Embed Size (px)
Citation preview

1
THE EFFECTS OF DIFFERENT TYPES OF ANTIDEPRESSANTS ON DENTAL IMPLANT FAILURE: A RETROSPECTIVE AND IN VITRO STUDY
By
GABRIELA VILA
A THESIS PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT
OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE
UNIVERSITY OF FLORIDA
2018

2
© 2018 Gabriela Vila

3
To my family who has been my rock and guidance throughout my life, always encouraging and supporting me to pursuit my goals

4
ACKNOWLEDGMENTS
I thank my boyfriend, friends and family for their support, unconditional love and
enthusiasm throughout my education. I thank Dr. Jia Chang for his great mentorship
and guidance through all phases of my project. I would also like to thank Dr. Abeer
Hakam, Dr. Marcia Mbadu, Dr. Hotoun Shuwaikan, and Dr. Dania Al Angany for their
help with the clinical and mechanism portions of my study. Additionally, I will like to
thank my committee members for their advice and supervision in the completion of my
thesis. And last but not least, I will like to express my appreciation and gratitude to the
faculty and staff of the UF Department of Periodontology for all their help and support
over the past three years. Furthermore, I will like to address that this research was
financially supported by UFCD Start-up grant 00127658 (to Dr. Jia Chang), and for that I
am deeply grateful.

5
TABLE OF CONTENTS page
ACKNOWLEDGMENTS .................................................................................................. 4
LIST OF TABLES ............................................................................................................ 7
LIST OF FIGURES .......................................................................................................... 8
LIST OF ABBREVIATIONS ............................................................................................. 9
ABSTRACT ................................................................................................................... 11
CHAPTER
1 INTRODUCTION .................................................................................................... 13
Implant Dentistry ..................................................................................................... 13
Peri-implant Disease ............................................................................................... 14 Peri-implant Diagnosis ............................................................................................ 14 Osseointegration ..................................................................................................... 15
Depression .............................................................................................................. 16 Antidepressants Prescription and Side Effects ....................................................... 16
Classification of Antidepressants ............................................................................ 17
Monoamine Oxidase Inhibitors ......................................................................... 17
Tricyclic Antidepressants .................................................................................. 18 Selective Serotonin and Serotonin Norepinephrine Reuptake Inhibitors .......... 18
Atypical Antidepressants .................................................................................. 19 Antidepressant Usage Distribution .......................................................................... 19 Retrospective Studies ............................................................................................. 19 In-Vitro Studies ....................................................................................................... 20
Study Aim ............................................................................................................... 21 Primary Outcome and Null Hypothesis ............................................................. 21
Secondary Outcomes ....................................................................................... 22
2 MATERIALS AND METHODS ................................................................................ 24
Retrospective Clinical Study ................................................................................... 24 Statistical Analysis .................................................................................................. 25 In-Vitro Mechanism Study ....................................................................................... 25
The Effect of Antidepressants on Osteogenesis During Bone Formation ......... 25 The Effect of Antidepressants on Osteoclastogenesis During Bone
Resorption ..................................................................................................... 26
3 RESULTS ............................................................................................................... 27
Retrospective Clinical Study ................................................................................... 27

6
In-Vitro Mechanism Study ....................................................................................... 28
4 DISCUSSION ......................................................................................................... 44
Retrospective Clinical Study ................................................................................... 44 In-Vitro Mechanism Study ....................................................................................... 46
LIST OF REFERENCES ............................................................................................... 50
BIOGRAPHICAL SKETCH ............................................................................................ 55

7
LIST OF TABLES
Table page 1-1 Classification of commonly prescribed antidepressants ..................................... 23
3-1 Effect of antidepressant users and healthy non-users on dental implant bone resorption and implant failure ............................................................................. 30
3-2 Dental implant failure association between antidepressant users vs. non-users of antidepressants .................................................................................... 31
3-3 Distribution of antidepressant prescription among the dental implant patients ... 32
3-4 Comparison of mRNA an protein expression of osteogenic markers among different type of antidepressant .......................................................................... 33
3-5 Comparison of effect on osteoclastogenesis between 4 types of antidepressants .................................................................................................. 34

8
LIST OF FIGURES Figure page 3-1 Dental implant failure rate among antidepressants users and nonusers. *,
P<0.05 (compared with no AD user) .................................................................. 35
3-2 Risk ratio of Dental implant failure rate among antidepressants users and nonusers. *, P<0.05 (compared with no AD user) .............................................. 36
3-3 The ALP staining of Mc3T3 cells with the different types of antidepressant treatment during their osteogenic induction ........................................................ 37
3-4 The mRNA expression of osteogenic marker genes in Mc3T3 cells grown on the surface of titanium plates .............................................................................. 38
3-5 The protein expression of a master osteogenic transcriptional factor, Runx-2 in MC3T3 cells .................................................................................................... 39
3-6 The TRAP staining of RAW cells with the different types of antidepressant treatment during their osteoclastogenesis .......................................................... 40
3-7 Counting of TRAP staining position cells (osteoclasts) in the previous experiments (*, P<0.05) ...................................................................................... 41
3-8 RNA assays gene expression on osteoclastogenesis in RAW cells treated with different antidepressants ............................................................................. 42
3-9 Protein assays in RAW cells with different types of antidepressants .................. 43
4-1 Comparison of different studies on dental implant failure associated with antidepressant use ............................................................................................. 49

9
LIST OF ABBREVIATIONS
2D Two dimensional
2- PCPA Tranylcypromine hydrochloride
AA Atypical Antidepressants
AD Antidepressants
ALP Alkaline Phosphatase
AR Androgen Receptor
ASA American Society of Anesthesiology
BOP Bleeding on probing
BSP Bone Sialoprotein
CAL Clinical Attachment Level
CDC Centers for Disease Control and Prevention
CNS Central nervous system
DNA Deoxy-Ribonucleic Acid
FPD Fixed Partial Denture
GEE Generalized Estimating Equation
hBMSCs Human primary bone marrow stromal cells
IL-6 Interleukin 6
MAOI Monoamine Oxidase Inhibitors
Mc3T3 Murine pre-osteoblast cells
MG63 Human osteoblast cells
MMP9 Matrix Metallopeptidase 9
mRNA Messenger RNA (see RNA)
NFATc-1 Nuclear factor of activated T-cells cytoplasmic 1
OPG Osteoprotegerin

10
OSX Osterix
PCR Polymerase Chain Reaction
PD Probing Depth
RANKL Receptor activator of nuclear factor kappa-B ligand
RAW Murine macrophage cell line
RNA Ribonucleic acid
RPD Removable Partial Denture
RT Reverse transcriptase
Runx-2 Runt-related transcription factor 2
SD Standard Deviation
SNRI Serotonin-Norepinephrine Reuptake Inhibitors
SSRI Selective Serotonin Reuptake Inhibitors
TCA Tricyclic Antidepressants
TRAP Tartrate Resistant Acid Phosphatase
TRIzol® Chemical solution used in RNA/DNA/protein extraction
VDO Vertical dimension of occlusion
α-MEM Alpha Minimal Essential Medium

11
Abstract of Thesis Presented to the Graduate School of the University of Florida in Partial Fulfillment of the Requirements for the Degree of Master of Science
THE EFFECTS OF DIFFERENT TYPES OF ANTIDEPRESSANTS ON DENTAL
IMPLANT FAILURE: A RETROSPECTIVE AND IN VITRO STUDY
By
Gabriela Vila
May 2018
Chair: Jia Chang Major: Dental Sciences−Periodontics
Recent clinical studies have reported an increased risk of dental implant failure
associated with the use of selective serotonin reuptake inhibitors (SSRI) family of
antidepressants [1, 2]. This can be attributed to the negative effects of SSRIs on bone
metabolism [3, 4]. However, studies by our group found that, in addition to SSRIs, other
types of antidepressants such as serotonin-norepinephrine reuptake inhibitors (SNRI),
tricyclic antidepressants (TCA), atypical antidepressants, and monoamine oxidase
inhibitors (MAOI) also affect bone metabolism and turnover.
The purpose of this study is (1) to examine the effects of antidepressant use on
implant failure, and (2) to study the effect of these antidepressants on the osteogenic
and osteoclastic activity of cells. To evaluate the effects of antidepressant use on
implant failure a retrospective study of patients who received dental implants in the
Graduate Periodontology Clinic at the University of Florida was performed. Additionally,
cells were cultured in vitro with different antidepressant dosages to assess the
osteogenic and osteoclastic effects.
Significant higher implant failure rates were observed in subjects who were
antidepressant users. SNRI antidepressants showed the highest implant failure among

12
all other types of antidepressants. SSRIs were the most popular group of
antidepressants used, while the MAOI group was rarely provided. Furthermore, the in
vitro studies showed that osteoblastic and osteoclastic cells exhibited different patterns
of function when treated with different types of antidepressants. SSRI, SNRI and TCA
antidepressants suppressed osteogenic differentiation, while MAOI antidepressant
stimulated their osteogenic differentiation. Conversely, SSRI, SNRI and TCA
antidepressants increased osteoclastogenesis in vitro, while MAOI antidepressant
inhibited osteoclastic differentiation and functions.

13
CHAPTER 1 INTRODUCTION
Implant Dentistry
Implant therapy has revolutionized dentistry over the past 30 years. The days
when missing teeth could only be replaced by fixed partial dentures (FPDs) or
removable partial dentures (RPDs) are long gone. While FPDs and RPDs can provide
adequate function and esthetics to patients, these treatment options are tooth-borne
prosthetics that could compromise soft and hard tissue structures of the mouth. Some of
the long-term complications of FPDs include damage to the tooth and pulp of the
abutment teeth, secondary caries, failure of the bridge due to fractures or loss of
retention, and increased plaque accumulation that can lead to inflammation of the
surrounding tissues resulting in periodontal disease [5]. Furthermore, RPDs are typically
not comfortable or esthetically pleasing to the patient; they can lack retention and
stability, and compromise the remaining dentition [6, 7].
In the last few decades, research has proven the successful use of dental
implants as an alternative to tooth-borne prosthetic restorations. Some of the
advantages of implant therapy include but are not limited to preventing the disuse
atrophy of the alveolar bone following tooth loss, superior esthetics, maintenance of
Vertical Dimension of Occlusion (VDO), establishment of proper occlusion, enhanced
function of other prosthesis, and improvement of patient’s psychological health [8, 9].
Therefore, implants have become an integral part of the dental field, and are the optimal
treatment option for replacing missing teeth. However, implants are not immune to
periodontal disease, and the literature suggests that over a period of 10 years,
approximately 1 in 20 implants is lost [10, 11].

14
Peri-implant Disease
Peri-implantitis is characterized by inflammation of the peri-implant tissues and
the loss of supporting bone, which can lead to failure of the dental implant [12, 13]. This
condition is comparable to periodontitis around natural dentition, and it is preceded by
peri-implant mucositis, which is comparable to gingivitis [11]. Peri-implantitis has been
reported to occur in between 28% and 56% of patients and comprising 12% to 40%
implants sites [14]. Peri-implant mucositis is defined as the presence of a plaque-related
inflammatory soft tissue infiltrate without concurrent loss of peri-implant bone tissue
[15]. It is a reversible condition. However, if left untreated it may progress to peri-
implantitis[11]. Therefore, early intervention of peri-implantitis is key in the prevention of
peri-implantitis. Peri-implant mucositis has been reported to occur in approximately 80%
of patients and involving 50% of implant sites [14]. Some of the risk indicators for peri-
implantitis are poor oral hygiene, a history of periodontitis, diabetes, and smoking [14,
16, 17]. As the use of dental implants become more and more popular for the
replacement of missing teeth, peri-implantitis is a present and future challenge for both
patients and dental practitioners [12].
Peri-implant Diagnosis
Following implant placement, it is critical to periodically evaluate the condition of
the surrounding tissues to ensure its maintenance and proper care. This can be done
during supportive periodontal treatment through clinical and radiographic examinations.
The clinical exam will entail a complete periodontal assessment measuring probing
depths (PD), evaluating the presence or absence of bleeding on probing (BOP) and
suppuration, monitoring clinical attachment levels (CAL), and calculating radiographic
bone levels. Increases in PDs are typically associated with inflammation resulting from

15
an increase in periodontal pathogens [18]. Periodontal probing can successfully monitor
the CAL changes in dental implants that may relate to radiographic bone levels [19].
Clinically, the presentation of peri-implantitis is similar to that of periodontitis,
which may include the presence of erythema, increased PD, the presence of BOP,
possible mucosal recession and suppuration, and bone resorpion [11, 13, 16]. The
mobility of an implant would be a sign of total failure due to complete lack of
osseointegration and it should be removed. Therefore, mobility is not a useful sign for
early diagnosis [10, 13, 16, 20].
Osseointegration
Osseointegration is defined as a “direct structural and functional connection
between ordered living bone and the surface of a load-carrying implant” [21].
Osseointegration refers to a histological term, that can only be partially confirmed
clinically and radiographically [22]. Osseointegration occurs at two different stages:
primary and secondary. Primary osseointegration is the mechanical engagement of the
implant with the surrounding bone directly after implant placement. Secondary
osseointegration takes place as bone remodeling occurs around the implant and bone
forms in the grooves in the surface of the implant [23]. Primary stability refers to the
strength of the primary osseointegration at time of implant placement and is a critical
factor for the long-term success of dental implants [24]. Over the years, implant therapy
and osseointegration have become a very reliable treatment option with mean survival
rates >95% to restore the function and esthetics of missing teeth
outperforming
conventional FPDs [25-27].

16
Depression
Depression is a psychiatric disorder, which affects a person’s mood, thoughts,
behavioral patterns, feelings, and sense of well-being over time. The usual symptoms of
depression include but may not be limited to sadness, apathy, and loss of interest in
daily activities [28]. It is a common disease in the United States, with increasing
prevalence among young adults (between 18 and 44 years of age), of which 6% of
women and 2% of men are afflicted with it in any 6-month period of time [29]. The World
Health Organization (WHO) estimates that more than 350 million people worldwide
suffer from depression [1]. Current management of acute episodes, as well as long-term
prophylaxis for depression, includes the use of potent antidepressive medications [30].
Antidepressants Prescription and Side Effects
Nowadays, antidepressants are being prescribed by physicians for a variety of
therapeutic reasons other than psychiatric disorders; these include insomnia, pain
management, eating disorders, substance abuse, and smoking cessation [31-36].
Numerous studies have identified adverse orofacial reactions that may occur with
antidepressant use. Many adverse effects have been reported among antidepressant
users. Patients on antidepressant therapy commonly report symptoms of dry mouth.
Xerostomia is one of the most concerning side effect in the dental field, which can
contribute to oral mucosal changes, increased susceptibility to caries, fungal infections,
changes in taste, difficulty and swallowing [37-40].
Other studies have found even more concerning side effects related to
antidepressant use affecting bone metabolism, such as osteoporosis [1-4, 41, 42]. In
general, the mechanism of function of many antidepressants involves the serotonin
system. Serotonin receptors are not exclusive to the nervous system and can also be

17
found in the digestive, cardiovascular and skeletal systems [43]. As serotonin is actively
involved in bone metabolism, this may play an integral role in implant dentistry and
osseointegration of implants. Both bone forming and bone degrading cells, osteoblasts
and osteoclasts respectively, express serotonin receptors that can be exposed to
serotonin via autocrine, paracrine and endocrine pathways [44]. Some studies have
shown antidepressants to have a direct negative effect on bone metabolism by
increasing osteoclast differentiation and inhibiting osteoblast proliferation [43, 45]. Thus,
it can be hypothesized that antidepressant use can affect osseointegration of implants,
and consequently, may result in implant failure. Therefore, it is of great importance for
the dental practitioner to be aware and familiar with the different antidepressant
medications and the common side effects that these may have on a patient’s dentition.
Classification of Antidepressants
The major categories of antidepressants include monoamine oxidase inhibitors
(MAOI), tricyclic antidepressants (TCA), selective serotonin reuptake inhibitors (SSRI),
serotonin-norepinephrine reuptake inhibitors (SNRI), and atypical antidepressants (AA)
(Table 1-1).
Monoamine Oxidase Inhibitors
The MAOIs were among the first antidepressants originated in the early 1950s.
These antidepressants inhibit the action of monoamine oxidase, MAO, an enzyme that
is responsible for the breakdown of several neurotransmitters, including serotonin and
norepinephrine. Inhibition of such enzyme is thought to relieve symptoms of depression
by allowing the accumulation of serotonin and norepinephrine in the presynaptic
junction, and thus enhancing neuronal activity. MAOIs can cause dizziness, orthostatic
hypotension, insomnia, central nervous system (CNS) stimulation, weight gain and

18
edema. Furthermore, MAOIs prevent the liver from inactivating tyramine and if the
patient does not follow dietary restrictions, a fatal hypertensive crisis can occur [37, 46].
Many psychiatrists are reluctant to prescribe MAOIs due to the potentially severe
adverse reactions [29].
Tricyclic Antidepressants
The TCAs were introduced in the late 1950s and greatly replaced the use of
MAOIs in the treatment of depression. They are effective in increasing serotonin and
norepinephrine in the synapse [47]. Major side effects associated with the use of TCAs
include peripheral anticholinergic side effects such as xerostomia, urinary retention,
constipation and blurred vision; as well as central anticholinergic side effects such as
impaired concentration and confusion [29, 37].
Selective Serotonin and Serotonin Norepinephrine Reuptake Inhibitors
Early researchers in psychopharmacology concluded that depressive symptoms
were the result of a decrease in the functional concentrations of serotonin and or
norepinephrine at the receptor sites in the brain [29]. Serotonin is a monoamine
neurotransmitter in the brain that contributes to the feelings of well-being and
happiness. Hence, lower levels of serotonin or its decreased use can lead to depression
[48]. Norepinephrine, also called noreadrenaline, is a catecholamine that functions in
the brain and body as a hormone and neurotransmitter [49]. The SSRIs debuted in the
1970s and dominated the market through the 1980s. Their mechanism of action
involved the blockage of serotonin reuptake by brain neurons, making the
neurotransmitter available to synaptic receptors. The SNRIs were introduced in the
early 1990s and gained popularity due to their dual mechanism of action involving the
blockage of both norepinephrine and serotonin reuptake from within the synaptic cleft

19
into the presynaptic terminal of neurons [49]. These groups of antidepressants can
frequently cause diarrhea, nausea, dizziness, insomnia, anxiety or agitation, tremor,
headache, sexual dysfunction and, on occasion, an increase in bleeding time [37].
Atypical Antidepressants
Lastly, in the 1980s and 1990s, the AAs made their way to the market. These
exert their effect through varied mechanisms, which include selective norepinephrine
reuptake inhibition, dopamine reuptake inhibition and antagonist, and reversible
inhibition ofmonoamine oxidase A. These antidepressants have been commonly
associated with orthostatic hypotension; electrocardiographic changes; tachycardia and
agranulocytosis; and infrequent reports of agranulocytosis and neutropenia have also
been reported [37, 49-51].
Antidepressant Usage Distribution
According to data from the Centers for Disease Control and Prevention (CDC),
more than one in ten Americans over the age of 12 use antidepressants, making it the
most prescribed type of drug in the United States. A study by Keen et al. reported a
21% prevalence of antidepressant use among a total of 1800 dental records. They
found that female antidepressant users outnumbered male users by a 2.3:1 ratio.
Furthermore, about 58% of patients were receiving treatment with more than one
medication that potentially caused xerostomia [52]. The antidepressant class more
frequently prescribed was SSRIs followed by TCAs, AAs and MOAIs.
Retrospective Studies
Osseointegration of implants is influenced by bone metabolism, and therefore,
antidepressant use may interfere with this process. A retrospective cohort study by Wu
et al. reported that compared to SSRIs non-users, SSRI usage was associated with

20
increased dental implant failure risk. A total of 914 implants were included in the study.
They found a 10.6% implant failure rate for SSRI users and 4.6% for SSRI non-users,
respectively[1]. Moreover, a pilot study conducted in 2016 by the University of Buffalo
also found an association between antidepressant use and dental implant failure. They
reported that patients taking antidepressants were four times more likely to have implant
failure compared to patients with no history of antidepressant use. Among 74 subjects
receiving dental implants, 33% of subjects with implant failures reported taking at least
one antidepressant drug [24].
Another retrospective study published in 2017, reported an implant failure rate of
12.5% for SSRI users and 3.3% for non-users. The total number of implants included in
the study was 931, of which 35 failed. However, they used a multivariate GEE model
that did not show a significant association between SSRI intake and increased risk of
dental implant failure [2]. Given the conflicting data, further studies are needed to
confirm or reject a direct association between SSRI antidepressant use and increased
implant failures. Meanwhile, the question remains whether dental implant failure is also
associated with the use of other major groups of antidepressants besides SSRIs.
In-Vitro Studies
Selective serotonin reuptake inhibitors (SSRIs), the most extensively used
antidepressants, have been reported to affect bone formation and consequently
increase the risk of bone fractures [53]. SSRIs have shown to be sequestered in the
bone marrow at considerably higher concentrations than in the blood or the brain [42].
However, the mechanism of action by which it affects human osteoblast and osteoclast
formation remains unclear. Gustafsson et al.[3] examined the in vitro effects of serotonin
and the serotonin transporter inhibitor fluoxetine, commonly known as “Prozac,” on

21
osteoblasts and osteoclasts. They found that serotonin at 1umol/L concentrations
increased osteoprotegerin (OPG) and decreased the receptor activator of RANKL
secretion from osteoblasts, which suggests that serotonin plays a role in osteoblast
induced inhibition of osteoclast differentiation. On the contrary, fluoxetine had the
opposite effect increasing RANKL in more than threefold, and decreasing OPG to about
43% aiding in the upregulation of osteoclast differentiation.
Another in vitro study by Hodge et al.[4] demonstrated that SSRIs differentially
inhibit bone cell formation via apoptosis, which may also explain the mechanisms of
bone resorption related to chronic use of antidepressants. More specifically, they found
that all SSRIs, except citaprolam, dose-dependently inhibited osteoclast formation and
resorption between the concentration of 1umol/L and 10umol/L. Sertraline was the most
potent antidepressant, followed by fluoxetine, paroxetine, fluvoxamine and citaprolam
being the least potent. Similarly, all SSRIs, except citaprolam, inhibited alkaline
phosphatase and bone mineralization by osteoblasts only when exposed to 30umol/L
concentrations. Lastly, they found that apoptosis was induced by SSRIs in both
osteoclasts and osteoblasts in an identical pattern to the inhibitory effects previously
described[4].
Study Aim
The purpose of this retrospective clinical study was to evaluate whether using
different types of antidepressants is associated with different levels of dental implant
bone resorption and failure.
Primary Outcome and Null Hypothesis
The primary outcome of the study is the effect of different antidepressant usage
among dental implant patients of the University of Florida Center for Advanced

22
Periodontics and Implant Dentistry from 2011 to 2016. The null hypothesis is that
antidepressant usage does not affect bone metabolism and turnover, and it does not
affect on implant failure in dental implant patients.
Secondary Outcomes
The secondary outcomes of this study is (1) to investigate the effect of four major
types of antidepressants (SSRI, SNRI, MAOI, TCA) on osteogenic differentiation of
osteoblastic cells; and on osteoclast development and functions in vitro; and (2) to
provide the proper guidelines or references for clinicians to choose antidepressants
showing less negative effects on dental implant survival.

23
Table 1-1. Classification of commonly prescribed antidepressants
Antidepressant Class
Generic drug name
AAs
Bupropion Mirtazapine Nefazodone Trazodone
MAOIs Phenelzine
Tranylcypromine
SNRIs Desvenlafaxine
Duloxetine Venlafaxine
SSRIs
Citaprolam Escitalopram
Fluoxetine Fluvoxamine Paroxetine Sertraline
TCAs
Amitriptyline Clomipramine Desipramine
Doxepine Imipramine Nortriptyline Protriptyline Trimipramine

24
CHAPTER 2 MATERIALS AND METHODS
Retrospective Clinical Study
This is a retrospective study of patients aged 18 or older who received dental
implants in the University of Florida Center for Advanced Periodontics and Implant
Dentistry between January 2011 and 2016. A search of the clinic’s electronic health
records (AXIUM) was used to obtain the medical background of the implant-receiving
patients. Implant failure was defined as loss of an implant; failing implants were defined
as those with 50% or more radiographic peri-implant bone resorption.
Inclusion criteria consisted of (1) Exposure group: patients who reported using at
least one type of antidepressant, who are healthy or with mild systemic disease that is
under control as classified by the American Society of Anesthesiology (ASA I and II); (2)
Control group: patients with no reported history of antidepressant use, who were healthy
or with mild systemic disease that is under control as classified by the American Society
of Anesthesiology (ASA I and II).
Exclusion criteria consisted of patients with severe systemic disease, such as
ASA III or IV. Patients were also excluded if they were pregnant, or had a medical
disorder known to substantially affect bone metabolism, such as smokers, osteoporosis,
osteomalacia, Paget’s disease, vitamin D deficiency, hyperthyroidism, cancer (excluding
melanoma skin cancer), as were those on bisphosphonates.
The antidepressants were categorized into five major groups, including selective
serotonin reuptake inhibitors (SSRI), serotonin-norepinephrine reuptake inhibitors
(SNRI), tricyclic antidepressants (TCA), atypical antidepressants, and monoamine
oxidase inhibitors (MAOI). The information of antidepressant usage for each patient who

25
fulfilled our inclusion cafeteria was recorded. Total 772 patients were included in this
study, and 71 patients among them took one or more type of antidepressants.
Statistical Analysis
This retrospective study was designed to examine the association between
dental implant failure and antidepressant intake. Implant failure rates for healthy
subjects and subjects taking different antidepressant was calculated using Binormal
proportion confidence intervals, and a 95% confidence interval for odd ratio. Failure
rates are presented in figures as means ± standard deviations (SD). The results were
considered statistically significant if the corresponding p-value was <0.05.
In-Vitro Mechanism Study
The Effect of Antidepressants on Osteogenesis During Bone Formation
The common prescribed drugs from four types of antidepressants such as
Sertraline (Zoloft, SSRI), Venlafaxine (Effexor, SNRI), Amitriptyline (TCA),
Tranylcypromine (Parnate, MAOI) were used to treat osteogenic cells such as murine
pre-osteoblast (Mc3T3) cells, human osteoblast (MG63) cells, and human primary bone
marrow stromal cells (hBMSCs), respectively.
The osteogenic cells were pretreated with 0.1mM Tranylcypromine, 10mM
Sertraline, 2uM Venlafaxine, and 20uM Amitriptyline for 24 hours before cultured in
osteogenic induction medium (α-MEM with 10% fetal bovine serum supplemented with
additional β-glycerophosphate, dexamethasone, and ascorbic acid) for 3, 7 and 14
days. The mRNA expression of osteogenic-specific marker genes (Runx-2, OSX, BSP,
and ALP) was examined for all groups by using real-time reverse-transcription (RT)
PCR. Cells from day 0 and day seven were used for ALP assays. Cells from day 0 and
day 14 were used for AR assays. Total RNA was extracted with TRIzol® Reagent.

26
Additionally, the protein expression of the key osteogenic transcriptional factor, Runx-2,
was detected by western blots.
Furthermore, osteogenic cells were seeded onto regular 2D cell culture in plastic
cell dishes and plates, as well as directly onto the surface of titanium plates to mimic the
growth environment around dental implants.
The Effect of Antidepressants on Osteoclastogenesis During Bone Resorption
The above-mentioned antidepressants were also used with distinctive dosages to
treat murine monocyte RAW cells during their osteoclastic differentiation. Raw cells
were pretreated with 0.1mM Tranylcypromine, 10mM Sertraline, 2uM Venlafaxine, and
20uM Amitriptyline for 24 hours before their osteoclastic induction with recombinant
protein RANKL at 20ng/ml. After six days of cultures, all groups of cells were fixed and
stained with TRAP staining kit (Sigma) according to our previous protocols[54].
The number of TRAP-positive osteoclast cells were counted and compared
between all groups of cells pretreated with the different type of antidepressants.
Meanwhile, the total RNA at this time point was harvested from all groups with TRIzol®
Reagent, and the mRNA expression of osteoclastogenesis related genes (TRAP,
RANKL, MMP9, and IL-6) was examined by using real-time reverse-transcription PCR.
Additionally, the protein expression of the key osteoclastic transcriptional factor, NFATc-
1, was detected by western blots in Raw cell protein extracts after 24 hours of
antidepressant treatment.

27
CHAPTER 3 RESULTS
Retrospective Clinical Study
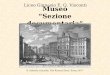
Patients on antidepressants showed an implant failure rate of 10.71% compared
to healthy individuals at 1.34%, and non-users of antidepressants with mild systemic
disease at 2.92% (Table 3-1). Among all groups of antidepressant users, SNRI users
showed the highest dental implant failure, with failure and failing rates of 21.43% and
16.07%, respectively (Table 3-1; Figure 3-1). Interestingly, SSRI users did not show a
very significant increase of dental implant failure rate compared to healthy individuals,
with failure rates at 2.79%. As a matter of fact, SSRIs showed decreased dental implant
failure rate compared with that of non-users with mild systemic disease. Furthermore,
AA and TCA users showed significant higher implant failure and failing rates than
nonusers or healthy individuals (Table 3-1). Additionally, we found an increased risk
ratio for antidepressant users at approximately 4.48. More specifically, SNRI and AA
groups showed statistically significant higher risk ratio for implant failure at
approximately 8.95 and 3.8, respectively (Table 3-2, Figure 3-2).
Among the 772 patients that received dental implants, 9.2% of them took
antidepressants (71 patients) and 107 antidepressant prescriptions were given. Among
all prescriptions of antidepressants, SSRI group was the most commonly provided
(n=51), followed by the atypical group (n=28), the SNRI group (n=22), the TCA group
(n=5), and finally, by the MAOI group (n=1). In regards to the frequency of
antidepressant prescription, Welbutrin (Bupropion, Atypical), Zoloft (Sertraline, SSRI),
Celexa (Citalopram, SSRI) and Effexor (Venlafaxine, SNRI) are the four most common
prescriptions of antidepressants given (Table 3-3).

28
In-Vitro Mechanism Study
To evaluate the effect of antidepressants on osteoblast function, in-vitro testing
was performed on osteogenic cells such as murine pre-osteoblast (Mc3T3) cells, human
osteoblast (MG63) cells, and human primary bone marrow stromal cells (hBMSCs).
Both ALP and mineralization staining, as well as RNA and protein assays, presented a
decreased osteogenic activity with Sertraline (SSRI), Venlafaxine (SNRI), and
Amitriptyline (TCA). Conversely, Tranylcypromine (MAOI) treatment induced osteogenic
activity in pre-osteoblasts and hBMSCs (Table 3-4, Figure 3-3). The osteogenic cells
cultured on titanium surface exhibited similar patterns of osteogenic gene mRNA
expression to the cells growing on titanium plates (Figure 3-4). The protein expression
of a master osteogenic transcriptional factor, Runx-2 in MC3T3 cells was reduced by
the treatment of Sertraline (SSRI), Venlafaxine (SNRI) and Amitriptilyne (TCA)
medications, but not by PCPA treatment (Figure 3-5).
To understand the effect of different antidepressants on osteoclastic
differentiation and function, in vitro testing was performed on murine monocyte RAW
cells during their osteoclastic differentiation. TRAP staining, RNA and protein assays
showed increased osteoclastogenesis in RAW cells treated with Sertraline (SSRI),
Venlafaxine (SNRI), and Amitriptyline (TCA). More specifically, Trap staining showed a
statistical significant increased in positive cell numbers with Sertraline (SSRI),
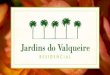
Venlafaxine (SNRI) and Amitriptyline (TCA) (Figures 3-6; 3-7). Furthermore, RNA
assays showed an increase in osteoclastogenesis gene expression of approximately
four-fold in TRAP cells treated with Venlafaxine (SNRI) and Amitriptyline (TCA); a two-
fold and four-fold increase in MMP9 gene expression in RAW cells treated with
Venlafaxine (SNRI) and Amitriptiline (TCA), respectively (Figures 3-8, 3-9). Interestingly,

29
Tranylcypromine (MAOI) treatment inhibited, NFATc-1, osteoclastogenesis-related gene
expression (Table 3-5; Figure 3-9).

30
Table 3-1. Effect of antidepressant users and healthy non-users on dental implant bone resorption and implant failure
No
failure Failure Failing Total
Failure
rate (%)
Failing
rate (%)
Healthy 591 8 2 599 1.34 0.33
Antidepressants (ADs) 176 21 22 197 10.71 11.22
Types
of ADs
SSRIs 105 3 2 108 2.78 1.85
SNRIs 44 12 9 56 21.43 16.07
TCAs 25 1 5 26 3.85 19.23
MAOIs 2 0 0 2 0 0
AAs 49 5 6 54 9.26 11.11
Systemic Disease 1162 35 0 1197 2.92 0

31
Table 3-2. Dental implant failure association between antidepressant users vs. non-users of antidepressants
Failure
No failure Total
Failure rate (%) Risk ratio Odd (95% CI)
P value
(<0.05)
SD of dental implant
failure (%)
No AD user* 43 1753 1796 2.39420935
1
0.706397
AD user 21 175 196 10.7142857 4.47508306 4.89
(4.35-5.44) yes 4.330127
SSRIs 3 105 108 2.77777778 1.16020672 1.17
(-0.02-2.35) no 3.099386
SNRIs 12 44 56 21.4285714 8.95016611 11.12
(10.41-11.82) yes 10.74709
TCAs 1 25 26 3.84615385 1.60644007 1.63
(-0.39-3.65) no 7.39207
MAOIs 0 2 2 0 0 0 no 0
AAs 5 49 54 9.25925926 3.86735573 4.16
(3.19-5.13) yes 7.731228
Total 64 1928 1992 3.21285141 * Includes: healthy and those with mild systemic disease

32
Table 3-3. Distribution of antidepressant prescription among the dental implant patients
Antidepressants Brand & generic name Prescription number
SSRI group
(n=51)
Zoloft (Sertraline) 16 (14.9%)
Celexa (Citalopram) 15 (14%)
Prozac (fluoxetine) 7 (6.5%)
Paxil (Paroxetine) 7 (6.5%)
Lexapro (escitalopram) 6 (5.6%)
SNRI group
(n=22)
Effexor (Venlafaxine) 15 (14%)
Cymbalta (Duloxetine) 6 (5.6%)
Pristiq (Desvenlafaxine) 1 (0.9%)
Atypical group
(n=28)
Welbutrin (Bupropion) 19 (17.7%)
Desyrel (Trazodone) 7 (6.5%)
Remeron (Mirtazapine) 2 (1.8%)
TCA group
(n=5)
Elavil (Amitriptyline) 5(4.6%)
MAO group
(n=1)
Nardil (Phenelzine) 1(0.9%)

33
Table 3-4. Comparison of mRNA and protein expression of osteogenic markers among different type of antidepressant
Sertraline
(SSRI)
Venlafaxine
(SNRI)
Amitriptyline
(TCA)
Tranylcypromine
(MAOI)
RNA expression
of osteogenic
genes
↓
↓
↓
↑
Protein
expression of
osteogenic
genes
↓
↓
↓
↑

34
Table 3-5. Comparison of effect on osteoclastogenesis between 4 types of antidepressants
Sertraline
(SSRI)
Venlafaxine
(SNRI)
Amitriptyline
(TCA)
Tranylcypromine
(MAOI)
RNA expression of
osteoclastogenesis-
related genes
↑
↑
↑
↓
Protein expression
of
osteoclastogenesis-
related genes
↑
↑
↑
↓
TRAP staining ↑ ↑ ↑ ↓

35
Figure 3-1. Dental implant failure rate among antidepressants users and nonusers.
*, P<0.05 (compared with no AD user)
2.39
*10.71
2.78
*21.43
3.85
0.00
*9.26
0
5
10
15
20
25
30
35
No ADuser
AD user SSRI SNRI TCA MAO Atypical
De
nta
l im
pla
nt
failu
re r
ate
(%
)

36
Figure 3-2. Risk ratio of Dental implant failure rate among antidepressants users and nonusers. *, P<0.05 (compared with no AD user)

37
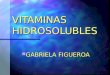
Figure 3-3. The ALP staining of Mc3T3 cells with the different types of antidepressant treatment during their osteogenic induction

38
Figure 3-4. The mRNA expression of osteogenic marker genes in Mc3T3 cells grown on the surface of titanium plates
0
1
2
3
4
Runx-2 OSX BSP ALP
Targ
et g
ene
exp
ress
ion
(fo
ld)
V
Sertraline
Venlafaxine
Amitriptyline
Tranylcypromine

39
Figure 3-5. The protein expression of a master osteogenic transcriptional factor, Runx-2 in MC3T3 cells
Runx-2
GAPDH

40
Figure 3-6. The TRAP staining of RAW cells with the different types of antidepressant
treatment during their osteoclastogenesis
Control RANKL RANKL + Tranylcypromine
RANKL + Sertraline
RANKL + Venlafaxine
RANKL + Amitriptyline

41
Figure 3-7. Counting of TRAP staining position cells (osteoclasts) in the previous experiments (*, P<0.05)

42
Figure 3-8. RNA assays gene expression on osteoclastogenesis in RAW cells treated
with different antidepressants
0
4
8
12
16
TRAP MMP9 IL-6
Gen
e ex
pre
ssio
n (
fold
)
Control
Sertraline
Venlafaxine
Amitriptyline
Tranylcypromine

43
Figure 3-9. Protein assays in RAW cells with different types of antidepressants

44
CHAPTER 4
DISCUSSION
Retrospective Clinical Study
The results of this present study demonstrated that different types of
antidepressants have a significant effect on dental implant failure. The retrospective
study was conducted on patients of the University of Florida Center for Advanced
Periodontics and Implant Dentistry between 2011 and 2016. The results showed that a
total of 9.2% of patients that took antidepressant medication prior to and during implant
treatment. More specifically, SSRIs were the most popular group of antidepressants
used, while the MAOI group was rarely provided to patients. Consistently with the
general population, we found that in our clinic SSRIs were the most widely used
antidepressants [55-57].
Among all antidepressant prescriptions, Welbutrin (Bupropion) in the atypical
group was the most frequently provided, followed by Zoloft (Sertraline) and Celexa
(Citalopram) in the SSRI group, and Effexor (Venlafaxine) in the SNRI group.
Furthermore, significant higher implant failure rates were observed in subjects who were
antidepressant users compared to non-users or healthy individuals, with SNRI
antidepressants having the highest dental implant failure rate at 23.43%. Additionally,
the AAs showed statistically significant higher dental implant failures with a rate of
9.26%. This is particularly concerning being that AAs, such as Welbutrin, are amongst
the most popular prescribed antidepressants in our clinic.
Our study is the first clinical retrospective study that screened for dental implant
failure rate among all five major groups of antidepressants used to date. Most
importantly, we found that SNRI group of antidepressants, rather than the SSRI group,

45
showed an increased risk of dental implant failure. This finding disagrees with Wu et al.
and Chrcanovic et al. studies, where SSRI medication users were exhibiting significant
higher dental implant failure rates [1, 2]. However, when taking a closer look at the
patient information in these mentioned studies, we noticed that patients taking
Venlafaxine, a SNRI drug, were included in their SSRI groups. Such grouping in these
two studies may have contributed to the inaccurate results of higher implant failure rates
among SSRI users. Therefore, for comparison purposes, we combined the data from
our SSRI and SNRI groups into one “SSRI” group as these two studies did.
Interestingly, this group showed a comparable trend of dental implant failure rate as
those reported by Wu et al. [1] and Chrcanovic et al. [2] studies.
Our findings showed a 3.83 fold increase in implant failure rate when comparing
to healthy non-users of antidepressants, versus 2.3 folds and 3.79 folds to that of Wu et
al.[1] and Chrcanovic et al.[2], respectively. Similarly, a pilot study conducted at the
University at Buffalo by Andreana et al.[58] grouped all types of antidepressants finding
a 2.95 fold increase in dental implant failure when comparing to healthy subjects (Figure
4-1). However, when we investigate SSRI and SNRI groups separately, SSRI shows
little effect on dental implant failure (2.78% implant failure rate); while SNRI group
showed the most significant implant failure among all the antidepressant users.
Nevertheless, this study indeed, for the first time, indicated an association between
SNRI usage and a higher risk of dental implant failure.
To avoid bias, comparable control and experimental groups with sufficient
sample size were included in the study as it involved healthy subjects as well as
subjects with mild systemic disease. However, there were still several factors that could

46
not be assessed in the study. For instance, lack of information on the patient
antidepressant’s drug compliance, dosage and treatment period; such information is
difficult to attain from patient charts and may be of influence on implant success rate
[53]. Thus, our findings indicate a strong association between antidepressant usage and
dental implant failure, in which SNRI groups exhibit the highest odds ratio
(approximately 8.95). To overcome the drawbacks of this cross-sectional study, further
prospective randomized control studies should be used to investigate whether it is a
caustic relationship between the use of antidepressants, especially SNRI, and dental
implant failure.
Within the limitations of this study, we have rejected the null hypothesis and have
demonstrated that antidepressants usage is associated with dental implant failure.
Thus, it is safe to say that antidepressant use may be identified as a potential risk factor
associated with the development of peri-implantitis, and ultimately, implant failure.
Moreover, the use of SNRI antidepressants, such as Cymbalta and Effexor, may be
associated with the greatest risk for implant failure among all other types of
antidepressants. Likewise, it can be concluded that SSRI medications, such as Zoloft
and Prozac, may be a safer alternative when compared to SNRIs and AAs in regards to
implant failure rates. Nevertheless, a preventive and interdisciplinary approach to the
treatment planning and management of dental implant receiving patients, particularly
those with a history of antidepressant medication usage, should be incorporated in
routine dental practice.
In-Vitro Mechanism Study
The results of this present study demonstrated the effect of different types of
antidepressants on osteoblasts and osteoclasts precursor cells. This study showed that

47
osteoblastic cells exhibited different patterns of osteogenic differentiation when treated
with different types of antidepressants in vitro. More specifically, Sertraline (SSRI),
Venlafaxine (SNRI) and Amitriptyline (TCA) antidepressants suppressed osteogenic
differentiation, while Tranylcypromine (MAOI) antidepressant stimulated their
osteogenic differentiation. On the contrary, Sertraline (SSRI), Venlafaxine (SNRI) and
Amitriptyline (TCA) increased osteoclastogenesis in vitro, while Tranylcypromine
(MAOI) antidepressant inhibited osteoclastic differentiation and functions. These results
are in agreement with Gustafsson et al.[3] and Hodge et al.[4] who have demonstrated
the inhibitory effects of certain antidepressant medications on bone formation through in
vitro studies on osteoblastic and osteoclastic cells.
Although MAOI may seem to be a better medication alternative given our results,
this group of antidepressants is associated with substantial side effects and are rarely
prescribed by physicians (<10% of antidepressant prescriptions) [59]. The rationale for
its limited use comes from its dangerous dietary and drug interactions, which can cause
fatal hypertensive crisis. Additionally, MAOIs can cause dizziness, orthostatic
hypotension, insomnia, CNS stimulation, edema and weight gain [60].
Limitations of the in vitro study model include using isolated cells that have been
removed from their natural environment, thereby eliminating the normal interaction and
protection mechanisms otherwise available in the organism [61]. To further verify the in
vitro results of antidepressants on osteoblast and osteoclast functions, animal
experiments are necessary. Likewise, the effects of antidepressants on bone
remodeling in a periodontal and peri-implant enviroments could be investigated in vivo.
In summary, within the limitations of this study, the results from our in vitro study further

48
support the findings of our retrospective clinical study; and may partially explain the
possible mechanisms in which different types of antidepressants, such as SNRI, may be
significantly associated with dental implant failure. Knowledge of these factors can
guide treatment-planning decisions by helping determine the possible need for proper
guidelines or references for clinicians to choose antidepressants showing less negative
effects on dental implant survival.

49
Figure 4-1. Comparison of different studies on dental implant failure associated with
antidepressant use

50
LIST OF REFERENCES
1. Wu, X., et al., Selective serotonin reuptake inhibitors and the risk of osseointegrated implant failure: a cohort study. J Dent Res, 2014. 93(11): p. 1054-61.
2. Chrcanovic, B.R., et al., Is the intake of selective serotonin reuptake inhibitors
associated with an increased risk of dental implant failure? Int J Oral Maxillofac Surg, 2017. 46(6): p. 782-788.
3. Gustafsson, B.I., et al., Serotonin and fluoxetine modulate bone cell function in
vitro. J Cell Biochem, 2006. 98(1): p. 139-51. 4. Hodge, J.M., et al., Selective serotonin reuptake inhibitors inhibit human
osteoclast and osteoblast formation and function. Biol Psychiatry, 2013. 74(1): p. 32-9.
5. Tan, K., et al., A systematic review of the survival and complication rates of fixed
partial dentures (FPDs) after an observation period of at least 5 years. Clin Oral Implants Res, 2004. 15(6): p. 654-66.
6. Leles, C.R., et al., Discriminant analysis of patients' reasons for choosing or
refusing treatments for partial edentulism. J Oral Rehabil, 2009. 36(12): p. 909-15.
7. Hummel, S.K., et al., Quality of removable partial dentures worn by the adult U.S.
population. J Prosthet Dent, 2002. 88(1): p. 37-43. 8. Isidor, F., Influence of forces on peri-implant bone. Clin Oral Implants Res, 2006.
17 Suppl 2: p. 8-18. 9. Albrektsson, Consensus report: implant therapy. 1994. 10. Mombelli, A., N. Müller, and N. Cionca, The epidemiology of peri-implantitis. Clin
Oral Implants Res, 2012. 23 Suppl 6: p. 67-76. 11. Zitzmann, N.U. and T. Berglundh, Definition and prevalence of peri-implant
diseases. J Clin Periodontol, 2008. 35(8 Suppl): p. 286-91. 12. Derks, J., et al., Peri-implantitis - onset and pattern of progression. J Clin
Periodontol, 2016. 43(4): p. 383-8. 13. Mombelli, A. and N.P. Lang, The diagnosis and treatment of peri-implantitis.
Periodontol 2000, 1998. 17: p. 63-76.

51
14. Lindhe, J., J. Meyle, and G.D.o.E.W.o. Periodontology, Peri-implant diseases: Consensus Report of the Sixth European Workshop on Periodontology. J Clin Periodontol, 2008. 35(8 Suppl): p. 282-5.
15. Derks, J. and C. Tomasi, Peri-implant health and disease. A systematic review of
current epidemiology. J Clin Periodontol, 2015. 42 Suppl 16: p. S158-71. 16. Heitz-Mayfield, L.J., Peri-implant diseases: diagnosis and risk indicators. J Clin
Periodontol, 2008. 35(8 Suppl): p. 292-304. 17. Rocchietta, I. and D. Nisand, A review assessing the quality of reporting of risk
factor research in implant dentistry using smoking, diabetes and periodontitis and implant loss as an outcome: critical aspects in design and outcome assessment. J Clin Periodontol, 2012. 39 Suppl 12: p. 114-21.
18. Quirynen, M., M. De Soete, and D. van Steenberghe, Infectious risks for oral
implants: a review of the literature. Clin Oral Implants Res, 2002. 13(1): p. 1-19. 19. Quirynen, M., et al., The reliability of pocket probing around screw-type implants.
Clin Oral Implants Res, 1991. 2(4): p. 186-92. 20. Heitz-Mayfield, L.J., Diagnosis and management of peri-implant diseases. Aust
Dent J, 2008. 53 Suppl 1: p. S43-8. 21. Brånemark, P.-I., G.A. Zarb, and T. Albrektsson, Tissue-Integrated Prostheses:
Osseointegration in Clinical Dentistry. 1985, Chicago: Quintessence Publ. Co. 22. Albrektsson, T., et al., The long-term efficacy of currently used dental implants: a
review and proposed criteria of success. Int J Oral Maxillofac Implants, 1986. 1(1): p. 11-25.
23. Greenstein, G., et al., Clinical recommendations for avoiding and managing
surgical complications associated with implant dentistry: a review. J Periodontol, 2008. 79(8): p. 1317-29.
24. Rabel, A., S.G. Köhler, and A.M. Schmidt-Westhausen, Clinical study on the
primary stability of two dental implant systems with resonance frequency analysis. Clin Oral Investig, 2007. 11(3): p. 257-65.
25. Coulthard, P., et al., Interventions for replacing missing teeth: preprosthetic
surgery versus dental implants. Cochrane Database Syst Rev, 2002(4): p. CD003604.
26. Derks, J., et al., Effectiveness of implant therapy analyzed in a Swedish
population: early and late implant loss. J Dent Res, 2015. 94(3 Suppl): p. 44S-51S.

52
27. Pjetursson, B.E., et al., A systematic review of the survival and complication rates of fixed partial dentures (FPDs) after an observation period of at least 5 years. Clin Oral Implants Res, 2004. 15(6): p. 667-76.
28. Association, A.P., Diagnostic and statistical manual of mental disorders, r.D.-R.
3rd Ed, Editor. 1987, American Psychiatric Association: Washington DC. 29. Friedlander, A.H. and L.J. West, Dental management of the patient with major
depression. Oral Surg Oral Med Oral Pathol, 1991. 71(5): p. 573-8. 30. Kaplan, H. and B. Sadock, Comprehensive textbook of psychiatry, ed. t. ed.
1989, Baltimore: William & Wilkins. 31. Fishbain, D., Evidence-based data on pain relief with antidepressants. Ann Med,
2000. 32(5): p. 305-16. 32. Egbunike, I.G. and B.J. Chaffee, Antidepressants in the management of chronic
pain syndromes. Pharmacotherapy, 1990. 10(4): p. 262-70. 33. Hajak, G., et al., Doxepin in the treatment of primary insomnia: a placebo-
controlled, double-blind, polysomnographic study. J Clin Psychiatry, 2001. 62(6): p. 453-63.
34. George, T.P., et al., A placebo controlled trial of bupropion for smoking cessation
in schizophrenia. Biol Psychiatry, 2002. 52(1): p. 53-61. 35. Robinson, P.H., Review article: recognition and treatment of eating disorders in
primary and secondary care. Aliment Pharmacol Ther, 2000. 14(4): p. 367-77. 36. Modigh, K., Antidepressant drugs in anxiety disorders. Acta Psychiatr Scand
Suppl, 1987. 335: p. 57-74. 37. Friedlander, A.H. and M.E. Mahler, Major depressive disorder. Psychopathology,
medical management and dental implications. J Am Dent Assoc, 2001. 132(5): p. 629-38.
38. Rindal, D.B., et al., Antidepressant xerogenic medications and restoration rates.
Community Dent Oral Epidemiol, 2005. 33(1): p. 74-80. 39. Greenspan, D., Xerostomia: diagnosis and management. Oncology (Williston
Park), 1996. 10(3 Suppl): p. 7-11. 40. Peeters, F.P., M.W. deVries, and A. Vissink, Risks for oral health with the use of
antidepressants. Gen Hosp Psychiatry, 1998. 20(3): p. 150-4.

53
41. Diem, S.J., et al., Use of antidepressants and rates of hip bone loss in older women: the study of osteoporotic fractures. Arch Intern Med, 2007. 167(12): p. 1240-5.
42. Bolo, N.R., Y. Hodé, and J.P. Macher, Long-term sequestration of fluorinated
compounds in tissues after fluvoxamine or fluoxetine treatment: a fluorine magnetic resonance spectroscopy study in vivo. MAGMA, 2004. 16(6): p. 268-76.
43. Tsapakis, E.M., et al., The adverse skeletal effects of selective serotonin
reuptake inhibitors. Eur Psychiatry, 2012. 27(3): p. 156-69. 44. Warden, S.J., et al., Serotonin (5-hydroxytryptamine) transporter inhibition
causes bone loss in adult mice independently of estrogen deficiency. Menopause, 2008. 15(6): p. 1176-83.
45. Battaglino, R., et al., Serotonin regulates osteoclast differentiation through its
transporter. J Bone Miner Res, 2004. 19(9): p. 1420-31. 46. Rabkin, J., et al., Adverse reactions to monoamine oxidase inhibitors. Part I. A
comparative study. J Clin Psychopharmacol, 1984. 4(5): p. 270-8. 47. Stahl, S.M., Neuroendocrine markers of serotonin responsivity in depression.
Prog Neuropsychopharmacol Biol Psychiatry, 1992. 16(5): p. 655-9. 48. Krishnan, V. and E.J. Nestler, The molecular neurobiology of depression. Nature,
2008. 455(7215): p. 894-902. 49. Coccaro, E.F. and L.J. Siever, Second generation antidepressants: a
comparative review. J Clin Pharmacol, 1985. 25(4): p. 241-60. 50. Stahl, S.M., Basic psychopharmacology of antidepressants, part 1:
Antidepressants have seven distinct mechanisms of action. J Clin Psychiatry, 1998. 59 Suppl 4: p. 5-14.
51. Lader, M.H., Tolerability and safety: essentials in antidepressant
pharmacotherapy. J Clin Psychiatry, 1996. 57 Suppl 2: p. 39-44. 52. Keene, J.J., G.T. Galasko, and M.F. Land, Antidepressant use in psychiatry and
medicine: importance for dental practice. J Am Dent Assoc, 2003. 134(1): p. 71-9.
53. Verdel, B.M., et al., Use of antidepressant drugs and risk of osteoporotic and
non-osteoporotic fractures. Bone, 2010. 47(3): p. 604-9.

54
54. Yu, B., et al., Wnt4 signaling prevents skeletal aging and inflammation by inhibiting nuclear factor-κB. Nat Med, 2014. 20(9): p. 1009-17.
55. Gibbons, R.D., et al., The relationship between antidepressant prescription rates
and rate of early adolescent suicide. Am J Psychiatry, 2006. 163(11): p. 1898-904.
56. Gibbons, R.D., et al., Relationship between antidepressants and suicide
attempts: an analysis of the Veterans Health Administration data sets. Am J Psychiatry, 2007. 164(7): p. 1044-9.
57. Newman, S.C. and D. Schopflocher, Trends in antidepressant prescriptions
among the elderly in Alberta during 1997 to 2004. Can J Psychiatry, 2008. 53(10): p. 704-7.
58. Andreana, S. and S. Gurung, A Pilot Study: Association between Antidepressant
Use and Implant Failure. 2016, University at Buffalo: Buffalo, NY. 59. Friedlander, A.H. and D.C. Norman, Late-life depression: psychopathology,
medical interventions, and dental implications. Oral Surg Oral Med Oral Pathol Oral Radiol Endod, 2002. 94(4): p. 404-12.
60. Livingston, M.G., Interactions with selective MAOIs. Lancet, 1995. 345(8949): p.
533-4. 61. Ghallab, A., In vitro test systems and their limitations. EXCLI J, 2013. 12: p.
1024-6.

55
BIOGRAPHICAL SKETCH
Gabriela Vila was born in Fort Lauderdale, Florida. At only 2 years old she
moved to Venezuela where she completed high school. She returned to South Florida
shortly after, to obtain her undergraduate degree with a Bachelor of Science in biology
at Florida International University. She continued her education at Nova Southeastern
University College of Dental Medicine and graduated in 2015 with a doctorate degree in
dental medicine. Currently, she is enrolled in her final semester of her post-doctoral
residency in Periodontology at the University of Florida College of Dentistry and
anticipates graduating in May 2018 with a certificate in periodontics and a Master of
Science. Following graduation, her plans are to return to South Florida to pursuit a
career in private practice as a Periodontist.