Embed Size (px)
Citation preview

lable at ScienceDirect
Journal of Psychiatric Research 45 (2011) 1366e1372
Contents lists avai
Journal of Psychiatric Research
journal homepage: www.elsevier .com/locate/psychires
White matter alterations in social anxiety disorder
Volker Baur a,b,*, Jürgen Hänggi b, Michael Rufer c, Aba Delsignore c, Lutz Jäncke b, Uwe Herwig a,Annette Beatrix Brühl a
aClinic for General and Social Psychiatry, Psychiatric University Hospital, Lenggstrasse 31, CH-8032 Zurich, SwitzerlandbDivision Neuropsychology, Institute of Psychology, University of Zurich, Binzmühlestrasse 14/25, CH-8050 Zurich, SwitzerlandcDepartment of Psychiatry and Psychotherapy, University Hospital Zurich, Culmannstrasse 8, CH-8091 Zurich, Switzerland
a r t i c l e i n f o
Article history:Received 6 January 2011Received in revised form9 May 2011Accepted 12 May 2011
Keywords:Social anxiety disorderDiffusion tensor imagingWhite matter connectivityFractional anisotropyUncinate fasciculusTrait anxiety
* Corresponding author. Division NeuropsycholoUniversity of Zurich, Binzmühlestrasse 14/25, CHTel.: þ41 44 635 7406; fax: þ41 44 635 7409.
E-mail address: [email protected] (V. Baur).
0022-3956/$ e see front matter � 2011 Elsevier Ltd.doi:10.1016/j.jpsychires.2011.05.007
a b s t r a c t
White matter architecture in patients with social anxiety disorder (SAD) has rarely been investigated, butmay yield insights with respect to altered structural brain connectivity. Initial evidence points to alter-ations in the uncinate fasciculus (UF). We applied diffusion tensor imaging in 25 patients with SAD and25 matched healthy subjects. Whole-brain fractional anisotropy (FA) maps were used for groupcomparison and voxel-wise correlation with psychometric and clinical measures. Additionally, a region-of-interest analysis of the UF was performed. Patients with SAD had reduced FA compared to healthysubjects in or near the left UF and the left superior longitudinal fasciculus. There were no regions withincreased FA in SAD. In the region-of-interest analysis, a negative correlation between FA and traitanxiety was identified in the left and right UF in patients, but not in healthy subjects. No correlationswith social anxiety scores were observed. The present study partially confirms previous results pointingto frontal WM alterations in or near the UF in patients with SAD. SAD-specific dimensional associationsof FA with trait anxiety might reflect general pathological and/or compensatory mechanisms as a func-tion of symptom severity in patients. Future studies should disentangle in which way the identified WMalterations match functional alterations.
� 2011 Elsevier Ltd. All rights reserved.
1. Introduction
Social anxiety disorder (SAD) is a common anxiety disorder(Jefferys, 1997) with a life-time prevalence of about 10% (Kessleret al., 1994). It is characterized by exaggerated fear during theanticipation of or confrontation with evaluation by others. Sincegenetic factors are known to play a role in SAD (Mosing et al., 2009;Stein and Stein, 2008) and based on the commonly early age ofonset (Stein and Stein, 2008), manifestations in the brain’s struc-tural architecture can be expected.
Examination of white matter (WM) may yield insights intostructural connectivity and complement functional neuroimagingstudies. Until now, little is known about WM architecture in SAD.First evidence points to alterations in the uncinate fasciculus (UF)(Phan et al., 2009), a fiber bundle connecting inferior frontalcortices including orbitofrontal cortex with the anterior temporallobe and the amygdala (Ebeling and von Cramon, 1992; Ghashghaei
gy, Institute of Psychology,-8050 Zurich, Switzerland.
All rights reserved.
et al., 2007; Petrides and Pandya, 2007). Since the amygdalamediates emotional arousal states (Davis and Whalen, 2001) andthe orbitofrontal cortex is implicated in cognitive control ofemotions (Ochsner and Gross, 2005), the UF may play a key role inthe emergence or regulation of fear. Therefore, the UF representsa WM structure of interest for diffusion tensor imaging (DTI)studies related to fear and anxiety. Theories of SAD point to biasesat different stages of cognitive-attentional processing (Hirsch andClark, 2004), probably not mediated by the UF alone. Therefore, itcan be expected that WM alterations are present in further brainareas mediating interpretative or associative processes.
DTI is a magnetic resonance based technique allowing theexamination of WM structural properties, such as microstructuralanisotropic diffusion reflected by fractional anisotropy (FA) (Basserand Pierpaoli, 1996). In the present study, we assessed FAthroughout the whole-brain in patients with SAD and in healthycontrol subjects. Additionally, we concentrated on FAwithin the UFin a region-of-interest approach. Given the results of relatedprevious studies (Kim and Whalen, 2009; Phan et al., 2009), whichfor the first time investigated associations between FA and anxiety,we expected that reduced rather than increased FA would bea characteristic of abnormal WM architecture in anxious individ-uals. First, we aimed at identifying altered WM structures in

V. Baur et al. / Journal of Psychiatric Research 45 (2011) 1366e1372 1367
patients with SAD compared to healthy subjects. Specifically, wehypothesized reduced FA in the UF. Further, we sought to deter-mine the dimensional impact of trait anxiety, social anxiety andSAD duration on FA.
2. Materials and methods
2.1. Subjects
Twenty-seven outpatients with current diagnosis of generalizedSAD participated in this study. They were recruited from theoutpatient clinic at the Department of Psychiatry and Psycho-therapy of the University Hospital Zurich. Control subjects wererecruited via direct address and email-advertisement. Due tosevere artifacts in DTI images related to technical problems duringdata acquisition, two patients with SAD had to be excluded fromfurther analyses. The remaining 25 patients with SAD werematched with 25 healthy subjects in terms of age and gender (seeTable 1). All subjects were right-handed according to a handednessquestionnaire (Annett, 1970). Diagnosis of generalized SAD andcomorbid Axis-I diagnoses were established using the Mini-International Neuropsychiatric Interview for DSM-IV (Sheehanet al., 1998) (German version by Ackenheil et al., 1999). Onepatient met life-time criteria for a depressive episode, but was notcurrently depressed; three patients met criteria for a currentdepressive episode in the course of a major depressive disorder,however, SAD was the primary diagnosis. One patient met criteriafor prior alcohol dependency, currently remitted. There were nofurther psychiatric comorbidities. Altogether, nine patients weretaking antidepressant medication due to depressive symptoms(selective serotonin reuptake inhibitors in five subjects, selectiveserotonin/norepinephrine reuptake inhibitors in two subjects,mirtazapine in one subject, and clomipramine/zolpidem in onesubject). Two of the mentioned subjects were additionally takinglithium, one quetiapin. In all subjects, the dose of drugs had beenstable for more than one month when participating in the study.Healthy control subjects were free of current or past psychiatricdisorders (semi-structured diagnostic interview) and of medication(except oral contraceptives). Exclusion criteria in all subjects wereneurological disorders, head trauma, pregnancy, excessiveconsummation of alcohol, cigarettes and caffeine, and contraindi-cations against magnetic resonance imaging. All subjects providedwritten informed consent and were compensated for their partic-ipation. The study was approved by the local ethics committee.
General anxiety was measured with the trait version of theSpielberger State-Trait Anxiety Inventory (STAI, Spielberger et al.,1970; German version by Laux et al., 1981) in all participants. Thedegree of social anxiety was assessed in patients with the self-rating version of the Liebowitz Social Anxiety Scale (LSAS,
Table 1Demographic, psychometric and clinical characteristics of the sample.
SAD a Healthy subje
Age 32 � 10.4 years (range: 19e53) 32 � 10.1 yeaGender 18 m, 7 f 18 m, 7 fSTAI-X2b e50 � 11.2 (range: 31e76) f33 � 7.4 (ranLSASc 66 � 23.0 (range: 26e107) e
BDId 15 � 10.8 (range: 0e41) e
Age of onset of SAD 15 � 5.9 years (range: 6e30) e
Duration of SAD 16 � 10.6 years (range: 3e44) e
a SAD: patients with social anxiety disorder.b STAI-X2: Spielberger State-Trait Anxiety Inventory, trait section.c LSAS: Liebowitz Social Anxiety Scale.d BDI: Beck’s Depression Inventory.e corresponds to increased values (Laux et al., 1981).f corresponds to values within the normal range (Laux et al., 1981).
Liebowitz, 1987; German version by Stangier and Heidenreich,2005). The LSAS self-rating version has been shown to have highreliability (retest-reliability r ¼ 0.82, Cronbach’s a ¼ 0.95) andvalidity (correlation with the clinician-administered versionr � 0.78) (Baker et al., 2002). Degree of depression in patients withSAD was assessed with Beck’s Depression Inventory (BDI, Becket al., 1961; German version by Hautzinger et al., 1994). Furtherpatient-specific characteristics were collected in addition to thediagnostic interview: The duration of symptoms of SAD wasassessed by retrospectively asking for the onset of symptoms(available in 20 patients). A positive family history of psychiatricdisorders was present in 88.9% of the patients (mostly SAD anddepression, assessed in 18 patients).
2.2. DTI data acquisition
DTI scans were acquired on a 3.0 T whole-body scanner (GEMedical Systems, Milwaukee, USA) equipped with a standard8-channel head coil. One diffusion-weighted spin-echo echo-planar imaging (EPI) scan was obtained from all participants.Slices were acquired sequentially in transversal orientation (matrix256 � 256 pixels, 39 slices, slice thickness 3.2 mm, field of view(FOV) ¼ 240 � 240 mm). Further imaging parameters were: echotime (TE) ¼ 87.8 ms, repetition time (TR) ¼ 12000 ms. Diffusionsensitization was achieved with 2 balanced diffusion gradientscentered on the 180� radio-frequency pulse. Diffusion wasmeasured in 21 non-collinear directions with a b-value ofb ¼ 1000 s/mm2. Five additional interleaved non-diffusion-weighted volumes (b ¼ 0 s/mm2) served as reference volumes.Scan timewas about 6 min. In addition to DTI, T1- and T2-weightedimages were consecutively acquired to exclude possible T1-/T2-sensitive tissue abnormalities.
2.3. Data preprocessing
We applied preprocessing procedures for DTI data as imple-mented in FMRIB Software Library (FSL, http://www.fmrib.ox.ac.uk/fsl) (Smith et al., 2004). Using FMRIB Diffusion Toolbox (FDT)(Behrens et al., 2003), FA maps as well as maps of primary (l1),secondary (l2) and tertiary (l3) eigenvalues were created. l1-mapswere used for analysis of axial diffusivity. Radial diffusivity mapswere calculated as l23 ¼ (l2 þ l3)/2. Preprocessing comprised thefollowing steps: 1) Eddy current and head movement correctionwere applied using FDT. 2) Individual binary brain masks werecreated on the non-diffusion weighted images using Brain Extrac-tion Tool (Smith, 2002). 3) Tensors were fitted to the data using FDT.4) Linear and non-linear normalization of the FA maps into a stan-dard stereo-tactic space (Montreal Neurological Institute, MNI;represented by the FMRIB58 FA template) were done with scripts
cts Test T df p
rs (range: 20e57) t 0.24 48 0.821.00
ge: 22e55) t 6.38 41.6 < 0.001

V. Baur et al. / Journal of Psychiatric Research 45 (2011) 1366e13721368
(FLIRT for linear and FNIRT for non-linear normalization) imple-mented in FSL. 5) These transformations were then also applied tothe l1- and l23-maps. 6) Images were resampled to a spatial reso-lution of 1 �1 �1 mm3. 7) We visually inspected the quality of theresulting, normalized FA-, l1- and l23-maps.
2.4. Whole-brain analyses
Statistical analysis was done using statistical parametric mapping(SPM 5) software (http://www.fil.ion.ucl.ac.uk/spm). FA maps weresmoothed with a Gaussian kernel of 6 mm FWHM (full width at halfmaximum) (e.g., seeKimandWhalen,2009;Parketal., 2004;Haetal.,2009) and thereafter thresholded considering only voxels with FAvalues greater than 10% of global mean FA for statistical analysis.Applying general linearmodels to the FAmaps, the significance of thedifferencesbetween the twogroupsaswell asof the correlationswithpsychometric and clinical measures was calculated by means ofvoxel-wise analysis of covariance. To examine effects of smoothing,we additionally applied smoothing with a Gaussian kernel of 3 mmFWHM and computed the voxel-based FA group comparison.
Differences between the two groups with respect to local FAwere assessed using a correction for multiple comparisons of thestatistical extent threshold combined with a non-stationaritysmoothness correction (Hayasaka and Nichols, 2004; Hayasakaet al., 2004; Worsley et al., 1999). We used a voxel-wise thresholdof p < 0.00001 uncorrected and a cluster-extent family-wise error(FWE) correction with p < 0.05 corrected for multiple comparisons(resulting in a cluster threshold of k � 48 voxels) for FA maps. SinceFA is influenced by the ratio of axial to radial diffusivity, weexamined post-hoc whether changes in FA in the respective clusterreflected changes in either axial or radial diffusivity or both. Foreach significant cluster in the group comparison of FA, we extractedpost-hoc individual mean values of FA, axial and radial diffusivityfrom unsmoothed maps using MarsBaR toolbox of SPM 5 (Brettet al., 2002). These values were used to show group-specificmagnitude values and to determine effect sizes (Cohen’s d) ofgroup differences. To assess medication-related effects on FA inpatients with SAD, we divided the SAD group into two subgroups,medicated (n ¼ 9) and medication-free (n ¼ 16) patients. Age andtrait anxiety were regressed out in these analyses to account fordifferences in these variables between the two SAD subgroups(p¼ 0.11 and p< 0.05, respectively). On the one hand, we examinedpost-hoc mean FA of the significant clusters obtained from thepooled FA group comparison (SAD vs. healthy subjects) usingmultivariate and univariate analysis of covariance with status ofmedication as between-subjects factor. On the other hand, weexamined FA exploratory across the whole-brain (medicated vs.medication-free patients) using the same statistical approach as forthe pooled FA group comparison stated above.
In addition to the FA group comparison (SAD vs. healthysubjects), we correlated STAI and LSAS scores as well as SADduration with local FA (Pearson correlation) in the whole-brain.Here, we used a voxel-wise height threshold of p< 0.001 combinedwith a cluster-extent FWE correction for multiple comparisons(p < 0.05, corresponding to k � 552 for STAI, k � 571 for LSAS, andk � 583 for SAD duration). As in the FA group comparison, clusters
Table 2Groupcomparisonof fractional anisotropy (patientswith social anxiety disorder<healthy
Cluster Size (mm3) MNI peak coordinates
x y z
UF/IFOF (left) 208 �24 38 �8SLF (left) 185 �32 �31 17
UF: uncinate fasciculus, IFOF: inferior fronto-occipital fasciculus, SLF: superior longitudin
from the correlation analyses were corrected for non-stationaritysmoothness. We extracted mean FA, mean axial and mean radialdiffusivity for each significant cluster from unsmoothedmaps usingMarsBaR toolbox of SPM 5 (Brett et al., 2002), which were thencorrelated post-hoc with the respective measure to obtain cluster-based correlation strength. Although trait anxiety was higher inpatients with SAD compared to healthy subjects (mean � standarddeviation: 50 � 11.2 vs. 33 � 7.4, p < 0.001), which was to beexpected, we assessed the voxel-wise correlation with STAI scoresacross all 50 subjects (25 patients and 25 healthy subjects). Becauseconcerns may be raised on performing a correlation with STAIacross both groups whereas a group difference with strong effectexists in this measure, we performed two post-hoc examinations.First, we correlated cluster-wise mean FA with trait anxiety sepa-rately for both groups to determine correlation strengthwithin eachof the two groups. Second, we computed step-wise linear regres-sion for each identified cluster using “group” and “STAI” as inde-pendent variables and mean FA as dependent variable toinvestigate the way these factors distinctively explain variance ofFA. In addition, we performed voxel-wise correlation with traitanxiety separately for both groups with the same statisticalthreshold as stated above. Correlations with LSAS and duration ofSAD symptoms were restricted to the patient group.
With respect to demographic, psychometric, and globalanatomical measures, we used independent two-tailed t-tests witha threshold of p < 0.05 uncorrected. WM regions obtained fromgroup statistical analyses in SPM were overlaid on the group meanFA map in MNI space and their anatomical identification was basedon the ‘JHUWhite Matter Tractography Atlas’ (Hua et al., 2008) andthe ‘Juelich Histological Atlas’ (Eickhoff et al., 2005) implemented inFSL. To assure validity of our data, we inspected magnitude valuesof FA of each identified cluster separately for both groups withregard to plausibility for WM tissue (see also Table 2).
2.5. Region-of-interest analysis
Due to previous findings in the UF (Kim andWhalen, 2009; Phanet al., 2009), we selected the left and right UF as regions of interest(ROI) based on probability maps from the ‘JHU White MatterTractography Atlas’ (Hua et al., 2008). Probability was thresholdedat 30% both for the left and for the right UF ROI, excluding voxelswith a low probability of being located within the UF. Resulting ROIsizes were 1074 mm3 for the left UF and 488 mm3 for the right UFROI. In support of a valid analysis, we considered equal probabilitiesmore important than equal sizes of left and right UF ROIs. Forstatistical analysis, voxel-wise FA mean values were extracted fromindividual, normalized and unsmoothed FA maps for both ROIsusing MarsBaR toolbox of SPM 5 (Brett et al., 2002). Subsequently,these values were inspected for plausibility to be located inWM foreach subject. To control for global mean FA, the ratio of within-UFmean FA to whole-brain mean FA (in the following referred to as“normalized” FA) was used for group comparison (independenttwo-tailed t-tests, p < 0.05) and correlation with trait anxiety(Pearson correlation and Spearman correlation). In addition to FA,axial and radial diffusivity were analyzed for both ROIs using therespective diffusivity maps.
subjects, p<0.00001voxel-wiseuncorrected,p<0.05 cluster-extent FWE-corrected).
T (max) FA (mean � SD) d
SAD HC
6.70 0.21 � 0.03 0.26 � 0.04 1.776.70 0.38 � 0.03 0.43 � 0.03 1.56
al fasciculus; SAD: patients with social anxiety disorder; HC: healthy subjects.
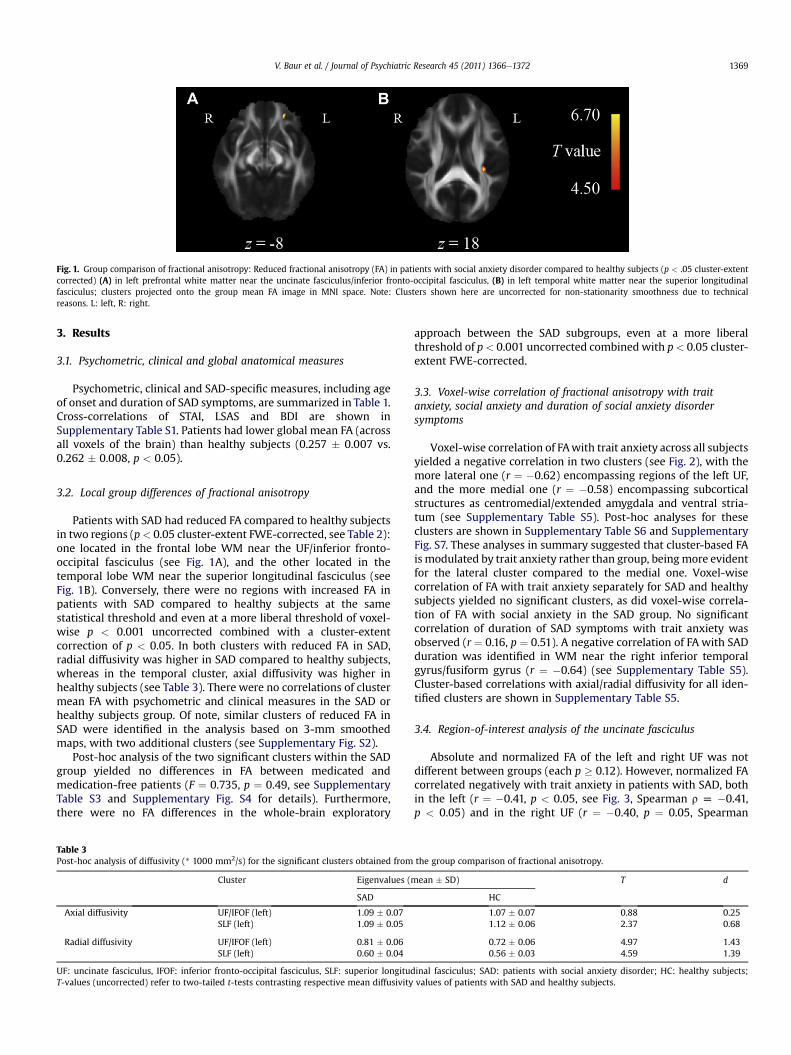
Fig. 1. Group comparison of fractional anisotropy: Reduced fractional anisotropy (FA) in patients with social anxiety disorder compared to healthy subjects (p < .05 cluster-extentcorrected) (A) in left prefrontal white matter near the uncinate fasciculus/inferior fronto-occipital fasciculus, (B) in left temporal white matter near the superior longitudinalfasciculus; clusters projected onto the group mean FA image in MNI space. Note: Clusters shown here are uncorrected for non-stationarity smoothness due to technicalreasons. L: left, R: right.
V. Baur et al. / Journal of Psychiatric Research 45 (2011) 1366e1372 1369
3. Results
3.1. Psychometric, clinical and global anatomical measures
Psychometric, clinical and SAD-specific measures, including ageof onset and duration of SAD symptoms, are summarized in Table 1.Cross-correlations of STAI, LSAS and BDI are shown inSupplementary Table S1. Patients had lower global mean FA (acrossall voxels of the brain) than healthy subjects (0.257 � 0.007 vs.0.262 � 0.008, p < 0.05).
3.2. Local group differences of fractional anisotropy
Patients with SAD had reduced FA compared to healthy subjectsin two regions (p< 0.05 cluster-extent FWE-corrected, see Table 2):one located in the frontal lobe WM near the UF/inferior fronto-occipital fasciculus (see Fig. 1A), and the other located in thetemporal lobe WM near the superior longitudinal fasciculus (seeFig. 1B). Conversely, there were no regions with increased FA inpatients with SAD compared to healthy subjects at the samestatistical threshold and even at a more liberal threshold of voxel-wise p < 0.001 uncorrected combined with a cluster-extentcorrection of p < 0.05. In both clusters with reduced FA in SAD,radial diffusivity was higher in SAD compared to healthy subjects,whereas in the temporal cluster, axial diffusivity was higher inhealthy subjects (see Table 3). There were no correlations of clustermean FA with psychometric and clinical measures in the SAD orhealthy subjects group. Of note, similar clusters of reduced FA inSAD were identified in the analysis based on 3-mm smoothedmaps, with two additional clusters (see Supplementary Fig. S2).
Post-hoc analysis of the two significant clusters within the SADgroup yielded no differences in FA between medicated andmedication-free patients (F ¼ 0.735, p ¼ 0.49, see SupplementaryTable S3 and Supplementary Fig. S4 for details). Furthermore,there were no FA differences in the whole-brain exploratory
Table 3Post-hoc analysis of diffusivity (* 1000 mm2/s) for the significant clusters obtained from
Cluster Eigenvalues (m
SAD
Axial diffusivity UF/IFOF (left) 1.09 � 0.07SLF (left) 1.09 � 0.05
Radial diffusivity UF/IFOF (left) 0.81 � 0.06SLF (left) 0.60 � 0.04
UF: uncinate fasciculus, IFOF: inferior fronto-occipital fasciculus, SLF: superior longitudT-values (uncorrected) refer to two-tailed t-tests contrasting respective mean diffusivity
approach between the SAD subgroups, even at a more liberalthreshold of p< 0.001 uncorrected combined with p< 0.05 cluster-extent FWE-corrected.
3.3. Voxel-wise correlation of fractional anisotropy with traitanxiety, social anxiety and duration of social anxiety disordersymptoms
Voxel-wise correlation of FAwith trait anxiety across all subjectsyielded a negative correlation in two clusters (see Fig. 2), with themore lateral one (r ¼ �0.62) encompassing regions of the left UF,and the more medial one (r ¼ �0.58) encompassing subcorticalstructures as centromedial/extended amygdala and ventral stria-tum (see Supplementary Table S5). Post-hoc analyses for theseclusters are shown in Supplementary Table S6 and SupplementaryFig. S7. These analyses in summary suggested that cluster-based FAis modulated by trait anxiety rather than group, beingmore evidentfor the lateral cluster compared to the medial one. Voxel-wisecorrelation of FA with trait anxiety separately for SAD and healthysubjects yielded no significant clusters, as did voxel-wise correla-tion of FA with social anxiety in the SAD group. No significantcorrelation of duration of SAD symptoms with trait anxiety wasobserved (r ¼ 0.16, p ¼ 0.51). A negative correlation of FA with SADduration was identified in WM near the right inferior temporalgyrus/fusiform gyrus (r ¼ �0.64) (see Supplementary Table S5).Cluster-based correlations with axial/radial diffusivity for all iden-tified clusters are shown in Supplementary Table S5.
3.4. Region-of-interest analysis of the uncinate fasciculus
Absolute and normalized FA of the left and right UF was notdifferent between groups (each p � 0.12). However, normalized FAcorrelated negatively with trait anxiety in patients with SAD, bothin the left (r ¼ �0.41, p < 0.05, see Fig. 3, Spearman r [ �0.41,p < 0.05) and in the right UF (r ¼ �0.40, p ¼ 0.05, Spearman
the group comparison of fractional anisotropy.
ean � SD) T d
HC
1.07 � 0.07 0.88 0.251.12 � 0.06 2.37 0.68
0.72 � 0.06 4.97 1.430.56 � 0.03 4.59 1.39
inal fasciculus; SAD: patients with social anxiety disorder; HC: healthy subjects;values of patients with SAD and healthy subjects.
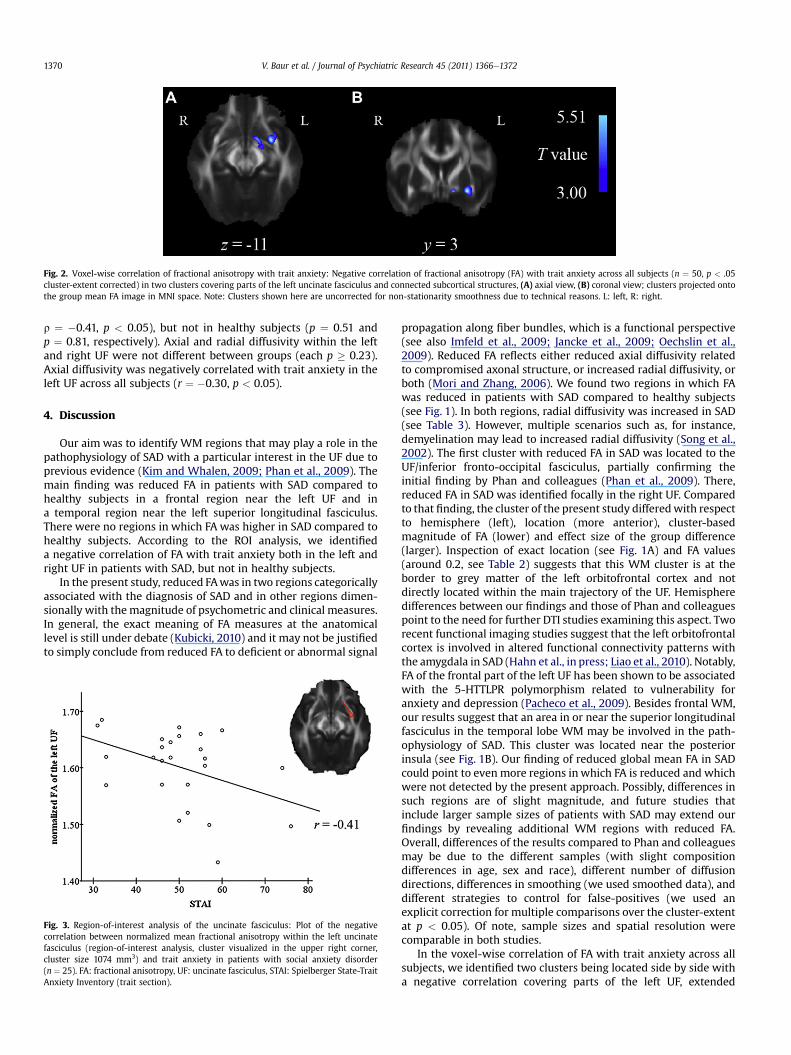
Fig. 2. Voxel-wise correlation of fractional anisotropy with trait anxiety: Negative correlation of fractional anisotropy (FA) with trait anxiety across all subjects (n ¼ 50, p < .05cluster-extent corrected) in two clusters covering parts of the left uncinate fasciculus and connected subcortical structures, (A) axial view, (B) coronal view; clusters projected ontothe group mean FA image in MNI space. Note: Clusters shown here are uncorrected for non-stationarity smoothness due to technical reasons. L: left, R: right.
V. Baur et al. / Journal of Psychiatric Research 45 (2011) 1366e13721370
r ¼ �0.41, p < 0.05), but not in healthy subjects (p ¼ 0.51 andp ¼ 0.81, respectively). Axial and radial diffusivity within the leftand right UF were not different between groups (each p � 0.23).Axial diffusivity was negatively correlated with trait anxiety in theleft UF across all subjects (r ¼ �0.30, p < 0.05).
4. Discussion
Our aim was to identify WM regions that may play a role in thepathophysiology of SAD with a particular interest in the UF due toprevious evidence (Kim and Whalen, 2009; Phan et al., 2009). Themain finding was reduced FA in patients with SAD compared tohealthy subjects in a frontal region near the left UF and ina temporal region near the left superior longitudinal fasciculus.There were no regions in which FA was higher in SAD compared tohealthy subjects. According to the ROI analysis, we identifieda negative correlation of FA with trait anxiety both in the left andright UF in patients with SAD, but not in healthy subjects.
In the present study, reduced FAwas in two regions categoricallyassociated with the diagnosis of SAD and in other regions dimen-sionally with themagnitude of psychometric and clinical measures.In general, the exact meaning of FA measures at the anatomicallevel is still under debate (Kubicki, 2010) and it may not be justifiedto simply conclude from reduced FA to deficient or abnormal signal
Fig. 3. Region-of-interest analysis of the uncinate fasciculus: Plot of the negativecorrelation between normalized mean fractional anisotropy within the left uncinatefasciculus (region-of-interest analysis, cluster visualized in the upper right corner,cluster size 1074 mm3) and trait anxiety in patients with social anxiety disorder(n ¼ 25). FA: fractional anisotropy, UF: uncinate fasciculus, STAI: Spielberger State-TraitAnxiety Inventory (trait section).
propagation along fiber bundles, which is a functional perspective(see also Imfeld et al., 2009; Jancke et al., 2009; Oechslin et al.,2009). Reduced FA reflects either reduced axial diffusivity relatedto compromised axonal structure, or increased radial diffusivity, orboth (Mori and Zhang, 2006). We found two regions in which FAwas reduced in patients with SAD compared to healthy subjects(see Fig. 1). In both regions, radial diffusivity was increased in SAD(see Table 3). However, multiple scenarios such as, for instance,demyelination may lead to increased radial diffusivity (Song et al.,2002). The first cluster with reduced FA in SAD was located to theUF/inferior fronto-occipital fasciculus, partially confirming theinitial finding by Phan and colleagues (Phan et al., 2009). There,reduced FA in SAD was identified focally in the right UF. Comparedto that finding, the cluster of the present study differedwith respectto hemisphere (left), location (more anterior), cluster-basedmagnitude of FA (lower) and effect size of the group difference(larger). Inspection of exact location (see Fig. 1A) and FA values(around 0.2, see Table 2) suggests that this WM cluster is at theborder to grey matter of the left orbitofrontal cortex and notdirectly located within the main trajectory of the UF. Hemispheredifferences between our findings and those of Phan and colleaguespoint to the need for further DTI studies examining this aspect. Tworecent functional imaging studies suggest that the left orbitofrontalcortex is involved in altered functional connectivity patterns withthe amygdala in SAD (Hahn et al., in press; Liao et al., 2010). Notably,FA of the frontal part of the left UF has been shown to be associatedwith the 5-HTTLPR polymorphism related to vulnerability foranxiety and depression (Pacheco et al., 2009). Besides frontal WM,our results suggest that an area in or near the superior longitudinalfasciculus in the temporal lobe WM may be involved in the path-ophysiology of SAD. This cluster was located near the posteriorinsula (see Fig. 1B). Our finding of reduced global mean FA in SADcould point to even more regions in which FA is reduced and whichwere not detected by the present approach. Possibly, differences insuch regions are of slight magnitude, and future studies thatinclude larger sample sizes of patients with SAD may extend ourfindings by revealing additional WM regions with reduced FA.Overall, differences of the results compared to Phan and colleaguesmay be due to the different samples (with slight compositiondifferences in age, sex and race), different number of diffusiondirections, differences in smoothing (we used smoothed data), anddifferent strategies to control for false-positives (we used anexplicit correction for multiple comparisons over the cluster-extentat p < 0.05). Of note, sample sizes and spatial resolution werecomparable in both studies.
In the voxel-wise correlation of FA with trait anxiety across allsubjects, we identified two clusters being located side by side witha negative correlation covering parts of the left UF, extended

V. Baur et al. / Journal of Psychiatric Research 45 (2011) 1366e1372 1371
amygdala (Heimer, 2003) and basal ganglia (see Fig. 2). We areaware that there may be conceptual issues concerning this corre-lation analysis, since there was a significant difference with a higheffect between SAD and healthy subjects in trait anxiety, whereasthe voxel-wise correlation was performed across all subjects (SADand healthy subjects). Post-hoc analyses (see Supplementarymaterial S6/S7) suggested that e at least for the lateral clusterlocated in the UFe the group difference in trait anxiety did not biasthe correlation. Yet, we explicitly prompt caution in interpretingthe results of this correlation analysis with regard to dimensionalassociations with general anxiety, especially for the medial cluster.It cannot be completely ruled out that disorder-related effects otherthan general anxiety have biased the results, since trait anxiety andgroup affiliation are highly correlated factors. In addition, we didnot identify similar clusters in the voxel-wise correlation separatelyfor the two groups. Notably, however, the mentioned clustersencompass posterior UF and connected subcortical structures,which replicates a recent study demonstrating in healthy subjectsa negative correlation between FA and trait anxiety in very similarareas (Kim and Whalen, 2009). Furthermore, structures as theextended amygdala and ventral striatum are implicated in modelsof anxiety-related processes (LeDoux and Gorman, 2001). Theymaybe considered part of cortico-striato-thalamo-cortical loops(Alexander et al., 1986) which have been implicated in the patho-physiology of a number of neuropsychiatric disorders (Heimer,2003). Projections from the centromedial amygdala to the ventralstriatum are considered important in the shift from passive-avoiding behavior towards active-coping reactions in response tofear-inducing stimuli (LeDoux and Gorman, 2001).
The ROI analysis in the bilateral UF according to our a-priorihypothesis based on previous findings of Phan and colleagues(Phan et al., 2009) revealed no significant group differences withinthe left and right UF, which was not according to our hypothesis.This was possibly due to the relatively large extent of theanatomically defined UF ROIs, if group differences were solelypresent in a small region within the ROIs. Although there were nogroup differences, FA correlated negatively with trait anxiety bothin the left (see Fig. 3) and right UF in the SAD group. In healthysubjects, no such correlation could be identified. This might reflectthat structural alterations are dimensionally associated withpathological mechanisms or increased compensatory efforts due tosevere anxiety, which is present in patients but not in healthysubjects. Moreover, we found a negative correlation of axial diffu-sivity with trait anxiety in the left UF across all subjects. As the UFinterconnects the amygdala and orbitofrontal cortex (Ghashghaeiet al., 2007), it may mediate inhibitory control over the amygdalaby frontal cortices, which may counteract pathological anxietystates (Bishop, 2007, 2009; Etkin et al., 2009). Albeit small, theidentified correlation suggests that there might be a link betweenthe integrity of UF fibers and the capacity of regulatory influence onanxiety. However, more research is still necessary to confirm thishypothesis.
Where may the identified WM alterations in SAD stem from?Because SAD has a considerable genetic component (Mosing et al.,2009; Stein and Stein, 2008) and an early age of onset (Stein andStein, 2008), mechanisms promoting the disorder may be man-ifested in the brain’s WM architecture, which might be reflected byaltered FA. Obviously, it cannot be stated by the present studywhether the identified changes of FA in patients with SAD stemfrom changes at an early developmental stage or from changesoccurring in the course of the disorder. The latter may be particu-larly possible given the mean duration of SAD of 16 (�10.6) years inthe examined sample of patients. In this context, it also cannot bestated whether the identified WM alterations are specific to SAD.More unspecific experiences like frequent exposure to stress, which
is present in any anxiety disorder, may also have lead to theobserved group differences. DTI studies comparing different statesof anxiety/anxiety disorders could help clarify this issue.
4.1. Limitations
The impact of medication on FA is still unknown. Several studiesreported no association between psychotropic medication and FA(McIntosh et al., 2008; Sussmann et al., 2009; Wang et al., 2008a,2008b; Yurgelun-Todd et al., 2007). Similarly, our analysessuggest that medication did not have any impact on FA in oursample. However, we are careful to generalize this finding to othersorts of medication and other psychiatric disorders. Another limi-tation is unequal statistical power (due to heterogeneous samplesizes) in the correlation analyses for trait anxiety, social anxiety andduration of SAD symptoms. This constrains the direct comparisonof the resulting statistical maps to a certain extent. We suggestconsidering the results from the correlation analyses with caution.
5. Conclusion
Taken together, our results partially confirm and extend theinitial study by Phan and colleagues (Phan et al., 2009). Evidence offrontal WM alterations in or near the UF in SAD converges, whereasthere may be further WM structures being involved in the patho-physiology of SAD. More research on functional correlates ofreduced FA has to be done in future studies, particularly to clarifythe role of the UF and related structures in fear, anxiety, generalemotion processing, and emotion regulation.
Role of the funding source
Funding for this study was provided by a grant of the SwissNational Foundation to UH. The funding source had no involvementin the study design, the collection, analysis and interpretation ofthe data, the writing of the report, and the decision to submit thepaper for publication.
Contributors
Volker Baur, Jürgen Hänggi, Uwe Herwig and Annette Brühldesigned the study. Michael Rufer, Aba Delsignore, Uwe Herwigand Annette Brühl were responsible for patient recruitment, diag-nosis and clinical assessment/testing. Volker Baur, Jürgen Hänggi,Lutz Jäncke, and Annette Brühl undertook the statistical analysis.All authors contributed to the discussion and interpretation of theresults. Volker Baur wrote the first draft of the manuscript. Allauthors contributed to and have approved the final manuscript.
Conflict of interestAll authors declare that they have no conflicts of interest.
Acknowledgments
We thank BeatWerner, University Children’s Hospital Zurich, fortechnical assistance with DTI data acquisition.
Appendix. Supplementary material
Supplementary data associated with this article can be found, inthe online version, at doi:10.1016/j.jpsychires.2011.05.007.

V. Baur et al. / Journal of Psychiatric Research 45 (2011) 1366e13721372
References
Ackenheil M, Stotz-Ingenlath G, Dietz-Bauer R, Vossen A. M.I.N.I. Mini Internationalneuropsychiatric interview, German version 5.0.0 DSM-IV. München: Psychia-trische Universitätsklinik München; 1999.
Alexander GE, DeLong MR, Strick PL. Parallel organization of functionally segregatedcircuits linking basal ganglia and cortex. Annual Review of Neuroscience 1986;9:357e81.
Annett M. A classification of hand preference by association analysis. British Journalof Psychology 1970;61:303e21.
Baker SL, Heinrichs N, Kim HJ, Hofmann SG. The liebowitz social anxiety scale asa self-report instrument: a preliminary psychometric analysis. BehaviourResearch and Therapy 2002;40:701e15.
Basser PJ, Pierpaoli C. Microstructural and physiological features of tissues eluci-dated by quantitative-diffusion-tensor MRI. Journal of Magnetic ResonanceSeries B 1996;111:209e19.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuringdepression. Archives of General Psychiatry 1961;4:561e71.
Behrens TE, Woolrich MW, Jenkinson M, Johansen-Berg H, Nunes RG, Clare S, et al.Characterization and propagation of uncertainty in diffusion-weighted MRimaging. Magnetic Resonance in Medicine 2003;50:1077e88.
Bishop SJ. Neurocognitive mechanisms of anxiety: an integrative account. Trends inCognitive Sciences 2007;11:307e16.
Bishop SJ. Trait anxiety and impoverished prefrontal control of attention. NatureNeuroscience 2009;12:92e8.
Brett M, Anton J, Valabregue R, Poline J. June 2-6, 2002, Sendai, Japan. Available onCD-ROM in Neuroimage. Region of interest analysis using an SPM toolbox[abstract] Presented at the 8th International Conference on functional mappingof the Human brain, Vol 16; 2002. No. 2.
Davis M, Whalen PJ. The amygdala: vigilance and emotion. Molecular Psychiatry2001;6:13e34.
Ebeling U, von Cramon D. Topography of the uncinate fascicle and adjacenttemporal fiber tracts. Acta Neurochirurgica (Wien) 1992;115:143e8.
Eickhoff SB, Stephan KE, Mohlberg H, Grefkes C, Fink GR, Amunts K, et al. A newSPM toolbox for combining probabilistic cytoarchitectonic maps and functionalimaging data. Neuroimage 2005;25:1325e35.
Etkin A, Prater KE, Schatzberg AF, Menon V, Greicius MD. Disrupted amygdalarsubregion functional connectivity and evidence of a compensatory network ingeneralized anxiety disorder. Archives of General Psychiatry 2009;66:1361e72.
Ghashghaei HT, Hilgetag CC, Barbas H. Sequence of information processing foremotions based on the anatomic dialogue between prefrontal cortex andamygdala. Neuroimage 2007;34:905e23.
Ha TH, Kang DH, Park JS, Jang JH, Jung WH, Choi JS, et al. White matter alterations inmale patientswith obsessive-compulsive disorder. Neuroreport 2009;20:735e9.
Hahn A, Stein P, Windischberger C, Weissenbacher A, Spindelegger C, Moser E,Kasper S, Lanzenberger R. Reduced resting-state functional connectivitybetween amygdala and orbitofrontal cortex in social anxiety disorder. Neuro-image, in press.
Hautzinger M, Bailer M, Worall H, Keller F. Beck-Depressions-Inventar (BDI). Bear-beitung der deutschen Ausgabe. Testhandbuch. Bern, Göttingen. Toronto,Seattle: Huber; 1994.
Hayasaka S, Nichols TE. Combining voxel intensity and cluster extent withpermutation test framework. Neuroimage 2004;23:54e63.
Hayasaka S, Phan KL, Liberzon I, Worsley KJ, Nichols TE. Nonstationary cluster-sizeinference with random field and permutation methods. Neuroimage 2004;22:676e87.
Heimer L. A new anatomical framework for neuropsychiatric disorders and drugabuse. American Journal of Psychiatry 2003;160:1726e39.
Hirsch CR, Clark DM. Information-processing bias in social phobia. ClinicalPsychology Review 2004;24:799e825.
Hua K, Zhang J, Wakana S, Jiang H, Li X, Reich DS, et al. Tract probability maps instereotaxic spaces: analyses of white matter anatomy and tract-specific quan-tification. Neuroimage 2008;39:336e47.
Imfeld A, Oechslin MS, Meyer M, Loenneker T, Jancke L. White matter plasticity inthe corticospinal tract of musicians: a diffusion tensor imaging study. Neuro-image 2009;46:600e7.
Jancke L, Koeneke S, Hoppe A, Rominger C, Hanggi J. The architecture of the golfer’sbrain. PLoS One 2009;4:e4785.
Jefferys D. Social phobia. The most common anxiety disorder. Australian FamilyPhysician 1997;26(1061):1064e7.
Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, et al. Lifetimeand 12-month prevalence of DSM-III-R psychiatric disorders in the Unitedstates. Results from the National Comorbidity Survey. Archives of GeneralPsychiatry 1994;51:8e19.
Kim MJ, Whalen PJ. The structural integrity of an amygdala-prefrontal pathwaypredicts trait anxiety. Journal of Neuroscience 2009;29:11614e8.
Kubicki M. Neurocognition and white matter imaging: can the relationship bereliably quantified? American Journal of Psychiatry 2010;167:373e5.
Laux L, Glanzmann P, Schaffner P, Spielberger CD. Das State-Trait-Angstinventar(Testmappe mit Handanweisung, Fragebogen STAI-G Form X 1 und Frageb-ogen STAI-G Form X 2). Weinheim: Beltz Testgesellschaft; 1981.
LeDoux JE, Gorman JM. A call to action: overcoming anxiety through active coping.American Journal of Psychiatry 2001;158:1953e5.
Liao W, Qiu C, Gentili C, Walter M, Pan Z, Ding J, et al. Altered effective connectivitynetwork of the amygdala in social anxiety disorder: a resting-state FMRI study.PLoS One; 2010:e15238.
Liebowitz MR. Social phobia. Modern Problems of Pharmacopsychiatry 1987;22:141e73.
McIntosh AM, Munoz Maniega S, Lymer GK, McKirdy J, Hall J, Sussmann JE, et al.White matter tractography in Bipolar Disorder and schizophrenia. BiologicalPsychiatry 2008;64:1088e92.
Mori S, Zhang J. Principles of diffusion tensor imaging and its applications to basicneuroscience research. Neuron 2006;51:527e39.
Mosing MA, Gordon SD, Medland SE, Statham DJ, Nelson EC, Heath AC, et al. Geneticand environmental influences on the co-morbidity between depression, panicdisorder, agoraphobia, and social phobia: a twin study. Depression and Anxiety2009;26:1004e11.
Ochsner KN, Gross JJ. The cognitive control of emotion. Trends in Cognitive Sciences2005;9:242e9.
Oechslin MS, Imfeld A, Loenneker T, Meyer M, Jancke L. The plasticity of thesuperior longitudinal fasciculus as a function of musical expertise: a diffusiontensor imaging study. Frontiers in Human Neuroscience 2009;3:76.
Pacheco J, Beevers CG, Benavides C, McGeary J, Stice E, Schnyer DM. Frontal-limbicwhite matter pathway associations with the serotonin transporter genepromoter region (5-HTTLPR) polymorphism. Journal of Neuroscience 2009;29:6229e33.
Park HJ, Westin CF, Kubicki M, Maier SE, Niznikiewicz M, Baer A, et al. White matterhemisphere asymmetries in healthy subjects and in schizophrenia: a diffusiontensor MRI study. Neuroimage 2004;23:213e23.
Petrides M, Pandya DN. Efferent association pathways from the rostral prefrontalcortex in the macaque monkey. Journal of Neuroscience 2007;27:11573e86.
Phan KL, Orlichenko A, Boyd E, Angstadt M, Coccaro EF, Liberzon I, et al. Preliminaryevidence of white matter abnormality in the uncinate fasciculus in generalizedsocial anxiety disorder. Biological Psychiatry 2009;66:691e4.
Sheehan DV, Lecrubier Y, Sheehan KH, Amorim P, Janavs J, Weiller E, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and vali-dation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10.Journal of Clinical Psychiatry 1998;59:22e33.
Smith SM. Fast robust automated brain extraction. Human Brain Mapping 2002;17:143e55.
Smith SM, Jenkinson M, Woolrich MW, Beckmann CF, Behrens TEJ, Johansen-Berg H,et al. Advances in functional and structural MR image analysis and imple-mentation as FSL. Neuroimage 2004;23:S208e19.
Song SK, Sun SW, Ramsbottom MJ, Chang C, Russell J, Cross AH. Dysmyelinationrevealed through MRI as increased radial (but unchanged axial) diffusion ofwater. Neuroimage 2002;17:1429e36.
Spielberger CD, Gorsuch RL, Lushene RE. State-Trait anxiety inventory, Manual forthe state-trait anxiety inventory. Palo Alto, CA: Consulting Psychologist Press;1970.
Stangier U, Heidenreich T. Die Liebowitz Soziale Angst Skala (LSAS). Göttingen:Hogrefe; 2005.
Stein MB, Stein DJ. Social anxiety disorder. Lancet 2008;371:1115e25.Sussmann JE, Lymer GK, McKirdy J, Moorhead TW, Munoz Maniega S, Job D, et al.
White matter abnormalities in Bipolar Disorder and schizophrenia detectedusing diffusion tensor magnetic resonance imaging. Bipolar Disorders 2009;11:11e8.
Wang F, Jackowski M, Kalmar JH, Chepenik LG, Tie K, Qiu M, et al. Abnormal anteriorcingulum integrity in Bipolar Disorder determined through diffusion tensorimaging. British Journal of Psychiatry 2008a;193:126e9.
Wang F, Kalmar JH, Edmiston E, Chepenik LG, Bhagwagar Z, Spencer L, et al.Abnormal corpus callosum integrity in Bipolar Disorder: a diffusion tensorimaging study. Biological Psychiatry 2008b;64:730e3.
Worsley KJ, Andermann M, Koulis T, MacDonald D, Evans AC. Detecting changes innonisotropic images. Human Brain Mapping 1999;8:98e101.
Yurgelun-Todd DA, Silveri MM, Gruber SA, Rohan ML, Pimentel PJ. White matterabnormalities observed in Bipolar Disorder: a diffusion tensor imaging study.Bipolar Disorders 2007;9:504e12.





























