Embed Size (px)
Citation preview

Ventilator-associated pneumonia- Understanding epidemiology and pathogenesis to guide prevention and empiric therapy
Patrick Francioli ?, Jean Chastr&?, Martin Langer3, Jose Ignacio Santos4, Pramod M Shah5 and Antonio Torres6
lDivisions of Hospital Preventive Medicine and of Infectious Diseases, CHUV, Lausanne, Switzerland; 2HBpital Claude-Bernard, Paris, France; 30spedale Maggiore - IKCCS, Milano, Italy; 413epartment of Experimental Medicine, School of Medicine, UNAM; Coordinacion de Vigilancia, Epidemiologica, SSA, Mexico; 5Goethe-Universitaet, Frankfurt am Main, Germany; 6Servei de Pnemologie, Hospital Clinic, Barcelona, Spain.
Nosocomial pneumonia is associated with a high rate of mortality, particularly in ventilated patients in the intensive care unit (ICU). There have recently been a number of advances in the diagnosis, prevention and treatment of ventilator- associated pneumonia (VAP), as well as in the understanding of its etiology and pathophysiology. New diagnostic techniques, such as protected specimen brushing (PSB) and bronchoalveolar lavage (BAL) have been developed and assessed. Potential sources of pathogens have been investigated with molecular techniques.
Progress in prevention has been made, with new measures, including putting intubated patients in a semi-recumbent position with continuous aspiration of subglottic secretions or selecting stress-ulcer prophylactic regimens which do not modify the gastric pH. Meta-analysis has shown that selective digestive decontamination (SDD) reduces the risk of developing ventilator-associated pneumonia and possibly mortality. Empirical treatment before culture results depends on various factors including the severity of the symptoms and the associated risk factors, but more importantly, the time of onset of pneumonia. Early-onset VAP (less than 4 days after admission) is likely to be caused by pathogens which originate in the oropharyngeal cavity (Staphylococcus aureus, Streptococcus pneumoniae, Haemophilus influenzae), whereas aerobic, multi-resistant, Gram-negative bacilli are less likely unless there are predisposing risk factors. Late-onset VAP is more likely to be caused by Gram-negative bacilli or S. aureus and may involve Pseudomonas aeruginosa and Acinetobacter spp.
Diagnostic work-up and antimicrobial treatment adapted to the individual patient with VAP is important and even crucial in patients with late-onset VAP and in patients with early-onset VAP and risk factors. Empirical treatment should be started after having collected adequate samples and should be modified according to microbiological results once they are available. Monotherapy with a p-lactam@-lactamase-inhibitor or a second- or third-generation cephalosporin is appropriate for empiric treatment of early-onset VAP with no risk factors which may alter the spectrum or susceptibility of microorganisms. A quinolone may be used in combination with clindamycin to ensure optimal coverage of S. aureus and anerobes, which are listed as potential pathogens. A third-generation cephalosporin may be chosen in areas where resistant pneumococci are frequently encountered.
In the case of late-onset pneumonia,. or early-onset pneumonia with risk factors, the j3-lactam should have anti- pseudomonal activity (broad-spectrum penicillins or third-generation cephalosporins with antipseudomonal activity, fourth-generation cephalosporins, carbapenems). A fluoroquinolone plus clindamycin could be used in patients with penicillin allergy. A fourth-generation cephalosporin or carbapenem would also cover the most probable pathogens, such as Gram-negative bacilli (even those with inducible p-lactamases), and would ensure a better coverage for S. aureus than a third-generation cephalosporin. In hospitals where methicillin-resistant S. aureus is a problem, these agents should be combined with a glycopeptide.
Key words: Nosocomial pneumonia, diagnosis, etiology, pathophysiology, prevention, treatment
Corresponding author and requests for reprints:
Professor P Francioli, Divisions of Hospital Preventive Medicine and of Infectious Diseases, CHUV, 101 1 Lausanne, Switzerland
Tel: +41 21 314 02 52 Fax: +41 21 314 02 62 e-mail: [email protected]
INTRODUCTION
Nosocomial pneumonia is the second most frequent hospital-acquired infection and is associated with high morbidity, mortality and increased hospital cost [l]. Nosocomial pneumonia occurs in 0.6-1%) of hospital
S61

S62 Clinical Microbiology a n d Infection, Volume 3 Supplement 1 , Apr i l 1997
admissions and 7-44% of ventilated patients in the intensive care unit (ICU). Overall, it accounts for 13-18% of all nosocomial infections, prolongs hospital stay by 7-10 days and is associated with a crude mortality of 20-60% and an attributable rnortality (the percentage of deaths which would not have occurred in the absence of pneumonia) of approximately 30%. In the ICU, pneumonia accounts for a higher proportion of nosocomial infections than in the hospital as a whole (35-45% in ventilated patients). Although the crude mortality is higher (40-80%) in the ICU, the attributable mortality in ventilated patients (27%) is similar to that seen in the hospital overall [2]. Nosocomial pneumonia is independently associated with death in ICU patients (Table l), although some recent studies have produced conflicting results [3,4].
In one of these studies, the predictors of mortality were examined in two populations of patients in the ICU, namely, those who survived and those who died. Nosocomial pneumonia was shown to be a significant factor associated with increased mortality, with an odds ratio of 2.08, similar to that of nosocomial bacteremia [3].
If the mortality rate in ventilated patients is examined in more detail, it can be seen that different niortality rates may be attributable to different causative organisms. For example, Pseudomonas spp. and Acinetobacter spp. may be responsible for a mortality rate of up to 43% and even > 70% [2]. An effective strategy for the prevention of nosocomial infections in the ICU should significantly reduce mortality, but to assess potential strategies, it is essential to achieve a consistent diagnosis.
DIAGNOSIS
All studies regarding epidemiology, pathophysiology, risk factors, treatment, prognosis and prevention of pneumonia are hampered by the same problem - the difficulty in diagnosing pneumonia. Criteria used
clinically to define nosocomial pneumonia include fever, new or progressive pulmonary infiltrate on X-rays, leukocytosis, purulent bronchial secretions and a tracheal aspirate Gram’s stain showing > 25 leukocytes and < 10 squamous epithelial cells (a sign of sample contamination) per low-power field, associated with recovery of a potential pathogen [5]. Fever and infiltrate, however, are by no means specific for pneumonia. In the case of mechanically ventilated patients in particular, there are many other alternatives which need to be considered. Fibroproliferation of late adult respiratory distress syndrome (ARDS), pulmonary embolism atelectasis, drug reactions, congestive heart failure and pulmonary hemorrhage all show similar clinical signs and may mimic pneumonia. The presence of microorganisms in a tracheobronchial specimen may represent colonization or infection. Thus, efforts have been made to develop appropriate diagnostic testing, including changes in plasma concentration of C-reactive protein [6] or changes in serum concentration of procalcitonin [7] to determine whether the patient has pneumonia, to identifj the pathogen and to help define the best therapeutic regimen. Lung specimens taken for histology and culture are considered to be the ‘gold standard’ in the diagnosis of pneumonia. The criteria for histopathologic diagnosis of pneumonia include the presence of neutrophilic infiltration of the terminal bronchioles and of the alveoli, which may be filled with neutrophils, fibrinous exudates and cellular debris (resulting from lung necrosis) which may be seen by Gram’s stain [8]. For certain microorganisms, specific methods should be used. The etiological diagnosis is established by identification of the pathogen(s), generally by culture. There are major problems, however, with the gold standard method. Firstly, the invasive nature of the technique means that these specimens cannot be obtained for most episodes of pneumonia; secondly, if there is a lung biopsy or autopsy, it may not be obtained at the same time as the pneumonic episode, making it difficult to
Table 1 Variables independently associated with death in ICU patients
Variable Odds ratio P
APACHE I1 score No. of dysfunctional organs Nosoconiial pneumonia Nosocomial bacteremia Fatal underlying disease Adnlission from other ICU
1.08 1.54 2.08 2.51 1.76 1.30
<0.001 <0.001 <0.001 <0.001 4 . 0 0 1 0.04
~ ~ ~ ~~~
From Fagon et al. 1996 [3 ] . With permission of the American Medical Association.

Franc io I i : V e n t i la t o r -ass o c i a t e d pn e u m o n i a S63
be sure that the findings relate to a particular clinical episode of pneumonia. Moreover, the empiric use of antibiotics to treat the episode may invalidate direct examination or culture results. In ventilated patients lung 1iistolobT is usually only used in post-mortem studies.
Given this problem of diagnosis, improved, less iiivasive methods have been developed. The most important of these are listed in Table 2 [4,9-321. It should be borne in mind that sensitivity and specificity are always measured in relation to another method which will, in itself, have advantages and disadvantages. Thresholds have evolved from various studies, for which the sensitivity and specificity vary, depending on how tlie criteria were balanced. Results from a recent meta-analysis suggest that the use of a predetermined threshold concentration of bacteria for either protected specimen brushing (PSB) or bronchoallveolar lavage (BAL) may riot be appropriate in all clinical settings and that incorporating the clinical :likelihood of pneumonia into the evaluation could significantly improve the sensitivity and specificity of these tests [33]. It can be seen from Table 2 that a n indisputable diagnosis cannot be reached using any of- the methods. Nevertheless, it is generally accepted i;hat PSB and BAL are currently the most accurate methods for diagnosing pneumonia. Although the sensitivity and specificity of these methods are highly variable, a recent study has shown sensitivities of 82% and 91% and specificities of 89% and 78% for PSB and BAL, respectively, compared with histologic and microbiologic post-mortem lung specimens, in the diagnosis of pneumonia [34]. However, other post- mortem studies have found lower sensitivities and/or specificities [4,35,36].
Both of these methods can be performed either through a bronchoscope or blindly, using an endobronchial catheter. PSB involves the passage of a
catheter into the distal airways and the extrusion of a small brush (protected inside the catheter by a biodegradable plug) for the recovery of secretions. BAL requires sequential instillation and aspiration of a physiological solution into a lung subsegnient through a catheter or a bronchoscope wedged in an airway. Mini-BAL (mBAL) refers to BAL using a smaller volume ofsolution (l(320 mL, rather than lO(3200 mL) instilled distally.
The specimen volume retrieved with PSB is much smaller (0.01-0.001 mL) than with BAL and the area of lung sampled is also smaller, such that the threshold for quantitative samples is usually higher for BAL (> lo4 CFU/mL) than for PSB (> lo3 CFU/mL). However, the risk of contamination is less for PSB and mBAL (protected) than for BAL. One advantage of BAL, however, is that it allows the sampling of enough material for direct examination by Gram’s stain and some studies have shown that the presence of visible intracellular bacteria is a good predictor of ventdator-associated pneumonia PAP) [37]. In addition, direct examination may help in the choice of initial antibiotic treatment.
PSB and BAL have their own problems. For example, when an examination was repeated using I’SB on the same patient twice, although 100% qualitative reproducibility was recorded, a 24-25% quantitative discordance in tlie numbers of niicroorganisms recovered was reported between the first and second examinations (16,381. This may have been caused by peripheral wedging of the brush, but means that for PSB, no quantitative threshold exists which absolutely separates patients with and without pneumonia [25], Also, many patients received antibiotics and it has been shown by Meduri et al. [39] that this can reduce the number of true positive results obtained by PSB quantitative culture from 77% in untreated patients, to 60% in those on antibiotic therapy. Recent studies
Table 2 Value of various methods for the nllcrobiological diagnosis of ventilator-associated pneumonia in patients with c h n i c ~ l and radiologcal signs compatible with pneumonia
Thrcshold Sensitivity Specificity Correct Diagnosis Refs (cfu/mL) (%) (“X) (%I)
Endotrachcal aspirate qualitative 57-88 33-14 quantitative 105- 1 Oh 67-9 1 92-59
Non bronchoscopic distal specimens 101-104 61-100 100-66 (naAL, PSB)
BAL B 104 72-1 00 100-69 Protected BAL t 104 82-92 97-83
Protected \pecinien brushing 2 103 64-100 95-60
9-13 72-83 14-10 70-100 4,i 0 3 - 2 2
69-90 23-26 72-03 27-29 84-96 30-32
Adapted from Griffin JJ et al. [51. With permission from Medical Clinics of North America.

S64 Cl in i ca l M i c r o b i o l o g y and In fec t i on , Volume 3 Supplement 1, April 1997
have shown that quantitative analysis of endotracheal aspirates appears to be of reasonable diagnostic value [40,41]. Investigations should be performed before introducing or changing antibiotic therapy [42]. If possible, antibiotic therapy should be discontinued for 48 h before PSB or BAL are used [42]. Increased levels of endotoxin has been shown to predict the prescence of Gram-negative pneumonia [43,44]. New diagnostic methods, such as the measure of procalcitonin levels in bronchial secretions are being investigated clinically [7].
In summary, despite the improvement in diagnostic methods, not all patients are correctly diagnosed as having pneumonia, with both under- and over- diagnosis being a problem. Better communication is necessary to achieve optimal diagnosis.
ETIOLOGY AND PATHOPHYSIOLOGY
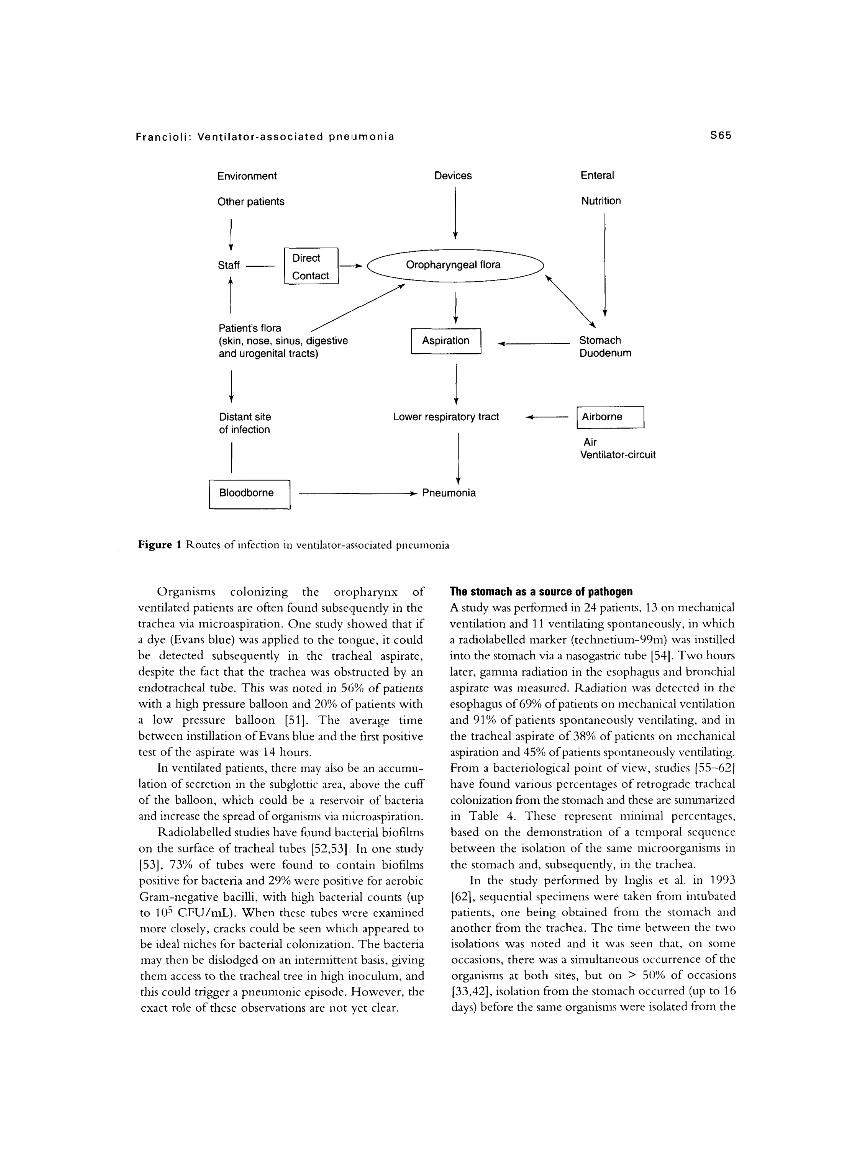
Table 3 shows the causative organisms of pneumonia in ventilated patients. The spectrum vanes according to regional differences, underlying disease and previous antibiotic treatment. In many cases knowledge of the sources of these organisms helps in understanding the pathophysiology of the infection. Often, the source is endogenous, but the organism may also come from the environment, from other patients or from hospital staff (Figure 1). Devices and other equipment are currently less of a problem, now that they are recognized sources of infection and aseptic handling and equipment have improved. Cross-infection from other patients and staff may be minimized, provided that human resources are adequate and that motivation is high.
Episodes occurring within the first few days after intubation (early-onset pneumonia: 4 days has been proposed as an arbitrary time point) [45] are mostly caused by bacteria of the normal oropharyngeal flora. If certain factors are present, such as prior antibiotic
therapy, prolonged hospitalization or special host factors, there may be a different spectrum of microorganisms with different antibiotic susceptibilities, and this has important diagnostic and therapeutic implications. Episodes occurring after 4 days of intubation (late-onset pneumonia) are mostly due to Gram-negative bacilli or S. aureus.
The oropharyngeal flora as a source of infection Microorganisms colonizing the trachea and the lung rarely originate from the hematogenous route, but are derived mainly from oropharyngeal flora or from the gut [46,47]. Infection ofthe respiratory tract will depend on the numbers and virulence of the inoculated organisms balanced against the efficiency of mechanical, cellular and humoral lung defence mechanisms. Soon after patients enter an ICU, their oropharynx becomes colonized with Gram-negative bacilli [48] and this is associated with a higher rate of pneumonia compared with patients who have no colonization. For example, in a study of 213 intensive care patients, 23% of those with oropharyngeal colonization developed nosocomial pneumonia, whereas pneumonia was seen in only 3.3% of non-colonized patients [49]. There are, of course, a number of other contributory risk factors and these will be addressed later.
It is not known precisely why the oropharynx becomes colonized with Gram-negative bacilli, but one important cause is thought to be stress, which leads to the secretion of enzymes that alter receptors at the surface of the pharyngeal cells. These alterations of pharyngeal cells promote adhesion by Gram-negative organisms. Johaiison et al. [SO] showed that brief exposure of buccal epithelial cells to trypsin increased the adherence of Pseudomonas aevuginosa ten-fold as compared to cells from non-colonized patients. This phenomenon has been recently discussed [47].
Table 3 Microorganisms causing ventilator-associated pneumonia
Early-onset pneumonia Late-onset pneumonia Other
Streptococcus pneumoniae Pseudomonas aenrginosa Haemophilus influenzae Enterobacter spp. Murawella catarrhalis Acinetubacter spp, Staphylococcus aureus K/ebsiella pneumoniae Aerobic Gram-negative bacillia Serratia marcescens
Escherichia coli Other Gram-negative bacilli Staphylococcur aureusb
Anerobic bacteria< Legionella pneumophila Influenza A and B Respiratory syncitial vims Fungi
a h patients with nsk factors. blncluchng methidin-resistant S aureus CFrom [46]
Franc i o I i : Vent i I at o r-a sso c i at e d p n e IJ rn o n i a S65
Environment Devices Enteral
Other patients Nutrition
Direct
Contact Staff -
Duodenum
Patient's flora
and urogenital tracts)
c Distant site of infection
c Lower respiratory tract - -1
Air Ventilator-circuit
J. - Pneumonia
Figure 1 Routes of infection in ventilator-associated pneumonia
Organisms colonizing the oropharynx of The stomach a s a source of pathogen - . ventilated patients are often found subsequently in the trachea via microaspiration. One study showed that if a dye (Evans blue) was applied to the tongue, it could be detected subsequently in the tracheal aspirate, despite the fact that the trachea was obstructed by an endotracheal tube. This was noted in 56% of patients with a high pressure balloon and 20% ofpatients with a low pressure balloon [51]. The average time between instillation of Evans blue and the first positive test of the aspirate was 14 hours.
In ventilated patients, there may also be an accumu- lation of secretion in the subglottic area, above the cuff of the balloon, which could be a reservoir of bacteria and increase the spread of organisms via microaspiration.
Radiolabelled studies haye found bacterial biofilms on the surface of tracheal tubes [52,53]. In one study [53], 73% of tubes were found to contain biofilms positive for bacteria and 29% were positive for aerobic Gram-negative bacilli, with high bacterial counts (up to lo5 CFU/mL). When these tubes were examined more closely, cracks could be seen which appeared to be ideal niches for bacterial colonization. The bacteria may then be dislodged on an intermittent basis, gving them access to the tracheal tree in high inoculum, and this could trigger a pneumonic episode. However, the exact role of these observations are not yet clear.
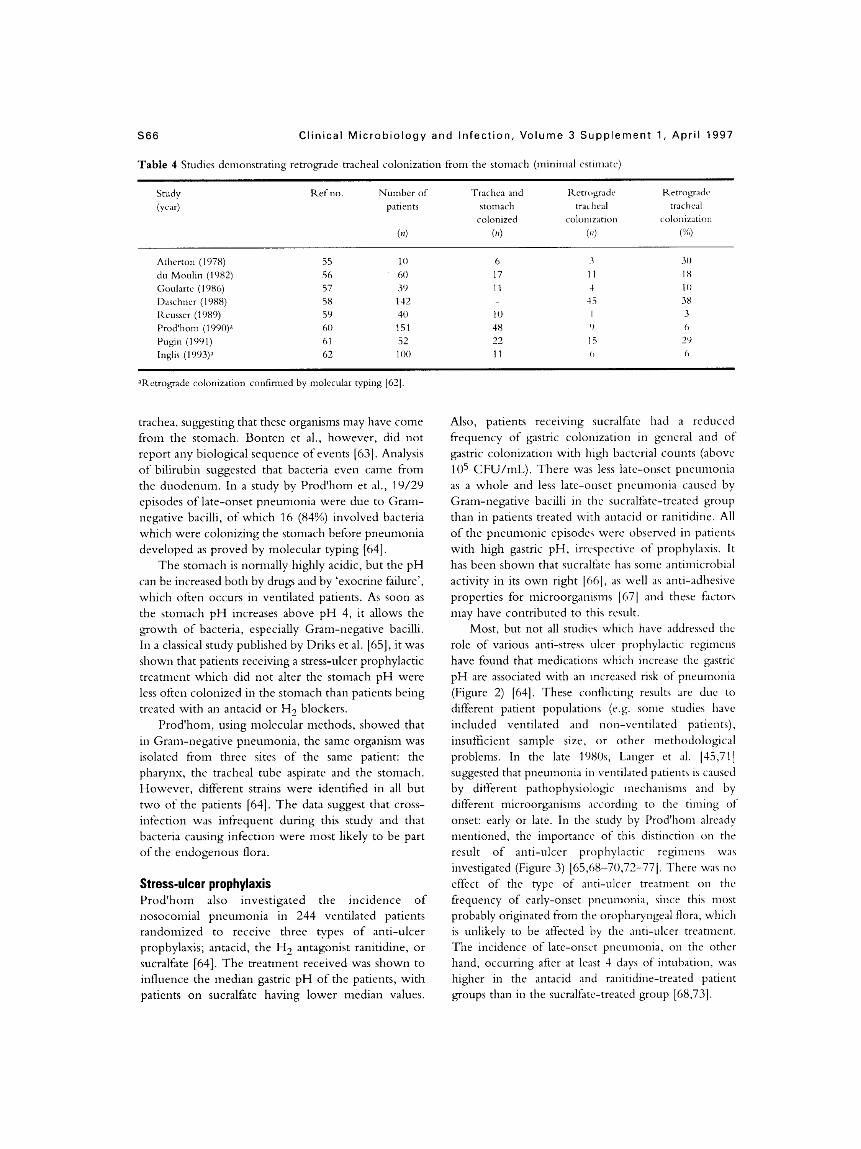
A study was performed in 24 patients, 13 on mechanical ventilation and 11 ventilating spontaneously, in which a radiolabelled marker (technetium-99m) was instilled into the stomach via a nasogastnc tube [54]. Two hours later, gamma radiation in the esophagus and bronchial aspirate was measured. Radiation was detected in the esophagus of 69% of patients on mechanical ventilation and 91% of patients spontaneously ventilating, and in the tracheal aspirate of 38% of patients on mechanical aspiration and 45% of patients spontaneously ventilating. From a bacteriologcal point of view, studies [55-621 have found various percentages of retrograde tracheal colonization f?om the stomach and these are summarized in Table 4. These represent minimal percentages, based on the demonstration of a temporal sequence between the isolation of the same microorganisms in the stomach and, subsequently, in the trachea.
In the study performed by Inglis et al. in 1993 [62], sequential specimens were taken from intubated patients, one being obtained from the stomach and another from the trachea. The time between the two isolations was noted and it was seen that, on some occasions, there was a simultaneous occurrence of the organisms at both sites, but on > 50% of occasions [33,42], isolation from the stomach occurred (up to 16 days) before the same organisms were isolated from the
S66 Cl in i ca l M i c r o b i o l o g y a n d In fec t i on , Vo lume 3 S u p p l e m e n t 1, A p r i l 1997
Table 4 Studies dcrnonstrating retrograde tracheal colonization from the stomach (minimal estimate) ~~~
Ketrograde Ketrogradc
colonized L~lO~llZdtlOil colonization
Ref no Number of Trachca and patients ctomach tracheal trachcd
(4 (4 (4 (Xj
Atherton (1978) 55 10 6 3 30 du Moulin (1982) 56 60 17 1 1 18 Goularte (1986) 57 39 11 4 1 0 Daqchner (1988) 58 142 45 38 Krusser (1989) 59 40 10 I 3 Prod'hom (1990)a 60 151 48 0 6 Pugin (1991) 61 52 22 15 29 Inglis (1993)a 62 100 11 0 6
aRetrograde colonization confirmed by molecular typing [62]
trachea, suggesting that these organisms may have come from the stomach. Bonten et al., however, did not report any biological sequence of events [63]. Analysis of bilirubin suggested that bacteria even came from the duodenum. In a study by Prod'hom et al., 19/29 episodes of late-onset pneumonia were due to Gram- negative bacilli, of which 16 (84%) involved bacteria which were colonizing the stomach before pneumonia developed as proved by molecular typing [64].
The stomach is normally highly acidic, but the pH can be increased both by drugs and by 'exocrine failure', which often occurs in Ventilated patients. As soon as the stomach pH increases above pH 4, it allows the growth of bacteria, especially Gram-negative bacilli. In a classical study published by Driks et al. [65], it was shown that patients receiving a stress-ulcer prophylactic treatment which did not alter the stomach pH were less often colonized in the stomach than patients being treated with an antacid or H2 blockers.
Prod'hom, using molecular methods, showed that in Gram-negative pneumonia, the same organism was isolated from three sites of the same patient: the pharynx, the tracheal tube aspirate and the stomach. However, different strains were identified in all but two of the patients [64]. The data suggest that cross- infection was infrequent during this study and that bacteria causing infection were most likely to be part of the endogenous flora.
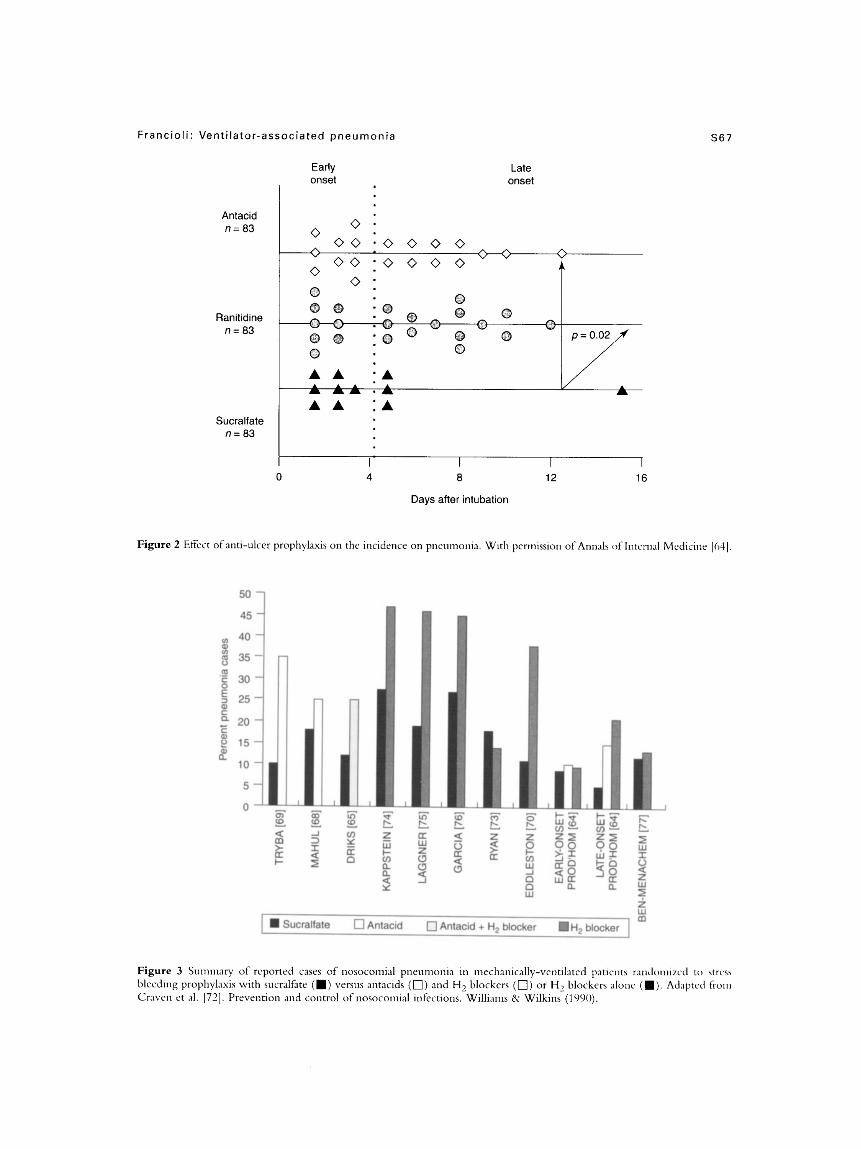
Stress-ulcer prophylaxis Prod'hom also investigated the incidence of nosocomial pneumonia in 244 ventilated patients randomized to receive three types of anti-ulcer prophylaxis; antacid, the H2 antagonist ranitidine, or sucralfate [64]. The treatment received was shown to influence the median gastric pH of the patients, with patients on sucralfate having lower median values.
Also, patients receiving sucralfate had a reduced frequency of gastric colonization in general and of gastric colonization with high bacterial counts (above lo5 CFU/mL). There was less late-onset pneumonia as a whole and less late-onset pneumonia caused by Gram-negative bacilli in the sucralfate-treated group than in patients treated with antacid or ranitidine. All of the pneurnonic episodes were observed in patients with high gastric pH, irrcspective of prophylaxis. It has been shown that sucralfate has some antimicrobial activity in its own right [MI, as well as anti-adhesive properties for microorganisms [67] and these factors may have contributed to this result.
Most, but not all studirs which have addressed the role of various anti-stress ulcer prophylactic regimens have found that medications which increase the gastric pH are associated with an increased risk of pneumonia (Figure 2) [64]. These conflicting results are due to different patient populations (e.g. some studies have included ventilated and non-ventilated patients), insufficient sample size, or other methodological problems. In the late 198Os, Langer et al. 145,711 suggested that pneumonia in ventilated patients is caused by different pathophysiologic mechanisms and by different microorganisms according to the timing of onset: early or late. In the study by Prod'hom already mentioned, the importance of this distinction on the result of anti-ulcer prophylactic regimens was investigated (Figure 3) [65,68-70,72-771. There was no effect of the type of anti-ulcer treatnient on the frequency of early-onset pneunionia, siiice this most probably originated from the oropharyngeal flora, which is unlikely to be affected by the anti-ulcer treatnient. The incidence of late-onset pneumonia, on the other hand, occurring after at least 4 days of intubation, wa7 higher in the antacid and ranitidine-treated patient groups than in the sucralfate-treated group [68,73].
Franc i o I i : Vent i I a t o r - a ss o c i a t e d p n e u m o n i a S67
Late onset
Early onset
Antacid n = 83
Ranitidine n = 8 3
Sucralfate n = 8 3
0 4 8 12 16
Days after intubation
Figure 2 Effect of anti-ulcer prophylaxis on the incidence on pneumonia. With permission of Annals of Intcmal Medicine 1641.
50 1
W
l rn
Figure 3 Summary of reported cases of nosocornial pneumonia in mechanically-ventilated patients randomized to <trCss bleeding prophylaxis with sucralfate (m) versus antacids (0) and H, blockers (0) or H2 blockers alone ( Craven et al. [72]. Prevention and control of nosocotnial infections. Willianis & Wilkins (1990).

S68 Clinical M ic rob io logy
Despite numerous studies addressing the choice of anti-stress ulcer prophylaxis, controversy persists as to whether or not sucralfate should be preferred to other regimens [69]. I n a large meta-analysis sucralfate was found to be associated with a lower incidence of nosocomial pneumonia when conipared with antacids (OR 0.80 CL 0.56-1.15) and H2 receptor antagonists
Selective digestive decontamination (SDD) is a controversial preventive nieasure [79]. It involves the use of oral, intestinal aiid often systemic antibiotics to eliminate all potential pathogeiis from the upper respiratory and gastrointestinal tracts. The use of SDD reduced thc incidence of pneumonia in a rneta-analysis carried out by the Selective Decontamination of the Digestive Tract Trialists’ Collaborative Group on 22 randonllzed, controlled studies, evaluating approximately 4,000 patients 1801. This nieta-arialysis showed that, although a significant reduction in the incidence of pneunionia/respiratory tract infection was seen in treated patients (OR 0.37 93% CL 0.31-0.43), the valuc of the coninion odds ratio for the overall mortality (OR 0.90 95% CL 0.79-1.04) suggested a t best a moderate treatment effect. Better results in the reduction of mortality were found only if trials that conipared topical SDD plus early systemic antimicrobial treatment or placebo (OR 0.80 95% CL 0.67-0.97) were included. A3 there were large variations in the case mix, the sevciity and the SDD protocols, no firm coiiclusions can be drawn regarding the effect of SDD on niortality in ventilated patients.
An important probleni with SDD is the potential for selection of antibiotic-resistaiit organisms 1811. Further investigation is required to more clearly
(OR 0.77 C L 0.60-1.01) [78].
and Infection, Volume 3 Supplement 1, Apr i l 1997
identify the patients who could benefit from such an approach (821.
PREVENTION
Risk factors and associated preventive measures are surnniarized in Table 5. Some risk Eictors, such AS age (> 60 years), pulmonary disease, organ hilure, coma, gr o s s asp ira t i o 11, c i gar e t t c sin o ki 11 g , di a b e t e s , hypotension, alcoholism, diseases of the central nervous system, chronic obstructive lung disease, azotemia and respiratoiy failure are patient-related [ 11 aiid thus difficult to modify. Other risk factors are dependent on drug prescription. The stress-ulcer prophylaxis regimen has been mentioned, but the use of certain other drug arc also risk factors. Sedatives, corticosteroids and cytotoxic agents niay impair host defences. Antibiotic prophylaxis or treatment given prior to an episode of nosocomial pneumonia niay select for resistance and thus reduce therapeutic options. Endotracheal prophylactic gentarnicin was shown to be ineffective in preventing pneumonia and associated with the occurrence of gentamicin-resistant bacteria
Effective preventive measures have been demonstrated in several studies [84]. Two studies have suggested that removal of subglottal secretions, using either a specifically designed endotracheal tube or a catheter, may decrease the risk of pneumonia 164,851. I n the study by Valles et al., patients with continuous subglottic aspiration were less likely to develop pneumonia than those without subglottic aspiration 1851. The incidence ratc of VAP was 19.9 episodes/1000 ventilator days in patients undergoing continuous
(831.
Table 5 Risk factors for ventilator-associated pneumonia and principles of prevention
Risk Factor Prevention
Host 0 age > 60 yexrs
pulinonary disease organ failure, coma gross aspiration
Medical 0 dui-ation of meclianical vcntilaaoii
route of intubation 0 rcintubation
cross infection 0 equipment 0 oropharyngeal aspiration 0 gastric pH and colonization 0 gastric tnicroaspiration 0 prior antibiotics
primary prevention
device rcnioval as ~ o o n as possible prefer oral intubation avoid sclf extubation/reintubation ascptic care, standard precautions, isolation appropriate maintenance, disinfection aspiration o f subglottic secretions prefer mcralfate to H, blockcrs/antacid semi-upright position proper use of antibiotics

F r a n c i o I i : Vent i l a t o r - a s s o c i a t e d p n E! u rn on ia S69
aspiration and 39.6 episodes/? 000 ventilator days in the coiitrol group. The difference caused by a significant reduction iii tlie number of infections due to Gramii-positive cocci and H . ir$irerrzoc in those receiving continuous aspiration (p < 0.03). New tubes x c currently bciiig introduced which allow aspiration 011 J continuous basis, although these tubes do have problems in their own right, such as ~:ontaiiiination and blockage of tlie luinen.
Aiiotlicr recommendation is that both endotracheal and gastric tubes are inserted orally, rather than nasally. Kouby et al. [Xh] sliowcd the incidcnct of sinusitis to be linked to nasal placemelit. Moreovrr, nosoconiial piieuiiioiiia occurred sigiiificaii tly iiiort frequently in patients with maxillary sinusitis (67%) than in those without (43%) (p = 0.002). These results have been confirmed in another study 1871.
A simple i i~cas~ire to partially prevent esophageal reflux is to put the patient in a semi-rccumbeiit position, which has been sliowii to decrease the recovery rate of identical niicroorga~iisnis in the storiiacli, pharynx and trachea (32'%,), con~pared with patients in the supine position (68'%1). However, this is not feasible for all veiitildted patients ISXI.
The incidence of pneuinonia is iiicreased if the ventilator circuit is inanipulatcd frequently and it is now reconimeiidcd to change it only evt-iy 72 hours or longer. Some recent studies suggest that it can be safely maintained for up to 7 days 1891. Cortdensatc in the tubing cai i also be a reservoir of pathogens and should be drained away from the patient; heat and moisture exchangers might avoid tlie problem of condensation a n d prevent colonization, thus perrnithg the use of the same circuit for a longer period of tinic.
Many pathogens, such as P. ncrtlginosu and S . ( I C ~ I T I ~ S ,
survive well in the external environnieiit. Handliiig of devices and equipment should therefore be minimal. Aseptic technique and good hygiene, with frequent hand washing or gloves for staff, isolation of patients with resistant pathogens and appropriate disinfection of equipnient can decrease environmental and cross-contaiiiiiiation.
Mal~ititrition is a known risk factor for nosocomial pneunionia a i i d has led to the use of nutritional support in hospitalized patients. There is no clear evidence that nutritional support reduces the risk of pneunioiiia, however, and care iiiust be taken regarding preparation, handling, route and voluiiie of feeding. Enteral nutrition niay stimulate the intestinal rnucosa and the immune system 1901, but any increase in gastric pH and volume could increase the number of potential pathogens in the stomach 1631. When possible, the tube should preferably be inserted beyond the stomach.
EMPlRlC TREATMENT
Appropriate diagnostic iiiicrobiologic'il procedures should be performed prior to the initiation o f treatment. Although a number of recent advcuices have been made in the diagiiosis, prevention and treatment of nosoconiial pneunionici, controversic~ still remain and a standardized managcnient approach docs not yet exist, mainly because of diagnostic problems. The clinical and radiologiccil signs of pneunionia caii be associated with a number of c;iiiscs, particularly in ventilated patients in thc ICU, and thc way in which these are interpreted differs bctwccti physicians. For example, if a p t ien t presents with lung infiltrate on X-ray, fever and raised whitc blood cell count, in most casc-s Iic wil l receive a n enipiric course of antibiotic treatment. If, howevcr, there is no iinprovement aftrr 48 hours and the diagnostic tests (e.g. PSI3 or BAL) do no t suggest a bacterial etiology, sonic physicians \vould suspciid antibiotic therapy and obsen-c tlie paticnt. Other physicians may prefer to continue a i l tihiotic therapy and increase the dosage o r modifi. the reginicii, suspecting the presence of a more resimnt or unusual pathogen which w x not detected. I n order t o guide physicians, various recoiii~iic~idationc have heel1 issued. Thew are based on a good uncierstanding of the etiopatliopliysi[)lo~~ and of risk factors. I t is iniportant to stress that therapeutic cipproaclics vary according to the type of patient. Only nosocomial pneumonia in ventilated patients is considered in the present article.
Early- and late-onset p i i ~ t i ~ n o i i i ~ ~ in ventilated patients have different bacterial etiology. For cxaniple, early-onset pneunioriia is likely to be c'iused by pathogens which are norni,il inli~ibitants of the oropharyngeal cavity, such as S. prrc~rn iorr inr~ , which c'aiises 5-10% of infections, H m ~ i z ~ y ~ ~ i i / i ~ ~ i ~ ! j ' / w t ~ ~ ,
responsible for 546 of infections, o r mixed flora, including ancrobes. S. U U ~ B M S is dso '1 frequent cause of early-onset pneumonia. Conversely, aerobic Gram- negative bacilli, which arc responsible for at least 60(% of cases of pneumonia, are more likcly to be involved in late-onset piicuinonia. S. O I I Y ~ Y I S also accounts for 20-25% of the episodes in late-onset pncmionia.
Pathogens which are more likely to arise from exogenous sources, such as P. ncriiyirrosn, i l c i r i c d m t w spp. and ~iicthicilliii-resistant S . nurcwx, Lire also usually involved in late-onset pneumonic episodes. The differences in likely causative organisins, depending on the time of onset of tlie pneumonic episode, should be borne in niind w-lien choosing enipiric therapy for these infections. It is also very iinportant

570 Clinical M icrob io logy and Infect ion, Volume 3 Supplement 1 , Apri l 1997
to take into account the epidemiology and antibiotic susceptibility pattern of each institution.
Patients with early-onset VAP and patients with no risk factors can be treated initially with agents such as p-lactams plus 0-lactamase inhibitors or second- or third-generation cephalosporins (Table 6). The choice of a third-generation cephalosporin in this situation may be justified by cost consideration in certain countries, such as the USA. For patients with late-onset pneumonia, or early-onset pneumonia plus associated risk factors, such as prior antibiotics, recent hospitalization or a severe underlying condition, a broader-spectrum antibiotic is recommended, such as broad-spectrum penicillin or thrd-generation cephalosporin, with anti-pseudomonal activity (including broad-spectrum p-lactam/p-lactamase inhibitors), or a carbapenem. A fourth-generation cephalosporin, such as cefpirome or cefepime as single agent may be considered. An alternative therapy for patients who cannot be treated with p-lactam antibiotics is the use of an intravenous fluoroquinolone. Vancomycin may be added for initial therapy in hospitals where there is a high prevalence of methicdhn-resistant staphylococci and anti-anerobic compounds added when anerobes are felt to play a predominant role.
In a recent consensus of the American Thoracic Society, two treatment schemes were recommended in this situation [l]. These are based on the severity of the infection, the timing of occurrence of pneumonia (early- versus late-onset) and the presence of risk factors. The main difference from our recommendations is the use of an aminoglycoside or fluoroquinolone in combination with a p-lactam. One study has shown no difference in the success rate between treatment with imipenem alone and imipenem plus netilmicin in patients with nosocomial pneumonia and sepsis
[91]. It has been suggested, however, that the presence of an aminoglycoside in severe cases may improve the activity of p-lactam antibiotics which are less potent than imipenem. For certain pathogens, such as Enterobactev and Pseudomonas spp. and in severe situations, combination therapy may be superior to monotherapy
Whichever treatment scheme is used, a p-lactam agent is generally included unless the patient is allergic to penicillin. This may be a p-lactam@-lactamase inhibitor combination, a second- or third-generation cephalosporin or a carbapenem. Considering the etiology of nosocomial pneumonia and the in vitro activity of various p-lactam antibiotics, fourth-generation cephalosporins, such as cefpirome or cefepime, are worthy of consideration as alternatives to the p-lactam antibiotics currently used. These compounds have excellent Gram-positive activity, covering penicillin- resistant pneumococci and methicillin-susceptible S . aureus, as well as an increased stability and lower affinity for inducible Gram-negative p-lactamases as compared to third-generation cephalosporins [92]. Although there is not yet a large amount of clinical data available on the efficacy of fourth-generation cephalosporins in nosocomial pneumonia, the Cefpirome Study Group reported on 91 patients with community-acquired or nosocomial pneumonia who received cefpirome intravenously [93]. Successhl clinical and bacteriological results were obtained in > 90% of patients. The authors concluded that cefpirome was an effective empiric treatment for moderate-to-severe pneumonia in hospitalized patients. However, difficult pathogens, such as Enterobacter cloacae and P. aevuginosa, were isolated in only a minority of patients. Although P. aevuginosa is probably covered adequately by
P11.
Table 6 Suggested initial empiric therapy of ventilator-associated pneumonia
Pneumonia Antimicrobial treatment”
Early-onsct, no risk factors p-lactam/p-lactamase inhibitorb Second- or thirdc-generation cephalosporin
Early-onset, risk factors, Late-onset d ~ k Broad-spectrum p-lactani/p-lactamase inhibitor“
p-lactam anti-pseudomonal spectrum
Fourth-generation cephalosporin Carbapenem Fluoroquinolone (iv)
aTo be adapted to microbiological data for the patient and institution. bThe combination of amoxicillin/clavulanic acid is supenor to anipicillin/sulbactam against pneumococci. ‘In sonie countries, third-generation cephalosporins are particularly cost-effective. %Some authorities would recommend the addition of an aminoglycoside in severe cases. CGlycopeptide to be added according to local epidemiology of methicillin-resistant staphylococci. fMetronidazole or clindamycin to be added when anti-anerobe coverage is indicated. rRisk factors (e.g. including prior antibiotic treatment) for alteration of the spectrum or susceptibility of microorganisms. “Ticarcillidclavulanic acid, piperacillidtazobactam.

F r a n cio I i : Ven t i l a t o r-asso cia t e d pn e u mon ia S7 1
cefpirome while awaiting microbiological results, other agents with improved activity against this organism should be selected when P. aevcrginosa is isolated.
A larger and more recent multicenter study compared the efficacy and safety of cefpirome and cefiazidime, either as monotherapy or in combination, with an aminoglycoside or metronidazole in the empiric treatment of 400 patients with nosocomial and community-acquired pneumonia in the ICU [94]. Clinical failure rates at the end of treatment were 34% vs 36% for cefpirome bid and ceftazidime tid, respectively, with no difference in outcome between monotherapy and combination therapy. In a non- comparative study, a satisfactory clinical response was obtained in 89% of patients receiving cefkpime bid [95]. Based on these studies, it can be assumed that fourth- generation cephalosporins are good alternatives to other broad-spectrum antibiotics for the treatment of nosocomial pneumonia.
CON CLU SI 0 N S
Nosoconllal pneumonia in ventilated patients is caused by a combination of factors resulting in a variety of etiologies. Precise microbiological diagnosis requires the appropriate critical use of invasive methods and close collaboration between clinicians and microbiologists. Understanding the pathogenesis and epidemiology of infection allows the clinician not only to define optimal preventive strategies, but also to decide upon optimal empiric therapy while awaiting microbiologcal results.
DISCUSSION
Prof. P. Francioli: The exact burden of VA pneumonia in terms of morbidity and rnortality is not well established and have been addressed specifically in only a few studies. Prof. A. Torres: Several papers have indicated that the attributable niortality of VA pneumonia is approximately 30%. However, this is controversial. For example, Papazian et al. recently suggested that the initial nlicrobiologcal diagnosis might be a confounding factor. In this study, attributable mortality was not due to VA pneumonia in itself but mostly related to the appropriateness of the initial empiric therapy. Prof. P. Francioli: Differences in the results of various studies might also be related 1.0 the method used for the diaposis of pneurnonix Hence, the diagnosis is the cornerstone of any study addressing the problem of VA pneumonia, but is hampered by the lack of a method which would be both highly sensitive and specific, and readily available. At the
present time, lung specimens taken for microbiological and histological examination are considered to be the ‘gold standard’ technique. Prof. A. Torres: There are problems associated with the ‘gold standard technique. In particular, these studies are almost exclusively post-mortem studies, and it is unlikely that a technique based on obtaining lung specimens is going to be widely available in clinical situation. Prof. W. Wilson: Given the problems of the ‘gold standard’ for the diagnosis of pneumonia, are there any recommendations regarding which technique is the most appropriate? Prof. J. Chastre: Several different techniques are available, but all of them are associated with methodological problems, and it remains unclear which is the most appropriate method. At this stage, BAL and PSB are considered to be the most accurate methods. Prof. P. Francioli: Recent studies have suggested quantitative culture of endotracheal aspirates might be as accurate as more invasive methods. Prof. J. Chastre: Yes, and this needs further investigation. It is important to emphasize that appropriate sampling should be obtained prior to initiation of antimicrobial treatment, when possible. Prof. P. Francioli: I n addition, appropriate samples should be obtained before any change in the antibiotic treatment. Prof. P. Shah: It should be mentioned that new methods for diagnosing pneumonia have been and are being investigated, such as measurement of the endotoxin or procalcitonine levels in bronchal secretions. These methods have shown promising results. Prof. P. Francioli: In recent years, progress in the prevention of VA pneumonia has been made. Environmental sources of infection have certainly been reduced by the systematic use of adequate hygienic measures. New devices such as cndotracheal tubes allowing the aspiration of subglottic secretions have been developed. Prof. A. Torres: Undoubtedly, these tubes appear to bring some progress. However. they Iiavc their ou7n problems, such as contamination or blockage of the lumen.
Moreover, studies were performed with prototypes and should probably be confirmed with the tubes which are now becoming available on the market. Prof. P. Francioli: Two preventive measures arc still controversial: the choice of anti-stress ulcer prophylaxis regimen and the selective digcstive decontaminatioii (SDD). Regarding the anti-stress ulcer prophylaxis regimen, meta-analysis of the existing studies suggest

572 Clinical M ic rob io logy a n d Infect ion, Volume 3 Supplement 1, Apri l 1997
that regmen which elevate the gastric pH might be associated with increased incidence of VA pneumonia. However, the most controversial measure is probably SDD. Dr. M. Langer: It is true that this measure is the most controversial, but this is more of an emotional than rational reaction. Hence, the data are very clear: there is no doubt that certain SDD regimens decrease the incidence of VA pneumonia. This is also confirmed by several meta-analysis. However, it is also true that no firm conclusion can be drawn regarding the effect of SDD on mortality. More studies are needed to identify which patients might benefit most from such a measure. The issue is emotional and controversial because of the risk of selecting resistant microorganisms. This risk might depend on the type of regimen used. More work is needed in this area. Prof. P. Shah: At the present time, one indication for the use of SDD might be an epidemic situation related to a multi-resistant microorganisms. Prof. P. Francioli: Regarding the initial empirical treatment of VA pneumonia, it is important to distinguish early-onset pneumonia from late-onset pneumonia. Prof. J. Acar: Could you clan@ this concept ? Prof. M. Langer: We were the first to describe the difference in the spectrum of microorpsms responsible for a pneumonia in relation to the time of onset of infection. In an Italian multicenter study, approximately 50% of the pneumonic episodes developed within the first 4 days after intubation. Most were due to bacteria recovered from the normal oropharyngal flora. In contrast, patients developing pneumonia at a later stage were most likely to be infected with Gram negative bacilli. The same was true for patients with early onset pneumonia and risk factors, such as patients with prior antibiotic treatment. This was confirmed by several other studies and fits with our present knowledge of the pathogenesis of VA pneumonia. This distinction is important for the treatment. Thus, initial empirical treatment of pneumonia will depend on the time of onset of the episode and the presence or not of risk factors. Prof. J. Acar: Anerobes are also responsible for episodes of early-onset pneumonia. Prof. M. Langer: This is particularly true when gross aspiration has occurred. In addition, some studies have showed that anerobes can be recovered in approximately 30% of pneumonic episodes. The exact role of this anerobes remain to be determined. Prof. P. Francioli: In patients with early-onset pneumonia and no risk factors, the first line regimen would be a p-lactam/p-lactamase inhibitor combination
or a second- generation cephalosporin. Should a third- generation cephalosporin (without antipseudomonal activity) also be recommended €or this indication? Prof. W. Wilson: Second-generation cephalosporin are unavailable in certain countries and are also more expensive than third-generation cephalosporins in many countries. This is true for the USA. Thus, third- generation cephalosporins should be included as alternative to second-generation cephalosporins in the treatment of early-onset pneumonia with no risk factors. Regarding the p-lactam@-lactamase inhibitor combinations, it should be mentioned that amoxicillin-clavulanate is more active than ampicillin- sulbactam against penicillin resistant pneumococci. However, parented amoxicillin-clavulanate is not available in the USA, where only ampicillin-sulbactam is commercialized. Prof. J. Acar: There are some data suggesting that nosocomial Gram-negative pneumonia may also occur after the first few days of intubation. Prof. A. Torres: This is true, but these patients generally have risk factors, mostly prior antibiotic treatment or a severe underlying disease. Prof. P. Francioli: Initial empirical therapy in these patients should be identical to that of patients with late-onset pneumonia. Prof. J, Chastre: We should emphasize that, whatever patient is considered, appropriate microbiological sampling should be performed before the initiation of empirical treatment. Moreover, empirical treatment should be adapted according to the microbiological results and the clinical response. Prof. P. Francioli: For late-onset pneumonia or for patients with early onset-pneumonia and risk factors, a broader coverage is needed as compared to early-onset pneumonia. This is due to the fact that the distribution of microorganisms is different and involves certain Gram-negative microorganisms such as the Pseudomonas, Enterobacter or Acinetobacter which are usually resistant to the antibiotics recommended for early-onset pneumonia. A broad-spectrum p-lactam with anti- pseudomonal activity or a carbapenem are the drugs of choice. In penicillin allergic patients, a fluoroquinolone combined with or without an anti-anerobe compound is an alternative. Prof. J. Acar: Third-generation cephalosporins with anti-pseudomonal activity carry the risk of encountering Enterobacteriacae producing inducible cephalosporinase and selecting for such resistant microorganisms. One should probably select agents such as cefpirome or cefepime, which may avoid the selection of resistant microorganisms. Prof. W. Wilson: The American Thoracic Society

Franc i o I i : V e n t i I a tor- a s s o c i a t e d p n e u m o n i a s73
recommends combination therapy for empirical treatment of VA pneumonia, mainly the combination of a broad-spectrum p-lactam (eg. a third-generation cephalosporin) and an aminoglycoside. Prof. P. Francioli: This is still a controversial issue. Some studies have demonstrated that adding gentamiciii or netilmicin to imipenem has not improved the outcome of patients with nosocomial pneumonia. Whether or not this is true for agents other than carbapenenu remains to be determined. However, some subgroups of patients might benefit from combination therapy, in particular those with Pseudornorzas, Enterobactcr or Acinetobacter infections. For the other cases, a carbapenem, a fourth-generation cephalosponn or piperacillin-tazobactam are probably :adequate first- line empiric therapy for late-onset pneumonia. Prof. P. Shah: A combination therapy should probably be envisioned in the initial regimen of all severe cases. Prof. P. Francioli: Glycopeptides should be added to the treatment regimen according to the local epidemiology of MRSA infections. This, is particularly true if Gram-strain of the bronchial sp'xirnen shows Gram-positive cocci. Dr. M. Langer: It should be remembered that S. aureus is also a frequent pathogen encountered in early-onset pneumonia. However, in this instance., S. au~eus has been community-acquired and is generally susceptible to methicillin. Prof. P. Francioli: This discussion illustrates that there are still many open questions in the field of ventilator- associated pneumonia.
References 1.
2.
3 .
4.
5.
6.
American Thoracic Society. Hospital-acquired pneumonia in adults: Diagnosis, assessment of severity, initial antimicrobial therapy and preventative strategies. Am J Kespir Crit Care Med 1995: 153: 1711-25. Fagon JY, Chastre J, Hance A, Montravers P, Novara A, Gibert C. Nosocomial pneumonia in ventilated patients: a cohoa study evaluating attributable morthty and hospital stay. Am J Med 1993: 94: 281-8. Fagon JY, Chastre J, Vuagnat A, Trouillet JL, Novara A, Gibert C . Nosocomial pneumonia and mortality among patients in intensive care units. JAMA 1996; 275: 866-9. Papazian L, Fabieiiue B, Thinon X, et al. Effect on ventilator-associated pneumonia on mortality and morbidity. Am J Respir Crit Care Med '1996; 154: 91-7. Griffin JJ, Meduri GU. New approaches in the diagnosis of nosocomial pneumonia. Med Clin North Am 1994; 78:
Adnet F, Bekka R, Vicaut E, et al. C-reactive protein (CKP) as an indicator to detect bacterial contamination of aspiration pneumonia. 9 t h European Congress on Intensive Care Medicine, Glasgow, 1996. (abstr. 527).
1091-112.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
Al-Nawas B, Krammer 1, Shah PM. Procalcitonin in diagnosis of severe infections. Eur J Med Res 1995/96;
Fabregas N, Torres A, El Ebiary M, et al. Histopathologic and Microbiologic aspects of ventilator-associated pneumonia. Anesthesiology 199h: 84: 760-71. Berger R, Arango L. Etiologic diagnosis of bactenal nosocomial pneumonia in serioudy ill patients. Crit Care Med 1985: 13: 833-6. Torres A, De la Bellacasa JP, Kodnguez-Kiosin R, L k Ante MT, Agusti-Vidal A. Diagnostic value of telescoping plugged catheters in niechanicdly ventilated patients with bacterial pneumonia using metras catheter. Am Rev Respir Dis 1988: 138: 11 7-20. Hill JD, Ratliff JL, Parrott JCW, et al. Pulmonary pathology in acute respiratory insufficiency: Lung biopsy as a diagnostic tool. J Thorac Cardio Surg 1976; 71: 64-71. Villers D, Derienic M, Raffi R, et al. Reliability of the bronchoscopic protected catheter brush i n intubated and ventilated patients. Chest 1985; X8: 527-30. Larnbert RS, Vereen LE, George RB. Cornparisori of tracheal aspirates and protected brush catheter specimens in identifying pathogenic bacteria in mechanically ventilated patients. Am J Med Sci 1989; 297: 377-82. El-Ebiary M, Torres A, Gonzalcz J, et al. Didgnosi\ of ventilator-associated pneumonia (VA). Ihagnostic value of quantitative cultures of endotracheal aspirates (EA). Am Rev Respir Dis 1991; 143: 108. Sauaia A, Moore FA, Moore EE, Haenel JB, Kaneer L, Kead R A . Diagnosing pneumonia in mechanically ventilated trauma patients. J Trauma 1993; 35: 512-7. Marquctte CH, Herengt F, Mathieu D, et al. Diagnosis of pneumonia in niechanically ventilated patients: Kcpeatability of protected specimen brush. Am Kev Resp Dis 1993; 147: 211-4. Torres A, El-Ebiary M, Gonzalez J. Gastric and pharyngeal flora in nosocomial pneumonia acquired during ventilation. Am Kev Respir Di\ 1993: 148: 352-7. Salata R A , Ledemian MM, Shlaes DM, ct al. Diagnosis of nosocomial pneumonia in intubated, intensive care unit patients. Am Rev Kespir r)is 1987; 135: 426-32. Novara A, Jourdain B, Jolly ML. Lhgnostic value of quantitative cultures of endotracheal aspirates in mechanically-ventilated patients clinically suspected of having developed bacterial pneumonia. In l'rograni and Abstracts of the 33rd Interscieuce Conference 1993 (abstract 857). Middleton RM, Huff W, Kirkpatrick MU. Comparison of four methods to assess ainvay bactenoloby in the intubated mechanically ventilated patient. Am J Med Sci 1992; 304: 239-45. Gaussorgues P, Piperrio Ll, Uachniann P, et al. Comparison of nonbronchoscopic bronchoalveolar lavage to open-lung biopsy fix bacterial diagnotis of pulmonary infections in mechanically ventilated patients. Intens Care Med 1989; 15: 94-8. Rouby JJ, Rossignon MD, Niccolas MH, et al. A prospective study of protected bronchoalveolar lavage in
1: 331-3.

s 7 4 Clinical Microbiology and Infection, Volume 3 Supplement 1, Apri l 1997
23.
24.
25.
26.
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
the diagnosis of nosocomial pneumonia. Anesthesiology
Chastre J, Viau F, Brun P, et al. Prospective evaluation of the protected brush catheter for the diagnosis of nosocomial pneumonia. Am Rev Respir Care Med 1984; 130: 924-9. Baughman RP, Thorpe JE, Staneck J , et al. Use of protected specimen brush in patients with endotracheal or tracheostomy tubes. Chest 1987; 91: 233-5. Fagon JY, Chastre J, Hance AJ, et al. Detection of nosocomial lung infection in ventilated patients: Use of a protected specimen brush and quantitative culture techniques in 147 patients. Am Rev Resp Dis 1988; 138: 110-6. Torres A, De La Bellacasa JP, Xaubet A, et al. Diagnostic value of quantitative cultures of telescoping plugged catheters in mechanically ventdated patients with bacterial pneumonia. Am Rev Respir Dis 1989; 140: 306-10. Chastre J, Fagon JY, Soler P, et al. Diagnosis of nosocomial bacterial pneumonia in intubated patients undergoing ventilation. Comparison of the usefulness of bronchoalveolar lavage and the protected specimen brush. Am J Med 1988;
Guerra LF, Baughman PP. Use of bronchoalveolar lavage to diagnose bacterial pneumonia in mechanically ventilated patients. Crit Care Med 1990; 18: 169-73. Chastre J, Fagon JY, Bomet M, et al. Diagnosis ofbacterial pneumonia in intubated patients undergoing ventilation. Comparison of the usefulness of bronchoalveolar lavage and protected specimen brush. Am J Med 1992; 85: 499-506. Meduri GU, Balesla V. The role of bronchoalveolar lavage in magnosing non-opportunistic bacterial pneumonia. Chest
Castella J, Puzo C, Ausina V, et al. Diagnosis of bacterial pneumonia with a method of protected bronchoalveolar lavage. Eur Respir J 1991; 4: 407. Barreiro B, Dorca J, Catala I . Protected bronchoalveolar lavage with balloon-tipped catheter in the diagnosis of ventilator-associated pneumonia. Am Rev Respir Dis 1993; 147: A39. Baker AM, Bowton DL, Haponik EF. Decision making in nosocomial pneumonia: an analytical approach to the use of quantitative cultures. Chest 1995; 107: 85-95. Chastre J, Fagon JY, Bomet-Lesco M, et al. Evaluation of bronchoscopic techniques for the diagnosis of nosocomial pneumonia. AmJ Respir Crit Care Med 1995; 152: 23140. Torres A, El-Ebiary M, Padro L, et al. Validation of hfferent techniques for the diagnosis of ventilator-associated pneumonia: comparisons with immediate post mortem pulmonary biopsy. Am J Resp Crit Care Med 1994; 149: 324-31. Marquette CH, Copin MC, Wallet F. Diagnostic tests for pneumonia in ventilated patients: prospective evaluation of diagnostic accuracy using histology as a diagnostic gold-standard. Am J Respir Crit Care Med 1995; 151:
Torres A, El-Ebiary M, Fabregas N. Value of intracellular bacteria detection in the diagnosis of ventilator-associated pneumonia. Thorax 1996; Vol 51 (4): 318-84. Timsit JF, Misset B, Francoual S, et al. Is protected
1989; 71: 679-85.
85: 499-506.
1991; 100: 179-90.
1878-88.
specimen brush a reproducible method to diagnose ICU- acquired pneumonia? Chest 1993; 104: 104-8.
39. Meduri GU, Chastre J. The standardization ofbronchoscopic techniques for ventilator-associated pneumonia. Chest 1992;
40. A Court CD, Garrard CS. Nosocomial pneumonia in the ICU. In: Vincent JL eds. New perspectives on current Controversies 1995 Year Book of Intensive Care Medicine. Springer Verlag. Heidelberg Germany. 1995; 7726-47.
41. Jordain B, Novara A, Joly-Guillou M, et al. Role of quantitative cultures of endotracheal aspirates in the diagnosis of nosocomial pneumonia. Am J Crit Care Med 1995; 152: 240-6.
42. Allen RM, Dunn WF, Limper AH. Diagnosing venulator- associated pneumonia: the role of bronchoscopy. Mayo Chn Proc 1994; 69: 962-8.
43. Kollef MH, Eisenberg PR, Ohlendorf MF, Wick MR. The accuracy of elevated concentrations of endotoxin in bronchoalveolar lavage fluid for the diagnosis of Gram-negative pneumonia. Am J Resp Crit Care Med 1996; 54: 1020-8.
44. Pugin J, Auckenthaler R , Delaspre 0, van Gessel E, Suter PM. Rapid diagnosis of Gram-negative pneumonia by assay of endotoxin in bronchoalveolar lavage fluid. Thorax
45. Langer M, Cigada M, Mandelli M, et al. Prevention of pneumonia in an intensive care unit, a randomized multicenter clinical trial. Int Care Med 1987; 13: 342-6.
46. Dori P, Robert R, Grolhier G, et al. Incidence of anerobes in ventilator-assisted pneumonia with use of a protected specimen brush. Am J Resp Crit Care Med
47. Estes RJ, Meduri GU. The pathogenesis of ventilator- associated pneumonia. I . Mechanisms of bacterial trans- colonization and airway inoculation. Intensive Care Med
48. Johanson WG, Pierce AK, Sanford J, et al. Nosocomial respiratory infections with gram-negative bacilli: the significance of colonization of the respiratory tract. Ann Intem Med 1972; 77: 701-6.
49. Johanson WG, Pierce AK, Sanford JP. Changing pharyngeal bacterial flora of hospitalized patients: emergence ofGram-negative bacdli. N Engl J Med 1969; 281: 1137-40.
50. Johanson WG, Higueth JH, Chaudhuri TR. Bacterial adherence to epithelial cells in bacillary colonization of the respiratory tract. Am Rev Respir Dis 1980; 121: 56-63.
51. Spray SB, Zuidema GD, Cameron JL. Aspiration pneumonia. Am J Surg 1976; 131: 701-3.
52. Sottile FD, Mame TJ, Prough DS, et al. Nosocomial pulmonary infection: possible etiologic significance of bacterial adhesion to endotracheal tubes. Crit Care Med
102: S557-64.
1992; 47: 547-549.
1996; 253: 1292-8.
1995; 21: 365-83.
1986; 14: 265-70. 53. Inglis TJJ, MiUar MR, Jones JG, et al. Tracheal tube
biofilm as a source of bacterial colonization of the lung. J Clin Microbiol 1989; 27: 2014-8.
54. Ibanez J, Penafiel A, Raurich J, et al. Gastroesophageal reflux and aspiration of gastric contents during nasogastric feedmg; the effect of posture (abstract). Intensive Care Med 1988; 14 (suppl 2): 296.
Franc io l i : Ven t i l a to r -assoc ia ted p n e u m o n i a s75
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
70.
Atherton ST, White DJ. Stomach as a source of bacteria colonizing the respiratory tract during artificial ventilation. Lancet 1978; 2: 968-9. du Moulin GC, Paterson DG, Hedley-White J, et al. Aspiration of gastric bacteria in antacid-treated patients: a frequent cause of postoperative colonization of the airway. Lancet 1982; 1: 242-5. Goularte TA, Lichtenberg DA, Craven DE. Gastric colonization in patients receiving antacids and mechanical ventilation: a mechanism for pharyngeal colonization. (Abstract) Am J Infect Control 1986; 14: 138. Daschner F, Kappstein I, Engels I, et al. Stress ulcer prophylaxis and ventilation pneumonia: prevention by antibacterial cytoprotective agents. Infect Control 1988; 9: 59-65. Reusser P, Zimmerli W, Scheidegger D, et 211. Role of gastric colonization in nosocomial infections and endotoxemia: a prospective study in neurosurgical patients on mechanical ventilation. J Infect Dis 1989; 160: 414-21. Prod’hom G, Koerfer J, Leuenberger PH, et al. Gastric colonization by Gram-negative bacilli in Nosocomial Pneumonia. 30th International Congress Antimicrobial Agents and Chemotherapy, Atlanta, 1990 (abst 217). Pugin J, Auckenthaler R, Mili N, et ;11. Diagnosis of ventilator-associated pneumonia by bacteriologic analysis of bronchoalveolar lavage fluid. Am Rev Respir Dis 1991; 143: 1121-9. Inglis TJJ, Sherrat MJ, Sproat LJ, Gibson JS, Hawkey PM. Gastroduodenal dysfunction and bacterial colonisation of the ventilated lung. Lancet 1993; 341: 91 1-3. Bonten M, Gaillard CA, vanTiel FH, Snieets HG, Geest SV, Stobberingh EE. The stomach is not a source for colonization of the upper respiratory tract and pneumonia in ICU patients. Chest 1994; 105: 878-84. Prod’hom G, Leuenberger P, Koerfer J, et al. Nosocomial pneumonia in mechanically ventilated patients receiving antacid, ranitidme or sucralfate as prophylaxis for stress ulcer: a randomized controlled trial. Ann Intern Med 1994; 120:
Driks MR, Craven DE, Celli BR, et al. Nosocomial pneumonia in intubated patients given sucralfate as compared with antacids or histamine type 2 blockers: the role of gastric colonization. N Engl J Med 1987; 317: 1376-82. Tryba M, Mantey-Stilers F. The antimicrobial activity of sucralfate in human gastric juice. Am J Med 1987; 83: 125-7. Daschner F, Kappstein I, Engels I, et al. Stress ulcer prophylaxis and ventilation pneumonia: prevention by antibacterial cytoprotective agents? Infect Control Hosp Epidemiol 1988; 9: 59-65. Mahul PH, Auboyer C, Jospe R, et al. Prevention of nosocomial pneunionia in intubated patients: respective role of mechanical subglottic secretions drainage and stress ulcer prophylaxis. Intensive Care Med 1992; 13: 2C-5. Tryba M. Sucralfate versus antacids or H2-antagonists for stress ulcer prophylaxis: a meta-analysis on efficacy and pneumonia rate. Crit Care Med 1991; 19: 942-9. Eddleston JM, Vohra A, Scott P, et al. A comparison of the frequency of stress ulceration and secondary pneumonia in sucralfate- or ranitidine-treated intensive care patients.
65 3-62.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
84.
85.
86.
Crit Care Med 1991; 19: 1491-6. Langer M, Mosconi P, Cigada M, et al. Long term respiratory support and risk of pneumonia in critically ill patients. Am Rev Resp Dis 1989; 140: 302-5. Craven DE, Steger KA, Duncan RA. Prevention and control of nosocomial pneumonia. In: Wenzel RP, ed. Prevention and control of nosocomial infections. Baltimore: Williams and Wilkins, 1993: 580-600. Ryan P, Dawson J, Teres D , Navab F. Continuous infu5ion of cimetidme versus sucralfate: incidence of pneumonia and bleeding compared. (Abstract) Crit Care Med 1990; 18: S253. Kappstein I, Friedrich T, Hellinger P, et al. Incidence of pneumonia in mechanically ventilated patients treated with sucralfate or cimetidine as prophylaxis for stress bleeding: bacterial colonization of the stoniach. Am J Med
Laggner AN, Lenz K, Grainger W, et al. Stress ulcer prophylaxis in a general intensive care ubit: sucralfate versus ranitidme. Anaesthesist 1988; 37: 704-710. Garcia-Labbattut A, Rodriquez-Munoz S, Boebernado- Serrano M, et al. Sucralfate versus cimetidine in the stress bleeding prophylaxis. Intensive Care Med 1990; 26 (Suppl 1): S19. Ben-Menachen T , Fogel R, Pate1 RV, et al. Prophylaxis for stress-related gastric hemorrhage in the medical intensive care unit. A randomized, controlled, single-blind study. Ann Intern Med 1994; 121: 568-575. Cook DJ, Reeve BK, Guyatt GH, et al. Stress ulcer prophylaxis in critically ill patients. Resolving discordant nieta-analysis. 1996; 275: 308-14. Baxby D , van Saene HKF, Stoutenbeck CP, Zandstra DF. Selective decontamination of the digestive tract: 13 years on, what it is and what it is not. Intensive Care Med 1996;
Selective Decontamination of the Digestive Tract Trialists’ Collaborative Group. Meta-analysis of randomized controlled trials of selective decontamination of the digestive tract. Brit Med J 1993; 307: 525-32. Bonten MJM, Gaillard CA, Johan5on WG, et al. Colonization in patients receiving and not receiving topical antimicrobial prophylaxis. Am J Respir Care Med 1994;
Ferrer M, Torres A, Gonzalez J, Puig de la Bellacasa J. Udty of selective dlgestive decontamination in mechanically ventilated patients. Ann Intern Med 1994; 120 (5): 389-95. Lode H, Gramm HJ, Goecke J, et al. Endotracheal gentamicin prophylaxis of pneumonia in ventilated patients. Chemotherapie J 1992; 4: 165-9. Torres A, Gatell JM, Aznar E, et al. Re-intubation increases the risk of nosocomial pneunionia in patients needing mechanical ventilation. Am J Respir Crit Care Med 1995; 152: 137-41. Valles J, Artigas A, Rello J. et al. Continuous aspiration of subglottic secretions in the prevention of ventilator-associated pneumonia. Ann Intern Med lV95; 122: 179-86. Rouby J-J, Laurent P, Gosnash M, et al. Risk factors and clinical relevance of maxillary sinusitis in the critically ill. Am J Respir Crit Care Med 1994; 150: 776-83.
1991; 91 (Suppl2A): 125-131.
22: 699-706.
150: 1332-40.

S76 Clinical Microbiology and Infection, Volume 3 Supplement 1, Apri l 1997
87. Holzapfel L, Chevret S, Madmier G, et al. Influence of long-term oro- or nasotracheal intubation on nosocomial maxillary sinusitis and pneumonia: results of a prospective, randomized, clinical trial. Crit Care Med 1993; 21: 1132-8.
88. Torres A, Serra-Batlles J, Ros E, et al. Pulmonary aspiration of gastric contents in patients receiving mechanical ventilation; the effect of body position. Ann Intern Med 1992, 116: 540-3.
89. Kollef MH, Shapiro SD, Fraser VJ, et al. Mechanical ventilation with or without 7-day circuit changes. A randomized control trial. Ann Intern Med 1995; 123:
90. Moore FA, Moore EE, Jones TN, McCroskey BL, Peterson VM. TEN versus TPN following major abdominal trauma: reduced septic mortality. J Trauma 1989; 29: 916-23.
91. Cometta A, Baumgartner JD. Lew D, et al. Prospective randomized comparison of imipenem monotherapy with imipenem plus netilmicin for treatment of severe infections
168-74.
in nonneutropenic patients. Antimicrob Agents Chemother
92. Verbist L, for the International Study Group. Epidemiology and sensitivity of 8625 ICU and hematology/oncology bacterial isolates in Europe. Scand J Infect Dis 1993; (suppl 91): 14-24.
93. Carbon C, and the Cefpirorne Study Group. Prospective randomized phase I1 study of intravenous cefpirome l g or 2g bd in the treatment of hospitahzed patients with dlfferent infections. J Antimicrob Chemother 1992; 29 (suppl A):
94. Wolff M, Carbon C, Falissard B, Geddes A, Verhoef J, Wilson W . Comparative study of cefpirome and ceEtazidime in ICU patients with pneumonia. 36th ICAAC 1996.
95. Mouton Y , Chidm C, Humbert G, et al. A non- comparative, multicentre study of cefepime in the treatment of serious bacterial infections. J Antimicrob Chemother 1993; 32 (suppl B): 13340.
1994; 38: 1309-13.
87-94.





























