Embed Size (px)
Citation preview

PRIORITY COMMUNICATION
Two Distinct Amnesic Profiles in Behavioral VariantFrontotemporal Dementia
Maxime Bertoux, Leonardo Cruz de Souza, Fabian Corlier, Foudil Lamari, Michel Bottlaender,Bruno Dubois, and Marie SarazinBackground: Whether or not episodic memory deficit is a characteristic of behavioral variant frontotemporal dementia (bvFTD) is acrucial question for its diagnosis and management.
Methods: We compared the episodic memory performance profile of bvFTD patients with healthy control subjects and patients withAlzheimer’s disease (AD) as defined by clinical and biological criteria. Episodic memory was assessed with the Free and Cued SelectiveReminding Test, which controls for effective encoding and identifies memory storage ability resulting from consolidation processing. Onehundred thirty-four participants were evaluated: 56 patients with typical clinical presentation of AD and pathophysiological evidence asdefined by cerebrospinal fluid AD biomarker profile and/or significant amyloid retention on Pittsburgh Compound B positron emissiontomography; 56 patients diagnosed with bvFTD with no evidence of AD-cerebrospinal fluid biomarkers when a profile was available (28/56),including 44 progressive (bvFTD) and 12 nonprogressive (phenocopies) patients; and 22 control subjects with negative amyloid imaging.
Results: Memory scores could not differentiate bvFTD from AD patients (sensitivity and specificity �50%). Taking into account theindividual distribution of Free and Cued Selective Reminding Test scores, half of bvFTD patients had a deficit of free recall, total (free �cued) recall, and delayed recall as severe as AD patients. The other half had subnormal scores similar to phenocopies and a delayed recallscore similar to control subjects.
Conclusions: We observed two distinct amnesic profiles in bvFTD patients that could reflect two types of hippocampal structure andPapez circuit involvement. These findings on episodic memory profiles could contribute to discussions on the recent internationalconsensus criteria for bvFTD.
Key Words: Alzheimer’s disease, amnesia, diagnosis, episodicmemory, frontotemporal dementia, neuropsychology
The revised criteria for the diagnosis of behavioral variantfrontotemporal dementia (bvFTD) are based on behavioralfeatures and a neuropsychological profile that include a
relative sparing of episodic memory (1). Severe amnesia is thusconsidered as an exclusion criterion to meet the neuropsychologicalcriterion for bvFTD, but studies with postmortem neuropathologicaldiagnosis confirmation have shown that bvFTD patients maymanifest severe episodic memory deficits, even at initial presentation(2–4). More recently, several studies have demonstrated that episodicmemory deficits are more common in bvFTD than previouslybelieved and that they may even be as severe as in Alzheimer’sdisease (AD) (5,6). Because the severe amnesia observed in bvFTD
Authors MB and LCdS contributed equally to this work.
From the Brain & Spine Institute (ICM) (MB, LCdS, FC, BD), INSERM UMRS975, Paris; Université Pierre et Marie Curie (MB, LCdS, FC, BD),Sorbonne Universités, Paris; Alzheimer Institute (MB, LCdS, BD, MS),Department of Neurology, Hôpital Pitié-Salpêtrière (Assistance Pub-lique - Hôpitaux de Paris), Paris; National Reference Centre for RareDementia (MB, BD), Hôpital Pitié-Salpêtrière (Assistance Publique -Hôpitaux de Paris), Paris; Department of Metabolic Biochemistry (FL),Groupe Hospitalier Pitié-Salpêtrière, Paris; CEA (MB), DSV, Institutd’Imagerie Biomédicale, Service Hospitalier Frédéric Joliot, Orsay;and Centre Psychiatrie et Neurosciences (MS), INSERM UMR S894,Université Paris Descartes, Paris V, and Department of Neurology,Centre Hospitalier Saint Anne, Paris, France.
Address correspondence to Maxime Bertoux, Ph.D., ICM, Neurologie,Institut de la Mémoire et de la Maladie d’Alzheimer – GHU Pitié-Salpêtrière, 83, Boulevard de l’hôpital, Paris 75013, France; E-mail:[email protected].
Received May 17, 2013; revised Jul 29, 2013; accepted Aug 15, 2013.
0006-3223/$36.00http://dx.doi.org/10.1016/j.biopsych.2013.08.017
contrasts with the preserved memory performance of phenocopypatients, who display typical behavioral features of bvFTD but do notprogress to dementia (7), it has been suggested that the admixtureof phenocopy and bvFTD could have led to an underestimation ofmemory impairment in previous studies of bvFTD (8,9).
Moreover, imaging studies have shown that hippocampalstructures and the Papez circuit are affected in bvFTD, suggestingthat amnesia could be due to defects in memory storage andconsolidation processing (9–11) rather than a deficit of frontal lobe-based strategies of memory recall, as was previously suggested(12,13). One way to assess which of these subprocesses of episodicmemory is compromised in bvFTD is to explore memory perform-ance with the Free and Cued Selective Reminding Test (FCSRT), atest that can control for effective encoding and identify memorystorage associated with consolidation processing. This testprovides objective measures of the main subprocesses of episodicmemory: 1) encoding, i.e., immediate registration of the item, whichinvolves attentional processes; 2) consolidation, i.e., formation of amemory trace; and 3) the retrieval of the learned material. The cuedrecall technique used in the FCSRT aims at enhancing both theencoding and the retrieval phases, to minimize the effect ofimpaired attention and inefficient retrieval strategies due to exec-utive dysfunction and therefore to identify a pure memory deficit.
In this context, we aimed to analyze episodic memory function in alarge group of bvFTD patients comparatively with AD patientsselected according to clinical and biological criteria to ensure exclusionof patients with atypical AD or atypical bvFTD with AD etiology.
Methods and Materials
ParticipantsOne hundred thirty-four participants were selected from
the database of the Memory and Alzheimer Institute of thePitié-Salpêtrière Hospital from May 2007 to June 2012, including
BIOL PSYCHIATRY 2013;]:]]]–]]]& 2013 Society of Biological Psychiatry

2 BIOL PSYCHIATRY 2013;]:]]]–]]] M. Bertoux et al.
the Biomage (ANR-07-LVIE-002-01) and Imabio3 studies (Pro-gramme Hospitalier de Recherche Clinique 2010). Fifty-six ADpatients were selected according to the following criteria: 1) typicalclinical presentation of AD with an amnestic presentation; and 2)biological evidence of the AD pathophysiological process as definedby cerebrospinal fluid (CSF)-AD biomarker profile and/or significantamyloid retention on positron emission tomography (PET) with 11C-labeled Pittsburgh Compound B (11C-PiB). A CSF-AD biomarkerprofile was defined as a phosphorylated tau/amyloid beta 42 (Aβ42)ratio greater than .21, which distinguishes AD from bvFTD with highsensitivity (91.2%) and specificity (92.6%) (14). Significant fixation of11C-PiB on PET was defined by a global index higher than 1.4. Allpatients underwent lumbar puncture (LP); 18 patients underwentboth LP and 11C-PiB-PET.
Fifty-six bvFTD patients met the following inclusion criteria:prominent changes in personality and social behavior accordingto the core clinical diagnostic criteria for frontotemporal dementia(FTD) (1) and normal CSF biomarker profile as defined by aphosphorylated tau/Aβ42 ratio lower than .21 when LP wasperformed (n ¼ 28/56). We included patients with memory impair-ment if the other core diagnostic criteria of bvFTD were present.None of the patients had a family history of dementia. As we aimedto distinguish bvFTD from phenocopies, we classed patientsdiagnosed with bvFTD according to their clinical progression duringat least 3 years of follow-up. Among the 56 patients, 44 showedclinical progression consistent with the diagnosis of bvFTD based oncognitive measures (Mini Mental State Examination [MMSE] andMattis Dementia Rating Scale [MDRS]) (15,16) and activities of dailyliving during at least 3 years of follow-up; these 44 patientsconstitute the bvFTD group. The 12 remaining patients showedno change in cognitive measures and activities of daily living over a3-year period and were therefore classified as phenocopies.
Twenty-two normal control subjects were selected accordingto the following criteria: 1) MMSE $27 and normal neuropsycho-logical testing; 2) negative amyloid imaging on 11C-PiB-PET, asdefined by a global 11C-PiB retention index lower than 1.4; and3) no history of psychiatric or neurologic conditions.
We did not include participants who presented with thefollowing: 1) clinical or neuroimaging evidence of focal lesions,2) severe cortical or subcortical vascular lesions, 3) severedepression, or 4) motor neuron disease.
Measurement of CSF BiomarkersCerebrospinal fluid samples were collected by LP and analyzed
for total tau, tau phosphorylated at threonine 181, and Aβ42 usinga double-sandwich enzyme-linked immunosorbent assay method(Innogenetics, Gent, Belgium). Assays were conducted at theMetabolic Biochemistry Department of the Pitié-Salpêtrière Hos-pital, as described elsewhere (14).
11C-PiB PET Imaging ProceduresPositron emission tomography imaging with 11C-PiB was per-
formed in all control subjects and in 21 AD patients. The method wasthe same as previously described (17). In summary, a global corticalindex was defined by the mean standard uptake value ratio (with thecerebellum as the reference region) of the following cortical regions:1) frontal cortex, by grouping the orbitofrontal, polar prefrontal, anddorsolateral cortex; 2) anterior cingulate; 3) medial cingulate;4) posterior cingulate; 5) precuneus; 6) occipital cortex, by groupingthe calcarine cortex, occipital cortex, and cuneus; 7) temporal cortex,by grouping the anterior and lateral temporal cortex; 8) hippo-campus; and 9) parietal cortex, by grouping the inferior and superiorparietal cortex and the parietotemporal junction.
www.sobp.org/journal
Neuropsychological AssessmentAll subjects underwent a neuropsychological assessment that
included the MMSE, the Frontal Assessment Battery (FAB) (18),semantic/morphologic verbal fluencies, and the FCSRT (seebelow) (19). In addition, patients in the bvFTD and phenocopygroups were tested with a frontal battery including the MDRS, themodified Wisconsin Card Sorting Task (20), the digit span forwardand backward for verbal working memory, the short version ofthe Social cognition and Emotional Assessment (21) for socialcognition, and a picture denomination task to identify semanticmemory deficits.
Assessment of Episodic Memory in All Participants. TheFCSRT (19) was selected because it is based on a semantic cueingmethod that controls for effective encoding of the list of wordsand facilitates retrieval by semantic cueing. The FCSRT wasadministered according to the procedure previously describedby Sarazin et al. (22). Immediate cued recall was tested in a firstphase to control for encoding (16 written words presented ingroups of 4 � 4, maximum score ¼ 16). Then, the memory phasewas performed in three successive recall trials. Each recall trialincluded a free recall attempt consisting of spontaneous recall ofas many items as possible, then a cued recall attempt using anaurally presented semantic category for items that were notspontaneously retrieved by the patient. The same semantic cuegiven in the initial encoding stage was used. This provided a freerecall score and a total (free � cued) recall score (maximum score¼ 48). Then, after an interval of 30 minutes, a last recall trial wasperformed, providing free and total delayed recall scores (maxi-mum score ¼ 16).
All control subjects and AD patients were included in eitherthe Biomage or Imabio3 studies, which were both approved bythe Ethics Committee of the Pitié-Salpêtrière Hospital, andparticipants provided written informed consent before participat-ing. For all other patients, the biological, clinical, and imagingdata were generated during routine clinical workups and wereretrospectively extracted for the purpose of this work. Accordingto French legislation, explicit informed consent was waived, aspatients and their relatives were informed that individual datamight be used in retrospective clinical research studies.
Statistical AnalysisData were analyzed using SPSS20 (SPSS Inc., Chicago, Illinois).
Before any analysis, variables were plotted and checked fornormality of distribution using the Shapiro-Wilk test. Parametricdata were compared across the four groups via analysis ofvariance, followed by Student t test. Nonparametric data wereanalyzed by Kruskal-Wallis analysis of variance followed by theMann-Whitney test for two-by-two comparisons. We used Spear-man’s rank coefficient for correlations. Bonferroni correction formultiple measures was applied for all analyses.
Receiver operating characteristic (ROC) curve analyses wereperformed to evaluate the discriminating power of FCSRT scoresand clinical diagnosis. The area under the curve was used as ameasure of the overall performance of each test (with a 95%confidence interval). Moreover, we assessed whether the areaunder the curve values were significantly different using a non-parametric method for correlated samples (Delong’s method).Optimal cutoff points for the FCSRT were calculated by selectingthe point on the ROC curve that maximized both sensitivity andspecificity. In addition to the ROC curve analyses, a logisticstepwise regression analysis (using the Enter method) was carriedout after selecting FCSRT scores with the least overlap betweengroups.
M. Bertoux et al. BIOL PSYCHIATRY 2013;]:]]]–]]] 3
Results
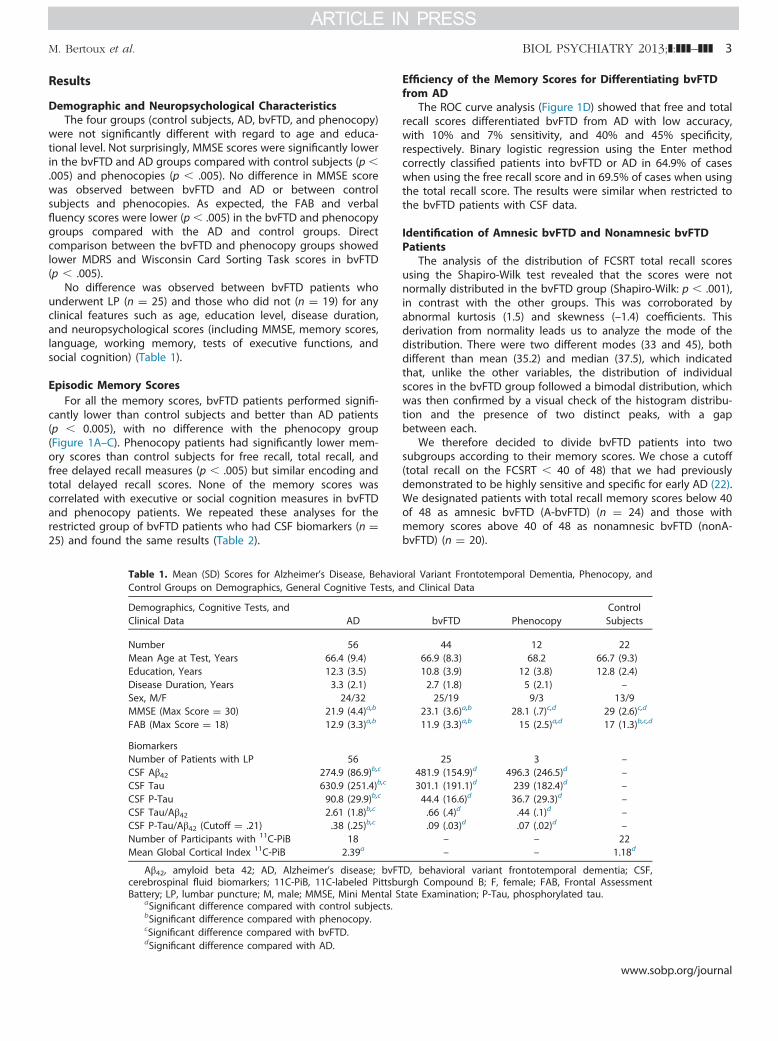
Demographic and Neuropsychological CharacteristicsThe four groups (control subjects, AD, bvFTD, and phenocopy)
were not significantly different with regard to age and educa-tional level. Not surprisingly, MMSE scores were significantly lowerin the bvFTD and AD groups compared with control subjects (p �.005) and phenocopies (p � .005). No difference in MMSE scorewas observed between bvFTD and AD or between controlsubjects and phenocopies. As expected, the FAB and verbalfluency scores were lower (p � .005) in the bvFTD and phenocopygroups compared with the AD and control groups. Directcomparison between the bvFTD and phenocopy groups showedlower MDRS and Wisconsin Card Sorting Task scores in bvFTD(p � .005).
No difference was observed between bvFTD patients whounderwent LP (n ¼ 25) and those who did not (n ¼ 19) for anyclinical features such as age, education level, disease duration,and neuropsychological scores (including MMSE, memory scores,language, working memory, tests of executive functions, andsocial cognition) (Table 1).
Episodic Memory ScoresFor all the memory scores, bvFTD patients performed signifi-
cantly lower than control subjects and better than AD patients(p � 0.005), with no difference with the phenocopy group(Figure 1A–C). Phenocopy patients had significantly lower mem-ory scores than control subjects for free recall, total recall, andfree delayed recall measures (p � .005) but similar encoding andtotal delayed recall scores. None of the memory scores wascorrelated with executive or social cognition measures in bvFTDand phenocopy patients. We repeated these analyses for therestricted group of bvFTD patients who had CSF biomarkers (n ¼25) and found the same results (Table 2).
Table 1. Mean (SD) Scores for Alzheimer’s Disease, BehavioControl Groups on Demographics, General Cognitive Tests, a
Demographics, Cognitive Tests, andClinical Data AD
Number 56Mean Age at Test, Years 66.4 (9.4)Education, Years 12.3 (3.5)Disease Duration, Years 3.3 (2.1)Sex, M/F 24/32MMSE (Max Score ¼ 30) 21.9 (4.4)a,b
FAB (Max Score ¼ 18) 12.9 (3.3)a,b
BiomarkersNumber of Patients with LP 56CSF Aβ42 274.9 (86.9)b,c
CSF Tau 630.9 (251.4)b,c
CSF P-Tau 90.8 (29.9)b,c
CSF Tau/Aβ42 2.61 (1.8)b,c
CSF P-Tau/Aβ42 (Cutoff ¼ .21) .38 (.25)b,c
Number of Participants with 11C-PiB 18Mean Global Cortical Index 11C-PiB 2.39a
Aβ42, amyloid beta 42; AD, Alzheimer’s disease; bvFTcerebrospinal fluid biomarkers; 11C-PiB, 11C-labeled PittsbuBattery; LP, lumbar puncture; M, male; MMSE, Mini Mental S
aSignificant difference compared with control subjects.bSignificant difference compared with phenocopy.cSignificant difference compared with bvFTD.dSignificant difference compared with AD.
Efficiency of the Memory Scores for Differentiating bvFTDfrom AD
The ROC curve analysis (Figure 1D) showed that free and totalrecall scores differentiated bvFTD from AD with low accuracy,with 10% and 7% sensitivity, and 40% and 45% specificity,respectively. Binary logistic regression using the Enter methodcorrectly classified patients into bvFTD or AD in 64.9% of caseswhen using the free recall score and in 69.5% of cases when usingthe total recall score. The results were similar when restricted tothe bvFTD patients with CSF data.
Identification of Amnesic bvFTD and Nonamnesic bvFTDPatients
The analysis of the distribution of FCSRT total recall scoresusing the Shapiro-Wilk test revealed that the scores were notnormally distributed in the bvFTD group (Shapiro-Wilk: p � .001),in contrast with the other groups. This was corroborated byabnormal kurtosis (1.5) and skewness (–1.4) coefficients. Thisderivation from normality leads us to analyze the mode of thedistribution. There were two different modes (33 and 45), bothdifferent than mean (35.2) and median (37.5), which indicatedthat, unlike the other variables, the distribution of individualscores in the bvFTD group followed a bimodal distribution, whichwas then confirmed by a visual check of the histogram distribu-tion and the presence of two distinct peaks, with a gapbetween each.
We therefore decided to divide bvFTD patients into twosubgroups according to their memory scores. We chose a cutoff(total recall on the FCSRT � 40 of 48) that we had previouslydemonstrated to be highly sensitive and specific for early AD (22).We designated patients with total recall memory scores below 40of 48 as amnesic bvFTD (A-bvFTD) (n ¼ 24) and those withmemory scores above 40 of 48 as nonamnesic bvFTD (nonA-bvFTD) (n ¼ 20).
ral Variant Frontotemporal Dementia, Phenocopy, andnd Clinical Data
bvFTD PhenocopyControlSubjects
44 12 2266.9 (8.3) 68.2 66.7 (9.3)10.8 (3.9) 12 (3.8) 12.8 (2.4)2.7 (1.8) 5 (2.1) –25/19 9/3 13/9
23.1 (3.6)a,b 28.1 (.7)c,d 29 (2.6)c,d
11.9 (3.3)a,b 15 (2.5)a,d 17 (1.3)b,c,d
25 3 –481.9 (154.9)d 496.3 (246.5)d –301.1 (191.1)d 239 (182.4)d –44.4 (16.6)d 36.7 (29.3)d –.66 (.4)d .44 (.1)d –.09 (.03)d .07 (.02)d –
– – 22– – 1.18d
D, behavioral variant frontotemporal dementia; CSF,rgh Compound B; F, female; FAB, Frontal Assessmenttate Examination; P-Tau, phosphorylated tau.
www.sobp.org/journal

Figure 1. Number of words correctly recalled in the Freeand Cued Selective Reminding Test during the free recall(A), the total recall (B), and the delayed total recall (C)phases for Alzheimer’s disease (AD), behavioral variantfrontotemporal dementia (bvFTD), phenocopy (Phcpy),and control (Ctrls) groups and receiver operating char-acteristic (ROC) curve for free, total, and delayed recall (D)for the diagnosis distinction between AD and bvFTD.
4 BIOL PSYCHIATRY 2013;]:]]]–]]] M. Bertoux et al.
There was no significant difference in age, gender, education,disease duration, MMSE, executive cognitive scores (MDRS, WSCT,FAB, verbal fluency), language (picture naming), working memory(forward and backward digit span), or social cognition scores (theshort version of the Social cognition and Emotional Assessment)between A-bvFTD and nonA-bvFTD patients. The number ofpatients who had an LP was similar in the two groups. Therewas no difference in CSF biomarker levels between A-bvFTD andnonA-bvFTD patients. There was no difference in clinical andcognitive measures between A-bvFTD patients with and withoutLP or between nonA-bvFTD patients with or without LP.
Amnesic bvFTD patients performed similarly to AD patients foreach memory score (Table 3, Figure 2,A–C), with both groupsscoring significantly lower than nonA-bvFTD, phenocopy, andcontrol patients (p � .001). For nonA-bvFTD patients, the free recallfell between that of AD and control patients (p� .005), whereas thetotal recall score was subnormal and similar to that of phenocopies.The free delayed recall score was also intermediate between AD andcontrol patients (p � .005) and the total delayed recall score wassimilar to phenocopies and control subjects. We further performed
Table 2. Mean (SD) Free and Cued Selective Reminding TFrontotemporal Dementia, Phenocopy and Control Groups
FCSRT Scores AD
Encoding (Max Score ¼ 16) 10.6 (3.9)a,b,c
Free Recall (Max score ¼ 48) 8.6 (6.5)a,b,c
Total Recall (Max Score ¼ 48) 23.4 (12.7)a,b,c
Free Delayed Recall (Max Score ¼ 16) 1.8 (2.9)a,b,c
Total Delayed Recall (Max Score ¼ 16) 6.6 (5.1)a,b,c
AD, Alzheimer’s disease; bvFTD, behavioral variant fronReminding Test.
aSignificant difference compared with bvFTD.bSignificant difference compared with control subjects.cSignificant difference compared with phenocopy.dSignificant difference compared with AD.
www.sobp.org/journal
analysis of covariance with encoding as a covariate to take intoaccount the differences between patient groups at encoding; resultsshowed the same pattern of differences between groups. Plus, sideanalyses were run with each demographic/cognitive variable as acovariate and the differences between A-bvFTD and nonA-bvFTDstill remained significant (all p � .001).
We repeated these analyses for the restricted group of bvFTDpatients who had CSF biomarkers, including both A-bvFTD (n ¼13) and nonA-bvFTD (n ¼ 12) subgroups, and obtained the sameresults (Table 3).
Discussion
This study analyzed the profile of episodic memory function inbvFTD patients compared with control subjects and AD patients.All control and AD patients and over half of the FTD patients wereselected according to clinical and biological criteria. We chose theFCSRT (19), which assesses the four main components of verbalepisodic memory (encoding, free recall, total [free � cued] recall,
est Scores for Alzheimer’s Disease, Behavioral Variant
bvFTD PhenocopyControlSubjects
12.9 (3.5)b,d 14 (3.4)d 16 (.5)a,d
14.9 (7.9)b,d 21 (7.6)b,d 33 (6.2)a,c,d
35.2 (12.4)b,d 41 (7.1)b,d 47 (1.0)a,c,d
5.3 (2.9)b,d 6 (2.5)b,d 12 (2)a,c,d
12.1 (4.3)b,d 15 (1.9)d 15 (.2)a,d
totemporal dementia; FCSRT, Free and Cued Selective

Table 3. Mean (SD) Free and Cued Selective Reminding Test Scores for Alzheimer’s Disease, Amnesic Behavioral Variant Frontotemporal Dementia,Nonamnesic Behavioral Variant Frontotemporal Dementia, Phenocopy Patients, and Control Subjects and Neuropsychological Scores for AmnesicBehavioral Variant Frontotemporal Dementia, Nonamnesic Behavioral Variant Frontotemporal Dementia, and Phenocopy Patients
AD A-bvFTD nonA-bvFTD Phenocopy Control Subjects
Number 56 24 20 12 22Mean Age at Test, Years 66.4 (9.4) 67.3 (6.9) 66.6 (9.9) 68.2 66.7 (9.3)Education, Years 12.3 (3.5) 10.7 (4.2) 11.4 (3.8) 12 (3.8) 12.8 (2.4)Disease Duration, Years 3.3 (2.1) 2.8 (1.7)a 2.6 (1.9)a 5 (2.1)b,c –Sex, M/F 24/32 12/12 13/7 9/3 13/9MMSE (Max Score ¼ 30) 21.9 (4.4)a,c,d 22.4 (3.9)a,d 24.4 (3.0)a,d,e 28.1 (.7)b,c,e 29 (2.6)b,c,e
FCSRT ScoresEncoding (/16) 10.6 (3.9)a,c,d 11.1 (3.9)a,c,d 15.1 (.9)b,e 14 (3.4)b,e 16 (.5)a,b,e
Free recall (/48) 8.6 (6.5)a,c,d 10.2 (6.2)a,c,d 20.6 (5.3)b,d,e 21 (7.6)b,d,e 33 (6.2)a,b,c,e
Total recall (/48) 23.4 (12.7)a,c,d 27.2 (11.3)a,c,d 44.9 (1.0)b,d,e 41 (7.1)b,d,e 47 (1.0)a,b,c,e
Free delayed recall (/16) 1.8 (2.9)a,c,d 3.1 (1.8)a,c,d 7.2 (2.4)b,d,e 6 (2.5)b,d,e 12 (2)a,b,c,e
Total delayed recall (/16) 6.6 (5.1)a,c,d 9.3 (4.0)a,c,d 15.3 (1.0)b,e 15 (1.9)b,e 15 (.2)b,e
Frontal Neuropsychological ScoresMDRS (/144) – 120.3 (13.2) 124.4 (11.5) 134 (3.9)b,c –Verbal fluency (morphologic) – 6.1 (3.9) 7.3 (4.1) 9 (3.0) –Verbal fluency (semantic) – 10.4 (3.9) 13.4 (4.8) 13 (5.4) –mWCST category (/6) – 2.5 (1.3)a 2.8 (4.9) 5 (1.8)b –mWCST perseveration errors – 7.9 (6.8) 7.2 (4.5) 5 (9.1) –mWCST attentional errors – 4.4 (3.5)a 3.1 (4.3) 1 (1.5)b –Words denomination (%) – 96.4 (1.2) 97 (.9) 100 (0) –Digit span forward – 4.8 (1.0) 5.6 (1.5) 6 (1.6) –Digit span backward – 3.0 (.7) 3.6 (1.4) 4 (.8) –Mini-SEA (/30) – 16.9 (2.9) 16.2 (3.9) 19 (4.9) –
A-bvFTD, amnesic behavioral variant frontotemporal dementia; AD, Alzheimer’s disease; F, female; FCSRT, Free and Cued Selective Reminding Test; M,male; MDRS, Mattis Dementia Rating Scale; mini-SEA, abbreviated version of the Social Cognition and Emotional Assessment; mWCST, modified WisconsinCard Sorting Task; nonA-bvFTD, nonamnesic behavioral variant frontotemporal dementia.
aSignificant difference compared with phenocopy.bSignificant difference compared with A-bvFTD.cSignificant difference compared with nonA-bvFTDdSignificant difference compared with control subjects.eSignificant difference compared with AD.
M. Bertoux et al. BIOL PSYCHIATRY 2013;]:]]]–]]] 5
and free and total delayed [free � cued] recall) to test memorystorage capacity, which is believed to be associated with hippo-campal structure and the Papez circuit.
After excluding phenocopies, we found that the memoryperformance of the bvFTD group was intermediate between thatof the AD and control groups and overlapped with the AD group.When taking into account the distribution of the FCSRT scores, weobserved two clearly distinct profiles of memory performance inbvFTD patients: half of them (A-bvFTD) showed a deficit in
Figure 2. Number of words correctly recalled in the Free and Cued Selective Retotal recall (C) phases for Alzheimer’s disease (AD), amnesic behavioral varfrontotemporal dementia (nonA-bvFTD), phenocopy, and control groups.
episodic memory similar to that observed in AD patients, whereasthe other half (nonA-bvFTD) had subnormal performance, espe-cially for the delayed recall score, which was similar to that ofcontrol subjects.
Recent studies have suggested that bvFTD could be associ-ated with severe anterograde amnesia. Severe amnesia has beenobserved in up to 15% of pathologically confirmed bvFTDpatients, even in the initial stages of the disease (3,23–25). Byclassifying patients with bvFTD into progressive versus
minding Test during the free recall (A), the total recall (B), and the delayediant frontotemporal dementia (A-bvFTD), nonamnesic behavioral variant
www.sobp.org/journal

6 BIOL PSYCHIATRY 2013;]:]]]–]]] M. Bertoux et al.
phenocopy cases based on their long-term outcome, Hornbergeret al. (5) showed that most patients with progressive bvFTD hadthe same degree of episodic memory impairment as observed inpatients with AD. One point of discussion regarding these lastresults is that biological disease markers were not available formost participants. Therefore, the possibility of having includedpatients with frontal presentations of AD cannot be ruled out.Several recent clinicopathological studies have highlighted therisk of misdiagnosis between AD and bvFTD: 22% of cases with aclinical presentation of bvFTD actually had AD pathology (24).Conversely, patients who had typical clinical presentations of ADwith temporoparietal hypometabolism suggestive of AD couldhave a diagnosis of FTD pathology at autopsy (25). In the currentstudy, in addition to clinical criteria, all AD patients were selectedon the basis of biological evidence of underlying AD patho-physiology (CSF biomarkers and/or 11C-PiB-PET), to excludeatypical FTD patients, and all control subjects had normal11C-PiB-PET results, thereby excluding asymptomatic AD. Cere-brospinal fluid data were available for 57% of FTD patients andnone of whom had a CSF-AD profile, thus excluding atypicalfrontal presentations of AD in this group. Importantly, weverified that bvFTD patients who underwent LP did not differfrom those without LP with regard to any clinical or cognitivefeatures. We also verified that our findings were similar when weconsidered only the results of the bvFTD subgroup that under-went LP. Additionally, we distinguished bvFTD from phenocopycases based on clinical change over a 3-year period to excludeambiguous etiology.
Based on these strict inclusion criteria, we observed a deficit ofepisodic memory scores in bvFTD patients, with an importantoverlap of their scores with those of AD patients, consistent witha previous study (5). Consequently, the sensitivity and specificityof all memory scores were below 50%, demonstrating that epi-sodic memory deficit is not an accurate criterion in the differentialdiagnosis between both diseases.
By analyzing the distribution of memory performances amongbvFTD patients, we observed two distinct profiles of episodicmemory functioning, which contrasted with the homogeneity ofthe AD and control groups. Half of the bvFTD patients wereclassified in the A-bvFTD subgroup, characterized by severeamnesia similar to that observed in the AD group. For this bvFTDsubgroup, scores of spontaneous (free) recall, total (free � cued)recall, and delayed recall were not significantly different fromthose in the AD group. In contrast, the nonA-bvFTD patients hadintermediate free recall and free delayed recall scores, betweenthose of the AD and control groups, and subnormal total recallscores, as well as normal total delayed recall. Nonamnesic bvFTDand phenocopy cases did not differ from each other on any of thememory scores.
Previous studies focused on episodic memory function inbvFTD used classical neuropsychological tests such as the Recog-nition Memory Test (26), the Rey-Osterrieth Complex Figure Test(27), the Rey Auditory Verbal Learning Test (28), or the logicalmemory test of the Wechsler Memory Scale-Revised (29). TheFCSRT is different from these tests in that it utilizes control ofattention and strategy to maximize performance by improvingencoding and retrieval of learned information. In addition, theFCSRT is the only test to employ a controlled distraction procedure(counting backwards) before each recall trial, thus ensuring thatitems cannot be recalled from working memory and that recallrelies exclusively on episodic memory. Total recall, which is thesum of the free and the cued recalls, as well as total delayed recall,are interesting parameters to consider because they reflect the
www.sobp.org/journal
amount of information that is really stored by the patient, themost important marker of long-term episodic memory reflective ofstorage and consolidation memory processes (30).
After administering the FCSRT to bvFTD patients, we foundthat 55% of bvFTD patients had severe amnesia similar to thatobserved in AD, suggesting a real deficit in memory storage(memory consolidation process). The remainder of the groupshowed a slight decrease of spontaneous recall that normalizedwith cueing; this finding is associated with a normal delayedrecall and suggests a deficit in memory recall strategy due toexecutive dysfunction without a deficit in memory storage per se.In our sample, these two different episodic memory profiles inbvFTD cannot be explained by different severity of executivedysfunction because A-bvFTD and nonA-bvFTD patients did notdiffer on any executive variables or on working memory ability orsocial cognition. Nor can the difference be explained by an effectof the severity of the disease or aging because both subgroupshad similar cognitive efficiency scores, ages, and disease dura-tions, although these analyses were conducted on relatively smallgroups (n ¼ 20 and n ¼ 24), which could have embedded themagnitude of potential differences. These results showed thatprefrontal cortex dysfunction does not account solely for thememory deficits seen in bvFTD.
Interestingly, several studies have demonstrated a similardegree of hippocampal atrophy in bvFTD to that observed inAD, especially in bvFTD pathology with transactive response DNAbinding protein-43 inclusions (10,31–35). Using structural magneticresonance imaging data and postmortem brain evaluations, arecent study showed that the atrophy in memory-network brainregions was not circumscribed to the hippocampus in bvFTD andthat Papez circuitry was affected in its entirety, including sub-cortical regions such as the fornix and anterior thalamus (9).According to these works, our results suggest that the neuro-psychological constructs of the FSCRT may thus distinguish bvFTDpatients with damage in the Papez circuit from those in whom thePapez circuit remains functional. However, this study did notprovide volumetric or imaging evidence to confirm this hypothesis.
In addition to the quite selective inclusion criteria of our study,it would have been important to obtain information about thegenetic status of bvFTD patients, as the patterns of episodicmemory deficit are different between subjects with C9ORF72, tau,or progranulin mutations or sporadic FTD. None of our patientshad a familial history of FTD, and thus, in accordance with Frenchlegislation, genetic testing was not performed. However, consid-ering that 55% of the bvFTD patients included in this study hadamnesia and that the proportion of patients with a genetic historyis estimated to be 10% to 20% (36), it is unlikely that our resultscould be explained by genetics alone.
Interestingly, the proportion of nonA-bvFTD and A-bvFTDpatients in our study was quite similar to that described inpostmortem reports for the two major pathologic subtypes: FTDwith tau-positive inclusions and FTD with transactive responseDNA binding protein-43 inclusions (36). Because no autopsy datawere available in our cohort, we cannot make any link withpathology: the numerical correspondence between a 50/50 ratioin memory functioning and a similar ratio in pathologic subtypescould be a coincidence. Future studies with autopsy-confirmeddiagnoses are needed to analyze the relationship betweenamnesia and the pathologic subtypes of FTD.
In conclusion, the findings reported in this study havemajor theoretical and clinical implications for the diagnosisand clinical care of bvFTD, suggesting that bvFTD has twodistinct amnesic presentations that could reflect two distinct

M. Bertoux et al. BIOL PSYCHIATRY 2013;]:]]]–]]] 7
patterns of neural network damage. The international consensuscriteria for bvFTD should be further discussed in light of theseresults.
This work was supported by Biomage - French Agence Nationalede la Recherche under reference ANR-07-LVIE-002-01 and Medipargroup with the Fondation Nationale de Gérontologie, ImaBio3–FrenchHealth Ministry (Clinical Cancer Research Hospital Programme), andInstitut Roche de Recherche et Médecine Translationnnelle.
We thank Aurélie Funkiewiez, Christina Rogan, Dalila Samri,Elodie Guichart-Gomez, Valérie Hahn-Barma, Virginie Czernecki,Hélène Corne, and Richard Gnassounou from the Alzheimer Institute(Pitié-Salpêtrière) for performing the neuropsychological assessmentsof the patients included. We also thank Marina Agen and MaryRouillé for their help in the acquisition of clinical data and GillesAllali for his strategic advice.
Leonardo Cruz de Souza reports no conflicts of interest and nofinancial interest. He received speaker honoraria from Lundbeck.Bruno Dubois reports no conflicts of interest and no financialinterest. He has consulted or served on advisory boards for Bristol-Myers Squibb, Roche, Elan, Eli Lilly, Eisai, and Janssen. His institutionhas received grants from Novartis and Sanofi-Aventis. Marie Sarazinreports no conflicts of interest and no financial interest. She hasreceived speaker honoraria from Eisai, Pfizer, Lundbeck, Janssen, andNovartis; she belongs to a scientific advisory board for EisaiCompany and serves as an Associate Editor for La Lettre duNeurologue. All other authors report no biomedical financialinterests or potential conflicts of interest.
1. Rascovsky K, Hodges JR, Knopman D, Mendez MF, Kramer JH,Neuhaus J, et al. (2011): Sensitivity of revised diagnostic criteria forthe behavioural variant of frontotemporal dementia. Brain 134:2456–2477.
2. Neary D, Snowden JS, Gustafson L, Passant U, Stuss D, Black S, et al.(1998): Frontotemporal lobar degeneration: A consensus on clinicaldiagnostic criteria. Neurology 51:1546–1554.
3. Graham A, Davies R, Xuereb J, Halliday G, Kril J, Creasey H, et al. (2005):Pathologically proven frontotemporal dementia presenting withsevere amnesia. Brain 128:597–605.
4. Shi J, Shaw CL, Du Plessis D, Richardson AM, Bailey KL, Julien C, et al.(2005): Histopathological changes underlying frontotemporal lobardegeneration with clinicopathological correlation. Acta Neuropathol110:501–512.
5. Hornberger M, Piguet O, Graham AJ, Nestor PJ, Hodges JR (2010): Howpreserved is episodic memory in behavioral variant frontotemporaldementia? Neurology 74:472–479.
6. Pennington C, Hodges JR, Hornberger M (2011): Neural correlates ofepisodic memory in behavioral variant frontotemporal dementia.J Alzheimers Dis 24:261–268.
7. Kipps CM, Nestor PJ, Dawson CE, Mitchell J, Hodges JR (2008):Measuring progression in frontotemporal dementia: Implications fortherapeutic interventions. Neurology 70:2046–2052.
8. Hornberger M, Piguet O (2012): Episodic memory in frontotemporaldementia: A critical review. Brain 135:678–692.
9. Hornberger M, Wong S, Tan R, Irish M, Piguet O, Kril J, et al. (2012): Invivo and post-mortem memory circuit integrity in frontotemporaldementia and Alzheimer’s disease. Brain 135:3015–3025.
10. de Souza LC, Chupin M, Bertoux M, Lehéricy S, Dubois B, Lamari F,et al. (2013): Is hippocampal volume a good marker to differentiateAlzheimer’s disease from frontotemporal dementia? J Alzheimers Dis36:57–66.
11. Barnes J, Whitwell JL, Frost C, Josephs KA, Rossor M, Fox NC (2006):Measurements of the amygdala and hippocampus in pathologicallyconfirmed Alzheimer disease and frontotemporal lobar degeneration.Arch Neurol 63:1434–1439.
12. Pasquier F, Grymonprez L, Lebert F, Van der Linden M (2001): Memoryimpairment differs in frontotemporal dementia and Alzheimer’sdisease. Neurocase 7:161–171.
13. Thomas-Anterion C, Jacquin K, Laurent B (2000): Differential mecha-nisms of impairment of remote memory in Alzheimer’s and fronto-temporal dementia. Dement Geriatr Cogn Disord 11:100–106.
14. de Souza LC, Lamari F, Belliard S, Jardel C, Houillier C, De Paz R, et al.(2011): Cerebrospinal fluid biomarkers in the differential diagnosis ofAlzheimer’s disease from other cortical dementias. J Neurol NeurosurgPsychiatry 82:240–246.
15. Folstein MF, Folstein SE, McHugh PR (1975): “Mini-mental state”.A practical method for grading the cognitive state of patients forthe clinician. J Psychiatr Res 12:189–198.
16. Mattis S (1976): Mental status examination for organic mentalsyndrome in the elderly patients. In: Bellak L, Karasu T, editors.Geriatrics Psychiatry: A Handbook for Psychiatrists and Primaty CarePhysicians. New York: Grune & Stratton, 77–121.
17. de Souza LC, Corlier F, Habert MO, Uspenskaya O, Maroy R, Lamari F,et al. (2011): Similar amyloid-beta burden in posterior cortical atrophyand Alzheimer’s disease. Brain 134:2036–2043.
18. Dubois B, Slachevsky A, Litvan I, Pillon B (2000): The FAB: A FrontalAssessment Battery at bedside. Neurology 55:1621–1626.
19. Grober E, Buschke H, Crystal H, Bang S, Dresner R (1988): Screening fordementia by memory testing. Neurology 38:900–903.
20. Nelson HE (1976): A modified card sorting test sensitive to frontal lobedefects. Cortex 12:313–324.
21. Bertoux M, Delavest M, de Souza LC, Funkiewiez A, Lépine JP, FossatiP, et al. (2012): Social cognition and emotional assessment differ-entiates frontotemporal dementia from depression. J Neurol NeurosurgPsychiatry 83:411–416.
22. Sarazin M, Berr C, De Rotrou J, Fabrigoule C, Pasquier F, Legrain S, et al.(2007): Amnestic syndrome of the medial temporal type identifiesprodromal AD: A longitudinal study. Neurology 69:1859–1867.
23. Hodges JR, Davies RR, Xuereb JH, Casey B, Broe M, Bak TH, et al.(2004): Clinicopathological correlates in frontotemporal dementia. AnnNeurol 56:399–406.
24. Mendez MF, Joshi A, Tassniyom K, Teng E, Shapira JS (2013):Clinicopathologic differences among patients with behavioral variantfrontotemporal dementia. Neurology 80:561–568.
25. Womack KB, Diaz-Arrastia R, Aizenstein HJ, Arnold SE, Barbas NR,Boeve BF, et al. (2011): Temporoparietal hypometabolism in fronto-temporal lobar degeneration and associated imaging diagnosticerrors. Arch Neurol 68:329–337.
26. Warrington EK (1984): Recognition Memory Test Manual. Windsor,England: NFER-Nelson.
27. Rey A (1964): L’examen Clinique en Psychologie. Paris: Presse Universi-taire de France.
28. Rey A (1941): L’examen psychologique dans les cas d’encéphalopathietraumatique. Archives de Psychologie 28:215–285.
29. Wechsler D (1987): Wechsler Memory Scale-Revised Manual. SanAntonio, TX: Harcourt Brace Jovanovich.
30. Sarazin M, Chauvire V, Gerardin E, Colliot O, Kinkingnéhun S,de Souza LC, et al. (2010): The amnestic syndrome of hippocampaltype in Alzheimer’s disease: An MRI study. J Alzheimers Dis 22:285–294.
31. Lindberg O, Walterfang M, Looi JC, Malykhin N, Ostberg P, Zandbelt B,et al. (2012): Hippocampal shape analysis in Alzheimer’s diseaseand frontotemporal lobar degeneration subtypes. J Alzheimers Dis 30:355–365.
32. Davatzikos C, Resnick SM, Wu X, Parmpi P, Clark CM (2008): Individualpatient diagnosis of AD and FTD via high-dimensional patternclassification of MRI. Neuroimage 41:1220–1227.
33. Rabinovici GD, Seeley WW, Kim EJ, Gorno-Tempini ML, Rascovsky K,Pagliaro TA, et al. (2007): Distinct MRI atrophy patterns in autopsy-proven Alzheimer’s disease and frontotemporal lobar degeneration.Am J Alzheimers Dis Other Demen 22:474–488.
34. Laakso MP, Frisoni GB, Kononen M, Mikkonen M, Beltramello A,Geroldi C, et al. (2000): Hippocampus and entorhinal cortex infrontotemporal dementia and Alzheimer’s disease: A morphometricMRI study. Biol Psychiatry 47:1056–1063.
35. Frisoni GB, Laakso MP, Beltramello A, Geroldi C, Bianchetti A, Soininen H,et al. (1999): Hippocampal and entorhinal cortex atrophy in frontotem-poral dementia and Alzheimer’s disease. Neurology 52:91–100.
36. Piguet O, Hornberger M, Mioshi E, Hodges JR (2011): Behavioural-variant frontotemporal dementia: Diagnosis, clinical staging, andmanagement. Lancet Neurol 10:162–172.
www.sobp.org/journal





























