Embed Size (px)
Citation preview

www.arquivosonline.com.br Sociedade Brasileira de Cardiologia • ISSN-0066-782X • Volume 102, Nº 2, February 2014
Special ArticleI Brazilian Position Paper on Prehypertension, White Coat
Hypertension and Masked Hypertension: Diagnosis and Management
Original ArticlesValue of Coronary Artery Calcium Score to Predict Severity or
Complexity of Coronary Artery Disease
Myocardial Revascularization in Dyalitic Patients: In-Hospital Period
Evaluation
Coronary Flow Velocity Reserve during Dobutamine Stress
Echocardiography
Study of Risk Factors Associated with Peripheral Arteriopathy in
Japanese-Brazilians from Bauru (SP)
Time of Exercise as Indicator of Quality Control in Ergometry Services
Influence of Term of Exposure to High-Fat Diet-Induced Obesity on
Myocardial Collagen Type I and III
Gene Expression Related to Oxidative Stress in the Heart of Mice after
Intestinal Ischemia
High Blood Pressure in Children and its Correlation with Three
Definitions of Obesity in Childhood
Acute Effects of Continuous Positive Airway Pressure on Pulse
Pressure in Chronic Heart Failure
Hypertrophic response of the Association of Thyroid Hormone and
Exercise in the Heart of Rats
Review ArticleQuality of Life and Congenital Heart Disease in Childhood and
Adolescence
Letter to the EditorChronotropic Incompetence in Diabetic Elderly on Echocardiography
Trastuzumab Cardiotoxicity in Patients with Breast Cancer
Eletronic Pages
Anatomopathological SessionCase 1/2014 - Syncope Due to Cardiogenic Shock in a 25-year-old
Male Patient
Case ReportClinically Manifested Myocarditis in Acute Rheumatic Fever
Point of ViewDetailing the Writing of Scientific Manuscripts: 25-30 Paragraphs
Figura 2 – Photomicrography of the left ventricle of a mouse in the Ischemia and Reperfusion Group (GIR). Please note smaller volume and pyknotic nuclei (yellow cell) of cardiomyocytes in the edge of the cell (white cell). Swollen cells and cardiac fibers in a disorganized direction. (HE 400x). Pág. 171

Arquivos Brasileiros de Cardiologia - Volume 102, Nº 2, February 2014
REVISTA DA SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Publicada desde 1948
Contents
Special Article
I Brazilian Position Paper on Prehypertension, White Coat Hypertension and Masked Hypertension: Diagnosis and ManagementBrazilian Society of Cardiology Arterial Hypertension Departmenta..................................................................................................................................................................página 110
Original Articles
Coronary Angioplasty with and without Stent
Value of Coronary Artery Calcium Score to Predict Severity or Complexity of Coronary Artery DiseaseTayyar Gökdeniz, Ezgi Kalaycıoğlu, Ahmet Çağrı Aykan, Faruk Boyacı, Turhan Turan, İlker Gül, Gökhan Çavuşoğlu, İhsan Dursun..................................................................................................................................................................página 120
Heart Surgery - Adults
Myocardial Revascularization in Dyalitic Patients: In-Hospital Period EvaluationMatheus Miranda, Nelson Américo Hossne Jr., João Nelson Rodrigues Branco, Guilherme Flora Vargas, José Honório de Almeida Palma da Fonseca, José Osmar Medina de Abreu Pestana, Yara Juliano, Enio Buffolo..................................................................................................................................................................página 128
Echocardiography (Adults)
Coronary Flow Velocity Reserve during Dobutamine Stress EchocardiographyJosé Sebastião de Abreu, José Wellington Oliveira Lima, Tereza Cristina Pinheiro Diógenes, Jordana Magalhães Siqueira, Nayara Lima Pimentel, Pedro Sabino Gomes Neto, Marília Esther Benevides de Abreu, José Nogueira Paes Júnior..................................................................................................................................................................página 134
Epidemiology
Study of Risk Factors Associated with Peripheral Arteriopathy in Japanese-Brazilians from Bauru (SP)Luciana Garofolo, Sandra Roberta G. Ferreira, Fausto Miranda Junior..................................................................................................................................................................página 143
Exercise Stress Testing
Time of Exercise as Indicator of Quality Control in Ergometry ServicesRomeu Sergio Meneghelo, Samira Saady Morhy, Paola Zucchi..................................................................................................................................................................página 151
Genetics/Molecular Biology
Influence of Term of Exposure to High-Fat Diet-Induced Obesity on Myocardial Collagen Type I and IIIDanielle Cristina Tomaz da Silva, Ana Paula Lima-Leopoldo, André Soares Leopoldo, Dijon Henrique Salomé de Campos, André Ferreira do Nascimento, Sílvio Assis de Oliveira Junior, Carlos Roberto Padovani, Antonio Carlos Cicogna..................................................................................................................................................................página 157

Arquivos Brasileiros de Cardiologia - Volume 102, Nº 2, February 2014
Gene Expression Related to Oxidative Stress in the Heart of Mice after Intestinal IschemiaFrederico Somaio Neto, Adauto Tsutomu Ikejiri, Paulo Roberto Bertoletto, José Carlos Bertoletto Chaves, Roberto Teruya, Djalma José Fagundes, Murched Omar Taha..................................................................................................................................................................página 165
Systemic Hypertension
High Blood Pressure in Children and its Correlation with Three Definitions of Obesity in ChildhoodLeonardo Iezzi de Moraes, Thaís Coutinho Nicola, Julyanna Silva Araújo de Jesus, Eduardo Roberty Badiani Alves, Nayara Paula Bernurdes Giovaninni, Daniele Gasparini Marcato, Jéssica Dutra Sampaio, Jeanne Teixeira Bessa Fuly, Everlayny Fiorot Costalonga..................................................................................................................................................................página 175
Heart Failure
Acute Effects of Continuous Positive Airway Pressure on Pulse Pressure in Chronic Heart FailureMônica Quintão, Sérgio Chermont, Luana Marchese, Lúcia Brandão, Sabrina Pereira Bernardez, Evandro Tinoco Mesquita, Nazareth de Novaes Rocha, Antônio Claudio L. Nóbrega..................................................................................................................................................................página 181
Ventricular Function/Cardiac Remodeling
Hypertrophic response of the Association of Thyroid Hormone and Exercise in the Heart of RatsFernanda Rodrigues de Souza, Elmiro Santos Resende, Leandro Lopes, Alexandre Gonçalves, Rafaella Chagas, Thiago Fidale, Poliana Rodrigues..................................................................................................................................................................página 187
Review Article
Quality of Life and Congenital Heart Disease in Childhood and AdolescenceJuliana Bertoletti, Giovana Caroline Marx, Sérgio Pedro Hattge Júnior, Lucia Campos Pellanda..................................................................................................................................................................página 192
Letter to the Editor
Chronotropic Incompetence in Diabetic Elderly on EchocardiographyEduardo Maffini da Rosa, Roberta Casanova Wilhelms, Rodrigo Borges Brandão..................................................................................................................................................................página 199
Trastuzumab Cardiotoxicity in Patients with Breast CancerAguinaldo Figueiredo Freitas Jr. e Salvador Rassi..................................................................................................................................................................página 200

Arquivos Brasileiros de Cardiologia - Volume 102, Nº 2, February 2014
Eletronic Pages
Anatomopathological Session
Case 1/2014 - Syncope Due to Cardiogenic Shock in a 25-year-old Male PatientTiago Rodrigues Politi and Paulo Gutierrez............................................................................................................................................................... página e11
Case Report
Clinically Manifested Myocarditis in Acute Rheumatic FeverJosé L. Xavier Jr., Alexandre de Matos Soeiro, Antonio S. S. A. Lopes, Guilherme S. Spina, Carlos V. Serrano Jr., Múcio T. Oliveira Jr................................................................................................................................................................ página e17
Viewpoint
Detailing the Writing of Scientific Manuscripts: 25-30 ParagraphsClaudio Gil Soares de Araújo............................................................................................................................................................... página e21
* Indicate manuscripts only in the electronic version. To view them, visit: http://www.arquivosonline.com.br/2014/english/10202/edicaoatual.asp
Editorial BoardBrasilAdib D. Jatene (SP)Alexandre A. C. Abizaid (SP)Alfredo José Mansur (SP)Álvaro Avezum (SP)Amanda G. M. R. Sousa (SP)André Labrunie (PR)Andrei Sposito (DF)Angelo A. V. de Paola (SP)Antonio Augusto Barbosa Lopes (SP)Antonio Carlos C. Carvalho (SP)Antônio Carlos Palandri Chagas (SP)Antonio Carlos Pereira Barretto (SP)Antonio Cláudio L. Nóbrega (RJ)Antonio de Padua Mansur (SP)Ari Timerman (SP)Armênio Costa Guimarães (BA)Ayrton Klier Péres (DF)Ayrton Pires Brandão (RJ)Barbara M. Ianni (SP)Beatriz Matsubara (SP)Braulio Luna Filho (SP)Brivaldo Markman Filho (PE)Bruce B. Duncan (RS)Bruno Caramelli (SP)Carisi A. Polanczyk (RS)Carlos Alberto Pastore (SP)Carlos Eduardo Negrão (SP)Carlos Eduardo Rochitte (SP)Carlos Eduardo Suaide Silva (SP)Carlos Vicente Serrano Júnior (SP)Celso Amodeo (SP)Charles Mady (SP)Claudio Gil Soares de Araujo (RJ)Cleonice Carvalho C. Mota (MG)Dalton Valentim Vassallo (ES)Décio Mion Jr (SP)Denilson Campos de Albuquerque (RJ)Dikran Armaganijan (SP)Djair Brindeiro Filho (PE)Domingo M. Braile (SP)Edmar Atik (SP)Edson Stefanini (SP)Elias Knobel (SP)Eliudem Galvão Lima (ES)Emilio Hideyuki Moriguchi (RS)Enio Buffolo (SP)
Eulógio E. Martinez Fº (SP)Evandro Tinoco Mesquita (RJ)Expedito E. Ribeiro da Silva (SP)Fábio Sândoli de Brito Jr. (SP)Fábio Vilas-Boas (BA)Fernando A. P. Morcerf (RJ)Fernando Bacal (SP)Flávio D. Fuchs (RS)Francisco Antonio Helfenstein Fonseca (SP)Francisco Laurindo (SP)Francisco Manes Albanesi Fº (RJ)Gilmar Reis (MG)Gilson Soares Feitosa (BA)Ínes Lessa (BA)Iran Castro (RS)Ivan G. Maia (RJ)Ivo Nesralla (RS)Jarbas Jakson Dinkhuysen (SP)João Pimenta (SP)Jorge Ilha Guimarães (RS)Jorge Pinto Ribeiro (RS)José A. Marin-Neto (SP)José Antonio Franchini Ramires (SP)José Augusto Soares Barreto Filho (SE)José Carlos Nicolau (SP)José Geraldo de Castro Amino (RJ)José Lázaro de Andrade (SP)José Péricles Esteves (BA)José Teles Mendonça (SE)Leopoldo Soares Piegas (SP)Luís Eduardo Rohde (RS)Luiz A. Machado César (SP)Luiz Alberto Piva e Mattos (SP)Lurildo Saraiva (PE)Marcelo C. Bertolami (SP)Marcia Melo Barbosa (MG)Marco Antônio Mota Gomes (AL)Marcus V. Bolívar Malachias (MG)Maria Cecilia Solimene (SP)Mario S. S. de Azeredo Coutinho (SC)Maurício I. Scanavacca (SP)Mauricio Wajngarten (SP)Max Grinberg (SP)Michel Batlouni (SP)Nabil Ghorayeb (SP)Nadine O. Clausell (RS)Nelson Souza e Silva (RJ)
Orlando Campos Filho (SP)Otávio Rizzi Coelho (SP)Otoni Moreira Gomes (MG)Paulo A. Lotufo (SP)Paulo Cesar B. V. Jardim (GO)Paulo J. F. Tucci (SP)Paulo J. Moffa (SP)Paulo R. A. Caramori (RS)Paulo R. F. Rossi (PR)Paulo Roberto S. Brofman (PR)Paulo Zielinsky (RS)Protásio Lemos da Luz (SP)Renato A. K. Kalil (RS)Roberto A. Franken (SP)Roberto Bassan (RJ)Ronaldo da Rocha Loures Bueno (PR)Sandra da Silva Mattos (PE)Sergio Almeida de Oliveira (SP)Sérgio Emanuel Kaiser (RJ)Sergio G. Rassi (GO)Sérgio Salles Xavier (RJ)Sergio Timerman (SP)Silvia H. G. Lage (SP)Valmir Fontes (SP)Vera D. Aiello (SP)Walkiria S. Avila (SP)William Azem Chalela (SP)Wilson A. Oliveira Jr (PE)Wilson Mathias Jr (SP)
ExteriorAdelino F. Leite-Moreira (Portugal)Alan Maisel (Estados Unidos)Aldo P. Maggioni (Itália)Cândida Fonseca (Portugal)Fausto Pinto (Portugal)Hugo Grancelli (Argentina)James de Lemos (Estados Unidos)João A. Lima (Estados Unidos)John G. F. Cleland (Inglaterra)Maria Pilar Tornos (Espanha)Pedro Brugada (Bélgica)Peter A. McCullough (Estados Unidos)Peter Libby (Estados Unidos)Piero Anversa (Itália)
Scientific Director Luiz Alberto Piva e Mattos
chief eDitor Luiz Felipe P. Moreira
ASSociAteD eDitorS
clinicAl cArDiology José Augusto Barreto-Filho
SurgicAl cArDiology Paulo Roberto B. Evora
interventioniSt cArDiology Pedro A. Lemos
PeDiAtric/congenitAl cArDiology Antonio Augusto Lopes
ArrhythmiAS/PAcemAker Mauricio Scanavacca
non-invASive DiAgnoStic methoDS Carlos E. Rochitte
BASic or exPerimentAl reSeArch Leonardo A. M. Zornoff
ePiDemiology/StAtiSticS Lucia Campos Pellanda
ArteriAl hyPertenSion Paulo Cesar B. V. Jardim
ergometricS, exerciSe AnD cArDiAc rehABilitAtion Ricardo Stein
firSt eDitor (1948-1953) † Jairo Ramos
A JOURNAL OF SOCIEDADE BRASILEIRA DE CARDIOLOGIA - Published since 1948www.arquivosonline.com.br
PresidentAngelo Amato V. de Paola
Vice-PresidentSergio Tavares Montenegro
Financial DirectorJacob Atié
Scientific DirectorMaria da Consolação Vieira Moreira
Administrative DirectorEmilio Cesar Zilli
Assistance Quality DirectorPedro Ferreira de Albuquerque
Communication DirectorMaurício Batista Nunes
Information Technology DirectorJosé Carlos Moura Jorge
Government Liaison DirectorLuiz César Nazário Scala
Director of State and Regional AffairsAbrahão Afiune Neto
Cardiovascular Health Promotion Director - SBC/FuncorCarlos Costa Magalhães
Department DirectorEspecializados - Jorge Eduardo Assef
Research DirectorFernanda Marciano Consolim Colombo
Chief Editor of the Brazilian Archives of CardiologyLuiz Felipe P. Moreira
Special Advisor to the PresidencyFábio Sândoli de Brito
Adjunct Coordination
SBC Newsletter EditorNabil Ghorayeb e Fernando Antonio Lucchese
Continuing Education Coordination Estêvão Lanna Figueiredo
Norms and Guidelines Coordination Luiz Carlos Bodanese
Governmental Integration Coordination Edna Maria Marques de Oliveira
Regional Integration Coordination José Luis Aziz
Presidents of State and Regional Brazilian Societies of Cardiology
SBC/AL - Carlos Alberto Ramos Macias
SBC/AM - Simão Gonçalves Maduro
SBC/BA - Mario de Seixas Rocha
SBC/CE - Ana Lucia de Sá Leitão Ramos
SBC/CO - Frederico Somaio Neto
SBC/DF - Wagner Pires de Oliveira Junior
SBC/ES - Marcio Augusto Silva
SBC/GO - Thiago de Souza Veiga Jardim
SBC/MA - Nilton Santana de Oliveira
SBC/MG - Odilon Gariglio Alvarenga de Freitas
SBC/MS - Mércule Pedro Paulista Cavalcante
SBC/MT - Julio César De Oliveira
SBC/NNE - Jose Itamar Abreu Costa
SBC/PA - Luiz Alberto Rolla Maneschy
SBC/PB - Catarina Vasconcelos Cavalcanti
SBC/PE - Helman Campos Martins
SBC/PI - João Francisco de Sousa
SBC/PR - Osni Moreira Filho
SBC/RJ - Olga Ferreira de Souza
SBC/RN - Rui Alberto de Faria Filho
SBC/RS - Carisi Anne Polanczyk
SBC/SC - Marcos Venício Garcia Joaquim
SBC/SE - Fabio Serra Silveira
SBC/SP - Francisco Antonio Helfenstein Fonseca
SBC/TO - Hueverson Junqueira Neves
Sociedade Brasileira de Cardiologia
Presidents of the Specialized Departaments and Study Groups
SBC/DA - Hermes Toros Xavier (SP)
SBC/DCC - Evandro Tinoco Mesquita (RJ)
SBC/DCM - Orlando Otavio de Medeiros (PE)
SBC/DCC/CP - Estela Suzana Kleiman Horowitz (RS)
SBC/DECAGE - Abrahão Afiune Neto (GO)
SBC/DEIC - João David de Souza Neto (CE)
SBC/DERC - Pedro Ferreira de Albuquerque (AL)
SBC/DFCVR - José Carlos Dorsa Vieira Pontes (MS)
SBC/DHA - Weimar Kunz Sebba Barroso de Souza (GO)
SBC/DIC - Jorge Eduardo Assef (SP)
SBC/SBCCV - Walter José Gomes (SP)
SBC/SBHCI - Marcelo Antonio Cartaxo Queiroga Lopes (PB)
SBC/SOBRAC - Adalberto Menezes Lorga Filho (SP)
SBC/DCC/GAPO - Daniela Calderaro (SP)
SBC/DCC/GECETI - João Fernando Monteiro Ferreira (SP)
SBC/DCC/GEECABE - Luis Claudio Lemos Correia (BA)
SBC/DCC/GEECG - Carlos Alberto Pastore (SP)
SBC/DCP/GECIP - Angela Maria Pontes Bandeira de Oliveira (PE)
SBC/DERC/GECESP - Daniel Jogaib Daher (SP)
SBC/DERC/GECN - José Roberto Nolasco de Araújo (AL)

Arquivos Brasileiros de Cardiologia
Affiliated at the Brazilian Medical Association
Volume 102, Nº 2, February 2014Indexing: ISI (Thomson Scientific), Cumulated Index Medicus (NLM), SCOPUS,
MEDLINE, EMBASE, LILACS, SciELO, PubMed
The ads showed in this issue are of the sole responsibility of advertisers, as well as the concepts expressed in signed articles are of the sole responsibility of their
authors and do not necessarily reflect the views of SBC.
This material is for exclusive distribution to the medical profession. The Brazilian Archives of Cardiology are not responsible for unauthorized access to its contents and
that is not in agreement with the determination in compliance with the Collegiate Board Resolution (DRC) N. 96/08 of the National Sanitary Surveillance Agency
(ANVISA), which updates the technical regulation on Drug Publicity, Advertising, Promotion and Information. According to Article 27 of the insignia, "the advertisement or publicity of prescription drugs should be restricted solely and exclusively to health
professionals qualified to prescribe or dispense such products (...)".
To ensure universal access, the scientific content of the journal is still available for full and free access to all interested parties at:
www.arquivosonline.com.br.
SUPPORT
Commercial Department
Phone: (11) 3411-5500
E-mail: [email protected]
Editorial Production
SBC - Internal Publication Department
Graphic Design and DiagrammingSBC - Internal Design Department
PrintStamppa
Circulation1.500
Address: Av. Marechal Câmara, 160 - 3º andar - Sala 330 20020-907 • Centro • Rio de Janeiro, RJ • Brasil
Phone.: (21) 3478-2700
E-mail: [email protected]
www.arquivosonline.com.br
SciELO: www.scielo.br
Special Article
I Brazilian Position Paper on Prehypertension, White Coat Hypertension and Masked Hypertension: Diagnosis and ManagementBrazilian Society of Cardiology Arterial Hypertension Department
KeywordsHypertension / therapy; Prehypertension / prevention &
control; White Coat Hypertension; Masked Hypertension.
Arq Bras Cardiol. 2014; 102(2):110-119
Mailing Address: Paulo César B. Veiga Jardim •Rua 115-F, nº 135, Setor Sul. CEP 74085-300, Goiânia, GO - BrazilE-mail: [email protected], [email protected] received November 13, 2013; revised manuscript December 03, 2013; accepted December 03, 2013.
DOI: 10.5935/abc.20140011
IntroductionArterial blood pressure (BP) is a very useful variable in
clinical practice. Its measurement is simple, inexpensive and easy; it is worth noting that BP should be accurately obtained, following the recommendations of the VI Brazilian Guidelines on Hypertension (DBH VI)1.
Office BP measurement is the central parameter for the diagnosis, treatment and follow-up of systemic arterial hypertension (SAH), being directly, continuously and independently related to the risk of fatal and non-fatal cardiovascular (CV) events1-3.
Thus, the consideration of BP values closer to the upper limits of normality, the so-called prehypertension (PH)2, and intervention on those values have been emphasized over the last decade, because PH represents an important opportunity to prevent established SAH, contributing to reduce the associated CV risk.
Repeated BP measurement at the office allows the diagnosis of hypertension and normotension. To better assess BP behavior, there are methods that analyze BP by using a higher number of measurements, minimizing interferences of the environment, situation and observer. Those alternatives are as follows: 24-hour ambulatory BP monitoring (ABPM); and dwelling BP measurement [home BP monitoring (HBPM) and BP self-measurement (BPSM)]. Based on those methods, two other BP classifications were adopted: white coat hypertension (WCH) and masked hypertension (MH)1,3-5 (Figure 1).
Epidemiological and clinical studies on those conditions are still limited; however, they deserve attention because of their higher CV risk as compared with normotension6,7.
This document represents the position of the Brazilian Society of Cardiology Arterial Hypertension Department (DHA/SBC) on the diagnosis and non-drug and drug therapy for PH, WCH and MH, aiming at contributing to a better clinical practice.
Prehypertension
EpidemiologyThe term PH was described in 2003 on the American
Guideline on Arterial Hypertension1 that emphasized the
importance of adopting strict preventive measures in the presence of PH, considering that individuals with such characteristics have a higher incidence of SAH in the following years and greater CV risk than those with optimal BP (lower than 120/80 mm Hg)2,3. A study has shown that among prehypertensive individuals aged 40-49 years, the incidence of hypertension in the following years is 80%8.
In the PURE (Prospective Urban and Rural Epidemiological) Study, assessing 153,996 individuals in 17 countries, PH prevalence was 36.8%, greater than the SAH rate (34.3%). Data on the North American adult population have shown a 40% prevalence9.
Prehypertension is known to be often associated with other CV risk factors, such as obesity, insulin resistance, diabetes mellitus, dyslipidemia and other metabolic syndrome phenotypes, resulting in early vascular abnormalities and progression to atherosclerosis10.
Diagnosis and clinical strategies of identificationPrehypertension has been defined as office measurements
of systolic blood pressure (SBP) between 120 and 139 mm Hg and/or of diastolic blood pressure (DBP) between 80 and 89 mmHg2. Its identification depends on regular BP measurement, which is recommended to be performed at least once a year.
The diagnosis of PH is based on BP measurement at the office, but that diagnosis can certainly be improved with 24-hour ABPM and/or HBPM. Such forms of out-of-office BP assessment have the advantage of providing a much higher number of measurements, outside sites where BP is usually taken, representing a more reliable BP registry4,5. It is important to identify the presence of MH among prehypertensive individuals.
There is evidence that the increase in left ventricular mass (LVM) in prehypertensive individuals is a strong predictor of the development of SAH within four years, regardless of other metabolic and anthropometric factors associated. The increase in LVM might be associated with a higher daily hemodynamic load that could be detected by measuring BP at the office. Increased BP variability, lack of its drop during sleep or sustained and prolonged increased BP during wakefulness could explain higher LVM values in prehypertensive individuals. In addition, PH progression to hypertension has been associated with increased arterial stiffness11,12.
Prognostic valuePrehypertension is a precursor of SAH, associates with
other CV risk factors, and has greater CV morbidity and mortality6,13.
110
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
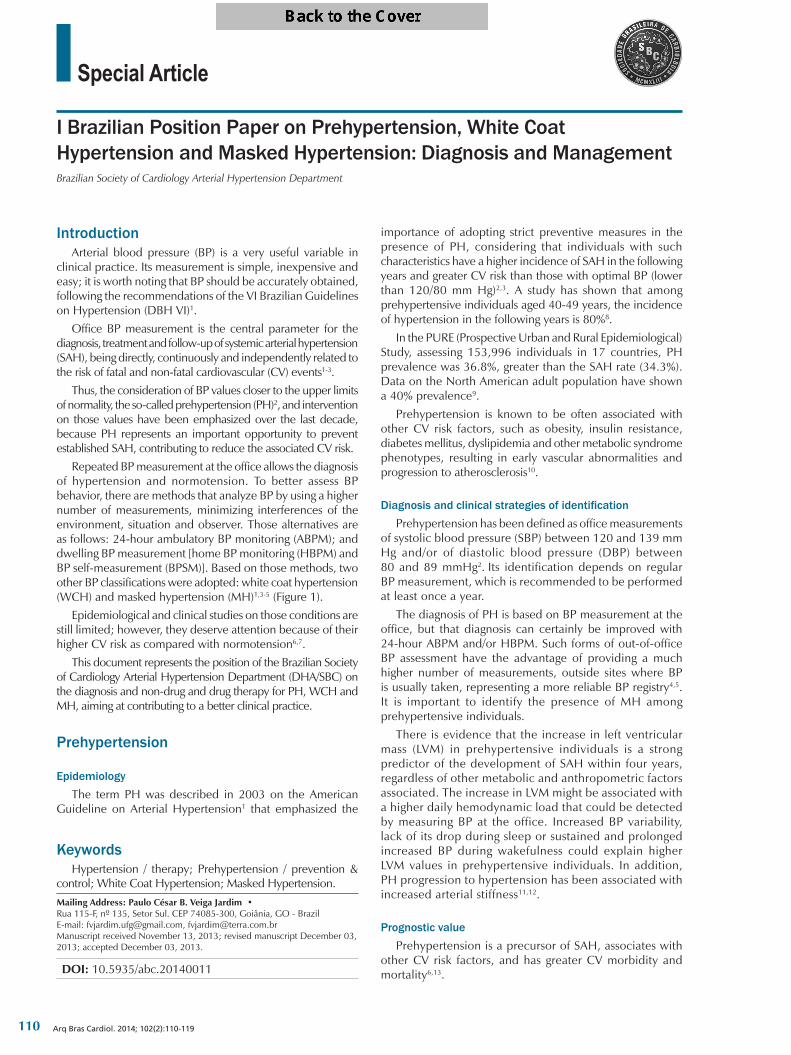
Figure 1 – Classification of blood pressure behavior considering office BP, ABPM and home BP measurements1. ABPM: ambulatory blood pressure monitoring; BP: blood pressure.
In the population assessed in the Framingham study, the following percentages of individuals younger than 65 years developed SAH within a four-year follow-up in the three BP strata considered normal: 5.3% of the individuals with optimal BP; 17.6% of those with normal BP; and 37.3% of those considered to have high-normal BP at the time. For individuals older than 65 years, those rates were 16%, 25.5% and 49.5%, respectively14. Data obtained from two British Health and Lifestyle Surveys conducted seven years apart have been used to form a subsample of 2,048 normotensive individuals, and have demonstrated a greater risk for developing SAH among those with higher BP levels, especially the younger ones15. Other studies have reported that individuals older than 45 years have a 56.4% progression rate to arterial hypertension in three years (56.9% for men and 55.9% for women)16.
A population-based study conducted in Brazil has reported that four out of five prehypertensive individuals aged 40-49 years developed SAH in ten years8.
Regarding the increased risk for CV events of patients with PH, data from longitudinal studies from the Framingham Heart Study have indicated that SBP levels between 130-139 mm Hg and DBP between 85-89 mm Hg are associated with a two-fold increase in the risk for CV diseases (CVD) as compared with 120/80 mmHg levels14. That association proved to be more significant in diabetic individuals and those with higher body mass index (BMI)17. Individuals with PH are more prone to acute myocardial infarction (AMI) or coronary artery disease (CAD) than those considered normotensive18. A Japanese study has reported a 45% increase in the risk of CV events in prehypertensive individuals as compared with normotensive ones, after adjusting for all other traditional risk factors19.
White coat hypertension
EpidemiologyThe prevalence of WCH varies because of the diversity
of the diagnostic criteria involving not only aspects related to BP measurement but also to the populations studied.
The mean overall prevalence of WCH, based on four population-based studies, was 13%, and reached 32% among hypertensives in those studies20. In the general population, those values range from 10% to 20%, being more common among children and the elderly, in the female sex, and in non-smokers21,22.
The prevalence of WCH is also related to office BP measurements, its percentage being 55% among stage 1 hypertensives, and only 10% among stage 3 hypertensives21. However, among individuals whose DBP at the office exceeds 105 mm Hg, WCH is an unlikely finding23. That phenomenon also occurs among hypertensives undergoing treatment, being called the white coat effect. Muxfeldt et al24 have assessed uncontrolled hypertensive patients on antihypertensive treatment, of whom more than 60% were on three or more drugs and 37% had the white coat effect. In the PAMELA (Pressione Arteriose Monitorate E Loro Associazioni) study, ongoing for ten years, 42.6% of the patients with metabolic syndrome and WCH at the first consultation developed sustained arterial hypertension25.
The greater the BMI, the higher the WCH prevalence. Helvaci et al26, studying the BP behavior of individuals assessed at check-up clinics, have reported the following WCH prevalences: 19.6% for individuals with IMC lower than 18.5 kg/m2; 35.6% for individuals with IMC between 18.5 and 24.9 kg/m2; and 68.4% for overweight individuals (IMC between 25 and 29.9 kg/m2)26.
The WCH frequency increases with age, and, among individuals older than 65 years, its prevalence usually ranges from 43% to 45%27.
In a follow-up period of up to 6.5 years, Verdecchia et al28 have reported a 37% risk of developing arterial hypertension in individuals with WCH. That percentage related to baseline values of ABPM rather than to office BP.
Diagnosis and clinical strategies of identificationThe diagnosis of WCH requires office and out-of-office BP
measurement, be it by use of ABPM or home measurements4. The thresholds recommended are those adopted at the most recent NICE29 and 2013 ESH/ESC3 guidelines, and ESH
111
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
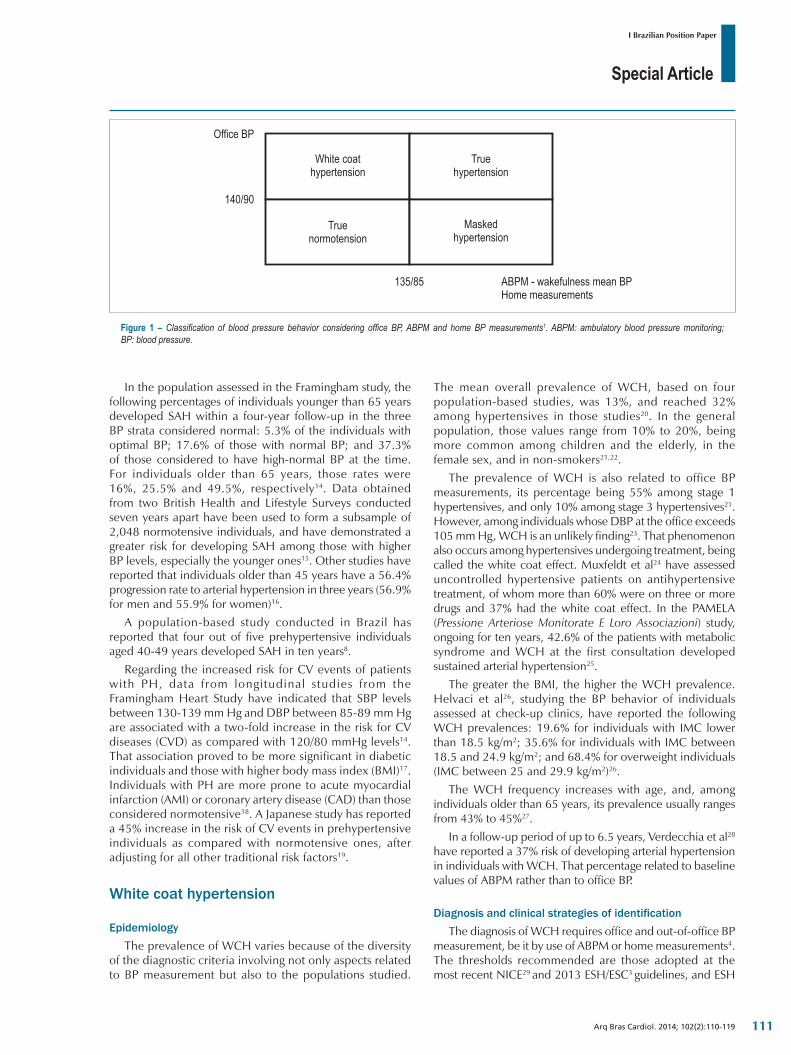
Figure 2 – Schematic representation of BP behavior at the office and on ABPM or home BP measurement for the diagnosis of white coat hypertension. ABPM: ambulatory blood pressure monitoring; HBPM: home blood pressure monitoring; BPSM: blood pressure self-measurement; SBP: systolic blood pressure; DBP: diastolic blood pressure.
Table 1 – Threshold of abnormality to diagnose hypertension on 24‑hour ABPM and home BP measurement
Out-of-office measurement SBP and/or DBP (mmHg)
ABPM
24-h mean ≥ 130/80
Wakefulness mean ≥ 135/85
Sleep mean ≥ 120/70
Home measurement ≥ 135/85
ABPM: ambulatory blood pressure monitoring; SBP: systolic blood pressure; DBP: diastolic blood pressure.
Position Paper on Ambulatory Blood Pressure Monitoring5, which maintain the values of the JNC 72 and 2003 and 2007 ESH/ESC30,31 guidelines, and were based on studies such as the IDACO (International Database on Ambulatory Blood Pressure monitoring in relation to Cardiovascular Outcomes Investigators)32 and Ohasama Study33 (table 1).
White coat hypertension is characterized as follows: 1) increased office BP levels (SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg); and 2) normal out-of-office BP levels (< 135/85 mmHg) measured on ABPM during wakefulness, or at home (HBPM or BPSM), as shown in table 1 and figures 1 and 2. The European Society of
Hypertension recommends that, on ABPM, the diagnosis of WCH requires normal mean values of 24-hour BP and of nocturnal BP5.
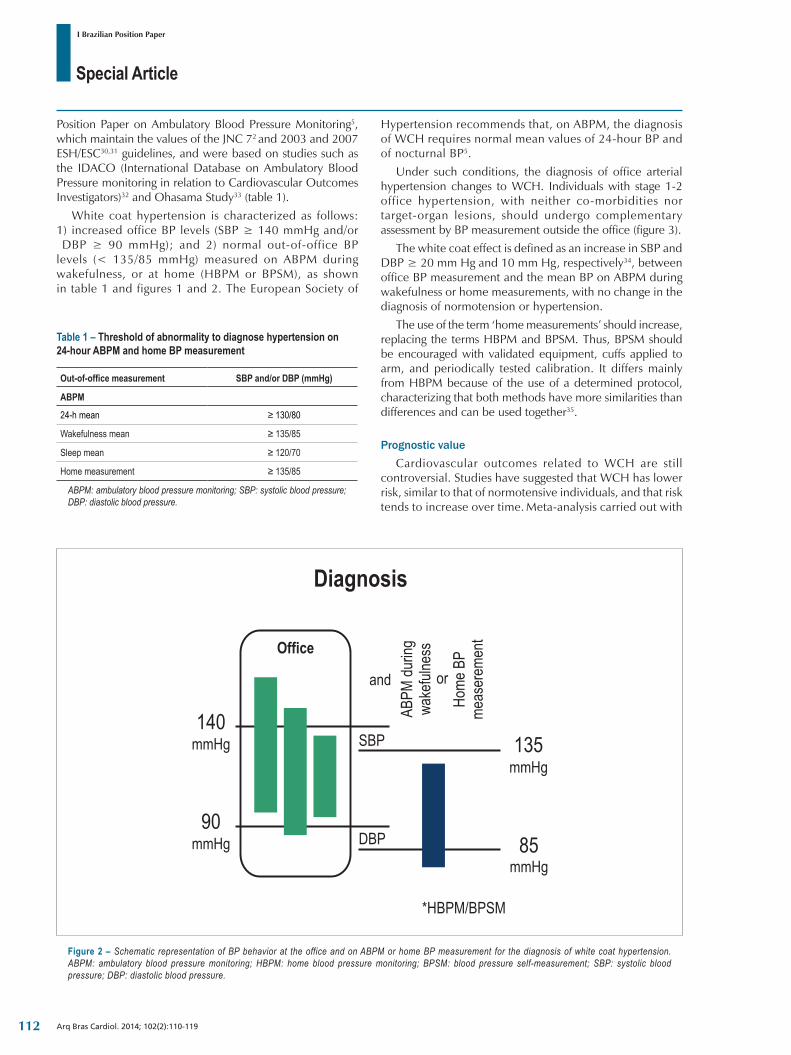
Under such conditions, the diagnosis of office arterial hypertension changes to WCH. Individuals with stage 1-2 office hypertension, with neither co-morbidities nor target-organ lesions, should undergo complementary assessment by BP measurement outside the office (figure 3).
The white coat effect is defined as an increase in SBP and DBP ≥ 20 mm Hg and 10 mm Hg, respectively34, between office BP measurement and the mean BP on ABPM during wakefulness or home measurements, with no change in the diagnosis of normotension or hypertension.
The use of the term ‘home measurements’ should increase, replacing the terms HBPM and BPSM. Thus, BPSM should be encouraged with validated equipment, cuffs applied to arm, and periodically tested calibration. It differs mainly from HBPM because of the use of a determined protocol, characterizing that both methods have more similarities than differences and can be used together35.
Prognostic valueCardiovascular outcomes related to WCH are still
controversial. Studies have suggested that WCH has lower risk, similar to that of normotensive individuals, and that risk tends to increase over time. Meta-analysis carried out with
112
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
Figure 3 – Flowchart for the identification of white coat hypertension. ABPM: ambulatory blood pressure monitoring; HBPM: home blood pressure monitoring; BPSM: blood pressure self-measurement.
7,030 individuals has evidenced the existence of increasing CV risk from normotension, to WCH, to MH, and finally, to hypertension20,36-39.
Regarding the risk of developing hypertension, the PAMELA study has shown that a significantly higher proportion of individuals previously diagnosed with WCH or MH, after ten years were diagnosed with sustained hypertension as compared with previously normotensive individuals25.
Masked hypertension
EpidemiologyMasked hypertension is characterized by normal BP
values at the office and abnormal out-of-office BP values, on either ambulatory or dwelling BP measurements (ABPM, HBPM or BPSM)40.
The prevalence of MH is estimated to range from 8% to 20% among adults with no treatment, and to be at least 50% among individuals on drug treatment41. A meta-analysis involving 28 studies has estimated a 16.8% MH prevalence in the general population. Among children, the estimated MH prevalence is 7%42. Higher MH prevalence has been observed when office BP is in the high-normal range41. Office BP within the normal range as compared to abnormal ambulatory values has been attributed, among other factors, to the "regression toward the mean" phenomenon40. Other factors have also correlated with MH30,40,43-48, as shown in Chart 1. In a study involving 3,400 treated hypertensives, the major factors associated with MH were overweight (1.38; 95% CI: 1.09-1.75) and regular alcohol consumption (OR, 1.37; 95% CI: 1.09-1.72)42. In another study, the risk for MH was higher among men than among women [relative risk (RR), 1.14; 95% CI: 1.01-1.28] and among smokers (RR, 1.16; 95% CI: 1.04-1.30)49. Another study has shown that women were less prone than men to have MH (OR, 0.39; 95% CI: 0.22- 0.68)47.
Classically, the presence of MH occurs among untreated individuals. Recently, the literature has emphasized the
occurrence of normal office BP and elevated out-of-office BP values in treated individuals. Lower levels of anxiety and the use of antihypertensive drugs only before the medical consultation, with a drug action peak at the time of medical examination, has also been listed as causing factors44,46,50.
Diagnosis and clinical strategies of identificationMasked hypertension refers to untreated patients
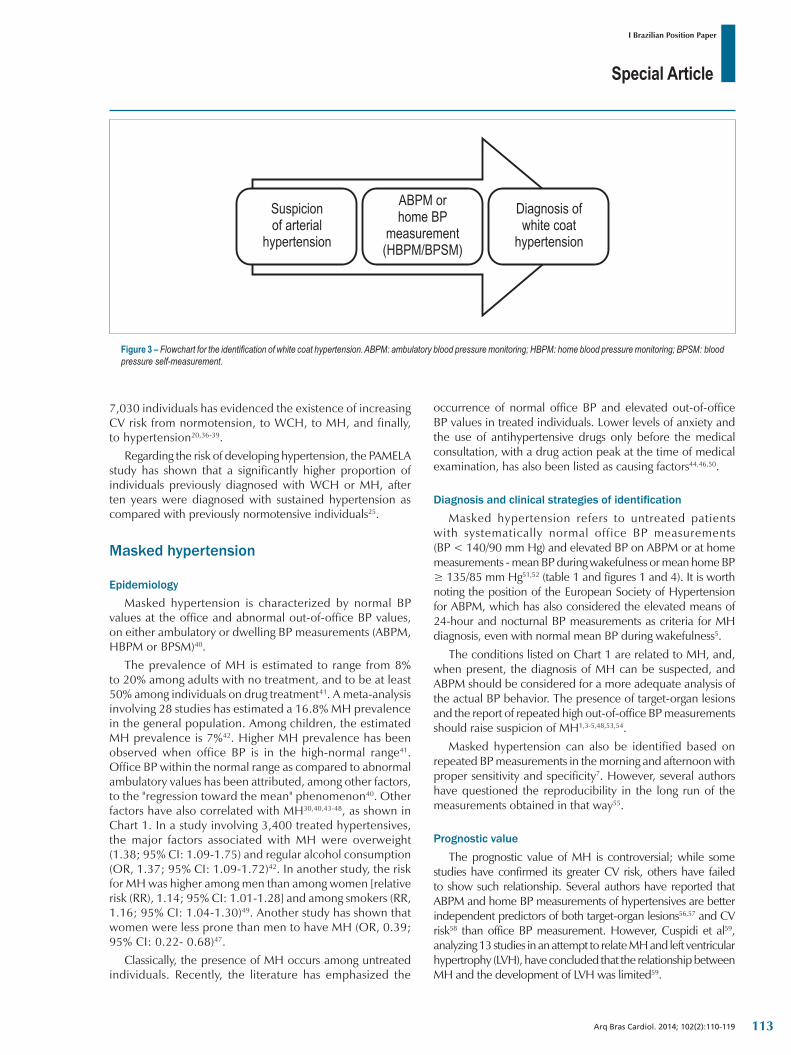
with systematically normal office BP measurements (BP < 140/90 mm Hg) and elevated BP on ABPM or at home measurements - mean BP during wakefulness or mean home BP ≥ 135/85 mm Hg51,52 (table 1 and figures 1 and 4). It is worth noting the position of the European Society of Hypertension for ABPM, which has also considered the elevated means of 24-hour and nocturnal BP measurements as criteria for MH diagnosis, even with normal mean BP during wakefulness5.
The conditions listed on Chart 1 are related to MH, and, when present, the diagnosis of MH can be suspected, and ABPM should be considered for a more adequate analysis of the actual BP behavior. The presence of target-organ lesions and the report of repeated high out-of-office BP measurements should raise suspicion of MH1,3-5,48,53,54.
Masked hypertension can also be identified based on repeated BP measurements in the morning and afternoon with proper sensitivity and specificity7. However, several authors have questioned the reproducibility in the long run of the measurements obtained in that way55.
Prognostic valueThe prognostic value of MH is controversial; while some
studies have confirmed its greater CV risk, others have failed to show such relationship. Several authors have reported that ABPM and home BP measurements of hypertensives are better independent predictors of both target-organ lesions56,57 and CV risk58 than office BP measurement. However, Cuspidi et al59, analyzing 13 studies in an attempt to relate MH and left ventricular hypertrophy (LVH), have concluded that the relationship between MH and the development of LVH was limited59.
113
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
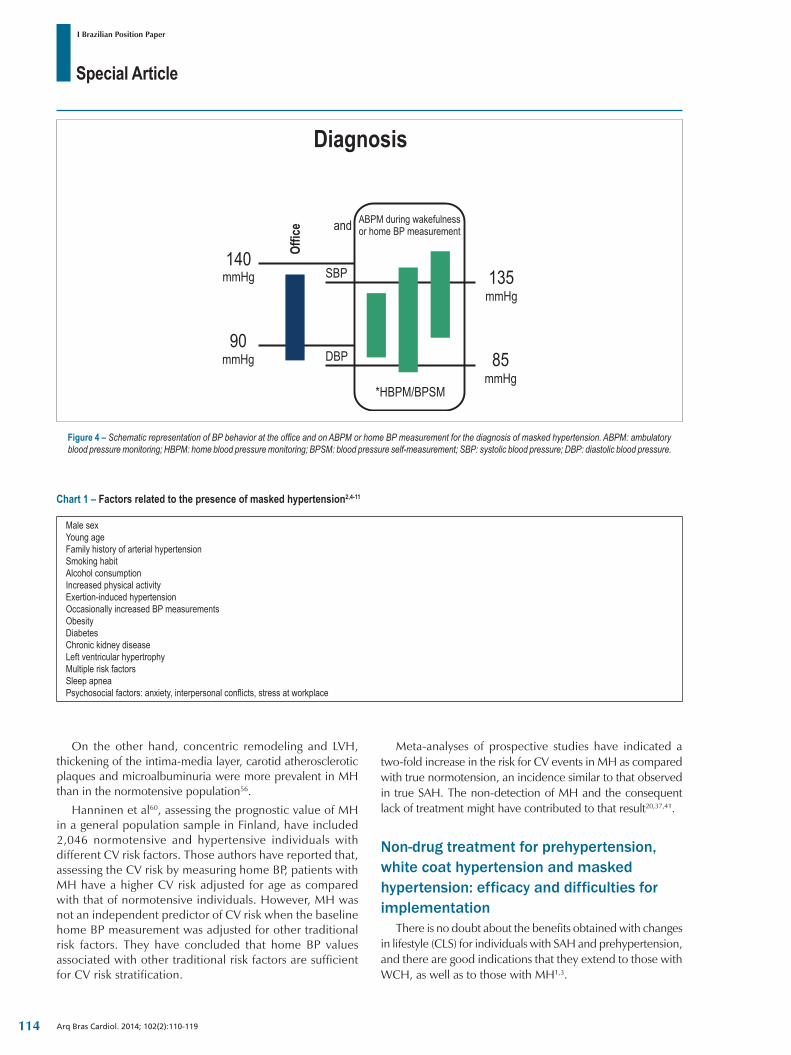
Figure 4 – Schematic representation of BP behavior at the office and on ABPM or home BP measurement for the diagnosis of masked hypertension. ABPM: ambulatory blood pressure monitoring; HBPM: home blood pressure monitoring; BPSM: blood pressure self-measurement; SBP: systolic blood pressure; DBP: diastolic blood pressure.
On the other hand, concentric remodeling and LVH, thickening of the intima-media layer, carotid atherosclerotic plaques and microalbuminuria were more prevalent in MH than in the normotensive population56.
Hanninen et al60, assessing the prognostic value of MH in a general population sample in Finland, have included 2,046 normotensive and hypertensive individuals with different CV risk factors. Those authors have reported that, assessing the CV risk by measuring home BP, patients with MH have a higher CV risk adjusted for age as compared with that of normotensive individuals. However, MH was not an independent predictor of CV risk when the baseline home BP measurement was adjusted for other traditional risk factors. They have concluded that home BP values associated with other traditional risk factors are sufficient for CV risk stratification.
Chart 1 – Factors related to the presence of masked hypertension2,4‑11
Male sexYoung ageFamily history of arterial hypertensionSmoking habitAlcohol consumptionIncreased physical activityExertion-induced hypertensionOccasionally increased BP measurementsObesityDiabetesChronic kidney diseaseLeft ventricular hypertrophyMultiple risk factors Sleep apneaPsychosocial factors: anxiety, interpersonal conflicts, stress at workplace
Meta-analyses of prospective studies have indicated a two-fold increase in the risk for CV events in MH as compared with true normotension, an incidence similar to that observed in true SAH. The non-detection of MH and the consequent lack of treatment might have contributed to that result20,37,41.
Non-drug treatment for prehypertension, white coat hypertension and masked hypertension: efficacy and difficulties for implementation
There is no doubt about the benefits obtained with changes in lifestyle (CLS) for individuals with SAH and prehypertension, and there are good indications that they extend to those with WCH, as well as to those with MH1,3.
114
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
The major CLS aimed at that purpose are as follows: weight control; change to the DASH diet (rich in fruits, vegetables, fibers, minerals and low-fat dairy products); reduced salt intake; reduced alcohol consumption; smoking cessation; physical exercise practice; and psychosocial stress control1,3.
Several clinical studies assessing those measures have shown a significant BP reduction in hypertensive and prehypertensive individuals, and a delay in the appearance of SAH in the latter61-68.
Regarding WCH, the encouragement of CLS is based on the following reasons: WCH is not harmless, because individuals with WCH can have changes in target organs; CLS should be the initial strategy to reduce BP in any type of BP behavior change; CLS are recommended as an important strategy to prevent or delay the appearance of SAH in the general population; patients with WCH are more likely to develop sustained SAH; CLS have clear benefits to other CV risk factors; the drug treatment of WCH is still controversial1,3,20.
In masked hypertension, the recommendations can be more specific according to the period of the day in which BP increases, such as morning, daytime and nocturnal hypertension69.
The reduction in alcohol consumption and in physical and mental stress is recommended for patients with morning hypertension70. Regarding hypertension during wakefulness, smoking cessation is necessary, as well as physical and mental stress control71. Those with hypertension during sleep should undergo salt restriction, because that type of hypertension is more often observed in salt-sensitive individuals72, as well as weight reduction, especially the obese individuals with obstructive sleep apnea syndrome73.
In addition to close follow-up by a medical professional, the multiprofessional team plays a fundamental role, motivating adherence to treatment and assuring that changes are permanent1,3,74-76.
Despite evidence, the great limitation and reason of distrust is the effectiveness of those CLS measures out of the context of clinical trials. In real life, even the most motivated individuals face difficulties to sustain CLS, pressed by cultural forces, deep-rooted habits, society rules and commercial interests that encourage sedentary lifestyle, improper diet, and excessive caloric intake77. This raises expectations about the potential of drug alternatives to face those situations78,79.
Drug treatment
PrehypertensionPrehypertension represents an intermediate stage for
established SAH, and its conversion to sustained arterial hypertension is more accelerated in black individuals8,80. The renin-angiotensin-aldosterone system (RAAS) is frequently activated in prehypertensive individuals81. That suggests that the early intervention with drugs might reduce the incidence of sustained hypertension and prevent the progression of CVD.
The Trial of Preventing Hypertension (TROPHY)13 and the Prevention of Hypertension with the Angiotensin-Converting Enzyme Inhibitor Ramipril in Patients with High-Normal
Blood Pressure (PHARAO) Study82 were the first to show that RAAS inhibitors reduce the incidence of hypertension. The TROPHY study has assessed 772 individuals with BP of 130-139/85-89 mm Hg, randomized to receive either placebo or candesartan (16 mg/day – intervention group). All individuals were instructed about CLS. After four years, a lower incidence of SAH (9.8%) was observed in the intervention group, with a 16% reduction in RR and number necessary to treat (NNT) of 1113. That study has been questioned regarding some methodological aspects, which might have overvalued its results. The PHARAO study has assessed 1,008 prehypertensive individuals with BP of 130-139/85-89 mm Hg, for three years, who have been randomly allocated to receive 5 mg/day of ramipril or placebo. The ramipril group showed a 34% reduction in RR in the incidence of SAH assessed by using office BP (NNT = 9) and ABPM (32.5% vs. 53.0%), with an increase in the incidence of cough (4.8% vs. 0.4%)82. However, if those are long-term benefits, if they prevent CV events and are cost-effective is yet to be clarified.
Current guidelines recommend CLS to all prehypertensive individuals, and drug intervention only to those with normal-high BP values at high risk, with CVD or established kidney disease, metabolic syndrome or diabetes1, at medical discretion. It is worth noting that so far there is only evidence for the use of RAAS blockers. Recent European guidelines on hypertension have highlighted the lack of sufficient scientific evidence supporting the beginning of drug treatment for normal-high BP levels.
In face of the evidence above and the low effectiveness of CLS in the long run, the use of low doses of antihypertensive drugs to prehypertensive individuals with no CVD, but at high risk to develop sustained arterial hypertension, should be considered83-85.
White-coat hypertension (WCH)The benefit of drug treatment to WCH remains undefined,
because there has never been a clinical trial specifically designed to test that hypothesis. In addition, large clinical studies designed to show target-organ protection with antihypertensive treatment have never used ABPM or home BP measurements, except in small subgroups, with a small number of CV events, which have not yielded definitive conclusions.
In the lack of direct evidence, and in the presence of high or very high CV risk (concomitance of CVD or kidney disease, target-organ lesions, metabolic syndrome or diabetes), antihypertensive treatment can be considered for WCH. Thus, assessing CV risk factors and determining the risk of individuals with WCH are required for customized decision making about their antihypertensive treatment86.
Those patients should be followed up by using ABPM or home BP measurements.
Masked hypertension (MH)There is plenty of scientific evidence of the negative impact
of MH on CV morbidity and mortality that justify identifying and treating those patients similarly to office hypertensive patients42.
115
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
1. Sociedade Brasileira de Cardiologia. Sociedade Brasileira de Nefrologia. Sociedade Brasileira de Hipertensão. VI Diretrizes Brasileiras de Hipertensão. Arq Bras Cardiol. 2010;95(1 supl 1):1-51.
2. Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL Jr, et al. The National High Blood Pressure Education Program Coordinating Committee. Seventh Report os the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure. Hypertension. 2003;42(6):1206-52.
3. Mancia G, Fagard R, Narkiewicz K, Rédon J, Zanchetti A, Böhm M, et al; Task Force Members. 2013 ESH/ESC Guidelines for the management of arterial hypertension: the Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2013;31(7):1281-357.
4. Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia. V Diretrizes Brasileiras de Monitorização Ambulatorial da Pressão Arterial (MAPA) e III Diretrizes Brasileiras de Monitorização Residencial de Pressão Arterial (MRPA). Arq Bras Cardiol. 2011;97 (3 supl.3):1-24.
5. O’Brien E, Parati G, Stergiou G, Asmar R, Beilin L, Bilo G, et al; European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension position paper on ambulatory blood pressure monitoring. J Hypertens. 2013;31(9):1731-68. Erratum in J Hypertens. 2013;31(12):2467.
6. Vasan RS, Larson MG, Leip EP, Evans JC, O´Donnel CJ, Kannel WB, et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med. 2001;345(18):1291-7.
7. Conen D, Ricker PM, Buring JE, Glynn RJ. Risk of cardiovascular events among women with high normal blood pressure or blood pressure progression: prospective cohort study. BMJ. 2007;335(7617):432-40.
8. Moreira LB, Fuchs SC, Wiehe M, Gus M, Moraes RS, Fuchs FD. Incidence of hypertension in Porto Alegre, Brazil: a population-based study. J Hum Hypertens. 2008;22(1):48-50.
9. Lloyd-Jones D, Adams R, Carnethon M, De Simone G, Ferguson B, Flegal K, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Heart disease and stroke statistics – 2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Circulation. 2009;119(3):e21-181.
10. De Marco M, de Simone G, Roman MJ, Chinalli M, Lee ET, Russel M, et al. Cardiovascular and metabolic predictors of progression of prehypertension into hypertension: the Strong Heart Study. Hypertension. 2009;54(5):974-80.
11. Safar ME, Frohlich ED. (eds): Atherosclerosis, large arteries and cardiovascular risk. Adv Cardiol. Basel: Karger; 2007. p. 117-24.
12. Kaess BM, Rong J, Larson MG, Hamburg NM, Vita JA, Levy D, et al. Aortic stiffness, blood pressure progression, and incident hypertension. JAMA. 2012;308(9):875-81.
13. Julius S, Nesbitt SD, Egan BM, Weber MA, Michelson EL, Kaciroti N, et al; Trial of Preventing Hypertension (TROPHY) Study Investigators. Feasibility of treating prehypertension with an angiotensin-receptor blocker. N Engl J Med. 2006;354(16):1685-97.
14. Vasan RS, Larson MG, Leip EP, Kannel WB, Levy D. Assessment of frequency of progression to hypertension in non-hypertensive participants in the Framingham Heart Study: a cohort study. Lancet. 2001;358(9294):1682-6.
15. Winegarden CR. From “prehypertension” to hypertension?: additional evidence. Ann Epidemiol. 2005;15(9):720-5.
16. Kim YM, Hong KS, Choi YH, Choi MG, Jeong JY, Lee JM, et al. Rates and related factors of progression to hypertension among prehypertensive local residents aged 45 or over in Chuncheon City: hallym aging study from a community-based cross-sectional study. Korean Circ J. 2008;38(1):43-50.
17. Kshirsagar AV, Carpenter M, Bang H, Wyatt SB, Colindres RE. Blood pressure usually considered normal is associated with an elevated risk of cardiovascular disease. Am J Med. 2006;119(2):133-41.
18. Qureshi AI, Suri MF, Kirmani JF, Divani AA, Mohammad Y. Is prehypertension a risk factor for cardiovascular diseases? Stroke. 2005;36(9):1859-63.
19. Ishikawa Y, Ishikawa J, Ishikawa S, Kayaba K, Nakamura Y, Shimada K, et al., Prevalence and determinants of prehypertension in a Japanese general population: the Jichi Medical School Cohort Study. Hypertens Res. 2008;31(7):1323-30.
20. Fagard RH, Cornelissen VA. Incidence of cardiovascular events in white-coat, masked and sustained hypertension vs. true normotension: a meta-analysis. J Hypertens. 2007;25(11):2193-8.
21. Staessen JA, O’Brien ET, Amery AK, Atkins N, Baumgart P, De Cort P, et al. Ambulatory blood pressure in normotensive and hypertensive subjects: results from an international database. J Hypertens Suppl. 1994;12(7):S1-12.
References
Clinical studies on patients with MH demonstrating the relationship between BP decrease and CV risk reduction still lack. The beginning of drug treatment for patients with MH is based on the fact that they actually have out-of-office hypertension, with CV risk similar to that of untreated hypertensives50,87.
Patients with MH should be stratified and treated similarly to conventional hypertensives50. The efficacy of antihypertensive treatment should be assessed by using out-of-office BP measurement.
Complete list of authorsAlexandre Alessi, Andréa Araujo Brandão, Annelise Machado
Gomes de Paiva, Armando da Rocha Nogueira, Audes Feitosa, Carolina de Campos Gonzaga, Celso Amodeo, Decio Mion, Dilma do Socorro Moraes de Souza, Eduardo Barbosa, Emilton Lima Junior, Fernando Nobre, Flavio Dani Fuchs, Hilton Chaves Junior, Jamil Cherem Schneider, João Gemelli, José Fernando Villela-Martin, Luiz Cesar Nazario Scala, Marco Antonio Mota
Gomes, Marcus Vinicus Bolivar Malachias, Nelson Siqueira de Morais, Osni Moreira Filho, Oswaldo Passarelli Junior, Paulo Cesar Brandão Veiga Jardim, Roberto Dischinger Miranda, Rui Póvoa, Sandra Cristina Fuchs, Sergio Baiocchi, Thiago Veiga Jardim, Weimar Kunz Sebba Barroso
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any post-graduation program.
116
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
22. Dolan E, Stanton A, Atkins N, Den Hond E, Thijs L, McCormack P, et al. Determinants of white-coat hypertension. Blood Press Monit. 2004;9(6):307-9.
23. Angeli F, Verdecchia P, Gattobigio R, Sardone M, Reboldi G. White-coat hypertension in adults. Blood Press Monit. 2005;10(6):301-5.
24. Muxfeldt ES, Bloch KV, Nogueira AR, Salles GF True resistant hypertension: is it possible to be recognized in the office? Am J Hypertens. 2005;18(12 Pt 1):1534-40.
25. Mancia G, Bombelli M, Facchetti R, Madotto F, Quarti-Trevano F, Polo Friz H, et al. Long-term risk of sustained hypertension in white-coat or masked hypertension. Hypertension. 2009;54(2):226-32.
26. Helvaci MR, Kaya H, Yalcin A, Kuvandik G. Prevalence of white coat hypertension in underweight and overweight subjects. Int Heart J. 2007;48(5):605-13.
27. Pickering TG, James GD, Boddie C, Harshfield GA, Blank S, Laragh JH. How common is white coat hypertension? JAMA. 1988;259(2):225-8.
28. Verdecchia P, Palatini P, Schillaci G, Mormino P, Porcellati C, Pessina AC. Independent predictors of isolated clinic (‘white-coat’) hypertension. J Hypertens. 2001;19(6):1015-20.
29. National Institute for Health and Clinical Excellence (NICE). Hypertension: the clinical management of primary hypertension in adults. Clinical Guideline CG 127; August 2011.
30. O’Brien E, Asmar R, Beilin L, Imai Y, Mallion JM, Mancia G, et al; European Society of Hypertension Working Group on Blood Pressure Monitoring. European Society of Hypertension recommendations for conventional, ambulatory and home blood pressure measurement. J Hypertens. 2003;21(5):821-48.
31. Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al; Management of Arterial Hypertension of the European Society of Hypertension; European Society of Cardiology. 2007 Guidelines for the Management of Arterial Hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). J Hypertens. 2007;25(6):1105-87. Erratum in: J Hypertens. 2007;25(8):1749.
32. Kikuya M, Hansen TW, Thijs L, Bjorklund-Bodegrd K, Kuznetsova T, Ohkubo T, et al; International Database on Ambulatory Blood Pressure monitoring in relation to Cardiovascular Outcomes Investigators. Diagnostic thresholds for ambulatory blood pressure monitoring based on 10-year cardiovascular risk. Circulation. 2007;115(16):2145-52.
33. Ohkubo T, Imai Y, Tsuji I, Nagai K, Ito S, Satoh H, et al. Reference values for 24-h ambulatory blood pressure monitoring based on a prognostic criterion: the Ohasama study. Hypertension. 1998;32(2):255-9.
34. Myers MG, Haynes RB, Rabkin SW. Canadian Hypertension Society guidelines for ambulatory blood pressure monitoring. Am J Hypertens. 1999;12(11 Pt 1):1149-57. Erratum in Am J Hypertens 2000;13(2):219.
35. Gomes MA, Paiva AM. MAPA e MRPA: o valor das medidas de pressão arterial fora do consultório. Revista Norte Nordeste de Cardiologia. 2013;3(2):10-20.
36. Verdecchia P, Reboldi GP, Angeli F, Schillaci G, Schwartz JE, Pickering TG, et al. Short and long-term incidence of stroke in white coat hypertension. Hypertension. 2005;45(2):203-8.
37. Pierdomenico SD, Cuccurullo F. Prognostic value of white-coat and masked hypertension diagnosed by ambulatory monitoring in initially untreated subjects: an update meta-analysis. Am J Hypertens. 2011;24(1):52-8.
38. Franklin SS, Thijs L, Hansen TW, Li Y, Boggia J, Kikuya M, et al; International Database on Ambulatory Blood Pressure in Relation to Cardiovascular Outcomes Investigators. Significance of white-coat hypertension in older persons with isolated systolic hypertension: a meta-analysis using the International Database on Ambulatory Blood Pressure Monitoring in Relation to Cardiovascular Outcomes population. Hypertension. 2012;59(3):564-71.
39. Hansen TW, Kikuya M, Thijs L, Bjorklund Bodegard K, Kuznetsova T, Ohkubo T, et al. Prognostic superiority of daytime ambulatory over conventional blood pressure in four populations: a meta-analysis of 7030 individuals. J Hypertens. 2007;25(8):1554-64.
40. Pickering TG, Davidson K, Gerin W, Schwartz JE. Masked hypertension. Hypertension. 2002;40(6):795-6.
41. Bobrie G, Clerson P, Menard J, Postel-Vinay N, Chatellier G, Plouin PF. Masked hypertension: a systematic review. J Hypertens. 2008;26(9):1715-25.
42. Verberk WJ, Kessels AG, de Leeuw PW. Prevalence, causes, and consequences of masked hypertension: a meta-analysis. Am J Hypertens. 2008;21(9):969-75.
43. Ogedegbe G. Causal mechanisms of masked hypertension: socio-psychological aspects. Blood Press Monit. 2010;15(2):90-2.
44. Aksoy I, Deinum J, Lenders JW, Thien T. Does masked hypertension exist in healthy volunteers and apparently well-controlled hypertensive patients? Neth J Med. 2006;64(3):72-7.
45. Obara T, Ohkubo T, Kikuya M, Asayama K, Metoki H, Inoue R, et al; J-HOME Study Group. Prevalence of masked uncontrolled and treated white-coat hypertension defined according to the average of morning and evening home blood pressure value: from the Japan Home Versus Office Measurement Evaluation Study. Blood Press Monit. 2005;10(6):311-6.
46. Ogedegbe G, Pickering TG, Clemow L, Chaplin W, Spruill TM, Albanese GM, et al. The misdiagnosis of hypertension: the role of patient anxiety. Arch Intern Med. 2008;168(22):2459-65.
47. Wang GL, Li Y, Staessen JA, Lu L, Wang JG. Anthropometric and lifestyle factors associated with white-coat, masked and sustained hypertension in a Chinese population. J Hypertens. 2007;25(12):2398-405.
48. Baguet JP, Hammer L, Levy P, Pierre H, Rossini E, Mouret S, et al. Night-time and diastolic hypertension are common and underestimated conditions in newly diagnosed apnoeic patients. J Hypertens. 2005;23(3):521-7.
49. Ungar A, Pepe G, Monami M, Lambertucci L, Torrini M, Baldasseroni S, et al. Isolated ambulatory hypertension is common in outpatients referred to a hypertension center. J Hum Hypertens. 2004;18(12):897-903.
50. Ogedegbe G, Agyemang C, Ravenell JE. Masked hypertension: evidence of the need to treat. Curr Hypertens Rep. 2010;12(5):349-55.
51. Pickering T, Eguchi K, Kario K. Masked hypertension: a review. Hypertens Res. 2007;30(6):479-88.
52. Terawaki H, Metoki H, Nakayama M, Ohkubo T, Kikuya M, Asayama K, et al. Masked hypertension determined by self-measured blood pressure at home and chronic kidney disease in the Japanese general population: the Ohasama study. Hypertens Res. 2008;31(12):2129-35.
53. Kawano Y, Horio T, Matayoshi T, Kamide K. Masked hypertension: subtypes and target organ damage. Clin Exp Hypertens. 2008;30(3):289-96.
54. Mallion JM, Genes N, Vaur L, Clerson P, Vaisse B, Bobrie G, et al. Detection of masked hypertension by home blood pressure measurement: is the number of measurements an important issue? Blood Press Monit. 2004;9(6):301-5.
55. Head GA, McGrath BP, Mihailidou AS, Nelson MR, Schlaich MP, Stowasser M, et al. Ambulatory blood pressure monitoring in Australia: 2011 consensus position statement. J Hypertens. 2012;30(3):253-66.
56. Verdecchia P, Porcellati C, Schillaci G, Borgioni C, Ciucci A, Battistelli M, et al. Ambulatory blood pressure: an independent predictor of prognosis in essential hypertension. Hypertension. 1994;24(6):793-801.
57. Liu JE, Roman MJ, Pini R, Schwartz JE, Pickering TG, Devereux RB. Cardiac and arterial target organ damage in adults with elevated ambulatory and normal office blood pressure. Ann Intern Med. 1999;131(8):564-72.
58. Bobrie G, Chatellier G, Genes N, Clerson P, Vaur L, Vaisse B, et al. Cardiovascular prognosis of “masked hypertension” detected by blood pressure self-measurement in elderly treated hypertensive patients. JAMA. 2004;291(11):1342-9.
117
Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119
59. Cuspidi C, Negri F, Sala C, Mancia G. Masked hypertension and echocardiographic left ventricular hypertrophy: an updated overview. Blood Press Monit. 2012;17(1):8-13.
60. Hanninen MR, Niiranen TJ, Puukka PJ, Johansson J, Jula AM. Prognostic significance of masked and white-coat hypertension in the general population: the Finn-Home Study. J Hypertens. 2012;30(4):705-12.
61. Effects of weight loss and sodium reduction intervention on blood pressure and hypertension incidence in overweight people with high-normal blood pressure. The Trials of Hypertension Prevention, phase II. The Trials of Hypertension Prevention Collaborative Research Group. Arch Intern Med. 1997;157(6):657-67.
62. Appel LJ, Moore TJ, Obarzanek E, Wollmer WM, Svetkey LP, Sacks FM, et al. A clinical trial of the effects of dietary patterns on blood pressure. DASH Collaborative Research Group. N Engl J Med. 1997;336 (16):1117-24.
63. Sacks FM, Svetkey LP, Vollmer WM, Appel LJ, Bray GA, Harsha D, et al. Effects on blood pressure of reduced dietary sodium and the Dietary Approaches to Stop Hypertension (DASH) diet. DASH-Sodium Collaborative Research Group. N Engl J Med. 2001;344(1):3-10.
64. Stevens VJ, Obarzanek E, Cook NR, Lee IM, Appel LJ, West DS, et al. Long-term weight loss and changes in blood pressure: results of the Trials of Hypertension Prevention, phase II. Ann Intern Med. 2001;134 (1):1-11.
65 Cook NR, Cutler JA, Obarzanek E, Buring JE, Rexrode KM, Kumanyika SK, et al. Long term effects of dietary sodium reduction on cardiovascular disease outcomes: observational follow-up of the trials of hypertension prevention (TOHP). BMJ. 2007;334(7599):885-8.
66. Appel LJ, Champagne CM, Harsha DW, Cooper LS, Obarzanek E, Elmer PJ, et al. Effects of comprehensive lifestyle modification on blood pressure control: main results of the PREMIER clinical trial. JAMA. 2003;289(16):2083-93.
67. Elmer PJ, Obarzanek E, Vollmer WM, Simons-Morton D, Stevens VJ, Young DR, et al. Effects of comprehensive lifestyle modification on diet, weight, physical fitness, and blood pressure control: 18-month results of a randomized trial. Ann Intern Med. 2006;144 (7):485-95.
68. Park S, Rink LD, Wallace JP. Accumulation of physical activity leads to a greater blood pressure reduction than a single continuous session, in prehypertension. J Hypertens. 2006;24(9):1761-70.
69. Kawano Y. Lifestyle modification for masked hypertension. Curr Hypertens Rev. 2011;7(1):9-12.
70. Leary AC, Struthers AC, Donnan PT, MacDonald TM, Murphy MB. The morning surge in blood pressure and heart rate is dependent on physical activity after waking. J Hypertens. 2002;20(5):865-70.
71. Verdecchia P, Schilatti G, Borgioni C, Ciucci A, Zampi I, Battistelli M, et al. Cigarette smoking, ambulatory blood pressure and cardiac hypertrophy in essential hypertension. J Hypertens. 1995;13(10):1209-15.
72. Uzu T, Nakao K, Kume S, Araki H, Isshiki K, Araki S, et al. High sodium intake is associated with masked hypertension in Japanese patients with type 2 diabetes and treated hypertension. Am J Hypertens. 2012;25(11):1170-4.
73. Baguet JP, Lévy P, Barone-Rochette G, Tamisier R, Pierre H, Peeters M, et al. Masked hypertension in obstructive sleep apnea syndrome. J Hypertens. 2008;26(5):885-92.
74. Tsai J, Liu J, Kao C, Tomlinson B, Kao P, Chen J, et al. Beneficial effects on blood pressure and lipid profile of programmed exercise training in subjects with white coat hypertension. Am J Hypertens. 2002;15(6):571-6.
75. Lima AS, Zanetti ML, Miyar LO, Machado MP. Fatores facilitadores / dificultadores para a implementação de um programa educativo por equipe multidisciplinar. Arq Bras Endocrinol Metab. 2003;47(5):568-78.
76. Margolius D, Wong J, Goldman ML, Rouse-Iniguez J, Bodenheimer T. Delegating responsibil ity from clinicians to nonprofessional personnel: the example of hypertension control. J Am Board Fam Med. 2012;25(2):209-15.
77. Appel LJ; American Society of Hypertension Writing Group. ASH position paper: dietary approaches to lower blood pressure. J Am Soc Hypertens. 2009;3(5):321-31.
78. Hooper L, Bartlett C, Davey Smith G, Ebrahim S. Systematic review of long term effects of advice to reduce dietary salt in adults. BMJ. 2002;325(7365):628.
79. Fuchs FD, Gus M, Moreira WD, Moraes RS, Rosito GA, Sorucco A, et al. Blood pressure effects of antyhypertensive drugs and lifestyle modification in a Brazilian hypertensive cohort. J Hypertens. 1997; 15:783–792.
80. Selassie A, Wagner CS, Laken ML, Ferguson ML, Ferdinand KC, Egan BM. Progression is accelerated from prehypertension to hypertension in blacks. Hypertension. 2011;58(4):579-87.
81. Fink GD, Arthur C. Corcoran Memorial Lecture. Sympathetic activity, vascular capacitance, and long-term regulation of arterial pressure. Hypertension. 2009;53(2)307-12.
82. Luders S, Schrader J, Berger J, Unger T, Zidek W, Bohm M, et al. The PHARAO study: prevention of hypertension with the angiotensin-converting enzyme inhibitor ramipril in patients with high-normal blood pressure – a prospective, randomized, controlled prevention trial of the German Hypertension League. J Hypertens. 2008;26(7):1487-96.
83. Fuchs FD, Fuchs SC, Moreira LB, Gus M, Nóbrega AC, Poli-de-Figueiredo CE, et al. Prevention of hypertension in patients with pre-hypertension: protocol for the PREVER-prevent trial. Trials. 2011;12:65.
84. McInnes G. Pre-hypertension: how low to go and do drugs have a role. Br J Clin Pharmacol. 2012;73(2):187-93.
85. Thompson AM, Hu T, Eshelbrenner CL, Reynolds K, He J, Bazzano LA. Antihypertensive treatment and secondary prevention of cardiovascular disease events among persons without hypertension: a meta-analysis. JAMA. 2011;305(9):913-22.
86. Mancia G, Bombelli M, Seravalle G, Grassi G. Diagnosis and management of patients with white-coat and masked hypertension. Nat Rev Cardiol. 2011;8(12):686-93.
87. Phillips RA. Controversies in blood pressure goal guidelines and masked hypertension. Ann NY Acad Sci. 2012;1254:115-22.
118

Special Article
I Brazilian Position Paper
Arq Bras Cardiol. 2014; 102(2):110-119 119
Original Article
Value of Coronary Artery Calcium Score to Predict Severity or Complexity of Coronary Artery DiseaseTayyar Gökdeniz1, Ezgi Kalaycıoğlu1, Ahmet Çağrı Aykan1, Faruk Boyacı1, Turhan Turan2, İlker Gül1, Gökhan Çavuşoğlu3, İhsan Dursun1
Departamento de Cardiologia - Ahi Evren Chest and Cardiovascular Surgery Education and Research Hospital1; Departamento de Cardiologia - Akçabat State Hospital2, Trabzon, Turquia; Departamento de Radiologia - Ahi Evren Chest and Cardiovascular Surgery Education and Research Hospital3
Mailing Address: Tayyar Gökdeniz •Trabzon Ahi Evren Gögüs ve Kalp Damar Cerrahisi Egitim ve Araştırma Hastanesi, Soguksu Mahallesi, Çamlık Caddesi, 61040 Trabzon, TurkeyE-mail: [email protected] received June 16, 2013, revised manuscript September 09, 2013, accepted September 18, 2013.
DOI: 10.5935/abc.20130241
Abstract
Background: Prediction of severity or complexity of coronary artery disease (CAD) is valuable owing to increased risk for cardiovascular events. Although the association between total coronary artery calcium (CAC) score and severity of CAD, Gensini score was not used, it has been previously demonstrated. There is no information about the association between total CAC score and complexity of CAD.
Objectives: To investigate the association between severity or complexity of coronary artery disease (CAD) assessed by Gensini score and SYNTAX score (SS), respectively, and coronary artery calcium (CAC) score, which is a noninvasive method for CAD evaluation in symptomatic patients with accompanying significant CAD.
Methods: Two-hundred-fourteen patients were enrolled. Total CAC score was obtained before angiography. Severity and complexity of CAD was assessed by Gensini score and SS, respectively. Associations between clinical and angiographic parameters and total CAC score were analyzed.
Results: Median total CAC score was 192 (23.0-729.8), and this was positively correlated with both Gensini score (r: 0.299, p<0.001) and SS (r: 0.577, p<0.001). At multivariate analysis, it was independently associated with age (β: 0.154, p: 0.027), male gender (β: 0.126, p: 0.035) and SS (β: 0.481, p< 0.001). Receiver-operating characteristic (ROC) curve analysis revealed a cut-off value > 809 for SS >32 (high SS tertile).
Conclusion: In symptomatic patients with accompanying significant CAD, total CAC score was independently associated with SS and patients with SS >32 may be detected through high Agatston score. (Arq Bras Cardiol. 2014; 102(2):120-127)
Keywords: Total coronary calcium score, Gensini score, SYNTAX score, Coronary artery disease.
IntroductionCoronary artery disease (CAD) is one of the leading
causes of mortality and morbidity1,2. Invasive conventional coronary angiography (CCA) is the gold standard technique for diagnosis and the selection of best treatment options for CAD and reveals the severity and complexity of CAD3. Previous studies have shown that CAD severity and complexity assessed by Gensini score and SYNTAX score (SS), respectively, are associated to increased cardiovascular events (CVE) a factor of mortality and morbidity4,5.
CAD severity and complexity have recently attracted increasing interest for CAD evaluation based on the clinical importance and treatment challenge. Gensini and
SS are easy-to-apply and reproducible scoring systems4,6. SS incorporates morphological features of lesions such as total occlusion, bifurcation, length and localizations of lesions based on the myocardial area at risk7. Therefore, some efforts have been made for the prediction of CAD severity and complexity using non-invasive methods in order to identify the patients at high risk for CVE and treatment challenges before CCA8,9.
Coronary artery calcification (CAC) has a role in atherosclerotic plaque formation10,11. It was quantitated by total CAC score called Agatston score. Multidetector computerized tomography (MDCT) currently represents a noninvasive method for accurate quantification of total CAC score12,13. The association between total CAC score and prognostic information about future cardiac events has been previously demonstrated. Some studies have shown that angiographically proven and significant CAD is related to total CAC score14-16.
The purpose of the present study was to investigate the association of total CAC score and CAD severity and complexity assessed by SS and Gensini score, respectively, and to find which one of the two, CAD severity or complexity, is better associated with total CAC score in symptomatic patients with accompanying significant CAD.
120

Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
MethodsData was retrospectively collected between January 2012
and February 2013. We enrolled 923 consecutive patients with symptoms suggestive of CAD who underwent 64 – slice computed tomography coronary angiography (CTA) for assessment of significant CAD. Non- enhanced CT scans were obtained for total CAC score immediately before CTA. Indications for CTA were patients with low to intermediate probability of significant CAD, indeterminate diagnostic test results, high clinical suspicion for CAD and, inability to perform non-invasive tests. 709 patients were not eligible for the study. Reasons for non-inclusion are shown in Table 1. Therefore, the remaining 214 patients with 50% or greater luminal stenosis in any major epicardial coronary artery constituted the study population. All patients underwent CCA within two weeks after CTA and performance of CCA was not influenced by total CAC scores.
All patients gave informed consent before enrollment, and the study protocol was approved by the local Ethical Committee. Baseline clinical and demographic characteristics were obtained from all patients. A detailed physical examination was performed including past medical history. Complete blood count, lipid profile and serum creatinine levels were obtained from all patients before CCA. Cardiovascular risk factors were recorded. Hypertension was identified based on prior prescription of antihypertensive drugs or when blood pressure exceeded 140/90 mmHg in at least three measurements. Dyslipidemia and diabetes were defined as prior prescription of antihyperlipidemic and antidiabetic medications or total cholesterol level > 200 mg/dL and fasting glucose levels above 126 mg/dL, respectively. Current smokers were defined as subjects with a positive history of cigarette smoking. Glomerular filtration rate (GFR) was calculated using the Cockcroft-Gault formula17.
Body mass index (BMI) was calculated (kg/m2). Comprehensive two-dimensional transthoracic echocardiography including M-mode and, Doppler echocardiography, were performed by an experienced cardiologist before CCA, using a Vivid-S5, GE (United States) instrument, with a 3.6 MHZ transducer. Measurements were performed according to the American Society of Echocardiography guidelines18. LV end-systolic and end-diastolic volumes and ejection fraction were calculated by the Simpson biplane method.
SYNTAX scoreAll patients underwent selective coronary angiography,
which was performed using the Judkins technique. Significant lesion was defined as a 50% or greater stenosis in the luminal diameter of any major epicardial coronary artery. The presence of significant lesions was determined based on visual estimation. Basal angiographic characteristics of patients such as diseased vessel, left main coronary artery (LMCA), left anterior descending (LAD) coronary artery; right coronary artery (RCA), circumflex coronary artery (Cx), and diseased vessel number were recorded.
SS is mainly associated with CAD complexity and it was calculated using dedicated software, which integrates two components (a) morphological features of each lesion such as dominance, chronic total occlusion (CTO), bifurcation,
trifurcation, tortuosity, heavy calcification, lesion length, presence of thrombus, aorto-ostial and diffuse lesions, and (b) weighting factors of lesions based on myocardial area distal to lesion. Lesions with ≥ 50% luminal obstruction in vessels with a diameter ≥1.5 mm were added to provide SS7,8. SS was calculated using dedicated software (version 2.11, www.syntaxscore.com) and all morphological features of each lesion included in SS were recorded.
The SS was divided into two tertiles as follows: low- intermediate risk tertile was ≤ 32 and high-risk tertile was > 32. All angiograms were scored by two experienced interventional cardiologists who were blinded to CAC measurement data.
Gensini scoreCAD severity was assessed by Gensini score, which is based
on the percentage of luminal narrowing (25%: 1 point; 50%: 2 points; 75%: 4 points; 90%: 8 points; 99%: 16 points, and total occlusion: 32 points). Each coronary lesion score was calculated using percentage of luminal narrowing multiplied by coefficient of coronary segment: the left main coronary artery (LMCA) x5; the proximal segment of the left anterior descending coronary artery (LAD) x 2.5; the proximal segment of the circumflex artery (CX) x 2.5; themid-segment of the LAD x 1.5; the distal segment of the LAD, all segments of the right coronary artery (RCA) and the obtuse marginal artery x 1; and other segments x 0.5. The Gensini score was calculated by summation of individual coronary segment scores4.
Coronary artery calcification measurementCAC measurement was performed immediately before CTA
in all patients. None of the patients had hyperthyroidism and all patients had sinus rhythm during the procedure. Imaging was performed using a 64 – slice CT scanner (Aquilion 64, Toshiba Medical Systems, Tochigi, Japan). CT scan for total CAC score was obtained by prospective gating with collimation (4 × 3.0 mm) with 3-mm reconstructed slice thickness. Tube current and tube voltage were 300 mA, 120 kV, respectively and gantry rotation time 0.4 s19.
Total CAC score was calculated using dedicated software (Vitrea2 version 3.0.9.1, Vital Images, Minnesota). Calcium based on the Agatston method was defined as the presence of a lesion with an area greater than 1 mm2, and peak intensity greater than
Table 1 ‑ Number of ineligible patients and reasons for non-inclusion
n: 709
Non-significant CAD in CTA, n (%) 665 (72.1%)
Patients with previous bypass surgery, n (%) 12 (1.3%)
Previous coronary stent implantation, n (%) 19 (2.1%)
End- stage renal failure, n (%) 4 (0.4%)
History of valvular replacement, n (%) 2 (0.2%)
Atrial fibrillation, n (%) 6 (0.6%)
Malignancy, n (%) 1 (0.1%)
CAD: coronary artery disease; CTA: computed tomography coronary angiography.
121
Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
Table 2 ‑ Baseline characteristics of the study population
Age (years) 63.5 ± 10.8
Male, n (%) 170(79.4%)
Diabetes mellitus, n (%) 63(29.4%)
Hypertension, n (%) 130(60.7%)
Current smokers, n (%) 64(29.9%)
Dyslipidemia, n (%) 119(55.6%)
Total cholesterol, mg/dL 206.7 ± 42.8
HDL cholesterol, mg/dL 40.8 ± 8.8
LDL cholesterol, mg/dL 144.5 ± 30.9
Triglycerides, mg/dL 153(110-191.3)
GFR, mL/min 95.7 ± 28.8
BMI, kg/m² 27.9 ± 2.7
Glucose, mg/dL 105(93-124)
Hemoglobin, g/dL 13.8 ± 1.6
RDW 13.4(12.8-14.1)
LVEF, % 55(48-60)
Gensini score 34(17-64)
SS 13(7.0-26.1)
Total CAC score 192(23.0-729.8)
Cardiovascular medications
ACE-I, n (%) 91(42.5%)
Beta-blocker, n (%) 124(57.9%)
Statin, n (%) 81(37.9%)
Ca++ channel blocker, n (%) 27(12.6%)
Data are expressed in numbers (percentages), mean or median and (interquartile range). Percentages are rounded. SS: SYNTAX score; BMI: body mass index; GFR: glomerular filtration rate; HDL: high density lipoprotein; LDL: low density lipoprotein; LVEF: left ventricular ejection fraction; ACE-I: angiotensin converting enzyme inhibitor; RDW: red cell distribution width; CAC: coronary artery calcium.
130 Hounsfield Units, which was automatically identified and marked with color by the software. All lesions were added to calculate the total CAC score by the Agatston method.
Statistical analysisSPSS 17.0 statistical software (SPSS Inc., Chicago, IL,
USA) and MedCalc software program, release 12.3.0.0 (MedCalc Software, Belgium) were used for statistical analysis. Continuous variables were expressed as mean ± standard deviation (SD) or median and interquartile range as appropriate. Categorical variables were expressed as percentages. The Kolmogorov Smirnov test was used to test normality of distribution of continuous variables. Group means for continuous variables were compared with the Student’s t-test or the Mann-Whitney U test, as appropriate. Pearson’s or Spearman’s correlation analysis was used for assessing correlation between total CAC score and continuous variables depending on Gaussian distributions.
To find independent associates of total CAC score, variables with a p value of ≤ 0.05 at the bivariate correlation analysis and univariate analysis were selected for multiple linear regression analyses. To account for the non-Gaussian distribution of total CAC scores, a log10 {x+1} transformation was made. Triglyceride, glucose, red cell distribution width (RDW), left ventricle ejection fraction (LVEF), Gensini score and SS were also transformed to the natural logarithmic scale and in order to avoid co-linearity when assessing the multivariate model, independent variables were tested for intercorrelation. A two-tailed p < 0.05 was considered statistically significant. The Chi-square test examined the correlation between categorical variables and continuous variables. Inter-observer agreement of SS and Gensini score was calculated by using Bland-Altman analysis and the intra-class correlation coefficient was used to assess intra-observer agreement. Receiver-operating characteristic (ROC) curve analysis was performed to detect the cut-off value of total CAC score in predicting SS >32 (high-risk tertile). A p value of ≤ 0.05 was considered statistically significant.
ResultsThe study population consisted of 214 patients, 170
(79.4%) were males with mean age of 63.5±10.8. A total of 558 lesions with 50% or greater stenosis in the luminal diameter of major epicardial coronary arteries were detected from the CCA data. Single-vessel disease was present in 44 (20.6%), 23 (10.7%), and 15 (7%) patients for LAD, RCA and Cx, respectively. Two- and three-vessel diseases were present in 37.9% and 23.8% of patients, respectively. Nineteen (8.9%) patients had a total CAC score = 0, among them, two and three-vessel disease were present in 4 (21.1%) and 1 (5.2%), respectively, while single-vessel disease was present in 14 (73.7%). Baseline clinical, laboratory and echocardiographic features of patients are shown in Table 2.
Independent associates of total CAC scoreSpearman’s correlation analysis showed a significant
correlation between total CAC score and SS (r: 0.577, p < 0.001) and Gensini score (r: 0.299, p < 0.001) (Figure 1). Univariate analysis showed that male patients
and patients with hypertension had significantly higher total CAC score, (p: 0.004 and p: 0.048), respectively. Total CAC score was significantly higher among patients taking angiotensin-converting enzyme inhibitors (ACE-I) (p: 0.013). Bivariate correlation analysis showed that total CAC score was associated with age (r: 0.320, p < 0.001), GFR (r: -0.236, p: 0.001), hemoglobin (r: -0.181, p: 0.008), LVEF (r: -0.268, p < 0.001) and RDW (r: 0.186, p: 0.006).
Multiple linear regression analysis was performed to find independent associates of total CAC score. Age (β: 0.154, p: 0.027), male gender (β: 0.126, p: 0.035) and SS (β: 0.481, p < 0.001) were independent predictors of total CAC score. Independent associates of total CAC score are shown in Table 3. Results of correlation analysis between total CAC score and morphological features of lesions included in SS are shown in Table 4. The mean values of total CAC scores based on presence or absence of morphological features of lesions is shown in Figure 2.
122
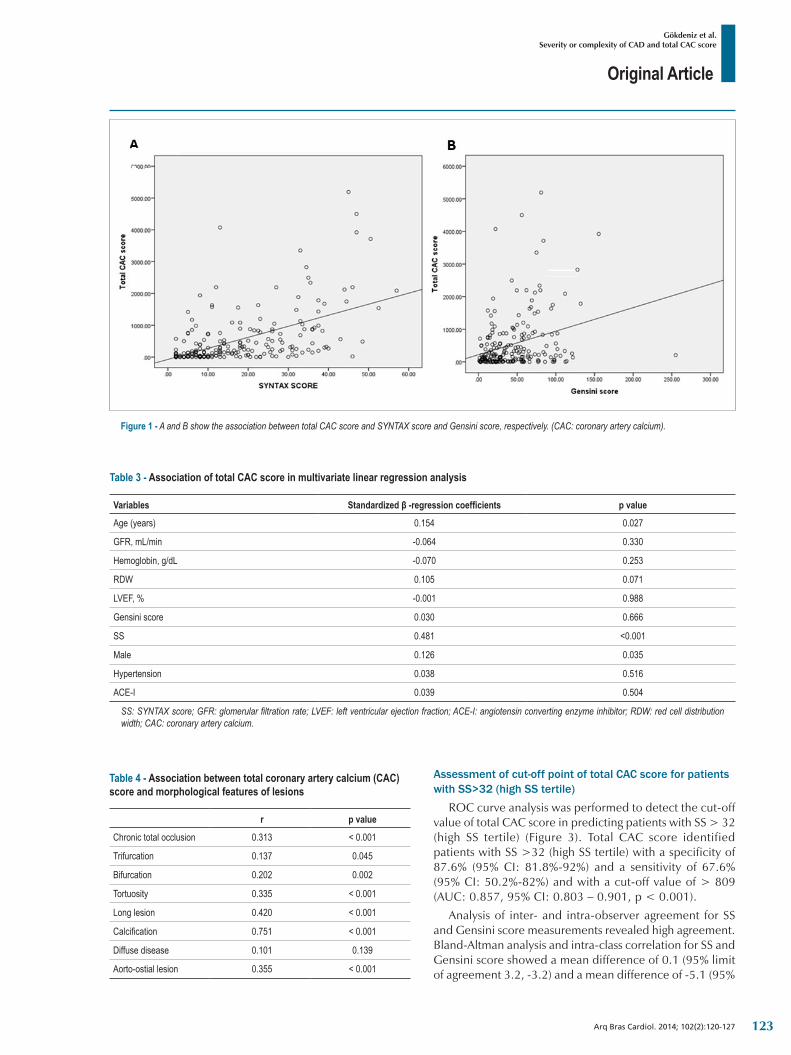
Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
Table 3 ‑ Association of total CAC score in multivariate linear regression analysis
Variables Standardized β -regression coefficients p value
Age (years) 0.154 0.027
GFR, mL/min -0.064 0.330
Hemoglobin, g/dL -0.070 0.253
RDW 0.105 0.071
LVEF, % -0.001 0.988
Gensini score 0.030 0.666
SS 0.481 <0.001
Male 0.126 0.035
Hypertension 0.038 0.516
ACE-I 0.039 0.504
SS: SYNTAX score; GFR: glomerular filtration rate; LVEF: left ventricular ejection fraction; ACE-I: angiotensin converting enzyme inhibitor; RDW: red cell distribution width; CAC: coronary artery calcium.
Table 4 ‑ Association between total coronary artery calcium (CAC) score and morphological features of lesions
r p value
Chronic total occlusion 0.313 < 0.001
Trifurcation 0.137 0.045
Bifurcation 0.202 0.002
Tortuosity 0.335 < 0.001
Long lesion 0.420 < 0.001
Calcification 0.751 < 0.001
Diffuse disease 0.101 0.139
Aorto-ostial lesion 0.355 < 0.001
Assessment of cut-off point of total CAC score for patients with SS>32 (high SS tertile)
ROC curve analysis was performed to detect the cut-off value of total CAC score in predicting patients with SS > 32 (high SS tertile) (Figure 3). Total CAC score identified patients with SS >32 (high SS tertile) with a specificity of 87.6% (95% CI: 81.8%-92%) and a sensitivity of 67.6% (95% CI: 50.2%-82%) and with a cut-off value of > 809 (AUC: 0.857, 95% CI: 0.803 – 0.901, p < 0.001).
Analysis of inter- and intra-observer agreement for SS and Gensini score measurements revealed high agreement. Bland-Altman analysis and intra-class correlation for SS and Gensini score showed a mean difference of 0.1 (95% limit of agreement 3.2, -3.2) and a mean difference of -5.1 (95%
Figure 1 ‑ A and B show the association between total CAC score and SYNTAX score and Gensini score, respectively. (CAC: coronary artery calcium).
123
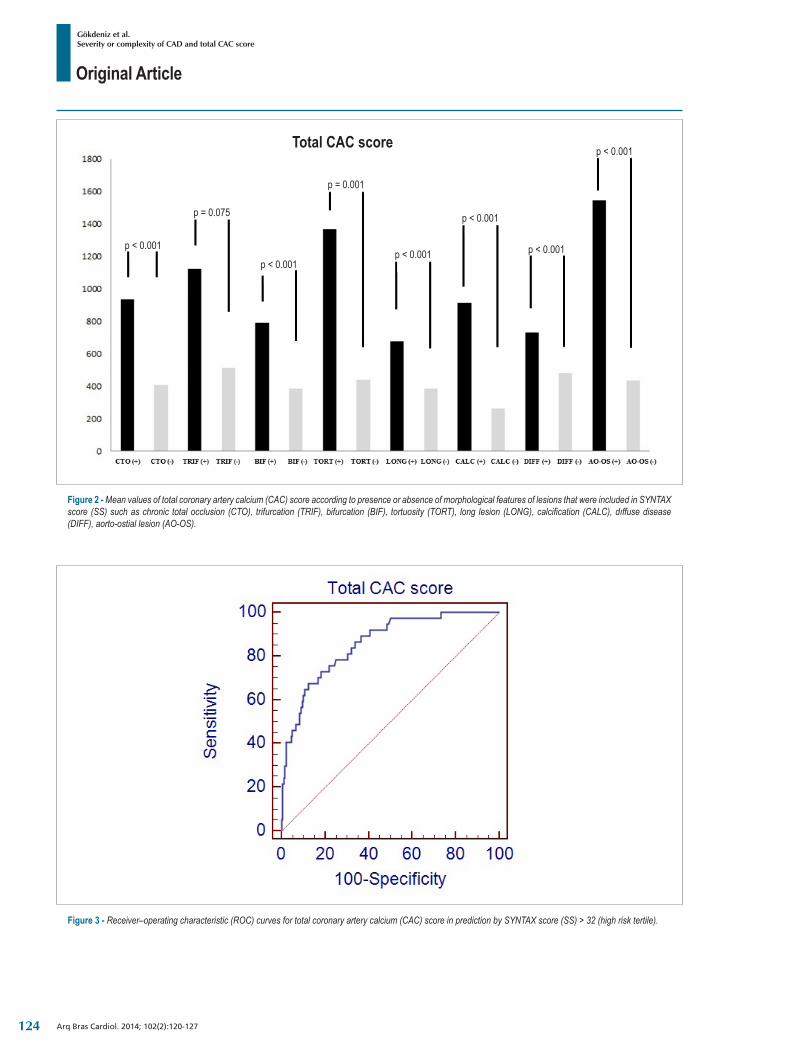
Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
Figure 3 ‑ Receiver–operating characteristic (ROC) curves for total coronary artery calcium (CAC) score in prediction by SYNTAX score (SS) > 32 (high risk tertile).
Figure 2 ‑ Mean values of total coronary artery calcium (CAC) score according to presence or absence of morphological features of lesions that were included in SYNTAX score (SS) such as chronic total occlusion (CTO), trifurcation (TRIF), bifurcation (BIF), tortuosity (TORT), long lesion (LONG), calcification (CALC), dıffuse disease (DIFF), aorto-ostial lesion (AO-OS).
Total CAC score
p < 0.001
p < 0.001
p = 0.001
p < 0.001
p < 0.001
p < 0.001
p < 0.001
p = 0.075
124

Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
limit of agreement 30.4, -40.6) as well as an intra-class correlation coefficient of 0.977 (95% CI 0.970 – 0.983) and 0.955 (95% CI 0.942 – 0.966), respectively.
DiscussionThe present study showed that Gensini score and
SS were significantly correlated with total CAC score. However, age, male gender and SS were independently associated with total CAC score in symptomatic patients with accompanying significant CAD. For total CAC score, a cut-off value > 809 with a specificity of 87.6% and a sensitivity of 67.6% were found for the identification of patients with SS > 32 (high SS tertile).
CAC is mainly limited to the subintimal space of coronary arteries and may occur around the second decade of life. Calcification of atherosclerotic plaque increases according to aging and atherosclerotic progression. CAC is therefore regarded as a marker of coronary atherosclerosis20. Previous studies have considered the association between coronary artery disease and CAC, especially in asymptomatic patients. The prognostic value of CAC in asymptomatic patients has been shown to be independent of traditional risk factors in studies such as the Multi-Ethnic Study of Atherosclerosis (MESA)20. In symptomatic patients, the association between presence of CAC and obstructive CAD has been demonstrated with high sensitivity and low specificity. Therefore, more efforts have been performed for CAC utilization as a useful filter for obstructive CAD before CCA21,22. A limited numbers of studies have examined the value of CAC for prediction of CAD severity and complexity beyond prediction of obstructive CAD in patients with symptoms suggestive of the disease9,23.
Schmermund et al9 reported that CAC score determined through the Agatston method predicts the angiographic extent of CAD in symptomatic patients. Extent of CAD was interpreted as the percentage of flow-limiting luminal narrowing. Likewise, Budoff et al16 reported similar results in symptomatic patients. In the present study, total CAC score was not independently associated with CAD severity assessed by Gensini score, although it was significantly correlated with Gensini score. Our study results did not contradict the results of these two previous studies, because of the different methods used. Our explanations about the results of the present study are: first of all, Gensini score is based on the percentage of luminal narrowing and coefficient of coronary segment that was affected. The percentage of luminal narrowing had a considerable impact on the scoring system and all lesions with ≥ 25% luminal narrowing that were included in the calculation. Previous studies have reported that not all coronary plaques are calcified and CAC score was weakly correlated with severity of luminal stenosis24,25. Therefore, Gensini score may not be associated with total CAC score. Secondly, the association between Gensini score and total CAC score was decreased depending on the effects of traditional risk factors and SS on the Gensini score. Intercorrelation was tested in order to avoid collinearity.
Our study results were compatible with previous reports that age and male gender are independently associated with
total CAC score20. The association between total CAC score and SS was evaluated first by Stähli et al23, who previously demonstrated higher Agatston scores in patients treated by complex percutaneous coronary interventions (PCIs) defined as use of the buddy wire technique, kissing balloon, necessity of high pressure balloon, pre or post-dilation and use of a rotablator23. In contrast to the definition of complex PCI by Stähli et al., the SS we used to define complex PCI has been shown in previous studies to be associated with cardiovascular mortality and treatment challenges5,7. SS incorporates a number of morphological features of lesions, such as CTO, bifurcation, trifurcation, tortuosity, heavy calcification, lesion length, aorto-ostial and diffuse lesions. Presence of calcification in CTO and right coronary ostial lesions was demonstrated by Srivatsa et al26 and Popma et al27, respectively. These findings support our study results. Additionally, calcification of lesions adds two points to the scoring system. All morphologic features of lesions were significantly correlated with total CAC score, except for diffuse disease. An association between coronary calcification and endothelial dysfunction and impaired myocardial blood flow in patients with angiographically normal coronary has been previously demonstrated28-30. Altered coronary blood flow in the presence of coronary calcification may affect atherosclerotic plaque progression and formation, which constitute the main determinants of complex CAD formation. Altered coronary blood flow may cause lesion formations including tortuosity, bifurcation or ostial lesion depending on impaired flow dynamics.
ConclusionTotal CAC score was independently associated with
complexity of CAD assessed by SS. Studies have shown that SS is associated with increased cardiovascular mortality and treatment challenge5,7. Total CAC score measurement represents a non-invasively anatomical imaging of coronary arteries with a relatively small radiation exposure. Therefore, in clinical practice, total CAC score measurement may predict cardiovascular mortality and treatment challenge before CCA in symptomatic patients with accompanying significant CAD.
LimitationsThe study population was relatively small. Quantification
of lesions was performed according to visual estimation. However, all angiograms were scored by two experienced interventional cardiologists. Analysis of our study was based on per-patient, rather than per-vessel levels. Therefore, CAC score per-coronary artery was not included in the study. Some large-scale studies, such as MESA, have reported that CAC was less predictive on a per-vessel than on a per-patient level. 64-slice MDCT determines coronary calcium with a slice thickness of 3-mm, which may result in missing low levels of coronary calcium. However, many authors concluded that MDCT is equivalent to electron beam tomography for CAC scoring. In our study, the Agatston method was used for CAC scoring, while other methods such as mass score and calcium volume score were
125
Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
1. Lloyd-Jones D, Adams RJ, Brown TM, Carnethon M, Dai S, De Simone G, et al; American Heart Association Statistics Committee and Stroke Statistics Subcommittee. Executive summary: heart disease and stoke statistics 2010 update: a report from the American Heart Association. Circulation. 2010;121(7):948-54. Erratum in Circulation. 2010;121(12):e259.
2. Gaziano TA, Bitton A, Anand S, Abrahams-Gessel S, Murphy A. Growing epidemic of coronary heart disease in low-and middle-income countries. Curr Probl Cardiol. 2010;35(2):72-115.
3. Higgins CB. Coronary angiography a decade of advances. Am J Cardiol. 1988;62(18):7K-10K.
4. Ndrepepa G, Tada T, Fusaro M, Cassese S, King L, Hadamitzky M, et al. Association of coronary atherosclerotic burden with clinical presentation and prognosis in patients with stable and unstable coronary artery disease. Clin Res Cardiol. 2012;101(12):1003-11.
5. Farooq V, Serruys PW, Bourantas C, Vranckx P, Diletti R, Garcia Garcia HM, et al. Incidence and multivariable correlates of long-term mortality in patients treated with surgical or percutaneous revascularization in the Synergy between Percutaneous Coronary Intervention with Taxus and Cardiac Surgery (SYNTAX) trial. Eur Heart J. 2012;33(24):3105-13.
6. Tanboga IH, Ekinci M, Isik T, Kurt M, Kaya A, Sevimli S. Reproducibility of syntax score: from core lab to real world. J Interv Cardiol. 2011;24(4):302-6.
7. Ong AT, Serruys PW, Mohr FW, Morice MC, Kappetein AP, Holmes DR Jr, et al. TheSYNergy between percutaneous coronary intervention with TAXus and cardiac surgery (SYNTAX) study: design, rationale, and run-in phase. Am Heart J. 2006;151(6):1194-204.
8. Gökdeniz T, Turan T, Aykan AC, Gül I, Boyacı F, Hatem E, et al. Relation of epicardial fat thickness and cardio-ankle vascular index to complexity of coronary artery disease in nondiabetic patients. Cardiology. 2013;124(1):41-8.
9. Schmermund A, Denktas AE, Rumberger JA, Christian TF, Sheedy PF 2nd, BaileyKR, et al. Independent and incremental value of coronary artery calcium for predicting the extent of angiographic coronary artery disease: comparison with cardiac risk factors and radionuclide perfusion imaging. J Am Coll Cardiol. 1999;34(3):777-86.
10. Gussenhoven EJ, Essed CE, Lancée CT, Mastik F, Frietman P, van Egmond FC, et al. Arterial wall characteristics determined by intravascular ultrasound imaging: an in vitro study. J Am Coll Cardiol. 1989;14(4):947-52.
11. Stary HC, Chandler AB, Dinsmore RE, Fuster V, Glagov S, Insull W Jr, et al. A definition of advanced types of atherosclerotic lesions and a histological classification of atherosclerosis. A report from the Committee on Vascular Lesions of the Council on Arteriosclerosis, American Heart Association. Circulation. 1995;92(5):1355-74.
12. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M Jr, Detrano R. Quantification of coronary artery calcium using ultrafast computed tomography. J Am Coll Cardiol. 1990;15(4):827-32.
13. Knez A, Becker C, Becker A, Leber A, White C, Reiser M, et al. Determination of coronary calcium with multi-slice spiral computed tomography: a comparative study with electron-beam CT. Int J Cardiovasc Imaging. 2002;18(4):295-303.
14. Raggi P, Callister TQ, Cooil B, He ZX, Lippolis NJ, Russo DJ, et al. Identification of patients at increased risk of first unheralded acute myocardial infarction by electron-beam computed tomography. Circulation. 2000;101(8):850-5.
15. Haberl R, Becker A, Leber A, Knez A, Becker C, Lang C, et al. Correlation of coronary calcification and angiographically documented stenoses in patients with suspected coronary artery disease: results of 1,764 patients. J Am Coll Cardiol. 2001;37(2):451-7.
16. Budoff MJ, Diamond GA, Raggi P, Arad Y, Guerci AD, Callister TQ, et al. Continuous probabilistic prediction of angiographically significant coronary artery disease using electron beam tomography. Circulation. 2002;105(15):1791-6.
17. Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31-41.
18. Gottdiener JS, Bednarz J, Devereux R, Gardin J, Klein A, Manning WJ, et al. American Society of Echocardiography. American Society of Echocardiography recommendations for use of echocardiography in clinical trials. J Am Soc Echocardiogr. 2004;17(10):1086-119.
19. Greenland P, Bonow RO, Brundage BH, Budoff MJ, Eisenberg MJ, Grundy SM, et al. American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography); Society of Atherosclerosis Imaging and Prevention; Society of Cardiovascular Computed Tomography. ACCF/AHA 2007 clinical expert consensus document on coronary artery calcium scoring by computed tomography in global cardiovascular risk assessment and in evaluation of patients with chest pain: a report of the American College of Cardiology Foundation Clinical Expert Consensus Task Force (ACCF/AHA Writing Committee to Update the 2000 Expert Consensus Document on Electron Beam Computed Tomography) developed in collaboration with the Society of Atherosclerosis Imaging and Prevention and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol. 2007;49(3):378-402.
20. Alexopoulos N, Raggi P. Calcification in atherosclerosis. Nat Rev Cardiol. 2009;6(11):681-8.
21. Becker A, Leber A, White CW, Becker C, Reiser MF, Knez A. Multislice computed tomography for determination of coronary artery disease in a symptomatic patient population. Int J Cardiovasc Imaging. 2007;23(3):361-7.
References
not included. However, many published studies have been based on the Agatston method and we continue to use this method in clinical practice.
AcknowledgementsThe authors wish to thank Dr İbrahim H. Tanboğa for his
constructive comments and assistance to statistical analysis.
Author contributionsConception and design of the research: Gökdeniz T,
Kalaycıoğlu E, Aykan AÇ, Boyacı F, Turan T, Gül I, Çavuşoğlu G; Acquisition of data: Gökdeniz T, Kalaycıoğlu E, Aykan AÇ, Boyacı F, Turan T, Gül I, Çavuşoğlu G, Dursun I; Analysis and interpretation of the data: Aykan AÇ, Gül I; Statistical analysis:
Gökdeniz T, Gül I; Writing of the manuscript: Gökdeniz T, Kalaycıoğlu E, Aykan AÇ; Critical revision of the manuscript for intellectual content: Kalaycıoğlu E.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any thesis or dissertation work.
126

Original Article
Gökdeniz et al.Severity or complexity of CAD and total CAC score
Arq Bras Cardiol. 2014; 102(2):120-127
22. Berman DS, Wong ND, Gransar H, Miranda-Peats R, Dahlbeck J, Hayes SW, et al. Relationship between stress-induced myocardial ischemia and atherosclerosis measured by coronary calcium tomography. J Am Coll Cardiol. 2004;44(4):923-30.
23. Stähli BE, Bonassin F, Goetti R, Küest SM, Frank M, Altwegg LA, et al. Coronary computed tomography angiography indicates complexity of percutaneous coronary interventions. J Invasive Cardiol. 2012;24(5):196-201.
24. Simons DB, Schwartz RS, Edwards WD, Sheedy PF, Breen JF, Rumberger JA. Noninvasive definition of anatomic coronary artery disease by ultrafast computed tomographic scanning: a quantitative pathologic comparison study. J Am Coll Cardiol. 1992;20(5):1118-26.
25. Rumberger JA, Simons DB, Fitzpatrick LA, Sheedy PF, Schwartz RS. Coronary artery calcium area by electron-beam computed tomography and coronary atherosclerotic plaque area: a histopathologic correlative study. Circulation. 1995;92(8):2157-62.
26. Srivatsa S, Holmes D Jr. The histopathology of angiographic chronic total coronary artery occlusions ñ changes in neovascular pattern and intimal
plaque composition associated with progressive occlusion duration. J Invasive Cardiol. 1997;9(4):294-301.
27. Popma JJ, Dick RJ, Haudenschild CC, Topol EJ, Ellis SG. Atherectomy of right coronary ostial stenoses: initial and long-term results, technical features and histologic findings. Am J Cardiol. 1991;67(5):431-3.
28. Lavi S, Bae JH, Rihal CS, Prasad A, Barsness GW, Lennon RJ, et al. Segmental coronary endothelial dysfunction in patients with minimal atherosclerosis is associated with necrotic core plaques. Heart. 2009;95(18):1525-30.
29. Kullo IJ, Malik AR, Bielak LF, Sheedy PF 2nd, Turner ST, Peyser PA. Brachial artery diameter and vasodilator response to nitroglycerine, but not flow-mediated dilatation, are associated with the presence and quantity of coronary arterycalcium in asymptomatic adults. Clin Sci (Lond). 2007;112(3):175-82.
30. Sekiya M, Mukai M, Suzuki M, Ohtani T, Abe M, Matsuoka H, et al. Clinical significance of the calcification of coronary arteries in patients with angiographically normal coronary arteries. Angiology. 1992;43(5):401-7.
127

Original Article
Myocardial Revascularization in Dyalitic Patients: In-Hospital Period EvaluationMatheus Miranda1, Nelson Américo Hossne Jr.1, João Nelson Rodrigues Branco1, Guilherme Flora Vargas1, José Honório de Almeida Palma da Fonseca1, José Osmar Medina de Abreu Pestana1, Yara Juliano2, Enio Buffolo1
Escola Paulista de Medicina (EPM), Universidade Federal de São Paulo (Unifesp)1; Universidade de Santo Amaro2, São Paulo, SP - Brazil
Mailing Address: Matheus Miranda •Rua Borges Lagoa, 1080, conj. 701, Vila Clementino. Postal Code 04038-002, São Paulo, SP - BrazilE-mail: [email protected], [email protected] received August 22, 2013; revised manuscript September 25, 2013; accepted September 26, 2013.
DOI: 10.5935/abc.20130231
Abstract
Background: Coronary artery bypass grafting currently is the best treatment for dialytic patients with multivessel coronary disease, but hospital morbidity and mortality related to procedure is still high.
Objective: Evaluate results and in-hospital outcomes of coronary artery bypass grafting in dialytic patients.
Methods: Retrospective unicentric study including 50 consecutive and not selected dialytic patients, who underwent coronary artery bypass grafting in a tertiary university hospital from 2007 to 2012.
Results: High prevalence of cardiovascular risk factors was observed (100% hypertensive, 68% diabetic and 40% dyslipidemic). There was no intra-operative death and 60% of the procedures were performed off-pump. There were seven (14%) in-hospital deaths. Postoperative infection, previous heart failure, cardiopulmonary bypass, abnormal ventricular function and surgical re-exploration were associated with increased mortality.
Conclusion: Coronary artery bypass grafting is feasible to dialytic patients although high in-hospital morbidity and mortality. It is necessary better understanding about metabolic aspects to plan adequate interventions. (Arq Bras Cardiol. 2014; 102(2):128-133)
Keywords: Myocardial Revascularization; Patients; Dialysis; Hospitalization.
IntroductionChronic renal failure (CRF) is an independent risk
factor for the development of coronapathies and its complications, and injury severity level is inversely proportional to the glomerular1,2 filtration rate, which makes ischemic cardiovascular diseases the main mortality cause in this group of patients2. In addition to uremia, other factors such as bad quality of distal coronary bed, hyperhomocysteinemia, increased calcium-phosphorus product, oxidative stress, chronic inflammation and exacerbated atherosclerosis are associated with the severity of coronary disease3-6. Coronary artery bypass grafting (CABG) has shown better long-term survival and lower risk of myocardial infarction and cardiovascular death when compared to coronary angioplasty with stent in patients with dialytic chronic kidney failure7-9, but surgery still has high morbidity and mortality in these patients10.
ObjectiveAnalyze CABG results in dialytic patients with chronic
kidney failure, as well as in-hospital complications, in order to identify its causes and define proper interventions.
MethodsWe analyzed the medical records of 50 chronic renal
failure on dialysis (hemodialysis), consecutive, non-selected patients enrolled in retrospective study, undergoing coronary artery bypass grafting at a public tertiary university hospital from 2007 to 2012. Patients with other concomitant procedures (valve, carotid, aortic surgery, etc.) were excluded from this study. We investigated demographic and clinical characteristics, intraoperative data and postoperative complications during the hospitalization period of these patients. The calculation of preoperative risk was performed by European System for Cardiac Operative Risk Evaluation II (EuroSCORE II)11. Subsequently, two subgroups were created ("deaths" and "survivors") in order to identify factors that indicate higher in-hospital mortality. The study was approved by the local research ethics committee.
Surgical techniqueSurgical indication for CABG was based on American
and European guidelines12,13. Surgical planning was carried out based on injuries found on cineangiocoronariography
128
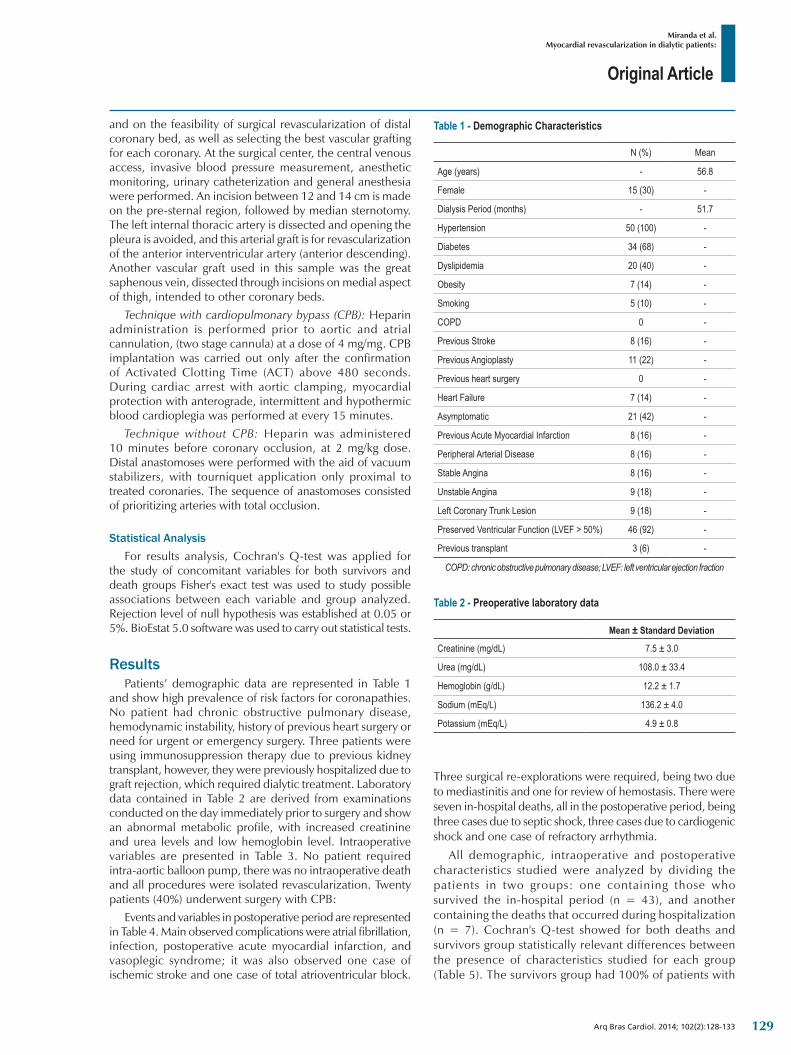
Original Article
Miranda et al.Myocardial revascularization in dialytic patients:
Arq Bras Cardiol. 2014; 102(2):128-133
and on the feasibility of surgical revascularization of distal coronary bed, as well as selecting the best vascular grafting for each coronary. At the surgical center, the central venous access, invasive blood pressure measurement, anesthetic monitoring, urinary catheterization and general anesthesia were performed. An incision between 12 and 14 cm is made on the pre-sternal region, followed by median sternotomy. The left internal thoracic artery is dissected and opening the pleura is avoided, and this arterial graft is for revascularization of the anterior interventricular artery (anterior descending). Another vascular graft used in this sample was the great saphenous vein, dissected through incisions on medial aspect of thigh, intended to other coronary beds.
Technique with cardiopulmonary bypass (CPB): Heparin administration is performed prior to aortic and atrial cannulation, (two stage cannula) at a dose of 4 mg/mg. CPB implantation was carried out only after the confirmation of Activated Clotting Time (ACT) above 480 seconds. During cardiac arrest with aortic clamping, myocardial protection with anterograde, intermittent and hypothermic blood cardioplegia was performed at every 15 minutes.
Technique without CPB: Heparin was administered 10 minutes before coronary occlusion, at 2 mg/kg dose. Distal anastomoses were performed with the aid of vacuum stabilizers, with tourniquet application only proximal to treated coronaries. The sequence of anastomoses consisted of prioritizing arteries with total occlusion.
Statistical AnalysisFor results analysis, Cochran's Q-test was applied for
the study of concomitant variables for both survivors and death groups Fisher's exact test was used to study possible associations between each variable and group analyzed. Rejection level of null hypothesis was established at 0.05 or 5%. BioEstat 5.0 software was used to carry out statistical tests.
ResultsPatients’ demographic data are represented in Table 1
and show high prevalence of risk factors for coronapathies. No patient had chronic obstructive pulmonary disease, hemodynamic instability, history of previous heart surgery or need for urgent or emergency surgery. Three patients were using immunosuppression therapy due to previous kidney transplant, however, they were previously hospitalized due to graft rejection, which required dialytic treatment. Laboratory data contained in Table 2 are derived from examinations conducted on the day immediately prior to surgery and show an abnormal metabolic profile, with increased creatinine and urea levels and low hemoglobin level. Intraoperative variables are presented in Table 3. No patient required intra-aortic balloon pump, there was no intraoperative death and all procedures were isolated revascularization. Twenty patients (40%) underwent surgery with CPB:
Events and variables in postoperative period are represented in Table 4. Main observed complications were atrial fibrillation, infection, postoperative acute myocardial infarction, and vasoplegic syndrome; it was also observed one case of ischemic stroke and one case of total atrioventricular block.
Three surgical re-explorations were required, being two due to mediastinitis and one for review of hemostasis. There were seven in-hospital deaths, all in the postoperative period, being three cases due to septic shock, three cases due to cardiogenic shock and one case of refractory arrhythmia.
All demographic, intraoperative and postoperative characteristics studied were analyzed by dividing the patients in two groups: one containing those who survived the in-hospital period (n = 43), and another containing the deaths that occurred during hospitalization (n = 7). Cochran's Q-test showed for both deaths and survivors group statistically relevant differences between the presence of characteristics studied for each group (Table 5). The survivors group had 100% of patients with
Table 1 ‑ Demographic Characteristics
N (%) Mean
Age (years) - 56.8
Female 15 (30) -
Dialysis Period (months) - 51.7
Hypertension 50 (100) -
Diabetes 34 (68) -
Dyslipidemia 20 (40) -
Obesity 7 (14) -
Smoking 5 (10) -
COPD 0 -
Previous Stroke 8 (16) -
Previous Angioplasty 11 (22) -
Previous heart surgery 0 -
Heart Failure 7 (14) -
Asymptomatic 21 (42) -
Previous Acute Myocardial Infarction 8 (16) -
Peripheral Arterial Disease 8 (16) -
Stable Angina 8 (16) -
Unstable Angina 9 (18) -
Left Coronary Trunk Lesion 9 (18) -
Preserved Ventricular Function (LVEF > 50%) 46 (92) -
Previous transplant 3 (6) -
COPD: chronic obstructive pulmonary disease; LVEF: left ventricular ejection fraction
Table 2 ‑ Preoperative laboratory data
Mean ± Standard Deviation
Creatinine (mg/dL) 7.5 ± 3.0
Urea (mg/dL) 108.0 ± 33.4
Hemoglobin (g/dL) 12.2 ± 1.7
Sodium (mEq/L) 136.2 ± 4.0
Potassium (mEq/L) 4.9 ± 0.8
129
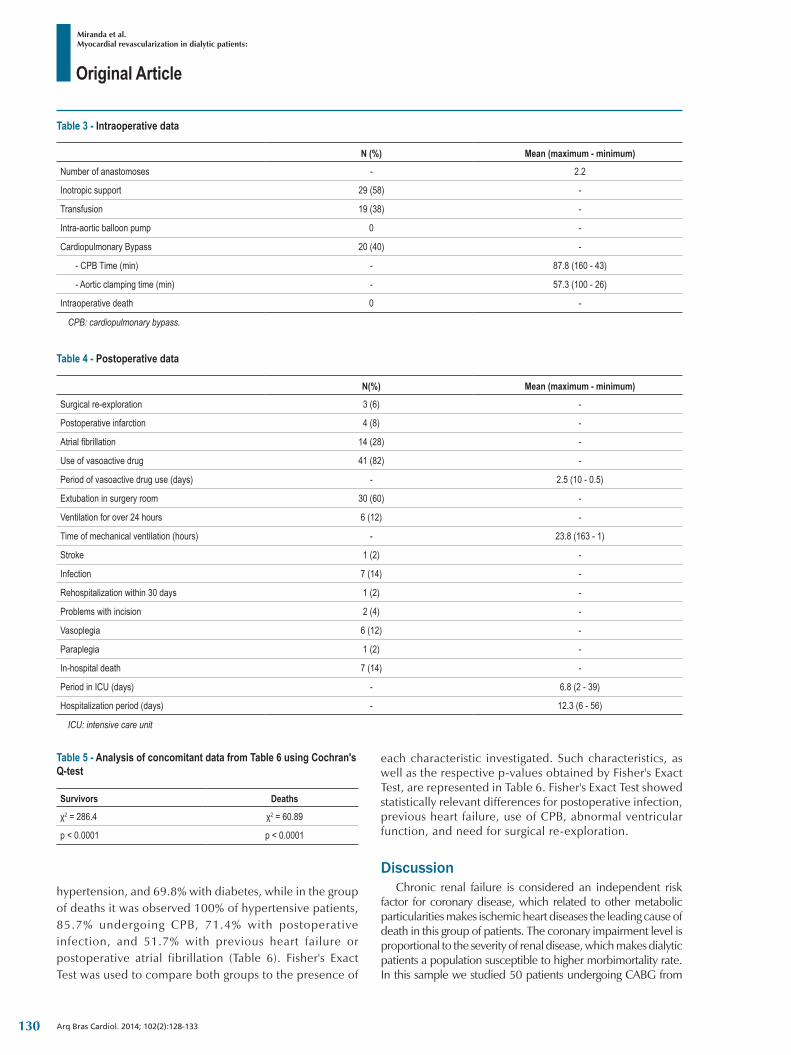
Original Article
Miranda et al.Myocardial revascularization in dialytic patients:
Arq Bras Cardiol. 2014; 102(2):128-133
Table 3 ‑ Intraoperative data
N (%) Mean (maximum ‑ minimum)
Number of anastomoses - 2.2
Inotropic support 29 (58) -
Transfusion 19 (38) -
Intra-aortic balloon pump 0 -
Cardiopulmonary Bypass 20 (40) -
- CPB Time (min) - 87.8 (160 - 43)
- Aortic clamping time (min) - 57.3 (100 - 26)
Intraoperative death 0 -
CPB: cardiopulmonary bypass.
Table 4 ‑ Postoperative data
N(%) Mean (maximum ‑ minimum)
Surgical re-exploration 3 (6) -
Postoperative infarction 4 (8) -
Atrial fibrillation 14 (28) -
Use of vasoactive drug 41 (82) -
Period of vasoactive drug use (days) - 2.5 (10 - 0.5)
Extubation in surgery room 30 (60) -
Ventilation for over 24 hours 6 (12) -
Time of mechanical ventilation (hours) - 23.8 (163 - 1)
Stroke 1 (2) -
Infection 7 (14) -
Rehospitalization within 30 days 1 (2) -
Problems with incision 2 (4) -
Vasoplegia 6 (12) -
Paraplegia 1 (2) -
In-hospital death 7 (14) -
Period in ICU (days) - 6.8 (2 - 39)
Hospitalization period (days) - 12.3 (6 - 56)
ICU: intensive care unit
Table 5 ‑ Analysis of concomitant data from Table 6 using Cochran's Q‑test
Survivors Deaths
χ2 = 286.4 χ2 = 60.89
p < 0.0001 p < 0.0001
hypertension, and 69.8% with diabetes, while in the group of deaths it was observed 100% of hypertensive patients, 85.7% undergoing CPB, 71.4% with postoperative infection, and 51.7% with previous heart failure or postoperative atrial fibrillation (Table 6). Fisher's Exact Test was used to compare both groups to the presence of
each characteristic investigated. Such characteristics, as well as the respective p-values obtained by Fisher's Exact Test, are represented in Table 6. Fisher's Exact Test showed statistically relevant differences for postoperative infection, previous heart failure, use of CPB, abnormal ventricular function, and need for surgical re-exploration.
DiscussionChronic renal failure is considered an independent risk
factor for coronary disease, which related to other metabolic particularities makes ischemic heart diseases the leading cause of death in this group of patients. The coronary impairment level is proportional to the severity of renal disease, which makes dialytic patients a population susceptible to higher morbimortality rate. In this sample we studied 50 patients undergoing CABG from
130
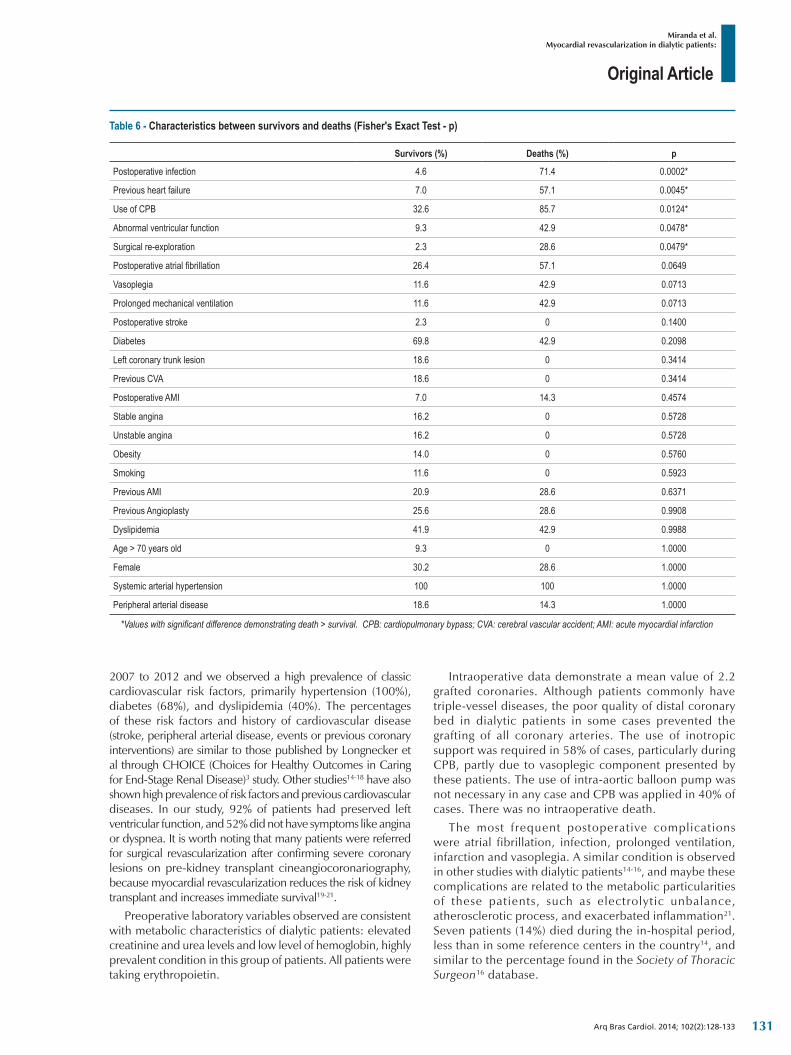
Original Article
Miranda et al.Myocardial revascularization in dialytic patients:
Arq Bras Cardiol. 2014; 102(2):128-133
Table 6 - Characteristics between survivors and deaths (Fisher's Exact Test - p)
Survivors (%) Deaths (%) p
Postoperative infection 4.6 71.4 0.0002*
Previous heart failure 7.0 57.1 0.0045*
Use of CPB 32.6 85.7 0.0124*
Abnormal ventricular function 9.3 42.9 0.0478*
Surgical re-exploration 2.3 28.6 0.0479*
Postoperative atrial fibrillation 26.4 57.1 0.0649
Vasoplegia 11.6 42.9 0.0713
Prolonged mechanical ventilation 11.6 42.9 0.0713
Postoperative stroke 2.3 0 0.1400
Diabetes 69.8 42.9 0.2098
Left coronary trunk lesion 18.6 0 0.3414
Previous CVA 18.6 0 0.3414
Postoperative AMI 7.0 14.3 0.4574
Stable angina 16.2 0 0.5728
Unstable angina 16.2 0 0.5728
Obesity 14.0 0 0.5760
Smoking 11.6 0 0.5923
Previous AMI 20.9 28.6 0.6371
Previous Angioplasty 25.6 28.6 0.9908
Dyslipidemia 41.9 42.9 0.9988
Age > 70 years old 9.3 0 1.0000
Female 30.2 28.6 1.0000
Systemic arterial hypertension 100 100 1.0000
Peripheral arterial disease 18.6 14.3 1.0000
*Values with significant difference demonstrating death > survival. CPB: cardiopulmonary bypass; CVA: cerebral vascular accident; AMI: acute myocardial infarction
2007 to 2012 and we observed a high prevalence of classic cardiovascular risk factors, primarily hypertension (100%), diabetes (68%), and dyslipidemia (40%). The percentages of these risk factors and history of cardiovascular disease (stroke, peripheral arterial disease, events or previous coronary interventions) are similar to those published by Longnecker et al through CHOICE (Choices for Healthy Outcomes in Caring for End-Stage Renal Disease)3 study. Other studies14-18 have also shown high prevalence of risk factors and previous cardiovascular diseases. In our study, 92% of patients had preserved left ventricular function, and 52% did not have symptoms like angina or dyspnea. It is worth noting that many patients were referred for surgical revascularization after confirming severe coronary lesions on pre-kidney transplant cineangiocoronariography, because myocardial revascularization reduces the risk of kidney transplant and increases immediate survival19-21.
Preoperative laboratory variables observed are consistent with metabolic characteristics of dialytic patients: elevated creatinine and urea levels and low level of hemoglobin, highly prevalent condition in this group of patients. All patients were taking erythropoietin.
Intraoperative data demonstrate a mean value of 2.2 grafted coronaries. Although patients commonly have triple-vessel diseases, the poor quality of distal coronary bed in dialytic patients in some cases prevented the grafting of all coronary arteries. The use of inotropic support was required in 58% of cases, particularly during CPB, partly due to vasoplegic component presented by these patients. The use of intra-aortic balloon pump was not necessary in any case and CPB was applied in 40% of cases. There was no intraoperative death.
The most frequent postoperative complications were atrial fibrillation, infection, prolonged ventilation, infarction and vasoplegia. A similar condition is observed in other studies with dialytic patients14-16, and maybe these complications are related to the metabolic particularities of these patients, such as electrolytic unbalance, atherosclerotic process, and exacerbated inflammation21. Seven patients (14%) died during the in-hospital period, less than in some reference centers in the country14, and similar to the percentage found in the Society of Thoracic Surgeon16 database.
131

Original Article
Miranda et al.Myocardial revascularization in dialytic patients:
Arq Bras Cardiol. 2014; 102(2):128-133
1. Ix JH, Shlipak MG, Liu HH, Schiller NB, Whooley MA. Association between renal insufficiency and inducible ischemia in patients with coronary artery disease: The Heart and Soul Study. J Am Soc Nephrol. 2003;14(12):3233-9. Erratum in J Am Soc Nephrol. 2004;15(2):508.
2. US Renal Data System. USRDS 2007 Annual Data report: atlas of end-stage renal disease in the United States. Am J Kidney Dis. 2008;51:S1-7.
3. Longenecker JC, Coresh J, Powe NR, Levey AS, Fink NE, Martin A, et al. Traditional cardiovascular disease risk factors in dialysis patients compared with the general population: The CHOICE Study. J Am Soc Nephrol. 2002;13(7):1918-27.
4. Lindner A, Charra B, Sherrard J, Scriber B. Accelerated atherosclerosis in prolonged maintenance hemodialysis. N Engl J Med. 1974;290(13):697-701.
5. Sarnak AC, Levey AS, Schoolwerth AC, Coresh J, Culleton B, Hamm LL, et al; American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Kidney disease as a risk factor for development of cardiovascular disease: a statement from the American Heart Association Councils on Kidney in Cardiovascular Disease, High Blood Pressure Research, Clinical Cardiology, and Epidemiology and Prevention. Circulation. 2003;108(17):2154-69.
6. Zoccali C, Mallamaci F, Tripepi G. Novel cardiovascular risk factors in end-stage renal disease. J Am Soc Nephrol. 2004;15 Suppl 1:S77-80.
7. Rinehart AL, Herzog CA, Collins AJ, Flack JM, Ma JZ, Opsahl JA. A comparison of coronary angioplasty and coronary artery bypass grafting outcomes in chronic dialysis patients. Am J Kidney Dis. 1995;25(2):281-90.
8. Herzog CA, Ma JZ, Collins AJ. Comparative survival of dialysis patients in the United States after coronary angioplasty, coronary artery stenting, and coronary artery bypass surgery and impact of diabetes. Circulation. 2002;106(17):2207-11.
9. Hannan EL, Racz MJ, Walford G, Jones RH, Ryan TJ, Bennett E, et al. Long term outcomes of coronary artery bypass grafting versus stent implantation. N Engl J Med. 2005;352(21):2174-83.
10. Wong D, Thompson G, Buth K, Sullivan J, Ali I. Angiographic coronary diffuseness and outcomes in dialysis patients undergoing coronary artery bypass grafting surgery. Eur J Cardiothorac Surg. 2003;24(3):388-92.
11. Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, et al. Euro SCORE II. Eur J Cardiothoracic Surg. 2012;41(4):734-44.
12. Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, et al. Guidelines on myocardial revascularization: the Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2010;31(20):2501-55.
13. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, et al. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: Executive Summary: A Report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124(23):2610-42. Erratum in: Circulation. 2011;124(25):e956. Circulation. 2012;126(7):e105.
14. Barbosa RR, Cestari PF, Capeletti JT, Peres GM, Ibañez TL, da Silva PV, et al. Impacto da disfunção renal na evolução intra-hospitalar após cirurgia de revascularização miocárdica. Arq Bras Cardiol. 2011;97(3):249-53.
15. Horai T, Fukui T, Tabata M, Takanashi S. Early and mid-term results of off-pump coronary artery bypass grafting in patients with end stage renal disease: surgical outcomes after achievement of complete revascularization. Interact Cardiovasc Thorac Surg. 2008;7(2):218-21.
16. Cooper WA, O’Brien SM, Thourani VH, Guyton RA, Bridges CR, Szczech LA, et al. Impact of renal dysfunction on outcomes of coronaryartery bypass surgery: results from the Society of Thoracic Surgeons National Adult Cardiac Database. Circulation. 2006;113(8):1063-70.
17. Milani R, Brofman PR, Souza JA, Barboza L, Guimarães MR, Barbosa A, et al. OPCAB in patients on hemodialysis. Rev Bras Cir Cardiovasc. 2007;22(1):104-8.
References
After comparative analysis between groups of survivors and deaths, we observed a statistically relevant difference between these groups regarding the following factors: postoperative infection, heart failure, use of CPB, abnormal ventricular function, and necessity of surgical re-exploration. Possibly these factors are related to a higher mortality rate during the in-hospital period, however, due to the limited number of patients, primarily the deaths group, caution is needed when interpreting the data.
The frequent exclusion of this group of patients from large cardiac studies perhaps even collaborate to the difficulty of selecting the best approach and to results still modest when compared to patients with preserved kidney function.
ConclusionCABG in dialytic patients with chronic renal failure
has high hospital morbimortality, and must consider the particular metabolic aspects in this group of patients for better orientation of approach, perioperatively. Factors as postoperative infection, previous heart failure, use of CPB, abnormal ventricular function, and necessity of surgical re-exploration may be related to a higher mortality rate during hospitalization. CABG without CBP can be a more satisfying alternative for treating these patients.
Author contributionsConception and design of the research: Miranda M, Hossne
Jr. NA, Branco JNR, Vargas GF, Fonseca JHAP, Pestana JOMA, Juliano Y, Buffolo E; Acquisition of data: Miranda M, Vargas GF; Analysis and interpretation of the data: Miranda M, Fonseca JHAP, Juliano Y, Buffolo E; Statistical analysis: Juliano Y; Writing of the manuscript: Miranda M, Hossne Jr. NA, Branco JNR, Pestana JOMA, Buffolo E; Critical revision of the manuscript for intellectual content: Hossne Jr. NA, Branco JNR, Vargas GF, Fonseca JHAP, Pestana JOMA, Juliano Y, Buffolo E.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This study is not associated with any post-graduation program.
132

Original Article
Miranda et al.Myocardial revascularization in dialytic patients:
Arq Bras Cardiol. 2014; 102(2):128-133
18. Manske CL, Wang Y, Rector T, Wilson RF, White CW. Coronary revascularization in insulin-dependent diabetic patients with chronic renal failure. Lancet. 1992;340(8826):998-1002.
19. Gowdak LH, Paula FJ, Giorgi DM, Vieira ML, Krieger EM, Lima JJ. [Cardiovascular disease and risk factors in candidates for renal transplantation]. Arq Bras Cardiol. 2005;84(2):156-60.
20. Delgado DS, Gerola LR, Hossne NA Jr, Branco JN, Buffolo E. Myocardial revascularization in renal transplant patients. Arq Bras Cardiol. 2002;79(5):476-83.
21. Oberg BP, McMenamin E, Lucas FL, McMonagle E, Morrow J, IkizlerTA, et al. Increased prevalence of oxidant stress and inflammation in patients with moderate to severe chronic kidney disease. Kidney Int. 2004;65(3):1009-1.
133
Original Article
Coronary Flow Velocity Reserve during Dobutamine Stress EchocardiographyJosé Sebastião de Abreu1-3, José Wellington Oliveira Lima4, Tereza Cristina Pinheiro Diógenes1, 2, Jordana Magalhães Siqueira3, Nayara Lima Pimentel3, Pedro Sabino Gomes Neto3, Marília Esther Benevides de Abreu1, 2, José Nogueira Paes Júnior1, 2 Prontocárdio - Pronto Atendimento Cardiológico SC Ltda1; Clinicárdio - JAC Métodos Diagnósticos SS2; Faculdade de Medicina da Universidade Federal do Ceará3; Universidade Estadual do Ceará4, Fortaleza, CE – Brazil
Mailing Address: José Sebastiao de Abreu • Rua Dr. José Lourenço, 500/700, Meireles. Postal Code 60115-280, Fortaleza, CE - BrazilE-mail: [email protected], [email protected] received May 21, 2013; revised manuscript received August 11, 2013; accepted August 20, 2013.
DOI: 10.5935/abc.20130242
Abstract
Background: A coronary flow velocity reserve (CFVR) ≥ 2 is adequate to infer a favorable prognosis or the absence of significant coronary artery disease.
Objective: To identify parameters which are relevant to obtain CFVR (adequate or inadequate) in the left anterior descending coronary artery (LAD) during dobutamine stress echocardiography (DSE).
Methods: 100 patients referred for detection of myocardial ischemia by DSE were evaluated; they were instructed to discontinue the use of β-blockers 72 hours prior to the test. CFVR was calculated as a ratio of the diastolic peak velocity (cm/s) (DPV) on DSE (DPV-DSE) to baseline DPV at rest (DPV-Rest). In group I, CFVR was < 2 and, in group II, CFVR was ≥ 2. The Fisher’s exact test and Student’s t test were used for the statistical analyses. P values < 0.05 were considered statistically significant.
Results: At rest, the time (in seconds) to obtain Doppler in LAD in groups I and II was not different (53±31 vs. 45±32; p=0.23). During DSE, LAD was recorded in 92 patients. Group I patients were older (65.9±9.3 vs. 61.2±10.8 years; p=0.04), had lower ejection fraction (61±10 vs. 66±6%; p=0.005), higher DPV-Rest (36.81±08 vs. 25.63 ± 06cm/s; p<0.0001) and lower CFVR (1.67 ± 0.24 vs. 2.53 ± 0.57; p<0.0001), but no difference was observed regarding DPV-DSE (61.40±16 vs. 64.23±16cm/s; p=0.42). β-blocker discontinuation was associated with a 4-fold higher chance of a CFVR < 2 (OR= 4; 95% CI [1.171-13.63], p=0.027).
Conclusion: DPV-Rest was the main parameter to determine an adequate CFVR. β-blocker discontinuation was significantly associated with inadequate CFVR. The high feasibility and the time to record the LAD corroborate the use of this methodology.(Arq Bras Cardiol. 2014; 102(2):134-142)
Keywords: Coronary artery disease; Echocardiography, stress / methods; Coronary flow velocity reserve.
IntroductionPharmacological-stress echocardiography is a safe and
accurate noninvasive method for the evaluation of coronary artery disease (CAD)1-4. It has been verified that enhancement of the diastolic component of the flow determined by dobutamine, dipyridamole or adenosine may be used for the calculation of the coronary flow velocity reserve (CFVR)5-19.
Measurement o f the CFVR by t rans thorac ic echocardiography has already been validated for the assessment of the right and left coronary systems15,16,20, and has become an important tool in the functional analysis of
the anterior descending coronary artery (LAD). Studies have demonstrated that a CFVR ≥ 2 is adequate and relevant to infer the absence of significant coronary occlusion, and is correlated with a favorable prognosis in the context of the coronary artery analyzed7,10-12,19,21-27. Several publications have shown that the authors succeed in recording the LAD flow in approximately 90% of cases; this allows high feasibility of the measurement of CFVR by echocardiography, thus corroborating the use of a safe, validated and reproducible method in the clinical practice5-13.
It has been verified that the invasive assessment of CFVR may be influenced by factors such as age, blood pressure, heart rate, left ventricular hypertrophy, degree of coronary impairment, and others28.
Few data are available in the literature regarding the assessment of the functional status of the LAD using dobutamine transthoracic echocardiography. However, regardless of the drug used, the CFVR calculation may be affected for different reasons. Thus, the objective of this study
134

Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
was to identify relevant parameters to obtain an adequate (≥ 2) or inadequate CFVR in the LAD during dobutamine stress echocardiography (DSE).
Methods
Study patientsThis is a cross-sectional study of 100 patients referred by
their physicians for the investigation of myocardial ischemia by means of DSE. The patients had been previously instructed to discontinue the use of betablockers (β-blocker) 72 hours before undergoing the test.
After history taking, the presence of risk factors for CAD and of possible contraindications for DSE was verified. Arterial hypertension29 was defined as a systolic blood pressure > 140mmHg or diastolic blood pressure > 90mmHg. Diabetes mellitus30 was confirmed by a fasting plasma glucose > 126mg/dL. Dyslipidemia31 was considered when total cholesterol > 220mg/dL. The use of antihypertensive drugs, oral hypoglycemic agents, insulin or lipid-lowering drugs was also considered a risk factor for CAD. Patients who had not quit smoking for less than one year prior to the study were considered smokers.
Exclusion criteria were uncontrolled hypertension, unstable angina, congestive heart failure, recent myocardial infarction (MI) (occurring less than one month prior to DSE), significant heart valve disease, prostate disease, or glaucoma with contraindication for the use of atropine, and non-sinus rhythm.
All patients were given information on the risks and objectives of the test, which was only performed after their giving verbal consent.
Dobutamine Stress EchocardiographyThe Vivid 7 (GE Healthcare) ultrasound system with
second-harmonic imaging and the M4S multifrequency transducer with frequency ranging from 2 to 4MHz were used. The left ventricle (LV) was visualized in the apical views (4 and 2-chamber) and parasternal views (long and short axes) at rest and during the use of dobutamine at the doses of 10 (low dose), 20, 30, up to 40µg/kg/min at 3-min intervals; the rest, low-dose, peak and recovery images were compared in a four-division screen. Atropine could be associated after the second stage at up-titration doses of 0.25mg, up to the maximum cumulative dose of 2mg, with the purpose of terminating the test. DSE was considered terminated when a target heart rate (HR) higher than 85% of the maximum HR (220 – age) was achieved, and/or myocardial ischemia had been determined. Ischemia was considered in the presence of a report of typical angina, new wall motion abnormality, or worsening of a pre-existing wall motion abnormality (except from akinesia to dyskinesia). Tests should be interrupted in the presence of intolerance to medication, hypertensive peak (blood pressure > 230 x 120 mmHg) or cardiac arrhythmia3,32.
The LV was divided into 16 segments. For the wall motion scoring of each segment, the following patterns were observed: normal = 1; hypokinesia = 2; akinesia = 3; or dyskinesia = 4. For the calculation of the segmental wall motion score index (SWMSI), the points obtained were divided by 161,5,6,10,12.
Anterior Descending Coronary Artery and Coronary Flow Reserve Velocity Recordings
In the same left lateral position in which DSE was performed, the LAD was recorded at its mid-distal portion with a specific pre-established preset. From the low parasternal long axis recording, with clockwise rotation of the transducer, disappearance of the right ventricle was determined, with visualization of the interventricular sulcus, region in which the LAD imaging would be obtained. Other options were visualization from the position of three modified chambers or two concomitant chambers, with slight angle adjustments or transducer rotation.
Using a small color-Doppler box with Nyquist limit of approximately 20 cm/s, the LAD was identified as a tubular image in which the greatest possible stretching and extension were determined, as well as the lowest angle with the Doppler cursor, whose sample volume measured 2mm. Using pulsed Doppler, the flow assessed was characterized by the biphasic spectrum with diastolic predominance, and antegrade curves above baseline were recorded. Initially, the Doppler velocity scale was limited to 80 cm/s and could be amplified during DSE, thus permitting caption of the subsequent increases in the velocities of the Doppler curves.
In the electrocardiogram-gated Doppler of the LAD, diastolic peak velocities (DPV) were recorded, and three spectral curves, not necessarily continuous, but with good quality and higher velocities were selected at rest and during stress. The CFVR was obtained by dividing DPV (mean of three peaks) found during DSE by the baseline DPV (mean of three peaks) recorded at rest6-8,10,12,15,20,22.
Study protocolAfter echocardiographic assessment for routine
measurements, the LAD was studied. Immediately after placement of the color box in the ultrasound scanner screen, the time spent to obtain the LAD recording by color and pulsed Doppler was counted. Only cases with recordings of Doppler spectral curves obtained in less than 180 seconds would remain in the study. Using the same transducer, visualization of two-dimensional LV imaging was alternated with Doppler of the LAD. Thus, the DSE four-division screen was filled in the different stages, concomitantly with the different DPV measurements until termination of the test. As soon as the test was terminated, the DSE result was defined and the CFVR was calculated. Patients with a CFVR < 2 comprised group I (GI) and those with an adequate CFVR (≥ 2) comprised group II (GII). SWMSI was calculated in a further stage.
Statistical AnalysisThe proportion of individuals with an adequate coronary
reserve was compared in the different categories of one same independent variable using the Fisher’s exact test. Likewise, the distributions of continuous independent variables, according to the presence or absence of an adequate coronary reserve, were compared using the Student’s t test.
Univariate logistic regression models between independent variables and coronary reserve (adequate and inadequate) were made, and variables with a p value < 0.250 were
135

Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
included in the multivariate models. The objective of the multivariate analysis was to describe the relationship between β-blocker discontinuation and coronary reserve, adjusted for potential confounders.
Results
FeasibilityOf the 110 cases initially assessed, 10 were excluded
because the time for LAD recording by Doppler exceeded 180 seconds. Consequently, the feasibility for recordings at rest to be obtained within the established time was 91%.
DSEs were performed uneventfully, and DPV could be verified in 92% (92/100) of patients. Of the eight patients not assessed during DSE, the LV twist determined by left bundle branch block impaired visualization in two cases; in the other six, the vigorous heart movements did not allow the recording. Atropine was added in 93% of patients, at a mean dose of 0.68 ± 0.53 mg.
Clinical CharacteristicsGI was comprised of 32 patients (CFVR < 2) and GII of 60
patients with CFVR ≥ 2 (Figures 1 and 2); patients in GI were older (66±9 vs. 61±11 years; p=0.04).
There was no difference between the groups (p=NS) as regards the distribution by gender, arterial hypertension, dyslipidemia, diabetes, history of CAD, and previous coronary intervention (whether surgical or by catheterization) or MI. Among patients receiving ASA, 48.5% had an inadequate CFVR; among those not receiving ASA, the proportion was 27% (p = 0.044) (Table 1).
All patients were instructed to discontinue β-blocker for 72 hours prior to DSE, and only two of them failed to do so. Both were from GI and their DSE was negative for ischemia. Considering the 22 patients who discontinued the medication, β-blocker was classified as selective in 8 (57%) of the 14 GI patients, whereas in GII, β-blocker was selective in 3 (37.5%) of the 8 cases. Among the 22 patients who discontinued β-blocker, 64% had an inadequate CFVR, whereas among those who did not take or did not discontinue β-blocker, the percentage of inadequate CFVR was 26% (p = 0.002).
There was no difference between the groups as regards their BMI (27.7±6.7 vs. 27.5±3.8 kg/m²; p= 0.87). Among the 92 patients, 40 (43.5%) were overweight (BMI≥ 25 kg/m²), 22 (24.5%) were obese (BMI ≥30 kg/m²) and one had morbid obesity (BMI ≥ 40 kg/m²)30,33.
Echocardiographic Recordings and Hemodynamic DataLV ejection fraction in GI and GII were different (61±10 vs.
65.8±5.7%; p= 0.005). There were no differences (p = NS) between the groups regarding LV mass, blood pressure (systolic and diastolic) at rest and in DSE, or the double product (Table 2). In GII, higher HR were achieved during DSE (148±12 vs. 141±20bpm; p= 0.04); however, in only 20% (18 cases) of the study patients the DSE was terminated with maximum HR. Among patients who achieved maximum HR, 66.7% showed
CFVR < 2, whereas CFVR was inadequate in 27% of those who did not achieve maximum HR (p = 0.002).
Five DSEs were inconclusive (all in GI); six were positive for myocardial ischemia, three in each group; and only in one case the anterior wall was affected (GI). SWMSI was not different between the groups (1.05±0.2 vs. 1.02±0.7; p= 0.24) during DSE.
Doppler recording of the LADThe mean time to obtain Doppler spectrum of the LAD in
both groups was shorter than one minute, with no differences between them (p = 0.23). Likewise, the mean HR at the moment the DPVs were obtained, whether at baseline or during DSE, were not significantly different between the groups either. In 33 (55%) of GII patients, an adequate CFVR was obtained before achieving the established target HR.
The baseline DPV in GI was higher than in GII (36.8 ± 8.4 vs. 25.6±5.7cm/s; p< 0.0001). However, there was no difference between DPVs obtained during DSE (61.4±16.6 vs. 64.2±15.9cm/s; p=0.42), thus resulting in CFVR of GI < GII (1.66±0.24 vs. 2.53±5.7; p< 0.0001) (Table 3).
Multivariate analysis of parametersIn the multivariate model, the logistic regression analysis
for CFVR < 2 showed significance for age and for β-blocker discontinuation (Table 4). The multivariate model was adjusted for potential confounders, and patients who had discontinued β-blocker had a four-fold higher chance of showing an inadequate CFVR (Table 5).
DiscussionIn the daily practice, it is important to consider the time
spent to perform the procedures. For this reason, we limited the time to obtain Doppler recordings (color and pulsed) of the LAD at rest at 180 seconds (period of one DSE stage), with a significant success rate (91%). During DSE, the high performance (92%) of Doppler recording of the LAD was maintained, and the feasibility rates were comparable to those of other studies using dobutamine or vasodilators.
In the present study, we sought to verify clinical, echocardiographic or hemodynamic parameters associated with the CFVR cut-off point established as adequate. Patient inclusion was not limited by the presence of cardiovascular risk factors, and these factors were not significantly associated with adequate or inadequate CFVR. GI patients were older and had a lower mean ejection fraction, factors that may be related to a low CFVR.
In the univariate analysis, the use of ASA was associated with inadequate CFVR. However, in the multivariate analysis, this was not demonstrated (Table 4).
β-blockers decrease the possibility of ischemia by reducing the cardiac work. Thus, discontinuation of these drugs promotes a higher HR, and this could increase the probability of a more frequent occurrence of DSE with achieved target HR or consistent with myocardial ischemia. Previous findings suggest that non-selective β-blocker increases coronary vascular resistance34. On
136
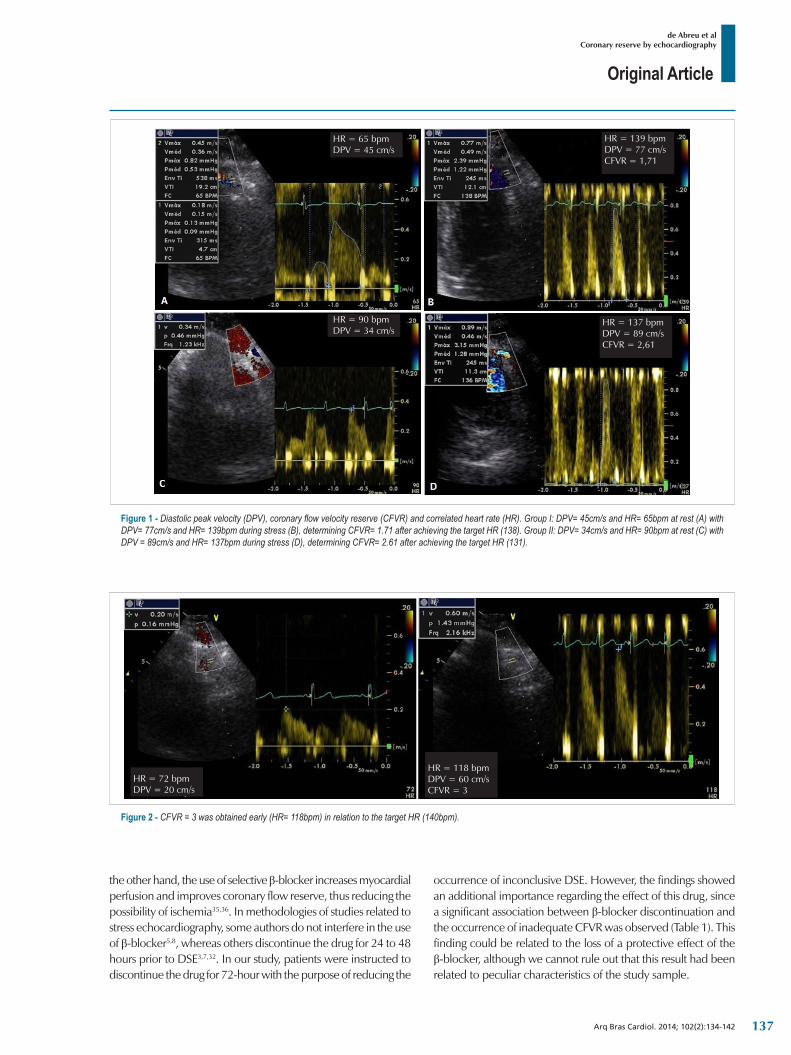
Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
the other hand, the use of selective β-blocker increases myocardial perfusion and improves coronary flow reserve, thus reducing the possibility of ischemia35,36. In methodologies of studies related to stress echocardiography, some authors do not interfere in the use of β-blocker5,8, whereas others discontinue the drug for 24 to 48 hours prior to DSE3,7,32. In our study, patients were instructed to discontinue the drug for 72-hour with the purpose of reducing the
occurrence of inconclusive DSE. However, the findings showed an additional importance regarding the effect of this drug, since a significant association between β-blocker discontinuation and the occurrence of inadequate CFVR was observed (Table 1). This finding could be related to the loss of a protective effect of the β-blocker, although we cannot rule out that this result had been related to peculiar characteristics of the study sample.
Figure 2 ‑ CFVR = 3 was obtained early (HR= 118bpm) in relation to the target HR (140bpm).
HR = 72 bpmDPV = 20 cm/s
HR = 118 bpmDPV = 60 cm/sCFVR = 3
Figure 1 ‑ Diastolic peak velocity (DPV), coronary flow velocity reserve (CFVR) and correlated heart rate (HR). Group I: DPV= 45cm/s and HR= 65bpm at rest (A) with DPV= 77cm/s and HR= 139bpm during stress (B), determining CFVR= 1.71 after achieving the target HR (138). Group II: DPV= 34cm/s and HR= 90bpm at rest (C) with DPV = 89cm/s and HR= 137bpm during stress (D), determining CFVR= 2.61 after achieving the target HR (131).
HR = 65 bpmDPV = 45 cm/s
HR = 137 bpmDPV = 89 cm/sCFVR = 2,61
HR = 139 bpmDPV = 77 cm/sCFVR = 1,71
HR = 90 bpmDPV = 34 cm/s
137
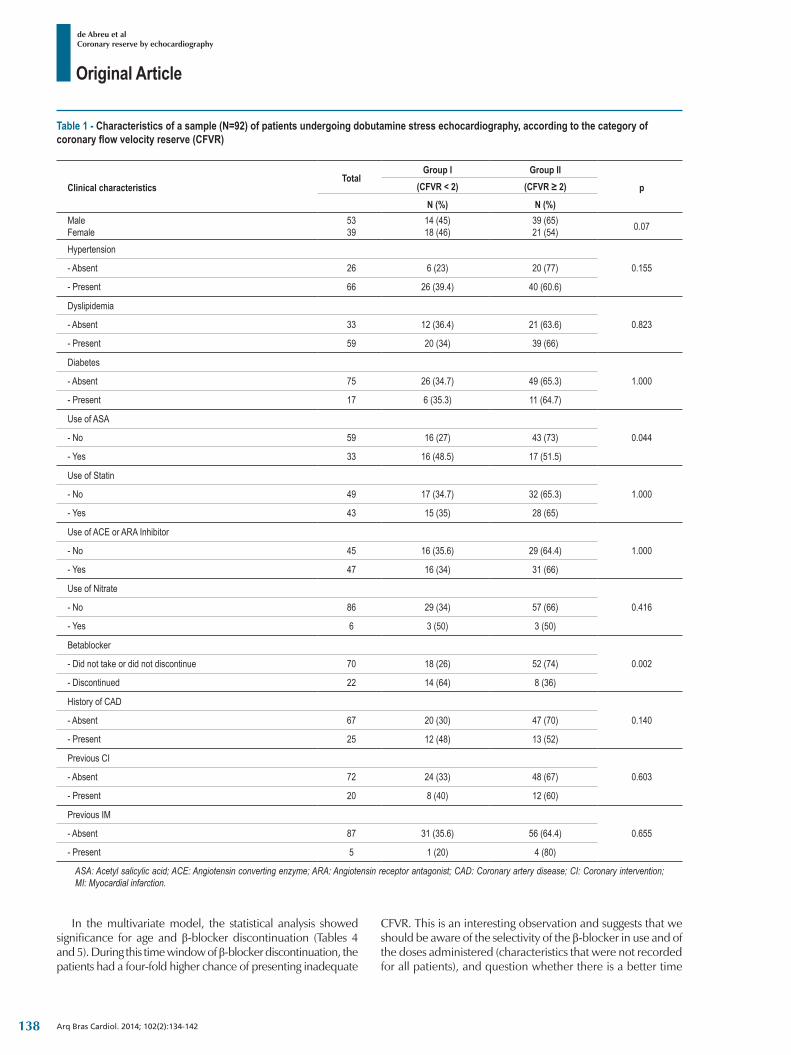
Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
Table 1 ‑ Characteristics of a sample (N=92) of patients undergoing dobutamine stress echocardiography, according to the category of coronary flow velocity reserve (CFVR)
Clinical characteristicsTotal
Group I Group II
p(CFVR < 2) (CFVR ≥ 2)
N (%) N (%)MaleFemale
5339
14 (45)18 (46)
39 (65)21 (54) 0.07
Hypertension
0.155- Absent 26 6 (23) 20 (77)
- Present 66 26 (39.4) 40 (60.6)
Dyslipidemia
0.823- Absent 33 12 (36.4) 21 (63.6)
- Present 59 20 (34) 39 (66)
Diabetes
1.000- Absent 75 26 (34.7) 49 (65.3)
- Present 17 6 (35.3) 11 (64.7)
Use of ASA
0.044- No 59 16 (27) 43 (73)
- Yes 33 16 (48.5) 17 (51.5)
Use of Statin
1.000- No 49 17 (34.7) 32 (65.3)
- Yes 43 15 (35) 28 (65)
Use of ACE or ARA Inhibitor
1.000- No 45 16 (35.6) 29 (64.4)
- Yes 47 16 (34) 31 (66)
Use of Nitrate
0.416- No 86 29 (34) 57 (66)
- Yes 6 3 (50) 3 (50)
Betablocker
0.002- Did not take or did not discontinue 70 18 (26) 52 (74)
- Discontinued 22 14 (64) 8 (36)
History of CAD
0.140- Absent 67 20 (30) 47 (70)
- Present 25 12 (48) 13 (52)
Previous CI
0.603- Absent 72 24 (33) 48 (67)
- Present 20 8 (40) 12 (60)
Previous IM
0.655- Absent 87 31 (35.6) 56 (64.4)
- Present 5 1 (20) 4 (80)
ASA: Acetyl salicylic acid; ACE: Angiotensin converting enzyme; ARA: Angiotensin receptor antagonist; CAD: Coronary artery disease; CI: Coronary intervention; MI: Myocardial infarction.
In the multivariate model, the statistical analysis showed significance for age and β-blocker discontinuation (Tables 4 and 5). During this time window of β-blocker discontinuation, the patients had a four-fold higher chance of presenting inadequate
CFVR. This is an interesting observation and suggests that we should be aware of the selectivity of the β-blocker in use and of the doses administered (characteristics that were not recorded for all patients), and question whether there is a better time
138
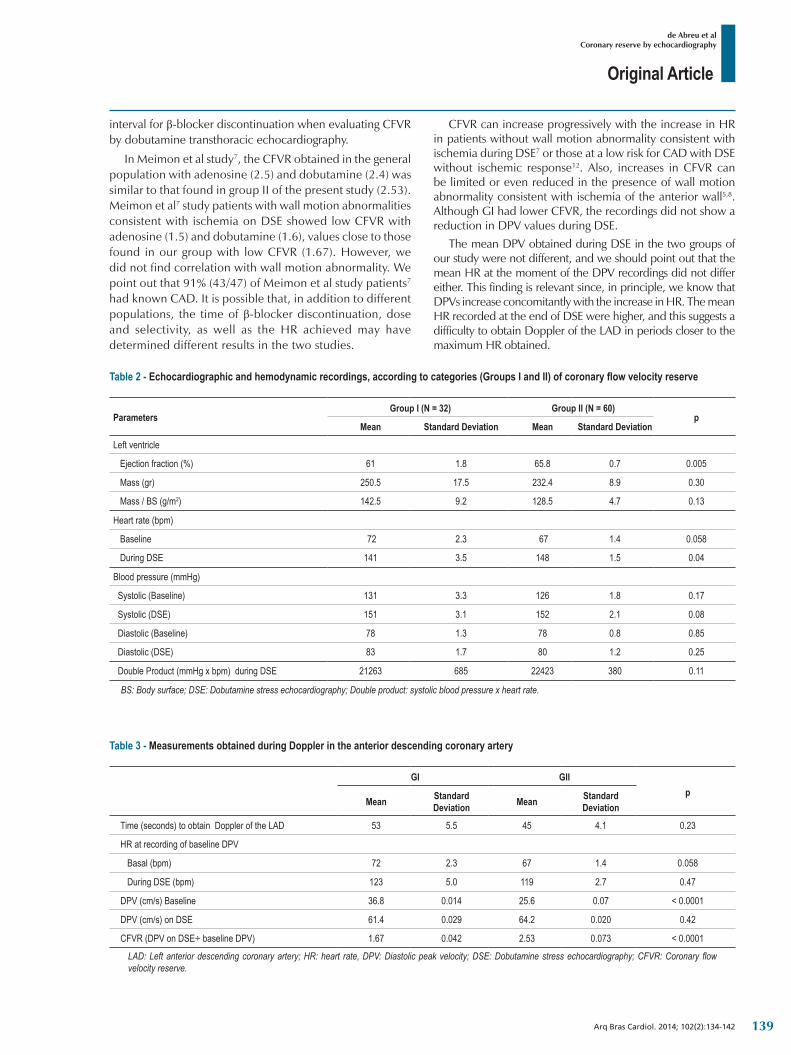
Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
Table 2 ‑ Echocardiographic and hemodynamic recordings, according to categories (Groups I and II) of coronary flow velocity reserve
ParametersGroup I (N = 32) Group II (N = 60)
pMean Standard Deviation Mean Standard Deviation
Left ventricle
Ejection fraction (%) 61 1.8 65.8 0.7 0.005
Mass (gr) 250.5 17.5 232.4 8.9 0.30
Mass / BS (g/m2) 142.5 9.2 128.5 4.7 0.13
Heart rate (bpm)
Baseline 72 2.3 67 1.4 0.058
During DSE 141 3.5 148 1.5 0.04
Blood pressure (mmHg)
Systolic (Baseline) 131 3.3 126 1.8 0.17
Systolic (DSE) 151 3.1 152 2.1 0.08
Diastolic (Baseline) 78 1.3 78 0.8 0.85
Diastolic (DSE) 83 1.7 80 1.2 0.25
Double Product (mmHg x bpm) during DSE 21263 685 22423 380 0.11
BS: Body surface; DSE: Dobutamine stress echocardiography; Double product: systolic blood pressure x heart rate.
Table 3 ‑ Measurements obtained during Doppler in the anterior descending coronary artery
GI GIIp
Mean Standard Deviation Mean Standard
Deviation
Time (seconds) to obtain Doppler of the LAD 53 5.5 45 4.1 0.23
HR at recording of baseline DPV
Basal (bpm) 72 2.3 67 1.4 0.058
During DSE (bpm) 123 5.0 119 2.7 0.47
DPV (cm/s) Baseline 36.8 0.014 25.6 0.07 < 0.0001
DPV (cm/s) on DSE 61.4 0.029 64.2 0.020 0.42
CFVR (DPV on DSE÷ baseline DPV) 1.67 0.042 2.53 0.073 < 0.0001
LAD: Left anterior descending coronary artery; HR: heart rate, DPV: Diastolic peak velocity; DSE: Dobutamine stress echocardiography; CFVR: Coronary flow velocity reserve.
interval for β-blocker discontinuation when evaluating CFVR by dobutamine transthoracic echocardiography.
In Meimon et al study7, the CFVR obtained in the general population with adenosine (2.5) and dobutamine (2.4) was similar to that found in group II of the present study (2.53). Meimon et al7 study patients with wall motion abnormalities consistent with ischemia on DSE showed low CFVR with adenosine (1.5) and dobutamine (1.6), values close to those found in our group with low CFVR (1.67). However, we did not find correlation with wall motion abnormality. We point out that 91% (43/47) of Meimon et al study patients7 had known CAD. It is possible that, in addition to different populations, the time of β-blocker discontinuation, dose and selectivity, as well as the HR achieved may have determined different results in the two studies.
CFVR can increase progressively with the increase in HR in patients without wall motion abnormality consistent with ischemia during DSE7 or those at a low risk for CAD with DSE without ischemic response12. Also, increases in CFVR can be limited or even reduced in the presence of wall motion abnormality consistent with ischemia of the anterior wall5,8. Although GI had lower CFVR, the recordings did not show a reduction in DPV values during DSE.
The mean DPV obtained during DSE in the two groups of our study were not different, and we should point out that the mean HR at the moment of the DPV recordings did not differ either. This finding is relevant since, in principle, we know that DPVs increase concomitantly with the increase in HR. The mean HR recorded at the end of DSE were higher, and this suggests a difficulty to obtain Doppler of the LAD in periods closer to the maximum HR obtained.
139
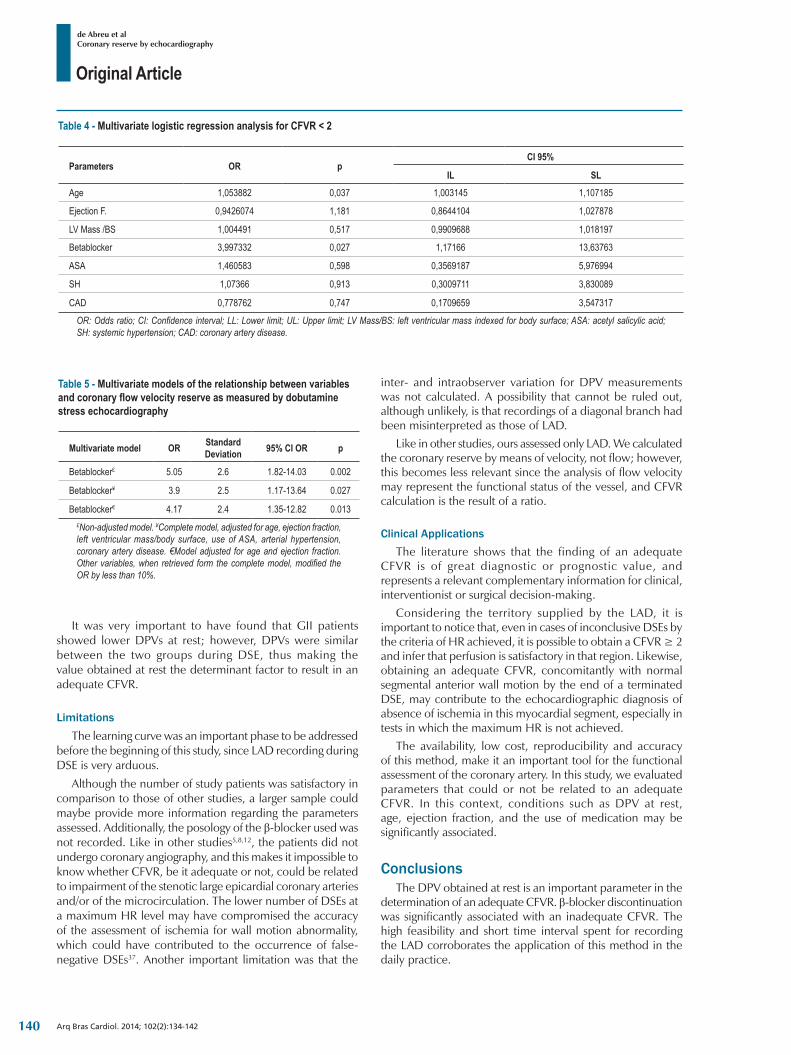
Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
Table 4 ‑ Multivariate logistic regression analysis for CFVR < 2
Parameters OR pCI 95%
IL SLAge 1,053882 0,037 1,003145 1,107185
Ejection F. 0,9426074 1,181 0,8644104 1,027878
LV Mass /BS 1,004491 0,517 0,9909688 1,018197
Betablocker 3,997332 0,027 1,17166 13,63763
ASA 1,460583 0,598 0,3569187 5,976994
SH 1,07366 0,913 0,3009711 3,830089
CAD 0,778762 0,747 0,1709659 3,547317
OR: Odds ratio; CI: Confidence interval; LL: Lower limit; UL: Upper limit; LV Mass/BS: left ventricular mass indexed for body surface; ASA: acetyl salicylic acid; SH: systemic hypertension; CAD: coronary artery disease.
Table 5 ‑ Multivariate models of the relationship between variables and coronary flow velocity reserve as measured by dobutamine stress echocardiography
Multivariate model OR Standard Deviation 95% CI OR p
Betablocker£ 5.05 2.6 1.82-14.03 0.002
Betablocker¥ 3.9 2.5 1.17-13.64 0.027
Betablocker€ 4.17 2.4 1.35-12.82 0.013£Non-adjusted model. ¥Complete model, adjusted for age, ejection fraction, left ventricular mass/body surface, use of ASA, arterial hypertension, coronary artery disease. €Model adjusted for age and ejection fraction. Other variables, when retrieved form the complete model, modified the OR by less than 10%.
It was very important to have found that GII patients showed lower DPVs at rest; however, DPVs were similar between the two groups during DSE, thus making the value obtained at rest the determinant factor to result in an adequate CFVR.
LimitationsThe learning curve was an important phase to be addressed
before the beginning of this study, since LAD recording during DSE is very arduous.
Although the number of study patients was satisfactory in comparison to those of other studies, a larger sample could maybe provide more information regarding the parameters assessed. Additionally, the posology of the β-blocker used was not recorded. Like in other studies5,8,12, the patients did not undergo coronary angiography, and this makes it impossible to know whether CFVR, be it adequate or not, could be related to impairment of the stenotic large epicardial coronary arteries and/or of the microcirculation. The lower number of DSEs at a maximum HR level may have compromised the accuracy of the assessment of ischemia for wall motion abnormality, which could have contributed to the occurrence of false-negative DSEs37. Another important limitation was that the
inter- and intraobserver variation for DPV measurements was not calculated. A possibility that cannot be ruled out, although unlikely, is that recordings of a diagonal branch had been misinterpreted as those of LAD.
Like in other studies, ours assessed only LAD. We calculated the coronary reserve by means of velocity, not flow; however, this becomes less relevant since the analysis of flow velocity may represent the functional status of the vessel, and CFVR calculation is the result of a ratio.
Clinical ApplicationsThe literature shows that the finding of an adequate
CFVR is of great diagnostic or prognostic value, and represents a relevant complementary information for clinical, interventionist or surgical decision-making.
Considering the territory supplied by the LAD, it is important to notice that, even in cases of inconclusive DSEs by the criteria of HR achieved, it is possible to obtain a CFVR ≥ 2 and infer that perfusion is satisfactory in that region. Likewise, obtaining an adequate CFVR, concomitantly with normal segmental anterior wall motion by the end of a terminated DSE, may contribute to the echocardiographic diagnosis of absence of ischemia in this myocardial segment, especially in tests in which the maximum HR is not achieved.
The availability, low cost, reproducibility and accuracy of this method, make it an important tool for the functional assessment of the coronary artery. In this study, we evaluated parameters that could or not be related to an adequate CFVR. In this context, conditions such as DPV at rest, age, ejection fraction, and the use of medication may be significantly associated.
ConclusionsThe DPV obtained at rest is an important parameter in the
determination of an adequate CFVR. β-blocker discontinuation was significantly associated with an inadequate CFVR. The high feasibility and short time interval spent for recording the LAD corroborates the application of this method in the daily practice.
140

Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
1. Mathias W Jr, Arruda A, Santos FC, Arruda AL, Mattos E, Osório A, et al. Safety of dobutamine-atropine stress echocardiography: a prospective experience of 4033 consecutive studies. J Am Soc Echocardiogr. 1999;12(10):785-91.
2. Geleijnse ML, Fioretti PM, Roelandt JR. Methodology, feasibility, safety and diagnostic accuracy of dobutamine stress echocardiography. J Am Coll Cardiol. 1997;30(3):595-606.
3. Abreu JS, Diógenes TC, Farias AG, Morais JM, Paes Júnior JN. Segurança e exeqüibilidade do ecocardiograma sob estresse com dobutamina e atropina em pacientes octogenários. Arq Bras Cardiol. 2005;85(3):198-204.
4. Geleijnse ML, Krenning BJ, Nemes A, et al. Incidence, pathophysiology, and treatment of complications during dobutamine-atropine stress echocardiography. Circulation. 2010; 121: 1756-67.
5. Takeuchi M, Miyazaki C, Yoshitani H, Otani S, Sakamoto K, Yoshikawa J. Assessment of coronary flow velocity with transthoracic Doppler echocardiography during dobutamine stress echocardiography. J Am Coll Cardiol. 2001;38(1):117-23.
6. Meimoun P, Benali T, Sayah S, Luycs-Bore A, Boulanger J, Zemir H, et al. Evaluation of left anterior descending coronary artery stenosis of intermediate severity using transthoracic coronary flow reserve and dobutamine stress echocardiography. J Am Soc Echocardiogr. 2005;18(12):1233-40.
7. Meimoun P, Sayah S, Tcheuffa JC, Benali T, Luycx-Bore A, Levy F, et al. Transthoracic coronary flow velocity reserve assessment: comparison between adenosine and dobutamine. J Am Soc Echocardiogr. 2006;19(10):1220-8.
8. Ahmari SA, Modesto K, Bunch J, Stussy V, Dichak A, Seward J, et al. Doppler derived coronary flow reserve during dobutamine stress echocardiography further improves detection of myocardial ischemia. Eur J Echocardiogr. 2006;7(2):134-40.
9. Soylu O, Celik S, Karakus G, Yldrim A, Ergelen M, Zencirci E, et al. Transthoracic Doppler echocardiographic coronary flow imaging in identification of left anterior descending coronary artery stenosis in patients with left bundle branch block. Echocardiography. 2008;25(10):1065-70.
10. D’Andrea A, Severino S, Mita C, Riegler L, Cocchia R, Gravina R, et al. Clinical outcome in patients with intermediate stenosis of left anterior descending coronary artery after deferral of revascularization on the basis of noninvasive coronary flow reserve measurement. Echocardiography. 2009;26(4):431-40.
11. Hyodo E, Hirata K, Hirose M, Sakanoue Y, Nishida Y, Aray K, et al. Detection of restenosis after percutaneous coronary intervention in three major coronary arteries by transthoracic Doppler echocardiography. J Am Soc Echocardiogr. 2010;23(5):553-9.
12. Forte EH, Rousse MG, Lowenstein JA. Target heart rate to determine the normal value of coronary flow reserve during dobutamine stress echocardiography. Cardiovasc Ultrasound. 2011;9:10.
13. Lowenstein J. Evaluation of the coronary flow reserve in three coronary territories by transthoracic echocardiography approach. Is it magic realism? Rev Bras Ecocardiogr Imagem Cardiovasc. 2010;23(3):82-98.
14. Murata E, Hozumi T, Matsumura Y, Fujimoto K, Sugioka K, Takemoto Y, et al. Coronary flow velocity reserve measurement in three major coronary arteries using transthoracic Doppler echocardiography. Echocardiography. 2006;23(4):279-86.
15. Hozumi T, Yoshida K, Akasaka T, Asami Y, Ogata Y, Takagi T, et al. Noninvasive assessment of coronary flow velocity and coronary flow velocity reserve in the left anterior descending coronary artery by Doppler echocardiography: comparison with invasive technique. J Am Coll Cardiol. 1998;32(5):1251-9.
16. Caiati C, Montaldo C, Zedda N, Montisci R, Ruscazio M, Lai G, et al. Validation of a new noninvasive method (contrast-enhanced transthoracic second harmonic echo Doppler) for the evaluation of coronary flow reserve: comparison with intracoronary Doppler flow wire. J Am Coll Cardiol. 1999;34(4):1193-200.
17. Saraste M, Koskenvuo J, Knuuti J, Toikka J, Laine H, Niemi P, et al. Coronary flow reserve: measurement with transthoracic Doppler echocardiography is reproducible and comparable with positron emission tomography. Clin Physiol. 2001;21(1):114-22.
18. Osório AF, Tsutsui JM, Kowatsch I, Guera VC, Ramires JA, Lemos PA, et al. Evaluation of blood flow reserve in left anterior descending coronary artery territory by quantitative myocardial contrast and Doppler echocardiography. J Am Soc Echocardiogr. 2007;20(6):709-16.
19. Cortigiani L, Rigo F, Sicari R, Gherardi S, Bovenzi F, Picano E. Prognostic correlates of combined coronary flow reserve assessment on left anterior descending and right coronary artery in patients with negative stress echocardiography by wall motion criteria. Heart. 2009;95(17):1423-8.
20. Ueno Y, Nakamura Y, Takashima H, Kinoshita M, Soma A. Noninvasive assessment of coronary flow velocity and coronary flow velocity reserve in the right coronary artery by transthoracic Doppler echocardiography: comparison with intracoronary Doppler guidewire. J Am Soc Echocardiogr. 2002;15(10 Pt 1):1074-9.
21. Holte E, Vegsundvåg J, Hegbom K, Hole T, Wiseth R. Transthoracic Doppler echocardiography for detection of stenoses in the left coronary artery by use of poststenotic coronary flow profiles: a comparison with quantitative coronary angiography and coronary flow reserve. J Am Soc Echocardiogr. 2013;26(1):77-85.
References
Author contributionsConception and design of the research: Abreu JS;
Acquisition of data: Abreu JS, Diógenes TCP, Gomes Neto PS; Analysis and interpretation of the data: Abreu JS, Lima JWO, Siqueira JM, Paes Júnior JN; Statistical analysis: Lima JWO; Writing of the manuscript: Abreu JS, Lima JWO, Siqueira JM, Pimentel NL, Gomes Neto PS, Abreu MEB, Paes Júnior JN; Critical revision of the manuscript for intellectual content: Abreu JS, Lima JWO.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis study is not associated with any thesis or dissertation work.
141
Original Article
de Abreu et alCoronary reserve by echocardiography
Arq Bras Cardiol. 2014; 102(2):134-142
22. Hozumi T, Yoshida K, Ogata Y, Akasaka T, Asami Y, Takagi T, et al. Noninvasive assessment of significant left anterior descending coronary artery stenosis by coronary flow velocity reserve with transthoracic color Doppler echocardiography. Circulation. 1998;97(16):1557-62.
23. Voci P, Pizzuto F, Mariano E, Puddu PE, Chiavari PA, Romeo F. Measurement of coronary flow reserve in the anterior and posterior descending coronary arteries by transthoracic Doppler ultrasound. Am J Cardiol. 2002;90(9):988-91.
24. Matsumura Y, Hozumi T, Watanabe H, Fujimoto K, Sugioka K, Takemoto Y, et al. Cut-off value of coronary flow velocity reserve by transthoracic Doppler echocardiography for diagnosis of significant left anterior descending artery stenosis in patients with coronary risk factors. Am J Cardiol. 2003;92(12):1389-93.
25. Dimitrow PP. Transthoracic Doppler echocardiography-noninvasive diagnostic window for coronary flow reserve assessment. Cardiovasc Ultrasound. 2003;1:4.
26. Rigo F. Coronary flow reserve in stress-echo lab: from pathophysiologic toy to diagnostic tool. Cardiovasc Ultrasound. 2005;3:8.
27. Mladenovic Z, Djordjevic-Dikic A, Tavciovski D, Angelkov AR, Jovic Z, Djuric P. The additive diagnostic role of coronary flow reserve in noninvasive evaluation of coronary stenosis on left descending artery previously detected by multislice computed tomography. Echocardiography. 2013;30(3):338-44.
28. Baumgart D, Haude M, Liu F, Ge J, Goerge G, Erbel R. Current concepts of coronary flow reserve for clinical decision making during cardiac catheterization. Am Heart J. 1998;136(1):136-49.
29. Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia. V Diretrizes brasileiras de hipertensão arterial. Arq Bras Cardiol. 2007;89(3):e24-e79
30. Standards of medical care in diabetes - 2013. Diabetes Care. 2013;36 Suppl 1:S11-66.
31. Sposito AC, Caramelli B, Fonseca FA, Bertolami MC, Afiune Neto A, Souza AD, et al.; Sociedade Brasileira de Cardiologia. IV Diretriz brasileira sobre dislipidemias e prevenção da aterosclerose. Arq Bras Cardiol. 2007;88(supl 1):1-18.
32. Abreu JS, Diógenes TC, Abreu AL, Barreto JE, Morais JM, Abreu ME, et al. Internal thoracic artery graft (ITAG): patency and functional status at rest and during dobutamine-stress echocardiography. Arq Bras Cardiol. 2008;90(1):37-45.
33. Brandão AP, Brandão AA, Nogueira AR, Suplicy H, Guimarães JI, Oliveira JEP, et al; Sociedade Brasileira de Cardiologia. I Diretriz brasileira de diagnóstico e tratamento da síndrome metabólica. Arq Bras Cardiol. 2005;84(supl 1):1-28.
34. Kern MJ, Ganz P, Horowitz JD, Gaspar J, Barry WH, Lorell BH, et al. Potentiation of coronary vasoconstriction by beta-adrenergic blockade in patients with coronary artery disease. Circulation. 1983;67(6):1178-85.
35. Böttcher M, Czernin J, Sun K, Phelps ME, Schelbert HR. Effect of beta 1 adrenergic receptor blockade on myocardial blood flow and vasodilatory capacity. J Nucl Med. 1997;38(3):442-6.
36. Billinger M, Seiler C, Fleisch M, Eberli FR, Meier B, Hess OM. Do beta-adrenergic blocking agents increase coronary flow reserve? J Am Coll Cardiol. 2001;38(7):1866-71.
37. Makani H, Bangalore S, Halpern D, Makwana HG, Chaudhry FA. Cardiac outcomes with submaximal normal stress echocardiography: a meta-analysis. J Am Coll Cardiol. 2012;60(15):1393-401.
142
Original Article
Study of Risk Factors Associated with Peripheral Arteriopathy in Japanese-Brazilians from Bauru (SP)Luciana Garofolo1, Sandra Roberta G. Ferreira2, Fausto Miranda Junior3
Universidade Federal de São Paulo (Unifesp)1; Faculdade de Saúde Pública - Universidade de São Paulo (USP)2; Departamento de Cirurgia - Universidade Federal de São Paulo (Unifesp)3, São Paulo, SP – Brazil
Mailing address: Luciana Garofolo • Rua Dr. Rafael de Barros, 497, Paraíso. CEP 04003-040, São Paulo, SP - BrazilE-mail: [email protected], [email protected] received on May 30, 2013; revised on October 13, 2013; manuscript accepted on October 16, 2013.
DOI: 10.5935/abc.20140018
AbstractBackground: Cardiovascular diseases are the major cause of morbidity and mortality in developed and emerging countries. Their main etiology, atherosclerosis, is a disseminated disease that affects the coronary, cerebral and peripheral territories. The peripheral arterial disease (PAD), as well as its consequences, indicates the involvement of the coronary territory. Therefore, its better understanding enables proper treatment, delaying local and long-term complications, reducing the cost to the health system.
Objective: This study estimates the percentage of PAD in Japanese-Brazilians from Bauru (SP), recognized by the high prevalence of metabolic disorders such as hypertension (43%), diabetes mellitus (33%) and hypercholesterolemia (60%), and examines the association with risk biomarkers.
Methods: This cross-sectional population study evaluated 1,330 Japanese-Brazilians of both genders aged ≥ 30 who underwent a complete physical examination, anthropometric measurements, laboratory tests and ankle-brachial index (ABI). Participants with ABI ≤ 0.90 were diagnosed as having PAD. After applying the exclusion criteria, 1,038 individuals were part of the analysis. We used Poisson regression to analyze associations with PAD.
Results: The mean age was 56.8 years and the percentage of PAD was 21.1%, equal among the genders. PAD was associated with smoking (PR 2.16 [1.33 to 3.48]) and hypertension (PR 1.56 [1.12-2.22]).
Conclusion: The percentage of PAD in Japanese-Brazilians was similar to other populations of adverse cardiometabolic profile (US PARTNERS and POPADAD). The independent association of PAD with smoking and hypertension, but not with other classical risk factors, may depend on the very high frequencies of metabolic disorders in this population. (Arq Bras Cardiol. 2014; 102(2):143-150)
Keywords: Risk factors; Peripheral arterial disease; Migration; Atherosclerosis; Diabetes mellitus; Coronary diseases.
and middle per capita income, and 13.1% in high-income countries2. The growing interest in the early diagnosis of PAD is occurring not only for its increased prevalence associated with an aging population, but also because it is related to atherosclerotic disease in other territories, such as coronary and cerebral3.
Being a chronic disease, the resources needed for treatment are high. In the U.S. population, the estimated cost per year was US$ 5,955 per patient with PAD4.
Moreover, the progression of PAD is associated with coronary artery disease. We found an increased risk of cardiovascular events of 2.8 times in three years in patients with PAD compared to those without the disease3. A study conducted in patients undergoing coronary angiography found concomitance between PAD and coronary artery disease in 90.7% of patients5.
Immigrants of Japanese descent in the Americas have high rates of diabetes mellitus and other metabolic disorders6. It is believed that exposure to the Western environment should have exacerbated a genetic tendency to accumulate body fat, increasing cardiovascular risk. Genetically homogenous populations with an adverse
IntroductionDespite changes in lifestyle and a growing therapeutic
arsenal, cardiovascular diseases are still the leading cause of morbidity and mortality in developed and emerging countries. Data from the Ministry of Health showed that they are the leading cause of death in Brazil. In 2006, they accounted for 29.4% of deaths in the country, while neoplasias accounted for 15.1%1.
PAD (peripheral arterial disease) of atherosclerotic etiology is increasingly prevalent in modern society, partly due to increased life expectancy, affecting 202 million people worldwide in 2010. In the last decade, there was an increase of 28.7% in its prevalence in countries of low
143
Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
cardiometabolic profile represent an opportunity to study the PAD, as well as other atherosclerotic manifestations and their relationship with risk factors6,7.
In view of this scenario, it can be argued that it is worth studying this population, the traditional and non-traditional risk factors for PAD, which are similar to those of coronary artery disease, enabling a better treatment of the disease, delaying complications and reducing the cost to the health system.
MethodsThis cross-sectional study was based on the Japanese-
Brazilian population living in Bauru (SP). The data used in this analysis belong to the second phase of the main study conducted in 2000. Individuals of both genders, aged ≥ 30, of Nipponese origin, first and second generations, were invited to participate. Methodological details were previously described7. The study was approved by the institutional ethics committee, and consent was signed by all participants. A total of 1,330 individuals, which corresponded to one third of the local Nipponese population, agreed to participate in the study and were interviewed using standardized questionnaires on clinical status (smoking and history of previous diseases) and nutrition. The participants were invited to undergo clinical examination (including anthropometric measurements, blood pressure and Doppler ankle-brachial index - ABI) and blood collection. Exclusion criteria for this analysis were incomplete questionnaire data and clinical and laboratory evaluation (255 participants), ABI > 1.40 (one participant) and concentration of C-reactive protein (hs-CRP) > 10 mg/L (36 participants). Therefore, 1,038 individuals were studied.
Weight (Filizola® scale) and height were determined with minimal clothing and no shoes for the calculation of body mass index (BMI)8. Waistline circumference8 was measured with a nondistensible measuring tape at the midpoint between the last floating rib and the iliac crest parallel to the ground, and hip measurement was determined by the buttock level, through the pubic symphysis. The waist-hip9 ratio was determined by the ratio between these circumferences. For diagnosing obesity and central obesity, the values recommended by the Japan Society for the Study of Obesity8 were employed, and for the waist-hip ratio, those of the World Health Organization were used9.
Blood pressure was measured in an automatic device (Omron HEM-712C, Omron Health Care, USA) after five minutes in the sitting position. The mean of the two last measurements was considered the final value of systolic and diastolic pressure. Hypertension was diagnosed in those with blood pressure values > 140 × 90 mmHg or those who reported drug treatment10.
After fasting for 12 hours and prior tracking with blood glucose, the participants underwent oral glucose tolerance testing with 75 g. Besides those who reported drug treatment, those who met the American Diabetes Association (ADA) criteria were diagnosed as diabetics11. The participants with fasting glucose < 100 mg/dL and two hours after overload < 140 mg/dL were considered normal. Those with fasting glucose ranging from 100 to 125 mg/dL and two-hour fasting
< 140 mg/dL were considered as having impaired fasting glucose (IFG). Impaired glucose tolerance (IGT) was diagnosed when fasting glucose was ≥ 100 mg/dL, but with glucose after overload between 140-199 mg/dL. Diabetes was diagnosed by fasting glucose ≥ 126 mg/dL or overload ≥ 200 mg/dL.
For the diagnosis of dyslipidemia, the criteria of the Executive Summary of the Third Report of the National Cholesterol Education Program - Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adults Treatment Panel III) were employed12. Participants with total cholesterol ≤ 200 mg/dL, LDL-cholesterol ≤ 130 mg/dL, HDL cholesterol ≥ 35 mg/dL for men and ≥ 45 mg/dL for women, and triglycerides ≤ 200 mg/dL were considered normal as to the lipid profile. Those with abnormalities in at least one of these parameters were considered dyslipidemic.
Uric acid concentrations of up to 6 mg/dL for women and of up to 7 mg/dL for men were considered normal13. For homocysteine, the cutoff value was 15 µmol/L14; for hs-CRP, the cutoff value corresponded to the median of the population: 1.1 mg/L.
Plasma glucose and lipoproteins were determined by enzymatic methods. The determination of homocysteine was based on the methodology described by Pfeiffer et al15 CRP concentrations were determined by chemiluminescence.
Diagnosis of PADThis diagnosis was done using continuous wave 8 MHz
Imbracios® Doppler. The ABI value was calculated by the quotient of the pressure auscultated in the ankle arteries by the highest pressure determined in the brachial arteries. As recommended by the Transatlantic Society Consensus16, an index of ≤ 0.9 and > 1.40 was considered abnormal. The PAD was diagnosed in the participant who presented an index of ≤ 0.9 in at least one of the arteries analyzed (posterior tibial artery or the dorsalis pedis artery) in one of the ends.
Statistical AnalysisData are presented as percentages or means and standard
deviations. Participants were stratified according to the presence of PAD or according to the ABI values (≤ 0.70; 0.71 to 0.90; ≥ 0.90)17.
Frequencies were compared by chi-square, and prevalence ratios (PR) are presented by point and interval with 95% confidence. In the comparison of means, Student’s t test or Bonferroni’s analysis of variance was used.
We used the Poisson regression model to determine the RP of PAD according to the risk factors. The initial model included all the variables associated with PAD with p < 0.15 in the crude analysis. One by one, these variables were removed from the model, considering the statistics of maximum verisimilitude. A similar procedure was adopted to determine the odds ratios in the ordered logistic regression analysis according to the ABI values (≤ 0.70; 0.71 to 0.90; ≥ 0.90).
The analyses used the software Stata 8.0 (Statacorp, 2004. Stata statistical software release 7.0 College Station, TX Stata Corporation). A p value < 0.05 was considered significant.
144
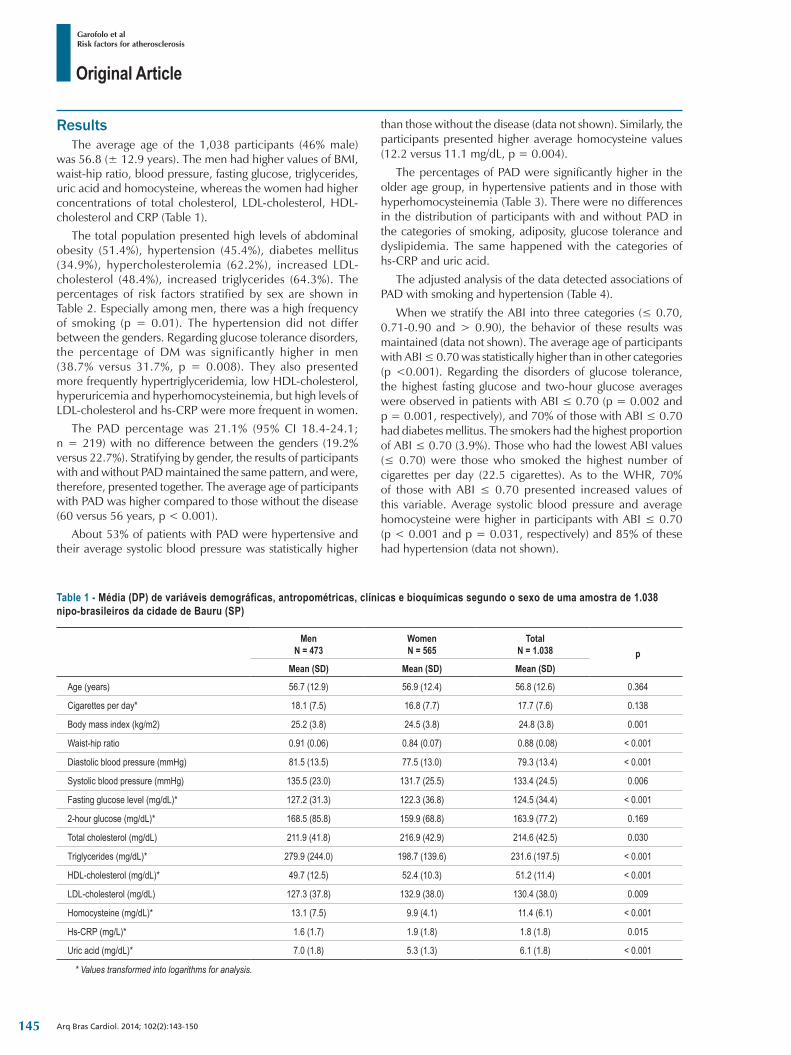
Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
ResultsThe average age of the 1,038 participants (46% male)
was 56.8 (± 12.9 years). The men had higher values of BMI, waist-hip ratio, blood pressure, fasting glucose, triglycerides, uric acid and homocysteine, whereas the women had higher concentrations of total cholesterol, LDL-cholesterol, HDL-cholesterol and CRP (Table 1).
The total population presented high levels of abdominal obesity (51.4%), hypertension (45.4%), diabetes mellitus (34.9%), hypercholesterolemia (62.2%), increased LDL-cholesterol (48.4%), increased triglycerides (64.3%). The percentages of risk factors stratified by sex are shown in Table 2. Especially among men, there was a high frequency of smoking (p = 0.01). The hypertension did not differ between the genders. Regarding glucose tolerance disorders, the percentage of DM was significantly higher in men (38.7% versus 31.7%, p = 0.008). They also presented more frequently hypertriglyceridemia, low HDL-cholesterol, hyperuricemia and hyperhomocysteinemia, but high levels of LDL-cholesterol and hs-CRP were more frequent in women.
The PAD percentage was 21.1% (95% CI 18.4-24.1; n = 219) with no difference between the genders (19.2% versus 22.7%). Stratifying by gender, the results of participants with and without PAD maintained the same pattern, and were, therefore, presented together. The average age of participants with PAD was higher compared to those without the disease (60 versus 56 years, p < 0.001).
About 53% of patients with PAD were hypertensive and their average systolic blood pressure was statistically higher
Table 1 ‑ Média (DP) de variáveis demográficas, antropométricas, clínicas e bioquímicas segundo o sexo de uma amostra de 1.038 nipo-brasileiros da cidade de Bauru (SP)
MenN = 473
WomenN = 565
TotalN = 1.038 p
Mean (SD) Mean (SD) Mean (SD)
Age (years) 56.7 (12.9) 56.9 (12.4) 56.8 (12.6) 0.364
Cigarettes per day* 18.1 (7.5) 16.8 (7.7) 17.7 (7.6) 0.138
Body mass index (kg/m2) 25.2 (3.8) 24.5 (3.8) 24.8 (3.8) 0.001
Waist-hip ratio 0.91 (0.06) 0.84 (0.07) 0.88 (0.08) < 0.001
Diastolic blood pressure (mmHg) 81.5 (13.5) 77.5 (13.0) 79.3 (13.4) < 0.001
Systolic blood pressure (mmHg) 135.5 (23.0) 131.7 (25.5) 133.4 (24.5) 0.006
Fasting glucose level (mg/dL)* 127.2 (31.3) 122.3 (36.8) 124.5 (34.4) < 0.001
2-hour glucose (mg/dL)* 168.5 (85.8) 159.9 (68.8) 163.9 (77.2) 0.169
Total cholesterol (mg/dL) 211.9 (41.8) 216.9 (42.9) 214.6 (42.5) 0.030
Triglycerides (mg/dL)* 279.9 (244.0) 198.7 (139.6) 231.6 (197.5) < 0.001
HDL-cholesterol (mg/dL)* 49.7 (12.5) 52.4 (10.3) 51.2 (11.4) < 0.001
LDL-cholesterol (mg/dL) 127.3 (37.8) 132.9 (38.0) 130.4 (38.0) 0.009
Homocysteine (mg/dL)* 13.1 (7.5) 9.9 (4.1) 11.4 (6.1) < 0.001
Hs-CRP (mg/L)* 1.6 (1.7) 1.9 (1.8) 1.8 (1.8) 0.015
Uric acid (mg/dL)* 7.0 (1.8) 5.3 (1.3) 6.1 (1.8) < 0.001
* Values transformed into logarithms for analysis.
than those without the disease (data not shown). Similarly, the participants presented higher average homocysteine values (12.2 versus 11.1 mg/dL, p = 0.004).
The percentages of PAD were significantly higher in the older age group, in hypertensive patients and in those with hyperhomocysteinemia (Table 3). There were no differences in the distribution of participants with and without PAD in the categories of smoking, adiposity, glucose tolerance and dyslipidemia. The same happened with the categories of hs-CRP and uric acid.
The adjusted analysis of the data detected associations of PAD with smoking and hypertension (Table 4).
When we stratify the ABI into three categories (≤ 0.70, 0.71-0.90 and > 0.90), the behavior of these results was maintained (data not shown). The average age of participants with ABI ≤ 0.70 was statistically higher than in other categories (p <0.001). Regarding the disorders of glucose tolerance, the highest fasting glucose and two-hour glucose averages were observed in patients with ABI ≤ 0.70 (p = 0.002 and p = 0.001, respectively), and 70% of those with ABI ≤ 0.70 had diabetes mellitus. The smokers had the highest proportion of ABI ≤ 0.70 (3.9%). Those who had the lowest ABI values (≤ 0.70) were those who smoked the highest number of cigarettes per day (22.5 cigarettes). As to the WHR, 70% of those with ABI ≤ 0.70 presented increased values of this variable. Average systolic blood pressure and average homocysteine were higher in participants with ABI ≤ 0.70 (p < 0.001 and p = 0.031, respectively) and 85% of these had hypertension (data not shown).
145
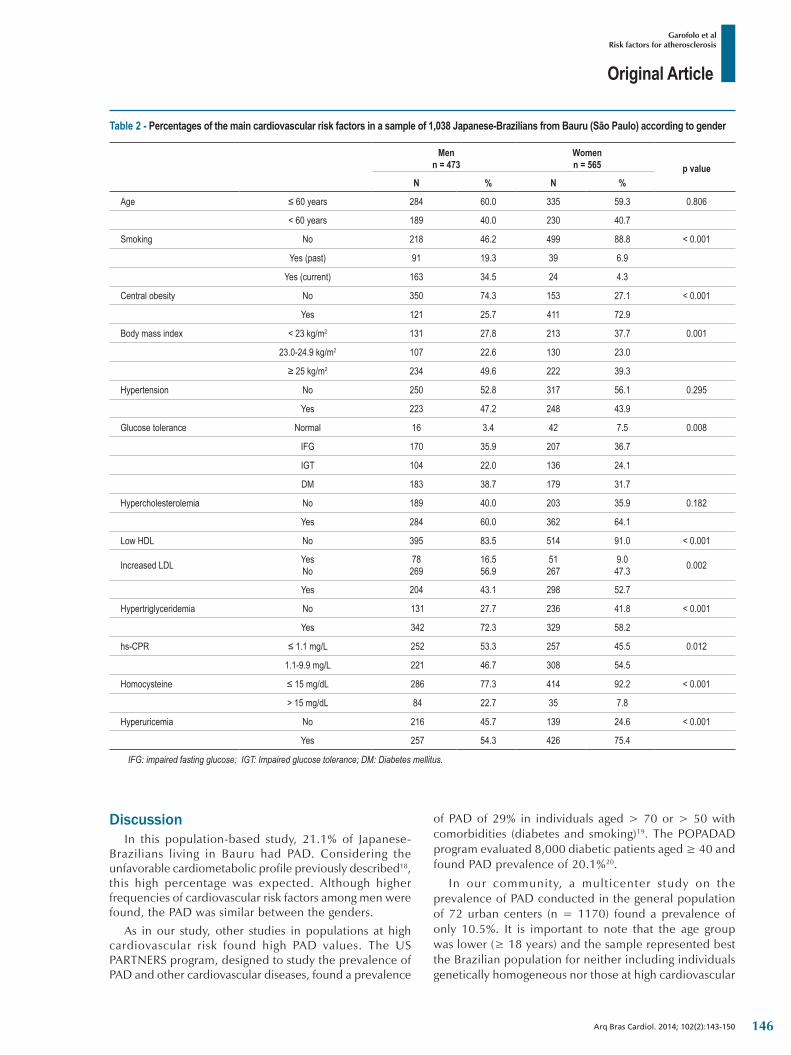
Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
DiscussionIn this population-based study, 21.1% of Japanese-
Brazilians living in Bauru had PAD. Considering the unfavorable cardiometabolic profile previously described18, this high percentage was expected. Although higher frequencies of cardiovascular risk factors among men were found, the PAD was similar between the genders.
As in our study, other studies in populations at high cardiovascular risk found high PAD values. The US PARTNERS program, designed to study the prevalence of PAD and other cardiovascular diseases, found a prevalence
of PAD of 29% in individuals aged > 70 or > 50 with comorbidities (diabetes and smoking)19. The POPADAD program evaluated 8,000 diabetic patients aged ≥ 40 and found PAD prevalence of 20.1%20.
In our community, a mult icenter study on the prevalence of PAD conducted in the general population of 72 urban centers (n = 1170) found a prevalence of only 10.5%. It is important to note that the age group was lower (≥ 18 years) and the sample represented best the Brazilian population for neither including individuals genetically homogeneous nor those at high cardiovascular
Table 2 ‑ Percentages of the main cardiovascular risk factors in a sample of 1,038 Japanese-Brazilians from Bauru (São Paulo) according to gender
Menn = 473
Womenn = 565 p value
N % N %
Age ≤ 60 years 284 60.0 335 59.3 0.806
< 60 years 189 40.0 230 40.7
Smoking No 218 46.2 499 88.8 < 0.001
Yes (past) 91 19.3 39 6.9
Yes (current) 163 34.5 24 4.3
Central obesity No 350 74.3 153 27.1 < 0.001
Yes 121 25.7 411 72.9
Body mass index < 23 kg/m2 131 27.8 213 37.7 0.001
23.0-24.9 kg/m2 107 22.6 130 23.0
≥ 25 kg/m2 234 49.6 222 39.3
Hypertension No 250 52.8 317 56.1 0.295
Yes 223 47.2 248 43.9
Glucose tolerance Normal 16 3.4 42 7.5 0.008
IFG 170 35.9 207 36.7
IGT 104 22.0 136 24.1
DM 183 38.7 179 31.7
Hypercholesterolemia No 189 40.0 203 35.9 0.182
Yes 284 60.0 362 64.1
Low HDL No 395 83.5 514 91.0 < 0.001
Increased LDL YesNo
78269
16.556.9
51267
9.047.3 0.002
Yes 204 43.1 298 52.7
Hypertriglyceridemia No 131 27.7 236 41.8 < 0.001
Yes 342 72.3 329 58.2
hs-CPR ≤ 1.1 mg/L 252 53.3 257 45.5 0.012
1.1-9.9 mg/L 221 46.7 308 54.5
Homocysteine ≤ 15 mg/dL 286 77.3 414 92.2 < 0.001
> 15 mg/dL 84 22.7 35 7.8
Hyperuricemia No 216 45.7 139 24.6 < 0.001
Yes 257 54.3 426 75.4
IFG: impaired fasting glucose; IGT: Impaired glucose tolerance; DM: Diabetes mellitus.
146
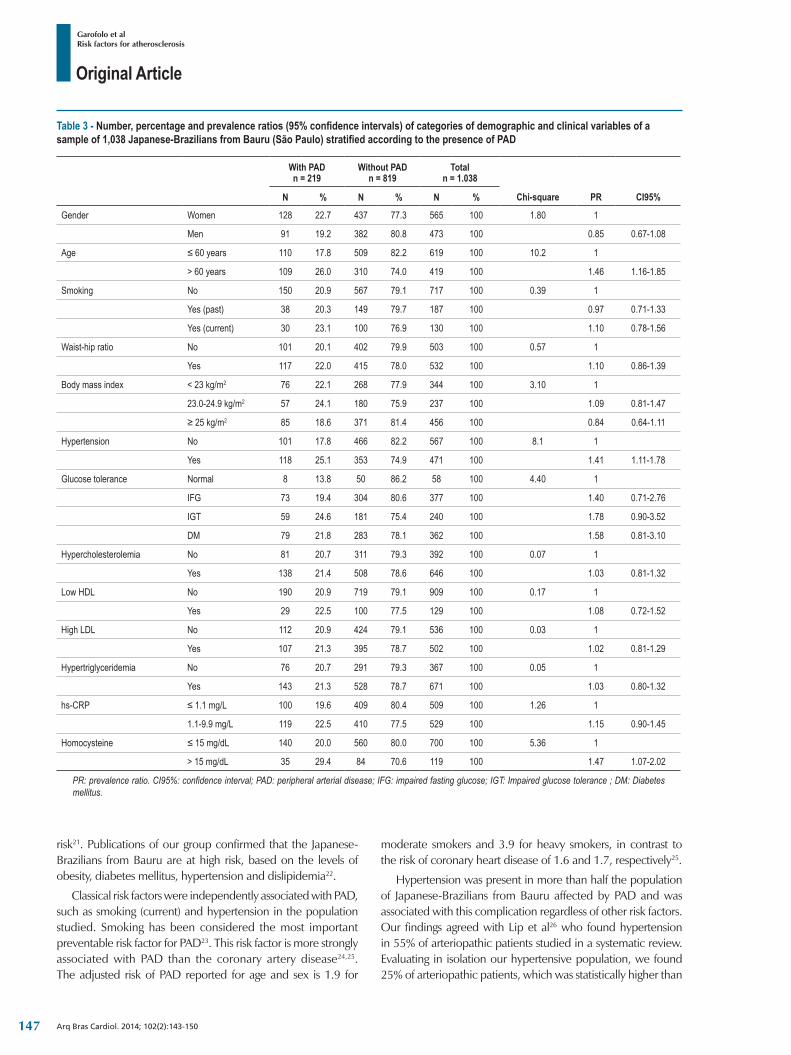
Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
risk21. Publications of our group confirmed that the Japanese-Brazilians from Bauru are at high risk, based on the levels of obesity, diabetes mellitus, hypertension and dislipidemia22.
Classical risk factors were independently associated with PAD, such as smoking (current) and hypertension in the population studied. Smoking has been considered the most important preventable risk factor for PAD23. This risk factor is more strongly associated with PAD than the coronary artery disease24,25. The adjusted risk of PAD reported for age and sex is 1.9 for
moderate smokers and 3.9 for heavy smokers, in contrast to the risk of coronary heart disease of 1.6 and 1.7, respectively25.
Hypertension was present in more than half the population of Japanese-Brazilians from Bauru affected by PAD and was associated with this complication regardless of other risk factors. Our findings agreed with Lip et al26 who found hypertension in 55% of arteriopathic patients studied in a systematic review. Evaluating in isolation our hypertensive population, we found 25% of arteriopathic patients, which was statistically higher than
Table 3 ‑ Number, percentage and prevalence ratios (95% confidence intervals) of categories of demographic and clinical variables of a sample of 1,038 Japanese-Brazilians from Bauru (São Paulo) stratified according to the presence of PAD
With PAD n = 219
Without PAD n = 819
Total n = 1.038
N % N % N % Chi-square PR CI95%
Gender Women 128 22.7 437 77.3 565 100 1.80 1
Men 91 19.2 382 80.8 473 100 0.85 0.67-1.08
Age ≤ 60 years 110 17.8 509 82.2 619 100 10.2 1
> 60 years 109 26.0 310 74.0 419 100 1.46 1.16-1.85
Smoking No 150 20.9 567 79.1 717 100 0.39 1
Yes (past) 38 20.3 149 79.7 187 100 0.97 0.71-1.33
Yes (current) 30 23.1 100 76.9 130 100 1.10 0.78-1.56
Waist-hip ratio No 101 20.1 402 79.9 503 100 0.57 1
Yes 117 22.0 415 78.0 532 100 1.10 0.86-1.39
Body mass index < 23 kg/m2 76 22.1 268 77.9 344 100 3.10 1
23.0-24.9 kg/m2 57 24.1 180 75.9 237 100 1.09 0.81-1.47
≥ 25 kg/m2 85 18.6 371 81.4 456 100 0.84 0.64-1.11
Hypertension No 101 17.8 466 82.2 567 100 8.1 1
Yes 118 25.1 353 74.9 471 100 1.41 1.11-1.78
Glucose tolerance Normal 8 13.8 50 86.2 58 100 4.40 1
IFG 73 19.4 304 80.6 377 100 1.40 0.71-2.76
IGT 59 24.6 181 75.4 240 100 1.78 0.90-3.52
DM 79 21.8 283 78.1 362 100 1.58 0.81-3.10
Hypercholesterolemia No 81 20.7 311 79.3 392 100 0.07 1
Yes 138 21.4 508 78.6 646 100 1.03 0.81-1.32
Low HDL No 190 20.9 719 79.1 909 100 0.17 1
Yes 29 22.5 100 77.5 129 100 1.08 0.72-1.52
High LDL No 112 20.9 424 79.1 536 100 0.03 1
Yes 107 21.3 395 78.7 502 100 1.02 0.81-1.29
Hypertriglyceridemia No 76 20.7 291 79.3 367 100 0.05 1
Yes 143 21.3 528 78.7 671 100 1.03 0.80-1.32
hs-CRP ≤ 1.1 mg/L 100 19.6 409 80.4 509 100 1.26 1
1.1-9.9 mg/L 119 22.5 410 77.5 529 100 1.15 0.90-1.45
Homocysteine ≤ 15 mg/dL 140 20.0 560 80.0 700 100 5.36 1
> 15 mg/dL 35 29.4 84 70.6 119 100 1.47 1.07-2.02
PR: prevalence ratio. CI95%: confidence interval; PAD: peripheral arterial disease; IFG: impaired fasting glucose; IGT: Impaired glucose tolerance ; DM: Diabetes mellitus.
147
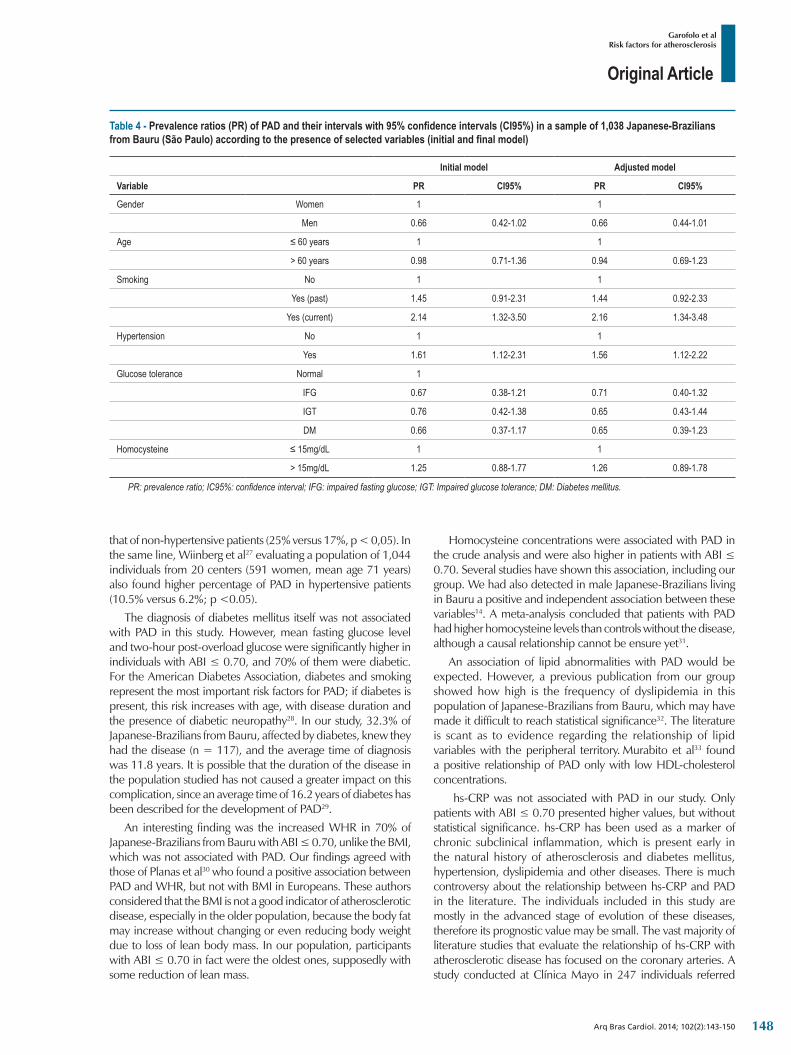
Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
that of non-hypertensive patients (25% versus 17%, p < 0,05). In the same line, Wiinberg et al27 evaluating a population of 1,044 individuals from 20 centers (591 women, mean age 71 years) also found higher percentage of PAD in hypertensive patients (10.5% versus 6.2%; p <0.05).
The diagnosis of diabetes mellitus itself was not associated with PAD in this study. However, mean fasting glucose level and two-hour post-overload glucose were significantly higher in individuals with ABI ≤ 0.70, and 70% of them were diabetic. For the American Diabetes Association, diabetes and smoking represent the most important risk factors for PAD; if diabetes is present, this risk increases with age, with disease duration and the presence of diabetic neuropathy28. In our study, 32.3% of Japanese-Brazilians from Bauru, affected by diabetes, knew they had the disease (n = 117), and the average time of diagnosis was 11.8 years. It is possible that the duration of the disease in the population studied has not caused a greater impact on this complication, since an average time of 16.2 years of diabetes has been described for the development of PAD29.
An interesting finding was the increased WHR in 70% of Japanese-Brazilians from Bauru with ABI ≤ 0.70, unlike the BMI, which was not associated with PAD. Our findings agreed with those of Planas et al30 who found a positive association between PAD and WHR, but not with BMI in Europeans. These authors considered that the BMI is not a good indicator of atherosclerotic disease, especially in the older population, because the body fat may increase without changing or even reducing body weight due to loss of lean body mass. In our population, participants with ABI ≤ 0.70 in fact were the oldest ones, supposedly with some reduction of lean mass.
Homocysteine concentrations were associated with PAD in the crude analysis and were also higher in patients with ABI ≤ 0.70. Several studies have shown this association, including our group. We had also detected in male Japanese-Brazilians living in Bauru a positive and independent association between these variables14. A meta-analysis concluded that patients with PAD had higher homocysteine levels than controls without the disease, although a causal relationship cannot be ensure yet31.
An association of lipid abnormalities with PAD would be expected. However, a previous publication from our group showed how high is the frequency of dyslipidemia in this population of Japanese-Brazilians from Bauru, which may have made it difficult to reach statistical significance32. The literature is scant as to evidence regarding the relationship of lipid variables with the peripheral territory. Murabito et al33 found a positive relationship of PAD only with low HDL-cholesterol concentrations.
hs-CRP was not associated with PAD in our study. Only patients with ABI ≤ 0.70 presented higher values, but without statistical significance. hs-CRP has been used as a marker of chronic subclinical inflammation, which is present early in the natural history of atherosclerosis and diabetes mellitus, hypertension, dyslipidemia and other diseases. There is much controversy about the relationship between hs-CRP and PAD in the literature. The individuals included in this study are mostly in the advanced stage of evolution of these diseases, therefore its prognostic value may be small. The vast majority of literature studies that evaluate the relationship of hs-CRP with atherosclerotic disease has focused on the coronary arteries. A study conducted at Clínica Mayo in 247 individuals referred
Table 4 ‑ Prevalence ratios (PR) of PAD and their intervals with 95% confidence intervals (CI95%) in a sample of 1,038 Japanese-Brazilians from Bauru (São Paulo) according to the presence of selected variables (initial and final model)
Initial model Adjusted model
Variable PR CI95% PR CI95%
Gender Women 1 1
Men 0.66 0.42-1.02 0.66 0.44-1.01
Age ≤ 60 years 1 1
> 60 years 0.98 0.71-1.36 0.94 0.69-1.23
Smoking No 1 1
Yes (past) 1.45 0.91-2.31 1.44 0.92-2.33
Yes (current) 2.14 1.32-3.50 2.16 1.34-3.48
Hypertension No 1 1
Yes 1.61 1.12-2.31 1.56 1.12-2.22
Glucose tolerance Normal 1
IFG 0.67 0.38-1.21 0.71 0.40-1.32
IGT 0.76 0.42-1.38 0.65 0.43-1.44
DM 0.66 0.37-1.17 0.65 0.39-1.23
Homocysteine ≤ 15mg/dL 1 1
> 15mg/dL 1.25 0.88-1.77 1.26 0.89-1.78
PR: prevalence ratio; IC95%: confidence interval; IFG: impaired fasting glucose; IGT: Impaired glucose tolerance; DM: Diabetes mellitus.
148

Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
for investigation of asymptomatic PAD using ABI also found no association between high levels of hs-CRP and PAD34.
There is evidence that the concentration of CRP has an hereditary component. It was found that certain polymorphisms in the PCR gene were able to influence their blood concentrations35. Genetic epidemiology has assisted in obtaining evidence about the involvement of CRP in atherosclerosis because, since PCR is causally involved in atherosclerosis, individuals carrying alleles that promote high plasma concentrations of CRP would present an increased risk of cardiovascular disease, where this risk is proportional to increased PCR35,36. However, studies published35,36 are still not able to ensure a causal role of CRP in atherosclerosis.
Our data indicated that, with the severity of PAD, there was an increase in the numbers of major cardiovascular risk factors, and individuals with ABI values ≤ 0.70 had the worst cardiometabolic profile. There is a need for early diagnosis and treatment of PAD, since its presence indicates widespread atherosclerotic process, compromising the survival of the individuals. Belch et al37 considered PAD a distinct atherothrombotic syndrome that is able to predict the occurrence of stroke, AMI and death. In the absence of concomitance with coronary disease, the PAD has been undertreated and poorly controlled38.
The REACH Registry39 a multicenter study of patients with established arterial disease (coronary disease, cerebrovascular or peripheral disease), concluded that the profile of risk factors is similar in the regions analyzed, with a high proportion of hypertensive patients (81.8%), diabetic patients ( 44.3%) and patients with hypercholesterolemia (72.4%). The treatment of these factors is inadequate and there is disparity between the established guidelines and clinical practice in sick individuals or patients at risk for atherothrombotic disease.
ConclusionOur study shows a high percentage of subclinical
atherosclerotic disease that is similar to other populations of adverse cardiometabolic profile. High frequencies of metabolic disorders in this population may explain the independent relationship of PAD only with smoking and hypertension but not with other classical risk factors. The associations with modifiable risk factors (smoking and hypertension) should serve to motivate and guide interventions and thereby reduce the cost to the health system.
Author contributionsConception and design of the research, Acquisition of data,
Writing of the manuscript and Critical revision of the manuscript for intellectual content: Garofolo L, Ferreira SRG; Analysis and interpretation of the data: Garofolo L, Ferreira SRG, Miranda Junior F; Statistical analysis: Garofolo L; Obtaining funding: Ferreira SRG.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThis study was funded by FAPESP.
Study AssociationThis article is part of the thesis of doctoral submitted by Luciana
Garofolo, from UNIFESP.
1. Ministério da Saúde. Saúde Brasil 2008: 20 anos de Sistema Único de Saúde (SUS) no Brasil, Brasília/DF, 2009. [Citado em 2013 ago 10]. Disponível em http://portal.saude.gov.br/portal/arquivos/pdf/ra t_brasil_2008_web_20_11.ppf
2. Fowkes F, Rudan D, Rudan I, Aboyans V, Denenberg JO, McDermott MM, et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: a systematic review and analysis. Lancet. 2013;382(9901):1329-40.
3. Criqui MH, Langer RD, Fronek A, Feigelson HS, Klauber MR, McCann TJ, et al. Mortality over a period of 10 years in patients with peripheral arterial disease. N Engl J Med. 1992;326(6):381-6.
4. Margolis J, Barron JJ, Grochulski WD. Health care resources and costs for treating peripheral arterial disease in a managed care population: results for analysis of administrative claims data. J Manag Care Pharm. 2005;11(9):727-34.
5. Gabriel S, Serafim P, Freitas C, Tristão CK, Taniguchi RS, Beteli CB, et al. Doença arterial obstrutiva periférica e índice tornozelo-braço em pacientes submetidos à angiografia coronariana. Rev Bras Cir Cardiovasc. 2007;22(1):49-59.
6. Fujimoto WY, Leonetti DL, Kinyoun JL, Newell-Morris L, Shuman WP, Storov WC, et al. Prevalence of diabetes mellitus and impaired glucose tolerance among second generation Japanese American men. Diabetes. 1987;36(6):721-9.
7. Lerario DD, Gimeno SG, Franco LJ, Iunes M, Ferreira SR. Weight excess and abdominal fat in the metabolic syndrome among Japanese-Brazilians. Rev Saúde Pública. 2002;36(1):4-11.
8. Examination Committee of Criteria for ‘Obesity Disease’ in Japan, Japan Society for the Study of Obesity (JASO). New criteria for ‘obesity disease’ in Japan. Circ J. 2002;66(11):987-92.
9. Steering Committee of the Western Pacific Region of the World Health Organization. The International Obesity Task Force (2000). The Asia-Pacific perspective: redefining obesity and its treatment. Melbourne, Australia: Health Communications Australia Pty Limited. [Cited in 2013 Jan 10]. Available from: http://www.diabetes.com.au/research/reportobesity.htm
10. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure: (JNC VII) 2004. [Cited in 2013 Aug 8]. Available from: http://www.nhlbi.nih.gov/guidelines/hypertension/jnc7full.pdf
11. Basevi V, Di Mario S, Morciano C, Nonino F, Magrini N. Comment on: American Diabetes Association. Standards of medical care in diabetes--2011. Diabetes Care 2011;34(Suppl. 1):S11-S61. Diabetes Care. 2011 May;34(5):e53. Erratum in Diabetes Care. 2011 Aug;34(8):1887.
12. Executive Summary of the Report of the Third Report of the National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults (Adults Treatment Panel III). JAMA. 2001;285(19):2486-97.
References
149
Original Article
Garofolo et alRisk factors for atherosclerosis
Arq Bras Cardiol. 2014; 102(2):143-150
13. Becker MA, Schumacher Jr. Febuxostat compared with allopurinol in patients with hyperuricemia and gout. N Engl J Med. 2005;353(23):2450-61.
14. Garofolo L, Barros N Jr, Miranda F Jr, D’Almeida V, Cardien LC, Ferreira SR. Association of increased levels of homocysteine and peripheral arterial disease In Japanese-Brazilian population. Eur J Vasc Endovasc Surg. 2007;34(1):23-8.
15. Pfeiffer CM, Huff DL, Gunter EW. Rapid and accurate HPLC assay for plasma total homocysteine and cysteine in a clinical laboratory setting. Clin Chem. 1999;45(2):290-2.
16. Norgren L, Hiatt WR, Dormandy JA, Nehler MR, Harris KA, Fowkes FG; TASC II Working Group. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J Vasc Surg. 2007;45 Suppl S:S5-67.
17. McDermott MM, Green D, Greenland P, Liu k, Criqui MH, Chan C, et al. Relation of levels of haemostatic levels and inflammatory markers to the ankle brachial in of hemostatic factors and inflammatory markers to the ankle brachial index. Am J Cardiol. 2003;92(2):194-9.
18. Ferreira SR, Almeida-Pittito B, Japanese-Brazilian Diabetes Study Group (JBDS Group). Reflexão sobre a imigração japonesa no Brasil sob o ângulo da adiposidade corporal. Arq Bras Endocrinol Metab. 2009;53(2):175-82.
19. Hirsch AT, Criqui MH, Treat-Jacobson D. Peripheral arterial disease detection, awareness, and treatment in primary care. JAMA. 2001;286(11):1317-24.
20. Elhadd TA, Robb R, Jung RT, Stonebrigde PA, Belch JJ. Pilot study of prevalence of asymptomatic peripheral arterial occlusive disease in patients with diabetes attending a hospital clinic. Practical Diabetes Int. 1999;16(6):163-6.
21. Makdisse M, Pereira AC, Brasil DP, Borges JL, Machado-Coelho JL, Krieger JE, et al. Prevalência dos fatores de risco associados à doença arterial periférica no Projeto Corações do Brasil. Arq Bras Cardiol. 2008;91(6):402-14.
22. Siqueira AF, Franco LJ, Gimeno SG, Matsumura LK, Barros-Junior N, Ferreira SR. Macrovascular disease in a Japanese-Brazilian population of high prevalence of metabolic syndrome: associations with classical and non-classical risk factors. Atherosclerosis. 2007;195(1):160-6.
23. Erb W. Klinische beiträge zur Pathologie des intermittierenden Hinkens. Munch Med Wochenschr. 1911;2:2487.
24. Fagerström K. The epidemiology of smoking: health consequences and benefits of cessation. Drugs. 2002;62 Suppl 2:1-9.
25. Price JF, Mowbray PI, Lee AJ, Rumley A, Lowe GD, Fowkes FG. Relationship between smoking and cardiovascular risk factors in the development of peripheral arterial disease and coronary artery disease. Edinburgh artery study. Eur Heart J. 1999;20(5):344-53.
26. Lip GY, Makin AJ. Treatment of hypertension in peripheral arterial disease. Cochrane Database Syst Rev. 2003;(4):CD003075.
27. Wiinberg N, Mehlsen J. High prevalence of peripheral arterial disease in hypertension. Am J Hypertens. 2005;18:46A-47A.
28. Clark N. Peripheral arterial disease in people with diabetes. Diabetes Care. 2003;26(12):3333-41.
29. Al-Delaimy WK, Merchant AT, Rimm EB, Willett WC, Stampfer MJ, Hu FB. Effect of type 2 diabetes and its duration on the risk of peripheral arterial disease among men. Am J Med. 2004;116(4):236-40.
30. Planas A, Clará A, Pou JM, Vidal-Barraquer F, Gasol A, de Moner A, et al. Relationship of obesity distribution and peripheral occlusive disease in elderly men. Int J Obes. 2001;25(7):1068-70.
31. Khandanpour N, Loke YK, Meyer FJ, Jennings B, Armon MP. Homocysteine and peripheral arterial disease: systematic review and meta-analysis. Eur J Vasc Endovasc Surg. 2009;38(3):316-22.
32. Siqueira AF, Harima HA, Osiro K, Hirai AT, Gimeno SG, Ferreira SR. Distúrbios do perfil lipídico são altamente prevalentes em população nipo-brasileira. Arq Bras Endocrinol Metab. 2008;52(1):40-6.
33. Murabito JM, Evans JC, Nieto K, Larson MG, Levy D, Wilson PW. Prevalence and clinical correlates of peripheral arterial disease in the Framingham Offspring Study. Am Heart J. 2002;143(6):961-5.
34. Santos S, Rooke TW, Bailey KR, McConnell JP, Kullo I. Relation of markers of inflammation (C-reactive protein, white blood cell count, and lipoprotein associated phospholipase A2) to the ankle-brachial index. Vasc Med. 2004;9(3):171-6.
35. Brul DJ, Serrano N, Zito F, Jones L, Montgomery HE, Rumley A, et al. Human CRP gene polymorphism influences CRP levels: implications for the prediction and pathogenesis of coronary heart disease. Atheroscler Thromb Vasc Biol. 2003;23(11):2063-9.
36. Elliot P, Chambers JC, Zhang W, Clarke R, Hopewell JC, Peden JF, et al. Genetic Loci associated with C-reactive protein levels and risk of coronary heart disease. JAMA. 2009;302(1):37-48.
37. Belch JJ, Topol EJ, Agnelli G, Bertrand M, Caloff RM, Clement DL, et al. Critical issues in peripheral arterial disease detection and management. Arch Intern Med. 2003;163(8):884-92.
38. Selvin E, Hirsch AT. Contemporary risk factor control and walking dysfunction in individuals with peripheral arterial disease: NHANES 1999-2004. Atherosclerosis. 2008;201(2):425-33.
39. Bhatt DL, Steg PG, Ohman EM, Hirsch AT, Ikeda Y, Mas JL, et al; REACH Registry Investigators. International prevalence, recognition, and treatment of cardiovascular risk factors in outpatients with atherothrombosis. JAMA. 2006;295(2):180-9.
150

Original Article
Time of Exercise as Indicator of Quality Control in Ergometry ServicesRomeu Sergio Meneghelo2, Samira Saady Morhy2, Paola Zucchi1Grupo Interdepartamental de Economia da Saúde-GRIDES-Universidade Federal de São Paulo-UNIFESP1; Hospital Israelita Albert Einstein São Paulo2, São Paulo, SP – Brazil
Mailing Address: Romeu Sergio Meneghelo • Rua Nicolau de Souza Queiroz, 194/161, Vila Mariana. Postal Code - 04105-000. São Paulo, SP - BrazilE-mail: [email protected] , [email protected] Manuscript received May 03, 2013; revised September 01, 2013; accepted September 19, 2013.
DOI: 10.5935/abc.20140005
Abstract
Background: The search for quality requires assessment tools in the various subdivisions of a health complex. In diagnostic medicine, they are scarce and in ergometry suggestions of indicators were not found.
Objective: To establish indicator for quality control on ergometry based on III Guidelines of the Brazilian Cardiology Society About Ergometric Test; to verify the percentage of tests that have presented the indicator within the compliance in two services of the same institution before and after the publication of the document.
Methods: A critical analysis of the guidelines in the search for indicator that would present: accuracy, reliability, simplicity, validity, sensitivity and ability to quantitatively measure the variations in the behavior of quality criteria and that would be applicable to all tests. The indicator was applied in tests of 2010 and 2011 prior to the publication, and after it was adopted by two services of the same institution.
Results: The indicator that has met the criteria was the percentage of ergometric tests with exercise duration between 8 and 12 minutes. In the years 2010 and 2011, respectively, the percentage of ergometric tests within compliance were 85.5% and 86.1% (p = 0.068) at the General Hospital, and 81.5% and 85.7% (p <0.001) the Service of Periodic Health Assessment.
Conclusion: The exercise time between 8 and 12 minutes can be used as a quality criterion in ergometric and services where it was applied, at least 80% of the ergometric tests were compliant.(Arq Bras Cardiol. 2014; 102(2):151-156)
Keywords: Ergometry; measures; exercise; quality indicators, health care.
IntroductionThe implementation of quality programs1 in public and
private health services, as well as its increase in those that are already in course, is growing in Brazil. The adoption of indicators as tools for control of programs is necessary in this context, but the institutions, due to their complexities and multiple subdivisions, not always present specific indicators for each one of their areas. The search for quality requires that assessment tools should exist in each subdivision of a complex of health. Except for clinical laboratories and pathology anatomy that for years have indicators in their processes, there is a shortage of them to other areas of diagnostic medicine2. Particularly, in the context of the ergometric tests, it was not possible to find the proposition of indicators for this area in indexed publications. Whereas examination is noninvasive, but of risk, and it requires the informed consent form for its
conduction, one deducts that tools of quality control can be useful and should be implemented.
In recent years, publications of Guidelines for medical practice, by specialty societies, have been increasing. The adoption of its recommendations has been strongly encouraged by representing the synthesis of reviews and analyzes of the available literature, according to the best scientific evidence.
The primary objective of this study was to establish a single indicator as a tool for quality control in ergometric testing, based on III Guidelines of the Brazilian Society of Cardiology about Ergometric Test3, which guides the Brazilian practice in the area. Secondly, the research sought to record the measurement of the chosen indicator before and after the publication of the guidelines in order to verify their baseline and any changes determined by its adoption as a reference for medical practice in the area. For this evaluation, ergometric tests were analyzed in a General Hospital and Service of Periodic Health Assessment, the same private institution.
Methods
Characteristics and criterion of choice of the indicatorInitially, the characteristics of the indicators to be identified
according to the criteria suggested by Saraceno and Levav4 were
151

Original Article
Meneghelo et al.Indicator for quality control in ergometry
Arq Bras Cardiol. 2014; 102(2):151-156
established. They preconize that the indicator should measure quantitatively the variations in the behavior of the quality criteria previously established and describe a reality, there it must have the characteristics of a valid measure in statistical terms. In order to make these assumptions more objective, the criteria suggested by Kluck et al5 were also incorporated into the present investigation, which are: accuracy, i.e., minimal chance of error, reliability, equal measures if they are made by other services with same methodology, simplicity, they may be collected by administrative staff; relevance, ability to measure the quality of the tests, validity, i.e., to effectively measure the phenomenon and sensitivity, the ability to detect variations in the behavior of the phenomenon that is examined.
The indicator chosen was the one that meet the highest number of characteristics considered: to be a quantitative measure able to indicate the quality of an ergometric test, to have accuracy, reliability, simplicity, relevance, validity and sensitivity, and to be applicable to all examinations.
Chartflow of the choiceCareful readings of the III Guidelines of the Brazilian Society
of Cardiology for Ergometric Test3 were made for the search of possible indicators of quality that would be derived from explicit and implicit recommendations. The indicators were analyzed according to the identified characteristics established beforehand and only one that would meet the highest number of criteria considered was chosen.
Evaluation of indicator values before and after the publication of Guidelines
The indicator chosen was applied in ergometric tests carried out at two moments: from January to September 2010, period prior to the publication of the Guidelines, and January-December 2011, at which time the guidelines were adopted as a standard. Data were collected in the Ergometry Sector of the General Hospital and in the specific Service of Periodic Health Assessment, both at a sole institution. Finally, a comparison was made of the indicator values at the two periods considered. No specific instruction was given to the physicians who performed the tests, after the publication of the Guidelines, except for the information that they should have read, understood and applied. In both systems, the executors of the test have always had the freedom to choose the protocol they deemed pertinent.
Statistical AnalysisAfter the definition of the indicator for quality control in
ergometric testing, it was evaluated the percentage of tests considered complaint performed in both services (Ergometry Sector of the General Hospital and Service of Periodic Health Assessment) in two periods: before the publication of guidelines (2010) and after standardization according to the Guidelines (2011). The results were summarized as absolute and relative frequencies (percentages). For comparison between the two periods for compliance examinations, we applied a Pearson’s chi-square test with Yates correction for continuity under the assumption that the tests performed in
the two periods within the same sector were independent. It was considered the usual significance level of 0.05. The statistical software was SPSS, version 19.0.
Results
Indicator chosenReadings and analysis of III Guidelines of the Brazilian
Society of Cardiology on Ergometric Test3 enabled to identify only two possible indicators, considering the criteria previously chosen. They were: exercise time of 10 minutes, with acceptable variations between 8 and 12 minutes recommended for an ergometric test, according to the item “5.6 - Choose the ergometer and protocol” of the document, and others described in “Item” 6.3.1 - Heart Rate”, where it is defined that normal behavior in the test is the patient achieve the recommended heart rate for its related age. The percentage of tests performed with treadmill exercise lasting 8 to 12 minutes was the one which met all criteria previously determined and was the chosen one4,5.
Evaluation of indicator values before and after the publication of Guidelines.
The results of the retrospective analysis of tests conducted in 2010 and 2011 in the Ergometry Sector of the General Hospital are shown in table 1. Data were available for 4,255 sequential tests in 2010, and 2,698 in 2011. It can be seen that the indicator chosen was considered optimal in the range 84.55% to 86.1% of the ergometric tests performed in 2010 and 2011, respectively (figure 1). We observed a reduction in the percentage of tests outside the range of 15.5% in 2010 to 14.9% in 2011, this difference was not statistically significant (p = 0.068). Considering only the tests below, the minimum time of 8 minutes for the duration of the exercise, the percentage decreased from 11.5% in 2010 to 8.8% in 2011. However, there was an increase in the percentage of tests over 12 minutes long. The percentage of 4% observed in 2010 rose to 5.1% in 2011.
The results of the application, retrospective, of the chosen indicator in ergometric tests performed in the years 2010 and 2011, in the Service of Periodic Health Assessment, are shown in Table 2. Data were available for 3,763 sequential tests in 2010, and 6,458 in 2011.
The indicator in this service in 2010, was in the optimal range considered in 81.5% of the ergometric tests performed, increasing to 85.7% in 2011 (figure 1). After standardization according to the guidelines, there was a reduction in the percentage of tests out of range (18.5% in 2010 to 14.3% in 2011, p <0.001). Considering only the tests below, the minimum time of 8 minutes for the duration of the test, the percentage decreased from 10.6% in 2010 to 7.1% in 2011. There was also a reduction of the percentage of tests lasting over 12 minutes between 2010 and 2011. The percentage of 7.9% in 2010 increased to 7.2% in 2011. It was observed in both periods and both services, the following protocols applied: Bruce modified, original Bruce, Ellestad and Naughton.
152
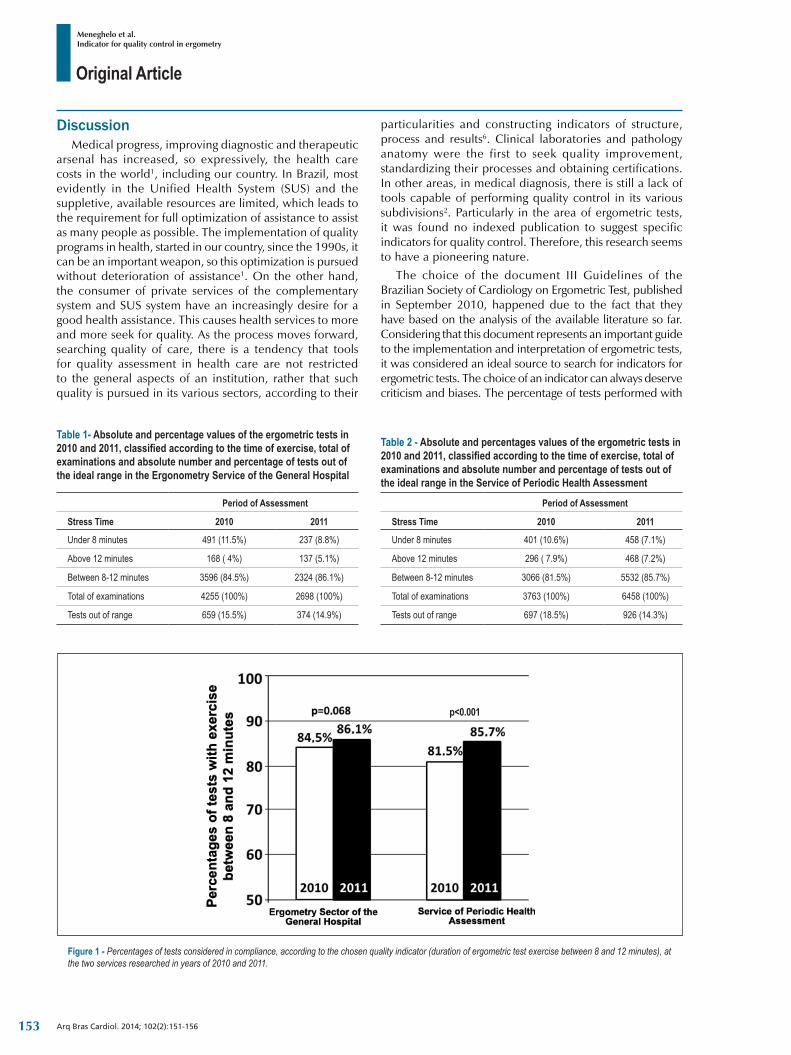
Original Article
Meneghelo et al.Indicator for quality control in ergometry
Arq Bras Cardiol. 2014; 102(2):151-156
Table 1‑ Absolute and percentage values of the ergometric tests in 2010 and 2011, classified according to the time of exercise, total of examinations and absolute number and percentage of tests out of the ideal range in the Ergonometry Service of the General Hospital
Period of Assessment
Stress Time 2010 2011
Under 8 minutes 491 (11.5%) 237 (8.8%)
Above 12 minutes 168 ( 4%) 137 (5.1%)
Between 8-12 minutes 3596 (84.5%) 2324 (86.1%)
Total of examinations 4255 (100%) 2698 (100%)
Tests out of range 659 (15.5%) 374 (14.9%)
Table 2 ‑ Absolute and percentages values of the ergometric tests in 2010 and 2011, classified according to the time of exercise, total of examinations and absolute number and percentage of tests out of the ideal range in the Service of Periodic Health Assessment
Period of Assessment
Stress Time 2010 2011
Under 8 minutes 401 (10.6%) 458 (7.1%)
Above 12 minutes 296 ( 7.9%) 468 (7.2%)
Between 8-12 minutes 3066 (81.5%) 5532 (85.7%)
Total of examinations 3763 (100%) 6458 (100%)
Tests out of range 697 (18.5%) 926 (14.3%)
DiscussionMedical progress, improving diagnostic and therapeutic
arsenal has increased, so expressively, the health care costs in the world1, including our country. In Brazil, most evidently in the Unified Health System (SUS) and the suppletive, available resources are limited, which leads to the requirement for full optimization of assistance to assist as many people as possible. The implementation of quality programs in health, started in our country, since the 1990s, it can be an important weapon, so this optimization is pursued without deterioration of assistance1. On the other hand, the consumer of private services of the complementary system and SUS system have an increasingly desire for a good health assistance. This causes health services to more and more seek for quality. As the process moves forward, searching quality of care, there is a tendency that tools for quality assessment in health care are not restricted to the general aspects of an institution, rather that such quality is pursued in its various sectors, according to their
Figure 1 ‑ Percentages of tests considered in compliance, according to the chosen quality indicator (duration of ergometric test exercise between 8 and 12 minutes), at the two services researched in years of 2010 and 2011.
p<0.001
particularities and constructing indicators of structure, process and results6. Clinical laboratories and pathology anatomy were the first to seek quality improvement, standardizing their processes and obtaining certifications. In other areas, in medical diagnosis, there is still a lack of tools capable of performing quality control in its various subdivisions2. Particularly in the area of ergometric tests, it was found no indexed publication to suggest specific indicators for quality control. Therefore, this research seems to have a pioneering nature.
The choice of the document III Guidelines of the Brazilian Society of Cardiology on Ergometric Test, published in September 2010, happened due to the fact that they have based on the analysis of the available literature so far. Considering that this document represents an important guide to the implementation and interpretation of ergometric tests, it was considered an ideal source to search for indicators for ergometric tests. The choice of an indicator can always deserve criticism and biases. The percentage of tests performed with
153

Original Article
Meneghelo et al.Indicator for quality control in ergometry
Arq Bras Cardiol. 2014; 102(2):151-156
treadmill exercise lasting 8 to 12 minutes, which meets all the criteria previously determined4,5, represents the expertise of the physician performing the examination, after analyzing anamnesis data for assessing the functional capacity of an individual patient. It is a quantitative measurement able to indicate the quality of an ergometric test having accuracy, reliability, simplicity, relevance, validity and sensitivity.
The stress time execution, ideally of 10 minutes, with acceptable variations from 8 to 12 minutes have justifications in the literature that have not been thoroughly commented in the III Guidelines of the Brazilian Society of Cardiology, perhaps because it is synthetic document and easy to read to facilitate its intended full dissemination. Since 1973 it is already known that load exercise may trigger intense ST segment depression, compatible with myocardial ischemic response7.
Barnard et al7, applying a run of only 30 seconds, no heating, in 10 normal firefighters discovered slight depression of the ST segment in three of them, significant depression in three of them and four of them with normal electrocardiographic response. After heating, with normal ergometric test with of increasing load, the repetition of the experiment showed very slight depression in just two firefighters and normal response in eight firefighters. Since then it is known that ergometric tests with short duration mean an imposition of improper load to the patient in question, which can generate false positive results. Based on research that measured concomitantly intra-arterial pressure in the brachial artery, the rationale for the onset of ST segment depression was a reduction of the subendocardial coronary flow due to lack of adequate cardio-circulatory adjustments before a sudden and intense stress.
Also since 1991, it is known that prolonged ergometric tests can minimize possible ischemic electrocardiographic manifestations in patients with coronary artery disease8. Panza et al8 have performed two tests on a treadmill in 70 patients with known coronary artery disease after discontinuation of medication in use, using the Bruce protocol and increment loads protocol, in a more attenuated manner, of the National Institutes of Health (NIH) in Bethesda, United States. The exercise time was 6.8 minutes (SD +2) in Bruce Protocol and 14.1 minutes (SD +5) in the NIH protocol. They have had positive ergometric tests of 82% of patients with the Bruce protocol and only 67 % with the protocol in a more attenuated manner and of longer duration. This publication assessed the findings of Bruchfuhrer et al9 published in 1983, which tested 10 healthy subjects in different protocols on a treadmill and stationary bike, finding in both ergometers the time of 10 minutes as the optimal duration of stress to obtain the highest oxygen consumption for each individual. Tests lasting less than eight minutes led to an average reduction of higher oxygen consumption by 10%, and when lasting more than 17 minutes it has a reduction of 5%.
All these publications have guided the Guidelines10,11 on ergometic tests and the Guideline from the American Heart Association recommends values between 6 and 12 minutes10, and the Brazilian one recommends 8 to 12 minutes. As seen, the duration of stress during ergometric test is an important variable in the quality of the examination and it may generate
false positive and negative diagnostic results, if not proper, therefore it measures the actual quality of the process of conducting an ergometric test.
To make an ergometric test to be within compliance, according to the indicator implies that the performer has medical expertise to choose the appropriate protocol from among those recommended by the Guidelines, which are the original Bruce, modified Bruce or ramped, Ellestad, Balke and Naughton. These protocols have different intensities of work increase, enabling patients with very low physical ability until those well-conditioned, to perform exercise between 8 and 12 minutes. There is still the possibility of applying a ramp-type protocol, the principles advocate that the stress should be in the range of 8 to 12 minutes, whereas 10 minutes is the ideal time12.
Questionnaires are available in the literature for the estimate of prior functional capacity and they can be of use in order to reach such objectives13-15.
The indicator chosen meets the recommendations of Saraceno and Lavav4 because, as it was seen, it quantitatively measures the variations in the behavior of the quality criteria and describes a reality, which can be considered as a valid measurement in statistical terms.
Considering the recommendations has as objective from Kluck et al5 one may affirm that the indicator is accurate because it is a measure of time easily obtained in computerized systems for testing; it is reliable, enabling it to be measured by other services with the same methodology, it is simple, it can be collected by administrative staff only by observation of the report, without the use of subjectivity, without specific technical knowledge, it is relevant for measuring the quality of an ergometric test with broad support in the pertinent medical literature, it is valid because it measures effectively a quality of the test, and, finally, it is sensitive because it can detect the changes in the phenomenon behavior that is examined.
Another possible indicator identified to achieve maximal predicted heart rate, is based on the formula (220 - age in years) (SD = 11) and (208 to 0.7 x age in years) is also a quantitative measure capable of indicate the quality of an ergometric test; it has accuracy, reliability, simplicity, relevance, validity and sensitivity. However, several conditions can influence the behavior of heart rate in ergometric test: the patient’s functional capacity, the presence of anxiety, neurovegetative dystonia, hypothyroidism, hyperthyroidism, Chagas disease, anemia, among others, and particularly the action of agents operating in chronotropism. Due to these influences, which cannot be applied to all tests, the indicator is deprecated. Although it might be considered simple and it can be applied by administrative staff, their use implies the application of formulas.
The adoption of such an indicator tool for quality control, once implemented, requires the establishment of limits to some degree of acceptability, particularly in the early stages of implementation. In the present investigation it was sought to establish with the chosen indicator, the actual world of the ergometric practice, the values obtained in diagnostic and in the service of periodic health assessment. There were differences in the indications of the ergometric tests between two selected services in most patients. At the General Hospital, it was
154

Original Article
Meneghelo et al.Indicator for quality control in ergometry
Arq Bras Cardiol. 2014; 102(2):151-156
1. Ribeiro MJ, Madureira MC. Qualidade nos serviços de saúde. In: Zucchi P, Ferraz MB, Economia e gestão em saúde. Barueri (SP): Manole; 2010. p. 255-64.
2. Bittar OJ. Gestão de processos e certificação para qualidade em saúde. Rev Assoc Med Bras. 2000;46(1):70-6.
3. Meneghelo RS, Araujo CG, Stein R, Mastrocolla LE, Albuquerque PF, Serra SM, et al; Sociedade Brasileira de Cardiologia. III Diretrizes da Sociedade Brasileira de Cardiologia sobre teste ergométrico. Arq Bras Cardiol. 2010;95(5 supl. 1):1-26.
4. Saraceno B, Levav I. La evaluación de servicios de salud mental en la comunidad. In: OPAS/PALTEX. (Temas Salud Mental, n. 19). Washington, DC; 1992. p. 56-77.
5. Klück M, Guimarães JR, Ferreira J, Prompt CA. A gestão da qualidade assistencial do Hospital de Clínicas de Porto Alegre: implementação e validação de indicadores. RAS. 2002;4(16):27-32.
6. Donabedian A. The quality of care how can it be assessed? JAMA. 1988;260(12):1743-8.
7. Barnard RJ, MacAlpin R, Kattus AA, Buckberg GD. Ischemic response to sudden strenuous exercise in healthy men. Circulation. 1973;48(5):936-42.
8. Panza JA, Quyumi AA, Diodati JG, Callahan TS, Epstein SE. Prediction of the frequency and duration of ambulatory myocardial ischemia in patients with stable coronary artery disease by determination of the ischemic threshold from exercise testing: importance of the exercise protocol. J Am Coll Cardiol. 1991;17(3):657-63.
9. Buchfuhrer MJ, Hansen JE, Robinson TE, Sue DY, Wasserman K, Whipp BJ. Optimizing the exercise protocol for cardiopulmonary assessment. J Appl Physiol Respir Environ Exerc Physiol. 1983;55(5):1558-64.
10. Gibbons RJ, Abrams J, Chatterjee K, Daley J, Deedwania PC, Douglas JS, et al; American College of Cardiology; American Heart Association Task Force on practice guidelines (Committee on the Management of Patients With Chronic Stable Angina). ACC/AHA 2002 guideline update for the management of patient with chronic stable angina--summary article: a report of the American College of Cardiology/American Heart Association Task Force on practice guidelines (Committee on the Management of Patients With Chronic Stable Angina). J Am Coll Cardiol. 2003;41(1):159-68.
11. American Thoracic Society; American College of Chest Physicians. ATS/ACCP Statement on cardiopulmonary exercise testing. Am J Respir Crit Care Med. 2003;167(2):211-77.
12. Myers J, Bellin D. Ramp exercise protocols for clinical and cardiopulmonary exercise testing. Sports Med. 2000;30(1):23-9.
13. Myers J, Buchanan N, Walsh D, Kraemer M, McAuley P, Hamilton-Wessler M, et al. Comparison of the ramp versus standard exercise protocols. J Am Coll Cardiol. 1991;17(6):1334-42.
14. Myers J, Do D, Herbert W, Ribisl P, Froelicher VF. A nomogram to predict exercise capacity from a specific activity questionnaire and clinical data. Am J Cardiol. 1994;73(8):591-6.
15. Bader DS, McInnis KJ, Maguire TE, Pierce GL, Balady GJ. Accuracy of a pretest questionnaire in exercise test protocol selection. Am J Cardiol. 2000;85(6):767-70.
References
predominant the indications targeting diagnosis of coronary artery disease in patients with any suspicious symptoms to clarify or patients with risk factors for coronary artery disease.
Most of the patients in the service of periodic health assessment consisted of asymptomatic individuals belonging to companies that hired the service to assess the health of their employees. The selected services has the scope of pursuing quality and are composed by physicians experienced in the method and knowledge of literature. The results of 85% and 81% in 2010 may suggest that these may be possible goals for the indicator in services with the same characteristic.
The application of the indicator, after the publication of the III Guidelines of the Brazilian Society of Cardiology on Ergometric Test3, adopted as a reference for the ergometric test in both services, demonstrated increased of tests within the range of 8 and 12 minutes of exercise in one of them, therefore one may speculate that this occurred under the influence of the document. The comparison, however, took place from January to September 2010, and throughout the year 2011. The exclusion of data from the last three months of 2010 was due to the fact that the Guidelines3 were available on the Internet in October of that year, and their knowledge could contaminate the desired baseline.
Conclusions The percentage of realization of the ergometric test with
exercise time between 8 and 12 minutes may be used as a quality indicator in ergometry services. At places where it was applied, an incidence of at least 80% of ergometric tests were within compliance provided by the indicator. The adoption
of the III Guidelines of the Brazilian Society of Cardiology on Ergometric Test may has had only a discrete influence in the increase of number of tests within compliance in one out of the two services researched.
AcknowledgementAuthors thank Dr. Mariza Klück for her valuable suggestions,
which has been incorporated to this paper.
Author contributionsConception and design of the research, Acquisition of
data, Critical revision of the manuscript for intellectual content and Analysis and interpretation of the data: Meneghelo RS, Morhy SS, Zucchi P; Statistical analysis and Writing of the manuscript: Meneghelo RS, Zucchi P.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part submitted by Romeu S. Meneghelo´s
specialization course in Universidade Federal de São Paulo - UNIFESP.
155

Original Article
Meneghelo et al.Indicator for quality control in ergometry
Arq Bras Cardiol. 2014; 102(2):151-156 156
Original Article
Influence of Term of Exposure to High-Fat Diet-Induced Obesity on Myocardial Collagen Type I and IIIDanielle Cristina Tomaz da Silva1, Ana Paula Lima-Leopoldo2, André Soares Leopoldo2, Dijon Henrique Salomé de Campos1, André Ferreira do Nascimento1, Sílvio Assis de Oliveira Junior3, Carlos Roberto Padovani4, Antonio Carlos Cicogna1
Departamento de Clínica Médica, Faculdade de Medicina de Botucatu, Universidade Estadual Paulista (UNESP)1, Botucatu, SP; Departamento de Esportes, Centro de Educação Física e Desportos da Universidade Federal do Espírito Santo (UFES)2, Vitória, ES; Escola de Fisioterapia da Universidade Federal de Mato Grosso do Sul (UFMS)3, Campo Grande, MS; Departamento de Bioestatística do Instituto de Ciências Biológicas da Universidade Estadual Paulista (UNESP)4, Botucatu, SP - Brazil
Mailing Address: Antonio Carlos Cicogna •Universidade Estadual de São Paulo (UNESP), Departamento de Clínica Médica, Faculdade de Medicina de Botucatu, Rubião Júnior, S/N. Postal Code 18618-000, Botucatu, SP - Brazil.E-mail: [email protected] Manuscript received April 02, 2013; revised manuscript August 21, 2013; accepted August 22, 2013.
DOI: 10.5935/abc.20130232
Abstract
Background: Obesity is a risk factor for many medical complications; medical research has shown that hemodynamic, morphological and functional abnormalities are correlated with the duration and severity of obesity.
Objective: Present study determined the influence of term of exposure to high-fat diet-induced obesity on myocardial collagen type I and III.
Methods: Thirty-day-old male Wistar rats were randomly distributed into two groups: a control (C) group fed a standard rat chow and an obese (Ob) group alternately fed one of four palatable high-fat diets. Each diet was changed daily, and the rats were maintained on their respective diets for 15 (C15 and Ob15) and 30 (C30 and Ob30) consecutive weeks. Obesity was determined by adiposity index.
Results: The Ob15 group was similar to the C15 group regarding the expression of myocardial collagen type I; however, expression in the Ob30 group was less than C30 group. The time of exposure to obesity was associated with a reduction in collagen type I in Ob30 when compared with Ob15. Obesity did not affect collagen type III expression.
Conclusion: This study showed that the time of exposure to obesity for 30 weeks induced by unsaturated high-fat diet caused a reduction in myocardial collagen type I expression in the obese rats. However, no effect was seen on myocardial collagen type III expression. (Arq Bras Cardiol. 2014; 102(2):157-164)
Keywords: Obesity; High-fat diet; Collagen Type I; Collagen Type III; Myocardium.
IntroductionObesity is a chronic metabolic disorder characterized
by excessive accumulation of adipose tissue in relation to lean tissue. Currently, it is a global epidemic and a major public health problem that affects developed as well as developing countries1,2. Behaviors associated with a modern industrialized society, including a sedentary lifestyle, inadequate eating habits or a combination of both, have led to an increasing prevalence of obesity3.
Obesity is also considered a risk factor for many medical complications, among them cardiovascular diseases4,5. Hemodynamic changes associated with hormonal ones
alter myocardial gene expression, promoting myocardial extracellular matrix remodeling6. Studies using either rabbits made obese by a high-fat diet7 or by genetic engineering, Zucker rats8, have reported an increase in myocardial collagen types I and III over 12 and 24 weeks, respectively. In contrast, Carroll et al9, found no change in the fraction of total collagen in obese rats subjected to a high-fat diet for 12 weeks. Previous studies carried out in our laboratory showed that Wistar rats made obese by a 15-week high fat diet10 and Wistar-Kyoto rats made obese by 20-week high fat and carbohydrate diet11 showed increased myocardial total collagen. In these studies, however, the fractions of collagen types I and III were not evaluated.
Medical research has shown that hemodynamic, morphological and functional abnormalities are correlated with the duration and severity of obesity12-14. Because of the scarcity of studies that have evaluated the influence of time of exposure to high fat diet-induced obesity on the fractions of myocardial collagen types I and III, this current study was designed to test the hypothesis that the time of exposure to obesity promotes a progressive increase in the amount of type I and type III myocardial collagen.
157

Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164
Methods
Animals and Experimental ProtocolAfter a 7-day period for acclimatization, 30-day-old
male Wistar rats were randomly assigned to one of two groups: control (C) and obese (Ob). The C group was fed a standard rat chow (RC Focus 1765, Agroceres®, Rio Claro, SP, Brazil) containing 12.3% of kilocalories from fat, 57.9% from carbohydrates, and 29.8% from protein, whereas the Ob group were fed one of four alternating high-fat diets (RC Focus 2413, 2414, 2415, and 2416, Agroceres®, Rio Claro, SP, Brazil) containing 49.2% of kilocalories from fat, 28.9% from carbohydrates, and 21.9% from protein. Each diet was changed daily, and the rats were maintained on their respective diets for 15 (C15 and Ob15; n = 22) and 30 (C30 and Ob30; n = 25) consecutive weeks. The high-fat diet was calorically rich compared to the standard diet (3.65 kcal/g vs. 2.95 kcal/g) due to the higher fat composition. The high-fat diet consisted of saturated and unsaturated fatty acids, which provided 20% and 80% of the fat-derived calories, respectively.
Rats were housed in individual cages in an environmentally-controlled clean-air room at 23 (± 3)°C with a 12-hour light/dark cycle and 60 (± 5)% relative humidity. All experiments and procedures were performed in accordance with the Guide for the Care and Use of Laboratory Animals, published by the National Research Council (1996) and were approved by the Faculdade de Medicina de Botucatu Ethics Committee (UNESP, Botucatu, SP, Brazil).
Nutritional, metabolic and endocrine profilesNutritional and metabolic profiles included adiposity
index, final body weight (FBW), and glucose tolerance; endocrine profiles included leptin and insulin concentrations. As obesity is defined as an excessive amount of body fat in relation to lean mass15, a criterion based on the adiposity index was used to determine obesity, according to data from earlier studies9,16.
After fasting for 12 to 15 hours, animals were anesthetized (using intraperitoneal sodium pentobarbital 50 mg/kg), decapitated, and thoracotomized; the fat pads of adipose tissue were dissected and weighed. The adiposity index was calculated by the following formula: adiposity index = (body fat [BF]/FBW) × 10017. Body fat was calculated as the sum the weight of the individual fat pads as follows: BF = epididymal fat + retroperitoneal fat + visceral fat.
As obesity can be accompanied by metabolic and endocrine disturbances18, all animals underwent testing for glucose tolerance, leptinemia and insulinemia. After 15 and 30 weeks of treatment, glucose tolerance and insulin resistance were evaluated in all animals through the glucose tolerance test (GTT). After a 4-to 6-hour fast, a blood sample was taken from the tip of the animal’s tail and collected in a heparinized tube. The blood glucose (as the basal condition) concentration of each animal was immediately determined using a handheld glucometer (Accuchek Advantage; Roche Diagnostics Co., Indianapolis, IN, USA). Subsequently, 2 g/kg of
glucose (Sigma-Aldrich®, St Louis, MO, USA) was given intravenously and blood glucose concentrations were measured after 15, 30, 60, 90, and 120 minutes19. Glucose intolerance was evaluated using the area under the curve (AUC) for glucose.
For hormonal analysis, trunk blood was collected in heparinized tubes and centrifuged at 3000 g for 15 minutes at 4°C. Serum leptin and insulin concentrations were determined by enzyme-linked immunosorbent assay (ELISA) using commercially available kits (Linco Research Inc., St. Louis, MO, USA).
Cardiovascular profileAs obesity can be associated with cardiovascular
comorbidities, the cardiovascular profile of the animals was also assessed, using systolic blood pressure, cardiac tissue morphology and left ventricular collagen types I and III protein expression.
Systolic blood pressureAt the end of the experiment, the systolic blood pressure
was assessed using the non-invasive tail-cuff method
with a Narco BioSystems® Electro-Sphygmomanometer (International Biomedical, Austin, TX, USA)20. The average of two readings was recorded for each measurement.
Morphological studiesThe heart was removed and dissected at the time of
euthanasia. LV weights, as well as their respective ratios with the tibia were determined as indexes of cardiac remodeling.
Myocardial collagen types I and III protein expressionLeft ventricular tissue was analyzed by Western Blot7 to
quantify collagen types I and III protein expression. Briefly, ventricles isolated from control (C15 and C30; n = 6 each group) and obese (Ob15 and Ob30; n = 6 each group) rats were frozen with liquid nitrogen and homogenized in a buffer containing 10 mM Tris (pH 7.4), 100 Mm NaCl, 1 mM EDTA, 1 Mm EGTA, 1% Triton X-100, 10% glycerol, 0.1% sodium dodecyl sulfate (SDS), and 0.5% deoxycholate. The homogenate was centrifuged at 4oC for 20 minutes at 12000 rpm. The supernatant was collected and total protein content was determined by the Bradford Method (Bradford 1976). Samples were subjected to SDS-polyacrylamide gel electrophoresis (SDS-PAGE) in polyacrylamide gels (6% or 10% depending on protein molecular weight). After electrophoresis, proteins were electro-transferred to nitrocellulose membrane (BioRad Biosciences; NJ, USC). Sample weights (50 µg) and transfers were monitored for equality and efficiency, respectively, with the use of 0.5% Ponceau S staining of the blot membrane. The blotted membrane was then blocked (using 5% nonfat dry milk, 10 mmol/L Tris-HCl [pH 7.6], 150 mmol/L NaCl, and 0.1% Tween 20) for 2 hours at room temperature and incubated with specific antibodies overnight at 4oC. Binding of the primary antibody was detected with the use of peroxidase-conjugated secondary antibodies (anti-rabbit or anti-mouse
158

Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164
depending on the protein at a 1:10000 dilution and incubated for 1.5 hours at room temperature), developed by enhanced chemiluminescence (Amersham Biosciences, NJ, USA) and detected by autoradiography. Quantification analysis of the blots was performed with use of Scion Image software (Scion, based on NIH Image). Mouse monoclonal antibodies to collagen types I and III (1:10000) and mouse monoclonal antibodies to β-actin (1:1000) were obtained from Abcam (UK, Cambridge) and Santa Cruz Biotechnology (CA, USA), respectively. Targeted bands were normalized to the expression of cardiac β-actin.
Statistical analysisAll results were reported as mean ± standard deviation
and groups were evaluated using two-way analysis of variance (ANOVA) for independent samples. When significant differences were found (p < 0.05), Bonferroni post hoc test for multiple comparisons was carried out21. The level of significance considered was 5% (α = 0.05).
ResultsFigure 1 shows the general characteristics of animals
in groups C15, C30, Ob15 and Ob30. The high-fat diet caused an increase in FBW and in the index of adiposity in obese animals compared to respective controls at all times evaluated. The duration of exposure to obesity did not result in a significant difference in FBW and adiposity index between the C15 and C30 groups and between the Ob15 and Ob30 groups. There was no difference in systolic blood pressure between the C and Ob groups in the two study periods and that did not change with the time of exposure to obesity. The glucose AUC was higher in Ob groups compared with controls; the time of exposure did not affect glucose levels. Obesity promoted an increase in insulin and leptin levels in Ob groups compared to respective controls. Insulin levels did not change with the time of exposure to obesity; leptin levels were higher in the Ob30 group compared with the Ob15 groups.
As shown in Figure 2, the presence of obesity increased the weight of the left ventricle and as well as LV/tibia length ratio in the Ob15 group as compared to the C15 group. However, the LV/tibia length ratio was similar in the Ob30 and C30 groups, suggesting that exposure to obesity did not have any effect on this variable.
There was no difference in myocardial type I collagen expression between the groups Ob15 and C15 (Figure 3); however, protein expression was lower in the Ob30 group compared with the C30 group. The time of exposure to obesity also resulted in a reduction of collagen type I expression in the Ob30 group as compared with the Ob15 group. Obesity did not alter collagen type III expression, and the time of exposure to obesity did not influence expression of this collagen.
DiscussionThe main finding of this study was that the time of
exposure to obesity induced by an unsaturated high-fat diet
affected the expression of myocardial collagen type I, but had no effect on myocardial collagen type III. Obesity that is experimentally induced by diet most closely resembles obesity found in the human population and it has been frequently used to reproduce possible morphological, molecular, biochemical and functional changes in different organs of the human body9,16,22.
The high-calorie diet used in this experiment contained enough calories and was of sufficient duration to promote obesity in rats; it was likely due to the high unsaturated fat content of the diet, which has a higher energy density and greater storage capacity in the body. This study showed that the final body weight and the index of adiposity of obese animals were increased as compared to respective controls at all times evaluated, and these data are consistent with the literature22. However, the time of exposure to the diet did not alter these two variables, which were similar in the two time periods studied - 15 and 30 weeks.
The glucose load in the obese groups resulted in glucose intolerance during the two treatment periods, 15 and 30 weeks. Another important aspect is that time of exposure to obesity did not influence the glycemic profile between obese animals, as glucose intolerance seen in the first 15 weeks remained stable until the 30th week of the experimental protocol. Impaired glucose tolerance, an intermediate stage between normal glucose homeostasis and type 2 diabetes mellitus23, may be related to the development of insulin resistance in obese animals. In support of this assumption, our data show that obesity led to hyperinsulinemia at both evaluations. The results of this study are in agreement with authors who observed that obesity induced by a diet high in unsaturated fat promotes glucose intolerance, hyperinsulinemia and insulin resistance in a short period of time24-27 and these effects are prolonged28.
An increase in leptin serum concentrations after 15 and 30 weeks was seen in obese animals compared with their controls. The time of exposure to obesity influenced the level of this hormone, with increases seen from 15 weeks onward. Leptin concentrations are correlated with body fat, thereby influencing both lipogenesis and lipolysis29. In this study, although the index of adiposity remained the same in the Ob15 and Ob30 groups, leptin concentrations were higher in the Ob30 compared with the Ob15. This fact was likely due to the emergence of resistance to the action of this hormone after the 30th week. Other studies have shown that long periods of obesity promote leptin resistance, which consequently leads to an increase in this hormone14,24,30.
Although the increase in adipose tissue led to metabolic and hormonal alterations, obesity did not result in an increase in blood pressure after 15 and 30 weeks, which remained stable over the two periods studied. The mechanisms responsible for altering blood pressure include hyperactivity of the sympathetic nervous system31, increased activity of the renin-angiotensin-aldosterone system (RAAS)16,32,33 and oxidative stress31, which can result in peripheral vasoconstriction and increased renal sodium reabsorption. The lack of effect on blood pressure suggests that obesity does not alter those factors involved in blood pressure control. These results are in agreement with some authors who observed no change in blood pressure in obese
159
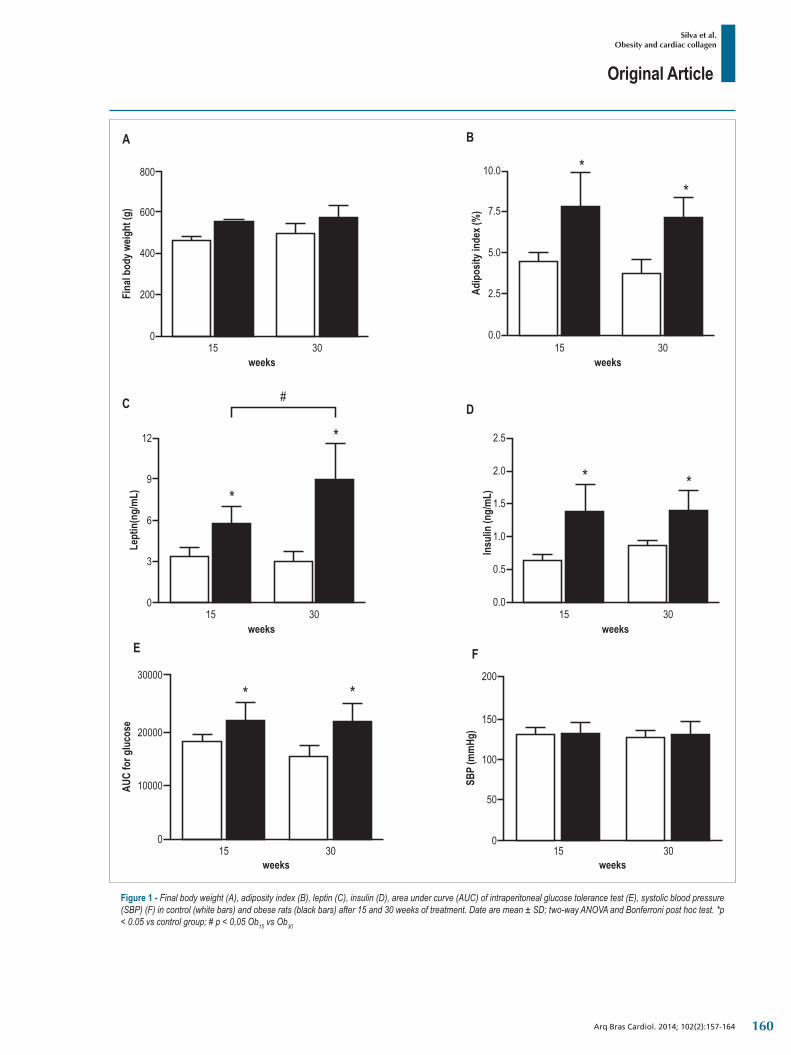
Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164
Figure 1 ‑ Final body weight (A), adiposity index (B), leptin (C), insulin (D), area under curve (AUC) of intraperitoneal glucose tolerance test (E), systolic blood pressure (SBP) (F) in control (white bars) and obese rats (black bars) after 15 and 30 weeks of treatment. Date are mean ± SD; two-way ANOVA and Bonferroni post hoc test. *p < 0.05 vs control group; # p < 0,05 Ob15 vs Ob30
160
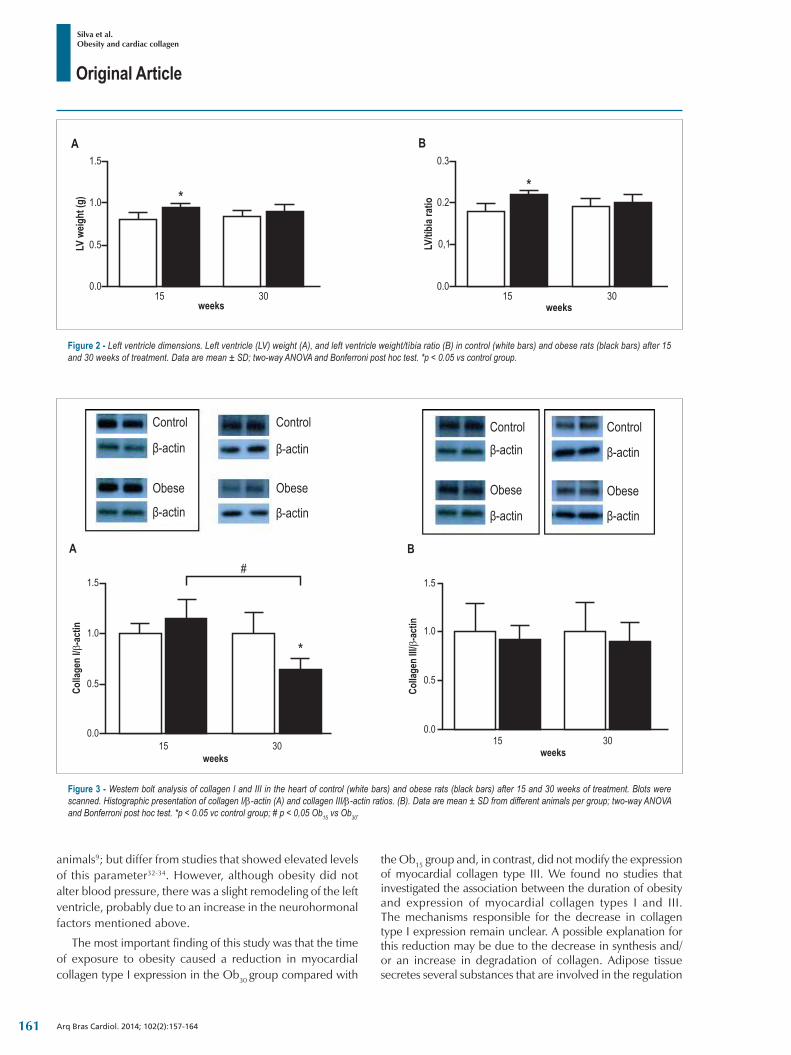
Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164
Figure 3 ‑ Westem bolt analysis of collagen I and III in the heart of control (white bars) and obese rats (black bars) after 15 and 30 weeks of treatment. Blots were scanned. Histographic presentation of collagen I/β-actin (A) and collagen III/β-actin ratios. (B). Data are mean ± SD from different animals per group; two-way ANOVA and Bonferroni post hoc test. *p < 0.05 vc control group; # p < 0,05 Ob15 vs Ob30.
Control Control Control Controlβ-actin β-actin β-actin
β-actin β-actin β-actin β-actin
β-actin
Obese Obese Obese Obese
Figure 2 ‑ Left ventricle dimensions. Left ventricle (LV) weight (A), and left ventricle weight/tíbia ratio (B) in control (white bars) and obese rats (black bars) after 15 and 30 weeks of treatment. Data are mean ± SD; two-way ANOVA and Bonferroni post hoc test. *p < 0.05 vs control group.
animals9; but differ from studies that showed elevated levels of this parameter32-34. However, although obesity did not alter blood pressure, there was a slight remodeling of the left ventricle, probably due to an increase in the neurohormonal factors mentioned above.
The most important finding of this study was that the time of exposure to obesity caused a reduction in myocardial collagen type I expression in the Ob30 group compared with
the Ob15 group and, in contrast, did not modify the expression of myocardial collagen type III. We found no studies that investigated the association between the duration of obesity and expression of myocardial collagen types I and III. The mechanisms responsible for the decrease in collagen type I expression remain unclear. A possible explanation for this reduction may be due to the decrease in synthesis and/or an increase in degradation of collagen. Adipose tissue secretes several substances that are involved in the regulation
161

Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164
of myocardial collagen, including the hormone leptin, which is produced mainly by adipocytes and is also synthesized by various tissues including the heart35. The effects of leptin on the heart have not been fully elucidated, but it has been thought to influence cardiomyocyte hypertrophy and regulate production of various components of the extracellular matrix of the myocardium that act on cardiac fibroblasts35. Although there is controversy about the association between leptin and myocardial collagen type I, such as increased expression of procollagen35-37 and decreased synthesis38, there is an agreement among authors that leptin increases the activity of metalloproteinases (MMP-2) 235-38 and mRNA expression of MMP-939,40, participants in myocardial collagen type I degradation. Therefore, it is possible that increased activity of both MMP-2 and MMP-9 is responsible for the reduction in myocardial collagen type I. As stated above, myocardial collagen type III did not change in obesity. No information was found in the literature as a possible explanation for this finding.
Importantly, our finding may have clinical relevance, as it shows that long-term obesity, common in patients, not accompanied by arterial hypertension, can cause a decrease in ventricular compliance due to the reduction in collagen type I. This phenomenon may result in a better adaptation of the heart to obesity because this pathology is associated with increased blood volume.
In conclusion, this study shows that the time of exposure to obesity induced by an unsaturated high-fat diet causes a reduction in myocardial collagen type I expression after 30 weeks, but no changes were seen in myocardial collagen type III. Future studies are needed to determine the mechanism responsible for the decrease in myocardial collagen type I and the lack of effect on collagen type III.
Sources of Funding:FAPESP - process n. 07/53267-3 and 08/50172-4.
AcknowledgmentsWe are grateful to José C. Georgette, Mário B. Bruno,
Sandra A. Fabio, Elenize J. Pereira, Sueli A. Clara, Vitor M. Souza, Camila R. C. Camacho and Corina J. Correa for their technical assistance. This manuscript has been proofread and edited by native English speakers with a related biomedical background in BioMed Proofreading (Cleveland, Ohio, USA).
Author contributionsConception and design of the research: da Silva DCT,
Padovani CR, Cicogna AC; Acquisition of data: da Silva DCT, Lima-Leopoldo AP, Leopoldo AS, de Campos DHS; Analysis and interpretation of the data: da Silva DCT, Lima-Leopoldo AP, Leopoldo AS, de Campos DHS, Nascimento AF, Oliveira Junior SA, Padovani CR, Cicogna AC; Statistical analysis: da Silva DCT, Padovani CR; Obtaining funding: Cicogna AC; Writing of the manuscript: da Silva DCT; Critical revision of the manuscript for intellectual content: da Silva DCT, Lima-Leopoldo AP, Nascimento AF, Oliveira Junior SA, Cicogna AC.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported.
Sources of FundingThis study was funded by FAPESP.
Study AssociationThis study is not associated with any thesis or dissertation
work.
1. Eckel RH, Barouch WW, Ershow AG. Report of the National Heart, Lung, and Blood Institute-National of Diabetes and Digestive and Kidney Diseases Working Group on the pathophysiology of obesity-associated cardiovascular disease. Circulation. 2002;105(24):2923-8.
2. Wong CY, O’ Moore-Sullivan T, Leano R, Byrne N, Beller E, Marwick TH. Alterations of left ventricular myocardial characteristics associated with obesity. Circulation. 2004;110(19):3081-7.
3. Stein CJ, Colditz GA. The epidemic of obesity. J Clin Endocrinol Metab. 2004;89(6):2522-5.
4. Malnick SD, Knobler H. The medical complications of obesity. QJM. 2006;99(9):565-79.
5. Poirier P, Giles TD, Bray GA, Hong Y, Stern JS, Pi-Sunyer X, et al; American Heart Association; Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Obesity and cardiovascular disease: pathophysiology, evaluation, and effect of weight loss: an update of the 1997 American Heart Association Scientific Statement on Obesity and Heart Disease from the Obesity Committee of the Council on Nutrition, Physical Activity, and Metabolism. Circulation. 2006;113(6):898-918.
6. Galinier M, Pathak A, Roncalli J, Massabuau P. [Obesity and cardiac failure]. Arch Mal Coeur Vaiss. 2005;98(1):39-45.
7. Carroll JF, Tyagi SC. Extracellular matrix remodelling in the heart of the homocysteinemic obese rabbit. Am J Hypertens. 2005;18(5 Pt 1):692-8.
8. Toblli JE, Cao G, DeRosa G, Forcada P. Reduced cardiac expression of plasminogen activator inhibitor 1 and transforming growth factor b1 in obese Zucker rats by perindopril. Heart. 2005;91(1):80-6.
9. Carroll JF, Zenebe WJ, Strange TB. Cardiovascular function in a rat model of diet-induced obesity. Hypertension. 2006;48(1):65-72.
10. Leopoldo AS, Sugizaki MM, Lima-Leopoldo AP, do Nascimento AF, Luvizotto Rde A, de Campos DH, et al. Cardiac remodeling in a rat model of diet-induced obesity. Can J Cardiol. 2010;26(8):423-9.
11. Oliveira SA Jr, Okoshi K, Lima-Leopoldo AP, Leopoldo AS, Campos DH, Martinez PF, et al. Nutritional and cardiovascular profiles of normotensive and hypertensive rats kept on a high fat diet. Arq Bras Cardiol. 2009;93(5):526-33.
12. Alpert MA. Obesity cardiomyopathy: pathophysiology and evolution of the clinical syndrome. Am J Med Sci. 2001;321(4):225-36.
References
162
Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164
13. Scaglione R, Dichiara A, Indovina A, Lipari R, Ganguzza A, Parrinello G, et al. Left ventricular diastolic and systolic function in normotensive obese subjects: influence of degree and duration of obesity. Eur Heart J. 1992;13(6):738-42.
14. Nascimento AF, Luvizotto RA, Leopoldo AS, Lima-Leopoldo AP, Seiva FR, Justulin LA Jr, et al. Long-term high-fat diet-induced obesity decreases the cardiac leptin receptor without apparent lipotoxicity. Life Sci. 2011;88(23-24):1031-8.
15. Nascimento TB, Baptista Rde F, Pereira PC, Campos DH, Leopoldo AS, Leopoldo AP, et al. Vascular alterations in high-fat diet-obese rats: role of endothelial L-arginine/NO pathway. Arq Bras Cardiol. 2011;97(1):40-5.
16. Boustany-Kari CM, Gong M, Akers WS, Guo Z, Cassis LA. Enhanced vascular contractility and diminished coronary artery flow in rats made hypertensive from diet-induced obesity. Int J Obes (Lond). 2007;31(11):1652-9.
17. Taylor BA, Phillips SJ. Detection of obesity QTLs on mouse chromosomes 1 and 7 by selective DNA pooling. Genomics. 1996;34(3):389-98.
18. Kopelman PG. Obesity as a medical problem. Nature. 2000;404(6778):635-43.
19. Ouwens DM, Boer C, Fodor M, de Galan P, Heine RJ, Maassen JA, et al. Cardiac dysfunction induced by high-fat diet is associated with altered myocardial insulin signalling in rats. Diabetologia. 2005;48(6):1229-37.
20. Pfeffer JM, Pfeffer MA, Frohlich ED. Validity of an indirect tail-cuff method for determining systolic arterial pressure in unanesthetized normotensive and spontaneously hypertensive rats. J Lab Clin Med. 1971;78(6):957-62.
21. Bayley BJ. Tables of the Bonferroni “t” statistic. J Am Stat Assoc. 1977;72:469-78.
22. Ghibaudi L, Cook J, Farley C, van Heek M, Hwa JJ. Fat intake affects adiposity, comorbidity factors, and energy metabolism of sprague-dawley rats. Obes Res. 2002;10(9):956-63.
23. Pereira LO, de Francischi RP, Lancha Jr AH. Obesidade: hábitos nutricionais, sedentarismo e resistência à insulina. Arq Bras Endocrinol Metab. 2003;47(2):111-27.
24. Woods SC, Seeley RJ, Rushing PA, D’Alessio DA, Tso P. A controlled high-fat diet induces an obese syndrome in rats. J Nutr. 2003;133(4):1081-7.
25. Huang BW, Chiang MT, Yao HT, Chiang W. The effect of high-fat and high-fructose diets on glucose tolerance and plasma lipid and leptin levels in rats. Diabetes Obes Metab. 2004;6(2):120-6.
26. Li L, Yang G, Li Q, Tang Y, Li K. High-fat- and Lipid-induced insulin resistance in rats: the comparison of glucose metabolism, plasm resistin and adiponectin levels. Ann Nutr Metab. 2006;50(6):499-505.
27. Winzell MS, Ahrén B. The high-fat diet-fed mouse: a model for studying mechanisms and treatment of impaired glucose tolerance and type 2 diabetes. Diabetes. 2004;53 Suppl 3:S215-9.
28. Nivoit P, Morens C, Van Assche FA, Jansen E, Poston L, Remacle C, et al. Established diet-induced obesity in female rats leads to offspring hyperphagia, adiposity and insulin resistance. Diabetologia. 2009;52(6):1133-42.
29. Ainslie DA, Proietto J, Fam BC, Thorburn AW. Short-term, high-fat diets lower circulating leptin concentrations in rats. Am J Clin Nutr. 2000;71(2):438-42.
30. Ren J, Zhu BH, Relling DP, Esberg LB, Ceylan-Isik AF. High-fat diet-induced obesity leads to resistance to leptin-induced cardiomyocyte contractile response. Obesity (Silver Spring). 2008;16(11):2417-23.
31. Pausova Z. From big fat cells to high blood pressure: a pathway to obesity-associated hypertension. Curr Opin Nephrol Hypertens. 2006;15(2):173-8.
32. Boustany CM, Bharadwaj K, Daugherty A, Brown DR, Randall DC, Cassis LA. Activation of the systemic and adipose renin-angiotensin system in rats with diet-induced obesity and hypertension. Am J Physiol Regul Integr Comp Physiol. 2004;287(4):R943-9.
33. Smith AD, Brands MW, Wang MH, Dorrance AM. Obesity-induced hypertension develops in young rats independently of the renin-angiotensin-aldosterone system. Exp Biol Med. 2006;231(3):282-7.
34. Dobrian AD, Davies MJ, Prewitt RL, Lauterio TJ. Development of hypertension in a rat model of diet-induced obesity. Hypertension. 2000;35(4):1009-15.
35. Schram K, De Girolamo S, Madani S, Munoz D, Thong F, Sweeney G. Leptin regulates MMP-2, TIMP-1 and collagen synthesis via p38 MAPK in HL-1 murine cardiomyocytes. Cell Mol Biol Lett. 2010;15(4):551-63.
36. Schram K, Wong MM, Palanivel R, No EK, Dixon IM, Sweeney G. Increased expression and cell surface localization of MT1-MMP plays a role in stimulation of MMP-2 activity by leptin in neonatal rat cardiac myofibroblasts. J Mol Cell Cardiol. 2008;44(5):874-81.
37. Madani S, De Girolamo S, Muñoz DM, Li RK, Sweeney G. Direct effects of leptin on size and extracellular matrix components of human pediatric ventricular myocytes. Cardiovasc Res. 2006;69(3):716-25.
38. Schram K, Ganguly R, No EK, Fang X, Thong FS, Sweeney G. Regulation of MT1-MMP and MMP-2 by leptin in cardiac fibroblasts involves Rho/ROCK-dependent actin cytoskeletal reorganization and leads to enhanced cell migration. Endocrinology. 2011;152(5):2037-47.
39. Tao M, Yu P, Nguyen BT, Mizrahi B, Savion N, Kolodgie FD, et al. Locally applied leptin induces regional aortic wall degeneration preceding aneurysm formation in apolipoprotein E-deficient mice. Arterioscler Thromb Vasc Biol. 2013;33(2):311-20.
40. Schroeter MR, Stein S, Heida NM, Leifheit-Nestler M, Cheng IF, Gogiraju R, et al. Leptin promotes the mobilization of vascular progenitor cells and neovascularization by NOX2-mediated activation of MMP9. Cardiovasc Res. 2012;93(1):170-80.
163

Original Article
Silva et al.Obesity and cardiac collagen
Arq Bras Cardiol. 2014; 102(2):157-164 164

Original Article
Gene Expression Related to Oxidative Stress in the Heart of Mice after Intestinal IschemiaFrederico Somaio Neto2, Adauto Tsutomu Ikejiri2, Paulo Roberto Bertoletto2, José Carlos Bertoletto Chaves2, Roberto Teruya3, Djalma José Fagundes1, Murched Omar Taha1
Universidade Federal de São Paulo – UNIFESP1, São Paulo, SP; Universidade Federal da Grande Dourados – UFGD2, Dourados, MS; Universidade Federal do Mato Grosso do Sul – UFMS3, Campo Grande, MS - Brazil
Mailling Address: Djalma José Fagundes •Rua Camé, 244, conjunto 33, 3º andar, Mooca. Postal Code 03121-020, São Paulo, SP - BrazilE-mail: [email protected], [email protected] received May 06, 2013; revised manuscript September 01, 2013; accepted September 04, 2013.
DOI: 10.5935/abc.20130240
Abstract
Background: Intestinal ischemia-reperfusion is a frequent clinical event associated to injury in distant organs, especially the heart.
Objective: To investigate the gene expression of oxidative stress and antioxidant defense in the heart of inbred mice subjected to intestinal ischemia and reperfusion (IR).
Methods: Twelve mice (C57BL / 6) were assigned to: IR Group (GIR) with 60 minutes of superior mesenteric artery occlusion followed by 60 minutes of reperfusion; Control Group (CG) which underwent anesthesia and laparotomy without IR procedure and was observed for 120 minutes. Intestine and heart samples were processed using the RT-qPCR / Reverse transcriptase-quantitative Polymerase Chain Reaction method for the gene expression of 84 genes related to oxidative stress and oxidative defense (Student’s “t” test, p < 0.05).
Results: The intestinal tissue (GIR) was noted to have an up-regulation of 65 genes (74.71%) in comparison to normal tissue (CG), and 37 genes (44.04%) were hyper-expressed (greater than three times the threshold allowed by the algorithm). Regarding the remote effects of intestinal I/R in cardiac tissue an up-regulation of 28 genes (33.33%) was seen, but only eight genes (9.52%) were hyper-expressed three times above threshold. Four (7.14%) of these eight genes were expressed in both intestinal and cardiac tissues. Cardiomyocytes with smaller and pyknotic nuclei, rich in heterochromatin with rare nucleoli, indicating cardiac distress, were observed in the GIR.
Conclusion: Intestinal I/R caused a statistically significant over expression of 8 genes associated with oxidative stress in remote myocardial tissue. (Arq Bras Cardiol. 2014; 102(2):165-174)
Keywords: Gene Expression; Mice; Oxidative Stress; Intestines / pathology.
IntroductionTissue ischemia and reperfusion (IR), and the cell and
humoral changes that follow have a great impact in human homeostasis1. Although reactive oxygen species (ROS) are involved in homeostasis, if a number greater than the natural limits of cell defense of antioxidants and sweepers is present, an unbalance will be seen, known as oxidative stress2. Although the oxygen is a critical substrate for relieving ischemia, it paradoxically acts as a harmful metabolite during the reperfusion period2-5, creating a predisposition for injury in distant organs, in addition to local lesions6.
IR, and the subsequent oxidative stress, is associated to clinical and surgical conditions, such as: sepsis, artery
occlusion, cardiac arrest, thrombosis, embolism, vasospasm, tumor, organ transplantation, organ excision, cerebrovascular accident and myocardial infarction2,6-8.
Oxidative stress in the cardiovascular system predisposes to severe cardiomyocyte and cardiac vessel injury, changing their contraction and relaxation mechanisms, having as consequence their disadaptation and impaired function6.
Gene expression assessment associated with oxidative stress in distant organs is a new tool for clarifying different aspects of the phenomenon, both related to diagnosis and monitoring, and therapeutic procedure results9,10. A recent technological resource makes it possible to assess a large number of genes in a safe and relatively simple way, using RT-qPCR (Reverse transcriptase–quantitative Polymerase Chain Reaction) method11-14. Thus, the genomic response of the heart to the oxidative stress caused by renal, hepatic, and mesenteric ischemia, infrarenal aortic occlusion or lower limb ischemia has been described in animal models13-14.
Considering splanchnic ischemia, especially of the small intestine, is a severe event, and that in addition to its local manifestations it has a systemic repercussion, this paper proposes to assess the expression of 84 genes related to
165

Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
the oxidative stress and the antioxidant defense in the cardiac tissue after intestinal ischemia and reperfusion in an inbred mice model.
MethodsThe research was approved by the Research Ethics
Committee of Hospital São Paulo, bonded to Universidade Federal de São Paulo-UNIFESP under number 1379-1308. The project was ratified by the Research Ethics Committee of Universidade Federal da Grande Dourados-UFGD (protocol 306/08). Experimental procedures followed international norms about animal research and the guidelines of the Brazilian Society of Lab Animal Science (SBCAL). The animals were kept according to the Guide for Caring and Using Lab Animals (Institute of Lab Animal Research, 1996).
SampleThe animals were kept under controlled conditions of
temperature and noise, and had a 12-hour cycle of light and darkness. They had free access to water and food adequate to the species. Surgical procedures were performed in the Experimental Surgery labs of the Surgical Department of Universidade Federal da Grande Dourados (UFGD). Twelve adult male mice were selected (C57BL/6 strain), with an average weight of 35 grams. They were supplied by the Center for the Development of Experimental Models for Medicine and Biology UNIFESP (CEDEME) and randomly assigned to either one of these two groups: Ischemia and Reperfusion Group (GIR), where six animals were subjected to superior mesenteric artery occlusion for 60 minutes followed by 60 minutes of reperfusion; and Control Group (GC), where six animals were subjected to median laparotomy under anesthesia, with no vascular clamping of the intestine, and observed for 120 minutes.
Anesthetic and surgical procedures The mice were administered the following anesthetics
intramuscularly: ketamine hydrochloride (44 mg.Kg-1, Ketamina Agener - União Química, São Paulo), xylazine hydrochloride (2.5 mg.Kg-1, Calmium - União Química, São Paulo) and acepromazine (0.75 mg.Kg-1, Acepran - Rhobifarma). Room temperature was kept at 38°C. The surgical procedure included median laparotomy, and after opening of the peritoneal cavity, abdominal viscera were kept away and identified, and the superior mesenteric artery and vein were isolated and occluded by a microsurgery clamp (metal vascular clip). Artery occlusion was confirmed by pale coloration of the intestine and no pulsing of the artery. After 60 minutes of vascular occlusion, the metal clamp was removed, and reperfusion was initiated, characterized by the return of artery pulsing and different coloration.
Material collection procedureAfter the reperfusion period in the GIR group or the
observation period in the GC group was finished, samples of the small intestine of the mice were collected for the assessment of ischemia effects and gene expression. Sample collection
was performed under anesthesia. Subsequently, the heart was removed, still beating, and sectioned lengthwise at the larger axis, by the ventricles. Heart fragments were imbibed into 10% formaldehyde individually and subjected to standard optical microscope histological processing for hematoxiline and eosin (HE). Another lengthwise fragment of the heart and a 30 mm segment of the intestine were carefully washed with saline solution, wrapped in aluminium foil, labeled and placed in cryogenic vials containing liquid nitrogen (-196°C). These samples were taken to the Molecular Biology Lab of the Gynecology Department - UNIFESP for gene expression processing.
Gene expression proceduresThe RNA of the 84 genes related to the effect of the
oxidative stress and antioxidant defense (Table 1) was extracted from the small intestine and heart samples of mice in the GC and GIR using TRIzol® (Life Technologies, Grand Island, NY, USA) reagent, and purified by inverse measures (Rneasy MiniKit Qiagen, Co - USA). The concentration of total RNA samples was determined by spectrophotometry, and result quality was assured by the same 2% agarose gel analysis. The first complementary DNA chain (cDNA) was synthesized using 1 µg of total RNA and RT2 First Strand kit (SABiosciences). Identical amounts of cDNA and Master Mix SYBR® Green qPCR Mastermix (SABiosciences, QIAGEN Company) were distributed to each PCR array well containing portions of specific genes, which had been previously selected. PCR was performed according to manufacturer’s instructions in 96 wells for the expression of 84 genes related to oxidative stress, five endogenous control genes used for measuring PCR array information (ACTB, Gapdh, Hsp90ab1, Hprt1, Gusb), and one negative control for checking for potential contamination with genomic DNA. The negative control primary sample detected non-transcribed and repetitive genomic DNA with a high level of sensitivity. Three reverse transcription control (RTC) wells were used to check for RT reaction efficiency with qPCR test, which aims at detecting patterns synthesized by the control RNA of the first strand synthesis kit. Replication of positive PCR controls (PPCs) was used to determine the efficiency of the polimerase chain reaction. These controls use an artificial DNA sequence predefined in the detection process. Replicated control wells (RTC and PPC) also assess the consistency among wells and plates. The equipment software (MxPro Equipment Real Time Systems, Stratagene, GE, Co) calculated the values of the beginning of the cycle (Ct) for all genes under analysis. At last, the software compared the pair by calculating gene expression change from the pure initial cycle, using [2-∆∆C] method. The method used for determining the relative expression of interest genes in this study was shown in the data analysis table of PCR Array v3.3 (PCR Array Data Analysis v3.3-SABiosciences – Qiagen, Company)15.
Statistical AnalysisEach sample was assessed in triplicate for gene
expression data. Student’s t-test (p < 0.05) was used to validate the homogeneity of each gene expression reaction. For comparison between the two groups, the computer
166
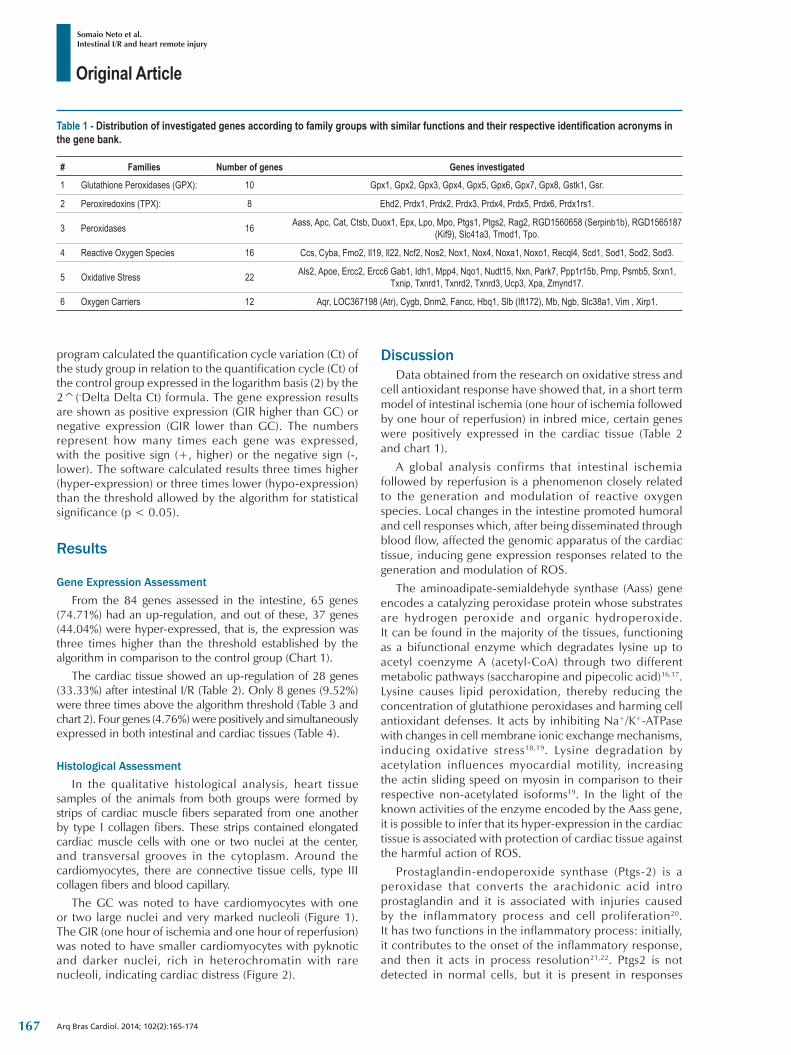
Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
Table 1 ‑ Distribution of investigated genes according to family groups with similar functions and their respective identification acronyms in the gene bank.
# Families Number of genes Genes investigated
1 Glutathione Peroxidases (GPX): 10 Gpx1, Gpx2, Gpx3, Gpx4, Gpx5, Gpx6, Gpx7, Gpx8, Gstk1, Gsr.
2 Peroxiredoxins (TPX): 8 Ehd2, Prdx1, Prdx2, Prdx3, Prdx4, Prdx5, Prdx6, Prdx1rs1.
3 Peroxidases 16 Aass, Apc, Cat, Ctsb, Duox1, Epx, Lpo, Mpo, Ptgs1, Ptgs2, Rag2, RGD1560658 (Serpinb1b), RGD1565187 (Kif9), Slc41a3, Tmod1, Tpo.
4 Reactive Oxygen Species 16 Ccs, Cyba, Fmo2, Il19, Il22, Ncf2, Nos2, Nox1, Nox4, Noxa1, Noxo1, Recql4, Scd1, Sod1, Sod2, Sod3.
5 Oxidative Stress 22 Als2, Apoe, Ercc2, Ercc6 Gab1, Idh1, Mpp4, Nqo1, Nudt15, Nxn, Park7, Ppp1r15b, Prnp, Psmb5, Srxn1, Txnip, Txnrd1, Txnrd2, Txnrd3, Ucp3, Xpa, Zmynd17.
6 Oxygen Carriers 12 Aqr, LOC367198 (Atr), Cygb, Dnm2, Fancc, Hbq1, Slb (Ift172), Mb, Ngb, Slc38a1, Vim , Xirp1.
program calculated the quantification cycle variation (Ct) of the study group in relation to the quantification cycle (Ct) of the control group expressed in the logarithm basis (2) by the 2^(-Delta Delta Ct) formula. The gene expression results are shown as positive expression (GIR higher than GC) or negative expression (GIR lower than GC). The numbers represent how many times each gene was expressed, with the positive sign (+, higher) or the negative sign (-, lower). The software calculated results three times higher (hyper-expression) or three times lower (hypo-expression) than the threshold allowed by the algorithm for statistical significance (p < 0.05).
Results
Gene Expression AssessmentFrom the 84 genes assessed in the intestine, 65 genes
(74.71%) had an up-regulation, and out of these, 37 genes (44.04%) were hyper-expressed, that is, the expression was three times higher than the threshold established by the algorithm in comparison to the control group (Chart 1).
The cardiac tissue showed an up-regulation of 28 genes (33.33%) after intestinal I/R (Table 2). Only 8 genes (9.52%) were three times above the algorithm threshold (Table 3 and chart 2). Four genes (4.76%) were positively and simultaneously expressed in both intestinal and cardiac tissues (Table 4).
Histological AssessmentIn the qualitative histological analysis, heart tissue
samples of the animals from both groups were formed by strips of cardiac muscle fibers separated from one another by type I collagen fibers. These strips contained elongated cardiac muscle cells with one or two nuclei at the center, and transversal grooves in the cytoplasm. Around the cardiomyocytes, there are connective tissue cells, type III collagen fibers and blood capillary.
The GC was noted to have cardiomyocytes with one or two large nuclei and very marked nucleoli (Figure 1). The GIR (one hour of ischemia and one hour of reperfusion) was noted to have smaller cardiomyocytes with pyknotic and darker nuclei, rich in heterochromatin with rare nucleoli, indicating cardiac distress (Figure 2).
DiscussionData obtained from the research on oxidative stress and
cell antioxidant response have showed that, in a short term model of intestinal ischemia (one hour of ischemia followed by one hour of reperfusion) in inbred mice, certain genes were positively expressed in the cardiac tissue (Table 2 and chart 1).
A global analysis confirms that intestinal ischemia followed by reperfusion is a phenomenon closely related to the generation and modulation of reactive oxygen species. Local changes in the intestine promoted humoral and cell responses which, after being disseminated through blood flow, affected the genomic apparatus of the cardiac tissue, inducing gene expression responses related to the generation and modulation of ROS.
The aminoadipate-semialdehyde synthase (Aass) gene encodes a catalyzing peroxidase protein whose substrates are hydrogen peroxide and organic hydroperoxide. It can be found in the majority of the tissues, functioning as a bifunctional enzyme which degradates lysine up to acetyl coenzyme A (acetyl-CoA) through two different metabolic pathways (saccharopine and pipecolic acid)16,17. Lysine causes lipid peroxidation, thereby reducing the concentration of glutathione peroxidases and harming cell antioxidant defenses. It acts by inhibiting Na+/K+-ATPase with changes in cell membrane ionic exchange mechanisms, inducing oxidative stress18,19. Lysine degradation by acetylation influences myocardial motility, increasing the actin sliding speed on myosin in comparison to their respective non-acetylated isoforms19. In the light of the known activities of the enzyme encoded by the Aass gene, it is possible to infer that its hyper-expression in the cardiac tissue is associated with protection of cardiac tissue against the harmful action of ROS.
Prostaglandin-endoperoxide synthase (Ptgs-2) is a peroxidase that converts the arachidonic acid intro prostaglandin and it is associated with injuries caused by the inflammatory process and cell proliferation20. It has two functions in the inflammatory process: initially, it contributes to the onset of the inflammatory response, and then it acts in process resolution21,22. Ptgs2 is not detected in normal cells, but it is present in responses
167
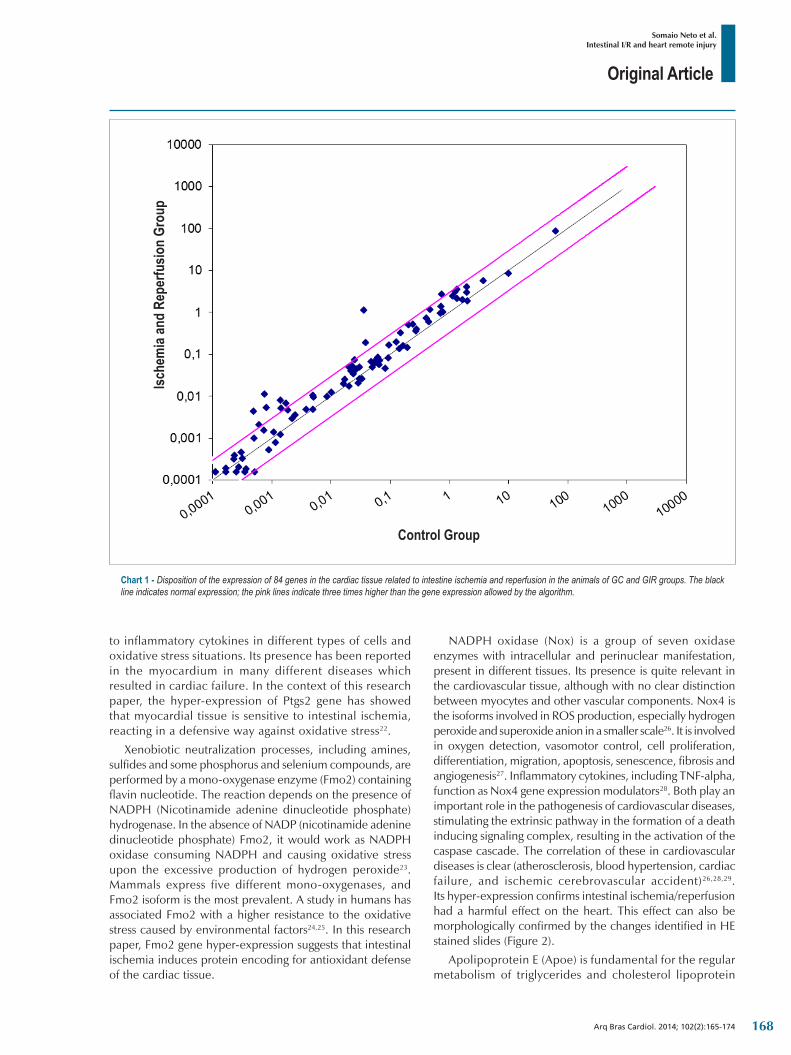
Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
Chart 1 ‑ Disposition of the expression of 84 genes in the cardiac tissue related to intestine ischemia and reperfusion in the animals of GC and GIR groups. The black line indicates normal expression; the pink lines indicate three times higher than the gene expression allowed by the algorithm.
Ische
mia
and
Repe
rfusio
n Gr
oup
Control Group
to inflammatory cytokines in different types of cells and oxidative stress situations. Its presence has been reported in the myocardium in many different diseases which resulted in cardiac failure. In the context of this research paper, the hyper-expression of Ptgs2 gene has showed that myocardial tissue is sensitive to intestinal ischemia, reacting in a defensive way against oxidative stress22.
Xenobiotic neutralization processes, including amines, sulfides and some phosphorus and selenium compounds, are performed by a mono-oxygenase enzyme (Fmo2) containing flavin nucleotide. The reaction depends on the presence of NADPH (Nicotinamide adenine dinucleotide phosphate) hydrogenase. In the absence of NADP (nicotinamide adenine dinucleotide phosphate) Fmo2, it would work as NADPH oxidase consuming NADPH and causing oxidative stress upon the excessive production of hydrogen peroxide23. Mammals express five different mono-oxygenases, and Fmo2 isoform is the most prevalent. A study in humans has associated Fmo2 with a higher resistance to the oxidative stress caused by environmental factors24,25. In this research paper, Fmo2 gene hyper-expression suggests that intestinal ischemia induces protein encoding for antioxidant defense of the cardiac tissue.
NADPH oxidase (Nox) is a group of seven oxidase enzymes with intracellular and perinuclear manifestation, present in different tissues. Its presence is quite relevant in the cardiovascular tissue, although with no clear distinction between myocytes and other vascular components. Nox4 is the isoforms involved in ROS production, especially hydrogen peroxide and superoxide anion in a smaller scale26. It is involved in oxygen detection, vasomotor control, cell proliferation, differentiation, migration, apoptosis, senescence, fibrosis and angiogenesis27. Inflammatory cytokines, including TNF-alpha, function as Nox4 gene expression modulators28. Both play an important role in the pathogenesis of cardiovascular diseases, stimulating the extrinsic pathway in the formation of a death inducing signaling complex, resulting in the activation of the caspase cascade. The correlation of these in cardiovascular diseases is clear (atherosclerosis, blood hypertension, cardiac failure, and ischemic cerebrovascular accident)26,28,29. Its hyper-expression confirms intestinal ischemia/reperfusion had a harmful effect on the heart. This effect can also be morphologically confirmed by the changes identified in HE stained slides (Figure 2).
Apolipoprotein E (Apoe) is fundamental for the regular metabolism of triglycerides and cholesterol lipoprotein
168
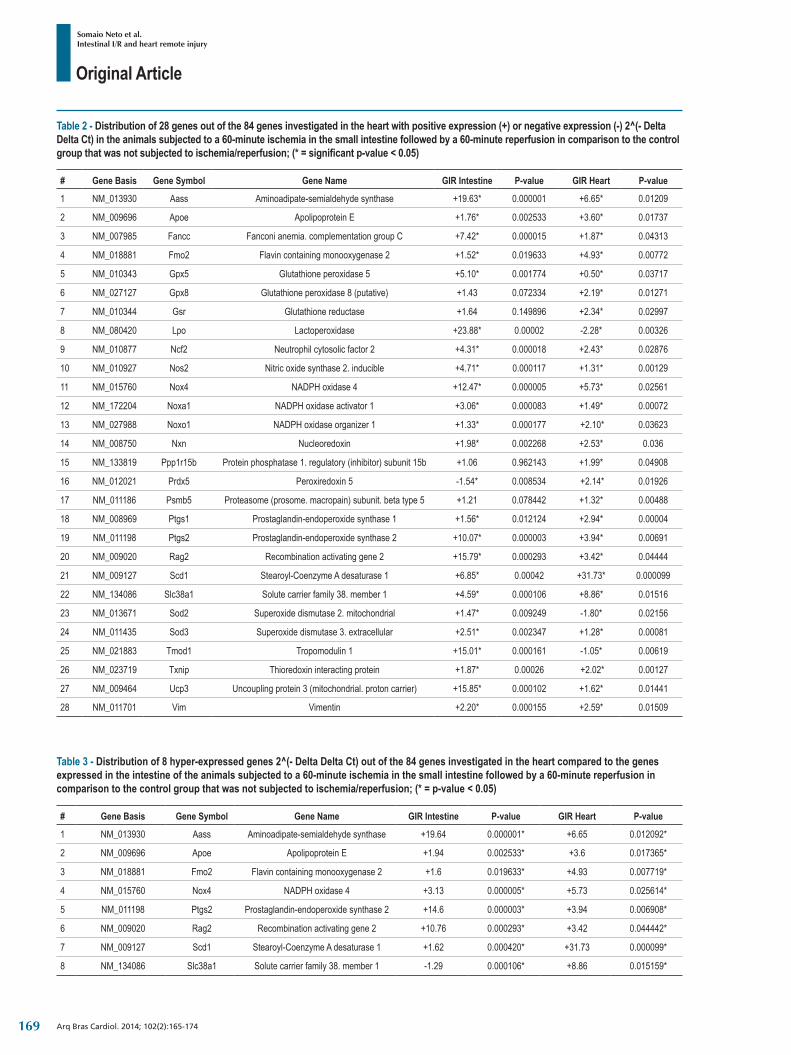
Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
Table 2 ‑ Distribution of 28 genes out of the 84 genes investigated in the heart with positive expression (+) or negative expression (-) 2^(- Delta Delta Ct) in the animals subjected to a 60-minute ischemia in the small intestine followed by a 60-minute reperfusion in comparison to the control group that was not subjected to ischemia/reperfusion; (* = significant p-value < 0.05)
# Gene Basis Gene Symbol Gene Name GIR Intestine P‑value GIR Heart P‑value
1 NM_013930 Aass Aminoadipate-semialdehyde synthase +19.63* 0.000001 +6.65* 0.01209
2 NM_009696 Apoe Apolipoprotein E +1.76* 0.002533 +3.60* 0.01737
3 NM_007985 Fancc Fanconi anemia. complementation group C +7.42* 0.000015 +1.87* 0.04313
4 NM_018881 Fmo2 Flavin containing monooxygenase 2 +1.52* 0.019633 +4.93* 0.00772
5 NM_010343 Gpx5 Glutathione peroxidase 5 +5.10* 0.001774 +0.50* 0.03717
6 NM_027127 Gpx8 Glutathione peroxidase 8 (putative) +1.43 0.072334 +2.19* 0.01271
7 NM_010344 Gsr Glutathione reductase +1.64 0.149896 +2.34* 0.02997
8 NM_080420 Lpo Lactoperoxidase +23.88* 0.00002 -2.28* 0.00326
9 NM_010877 Ncf2 Neutrophil cytosolic factor 2 +4.31* 0.000018 +2.43* 0.02876
10 NM_010927 Nos2 Nitric oxide synthase 2. inducible +4.71* 0.000117 +1.31* 0.00129
11 NM_015760 Nox4 NADPH oxidase 4 +12.47* 0.000005 +5.73* 0.02561
12 NM_172204 Noxa1 NADPH oxidase activator 1 +3.06* 0.000083 +1.49* 0.00072
13 NM_027988 Noxo1 NADPH oxidase organizer 1 +1.33* 0.000177 +2.10* 0.03623
14 NM_008750 Nxn Nucleoredoxin +1.98* 0.002268 +2.53* 0.036
15 NM_133819 Ppp1r15b Protein phosphatase 1. regulatory (inhibitor) subunit 15b +1.06 0.962143 +1.99* 0.04908
16 NM_012021 Prdx5 Peroxiredoxin 5 -1.54* 0.008534 +2.14* 0.01926
17 NM_011186 Psmb5 Proteasome (prosome. macropain) subunit. beta type 5 +1.21 0.078442 +1.32* 0.00488
18 NM_008969 Ptgs1 Prostaglandin-endoperoxide synthase 1 +1.56* 0.012124 +2.94* 0.00004
19 NM_011198 Ptgs2 Prostaglandin-endoperoxide synthase 2 +10.07* 0.000003 +3.94* 0.00691
20 NM_009020 Rag2 Recombination activating gene 2 +15.79* 0.000293 +3.42* 0.04444
21 NM_009127 Scd1 Stearoyl-Coenzyme A desaturase 1 +6.85* 0.00042 +31.73* 0.000099
22 NM_134086 Slc38a1 Solute carrier family 38. member 1 +4.59* 0.000106 +8.86* 0.01516
23 NM_013671 Sod2 Superoxide dismutase 2. mitochondrial +1.47* 0.009249 -1.80* 0.02156
24 NM_011435 Sod3 Superoxide dismutase 3. extracellular +2.51* 0.002347 +1.28* 0.00081
25 NM_021883 Tmod1 Tropomodulin 1 +15.01* 0.000161 -1.05* 0.00619
26 NM_023719 Txnip Thioredoxin interacting protein +1.87* 0.00026 +2.02* 0.00127
27 NM_009464 Ucp3 Uncoupling protein 3 (mitochondrial. proton carrier) +15.85* 0.000102 +1.62* 0.01441
28 NM_011701 Vim Vimentin +2.20* 0.000155 +2.59* 0.01509
Table 3 ‑ Distribution of 8 hyper-expressed genes 2^(- Delta Delta Ct) out of the 84 genes investigated in the heart compared to the genes expressed in the intestine of the animals subjected to a 60-minute ischemia in the small intestine followed by a 60-minute reperfusion in comparison to the control group that was not subjected to ischemia/reperfusion; (* = p-value < 0.05)
# Gene Basis Gene Symbol Gene Name GIR Intestine P‑value GIR Heart P‑value
1 NM_013930 Aass Aminoadipate-semialdehyde synthase +19.64 0.000001* +6.65 0.012092*
2 NM_009696 Apoe Apolipoprotein E +1.94 0.002533* +3.6 0.017365*
3 NM_018881 Fmo2 Flavin containing monooxygenase 2 +1.6 0.019633* +4.93 0.007719*
4 NM_015760 Nox4 NADPH oxidase 4 +3.13 0.000005* +5.73 0.025614*
5 NM_011198 Ptgs2 Prostaglandin-endoperoxide synthase 2 +14.6 0.000003* +3.94 0.006908*
6 NM_009020 Rag2 Recombination activating gene 2 +10.76 0.000293* +3.42 0.044442*
7 NM_009127 Scd1 Stearoyl-Coenzyme A desaturase 1 +1.62 0.000420* +31.73 0.000099*
8 NM_134086 Slc38a1 Solute carrier family 38. member 1 -1.29 0.000106* +8.86 0.015159*
169
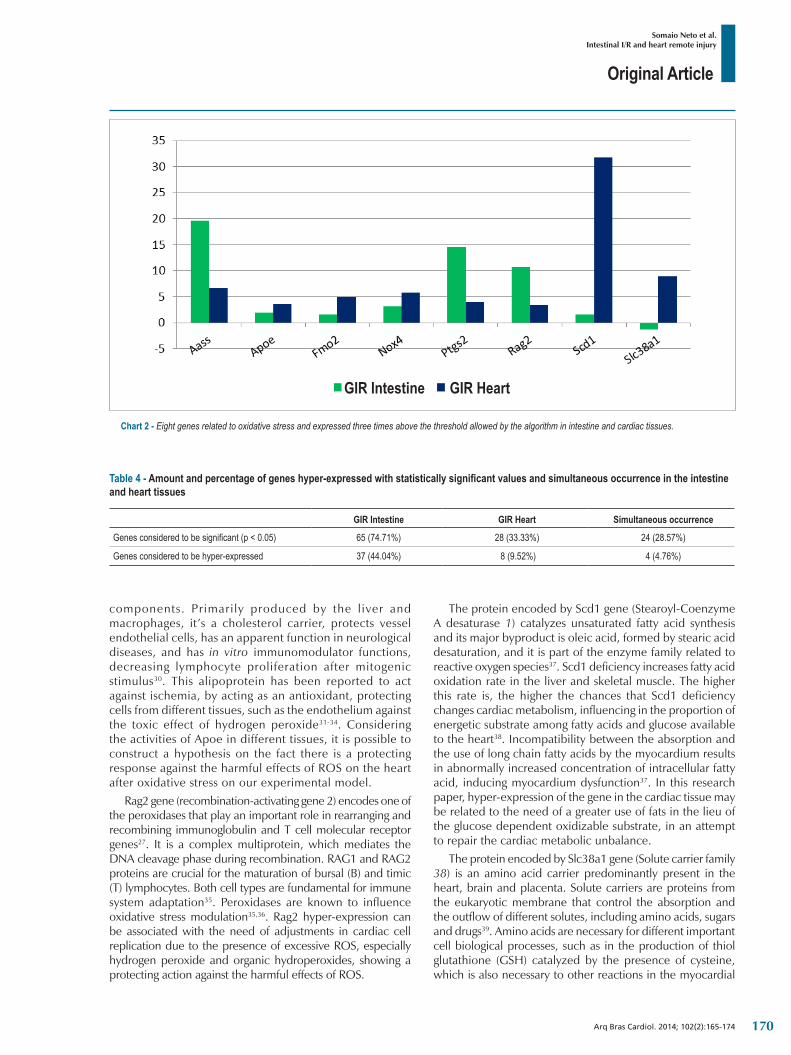
Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
Chart 2 ‑ Eight genes related to oxidative stress and expressed three times above the threshold allowed by the algorithm in intestine and cardiac tissues.
GIR Intestine GIR Heart
Table 4 ‑ Amount and percentage of genes hyper-expressed with statistically significant values and simultaneous occurrence in the intestine and heart tissues
GIR Intestine GIR Heart Simultaneous occurrence
Genes considered to be significant (p < 0.05) 65 (74.71%) 28 (33.33%) 24 (28.57%)
Genes considered to be hyper-expressed 37 (44.04%) 8 (9.52%) 4 (4.76%)
components. Primarily produced by the liver and macrophages, it’s a cholesterol carrier, protects vessel endothelial cells, has an apparent function in neurological diseases, and has in vitro immunomodulator functions, decreasing lymphocyte proliferation after mitogenic stimulus30. This alipoprotein has been reported to act against ischemia, by acting as an antioxidant, protecting cells from different tissues, such as the endothelium against the toxic effect of hydrogen peroxide31-34. Considering the activities of Apoe in different tissues, it is possible to construct a hypothesis on the fact there is a protecting response against the harmful effects of ROS on the heart after oxidative stress on our experimental model.
Rag2 gene (recombination-activating gene 2) encodes one of the peroxidases that play an important role in rearranging and recombining immunoglobulin and T cell molecular receptor genes27. It is a complex multiprotein, which mediates the DNA cleavage phase during recombination. RAG1 and RAG2 proteins are crucial for the maturation of bursal (B) and timic (T) lymphocytes. Both cell types are fundamental for immune system adaptation35. Peroxidases are known to influence oxidative stress modulation35,36. Rag2 hyper-expression can be associated with the need of adjustments in cardiac cell replication due to the presence of excessive ROS, especially hydrogen peroxide and organic hydroperoxides, showing a protecting action against the harmful effects of ROS.
The protein encoded by Scd1 gene (Stearoyl-Coenzyme A desaturase 1) catalyzes unsaturated fatty acid synthesis and its major byproduct is oleic acid, formed by stearic acid desaturation, and it is part of the enzyme family related to reactive oxygen species37. Scd1 deficiency increases fatty acid oxidation rate in the liver and skeletal muscle. The higher this rate is, the higher the chances that Scd1 deficiency changes cardiac metabolism, influencing in the proportion of energetic substrate among fatty acids and glucose available to the heart38. Incompatibility between the absorption and the use of long chain fatty acids by the myocardium results in abnormally increased concentration of intracellular fatty acid, inducing myocardium dysfunction37. In this research paper, hyper-expression of the gene in the cardiac tissue may be related to the need of a greater use of fats in the lieu of the glucose dependent oxidizable substrate, in an attempt to repair the cardiac metabolic unbalance.
The protein encoded by Slc38a1 gene (Solute carrier family 38) is an amino acid carrier predominantly present in the heart, brain and placenta. Solute carriers are proteins from the eukaryotic membrane that control the absorption and the outflow of different solutes, including amino acids, sugars and drugs39. Amino acids are necessary for different important cell biological processes, such as in the production of thiol glutathione (GSH) catalyzed by the presence of cysteine, which is also necessary to other reactions in the myocardial
170
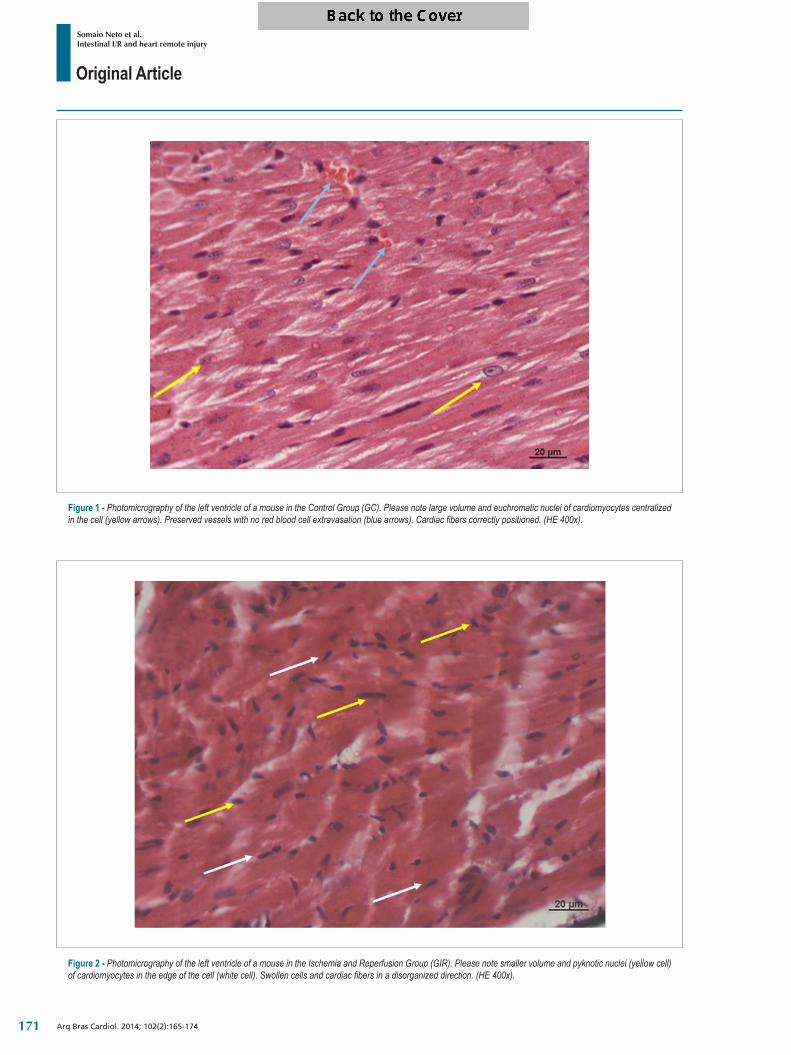
Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
Figure 1 ‑ Photomicrography of the left ventricle of a mouse in the Control Group (GC). Please note large volume and euchromatic nuclei of cardiomyocytes centralized in the cell (yellow arrows). Preserved vessels with no red blood cell extravasation (blue arrows). Cardiac fibers correctly positioned. (HE 400x).
Figure 2 ‑ Photomicrography of the left ventricle of a mouse in the Ischemia and Reperfusion Group (GIR). Please note smaller volume and pyknotic nuclei (yellow cell) of cardiomyocytes in the edge of the cell (white cell). Swollen cells and cardiac fibers in a disorganized direction. (HE 400x).
171

Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
tissue and is provided by the Slc38a1 carrier protein40. The duration of the oxidative stress stimulates its uptaking, causing increased Slc38a1 expression in the myocardium of mammals, consequently with a higher expression of GSH39,40. In this study, hyper-expression of Slc38a1 corroborates with the indication of similar action in other tissues and shows that its presence can implicate in a protecting action in the energy transportation mechanism of the myocardium cell.
The rationale of this research paper was developing the gene response profile of the cardiac tissue when subjected to stimuli from distant organs affected by oxidative stress. In the light of the unprecedented nature of the results and the complexity of the gene expression, the results can only be confirmed with a subsequent proteomic analysis, where protein identification and quantification in the tissue may provide resources to determine whether the gene expression acted as a real stimulus for protein encoding or whether the gene expression is related to signaling or modulation of other oxidative stress response metabolic pathways. As a starting point to future research, the mapping activity performed allowed eight genes to be identified, which showed to be more responsive to oxidative stress and can, therefore, be initially targeted as new study subject. This research line is very promising, because gene expression understanding may allow evolution monitoring procedures and treatment of multiple organ dysfunction syndrome, especially concerning the participation of the cardiac tissue in this phenomenon.
ConclusionsThe gene response profile associated to oxidative stress
has identified eight genes in the cardiac tissue that respond in a hyper-expressive way when the intestine is subjected to ischemia and reperfusion. This study presents the perspective of creating a monitoring protocol in ischemia and reperfusion scenarios from real-time gene expression.
AcknowledgmentsThe authors would like to thank Professor Dr. Ismael Dale
Cotrim Guerreiro da Silva, UNIFESP Molecular Gynecology Department, for his logistic and lab support. Professor Dr. Marcos Azevedo Junior for his support and gene expression procedures. Professor Manuel de Jesus Simões for his support in histological assessment procedures.
Author contributionsConception and design of the research: Somaio Neto F,
Fagundes DJ; Acquisition of data, Analysis and interpretation of the data and Writing of the manuscript: Somaio Neto F, Ikejiri AT, Bertoletto PR, Chaves JCB, Teruya R, Fagundes DJ, Taha MO; Statistical analysis: Somaio Neto F, Teruya R, Fagundes DJ; Obtaining funding: Somaio Neto F, Ikejiri AT, Bertoletto PR, Chaves JCB, Taha MO; Critical revision of the manuscript for intellectual content: Fagundes DJ.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
This study was partially funded by Universidade Federal da Grande Dourados- UFGD - Mato Grosso do Sul.
Study Association
This article is part of the thesis of master submitted by Frederico Somaio Neto from Universidade Federal de São Paulo.
1. Pashkow FJ. Oxidative stress and inflammation in heart disease: do antioxidants have a role in treatment and/or prevention? Int J Inflamm. 2011;2011:514623.
2. Kohen R, Nyska A. Oxidation of biological systems: oxidative stress phenomena, antioxidants, redox reactions, and methods for their quantification. Toxicol Pathol. 2002;30(6):620-50.
3. Ondiveeran HK, Fox-Robichaud A. New developments in the treatment of ischemia/reperfusion injury. Curr Opin Investig Drugs. 2001;2(6):783-91.
4. Chamoun F, Burne M, O’Donnell M, Rabb H. Pathophysiologic role of selectins and their ligands in ischemia reperfusion injury. Front Biosci. 2000;5:E103-9.
5. Zweier JL, Talukder MA. The role of oxidants and free radicals in reperfusion injury. Cardiovasc Res. 2006;70(2):181-90.
6. Cantor EJ, Mancini EV, Seth R, Yao XH, Netticadan T. Oxidative stress and heart disease: cardiac dysfunction, nutrition, and gene therapy. Curr Hypertens Rep. 2003;5(3):215-20.
7. Asyali MH, Colak D, Demirkaya O, Inan MS. Gene expression profile classification: a review. Current Bioinformatics. 2006;1(1):55-73.
8. Santos-Silva MA, Nagato AC, Trajano ET, Alves JN, Bandeira AC, Porto LC, et al. A resposta oxidativa em corações de camundongos é modulada por background genético. Arq Bras Cardiol. 2013;100(2):157-63.
9. Konstantinov IE, Arab S, Li J, Coles JG, Boscarino C, Mori A, et al. The remote ischemic preconditioning stimulus modifies gene expression in mouse myocardium. J Thorac Cardiovasc Surg. 2005;130(5):1326-32.
10. Bertoletto PR, Ikejiri AT, Somaio Neto F, Chaves JC, Teruya R, Bertoletto ER, et al. Oxidative stress gene expression profile in inbred mouse after ischemia/reperfusion small bowel injury. Acta Cir Bras. 2012;27(11):773-82.
11. Huda R, Chung DH, Mathru M. Ischemic preconditioning at a distance: altered gene expression in mouse heart and other organs following brief occlusion of the mesenteric artery. Heart Lung Circ. 2005;14(1):36-43.
12. Colombo J, Rahal P. A tecnologia de microarray no estudo do câncer de cabeça e pescoço. R Bras Bioci. 2010;8(1):64-72.
13. Moore-Olufemi SD, Olufemi SE, Lott S, Sato N, Kozar RA, Moore FA, et al. Intestinal ischemic preconditioning after ischemia/reperfusion injury in rat intestine: profiling global gene expression patterns. Dig Dis Sci. 2010;55(7):1866-77.
References
172
Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174
14. O’Donnell CJ, Nabel EG. Genomics of cardiovascular disease. N Engl J Med. 2011;365(22):2098-109.
15. Deepak SA, Kottapalli KR, Rakwal R, Oros G, Rangappa KS, Iwahashi H, et al. Real-time PCR: revolutionizing detection and expression analysis of genes. Curr Genomics. 2007;8(4):234-51.
16. Sacksteder KA, Biery BJ, Morrell JC, Goodman BK, Geisbrecht BV, Cox RP, et al. Identification of the alpha-aminoadipic semialdehyde synthase gene, which is defective in familial hyperlysinemia. Am J Hum Genet. 2000;66(6):1736-43.
17. Struys EA, Jakobs C. Metabolism of lysine in alpha-aminoadipic semialdehyde dehydrogenase-deficient fibroblasts: evidence for an alternative pathway of pipecolic acid formation. FEBS Lett. 2010;584(1):181-6.
18. Seminotti B, Leipnitz G, Amaral AU, Fernandes CG, da Silva Lde B, Tonin AM, et al. Lysine induces lipid and protein damage and decreases reduced glutathione concentrations in brain of young rats. Int J Dev Neurosci. 2008;26(7):693-8.
19. Cleveland BM. The effect of alpha-aminoadipate delta-semialdehyde synthase knockdown on the lysine requirement and urate oxidase knockdown on oxidative stress in a murine hepatic cell line. [thesis]. Morgantown, (WV): West Virginia University; 2007.
20. Buetler TM, Leclerc E, Baumeyer A, Latado H, Newell J, Adolfsson O, et al. N (epsilon)-carboxymethyllysine-modified proteins are unable to bind to RAGE and activate an inflammatory response. Mol Nutr Food Res. 2008;52(3):370-8.
21. Mason RP, Kalyanaraman B, Tainer BE, Eling TE. A carbon-centered free radical intermediate in the prostaglandin synthetase oxidation of arachidonic acid. Spin trapping and oxygen uptake studies. J Biol Chem. 1980;255(11):5019-22.
22. Gilroy DW, Colville-Nash PR, Willis D, Chivers J, Paul-Clark MJ, Willoughby DA. Inducible cyclooxygenase may have anti-inflammatory properties. Nat Med. 1999;5(6):698-701.
23. Wong SC, Fukuchi M, Melnyk P, Rodger I, Giaid A. Induction of cyclooxygenase-2 and activation of nuclear factor-kappaB in myocardium of patients with congestive heart failure. Circulation. 1998;98(2):100-3.
24. Yueh MF. Identification and characterization of flavin-containing monooxygenase isoform 2 (FMO2) in Rhesus monkey and examination of a human FMO2 polymorphism. [thesis]. Corvallis (OR): Oregon State University; 1999.
25. Krueger SK, Siddens LK, Martin SR, Yu Z, Pereira CB, Cabacungan ET, et al. Differences in FMO2*1 allelic frequency between Hispanics of Puerto Rican and Mexican descent. Drug Metab Dispos. 2004;32(12):1337-40.
26. Chen F, Haigh S, Barman S, Fulton DJ. From form to function: the role of Nox4 in the cardiovascular system. Front Physiol. 2012;3:412.
27. Yin FF, Bailey S, Innis CA, Ciubotaru M, Kamtekar S, Steitz TA, et al. Structure of the RAG1 nonamer binding domain with DNA reveals a dimer that mediates DNA synapsis. Nat Struct Mol Biol. 2009;16(5):499-508.
28. Basuroy S, Bhattacharya S, Leffler CW, Parfenova H. Nox4 NADPH oxidase mediates oxidative stress and apoptosis caused by TNF-alpha in cerebral vascular endothelial cells. Am J Physiol Cell Physiol. 2009;296(3):C422-32.
29. Santos CX, Anilkumar N, Zhang M, Brewer AC, Shah AM. Redox signaling in cardiac myocytes. Free Radic Biol Med. 2011;50(7):777-93.
30. Zhou S, Wu H, Zeng C, Xiong X, Tang S, Tang Z, et al. Apolipoprotein E protects astrocytes from hypoxia and glutamate-induced apoptosis. FEBS Lett. 2013;587(2):254-8.
31. Laskowitz DT, Sheng H, Bart RD, Joyner KA, Roses AD, Warner DS. Apolipoprotein E-deficient mice have increased susceptibility to focal cerebral ischemia. J Cereb Blood Flow Metab. 1997;17(7):753-8.
32. Miyata M, Smith JD. Apolipoprotein E allele-specific antioxidant activity and effects on cytotoxicity by oxidative insults and beta-amyloid peptides. Nat Genet. 1996;14(1):55-61.
33. Tarnus E, Wassef H, Carmel JF, Rondeau P, Roche M, Davignon J, et al. Apolipoprotein E limits oxidative stress-induced cell dysfunctions in human adipocytes. FEBS Lett. 2009;583(12):2042-8.
34. Yue L, Bian JT, Grizelj I, Cavka A, Phillips SA, Makino A, et al. Apolipoprotein E enhances endothelial-NO production by modulating caveolin 1 interaction with endothelial NO synthase. Hypertension. 2012;60(4):1040-6.
35. Arbuckle JL, Rahman NS, Zhao S, Rodgers W, Rodgers KK. Elucidating the domain architecture and functions of non-core RAG1: the capacity of a non-core zinc-binding domain to function in nuclear import and nucleic acid binding. BMC Biochem. 2011;12:23.
36. Gorsuch WB, Chrysanthou E , Schwaeble WJ, S tah l GL. The complement system in ischemia-reperfusion injuries. Immunobiology. 2012;217(11):1026-33.
37. Matsui H, Yokoyama T, Sekiguchi K, Iijima D, Sunaga H, Maniwa M, et al. Stearoyl-CoA desaturase-1 (SCD1) augments saturated fatty acid-induced lipid accumulation and inhibits apoptosis in cardiac myocytes. PLoS One. 2012;7(3):e33283.
38. Dobrzyn P, Sampath H, Dobrzyn A, Miyazaki M, Ntambi JM. Loss of stearoyl-CoA desaturase 1 inhibits fatty acid oxidation and increases glucose utilization in the heart. Am J Physiol Endocrinol Metab. 2008;294(2):E357-64.
39. Schlessinger A, Matsson P, Shima JE, Pieper U, Yee SW, Kelly L, et al. Comparison of human solute carriers. Protein Sci. 2010;19(3):412-28.
40. King N, Lin H, Suleiman MS. Oxidative stress increases SNAT1 expression and stimulates cysteine uptake in freshly isolated rat cardiomyocytes. Amino Acids. 2011;40(2):517-26.
173

Original Article
Somaio Neto et al.Intestinal I/R and heart remote injury
Arq Bras Cardiol. 2014; 102(2):165-174 174

Original Article
High Blood Pressure in Children and its Correlation with Three Definitions of Obesity in ChildhoodLeonardo Iezzi de Moraes, Thaís Coutinho Nicola, Julyanna Silva Araújo de Jesus, Eduardo Roberty Badiani Alves, Nayara Paula Bernurdes Giovaninni, Daniele Gasparini Marcato, Jéssica Dutra Sampaio, Jeanne Teixeira Bessa Fuly, Everlayny Fiorot CostalongaUniversidade Vila Velha - UVV, Vila Velha, ES - Brazil
Mailing Address: Leonardo Iezzi de Moraes •Desembargador Augusto Botelho, 108, apto. 303, Praia da Costa. Postal Code 29101-110, Vila Velha, ES - BrazilE-mail: [email protected], [email protected] received April 13, 2013; revised manuscript July 23, 2013; accepted September 16, 2013.
DOI: 10.5935/abc.20130233
Abstract
Background: Several authors have correlated the increase of cardiovascular risk with the nutritional status, however there are different criteria for the classification of overweight and obesity in children.
Objectives: To evaluate the performance of three nutritional classification criteria in children, as definers of the presence of obesity and predictors of high blood pressure in schoolchildren.
Methods: Eight hundred and seventeen children ranging 6 to 13 years old, enrolled in public schools in the municipality of Vila Velha (ES) were submitted to anthropometric evaluation and blood pressure measurement. The classification of the nutritional status was established by two international criteria (CDC/NCHS 2000 and IOTF 2000) and one Brazilian criterion (Conde e Monteiro 2006).
Results: The prevalence of overweight was higher when the criterion of Conde e Monteiro (27%) was used, and inferior by the IOTF (15%) criteria. High blood pressure was observed in 7.3% of children. It was identified a strong association between the presence of overweight and the occurrence of high blood pressure, regardless of the test used (p < 0.001). The test showing the highest sensitivity in predicting elevated BP was the Conde e Monteiro (44%), while the highest specificity (94%) and greater overall accuracy (63%), was the CDC criterion.
Conclusions: The prevalence of overweight in Brazilian children is higher when using the classification criterion of Conde e Monteiro, and lower when the criterion used is IOTF. The Brazilian classification criterion proved to be the most sensitive predictor of high BP risk in this sample. (Arq Bras Cardiol. 2014; 102(2):175-180)
Keywords: Hypertension; Child; Obesity; Body mass index.
IntroductionDiseases of modern life have been worryingly affecting
children. Obesity is now seen as a global epidemic, which is accompanied by increase of cardiovascular risk factors such as Systemic Hypertension (SH)1,2. High blood pressure levels in children predict SH of the adult and contribute to the occurrence of cardiovascular events1,2. Therefore, early identification and treatment of high blood pressure in childhood have the potential to cause a great impact on future adverse outcomes.
Currently, it is considered mandatory the measurement of Blood Pressure (BP) since the age of three, annually or sooner, if there is any risk factors3-5. However, the complex methodology required for the verification of BP in children causes many
professionals to exclude it from their routine or interpret the values measured incorrectly, which can result in underdiagnosis and incorrigible consequences for these individual6,7.
Excess weight, commonly assessed by Body Mass Index (BMI) is an important predictor of high BP in children. The risk of high BP can increase more than twice at every unit increased in BMI z-score8-12. Therefore, the proper classification of nutritional status in children is a warning instrument for the risk of hypertension.
This classification can be established using different criteria. In 2000, the Centers for Disease Control (CDC) defined the 85th and 95th percentiles of distribution in the U.S. population as cut-off points for overweight and obesity, respectively13. In the same year, Cole et al14,15, through the International Obesity Task Force (IOTF), involving six countries, established BMI cut-offs for age and sex corresponding to values of 25 kg/m² for overweight, and 30 kg/m² for obesity at age 18. In 2006, Conde and Monteiro used similar methodology to propose to the IOTF cut-off points based on the Brazilian population16.
The purpose of this present study is to evaluate the performance of those criteria as predictors of high blood pressure levels in schoolchildren in the municipality of Vila Velha (ES).
175

Original Article
Moraes et al.Definition of obesity and high blood pressure in children
Arq Bras Cardiol. 2014; 102(2):175-180
MethodsThe study involved students enrolled in School District
elementary public school in the city of Vila Velha (ES). It only included children whose parents or legal guardians agreed in the participation through an informed consent form, as approved by the Ethics Committee of the institution (procedure no. 34/2011).
The sample size calculation was performed using Epi Info, version 6.04, available for free on the internet. For calculation purposes, we considered the number of students enrolled in UMEF in the year of the study, the average prevalence of hypertension in children of 4%, the absolute error of 2%, confidence interval of 95%, 80% statistical power and effect of design of 2, reaching an amount of 730 children, whose objectified number was rounded to 800, predicting eventual losses.
Sampling was the complex type, in two stages. The first stage consisted of random selection by draw from a school of each of the five political-geographical regions of the municipality. In the second stage, we conducted an unsystematic selection of students from each school, according to the adhesion of such and the informed consent form in writing of their guardians or parents.
Children under the age of six years or with age superior to 13 years, which accounted for less than 2% of the sample, were excluded in order to ensure homogeneity.
The students were assessed with respect to height, weight and blood pressure. Measurements of height were performed by using a wall fixed stadiometer, graduated 20-200 cm, with scale accuracy of 0.1 cm, and represented by the average of three consecutive measurements. The child was placed in the standing position, without shoes, with hips and shoulders perpendicular to the central axis of the body, heels firmly planted on the ground, knees close and extended, relaxed arms and head in the Frankfurt plane. Body weight was determined by a digital anthropometric scale graduated from 0 to 150 kg, with a resolution of 0.05 kg, previously calibrated. The Body Mass Index (BMI) was calculated by the quotient of body weight in kilograms by height in m2 and converted into Z-scores adjusted by age and sex.
The classification of children according to nutritional status (underweight, healthy weight, overweight or obese) was established through the three criteria mentioned above: CDC / NCHS 2000 IOTF (Cole et al14) and Conde and Monteiro16.
The measurement methodology and classification of blood pressure followed the recommendations of the last international consensus on the subject, established in 4th National Task Force on Hypertension of the National Heart, Lung and Blood Institute4. Blood pressure levels were assessed by auscultation using a periodically calibrated aneroid sphygmomanometer and a stethoscope placed over the brachial artery pulse 2 cm above the cubital fossa/elbow pits. The cuff was selected according to arm circumference, measured at the midpoint between the acromion and the elbow, with the arm flexed at 90 degrees with the forear, according to the recommendations of the guidelines above4. The measurements were performed with the child in a sitting position, with their right arm flexed at 90 degrees at the heart level and supported on a fixed surface, in a calm environment. During preparation, the
child remained at rest for at least 5 minutes, the child was instructed not to talk during the measurement. The average of three measurements taken within an interval of 3 minutes was used for classification as blood pressure levels and to calculate the Z-score for blood pressure, adjusted by age, sex, and height percentile. Children with average Systolic Blood Pressure (SBP) and/or Diastolic Blood Pressure (DBP) equal to or greater than the 95th percentile for sex, age and height percentile were classified as having high BP, whereas children with average SBP and/or DBP between the 90th and 95th percentiles were classified as pre-hypertensive.
For statistical analyzes, the outcomes of interest (nutritional status and blood pressure) were analyzed both as categorical variables as continuous variables in the form. For continuous analysis, the absolute values of weight, height and BMI were converted into Z-scores by age and sex, using the software Growth Analyser® version 3.513. The values of mean blood pressure, systolic and diastolic blood pressure were adjusted by sex, age and height percentile, according to the recommendations of the 4th National Task Force on Hypertension of the National Heart, Lung and Blood Institute4.
Association analyzes were performed by means of group comparisons, correlations and regressions. Comparisons between groups with respect to quantitative variables were made by Student t test or Mann-Whitney test, as appropriate. Qualitative variables were analyzed using the chi-square test.
Using the presence of excess weight as a predictor of high blood pressure, the profiles of sensitivity, specificity, and overall accuracy (area under the ROC curve) were calculated of each nutritional classification criteria regarding detection capability of high BP in these children.
All statistical analyzes were performed using the SigmaStat for Windows (version 3.5, SPSS, Inc., San Rafael, CA). It was considered statistically significant at p < 0.05.
ResultsRegarding the general characteristics of the sample
studied, it was obtained homogeneity in relation to sex, being represented by 51% (n = 417) of boys and 49% girls (n = 400). The mean age was 8.8 ± 1.6 years. Depending on the criteria used to evaluate nutritional status, the percentage of eutrophic children ranged between 67% and 73%, and the percentage of children presenting excess weight (overweight or obese), between 21% and 27% (Figure 1).
The highest prevalence of overweight, including both overweight and obesity, was observed by the criterion of Conde and Monteiro (27%), although the CDC criterion has shown the highest percentage of obesity (11%). Using the IOTF criterion, we observed the lowest percentage of children classified as having excess weight (21%) and the highest percentage of underweight (12%).
It was observed that 3.4% of the children had average levels of BP, adjusted by age, sex and height percentile, consistent with the diagnosis of pre-hypertension, and 3.9% diagnosed with hypertension. There was no significant association between the presence of high blood pressure
176
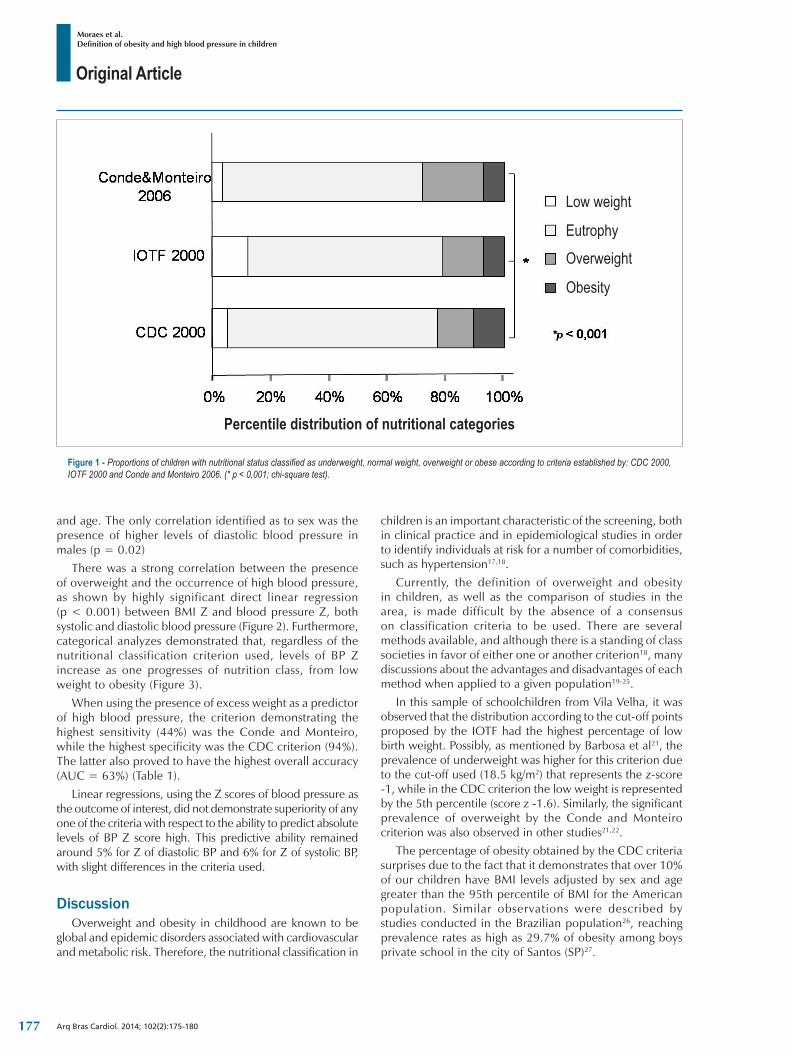
Original Article
Moraes et al.Definition of obesity and high blood pressure in children
Arq Bras Cardiol. 2014; 102(2):175-180
Figure 1 ‑ Proportions of children with nutritional status classified as underweight, normal weight, overweight or obese according to criteria established by: CDC 2000, IOTF 2000 and Conde and Monteiro 2006. (* p < 0,001; chi-square test).
Percentile distribution of nutritional categories
Low weight
Eutrophy
Overweight
Obesity
and age. The only correlation identified as to sex was the presence of higher levels of diastolic blood pressure in males (p = 0.02)
There was a strong correlation between the presence of overweight and the occurrence of high blood pressure, as shown by highly significant direct linear regression (p < 0.001) between BMI Z and blood pressure Z, both systolic and diastolic blood pressure (Figure 2). Furthermore, categorical analyzes demonstrated that, regardless of the nutritional classification criterion used, levels of BP Z increase as one progresses of nutrition class, from low weight to obesity (Figure 3).
When using the presence of excess weight as a predictor of high blood pressure, the criterion demonstrating the highest sensitivity (44%) was the Conde and Monteiro, while the highest specificity was the CDC criterion (94%). The latter also proved to have the highest overall accuracy (AUC = 63%) (Table 1).
Linear regressions, using the Z scores of blood pressure as the outcome of interest, did not demonstrate superiority of any one of the criteria with respect to the ability to predict absolute levels of BP Z score high. This predictive ability remained around 5% for Z of diastolic BP and 6% for Z of systolic BP, with slight differences in the criteria used.
DiscussionOverweight and obesity in childhood are known to be
global and epidemic disorders associated with cardiovascular and metabolic risk. Therefore, the nutritional classification in
children is an important characteristic of the screening, both in clinical practice and in epidemiological studies in order to identify individuals at risk for a number of comorbidities, such as hypertension17,18.
Currently, the definition of overweight and obesity in children, as well as the comparison of studies in the area, is made difficult by the absence of a consensus on classification criteria to be used. There are several methods available, and although there is a standing of class societies in favor of either one or another criterion18, many discussions about the advantages and disadvantages of each method when applied to a given population19-25.
In this sample of schoolchildren from Vila Velha, it was observed that the distribution according to the cut-off points proposed by the IOTF had the highest percentage of low birth weight. Possibly, as mentioned by Barbosa et al21, the prevalence of underweight was higher for this criterion due to the cut-off used (18.5 kg/m2) that represents the z-score -1, while in the CDC criterion the low weight is represented by the 5th percentile (score z -1.6). Similarly, the significant prevalence of overweight by the Conde and Monteiro criterion was also observed in other studies21,22.
The percentage of obesity obtained by the CDC criteria surprises due to the fact that it demonstrates that over 10% of our children have BMI levels adjusted by sex and age greater than the 95th percentile of BMI for the American population. Similar observations were described by studies conducted in the Brazilian population26, reaching prevalence rates as high as 29.7% of obesity among boys private school in the city of Santos (SP)27.
177
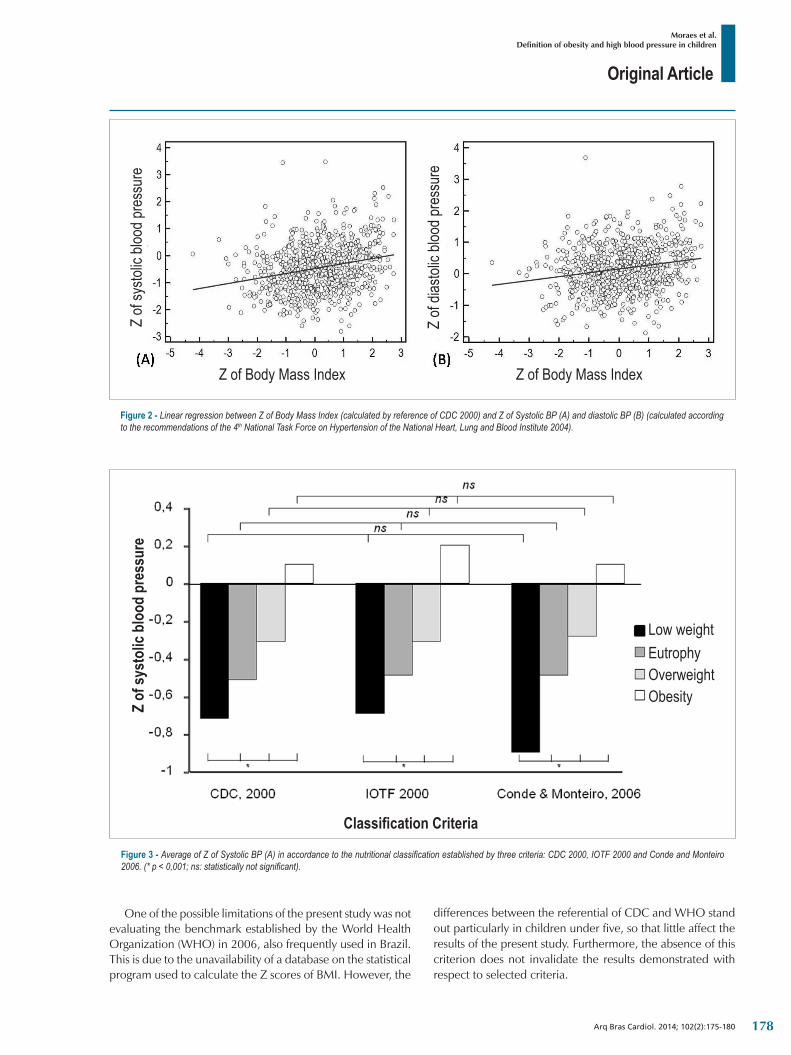
Original Article
Moraes et al.Definition of obesity and high blood pressure in children
Arq Bras Cardiol. 2014; 102(2):175-180
Figure 2 ‑ Linear regression between Z of Body Mass Index (calculated by reference of CDC 2000) and Z of Systolic BP (A) and diastolic BP (B) (calculated according to the recommendations of the 4th National Task Force on Hypertension of the National Heart, Lung and Blood Institute 2004).
Z of Body Mass Index
Z of
systo
lic bl
ood p
ress
ure
Z of Body Mass Index
Z of
diasto
lic bl
ood p
ress
ure
Figure 3 ‑ Average of Z of Systolic BP (A) in accordance to the nutritional classification established by three criteria: CDC 2000, IOTF 2000 and Conde and Monteiro 2006. (* p < 0,001; ns: statistically not significant).
Classification Criteria
Low weightEutrophyOverweightObesityZ
of sy
stol
ic bl
ood
pres
sure
One of the possible limitations of the present study was not evaluating the benchmark established by the World Health Organization (WHO) in 2006, also frequently used in Brazil. This is due to the unavailability of a database on the statistical program used to calculate the Z scores of BMI. However, the
differences between the referential of CDC and WHO stand out particularly in children under five, so that little affect the results of the present study. Furthermore, the absence of this criterion does not invalidate the results demonstrated with respect to selected criteria.
178
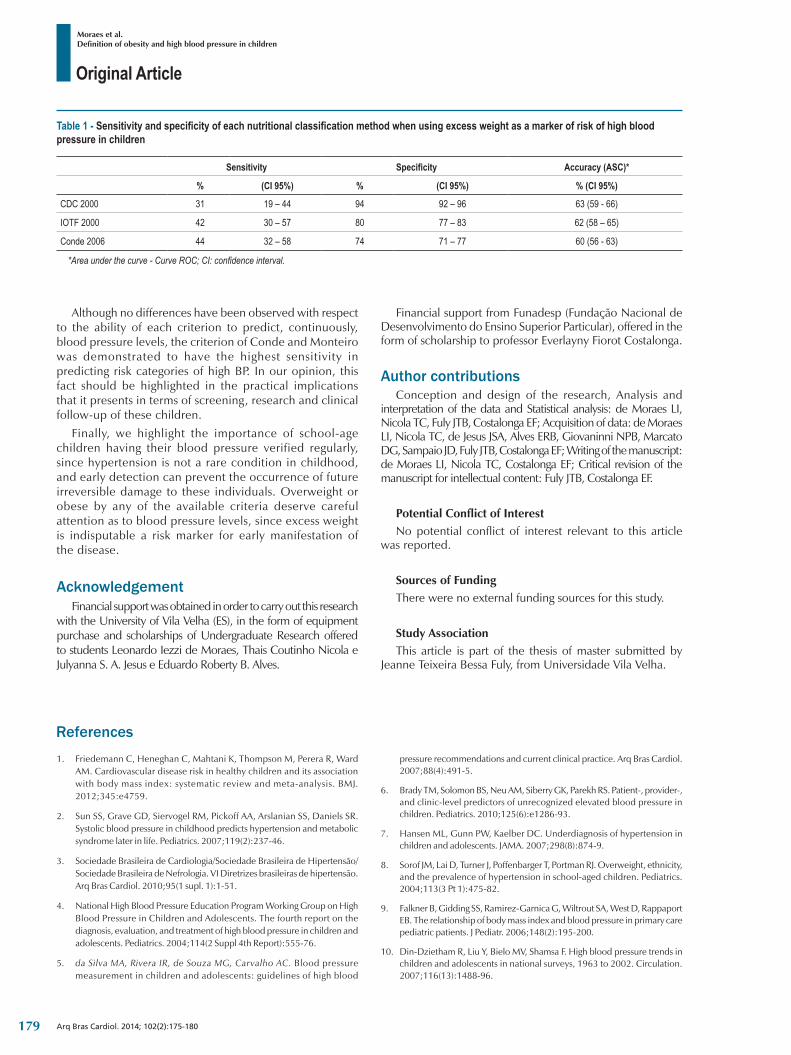
Original Article
Moraes et al.Definition of obesity and high blood pressure in children
Arq Bras Cardiol. 2014; 102(2):175-180
1. Friedemann C, Heneghan C, Mahtani K, Thompson M, Perera R, Ward AM. Cardiovascular disease risk in healthy children and its association with body mass index: systematic review and meta-analysis. BMJ. 2012;345:e4759.
2. Sun SS, Grave GD, Siervogel RM, Pickoff AA, Arslanian SS, Daniels SR. Systolic blood pressure in childhood predicts hypertension and metabolic syndrome later in life. Pediatrics. 2007;119(2):237-46.
3. Sociedade Brasileira de Cardiologia/Sociedade Brasileira de Hipertensão/Sociedade Brasileira de Nefrologia. VI Diretrizes brasileiras de hipertensão. Arq Bras Cardiol. 2010;95(1 supl. 1):1-51.
4. National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics. 2004;114(2 Suppl 4th Report):555-76.
5. da Silva MA, Rivera IR, de Souza MG, Carvalho AC. Blood pressure measurement in children and adolescents: guidelines of high blood
pressure recommendations and current clinical practice. Arq Bras Cardiol. 2007;88(4):491-5.
6. Brady TM, Solomon BS, Neu AM, Siberry GK, Parekh RS. Patient-, provider-, and clinic-level predictors of unrecognized elevated blood pressure in children. Pediatrics. 2010;125(6):e1286-93.
7. Hansen ML, Gunn PW, Kaelber DC. Underdiagnosis of hypertension in children and adolescents. JAMA. 2007;298(8):874-9.
8. Sorof JM, Lai D, Turner J, Poffenbarger T, Portman RJ. Overweight, ethnicity, and the prevalence of hypertension in school-aged children. Pediatrics. 2004;113(3 Pt 1):475-82.
9. Falkner B, Gidding SS, Ramirez-Garnica G, Wiltrout SA, West D, Rappaport EB. The relationship of body mass index and blood pressure in primary care pediatric patients. J Pediatr. 2006;148(2):195-200.
10. Din-Dzietham R, Liu Y, Bielo MV, Shamsa F. High blood pressure trends in children and adolescents in national surveys, 1963 to 2002. Circulation. 2007;116(13):1488-96.
References
Table 1 ‑ Sensitivity and specificity of each nutritional classification method when using excess weight as a marker of risk of high blood pressure in children
Sensitivity Specificity Accuracy (ASC)*
% (CI 95%) % (CI 95%) % (CI 95%)
CDC 2000 31 19 – 44 94 92 – 96 63 (59 - 66)
IOTF 2000 42 30 – 57 80 77 – 83 62 (58 – 65)
Conde 2006 44 32 – 58 74 71 – 77 60 (56 - 63)
*Area under the curve - Curve ROC; CI: confidence interval.
Although no differences have been observed with respect to the ability of each criterion to predict, continuously, blood pressure levels, the criterion of Conde and Monteiro was demonstrated to have the highest sensitivity in predicting risk categories of high BP. In our opinion, this fact should be highlighted in the practical implications that it presents in terms of screening, research and clinical follow-up of these children.
Finally, we highlight the importance of school-age children having their blood pressure verified regularly, since hypertension is not a rare condition in childhood, and early detection can prevent the occurrence of future irreversible damage to these individuals. Overweight or obese by any of the available criteria deserve careful attention as to blood pressure levels, since excess weight is indisputable a risk marker for early manifestation of the disease.
AcknowledgementFinancial support was obtained in order to carry out this research
with the University of Vila Velha (ES), in the form of equipment purchase and scholarships of Undergraduate Research offered to students Leonardo Iezzi de Moraes, Thais Coutinho Nicola e Julyanna S. A. Jesus e Eduardo Roberty B. Alves.
Financial support from Funadesp (Fundação Nacional de Desenvolvimento do Ensino Superior Particular), offered in the form of scholarship to professor Everlayny Fiorot Costalonga.
Author contributionsConception and design of the research, Analysis and
interpretation of the data and Statistical analysis: de Moraes LI, Nicola TC, Fuly JTB, Costalonga EF; Acquisition of data: de Moraes LI, Nicola TC, de Jesus JSA, Alves ERB, Giovaninni NPB, Marcato DG, Sampaio JD, Fuly JTB, Costalonga EF; Writing of the manuscript: de Moraes LI, Nicola TC, Costalonga EF; Critical revision of the manuscript for intellectual content: Fuly JTB, Costalonga EF.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported.
Sources of FundingThere were no external funding sources for this study.
Study AssociationThis article is part of the thesis of master submitted by
Jeanne Teixeira Bessa Fuly, from Universidade Vila Velha.
179
Original Article
Moraes et al.Definition of obesity and high blood pressure in children
Arq Bras Cardiol. 2014; 102(2):175-180
11. Dasgupta K, O’Loughlin J, Chen S, Karp I, Paradis G, Tremblay J, et al. Emergence of sex differences in prevalence of high systolic blood pressure: analysis of a longitudinal adolescent cohort. Circulation. 2006;114(24):2663-70.
12. Tu W, Eckert GJ, DiMeglio LA, Yu Z, Jung J, Pratt JH. Intensified effect of adiposity on blood pressure in overweight and obese children. Hypertension. 2011;58(5):818-24.
13. Kuczmarski RJ, Ogden CL, Guo SS, Grummer-Strawn LM, Flegal KM, Mei Z, et al. 2000 CDC growth charts for the United States: methods and development. Vital Health Stat 11. 2002;246:1-190.
14. Cole TJ, Bellizzi MC, Flegal KM, Dietz WH. Establishing a standard definition for child overweight and obesity worldwide: international survey. BMJ. 2000;320(7244):1240-3.
15. Cole TJ, Flegal KM, Nicholls D, Jackson AA. Body mass index cut offs to define thinness in children and adolescents: international survey. BMJ. 2007;335(7612):194.
16. Conde WL, Monteiro CA. Body mass index cutoff points for evaluation of nutritional status in Brazilian children and adolescents. J Pediatr (Rio J). 2006;82(4):266-72.
17. Bergmann GG, Gaya A, Halpern R, Bergmann ML, Rech RR, Constanzi CB, et al. Índice de massa corporal para triagem de fatores de risco para doenças cardiovasculares na infância. Arq Bras Endocrinol Metab. 2011;55(2):114-20.
18. August GP, Caprio S, Fennoy I, Freemark M, Kaufman FR, Lustig RH, et al. Prevention and treatment of pediatric obesity: an endocrine society clinical practice guideline based on expert opinion. J Clin Endocrinol Metab. 2008;93(12):4576-99.
19. Tomkins A. Que padrões usar para medir obesidade em crianças? J Pediatr. (Rio J). 2006;82(4):246-8.
20. Reilly JJ. Assessment of childhood obesity: national reference data or international approach? Obes Res. 2002;10(8):838-40.
21. Barbosa RMS, Soares EA, Lanzillotti HS. Avaliação do estado nutricional de escolares segundo três referências. Rev Paul Pediatr. 2009;27(3):243-50.
22. Vitolo MR, Campagnolo PD, Barros ME, Gama CM, Ancona Lopez F. Evaluation of two classifications for overweight among Brazilian adolescents. Rev Saude Publica. 2007;41(4):653-6.
23. Monasta L, Lobstein T, Cole TJ, Vignerová J, Cattaneo A. Defining overweight and obesity in pre-school children: IOTF reference or WHO standard? Obes Rev. 2011;12(4):295-300.
24. Passos MA, Cintra Ide P, Branco LM, Machado Hda C, Fisberg M. Body mass index percentiles in adolescents of the city of São Paulo, Brazil, and their comparison with international parameters. Arq Bras Endocrinol Metabol. 2010;54(3):295-302.
25. Reilly JJ. Assessment of obesity in children and adolescents: synthesis of recent systematic reviews and clinical guidelines. J Hum Nutr Diet. 2010;23(3):205-11.
26. Pereira A, Guedes AD, Verreschi IT, Santos RD, Martinez TL. A obesidade e sua associação com os demais fatores de risco cardiovascular em escolares de Itapetininga, Brasil. Arq Bras Cardiol. 2009;93(3):253-60.
27. Costa RF, Cintra Ide P, Fisberg M. Prevalência de sobrepeso e obesidade em escolares da cidade de Santos, SP. Arq Bras Endocrinol Metabol. 2006;50(1):60-7.
180
Original Article
Acute Effects of Continuous Positive Air way Pressure on Pulse Pressure in Chronic Heart FailureMônica Quintão1,2, Sérgio Chermont1,2, Luana Marchese1,2, Lúcia Brandão2, Sabrina Pereira Bernardez1, Evandro Tinoco Mesquita1, Nazareth de Novaes Rocha1, Antônio Claudio L. Nóbrega1
Programa de Pós-graduação em Ciências Cardiovasculares/Universidade Federal Fluminense1; Clínica de Insuficiência Cardíaca (CLIC)/Centro Universitário Serra dos Órgãos2, Teresópolis, RJ - Brazil
Mailing Address: Sergio Chermont • Estrada da Prata s/n. Prata. CEP 25976-340, Teresópolis, RJ – BrazilE-mail: [email protected] Manuscript received June 08, 2013, revised manuscript August 10, 2013, accepted September 19, 2013.
DOI: 10.5935/abc.20140006
Abstract
Background: Patients with heart failure (HF) have left ventricular dysfunction and reduced mean arterial pressure (MAP). Increased adrenergic drive causes vasoconstriction and vessel resistance maintaining MAP, while increasing peripheral vascular resistance and conduit vessel stiffness. Increased pulse pressure (PP) reflects a complex interaction of the heart with the arterial and venous systems. Increased PP is an important risk marker in patients with chronic HF (CHF). Non-invasive ventilation (NIV) has been used for acute decompensated HF, to improve congestion and ventilation through both respiratory and hemodynamic effects. However, none of these studies have reported the effect of NIV on PP.
Objective: The objective of this study was to determine the acute effects of NIV with CPAP on PP in outpatients with CHF.
Methods: Following a double-blind, randomized, cross-over, and placebo-controlled protocol, twenty three patients with CHF (17 males; 60 ± 11 years; BMI 29 ± 5 kg/cm2, NYHA class II, III) underwent CPAP via nasal mask for 30 min in a recumbent position. Mask pressure was 6 cmH2O, whereas placebo was fixed at 0-1 cmH2O. PP and other non invasive hemodynamics variables were assessed before, during and after placebo and CPAP mode.
Results: CPAP decreased resting heart rate (Pre: 72 ± 9; vs. Post 5 min: 67 ± 10 bpm; p < 0.01) and MAP (CPAP: 87 ± 11; vs. control 96 ± 11 mmHg; p < 0.05 post 5 min). CPAP decreased PP (CPAP: 47 ± 20 pre to 38 ± 19 mmHg post; vs. control: 42 ± 12 mmHg, pre to 41 ± 18 post p < 0.05 post 5 min).
Conclusion: NIV with CPAP decreased pulse pressure in patients with stable CHF. Future clinical trials should investigate whether this effect is associated with improved clinical outcome.(Arq Bras Cardiol. 2014; 102(2):181-186)
Keywords: Heart Failure; Pulse Pressure; CPAP.
IntroductionHeart failure (HF) is one of the main public burdens in
developing countries, and despite medical advances, the mortality of HF remains elevated 1. Neurohumoral activation in HF leads to left ventricular dysfunction and reduced mean arterial pressure (MAP). Compensatory mechanisms to maintain MAP causes vasoconstriction, which increases peripheral vascular resistance and conduit vessel stiffness 2. These effects increase pulse pressure (PP), which reflects a complex interaction of the heart with the arterial and venous systems 3,4. Pulse pressure is determined by two hemodynamic components: a direct component, which is a product of
ventricular ejection (stroke volume and ventricular ejection swiftness) and great vessel viscoelastic property interactions, as well as an indirect component resulting from the pulse wave 5,6. As increased PP expresses progression of HF, it is has been related to increased ventricular afterload 7 and myocardial oxygen demand 8, impaired ventricular relaxation 9, and subendocardial ischemia 10. Therefore, increased PP is an important risk marker for subsequent cardiovascular events in patients with chronic HF (CHF)11,12. Previous studies have reported that a PP of 50 mm Hg is the mean normal value for clinic reference in both men and women 13, and above 53 mm Hg it increases risk of cardiovascular events 14,15.
Noninvasive ventilation (NIV) has been used in decompensated HF to decrease pulmonary congestion and improve ventilation through both mechanical and hemodynamic effects 16,17. In patients with stable CHF, NIV has not been extensively studied. Naughton et al 18 have shown that the administration of continuous positive airway pressure (CPAP) to patients with stable HF at rest acutely improved cardiac performance and also reduced the work of breathing. Others have shown increases in cardiac output and stroke
181
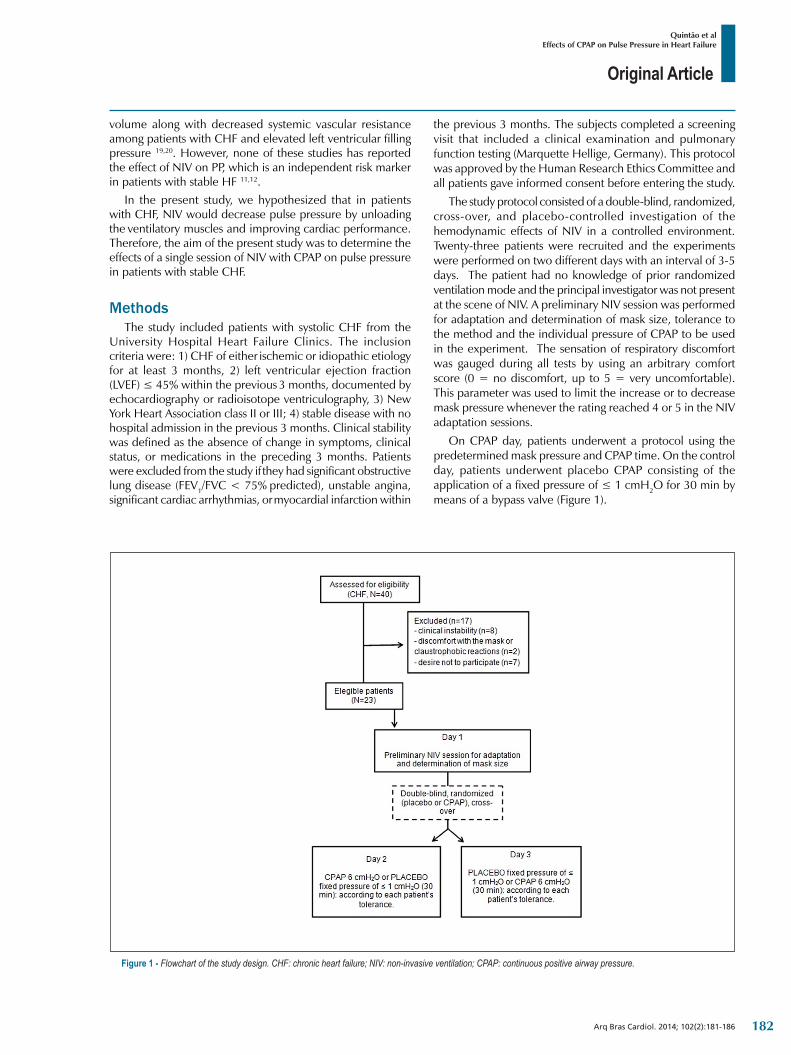
Original Article
Quintão et alEffects of CPAP on Pulse Pressure in Heart Failure
Arq Bras Cardiol. 2014; 102(2):181-186
volume along with decreased systemic vascular resistance among patients with CHF and elevated left ventricular filling pressure 19,20. However, none of these studies has reported the effect of NIV on PP, which is an independent risk marker in patients with stable HF 11,12.
In the present study, we hypothesized that in patients with CHF, NIV would decrease pulse pressure by unloading the ventilatory muscles and improving cardiac performance. Therefore, the aim of the present study was to determine the effects of a single session of NIV with CPAP on pulse pressure in patients with stable CHF.
MethodsThe study included patients with systolic CHF from the
University Hospital Heart Failure Clinics. The inclusion criteria were: 1) CHF of either ischemic or idiopathic etiology for at least 3 months, 2) left ventricular ejection fraction (LVEF) ≤ 45% within the previous 3 months, documented by echocardiography or radioisotope ventriculography, 3) New York Heart Association class II or III; 4) stable disease with no hospital admission in the previous 3 months. Clinical stability was defined as the absence of change in symptoms, clinical status, or medications in the preceding 3 months. Patients were excluded from the study if they had significant obstructive lung disease (FEV1/FVC < 75% predicted), unstable angina, significant cardiac arrhythmias, or myocardial infarction within
Figure 1 ‑ Flowchart of the study design. CHF: chronic heart failure; NIV: non-invasive ventilation; CPAP: continuous positive airway pressure.
the previous 3 months. The subjects completed a screening visit that included a clinical examination and pulmonary function testing (Marquette Hellige, Germany). This protocol was approved by the Human Research Ethics Committee and all patients gave informed consent before entering the study.
The study protocol consisted of a double-blind, randomized, cross-over, and placebo-controlled investigation of the hemodynamic effects of NIV in a controlled environment. Twenty-three patients were recruited and the experiments were performed on two different days with an interval of 3-5 days. The patient had no knowledge of prior randomized ventilation mode and the principal investigator was not present at the scene of NIV. A preliminary NIV session was performed for adaptation and determination of mask size, tolerance to the method and the individual pressure of CPAP to be used in the experiment. The sensation of respiratory discomfort was gauged during all tests by using an arbitrary comfort score (0 = no discomfort, up to 5 = very uncomfortable). This parameter was used to limit the increase or to decrease mask pressure whenever the rating reached 4 or 5 in the NIV adaptation sessions.
On CPAP day, patients underwent a protocol using the predetermined mask pressure and CPAP time. On the control day, patients underwent placebo CPAP consisting of the application of a fixed pressure of ≤ 1 cmH2O for 30 min by means of a bypass valve (Figure 1).
182
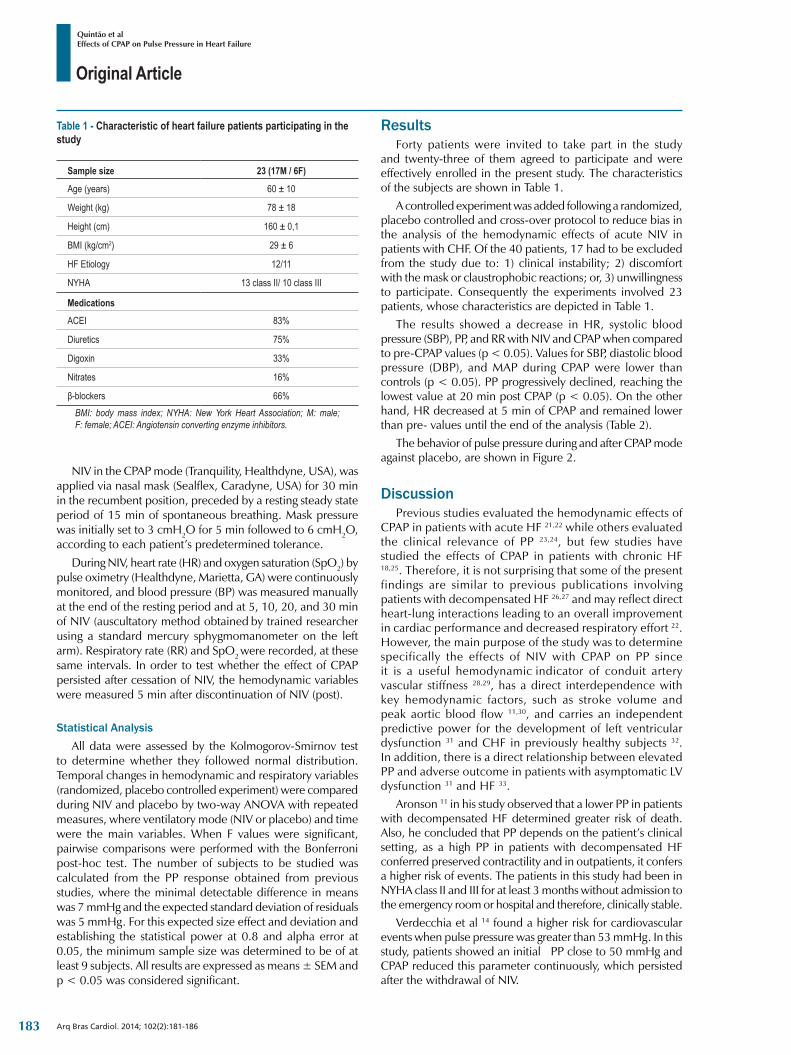
Original Article
Quintão et alEffects of CPAP on Pulse Pressure in Heart Failure
Arq Bras Cardiol. 2014; 102(2):181-186
Table 1 ‑ Characteristic of heart failure patients participating in the study
Sample size 23 (17M / 6F)
Age (years) 60 ± 10
Weight (kg) 78 ± 18
Height (cm) 160 ± 0,1
BMI (kg/cm2) 29 ± 6
HF Etiology 12/11
NYHA 13 class II/ 10 class III
Medications
ACEI 83%
Diuretics 75%
Digoxin 33%
Nitrates 16%
β-blockers 66%BMI: body mass index; NYHA: New York Heart Association; M: male; F: female; ACEI: Angiotensin converting enzyme inhibitors.
NIV in the CPAP mode (Tranquility, Healthdyne, USA), was applied via nasal mask (Sealflex, Caradyne, USA) for 30 min in the recumbent position, preceded by a resting steady state period of 15 min of spontaneous breathing. Mask pressure was initially set to 3 cmH2O for 5 min followed to 6 cmH2O, according to each patient’s predetermined tolerance.
During NIV, heart rate (HR) and oxygen saturation (SpO2) by pulse oximetry (Healthdyne, Marietta, GA) were continuously monitored, and blood pressure (BP) was measured manually at the end of the resting period and at 5, 10, 20, and 30 min of NIV (auscultatory method obtained by trained researcher using a standard mercury sphygmomanometer on the left arm). Respiratory rate (RR) and SpO2 were recorded, at these same intervals. In order to test whether the effect of CPAP persisted after cessation of NIV, the hemodynamic variables were measured 5 min after discontinuation of NIV (post).
Statistical AnalysisAll data were assessed by the Kolmogorov-Smirnov test
to determine whether they followed normal distribution. Temporal changes in hemodynamic and respiratory variables (randomized, placebo controlled experiment) were compared during NIV and placebo by two-way ANOVA with repeated measures, where ventilatory mode (NIV or placebo) and time were the main variables. When F values were significant, pairwise comparisons were performed with the Bonferroni post-hoc test. The number of subjects to be studied was calculated from the PP response obtained from previous studies, where the minimal detectable difference in means was 7 mmHg and the expected standard deviation of residuals was 5 mmHg. For this expected size effect and deviation and establishing the statistical power at 0.8 and alpha error at 0.05, the minimum sample size was determined to be of at least 9 subjects. All results are expressed as means ± SEM and p < 0.05 was considered significant.
ResultsForty patients were invited to take part in the study
and twenty-three of them agreed to participate and were effectively enrolled in the present study. The characteristics of the subjects are shown in Table 1.
A controlled experiment was added following a randomized, placebo controlled and cross-over protocol to reduce bias in the analysis of the hemodynamic effects of acute NIV in patients with CHF. Of the 40 patients, 17 had to be excluded from the study due to: 1) clinical instability; 2) discomfort with the mask or claustrophobic reactions; or, 3) unwillingness to participate. Consequently the experiments involved 23 patients, whose characteristics are depicted in Table 1.
The results showed a decrease in HR, systolic blood pressure (SBP), PP, and RR with NIV and CPAP when compared to pre-CPAP values (p < 0.05). Values for SBP, diastolic blood pressure (DBP), and MAP during CPAP were lower than controls (p < 0.05). PP progressively declined, reaching the lowest value at 20 min post CPAP (p < 0.05). On the other hand, HR decreased at 5 min of CPAP and remained lower than pre- values until the end of the analysis (Table 2).
The behavior of pulse pressure during and after CPAP mode against placebo, are shown in Figure 2.
DiscussionPrevious studies evaluated the hemodynamic effects of
CPAP in patients with acute HF 21,22 while others evaluated the clinical relevance of PP 23,24, but few studies have studied the effects of CPAP in patients with chronic HF 18,25. Therefore, it is not surprising that some of the present findings are similar to previous publications involving patients with decompensated HF 26,27 and may reflect direct heart-lung interactions leading to an overall improvement in cardiac performance and decreased respiratory effort 22. However, the main purpose of the study was to determine specifically the effects of NIV with CPAP on PP since it is a useful hemodynamic indicator of conduit artery vascular stiffness 28,29, has a direct interdependence with key hemodynamic factors, such as stroke volume and peak aortic blood flow 11,30, and carries an independent predictive power for the development of left ventricular dysfunction 31 and CHF in previously healthy subjects 32.
In addition, there is a direct relationship between elevated PP and adverse outcome in patients with asymptomatic LV dysfunction 31 and HF 33.
Aronson 11 in his study observed that a lower PP in patients with decompensated HF determined greater risk of death. Also, he concluded that PP depends on the patient’s clinical setting, as a high PP in patients with decompensated HF conferred preserved contractility and in outpatients, it confers a higher risk of events. The patients in this study had been in NYHA class II and III for at least 3 months without admission to the emergency room or hospital and therefore, clinically stable.
Verdecchia et al 14 found a higher risk for cardiovascular events when pulse pressure was greater than 53 mmHg. In this study, patients showed an initial PP close to 50 mmHg and CPAP reduced this parameter continuously, which persisted after the withdrawal of NIV.
183
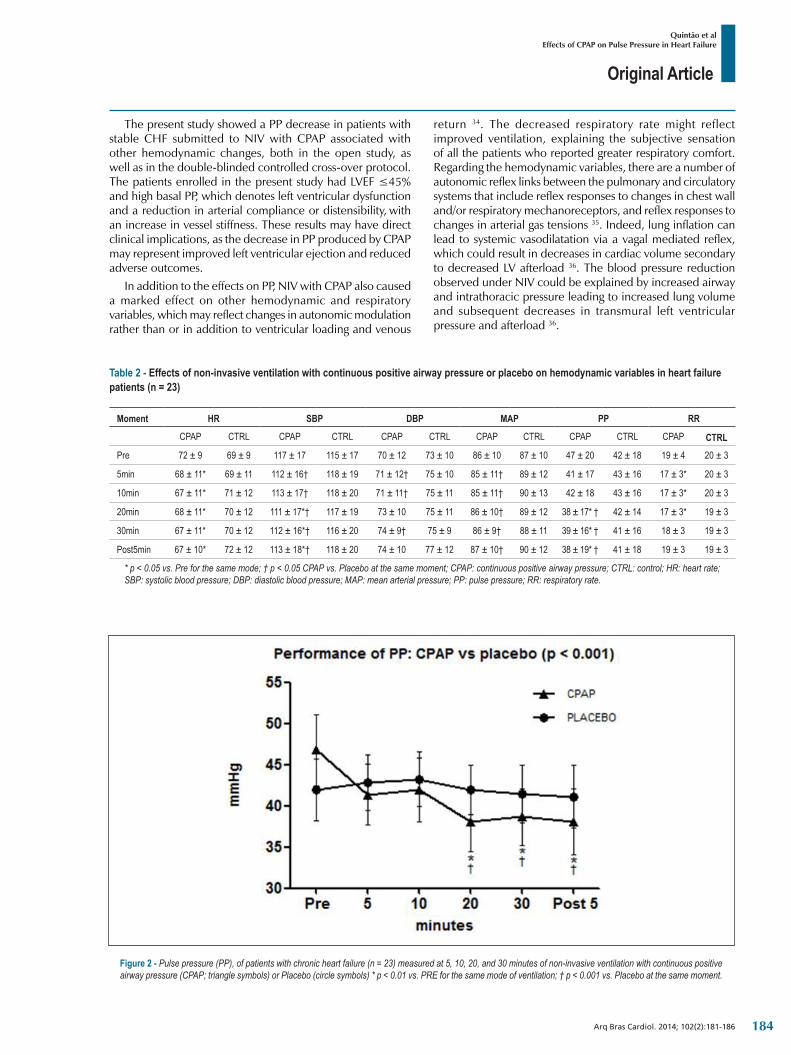
Original Article
Quintão et alEffects of CPAP on Pulse Pressure in Heart Failure
Arq Bras Cardiol. 2014; 102(2):181-186
Table 2 ‑ Effects of non-invasive ventilation with continuous positive airway pressure or placebo on hemodynamic variables in heart failure patients (n = 23)
Moment HR SBP DBP MAP PP RR
CPAP CTRL CPAP CTRL CPAP CTRL CPAP CTRL CPAP CTRL CPAP CTRL
Pre 72 ± 9 69 ± 9 117 ± 17 115 ± 17 70 ± 12 73 ± 10 86 ± 10 87 ± 10 47 ± 20 42 ± 18 19 ± 4 20 ± 3
5min 68 ± 11* 69 ± 11 112 ± 16† 118 ± 19 71 ± 12† 75 ± 10 85 ± 11† 89 ± 12 41 ± 17 43 ± 16 17 ± 3* 20 ± 3
10min 67 ± 11* 71 ± 12 113 ± 17† 118 ± 20 71 ± 11† 75 ± 11 85 ± 11† 90 ± 13 42 ± 18 43 ± 16 17 ± 3* 20 ± 3
20min 68 ± 11* 70 ± 12 111 ± 17*† 117 ± 19 73 ± 10 75 ± 11 86 ± 10† 89 ± 12 38 ± 17* † 42 ± 14 17 ± 3* 19 ± 3
30min 67 ± 11* 70 ± 12 112 ± 16*† 116 ± 20 74 ± 9† 75 ± 9 86 ± 9† 88 ± 11 39 ± 16* † 41 ± 16 18 ± 3 19 ± 3
Post5min 67 ± 10* 72 ± 12 113 ± 18*† 118 ± 20 74 ± 10 77 ± 12 87 ± 10† 90 ± 12 38 ± 19* † 41 ± 18 19 ± 3 19 ± 3
* p < 0.05 vs. Pre for the same mode; † p < 0.05 CPAP vs. Placebo at the same moment; CPAP: continuous positive airway pressure; CTRL: control; HR: heart rate; SBP: systolic blood pressure; DBP: diastolic blood pressure; MAP: mean arterial pressure; PP: pulse pressure; RR: respiratory rate.
The present study showed a PP decrease in patients with stable CHF submitted to NIV with CPAP associated with other hemodynamic changes, both in the open study, as well as in the double-blinded controlled cross-over protocol. The patients enrolled in the present study had LVEF ≤45% and high basal PP, which denotes left ventricular dysfunction and a reduction in arterial compliance or distensibility, with an increase in vessel stiffness. These results may have direct clinical implications, as the decrease in PP produced by CPAP may represent improved left ventricular ejection and reduced adverse outcomes.
In addition to the effects on PP, NIV with CPAP also caused a marked effect on other hemodynamic and respiratory variables, which may reflect changes in autonomic modulation rather than or in addition to ventricular loading and venous
return 34. The decreased respiratory rate might reflect improved ventilation, explaining the subjective sensation of all the patients who reported greater respiratory comfort. Regarding the hemodynamic variables, there are a number of autonomic reflex links between the pulmonary and circulatory systems that include reflex responses to changes in chest wall and/or respiratory mechanoreceptors, and reflex responses to changes in arterial gas tensions 35. Indeed, lung inflation can lead to systemic vasodilatation via a vagal mediated reflex, which could result in decreases in cardiac volume secondary to decreased LV afterload 36. The blood pressure reduction observed under NIV could be explained by increased airway and intrathoracic pressure leading to increased lung volume and subsequent decreases in transmural left ventricular pressure and afterload 36.
Figure 2 ‑ Pulse pressure (PP), of patients with chronic heart failure (n = 23) measured at 5, 10, 20, and 30 minutes of non-invasive ventilation with continuous positive airway pressure (CPAP; triangle symbols) or Placebo (circle symbols) * p < 0.01 vs. PRE for the same mode of ventilation; † p < 0.001 vs. Placebo at the same moment.
184

Original Article
Quintão et alEffects of CPAP on Pulse Pressure in Heart Failure
Arq Bras Cardiol. 2014; 102(2):181-186
1. McMurray JJ, Adamopoulos S, Anker SD, Auricchio A, Böhm M, Dickstein K, et al; ESC Committee for Practice Guidelines. ESC guidelines for the diagnosis and treatment of acute and chronic heart failure 2012: the Task Force for the Diagnosis and Treatment of Acute and Chronic Heart Failure 2012 of the European Society of Cardiology. Developed in collaboration with the Heart Failure Association (HFA) of the ESC. Eur J Heart Fail. 2012;14(8):803-69. Erratum in: Eur J Heart Fail. 2013;15(3):361-2.
2. Wilbur J, James P. Diagnosis and management of heart failure in the outpatient setting. Prim Care. 2005;32(4):1115-29.
3. Stergiopulos N, Meister JJ, Westerhof N. Determinants of stroke volume and systolic and diastolic aortic pressure. Am J Physiol. 1996;270(6 Pt 2):H2050-9.
4. Stergiopulos N, Westerhof N. Determinants of pulse pressure. Hypertension. 1998;32(3):556-9.
5. Safar ME, Levy BI, Struijker-Boudier H. Current perspectives on arterial stiffness and pulse pressure in hypertension and cardiovascular diseases. Circulation. 2003;107(22):2864-9.
6. Dart AM, Kingwell BA. Pulse pressure - a review of mechanisms and clinical relevance. J Am Coll Cardiol. 2001;37(4):975-84.
7. Milnor WR. Arterial impedance as ventricular afterload. Circ Res. 1975;36(5):565-70.
8. Kelly RP, Tunin R, Kass DA. Effect of reduced aortic compliance on cardiac efficiency and contractile function of in situ canine left ventricle. Circ Res. 1992;71(3):490-502.
9. Kohno F, Kumada T, Kambayashi M, Hayashida W, Ishikawa N, Sasayama S. Change in aortic end-systolic pressure by alterations in loading sequence and its relation to left ventricular isovolumic relaxation. Circulation. 1996;93(11):2080-7.
10. Kass DA, Saeki A, Tunin RS, Recchia FA. Adverse influence of systemic vascular stiffening on cardiac dysfunction and adaptation to acute coronary occlusion. Circulation. 1996;93(8):1533-41.
11. Aronson D, Burger AJ. Relation between pulse pressure and survival in patients with decompensated heart failure. Am J Cardiol. 2004;93(6):785-8.
12. Lee TT, Chen J, Cohen DJ, Tsao L. The association between blood pressure and mortality in patients with heart failure. Am Heart J. 2006;151(1):76-83.
13. Asmar R, Vol S, Brisac AM, Tichet J, Topouchian J. Reference values for clinic pulse pressure in a nonselected population. Am J Hypertens. 2001;14(5 Pt 1):415-8.
References
NIV is a safe and feasible ventilation method easily applied in the ambulatory setting, but its effectiveness is critically dependent on patient comfort and acceptance 25,27. Therefore, in the present study, a preliminary NIV session (phase 1) for adaptation and determination of the mask was performed. This preliminary session was also employed to determine the individual CPAP pressure to be used in the subsequent experiments, which was determined to be the lowest pressure that resulted in greater hemodynamic responses, while being comfortable for the patient. The CPAP pressure level that resulted in significant hemodynamic responses was close to 6 cmH2O. These values of CPAP pressure were similar to those in previous studies that demonstrated improved cardiac output with low CPAP levels 19,37. As previous publications had shown myocardial ischemia in patients with ischemic heart failure during the administration of bilevel positive airway pressure (Bipap)38,39, the CPAP mode was chosen in order to decrease the occurrence of potential adverse outcomes. Accordingly, there were no events triggered by CPAP in the patients participating in the present study.
Limitations In our study it was not possible to determine the exact
mechanism responsible for the hemodynamic changes; however, it is already known from previous studies that increases in cardiac output with CPAP might be explained by systemic vasodilatation, possibly on a reflex basis, leading to a decrease in the left ventricular afterload and consequent increased stroke volume and cardiac output 35. We observed that the hemodynamic effects of NIV with CPAP remained up to five minutes after CPAP withdrawal; however, we understand that further studies are needed to determine the duration of these effects after CPAP cessation. Although in the present study clinic outcomes were not measured, in a previous study an improvement was observed in the exercise
tolerance with CHF patients after NIV with CPAP (placebo vs. CPAP)40.
ConclusionsWe conclude that NIV with CPAP is an effective non-
pharmacological method to reduce pulse pressure in patients with stable chronic heart failure with potential clinical implications for the management of this group of patients.
Author contributionsConception and design of the research: Quintão M,
Chermont S, Mesquita ET, Nóbrega ACL; Acquisition of data: Quintão M, Chermont S, Rocha NN; Analysis and interpretation of the data: Quintão M, Chermont S, Marchese L, Brandão L, Bernardez SP, Mesquita ET, Rocha NN, Nóbrega ACL; Statistical analysis: Quintão M, Chermont S, Nóbrega ACL; Writing of the manuscript: Quintão M, Chermont S, Marchese L, Bernardez SP, Mesquita ET, Nóbrega ACL; Critical revision of the manuscript for intellectual content: Quintão M, Chermont S, Marchese L, Brandão L, Bernardez SP, Mesquita ET, Nóbrega ACL.
Potential Conflict of InterestNo potential conflict of interest relevant to this article was
reported. Sources of FundingThere were no external funding sources for this study. Study AssociationThis article is part of the thesis of master submitted by
Mônica Quintão from Universidade Federal Fluminense.
185

Original Article
Quintão et alEffects of CPAP on Pulse Pressure in Heart Failure
Arq Bras Cardiol. 2014; 102(2):181-186
14. Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Pede S, Porcellati C. Ambulatory pulse pressure: a potent predictor of total cardiovascular risk in hypertension. Hypertension. 1998;32(6):983-8.
15. Sociedade Brasileira de Cardiologia, Sociedade Brasileira de Hipertensão, Sociedade Brasileira de Nefrologia. V Diretrizes Brasileiras de Monitorização Ambulatorial da Pressão Arterial (MAPA) e III Diretrizes Brasileiras de Monitorização Residencial de Pressão Arterial (MRPA). Arq Bras Cardiol. 2011;97(3 supl.3):1-24.
16. Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med. 2001;163:540-77.
17. Rogers RL, Feller ED, Gottlieb SS. Acute congestive heart failure in the emergency department. Cardiol Clin. 2006;24(1):115-23.
18. Naughton MT, Rahman MA, Hara K, Floras JS, Bradley TD. Effect of continuous positive airway pressure in intrathoracic and left ventricular transmural pressures in patients with congestive heart failure. Circulation. 1995;91(6):1725-31.
19. Bradley TD, Holloway RM, McLaughlin PR, Ross BL, Walters J, Liu PP. Cardiac output response to continuous positive airway pressure in congestive heart failure. Am Rev Respir Dis. 1992;145(2 Pt 1):377-82.
20. De Hoyos A, Liu PP, Benard DC, Bradley TD. Hemodynamic effects of continuous positive airway pressure in humans with normal and impaired left ventricular function. Clin Sci (Lond). 1995;88(2):173-8.
21. Bendjelid K, Schütz N, Suter PM, Fournier G, Jacques D, Fareh S, et al. Does continuous positive airway pressure by face mask improve patients with acute cardiogenic pulmonary edema due to left ventricular diastolic dysfunction? Chest. 2005;127(3):1053-8.
22. Pinsky MR. Cardiovascular issues in respiratory care. Chest. 2005;128(5 Suppl 2):592S-597S.
23. Zieman SJ, Melenovsky V, Kass DA. Mechanisms, pathophysiology, and therapy of arterial stiffness. Arterioscler Thromb Vasc Biol. 2005;25(5):932-43.
24. London GM, Marchais SJ, Guerin AP, Pannier B. Arterial stiffness: pathophysiology and clinical impact. Clin Exp Hypertens. 2004;26(7-8):689-99.
25. Nadar S, Prasad N, Taylor RS, Lip GY. Positive pressure ventilation in the management of acute and chronic cardiac failure: a systematic review and meta-analysis. Int J Cardiol. 2005;99(2):171-85.
26. Baratz DM, Westbrook PR, Shah PK, Mohsenifar Z. Effect of nasal continuous positive airway pressure on cardiac output and oxygen delivery in patients with congestive heart failure. Chest. 1992;102(5):1397-401.
27. Bersten AD, Holt AW, Vedig AE, Skowronki GA, Baggoley CJ. Treatment of severe cardiogenic pulmonary edema with continuous positive airway pressure delivered by face mask. N Engl J Med. 1991;325(26):1825-30.
28. Dart AM, Kingwell BA. Pulse pressure-a review of mechanisms and clinical relevance. J Am Coll Cardiol. 2001;37(4):975-84.
29. Domanski MJ, Davis BR, Pfeffer MA, Kastantin M, Mitchell GF. Isolated systolic hypertension prognostic information provided by pulse pressure. Hypertension. 1999;34(3):375-80.
30. Milnor WR. Arterial impedance as ventricular afterload. Circ Res. 1975;36(5):565-70.
31. Mitchell GF, Moyé LA, Braunwald E, Rouleau JL, Bernstein V, Geltman EM, et al. Sphygmomanometric determined pulse pressure is a powerful independent predictor of recurrent events after myocardial infarction in patients with impaired left ventricular function. SAVE investigators. Survival and Ventricular Enlargement. Circulation. 1997;96(12):4254-60.
32. Chae CU, Pfeffer MA, Glynn RJ, Mitchell GF, Taylor JO, Hennekens CH. Increased pulse pressure and risk of heart failure in the elderly. JAMA. 1999;281(7):634-9.
33. D o m a n s k i M J, M i t c h e l l G F, N o r m a n J E , E x n e r D V, P i t t B , Pfeffer MA. Independent prognostic information provided by sphygmomanometrically determined pulse pressure and mean arterial pressure in patients with left ventricular dysfunction. J Am Coll Cardiol. 1999;33(4):951-8.
34. Kaye DM, Mansfield D, Aggarwal A, Naugthton MT, Esler MD. Acute effects of continuous positive airway pressure on cardiac sympathetic tone in congestive heart failure. Circulation. 2001;103(19):2336-8.
35. Scharf SM. Respiratory-circulatory interactions in health and disease: lung biology in health and disease. New York, NY: Marcel Dekker; 2001. p. 519-49.
36. Pinsky MR. Heart-lung interactions in health and disease: lung biology in health and disease. New York, NY: Marcel Dekker; 1989. p. 839-76.
37. Pery M, Payen D, Pinsky MR. Monitoring the effect of CPAP on left ventricular function using continuous blood saturation. Chest. 1991;99(2):512-3.
38. Mehta S, Jay GD, Woolard RH, Hipona RA, Connolly EM, Cimini DM, et al. Randomized, prospective trial of bilevel versus continuous positive airway pressure in acute pulmonary edema. Crit Care Med. 1997;25(4):620-8.
39. Bellone A, Monari A, Cortellaro F, Vettorello M, Arlati S, Coen D. Myocardial infarction rate in acute pulmonary edema: noninvasive pressure support ventilation versus continuous positive airway pressure. Crit Care Med. 2004;32(9):1860-5.
40. Chermont S, Quintão MM, Mesquita ET, Rocha NN, Nóbrega AC. Non-invasive ventilation with continuous positive airway pressure acutely improves 6-minute walk distance in chronic heart failure. J Cardiopulm Rehabil Prev. 2009;29(1):44-8.
186
Original Article
Hypertrophic response of the Association of Thyroid Hormone and Exercise in the Heart of RatsFernanda Rodrigues de Souza, Elmiro Santos Resende, Leandro Lopes, Alexandre Gonçalves, Rafaella Chagas, Thiago Fidale, Poliana RodriguesUFU - Universidade Federal de Uberlândia, Uberlândia, MG - Brazil
Mailing Address: Fernanda Rodrigues de Souza •Rua Cachoeira Dourada, 115, Granada. Postal Code 38540-410, Uberlândia MG - BrazilE-mail: [email protected] Manuscript received June 06, 2013; revised manuscript September 20, 2013; accepted September 26, 2013.
DOI: 10.5935/abc.20130243
Abstract
Background: Cardiac hypertrophy is a component of cardiac remodeling occurring in response to an increase of the activity or functional overload of the heart.
Objective: Assess hypertrophic response of the association of thyroid hormone and exercise in the rat heart.
Methods: We used 37 Wistar rats, male, adults were randomly divided into four groups: control, hormone (TH), exercise (E), thyroid hormone and exercise (H + E); the group received daily hormone levothyroxine sodium by gavage at a dose of 20 µg thyroid hormone/100g body weight, the exercise group took swimming five times a week, with additional weight corresponding to 20% of body weight for six weeks; in group H + E were applied simultaneously TH treatment groups and E. The statistics used was analysis of variance, where appropriate, by Tukey test and Pearson correlation test.
Results: The T4 was greater in groups TH and H + E. The total weight of the heart was greater in patients who received thyroid hormone and left ventricular weight was greater in the TH group. The transverse diameter of cardiomyocytes increased in groups TH, E and H + E. The percentage of collagen was greater in groups E and H + E Correlation analysis between variables showed distinct responses.
Conclusion: The association of thyroid hormone with high-intensity exercise produced cardiac hypertrophy, and generated a standard hypertrophy not directly correlated to the degree of fibrosis. (Arq Bras Cardiol. 2014; 102(2):187-191)
Keywords: Thyroid Hormones; Exercise; Rats; Heart; Hyperthyroidism.
IntroductionThe thyroid hormone and physical exercise produce
general elevation of basal metabolism and as a consequence, there occurs a greater oxygen consumption by the tissues. This increased demand is supplied, in part, by elevation of cardiac frequency, blood pressure, both systolic and diastolic, and cardiac output1.
Clinical and experimental trials suggest that cardiac adaptations are the result of direct effects of the hormone on the heart and blood vessels, and indirectly result from serum elevation of cathecolamines2.
Cardiac hypertrophy is a component of cardiac remodeling involving changes in the geometric structure, the biochemical composition, the generation and electric
conduction, the volume of muscle cells in the organization of collagen matrix and blood vessels. It results from changes of genetic, humoral and molecular nature that can arise spontaneously or be induced by stressing mechanisms of different types and various forms of action3.
Physical training, within reasonable limits, induces cardiac hypertrophy of the physiological type, producing adaptations that improve the performance of the cardiovascular system allowing the heart to withstand increases in demands during exercise. Cardiac hypertrophy is accompanied by increase in ventricular filling time and ejection fraction of the left ventricle, with consequent reduction of the heart rate at rest4,5.
The main differences that determine the pattern of cardiac hypertrophy are the type and duration of stimulation that the heart receives. In situations in which athletes receive pressure overloads only during physical activity, cardiac hypertrophy is usually physiological. In contrast, in pathological situations the heart is continuously exposed to functional overload that occurs for a long time, determining pathological hypertrophy6.
The excess thyroid hormone can promote these two patterns of hypertrophy described above (mixed cardiac hypertrophy). This response appears to be due, in part, the volume of overload due to increased venous return produced by the TH and also the direct effects of hormônio7,8.
187

Original Article
Souza et al.Exercise and experimental hyperthyroidism
Arq Bras Cardiol. 2014; 102(2):187-191
ObjectiveEvaluate the hypertrophic response of the association of the
thyroid hormone and exercise in the heart of rats.
MethodThe procedures were performed after approval of the
study protocol by the Ethics Committee on animal use of the institution under the numbers 077/10. The study conducted was of the experimental type.
We used 37 adult Wistar rats, male, weighing approximately 250 grams, derived from the laboratory of animal experiments (CEBEA-UFU). The environmental conditions for all groups were similar with regard to temperature, relative humidity of the air, level of noise and brightness in accordance with the circadian rhythm. The rats were fed with ration and water “ad libitum”.
The rats were weighed and randomly divided into four groups identified as: control (C) 8 animals, hormone (TH) 10 animals, exercise (E) 9 animals, hormone and exercise (H+E) 10 animals; after distributed, the animals underwent an adjustment period of 15 days in the laboratory before the experiment started.
The type of exercise used was of an anaerobic character. For training, we used a glass with 250 mm in diameter9. The water column height in the glass corresponded to 150% of the rat’s body length. The water temperature was maintained between 30°C and 32°C, which is considered thermally neutral in relation to body temperature of the animal10. The load used in training was that corresponding to 20% of body weight of the rate because this is considered to be an overload that increases the concentration of lactate11. The referred work load consisted of lead blocks fixed to a vest in the region before the rats’ trunk. The load was adjusted weekly according to the variation in the weight of the animals.
The training period was started after 7 days of adaptation to the water mean. Training was conducted in 6 weeks and consisted of five weekly sessions of swimming limited by exhaustion.
The hormone was administered by means of oro-gastric probing performed once a day for 6 weeks. The dose of thyroid hormone was 20 µg/100 g of body weight of a suspension of T4 at 0.1% which was obtained from 10 mg tablets of 100 µg of T4 diluted in 10 ml of distilled water12.
After the 6 weeks of the experiment, the rats were sacrificed under anesthesia, proceeding to open the chest for blood collection by direct cardiac puncture and removal of the heart. Confirmation of exposure to high levels of thyroid hormone was performed by serum dosage of T3 and T4 by the ELISA method.
The heart was weighed and preserved in formaldehyde; this process lasted 24 hours. After the use of formaldehyde, the atria were removed and separated from the ventricles for weighing; the material was then forwarded for histological processing.
To analyze the transverse diameters of cardiomyocytes, slides were stained with eosin/ hematoxylin and to
quantify collagen, the slides were stained with picrosirius. We obtained five sections of each ventricle and measured the smallest diameters of five cells (with visible core) in five different fields. For measures, we made analyses on digital images captured randomly by an Olympus BX40 binocular microscope with a 40× objective. To measure the values of the diameters of cardiomyocytes, we used software HL Image (Western Vision).
The quantification of collagen was made by suppression technique of pixels, where three sections were obtained from each ventricle and selected five different fields of each histological section. It was suggested that the area located in the middle portion between the visceral endocardium and epicardium. The measurement was performed by a single observer who was unaware of which group belonged to the slide examined.
To compare the level of hormone, total weight of the heart, left ventricular weight, cardiomyocyte transversal diameter and percent of collagen between the groups after treatment, was carried out using complemented variance analysis (ANOVA) where necessary by Tukey’s test. To analyze the existence or not of correlation between total weight of the heart, left ventricular weight, cardiomyocyte transversal diameter and percentage of collagen, we used Pearson’s correlation test.
ResultsThe serum T4 was greater in groups TH and H+E, compared
to groups C and E. The values of T3 did not differ among the groups. The results found are shown in Table 1.
The results relative to the total weight of the heart (Pcor), left ventricular weight (LVW), cardiomyocyte transversal diameter (CTD) and the percentage of collagen are shown in Table 2.
PCor was greater in groups TH and HE, compared to groups C and E. LVW was greater in group TH in comparison with E. CDT of the left ventricle was greater in groups TH, E and H+E in comparison to C, being observed the highest values in group TH.
Correlation analysis between variables PCor, LVW, CDT and percentage of collagen of the groups showed different responses. The variables in group C showed positive correlation between LVW and PCor (r = 0.74; p < 0.05). The other comparisons did not prove significant.
Applying the same analyses to group TH, we found a positive correlation only between CDT and PCor (r = 0.70; p < 0.05).
In group E there was a positive correlation between LVW and PCor (r = 0.67, p < 0.05) and between the percentage of collagen and LVW (r = 0.79, p < 0.05). There was also a negative correlation between CDT and LVW (r = 0.62; p < 0.05) and between the percentage of collagen and CDT (r = 0.67; p < 0.05).
In the H+E group was a positive correlation between LVW and PCor (r = 0.80, p < 0.05) and between CDT and LVW (r = 0.71, p < 0.05).
188
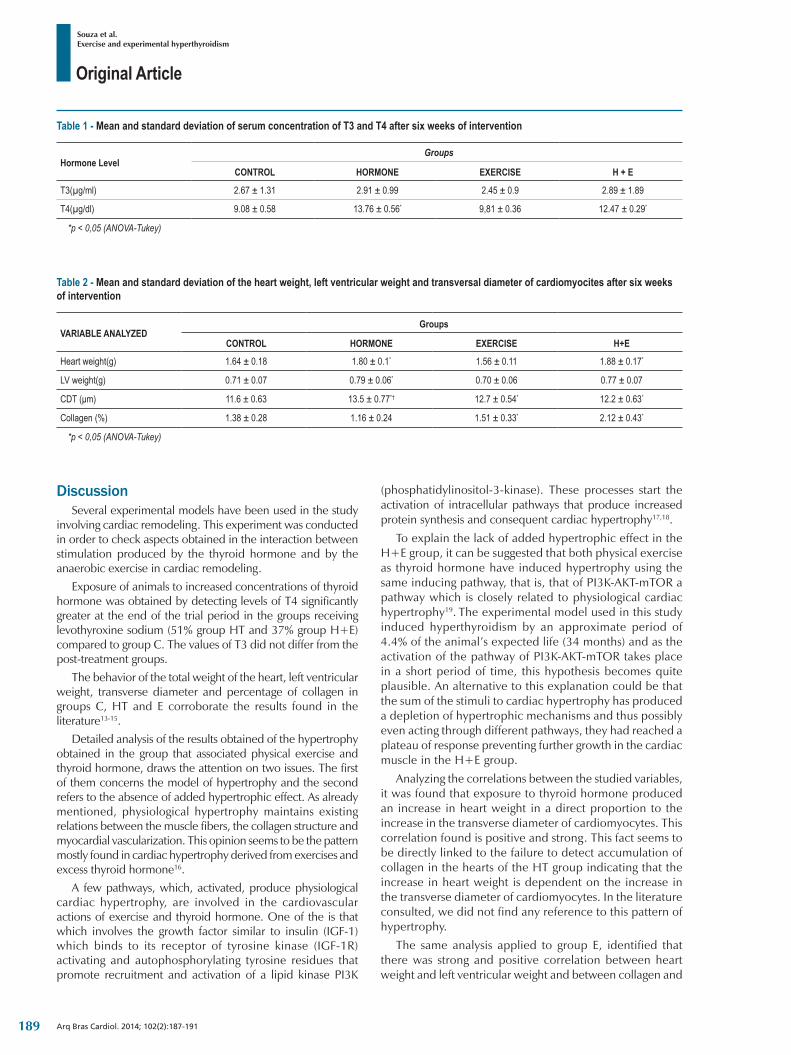
Original Article
Souza et al.Exercise and experimental hyperthyroidism
Arq Bras Cardiol. 2014; 102(2):187-191
Table 2 ‑ Mean and standard deviation of the heart weight, left ventricular weight and transversal diameter of cardiomyocites after six weeks of intervention
VARIABLE ANALYZEDGroups
CONTROL HORMONE EXERCISE H+E
Heart weight(g) 1.64 ± 0.18 1.80 ± 0.1* 1.56 ± 0.11 1.88 ± 0.17*
LV weight(g) 0.71 ± 0.07 0.79 ± 0.06* 0.70 ± 0.06 0.77 ± 0.07
CDT (μm) 11.6 ± 0.63 13.5 ± 0.77*† 12.7 ± 0.54* 12.2 ± 0.63*
Collagen (%) 1.38 ± 0.28 1.16 ± 0.24 1.51 ± 0.33* 2.12 ± 0.43*
*p < 0,05 (ANOVA-Tukey)
Table 1 ‑ Mean and standard deviation of serum concentration of T3 and T4 after six weeks of intervention
Hormone LevelGroups
CONTROL HORMONE EXERCISE H + E
T3(µg/ml) 2.67 ± 1.31 2.91 ± 0.99 2.45 ± 0.9 2.89 ± 1.89
T4(µg/dl) 9.08 ± 0.58 13.76 ± 0.56* 9,81 ± 0.36 12.47 ± 0.29*
*p < 0,05 (ANOVA-Tukey)
DiscussionSeveral experimental models have been used in the study
involving cardiac remodeling. This experiment was conducted in order to check aspects obtained in the interaction between stimulation produced by the thyroid hormone and by the anaerobic exercise in cardiac remodeling.
Exposure of animals to increased concentrations of thyroid hormone was obtained by detecting levels of T4 significantly greater at the end of the trial period in the groups receiving levothyroxine sodium (51% group HT and 37% group H+E) compared to group C. The values of T3 did not differ from the post-treatment groups.
The behavior of the total weight of the heart, left ventricular weight, transverse diameter and percentage of collagen in groups C, HT and E corroborate the results found in the literature13-15.
Detailed analysis of the results obtained of the hypertrophy obtained in the group that associated physical exercise and thyroid hormone, draws the attention on two issues. The first of them concerns the model of hypertrophy and the second refers to the absence of added hypertrophic effect. As already mentioned, physiological hypertrophy maintains existing relations between the muscle fibers, the collagen structure and myocardial vascularization. This opinion seems to be the pattern mostly found in cardiac hypertrophy derived from exercises and excess thyroid hormone16.
A few pathways, which, activated, produce physiological cardiac hypertrophy, are involved in the cardiovascular actions of exercise and thyroid hormone. One of the is that which involves the growth factor similar to insulin (IGF-1) which binds to its receptor of tyrosine kinase (IGF-1R) activating and autophosphorylating tyrosine residues that promote recruitment and activation of a lipid kinase PI3K
(phosphatidylinositol-3-kinase). These processes start the activation of intracellular pathways that produce increased protein synthesis and consequent cardiac hypertrophy17,18.
To explain the lack of added hypertrophic effect in the H+E group, it can be suggested that both physical exercise as thyroid hormone have induced hypertrophy using the same inducing pathway, that is, that of PI3K-AKT-mTOR a pathway which is closely related to physiological cardiac hypertrophy19. The experimental model used in this study induced hyperthyroidism by an approximate period of 4.4% of the animal’s expected life (34 months) and as the activation of the pathway of PI3K-AKT-mTOR takes place in a short period of time, this hypothesis becomes quite plausible. An alternative to this explanation could be that the sum of the stimuli to cardiac hypertrophy has produced a depletion of hypertrophic mechanisms and thus possibly even acting through different pathways, they had reached a plateau of response preventing further growth in the cardiac muscle in the H+E group.
Analyzing the correlations between the studied variables, it was found that exposure to thyroid hormone produced an increase in heart weight in a direct proportion to the increase in the transverse diameter of cardiomyocytes. This correlation found is positive and strong. This fact seems to be directly linked to the failure to detect accumulation of collagen in the hearts of the HT group indicating that the increase in heart weight is dependent on the increase in the transverse diameter of cardiomyocytes. In the literature consulted, we did not find any reference to this pattern of hypertrophy.
The same analysis applied to group E, identified that there was strong and positive correlation between heart weight and left ventricular weight and between collagen and
189

Original Article
Souza et al.Exercise and experimental hyperthyroidism
Arq Bras Cardiol. 2014; 102(2):187-191
1. Artur C, Guyton MD. Tratado de fisiologia médica. 9ª ed. Rio de Janeiro: Elsevier; 2009.
2. Roffi M, Cattaneo F, Topol EJ. Thyrotoxicosis and the cardiovascular system: subtle but serious effects. Cleve Clin J Med. 2003;70(1):57-63.
3. Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling – concepts and clinical implications: a consensus paper from an international forum on cardiac remodeling. Behalf of an International Forum on Cardiac Remodeling. J Am Coll Cardiol. 2000;35(3):569-82.
4. Vassalo DV, Lima EG. Contratilidade miocárdica: aspectos básicos e clínicos. São Paulo: BYK; 1993.
5. Evangelista FS, Brum PC, Krieger JE. Duration-controlled swimming exercise training induces cardiac hypertrophy in mice. Braz J Med Biol Res. 2003;36(12):1751-9.
6. Faggard RH. Impact of different sports and training on cardiac structure and function. Cardiol Clin. 1997; 15(3):397-412.
7. Klein I, Ojamaa K. Thyroid hormone and the cardiovascular system. N Engl J Med. 2001;344(7):501-9.
8. Dilmann W. Cardiac hypertrophy and thyroid hormone signaling. Heart Fail Rev. 2010;15(2):125-32.
9. Rogatto GP, Luciano E. Efeitos do treinamento físico intenso sobre o metabolismo de carboidratos. Rev bras ativ fis saúde. 2001;6(2):39-46.
10. Harri M, Kuusela P. Is swimming exercise or cold exposure for rats? Acta Physiol Scand. 1986;126(2):189-97.
11. Manchado FB, Gobatto CA, Contarteze RV, Papoti M, Mello MA. Máxima fase estável de lactato é ergometrodependente em modelo experimental utilizando ratos. Rev Bras Med Esporte. 2006;12(5):259-62.
12. Engelman MF, Guidugli Neto J, Andrade CH, Hernandez R, Goulart LB. Estudo morfométrico do fígado de ratos submetidos a doses supra-fisiológicas de tiroxina. Arq Bras Endocrinol Metab. 2001;45(2):173-9.
13. Olivetti G, Cigola E, Maestri R, Lagrasta C, Corradi D, Quaini F. Recent advances in cardiac hypertrophy. Cardiovasc Res. 2000;45(1):68-75.
14. Colan SD. Mechanics of left ventricular systolic and diastolic function in physiologic hypertrophy of the athlete’s heart. Cardiol Clin. 1997;15(3):355-72.
15. Shapiro LM. The morphologic consequences of systemic training. Cardiol Clin. 1997;15(3):373-9.
16. Ojamaa K. Signaling mechanisms in thyroid hormone-induced cardiac hypertrophy. Vasc Pharm. 2010;52(3-4):113-9.
17. Kim J, Wende AR, Sena S, Theobald HA, Soto J, Sloan C, et al. Insulin-like growth factor I receptor signaling is required for exercise-induced cardiac hypertrophy. Mol Endocrinol. 2008;22(11):2531-43.
18. Ikeda H, Shiojima I, Ozasa Y, Toshida M, Holzenberger M, Kahn CR, et al. Interaction of myocardial insulin receptor and IGF receptor signaling in exercise-induced cardiac hypertrophy. J Mol Cell Cardiol. 2009;47(5):664-75.
19. Dorn II GW. The fuzzy logic of physiological cardiac hypertrophy. Hypertension. 2007;49(5):962-970.
References
left ventricular weight. There was also a negative correlation between the transverse diameter of cardiomyocytes and left ventricular weight and between collagen and transverse diameter of cardiomyocytes.
The detected correlation between the weight of the heart and left ventricular weight restores the pattern obtained in group C and indicates that the increased collagen may be directly implicated in increased left ventricular weight. At the same time, the negative correlation between the transverse diameter of cardiomyocytes and left ventricular weight and the percentage of collagen and the transverse diameter of cardiomyocytes reinforce this hypothesis and seem to suggest that the participation of cardiomyocytes, although showing a transverse diameter of cardiomyocytes greater than that of group C, has a less important role on cardiac hypertrophy.
The association of exercise to the hormone maintained the positive correlation between left ventricular weight and heart weight and between the transverse diameter of cardiomyocytes and left ventricular weight, although no correlation has been found involving collagen. This result is interesting because the sum of the effects appears to reduce the accumulation of collagen, a fact which may have clinical relevance and needs to be further studied in future experimental models.
ConclusionThe association of thyroid hormone with high-intensity
exercise produced cardiac hypertrophy characterized
by increased heart weight and transverse diameter of cardiomyocytes without concomitant increase of the left ventricle.
This association led to a hypertrophic pattern not directly correlated to the degree of fibrosis.
Author contributionsConception and design of the research and Critical
revision of the manuscript for intellectual content: Souza FR, Resende ES; Acquisition of data, Statistical analysis and Obtaining funding: Souza FR; Analysis and interpretation of the data: Souza FR, Lopes L, Gonçalves A; Writing of the manuscript: Souza FR, Chagas R, Fidale T, Rodrigues P.
Potential Conflict of InterestNo potential conflict of interest relevant to this article
was reported. Sources of FundingThis study was funded by CAPES. Study AssociationThis article is part of the thesis of master submitted by
Fernanda Rodrigues de Souza from Universidade Federal de Uberlândia (UFU).
190

Original Article
Souza et al.Exercise and experimental hyperthyroidism
Arq Bras Cardiol. 2014; 102(2):187-191191

Review Article
Quality of Life and Congenital Heart Disease in Childhood and AdolescenceJuliana Bertoletti1, Giovana Caroline Marx2, Sérgio Pedro Hattge Júnior2, Lucia Campos Pellanda1,2
Instituto de Cardiologia/Fundação Universitária de Cardiologia - IC/FUC1, Porto Alegre, RS; Universidade Federal de Ciências da Saúde de Porto Alegre2, Porto Alegre, RS - Brazil
KeywordsQuality of life; heart disease; congenital abnormalities;
childhood; adolescence.Mailling Address: Lucia Campos Pellanda •Instituto de Cardiologia do Rio Grande do Sul / Fundação Universitária de Cardiologia e Universidade Federal de Ciências da Saúde de Porto Alegre, Av. Princesa Isabel, 370, 3º andar, Santana. Postal Code 99620-000, Porto Alegre, RS - BrazilE-mail: [email protected] received May 08, 2013; revised manuscript August 05, 2013; accepted September 26, 2013.
DOI: 10.5935/abc.20130244
AbstractAdvances in cardiac surgery techniques and early diagnosis
have enabled the increased survival of individuals with congenital heart disease. The investigation of the quality of life in children and adolescents with congenital heart disease provides complementary information to clinical data that can assist in decision making on the part of health professionals. Although many studies have been conducted to investigate the quality of life of children and adolescents with congenital heart disease, the results prove to be contradictory; while some studies show that congenital heart disease can impact the quality of life, others describe a better perception of quality of life among children and adolescents who suffer from the disease when compared with healthy control subjects. The purpose of this study is to review the literature on the assessment of health related quality of life in children and adolescents with congenital heart disease, in order to systematize the existing knowledge on this topic today. It is observed that research seeks to investigate aspects of personality in cardiac patients, their coping strategies used and perceived social support, aiming at better understanding the association of these variables with the level of quality of life in this population.
IntroductionAdvances in treatments and the effective possibilities
of control of chronic-degenerative and congenital diseases have resulted in longer life time to people afflicted by these diseases1. In relation to cardiac malformations, it is estimated that about 10 out of 1000 newborns alive are affected by some sort of congenital anomaly, being one-third of these with critical diagnoses requiring surgical intervention1,2. In the last decades, early diagnosis has contributed to the increase of incidence in the findings3, and the advance of surgical techniques has led to the increase in the number of heart disease children and adolescents.
In face of this context, it is important to consider the repercussions of physical, psychological and social order that accompany congenital heart disease (CHD) and that can bring losses to these patients’ quality of life. The Health related quality of life (HRQoL) initially investigated further in the adult population, has gained special attention in childhood and adolescence due to the impact that its injury can cause in long-term, in addition to the benefit that early interventions focusing on its improvement can provide, especially in chronic diseases.
The assessment of HRQoL in children and adolescents with heart disease has been used as an important health outcome, to identify groups and subgroups that are at risk, track health habits and to better understand the impact of different diagnoses of heart disease on the quality of life of this population. The objective of this study is to review the current literature on the evaluation of health related quality of life in childhood and adolescence, with emphasis on the patient with congenital heart disease.
MethodA search was conducted in Pubmed and Scielo databases
for articles published between 2000 and 2012. The following key-words were used: "quality of life", "congenital heart disease", "children", "adolescents". 350 articles were found, of which 58 were selected for this review according to the following selection criteria: cross-sectional studies, longitudinal and systematic reviews, whose methodological procedures were well described, as well as statistical analysis, studies using measurement instruments valid and recognized; studies performed with children and adolescents with significant sample size. Additionally, references were sought in books authored by specialists in the field of literature review articles with adequate theoretical quality for the discussion of the topic, in order to complement and deepen the analysis of the current literature.
Review results and discussion
Health related quality of life in children and adolescentsWhile the quality of life (QoL) in adults has been
investigated in the past decade, this study among children and adolescents is a recent area. The difficulty of defining and conceptualizing QoL becomes a constant challenge for researchers in this area, especially in the construction of valid and reliable instruments, including all its scales and considering the perception of the individual under development.
192

Review Article
Bertoletti et al.Quality of life in congenital heart diseases
Arq Bras Cardiol. 2014; 102(2):192-198
In general, the QoL assessment tools in childhood have little congruence in relation to the content covered, with different conceptions about normal childhood development in different age groups and the importance of family function and social context as factors necessary for their well being. The broad spectrum of contents and the variety of scales and items envisaged in the QoL instruments in childhood reflect the differences in their process of preparation, in the theoretical line used, in the target population and in the objectives of application of the instrument4,5.
Some areas of discussion of an ideal model of QoL in childhood and adolescence, as highlighted by Kuczynski4, suggest that it is important to assess the global sphere (related to society and its macro environment) and external sphere (related to socioeconomic conditions) on top of personal and interpersonal aspects as children need, overall, to develop themselves in adequate and health-promoting conditions. Reinforcing this idea, Matza et al.6 consider that in general children do not have the choice to significantly change an environmental problem, unlike adults, who have financial resources and adequate social support, for example, to leave a job or an unsatisfactory marriage.
Contextual factors, therefore, may have an influence in the long-term on social and psychological development of children, and it is important to consider variables such as family, peers, school and community when assessing their QoL. In the case of children with chronic disease, there are few attempts at developing methods and tools for assessment of HRQoL, and it still is uncommon concern in apprehending the perception and impact of the disease from the point of view of the patient, resulting in large discrepancies as to the response and clinical evolution4.
To Lawford and Eiser7, the child's ability to adapt to their experiences and how they interpret adverse experiences will have impact on their QoL. The reactions of each child to face adverse experience, such as dealing with the disease, show that there is a level of individual adjustment and coping styles that are related to their perception of QoL. The concept of resilience, understood as the process of positive adaptation of the individual in contexts of extreme adversity, has been used to explain individual differences found in children who show high levels of action in some domains of QoL despite facing adverse life conditions.
In a systematic review of instruments to assess the QoL for children and adolescents, Solans et al.5 have identified the existence of 30 generic and 64 specific-disease instruments, published between years 2001 and 2005. Samples of generic instruments for pediatric population are: “Pediatric Quality of Life Inventory (PedsQL)8”, “Autoquestionnaire de Qualité de Vie Enfant Imagé” (AUQUEI)9, “Child Health Questionnaire (CHQ)10 and Kidscreen11. The specific measures are tools capable of detecting the improvement or worsening of symptoms and functioning of the health condition under study, with higher sensitivity to measure changes to effects of the treatments of certain diseases12,13. In the pediatric population, health conditions that have a higher number of specific measuring instruments are asthma, cancer and epilepsy, and the countries that mostly develop this type of instrument are the United States, UK and Canada5.
Although the study of Solans et al. where most of the instruments present acceptable standards in relation to psychometric properties, few presented criterion validity analyses (n = 5), structure validity (n = 15) or sensitivity to change (n = 14). The challenge in accessing child perception is also revealed in the study, since 26% of the disease-specific instruments are destined exclusively to the parents as respondents (Proxy)5.
With regard to measures of HRQoL for children and adolescents, Matza et al.6 point out some methodological aspects that must be considered in the preparation of the instruments. According to the authors one must consider the minimum age at which children can answer questions about their quality of life as well as the appropriateness of the format of the instrument to the level of understanding of each age group. In addition, there is disagreement among researchers about the need to evaluate the agreement between the assessment of parents and that of children as respondents, especially when evaluating younger children who may not be able to respond on more subjective domains. Thus, before drawing a measure of HRQoL for children, it is essential for researchers to assess the adequacy of the tool to age, including vocabulary, instructions, question structure, content and response options.
In congenital heart disease, specific HRQoL measures have begun to emerge recently and are still in the process of being tested and validated in different cultural contexts. In the UK, the development of ConQol Index (CQI) occurred from a multicenter study involving 730 children from five pediatric cardiology centers, funded by the British Heart Foundation. It is an instrument to measure HRQoL for children with congenital heart disease at the age of 8 to 16 years old, and seeks to assess the impact of heart disease on daily life measured from the perspective of the child or adolescent. Two versions are available for different age groups: the first, for children 8-11 years old, it includes the scales, symptoms, activities and relationships, and second, for teens 12-16 years old, it adds a scale to the others on coping and control14.
In the United States, the project of creating the Pediatric Cardiac Quality of Life Inventory (PCQLI) aimed at the development of an inventory covering a wider age group - children 8-12 years old and adolescents aged 13 to 18 years old - including versions for patients and parents (Proxy), having the ability to discriminate the different types of congenital and acquired heart diseases. The results of the pilot study, conducted in three cardiac clinics with 655 pairs of parents and patients, showed content validity, good internal consistency and construct validity of the instrument, with a good correlation between the components that measure the impact of the disease and the psychosocial impact15.
In Brazil, Soares et al.16 analyzed the national scientific production on QoL of children and adolescents, finding 30 articles published between 1990 and 2008. The results showed predominance of quantitative approach research (70%) and a higher index of research with quality of life evaluation instruments related to health (66.7%) than generic instruments (28.6%). It was also observed a greater number of articles published in the field of Medicine
193

Review Article
Bertoletti et al.Quality of life in congenital heart diseases
Arq Bras Cardiol. 2014; 102(2):192-198
(40%), followed by Nursing (30%) and Psychology (26.6%). Regarding the assessment of QoL in chronic diseases, Brazil stood out in pioneering studies conducted by the Faculty of Medical Sciences, State University of Campinas (UNICAMP) on QoL and epilepsy, which served as a starting point for the advancement of discussions on the theme.
Although 50% of national publications found in the study by Soares et al.16 the QoL of children and adolescents from the perspective of their parents and caregivers, the authors concluded that the scientific community is looking to enhance the perception of children and adolescents as reporters of their experience, considering the particularities of this period of life in the application of adequate research methodologies. Despite all the difficulties encountered in developing tools for the pediatric population, it is important to remember, as pointed out by Kuczynski17, that "the individual under development can express himself, it is we who cannot (or are not willing) to understand him.”
Congenital heart diseases in childhood and adolescenceCardiac malformations are considered one of the most
frequent forms of congenital anomalies at birth. Studies performed in the Brazilian population evaluated the predominance of CHD in live newborns, identifying the ratio of 5.5:1000 live newborns between the years of 1889 and 1998 in the state of Paraná18, and 9.58:1000 newborns between the years of 1990 and 2003 in the state of Minas Gerais1. To Huber et al.3, early diagnosis and detection of cardiac malformations in the prenatal period have contributed to the increase of incidence in the findings, both in national and international studies.
In childhood, there is evidence that the presence of CHD can affect physical and ponderal development, motor, cognitive and neurological operation19,20, and there is even a higher incidence of academic difficulties, behavioral problems, speech delay, lack of attention and hyperactivity in patients with complex congenital heart disease21,22. In addition to such clinical evidence, the need for ongoing medical monitoring, use of medication and recurrent hospitalizations may affect self-esteem and self-image of this group of children and adolescents, resulting in delays in normal development tasks22. The maintenance of health in children with CHD still requires care from parents and medical staff with nutrition, immunization, winter disease prevention and prophylaxis of bacterial endocarditis, all these aspects vital to their long-term survival23.
Upon entering adolescence, patients with CHD face the challenge of autonomy in the face of parental overprotection, usually exercised during childhood. Furthermore, adolescence is a crucial consolidation phase of health healthy behavior, such as for instance, the adoption of good food practices and exercises, but also a period in which risk behavior is manifested for the first time, such as the use of drugs and alcohol and risk sexual practices24,25. Some studies highlight the importance of a transition program in assisting health22,26-28, with the objective to educate adolescents with CHD on their medical condition and guide them with regard to physical exercises29,30, sexuality31 and entrance into the labor market.
Some qualitative studies conducted with adolescents with CHD32,33, using semi-structured interview and in-depth techniques, pointed out some difficulties faced by these patients, such as: coping with the illness and physical limitations, social exclusion, discrimination and bullying, in addition to the challenge of normality, becoming independent, the uncertainty about the future and how to use coping strategies to develop self-esteem, among other dilemmas. Thus, health care to patients with congenital heart disease should include the care of their psychological and social needs as well as the physiological, as a means of improving their quality of life.
Although many cardiac patients acquire a stable health condition, some of them have residual defects and important sequelae in adulthood, even after numerous surgical corrections. CHDs are considered chronic conditions, due to the factors that accompany them in the long term and that interfere with the daily life of these patients, including uncertainty about the course of the disease, prognosis, signs and symptoms, and restrictions on physical activity34. The investigation of the quality of life in this population in all age groups, has gained increased attention as an important health outcome, not only related to symptoms and clinical conditions, but also in terms of their level of well-being and satisfaction with life as a whole.
Congenital Heart Diseases and Quality of LifeStudies conducted to evaluate the QoL of children and
adolescents with CHD have yielded inconclusive results, possibly due to a lack of conceptual and methodological rigor in research, according Moons et al.34. Methodological differences among the studies, such as outline, inclusion criteria, evaluation tools used, follow-up and outcome measures make it difficult to compare results.
However, one can ascertain that a large part of the studies performed is at a lower level of HRQoL among children and adolescents with CHD when compared to healthy control35-37. According the findings of a systematic review conducted by Dahan-Oliel, Majnemer and Mazer38, such results are related in part to the physical limitations - actual or perceived - in subjects with CHD, which can lead to unnecessary restrictions and overprotective behavior that possibly interfere in their perception over QoL.
Janiec et al.35 report that children and adolescents with mitral valve prolapse have a lower QoL than the healthy population only in the scale of physical well-being, although among the group with CHD the frequency and severity of clinical symptoms have a negative impact on other scales assessed. The study of Krol et al.36 found that children with CHD had worsening in motor functioning and autonomy compared to healthy children; however, the severity of the diagnosis was not associated with the level of QoL of the heart disease population.
In the study by Uzark et al.37, one in five children with CHD refers significant worsening in psychosocial functioning when compared to the control group, including those with mild or corrected heart disease; on the other hand, in the CHD group, children with more serious injuries presented
194

Review Article
Bertoletti et al.Quality of life in congenital heart diseases
Arq Bras Cardiol. 2014; 102(2):192-198
lower results only in physical function, and there is no relation between the disease severity and psychosocial functioning. These findings show that the association between severity of diagnosis and QoL has not yet been elucidated among children and adolescents with CHD, possibly due to the methodological differences mentioned above.
Studies by Landolt et al.39 and Spijkerboer et al.40 investigated the QoL of children and adolescents after cardiac surgery and/or invasive treatment by catheterization for CHD, respectively, using the same measuring instrument. Their results were similar, indicating worse motor cognitive, social and emotional functioning than healthy children. Multivariate analysis in the study Landolt et al.39 further disclosed that the duration of cardiopulmonary bypass, time of hospitalization, need for medication and adverse family relationships had a negative impact on QoL of the children, only in accordance with the evaluation of their parents and caregivers.
In the systematic review conducted by Latal et al.41 studies published between 1990 and 2008 on psychological adjustment and QoL in children and adolescents submitted to cardiac surgery were included in order to check the current knowledge on the outcomes in this population. Although there is great variability between studies, the results show that QoL is impaired in some children, especially those with more complex CHDs. The results also show that there are differences in the perception of parents and children regarding the psychological adjustment: while children are evaluated positively in this aspect, parents in general consider that psychological adjustment of their children has impairments, relating them mainly to the severity of the CHD and developmental delays.
Other studies corroborate and expand these findings, indicating that the QoL of parents and caregivers of children with CHD can also be affected due to the impact of the diagnosis on the level of stress and adjustment of these families42-45. Current literature on QoL of children with special health care needs indicates important factors of positive adaptation to motivation and attitudes of the child as well as the resources and social support available to the family. Such factors are considered more important predictors for a good QoL than the complexity of the medical condition, so strategies that strengthen family welfare and building of social support networks should be valued and offered in health care services45.
Contrary to studies that showed impairment of QoL in children and adolescents with CHD, some authors found surprising results. Teixeira et al.46 evaluated adolescents and young adults with CHD and their findings indicated a level of QoL higher than the general population, especially in the environmental and social relationship scale. Culbert et al.47 studies evaluated the QoL of 306 children diagnosed with Transposition of the Great Arteries (TGA) using the Child Health Questionnaire, and found significantly higher results between the group with CHD when compared to the general population, with the exception of self-esteem scale. Other studies found a small difference between the QL of congenital heart disease patients, when compared to population standards48-50.
Silva et al.51 investigated the variables that would have a negative impact on the Quality of Live in adolescents and young adults with CHD, applying the WHOQoL-BREF tool, and found a better perception of QoL in this group when compared to the general population. The presence of cyanosis was not associated with worsening of QoL; however, the number of surgical procedures and moderate to severe residual lesions had a significant impact on it. It was also highlighted, among the findings, the importance of social support as a variable related to increased resilience among heart disease patients, which consequently promotes better adaptation to the disease.
But how to explain these findings? Surprised by research that found a higher QoL in CHDs, Moons et al.52 introduced the term "sense of coherence" as a hypothesis to understand why patients that grow with chronic diseases may be satisfied with their life. The term Sense of Coherence (SOC) was developed by Antonovsky in 1987 to explain why some people get sick when they are under stress, while others remain healthy. Contrary to the pathogenic model with focus on disease, it was based on the premise that the individual should focus positively on his resources and capabilities to maintain his health and well-being.
So, the term Sense of Coherence can be defined as an expression of the world view of the individual, a global orientation based on a dynamic and enduring feeling of confidence in themselves and in their environment. It consists of three components: 1) understandability, or how much the internal and external stimuli received during childhood are structured, predictable and explicable; 2) management, which refers to the perception of the resources available to deal with stressful situations, such as for instance living with heart disease and 3) meaning, or the ability of the individual to believe that his life has meaning, find motivation and assume the control over his life52.
In a longitudinal study performed by Apers et al.53, with 429 adolescents with congenital heart disease, the Sense of Coherence showed up as a positive predictor of all domains of perceived general health (physical, emotional, social and school functioning), also positively associated with specific aspects of the disease, such as symptoms, physical appearance and cognitive problems. In another study on the individual and contextual determinants of quality of life in adolescents with heart disease, Luyckx et al.54 concluded that the perceived level of health, the Sense of Coherence and parental support correlated positively with quality of life over time. These results confirm the importance of considering the biopsychosocial functioning of the adolescent with heart disease in the evaluation of their QoL, and the Sense of Coherence emerges as a valuable resource to be developed.
Studies performed by Luyckx et al.55-57 have advanced in the investigation of QoL as a variable of the outcome of other predictors, such as perceived parental styles55 and the process of formation of identity of the adolescents with CDH56, to explain their functioning and describe the main variables that interact in their perception of QoL.
With regard to parental styles, no significant differences were found between adolescents with heart disease and
195

Review Article
Bertoletti et al.Quality of life in congenital heart diseases
Arq Bras Cardiol. 2014; 102(2):192-198
1. Amorim LF, Pires CA, Lana AM, Campos AS, Aguiar RA, Tibúrcio JD, et al. Presentation of congenital heart disease diagnosed at birth: analysis of 29,770 newborn infants. J Pediatr (Rio J). 2008;84(1):83-90.
2. Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39(12):1890-900.
3. Huber J, Peres VC, Santos TJ, Beltrão Lda F, Baumont AC, Cañedo AD, et al. Congenital heart diseases in a reference service: clinical evolution and associated illnesses. Arq Bras Cardiol. 2010; 94(3):313-8, 333-8.
4. Kuczynski E, Assumpção Jr F. Qualidade de vida na infância e na adolescência: orientações para pediatras e profissionais da saúde mental. Porto Alegre: Artmed; 2010.
5. Solans M, Pane S, Estrada MD, Serra-Sutton V, Berra S, Herdman M, et al. Health-related quality of life measurement in children and adolescents: a systematic review of generic and disease-specific instruments. Value Health. 2008;11(4):742-64.
6. Matza LS, Swensen AR, Flood EM, Secnik K, Leidy NK. Assessment of health-related quality of life in children: a review of conceptual, methodological, and regulatory issues. Value Health. 2004;7(1):79-92.
7. Lawford J, Eiser C. Exploring links between the concepts of quality of life and resilience. Pediatr Rehabil. 2001;4(4):209-16.
8. Klatchoian DA, Len CA, Terreri MT, Silva M, Itamoto C, Ciconelli RM, et al. Qualidade de vida de crianças e adolescentes de São Paulo: confiabilidade e validade da versão brasileira do questionário genérico Pediatric Quality of Life InventoryTM versão 4.0. J Pediatr (Rio J). 2008;84(4):308-15.
9. Assumpção FB Jr, Kuczynski E, Sprovieri MH, Aranha EM. [Quality of life evaluation scale (AUQEI--Autoquestionnaire Qualité de Vie Enfant Imagé): validity and reliability of a quality of life scale for children from 4 to 12 years-old]. Arq Neuro-Psiquiatr. 2000;58(1):119-27.
10. Machado CS, Ruperto N, Silva CH, Ferriani VP, Roscoe I, Campos LM, et al; Rheumatology International Trials Organisation. The Brazilian version of the Childhood Health Assessment Questionnaire (CHAQ) and the Child Health Questionnaire (CHQ). Clin Exp Rheumatol. 2001;19(4 Suppl 23):S25-9.
11. Ravens-Sieberer U, Gosch A, Rajmil L, Erhart M, Bruil J, Duer W, et al; Kidscreen Group E. KIDSCREEN-52 quality-of-life measure for children and adolescents. Expert Rev Pharmacoecon Outcomes Res. 2005;5(3):353-64.
12. Minayo MC, Hartz ZM, Buss PM. Quality of life and health: a necessary debate. Ciênc saúde coletiva. 2000;5(1):7-18.
13. Prebianchi HB. Medidas de qual idade de vida para cr ianças: aspectos conceituais e metodológicos. Psicologia: Teoria e Prática. 2003;5(1):57-69.
14. Birks Y, Macran S, Lewin B. The ConQol Questionnaire – a disease-specific measure of health-related quality of life for children with congenital heart conditions. A brief user’s guide. New York: Department of Health Sciences, University of York; 2004.
15. Marino BS, Shera D, Wernovsky G, Tomlinson RS, Aguirre A, Gallagher M, et al. The development of the pediatric cardiac quality of life inventory: a quality of life measure for children and adolescents with heart disease. Qual Life Res. 2008;17(4):613-26.
References
the control group. The democratic style obtained better results among adolescents with heart disease, while the controlling style showed the worst among the evaluated outcomes (depressive symptoms, loneliness, quality of life, health status, and substance abuse)55. The process of identity formation in adolescents with heart disease proved to be similar to the one of control subjects, in a standard within average. Individuals with a strong sense of identity presented better results in terms of quality of life and psychosocial functioning, while those with a diffuse sense of identity had higher scores on depressive symptoms and loneliness, and lower in quality of life56.
It is possible that children with chronic diseases, which include children with cardiac disease, are challenged to develop a Sense of Coherence earlier than healthy children, by experiences that derive from the disease and require a great capacity for adaptation. Growing with CHD requires attention to medical treatment and often living with some restrictions on activities that are part of any child's life. Perhaps because they do not know a different reality these children acquire a greater sense of appreciation for life and expectations consistent with their capabilities and limitations, which will influence their perception of QoL in the course of their development.
ConclusionThe number of studies on quality of life in children and
adolescents with congenital heart disease has increased in recent years due to increased survival in this population.
Studies show conflicting results, and currently, there is a tendency to investigate factors such as parental styles, social support and coping strategies to better understand the quality of life in these patients. All of these variables that interact in the perception of quality of life are difficult to grasp by a single measuring instrument.
Author contributionsConception and design of the research and Writing of the
manuscript: Bertoletti J, Pellanda LC; Acquisition of data, Analysis and interpretation of the data, Statistical analysis and Critical revision of the manuscript for intellectual content: Bertoletti J, Marx GC, Hattge Jr SP, Pellanda LC; Obtaining funding: Pellanda LC.
Potential Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Sources of Funding
There were no external funding sources for this study.
Study Association
This article is part of the thesis of master submitted by Juliana Bertoletti from Instituto de Cardiologia/Fundação Universitária de Cardiologia.
196

Review Article
Bertoletti et al.Quality of life in congenital heart diseases
Arq Bras Cardiol. 2014; 102(2):192-198
16. Soares AH, Martins AJ, Lopes MC, Britto JA, Oliveira CQ, Moreira MC. Quality of life of children and adolescents: a bibliographical review. Ciênc saúde coletiva. 2011;16(7):3197-206.
17. Kuczynski E. Avaliação da qualidade de vida em crianças e adolescentes sadios e portadores de doenças crônicas e/ou incapacitantes. [Tese]. São Paulo: Universidade de São Paulo; 2002.
18. Guitti JC. Epidemiological characteristics of congenital heart diseases in Londrina, Paraná south Brazil. Arq Bras Cardiol. 2000;74(5):400-4.
19. Marino BS, Lipkin PH, Newburger JW, Peacock G, Gerdes M, Gaynor JW, et al; American Heart Association Congenital Heart Defects Committee, Council on Cardiovascular Disease in the Young, Council on Cardiovascular Nursing , and Stroke Council. Neurodevelopmental Outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation. 2012;126(9):1143-72.
20. Wernovsky G. Current insights regarding neurological and developmental abnormalities in children and young adults with complex congenital cardiac disease. Cardiol Young. 2006;16 Suppl 1:92-104.
21. Shillingford AJ, Glanzman MM, Ittenbach RF, Clancy RR, Gaynor JW, Wernovsky G. Inattention, hyperactivity, and school performance in a population of school-age children with complex congenital heart disease. Pediatrics. 2008;121(4):e759-67.
22. Sable C, Foster E, Uzark K, Bjornsen K, Canobbio MM, Connolly HM, et al; American Heart Association Congenital Heart Defects Committee of the Council on Cardiovascular Disease in the Young, Council on Cardiovascular Nursing, Council on Clinical Cardiology, and Council on Peripheral Vascular Disease. Best practices in managing transition to adulthood for adolescents with congenital heart disease: the transition process and medical and psychosocial issues: a scientific statement from the American Heart Association. Circulation. 2011;123:1454-1485.
23. Woodward CS. Keeping children with congenital heart disease healthy. J Pediatr Health Care. 2011;25(6):373-8.
24. Williams PG, Holmbeck GN, Greenley RN. Adolescent health psychology. J Consult Clin Psychol. 2002;70(3):828-42.
25. Chen CW, Chen YC, Chen MY, Wang JK, Su WJ, Wang HL. Health-promoting behavior of adolescents with congenital heart disease. J Adolesc Health. 2007;41(6):602-9.
26. Van Deyk K, Pelgrims E, Troost E, Goossens E, Budts W, Gewillig M, et al. Adolescents’ understanding of their congenital heart disease on transfer to adult-focused care. Am J Cardiol. 2010;106(12):1803-7.
27. Kovacs AH, Verstappen A. The whole adult congenital heart disease patient. Prog Cardiovasc Dis. 2011;53(4):247-53.
28. Wilson DG. Congenital heart disease in teenagers. Paediatr Child Health. 2011;21(1):13-8.
29. Dal Bianco L, Russo G, Bagato F, Resta R, Daliento L. Physical exercise in young patients with congenital heart disease. Minerva Cardioangiol. 2011;59(6):555-67.
30. Moola F, Fusco C, Kirsh JA. The perceptions of caregivers toward physical activity and health in youth with congenital heart disease. Qual Health Res. 2011;21(2):278-91.
31. Reid GJ, Siu SC, McCrindle BW, Irvine MJ, Webb GD. Sexual behavior and reproductive concerns among adolescents and young adults with congenital heart disease. Int J Cardiol. 2008;125(3):332-8.
32. McMurray RL, Parsons JM, Quirk J, Veldtman GR, Lewin RJ, Sloper P. A life less ordinary: growing up and coping with congenital heart disease. Coron Health Care. 2001;5(1):51-7.
33. Lee S, Kim SS. [The life of adolescent patients with complex congenital heart disease]. J Korean Acad Nurs. 2010;40(3):411-22.
34. Moons P, De Geest S, Budts W. Comprehensive care for adults with congenital heart disease: expanding roles for nurses. Eur J Cardiovasc Nurs. 2002;1(1):23-8.
35. Janiec I, Werner B, Sieminska J, Ravens-Sieberer U. Quality of life of children with mitral valve prolapse. Qual Life Res. 2011;20(4):537-41.
36. Krol Y, Grootenhuis MA, Destrée-Vonk A, Lubbers LJ, Koopman HM, Last BF. Health related quality of life in children with congenital heart disease. Psychol Health. 2003;18(2):251-60.
37. Uzark K, Jones K, Slusher J, Limbers CA, Burwinkle TM, Varni JW. Quality of life in children with heart disease as perceived by children and parents. Pediatrics. 2008;121(5):e1060-7.
38. Dahan-Oliel N, Majnemer A, Mazer B. Quality of life of adolescents and young adults born at high risk. Phys Occup Ther Pediatr. 2011;31(4):362-89.
39. Landolt MA, Valsangiacomo Buechel ER, Latal B. Health-related quality of life in children and adolescents after open-heart surgery. J Pediatr. 2008;152(3):349-55.
40. Spijkerboer AW, Utens EM, De Koning WB, Bogers AJ, Helbing WA, Verhulst FC. Health-related quality of life in children and adolescents after invasive treatment for congenital heart disease. Qual Life Res. 2006;15(4):663-73.
41. Latal B, Helfricht S, Fischer JE, Bauersfeld U, Landolt MA. Psychological adjustment and quality of life in children and adolescents following open-heart surgery for congenital heart disease: a systematic review. BMC Pediatr. 2009;9:6.
42. Goldbeck L, Melches J. Quality of life in families of children with congenital heart disease. Qual Life Res. 2005;14(8):1915-24.
43. Arafa MA, Zaher SR, El-Dowaty AA, Moneeb DE. Quality of life among parents of children with heart disease. Health Qual Life Outcomes. 2008;6:91.
44. Montalvo Prieto A, Romero Massa E, Flórez Torres IE. Quality of life of caregivers of children with cardiopathy in Cartagena, Colombia. Investigación y Educación en Enfermería. 2011;29(1):9-18.
45. Majnemer A, Limperopoulos C, Shevell M, Rohlicek C, Rosenblatt B, Tchervenkov C. Health and well-being of children with congenital cardiac malformations, and their families, following open-heart surgery. Cardiol Young. 2006;16(2):157-64.
46. Teixeira FM, Coelho RM, Proenca C, Silva AM, Vieira D, Vaz C, et al. Quality of life experienced by adolescents and young adults with congenital heart disease. Pediatr Cardiol. 2011;32(8):1132-8.
47. Culbert EL, Ashburn DA, Cullen-Dean G, Joseph JA, Williams WG, Blackstone EH, et al; Congenital Heart Surgeons Society. Quality of life of children after repair of transposition of the great arteries. Circulation. 2003;108(7):857-62.
48. Laane KM, Meberg A, Otterstad JE, Froland G, Sorland S, Lindstrom B, et al. Quality of life in children with congenital heart defects. Acta Paediatrica. 1997;85(9):975-80.
49. Dunbar-Masterson C, Wypij D, Bellinger DC, Rappaport LA, Baker AL, Jonas RA, et al. General health status of children with D-transposition of the great arteries after the arterial switch operation. Circulation. 2001;104(12 Suppl 1):I138-42.
50. Kwon EN, Mussatto K, Simpson PM, Brosig C, Nugent M, Samyn MM. Children and adolescents with repaired tetralogy of fallot report quality of life similar to healthy peers. Congenit Heart Dis. 2011;6(1):18-27.
51. Silva AM, Vaz C, Areias ME, Vieira D, Proença C, Viana V, et al. Quality of life of patients with congenital heart diseases. Cardiol Young. 2011;21(6):670-6.
52. Moons P, Norekvål T. Is sense of coherence a pathway for improving the quality of life of patients who grow up with chronic diseases? A hypothesis. Eur J Cardiovasc Nurs. 2006;5(1):16-20.
197

Review Article
Bertoletti et al.Quality of life in congenital heart diseases
Arq Bras Cardiol. 2014; 102(2):192-198
53. Apers S, Luyckx K, Rassart J, Goossens E, Budts W, Moons P. Sense of coherence is a predictor of perceived health in adolescents with congenital heart disease: a cross-lagged prospective study. Int J Nurs Stud. 2013;50(6):776-85.
54. Luyckx K, Missotten L, Goossens E, Moons P; i-DETACH Investigators. Individual and contextual determinants of quality of life in adolescents with congenital heart disease. J Adolesc Health. 2012;51(2):122-8.
55. Luyckx K, Goossens E, Missotten L, Moons P; i-DETACH Investigators. Adolescents with congenital heart disease: the importance of perceived parenting for psychosocial and health outcomes. J Dev Behav Pediatr. 2011;32(9):651-9.
56. Luyckx K, Goossens E, Van Damme C, Moons P; i-DETACH Investigators. Identity formation in adolescents with congenital cardiac disease: a forgotten issue in the transition to adulthood. Cardiol Young. 2011;21(4):411-20.
57. Luyckx K, Goossens E, Rassart J, Apers S, Vanhalst J, Moons P. Parental support, internalizing symptoms, perceived health status, and quality of life in adolescents with congenital heart disease: influences and reciprocal effects. J Behav Med. 2012 Nov. [Epub ahead of print].
198

Letter to the Editor
Chronotropic Incompetence in Diabetic Elderly on EchocardiographyEduardo Maffini da Rosa, Roberta Casanova Wilhelms, Rodrigo Borges BrandãoUniversidade de Caxias do Sul, Caxias do Sul, RS - Brazil
Mailing Address: Roberta Casanova Wilhelms •Rua Humberto de Campos, 1.113, Cristo Redentor. Postal Code 95084-440, Caxias do Sul, RS - BrazilE-mail: [email protected], [email protected] Manuscript received July 24, 2013; revised manuscript July 29, 2013; accepted September 17, 2013.
KeywordsAgeing; Diabetes Mell i tus; Stress Mechanical;
Echocardiography, Heart Rate.
1. Santana JS, Sá Neto AA, Melo EV, Santana NO, Barreto AT, et al. Prognóstico da incompetência cronotrópica em idosos diabéticos à ecocardiografia sob estresse físico. Arq Bras Cardiol. 2013;100(5):429-43.
2. Linhares RR, Gil MA, Ferreira LD, Monaco CG. Ecocardiografia sob estresse com dobutamina: revisão. Rev Bras Ecocardiogr Imagem Cardiovasc. 2012;25(1):28-35
3. Bogaz FA, Saroute AN, Tsutsui, JM, Kowatsch I, Neto F, Francisco M, et al. Vasoespasmo coronariano induzido pela ecocardiografia sob estresse pela dobutamina-atropina. Arq Bras Cardiol. 2006;87(6):e250-3.
References
ReplyOur group has experience with chronotropic incompetence
(CI) by using physical stress echocardiography as the diagnostic method; according to already performed cohorts, CI has shown prognostic value. That is the preferred method for individuals with preserved physical capacity.
Despite the well-known clinical implications, the underlying mechanism of CI has not been well clarified, autonomic dysfunction being the most frequently found hypothesis in the studies. The use of dobutamine is known to involve an autonomic system participant, the myocardial beta 1 adrenergic receptor, and is more restrictive than physical effort, which involves all the complexity of the system.
For practical purpose, most studies define CI as the incapacity to reach 80% of heart rate (HR) reserve according to the formula: HR reserve = (peak HR – resting HR) / (maximum HR – resting HR) x 100.
It has been suggested that the definition of CI should be assessed when the diagnostic method uses positive inotropic drugs to induce HR increase. It is necessary to better understand which practical concept of CI applies to the pharmacological stress echocardiography method to study the prognosis of those who have chronotropic incompetence according to that method.
The prognostic value of CI probably does not depend on the method used; however, the diagnosis of patients with CI should be well established.
Sincerely,Juliana Silva Santana
Antônio Carlos Sobral SousaJoselina Luzia Menezes Oliveira
Enaldo Vieira de Melo
DOI: 10.5935/abc.20140007
Dear editor,We congratulate the authors of the article on the prognosis
of chronotropic incompetence in diabetic elderly undergoing physical stress echocardiography, published in the Arq Bras Cardiol. 2013;100(5):429-431.
When chronotropic deficit is observed on pharmacological stress echocardiography, a relationship is observed with
neither prognosis nor prevalence of coronary artery disease, but with sinus node disorders, extrasystoles or dysautonomia, which might be due to dobutamine effects2,3. We would like to know whether, in those authors’ opinion, the chronotropic deficit can play any prognostic role in pharmacological stress echocardiography.
199

Letter to the Editor
Trastuzumab Cardiotoxicity in Patients with Breast CancerAguinaldo Figueiredo Freitas Jr. e Salvador RassiDepartamento de Cardiologia, Faculdade de Medicina da Universidade Federal de Goias, Goiânia, GO - Brazil
Mailing Address: Aguinaldo Figueiredo Freitas Jr. •Rua T-51, 964, ap. 1902, Bueno – Postal Code 74215-210, Goiânia, GO, BrazilE-mail: [email protected], [email protected] received August 10, 2013; revised manuscript October 04, 2013; accepted October 04, 2013.
KeywordsImmunosupressive Agents; Breast Neoplasms / adverse
effects; Antineoplstic Agents / adverse effects; Heart Failure; Ventricular Dysfunction.
1. Dores H, Abecasis J, Correia MJ, Gandara F, Fonseca C, Azevedo J, et al. Detecção de cardiotoxicidade subclínica induzida por trastuzumabe em portadoras de câncer de mama. Arq Bras Cardiol. 2013;100(4):328-32.
2. Curigliano G, Cardinale D, Suter T, Plataniotis G, de Azambuja E, Sandri MT, et al. Cardiovascular toxicity induced by chemotherapy, targeted agents and radiotherapy: ESMO clinical practice guidelines. Ann Oncol. 2012;23 Suppl 7:vii155-66.
3. Bowles EJA, Wellman R, Feigelson HS, Onitilo AA, Freedman AN, Delate T, et al. Risk of heart failure in breast cancer patients after anthracycline and trastuzumab treatment: a retrospective cohort study. J Natl Cancer Inst. 2012;104(17):1293-305.
4. Kalil Filho R, Hajjar LA, Bacal F, Hoff PM, Diz M del P, Galas FR, et al. I Diretriz Brasileira de cardio-oncologia da Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2011;96(2 supl.1):1-52.
References
DOI: 10.5935/abc.20140008
Dear Editor,
We read the article “Detection of Subclinical Trastuzumab-Induced Cardiotoxicity in Patients with Breast Cancer”1. Cardio-oncology is a current challenge for cardiologists, due to the high prevalence of cardiovascular toxicity secondary to chemotherapy agents, in addition to the need to determine effective measures to reduce the incidence of that complication2-4.
The above-cited article is extremely relevant and we would like to congratulate its authors. Its title and objective lead us immediately to believe that a method capable of early detecting subclinical cardiotoxicity (defined as a reduction in
ventricular ejection fraction) would be described. However, we could not understand how the authors assumed that the change in diastolic function found preceded systolic dysfunction, because none of the patients studied showed a significant reduction in ventricular ejection fraction in the three-month follow-up. We would like to ask the authors if they attribute the lack of ejection fraction reduction to the short follow-up, to the lack of previous cardiac changes (coronary artery disease, cerebral vascular accident or heart failure), or to the fact that the prevalence of comorbidities (arterial hypertension and diabetes) in the population studied was lower than that reported in the large studies.
Thank you and congratulations for your article.
200

Anatomopathological Session
Case 1/2014 - Syncope Due to Cardiogenic Shock in a 25-year-old Male PatientTiago Rodrigues Politi and Paulo GutierrezInstituto do Coração, Hospital das Clínicas, Faculdade de Medicina, Universidade de São Paulo - USP, São Paulo, SP - Brazil
Mailing Address: Vera Demarchi Aiello •Avenida Dr. Enéas de Carvalho Aguiar, 44, subsolo, bloco I, Cerqueira César. Postal Code 05403-000, São Paulo, SP – BrazilE-mail: [email protected], [email protected]
KeywordsSyncope; Shock, Cardiogenic; Aortic Aneurysm; Aneurysm,
Dissecting.
Section Editor: Alfredo José Mansur ([email protected])
Associated Editors: Desidério Favarato ([email protected])
Vera Demarchi Aiello ([email protected])
DOI: 10.5935/abc.20140020
The patient was a twenty-five-year-old male individual, who suddenly started feeling faint and malaise at fainted on February 18th, 2009. He was taken to the medical emergency service of the local hospital by family members approximately one hour after symptom onset. The patient was previously healthy and asymptomatic. There was no history of hypertension, diabetes, dyslipidemia, heart disease or use of illegal drugs.
At physical examination the patient had lowered level of consciousness, 60/50 mmHg blood pressure, heart rate (HR) of 150 beats per minute (bpm), no palpable pulses in the upper limbs and symmetrical pulses in the lower limbs.
Several tests were performed on the day of hospital admission. The electrocardiogram (ECG) showed sinus tachycardia, with a HR of 150 bpm, PR interval of 120 ms, QRS duration of 80 ms (Figure 1). Chest radiography showed cardiomegaly, mediastinal enlargement and clear pulmonary fields (Figure 2). The transthoracic echocardiography showed dissection of the ascending aorta with cardiac tamponade (compression of the right atrium).
Laboratory assessment showed hemoglobin of 14.2 g/dL, hematocrit 42.9%, leukocytes 12,400/mm³ (78% neutrophils, 2% eosinophils, 14% lymphocytes and 6% monocytes), platelets 202.000/mm³, urea 30.5 mg/dL, creatinine 1.2 mg/dL, potassium 3.8 mEq / L, sodium 146 mEq/L, glucose 132 mg/dL, alkaline phosphatase 46 IU/L, gamma-glutamyl transpeptidase 37 IU/L, aspartate aminotransferase 21 IU/L and alanine aminotransferase 34 IU/L.
Due to the patient’s clinical instability, tracheal intubation for ventilatory support was required, as well as volemic expansion with 0.9% saline solution and a vasoactive drug (norepinephrine) to elevate blood pressure.
After volume expansion and noradrenaline administration, blood pressure increased to 126/40 mmHg, with a heart rate of 135 bpm, and due to the severity of the clinical picture, his transfer to the Emergency Department of Instituto do Coração (InCor) was requested in the same evening.
Upon admission to InCor on February 19, 2009, the patient was sedated, assisted by mechanical ventilation and with pallor (++/6). The cardiorespiratory examination, showed a heart rate of 110 bpm, blood pressure 110/70 mmHg, normal pulmonary auscultation; however, cardiac auscultation showed muffled heart sounds (no accessory heart sounds, murmurs or pericardial friction rubs were identified). Abdominal examination was normal and there were no arterial pulses in the upper limbs, with bilateral cyanosis in the fingers. The arterial pulses were palpable and symmetrical in the lower limbs.
The laboratory assessment performed on February 19, 2009 showed: hemoglobin of 17.1 g / dL, hematocrit 54%, 26,900/mm ³ leukocytes (1% rods, 84% segmented neutrophils, 7% lymphocytes and 8% monocytes), 107.000/mm ³ platelets, urea 39 mg/dL, creatinine 2.6 mg/dL (glomerular filtration, 32 mL/min/1.73m²), sodium 134 mEq/L, potassium 4.9 mEq/L, lactate 33 mg/dL, prothrombin time (International Normalized Index, INR) of 3.8 and activated partial thromboplastin time ratio of 1.53. Arterial blood gas analysis showed a pH of 7.22, partial pressure of Carbon Dioxide (pCO2) of 32.9 mmHg, partial pressure of oxygen (pO2) of 206 mm Hg, O2 saturation of 99.9%, bicarbonate 13 mEq/L and excess of base (-) of 13.7 mEq/L.
The ECG was suggestive of electrical alternans (Figure3).Transesophageal echocardiography showed left ventricular
hypertrophy with normal systolic function and a 62-mm aneurysmal dilation in the ascending aorta with the dissection lamina starting 1.7 cm from the valve. The dissection extended up after the aortic arch and affected the innominate artery, the left common carotid artery and the left subclavian artery. Severe aortic valve regurgitation and large pericardial effusion were also observed, with signs of right ventricular restriction to diastolic inflow.
Surgical treatment of the aortic dissection was indicated; however, the patient had bradycardia in the perioperative period, followed by asystole unresponsive to resuscitation maneuvers and died.
Clinical aspectsThis is a case of a male patient, 25 years of age
with no previously described clinical history that sought medical attention complaining of malaise and feeling faint. The clinical picture had started 1 hour before he sought the local hospital emergency room. The patient clinical evolution was dramatic, presenting at the examination as shock, initially of undetermined etiology, going to aortic dissection and cardiac tamponade, and culminating in death within hours of symptom onset, before any surgical intervention. Acute dissection of the ascending aorta was then identified, with rapid and catastrophic clinical deterioration, a determining factor for the diagnosis to be attained as early as possible, as well as an early and accurate intervention.
e11
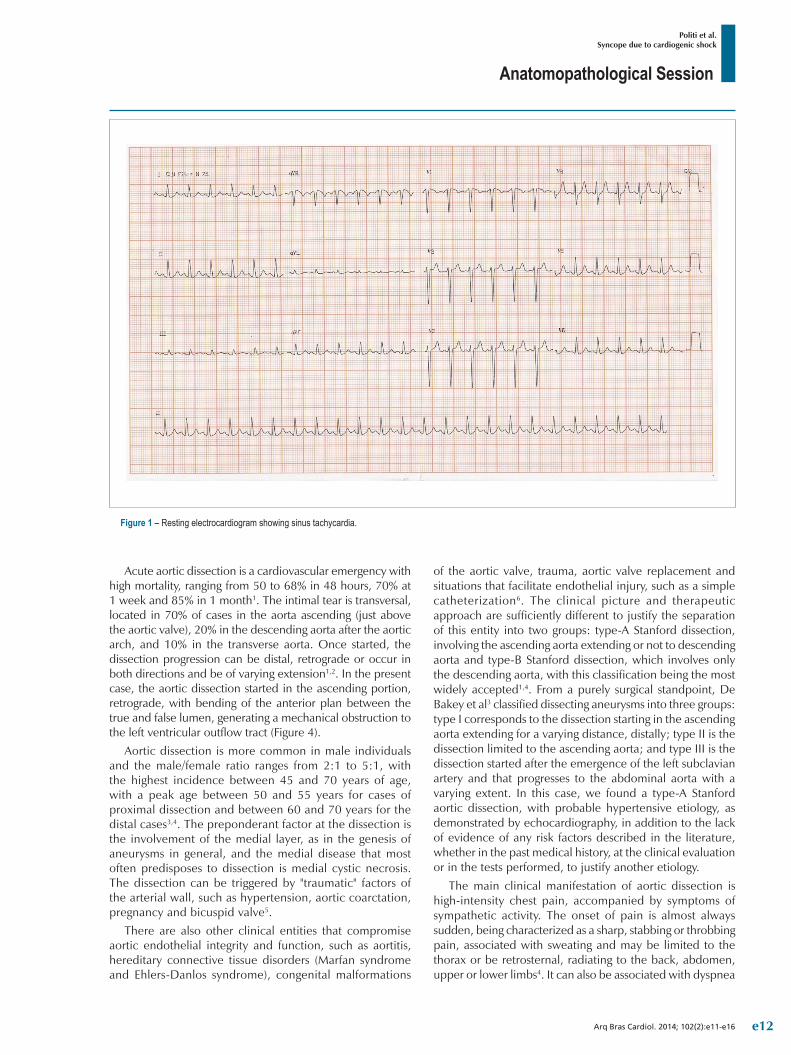
Anatomopathological Session
Politi et al.Syncope due to cardiogenic shock
Arq Bras Cardiol. 2014; 102(2):e11-e16
Figure 1 – Resting electrocardiogram showing sinus tachycardia.
Acute aortic dissection is a cardiovascular emergency with high mortality, ranging from 50 to 68% in 48 hours, 70% at 1 week and 85% in 1 month1. The intimal tear is transversal, located in 70% of cases in the aorta ascending (just above the aortic valve), 20% in the descending aorta after the aortic arch, and 10% in the transverse aorta. Once started, the dissection progression can be distal, retrograde or occur in both directions and be of varying extension1,2. In the present case, the aortic dissection started in the ascending portion, retrograde, with bending of the anterior plan between the true and false lumen, generating a mechanical obstruction to the left ventricular outflow tract (Figure 4).
Aortic dissection is more common in male individuals and the male/female ratio ranges from 2:1 to 5:1, with the highest incidence between 45 and 70 years of age, with a peak age between 50 and 55 years for cases of proximal dissection and between 60 and 70 years for the distal cases3,4. The preponderant factor at the dissection is the involvement of the medial layer, as in the genesis of aneurysms in general, and the medial disease that most often predisposes to dissection is medial cystic necrosis. The dissection can be triggered by "traumatic" factors of the arterial wall, such as hypertension, aortic coarctation, pregnancy and bicuspid valve5.
There are also other clinical entities that compromise aortic endothelial integrity and function, such as aortitis, hereditary connective tissue disorders (Marfan syndrome and Ehlers-Danlos syndrome), congenital malformations
of the aortic valve, trauma, aortic valve replacement and situations that facilitate endothelial injury, such as a simple catheterization6. The clinical picture and therapeutic approach are sufficiently different to justify the separation of this entity into two groups: type-A Stanford dissection, involving the ascending aorta extending or not to descending aorta and type-B Stanford dissection, which involves only the descending aorta, with this classification being the most widely accepted1,4. From a purely surgical standpoint, De Bakey et al3 classified dissecting aneurysms into three groups: type I corresponds to the dissection starting in the ascending aorta extending for a varying distance, distally; type II is the dissection limited to the ascending aorta; and type III is the dissection started after the emergence of the left subclavian artery and that progresses to the abdominal aorta with a varying extent. In this case, we found a type-A Stanford aortic dissection, with probable hypertensive etiology, as demonstrated by echocardiography, in addition to the lack of evidence of any risk factors described in the literature, whether in the past medical history, at the clinical evaluation or in the tests performed, to justify another etiology.
The main clinical manifestation of aortic dissection is high-intensity chest pain, accompanied by symptoms of sympathetic activity. The onset of pain is almost always sudden, being characterized as a sharp, stabbing or throbbing pain, associated with sweating and may be limited to the thorax or be retrosternal, radiating to the back, abdomen, upper or lower limbs4. It can also be associated with dyspnea
e12
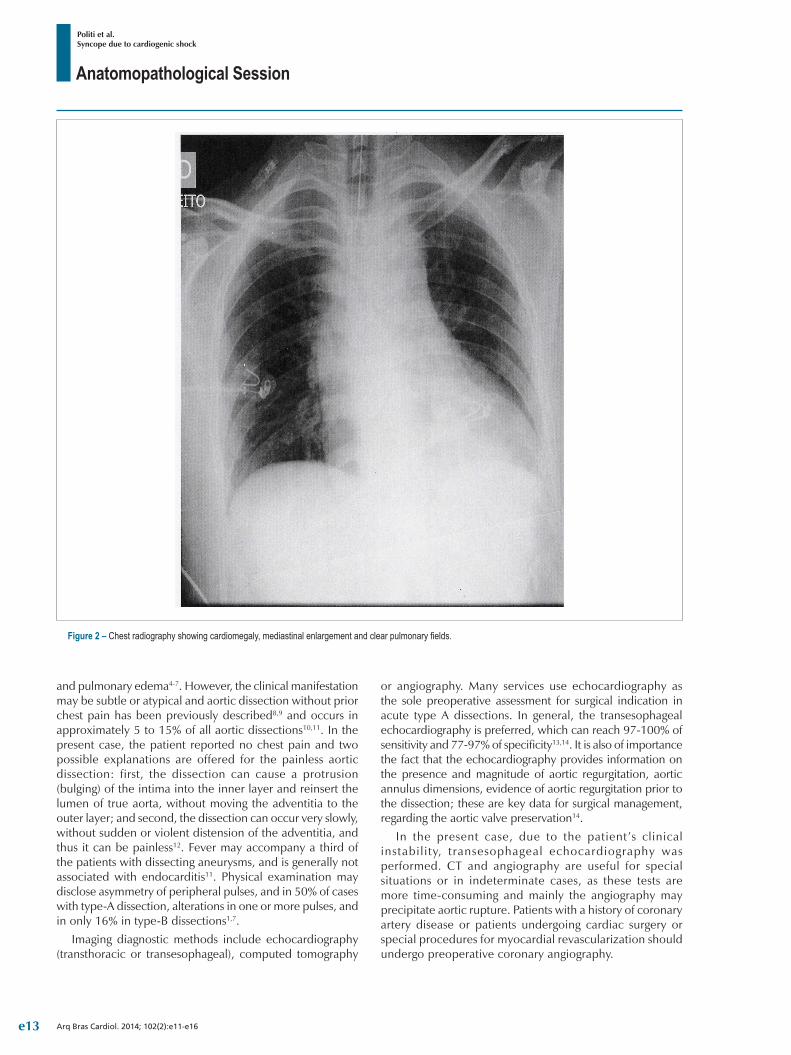
Anatomopathological Session
Politi et al.Syncope due to cardiogenic shock
Arq Bras Cardiol. 2014; 102(2):e11-e16
Figure 2 – Chest radiography showing cardiomegaly, mediastinal enlargement and clear pulmonary fields.
and pulmonary edema4-7. However, the clinical manifestation may be subtle or atypical and aortic dissection without prior chest pain has been previously described8,9 and occurs in approximately 5 to 15% of all aortic dissections10,11. In the present case, the patient reported no chest pain and two possible explanations are offered for the painless aortic dissection: first, the dissection can cause a protrusion (bulging) of the intima into the inner layer and reinsert the lumen of true aorta, without moving the adventitia to the outer layer; and second, the dissection can occur very slowly, without sudden or violent distension of the adventitia, and thus it can be painless12. Fever may accompany a third of the patients with dissecting aneurysms, and is generally not associated with endocarditis11. Physical examination may disclose asymmetry of peripheral pulses, and in 50% of cases with type-A dissection, alterations in one or more pulses, and in only 16% in type-B dissections1,7.
Imaging diagnostic methods include echocardiography (transthoracic or transesophageal), computed tomography
or angiography. Many services use echocardiography as the sole preoperative assessment for surgical indication in acute type A dissections. In general, the transesophageal echocardiography is preferred, which can reach 97-100% of sensitivity and 77-97% of specificity13,14. It is also of importance the fact that the echocardiography provides information on the presence and magnitude of aortic regurgitation, aortic annulus dimensions, evidence of aortic regurgitation prior to the dissection; these are key data for surgical management, regarding the aortic valve preservation14.
In the present case, due to the patient’s clinical instabil i ty, transesophageal echocardiography was performed. CT and angiography are useful for special situations or in indeterminate cases, as these tests are more time-consuming and mainly the angiography may precipitate aortic rupture. Patients with a history of coronary artery disease or patients undergoing cardiac surgery or special procedures for myocardial revascularization should undergo preoperative coronary angiography.
e13
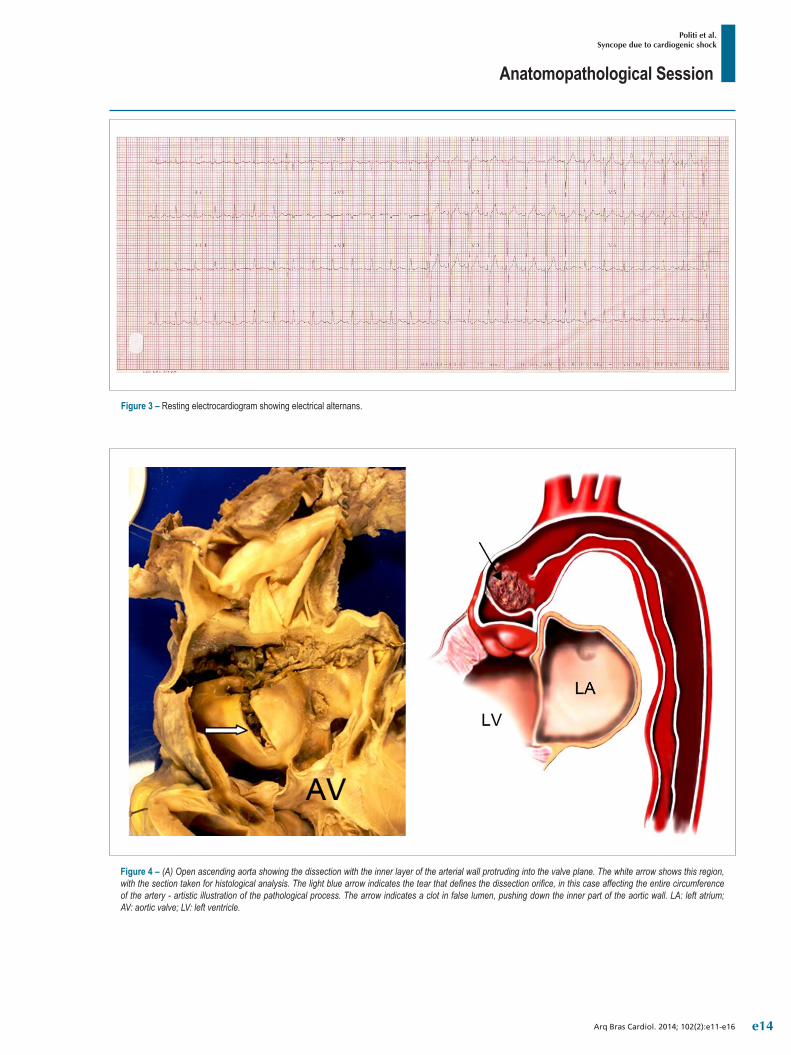
Anatomopathological Session
Politi et al.Syncope due to cardiogenic shock
Arq Bras Cardiol. 2014; 102(2):e11-e16
Figure 3 – Resting electrocardiogram showing electrical alternans.
Figure 4 – (A) Open ascending aorta showing the dissection with the inner layer of the arterial wall protruding into the valve plane. The white arrow shows this region, with the section taken for histological analysis. The light blue arrow indicates the tear that defines the dissection orifice, in this case affecting the entire circumference of the artery - artistic illustration of the pathological process. The arrow indicates a clot in false lumen, pushing down the inner part of the aortic wall. LA: left atrium; AV: aortic valve; LV: left ventricle.
e14

Anatomopathological Session
Politi et al.Syncope due to cardiogenic shock
Arq Bras Cardiol. 2014; 102(2):e11-e16
1. Buffolo E, Carvalho ACC. Dissecção aórtica aguda. In: Knobel E, editor. Condutas no paciente grave. 2a ed. São Paulo:Atheneu;1998. p. 272-8.
2. Mészáros I, Mórocz J, Szlávi J, Schmidt J, Tornóci L, Nagy L, et al. Epidemiology and clinicopathology of aortic dissection: a population-based longitudinal study over 27 years. Chest. 2000;117(5):1271-8.
3. De Bakey ME, McCollum CH, Crawford ES, Morris GC Jr, Howell J, Noon GP, et al. Dissection and dissecting aneurysms of the aorta: twenty-year follow-up of five hundred twenty-seven patients treated surgically. Surgery .1982;92(6):1118-34.
4. Khan IA, Nair CK. Clinical, diagnostic, and management perspectives of aortic dissection. Chest. 2002;122(1):311-28.
5. Crawford ES, Crawford JL.Diseases of aorta. Baltimore: Williams & Wilkins;1986.
6. O’Gara PT, Greenfield AJ, Afridi NA, Hoyser SL, Case records of the Massachussets General Hospital. Weekley clinicopathological exercises. Case 12-2004: 38-year-oldwoman with acute onset of pain in the chest. N Engl J Med. 2004;350(16):1666-74.
7. Pamplona D, Ferreira JFM. Dissecção de aorta: fisiopatologia, diagnóstico clínico e prognóstico. In: Timerman A, César LAM. Manual de cardiologia. Sociedade de Cardiologia do Estado de São Paulo - SOCESP. São Paulo:Atheneu;2000. p.218-21.
8. Steinberg I, Stein HL. Painless chronic dissecting aneurysm of the aorta: report of a case.Am J Roentgenol Radium Ther Nucl Med. 1966;97(2): 416-21.
9. Friessekk, Steffens JC, Caputo GR, Higgins CB.Evaluation of painless aortic dissection whith MR imaging. Am Heart J. 1991; 122(4Pt1):1169-73.
10. Hirst AE, Johns VJ, Kime SW. Dissecting aneurysm of the aorta: A review of 505 cases. Medicine. 1958; 37(3):217-79.
11. Slater EE, De Sanctis RW. The clinical recognition of dissecting aortic aneurysm. Am J Med. 1976; 60(5):625-33.
12. Wood FC, Pendergrass EP, Ostrum HW. Dissecting aneurysm of the aorta: With special reference to its roentgenographic features. Am J Roentgenol. (AJR).1932;28:437-52.
13. Gontijo Filho B, Colluci FC, Fantini FA, Vrandecic MO. Resultados imediatos tardios da correção cirúrgica da dissecção aguda da aorta (tipo A). Rev Bras Cir Cardiovasc. 1997;12(4):311-8.
References
Thus, as this is a condition in which mortality is very high, surgical treatment should be immediate, and late survival is not free of complications (mainly due to the high persistence of patent false lumen in the segments of the aortic arch, descending and abdominal aorta). The need for surgical treatment immediately after diagnosis aims at preventing its life-threatening complications, such as cardiac tamponade secondary to rupture of the aorta, as reported in this case, acute myocardial infarction, symptomatic aortic insufficiency, neurological complications, among others, with a dramatic impact on mortality15,16. The gold standard treatment is the surgical intervention and the traditionally proposed surgery is the interposition of the supracoronary tube, of which in-hospital mortality rate varies, ranging between 10 and 30%17,18. Unfortunately, this patient did not survive long enough to undergo such treatment.
(Dr. Tiago Rodrigues Politi)
Diagnostic hypothesis: ascending aorta dissection. (Dr. Tiago Rodrigues Politi)
Other diagnoses: Systemic arterial hypertension, ascending aorta aneurysm, cardiac tamponade. (Dr. Tiago Rodrigues Politi).
NecropsyNecropsy disclosed dissection of the ascending aorta,
starting approximately 4 cm above the valve, affecting the entire ascending aorta in retrograde fashion. As it affected only the ascending aorta, the dissection was characterized as type II, according to the DeBakey classification, and Stanford type A. The dissection orifice affected the entire arterial circumference, being perpendicular to its axis. There was protrusion of the inner layer of the dissected aorta, leading to
artery obstruction (Figure 4). This obstruction caused multiple organ ischemia, including almost total infarction of both kidneys and cerebral infarction in the right parietal region (the carotid arteries had no dissection). There was rupture of the aorta into the pericardial sac, leading to cardiac tamponade, which was the final event which led to the patient’s death.
The patient had signs of hypertension such as alterations in renal microcirculation, as well as in the afferent arterioles, and left ventricular concentric hypertrophy.
The patient’s age suggested a genetic syndrome underlying the dissection, but he had no clear phenotype of Marfan syndrome and, moreover, showed indicators of hypertension described above.
It is noteworthy, in this case, the prolapse of internal layer of the dissection, leading to blood flow obstruction. It is an unusual complication of acute aortic dissection, which does not appear even in some fairly comprehensive anatomopathological descriptions of this disease19,20. (Dr. Paulo Gutierrez)
Anatomopathological diagnosisAcute aortic dissection and aortic obstruction by the
internal lamina of the sliced arterial wall; probable systemic arterial hypertension.
(Dr. Paulo Gutierrez)
CommentaryCause of death: cardiac tamponade. (Dr. Paulo Gutierrez)
AcknowledgementThe authors would like to thank Falcetti Junior, for his
illustration of the pathological process.
e15

Anatomopathological Session
Politi et al.Syncope due to cardiogenic shock
Arq Bras Cardiol. 2014; 102(2):e11-e16
14. Cigarroa J E, Isselbacher E M, Desanctis R M, Eaglec KA. Diagnosis imaging in the evaluation of suspected aortic dissection. N Engl J Med. 1993; 323(1): 35-43.
15. Daily PO, Trueblood HW, Stinson EB, Wuerflein RD, Schumway NE. Management of acute aortic dissections. Ann Thorac Surg . 1970;10(3):237-47.
16. Miller DC. Surgical management of acute aortic dissection: new data. Semin Thorac Cardiovasc Surg. 1991; 3(3):225-37.
17. Dias RR, Silva IA, Fiorelli AI, Stolf NA. New surgical strategy for acute type A aortic dissection: hybrid procedure. Rev Bras Cir Cardiovasc. 2007;22(4):495-7.
18. Borst HG, Heinemann MK, Stone CD. Surgical treatment of aortic dissection.NewYork:Churchill & Livingstone;1996. p.357.
19. Hirst Jr AE, Johns VJ Jr, Kime SW Jr. Dissecting aneurysm of the aorta: a review of 505 cases. Medicine. 1958; 37(3): 217-80.
20. Roberts WC. Aortic dissection: anatomy, consequences, and causes. Am Heart J .1981; 101(2):195-214.
e16

Case Report
Clinically Manifested Myocarditis in Acute Rheumatic FeverJosé L. Xavier Jr.1, Alexandre de Matos Soeiro1, Antonio S. S. A. Lopes2, Guilherme S. Spina2, Carlos V. Serrano Jr.1, Múcio T. Oliveira Jr.1
Unidade Clínica de Emergência - Instituto do Coração (InCor) - HCFMUSP1; Unidade Clínica de Valvopatias - Instituto do Coração (InCor) - HCFMUSP2, São Paulo, SP - Brazil
IntroductionThe development of acute myocarditis in the postoperative
period of cardiac surgery is a challenge for the doctor who treats this type of patient. In most cases, myocarditis can be only a consequence of procedural-related inflammation. However, differential diagnoses must be observed. Among them, rheumatic fever must be considered as an important mechanism. Although its cardiac manifestation is predominantly related to the involvement of the valvular apparatus, its diagnosis is essentially clinical and it can acutely impair the myocardium. In this context, the occurrence of acute rheumatic myocarditis is rare and its immunosuppressive treatment remains uncertain.
Case ReportThe patient was a 23-year-old Caucasian female, born
and raised in São Paulo, who came to the emergency department complaining of dyspnea at rest (functional class IV of the New York Heart Association), palpitations, nausea, unmeasured fever and increased abdominal volume for six days. She reported a personal history of rheumatic fever, with two mitral and tricuspid valve plastic surgeries, in 1996 and 2011, and subsequent mitral valve replacement with a biological prosthesis four months before, in 2012. She also had chronic atrial fibrillation on anticoagulation. She denied other symptoms and comorbidities. She was an irregular user of warfarin, furosemide 40 mg / day, spironolactone 50 mg/day, captopril 37.5 mg/day, diltiazem 180 mg/day and sulfadiazine 1 g/day (due to allergy to penicillin).
In February 2012, the patient started to have dyspnea at rest due to symptomatic mitral valve regurgitation and remained hospitalized until heart surgery for mitral valve replacement with a biological prosthesis. At this time she was submitted to preoperative myocardial scintigraphy with gallium-67, which was negative for myocardial inflammatory process. The surgery had no complications and the
postoperative transthoracic echocardiography showed left atrium (LA) with 50 mm in diameter, left ventricle (LV) of 56 x 39 mm, ejection fraction (EF) of 57% and unchanged mitral bioprosthesis structure. She was discharged receiving the medications listed above.
On physical examination, the patient was in good general health status, afebrile, tachycardic (heart rate = 180 beats per minute), blood pressure of 90 x 60 mmHg, tachydyspneic (respiratory rate = 25 breaths per minute), arterial oxygen saturation in ambient air was 93% and she had intercostal retraction. Apex beat was visible and palpable in the fifth intercostal space on the left midclavicular line; presence of arrhythmic heart sounds with a loud B2 sound, holosystolic mitral regurgitation murmur of 2 +/6+ intensity, breath sounds present with fine rales in the lung bases bilaterally, hardened liver that was palpable about 7 cm from the right costal margin and bilateral and symmetric 2+/ 4+ lower limb edema.
At this time, a diagnosis of heart failure due to probable infective endocarditis or active rheumatic fever was attained, considering the presence of fever and clinical signs of pulmonary and systemic congestion, after which three pairs of blood cultures were collected, an echocardiogram was requested and empirical antibiotic therapy with intravenous ceftriaxone and oxacillin was initiated.
The electrocardiogram initially showed atrial fibrillation with high ventricular response. Chest X-ray showed interstitial infiltrates in the lower two-thirds of both hemithoraxes, as well as cardiomegaly.
Transesophageal echocardiography showed LA = 56 mm, LV = 71 x 62 mm, EF 20% with diffuse hypokinesis of LV and bioprosthetic mitral valve with no signs dysfunction or evidence of vegetation. Blood cultures were negative. At this time, we chose to maintain adequate control of heart rate and administration of intravenous furosemide. To confirm the rheumatic myocarditis, myocardial scintigraphy with gallium-67 was requested, which showed positive for ongoing inflammatory process (Figure 1). Cardiac magnetic resonance imaging was performed, which showed significant diffuse biventricular dysfunction and presence of myocardial inflammatory process (Figure 2). Laboratory assessment showed C-reactive protein of 89.3 mg/L, brain natriuretic peptide (BNP) of 2,553 pg/mL, ASLO = 693 IU/mL, erythrocyte sedimentation rate of 50 mm and alpha-1-acid glycoprotein = 136 mg/dL.
Due to the diagnosis of myocarditis, Prednisone 2 mg/kg/day was started. Two hypotheses were then considered: postoperative myocarditis (procedure-related) and acute attack of rheumatic fever. The patient showed significant symptom improvement and was discharged on the 14th day after admission using prednisone 1 mg/kg/day, captopril, furosemide, spironolactone, carvedilol, digoxin and warfarin. In addition, she was referred to immunology
Mailing Address: Alexandre de Matos Soeiro •Rua Maranhão, 680, apt.º 81, Santa Paula. Postal Code 09530-440, São Caetano do Sul, SP - BrazilE-mail: [email protected] received February 17, 2013; revised manuscript May 27, 2013; accepted June 11, 2013.
KeywordsMyocarditis; Cardiomyopathy, Dilated; Rheumatic Fever/
epidemiology.
DOI: 10.5935/abc.20140017
e17
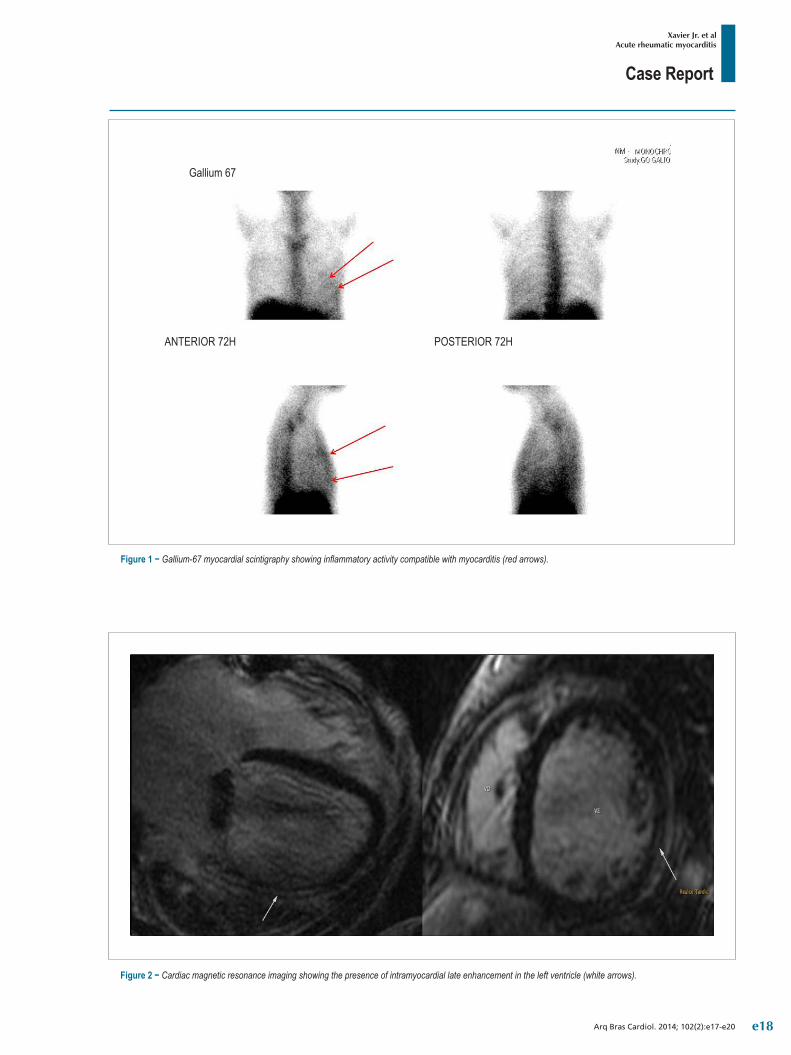
Case Report
Xavier Jr. et alAcute rheumatic myocarditis
Arq Bras Cardiol. 2014; 102(2):e17-e20
Figure 2 − Cardiac magnetic resonance imaging showing the presence of intramyocardial late enhancement in the left ventricle (white arrows).
Figure 1 − Gallium-67 myocardial scintigraphy showing inflammatory activity compatible with myocarditis (red arrows).
Gallium 67
ANTERIOR 72H POSTERIOR 72H
e18

Case Report
Xavier Jr. et alAcute rheumatic myocarditis
Arq Bras Cardiol. 2014; 102(2):e17-e20
for desensitization to penicillin and started to receive a dose of benzathine penicillin of 1.200.000 IU every 15 days without complications.
DiscussionThe occurrence of postoperative myocarditis is
underdiagnosed. Most of the time, it is not associated with ventricular dysfunction. It usually occurs on the days following the procedure and, in rare cases, remains for a long time. The diagnosis of acute rheumatic fever attack was established by the Jones criteria of the American Heart Association. The presence of myocarditis associated with elevation in inflammatory markers, fever, previous valvular sequelae and high ASLO levels are enough for the diagnosis of acute rheumatic fever attack, which makes this the main hypothesis in the case1-3.
In literature, and in classic rheumatic fever, the three leaflets (pericardium, myocardium and endocardium) are simultaneously affected, although in unequal proportions, with usually subclinical myocardial lesion only. In most cases in which there is a picture of heart failure during an acute attack of rheumatic fever, it is due to a mechanical cause, due to valvular dysfunction, and clinically manifest myocarditis is uncommon4. In this case, the patient met the criteria for acute rheumatic fever; however, the echocardiogram showed no biological valve prosthesis dysfunction and showed significant biventricular myocardial dysfunction. Myocardial scintigraphy and cardiac MRI confirmed the diagnosis, by demonstrating the presence of myocardial inflammation.
In the diagnosis of myocarditis, clinical, electrocardiographic, laboratory and radiographic findings have low sensitivity and specificity. Troponin I is increased in only 34% of cases of myocarditis. Sinus tachycardia, changes in the ST segment or T wave, as well as bundle branch blocks, can be found, but they are not specific and infrequent5.
The gold standard for the diagnosis of myocarditis would be the endomyocardial biopsy of the right ventricle, but its sensitivity is questionable due to its focal nature, in addition to being an invasive test. Scintigraphy and MRI have emerged as important tools in the diagnosis of myocarditis. Recent studies have demonstrated the usefulness of scintigraphy, not only in the diagnosis but also the prognosis of myocarditis, with a sensitivity of 91-100% and negative predictive value ranging from 93-100%6.
Sun et al7 found a good association between the degree of perfusion reduction at the scintigraphy and elevated markers of myocardial necrosis and ST-T changes related to myocarditis. Regarding the role of magnetic resonance imaging, Abdel-Aty et al stuyding 25 patients with suspected myocarditis and 23 controls, found a sensitivity of 84% and specificity of 74%5,8,9. However, specifically in rheumatic myocarditis, the literature is scarce and there is no clear radiological evidence of this event, as shown in this case. This fact makes this report unique due to image capture in cardiac MRI, demonstrating myocardial inflammation during a probable attack of acute rheumatic fever.
As for treatment, most patients with acute myocarditis respond very well to the general measures used in acute
heart failure, such as neurohumoral blocking5. In acute attacks of rheumatic fever with myocardial impairment, the dose used in immunosuppression and how it should be performed are yet to be determined. Due to the rarity of cases, the best therapeutic method is based on case reports, only. In our case there was clinical improvement after the use of prednisone at a dose of 2 mg/kg/day for 14 days, which was reduced to 1 mg/kg/day thereafter. The treatment time is also unknown and must be based on ventricular function recovery associated with the reduction in inflammatory markers10.
Despite all the advances in Medicine, the higher cost-effectiveness intervention in rheumatic fever is still secondary prevention, preventing acute attacks and, thus, early and more severe valve sequelae. Intramuscular injections of benzyl penicillin every three weeks were able to reduce hospital admissions and are preferred to the use of oral medication, due to its proven efficacy3, which justified the conduct of attempting desensitization to penicillin in this case.
Furthermore, it is noteworthy, based on this case report, the importance of maintaining secondary prophylaxis even after the occurrence of valve replacement, as the acute attack can manifest in other organs or in the heart itself, but in another segment.
ConclusionThe demonstration of probable rheumatic myocarditis
in cardiac MRI makes this case unique. The presence of an acute attack of rheumatic fever should always be considered in young patients with a previous diagnosis and who are not receiving adequate secondary prophylaxis. Its treatment is still uncertain, but it is based on immunosuppression and recurrence prevention, maintaining the prophylaxis even in patients who have already undergone valve replacement.
Author contributionsConception and design of the research: Xavier Jr. JL, Soeiro
AM, Lopes ASSA, Oliveira Jr. MT. Acquisition of data: Xavier Jr. JL, Soeiro AM, Lopes ASSA, Oliveira Jr. MT. Analysis and interpretation of the data: Xavier Jr. JL, Soeiro AM, Serrano Jr. CV. Writing of the manuscript: Xavier Jr. JL, Soeiro AM. Critical revision of the manuscript for intellectual content: Soeiro AM, Lopes ASSA, Spina GS, Serrano Jr. CV, Oliveira Jr. MT.
Potential Conflict of Interest No potential conflict of interest relevant to this article was
reported.
Sources of Funding There were no external funding sources for this study.
Study Association This study is not associated with any post-graduation
program.
e19

Case Report
Xavier Jr. et alAcute rheumatic myocarditis
Arq Bras Cardiol. 2014; 102(2):e17-e20
1. Azevedo PM, Pereira RR, Guilherme L. Understanding rheumatic fever. Rheumatol Int. 2012;32(5):1113-20.
2. Cunningham MW. Streptococcus and rheumatic fever. Curr Opin Rheumatol. 2012;24(4):408-16.
3. World Health Organization (WHO). Rheumatic fever and rheumatic heart disease: report of a WHO expert consultation on rheumatic fever and rheumatic heart disease. Geneva; 2004.
4. Kamblock J, Payot L, Iung B, Costes P, Gillet T, Le Goanvic C, et al. Does rheumatic myocarditis really exists? Systematic study with echocardiography and cardiac troponin I blood levels. Eur Heart J. 2003;24:855-862.
5. Sagar S, Liu PP, Cooper LT Jr. Myocarditis. Lancet. 2012;379(9817):738-47.
6. Javadi H, Jallalat S, Pourbehi G, Semnani S, Mogharrabi M, Nabipour I, et al. The role of gated myocardial perfusion scintigraphy (GMPS) in
myocarditis: a case report and review of the literature. Nucl Med Med RevCent East Eur. 2011;14(2):112-5.
7. Sun Y, Ma P, Bax JJ, Blom N, Yu Y, Wang Y, et al. 99mTc-MIBI myocardial perfusion imaging in myocarditis. Nucl Med Commun. 2003;24(7):779-83.
8. Abdel-Aty H, Boye P, Zagrosek A, Wassmuth R, Kumar A, Messroghli D, et al. Diagnostic performance of cardiovascular magnetic resonance in patients with suspected acute myocarditis: comparison of different approaches. J Am Coll Cardiol. 2005;45(11):1815-22.
9. Liu PP, Yan AT. Cardiovascular magnetic resonance for the diagnosis of acute myocarditis: prospects for detecting myocardial inflammation. J Am Coll Cardiol. 2005;45(11):1823-5.
10. Mason JW, O’Connell JB, Herskowitz A, Rose NR, McManus BM, Billingham ME, et al. A clinical trial of immunosuppressive therapy for myocarditis. The Myocarditis Treatment Trial Investigators. N Engl J Med. 1995;333(5):269-75.
References
e20

Viewpoint
Detailing the Writing of Scientific Manuscripts: 25-30 ParagraphsClaudio Gil Soares de AraújoPrograma de Pós-Graduação em Ciências do Exercício e do Esporte - Universidade Gama Filho, Rio de Janeiro, RJ; Clínica de Medicina do Exercício - Clinimex, Rio de Janeiro, RJ - Brazil
Mailing Address: Claudio Gil Soares de Araújo •Rua Siqueira Campos, 93/101, Copacabana. Postal Code 22071-030, Rio de Janeiro, RJ - BrazilEmail: [email protected]; [email protected] received July 24, 2013, revised manuscript August 9, 2013, accepted August 12, 2013.
KeywordsJournal of Article; Writing; Methodology; Bibliometrics.
DOI: 10.5935/abc.20140019
In their professional practices, physicians often face unexpected situations or chance on innovative proposals and ideas. As a result of their training and competence, they usually come up with hypotheses to be tested and research is conducted. This research is completed and their results submitted for presentations at conferences as free communications. Nevertheless, the realization of this creative process is only complete when a scientific manuscript is published in a journal. At this ultimate stage, most efforts seem not be brought to a standstill1,2. There are several reasons why scholars, interns, residents, graduate students and even experienced physicians may find it difficult to move forward from congress’ abstracts to full manuscripts published in journals. However, the most significant hindrance rests with the difficulty writing the mere 25-30 paragraphs of an original manuscript. Many freeze and give up in front of a blank paper or a blinking cursor on a blank word processor’s page on the monitor screen. In the previous manuscript3, we analyzed and suggested improvements to the process of peer review. In this point of view, we propose a practical strategy to systematize the writing of scientific paragraphs, aiming to simplify the task of scientific writing. This way, our intent is to increase the rate of publication of full manuscripts based on several outstanding abstracts presented annually at major medical conferences, and facilitate the currently overburdened process of peer review.
The format of scientific communication has been evolving greatly over the centuries4-7, making reading more objective and standardized. One of the important tools in this process is the IMRaD format4,5,7, an acronym derived from the initials of the main sections of a manuscript - introduction, methods, results and discussion. Throughout the twentieth century, the IMRaD format has been increasingly applied, accounting for about 10% of the manuscripts in the 1950s, being dominant in the 1960s, and reaching 80% in the 1970s7. Presently, IMRad is the format recommended and adopted by the main medical journals all over the world, including the ABC (Arquivos Brasileiros de Cardiologia).
In addition to the IMRaD format, original manuscripts submitted for publication should meet specific standards and rules of each journal. Although a fairly uniform pattern tends to prevail, there are differences that should be observed at the time of writing. For instance, the number of words is limited to 4,500 in ABC and 5,000 in JACC, including text and references. Considering that the references are usually limited to 30-40, and have around 1,000 words, circa 3,500-4,000 are left for the text’s body, i.e., to be used in the 25-30 paragraphs of IMRaD, representing about 130 words each.
In the pursuit for evidence and objective data, as a convenience sample, all original manuscripts published in the January 2012 and 2013 editions of ABC and JACC journals have been analyzed (the first two numbers of these months for the latter). There was a fairly clear trend about the total number of paragraphs and distribution of paragraphs in four sections of the IMRaD of a manuscript. For the 20 ABC’s manuscripts and 34 JACC’s ones, the average number of paragraphs was 28.9 and 28.2 (p = 0.703), respectively, with 1/3 of them having 25-30 paragraphs, and 57% of the total manuscripts having overall 22-33 paragraphs. This relative constancy should be observed and highlighted, considering that the topics and areas covered, as well as the background and the nationality of the authors, are quite different. Thus, this confirms the assumption that there is a basic format to be followed for an effective publication.
Figure 1 illustrates the distribution of paragraphs for the various IMRaD sections in the two journals analyzed. Although there is some variability among the manuscripts, the introduction is clearly a section with fewer paragraphs (p < 0.001), while the remaining sections are somewhat balanced (p > 0.05), especially for original manuscripts of JACC, in which the sections of methods, results and discussion tend to have eight to nine paragraphs. When the distributions of paragraphs between ABC and JACC are compared, introductions and discussions tend to have more paragraphs in ABC than in JACC, respectively, 3.8 versus 2.4 (p < 0.01) and 10.4 versus 8.8 (p = 0.04).
Based on these results, in our personal experience as authors of original manuscripts and according to other authors’ opinions4,8-10, a simple content model may be proposed within the IMRaD format, taking 25-30 paragraphs as standard for an original manuscript. For practical purposes, one page is considered one page in a word processor, with conventional margins and with a 1.5 line spacing and font size 11.
Unfolding the sectionsIntroduction: 1 page (ideally), maximum 400 words over
1-4 paragraphs (ideally 3) – some journals restrict this to 350 words (E.g.: ABC); 5-10 references.
e21
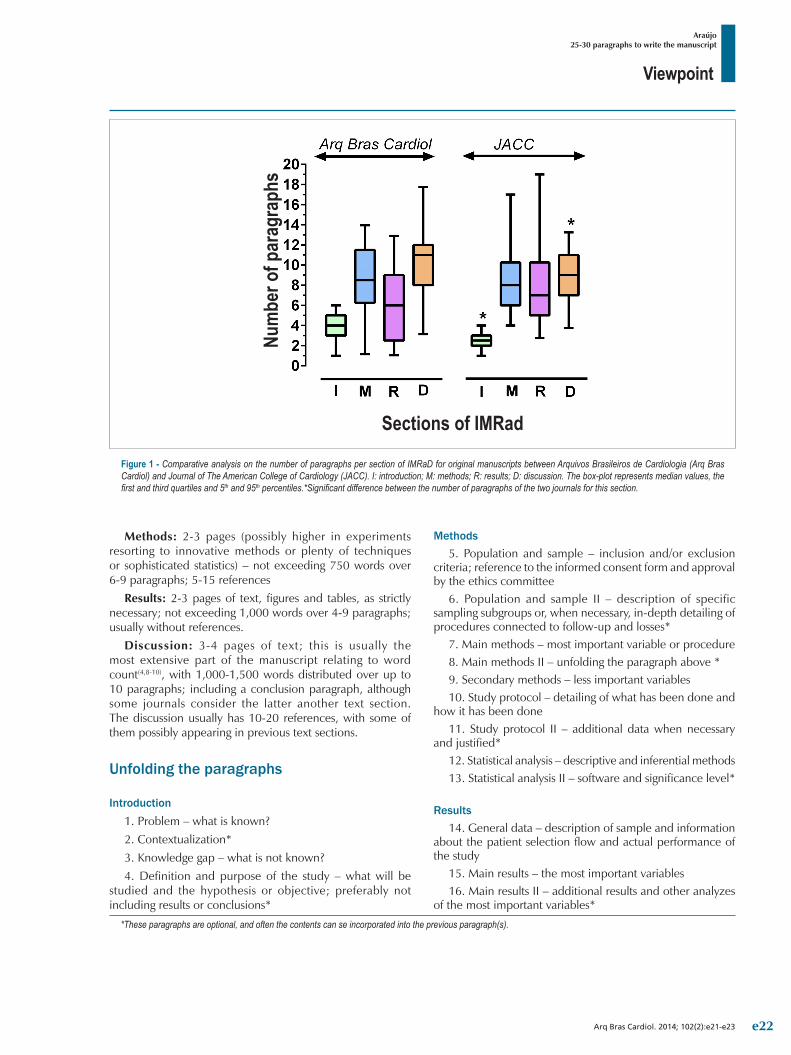
Viewpoint
Araújo25-30 paragraphs to write the manuscript
Arq Bras Cardiol. 2014; 102(2):e21-e23
*These paragraphs are optional, and often the contents can se incorporated into the previous paragraph(s).
Figure 1 - Comparative analysis on the number of paragraphs per section of IMRaD for original manuscripts between Arquivos Brasileiros de Cardiologia (Arq Bras Cardiol) and Journal of The American College of Cardiology (JACC). I: introduction; M: methods; R: results; D: discussion. The box-plot represents median values, the first and third quartiles and 5th and 95th percentiles.*Significant difference between the number of paragraphs of the two journals for this section.
Num
ber o
f par
agra
phs
Sections of IMRad
Methods: 2-3 pages (possibly higher in experiments resorting to innovative methods or plenty of techniques or sophisticated statistics) – not exceeding 750 words over 6-9 paragraphs; 5-15 references
Results: 2-3 pages of text, figures and tables, as strictly necessary; not exceeding 1,000 words over 4-9 paragraphs; usually without references.
Discussion: 3-4 pages of text; this is usually the most extensive part of the manuscript relating to word count(4,8-10), with 1,000-1,500 words distributed over up to 10 paragraphs; including a conclusion paragraph, although some journals consider the latter another text section. The discussion usually has 10-20 references, with some of them possibly appearing in previous text sections.
Unfolding the paragraphs
Introduction1. Problem – what is known?2. Contextualization*3. Knowledge gap – what is not known?4. Definition and purpose of the study – what will be
studied and the hypothesis or objective; preferably not including results or conclusions*
Methods5. Population and sample – inclusion and/or exclusion
criteria; reference to the informed consent form and approval by the ethics committee
6. Population and sample II – description of specific sampling subgroups or, when necessary, in-depth detailing of procedures connected to follow-up and losses*
7. Main methods – most important variable or procedure8. Main methods II – unfolding the paragraph above *9. Secondary methods – less important variables10. Study protocol – detailing of what has been done and
how it has been done11. Study protocol II – additional data when necessary
and justified*12. Statistical analysis – descriptive and inferential methods 13. Statistical analysis II – software and significance level*
Results14. General data – description of sample and information
about the patient selection flow and actual performance of the study
15. Main results – the most important variables16. Main results II – additional results and other analyzes
of the most important variables*
e22
Viewpoint
Araújo25-30 paragraphs to write the manuscript
Arq Bras Cardiol. 2014; 102(2):e21-e23
*These paragraphs are optional, and often the contents can se incorporated into the previous paragraph(s).
1. Ramos PS, Furtado EC, Carvalho ER, Campos MO, Souza DV, Almeida LD, et al. Dissertações e teses de pós-graduação geram publicação de artigos científicos? Análise baseada em três programas da área de educação física. Braz J Biomotricty. 2009;3(4):315-24.
2. Scherer RW, Langenberg P, von Elm E. Full publication of results initially presented in abstracts. Cochrane Database Syst Rev. 2007;(2):MR000005.
3. Araújo CG. Revisão por pares: um processo científico em constante aprimoramento. Arq Bras Cardiol. 2012;98(2):e32-5.
4. Liumbruno GM, Velati C, Pasqualetti P, Franchini M. How to write a scientific manuscript for publication. Blood Transfus. 2013;11(2):217-26.
5. Oriokot L, Buwembo W, Munabi IG, Kijjambu SC. The introduction, methods, results and discussion (IMRAD) structure: a survey of its use in different authoring partnerships in a students’ journal. BMC Res Notes. 2011;4:250.
6. Araújo CG, Sardinha A. Submetendo um manuscrito a revistas científicas de alto impacto: maximizando a chance de aceitação. In: Brandão ML. (editor). Manual de publicação científica. Rio de Janeiro: Elsevier; 2009. p. 33-47.
7. Sollaci LB, Pereira MG. The introduction, methods, results, and discussion (IMRAD) structure: a fifty-year survey. J Med Libr Assoc. 2004;92(3):364-7.
8. Earnsham JJ. How to write a clinical paper for publication. Surgery. 2012;30(9):437-41.
9. Deheinzelin D. Introdução ou por que os seus dados são importantes. Rev Assoc Med Bras. 2012; 58(1):1.
10. Singer AJ, Hollander JE. How to write a manuscript. J Emerg Med. 2009;36(1):89-93.
References
17. Secondary results – the other study variables18. Secondary results II – additional results of variables or
the interrelation or interaction between them*19. Secondary results III – additional results of variables or
the interrelation or interaction between them*20. Other results and analysis carried out in the study*
Discussion21. The problem and the study’s “original” proposal –
discussing again the study’s problem22. Interpretation of the main result – meaning of what
has been found23. Comparison with the literature – how this result
confirms previous data24. Further comparison with the literature* – exploring
methodological or mechanistic differences25. The main result’s contribution to knowledge – the
“novelty” or main message or contribution of the research to the current state-of-the-art
26. Interpretation of secondary results – what these results inform or mean
27. Interpretation of secondary results II*28. Comparison of this study with previous ones – the
contribution and developments in this study for the area’s knowledge
29. Limits of the study – strengths and weaknesses; the weaknesses and methodological problems of the study and, especially, how these limitations may hinder the practical application of the results and their interpretations. The strengths of the study may also be stressed, possibilities may be pointed out, as well as issues to be further researched — other knowledge gaps
30. Conclusions and implications – this represents a synthesis of the study, usually answering the hypothesis
reported in the final paragraph of the introductory section, solving the study objective.
* These paragraphs are optional, and often the contents can be incorporated into the previous paragraph(s).
A rather practical observation is that the writing of paragraphs does not need to follow the order of sections or, even, the several paragraphs making up the given section. In practice, most of the experienced authors start with the methods and results, hence following to the discussion, and only then proceeding to the introduction. The title is typically their last concern.
Grounded on the practical strategy presented in this point of view, in keeping with the IMRaD format, we may assert that potential authors will deal better with blinking cursors on the word processor and will deal easily and objectively with the final stage of transforming an outstanding communication at a conference into an excellent original manuscript. This will allow a much larger audience to benefit from their findings and interpretations, forever.
Author contributionsConception and design of the research, Acquisition of data,
Analysis and interpretation of the data, Statistical analysis, Obtaining funding, Writing of the manuscript, Critical revision of the manuscript for intellectual content: Araújo CGS.
Potential Conflict of Interest No potential conflict of interest relevant to this article was
reported.
Sources of Funding This study was partly funded by CNPq and FAPERJ.
Study AssociationThis study is not associated with any thesis or dissertation work.
e23