor andis superior to the immunohistochemical assessment of pro-liferation. J Pathol. 2000;191:154–161.
18. Adsay NV, Basturk O, Bonnett M, et al. A proposal for anew and more practical grading scheme for pancreaticductal adenocarcinoma. Am J Surg Pathol. 2005;29:724–733.
19. Hruban RH, Adsay NV, Albores-Saavedra J, et al. Pancre-atic intraepithelial neoplasia: a new nomenclature and clas-sification system for pancreatic duct lesions. Am J SurgPathol. 2001;25:579–586.
20. Furukawa T, Klöppel G, Adsay NV, et al. Classification oftypes of intraductal papillary-mucinous neoplasm of the pan-creas: a consensus study. Virchows Arch. 2005;447:794–799.





























