Embed Size (px)
Citation preview

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 1Clinical Practice
Annette Quinn, MSNProgram Manager, Stereotactic Radiosurgery Uni-versity of Pittsburgh Cancer CentersUPMC [email protected]
Key Session Takeaways1. Radiation therapy delivery continues to become more
precise, resulting in less damage to normal surround-ing tissues and thus decreasing the number of frac-tions delivered.
2. Radiation planning is a very complex, tedious process that requires anywhere from one day to several weeks to be completed. It is not simply giving an x-ray treat-ment.
3. With more conformal techniques of delivering radi-ation therapy, we continue to improve quality of life with a decrease in toxicity and number of fractions needing to be delivered.
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
What’s the Buzz About Radiation?
What’s the Buzz About Radiation Therapy
Annette Quinn, RN, MSN
Program Manager, Radiation Oncology
University of Pittsburgh Cancer Center
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
I have no disclosures

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO2 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Overview
What is the physical and biological basis for radiation What are the clinical applications of radiation in the
management of cancer What is the process for treatment Simulation Treatment planning Delivery of radiation
What types of radiation are available Summary
Introduction
Radiation has been an effective tool for treating cancer for more than 100 years
More than 60 percent of patients diagnosed with cancer will receive radiation therapy as part of their treatment
Radiation oncologists are cancer specialists who manage the care of cancer patients with radiation for either cure or palliation
What is Radiation Therapy?
The use of ionizing radiation in the treatment of disease, especially cancer.

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 3Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Radiation: A Brief History
Marie Curie (1867-1934)
1895 – Röntgen discovers x-rays (Nobel Prize 1901)1896 – Becquerel discovers natural radioactive decay
Marie and Pierre Curie further characterize radioactive compounds. (All three win Nobel Prize in 1903)
1896 – First patients with cancer treated with x-rays by Emil Grubbe in Chicago
1901 – Thomas Edison is displaying X-ray machine at the World’s Fair when President McKinley is assassinated.
1952 – first “linear accelerator” used for treatment (USA in 1957)
1968 – Radiosurgery1970 – CT1975 – PET1980 – Multi-leaf collimators, Proton therapy1988 – Intensity modulated radiation treatment (IMRT)2000’s – Image-guided RT (IGRT)
Ionizing Radiation
Ionizing radiation is energy sufficiently strong to remove an orbital electron from an atom.
This radiation can have an electromagnetic form, such as a high-energy photon (xrays, gamma rays) or a particulate form such as an electron, proton or neutron.
Ionizing Radiation
Ionizing radiation is so named because its reaction with neutral atoms or molecules causes those atoms or groups of atoms to become ions, or electrically charged entities.
Ionizing radiation includes both electromagnetic waves and particle radiation. Electromagnetic waves are the broad spectrum of waves that includes radio waves, microwaves, visible light, X-rays, and gamma rays.
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO4 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Ionizing Radiation (cont.) Many types of Radiation:
Light that comes from the sun Heat that is constantly coming off our bodies.
Cancer Treatment deals mostly with X-rays and Gamma Rays X-rays and gamma rays can come from natural sources:
radon gas radioactive elements in the earth cosmic rays that hit the earth from outer space.
Can also be man-made. X-rays and gamma rays are created in power plants for nuclear
energy, and are also used in smaller amounts for medical imaging tests, cancer treatment, food irradiation, and airport security scanners.
Ionizing Radiation (cont.)
X-rays and gamma rays are both types of high energy (high frequency) electromagnetic radiation. They are packets of energy that have no charge or mass (weight). These packets of energy are known as photons.
They are forms of ionizing radiation, which means they have enough energy to remove an electron from (ionize) an atom or molecule. Ionized molecules are unstable and quickly undergo chemical changes.
Ionizing Radiation (cont.)
If ionizing radiation passes through a cell in the body, it can lead to mutations in the cell’s DNA Sometimes this causes the cell to die, but
sometimes it can lead to cancer later on. The amount of damage caused in the cell is related to the dose of radiation it receives.

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 5Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Major Differences Between Gamma Rays and X-Rays
Gamma rays are produced during nuclear decay by nuclei of atoms, whereas X-rays are produced by electrons. X-rays are produced by accelerating some
electrons and then making them collide with a metal target.
Differences (cont.)
We can control the maximum energy of the resulting x-ray spectrum, and we can control, like an on-off switch, when the x-rays are produced.
Since gamma rays come from the nuclei of an radioactive atoms, we can't turn the gamma radiation on or off. We can only shield the radiation. In addition, beyond selecting which radioactive materials we use, we can't control the energies of the gamma radiations.
What Is the Biologic Basis for Radiation Therapy?
Radiation therapy works by damaging the DNA of cells and destroys their ability to reproduce
Both normal and cancer cells can be affected by radiation, but cancer cells have generally impaired ability to repair this damage, leading to cell death
All tissues have a tolerance level, or maximum dose, beyond which irreparable damage may occur

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO6 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Directly/Indirectly Ionizing
Directly ionizing radiation: This process occurs when charged particles such as electrons (e-) with sufficient kinetic energy interact with atoms and molecules to liberate electrons and create free radicals.
Protons Electrons
Directly/Indirectly Ionizing (cont.)
Indirectly ionizing radiation: When non-charged particles pass through tissues, and
interact with atoms and molecules. Interactions result in the release of charged particles (such
as electrons) that then go on to interact with atoms and molecules.
The term "indirect" refers to the fact that the uncharged particles themselves do not create the free radicals that ultimately cause biological damage.

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 7Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Thus…
Photons are indirectly ionizing. To damage DNA they must first create a free radical to ionize and cause damage. Electrons are directly ionizing can also interact
with tissue through “Bremsstrahlung” (braking radiation) and create photons that will then further interact with tissue.
Radiation Units
Absorbed Dose Conventional Units = Rads Standard International Units = Gray 1 Gray (Gy) = 100 Rads 1 cGy = 1 Rad
Incident x-ray photon
Fast Electron
Free Radical
Cellular DNA Damage
Biologic Effects of Radiation

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO8 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Radiation Biology
Single-strand breaks: Easily repaired
Normal cells complete repair in 6 hours
This time interval is relevant to fractionation
If another fraction is given and another single-strand break occurs in the right place before repair of the first is complete, a double-strand break can occur
Fractionation: A Basic RadiobiologicPrinciple
Fractionation, or dividing the total dose into small daily fractions over several weeks, takes advantage of differential repair abilities of normal and malignant tissues
Fractionation spares normal tissue through repairand repopulation while increasing damage to tumor cells through redistribution and reoxygenation
Single-Strand DNA Break
Repaired in ~6 hours

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 9Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
2 Single-Strand DNA Breaks Close in Time Lead to a Double-Strand
Break
~2 hours
The Four R’s of Radiobiology
Four major factors are believed to affect tissue’s response to fractionated radiation:
1. Repair of sublethal damage to cells between fractions caused by radiation
2. Repopulation or regrowth of cells between fractions3. Redistribution of cells into radiosensitive phases of cell
cycle4. Reoxygenation of hypoxic cells to make them more
sensitive to radiation
Repair Repair is the one of the primary reasons to fractionate
radiotherapy. By splitting radiation dose into small parts, cells are allowed
to repair sublethal damage. Amount of damage that is repaired depends on the ability
of the cell to recognize the damage and activatea) repair pathways b) cell cycle arrest
Malignant cells have often suppressed these pathways, often through mutation or inhibition of TP53, preventing them from undergoing efficient repair. Normal tissue cells with intact repair pathways are able to repair the sublethaldamage by the time the next fraction is delivered.

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO10 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Repair
Repair half life is an important consideration when fractionating radiotherapy. Some tissues, notably the spinal cord, appear
to have a slow repair mechanism with a half life of about 4 hours. It is important to separate dose by at least 6
hours and preferably 8 hours if two fractions are given on the same day.
Repopulation Repopulation is the increase in cell division that is seen
in normal and malignant cells at some point after radiation is delivered
Some tumors exhibit accelerated repopulation, a marked increase in their growth fraction and doubling time, at 4 - 5 weeks.
Seen most notably in squamous cell carcinoma of the head and neck as well as the cervix. Accelerated repopulation is a dangerous phenomenon that must be countered if treatment time extends over five weeks. Methods to do this include accelerated treatment with hyperfractionation to minimize late effects.
Redistribution When radiotherapy is given to a population of cells, they
may be in different parts of the cell cycle. Cells in S-phase are typically radioresistant, whereas those
in late G2 and M phase are relatively sensitive. A small dose of radiation delivered over a short time period
(external beam or high dose brachytherapy) will kill a lot of the sensitive cells and less of the resistant cells.
Over time, the surviving cells will continue to cycle. If a second dose of radiation is delivered some time later, some of these cells will have left the resistant phase and be in a more sensitive phase, allowing them to be killed more easily.

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 11Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Cell-Cycle Effect
Radiosensitivity varies with positions in the cell cycle
Mitotic cells are most susceptible (G2 & M phase)
Cells in S phase are least susceptible
Reoxygenation
Chronic hypoxia is due to the poor vasculature of tumors and the distance oxygen must travel to reach cells that are far from the capillaries.
These chronically hypoxic cells are also resistant to radiation.
Fractionated radiotherapy kills cells that lie close to the capillary more effectively.
As these cells are removed, the chronically hypoxic cells are able to move closer to their nutrient source, and therefore become relatively oxic.
Oxic cells can be killed.
Fractionation Regaud and The French Ram
A single dose of radiation that is sufficient to sterilize a ram also causes significant skin toxicity
If the same dose is delivered in several fractions, the ram is sterilized, but there is no skin toxicity
1920’s – 1930’s Regaud – extended treatment
time for uterine cancer improved outcomes
Coutard – fractionated treatment for head and neck cancer reduced toxicity with better outcomes

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO12 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Treatment planning
Dosimetry Originally done using hand calculations, graph
paper Computer planning revolutionized our ability to
deliver radiation accurately and precisely Modern treatment planning systems use CT data
to accurately calculate dose to entire target volume (3D-CRT) and computers to determine optimum dose delivery from multiple beams (IMRT)
Volumes defined prior to treatment planning :
Gross Tumor Volume (GTV) Clinical Target Volume (CTV)
Volumes defined during the treatment planning :
Planning Target Volume (PTV) Organs at Risk Treated Volume Irradiated Volume
ICRU 50
GROSS TUMOR VOLUME ( GTV )
Gross palpable or visible/demonstrable extent and location of the malignant growth.
It consists of:1. Primary tumor2. Metastatic lymphadenopathy3. Other metastasis
Corresponds to those parts of the malignant growth where the tumor density is largest.
If the tumor has been removed prior to radiotherapy then no GTV can be defined.
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 13Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
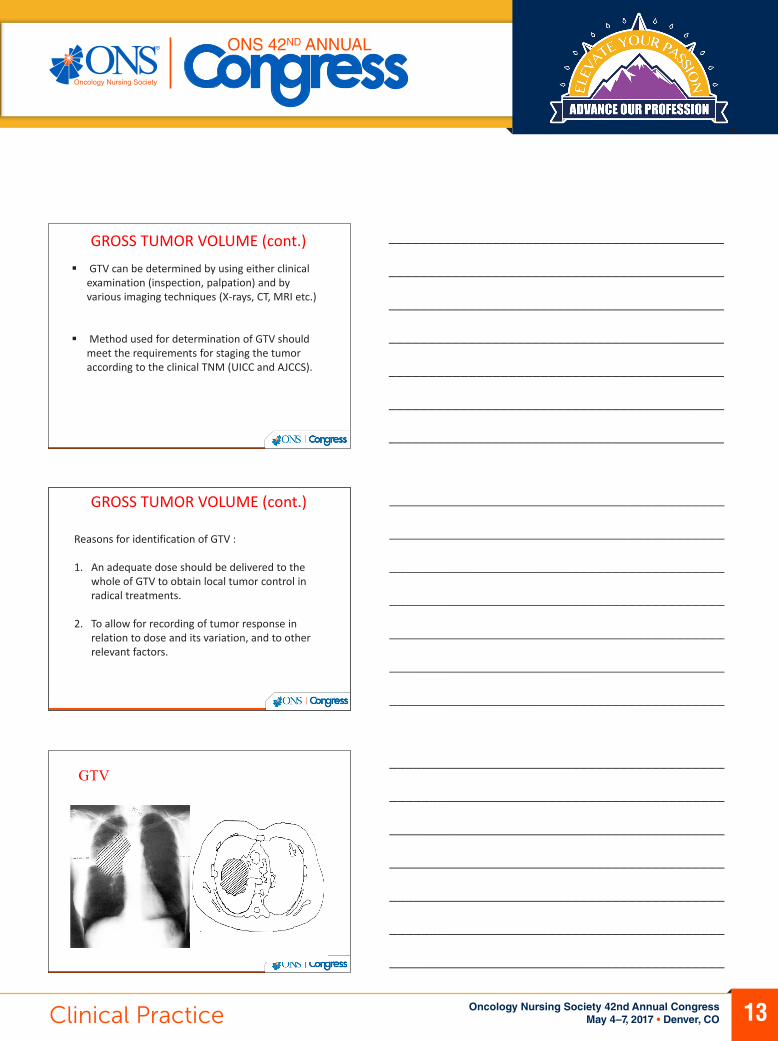
GTV can be determined by using either clinical examination (inspection, palpation) and by various imaging techniques (X-rays, CT, MRI etc.)
Method used for determination of GTV should meet the requirements for staging the tumor according to the clinical TNM (UICC and AJCCS).
GROSS TUMOR VOLUME (cont.)
Reasons for identification of GTV :
1. An adequate dose should be delivered to the whole of GTV to obtain local tumor control in radical treatments.
2. To allow for recording of tumor response in relation to dose and its variation, and to other relevant factors.
GROSS TUMOR VOLUME (cont.)
GTV

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO14 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
CLINICAL TARGET VOLUME ( CTV )
It is a tissue volume that contains a GTV and/or subclinical microscopic disease, which has to be eliminated.
This volume has to be treated adequately in order to achieve the aim of therapy : cure or palliation.
The delineation of this volume requires consideration of factors like local invasive capacity of the tumor and its potential to spread to different regions (eg: regional lymph nodes).
CTV
The delineation of GTV and CTV are based on purely anatomic-topographic and biological considerations without regard to technical factors of treatment.
GTV versus CTV
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 15Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
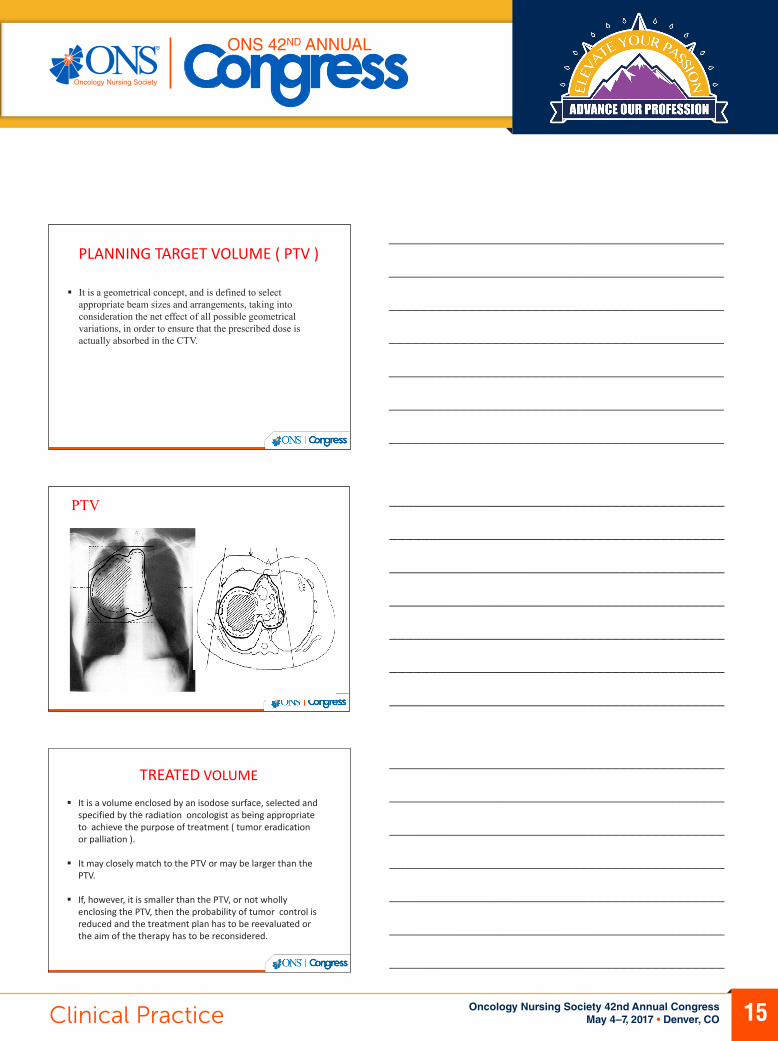
PLANNING TARGET VOLUME ( PTV )
It is a geometrical concept, and is defined to select appropriate beam sizes and arrangements, taking into consideration the net effect of all possible geometrical variations, in order to ensure that the prescribed dose is actually absorbed in the CTV.
PTV
TREATED VOLUME
It is a volume enclosed by an isodose surface, selected and specified by the radiation oncologist as being appropriate to achieve the purpose of treatment ( tumor eradication or palliation ).
It may closely match to the PTV or may be larger than the PTV.
If, however, it is smaller than the PTV, or not wholly enclosing the PTV, then the probability of tumor control is reduced and the treatment plan has to be reevaluated or the aim of the therapy has to be reconsidered.

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO16 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
IRRADIATED VOLUME ( IrV )
It is that tissue volume which receives a dose that is considered significant in relation to normal tissue tolerance.
It depends on the treatment technique used.
ORGANS AT RISK ( OR )
These are normal tissues whose radiation sensitivity may significantly influence the treatment planning and/or prescribed dose.
They may be divided into 3 classes : Class I : Radiation lesions are fatal or result in severe
morbidity. Class II : Radiation lesions result in mild to moderate
morbidity. Class III : Radiation lesions are mild, transient, and
reversible, or result in no significant morbidity.
ICRU 50
Irradiated Volume
Treated Volume
Planning Target Volume (PTV)
Clinical Target Volume (CTV)Gross Tumor Volume(GTV)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 17Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Treatment PlanningPlan Evaluation: Early stage breast cancer (supine)
Treatment Planning Plan Evaluation: Intermediate-risk prostate cancer
Treatment PlanningPlan Evaluation: Intermediate-risk prostate cancer

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO18 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Treatment Planning
How can we modulate dose? Adjust number,
intensity, angle of beams
Treatment Planning Examples
How Can We Modulate Dose?
Use computer planning to modulate dose from multiple beams (IMRT)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 19Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Types of External Beam Radiation Therapy
Two-dimensional radiation therapy Three-dimensional conformal radiation therapy (3-D CRT) Intensity modulated radiation therapy (IMRT) Image Guided Radiation Therapy (IGRT) Intraoperative Radiation Therapy (IORT) Stereotactic Radiotherapy (SRS/SBRT) Particle Beam Therapy
2D Treatment Planning
Anatomical landmark Simple radiation principles
Intensity falls off by distance squared
Simple beam arrangement With or without custom blocks
Still very useful for some routine rudimentary cases Simple bone mets where there
is little critical tissue in field
CT simulator most common PET/CT simulator CT/MR and CT/PET fusion
programs available Multiple treatment fields converge Most frequently utilizes a trial &
error process called forward planning
Coplanar or non-coplanar Minimizes radiation to normal
tissue. Allows calculation of a “Dose-
Volume Histogram” (DVH)
3D Conformal Treatment Planning

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO20 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
3-D CRT Uses CT, PET or MRI scans
to create a 3-D picture of the tumor and surrounding anatomy Improved precision,
decreased normal tissue damage
Breast cancers, lung cancers
3D Conformal Radiation Therapy
What is IMRT???
IMRT = Intensity Modulated Radiation Treatment
Inverse planning MD denotes what tissues will receive what dose The planning computer decides how to deliver it “Blocks” are not used The beam is modified as it leaves the accelerator
The target receives the minimum dose. The nature of the beam modification results in
inhomogeneity of dose within the target Multiple treatment beams with dynamic multileaf Arcs (Rapid Arc) Static fields (IMRT)

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 21Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
IMRT A highly sophisticated form of 3-D
CRT allowing radiation to be shaped more exactly to fit the tumor Radiation is broken into many
“beamlets,” the intensity of each can be adjusted individually
IMRT allows higher doses of radiation to be delivered to the tumor while sparing more healthy surrounding tissue
Head and neck cancers, esophageal and prostate cancers
3D CRT vs. IMRT
Definition of Targets & Normal Tissues

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO22 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Delivery of Radiation Therapy
External beam radiation therapy typically delivers radiation using a linear accelerator
Internal radiation therapy, called brachytherapy, involves placing radioactive sources into or near the tumor
The modern unit of radiation is the Gray (Gy), traditionally called the rad 1Gy = 100 centigray (cGy) 1cGy = 1 rad
Image Guidance
For patients treated with 3-D CRT or IMRT
Physicians use frequent imaging of the tumor, bony anatomy or implanted fiducial markers for daily set-up accuracy Imaging performed using CT
scans, high quality X-rays, MRI or ultrasound
Motion of tumors can be tracked to maximize tumor coverage and minimize dose to normal tissues
Fiducial markers in prostate visualized and aligned.
4-Dimensional Radiation Therapy
Treatment for the New Millennium—the addition of the TIME dimension

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 23Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Stereotactic RadiationRadiosurgery (1 treatment fraction) Gamma Knife or Linac (TruBeam) Minimally invasive procedure (head frame) Sub-millimeter accuracy
Radiotherapy (Up to 5 treatment fractions) Linac Arc therapy Framed (re-locatable) or frameless
Cyber Knife Compact linear accelerator mounted on a robotic arm Frameless
The Gamma Knife
Metastasis

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO24 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
The CyberKnifeOrthogonal diagnostic x-ray
imaging system
6 MV Linear Accelerator
– compact
– 280 pounds
Robot manipulator
– 0.5 mm accuracy
Clinical Uses for Radiation TherapyTwo major functions:1. To cure cancer Destroy tumors that have not spread Kill residual microscopic disease left
after surgery or chemotherapy
2. To reduce or palliate symptoms Shrink tumors affecting quality of
life, e.g., a lung tumor causing shortness of breath
Alleviate pain or neurologic symptoms by reducing the size of a tumor
External beam radiation treatments are usually scheduled five days a week and continue for one to ten weeks
Stereotactic Body Radiotherapy (SBRT)SBRT refers to stereotactic radiation treatments in 1-5 fractions on specialized linear accelerators Uses sophisticated imaging,
treatment planning and immobilization techniques Respiratory gating may be
necessary for motions management, e.g., lung tumors
SBRT is used for a number of sites: spine, lung, liver, brain, adrenals, pancreas
Data maturing for sites such as prostate

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 25Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Proton Beam Therapy Protons are charged particles that
deposit most of their energy at a given depth, minimizing risk to tissues beyond that point
Allows for highly specific targeting of tumors located near critical structures
Increasingly available in the U.S. Most commonly used in treatment
of pediatric, CNS and intraocular malignancies Data maturing for use in other tumor
sites
Types of Internal Radiation Therapy
Intracavitary implants Radioactive sources are placed in a cavity near
the tumor (breast, cervix, uterine) Interstitial implants Sources placed directly into the tissue (prostate,
vagina) Intra-operative implants Surface applicator is in direct contact with the
surgical tumor bed
Brachytherapy Dose Rate
Low-Dose-Rate (LDR) Radiation delivered over days and
months Prostate, breast, head and neck,
and gynecologic cancers may be treated with LDR brachytherapy
High-Dose-Rate (HDR) High energy source delivers the dose
in a matter of minutes rather than days
Gynecologic, breast, head and neck, lung, skin and some prostate implants may use HDR brachytherapy
LDR prostate implant

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO26 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Brachytherapy
Radioactive sources are implanted into the tumor or surrounding tissue 125I, 103Pd, 192Ir, 137Cs
Purpose is to deliver high doses of radiation to the desired target while minimizing the dose to surrounding normal tissues
Radioactive seeds for a permanent prostate implant, an example of low-dose-rate brachytherapy.
Permanent vs. Temporary Implants
Permanent Implants Release small amounts of
radiation over a period of several months
Examples include low-dose-rate prostate implants (“seeds”)
Patients receiving permanent implants may be minimally radioactive and should avoid close contact with children or pregnant women
Temporary Implants Temporary implants are left
in the body for several hours to several days
Examples include low-dose-rate GYN implants and high-dose-rate prostate or breast implants
Patient may require hospitalization during the implant depending on the treatment site
Intraoperative Radiation Therapy (IORT)
IORT delivers a concentrated dose of radiation therapy to a tumor bed during surgery Advantages
Decrease volume of tissue in boost field
Ability to exclude part or all of dose-limiting normal structures
Increase the effective dose
Multiple sites Pancreas, stomach, lung, esophagus,
colorectal, sarcomas, pediatric tumors, bladder, kidney, gyn
Several recent trials have shown efficacy for breast cancer

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 27Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Radiation Therapy in Multidisciplinary Care
Radiation therapy plays a major role in the management of many common cancers either alone or as an adjuvant therapy with surgery and chemotherapy Sites commonly treated include
breast, prostate, lung, colorectal, pancreas, esophagus, head and neck, brain, skin, gynecologic, lymphomas, bladder cancers and sarcomas
Radiation is also frequently used to treat brain and bone metastases as well as cord compression
Radiation Therapy Basics The delivery of external beam
radiation treatments is painless and usually scheduled five days a week for one to ten weeks
The effects of radiation therapy are cumulative with most significant side effects occurring near the end of the treatment course. Side effects usually resolve over the
course of a few weeks There is a slight risk that radiation
may cause a secondary cancer many years after treatment, but the risk is outweighed by the potential for curative treatment with radiation therapy
{Sabin Motwani will send us image of mild skin redness after RT in a treatment field}.
Example of erythroderma after several weeks of radiotherapy with moist desquamation
Common Radiation Side Effects Vary depending on site of the treatment and affect the tissues in
radiation field: Breast – swelling, skin redness Abdomen – nausea, vomiting, diarrhea Chest – cough, shortness of breath, esophageal irritation Head and neck – taste alterations, dry mouth, mucositis, skin redness Brain – hair loss, scalp redness Pelvis – diarrhea, cramping, urinary frequency, vaginal irritation Prostate – impotence, urinary symptoms, diarrhea Fatigue is often seen when large areas are irradiated
Modern radiation therapy techniques have decreased these side effects significantly
Unlike the systemic side effects from chemotherapy, radiation therapy usually only impacts the area that received radiation
Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO28 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Palliative Radiation Therapy Commonly used to relieve pain from bone
cancers ~ 50 percent of patients receive total relief
from their pain 80 to 90 percent of patients will derive some
relief Other palliative uses:
Spinal cord compression Vascular compression, e.g., superior vena
cava syndrome Bronchial obstruction Bleeding from gastrointestinal or gynecologic
tumors Esophageal obstruction
The Radiation Oncology Team
Radiation Oncologist The doctor who prescribes and oversees the radiation therapy treatments
Medical Physicist Ensures that treatment plans are properly tailored for each patient, and is
responsible for the calibration and accuracy of treatment equipment
Dosimetrist Works with the radiation oncologist and medical physicist to calculate the
proper dose of radiation given to the tumor
Radiation Therapist Administers the daily radiation under the doctor’s prescription and supervision
Radiation Oncology Nurse Interacts with the patient and family at the time of consultation, throughout the
treatment process and during follow-up care
The Treatment Process
1. Referral2. Consultation3. Simulation4. Treatment Planning5. Quality Assurance

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 29Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Referral
Tissue diagnosis has been established
Referring physician reviews potential treatment options with patient
Treatment options may include radiation therapy, surgery, chemotherapy or a combination
It is important for a referring physician to discuss all possible treatment options available to the patient
Consultation
Radiation oncologist determines whether radiation therapy is appropriate
A treatment plan is developed
Care is coordinated with other members of patient’s oncology team
The radiation oncologist will discuss with the patient which type of radiation therapy treatment is best for their type of cancer
Simulation
Patient is set up in treatment position on a dedicated CT scanner Immobilization devices may be
created to assure patient comfort and daily reproducibility
Reference marks or “tattoos” may be placed on patient
CT simulation images are often fused with PET or MRI scans for treatment planning

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO30 Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Treatment Planning
Physician outlines the target and organs at risk Sophisticated software is used
to carefully derive an appropriate treatment plan Computerized algorithms enable the
treatment plan to spare as much healthy tissue as possible
Medical physicist checks the chart and dose calculations
Radiation oncologist reviews and approves final plan
Radiation oncologists work with medical physicists and dosimetrists to create the optimal treatment plan for each individualized patient
Safety and Quality Assurance
Each radiation therapy treatment plan goes through many safety checks The medical physicist checks the calibration of the linear
accelerator on a regular basis to assure the correct dose is being delivered
The radiation oncologist, along with the dosimetrist and medical physicist go through a rigorous multi-step QA process to be sure the plan can be safely delivered
QA checks are done by the radiation therapist daily to ensure that each patient is receiving the treatment that was prescribed for them
Systemic Radiation Therapy
Radiation can also be delivered by an injection: Metastron (89Strontium), Quadramet (153Samarium)
and Xofigo (223Radium) are radioactive isotopes absorbed primarily by cancer cells Used for treating bone metastases
Radioactive isotopes may be attached to an antibody targeted at tumor cells Zevalin, Bexxar for Lymphomas
Radioactive “beads” may be used to treat primary or metastatic liver cancer Y90-Microspheres

Oncology Nursing Society 42nd Annual CongressMay 4–7, 2017 • Denver, CO 31Clinical Practice
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
__________________________________________
Public Awareness of Radiation Therapy
Patients report going to friends and family and their referring physician to get cancer treatment information
Take Away Points
Radiation therapy delivery continues to become more precise resulting in less damage to normal surrounding tissues and thus decreasing number of fractions delivered. Radiation planning is a very complex, tedious
process that requires anywhere from one day to several weeks. With more conformal techniques, side effects
from radiation therapy are diminishing.
For More Information…
The American Society for Radiation Oncology (ASTRO) can provide information on radiation therapy
Visit www.rtanswers.org to view information on how radiation therapy works to treat various cancers





























