Embed Size (px)
Citation preview

R
U
TGa
b
Oc
d
a
ARA
KAUUDMAAT
1
mwfdrfgiiipo
tIc
oT
0d
European Journal of Radiology 71 (2009) 197–203
Contents lists available at ScienceDirect
European Journal of Radiology
journa l homepage: www.e lsev ier .com/ locate /e j rad
eview
S guided injections in arthritis
obias De Zordoa,b, Erich Murc, Rosa Bellmann-Weilerc, Michaela Sailer-Höckd, Rethy Chhemb,udrun M. Feuchtnera, Werner Jaschkea, Andrea S. Klausera,∗
Department of Diagnostic Radiology, Medical University Innsbruck, Anichstrasse 35, 6020 Innsbruck, AustriaDepartment of Diagnostic Radiology, University of Western Ontario, London Health Science Centre - University Hospital, 339 Windermere Road, London,ntario, Canada N6A 5A5Department of Internal Medicine, Medical University Innsbruck, Anichstrasse 35, 6020 Innsbruck, AustriaDepartment of Pediatrics, Medical University Innsbruck, Anichstrasse 35, 6020 Innsbruck, Austria
r t i c l e i n f o
rticle history:eceived 15 April 2009ccepted 16 April 2009
eywords:
a b s t r a c t
US guided procedures for diagnosis or treatment of different forms of arthritis are becoming more andmore important. This review describes general considerations for fluid aspiration, articular or periarticularinjections and biopsies by US guidance according to the recent literature. Guidelines regarding instrumen-tation, different techniques, pre- and postprocedural care as well as complications are outlined and in thesecond part a more detailed overview of different interventions in joints, tendons and other periarticular
rthritisltrasoundS guided injectionisease activityinimal invasive
spirationrthritis
regions (nerves, bursae, etc.) is included. Furthermore, some newer, more sophisticated techniques arebriefly discussed.
© 2009 Elsevier Ireland Ltd. All rights reserved.
enosynovitis
. Introduction
US is a readily available, non-ionizing, lower cost imagingodality for evaluating arthritis, which has improved significantlyith the use of newer high-frequency probes and diagnostic use-
ulness in arthritis has been described in many studies. However,ifferentiation between different forms of arthritis sometimesemains challenging and joint aspiration or biopsy has to be per-ormed. Although clinically guided techniques, using palpation asuidance, are mainly used by orthopedists and rheumatologists, its known that reliability of intra-articular localization of the needles relatively low [1,2]. However, it has already been stated that USs an excellent tool for guiding minimally invasive interventionalrocedures in the musculoskeletal system, when lesions are visiblen US [3–7].
On the other hand, US guided interventions can also be used forreatment of arthritis besides physical therapies and oral therapies.ntra-articular administration of anti-inflammatory drugs, espe-ially corticosteroids, is widely used as an alternative or adjunct
∗ Corresponding author at: Department of Diagnostic Radiology, Diagnostic Radi-logy II, Medical University Innsbruck, Anichstrasse 35, 6020 Innsbruck, Austria.el.: +43 512 504 81923; fax: +43 512 504 27006.
E-mail address: [email protected] (Andrea S. Klauser).
720-048X/$ – see front matter © 2009 Elsevier Ireland Ltd. All rights reserved.oi:10.1016/j.ejrad.2009.04.047
treatment in many forms of arthritis (e.g. rheumatoid arthritis,spondyloarthritis, and osteoarthritis). In many forms of arthritis inrheumatic diseases not only articular inflammation is present, butalso inflammation of tendons and ligaments (e.g. spondyloarthritis,psoriatic arthritis, rheumatoid arthritis, etc.), therefore therapeuticinjections of tendon sheaths will also be considered in this review.
Diagnostic procedures have to be distinguished from therapeu-tic procedures [3]. When fluid from joints or tendons is aspirated todifferentiate inflammatory from infective synovitis, or when biopsyof synovium or soft tissue masses is performed or when local anes-thetics are injected to confirm clinical diagnosis we speak in termsof diagnostic interventions. Therapeutic interventions are aspira-tion, with or without injection, of cysts and injections of drugsinto joints, tendon sheaths, bursae and around ligaments or nerves.Under US guidance direct visualization of the underlying pathologyis possible and needle insertion can be seen in real-time. Surround-ing vessels and tendons, but also nerves and articular cartilage canbe displayed and therefore avoided during needle insertion, whichleads to a more painless procedure for the patient and results inminimization of adverse effects. Clinically guided injections accord-
ing to standardized methods are widely used and supported indifferent studies [8,9], but it is also known that best results wereachieved by correct intra-articular injection [10]. US guidance hasshown to improve intra-articular placement in various regions, butis particularly useful in obese patients, poorly accessible joints (e.g.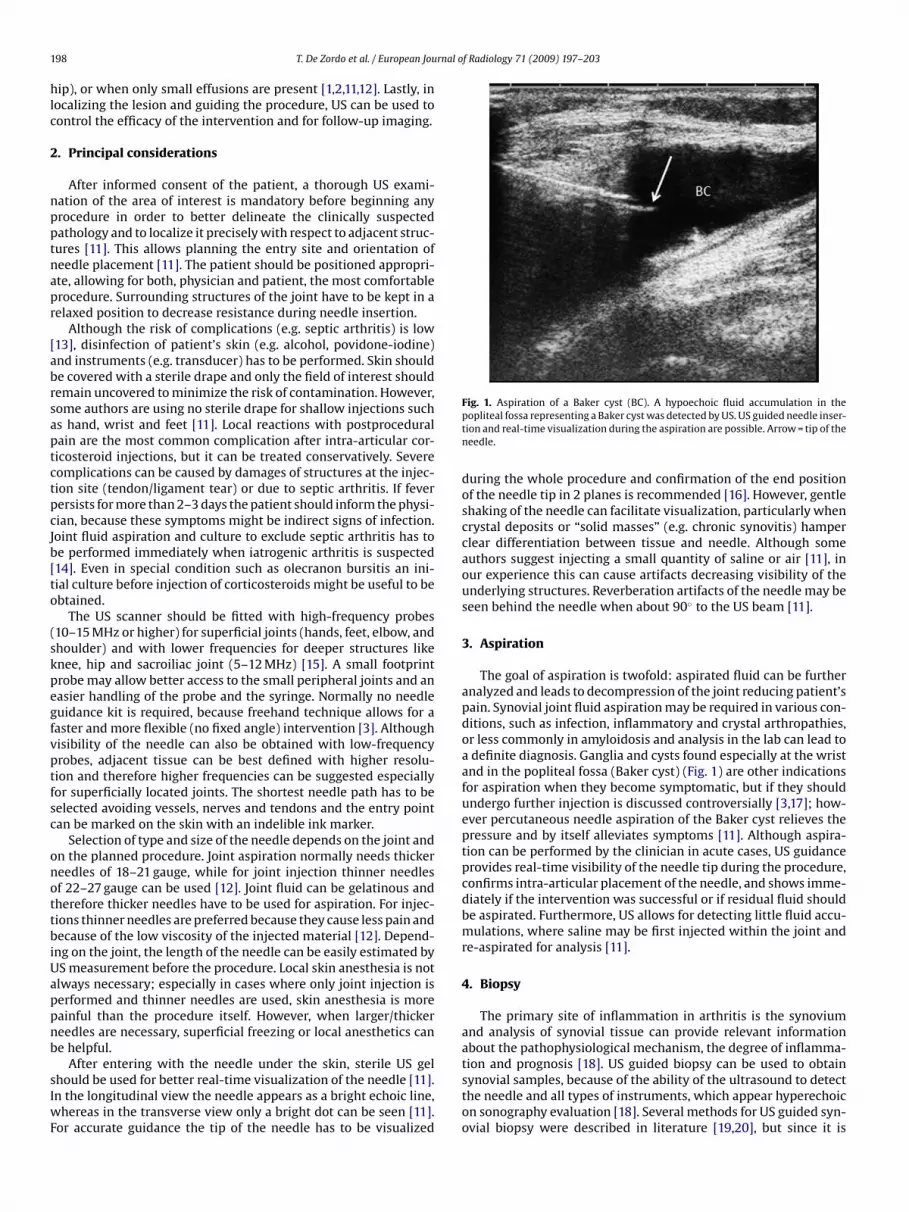
1 rnal of Radiology 71 (2009) 197–203
hlc
2
npptnapr
[abrsaptctpcJb[to
(skpegfvptfsc
onottbiUappnb
sIwF
98 T. De Zordo et al. / European Jou
ip), or when only small effusions are present [1,2,11,12]. Lastly, inocalizing the lesion and guiding the procedure, US can be used toontrol the efficacy of the intervention and for follow-up imaging.
. Principal considerations
After informed consent of the patient, a thorough US exami-ation of the area of interest is mandatory before beginning anyrocedure in order to better delineate the clinically suspectedathology and to localize it precisely with respect to adjacent struc-ures [11]. This allows planning the entry site and orientation ofeedle placement [11]. The patient should be positioned appropri-te, allowing for both, physician and patient, the most comfortablerocedure. Surrounding structures of the joint have to be kept in aelaxed position to decrease resistance during needle insertion.
Although the risk of complications (e.g. septic arthritis) is low13], disinfection of patient’s skin (e.g. alcohol, povidone-iodine)nd instruments (e.g. transducer) has to be performed. Skin shoulde covered with a sterile drape and only the field of interest shouldemain uncovered to minimize the risk of contamination. However,ome authors are using no sterile drape for shallow injections suchs hand, wrist and feet [11]. Local reactions with postproceduralain are the most common complication after intra-articular cor-icosteroid injections, but it can be treated conservatively. Severeomplications can be caused by damages of structures at the injec-ion site (tendon/ligament tear) or due to septic arthritis. If feverersists for more than 2–3 days the patient should inform the physi-ian, because these symptoms might be indirect signs of infection.oint fluid aspiration and culture to exclude septic arthritis has toe performed immediately when iatrogenic arthritis is suspected14]. Even in special condition such as olecranon bursitis an ini-ial culture before injection of corticosteroids might be useful to bebtained.
The US scanner should be fitted with high-frequency probes10–15 MHz or higher) for superficial joints (hands, feet, elbow, andhoulder) and with lower frequencies for deeper structures likenee, hip and sacroiliac joint (5–12 MHz) [15]. A small footprintrobe may allow better access to the small peripheral joints and anasier handling of the probe and the syringe. Normally no needleuidance kit is required, because freehand technique allows for aaster and more flexible (no fixed angle) intervention [3]. Althoughisibility of the needle can also be obtained with low-frequencyrobes, adjacent tissue can be best defined with higher resolu-ion and therefore higher frequencies can be suggested especiallyor superficially located joints. The shortest needle path has to beelected avoiding vessels, nerves and tendons and the entry pointan be marked on the skin with an indelible ink marker.
Selection of type and size of the needle depends on the joint andn the planned procedure. Joint aspiration normally needs thickereedles of 18–21 gauge, while for joint injection thinner needlesf 22–27 gauge can be used [12]. Joint fluid can be gelatinous andherefore thicker needles have to be used for aspiration. For injec-ions thinner needles are preferred because they cause less pain andecause of the low viscosity of the injected material [12]. Depend-
ng on the joint, the length of the needle can be easily estimated byS measurement before the procedure. Local skin anesthesia is notlways necessary; especially in cases where only joint injection iserformed and thinner needles are used, skin anesthesia is moreainful than the procedure itself. However, when larger/thickereedles are necessary, superficial freezing or local anesthetics cane helpful.
After entering with the needle under the skin, sterile US gelhould be used for better real-time visualization of the needle [11].n the longitudinal view the needle appears as a bright echoic line,
hereas in the transverse view only a bright dot can be seen [11].or accurate guidance the tip of the needle has to be visualized
Fig. 1. Aspiration of a Baker cyst (BC). A hypoechoic fluid accumulation in thepopliteal fossa representing a Baker cyst was detected by US. US guided needle inser-tion and real-time visualization during the aspiration are possible. Arrow = tip of theneedle.
during the whole procedure and confirmation of the end positionof the needle tip in 2 planes is recommended [16]. However, gentleshaking of the needle can facilitate visualization, particularly whencrystal deposits or “solid masses” (e.g. chronic synovitis) hamperclear differentiation between tissue and needle. Although someauthors suggest injecting a small quantity of saline or air [11], inour experience this can cause artifacts decreasing visibility of theunderlying structures. Reverberation artifacts of the needle may beseen behind the needle when about 90◦ to the US beam [11].
3. Aspiration
The goal of aspiration is twofold: aspirated fluid can be furtheranalyzed and leads to decompression of the joint reducing patient’spain. Synovial joint fluid aspiration may be required in various con-ditions, such as infection, inflammatory and crystal arthropathies,or less commonly in amyloidosis and analysis in the lab can lead toa definite diagnosis. Ganglia and cysts found especially at the wristand in the popliteal fossa (Baker cyst) (Fig. 1) are other indicationsfor aspiration when they become symptomatic, but if they shouldundergo further injection is discussed controversially [3,17]; how-ever percutaneous needle aspiration of the Baker cyst relieves thepressure and by itself alleviates symptoms [11]. Although aspira-tion can be performed by the clinician in acute cases, US guidanceprovides real-time visibility of the needle tip during the procedure,confirms intra-articular placement of the needle, and shows imme-diately if the intervention was successful or if residual fluid shouldbe aspirated. Furthermore, US allows for detecting little fluid accu-mulations, where saline may be first injected within the joint andre-aspirated for analysis [11].
4. Biopsy
The primary site of inflammation in arthritis is the synoviumand analysis of synovial tissue can provide relevant informationabout the pathophysiological mechanism, the degree of inflamma-
tion and prognosis [18]. US guided biopsy can be used to obtainsynovial samples, because of the ability of the ultrasound to detectthe needle and all types of instruments, which appear hyperechoicon sonography evaluation [18]. Several methods for US guided syn-ovial biopsy were described in literature [19,20], but since it is
rnal o
mm
5
eiooipmio
iadtljjav
jttwtdjojiocascwceotidwdie
6
cdirmaebr
T. De Zordo et al. / European Jou
ainly performed for research purposes, we will not discuss it inore detail.
. Injection
US guided local steroid injection is relatively simple, cost-ffective, and an alternative or adjunction to systemic drug therapyn several rheumatologic conditions [21]. In rheumatoid arthritisr other forms of systemic disease with joint involvement (e.g.steoarthritis, juvenile idiopathic arthritis, reactive arthritis, etc.)njections can be performed into the joint cavity, but in someathologies (e.g. psoriasis) bursa, tendon or tendon sheath involve-ent might be more dominant and can be treated by US guided
njection. Before injection of corticosteroids, infection of the regionf interest should be excluded.
The main goal of corticosteroid injection is the reduction ofnflammation resulting in a decrease of vascularity, what can bessessed by US [22]. As mainly no intra-articular vessels can beetected in healthy joints, no Doppler signal means remission ofhe disease; a goal, which should be reached by systemic and/orocal therapy. At our Department only patients with up to five activeoints are injected, in patients with equal or more than five activeoints systemic therapy is modified. A follow-up examination inpproximately six weeks after injection might be helpful to proveascularity decrease.
In general, the injection within bursae, tendon sheaths, andoints consists of corticosteroids alone or a mixture of corticos-eroid and local anesthetic. In our Department we use a mixture ofriamcinolone acetonide, a long-acting steroid, and 0.5% marcaineith a corticosteroid dosage of 2–10 mg for small joints and up
o 40 mg/ml for large joints. The volume of the injected materialepends on individual size of joint cavity: less in interphalangeal
oints (sometimes injected medication is limitated to 1–2 dropsnly in very small joints), compared to more in larger joints oroints with large synovial proliferation, where injection of 1–3 mls possible. However, injection has to be stopped when a “sensationf ballooning” is reported by the patient, because of the risk ofapsular disruption. For bursal injections the same corticosteroids in joints is used with a volume up to 1–2 ml depending on theize of the bursa, while for tendon sheath injections a short-actingorticosteroid (e.g. celestan) by avoiding crystalline corticosteroids,hich might damage vulnerable tendons, is mixed with 0.5% mar-
aine and a volume of up to 1–2 ml is injected. However, thefficacy of local therapy depends not only on the amount and typef injected drugs [23], but also on the appropriate space or struc-ure into which the solution is injected. A small dose of steroidsnstilled within an inflamed bursa is far more effective than a largerose injected in the adjacent tissues and has fewer side effects,hich highlight the usefulness of US guidance [14]. Furthermore,ifferentiation of fibrotic pannus and highly active synovitis might
mpact on dosage of corticosteroids: highly active joints mightffort whole dosage, lower inflammation might enable reduction.
. Other treatment options
Corticosteroids are widely considered as the medication ofhoice for injection, but more recent studies report results of otherrugs and therapeutic procedures. In osteoarthritis for example
ntra-articular injection of hyaluronic acid has shown promising
esults [24] but one comparative study did not find any improve-ent compared to corticosteroid injections [25]. In rheumatoidrthritis and psoriatic arthritis biologicals (methotrexate and etan-rcept) have shown good preliminary results; however, the cost ofiologicals will presumably limit its use to patients with adverseeactions to steroids [26,27].
f Radiology 71 (2009) 197–203 199
7. Considerations of individual regions
Aspiration is more commonly necessary in large joints such aships, knees, shoulders and elbows, whereas injection has no prefer-ences. The US guided approach of each region remains mainly thesame for all interventions and in the following paragraph we willdiscuss the most common procedures in more detail.
7.1. Hip
Indications for US guided interventions besides septic arthritisand fluid accumulations (e.g. osteoarthritis), are transient syn-ovitis in children or painful prosthesis [11]. With the patient insupine position an anterolateral access under the inguinal ligamenttowards the anterior synovial recess at the junction of the femoralhead and neck should be chosen [28,29]. A slight increase in resis-tance is appreciated as the needle passes the iliofemoral ligament,but direct injection in the ligament should be avoided. With fur-ther advance, the needle can be felt to pop through the ligamentand enter the hip joint. Caution has to be taken to avoid large ves-sels and nerves at this region. The trochanteric bursa is anotheranatomic structure in this area where US guidance for injection isuseful. Once a referred pain from a lumbar or hip source as wellas other local pathology has been clinically excluded, pain loca-tion plus greater trochanter tenderness are usually sufficient fordiagnosis and with the patient lying laterally on the bed, real-timeguidance of the needle towards the peritrochanteric bursa can beperformed.
7.2. Knee
Most studies of knee joint injection are reported for osteoarthri-tis, but also in inflammatory rheumatologic disorders the knee jointmight be affected. Although injection without image guidance canbe readily performed with a high degree of accuracy, there are occa-sions when confirmation of needle placement is essential: obesepatients, patients with swollen legs, and when only a small amountof fluid is present [11,12]. According to clinical guided injectionsthe patient is in supine position and the knee angulated of 20–30◦,the needle is inserted from the lateral aspect of the joint at thesuperior margin of the patella towards the suprapatellar recess,where in pathological conditions fluid is detectable. We suggestanother very easy and less painful approach using a cranial to cau-dal path, medially or laterally to the quadriceps tendon, directlyinto the fluid collection. Using this method the tip of the needlecan be followed all the way by using a parasagittal, longitudi-nal US scan. If the recess is not discernible on US the needle canbe placed in the joint cavity, but with this traditional approachthe needle is covered by bone and intra-articular placement canonly be detected by injecting air inside the joint cavity, whichwill move to the suprapatellar recess, thus making it visible [28].When a symptomatic Baker cyst (functional limitation of the knee,inflammation, rupture of the cyst, compression of surroundingstructures) is present a dorsal approach is necessary, but recur-rence might happen and a second aspiration may lead to long-termbenefit [3].
7.3. Ankle
For injection or aspiration of the ankle an anterior approach isrecommended [30], however, first the anterior tibial artery should
be localized by Doppler US [11]. Avoiding artery and extensor ten-dons the needle can be directly inserted towards the joint, wherein most pathological conditions fluid or synovial proliferation canbe detected. In many conditions (e.g. psoriatic arthritis, rheuma-toid arthritis, etc.) tendons or tendon sheaths at the ankle are
2 rnal of Radiology 71 (2009) 197–203
iofmcmrctnat
7
iralTwanmtjr
tstc
srifirtaop
tov
7
rtrlroapj
cAto
Fig. 2. (A) Injection of subdeltoid bursa. A thickened, hypoechoic subdeltoid bursawas detected by US. RCT = rotator cuff tendons, D = deltoid muscle, and A = acromion.(B) US guided needle insertion, sparing the rotator cuff tendons (RCT), can be easily
00 T. De Zordo et al. / European Jou
nvolved, where injections of corticosteroids into the tendon sheathr paratenon are a therapeutic option. Achilles tendon, plantarascia, flexor hallucis longus, peroneus and tibialis tendons are com-
only involved in systemic diseases [30–32]. No general techniquean be described in these cases; however, an intratendinous place-ent of medication should be avoided, because of the risk of tendon
upture. After assessing needle position in relation to the neurovas-ular bundles and other tendons a longitudinal scan perpendicularo the needle should be attempted, for better visualization of theeedle tip. During injection fluid distension of the sheath results intenosonographic effect, also enabling improved visualization of
he tendon margins [32].
.4. Shoulder
There are three major indications for a glenohumeral jointnjection: osteoarthritis, adhesive capsulitis (frozen shoulder), andheumatoid arthritis [33]. The shoulder joint can be punctured fromposterior or anterior approach; however, fluid tends to accumu-
ate first in the posterior aspect of the glenohumeral joint [16,34].herefore, a posterior approach through the infraspinatus muscleith the patient sitting or in a semiprone position seems to be most
ppropriate. The path of the needle should be adjusted so that theeedle passes into the joint space immediately deep to the freeargin of the glenoid labrum and tangential to the curvature of
he humeral head [35]. Relative contraindications of glenohumeraloint injections are avascular necrosis of the humeral head andecent rotator cuff tendon rupture [35].
The most common indication for acromioclavicular joint injec-ion is osteoarthritis [33]. A superior approach with the patientupine or sitting can be suggested; however, care has to be takeno inject only small amounts of medication, because of the risk ofapsule or ligament rupture.
Another frequently injected region of the shoulder is theubdeltoid–subacromial bursa (Fig. 2). Although a recent studyeported no difference in accuracy between clinically and US guidednjections [9], in different reports, the incidence of blind injectionailure has ranged from 13 to 71% [36,37]. Therefore, US guidednjections should be indicated, at least, in patients with pooresponse to previous blind injection to ensure accurate medica-ion placement in order to improve therapeutic effectiveness [4]. Annterior or lateral approach with the patient sitting or supine is rec-mmended, with real-time visualization of the needle in a parallelosition.
US guided injection is also useful for treatment of inflamma-ion of the long head of the biceps tendon [38]. A longitudinal viewf the tendon with the patient sitting or supine allows for bestisualization of the procedure.
.5. Elbow
The aetiology of elbow arthritis can be osteoarthritis, but evenheumatoid arthritis and other rheumatologic diseases can affecthis joint. The cubital joint may be punctured from a poste-ior approach allowing access to the olecranon recess when aarge amount of fluid is present or anterolaterally through theadiocapitellar joint [11,14]. With the elbow flexed at 90◦ thelecranon recess can be easily accessed from laterally or medi-lly of the triceps tendon or direct injection of the joint can beerformed through the extensor tendons and the radiocapitellar
oint.
Enthesopathies at the lateral (tennis elbow) or medial epi-ondyle (golfer’s elbow) are other common causes of elbow pain.lthough superficially located, US guidance can be used for peri-
endinous injection in order to avoid intratendinous placementf corticosteroids. Alternative to steroids, “dry needeling” (nee-
performed. Arrow = tip of the needle, RCT = rotator cuff tendons, and D = deltoid mus-cle. (C) During injection swelling of the bursa confirms correct intrabursal injection.RCT = rotator cuff tendons, arrow = tip of the needle with reverberation artifacts andD = deltoid muscle.
dle tenotomy) or intratendinous autologous blood injections aredescribed in literature [39,40].
7.6. Wrist
The radiocarpal joint is one of the most commonly involvedjoints in rheumatoid arthritis and can be easily injected under USguidance by means of a dorsal approach. The injection point islocalized about 1–2 cm distal to the Lister’s tubercle, between thesecond and third or third and fourth extensor tendon compartment,
in order that needle placement through tendon sheaths and smallvessels can be avoided [41]. However, a recent study has shownthat a single injection cannot be assumed to distribute – and treat– the whole joint [42], therefore repeated injections and a separateinjection of the DRU joint might be necessary.
T. De Zordo et al. / European Journal of Radiology 71 (2009) 197–203 201
Fig. 3. (A) Injection of the first carpometacarpal joint. The tip of the needle is locatedsUi
7
pb(epab
ptbsDsoratcadid
Fig. 4. (A) Longitudinal scan of second metacarpophalangeal joint presenting withrheumatoid arthritis. Tip of the needle (arrow) is placed inside the large amount of
Perineural injections are often performed in peripheral neuro-mas or in compression neuropathy. US has been used as a diagnosticaid in carpal tunnel syndrome, particularly if a compressive lesionis suspected, as it occurs due to ganglia, synovitis of the fingerflexors or synovitis of the wrist in inflammatory conditions. Even
uperficially to the joint in the muscle (arrow). 1st MC = first metacarpal bone. (B)S guides the procedure and in this image the tip of the needle can be appreciated
n the intra-articular space (arrow). 1st MC = first metacarpal bone.
.7. Finger and toe joints
Intercarpal, intertarsal, metacarpo-, metatarso-phalangeal,roximal and distal interphanlangeal joints are typically affectedy rheumatoid arthritis, osteoarthritis and psoriatic arthritisFigs. 3–5). A dorsal oblique approach, laterally or medially of thextensor tendon, using a hockey stick probe is an easy and safeath. Fluid accumulations are normally very small in these jointsnd therefore injection by real-time US guidance seems to be theest way for these small joints [43].
Tenosynovitis is a frequent finding in rheumatoid arthritis andsoriatic arthritis, but may also result from overuse injury. Differen-iation of fluid accumulation and hypertrophy should be obtainedefore the intervention, because fluid should be aspirated if pos-ible. Tenosynovitis can present with increased vascularity onoppler US and the underlying tendon may be normal or may
how loss of the fibrillar echotexture and loss of echogenicity withr without swelling, indicating tendinopathy. Detailed assessmentegarding tendon involvement seen by Doppler US, what reflects
higher degree of tendinopathy and therefore a higher risk ofendon damage, should be reported in the medical report and dis-ussed with the patient. All tendon sheaths can be injected, if
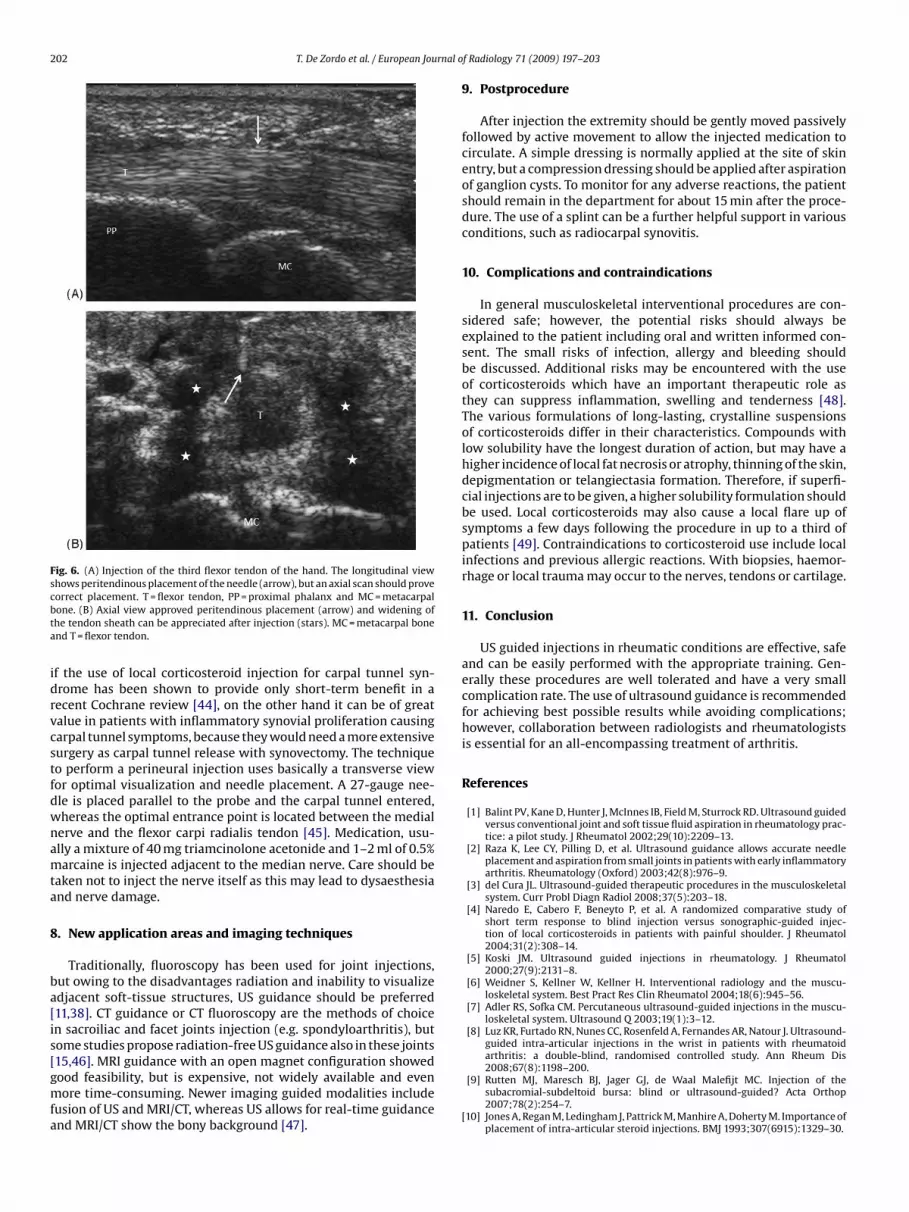
ffected by inflammatory rheumatic conditions. The affected ten-on is best approached first longitudinally and when the needle tips placed into the tendon sheath the axial plane verifies correct nee-le placement (Fig. 6). Both planes should be used during injection
synovitis (stars). PP = proximal phalanx and second MC = second metacarpal bone.(B) During injection extending of the joint capsule and hyperechoic drug accumu-lation can be observed. Stars = synovitis, arrow = needle, PP = proximal phalanx andsecond MC = second metacarpal bone.
to ascertain not to inject the tendon itself as this may result in localdamage and increased risk of rupture. If needle placement is cor-rect, the injection should result in distension of the sheath, howeverthis can be compromised by tendon sheath adhesions, resulting inlocal accumulation of the administrated drug. A 27-gauge needlecan be used in most cases for tendon injection, making the inter-vention very well tolerated even for children. Generally, injection ofthe tendon sheath is a safe procedure with very few complications.
7.8. Nerves
Fig. 5. US guided joint injection of the third interphalangeal joint in rheumatoidarthritis. Generally, only a small amount of synovitis is present in these joints, butusing US it can be detected and the needle can be directed towards the synovitis.MP = middle phalanx, PP = proximal phalanx and arrow = needle.
202 T. De Zordo et al. / European Journal o
Fig. 6. (A) Injection of the third flexor tendon of the hand. The longitudinal viewshows peritendinous placement of the needle (arrow), but an axial scan should provecbta
idrvcstfdwnamta
8
ba[is[gmfa
orrect placement. T = flexor tendon, PP = proximal phalanx and MC = metacarpalone. (B) Axial view approved peritendinous placement (arrow) and widening ofhe tendon sheath can be appreciated after injection (stars). MC = metacarpal bonend T = flexor tendon.
f the use of local corticosteroid injection for carpal tunnel syn-rome has been shown to provide only short-term benefit in aecent Cochrane review [44], on the other hand it can be of greatalue in patients with inflammatory synovial proliferation causingarpal tunnel symptoms, because they would need a more extensiveurgery as carpal tunnel release with synovectomy. The techniqueo perform a perineural injection uses basically a transverse viewor optimal visualization and needle placement. A 27-gauge nee-le is placed parallel to the probe and the carpal tunnel entered,hereas the optimal entrance point is located between the medialerve and the flexor carpi radialis tendon [45]. Medication, usu-lly a mixture of 40 mg triamcinolone acetonide and 1–2 ml of 0.5%arcaine is injected adjacent to the median nerve. Care should be
aken not to inject the nerve itself as this may lead to dysaesthesiand nerve damage.
. New application areas and imaging techniques
Traditionally, fluoroscopy has been used for joint injections,ut owing to the disadvantages radiation and inability to visualizedjacent soft-tissue structures, US guidance should be preferred11,38]. CT guidance or CT fluoroscopy are the methods of choicen sacroiliac and facet joints injection (e.g. spondyloarthritis), butome studies propose radiation-free US guidance also in these joints15,46]. MRI guidance with an open magnet configuration showed
ood feasibility, but is expensive, not widely available and evenore time-consuming. Newer imaging guided modalities includeusion of US and MRI/CT, whereas US allows for real-time guidancend MRI/CT show the bony background [47].
f Radiology 71 (2009) 197–203
9. Postprocedure
After injection the extremity should be gently moved passivelyfollowed by active movement to allow the injected medication tocirculate. A simple dressing is normally applied at the site of skinentry, but a compression dressing should be applied after aspirationof ganglion cysts. To monitor for any adverse reactions, the patientshould remain in the department for about 15 min after the proce-dure. The use of a splint can be a further helpful support in variousconditions, such as radiocarpal synovitis.
10. Complications and contraindications
In general musculoskeletal interventional procedures are con-sidered safe; however, the potential risks should always beexplained to the patient including oral and written informed con-sent. The small risks of infection, allergy and bleeding shouldbe discussed. Additional risks may be encountered with the useof corticosteroids which have an important therapeutic role asthey can suppress inflammation, swelling and tenderness [48].The various formulations of long-lasting, crystalline suspensionsof corticosteroids differ in their characteristics. Compounds withlow solubility have the longest duration of action, but may have ahigher incidence of local fat necrosis or atrophy, thinning of the skin,depigmentation or telangiectasia formation. Therefore, if superfi-cial injections are to be given, a higher solubility formulation shouldbe used. Local corticosteroids may also cause a local flare up ofsymptoms a few days following the procedure in up to a third ofpatients [49]. Contraindications to corticosteroid use include localinfections and previous allergic reactions. With biopsies, haemor-rhage or local trauma may occur to the nerves, tendons or cartilage.
11. Conclusion
US guided injections in rheumatic conditions are effective, safeand can be easily performed with the appropriate training. Gen-erally these procedures are well tolerated and have a very smallcomplication rate. The use of ultrasound guidance is recommendedfor achieving best possible results while avoiding complications;however, collaboration between radiologists and rheumatologistsis essential for an all-encompassing treatment of arthritis.
References
[1] Balint PV, Kane D, Hunter J, McInnes IB, Field M, Sturrock RD. Ultrasound guidedversus conventional joint and soft tissue fluid aspiration in rheumatology prac-tice: a pilot study. J Rheumatol 2002;29(10):2209–13.
[2] Raza K, Lee CY, Pilling D, et al. Ultrasound guidance allows accurate needleplacement and aspiration from small joints in patients with early inflammatoryarthritis. Rheumatology (Oxford) 2003;42(8):976–9.
[3] del Cura JL. Ultrasound-guided therapeutic procedures in the musculoskeletalsystem. Curr Probl Diagn Radiol 2008;37(5):203–18.
[4] Naredo E, Cabero F, Beneyto P, et al. A randomized comparative study ofshort term response to blind injection versus sonographic-guided injec-tion of local corticosteroids in patients with painful shoulder. J Rheumatol2004;31(2):308–14.
[5] Koski JM. Ultrasound guided injections in rheumatology. J Rheumatol2000;27(9):2131–8.
[6] Weidner S, Kellner W, Kellner H. Interventional radiology and the muscu-loskeletal system. Best Pract Res Clin Rheumatol 2004;18(6):945–56.
[7] Adler RS, Sofka CM. Percutaneous ultrasound-guided injections in the muscu-loskeletal system. Ultrasound Q 2003;19(1):3–12.
[8] Luz KR, Furtado RN, Nunes CC, Rosenfeld A, Fernandes AR, Natour J. Ultrasound-guided intra-articular injections in the wrist in patients with rheumatoidarthritis: a double-blind, randomised controlled study. Ann Rheum Dis
2008;67(8):1198–200.[9] Rutten MJ, Maresch BJ, Jager GJ, de Waal Malefijt MC. Injection of thesubacromial-subdeltoid bursa: blind or ultrasound-guided? Acta Orthop2007;78(2):254–7.
[10] Jones A, Regan M, Ledingham J, Pattrick M, Manhire A, Doherty M. Importance ofplacement of intra-articular steroid injections. BMJ 1993;307(6915):1329–30.

rnal o
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
T. De Zordo et al. / European Jou
11] Cardinal E, Chhem RK, Beauregard C. Ultrasound-guided interventional proce-dures in the musculoskeletal system. Radiol Clin North Am 1998;36:597–604.
12] De Smet AA. Ultrasound-guided injections and aspirations of the extremities.Semin Roentgenol 2004;39(1):145–54.
13] Cheng J, Abdi S. Complications of joint, tendon, and muscle injections. Tech RegAnesth Pain Manage 2007;11(3):141–7.
14] Bianchi S, Zamorani MP. US-guided interventional procedures. In: Baert AL,Knauth M, Sartor K, editors. Ultrasound of the musculoskeletal system. Berlin:Springer; 2006. p. 891–918.
15] Klauser A, De Zordo T, Feuchtner G, et al. Feasibility of ultrasound-guidedsacroiliac joint injection considering sonoanatomic landmarks at two differentlevels in cadavers and patients. Arthritis Rheum 2008;59:1618–24.
16] Van Holsbeek MT, Introcaso JH. Musculoskeletal ultrasound. 2nd ed. St. Louis,MO: CV Mosby; 2001.
17] Breidahl WH, Adler RS. Ultrasound-guided injection of ganglia with coricos-teroids. Skeletal Radiol 1996;25(7):635–8.
18] Epis O, Iagnocco A, Meenagh G, et al. Ultrasound imaging for the rheumatologist.XVI. Ultrasound-guided procedures. Clin Exp Rheumatol 2008;26(4):515–8.
19] Koski JM, Helle M. Ultrasound guided synovial biopsy using portal and forceps.Ann Rheum Dis 2005;64(6):926–9.
20] Scirè CA, Epis O, Codullo V, et al. Immunohistological assessment of thesynovial tissue in small joints in rheumatoid arthritis: validation of a mini-mally invasive ultrasound-guided synovial biopsy procedure. Arthritis Res Ther2007;9(5):R101.
21] Grassi W, Farina A, Filippucci E, Cervini C. Sonographically guided proceduresin rheumatology. Semin Arthritis Rheum 2001;30(5):347–53.
22] Filippucci E, Farina A, Carotti M, Salaffi F, Grassi W. Grey scale and power Dopplersonographic changes induced by intra-articular steroid injection treatment.Ann Rheum Dis 2004;63(6):740–3.
23] Robinson P, Keenan AM, Conaghan PG. Clinical effectiveness and dose responseof image-guided intra-articular corticosteroid injection for hip osteoarthritis.Rheumatology (Oxford) 2007;46(2):285–91.
24] Migliore A, Tormenta S, Martin LS, et al. The symptomatic effects of intra-articular administration of hylan G-F 20 on osteoarthritis of the hip: clinicaldata of 6 months follow-up. Clin Rheumatol 2006;25(3):389–93.
25] Qvistgaard E, Christensen R, Torp-Pedersen S, Bliddal H. Intra-articular treat-ment of hip osteoarthritis: a randomized trial of hyaluronic acid, corticosteroid,and isotonic saline. Osteoarthritis Cartilage 2006;14(2):163–70.
26] Iagnocco A, Cerioni A, Coari G, Ossandon A, Masciangelo R, Valesini G. Intra-articular methotrexate in the treatment of rheumatoid arthritis and psoriaticarthritis: a clinical and sonographic study. Clin Rheumatol 2006;25(2):159–63.
27] Bliddal H, Terslev L, Qvistgaard E, et al. A randomized, controlled study of asingle intra-articular injection of etanercept or glucocorticosteroids in patientswith rheumatoid arthritis. Scand J Rheumatol 2006;35(5):341–5.
28] Qvistgaard E, Kristoffersen H, Terslev L, Danneskiold-Samsøe B, Torp-Pedersen
S, Bliddal H. Guidance by ultrasound of intra-articular injections in the kneeand hip joints. Osteoarthritis Cartilage 2001;9(6):512–7.29] Sofka CM, Saboeiro G, Adler RS. Ultrasound-guided adult hip injections. J VascInterv Radiol 2005;16(8):1121–3.
30] Sofka CM, Adler RS. Ultrasound-guided interventions in the foot and ankle.Semin Musculoskelet Radiol 2002;6(2):163–8.
[
[
f Radiology 71 (2009) 197–203 203
31] Cunnane G, Brophy DP, Gibney RG, FitzGerald O. Diagnosis and treatment ofheel pain in chronic inflammatory arthritis using ultrasound. Semin ArthritisRheum 1996;25(6):383–9.
32] Mehdizade A, Adler RS. Sonographically guided flexor hallucis longus tendonsheath injection. J Ultrasound Med 2007;26(2):233–7.
33] Tallia AF, Cardone DA. Diagnostic and therapeutic injection of the shoulderregion. Am Fam Physician 2003;67(6):1271–8.
34] Schmidt WA, Schicke B, Krause A. Which ultrasound scan is thebest to detect glenohumeral joint effusions? Ultraschall Med 2008,doi:10.1055/s-2008-1027330.
35] Zwar RB, Read JW, Noakes JB. Sonographically guided glenohumeral joint injec-tion. AJR Am J Roentgenol 2004;183(1):48–50.
36] Eustace JA, Brophy DP, Gibney RP, Bresnihan B, FitzGerald O. Comparison of theaccuracy of steroid placement with clinical outcome in patients with shouldersymptoms. Ann Rheum Dis 1997;56(1):59–63.
37] Esenyel CZ, Esenyel M, Yesiltepe R, et al. The correlation between the accuracyof steroid injections and subsequent shoulder pain and function in subacromialimpingement syndrome. Acta Orthop Traumatol Turc 2003;37(1):41–5.
38] Sofka CM, Collins AJ, Adler RS. Use of ultrasonographic guidance in inter-ventional musculoskeletal procedures: a review from a single institution. JUltrasound Med 2001;20(1):21–6.
39] McShane JM, Nazarian LN, Harwood MI. Sonographically guided percutaneousneedle tenotomy for treatment of common extensor tendinosis in the elbow. JUltrasound Med 2006;25(10):1281–9.
40] Connell DA, Ali KE, Ahmad M, Lambert S, Corbett S, Curtis M. Ultrasound-guidedautologous blood injection for tennis elbow. Skeletal Radiol 2006;35(6):371–7.
41] Lohman M, Vasenius J, Nieminen O. Ultrasound guidance for puncture andinjection in the radiocarpal joint. Acta Radiol 2007;48(7):744–7.
42] Boesen M, Jensen KE, Torp-Pedersen S, Cimmino MA, Danneskiold-Samsøe B,Bliddal H. Intra-articular distribution pattern after ultrasound-guided injec-tions in wrist joints of patients with rheumatoid arthritis. Eur J Radiol 2007,doi:10.1016/j.ejrad.2007.08.037.
43] Grassi W, Lamanna G, Farina A, Cervini C. Synovitis of small joints:sonographic guided diagnostic and therapeutic approach. Ann Rheum Dis1999;58(10):595–7.
44] Marshall S, Tardif G, Ashworth N. Local corticosteroid injection for carpal tunnelsyndrome. Cochrane Database Syst Rev 2007;(2):CD001554.
45] Grassi W, Farina A, Filippucci E, Cervini C. Intralesional therapy in carpaltunnel syndrome: a sonographic-guided approach. Clin Exp Rheumatol2002;20(1):73–6.
46] Pekkafahli MZ, Kiralp MZ, Basekim CC, et al. Sacroiliac joint injections per-formed with sonographic guidance. J Ultrasound Med 2003;22(6):553–9.
47] Klauser A, Moriggl B, Feuchtner G, et al. Feasibility of virtual realtime sonog-raphy to guide sacroiliac joint injections. In: 2007 European Congress of
Radiology. 2007.48] Kumar N, Newman RJ. Complications of intra- and peri-articular steroid injec-tions. Br J Gen Pract 1999;49(443):465–6.
49] Goldfarb CA, Gelberman RH, McKeon K, Chia B, Boyer MI. Extra-articular steroidinjection: early patient response and the incidence of flare reaction. J Hand Surg2007;32(10):1513–20.





























