Embed Size (px)
Citation preview

Updated evidence on early statin therapy for acute coronary syndromes:
International Journal of Cardiology xxx (2011) xxx–xxx
IJCA-13263; No of Pages 8
Contents lists available at ScienceDirect
International Journal of Cardiology
j ourna l homepage: www.e lsev ie r.com/ locate / i j ca rd
Meta-analysis of 18 randomized trials involving over 14,000 patients
Matthias Briel a,b,⁎,1, Noah Vale c,1, Gregory G. Schwartz d, James A. de Lemos e, Furio Colivicchi f,Frank R. den Hartog g, Petr Ostadal h, Stella M. Macin i, Anho Liem j, Ed Mills k, Neera Bhatnagar b,Heiner C. Bucher a, Alain J. Nordmann a
a Basel Institute for Clinical Epidemiology and Biostatistics, University Hospital Basel, Switzerlandb Department of Clinical Epidemiology and Biostatistics, McMaster University, Hamilton, Ontario, Canadac Department of Family Medicine, McGill University, Montreal, Quebec, Canadad VA Medical Center and University of Colorado Health Sciences Center, Denver, USAe University of Texas Southwestern Medical School, Dallas, USAf S. Filippo Neri Hospital, Rome, Italyg Gelderse Vallei Hospital, Ede, the Netherlandsh Department of Cardiology, Heart Center, Na Homolce Hospital, Prague, Czech Republici Coronary Intensive Care Unit, Instituto de Cardiología “Juana F. Cabral”, Corrientes, Argentinaj Department of Cardiology, Admiraal de Ruyter Ziekenhuis, Goes, the Netherlandsk Faculty of Health Sciences, University of Ottawa, Ottawa, Canada
a b s t r a c ta r t i c l e i n f o
Article history: Background: The short-term effects of early statin therapy in acute coronary syndromes (ACS) on clinical
Systematic reviews and meta-analyses o
265 3100; fax: +41 61 265 3109.E-mail address: [email protected] (M. Briel).
1 These authors contributed equally to the manuscrip
0167-5273/$ – see front matter © 2011 Elsevier Irelanddoi:10.1016/j.ijcard.2011.01.033
Please cite this article as: Briel M, et al, Urandomized trials involving over 14,000 pa
outcomes remain unclear. Our objective was to update the evidence on patient relevant outcomes from allrandomized trials comparing early statin therapy with placebo or usual care at 1 and 4 months following ACS.Methods:We performed a systematic review and meta-analysis of randomized trials that compared statins to
Received 6 September 2010Received in revised form 20 December 2010
Accepted 9 January 2011Available online xxxx control, initiated within 14 days after onset of ACS and with minimal follow-up of 30 days. Data wereextracted in duplicate and analyzed by a random effects model. Investigators from individual trialscontributed additional data where needed.Results: A total of 18 trials involving 14,303 patients with ACS were included in the meta-analysis. We found noevidence for further trials on the topic. Risk ratios for the combined endpoint of death,myocardial infarction, andstroke of early statin therapy compared to control were 0.93 (95% confidence interval [CI], 0.80–1.08; P=0.34)
at 1 month and 0.93 (95% CI, 0.81–1.06; P=0.27) at 4 months following ACS. There were favorable trendsrelated to statin use for all individual secondary endpoints but therewas no statistically significant risk reductionexcept for unstable angina with a risk ratio of 0.76 (95% CI, 0.59–0.96; P=0.02) at 4 months following ACS.Conclusions: Initiation of statin therapy within 14 days following ACS results in directionally favorable but non-significant reduction in death, myocardial infarction, or stroke up to 4 months, and significant reduction in theoccurrence of unstable angina at 4 months following ACS.© 2011 Elsevier Ireland Ltd. All rights reserved.
1. Introduction
benefits of early statin therapy in unstable patients with acutef randomized controlledcoronary syndrome (ACS), however, are less clear. Two previousmeta-analyses on the topic including 12 RCTs suggested that early
trials (RCTs) have provided convincing evidence that statins reducethe risk for myocardial infarction, stroke, and overall mortality inpatients at high risk for coronary heart disease, as well as in patientswith established, but stable, coronary heart disease [1–3]. The
⁎ Corresponding author. Basel Institute for Clinical Epidemiology and Biostatistics,University Hospital Basel, Hebelstrasse 10, CH-4031 Basel, Switzerland. Tel.: +41 61
t.
Ltd. All rights reserved.
pdated evidence on early stients, Int J Cardiol (2011),
treatment with statins does not reduce death, myocardial infarction,or stroke up to 4 months following ACS [4,5]. The early periodfollowing an ACS (myocardial infarction or unstable angina)represents a critical stage of coronary heart disease with a high riskfor recurrent events and death due to vessel occlusions from unstablecoronary plaques [6]. Experimental data suggest that statins have thepotential to stabilize coronary plaques, improve endothelial function,and reduce thrombus formation [7]. Hereby early ischemic eventsduring the vulnerable coronary situation following ACS which lastsabout 4 months could be reduced [8]. Recently, Morrissey et
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033

al o
al. questioned the Level of Evidence: 1A recommendation of thecurrent American College of Cardiology/American Heart Association(ACC/AHA) guidelines that statin therapy should be initiated inpatients before hospital discharge after an episode of ACS regardlessof the baseline low density lipoprotein (LDL) level because of amismatch with the underlying evidence [9].
The purpose of the present studywas to comprehensively update aprevious systematic review and meta-analysis of RCTs [4] evaluatingan early use of statins on relevant clinical endpoints of cardiovascularmorbidity and overall mortality during early stages at 1 and 4 monthsfollowing the onset of ACS. In addition, we expanded the scope of theprevious review to include data on acute heart failure and changes inhigh-sensitivity C-reactive protein (hsCRP). The quality of this evi-dence may inform guidelines like the new National CholesterolEducation Program Adult Treatment Panel (NCEP ATP IV) recommen-dations that are currently in preparation.
2. Methods
2.1. Eligibility criteria, literature search, and study selection
We included in this systematic review any RCT comparing statinwith placebo or usual care in patients with ACS (myocardial infarctionor unstable angina) provided statin therapy was initiated within14 days following the onset of ACS. The trialswere required to report atleast one clinical outcome and to have aminimal follow-up of 30 days.We excluded trials that compared two statin regimens [10–13]. Trialsusing cerivastatin [14] were only considered for sensitivity analysissince this compound was withdrawn from the market in 2001 [15].
We updated our previous search of MEDLINE, EMBASE, and theCochrane Controlled Trials Registry until February 2010 [4]. Authors ofincluded primary trials contributed additional data to this analysis.We were unable to contact investigators from 3 trials [16–18].
Two of the authors (NV, AN) independently assessed trial eli-gibility and quality. We assessed the quality of trials according toconcealment of treatment allocation; blinding of patients, caregivers,and clinical outcome assessors; the proportion of patients withcomplete clinical follow-up; and not stopping early for benefit.
2.2. Endpoints and statistical analysis
We chose the combined outcome of death from any cause, nonfatalmyocardial infarction, and nonfatal stroke, as the primary outcome.Secondary individual outcomes were death from any cause, totalmyocardial infarction, total stroke, cardiovascular death, revasculariza-tion procedures (coronary artery bypass surgery or percutaneouscoronary intervention), unstable angina (recurrentmyocardial ischemiarequiring emergency hospitalization), and new or worsening heartfailure. The vulnerable coronary situation following ACS usuallystabilizes within 3–4 months and various studies have already shownsignificant risk reductionswith long-term statin therapy on hard clinicaloutcomes such asmyocardial infarction, stroke or death in patientswithstable coronary heart disease [1,2,19,20]. Therefore, we aimed to assessall endpoints at 1 and 4 months following onset of ACS. Adverse events(rhabdomyolysis, creatinine kinase levels N10 times the upper limit ofnormal values, and liver aminotransferase levels N3 times the upperlimit of normal values) were recorded at the end of follow-up of eachtrial. In addition, we collected data on total cholesterol, LDL-cholesterol,high density lipoprotein (HDL)-cholesterol, triglycerides, and hsCRP.Two authors independently extracted all trial data and the additionaldata provided by the original investigators.
We pooled treatment effects and calculated risk ratios for allendpoints in the treatment and control groups by using a randomeffects model [21]. We investigated the presence of publication bias
2 M. Briel et al. / International Journ
by means of funnel plots [22]. We tested for heterogeneity with theCochran Q test and calculated I2 as a measure of the proportion of the
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
overall variation that is attributable to between-study heterogeneity[23]. We carried out pre-specified sensitivity analyses according toquality components (concealed treatment allocation, blinding ofpatients and caregivers, blinded outcome assessment), and weconducted a post-hoc sensitivity analysis by including unpublisheddata from one trial using cerivastatin [14]. We used Stata 9.2(StataCorp, College Station/Texas) for data analysis.
3. Results
In addition to the previous 12 trials [4] we identified 6 furtherrandomized controlled trials that fulfilled the inclusion criteria(Fig. 1). Data from the 4.5 months follow-up of a trial usingcerivastatin were excluded from the primary analysis, but includedin a sensitivity analysis [14]. The 18 RCTs enrolled a total of 14,303patients (7172 treatment, 7131 control). We found no evidence forongoing eligible trials.
Seventeen of the 18 included trials investigated four differentstatins: pravastatin (7 trials) [16,24–29], atorvastatin (4 trials) [30–33], fluvastatin (3 trials) [34–36], and simvastatin (3 trials) [18,37,38](Table 1). One trial allowed any statin to be used in the interventiongroup [17]. Analysis for publication bias indicated no evidence forsuch bias for any of the endpoints. The methodological quality ofincluded trials is summarized in Table 1. The reported mean age ofparticipants in trials ranged from 53 to 69 years (Appendix Table). Alltrials enrolled mostly men. The prevalence of individual cardiovascu-lar risk factors and co-interventions for the index event such asfibrinolysis therapy or percutaneous coronary interventions (PCI)varied considerably among included trials.
3.1. Effects on lipids and C-reactive protein
The average weighted mean baseline LDL-cholesterol level ofincluded participants was 120 mg/dL (3.1 mmol/L) (range, 78–178 mg/dL [2.0–4.6 mmol/L]) (Table 2a). Mean reduction of LDL-cholesterol ranged from 15% to 53% and total cholesterol from 9% to37%, with greater reductions in trials using higher drug doses and/ormore potent drugs. The effects on HDL-cholesterol and triglycerideswere less pronounced and inconsistent among trials.
Six trials [17,18,30,33,36,37] reported hsCRP (Table 2b). The rangeof mean baseline hsCRP in trials was 5.3 mg/L to 20 mg/L with largerreductions in statin groups during follow-up.
3.2. Effects on clinical outcomes
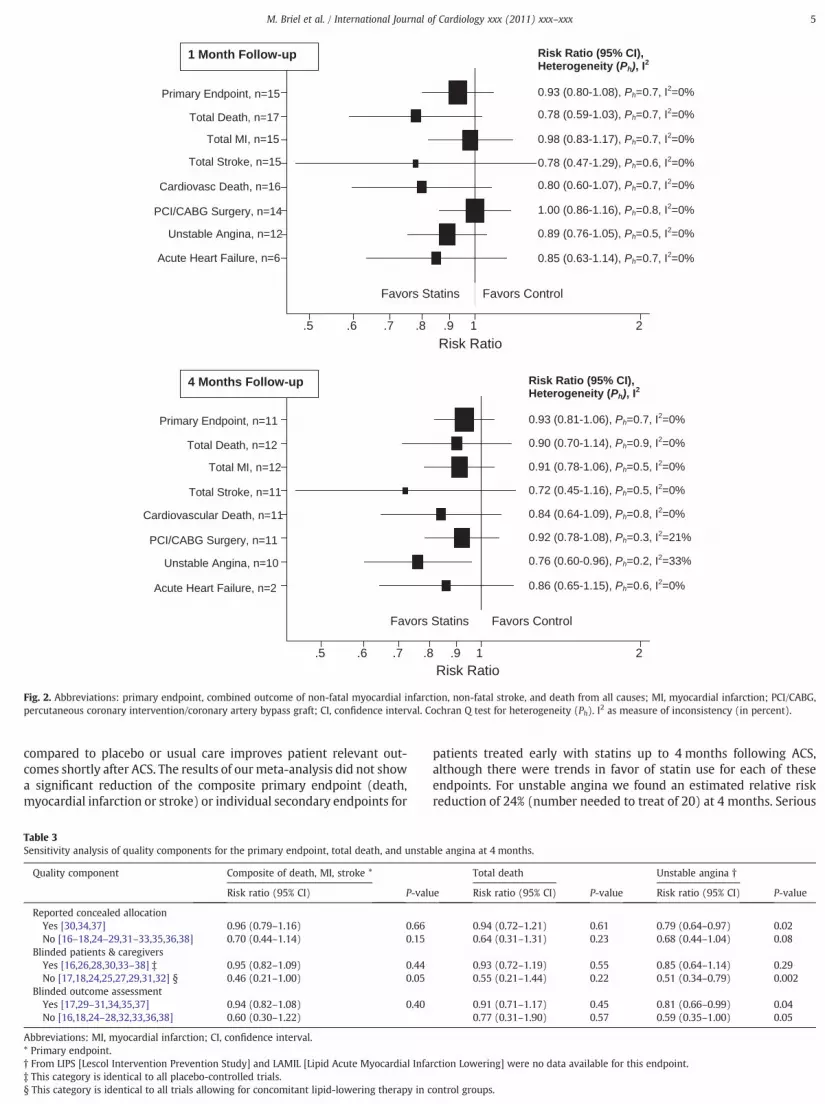
During the first month following ACS, 305 (4.5%) individuals in theearly statin groups experienced the primary composite outcome ofdeath, myocardial infarction or stroke compared to 331 (4.9%) in thecontrol groups (summary risk ratio (RR), 0.93; 95% CI, 0.80–1.08;P=0.34). At 4 months of follow-up, there were 358 (7.4%) individualsin the early statin groups with a primary endpoint event compared to385 (8.0%) in the control groups (summary RR, 0.93; 95% CI, 0.81–1.06;P=0.27) (Fig. 2). We found no evidence for relevant heterogeneityamong trials at both follow-up time points. In sensitivity analyses,summary estimates of the primary endpoint at 1 and 4 monthssuggested smaller risk reductions for trials with higher compared totrials with lower methodological quality (Table 3).
There were no statistically significant risk reductions from earlystatin therapy for total death, total myocardial infarction, total stroke,cardiovascular death, fatal or non-fatal myocardial infarction, revas-cularization procedures (PCI or coronary artery bypass grafts), new orworsening heart failure at 1 and 4 months of follow-up, and forunstable angina at 1 month follow-up, although there were favorabletrends related to statin use for each of these endpoints (Fig. 2). At
f Cardiology xxx (2011) xxx–xxx
4 months following ACS unstable angina was reduced, with 213(4.8%) of 4436 individuals experiencing unstable angina in the early
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033

2324 Potentially relevant articlesidentified and screened for retrieval
58 Full text articles retrieved for more detailed evaluation
29 Potentially appropriate RCTs to be included in the meta-analysis
19 RCTs included in the meta-analysis
18 RCTs with usable information, by outcome
29 Studies excluded, with reasons:6x no RCT, 4x follow-up <1month, 2x treatment given <1 month, 12x head-to-head comparison of statins, 5x initiation of statin therapy >14 days
1 RCT included only in a sensitivity analysis, with reason: cerivastatin withdrawn from the market.
10 RCTs excluded, with reasons: 9x no clinical outcome data, 1x unclear outcome data at pre-specified time points.
Fig. 1. Abbreviation: RCT, randomized controlled trial.
3M. Briel et al. / International Journal of Cardiology xxx (2011) xxx–xxx
statin groups compared to 275 (6.2%) of 4404 in the control groups(summary RR, 0.76; 95% CI, 0.59–0.96; P=0.02).
The heterogeneity among treatment effects was low except forunstable angina at 4 months, where we found moderate heterogene-
Table 1Characteristics of included trials.
Trial (reference) Year ofpublication
Dailyintervention
Control No. of inrandomi
LAMIL [16] 1997 Pravastatin 10–20 mg Placebo 69RECIFE [24] 1999 Pravastatin 40 mg Placebo 60L-CAD [25] 2000 Pravastatin 20–40 mg * Usual care † 126PAIS [26] 2001 Pravastatin 40 mg Placebo 99PTT [27] 2002 Pravastatin 40 mg Usual care † 164.‡PACT [28] 2004 Pravastatin 20–40 mg Placebo 3408LIPS [34] 2002 Fluvastatin 80 mg Placebo 824.§FLORIDA [35] 2002 Fluvastatin 80 mg Placebo 540MIRACL [30] 2001 Atorvastatin 80 mg Placebo 3086Colivicchi et al. [31] 2002 Atorvastatin 80 mg Usual care † 81ESTABLISH [32] 2004 Atorvastatin 20 mg Usual care † 70A to Z [37] 2004 Simvastatin 40–80 mg Placebo 4497FACS [36] 2010 Fluvastatin 80 mg Placebo 156Macin et al. [33] 2005 Atorvastatin 40 mg Placebo 90OACIS-LIPID [29] 2008 Atorvastatin 10 mg Placebo 353Ren et al. [38] 2009 Simvastatin 40 mg Placebo 86Sakamoto et al. [17] 2005 Any statin Usual care † 486Shalnev VI [18] 2007 Simvastatin 40 mg Usual care † 108
Abbreviations: ACS, acute coronary syndrome; LAMIL, Lipid Acute Myocardial Infarction LowCAD, Lipid-Coronary Artery Disease; PAIS, Pravastatin in Acute Ischemic Syndromes; PTT,Intervention Prevention Study; FLORIDA, FLuvastatin On RIsk Diminishment after Acute myoLowering; FACS, Fluvastatin in the first-line therapy of Acute Coronary Syndrome; OACIS-L* 8 of 70 individuals received additionally cholestyramine or nicotinic acid.† Individuals in the control group were allowed conventional medical treatment including‡ All 164 individuals were followed-up for 1 month, a subgroup of 77 (40/37) individuals w§ These 824 individuals represent just the subgroup with unstable angina; the LIPS [Lescolstable angina.|| After 4 months individuals in the control group received simvastatin 20 mg.
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
ity. This may be due to differences in the definition of the endpoint ofunstable angina among trials (Appendix Table).
In sensitivity analysis of secondary endpoints, trials of adequatemethodological quality were associated with smaller risk reductions
dividualszed
Initiation ofstatin afteronset of ACS(days, mean)
Duration offollow-upavailable(months)
No. (%) ofindividualsfollow-up
Reported concealedallocation/blindedpatients/caregivers/outcome assessors/notstopped early for benefit
2 1 and 3 56 (81) No/yes/yes/no/yes10 1.5 60 (100) No/yes/yes/no/yes6 1, 4 and 6 126 (100) No/no/no/no/yes2 1 and 3 97 (98) No/yes/yes/no/yes1 1 and 6 ‡ 164 (100) No/no/no/no/yes1 1 3323 (98) No/yes/yes/no/yes2 1, 4 and 6 824 (100) Yes/yes/yes/yes/yes8 1, 4 and 6 540 (100) No/yes/yes/yes/yes3 1 and 4 3075 (100) Yes/yes/yes/yes/yes
12 1, 3 and 6 81 (100) No/no/no/yes/no1 1, 4 and 6 69 (99) No/no/no/no/yes4 1 and 4 || 4453 (99) Yes/yes/yes/yes/yes1 1 and 3 156 (100) No/yes/yes/no/yes2 1 90 (100) No/yes/yes/no/yes7 1 348 (99) No/no/no/yes/yes
b3 1 86 (100) No/yes/yes/no/yesb4 Acute phase 451 (93) No/no/no/yes/yes1 6 106 (98) No/no/no/no/yes
ering; RECIFE, REduction of Cholesterol in Ischemia and Function of the Endothelium; L-Pravastatin Turkish Trial; PACT, Pravastatin in Acute Coronary Treatment; LIPS, Lescolcardial infarction; MIRACL, Myocardial Ischemia Reduction with Aggressive CholesterolIPID, Osaka Acute Coronary Insufficiency Study-LIPID.
lipid-lowering therapy.ith additional coronary angioplasty were followed-up for 6 months.Intervention Prevention Study]-trial originally included another 853 individuals with
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033

Table 2aLipid values at baseline and changes during follow-up.
Trial (reference) Intervention Follow-up * Total cholesterol LDL-cholesterol HDL-cholesterol Triglycerides
Baseline mean, mg/dL(% mean change in difference between treatment and control groups) †
LAMIL [16] Pravastatin 10–20 mg 3 months 228 (−13) 158 (−23) 36 (+5.3) NARECIFE [24] Pravastatin 40 mg 1.5 months 247 (−21) 164 (−27) 42 (+13) 194 (−21)L-CAD [25] ‡ Pravastatin 20–40 mg 1 month 237 (−24) 178 (−25) 32 (−6.0) NAPAIS [26] Pravastatin 40 mg 3 months 255 (−23) 176 (−24) 43 (+9.1) 199 (−13)PTT [27] ‡ Pravastatin 40 mg 1 month 230 (−12) 133 (−25) 39 (+3.0) 214 (−5.8)PACT [28] Pravastatin 20–40 mg NA 219 (NA) NA NA NALIPS [34] Fluvastatin 80 mg 1.5 months 201 (−28) 131 (−39) 39 (−2.0) 155 (−21)FLORIDA [35] Fluvastatin 80 mg 12 months 207 (−22) 137 (−31) 46 (+3.3) 146 (−22)MIRACL [30] Atorvastatin 80 mg 1.5 months 206 (−37) 124 (−53) 47 (±0) 183 (−28)Colivicchi et al. [31]‡ Atorvastatin 80 mg 2 months 220 (−9) 131 (−15) 39 (+1.0) 167 (−13)ESTABLISH [32] ‡ Atorvastatin 20 mg 6 months 191 (−28) 124 (−41) 44 (−8.7) 109 (+4.9)A-to-Z [37] Simvastatin 40–80 mg 1 month 184 (−33) 113 (−45) 39 (+2.0) 149 (−22)FACS [36] Fluvastatin 80 mg 1 month 212 (−26) 135 (−31) 47 (−4.1) 162 (+10)Macin et al. [33] Atrovastain 40 mg 1 month 194 (−19) 124 (−30) 37 (+11) 189 (+0.8)OACIS-LIPID [29] Pravastatin 10 mg 9 months 220 (NA) 49 (NA) 117 (NA) 148 (NA)Ren et al. [38] Simvastatin 40 mg 1 month 228 (−23%) 139 (−31) 40 (+9.6) NASakamoto et al. [17] Any Statin 3 months 207 (−12) 134 (−23) 47 (+2.2) 135 (−5.2)Shalnev VI [18] Simvastatin 40 mg 0.5 months 212 (−29) 131 (−46) 49 (−9.5) 146 (−15)
Abbreviations: NA, not available; LDL, low density lipoprotein; HDL, high density lipoprotein. See Table 1 footnote for expansions of trial names.* Lipid values in individual trials were measured at different time points during follow-up; we report those closest to the 4 months follow-up date.† Baseline lipid levels were defined as the average (mean) before treatment in intervention and control groups. The percentage of change for each trial was calculated as thedifference in the mean change in lipid levels from baseline to follow-up in the intervention and the control groups. To convert from mg/dL to mmol/L, multiply by 0.02586 forcholesterol and by 0.01129 for triglycerides.
ing
4 M. Briel et al. / International Journal of Cardiology xxx (2011) xxx–xxx
than trials lacking quality components (Table 3). However, forunstable angina we found statistically significant risk reductionsfrom statins at 4 months in trials that reported concealed allocationand in trials with blinded outcome assessment.
Whenwe additionally included 4.5 month data from 3605 patientswith ACS from PRINCESS [Prevention of Ischemic Events by EarlyTreatment of Cerivastatin Study] in sensitivity analysis, summary RRwere 0.95 (95% CI, 0.78–1.17; P=0.65) for total mortality, 0.90 (95%CI, 0.78–1.03; P=0.13) for total myocardial infarction, 0.79 (95% CI,0.52–1.18; P=0.25) for total stroke, and 0.78 (95% CI, 0.65–0.95;P=0.01) for unstable angina.
3.3. Adverse events
‡ Individuals in the control group were allowed conventional medical treatment includ
Among all included trials, only 3 incidents of rhabdomyolysis werereported (0.04%) in patients treated with statins; all occurred with
Table 2bC-reactive protein levels at baseline and changes during follow-up.
Trial (reference) Intervention F
MIRACL [30] Atorvastatin 80 mg B4C
A-to-Z [37] Simvastatin 40–80 mg B1C4C
Sakamoto et al. [17] Any statin B1C6C
Macin et al. [33] Atorvastatin 40 mg B1C
FACS [36] Fluvastatin 80 mg B1C
Shal'nev et al. [18] Simvastatin 40 mg B2C
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
simvastatin 80 mg in the A to Z trial [37]. There were 9 individualswithmyopathy (elevated creatinine kinase levels N10 times the upperlimit of normal) in the statin groups versus 1 in the control groups(0.13% versus 0.015%); the summary RR for myopathy was signifi-cantly higher with statins than with control (RR 4.69, 95% CI 1.01–21.67; P=0.05). All 9 cases occurred beyond the first month of statintreatment and 7 of the 9 patients were treated with high dosesimvastatin (80 mg/d). None of the 9 patients died. The risk forelevated liver aminotransferase levels (ALT N3 times the upper limitof normal) was significantly higher in the early statin groups than inthe control groups (1.1% vs 0.4%; RR 2.49, 95% CI 1.16–5.32; P=0.02).
4. Discussion
lipid-lowering therapy.
This systematic review of 18 randomized controlled trials in over14,000 patients with ACS investigated whether early statin therapy
ollow-up Statin Control
aseline (mean, mg/L) 11.5 11.0months (mean, mg/L) 1.9 2.9hange (%) −83.% −74.%aseline (mean, mg/L) 20.1 20.4month (mean, mg/L) 2.4 2.5hange (%) −88.% −88.%months (mean, mg/L) 1.7 2.3hange (%) −92.% −89.%aseline (mean, mg/L) 5.33 5.43month (mean, mg/L) 4.62 5.26hange (%) −13.% −3.1%months (mean, mg/L) 1.71 2.57hange (%) −68.% −53.%aseline (mean, mg/L) 5.97 4.64month (mean, mg/L) 0.50 2.91hange (%) −92.% −37.%aseline (mean, mg/L) 17.57 8.27month (mean, mg/L) 3.17 4.83hange (%) −82.% −42.%aseline (mean, mg/L) 14.90 16.10weeks (mean, mg/L) 7.60 13.2hange (%) −49.% −18.%
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033
.5 .6 .7 .8 .9 1 2
Acute Heart Failure, n=6
Unstable Angina, n=12
PCI/CABG Surgery, n=14
Cardiovasc Death, n=16
Total Stroke, n=15
Total MI, n=15
Total Death, n=17
Primary Endpoint, n=15
Risk Ratio
Favors Statins Favors Control
1 Month Follow-up Risk Ratio (95% CI), Heterogeneity (Ph), I2
0.93 (0.80-1.08), Ph=0.7, I2=0%
0.78 (0.59-1.03), Ph=0.7, I2=0%
0.98 (0.83-1.17), Ph=0.7, I2=0%
0.78 (0.47-1.29), Ph=0.6, I2=0%
0.80 (0.60-1.07), Ph=0.7, I2=0%
1.00 (0.86-1.16), Ph=0.8, I2=0%
0.89 (0.76-1.05), Ph=0.5, I2=0%
0.85 (0.63-1.14), Ph=0.7, I2=0%
.5 .6 .7 .8 .9 1 2
Acute Heart Failure, n=2
Unstable Angina, n=10
PCI/CABG Surgery, n=11
Cardiovascular Death, n=11
Total Stroke, n=11
Total MI, n=12
Total Death, n=12
Primary Endpoint, n=11
Risk Ratio (95% CI), Heterogeneity (Ph), I2
0.93 (0.81-1.06), Ph=0.7, I2=0%
0.90 (0.70-1.14), Ph=0.9, I2=0%
0.91 (0.78-1.06), Ph=0.5, I2=0%
0.72 (0.45-1.16), Ph=0.5, I2=0%
0.84 (0.64-1.09), Ph=0.8, I2=0%
0.92 (0.78-1.08), Ph=0.3, I2=21%
0.76 (0.60-0.96), Ph=0.2, I2=33%
0.86 (0.65-1.15), Ph=0.6, I2=0%
4 Months Follow-up
Favors Statins Favors Control
Risk Ratio
Fig. 2. Abbreviations: primary endpoint, combined outcome of non-fatal myocardial infarction, non-fatal stroke, and death from all causes; MI, myocardial infarction; PCI/CABG,al. C 2
5M. Briel et al. / International Journal of Cardiology xxx (2011) xxx–xxx
compared to placebo or usual care improves patient relevant out-comes shortly after ACS. The results of our meta-analysis did not show
percutaneous coronary intervention/coronary artery bypass graft; CI, confidence interv
a significant reduction of the composite primary endpoint (death,myocardial infarction or stroke) or individual secondary endpoints for
Table 3Sensitivity analysis of quality components for the primary endpoint, total death, and unsta
Quality component Composite of death, MI, stroke *
Risk ratio (95% CI) P-valu
Reported concealed allocationYes [30,34,37] 0.96 (0.79–1.16) 0.66No [16–18,24–29,31–33,35,36,38] 0.70 (0.44–1.14) 0.15
Blinded patients & caregiversYes [16,26,28,30,33–38] ‡ 0.95 (0.82–1.09) 0.44No [17,18,24,25,27,29,31,32] § 0.46 (0.21–1.00) 0.05
Blinded outcome assessmentYes [17,29–31,34,35,37] 0.94 (0.82–1.08) 0.40No [16,18,24–28,32,33,36,38] 0.60 (0.30–1.22)
Abbreviations: MI, myocardial infarction; CI, confidence interval.* Primary endpoint.† From LIPS [Lescol Intervention Prevention Study] and LAMIL [Lipid Acute Myocardial Infa‡ This category is identical to all placebo-controlled trials.§ This category is identical to all trials allowing for concomitant lipid-lowering therapy in c
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
patients treated early with statins up to 4 months following ACS,although there were trends in favor of statin use for each of these
ochran Q test for heterogeneity (Ph). I as measure of inconsistency (in percent).
endpoints. For unstable angina we found an estimated relative riskreduction of 24% (number needed to treat of 20) at 4 months. Serious
ble angina at 4 months.
Total death Unstable angina †
e Risk ratio (95% CI) P-value Risk ratio (95% CI) P-value
0.94 (0.72–1.21) 0.61 0.79 (0.64–0.97) 0.020.64 (0.31–1.31) 0.23 0.68 (0.44–1.04) 0.08
0.93 (0.72–1.19) 0.55 0.85 (0.64–1.14) 0.290.55 (0.21–1.44) 0.22 0.51 (0.34–0.79) 0.002
0.91 (0.71–1.17) 0.45 0.81 (0.66–0.99) 0.040.77 (0.31–1.90) 0.57 0.59 (0.35–1.00) 0.05
rction Lowering] were no data available for this endpoint.
ontrol groups.
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033

al o
side effects from early treatment with statins were rare (0.1%), andserious muscle toxicity was mostly observed with simvastatin 80 mg.Early statin therapy effectively reduced LDL-cholesterol and hsCRP.
The present study updates and expands the scope of a previoussystematic review [4] by including an additional 6 trials and ad-ditional data on acute heart failure and changes in hsCRP. Wecomprehensively searched trial registries and found no evidence forongoing eligible trials. Thus, the summarized trials in this review mayconstitute the totality of the available evidence on the topic.
Our study has the following strengths and limitations. We haveconducted an extensive literature search to retrieve all relevanteligible trials and collaborated with experts in the field to minimizepublication bias. Formal testing indicated little evidence for such bias.We were unable to include one small trial with 151 randomizedindividuals because the original investigators failed to clarify outcomeevents [39]. Two other trials including 3468 patients had only afollow-up of 1 [28] and 1.5 months [24]. As a consequence, the powerof our analysis at 4 months, was compromised.
It may well be that early use of statins in ACS is associated with abeneficial effect on total mortality, myocardial infarction and stroke inthe short-term; summary estimates for all efficacy outcomes show atrend towards risk reduction with early statin therapy, but this meta-analysis may lack the power to detect a significant risk reduction forhard outcomes. Our sensitivity analyses indicated smaller treatmenteffects when restricting the analysis to trials of adequate methodo-logical quality, or when we additionally included secondary endpointdata from a large, prematurely terminated trial using cerivastatin in3605 patients [14]. To rule out effects of 10% risk reduction or less onour combined primary endpoint (death, MI, and stroke), more than34,000 patients with ACS would need to be randomized [40].
As expected, statins lowered LDL-cholesterol and hsCRP levels moreefficiently than placebo or usual care. There were larger reductions inLDL cholesterol in trials usinghigher doses of statins. However, availabledata precluded adequate exploration of an association between clinicaloutcomes and lipid-lowering or C-reactive protein lowering potency ofdifferent statin types and doses. Finally, this systematic review cannotaddress the benefit of the use of early statins in patients with ACSundergoing early PCI of culprit lesions, since only a minority of patientsof included trials underwent PCI.
Statins impact lipid profiles within days, [41] and in vitro studiesshow immediate inhibition of smooth-muscle cell proliferation andstimulation of re-endothelialization by statins [42]. Similarly, statinsreduce high-sensitivity C-reactive protein and have demonstrated avariety of anti-inflammatory effects in vitro [43,44]. These anti-inflammatory effects may translate into a reduction of unstable anginapectoris at 4 months following ACS, but why should effects on unstableangina be stronger than effects on myocardial infarction? One couldargue that statins might ameliorate coronary vascular endothelialdysfunction, but that doing so does not directly influence atherothrom-bosis. Or one might also posit that there actually are concordant effectson all of these endpoints (trends are all in a favorable direction withstatins), but the composite sample size and duration of observation inthis group of trials are inadequate to ascertain an effect with sufficientlylow type I error rate. Another important point is the biomarkermethodsused for ascertainment of MI in many of these studies. In the late 1990sor even early 2000s,many sites continued to use CK-MBor even total CKas the biomarker to detect myocardial injury. Multicenter trialsgenerally do not specify one biomarker to define myocardial injury inendpoint events. Thus many endpoint events that would be associatedwith a small rise in troponin and today be categorized as acute MIaccording to the current International Definition of MyocardialInfarction [45] were likely to have been considered biomarker negativeand categorized as unstable angina using the older and less sensitivebiomarker methods prevalent during the conduct of the trials in
6 M. Briel et al. / International Journ
question. Therefore, one might reasonably expect that had contempo-rary diagnostic criteria andmethods been applied to the events in these
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
trials, there might have been more events categorized as acute MI (andfewer as unstable angina), affording greater power to detect an effect ofearly statin therapy on acute MI. Finally, it should be noted that of theevents that occurred within the 4 month follow up period, 86% wererecorded within the first month of treatment. These very early eventsmay be mediated to a greater extent than are later events bycharacteristics of the index ACS presentation such as the extent andcomplexity of coronary artery disease, as well as acute treatment withregard to use of antiplatelet and antithrombotic therapies and earlycoronary revascularization. Thus, very early events may be lessmodifiable with statin therapy than later events.
In our meta-analysis we considered only endpoint events thatoccurred during the period of randomized treatment. It is likely thatthe beneficial effects of statins are cumulative. In most of the land-mark trials of statins in patients with chronic coronary artery disease abenefit of treatment was not evident until 1–2 years after random-ization [19,20]. Similarly, there appeared to be a delayed benefit ofmore intensive statin treatment, compared to less intensive statintreatment, in the late phase of the A to Z trial [37]. Therefore, some ofthe benefit of statin treatment in the period up to 4 months after ACSmay only become manifested after 4 months.
This systematic review confirms that early treatment with statinsin ACS can, in general, be considered to be safe even when high dosesof statins are used. However, physicians and patients should pay closeattention to muscle-related symptoms, especially when maximumavailable doses – in particular of simvastatin 80 mg – are administered[46]. A specific caveat about simvastatin 80 mg has not yet beenadopted by current guidelines [47,48].
There are concerns thatwhen administered in clinical practice, long-term adherence to statins among patients with recent onset of ACS ispoor [49]. Evidence from a small randomized trial and from observa-tional studies suggests improved adherence to statins when therapy isstarted in-hospital shortly after an acute event rather than later duringfollow-up [50,51]. A large, population-based longitudinal observationalstudy showed that adherence to statin therapy was associated withimproved survival [52]. Thus, even if the early benefits of statin therapyare modest, it may be important to initiate them early to ensure long-term benefits are achieved. These arguments provide the basis torecommend initiation of statins before hospital discharge in all patientswith ACS which is in line with current ACC/AHA treatment guidelines[47,48]. Starting statin therapy before hospital discharge has recentlybecome formally endorsed as a performance measure for patients withacute ST-elevation and non-ST-elevation myocardial infarction [53].
In summary, basedon abodyof evidence including18RCTs initiationof statin therapy within 14 days following ACS produces favorabletrends but does not significantly reduce death, myocardial infarction, orstroke up to 4 months after the index event. Early initiation of statintherapy does significantly reduce the occurrence of unstable angina at4 months following ACS. Serious muscle toxicity was more commonwith early statin therapy than with placebo, but was rare and mostlylimited to treatment with simvastatin 80 mg. Taking into considerationthe long-term benefit of statin therapy in coronary artery disease, earlystatin therapy should be recommended to patients hospitalized for ACS.
Financial disclosures
Dr Schwartz has received research support from Pfizer. Dr de Lemoshas received honoraria from Bristol-Myers Squibb. Dr. Ostadal hasreceived honoraria and research support from Pfizer and Novartis. DrBucherhas receivedgrant support fromMerckandBristol-Myers Squibb.
Funding/support
Dr Briel, Dr Nordmann andDr Bucher are supported by Santésuisse,
f Cardiology xxx (2011) xxx–xxx
Solothurn, Switzerland, and the Gottfried and Julia Bangerter-Rhyner-Foundation, Berne, Switzerland.
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033

nal o
Role of the sponsor
Santésuisse, and the Gottfried and Julia Bangerter-Rhyner-Foundationhad no role in the design and conduct of the study; the collection,management, analysis, and interpretationof the study; or thepreparation,review, or approval of the manuscript.
Acknowledgment
We would like to thank all investigators of original trials whoprovided additional unpublished data for this study.
The authors of this manuscript have certified that they complywith the Principles of Ethical Publishing in the International Journal ofCardiology [54].
Appendix A. Supplementary data
Supplementary data to this article can be found online atdoi:10.1016/j.ijcard.2011.01.033.
References
[1] Studer M, Briel M, Leimenstoll B, Glass TR, Bucher HC. Effect of differentantilipidemic agents and diets on mortality: a systematic review. Arch InternMed 2005;165:725–30.
[2] Briel M, Studer M, Glass TR, Bucher HC. Effects of statins on stroke prevention inpatients with and without coronary heart disease: a meta-analysis of randomizedcontrolled trials. Am J Med 2004;117:596–606.
[3] Baigent C, Keech A, Kearney PM, et al. Efficacy and safety of cholesterol-loweringtreatment: prospective meta-analysis of data from 90, 056 participants in 14randomised trials of statins. Lancet 2005;366:1267–78.
[4] Briel M, Schwartz GG, Thompson PL, et al. Effects of early treatment with statins onshort-term clinical outcomes in acute coronary syndromes: a meta-analysis ofrandomized controlled trials. JAMA 2006;295:2046–56.
[5] Hulten E, Jackson JL, Douglas K, George S, Villines TC. The effect of early, intensivestatin therapy on acute coronary syndrome: a meta-analysis of randomizedcontrolled trials. Arch Intern Med 2006;166:1814–21.
[6] Wood D, de Backer G, Faergeman O, et al. Prevention of coronary heart disease inclinical practice. Recommendations of the Second Joint Task Force of European andother Societies on coronary prevention. Eur Heart J 1998;19:1434–503.
[7] Sposito AC, ChapmanMJ. Statin therapy in acute coronary syndromes: mechanisticinsight into clinical benefit. Arterioscler Thromb Vasc Biol 2002;22:1524–34.
[8] Schwartz GG, Oliver MF, Ezekowitz MD, et al. Rationale and design of theMyocardial Ischemia Reduction with Aggressive Cholesterol Lowering (MIRACL)study that evaluates atorvastatin in unstable angina pectoris and in non-Q-waveacute myocardial infarction. Am J Cardiol 1998;81:578–81.
[9] Morrissey RP, Diamond GA, Kaul S. Statins in acute coronary syndromes: do theguideline recommendations match the evidence? J Am Coll Cardiol 2009;54:1425–33.
[10] Cannon CP, Braunwald E, McCabe CH, et al. Intensive versus moderate lipidlowering with statins after acute coronary syndromes. N Engl J Med 2004;350:1495–504.
[11] Hiro T, Kimura T, Morimoto T, et al. Effect of intensive statin therapy on regressionof coronary atherosclerosis in patients with acute coronary syndrome: amulticenter randomized trial evaluated by volumetric intravascular ultrasoundusing pitavastatin versus atorvastatin (JAPAN-ACS [Japan assessment of pitavas-tatin and atorvastatin in acute coronary syndrome] study). J Am Coll Cardiol2009;54:293–302.
[12] Pitt B, Loscalzo J, Ycas J, Raichlen JS. Lipid levels after acute coronary syndromes. JAm Coll Cardiol 2008;51:1440–5.
[13] Colivicchi F, Tubaro M, Mocini D, et al. Full-dose atorvastatin versus conventionalmedical therapy after non-ST-elevation acute myocardial infarction in patientswith advanced non-revascularisable coronary artery disease. Curr Med Res Opin2010;26:1277–84.
[14] Wright RS, JukemaW, LaBlanche JM. PRINCESS: prevention of ischaemic events byearly treatment of cerivastatin after acute myocardial infarction. European Societyof Cardiology, Hot Line Session III; 2004. http://cic.escardio.org/SessionDetails.aspx?id=40551.
[15] Staffa JA, Chang J, Green L. Cerivastatin and reports of fatal rhabdomyolysis. N EnglJ Med 2002;346:539–40.
[16] Kesteloot H, Claeys G, Blanckaert N, Lesaffre E. Time course of serum lipids andapolipoproteins after acute myocardial infarction: modification by pravastatin.Acta Cardiol 1997;52:107–16.
[17] Sakamoto T, Kojima S, Ogawa H, et al. Effects of early statin treatment onsymptomatic heart failure and ischemic events after acute myocardial infarctionin Japanese. Am J Cardiol 2006;97:1165–71.
[18] Shal'nev VI. The effects of early application of simvastatin on C-reactive protein
M. Briel et al. / International Jour
level, blood lipids, and the clinical course of acutecoronary syndrome. Klin Med2007;85:46–50.
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
[19] Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterollowering in 4444 patients with coronary heart disease: the ScandinavianSimvastatin Survival Study (4 S). Lancet 1994;344:1383–9.
[20] The Long-term Intervention with Pravastatin in Ischaemic Disease (LIPID) StudyGroup. Prevention of cardiovascular events and death with pravastatin in patientswith coronary heart disease and a broad range of initial cholesterol levels. N Engl JMed 1998;339:1349–57.
[21] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin Trials 1986;7:177–88.
[22] Sterne JA, Egger M, Smith GD. Systematic reviews in health care: Investigating anddealing with publication and other biases in meta-analysis. BMJ 2001;323:101–5.
[23] Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60.
[24] Dupuis J, Tardif JC, Cernacek P, Theroux P. Cholesterol reduction rapidly improvesendothelial function after acute coronary syndromes. The RECIFE (reduction ofcholesterol in ischemia and function of the endothelium) trial. Circulation1999;99:3227–33.
[25] Arntz HR, Agrawal R, Wunderlich W, et al. Beneficial effects of pravastatin (+/−colestyramine/niacin) initiated immediately after a coronary event (therandomized Lipid-Coronary Artery Disease [L-CAD] Study). Am J Cardiol2000;86:1293–8.
[26] Den Hartog FR, Van Kalmthout PM, Van Loenhout TT, Schaafsma HJ, Rila H,Verheugt FW. Pravastatin in acute ischaemic syndromes: results of a randomisedplacebo-controlled trial. Int J Clin Pract 2001;55:300–4.
[27] Kayikcioglu M, Can L, Kultursay H, Payzin S, Turkoglu C. Early use of pravastatin inpatients with acute myocardial infarction undergoing coronary angioplasty. ActaCardiol 2002;57:295–302.
[28] Thompson PL, Meredith I, Amerena J, Campbell TJ, Sloman JG, Harris PJ. Effect ofpravastatin compared with placebo initiated within 24 hours of onset of acutemyocardial infarction or unstable angina: the Pravastatin in Acute CoronaryTreatment (PACT) trial. Am Heart J 2004;148:e2.
[29] Sato H, Kinjo K, Ito H, et al. Effect of early use of low-dose pravastatin on majoradverse cardiac events in patients with acute myocardial infarction: the OACIS-LIPID Study. Circ J 2008;72:17–22.
[30] Schwartz GG, Olsson AG, Ezekowitz MD, et al. Effects of atorvastatin on earlyrecurrent ischemic events in acute coronary syndromes: the MIRACL study: arandomized controlled trial. JAMA 2001;285:1711–8.
[31] Colivicchi F, Guido V, Tubaro M, et al. Effects of atorvastatin 80 mg daily early afteronset of unstable angina pectoris or non-Q-wave myocardial infarction. Am JCardiol 2002;90:872–4.
[32] Okazaki S, Yokoyama T, Miyauchi K, et al. Early statin treatment in patients withacute coronary syndrome: demonstration of the beneficial effect on atheroscle-rotic lesions by serial volumetric intravascular ultrasound analysis during half ayear after coronary event: the ESTABLISH Study. Circulation 2004;110:1061–8.
[33] Macin SM, Perna ER, Farias EF, et al. Atorvastatin has an important acute anti-inflammatory effect in patients with acute coronary syndrome: results of arandomized, double-blind, placebo-controlled study. Am Heart J 2005;149:451–7.
[34] Serruys PW, de Feyter P, Macaya C, et al. Fluvastatin for prevention of cardiacevents following successful first percutaneous coronary intervention: a random-ized controlled trial. JAMA 2002;287:3215–22.
[35] Liem AH, van Boven AJ, Veeger NJ, et al. Effect of fluvastatin on ischaemia followingacute myocardial infarction: a randomized trial. Eur Heart J 2002;23:1931–7.
[36] Ostadal P, Alan D, Vejvoda J, et al. Fluvastatin in the first-line therapy of acutecoronary syndrome: results of the multicenter, randomized, double-blind,placebo-controlled trial (the FACS-trial). Trials 2010;11:61.
[37] De Lemos JA, Blazing MA, Wiviott SD, et al. Early Intensive vs a DelayedConservative Simvastatin Strategy in Patients With Acute Coronary Syndromes:phase Z of the A to Z Trial. JAMA 2004;292:1307–16.
[38] Ren HZ, Ma LL, Wang LX. Effect of simvastatin on plasma interleukin-6 in patientswith unstable angina. Clin Invest Med 2009;32:E280–4.
[39] Pedersen TR, Jahnsen KE, Vatn S, et al. Benefits of early lipid-lowering interventionin high-risk patients: the lipid intervention strategies for coronary patients study.Clin Ther 2000;22:949–60.
[40] Lachin JM. Sample size, power, and efficiency. In: Lachin JM, editor. BiostatisticalMethods. New York, NY: John Wiley & Sons; 2000.
[41] Correia LC, Sposito AC, Passos LC, et al. Short-term effect of atorvastatin (80 mg)on plasma lipids of patients with unstable angina pectoris or non-Q-wave acutemyocardial infarction. Am J Cardiol 2002;90:162–4.
[42] Walter DH. Insights into early and rapid effects of statin therapy after coronaryinterventions. Curr Pharm Des 2004;10:369–73.
[43] Bustos C, Hernandez-Presa MA, Ortego M, et al. HMG-CoA reductase inhibition byatorvastatin reduces neointimal inflammation in a rabbit model of atherosclerosis.J Am Coll Cardiol 1998;32:2057–64.
[44] Rosenson RS, Tangney CC, Casey LC. Inhibition of proinflammatory cytokineproduction by pravastatin. Lancet 1999;353:983–4.
[45] Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. EurHeart J 2007;28:2525–38.
[46] Ara R, Pandor A, Stevens J, Rees A, Rafia R. Early high-dose lipid-lowering therapyto avoid cardiac events: a systematic review and economic evaluation. HealthTechnol Assess 2009;13:1–118.
[47] Antman EM, Hand M, Armstrong PW, et al. 2007 focused update of the ACC/AHA2004 guidelines for the management of patients with ST-elevation myocardialinfarction: a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines. J Am Coll Cardiol 2008;51:210–47.
7f Cardiology xxx (2011) xxx–xxx
[48] Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for themanagement of patients with unstable angina/non-ST-Elevation myocardial
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033

infarction: a report of the American College of Cardiology/American HeartAssociation Task Force on Practice Guidelines (Writing Committee to Revise the2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the AmericanCollege of Emergency Physicians, the Society for Cardiovascular Angiography andInterventions, and the Society of Thoracic Surgeons endorsed by the AmericanAssociation of Cardiovascular and Pulmonary Rehabilitation and the Society forAcademic Emergency Medicine. J Am Coll Cardiol 2007;50:e1–e157.
[49] Jackevicius CA, Mamdani M, Tu JV. Adherence with statin therapy in elderlypatients with and without acute coronary syndromes. JAMA 2002;288:462–7.
[50] Nordmann A, Blattmann L, Gallino A, et al. Systematic, immediate in-hospitalinitiation of lipid-lowering drugs during acute coronary events improves lipidcontrol. Eur J Intern Med 2000;11:309–16.
[51] Smith CS, Cannon CP, McCabe CH, Murphy SA, Bentley J, Braunwald E. Earlyinitiation of lipid-lowering therapy for acute coronary syndromes improvescompliance with guideline recommendations: observations from the Orbofiban inPatients with Unstable Coronary Syndromes (OPUS-TIMI 16) trial. Am Heart J2005;149:444–50.
8 M. Briel et al. / International Journal o
Please cite this article as: Briel M, et al, Updated evidence on early srandomized trials involving over 14,000 patients, Int J Cardiol (2011),
[52] Rasmussen JN, Chong A, Alter DA. Relationship between adherence to evidence-based pharmacotherapy and long-term mortality after acute myocardial infarc-tion. JAMA 2007;297:177–86.
[53] Krumholz HM, Anderson JL, Bachelder BL, et al. ACC/AHA 2008 performancemeasures for adults with ST-elevation and non-ST-elevation myocardial infarc-tion: a report of the American College of Cardiology/American Heart AssociationTask Force on Performance Measures (Writing Committee to Develop Perfor-mance Measures for ST-Elevation and Non-ST-Elevation Myocardial Infarction)Developed in Collaboration With the American Academy of Family Physicians andAmerican College of Emergency Physicians Endorsed by the American Associationof Cardiovascular and Pulmonary Rehabilitation, Society for CardiovascularAngiography and Interventions, and Society of Hospital Medicine. J Am CollCardiol 2008;52:2046–99.
[54] Shewan LG and Coats AJ. Ethics in the authorship and publishing of scientificarticles. Int J Cardiol 2010;144:1–2.
f Cardiology xxx (2011) xxx–xxx
tatin therapy for acute coronary syndromes: Meta-analysis of 18doi:10.1016/j.ijcard.2011.01.033





























