Embed Size (px)
Citation preview

R3 Comference
報告 : R3 李廣祚

Patient Profile
Name 傅 x xAge 30 years oldGender femaleNumber 8xxxxxx

Background History
Amenorrhea, under hormone therapy and induced menstruation in Gyn OPD since 2009
Pregnancy GA 14+ weeks

LMP : 2011-07-20 (induced)
2011/08Icon (+), stop E2 and P supplement
Then, she received first time CBC exam in 2011/10

2011/10/08
WBC 5.2 1000/uL RBC 4.39 million/uL Hemoglobin Hemoglobin 12.2 12.2 g/dLg/dLHematocrit 36.1 %MCV 82.2 fL MCH 27.8 pg/Cell MCHC 33.8 gHb/dL RDW 13.7 % Platelets Platelets 45 45 1000/uL1000/uL

2011/11/03
Intermittent low grade fever for 3-4 weeksMultiple petechiae and ecchymosis at trunk and limbs.

No travel history within recent monthsNo URI symptom, productive cough, dysuria, diarrhea, dysuria, or abdominal painNo tarry stoolNo hypertensionNo general or lower limbs edemaNo self medication or herb usage

WBC 7.7 1000/uL RBC 2.54 million/uL Hemoglobin Hemoglobin 7.4 7.4 g/dLg/dLHematocrit 21.3 %MCV 83.9 fL RDW 17.4 % Platelets Platelets 5 5 1000/uL1000/uL

Nucleated RBC 0.9 /100 WBC Atypical-Lympho 1.0 % Myelocyte 1.0 % Segment 84.0 % Lymphocyte 6.0 % Monocyte 8.0 %

P.T 10.7 sec Nor.plasma mean 10.5 sec INR 1.0
APTT 31.9 sec Nor.plasma mean 28.5 sec

Creatinine(B) 0.46 mg/dL D.Bilirubin 0.4 mg/dL Total Bilirubin 1.7 mg/dLTotal Bilirubin 1.7 mg/dL AST/GOT 45 U/L ALT/GPT 39 U/L Na(Sodium) 134 mEq/L K(Potassium) 3.7 mEq/L LDH LDH 887.0 U/L887.0 U/L

Then, blood smear was done, and steroid therapy had been started in ER
Prednisolone 5mg/tab 2 PC QID
However, progressive anemia occurred on 11/05:

WBC 9.6 1000/uL RBC 1.84 million/uL Hemoglobin Hemoglobin 5.5 5.5 g/dLg/dLHematocrit 16 %RDW 20.7 % Platelets Platelets < 5 < 5 1000/uL1000/uLReticulocyte Reticulocyte 9.19.1

Fibrinogen 191
D-dimer D-dimer 21202120
LDH LDH 1422.01422.0
Urinalysis : No proteinuria

Then, RBC 2u transfusion was done, and she had been admitted in Hematology ward since 11/05

Physical Examination
Conscious: clearPale conjunctivaNo palpable lymph nodeNo palpable spleen or liverPetechiae and ecchymosis over bil. lower limb and upper limb

Past history
Hyperprolactinemia without definite diagnosis, under regular following up in Meta OPD till 2008/12
No previous pregnancy record

Approach to Thrombocytopenia
Under-productionNutritional deficiencyAbnormalities within bone marrow
Increased peripheral destructionHypersplenismImmune-mediated destructionNon-immune-medicated destruction

Under Production
Nutritional deficiencyNot favored by history and onset time
Bone marrow abnormalitiesAbsent leukoerythroblastic pictureNo leukopenia

Increased peripheral destruction
HypersplenismNo palpable spleen
Immune-mediated destructionAutoimmune disorder : possibleSystemic infection : less likelyIdiopathic thrombocytopenia : less likely due to concurrent severe anemia

Non-immune-medicated destructionPre-eclampsia, HELLP : possibleTTP : possibleDIC
No evidence of sepsis or metastatic malignancyNo coagulopathy

Initial Impression
Severe thrombocytopenia with anemia, possibly :
Pre-eclampsia or HELLP syndromeThrombotic thrombocytopenic purpuraSystemic lupus erythematosus or other autoimmune disorderBone marrow disorder

Steroid was titrated up to Methylprednisolone 40mg 1pc IV Q12H since 11/05, and blood test was followed on 11/07 :

2011/11/07
WBC 8.962 1000/uL RBC 1.59 million/uL Hemoglobin Hemoglobin 5.2 5.2 g/dLg/dLHematocrit 14.1 %MCV 83.9 fL RDW 21.6 % Platelets Platelets 3 3 1000/uL1000/uLReticulocyteReticulocyte 22.522.5

ANA ( 1:640 ) (Speckled) A-DSDNA < 40.5 (Negative)C3, C4 (not decreased)
D-COOMBS D-COOMBS NegativeNegative Anti-Cardiolipin Negative
Bilirubin (D) 0.4Bilirubin (T) 0.5LDHLDH 19201920

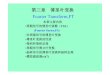
Peripheral Blood Smear (11/07)

Schistocytes

Schistocytes

ImpresssionMicroangiopathic hemolytic anemiaMarkedly thrombocytopenia

Impression - Revised
Severe thrombocytopenia with anemia, possibly :
Pre-eclampsia or HELLP syndromeThrombotic thrombocytopenic purpuraSystemic lupus erythematosus or other autoimmune disorderBone marrow disorder

Hb 5.5 = 5.2 = 8.4Platelet <5000 = 3000 = 3000AST 66 = 59 = 47Bilirubin 1.4 = 1.5 = 1.7LDH 1422 = 1920 = 1850
Plasma Plasma ExchangeExchange

2011/11/09
No obvious response to steroid, start plasma exchange, QOD x 5 course(9, 11, 14, 16, 18)

Hb = 8.5 = = 8.9Platelet
= 22000 = = 100000
AST = 21 = = =Bilirubin = 0.8 = = =LDH = 646 = = =
Plasma Plasma ExchangeExchange
Plasma Plasma ExchangeExchange

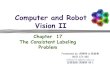
Peripheral Blood Smear (11/15)


11/07 11/15

Hb = = 8.6 = 9.3
Platelet = = 71000 = 39000
AST = = = = =
Bilirubin = = 0.6 = =
LDH = = 198 = =
Plasma Plasma ExchangeExchange
Plasma Plasma ExchangeExchange

The response to plasma exchange was not consistently. The dosage was titrated up to QD since 11/20 - 11/24.

Hb = 9.5 = = 10.3Platelet = 67000 = = 148000AST = = = = 18Bilirubin = = = = 0.3LDH = = = = 157
Plasma Plasma ExchangeExchange
Plasma Plasma ExchangeExchange
Plasma Plasma ExchangeExchange
Plasma Plasma ExchangeExchange
Plasma Plasma ExchangeExchange

11/28Hb 10.8Platelet 207000
Plasma Exchange was tapered to QOD:11/28, 11/30, 12/02, 12/04
Steroid was tapered (12/05)From Methylprednisolone 40mg IV Q12H, To Methylprednisolone 4mg/tab 4PC QID

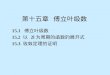
Peripheral Blood Smear (12/05)


While Discharge(12/08)
WBC 8400
Segment 83%
Lymphocyte
10%
Hb 11.6
RDW 15.5
Platelet Platelet 179000179000
Bilirubin (T) 0.3
AST 15
LDH 182

Final Diagnosis
Pregnancy-related Thrombotic
Thrombocytopenic Purpura

Difficult Decision
Since plasma exchange might be harmful to pregnant woman and fetus, how could we improve our decision making ?

Some Questions
Pathogenesis and definition of TTP ?
TTP and pregnancy ?
Some diseases which mimic TTP during pregnancy; how to differentiate them ?

Pathogenesis

ADAMTS13 deficiency (A Disintegrin And Metalloprotease with a ThromboSpondin type 1 motif, member 13)
Low plasma level Presence of Autoantibody or Inhibitor
Endothelial injury, increased platelet aggregation, and genetic factors …
MOAKE. Thrombotic microangiopathiesThrombotic microangiopathies. N Engl J Med, Vol. 347, No. 8·August 22, 2002


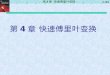
ADAMTS13 in Pregnancy
Mannucci PM, Canciani MT, Forza I, Lussana F, Lattuada A, Rossi E. Changes in hChanges in health and disease of the metalloproteaealth and disease of the metalloprotease that cleaves von Willebrand factorse that cleaves von Willebrand factor. Blood. 2001 Nov 1;98(9):2730-5.




The protein seems to be infuenced by hihigh levels of estrogensgh levels of estrogens because plasma levels decreased progressively from the first trimester of pregnancy.

Differential Diagnosis

Pre-eclampsia / EclampsiaHELLP syndromeSepsisExacerbation of SLE …

Pre-eclampsiaAbnormalities in the development of pAbnormalities in the development of placental vasculaturelacental vasculature early in pregnancy may result in relative placental underpeplacental underperfusion/hypoxia/ischemiarfusion/hypoxia/ischemia, which then leads to release of antiangiogenic factors into the maternal circulation that alter maternal systemic endothelial function and cause manifestations of the disease.



HELLP syndrome
Unknown etiology; probably severe form of preeclampsia
Microangiopathic hemolytic anemia Platelet count ≤100,000 cells/microLTotal bilirubin ≥1.2 mg/dLSerum AST ≥70 IU/L

The onset of TTP tends to be earlier in gestation First trimester : 12 percentSecond trimester : 56 percent Third trimester/postpartum : 33 percent
Preeclampsia-HELLP does not occur before 20 weeks of gestation and most cases are diagnosed in the third trimester
Martin JN Jr, Bailey AP, Rehberg JF, Owens MT, Keiser SD, May WL. Thrombotic thrombocytopenic purpura in 166 pregnancies: 1955-2006. Am J Obstet Gynecol. 2008 Aug;199(2):98-104. Epub 2008 May 23.

HELLP is associated with thrombocytopenia, and in severe cases, there may be DIC with the attendant prolongation of the PT and aPTT.
The percentage of schistocytespercentage of schistocytes on peripheral smear is often higher in TTP (2 to 5 percent) than in HELLP (less than 1 percent)
Stella CL, Dacus J, Guzman E, Dhillon P, Coppage K, How H, Sibai B. The diagnostic dilemma of thrombotic thrombocytopenic purpura/hemolytic uremic syndrome in the obstetric triage and emergency department: lessons from 4 tertiary hospitals. Am J Obstet Gynecol. 2009 Apr;200(4):381.e1-6. Epub 2008 Dec 25.


Sibai BM. Imitators of severe pre-eclampsiaImitators of severe pre-eclampsia. Semin Perinatol. 2009 Jun;33(3):196-205.


Following Delivery
Pre-eclampsia / HELLPAlmost all women spontaneously recovered platelet count > 100000 by 5 days after delivery
HELLPAll recovered by postpartum day 11

So …
If thrombotic microangiopathy :First and Second trimester < GA 20w
Consider TTP
Second trimester > GA 20More consideration
Third trimesterEvaluate the possibility of successful deliveryObserve course after delivery

Initiation of Plasma Exchange
McMinn JR, George JN. Evaluation of women with clinicaEvaluation of women with clinically suspected thrombotic thrombocytopenic purpura-hlly suspected thrombotic thrombocytopenic purpura-hemolytic uremic syndrome during pregnancy.emolytic uremic syndrome during pregnancy. J Clin Apher. 2001;16(4):202-9.

Thanks For Your Thanks For Your ListeningListening