Embed Size (px)
Citation preview
Management of Rh alloimmunization
CDE (Rhesus) System• Includes c, C, D, e, E
• D negativity defined as absence of D antigen
Antibodies Associated with
• Anti-c, Anti-D, Anti-E, and Anti-Kell
• Anti-D-immunoglobulin prophylaxis reduced the hemolytic disease caused by anti-D, but not the others
Minor RBC Antigens causes hemolyisis
• Kell is most common of minor
• Responsible for 10% of cases of severe antibody-mediated anemia
**Transfuse women with Kell(-) blood**
Inert Antibodies
• Antigens such as A, P, Le (a), M, I, IH, and Sd (a) are innocuous
• Mostly are IgM
• Lewis antibodies is the commonest one detected
Sensitization rate
• 16 percent without prophylaxis
• 2 percent with routine postpartum administration
• 0.1 percent with routine antenatal administration

Causes of Rh isoimmunization
• Delivery
• Induced abortion
• Spontaneous abortion
• Ectopic pregnancy
• Partial molar pregnancy
• Chorionic villus sampling
• Cordocentesis
• Amniocentesis • External cephalic version• Abruptio placenta • Antenatal hemorrhage • Maternal abdominal trauma • Spontaneous• Needles• Blood and blood product
Clinical Management Routine booking blood group
&Antibodies screenRh –v Ab –v Determine father’s RhBC status if -v No risk
If the father is +ve for-D-antigen, fetus is at RISK
- Repeat Antibodies screen at 28 weeks for Rh-ve women prior to receiving Anti-D immunoglobulin
-Determine father’s RBC antigen status and zygosity
Clinical Management If Antibody screen is +ve, identify
antibody type• Identify the risk factors for
alloimmunization (past pregnancies, transfusions, shared needles)
Clinical Management • Obtain antibody titer from the
mother if the past history is not significant for an affected pregnancy.
**Titers less reliable after a sensitized pregnancy**
Consider invasive testing at titer of 1:16 or greater by indirect Coombs
Clinical Management • If Antibodies titer remains below
critical titer- invasive testing is not indicated and the patient can be followed up by serial Antibodies titter
• Serial titers before 18-20 weeks not necessary
If Antibodies titer is above the critical level or the past history is positive regardless of the antibodies titer - invasive testing is indicated
Clinical Management • Amniocentesis for amniocytes at
15 weeks by (PCR) to determine fetal blood type if father is heterozygous.
• Free fetal DNA in maternal circulation.
Fetal antigenic determination
Amniocentesis, CVS, cordocentesis samples can be usedto determine fetal antigen status by DNA typing
100% accuracy in 390 samplesBennett et al. 1993
Molecular analysis of maternal plasma: fetal DNA for RhD100% accuracy in 45 fetuses second/third trimester
Lo et al. N Engl J Med 1998;339:1734-8.
PCR from cell free DNA in maternal serum100% accuracy in 137 fetuses (including 21 female fetuses)
Finning et al. Transfusion 2002;42:1079-85.
Possible utility in embryo selection for sensitized mothers
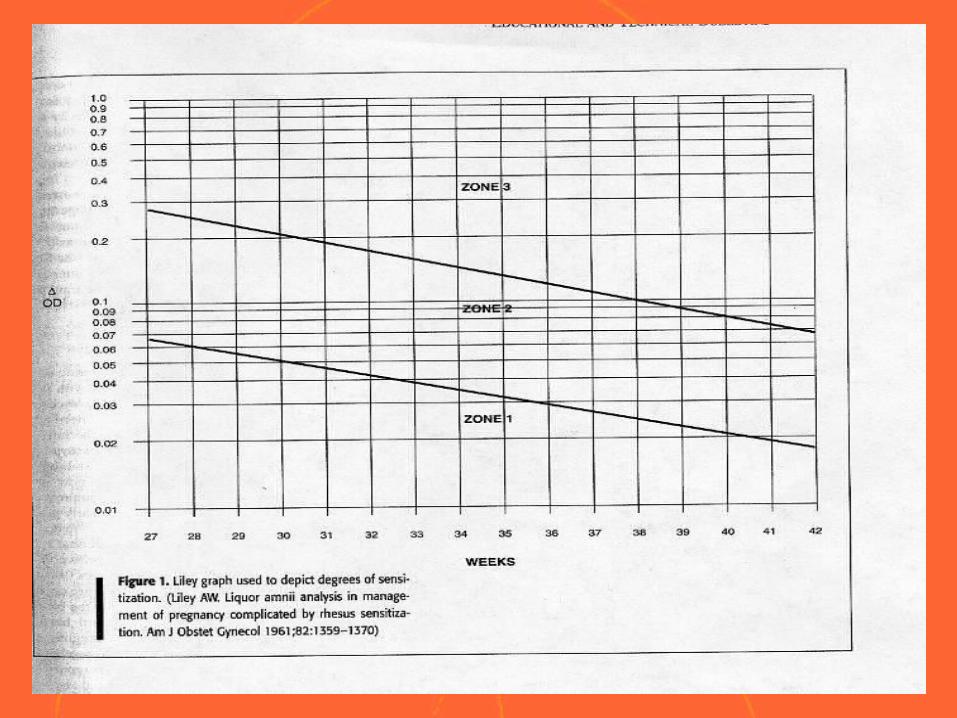
Clinical Management • Serial amnio to measure delta
OD450 and plot values on Liley or Queenan graph
Delta OD450• Spectral analysis of amniotic fluid
at 450 nm proposed in 1961 by Liley- measures change in OD
• Measures the level of bilirubin and predicts severity of hemolytic disease after 27 weeks
• Delivery or intrauterine transfusion if delta OD450 falls into zone III or upper zone II
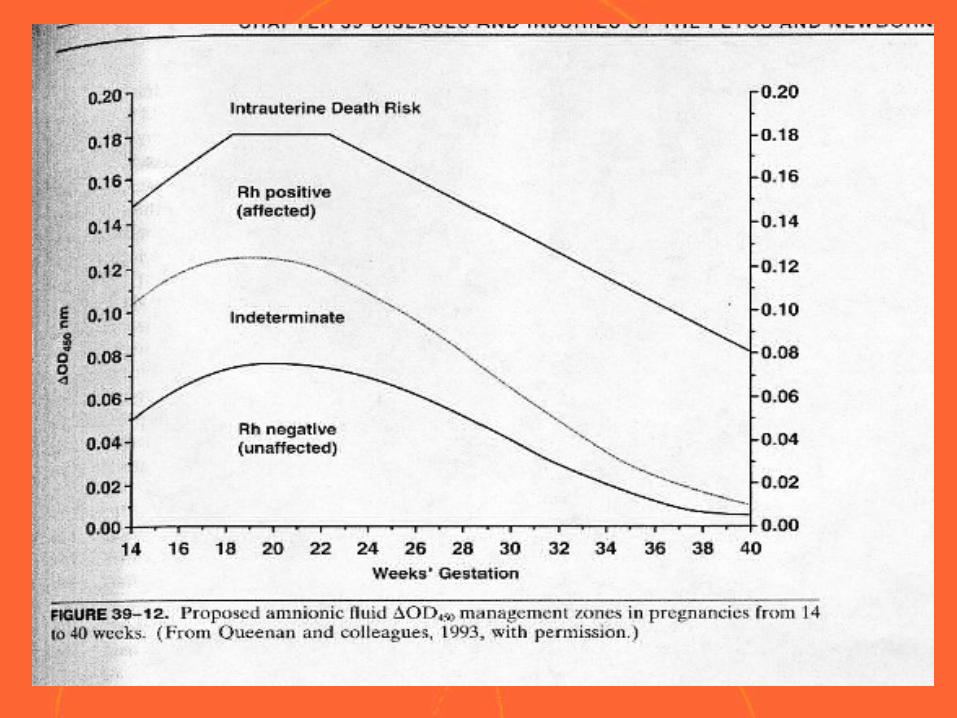
Queenan Curve• Proposed another method of using
delta OD450
• Suggested four zones and extended the gestational age to 14 weeks
Limitations of Amniocentesis
May give a falsely elevated bilirubin level in presence of mec or blood
May be low after exposure to light or in Kell alloimmunization
Cordocentesis
• Gold standard for detection of fetal anemia
• Complications!• 2.7% total risk of fetal loss• Reserved for patients with increased
MCA-PSV or delta OD450
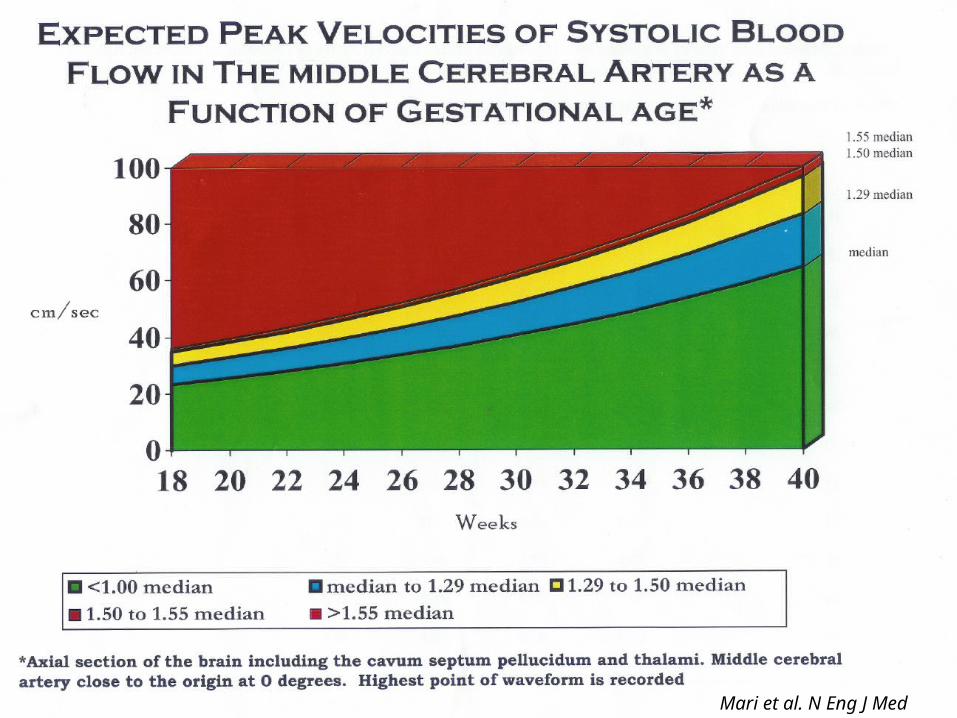
MCA-PSV• Velocity of blood flow in brain
increased with anemia 1. Increased cardiac output
2. Vasodilatation in the brain 3. Decreased blood viscosity
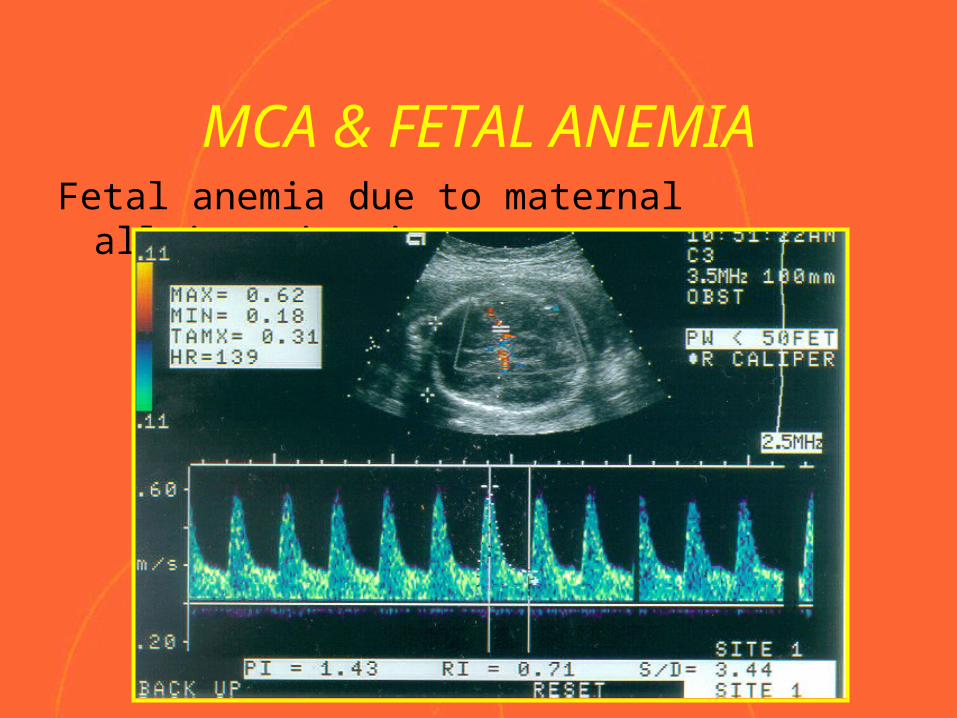
MCA & FETAL ANEMIA
The MCA PSV correlated well with hematocrit and hemoglobin concentrations and is useful for predicting the severity of fetal anemia
(Mari G. 1995)
The MCA PSV increases in fetuses with anemia (Roberts AB. 2001)
Bahauddin Sallout
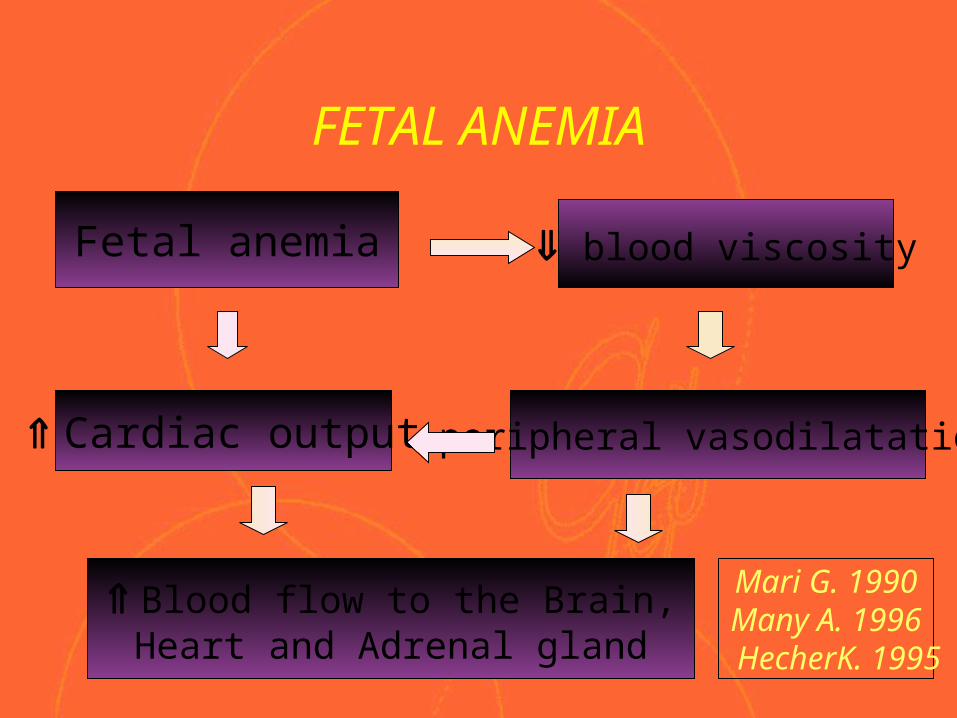
FETAL ANEMIA
Fetal anemia
Cardiac output
blood viscosity
Blood flow to the Brain, Heart and Adrenal gland
peripheral vasodilatation
Mari G. 1990Many A. 1996
HecherK. 1995
Correct Technique for MCA Doppler
• Fetus resting
• Circle of Willis imaged in axial image using color Doppler
• Entire length of MCA
• Close to origin of internal carotid artery
Bahauddin Sallout 30
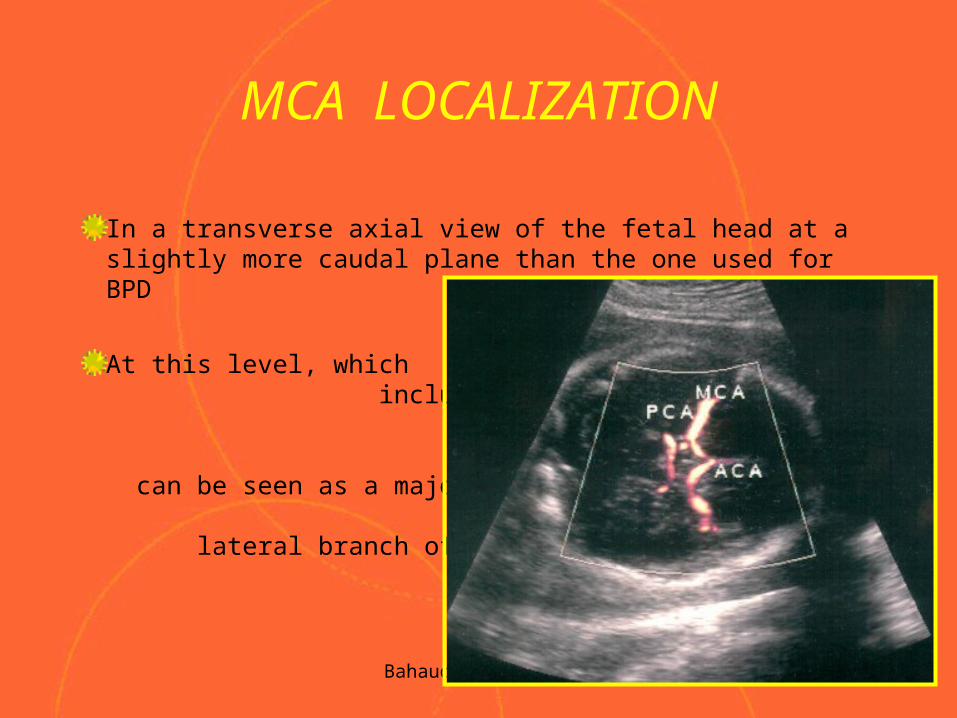
MCA LOCALIZATION
In a transverse axial view of the fetal head at a slightly more caudal plane than the one used for BPD
At this level, which include the cerebral peduncles, the MCA can be seen as a major lateral branch of the
circle of Willis
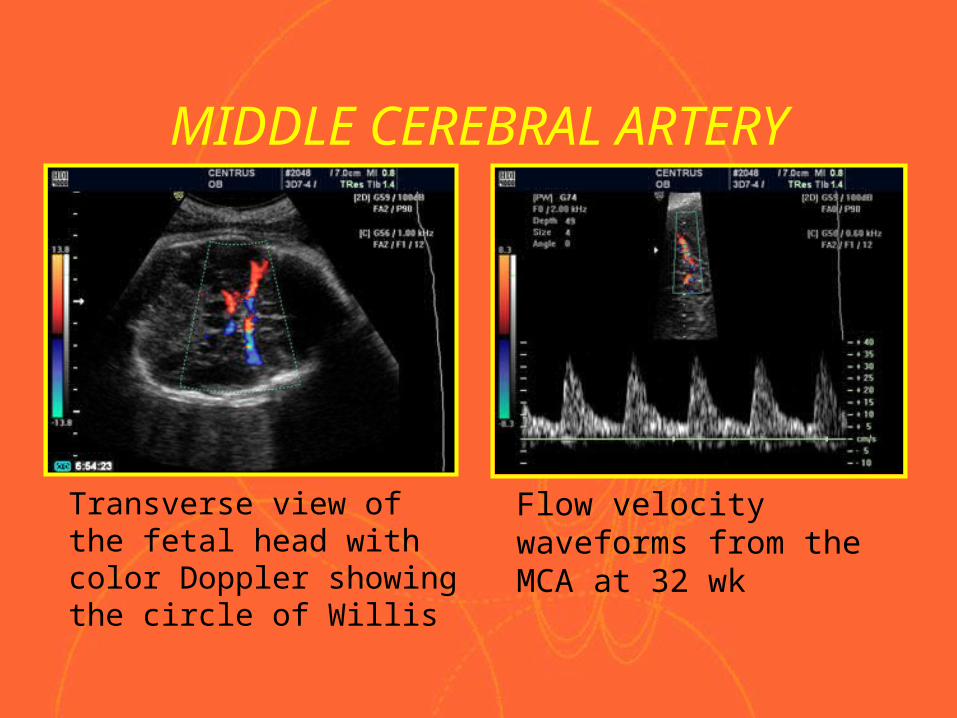
MIDDLE CEREBRAL ARTERY
Transverse view of the fetal head with color Doppler showing the circle of Willis
Flow velocity waveforms from the MCA at 32 wk
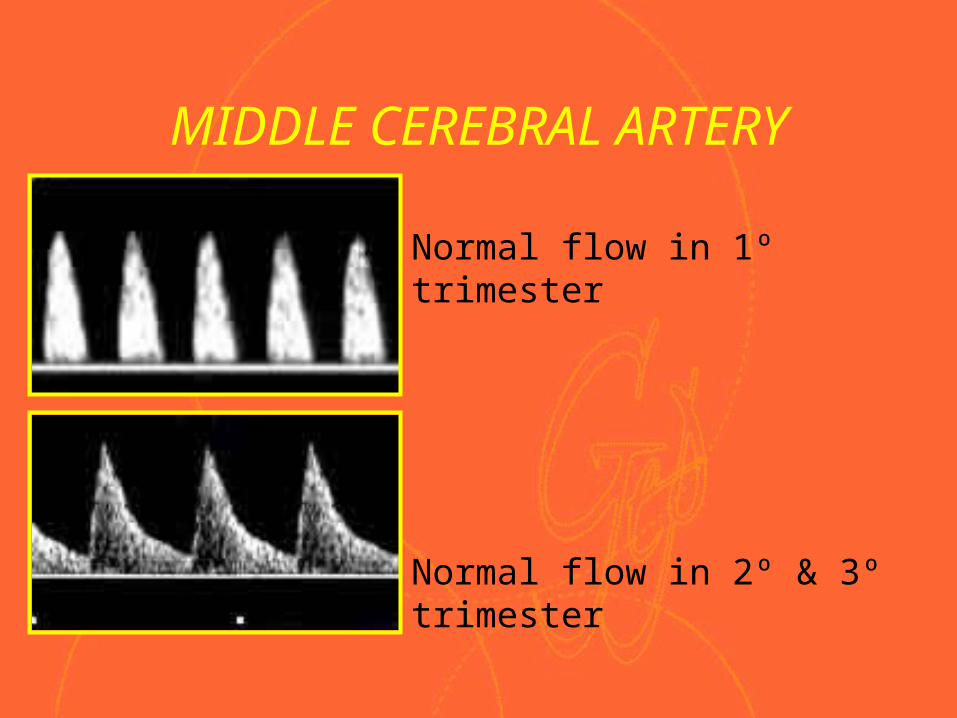
MIDDLE CEREBRAL ARTERY
• Normal flow in 1º trimester
• Normal flow in 2º & 3º trimester
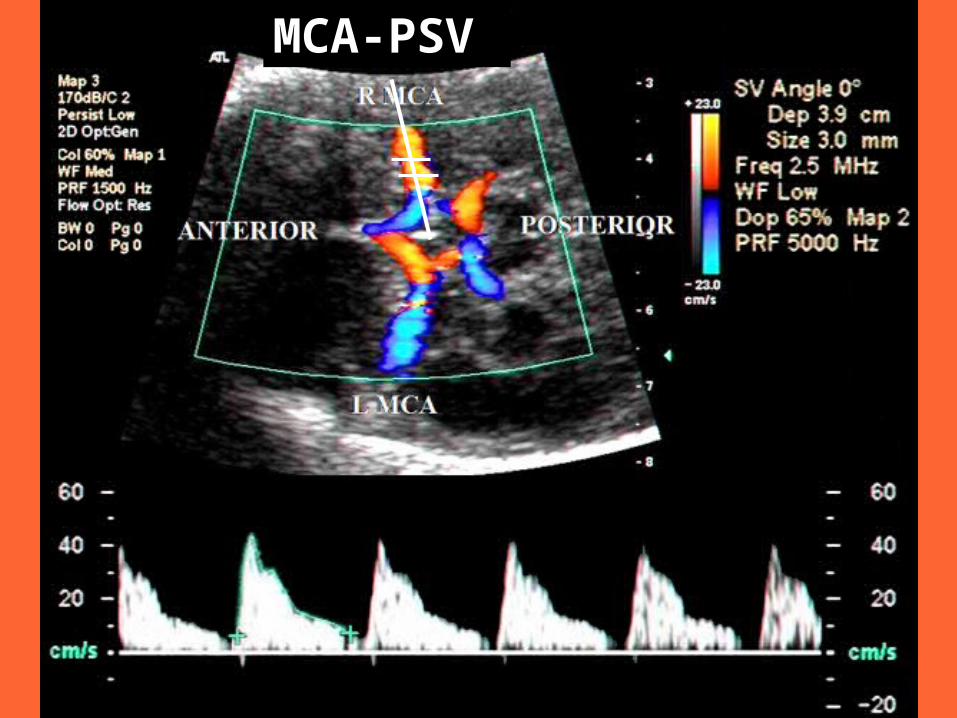
MCA-PSV
Bahauddin Sallout
MCA & FETAL ANEMIAFetal anemia due to maternal alloimmunization
Bahauddin Sallout
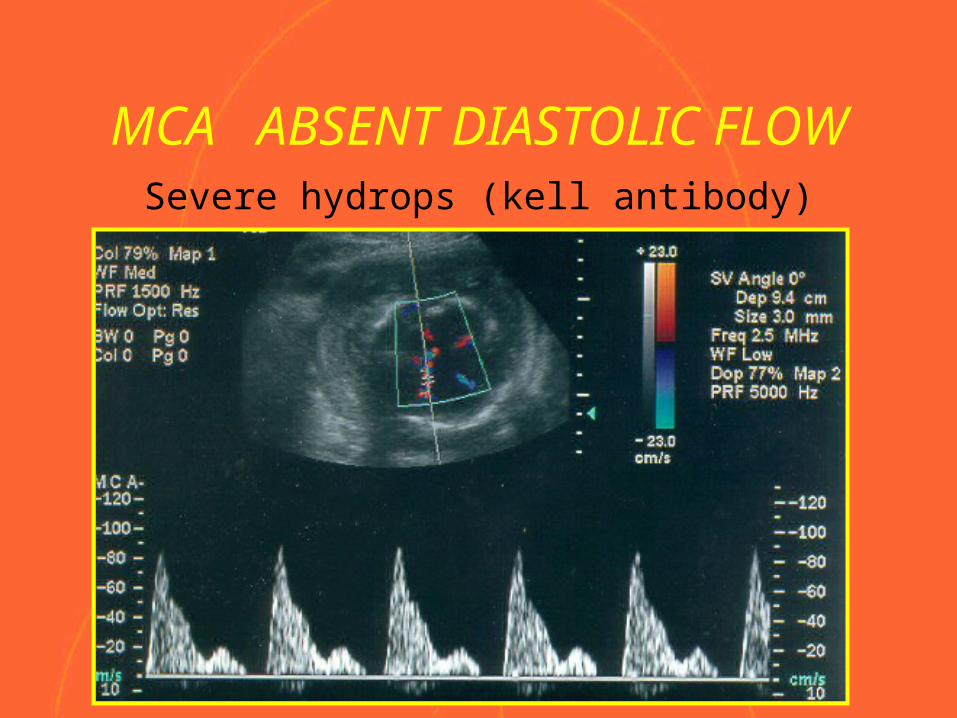
MCA ABSENT DIASTOLIC FLOWSevere hydrops (kell antibody)
Rh Alloimmunization management
If using MCA-PSV, and initial is less than 1.5 MoM, weekly testing
Cordocentesis or delivery depends on the gestational age once the MCA-PSV reaches 1.5 MoM
Mari et al. N Eng J Med 2000
Advantages of MCA-PSV
• Non-invasive
• Mother not put at risk for worsening alloimmunization
• Can be used with all antibodies other than RhD, including anti-Kell antibodies
Disadvantages of MCA-PSV
• Need skill
• Done weekly
• Accuracy decreases after 35 weeks
• False +ve results 12 percent
Initial prospective study of 16 fetuses: 14 anti-D, 2 anti-c
Mari et al. Ultrasound Obstet Gynecol 1995;5:400-5.
Since then several prospective and retrospective studies: over 200 additional casesRbc alloimmunization and parvovirus B19
1-Scott et al. Prenat Diagn 1998;18:1143-8.2-Teixeira et al. Ultrasound Obstet Gynecol 2000;15:205-
8.3-Delle Chiaie et al. Ultrasound Obstet Gynecol
2001;18:232-6.4-Mari et al. N Eng J Med 2000;342:9-14.5-Zimmermann et al. Br J Obstet Gynecol 2002;109:746-
52.6-Mari et al. Ultrasound Obstet Gynecol 2002;99:589-93.
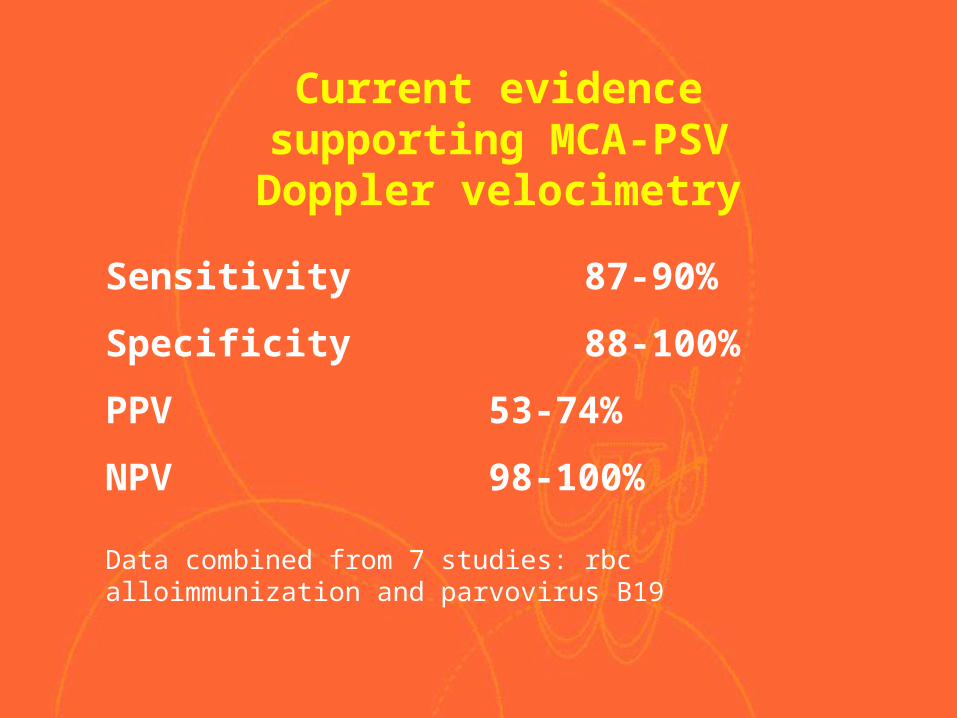
Current evidence supporting MCA-PSV Doppler velocimetry
Current evidence supporting MCA-PSV Doppler velocimetry
Sensitivity 87-90%
Specificity 88-100%
PPV 53-74%
NPV 98-100%
Data combined from 7 studies: rbc alloimmunization and parvovirus B19
4 Comparative Studies
N = 28 Nishie EN, et al. Am J Obstet Gynecol 2003;188:214-9
N = 28 Pereira L et al. Am J Obstet Gynecol 2003;189:1002-6
N = 38 Bullock ,et al. Ultrasound Obstet Gynecol 2005
N = 165 Oepkes D, et al. N Engl J Med 2006;355:156-64.
Prediction of fetal anemia by MCA-PSV Doppler compared to Amniocentesis
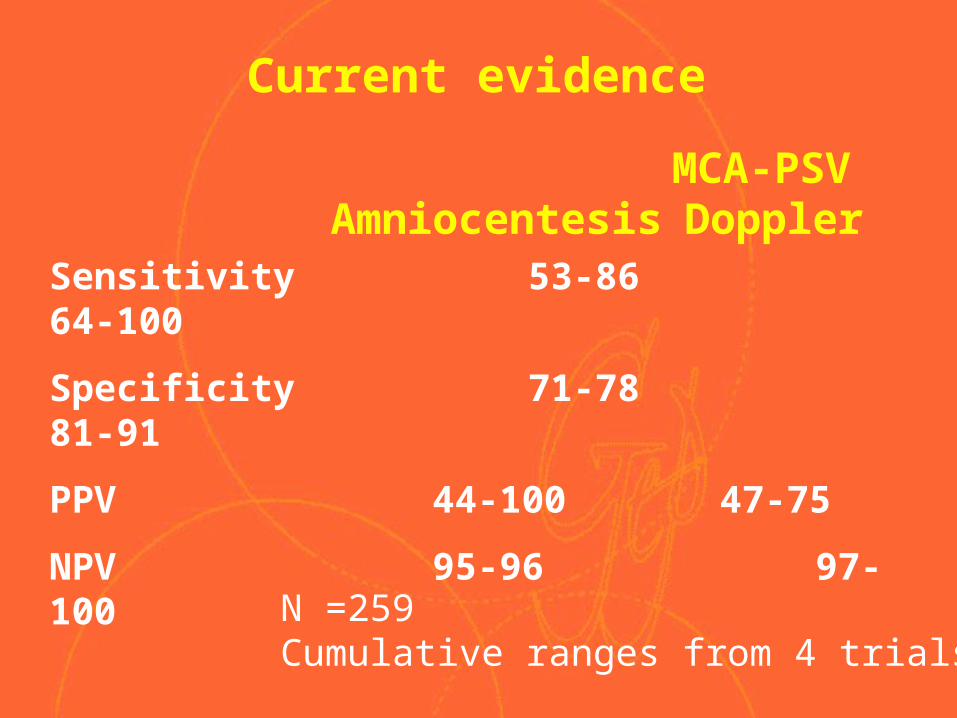
Current evidence
Sensitivity 53-86 64-100
Specificity 71-78 81-91
PPV 44-100 47-75
NPV 95-96 97-100
MCA-PSV Doppler Amniocentesis
N =259 Cumulative ranges from 4 trials
Conclusion
MCA-PSV accurately predicted moderate to severe fetal anemia
Compared to conventional management, MCA-PSV may have a better predictive accuracy for moderate or severe anemia in alloimmunization
Management by MCA-PSV may eliminate the need for amniocentesis and reduce the number of PUBS performed in alloimmunized pregnancies
14,000 cases of alloimmunization per year in the U.S.
Avoid 24,500 amniocenteses and 900 PUBS
Avoid 1 pregnancy loss/preterm delivery for every 100 patients; 142 nationwide per year
Avoid worsening sensitization from procedurerelated bleeding complications – TPH risk 2-10% following amniocentesis, 50% following PUBS
Potential Benefits of Management by MCA-PSV
Prevention of Alloimmunization
Doses of ani-D-immuonoglubuline for Rh-ve)
50 mcg dose protects against 2.5 ml of Rh (+) RBC’s
300 mcg dose protects against 15 ml of RBC’s or 30 ml of Rh (+) blood
20 mcg per ml RBC
Preventionstandard recommendations 300 mcg dose within 72 hrs of
delivery to unsensitized Rh (-) women (Rh positive infant) 13 days , 28 days
300 mcg at 28 weeks UNLESS father known to be Rh (-)
Repeat Antibody Screen before giving the prophylactic dose?
•At 28 weeks of gestation
•Spontaneous abortion, threatened abortion, induced abortion
•Ectopic pregnancy
•Invasive procedures: genetic amniocentesis; chorionic villus sampling; multi-fetal reduction; fetal blood sampling
•Hydatidiform mole
Indications for administration of anti-(D) immune globulin
• Fetal death in the second or third trimester• Blunt trauma to the abdomen• Antepartum hemorrhage in the second or third
trimester (eg, placenta previa or abruption)• External cephalic version
Prevention • Test for excessive fetal-maternal
hemorrhage after blunt trauma, abruption, cordocentesis, and bleeding assoc. with previa
• Kleihauer Betke

Thank you