Embed Size (px)
Citation preview



•
•
•
•



3%
8%
25%
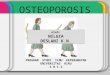
Asthma 8%
Bipolar Disorder 1.5%
Depression 30%
Diabetes 11%
Epilepsy 3%
Heart problems 1.5%
Multiple Sclerosis 1.5%
Osteoporosis 8%
Schizophrenia 3%
Spina Bifida 1.5%
Visual Impairment 6%
55%
4%
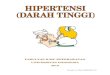
Hot stone massage 25%
Reiki 10%
Indian head massage 6%


Figure 3: Gender of participants
83% Women
17% Men
Figure 4: Age of participants
7% 80-84
12% 75-80
20% 66-74
23% 55-65
22% 45-54
12% 35-441% 26-34
3% 85+
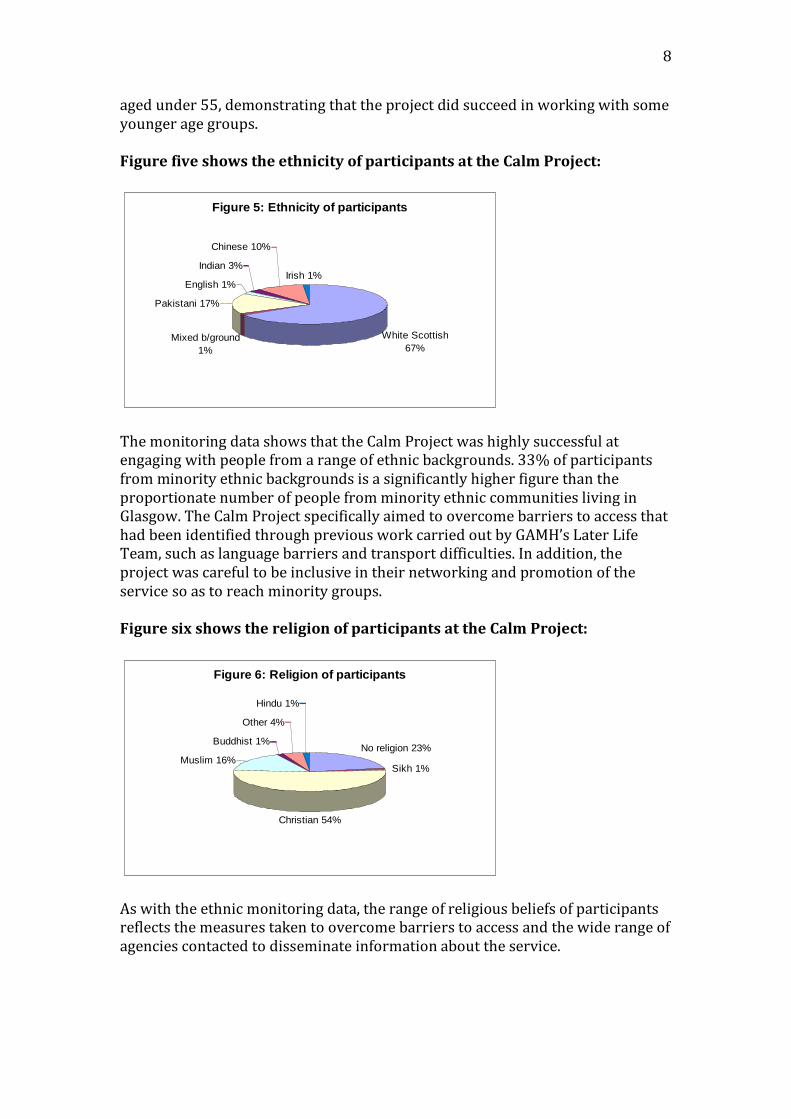
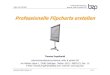
Figure 5: Ethnicity of participants
Indian 3%
Chinese 10%
Irish 1%
White Scottish
67%Mixed b/ground
1%
Pakistani 17%
English 1%
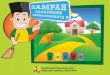
Figure 6: Religion of participants
Muslim 16%
Other 4%
Buddhist 1%
Christian 54%
Sikh 1%
No religion 23%
Hindu 1%

Figure 7: Percentage of participants with a
disability
No disability
24%
Disability 76%

.







•
•


Calm Project
Assessment form
It can be hard to share information about yourself with people
that you don’t know. The information that we ask you for on
this form is to help us to find out if this service is right for you
and, if it is, to find the most appropriate therapy for you.
The information you give us will not be shared (without your
permission) with anyone outside Calm unless there is a risk to
yourself or someone else involved. We may wish to share
information to access other supports for you, instead of or in
addition to complementary therapies or mindfulness. If that
situation occurs, we will discuss this with you.
Name
What do you like to be
called?
Address
Telephone
Date of birth
How did you hear about the
Calm Project?


Complementary therapies are therapies that work alongside
conventional medicine. They usually adopt a holistic approach
whereby the whole person is treated rather than just the
symptoms of an illness.
The Calm Project offers a range of complementary therapies
including Indian head massage, reflexology, massage, hot stone
massage and Reiki. Would you like further information about
what these are? (information sheets available)
Are you interested in receiving complementary therapies?
Yes No
What complementary therapies have you received in the past?
___________________________________________________
___________________________________________________
___________________________________________________
___________________________________________________
If so, can you tell us about this? (eg. what was helpful? What
was not helpful?)_____________________________________
___________________________________________________
___________________________________________________
___________________________________________________
___________________________________________________

What change would you like to experience as a result of
receiving complementary therapies?______________________
___________________________________________________
___________________________________________________
___________________________________________________
___________________________________________________
If you receive complementary therapies, would you prefer to
receive them at home or in another community setting?______
__________________________________________________
__________________________________________________
Can you tell us about this? (eg mobility problems, want to be
out of house)_______________________________________
__________________________________________________
__________________________________________________
__________________________________________________
__________________________________________________
You cannot have some complementary therapies if you have
particular health problems. We will talk about this further if you
are going to receive complementary therapies through the
project.
Mindfulness teaches greater awareness of thoughts and feelings
through simple techniques like meditation and gentle
movement. It also helps you develop ways of thinking and
living that can improve well-being.
Would you like further information about mindfulness?
(information sheet available)

Are you interested in attending a mindfulness group?
Yes No
Have you used mindfulness techniques in the past?
Yes No
If so, can you tell us about this? (eg. what was helpful? What
was not helpful?)___________________________________
_________________________________________________
_________________________________________________
_________________________________________________
What change would you like to experience as a result of
attending a mindfulness group?________________________
_________________________________________________
_________________________________________________
_________________________________________________
_________________________________________________
If you attend a mindfulness group, do you have any preference
about whether the group includes men and women, or women
only or men only?
Yes No
If yes, can you tell us about this?_______________________
_________________________________________________
_________________________________________________
_________________________________________________
_________________________________________________

If you attend a mindfulness group, would you require any
assistance with travel to and from the venue? Yes No
If yes, can you tell us about this? (eg. mobility problems)____
__________________________________________________
__________________________________________________
__________________________________________________
The mindfulness group may involve reading some simple
written information, either in handouts or on powerpoint or
flipchart in the group. We will try and keep this to a minimum.
Is reading or writing something you would require support with?
Yes No
If yes, what kind of support would be helpful?_____________
__________________________________________________
__________________________________________________
__________________________________________________
The group will run for 2 hours each week for 12 weeks. We’re
aware that this is a big commitment to make. Do you think you
would be able to attend regularly/have any concerns about being
able to attend regularly?_______________________________
__________________________________________________
__________________________________________________
__________________________________________________
If you participate in the mindfulness group, you will be offered
the opportunity to come back for a follow up session at a later
point. Is that something you would be interested in participating
in?
Yes No

Would you consider attending for a full day session for the
follow up?
Yes No
Can you tell us about any time constraints that may affect you
ability to participate in a follow up day? (eg. caring
responsibilities)_____________________________________
__________________________________________________
__________________________________________________

Risk Assessment
Can you tell me a bit about any mental health difficulties you
experience?
What things do you do on a regular basis to help you stay well
(in relation to both your physical and mental wellbeing)?

What helps you when you feel like this? What can a member of
staff or therapist do?
Are there any areas of safety/risk we should know about? (eg.
have you ever harmed or threatened to harm yourself or anyone
else, is there anything about the local area that we should know
about?)
If yes, can you tell me a bit about it?
Do you have any criminal convictions or have you ever had any
incidents involving the police that you think we should know
about?
If yes, can you tell me a bit about it?
If you aren’t feeling good or are becoming unwell how do you
know? How would we know?

Is drug or alcohol use a problem for you, or has it been in the
past?
If yes, can you tell me a bit about it?
Is there anything else about yourself that you think we should
know in order for us to support you appropriately?
Emergency Contact details
Please provide us with the names and addresses of two people
that we can contact in case of any emergency? One of these
contacts should be your GP.
Name (GP)
Address
Telephone
Name
Address
Telephone
Relationship to
you
GAMH Equal Opportunities Monitoring form
If you have difficulty reading or understanding this form please contact one of the staff at the Calm Project.
You are asked to complete this form for the purposes of
monitoring so that we can ensure our services are accessible
to everyone. The information you provide on this form
will be treated as strictly confidential. We do not ask for
your name.
None of the questions are compulsory, you may answer as
many or as few as you choose.
1. Your gender (please tick one box for each question)

Male
Female
Other
Have you ever considered yourself to be transgender?
Yes No
I prefer not to answer this question
2. Your age (please tick one box)
12 - 15
16 - 25
26 - 34
35 - 44
45 - 54
55 - 65
66 – 74
75 – 80
80 – 84
85+
I prefer not to answer this question
Confidential
3. Your ethnic background The options are listed in alphabetical order, please tick one main category and if you wish one subcategory. Please note these categories are based on the Scottish census categories.
Please tick
African, Caribbean or Black; African, Caribbean or Black Scottish; any other African, Caribbean or Black British or Black Irish
African (please specify), African Scottish, any other African British or African Irish
Caribbean, Caribbean Scottish, any other Caribbean British or Caribbean Irish

Any other African, Caribbean or Black background (please specify)
Please tick
Asian, Asian Scottish, any other Asian British or Asian Irish
Bangladeshi, Bangladeshi Scottish, Bangladeshi Irish, any other Bangladeshi British
Indian, Indian Scottish, Indian Irish or any other Indian British
Pakistani, Pakistani Scottish, Pakistani Irish or any other Pakistani British
Any other Asian background (please specify)
Please tick
Chinese, Chinese Scottish, Chinese Irish, Chinese British
Any other Chinese background (please specify)
Confidential Please tick
Gypsy/Traveller
Irish Traveller
New Traveller
Roma
Scottish Gypsy/Traveller
Showperson
Any other Gypsy/Traveller background (please specify)
Please tick
White
British

English
Irish
Northern Irish
Scottish
Welsh
Polish
Any other white background (please specify)
Please tick
Mixed or multiple background
Any mixed or multiple background (please specify)
Please tick
Other ethnic background
Any other background (please specify)
I prefer not to answer this question
Confidential
4. Your current religion or belief
No religion
Bahai
Buddhist
Christian
Hindu
Humanist
Jain
Jewish
Muslim
Pagan
Sikh
Other

I prefer not to answer this question
5. Your sexual orientation
Bisexual
Gay man/ homosexual
Lesbian / Gay woman
Heterosexual / straight
Other
I prefer not to answer this question
6. Caring Responsibilities: Are you responsible for caring for a family member or other person?
Yes
No
I prefer not to answer this question
Confidential 7. Disability
Definition of Disability The Disability Act 1995 & 2005 protects disabled people. It defines a person as disabled if they ‘have a physical or mental impairment, which has a substantial and long term (i.e. has lasted, or is expected to last at least 12 months) and has an adverse effect on the person’s ability to carry out day to day activities.’ Do you consider yourself to have a disability according to the definition given in the Disability Discrimination Act described above?
Yes
No

Please state the type of impairment which applies to you. People may experience more than one type of disability or impairment, in which case please tick more than one box.
Physical disability or impairment
Visual disability or impairment, such as serious visual impairment, being blind.
Deafened, deaf, hard of hearing
Deaf BSL
Mental Health problem, such as depression
Learning disability or difficulty such as dyslexia, autism, Down’s syndrome; or head injury
Long-standing illness or health condition, such as cancer, HIV, diabetes, chronic heart disease or epilepsy
Other disability or impairment, such as disfigurement (please specify)
I prefer not to answer this question
Confidential 8. Immigration status Asylum seeker
Yes
No
Refugee
Yes
No
I prefer not to answer this question

Thank you for taking the time to complete this information. It is helpful to us in making our service accessible to everyone.
Calm Project
Review Form


1 2 3 4
Quite Indifferent Mostly Very
dissatisfied or mildly satisfied satisfied
dissatisfied
Comments

Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good
Very Poor Poor Okay Good Very Good

Very Poor Poor Okay Good Very Good