Embed Size (px)
Citation preview
Current reimbursement standards for hospitals receiving Medicare reimbursement are held to specific clinical core measures
One such measure is the time from door to antibiotic administration for patients with community acquired pneumonia
The standard was based on two research studies that found a relationship between time and morbidity and mortality in the elderly
Antibiotic administration within 4 hours of
arrival in random sample of older inpatients with community-acquired pneumonia who had not received antibiotics as outpatients› Decreased mortality › Decreased LOS
Administration within 4 hours› Prevent deaths in the Medicare population,› Offers cost savings for hospitals, › Feasible for most inpatients
Houck, P., Bratzler, D., Nsa, W., Ma, A., & Bartlett, J. (2004). Timing of antibiotic administration and outcomes for Medicare patients hospitalized with community acquired pneumonia. Archives of Internal Medicine, 164, 637-644
As an advanced practice nurse you will be held to meet clinical standards
One way to understand causation is through process flow chart
Flowing the process and identifying gaps in care will elucidate opportunities for quality improvement

Picture of the sequence of steps in a process
Maps out the action steps and decisions within a process, from beginning to end
Different steps or actions represented by boxes or other symbols
Help you identify and understand a process
Sources of information:› Chart Audits› Discussions with
Providers› Interviews with Patients
Often focus first on index case – › “What happened in this case?”
Then flow chart the usual course of events › “What usually happens?”
Once you have established an overview of the usual process, if needed, you may drill down to progressive levels of detail to understand nuances of the process.
Community-acquired pneumonia improvement team
ER admits - antibiotic administration times much improved
Ongoing delays noted on patients admitted directly to inpatient unit from clinic
Why the delays?
Pt arriveson ward
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. Verifiesorder
Pharm Tech
fills order
Medgiven
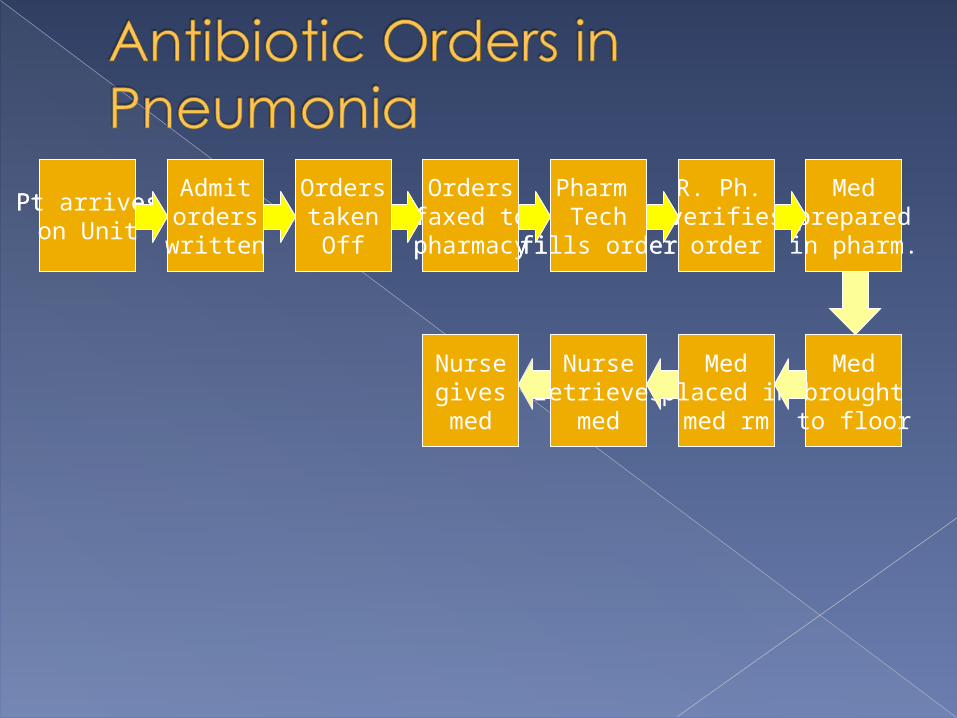
Pt arriveson Unit
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. verifiesorder
Pharm Tech
fills order
Medpreparedin pharm.
Medbroughtto floor
Medplaced inmed rm
Nurseretrieves
med
Nursegivesmed
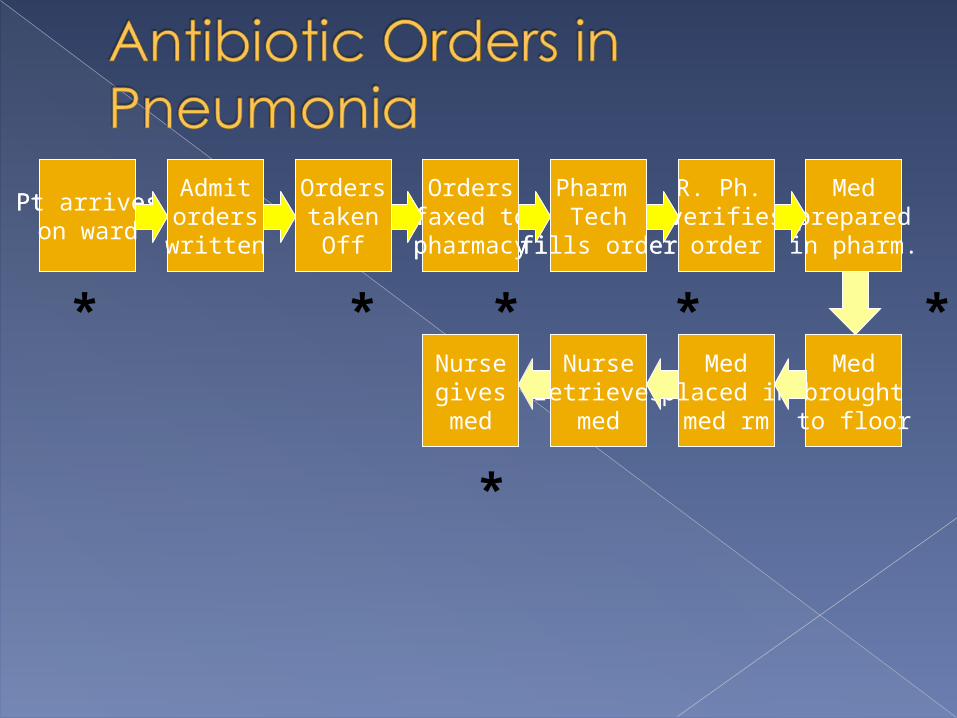
Pt arriveson ward
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. Verifiesorder
Pharm Tech
fills order
Medgiven
Pt arriveson ward
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. verifiesorder
Pharm Tech
fills order
Medpreparedin pharm.
Medbroughtto floor
Medplaced inmed rm
Nurseretrieves
med
Nursegivesmed
* * * * * *
*
Pt arriveson ward
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. Verifiesorder
Pharm Tech
fills order
Medgiven
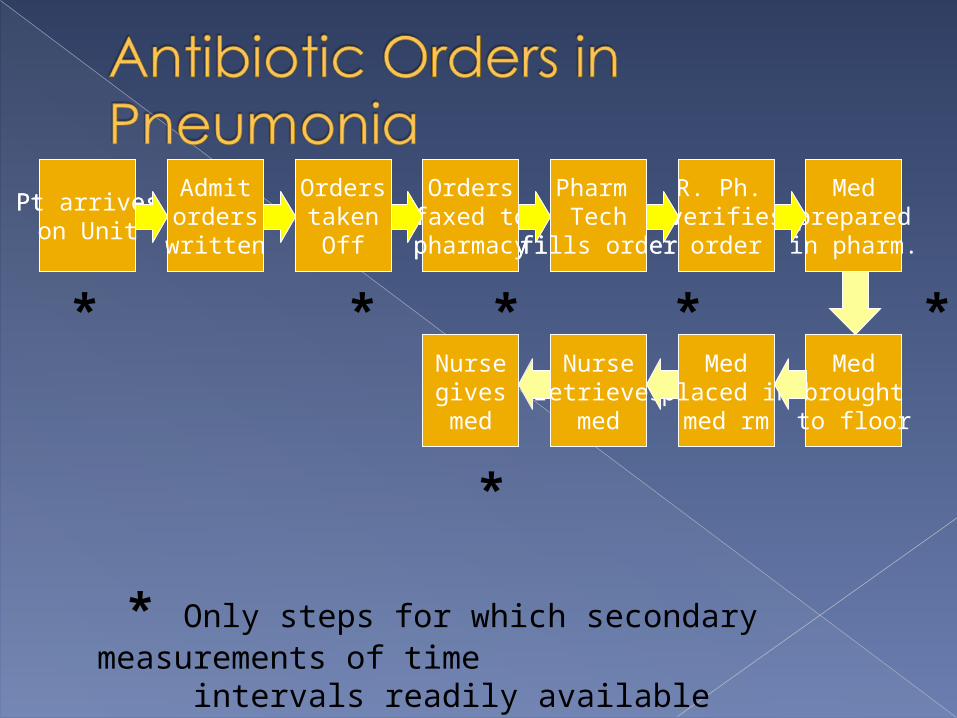
Pt arriveson Unit
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. verifiesorder
Pharm Tech
fills order
Medpreparedin pharm.
Medbroughtto floor
Medplaced inmed rm
Nurseretrieves
med
Nursegivesmed
* * * * * *
*
* Only steps for which secondary measurements of time intervals readily available
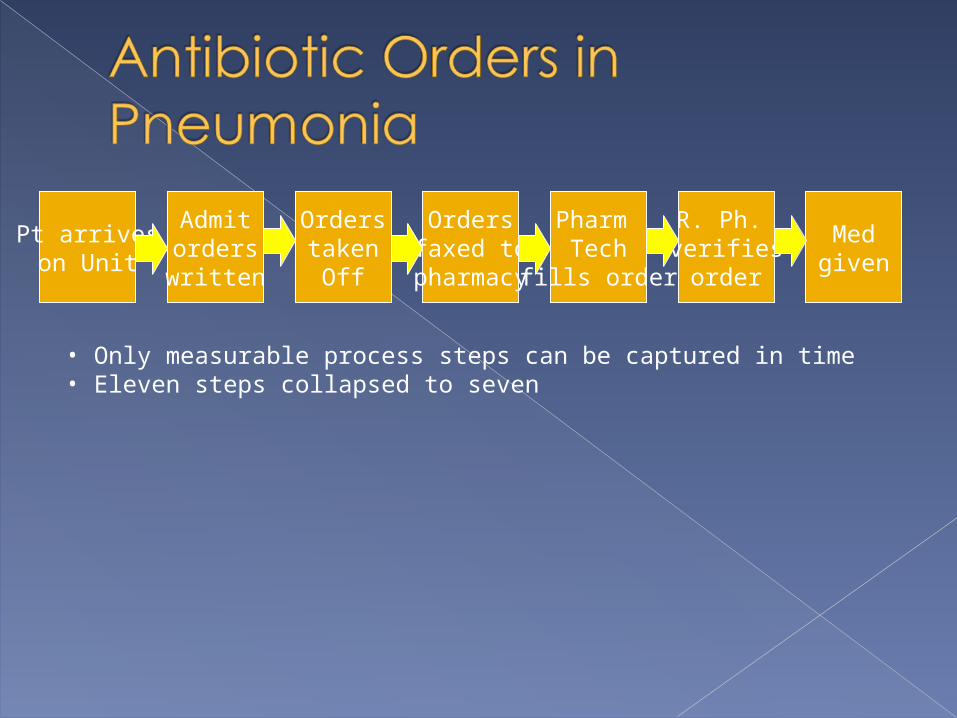
Pt arriveson Unit
Admitorderswritten
OrderstakenOff
Ordersfaxed to
pharmacy
R. Ph. verifiesorder
Pharm Tech
fills order
Medgiven
• Only measurable process steps can be captured in time• Eleven steps collapsed to seven
Study the patients represented on the flow chart attached.› Where are the areas of greatest delay?› Is any variability in practice noted?› From this information, does the pharmacy appear
to be the area where intervention is needed to shorten the time to antibiotic administration?
› Do you see any evidence of variation in care that might be contributing to the delays?
› What would you consider the most productive areas for intervention?
Mapping out a flow chart may allow to you identify problem areas within the process you are trying to improve.
Within each problem focus area, you will need to dig deeper to understand the cause of the problem.





























