Embed Size (px)
Citation preview
+Community-Level Systems Change In OHIO:The Autism Diagnosis Education Project
John C. Duby, MD,Director, Division of Developmental-Behavioral PediatricsAkron Children’s HospitalProfessor of PediatricsNortheast Ohio Medical [email protected]

LocalPeople
LocalSolutions
Autism DiagnosisEducation PilotProject
LocalSituations
June 2007: ADEPP Objectives• Heighten public awareness of early signs
of autism• Improve access to developmental
screening• Improve coordination of medical
diagnosis• Enhance access to evidence-based
services
+
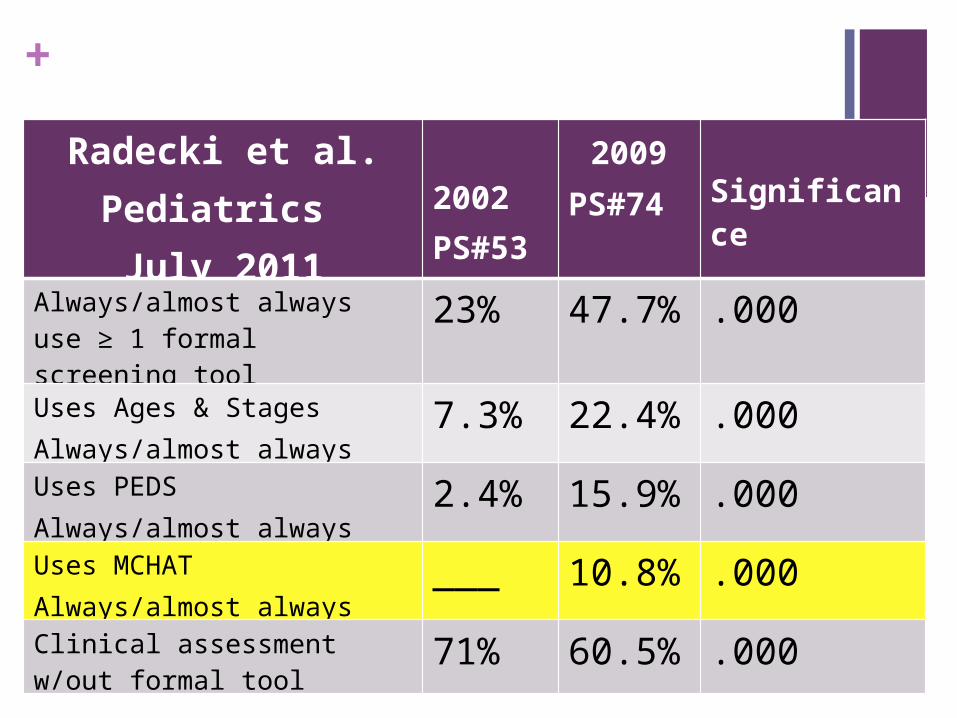
Radecki et al.Pediatrics July 2011
2002 PS#53
2009 PS#74
Significance
Always/almost always use ≥ 1 formal screening tool
23% 47.7% .000
Uses Ages & StagesAlways/almost always
7.3% 22.4% .000
Uses PEDSAlways/almost always
2.4% 15.9% .000
Uses MCHATAlways/almost always
___ 10.8% .000
Clinical assessment w/out formal tool
71% 60.5% .000

+ Ohio Chapter AAP Recommendations
A system of continuous developmental care that includes
emphasis on all aspects of surveillance at every well visit, and use of select standardized screening tools at certain visits.
Approved July 24, 2009

+Surveillance for Autism
Behavior 8 months
12 months
18 months 24 months
Eye Contact X X X
Turning to Name Call
X X
Imitation X
Pointing X X X
Gestures-Waving X X X
Pretend Play X X
Showing Behaviors
X
Fail Criteria
Fail 2/2
Fail 3/4
Fail 3/4 Fail 3/5
Barbaro, J. and Dissanayake, C. Prospective Identification of Autism Spectrum Disorders in Infancy and Toddlerhood Using Developmental Surveillance: The Social Attention and Communication Study. Journal of Developmental & Behavioral Pediatrics. 31(5):376-385, June 2010.
Positive Predictive Value 81%

Behavior Strategy
Eye Contact Has the child spontaneously made eye contact with you? If not interact with the child to elicit eye contact.
Turning to Name Call
Call the child’s name. Does he turn to look at you? Be sure not already looking at you!
Imitation Get the child’s attention. Clap your hands or smack your lips in front of the child. Does he imitate you?( Brush/comb?)
Pointing Get an object. Show it to the child and say” this is…” then put it across the room where it can be seen, and say “Where is …?” Does the child point to the object and look at your face?
Gestures-Waving Elicit the social routine of waving bye-bye. Does she wave back?
Pretend Play Give the child a toy cup and pot, a spoon, or a phone. Ask him to pour and drink, or feed a teddy, or make a phone call.
Showing Behaviors
PARENT REPORT: Does the child try to communicate with the parent in a SOCIAL manner? Not just to request food or an object.

Recommended Use of Standardized Screening Tools
Age Recommended Tool
9 months PEDS or ASQ:3
12 months ASQ:SE
18 months PEDS or ASQ:3
24 months M-CHAT with M-CHAT Follow-up Interview for those who fail
30 months PEDS or ASQ:3
Approved July 24, 2009
Ohio Chapter AAP Recommendations

Recommended Use of Standardized Screening Tools
Age Recommended Tool
36 months ASQ:SE
48 months PEDS or ASQ:3
60 months PEDS or ASQ:3 or Pediatric Symptom Checklist
Annually age 6-18
Pediatric Symptom Checklist
Annually age 11-18
Pediatric Symptom Checklist and/or Pediatric Symptom Checklist Youth Self Report
Approved July 24, 2009
Ohio Chapter AAP Recommendations
+
At this stage, on the basis of scientific principles and the available evidence, we
believe that we do not have enough sound
At this stage, on the basis of scientific principles and the available evidence, we
believe that we do not have enough sound evidence to support the
implementation of a routine communitywide screening program for
ASDs. Ongoing research is certainly needed to assess the effectiveness and acceptability of screening programs for
ASDs.

+The 7 Questions Has the Effectiveness of the Screening Program (for That
Condition) Been Demonstrated in a Randomized Trial? NO NO
Are There Efficacious Treatments for the PrimaryDisorder and/or Efficacious Preventive Maneuvers? Not really YES, if we look at the broad role of early intervention
Does the Current Burden of Suffering Warrant Screening? YES YES
Is a Good Screening Test Available? NO There will never be a perfect screening test We need to consider screening as part of a system of care

+The 7 Questions
Will the Screening Program Reach a High Proportion of the Persons for Whom It Was Intended? YES, if integrated into well child care YES, if integrated into well child care
Can the Health Care System Cope With the Screening Program? Maybe/Maybe Not YES
Will Those With Positive Screen Results Comply With Subsequent Advice and Interventions? Nobody Knows YES



Modified Checklist for Autism in Toddlers (M-CHAT)
23 yes-no questions Measures social reciprocity, language, some motor
18 months to 4 years of age Detects ASD, language impairment, cognitive disabilities
Available in over 20 languages
http://www2.gsu.edu/~psydlr/Diana_L._Robins,_Ph.D..html
M-CHAT and Autism screening
Failing score if 2 or more critical items or any 3 items are failed
2 page scoring guideTakes 5 minutes to complete, 1 to score
Autism screen recommended by AAP Autism Expert Panel for use at 18 and 24 month well-child visit

Screening for autism in older and younger toddlers withthe Modified Checklist for Autism in ToddlersPandhy et al. Autism, 2008
Comparisons of PPP for ASD between age groups show that it is lowest for the younger/low-risk toddlers (0.28), those below the age of 24 months screened routinely at a well-child visit
PPP was significantly lower than the older/low-risk toddlers (0.61).
For children already identified to be at some developmental risk, PPP (0.79 for younger children and 0.74 for older children)


24

M-CHAT Follow-up Interview
Ask the follow up questions for the failed itemsIncreases positive predictive value to 0.74

Laura

xxx
xx
x

Laura

xx
xx

+ CADLC Wave 2009
+Take Away Messages
When the doctor is worried, she is almost always right!
BUT, clinical impression alone is not quite good enough.
Comprehensive surveillance and periodic use of parent report screening tools appears judicious.
Repeated observations are better than single.
Screening tools should not be used in isolation.
Change is happening!






![What Brecht did for theater [sic] was to heighten the ... · 194 What Brecht did for theater [sic] was to heighten the spectator’s participation, but in an intellectual way, whereas](https://img.pdfslide.net/doc/110x75/5c13d3c509d3f224238d0b69/what-brecht-did-for-theater-sic-was-to-heighten-the-194-what-brecht-did.jpg)