Embed Size (px)
Citation preview

Asthma? Eosinophilia?
Yazeed Toukan, MD
Pediatric Pulmonary Institute,
Ruth Rappaport Children`s Hospital
October 2018

הצגת מקרה
כ"בריא בד, שנים13בן •
2016תסמינים נשימתיים עד יולי ללא •
שיעול וקושי נשימתי–שחיה במהלך קורס אז •
של חשיפה משמעותית לכלורארועללא •
זיהומים אחרים שהצריכו /אוזניים/ריאהללא דלקות •
אנטיביוטיקה

הצגת מקרה
: 6.4.17-באצלנו ראשונה ביקורת •
–FEV1 63%, CHG 28%
160/4.5סימביקורטמונע במשאף הוחל טיפול –
סינגולרהוסף גם טיפול ב ... נשנותהחמרותהמשיך עם •
ירידה , סטורציות-דה, קושי נשימתי: אשפוזים חוזרים•
בתפקודי נשימה
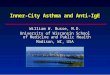
, פרידניזוןקורסים חוזרים של •
מהירהתגובה עם
↓
טיפול בסטרואידיםתלוי •

Severe and Difficult-to-Treat Asthma?
• Sweat test - Cl- 33, 31
• Nasal NO - 399
• Exhaled NO - 39
• Macloride x3/wk – failed
• Chest CT - Atelectasis LLL
• Bronchoscopy + BAL - Normal AW anatomy;– High leukocytes; “some” Eosinophils
• Echo - Normal
• Medication adherence & technique
• Smoking
√

05.201802.201810.201707.201711.2016
13,30010,20011,8809,3006,500WBC
950(7%)
816(8%)
10(0.08%)
300(3%)
1000(15%)
Eos.
Blood smear - Normal

Eosinophilia?
• ≥ 500/µL is abnormal in the vast majority of cases
– Mild - 500 -1500
– Moderate – 1500-5000
– Severe - >5000
• The primary stimuli for Eosinophil production: IL-3,
IL-5 & GM-CSF

Eosinophilia & Lungs?

Differential diagnosis of eosinophiliaC H I N A
C Connective tissue diseases
H Helminth infections
I Idiopathic HES
N Neoplasia
A Allergies

More tests…
• “Collagenogram”
– ANA levels – Normal; C3 & C4 levels – Normal
– ANCA – Neg.
– Angiotensin converting enzyme (ACE) levels – Normal
– Celiac serology – Neg.
• Immunologic
– IgA, IgG (+subclasses), IgM – Normal levels
– Immunophenotyping – Normal
• Allergic
– Allergy skin tests (twice) – Neg.
– Aspergillus skin test – Neg.
– IgE: 544 609

Hyper-Eosinophilic Syndromes (HES)
Definition
• Blood eosinophilia of ≥1500/µL, for > 6 mo
• No other apparent etiologies for eosinophilia
• Eosinophil-mediated end-organ dysfunction– Cardiac
– Pulmonary
– Myeloproliferative
– Lymphoproliferative

Hyper-Eosinophilic Syndromes (HES)
Etiology
• Idiopathic
• Myeloproliferative variant - FIP1L1-PDGFRA fusiongene
• Abnormal clones of T cells producing IL-5

Hypersensitivity pneumonitis
[Extrinsic allergic alveolitis]

Hypersensitivity pneumonitis [Extrinsic allergic alveolitis]
• Immunological reaction of the lung in response to repetitive inhalation of a sensitized allergen
• >300 antigens: Bacteria, Fungi, Animal proteins, Plant proteins,…
– In up to 60% of cases, a trigger is not identified
• The most commonly occupational exposures– Farmer's lung
– Bird or Pigeon fancier’s lung
– Hot tub lung [MAC?]
– Workers lung
Hypersensitivity pneumonitis [Extrinsic allergic alveolitis]
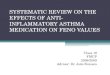
History and Physical
• Acute: fever, cough, and dyspnea within a few hours
• Subacute and chronic: prolonged exposure, cough is predominant
Evaluation
• ↑WBC, ↑↑ESR & CRP
• Serum precipitins IgG against potential organic antigens
• Skin testing has a limited value

Hypersensitivity pneumonitis [Extrinsic allergic alveolitis]
Spirometry: Restrictive pattern (also obstructive/mixed)
Bronchoscopy: BAL: lymphocytosis (> 50%)
CXR: Normal
Chest CT
• Heterogeneous appearance: areas of ground glass or nodular opacities (high attenuation), air trapping (low attenuation) and normal parenchyma “head cheese sign“
• Accuracy of diagnosis based on HRCT can be as high as 92%

Hypersensitivity pneumonitis [Extrinsic allergic alveolitis]
Treatment / Management
• Antigen Avoidance
• Glucocorticoids
• Alternative Agents
– Azathioprine; Mycophenolate mofetil; Rituximab
• Lung Transplantation

Our patient
בעדאוליהשיפור המהיר •
?האם קיים גורם סביבתי, אבל•
סביבה/אין חיות בבית–
ללא שינוי–שינוי מקום מגורים –
,בנוסף•
חסימתי –תפקודי נשימה –
פריפרית לא אופייניתאאוזינופיליה–
הדמיה לא תומכת–
ספיציפיIgGאין לנו •


Ulceration
Vasculitis
Necrosis
מלאנמקעםמלאההתכייבות-אפידרמיס•
(וסקוליטיס)גרעיניואבקנויטרופילים-דםכלידפנות•
רבגרעיניואבקנויטרופיליםעםכחלחלנקרוביוזיסשלאזורים-בדרמיסעמוק•פיבריןומשקעילוסקוליטיסחשדעם
Skin Biopsy

Skin Biopsy
לסיכום
•Acute necrotizing vasculitis
Wegener-לביטויגםלהיותשיכולה)– granulomatosisבעור).
,הביופסיהביצועבעתפרדניזוןבטיפולתחתהיההמטופל•(אאוזינופיליםהעדר)התסניןהרכבאתלשנותשיכול

Wegener granulomatosis?
!הפריחה חלפה מהר•
•ANCAשלילי
תקין-שתן כללית •
•CT סינוסים מלאים-סינוסים
(?ביופסיה)ג "בדיקה רופא אא•
–FO-מחיצה תקינה
שינויים מתאימים לווגנר/קרוסטותללא –
ביופסיההניתן לקחת ממנו ללא ממצא –

Other Vasculitis…
Eosinophilic granulomatosis with polyangiitis[Churg–Strauss syndrome]?
- CSS To begin with?
- Drug-induced (Singulair)?

Churg–Strauss syndrome
• A rare syndrome, affects small-medium-sized vessels
• Allergic dis. (asthma/allergic rhinitis) - 8-10 yrs before presentation
• Eosinophilic tissue infiltration
• Mean age (vasculitis) – 38-48 yr
• ↑ IgE, p-ANCA (pos/neg)

Churg–Strauss syndrome
• In 1990, the American College of Rheumatology – Asthma
– Eosinophilia > 10% in peripheral blood
– Paranasal sinusitis
– Pulmonary infiltrates (patch & transient)
– Histological proof of vasculitis with extravascular eosinophils
– Mononeuritis multiplex or polyneuropathy
• The presence of ≥ 4 criteria
– sensitivity 85% & specificity of 99.7%
❶
❷
❸
❹


Churg-Strauss syndrome &Montelukast therapy
• It is stated that CSS will occur in <0.01% of patients
• Former studies - the association is somewhat doubtful
• Most patients were also receiving other medications
• And, some patients had a decrease in the intake of steroids concomitantly
The disease could be masked by the use of steroids and the patient already had angiitis

Churg-Strauss syndrome &Montelukast therapy
• However, the symptoms disappeared in some patients after withdrawing Montelukast
This can be seen regarded as an argument for a causal relationship

Churg–Strauss syndrome
• Systemic glucocorticoids
• Stop Montelukast
• However, most patients remain dependent on glucocorticoid therapy, and relapses are common
• Given the side effects of glucocorticoids, there is a need for additional, more effective therapies

Churg–Strauss syndrome
• The cytokine IL-5 regulates eosinophil proliferation, maturation, and differentiation
• It is present at increased levels in these patients
→ The neutralization of IL-5 - a potential therapeutic option

Asthma - Eosinophilic Refractory?
vsChurg–Strauss syndrome?

• 13 studies on 6000 participants
– 4 – Mepolizumab
– 4 – Reslizumab
– 5 - Benralizumab
• 8 included children > 12yr
• People with severe eosinophilic asthma

Anti-IL5 therapies for asthma
• The studies support the use of anti-IL-5 treatments as an adjunct to standard of care
• Halve the rate of asthma exacerbations
• Limited evidence for improved HRQoL scores & lung function
• No safety concerns

Anti-IL5 therapies for asthma
• Further research is needed on biomarkers for
– assessing treatment response
– optimal duration and long-term effects of treatment
– risk of relapse on withdrawal
– non-eosinophilic patients
– children (particularly < 12yr)
Funded by GlaxoSmithKline and the National Institute of Allergy and Infectious Diseases

Churg–Strauss syndrome
• In participants (>18yr), Mepolizumab resulted in
– significantly more weeks in remission
– allowing for reduced glucocorticoid use
• Even so, only ~1/2 the participants treated with mepolizumab had protocol-defined remission

Back to our patient

Back to our patient
רפרקטוריתאיזונופיליתאסתמה –קלינית •
סטרואידיםתלוי טיפול ב•
חלף אחר מספר ימים, בודד של פריחהארוע•
וסקוליטיסממצאים של –ביופסיה עורית •
הופסקסינגולרבטיפול •
ירידה/מחמיר בהפסקה... פרידניזוןבממשיך טיפול •

Anti-IL5 therapies
, שנים12מאושר בארץ מעל ]
[שנים12-18נתונים לגילאים אין מספיק אך
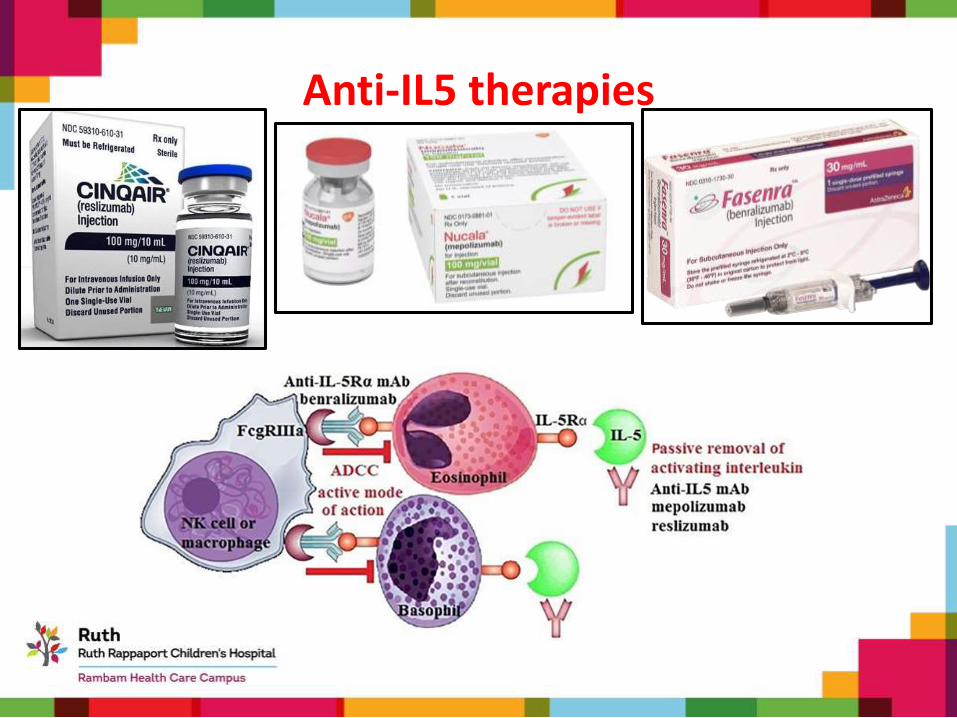
Anti-IL5 therapies

Anti-IL5 therapies

Back to our patient
Mepolizumab-הוחל טיפול ב•
יום כן יום לא, ג"מ5פרידניזון•
?מינון•

Asthma - Eosinophilic Refractory?
vsChurg–Strauss syndrome?
or
Other?










![ANTI-Ige: An Overview such as atopic dermatitis, asthma, allergic rhinitis and eosinophilic . esophagitis [6]. The response to drug treatment in asthma is a complex trait and . is](https://img.pdfslide.net/doc/110x75/5f10c73c7e708231d44ac5b3/anti-ige-an-overview-such-as-atopic-dermatitis-asthma-allergic-rhinitis-and-eosinophilic.jpg)