Embed Size (px)
Citation preview

Uses of Negative PressureWound Therapy in
Orthopedic Trauma Mark J. Gage, MDa, Richard S. Yoon, MDa,Kenneth A. Egol, MDa, Frank A. Liporace, MDa,b,*KEYWORDS
� Negative pressure wound therapy � VAC � Infection � Trauma � Open wound � Wound dehiscence� Limb salvage � Open fracture
KEY POINTS
� Negative pressure wound therapy (NPWT) is ideal for soft tissue defects that can heal through sec-ondary intention or require skin grafting.
� NPWT prevents desiccation, reduces edema, limits hematoma, and facilitates wound drainage.
� NPWT is an effective way to downscale the complexity of soft tissue reconstruction.
� NPWT can decreases the risk of wound complication when applied to high-risk incisions after frac-ture surgery.
INTRODUCTION
Since its inception more than 20 years ago, nega-tive pressure wound therapy (NPWT) has had amajor impact in the management of orthopedicinjuries. NPWT has been widely adopted for usein a variety of clinical scenarios, and has had re-ported success in the setting of high-energytrauma, open fractures, infections, and excessivesoft tissue damage. However, although its suc-cess has led to widespread use in orthopedictrauma, a deeper understanding of its mechanismof action, along with the ideal clinical scenariosfor use, is required. This article reviews the nu-ances of NPWT application, including its mecha-nism of action, clinical indications, and specificstrategies used in order to achieve desired clinicaloutcomes.
Conflicts of interest: The authors report no conflict of ina Division of Orthopaedic Trauma, Department of OrthoYork, NY, USA; b Orthopaedic Trauma and Adult ReconsCity Medical Center, 377 Jersey Avenue, Suite 220, Jersey* Corresponding author. Orthopaedic Trauma Research,thopaedic Surgery, NYU Hospital for Joint Diseases, NewE-mail address: [email protected]
Orthop Clin N Am 46 (2015) 227–234http://dx.doi.org/10.1016/j.ocl.2014.11.0020030-5898/15/$ – see front matter � 2015 Elsevier Inc. All
WHAT IS IT?
To administer NPWT, there are 3main componentsthat create a subatmospheric pressure environ-ment: a porous dressing sealed via an occlusiveadhesive, a vacuum device, and a connector thatallows communication (Fig. 1). In orthopedictrauma, the dressing of choice is a dry, black, hy-drophobic, reticulated polyurethane-ether foamwith a pore size of 400 to 600 mm (KCI, San Antonio,TX). A polyvinyl alcohol (PVA) foam is also available(KCI, San Antonio, TX). It differs from the large-porefoam because it has a smaller pore size(60–270 mm) and comes premoistened with sterilewater. The hydrophilic nature and smaller poresize of the PVA foam offers a less-adherent appli-cation and has significantly less granulation andperfusion than the large-pore dressing.1 Thus, for
terest.paedic Surgery, NYU Hospital for Joint Diseases, Newtruction, Department of Orthopaedic Surgery, JerseyCity, NJ 07302, USADivision of Orthopaedic Trauma, Department of Or-York, NY.
rights reserved. orthopedic.th
eclinics.com

Fig. 1. NPWT disrupts the inflammatory cascade by reducing edema, limiting hematoma, and facilitating wounddrainage to augment wound healing.
Gage et al228
most of the clinical scenarios in orthopedic trauma,the large-pore foam is preferred. Placed on thearea of interest, the wound and sponge dressingare sealed off with a plastic adhesive and occlusivedressing, and communicate with the vacuum de-vice via a connector creating a localized negativepressure environment.
HOW DOES IT WORK?
NPWT allows improved wound management andhealing via 2 main mechanisms. Following initialinjury, a substantial inflammatory response isgenerated from damaged tissue, initiating a vi-cious cycle of increasing interstitial edema andpressure, leading to cell death and necrosis sec-ondary to lack of nutrient inflow combined with acongested outflow of cellular waste (see Fig. 1).With the use of NPWT, a subatmospheric environ-ment is created, acting at the level of the intersti-tium to eliminate unwanted edema, inflammatorymediators, and bacteria (see Fig. 1). This environ-ment creates more favorable healing conditions byremoving the volume that obstructs inflow and
outflow, allowing greater nutrient and oxygeninflow as well as venous drainage.2
In addition, NPWT promotes mitogenesis andgranulation tissue formation via increased cellularsubstrate recruitment. Dynamic tissue formationis facilitated by the mechanical strain placed onthe tissue by the negative pressure environment.The strain created by the vacuum allows microde-formation and stretch at the cellular level, allowingcellular chemotaxis, angiogenesis, and new tissueformation via the recruitment of growth factors(ie, vascular endothelial growth factor [VEGF],Fibroblastic Growth Factor [FGF]-2).3,4 Labler andcolleagues3 analyzed wound fluid from NPWTdressings and noted significantly higher levels ofinterleukin-8 and VEGF compared with fluidanalyzed from a standard dressing. Furthermore,histologic analysis noted significantly higher levelsof angiogenesis and granulation tissue formation.The effect of the subatmospheric environment is
also evident at the genetic transcriptional level.Chen and colleagues5 measured the presence ofproto-oncogenes during NPWT in a pig model.The negative pressure environments produced

Negative Pressure Wound Therapy 229
significantly higher levels of C-MYC, C-JUN, andBCL-2, corresponding with proportional increasesin the cells required for granulation tissue forma-tion.4 These cellular-level changes serve as the ba-sis for the clinical advantages seen with NPWT.
Fig. 2. (A, B) The incisional dressing has resulted indecreased rates of infection and other wound compli-cations in patients with total ankle or hip arthroplasty,as well as high-risk incisions after fracture surgery.
INDICATIONS
In addressing purely soft tissue traumatic wounds,the best-supported indication for NPWT is to pro-vide temporary wound cover following thoroughdebridement when definitive closure is notpossible, such as in cases of significant woundcontamination, need for subsequent debridement,significant edema, or in a patient who is criticallyill. This form of therapy can be quickly appliedand accomplishes the goals of prevention of desic-cation, minimizing microbial contamination, reduc-tion of edema, and facilitation of wound drainage.Because it is changed less frequently than wet-to-dry dressings and subsequently provides lessdiscomfort for the patient, NPWT is less labor inten-sive for hospital staff. With regard to indications forits use, NPWT has been particularly successful inthe treatment of fasciotomy incisions because de-layed primary closure allows for edema to subsideand compartment pressures to normalize.6,7 Forsimilar reasons, NPWT has also been shown to bemore effective when applied over surgical woundsor incisions at fracture sites known to have a highincidence of wound complications compared withdry dressings (Fig. 2). Several randomized trials inthe orthopedic literature support these findings,particularly in high-risk closed extremity andacetabular fractures.8 In a randomized trial of 263patients, Stannard and colleagues9 showed adecreased risk of deep infection and dehiscencein high-risk lower extremity fractures using contin-uous negative pressure at 125 mm Hg for 2 to3 days. Animalmodels have reproduced these find-ings, showing a mechanism of action throughedema reduction, accelerated wound healing,decreased lateral tension on wound edges, andreduction in hematoma or seroma.10–12
This therapy has also proved to be a superiormeans to preserve skin grafts, improve skin graftincorporation, and reepithelialize the donor site.When applied directly over a newly applied skingraft, Llanos and colleagues13 showed in a ran-domized trial of 60 subjects that the median rateof skin graft loss and the median hospital staywere significantly reduced compared with a con-trol group.
NPWT has also been successful as a means todownscale the complexity of soft tissue recon-struction (Fig. 3). Parrett and colleagues14 showeda decrease in the number of free flaps needed
when NPWT was used in reconstruction with nodifference in infection, nonunion, amputation, orreoperation rates between groups. In progressinga complex wound to a smaller and simpler state,clinicians may avoid morbidity for patients andalso reduce cost of care.15 Although first perform-ing an aggressive debridement of all nonviable softtissue is advised, NPWT can be a useful tool topromote granulation tissue growth during a stateof wound bed unsuitability. Exposed bone,tendon, and orthopedic implants can precludedefinitive wound closure. NPWT may enhance tis-sue granulation over these substrates to allowstaged closure.16–18 However, care must be taken

Fig. 3. (A) NPWT is ideal for soft tissue defects that can heal through secondary intention or require skin grafting.(B) It can serve as an effective way to downscale the complexity of soft tissue reconstruction, as shown after1 week of NPWT treatment.
Gage et al230
to protect any exposed blood vessels or nervesand not place the dressing within too close prox-imity (Fig. 4).The delivery of negative pressure may also influ-
ence its effect on wound healing. These dressingsare commonly applied in a continuous negativepressure setting. A standard pressure of�125 mm Hg is applied, based on literatureshowing a 4-fold increase in blood flow comparedwith conventional dressings.19 However, there ismore recent support from work performed in a pigmodel for intermittent or variable pressure applica-tion to increase blood flow, wound contraction, andgranulation rate.19,20 These findings have yet totranslate into a change of NPWT practice becauseof a lack of clinical data to corroborate them. Inaddition, patients find variable and intermittent ther-apy to be painful, which decreases compliance.Although the literature is limited, there is evidence
to support the use of NPWT in the setting of woundcomplications when approaching wounds withincreased drainage or hematoma (Fig. 5). In a pro-spective randomized study comparing pressure
Fig. 4. NPWT can provide a bed of granulation tissueover exposed bone and tendon. However, in tenuousareas, care must be taken to dissect out and protectany exposed blood vessels and/or nerves.
Fig. 5. NPWT can help to manage hematomas anddrainage from long wounds, especially in tenuousareas. In this patient, who is status post–revision totalknee arthroplasty for periprosthetic fracture, inci-sional NPWT was placed after hematoma formationin the acute setting. Incisional NPWT is now typicallyplaced as the primary dressing for large wounds andin the obese.
Negative Pressure Wound Therapy 231
dressings with NPWT in 44 patients, NPWT hadcontinued drainage for approximately half thelength of time (1.6 vs 3.1 days) and a decreasedinfection rate, from 16% to 8%.21 There is someliterature to support NPWT to decrease bacterialload in a contaminated wound.19 However, morerecent literature has refuted this conclusion withmixed findings on its effect on bacterial load.22–24
Although these dressings can be used to provideprovisional coverage of infected wounds, theyshould not take the place of formal irrigation,debridement, and systemic antibiotics when ad-dressing infection.
COMPLICATIONS AND CHALLENGES
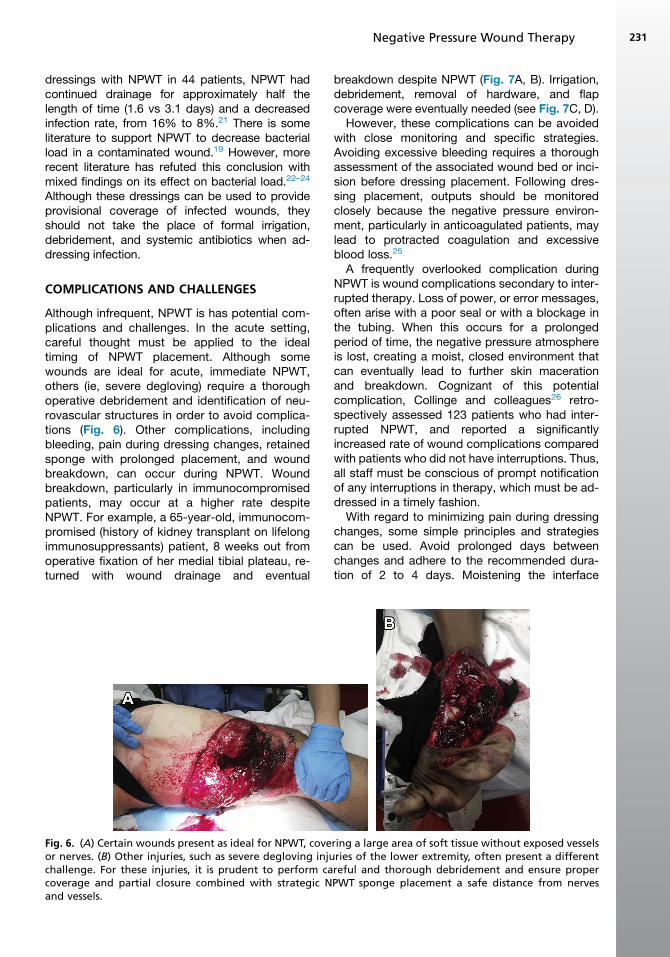
Although infrequent, NPWT is has potential com-plications and challenges. In the acute setting,careful thought must be applied to the idealtiming of NPWT placement. Although somewounds are ideal for acute, immediate NPWT,others (ie, severe degloving) require a thoroughoperative debridement and identification of neu-rovascular structures in order to avoid complica-tions (Fig. 6). Other complications, includingbleeding, pain during dressing changes, retainedsponge with prolonged placement, and woundbreakdown, can occur during NPWT. Woundbreakdown, particularly in immunocompromisedpatients, may occur at a higher rate despiteNPWT. For example, a 65-year-old, immunocom-promised (history of kidney transplant on lifelongimmunosuppressants) patient, 8 weeks out fromoperative fixation of her medial tibial plateau, re-turned with wound drainage and eventual
Fig. 6. (A) Certain wounds present as ideal for NPWT, coveor nerves. (B) Other injuries, such as severe degloving injuchallenge. For these injuries, it is prudent to perform cacoverage and partial closure combined with strategic Nand vessels.
breakdown despite NPWT (Fig. 7A, B). Irrigation,debridement, removal of hardware, and flapcoverage were eventually needed (see Fig. 7C, D).
However, these complications can be avoidedwith close monitoring and specific strategies.Avoiding excessive bleeding requires a thoroughassessment of the associated wound bed or inci-sion before dressing placement. Following dres-sing placement, outputs should be monitoredclosely because the negative pressure environ-ment, particularly in anticoagulated patients, maylead to protracted coagulation and excessiveblood loss.25
A frequently overlooked complication duringNPWT is wound complications secondary to inter-rupted therapy. Loss of power, or error messages,often arise with a poor seal or with a blockage inthe tubing. When this occurs for a prolongedperiod of time, the negative pressure atmosphereis lost, creating a moist, closed environment thatcan eventually lead to further skin macerationand breakdown. Cognizant of this potentialcomplication, Collinge and colleagues26 retro-spectively assessed 123 patients who had inter-rupted NPWT, and reported a significantlyincreased rate of wound complications comparedwith patients who did not have interruptions. Thus,all staff must be conscious of prompt notificationof any interruptions in therapy, which must be ad-dressed in a timely fashion.
With regard to minimizing pain during dressingchanges, some simple principles and strategiescan be used. Avoid prolonged days betweenchanges and adhere to the recommended dura-tion of 2 to 4 days. Moistening the interface
ring a large area of soft tissue without exposed vesselsries of the lower extremity, often present a differentreful and thorough debridement and ensure properPWT sponge placement a safe distance from nerves

Fig. 7. (A, B) This 65-year-old woman on chronic immunosuppressants for a prior kidney transplant returned withdrainage, infection, and subsequent dehiscence 8 weeks following operative fixation of her medial tibial plateau.(C, D) Despite NPWT, eventual debridement later required flap coverage and skin graft to close the site.
Gage et al232
between the sponge and the soft tissue can easedressing removal. Furthermore, although anecdot-ally used by the senior authors, application of anonocclusive protective dressing between thesponge and skin (eg, cellulose acetate siliconedressing, petroleum gauze dressing) can also aidin making dressing removal more facile andprevent irritation or maceration of the skin afterprolonged dressing application. Christensen and
colleagues27 performed a prospective, random-ized trial comparing the use of topical lidocaine(1%) without epinephrine versus placebo beforedressing removal. Patients who received the lido-caine injection directly into the sponge beforeremoval had significantly less pain beforeremoval.27 Following sponge removal, careful in-spection of the wound bed should be performedto avoid leaving behind any free foam material.

Negative Pressure Wound Therapy 233
SUMMARY
NPWT can be beneficial by optimizing orthopedicwounds and decreasing potential complications.Practical applications include use in open frac-tures, areas of extensive soft tissue loss, andeven primarily closed incisions in high-risk pa-tients. Continuous therapy at 125 mm Hg usingthe standard large-pore foam sponge is recom-mended. Outputs should be carefully monitoredto avoid excessive bleeding. Pain during dressingchanges can be avoided by using a nonadherentbarrier between the sponge and the soft tissue,and the use of topical lidocaine can also signifi-cantly reduce associated pain. Interruptions intherapy should be avoided and correctedpromptly. Although NPWT has advantages, withsupportive data, the right indications coupledwith diligent ancillary staff education and moni-toring are crucial for good outcomes.26
REFERENCES
1. Timmers MS, Le Cessie S, Banwell P, et al. The ef-
fects of varying degrees of pressure delivered by
negative-pressure wound therapy on skin perfusion.
Ann Plast Surg 2005;55(6):665–71.
2. Tarkin IS. The versatility of negative pressure wound
therapy with reticulated open cell foam for soft tissue
management after severe musculoskeletal trauma.
J Orthop Trauma 2008;22(10 Suppl):S146–51.
3. Labler L, Rancan M, Mica L, et al. Vacuum-assisted
closure therapy increases local interleukin-8 and
vascular endothelial growth factor levels in traumatic
wounds. J Trauma 2009;66(3):749–57.
4. McNulty AK, Schmidt M, Feeley T, et al. Effects of
negative pressure wound therapy on fibroblast
viability, chemotactic signaling, and proliferation in
a provisional wound (fibrin) matrix. Wound Repair
Regen 2007;15(6):838–46.
5. Chen SZ, Cao DY, Li JQ, et al. Effect of vacuum-
assisted closure on the expression of proto-
oncogenes and its significanceduringwoundhealing.
Zhonghua Zheng Xing Wai Ke Za Zhi 2005;21(3):
197–200 [in Chinese].
6. Yang CC, Chang DS, Webb LX. Vacuum-assisted
closure for fasciotomy wounds following compart-
ment syndrome of the leg. J Surg Orthop Adv
2006;15(1):19–23.
7. Zannis J, Angobaldo J, Marks M, et al. Comparison
of fasciotomy wound closures using traditional dres-
sing changes and the vacuum-assisted closure de-
vice. Ann Plast Surg 2009;62(4):407–9.
8. Reddix RN Jr, Leng XI, Woodall J, et al. The effect of
incisional negative pressure therapy on wound com-
plications after acetabular fracture surgery. J Surg
Orthop Adv 2010;19(2):91–7.
9. Stannard JP, Volgas DA, McGwin G 3rd, et al. Inci-
sional negative pressure wound therapy after high-
risk lower extremity fractures. J Orthop Trauma
2012;26(1):37–42.
10. Kilpadi DV, Cunningham MR. Evaluation of closed
incision management with negative pressure wound
therapy (CIM): hematoma/seroma and involvement
of the lymphatic system. Wound Repair Regen
2011;19(5):588–96.
11. Meeker J, Weinhold P, Dahners L. Negative pressure
therapy on primarily closed wounds improves
wound healing parameters at 3 days in a porcine
model. J Orthop Trauma 2011;25(12):756–61.
12. Wilkes RP, Kilpad DV, Zhao Y, et al. Closed incision
management with negative pressure wound ther-
apy (CIM): biomechanics. Surg Innov 2012;19(1):
67–75.
13. Llanos S, Danilla S, Barraza C, et al. Effectiveness of
negative pressure closure in the integration of split
thickness skin grafts: a randomized, double-
masked, controlled trial. Ann Surg 2006;244(5):
700–5.
14. Parrett BM, Matros E, Pribaz JJ, et al. Lower extrem-
ity trauma: trends in the management of soft-tissue
reconstruction of open tibia-fibula fractures. Plast
Reconstr Surg 2006;117(4):1315–22 [discussion:
1323–4].
15. Herscovici D Jr, Sanders RW, Scaduto JM, et al.
Vacuum-assisted wound closure (VAC therapy)
for the management of patients with high-energy
soft tissue injuries. J Orthop Trauma 2003;17(10):
683–8.
16. Lee HJ, Kim JW, Oh CW, et al. Negative pressure
wound therapy for soft tissue injuries around the
foot and ankle. J Orthop Surg Res 2009;4:14.
17. Pelham FR, Kubiak EN, Sathappan SS, et al. Topical
negative pressure in the treatment of infected
wounds with exposed orthopaedic implants.
J Wound Care 2006;15(3):111–6.
18. DeFranzo AJ, Argenta LC, Marks MW, et al. The use
of vacuum-assisted closure therapy for the treat-
ment of lower-extremity wounds with exposed
bone. Plast Reconstr Surg 2001;108(5):1184–91.
19. Morykwas MJ, Argenta LC, Shelton-Brown EI, et al.
Vacuum-assisted closure: a new method for wound
control and treatment: animal studies and basic
foundation. Ann Plast Surg 1997;38(6):553–62.
20. Malmsjo M, Gustafsson L, Lindstedt S, et al. The
effects of variable, intermittent, and continuous
negative pressure wound therapy, using foam or
gauze, on wound contraction, granulation tissue for-
mation, and ingrowth into the wound filler. Eplasty
2012;12:e5.
21. Stannard JP, Robinson JT, Anderson ER, et al. Nega-
tive pressure wound therapy to treat hematomas
and surgical incisions following high-energy trauma.
J Trauma 2006;60(6):1301–6.
Gage et al234
22. Moisidis E, Heath T, Boorer C, et al. A prospective,
blinded, randomized, controlled clinical trial of
topical negative pressure use in skin grafting. Plast
Reconstr Surg 2004;114(4):917–22.
23. Weed T, Ratliff C, Drake DB. Quantifying bacterial
bioburden during negative pressure wound ther-
apy: does the wound VAC enhance bacterial
clearance? Ann Plast Surg 2004;52(3):276–9 [dis-
cussion: 279–80].
24. Moues CM, Vos MC, van den Bemd GJ, et al. Bac-
terial load in relation to vacuum-assisted closure
wound therapy: a prospective randomized trial.
Wound Repair Regen 2004;12(1):11–7.
25. Li Z, Yu A. Complications of negative pressure
wound therapy: a mini review. Wound Repair Regen
2014;22(4):457–61.
26. Collinge C, Reddix R. The incidence of wound com-
plications related to negative pressure wound ther-
apy power outage and interruption of treatment in
orthopaedic trauma patients. J Orthop Trauma
2011;25(2):96–100.
27. Christensen TJ, Thorum T, Kubiak EN. Lidocaine
analgesia for removal of wound vacuum-assisted
closure dressings: a randomized double-blinded
placebo-controlled trial. J Orthop Trauma 2013;
27(2):107–12.




























