Embed Size (px)
Citation preview
香港醫學會THE HONG KONG
MEDICAL ASSOCIATION
www.hkmacme.org May 2015
持 續 醫 學 進 修 專 訊B U L L E T I N
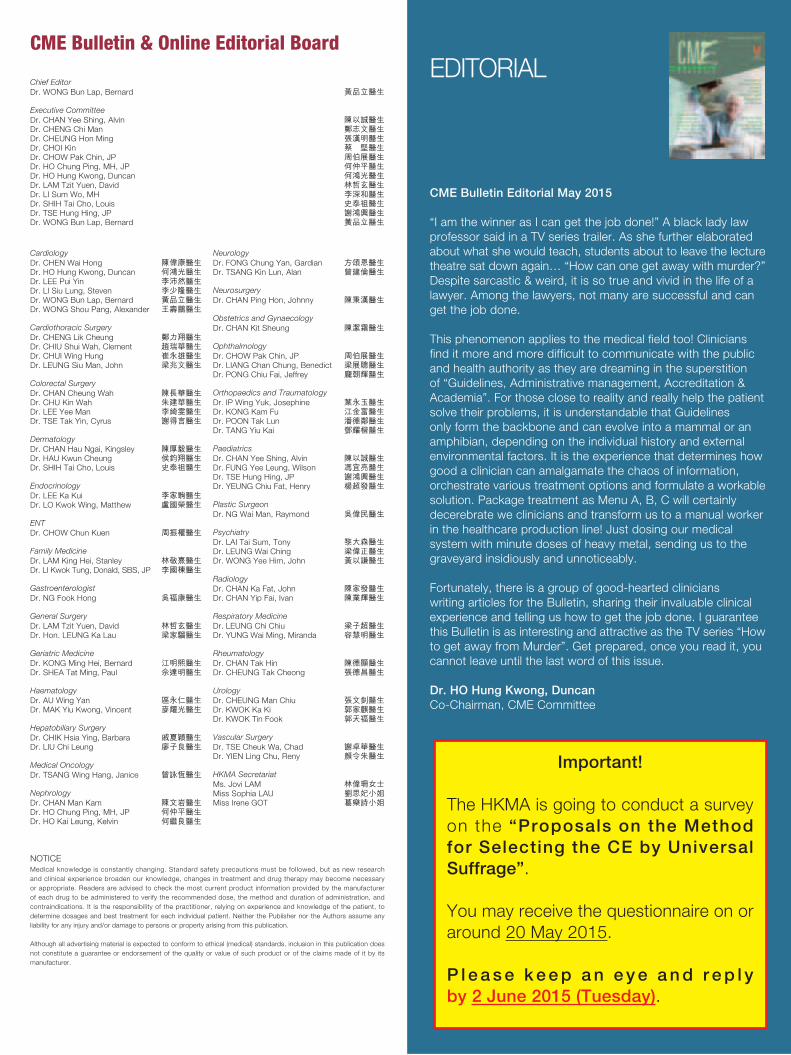
Overview ofChronic Kidney
Disease in Elderly
Patients-A Local Perspective
by Dr. TSE Kai Chung
Dr. LAM Chi Leung
Prof. Helen CHIU
Mind the Gap: Assessing
Financial Capacity for the Elderly
Dr. CHUI Wing Hung
Video-assisted Thoracoscopic Lobectomy and Sublobar Resection for Early Non-small Cell Lung Cancer
HKMA Constitutional Reform Survey in MayPage 1 – Editorial page

HKMA CME Bulletin
Editorial 1
Spotlight 1 2Overview of Chronic Kidney Disease in Elderly Patients – A Local Perspective
Spotlight 2 5Video-assisted Thoracoscopic Lobectomy and Sublobar Resection for Early Non-small Cell Lung Cancer
Spotlight 3 11Mind the Gap: Assessing Financial Capacity for the Elderly
Cardiology 19A Patient with Acute Pulmonary Edema
Dermatology 22A 10-year-old Boy With Itchy Skin Rash Over Body and Limbs
Complaints & Ethics 23
Answer Sheet 25
CME Notifications 26
Meeting Highlights 32
CME Calendar 35
Contents
持續醫學進修專訊
Advertising Enquiry: 2527 8452 Fax: 2865 0943 / Email: [email protected]
HKMA CME Enquiry Hotline
Tel: 2527 8452 / 2861 1979
The Hong Kong Medical Association is dedicated to providing a coordinated CME
programme for all members of the medical profession. Under the HKMA CME
Programme, a CME registration process has been created to document the CME
efforts of doctors and to provide special CME avenues. The Association strives to
foster a vibrant environment of CME throughout the medical profession. Both members
as well as non-members of the Association are welcome to join us. You may contact
the HKMA Secretariat for details of the programme.
Please read the fol lowing art icles and answer the
questions. Participants in the HKMA CME Programme
will be awarded credit points under the Programme
for returning the completed answer sheet v ia fax
(2865 0943) or by mail to the HKMA Secretariat on
or before 15 June 2015. Answers to questions will
be provided in the next issue of the HKMA CME
Bulletin. (Questions may also be answered online at
www.hkmacme.org)
HKMA CME Bulletin – MONTHLY SELF-STUDY
SERIES to help you grow!
香港醫學會體察到業界有必要設立完善的持續進修計劃,致力推動持續醫學進修,為同僚建立有系統的進修記錄機制,以及為全科醫生提供適切的進修課程。藉著這個計劃,我們期望將優良的進修傳統推展至醫學界中每一角落,同時為業界締造一個充滿活力的進修文化。我們誠意邀請您參與醫學會持續進修計劃,不論您是否醫學會的會員,均歡迎您同來與我們一起學習,以及享用醫學會為所有醫生設立的進修記錄機制。如欲了解香港醫學會持續醫學進修計劃的詳情,請聯絡本會秘書處查詢。
請細閱本期文章,並利用答題紙完成自我評估測驗,於2015年6月15日前,將已填妥之答題紙傳真(號碼:2865 0943)或寄回本會秘書處,您將可獲持續醫學進修的積分點; 至於是期自我評估測驗之答案,將刊於下一期《持續醫學進修專訊》之中。(您亦可透過網站www.hkmacme.org 完成自我評估測驗)
Spotlight 3Mind the Gap: Assessing
Financial Capacity for the
Elderly
Spotlight 1Overview of Chronic
Kidney Disease in
Elderly Patients –
A Local Perspective
Spotlight 2Video-assisted
Thoracoscopic Lobectomy
and Sublobar Resection
for Early Non-small Cell
Lung Cancer
NOTICEMedical knowledge is constantly changing. Standard safety precautions must be followed, but as new research
and clinical experience broaden our knowledge, changes in treatment and drug therapy may become necessary
or appropriate. Readers are advised to check the most current product information provided by the manufacturer
of each drug to be administered to verify the recommended dose, the method and duration of administration, and
contraindications. It is the responsibility of the practitioner, relying on experience and knowledge of the patient, to
determine dosages and best treatment for each individual patient. Neither the Publisher nor the Authors assume any
liability for any injury and/or damage to persons or property arising from this publication.
Although all advertising material is expected to conform to ethical (medical) standards, inclusion in this publication does
not constitute a guarantee or endorsement of the quality or value of such product or of the claims made of it by its
manufacturer.
EDITORIAL
CME Bulletin Editorial May 2015
“I am the winner as I can get the job done!” A black lady law
professor said in a TV series trailer. As she further elaborated
about what she would teach, students about to leave the lecture
theatre sat down again… “How can one get away with murder?”
Despite sarcastic & weird, it is so true and vivid in the life of a
lawyer. Among the lawyers, not many are successful and can
get the job done.
This phenomenon applies to the medical field too! Clinicians
find it more and more difficult to communicate with the public
and health authority as they are dreaming in the superstition
of “Guidelines, Administrative management, Accreditation &
Academia”. For those close to reality and really help the patient
solve their problems, it is understandable that Guidelines
only form the backbone and can evolve into a mammal or an
amphibian, depending on the individual history and external
environmental factors. It is the experience that determines how
good a clinician can amalgamate the chaos of information,
orchestrate various treatment options and formulate a workable
solution. Package treatment as Menu A, B, C will certainly
decerebrate we clinicians and transform us to a manual worker
in the healthcare production line! Just dosing our medical
system with minute doses of heavy metal, sending us to the
graveyard insidiously and unnoticeably.
Fortunately, there is a group of good-hearted clinicians
writing articles for the Bulletin, sharing their invaluable clinical
experience and telling us how to get the job done. I guarantee
this Bulletin is as interesting and attractive as the TV series “How
to get away from Murder”. Get prepared, once you read it, you
cannot leave until the last word of this issue.
Dr. HO Hung Kwong, Duncan
Co-Chairman, CME Committee
CME Bulletin & Online Editorial Board
Chief Editor
Dr. WONG Bun Lap, Bernard 黃品立醫生
Executive Committee
Dr. CHAN Yee Shing, Alvin 陳以誠醫生Dr. CHENG Chi Man 鄭志文醫生Dr. CHEUNG Hon Ming 張漢明醫生Dr. CHOI Kin 蔡 堅醫生Dr. CHOW Pak Chin, JP 周伯展醫生Dr. HO Chung Ping, MH, JP 何仲平醫生Dr. HO Hung Kwong, Duncan 何鴻光醫生Dr. LAM Tzit Yuen, David 林哲玄醫生Dr. LI Sum Wo, MH 李深和醫生Dr. SHIH Tai Cho, Louis 史泰祖醫生Dr. TSE Hung Hing, JP 謝鴻興醫生Dr. WONG Bun Lap, Bernard 黃品立醫生
Cardiology
Dr. CHEN Wai Hong 陳偉康醫生Dr. HO Hung Kwong, Duncan 何鴻光醫生Dr. LEE Pui Yin 李沛然醫生Dr. LI Siu Lung, Steven 李少隆醫生Dr. WONG Bun Lap, Bernard 黃品立醫生Dr. WONG Shou Pang, Alexander 王壽鵬醫生
Cardiothoracic Surgery
Dr. CHENG Lik Cheung 鄭力翔醫生Dr. CHIU Shui Wah, Clement 趙瑞華醫生Dr. CHUI Wing Hung 崔永雄醫生Dr. LEUNG Siu Man, John 梁兆文醫生
Colorectal Surgery
Dr. CHAN Cheung Wah 陳長華醫生Dr. CHU Kin Wah 朱建華醫生Dr. LEE Yee Man 李綺雯醫生Dr. TSE Tak Yin, Cyrus 謝得言醫生
Dermatology
Dr. CHAN Hau Ngai, Kingsley 陳厚毅醫生Dr. HAU Kwun Cheung 侯鈞翔醫生Dr. SHIH Tai Cho, Louis 史泰祖醫生
Endocrinology
Dr. LEE Ka Kui 李家駒醫生Dr. LO Kwok Wing, Matthew 盧國榮醫生
ENT
Dr. CHOW Chun Kuen 周振權醫生
Family Medicine
Dr. LAM King Hei, Stanley 林敬熹醫生Dr. LI Kwok Tung, Donald, SBS, JP 李國棟醫生
Gastroenterologist
Dr. NG Fook Hong 吳福康醫生
General Surgery
Dr. LAM Tzit Yuen, David 林哲玄醫生Dr. Hon. LEUNG Ka Lau 梁家騮醫生
Geriatric Medicine
Dr. KONG Ming Hei, Bernard 江明熙醫生Dr. SHEA Tat Ming, Paul 佘達明醫生
Haematology
Dr. AU Wing Yan 區永仁醫生Dr. MAK Yiu Kwong, Vincent 麥耀光醫生
Hepatobiliary Surgery
Dr. CHIK Hsia Ying, Barbara 戚夏穎醫生Dr. LIU Chi Leung 廖子良醫生
Medical Oncology
Dr. TSANG Wing Hang, Janice 曾詠恆醫生
Nephrology
Dr. CHAN Man Kam 陳文岩醫生Dr. HO Chung Ping, MH, JP 何仲平醫生Dr. HO Kai Leung, Kelvin 何繼良醫生
Neurology
Dr. FONG Chung Yan, Gardian 方頌恩醫生Dr. TSANG Kin Lun, Alan 曾建倫醫生
Neurosurgery
Dr. CHAN Ping Hon, Johnny 陳秉漢醫生
Obstetrics and Gynaecology
Dr. CHAN Kit Sheung 陳潔霜醫生
Ophthalmology
Dr. CHOW Pak Chin, JP 周伯展醫生Dr. LIANG Chan Chung, Benedict 梁展聰醫生Dr. PONG Chiu Fai, Jeffrey 龐朝輝醫生
Orthopaedics and Traumatology
Dr. IP Wing Yuk, Josephine 葉永玉醫生Dr. KONG Kam Fu 江金富醫生Dr. POON Tak Lun 潘德鄰醫生Dr. TANG Yiu Kai 鄧耀楷醫生
Paediatrics
Dr. CHAN Yee Shing, Alvin 陳以誠醫生Dr. FUNG Yee Leung, Wilson 馮宜亮醫生Dr. TSE Hung Hing, JP 謝鴻興醫生Dr. YEUNG Chiu Fat, Henry 楊超發醫生
Plastic Surgeon
Dr. NG Wai Man, Raymond 吳偉民醫生
Psychiatry
Dr. LAI Tai Sum, Tony 黎大森醫生Dr. LEUNG Wai Ching 梁偉正醫生Dr. WONG Yee Him, John 黃以謙醫生
Radiology
Dr. CHAN Ka Fat, John 陳家發醫生Dr. CHAN Yip Fai, Ivan 陳業輝醫生
Respiratory Medicine
Dr. LEUNG Chi Chiu 梁子超醫生Dr. YUNG Wai Ming, Miranda 容慧明醫生
Rheumatology
Dr. CHAN Tak Hin 陳德顯醫生Dr. CHEUNG Tak Cheong 張德昌醫生
Urology
Dr. CHEUNG Man Chiu 張文釗醫生Dr. KWOK Ka Ki 郭家麒醫生Dr. KWOK Tin Fook 郭天福醫生
Vascular Surgery
Dr. TSE Cheuk Wa, Chad 謝卓華醫生Dr. YIEN Ling Chu, Reny 顏令朱醫生
HKMA Secretariat
Ms. Jovi LAM 林偉珊女士Miss Sophia LAU 劉思妃小姐Miss Irene GOT 葛樂詩小姐
Important!
The HKMA is going to conduct a survey
on the “Proposals on the Method
for Selecting the CE by Universal
Suffrage”.
You may receive the questionnaire on or
around 20 May 2015.
P l e a s e k e e p a n e y e a n d r e p l y
by 2 June 2015 (Tuesday).

2 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -1
Overview of Chronic Kidney Disease in Elderly Patients – A Local Perspective
hour urine collection. Creatinine clearance can then
be stratified using the international staging of CKD by
the National Kidney Foundation, and an arbitrary cut
off of GFR below 60ml/min/1.73m2 for more than 3
months is used for definition of CKD and below 15ml/
min/1.73m2 as definition for kidney failure [2,3] (Table).
This system is simple to use, but there are special
considerations in elderly patients. The normal GFR for
adults is approximately 120-130ml/min/1.73m2 and
depends on age, sex and body size, but there are
considerable variations even among normal individuals
[4]. With normal aging, there is a variable decline in
creatinine clearance, with an approximate drop of
creatinine clearance by 1ml/min/1.73m2 per year from
age 30 onwards. In this context, some patients who
are old enough may have creatinine clearance below
the threshold for CKD cutoff. This is attr ibuted to
normal aging and does not necessarily reflect genuine
CKD. It is therefore important to document evidence
of chronic kidney damage in addition to low creatinine
clearance in these elderly patients to define CKD.
This will include simple assessment by urine routine,
microscopy, assessment of proteinuria (or albuminuria)
and ultrasound (USG) imaging of kidneys. Abnormal
urinary casts, microscopic hematuria and proteinuria
are important clues of underlying CKD. USG kidneys
wi l l a lso document ev idence of chronic damage
including small kidney size, cortical thinning, loss of
corticomedullary differentiation and may give specific
diagnosis of CKD, e.g. polycystic kidney disease,
obstructive uropathy, etc. Among these tests proteinuria
is the most important factor for chronic kidney damage,
and renal biopsy is sometimes necessary for patients
with heavy proteinuria for definitive diagnosis. In the
circumstance of elderly patients with GFR < 60ml/
min/1.73m2 without evidence of chronic kidney damage,
they should not be labelled as having CKD.
Introduction
T h e b u r d e n o f c h r o n i c k i d n e y d i s e a s e ( C K D )
i s increas ing in the loca l popu la t ion. I t may be
unrecognized in the early stage as patient may be
asymptomatic or having non-specific symptoms only.
There is an increasing trend in the overall number of
patients with end stage renal failure (ESRF) entering
into the dialysis program in the public sector in the past
decades with more patients belonging to the 75+ age
group [1]. This number does not include patients who
are managed in the private sector, with a significant
proport ion being elderly patients, some of whom
are declined long term dialysis due to old age in the
public sector and come to private sector for long term
hemodialysis (HD). The overall increase in prevalence
of CKD is partly due to a longer life expectancy in the
population with improved standard of life and a higher
prevalence of hypertension (HT), diabetes mellitus (DM)
and atherosclerosis related disease in elderly patients.
Assessment of renal function in elderly patients
In the primary health care setting, routine blood tests
may identify patients with elevated serum creatinine
and raise suspicion for CKD. However, there are other
causes of high serum creatinine apart from genuine
impairment of kidney function. On the other hand, a
normal serum creatinine in elderly patients may not
truly ref lect normal renal function due to reduced
muscle mass commonly seen in old age. A more
accurate assessment of glomerular filtration rate (GFR)
using creatinine clearance is therefore necessary.
In this regard, common methods for assessment of
creatinine clearance include calculation equations
such as the Cockcroft-Gault formula or abbreviated
MDRD study equation and measurement using 24
Dr. TSE Kai ChungMBBS (Hons), MRCP (UK), FHKCP, FHKAM,
FRCP (Edin), FRCP RCPS (Glasg)
Staff Consultant, St. Paul’s Hospital

3HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -1
Management of CKD
Regardless of etiology, elderly patients with confirmed
CKD should be managed with diet control with protein
restriction but one may need to balance the risk of
malnutr it ion and renal protection, and referral for
dietitian assessment may be necessary. More stringent
blood pressure (BP) control to aim for BP target of <
130/80 and control of proteinuria are also important as
both are risk factors linked to more rapid progression
of CKD. In this regard, angiotensin inhibition drugs
are usually the first line medical therapy for their dual
antihypertensive and proteinuria reduction effect.
Even in normotensive patients with proteinuric CKD,
angiotensin inhibition therapy should also be given if
tolerated for renal protection. There is no therapeutic
advantage of angiotensin converting enzyme inhibitor,
angiotensin blocker or renin inhibitor over one another
and choice of medication really depends on their side
effect profile, price and physician’s preference. The use
of combination of angiotensin inhibition drugs, however,
remains controversial. In any case, close monitoring
during initiation of angiotensin inhibition therapy is
important for potential side effects of hyperkalemia and
transient increase in serum creatinine in the initial stage
of therapy.
Specif ic management of CKD is directed towards
the underlying cause. In elderly patients, common
causes of CKD include DM nephropathy, HT related
kidney disease and chronic glomerulonephritis (GN).
These shou ld be managed accord ing ly and DM
should best be managed by insulin injection to achieve
optimal control. In patients with chronic GN, steroid
or immunosuppressive agents may sometimes be
necessary, but once again this needs close monitoring
for the risk of serious infections in elderly patients.
For elderly patients with a low creatinine clearance in
whom no definite cause of CKD is identified, no specific
therapy is required. However, they are more susceptible
to various nephrotoxic insults and are more prone to
acute kidney injury. Common scenarios include use
of non-steroidal anti-inflammatory drugs (NSAID) for
treatment of common conditions in elderly patients
and intravenous contrast for computer tomogram
examination. One should therefore have caution and
prescribe these agents only when necessary.
Renal replacement therapy in elderly patients
In elderly patients with ESRF, decision should be made
regarding conservative therapy or renal replacement
therapy (RRT). Life expectancy, social support, quality of
life and personal decision should be taken into account.
While elderly patients may still be considered for long
term dialysis, renal transplantation is in general not an
option due to scarcity of cadaveric kidneys in Hong
Kong.
From a local perspective, there is an increasing number
of elderly patients with ESRF started on dialysis and
most of them are doing peritoneal dialysis (PD) in the
public sector. It is generally held true that PD is more
cardiovascular friendly in elderly patients in whom a
higher prevalence of underlying cardiovascular disease
is expected, and thus PD is more suitable for them
compared with HD. However, there are also elderly
patients who opt for long term HD in the private sector
either out of their own choice or because they are
declined PD in the public sector. Compared with their
younger counterparts, there is a higher proportion of
elderly patients using Gortex graft or tunneled catheters
for long term HD due to more frequent access problems
related to arteriovenous fistula (AVF) in elderly patients,
but it is generally observed that most of them in fact
tolerate HD quite well with a reasonable quality of life.
This may be related to better technological advances
in HD therapy such as use of dialyzers with more
biocompatible membranes, hemodiafiltration, body
composition monitoring allowing better assessment
of dry weight and online blood volume monitoring to
prevent excessive ultrafiltration and hence hypotension
during HD, etc. These wil l al l contr ibute to better
tolerance and hemodynamic stability during HD for
elderly patients. Local data in this aspect is limited and
further studies on the tolerability and outcomes of long
term HD in elderly patients are recommended to confirm
these observations.
4 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -1
References
1. Yiu-Wing Ho, Ka-Foon Chau, Bo-Ying Choy et al: Hong Kong Renal Registry Report 2012, Hong Kong Journal of Nephrology, Apr 2013 vol 15, issue 1, pp28-43
2. KDIGO. Summary of recommendation statements. Kidney Int 2013; 3 (Suppl): 5
3. National Kidney Foundation. K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 2002; 39 (Suppl 1): S1
4. Stevens LA, Coresh J, Greene T et al: Assessing kidney function – measured and estimated glomerular filtration rate. N Engl J Med 2006; 354: 2473
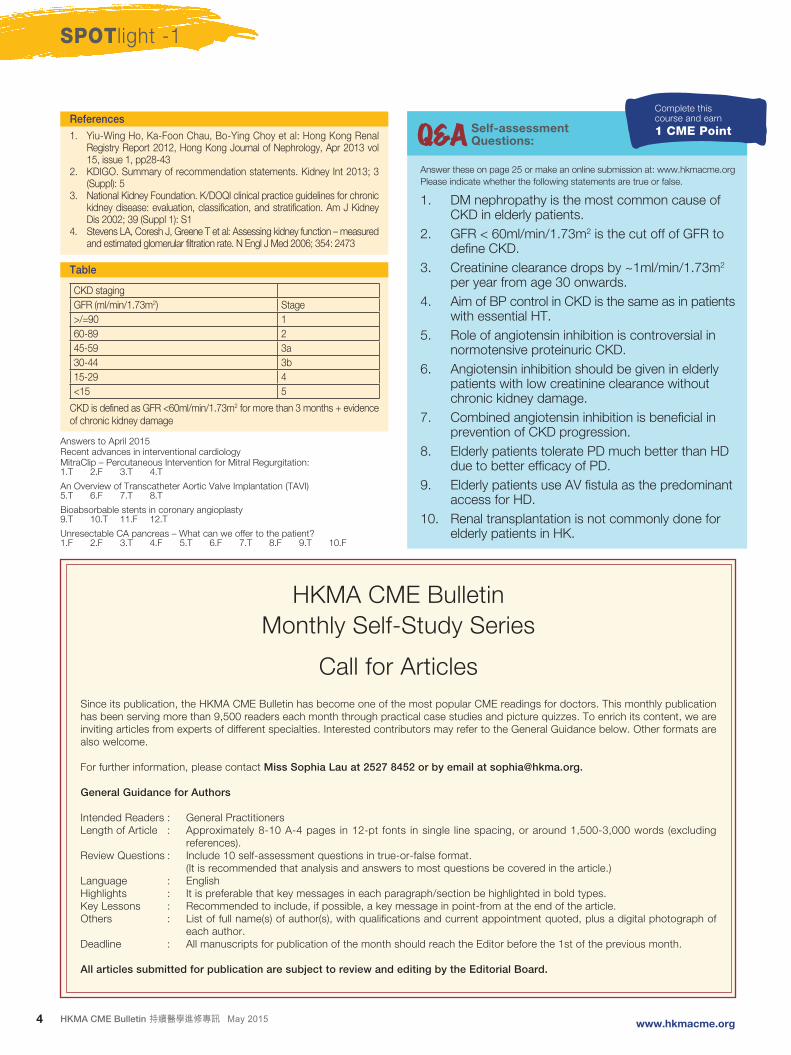
Table
CKD staging
GFR (ml/min/1.73m2) Stage
>/=90 1
60-89 2
45-59 3a
30-44 3b
15-29 4
<15 5
CKD is defined as GFR <60ml/min/1.73m2 for more than 3 months + evidence of chronic kidney damage
Answer these on page 25 or make an online submission at: www.hkmacme.org
Please indicate whether the following statements are true or false.
1. DM nephropathy is the most common cause of CKD in elderly patients.
2. GFR < 60ml/min/1.73m2 is the cut off of GFR to define CKD.
3. Creatinine clearance drops by ~1ml/min/1.73m2 per year from age 30 onwards.
4. Aim of BP control in CKD is the same as in patients with essential HT.
5. Role of angiotensin inhibition is controversial in normotensive proteinuric CKD.
6. Angiotensin inhibition should be given in elderly patients with low creatinine clearance without chronic kidney damage.
7. Combined angiotensin inhibition is beneficial in prevention of CKD progression.
8. Elderly patients tolerate PD much better than HD due to better efficacy of PD.
9. Elderly patients use AV fistula as the predominant access for HD.
10. Renal transplantation is not commonly done for elderly patients in HK.
Q&A Self-assessment Questions:
Complete thiscourse and earn
1 CME Point
Answers to April 2015Recent advances in interventional cardiologyMitraClip – Percutaneous Intervention for Mitral Regurgitation:1.T 2.F 3.T 4.T
An Overview of Transcatheter Aortic Valve Implantation (TAVI)5.T 6.F 7.T 8.T
Bioabsorbable stents in coronary angioplasty9.T 10.T 11.F 12.T
Unresectable CA pancreas – What can we offer to the patient?1.F 2.F 3.T 4.F 5.T 6.F 7.T 8.F 9.T 10.F
HKMA CME Bulletin
Monthly Self-Study Series
Call for Articles
Since its publication, the HKMA CME Bulletin has become one of the most popular CME readings for doctors. This monthly publication has been serving more than 9,500 readers each month through practical case studies and picture quizzes. To enrich its content, we are inviting articles from experts of different specialties. Interested contributors may refer to the General Guidance below. Other formats are also welcome.
For further information, please contact Miss Sophia Lau at 2527 8452 or by email at [email protected].
General Guidance for Authors
Intended Readers : General PractitionersLength of Article : Approximately 8-10 A-4 pages in 12-pt fonts in single line spacing, or around 1,500-3,000 words (excluding
references).Review Questions : Include 10 self-assessment questions in true-or-false format. (It is recommended that analysis and answers to most questions be covered in the article.)Language : EnglishHighlights : It is preferable that key messages in each paragraph/section be highlighted in bold types.Key Lessons : Recommended to include, if possible, a key message in point-from at the end of the article.Others : List of full name(s) of author(s), with qualifications and current appointment quoted, plus a digital photograph of
each author.Deadline : All manuscripts for publication of the month should reach the Editor before the 1st of the previous month.
All articles submitted for publication are subject to review and editing by the Editorial Board.
SPOTlight -2
5HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Video-assisted Thoracoscopic Lobectomy and Sublobar Resection for Early Non-small Cell Lung Cancer
Dr. CHUI Wing HungMBBS (HK), FRCS (Edin), FCSHK, FHKAM (Surgery)
Specialist in Cardiothoracic Surgery
Introduction
Surgery currently offers the greatest opportunity for
long-term cure for early stage non-small cel l lung
cancer (NSCLC) and remains the cornerstone of any
multimodality approach to locally advanced disease.
Tradit ional ly , the pr imary and preferred surgical
treatment has been performed by lobectomy or greater
resection procedures (1). Minimally invasive lobectomy
— predominantly the video-assisted thoracic surgery
(VATS) approach — has achieved equipoise with open
lobectomy in terms of safety and efficacy, and the role of
VATS continues to expand.
Although lobectomy has generally been accepted as
the standard extent of resection required for NSCLC
surgery, sublobar resections in the form of wedge
resections or segmentectomies have been reported as
an alternative surgical technique, especially in patients
with significant comorbidities or l imited pulmonary
function. Surgical leaders in the thoracic oncology
community continue to vigorously debate the relative
merits of using less invasive techniques for cancer
resection, while also re-initiating discussions of sublobar
resection in an era of screening detection of very small
and peripheral lung cancers.
Two important developments in lung cancer wi l l
challenge the thoracic surgery community to reconsider
the role of more limited pulmonary resection using a
minimally invasive approach (2). First, with the generally
longer life expectancy of the worldwide population, and
therefore the incidence of lung cancer in the elderly
population will increase; and second, the provocative
results of the National Lung Screening Trial showed that
low-dose computed tomography (LDCT) lung cancer
screening irrefutably saves lives (3). These two trends
predict that patients with lung cancer will be older
and diagnosed at an earlier stage and will therefore
most likely have a preference for less invasive surgical
intervention.
VATS lobectomy: current evidence for outcomes in
surgery for NSCLC
Numerous reports have been published over the past
decade that promote the benefits of using the VATS
approach for lung cancer resection — benefits achieved
without compromising oncological eff icacy. Early
proponents argued that VATS offered less perioperative
morbidity, shorter hospitalizations, and less surgical
stress, with decreased serum levels of measured pro-
inflammatory cytokines, implying an immunological
benefit in cancer survival over the traditional open
thoracotomy (4-8). However, most of these studies
were criticized for selection bias because patients with
smaller, peripheral tumours underwent VATS, whereas
those patients with larger, more central tumours were
resected using the traditional open approach.

SPOTlight -2
6 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
In fact, there are very few direct comparisons between
VATS lobectomy and open lobectomy approach
for lung cancer resect ion. There have only been
two small, prospective, randomized controlled trials
comparing VATS with open lobectomy (9,10). Kirby et
al randomly assigned 61 stage I lung cancer patients
to either VATS or open lobectomy and found that
postoperative air leaks were reduced in the VATS
group, with no signif icant differences observed in
operating time, intraoperative blood loss, duration of
chest tube drainage, or length of hospital stay (9). The
other prospective study, by Sugi et al, randomized 100
patients with early stage lung cancer and likewise found
no significant differences between those patients who
received VATS lobectomy and those who underwent
open thoracotomy; 5-year survival after surgery was
90% in the VATS group and 85% in the open cohort
(10). These two small randomized studies suggested
that the results of the VATS procedure were comparable
to the conventional open approach, but that VATS
did not provide the purported improvement in early
postoperative outcomes reported in multiple non-
randomized case series. The widespread acceptance
of these studies was limited by the small numbers of
patients enrolled, their single-centre design, and the
fact that they were conducted during the early VATS
experience (2).
However, as the thoracoscopic approach to lung
surgery gained popularity worldwide, a substantial
body of literature accrued — including several large
published studies and systematic reviews — promoting
the benefits of the VATS lobectomy and comparing the
VATS approach with open anatomical lung resection
(11-15). These studies have emphasized improvements
in perioperative patient outcomes (presumably due to
the limited chest wall trauma with the VATS approach),
c i t ing less pulmonary morbidity, shorter hospital
lengths of stay, and less acute postoperative pain, with
improved immediate postoperative pulmonary function.
The faster postoperative recovery and return to baseline
quality of life associated with the VATS lobectomy has
also arguably implied quicker recovery for administration
of adjuvant chemotherapy in those patients who require
it.
In a comparison of VATS lobectomy and thoracotomy,
Whitson et al collected 39 studies, with a total of 3,114
VATS patients and 3,256 thoracotomy patients, and
found statistically significant decreased chest tube
duration and hospitalization, and improved 4-year
postresection survival in the VATS group (14). A similar
review published in 2009 by Yan et al also suggested
that the VATS approach had more favourable outcomes
than open lobectomy. These authors analyzed 21
comparative studies of VATS and open resection
and found no overal l d i f ference in postoperat ive
morbidity (defined as prolonged air leaks, arrhythmia,
and pneumonia) or mortality with VATS, but did find
improvement in systemic recurrence and long-term
mortality (15). These large meta-analyses had their
limitations, however, including lack of correction for
important variables, such as surgeon experience/
expertise, and nuances of tumour characteristics not
accounted for in staging (i.e. peripheral rather than
central location).
Although the accumulated body of evidence suggests
that VATS lobectomy for early NSCLC can be safely
performed with minimal, and arguably less procedural
morbidity, the oncological equivalence of this approach
compared with the gold standard of thoracotomy has
been justifiably scrutinized (16) Central to this issue
has been the thoroughness of mediast inal lymph
node dissection and subsequent accuracy of lung
cancer staging. The lack of contemporary multicentre,
prospective, randomized controlled trials limits the
evaluat ion of the oncological ef f icacy of VATS in
retrospective studies. A number of single-institution
experiences with VATS resection have suggested that
fewer mediastinal lymph nodes have been examined
compared with the open approach, thereby potentially
understaging patients with early stage lung cancer who
might have benefited from adjuvant therapy if they had
been accurately staged. Denlinger et al found in their
relatively early VATS experience that significantly fewer
mediastinal lymph node samples were obtained with the
VATS approach compared with thoracotomy; notably,
fewer N2 nodes (particularly station 7) and N2 stations
were sampled in the VATS group (17). Other recently
published retrospective single-institution studies have

SPOTlight -2
7HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
found similar results (18,19). Despite the significant
statistical differences reported in these studies with
regard to the number of lymph nodes and nodal stations
evaluated in VATS resection vs open resection for early-
stage lung cancer, significant differences in rates of
disease-free or overall survival have not been reported.
Weighing the cumulative evidence from the past decade
evaluating the oncological efficacy of VATS lobectomy in
early NSCLC treatment, the current recommendations
by the National Comprehensive Cancer Network (NCCN)
and the American College of Chest Physicians for stage
I NSCLC propose that VATS lobectomy is not inferior
to open lobectomy when performed at experienced
centres in appropriately selected patients (20,21).
More importantly, regardless of the selected method,
a systematic approach to lymph node evaluat ion
for accurate cancer staging is paramount when
making decisions regarding multimodality treatment
requirements. NCCN guidelines recommend N1 and
N2 lymph node resection and mapping during curative
surgery, with a minimum of three different N2 stations
sampled (22).
VATS lobectomy/sublobar resection in an aging
population
NSCLC remains a disease that is especially common
in the elderly; two-thirds of NSCLC patients are older
than 65 years, with an average age at diagnosis of
70 years (23). Historically, surgeons were reluctant to
offer surgery to older patients, presumably because
of increased perioperative morbidity and mortality
independently associated with advanced age. Different
single-institution studies suggest that minimally invasive
lung cancer resect ion in the very e lder ly can be
conducted with acceptable perioperative morbidity and
mortality (24-26).
Furthermore, a l though lobectomy is the current
standard of care for early stage lung cancer, a less
invasive approach combined with limited lung resection
for curative intent may also be considered in elderly
patients with lung cancer who are too debil i tated
to undergo lobectomy but might otherwise tolerate
surgery. A less extensive lung resection using VATS
that achieves negative tumour margins is currently still
preferred over non-surgical options for treating early-
stage NSCLC when a patient is unable to tolerate
the physiological impact of a lobectomy — although
outcomes of stereotactic radiation are promising and
may provide a reasonable alternative to surgery in
some patients. On the other hand, a practical but still
unanswered question is whether healthy individuals with
very advanced age should undergo sublobar resection,
trading the oncological superiority of a lobectomy —
open or VATS — for the perceived lesser perioperative
morbidity of a resection of lesser extent. The effect of
limited resection on overall long-term functional status
and quality of life balanced with overall actuarial survival
in this cohort has not been well studied (2).
VATS sublobar resection for very small/indolent
NSCLC detected by LDCT lung cancer screening
The increasingly used LDCT lung cancer screening
programmes allow more very early stage NSCLC to be
detected. Additionally, CT imaging technology allows
better characterization and detection of subcentimetre
lung lesions, which has generated interest among
thoracic surgeons in evaluating whether lobectomy is
uniformly superior to more limited resections.
Two large retrospective studies found statistically
significant worse 5-year survival in patients with stage IA
NSCLC who underwent sublobar resection compared
with lobectomy; Chang et al found that 5-year survival
was 44% for sublobar resection compared with 61%
for anatomical resection (27), and Whitson et al found
decreased overall and cancer-specific survival in the
sublobar group compared with the lobectomy group
(28). In contrast, other investigators have not found
inferior outcomes following sublobar resections —
particularly anatomical segmentectomy — compared
with lobectomy in early stage lung cancer patients
(29-32) and this is likely to be especially true for less
invasive or more indolent cancers detected during lung
cancer screening. Although both types of sublobar
resection preserve greater lung volume than lobectomy,
wedge resections are performed without regard to
anatomical bronchial segmental anatomy and do not
allow intrapulmonary lymph node sampling, which may
SPOTlight -2
9HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
result in higher rates of cancer recurrence. Performing
segmentectomy does allow for lymph node sampling but
is technically more challenging, particularly if performed
with VATS, as it requires detailed dissection of the
bronchial segment and pulmonary arterial supply.
A number of Japanese studies have shown promising
outcomes with VATS segmentectomy (30-32). These
studies reported that VATS segmentectomy compared
favourably with VATS lobectomy and had simi lar
perioperative outcomes without evidence of increased
locoregional recurrence. Altorki et al found adjusted
10-year survival outcomes comparable to those seen
with lobectomy when sublobar resection was used
to treat early solid nodule lung cancers (clinical stage
1A tumors) identified by a lung cancer CT screening
protocol (31). At this time, larger prospective clinical
studies are needed to more decisively qualify the role
of VATS segmentectomy in early stage lung cancer;
consequently, the thoracic oncology community awaits
the completion of two randomized studies investigating
the extent of lung resection necessary — lobectomy or
sublobar resection — for optimal surgical outcomes in
early stage NSCLC (33,34).
Conclusion
The popularity of minimally invasive thoracic surgery has
expanded the surgical options that thoracic surgeons
can offer to patients with early stage lung cancer.
VATS lobectomy has been associated with decreased
perioperative morbidity, and similar rates of locoregional
recurrence and cancer-free survival can be achieved
compared with the standard open surgical procedure.
The growth of the elderly population and the support
for LDCT screening of individuals at high risk for lung
cancer portends a growing demand for minimal ly
invasive approaches as surgically curable lung cancer is
identified at earlier stages. Although lobectomy currently
remains the standard of care for early NSCLC, for
patients with very small-sized lung tumours and indolent
lesions, cancer-free survival may not necessarily be
compromised by undergoing less invasive approaches
that intentionally resect less lung tissue by performing
sublobar resections.
References
1. Howington JAQ, Blum MG, Chang AC, et al. Treatment of stage I and II non-small cell lung cancer: Daignosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest 2013;143:e278S-313S.
2. Cheng AM, Wood DE. Minimally invasive resection of early lung cancers. Available from: http://www.cancernetwork.com/oncology-journal/minimally-invasive-resection-early-lung-cancers. Accessed March 15, 2015.
3. Aberle DR, Adams AM, Berg CD, et al. Reduced lung-cancer mortality with low-dose computed tomographic screening. N Engl J Med. 2011;365:395-409.
4. Yim AP, Wan S, Lee TW, Arifi AA. VATS lobectomy reduces cytokine responses compared with conventional surgery. Ann Thorac Surg. 2000;70:243-7.
5. Craig SR, Leaver HA, Yap PL, et al. Acute phase responses following minimal access and conventional thoracic surgery. Eur J Cardiothorac Surg. 2001;20:455-63.
6. Whitson BA, D’Cunha J, Maddaus MA. Minimally invasive cancer surgery improves patient survival rates through less perioperative immunosuppression. Med Hypotheses. 2007;68:1328-32.
7. Ng CS, Wan S, Hui CW, et al. Video-assisted thoracic surgery for early stage lung cancer – can short-term immunological advantages improve long-term survival? Ann Thorac Cardiovasc Surg. 2006;12:308-12.
8. Whitson BA, D’Cunha J, Andrade RS, et al. Thoracoscopic versus thoracotomy approaches to lobectomy: differential impairment of ce l lu lar immunity. Ann Thorac Surg. 2008;86:1735-44.
9. Kirby TJ, Mack MJ, Landreneau RJ, Rice TW. Lobectomy – video-assisted thoracic surgery versus muscle-sparing thoracotomy. A randomized trial. J Thorac Cardiovasc Surg. 1995;109:997-1001; discussion 01-2.
10. Sugi K, Kaneda Y, Esato K. Video-assisted thoracoscopic lobectomy achieves a satisfactory long-term prognosis in patients with clinical stage IA lung cancer. World J Surg. 2000;24:27-30; discussion 30-1.
11. Gopaldas RR, Bakaeen FG, Dao TK, et al. Video-assisted thoracoscopic versus open thoracotomy lobectomy in a cohort of 13,619 patients. Ann Thorac Surg. 2010;89:1563-70.
12. Paul S, Altorki NK, Sheng S, et al. Thoracoscopic lobectomy is associated with lower morbidity than open lobectomy: a propensity-matched analysis from the STS database. J Thorac Cardiovasc Surg. 2010;139:366-78.
13. Scott WJ, Allen MS, Darling G, et al. Video-assisted thoracic surgery versus open lobectomy for lung cancer: a secondary analysis of data from the American College of Surgeons Oncology Group Z0030 randomized clinical trial. J Thorac Cardiovasc Surg. 2010;139:976-81; discussion 81-3.
14. Whitson BA, Groth SS, Duval SJ, et al. Surgery for early-stage non-small cell lung cancer: a systematic review of the video-assisted thoracoscopic surgery versus thoracotomy approaches to lobectomy. Ann Thorac Surg. 2008;86:2008-16; discussion 16-8.
SPOTlight -2
10 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
15. Yan TD, Black D, Bannon PG, McCaughan BC. Systematic review and meta-analysis of randomized and nonrandomized trials on safety and efficacy of video-assisted thoracic surgery lobectomy for early-stage non-small-cell lung cancer. J Clin Oncol. 2009;27:2553-62.
16. Mathisen DJ. Is video-assisted thoracoscopic lobectomy inferior to open lobectomy oncologically? Ann Thorac Surg. 2013;96:755-6.
17. Denlinger CE, Fernandez F, Meyers BF, et al. Lymph node evaluation in video-assisted thoracoscopic lobectomy versus lobectomy by thoracotomy. Ann Thorac Surg. 2010;89:1730-5; discussion 36.
18. Merritt RE, Hoang CD, Shrager JB. Lymph node evaluation achieved by open lobectomy compared with thoracoscopic l obec tomy fo r N0 l ung cance r . Ann Tho rac Su rg 2013;96:1171-7.
19. Lee PC, Nasar A, Port JL, et al. Long-term survival after lobectomy for non-small cell lung cancer by video-assisted thoracic surgery versus thoracotomy. Ann Thorac Surg. 2013;96:951-60; discussion 60-1.
20. Howington JA, Blum MG, Chang AC, et al. Treatment of stage I and II non-small cell lung cancer: diagnosis and management of lung cancer, 3rd ed. American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143:e278S-e313S.
21. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®) non-small cell lung cancer, version 4.2015. Available from: http://www.nccn.org/professionals/physician_glos/PDF/nscl.pdf. Accessed February 11, 2015.
22. Farjah F, Flum DR, Varghese TK, Jr, et al. Surgeon specialty and long-term survival after pulmonary resection for lung cancer. Ann Thorac Surg. 2009;87:995-1004; discussion 05-6.
23. American Cancer Society. What are the key statistics about lung cancer? Available from: http://www.cancer.org/cancer/lungcancer-non-smallcell/detailedguide/non-small-cell-lung-cancer-key-statistics. Accessed February 11, 2015.
24. Cattaneo SM, Park BJ, Wilton AS, et al. Use of video-assisted thoracic surgery for lobectomy in the elderly results in fewer complications. Ann Thorac Surg. 2008;85:231-5; discussion 35-6.
25. Mun M Kohno T. Video-assisted thoracic surgery for clinical stage I lung cancer in octogenarians. Ann Thorac Surg. 2008;85:406-11.
26. Port JL, Mirza FM, Lee PC, et al. Lobectomy in octogenarians with non-small cell lung cancer: ramifications of increasing life expectancy and the benefits of minimally invasive surgery. Ann Thorac Surg. 2011;92:1951-7.
27. Chang MY, Mentzer SJ, Colson YL, et al. Factors predicting poor survival after resection of stage IA non-small cell lung cancer. J Thorac Cardiovasc Surg. 2007;134:850-6.
28. Whitson BA, Groth SS, Andrade RS, et al. Survival after lobectomy versus segmentectomy for stage I non-small cell lung cancer: a population-based analysis. Ann Thorac Surg. 2011;92:1943-50.
29. Okada M, Koike T, Higashiyama M, et al. Radical sublobar resection for small-sized non-small cell lung cancer: a multicenter study. J Thorac Cardiovasc Surg. 2006;132:769-75.
Answer these on page 25 or make an online submission at: www.hkmacme.org
Please indicate whether the following statements are true or false.
1. Surgery offers the greatest opportunity for cure of
NSCLC.
2. Lobectomy has been the standard operation for
early NSCLC.
3. VATS lobectomy leads to higher level of serum
pro-inflammatory cytokines.
4. VATS lobectomy leads to less pulmonary
morbidity.
5. Many randomized control studies compared VATS
vs open lobectomy.
6. Thoroughness of mediastinal lymph node
dissection should be the same in VATS and open
lobectomy.
7. Sublobar resection should be considered in elderly
with marginal lung function.
8. LDCT screening does not identify more very early
NSCLC.
9. Segmentectomy is technically more demanding
than wedge resection.
10. Wedge resection is preferred to segmentectomy in
surgery for early NSCLC.
Q&A Self-assessment Questions:
Complete thiscourse and earn
1 CME Point
30. Yamashita S, Chujo M, Kawano Y, et al. Clinical impact of segmentectomy compared with lobectomy under complete video-assisted thoracic surgery in the treatment of stage I non-small cell lung cancer. J Surg Res. 2011;166:46-51.
31. Altorki NK, Yip R, Hanaoka T, et al. Sublobar resection is equivalent to lobectomy for clinical stage 1A lung cancer in solid nodules. J Thorac Cardiovasc Surg. 2014;147:754-62; Discussion 62-4.
32. Watanabe A, Ohori S, Nakashima S, et al. Feasibility of video-assisted thoracoscopic surgery segmentectomy for selected peripheral lung carcinomas. Eur J Cardiothorac Surg. 2009;35:775-80; discussion 80.
33. Cancer and Leukemia Group B. A phase III randomized trial of lobectomy versus sublobar resection for small (≤ 2 cm) peripheral non-small cell lung cancer. ClinicalTrials.gov identifier: NCT00499330. Available from: https://clinicaltrials.gov/ct2/show/NCT00499330. Accessed February 11, 2015.
34. Nakamura K, Saji H, Nakajima R, et al. A phase III randomized tr ial of lobectomy versus l imited resection for small-sized peripheral non-small cell lung cancer (JCOG0802/WJOG4607L). Jpn J Clin Oncol. 2010;40:271-4.
11HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -3
Older people in Hong Kong are often challenged by
difficult decisions related to their estates in a filial culture.
In the very first community survey in 201310, 55.4% of
local older people required assistance in financial affairs
because of poor health, refusal and mental incapacity
but only 2% of the older people are using the Enduring
Power of Attorney11. Cognitive ageing in tandem with
other common risk factors such as sensory impairment,
medical and psychiatric co-morbidit ies and social
isolation can put the older people at risk for impaired
capacities and also become vulnerable to exploitation12.
There are more frequent court hearings for dispute in
wills and/or ownership of business in the last decade13.
On the other hand, more than 70% of the applications
for guardianship order are for the older people incapable
of managing their financial affairs since the inception
of the Hong Kong Guardianship Board every year14-16.
As a result, the Guardianship Board is promoting wider
coverage of the Enduring Power of Attorney with the
rationale of prevention is always better than cure16.
Like many western societies, a registered medical
practitioner in Hong Kong has de facto authority to
perform capacity assessment. Nonetheless, there are
few researches, guidelines or training opportunities on
the assessment of mental capacity in general, and in
particular, on the financial capacity assessment for the
elderly. Recent studies3,17-20 reveal that subtle cognitive
decline may result in financial incapacity among the
apparent “cognitively healthy” older people. On the
other hand, not all the older people with dementia are
incapable of managing financial affairs19-21. There is
a notable gap in the appreciation of the clinical and
Mind the Gap: Assessing Financial Capacity for the Elderly
In the last few decades, the alarm of ageing populations
has been ringing repeatedly across countries and
boundaries. Governments and healthcare providers
often share pessimistic views for the risk of encumbering
the public systems. On the contrary, the business and
financial sector are uncovering potential “longevity
economy” or “si lver hair market” among the older
people1-2. Their optimistic views are based on the forecast
that upcoming cohorts are more “healthy and wealthy”,
especially in the western countries. For instance, the
baby-boomers comprise of 13% of the population and are
holding 34% of the national wealth in the United States3.
They have to manage their investment and financial
affairs in order to arrange better healthcare schemes and
maintain their living standards after retirement 3-5.
In Hong Kong, the number of millionaires and multi-
millionaires is increasing over the past decade. In a
recent community survey, it is estimated that 12% of the
adult population are millionaires as defined by having at
least one million of “liquid cash” and 56,000 out of the
7.2 million Hong Kong people are multi-millionaires6.
They will become the upcoming cohorts of older people
and wil l constitute up to 30% of the population by
20417. Even for the present cohort of older people,
according to a population-based survey conducted by
the government in mid-2008, twenty-seven percent of
them own a flat and 3% of them has rented out a flat
or shop8. The crux is that the average price of a private
domestic flat has been escalating, for example, the
price of a flat in Kowloon has been nearly tripled for the
last two decades9 and the owners are multi-millionaires
owing to their estates.
Dr. LAM Chi LeungMBChB (CUHK), MSc Clinical Gerontology (CUHK),
MSc (Health and Hospital Mgt) (Birm), FHKCPsych, FHKAM (Psychiatry),
Specialist in Psychiatry
Prof. Helen CHIUMBBS(HK), MRCPsych, FRCPsych, FHKCPsych, FHKAM(Psychiatry)
Professor of Psychiatry, Department of Psychiatry, Faculty of Medicine,
Chinese University of Hong Kong
12 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -3
ethical aspects, risks and problems associated with the
assessment of financial capacity in ageing societies19,20.
This article will review the basic principles of capacity
assessment and wi l l prov ide pract ica l s teps on
assessing testamentary capacity and general financial
capacity in the older people with cognitive impairment
via the below case scenarios.
Case scenarios
A. Mr. X, a 70-year-old widower who has just handed
over h is business to h is son. He has stable
hypertension and diabetes mellitus and has been
attending your clinic for more than a decade. Mr. X
is lately admitted to a private hospital for syncope
due to transient ischaemic attack. His son, who
was your high school classmate, invites you to visit
Mr. X at the hospital and sign on his father’s living
will….
B. Mr. X attends your clinic after the discharge. His
daughter comes along and reports that Mr. X
becomes less smart than before. She explains to
you that Mr. X has had a heated argument with his
son just before the admission. Mr. X is angry about
his son. They worry about his health and assets
and ask you to complete a medical certificate for
applying Mr. X’s enduring power of attorney….
As the family doctor who knows Mr. X and his family
well, will you sign on the documents as per request at
the hospital (scenario A) and at your clinic (scenario B)?
Do you have any areas of concern before signing the
legal documents for Mr. X? If you are going to complete
the legal procedures, what will be included in your
assessment?
Basic principles in capacity assessment
Capacity is pivotal in everyday decision-making, which
may or may not have legal consequences. Everyone
is f ree to make his own choices. Unless there is
evidence to the contrary, an adult is presumed to have
the capacity under common law24,25. It reflects the
fundamental legal (and ethical) principle of respecting
autonomy of an adult24-26. Different professionals such
as lawyer, medical practitioner and social worker have
been observing these principles in their daily practices.
In the same vein, medical and legal professionals
are presumed to have tested his cl ient’s capacity
before offering treatments and taking their instructions
respectively24. An important consideration in capacity
assessment is whether there is undue influence act
upon the decision process26,27. Undue influence refers
to dynamic between an individual and another person.
It describes the intentional use of social influence,
deception and manipulation to gain control of the
decision making of another person27.
The functional approach
There are dif ferent approaches, namely outcome
approach, status approach and functional approach
in contemporary capac i ty assessment 26,27. The
Mental Capacity Act in the United Kingdom has laid
down important pr inciples and guidel ines for the
assessment28. Hong Kong jurisdiction has adopted
a functional approach to assess the mental capacity
for adult older than 18 years old, i.e. the assessment
is specific to time and task25,26,29. In other words, the
standard of capabil i ty may vary with the t ime and
situation of assessment and the complexity of the task
involved in the same person. For example, an elderly
man with mild dementia may be capable to give consent
for surgical procedure to remove his skin nodule but
he may have big problem in deciding his future mode
of care. Ferrars and Shankar30 suggest a few key
questions to help the capacity assessment (Table 1). In
essence, the older person should show his capability
to remember and understand specific and relevant
information. He should have the ability to appreciate
and reason the given information and arrive at the
decision and communicate his decision to the assessor
voluntarily29,30.
13HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -3
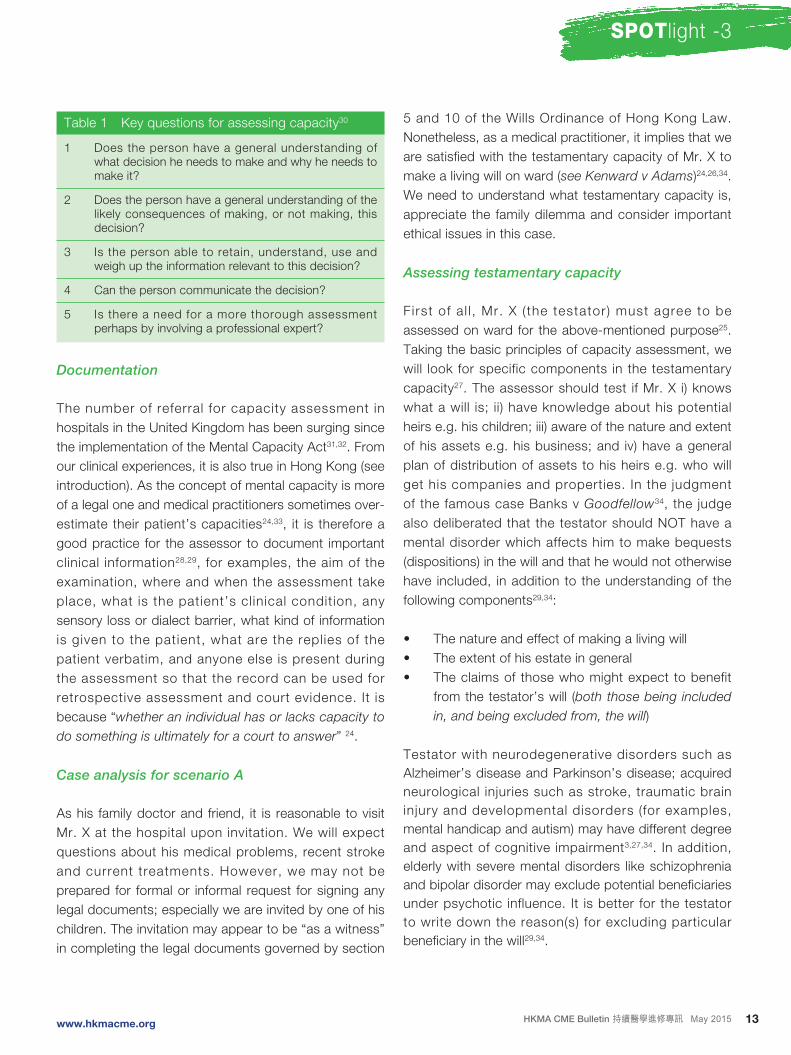
Table 1 Key questions for assessing capacity30
1 Does the person have a general understanding of what decision he needs to make and why he needs to make it?
2 Does the person have a general understanding of the likely consequences of making, or not making, this decision?
3 Is the person able to retain, understand, use and weigh up the information relevant to this decision?
4 Can the person communicate the decision?
5 Is there a need for a more thorough assessment perhaps by involving a professional expert?
Documentation
The number of referral for capacity assessment in
hospitals in the United Kingdom has been surging since
the implementation of the Mental Capacity Act31,32. From
our clinical experiences, it is also true in Hong Kong (see
introduction). As the concept of mental capacity is more
of a legal one and medical practitioners sometimes over-
estimate their patient’s capacities24,33, it is therefore a
good practice for the assessor to document important
clinical information28,29, for examples, the aim of the
examination, where and when the assessment take
place, what is the patient’s cl inical condition, any
sensory loss or dialect barrier, what kind of information
is given to the patient, what are the replies of the
patient verbatim, and anyone else is present during
the assessment so that the record can be used for
retrospective assessment and court evidence. It is
because “whether an individual has or lacks capacity to
do something is ultimately for a court to answer” 24.
Case analysis fo r scenario A
As his family doctor and friend, it is reasonable to visit
Mr. X at the hospital upon invitation. We will expect
questions about his medical problems, recent stroke
and current treatments. However, we may not be
prepared for formal or informal request for signing any
legal documents; especially we are invited by one of his
children. The invitation may appear to be “as a witness”
in completing the legal documents governed by section
5 and 10 of the Wills Ordinance of Hong Kong Law.
Nonetheless, as a medical practitioner, it implies that we
are satisfied with the testamentary capacity of Mr. X to
make a living will on ward (see Kenward v Adams)24,26,34.
We need to understand what testamentary capacity is,
appreciate the family dilemma and consider important
ethical issues in this case.
Assessing testamentary capacity
First of a l l , Mr. X ( the testator) must agree to be
assessed on ward for the above-mentioned purpose25.
Taking the basic principles of capacity assessment, we
will look for specific components in the testamentary
capacity27. The assessor should test if Mr. X i) knows
what a will is; ii) have knowledge about his potential
heirs e.g. his children; iii) aware of the nature and extent
of his assets e.g. his business; and iv) have a general
plan of distribution of assets to his heirs e.g. who will
get his companies and properties. In the judgment
of the famous case Banks v Goodfellow34, the judge
also deliberated that the testator should NOT have a
mental disorder which affects him to make bequests
(dispositions) in the will and that he would not otherwise
have included, in addition to the understanding of the
following components29,34:
• The nature and effect of making a living will
• The extent of his estate in general
• The claims of those who might expect to benefit
from the testator’s will (both those being included
in, and being excluded from, the will)
Testator with neurodegenerative disorders such as
Alzheimer’s disease and Parkinson’s disease; acquired
neurological injuries such as stroke, traumatic brain
injury and developmental disorders (for examples,
mental handicap and autism) may have different degree
and aspect of cognitive impairment3,27,34. In addition,
elderly with severe mental disorders like schizophrenia
and bipolar disorder may exclude potential beneficiaries
under psychotic influence. It is better for the testator
to write down the reason(s) for excluding particular
beneficiary in the will29,34.
14 HKMA CME Bulletin 持續醫學進修專訊 May 2015 www.hkmacme.org
SPOTlight -3
Recent studies20,22,27 note that the testator relies heavily on the verbal (language) and executive function instead of using pragmatic skills in forming the testamentary capacity. Executive function refers to higher cerebral processes in the areas of goal formation, planning, response inhibition, self-monitoring, and coordination of series of complex behaviors20. For instance, the testator with cognitive impairment may give clear account of all the specific components except he may have problem to form working estimates of the value for key assets (which should reasonably approximate their true value in a capable person)20,27. If there is evidence that Mr. X has problem with one or more of above components, the assessment should be concluded with incapacity.
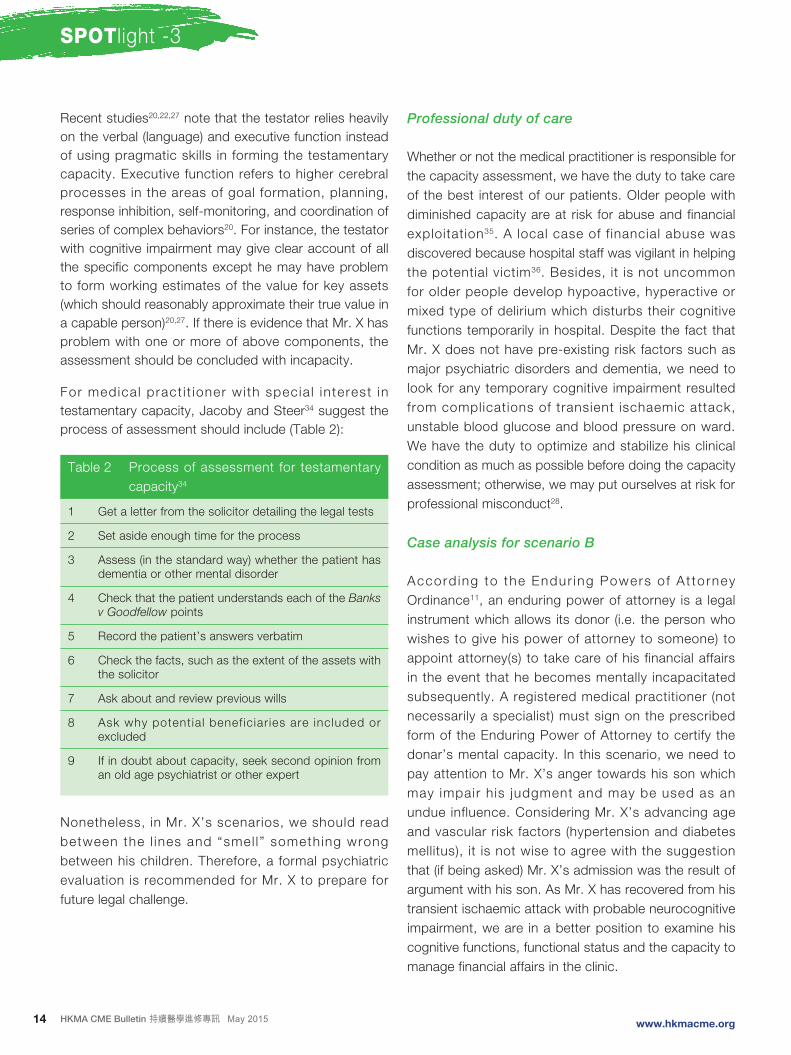
For medica l pract i t ioner wi th specia l in terest in testamentary capacity, Jacoby and Steer34 suggest the process of assessment should include (Table 2):
Table 2 Process of assessment for testamentary capacity34
1 Get a letter from the solicitor detailing the legal tests
2 Set aside enough time for the process
3 Assess (in the standard way) whether the patient has dementia or other mental disorder
4 Check that the patient understands each of the Banks v Goodfellow points
5 Record the patient’s answers verbatim
6 Check the facts, such as the extent of the assets with the solicitor
7 Ask about and review previous wills
8 Ask why potential beneficiar ies are included or excluded
9 If in doubt about capacity, seek second opinion from an old age psychiatrist or other expert
Nonetheless, in Mr. X’s scenarios, we should read between the l ines and “smel l ” something wrong between his children. Therefore, a formal psychiatric evaluation is recommended for Mr. X to prepare for future legal challenge.
Professional duty of care
Whether or not the medical practitioner is responsible for the capacity assessment, we have the duty to take care of the best interest of our patients. Older people with diminished capacity are at risk for abuse and financial exploitation35. A local case of f inancial abuse was discovered because hospital staff was vigilant in helping the potential victim36. Besides, it is not uncommon for older people develop hypoactive, hyperactive or mixed type of delirium which disturbs their cognitive functions temporarily in hospital. Despite the fact that Mr. X does not have pre-existing risk factors such as major psychiatric disorders and dementia, we need to look for any temporary cognitive impairment resulted from complications of transient ischaemic attack, unstable blood glucose and blood pressure on ward. We have the duty to optimize and stabilize his clinical condition as much as possible before doing the capacity assessment; otherwise, we may put ourselves at risk for professional misconduct28.
Case analysis for scenario B
Accord ing to the Endur ing Powers o f A t to rney Ordinance11, an enduring power of attorney is a legal instrument which allows its donor (i.e. the person who wishes to give his power of attorney to someone) to appoint attorney(s) to take care of his financial affairs in the event that he becomes mentally incapacitated subsequently. A registered medical practitioner (not necessarily a specialist) must sign on the prescribed form of the Enduring Power of Attorney to certify the donar’s mental capacity. In this scenario, we need to pay attention to Mr. X’s anger towards his son which may impair his judgment and may be used as an undue influence. Considering Mr. X’s advancing age and vascular risk factors (hypertension and diabetes mellitus), it is not wise to agree with the suggestion that (if being asked) Mr. X’s admission was the result of argument with his son. As Mr. X has recovered from his transient ischaemic attack with probable neurocognitive impairment, we are in a better position to examine his cognitive functions, functional status and the capacity to manage financial affairs in the clinic.

15HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -3
Assessing f inancial capacity in cognit ively
impaired elderly
Marson et al3,19,22,23 def ine f inancial capacity as a
medico-legal construct that “represents the abil ity
to manage one ’s f i nanc ia l a f f a i r s i n a manne r
consistent with one’s personal se l f- interest and
values”. It also includes specific capacities, namely
contractual, donative and testamentary in the United
States27. In contrast to the capacity for consent to
medical treatments, this concept is broadly based
and depends on the older person’s socioeconomic
status, occupational achievement and overall financial
experience3,23. The capacity to manage one’s financial
affairs, ranging from basic skills like counting coins
and currency to more complex skills such as paying
bills, managing a checkbook and exercising financial
j udgment has impor tan t economic and sa fe t y
consequences for the older people23,35. The problem is
that financial capacity is highly susceptible to cognitive
impai rment which is o f ten missed by the fami ly
caregivers. One of the reasons is that the older people
with early dementia may still be able to perform some
financial activities (e.g. handle basic cash transactions)
but not the others (e.g. make investment decisions or
asset transfers)37. In fact, the ability to manage financial
affairs is one of the first instrumental ADLs to decline in
mild cognitive impairment and Alzheimer disease17.
The importance of obtaining information regarding one’s
lifelong values and approaches in managing money and
financial affairs has been emphasized in the assessment
of financial capacity for the older people23,27. A number of
general or specific rating scales can be used to aid the
assessment18,21,27. It is noteworthy that the commonly
used Mini-Mental State Examination38 is now protected
by copyright and is charged for use. In fact, making
a referral to experienced occupational therapist or
psychologist for testing the neurocognitive functions
of older people can be an option and use of modern
technology e.g. voice or video recording is increasingly
common in complicated situation29,39.
The role of family doctor
Mr. X’s fami ly has been seeking the advices and
treatments from family doctor for more than a decade.
The rapport and duration of contact is a powerful mean
to monitor the financial capacity of older people. In
western countries, the family doctor may share the role
of (1) educating the patients and families about the need
for advance financial planning; (2) recognizing signs of
diminished financial capacity; (3) assessing financial
impairments in cognitively impaired older people; (4)
recommend interventions to help patients maintain
financial independence; and (5) knowing when and
to whom to make medical and legal referrals12,30. The
World Psychiatric Association also reminds medical
professionals against ageism and discrimination in
examining the older people with mental problems40.
The court always considers the expertise of medical
professionals in giving expert evidence in writing or
in person41. In order to safeguard our profession, we
need to consider five main questions29 before doing
the capacity assessment and then proceed with the
suggested framework for the older people in the
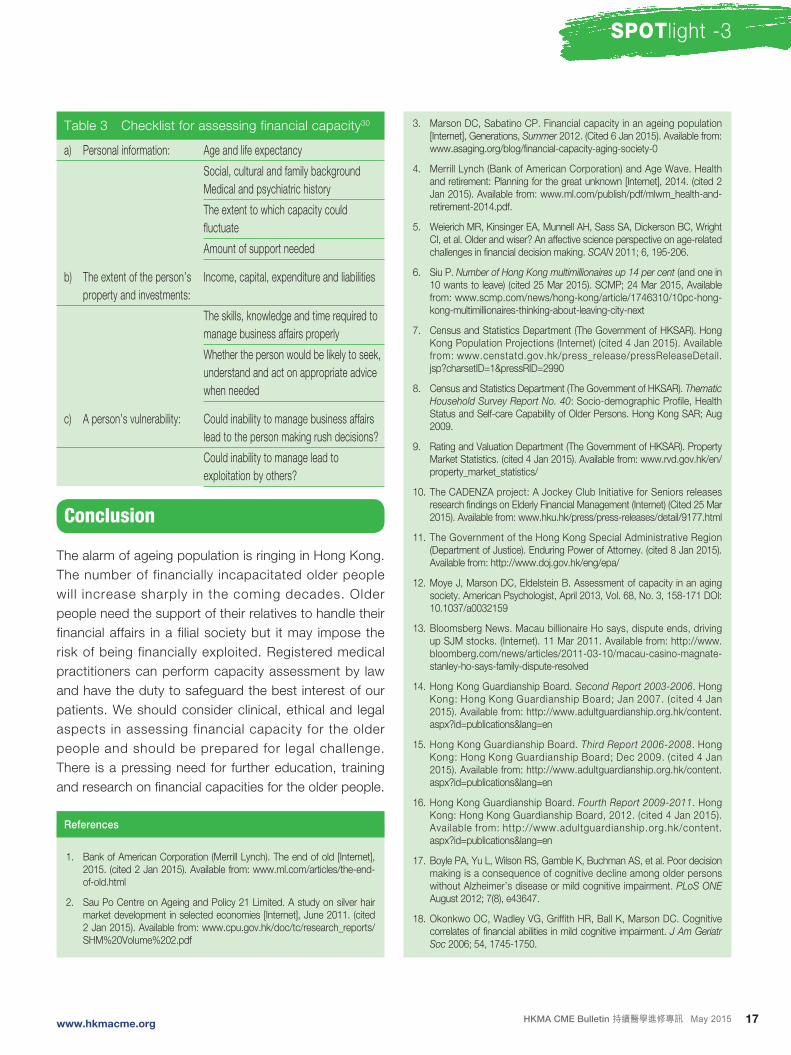
community (Table 3)30:
What: What types of decisional or functional processes
are in quest ion? What data are needed? Am I an
appropriately qualified evaluator? Do I have a conflict of
interest?
Who: Who is the client? What is the older person’s
background? Who is requesting the evaluation? Who are
the interested parties? Who sees the report? Is the court
or litigants involved?
When: How urgent is the request? Is there a court
date? What is the time frame of interest? Is the individual
medically stable?
Where: In what context/setting does the evaluation take
place?
Why: Why now? What is the history of the case? Will a
capacity evaluation resolve the problem?
17HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -3
Table 3 Checklist for assessing financial capacity30
a) Personal information: Age and life expectancy
Social, cultural and family background
Medical and psychiatric history
The extent to which capacity could
fluctuate
Amount of support needed
b) The extent of the person’s
property and investments:
Income, capital, expenditure and liabilities
The skills, knowledge and time required to
manage business affairs properly
Whether the person would be likely to seek,
understand and act on appropriate advice
when needed
c) A person’s vulnerability: Could inability to manage business affairs
lead to the person making rush decisions?
Could inability to manage lead to
exploitation by others?
Conclusion
The alarm of ageing population is ringing in Hong Kong.
The number of financially incapacitated older people
will increase sharply in the coming decades. Older
people need the support of their relatives to handle their
financial affairs in a filial society but it may impose the
risk of being financially exploited. Registered medical
practitioners can perform capacity assessment by law
and have the duty to safeguard the best interest of our
patients. We should consider clinical, ethical and legal
aspects in assessing financial capacity for the older
people and should be prepared for legal challenge.
There is a pressing need for further education, training
and research on financial capacities for the older people.
References
1. Bank of American Corporation (Merrill Lynch). The end of old [Internet], 2015. (cited 2 Jan 2015). Available from: www.ml.com/articles/the-end-of-old.html
2. Sau Po Centre on Ageing and Policy 21 Limited. A study on silver hair market development in selected economies [Internet], June 2011. (cited 2 Jan 2015). Available from: www.cpu.gov.hk/doc/tc/research_reports/SHM%20Volume%202.pdf
3. Marson DC, Sabatino CP. Financial capacity in an ageing population [Internet], Generations, Summer 2012. (Cited 6 Jan 2015). Available from: www.asaging.org/blog/financial-capacity-aging-society-0
4. Merrill Lynch (Bank of American Corporation) and Age Wave. Health and retirement: Planning for the great unknown [Internet], 2014. (cited 2 Jan 2015). Available from: www.ml.com/publish/pdf/mlwm_health-and-retirement-2014.pdf.
5. Weierich MR, Kinsinger EA, Munnell AH, Sass SA, Dickerson BC, Wright CI, et al. Older and wiser? An affective science perspective on age-related challenges in financial decision making. SCAN 2011; 6, 195-206.
6. Siu P. Number of Hong Kong multimillionaires up 14 per cent (and one in 10 wants to leave) (cited 25 Mar 2015). SCMP; 24 Mar 2015, Available from: www.scmp.com/news/hong-kong/article/1746310/10pc-hong-kong-multimillionaires-thinking-about-leaving-city-next
7. Census and Statistics Department (The Government of HKSAR). Hong Kong Population Projections (Internet) (cited 4 Jan 2015). Available from: www.censtatd.gov.hk/press_release/pressReleaseDetail.jsp?charsetID=1&pressRID=2990
8. Census and Statistics Department (The Government of HKSAR). Thematic Household Survey Report No. 40: Socio-demographic Profile, Health Status and Self-care Capability of Older Persons. Hong Kong SAR; Aug 2009.
9. Rating and Valuation Department (The Government of HKSAR). Property Market Statistics. (cited 4 Jan 2015). Available from: www.rvd.gov.hk/en/property_market_statistics/
10. The CADENZA project: A Jockey Club Initiative for Seniors releases research findings on Elderly Financial Management (Internet) (Cited 25 Mar 2015). Available from: www.hku.hk/press/press-releases/detail/9177.html
11. The Government of the Hong Kong Special Administrative Region (Department of Justice). Enduring Power of Attorney. (cited 8 Jan 2015). Available from: http://www.doj.gov.hk/eng/epa/
12. Moye J, Marson DC, Eldelstein B. Assessment of capacity in an aging society. American Psychologist, April 2013, Vol. 68, No. 3, 158-171 DOI: 10.1037/a0032159
13. Bloomsberg News. Macau billionaire Ho says, dispute ends, driving up SJM stocks. (Internet). 11 Mar 2011. Available from: http://www.bloomberg.com/news/articles/2011-03-10/macau-casino-magnate-stanley-ho-says-family-dispute-resolved
14. Hong Kong Guardianship Board. Second Report 2003-2006. Hong Kong: Hong Kong Guardianship Board; Jan 2007. (cited 4 Jan 2015). Available from: http://www.adultguardianship.org.hk/content.aspx?id=publications&lang=en
15. Hong Kong Guardianship Board. Third Report 2006-2008. Hong Kong: Hong Kong Guardianship Board; Dec 2009. (cited 4 Jan 2015). Available from: http://www.adultguardianship.org.hk/content.aspx?id=publications&lang=en
16. Hong Kong Guardianship Board. Fourth Report 2009-2011. Hong Kong: Hong Kong Guardianship Board, 2012. (cited 4 Jan 2015). Available from: http://www.adultguardianship.org.hk/content.aspx?id=publications&lang=en
17. Boyle PA, Yu L, Wilson RS, Gamble K, Buchman AS, et al. Poor decision making is a consequence of cognitive decline among older persons without Alzheimer’s disease or mild cognitive impairment. PLoS ONE August 2012; 7(8), e43647.
18. Okonkwo OC, Wadley VG, Griffith HR, Ball K, Marson DC. Cognitive correlates of financial abilities in mild cognitive impairment. J Am Geriatr Soc 2006; 54, 1745-1750.
18 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
SPOTlight -3
19. Widera E, Steenpass V, Marson D, Sudore R. Finances in the older patient with cognitive impairment. JAMA Feb 16 2011; 305, 7, 698-706.
20. Kim SYH, Kalawish JHT, Caine ED. Current state of research on decision making competence of cognitively impaired elderly persons. Am J Geriatr Psychiatry Mar 2002; 10(2), 151-165.
21. Lui VWC, Lam LCW, Chau RCM, Fung AWT, Wong BML, Leung GTY, et al. Structured assessment of mental capacity to make financial decisions in Chinese older persons with mild cognitive impairment and mild Alzheimer disease. J Geriatr Psychiatry Neurol 2013; 26(2), 69-77.
22. Knight AJ, Marson DC. The emerging neuroscience of financial capacity. [Internet] Generations, Summer 2012; 36, 2, 46-52. (Cited 6 Jan 2015). Available from: www.asaging.org/blog/emerging-neuroscience-financial-capacity
23. Marson DC. Clinical and ethical aspects of financial capacity in dementia: a commentary. Am J Geriatr Psychiatry, April 2013; 21, 4, 382-390.
24. British Medical Association. Assessment of Mental Capacity: Guidance for doctors and lawyers, 2nd edition. London: BMJ Publishing; 2004, Chapter 1&3.
25 Wong JG, Scully P. A practical guide to capacity assessment and patient consent in Hong Kong. Hong Kong Med J 2003; 9, 284-289.
26. Lam TCP. Testamentary Capacity, HKMA CME Bulletin, May 2012. (Cited 6 Jan 2015). Available from: www.hkma.org/english/cme/cmebulletin.htm
27. American Psychological Association. Assessment of Older Adults with
Diminished Capacity: A Handbook for Psychologists. United States:
American Bar Association Commission on Law and Aging – American
Psychological Association. (cited 6 Jan 2015). Available from: www.apa.
org/pi/aging/programs/assessment/capacity-psychologist-handbook.pdf
28. British Medical Association. The Mental Capacity Act 2005: Guidance for
health professionals. Sep 2009
29. Jacoby R. Mental Capacity in Old Age Psychiatry, Presented at the
Workshop on Testamentary Capacity and Other Types of Mental
Capacities. Hong Kong, 11 Nov 2011.
30. Ferrars F, Shankar R. Assessing Mental Capacity [Internet], InnovAiT 2011;
4, 2, 98-103. (cited 8 Jan 2015). Available from: http://ino.sagepub.com/
content/4/2/98
31. Mujic F, Heising MV, Stewart RJ, Prince MJ. Mental capacity assessments
among general hospital inpatients referred to a specialist liaison psychiatry
service for older people. Int Psychogeriatr 2009; 21:4, 729-737.
32. Kornfeld DS, Muskin PR, Tahil FA. Psychiatric evaluation of mental
capacity in the general hospital: a significant teaching opportunity.
Psychosomatics 2009; 50: 468-473.
33. Lepping P. Overestimating patients’ capacity, Br J Psychiatry 2011; 199,
355-356. doi: 10.1192/bjp.bp.111.094938
34. Jacoby R, Steer P. How to assess capacity to make a will. BMJ 2007;
335:155-7.
35. Centre for Policy on Ageing. The financial abuse of older people [Internet].
(cited 8 Jan 2015). Available from: www.cpa.org.uk/policy/briefings/
financial_abuse.pdf
36. Chan TC, Luk JKH, Liu A, Chiu PKC, Chan FHW, Chu LW. Financial abuse
in a mentally incapacitated old man. Hong Kong Med J 2009; 15, 213-
216.
37. Martin R, Griffith HR, Belue K, Harrell L, Zamrini V, Anderson B, et al.
Declining financial capacity in patients with Alzheimer’s disease: a one-
year longitudinal study. Am J Geriatr Psychiatry, March 2008; 16, 3, 209-
219.
38. Folstein MF, Folstein SE, McHugh PR. “Mini-mental state”: a practical
method for grading the cognitive state of patients for the clinician. J
Psychiatr Research 1975; 12, 3, 189-98.
39. Appelbaum PS. Assessing and reporting other mental capacities.
Presented at the Workshop on Assessment of Mental Capacities. Hong
Kong, 22 June 2012.
40. Katona C, Chiu E, Adelman S, Baloyannis S, Camus V, Firmino H, et al.
World psychiatric association section of old age psychiatry consensus
statement on ethics and capacity in older people with mental disorders. Int
J Geriatr Psychiatry 2009; 24: 1319-1324.
41. The Academy of Experts. Role & responsibilities of the expert. Expert
Witness Training, March 2015; Hong Kong.
Answer these on page 25 or make an online submission at: www.hkmacme.org
Please indicate whether the following statements are true or false.
1. Medical practitioner in Hong Kong is entitled to
perform capacity assessment by law.
2. An adult is presumed to have capacity and is
responsible for his decisions.
3. A diagnosis of dementia or mental disorder can
justify mental incapacity.
4. Basic capacity assessment should be specific
to time and task irrespective of the patient’s
diagnoses.
5. A medical practitioner’s signature on a living will
makes no difference as an ordinary witness in
court.
6. Medical practitioner is encouraged to assess
financial capacity when the patient is hospitalized.
7. The Enduring Power of Attorney is authorized by
the Mental Capacity Act in Hong Kong.
8. Financial capacity is the first instrumental ADL to
decline in the elderly.
9. If an elderly lost his money in the stock market, he
must have diminished financial capacity.
10. Guardianship order can cover the financial affairs
of the mentally incapacitated person.
Q&A Self-assessment Questions:
Complete thiscourse and earn
1 CME Point
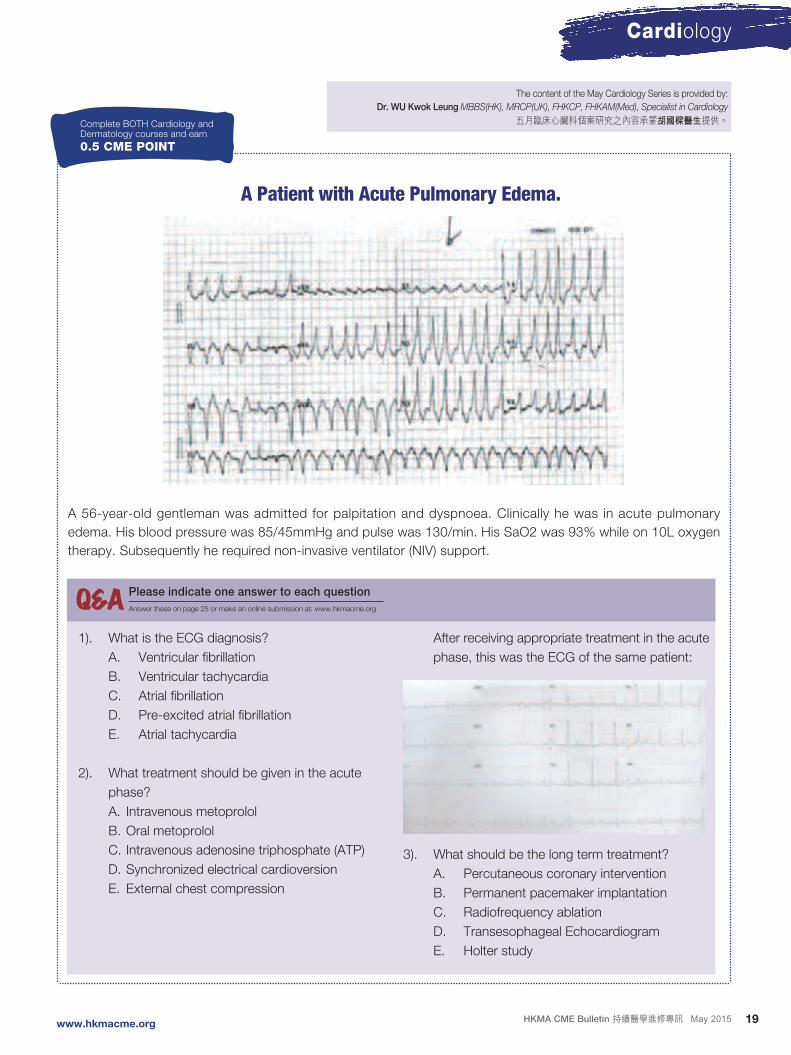
19HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Cardiology
A Patient with Acute Pulmonary Edema.
Complete BOTH Cardiology andDermatology courses and earn
0.5 CME POINT
The content of the May Cardiology Series is provided by:
Dr. WU Kwok Leung MBBS(HK), MRCP(UK), FHKCP, FHKAM(Med), Specialist in Cardiology
五月臨床心臟科個案研究之內容承蒙胡國樑醫生提供。
A 56-year-old gentleman was admitted for palpitation and dyspnoea. Clinically he was in acute pulmonary
edema. His blood pressure was 85/45mmHg and pulse was 130/min. His SaO2 was 93% while on 10L oxygen
therapy. Subsequently he required non-invasive ventilator (NIV) support.
1). What is the ECG diagnosis?
A. Ventricular fibrillation
B. Ventricular tachycardia
C. Atrial fibrillation
D. Pre-excited atrial fibrillation
E. Atrial tachycardia
2). What treatment should be given in the acute
phase?
A. Intravenous metoprolol
B. Oral metoprolol
C. Intravenous adenosine triphosphate (ATP)
D. Synchronized electrical cardioversion
E. External chest compression
After receiving appropriate treatment in the acute
phase, this was the ECG of the same patient:
3). What should be the long term treatment?
A. Percutaneous coronary intervention
B. Permanent pacemaker implantation
C. Radiofrequency ablation
D. Transesophageal Echocardiogram
E. Holter study
Q&A Please indicate one answer to each question
Answer these on page 25 or make an online submission at: www.hkmacme.org
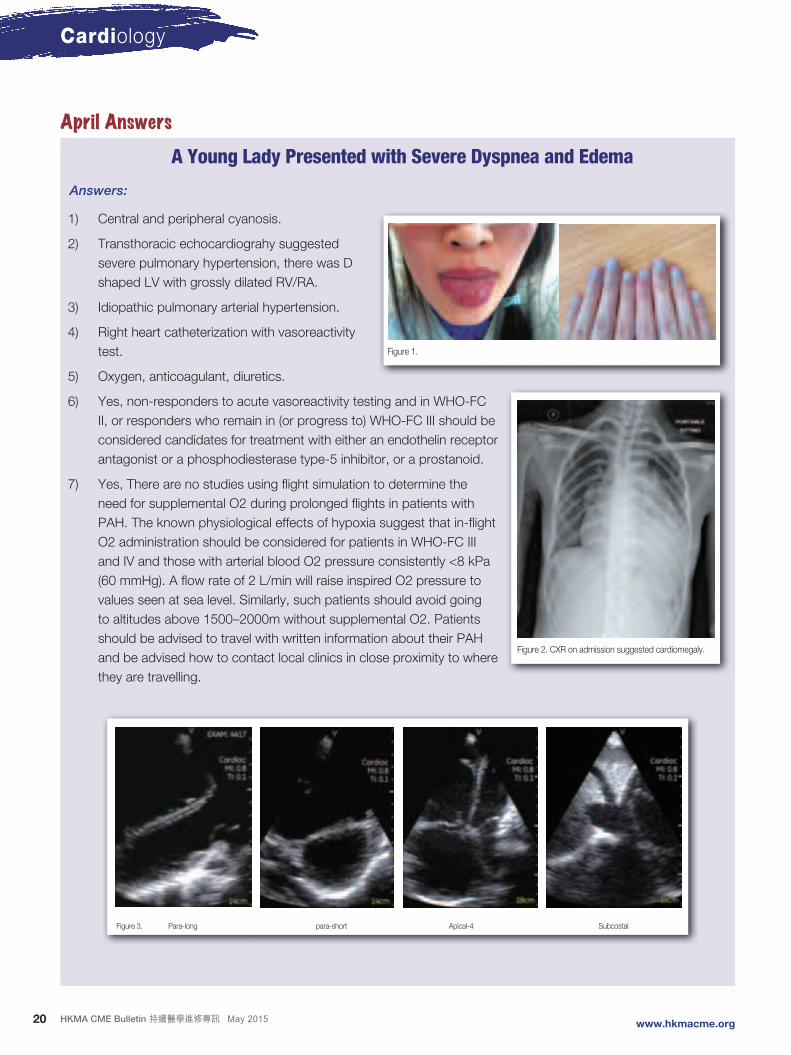
20 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Cardiology
April AnswersA Young Lady Presented with Severe Dyspnea and Edema
Answers:
1) Central and peripheral cyanosis.
2) Transthoracic echocardiograhy suggested
severe pulmonary hypertension, there was D
shaped LV with grossly dilated RV/RA.
3) Idiopathic pulmonary arterial hypertension.
4) Right heart catheterization with vasoreactivity
test.
5) Oxygen, anticoagulant, diuretics.
6) Yes, non-responders to acute vasoreactivity testing and in WHO-FC
II, or responders who remain in (or progress to) WHO-FC III should be
considered candidates for treatment with either an endothelin receptor
antagonist or a phosphodiesterase type-5 inhibitor, or a prostanoid.
7) Yes, There are no studies using flight simulation to determine the
need for supplemental O2 during prolonged flights in patients with
PAH. The known physiological effects of hypoxia suggest that in-flight
O2 administration should be considered for patients in WHO-FC III
and IV and those with arterial blood O2 pressure consistently <8 kPa
(60 mmHg). A flow rate of 2 L/min will raise inspired O2 pressure to
values seen at sea level. Similarly, such patients should avoid going
to altitudes above 1500–2000m without supplemental O2. Patients
should be advised to travel with written information about their PAH
and be advised how to contact local clinics in close proximity to where
they are travelling.
Figure 1.
Figure 2. CXR on admission suggested cardiomegaly.
Figure 3. Para-long para-short Apical-4 Subcostal
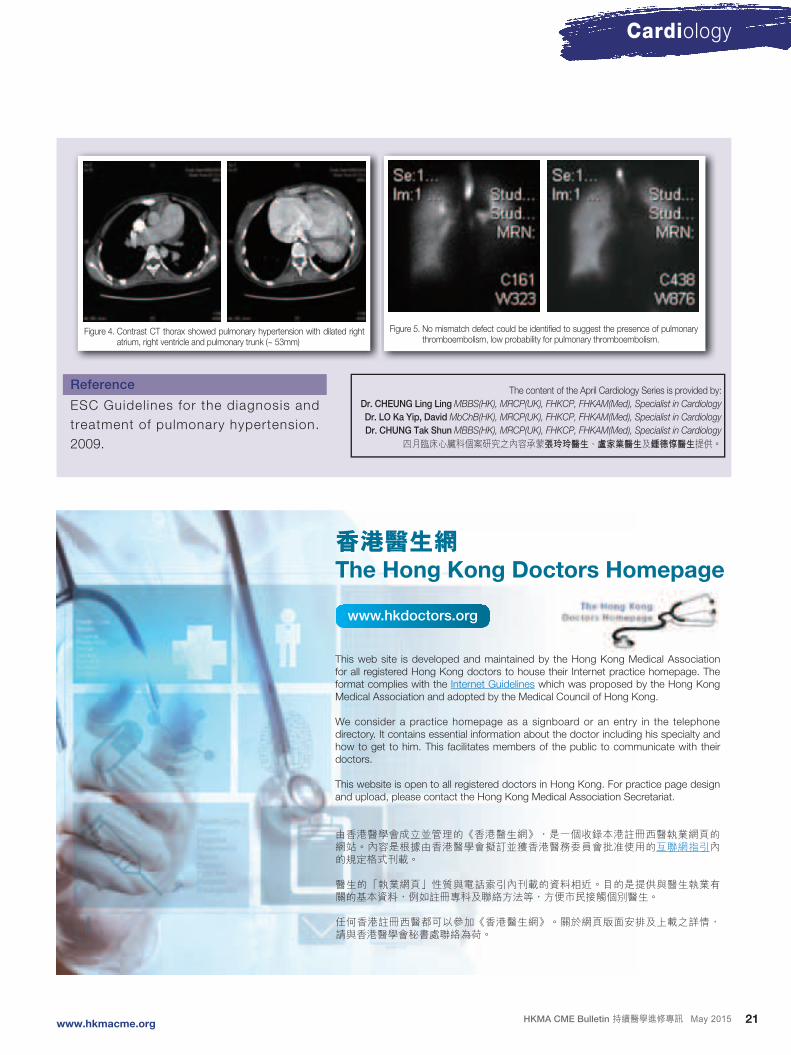
21HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Cardiology
The content of the April Cardiology Series is provided by:
Dr. CHEUNG Ling Ling MBBS(HK), MRCP(UK), FHKCP, FHKAM(Med), Specialist in Cardiology
Dr. LO Ka Yip, David MbChB(HK), MRCP(UK), FHKCP, FHKAM(Med), Specialist in Cardiology
Dr. CHUNG Tak Shun MBBS(HK), MRCP(UK), FHKCP, FHKAM(Med), Specialist in Cardiology
四月臨床心臟科個案研究之內容承蒙張玲玲醫生、盧家業醫生及鍾德惇醫生提供。
Figure 4. Contrast CT thorax showed pulmonary hypertension with dilated right atrium, right ventricle and pulmonary trunk (~ 53mm)
Figure 5. No mismatch defect could be identified to suggest the presence of pulmonary thromboembolism, low probability for pulmonary thromboembolism.
Reference
ESC Guidel ines for the diagnosis and
treatment of pulmonary hypertension.
2009.
香港醫生網The Hong Kong Doctors Homepage
www.hkdoctors.org
This web site is developed and maintained by the Hong Kong Medical Association for all registered Hong Kong doctors to house their Internet practice homepage. The format complies with the Internet Guidelines which was proposed by the Hong Kong Medical Association and adopted by the Medical Council of Hong Kong.
We consider a practice homepage as a signboard or an entry in the telephone directory. It contains essential information about the doctor including his specialty and how to get to him. This facilitates members of the public to communicate with their doctors.
This website is open to all registered doctors in Hong Kong. For practice page design and upload, please contact the Hong Kong Medical Association Secretariat.
由香港醫學會成立並管理的《香港醫生網》,是一個收錄本港註冊西醫執業網頁的網站。內容是根據由香港醫學會擬訂並獲香港醫務委員會批准使用的互聯網指引內的規定格式刊載。
醫生的「執業網頁」性質與電話索引內刊載的資料相近。目的是提供與醫生執業有關的基本資料,例如註冊專科及聯絡方法等,方便市民接觸個別醫生。
任何香港註冊西醫都可以參加《香港醫生網》。關於網頁版面安排及上載之詳情,請與香港醫學會秘書處聯絡為荷。
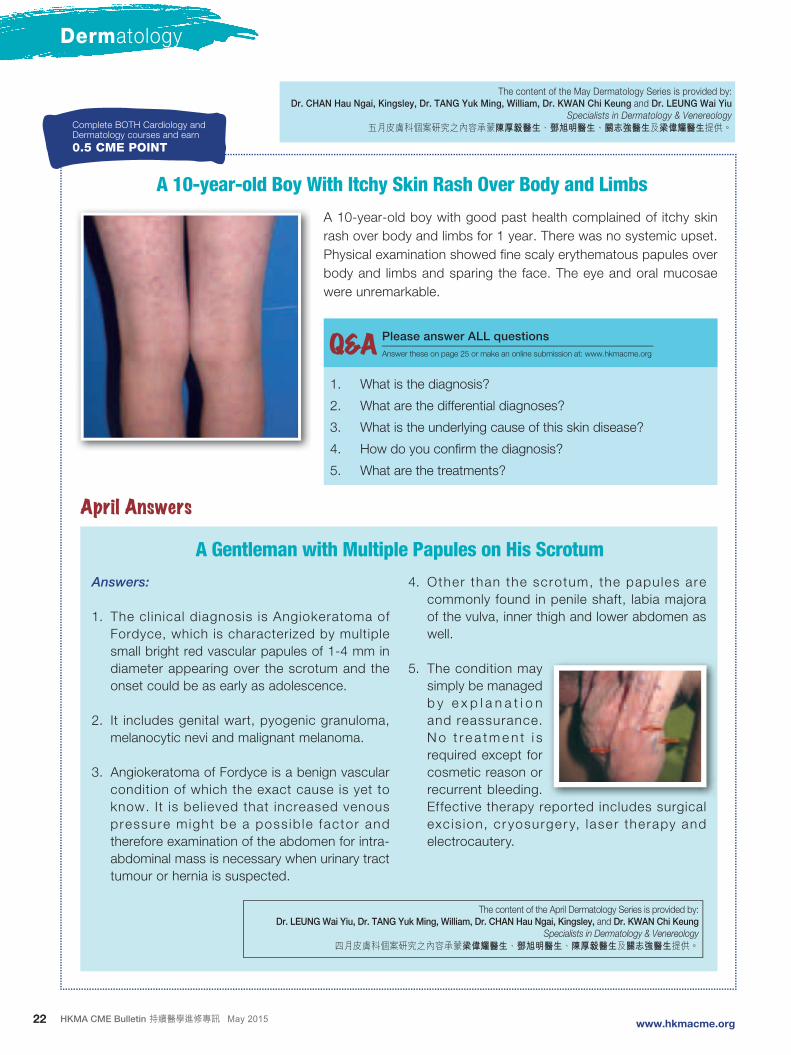
22 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Dermatology
A 10-year-old Boy With Itchy Skin Rash Over Body and Limbs
The content of the May Dermatology Series is provided by:
Dr. CHAN Hau Ngai, Kingsley, Dr. TANG Yuk Ming, William, Dr. KWAN Chi Keung and Dr. LEUNG Wai Yiu
Specialists in Dermatology & Venereology
五月皮膚科個案研究之內容承蒙陳厚毅醫生、鄧旭明醫生、關志強醫生及梁偉耀醫生提供。
A 10-year-old boy with good past health complained of itchy skin
rash over body and limbs for 1 year. There was no systemic upset.
Physical examination showed fine scaly erythematous papules over
body and limbs and sparing the face. The eye and oral mucosae
were unremarkable.
1. What is the diagnosis?
2. What are the differential diagnoses?
3. What is the underlying cause of this skin disease?
4. How do you confirm the diagnosis?
5. What are the treatments?
Q&A Please answer ALL questions
Answer these on page 25 or make an online submission at: www.hkmacme.org
Answers:
1. The cl inical diagnosis is Angiokeratoma of
Fordyce, which is characterized by multiple
small bright red vascular papules of 1-4 mm in
diameter appearing over the scrotum and the
onset could be as early as adolescence.
2. It includes genital wart, pyogenic granuloma,
melanocytic nevi and malignant melanoma.
3. Angiokeratoma of Fordyce is a benign vascular
condition of which the exact cause is yet to
know. It is believed that increased venous
pressure might be a poss ib le factor and
therefore examination of the abdomen for intra-
abdominal mass is necessary when urinary tract
tumour or hernia is suspected.
4. Other than the scrotum, the papules are
commonly found in penile shaft, labia majora
of the vulva, inner thigh and lower abdomen as
well.
5. The condition may
simply be managed
b y e x p l a n a t i o n
and reassurance.
N o t r e a t m e n t i s
required except for
cosmetic reason or
recurrent bleeding.
Effective therapy reported includes surgical
exc is ion, cr yosurger y, laser therapy and
electrocautery.
April Answers
A Gentleman with Multiple Papules on His Scrotum
The content of the April Dermatology Series is provided by:
Dr. LEUNG Wai Yiu, Dr. TANG Yuk Ming, William, Dr. CHAN Hau Ngai, Kingsley, and Dr. KWAN Chi Keung
Specialists in Dermatology & Venereology
四月皮膚科個案研究之內容承蒙梁偉耀醫生、鄧旭明醫生、陳厚毅醫生及關志強醫生提供。
Complete BOTH Cardiology andDermatology courses and earn
0.5 CME POINT

23HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Complaints & Ethics
Some 30 years ago when I first started private practice,
I was approached by a surgeon who came to me with
two gold coins to thank me for my two referrals. When I
opened the package and realized what he did, I had to
rush out to the lift to push back the coins into his pocket
with a firm ‘NO’.
At around the same period, I was phoned up by a
doctor who graduated outside of Hong Kong and
referred me some patients in internal medicine. He
very frankly asked me how much I would rebate him
for each referral. I had to tell him that with the rate I
charged ($250 per consultation at that time), I didn’t
think it was appropriate to send him any kickbacks, and
furthermore, it was immoral.
Nearly two decades ago, one of the disputing partners
of a laboratory passed to the ICAC a little black book
listing the names of doctors who were given rebates for
sending their patients to the laboratory. It was fortunate
that no charge was laid subsequently or it would be a
most damaging scandal for the profession.
On 5 January 2003, the HKMA, in collaboration with
the ICAC, released a guidebook entitled “Integrity in
Practice: A Practical Guide for Medical Practitioners
on Corruption Prevention”. The Guidebook contains
information on the anti-corruption laws and on the
corruption prone areas in the practice of medicine,
illustrated by cases or hypothetical cases from both
the public and private sectors. All doctors in Hong
Kong received a CD with the electronic version of the
Guidebook then and printed copies were distributed
via HA, DH and the private hospitals. They were also
available through HKMA secretariat and the ICAC
Regional Offices. It is regrettable that doctors graduating
after 2003 may not be aware of the guidebook and may
commit offences punishable in a Court of Law as well as
by the Medical Council Inquiry.
In the Code of Professional Conduct, 13.1 states that
‘a doctor may refer a patient to any hospital, nursing
home, health center or similar institution, for treatment
by himself or other persons only if it is, and is seen
to be, in the best interest of the patient……doctors
proposing to refer a patient to an institution in which they
have a financial interest, whether by reason of a capital
investment or a remunerative position, should always
disclose the interest to the patient before making the
referral’. 14.1 stipulates that ‘a doctor shall not offer to,
or accept from, any person or organization (including
diagnostic laboratories, hospitals, nursing homes,
health centers, beauty centers or similar institutions)
any financial or other inducement (including free or
subsidized consulting premises or secretarial support)
for referral of patients for consultation, investigation or
treatment’. 14.2 makes it clear that ‘a doctor shall not
share his professional fees with any person other than
the bona fide partners of his practice. However, it is not
a form of fee-sharing for a doctor to make payment to
other doctors and healthcare professionals collaborating
in the provision of bona fide medical services to the
patient, provided that the patient is informed of their
involvement and services as soon as reasonably
practicable.’
Integrity in Practice MBBS (HK), MFM (Clin)(Monash), LRCP (Lond), MRCS (Eng), MRCP (UK), FRCP (Irel), FHKCP, FRACGP, FHKCFP, DFM (CUHK), FHKAM (Medicine), FHKAM (Family Medicine), DCH (Lond), DOM (CUHK), DPD (Cardiff), PDipID (HK), PDipComPsychMed (HK), PDipCommunityGeriatrics (HK), Dip Ger Med RCPS (Glasg)Specialist in NephrologyDr. CHOI Kin

24 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Complaints & Ethics
As PIC Chairman, I sti l l receive complaints on this
issue of fee spl i t t ing and rebate, even from non-
loca l g raduates , but the cases are few and in-
between. Recently, however, a rather senior doctor
asked the duty council member of HKMA whether
he could, as a surgeon, write a cheque of $1000 to
the referring doctor, as a gesture of thanks, for ‘the
trouble of referring which would involve a detailed and
comprehensive letter with chronological events, copies
of laboratory reports, ECGs and other investigations
etc. as well as physically writing down the address,
telephone numbers and office hours and ringing on
behalf of the patient to make a booking and telephone
communications between each other for the sake of
understanding the patient’s case’?
The Guide in 2.1.1 talked about the PBO – Prevention
of Bribery Ordinance, which is the piece of legislation
against corruption in Hong Kong. Doctors in private
practice are required to observe Section 9 of the PBO.
The spirit of Section 9 is to maintain fair play in the
private sector and to uphold market integrity. The gist of
the law follows:
1) It is an offence for the agent to solicit or accept an
advantage when conducting his principal’s affairs
or business without the permission of his principal.
2) Any person who offers such an advantage is also
guilty of an offence.
3) I t is an offence for an agent to use any false
document, receipt or account to deceive his
principal.
In the above description, agent is a person acting for,
or employed by, the principal, and hence is the doctor.
The Principal generally refers to an employer and in this
case should be the patient who is paying. Advantage
refers to anything that is of value such as money, gift,
employment, service or favor etc. but does not include
entertainment which is def ined as food or dr inks
provided for immediate consumption on the occasion. If
the agent is given permission by his principal to accept
an advantage in relation to his official duties, then it is
lawful. A person convicted of an offence under Section 4
or Section 9 of the PBO is subject to a maximum penalty
of seven years’ imprisonment and a fine of $500,000
while the maximum penalty of violating Section 5 is ten
years’ imprisonment and $500,000 fine.
In the member’s inquiry, he challenged why he cannot
thank the doctor who referred him the case with a
monetary reward – that referring doctor has done so
much during the process of referral, writing a proper
referral letter etc. The questions ar is ing from the
challenge are obvious: did the referring doctor not
receive his fees for writing the referral letter already?
Was it not his duty to write a proper referral letter for
his patient with the proper details? By accepting the
$1000, was he referring because of the skil l of the
surgeon or because of the rebate? Has the referring
doctor informed the principal, his patient who paid him,
that he will be receiving such a monetary reward for
the referral? Did the principal (patient) agree to such a
financial arrangement between the referring doctor and
the surgeon to whom he/she was referred to? Was a
level playing field for other surgeons created who might
be more competent than the one dishing out the $1000
when such an arrangement was allowed?
It is obvious that the surgeon has committed a crime if
he provided the rebate and it is obvious that he should
stop lest he be thrown to prison. The same would apply
to doctors who are in partnership with laboratories and
refer patients to the laboratory with which they have
financial arrangements. The only allowance permitted
under the Code is proper explanation to the patient
that they are financially involved with the laboratory to
which they are sending the patient and with the patient’s
agreement. Receiving rebates for looking at laboratory
reports and radiological reports are not allowed. It is
time that doctors are aware of the risk they are taking
for these improper financial transactions lest they be
brought to a criminal court.
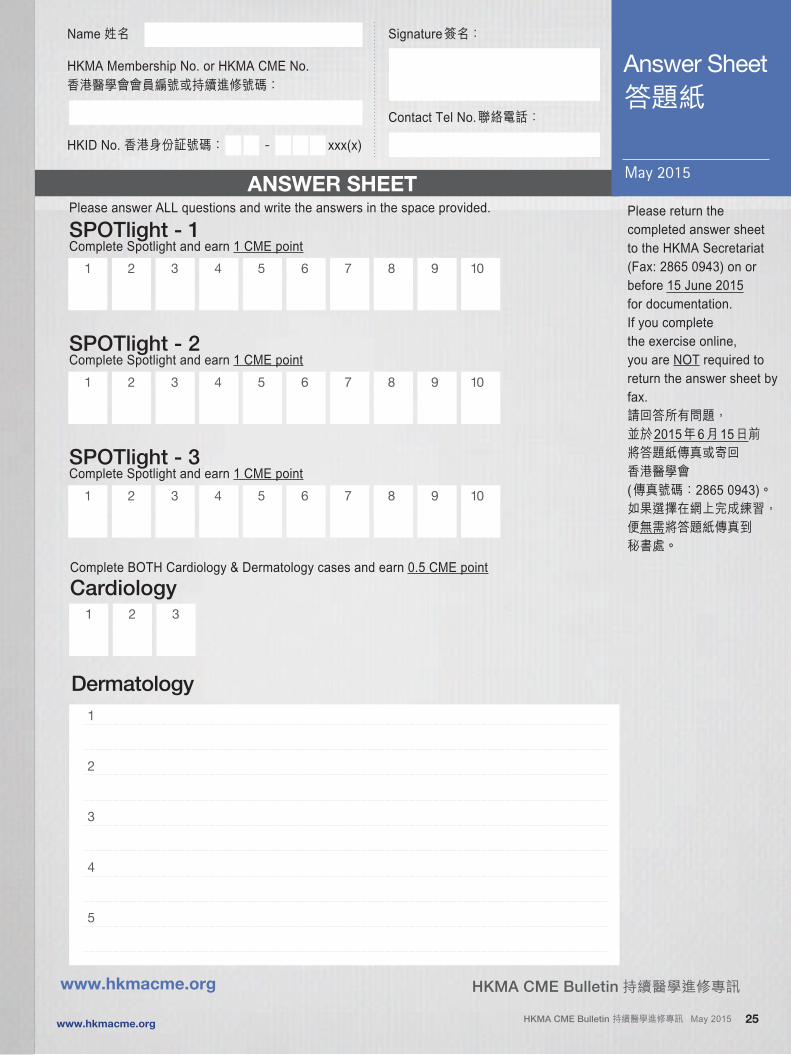
25HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Dermatology
1
2
3
4
5
1 2 3
Complete BOTH Cardiology & Dermatology cases and earn 0.5 CME point
Cardiology
HKMA CME Bulletin 持續醫學進修專訊www.hkmacme.org
Name 姓名 Signature簽名:
HKMA Membership No. or HKMA CME No.香港醫學會會員編號或持續進修號碼:
Contact Tel No.聯絡電話:
HKID No. 香港身份証號碼: - xxx(x)
Please answer ALL questions and write the answers in the space provided.
SPOTlight - 1Complete Spotlight and earn 1 CME point
ANSWER SHEETPlease return thecompleted answer sheetto the HKMA Secretariat(Fax: 2865 0943) on orbefore 15 June 2015for documentation.If you completethe exercise online,you are NOT required toreturn the answer sheet byfax.請回答所有問題,並於2015年6月15日前將答題紙傳真或寄回香港醫學會 (傳真號碼:2865 0943)。如果選擇在網上完成練習,便無需將答題紙傳真到秘書處。
Answer Sheet
May 2015
答題紙
1 2 3 4 5 6 7 8 9 10
1 2 3 4 5 6 7 8 9 10
SPOTlight - 2Complete Spotlight and earn 1 CME point
1 2 3 4 5 6 7 8 9 10
1 2 3 4 5 6 7 8 9 10
1 2 3 4 5 6 7 8 9 10
SPOTlight - 3Complete Spotlight and earn 1 CME point
1 2 3 4 5 6 7 8 9 10
26 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
CMEnotifications
HKMA CME Programme香港醫學會持續進修計劃
CME Lecture – June 2015 進修講課 - 二零一五年六月
HKMA Structured CME Programme with HKS&H Session VI: Ultrasound for Head & Neck Disease
Dr. WONG Kim Ping, RexMBBS (HK), FRCR, FHKCR, FHKAM (Radiology), Specialist in Radiology
Date: 11 June 2015 (Thursday)
Time: 2:00–3:00 p.m. [Light lunch starts at 1:15 p.m.]
Venue: The HKMA Dr. Li Shu Pui Professional Education Centre, 2/F,
Chinese Club Building, 21–22 Connaught Road Central, HK
香港醫學會分科持續醫學進修計劃第六節:頭和頸部疾病的超聲波檢查
講者:黃劍平醫生香港大學內外全科醫學士、英國皇家放射科學醫學院院士、香港放射科醫學院院士、香港醫學專科學院院士(放射科)、放射科專科醫生
日期:二零一五年六月十一日(星期四)時間:下午二時至三時正 [輕膳於下午一時十五分開始]地點: 香港中環干諾道中二十一至二十二號華商會所大廈二樓
香港醫學會李樹培醫生專業教育中心
This symposium is co-organized with Hong Kong Sanatorium & Hospital. 講課與養和醫院合辦
Registration:Please fill in and return the Registration Form together with a cheque of adequate amount made payable to “The Hong Kong Medical Association” to 5/F Duke of Windsor Social Service Building, 15 Hennessy Road, Hong Kong. Each lecture will carry 1 CME point under the MCHK/HKMA CME Programme (unless otherwise stated). Accreditation from other colleges is pending. (The Secretariat fax no.: 2865 0943)
To be more eco-friendly and avoid postal delay, notification to registrants will no longer be made through sending confirmation letters but via SMS. Please fill in your updated mobile number so that you can be notified of your application. If you do not have a mobile phone number, the Secretariat will issue a confirmation letter to you. If you have not received any replies, please do not hesitate to contact us at 2527 8452.
報名方法:請填妥表格連同支票寄交香港灣仔軒尼詩道十五號溫莎公爵社會服務大廈五樓,支票抬頭請書明支付「香港醫學會」。參加者可獲醫務委員會/香港醫學會持續醫學進修計劃積分一分(除特別註明外)。其他專科學院之學分尚在申請中。(秘書處傳真號碼:2865 0943)
為響應環保及為免郵遞延誤,秘書處將以手機短訊通知講課報名結果。因此,請準確填上 閣下之手機號碼以便接收通知,倘若 閣下沒有手提電話,秘書處仍會以郵寄方式把講課確認通知書寄上。參加者如沒有收到任何通知,請致電2527 8452查詢。
Please register for participation. First come, first served. 名額有限請早登記TYPHOON/BLACK RAINSTORM POLICY
When Tropical Storm Warning Signal No. 8 (or above) or the Black Rainstorm Warning Signal is hoisted within 3 hours of the commencement time, the relevant CME function will be cancelled. (i.e. CME starting at 2:00 pm will be cancelled if the warning signal is hoisted or in force any time between 11:00 am and 2:00 pm).
The function will proceed as scheduled if the signal is lowered three hours before the commencement time. (i.e. CME starting at 2:00 pm will proceed if the warning signal is lowered at 11:00 am, but will be cancelled even if it is lowered at 11:01 am).
When Tropical Storm Warning Signal No. 8 (or above) or the Black Rainstorm Warning Signal is hoisted after CME commencement, announcement will be made depending on the conditions as to whether the CME will be terminated earlier or be conducted until the end of the session.
The above are general guidelines only. Individuals should decide on their CME attendance according to their own transportation and work/home location considerations to ensure personal safety.
Reply Slip 回條I would like to register for the following CME lecture(s): 本人欲報名參加以下講課:
Please “✓” as appropriate. 請在適用處加上✓號
Name 姓名 :
I enclose herewith a cheque of
現隨表格付上支票一張作為講課之報名費用: HK$ 港幣
HKMA Membership No. or HKMA CME No. 會員編號或進修號碼:
Fax No. 傳真 : Date 日期:
Data collected will be used and processed for the purposes related to the MCHK/HKMA CME Programme only. All registration fees are not refundable or transferable.
個人資料將用於有關香港醫學會持續醫學進修計劃之事宜。所有報名費用將不給予退還或轉授予其他會員。
(Mandatory for emergency contact or SMS 必須填寫用以緊急聯絡或接收短訊)
Mobile No. 手機號碼 : Signature 簽名 :
HKMA Member
HK$50
CME Participants
HK$80
11 June 2015
(Thursday)
HKMA Structured CME Programme with HKS&H Year
2015 session VI: Ultrasound for Head & Neck Disease
HKMA Structured CME Programme with HKS&H
香港醫學會THE HONG KONG
MEDICAL ASSOCIATION
27HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
CME Lectures in June 2015
REPLY SLIP
Organizer : HKMA Yau Tsim Mong Community Network
Date : Tuesday, 9 June 2015 Friday, 26 June 2015
Topic and Speaker : Diet and Chest Pain
Dr. KO Wai Chin
Specialist in Cardiology
Update on the Management of Hypertension
Dr. LEUNG Tat Chi, Godwin
Specialist in Cardiology
Time : 1:00 – 2:00 p.m. Registration & Lunch
2:00 – 2:45 p.m. Lecture
2:45 – 3:00 p.m. Q&A Session
Venue : Pearl Ballroom, Level 2, Eaton, Hong Kong, 380 Nathan Road, Kowloon
Moderator : Dr. SO Chun
Committee Member,
HKMA YTM Community Network
Dr. HO Fung
Committee Member,
HKMA YTM Community Network
Deadline : Friday, 22 May 2015 Friday, 12 June 2015
Fee : Free-of-charge
Capacity : 60. Registration is strictly required on a first come, first served basis. Priority will be given to
doctors practising in Yau Tsim Mong districts.
Enquiry : Ms. Candice TONG, Tel: 2527 8285
*Please call and confirm that your facsimile has been successfully transmitted to the HKMA
Secretariat if you do not receive confirmation 14 days before the event.
Sponsor :
CME
Accreditation
: Pending
HKMA Yau Tsim Mong Community Network Fax: 2865 0943CME Lectures in June 2015
I would like to register for the following lecture(s): Please “✓” as appropriate
9 June 2015 26 June 2015
Name: HKMA No.:
Mobile No.*: Fax:
*Please fill in your updated mobile number so that you can be notified of your application via SMS. If you do not have a mobile phone, the Secretariat will still issue a confirmation letter to you.
Practising location: In Yau Tsim Mong (Please specify *: )
Others (Please specify: )
* Null entry will be treated as non-Yau Tsim Mong member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to these events only.
THE HONG KONGMEDICAL ASSOCIATION
CMEnotifications
28 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Reference Framework for Preventive Care
for Older Adults in Primary Care Settings
HKMA Hong Kong East Community Network
and Primary Care Office of the Department of Health
REPLY SLIP
Date : Thursday, 11 June 2015
Speaker : Dr. LUK Kam Hung
Deputy Consultant in-charge (Primary Care), Primary Care Office, Department of Health
Time : 1:00 – 2:00 p.m. Registration & Lunch
2:00 – 2:45 p.m. Lecture
2:45 – 3:00 p.m. Q & A Session
Venue : The HKMA Wanchai Premises,
5/F, Duke of Windsor Social Services Building,
15 Hennessy Road, Wanchai
Moderator : Dr. LAM See Yui, Joseph
Committee Member, HKMA Hong Kong Community Network
Deadline : Friday, 29 May 2015
Fee : Free-of-charge
Capacity : 80. Registration is strictly required on a first come, first served basis. Priority will be given to
doctors practising in Hong Kong East districts.
Enquiry : Ms. Candice TONG, Tel: 2527 8285
*Please call and confirm that your facsimile has been successfully transmitted to the HKMA Secretariat if you do not
receive confirmation 14 days before the event.
CME Accreditation : Pending
HKMA Hong Kong East Community Network Fax: 2865 0943Reference Framework for Preventive Care for Older Adults in Primary Care Settings
I would like to register for the above lecture. Please “✓” as appropriate
Name: HKMA No.:
Mobile No.*: Fax:
* Please fill in your updated mobile number so that you can be notified of your application via SMS. If you do not have a mobile phone, the Secretariat will still issue a confirmation letter to you.
Practising location: In Hong Kong East (Please specify *: )
Others (Please specify: )* Null entry will be treated as non-Hong Kong East member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to this event only.
香港醫學會THE HONG KONG
MEDICAL ASSOCIATIONCo-organised by
CMEnotifications
29HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Reference Framework for Preventive Care
for Older Adults in Primary Care Settings
The HKMA Kowloon West Community Network
and Primary Care Office of the Department of Health
Date : Tuesday, 23 June 2015
Speaker : Dr. MOK Chun Keung, Francis
Chief of Service, Department of Medicine and Geriatrics, Tuen Mun Hospital
Time : 1:00 – 2:00 p.m. Registration & Lunch
2:00 – 2:45 p.m. Lecture
2:45 – 3:00 p.m. Q & A Session
Venue : Crystal Room I-III, 30/F., Panda Hotel,
3 Tsuen Wah Street, Tsuen Wan, N.T.
Moderator : Dr. WONG Wai Hong, Bruce
Hon. Secretary, HKMA Kowloon West Community Network
Deadline : Friday, 12 June 2015
Fee : Free-of-charge
Capacity : 50. Registration is strictly required on a first come, first served basis. Priority will be given to
doctors practising in Kowloon West district.
Enquiry : Miss Hana YEUNG, Tel: 2527 8285
*Please call and confirm that your facsimile has been successfully transmitted to the HKMA
Secretariat if you do not receive confirmation 14 days before the event.
CME Accreditation : Pending
REPLY SLIP
HKMA Kowloon West Community Network Fax: 2865 0943Reference Framework for Preventive Care for Older Adults in Primary Care Settings
I would like to register for the above event. Please “✓” as appropriate
Name: HKMA No.:
Mobile No.*: Fax No.:
*Please fill in your updated mobile number so that you can be notified of your application via SMS. If you do not have a mobile phone, the Secretariat will still issue a confirmation letter to you.
Practising location: In Kowloon West (Please specify *: )
Others (Please specify: )
* Null entry will be treated as non-Kowloon West member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to this event only.
THE HONG KONGMEDICAL ASSOCIATION Co-organized by
CMEnotifications
30 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
REPLY SLIP
香港醫學會THE HONG KONG
MEDICAL ASSOCIATION
Date (All Tuesdays) Topic and Speaker Moderator
16 June 2015
Sponsored by
1. Can We Prevent Sudden Cardiac Death during Sports Event?
Dr. CHAN Wai Kwong, Andy
Specialist in Cardiology
Dr. LAM Tzit Yuen, DavidChairman,
HKMA Yau Tsim Mong
Community NetworkSponsored by 2. Common Sports Lower Limbs Injuries
Dr. HO Hok Ming
Specialist in Orthopaedics & Traumatology
30 June 2015
Sponsored by
1. Exercises-Induced Asthma
Dr. CHAN Ka Wing, Joseph
Specialist in Respiratory Medicine
Dr. CHENG Kai Chi, ThomasHon. Secretary,
HKMA Yau Tsim Mong
Community NetworkSponsored by 2. Common Sports Upper Limbs Injuries
Dr. HO Hok Ming
Specialist in Orthopaedics & Traumatology
7 July 2015
Sponsored by
1. Musculoskeletal Ultrasound as a Point of Care for Diagnosing
and Managing Common Musculoskeletal and Sports Injuries
Dr. LAM King Hei, Stanley
Specialist in Family Medicine
Dr. CHAN Wai Keung, RickyVice-chairman,
HKMA Yau Tsim Mong
Community Network
2. Fundamentals of Sports and Exercise Nutrition
Ms. Sylvia LAM
Senior Registered Dietitian,
Chairman of Hong Kong Dietitians Association
Time : 1:00 – 1:45 p.m. Registration & Lunch1:45 – 2:15 p.m. Lecture 1 and Q&A session2:15 – 2:45 p.m. Lecture 2 and Q&A session
Venue : Jade Ballroom, Level 2, Eaton, Hong Kong, 380 Nathan Road, Kowloon
Deadline : Monday, 1 June 2015
Fee : Free-of-charge
Capacity : 80. Registration is strictly required on a first come, first served basis. Priority will be given to doctors practising in Yau Tsim Mong districts.
Enquiry : Ms. Candice TONG, Tel: 2527 8285 (HKMA Secretariat)* Please call and confirm that your facsimile has been successfully transmitted to the HKMA Secretariat if you do not receive confirmation 14 days before the event.
Certification : Certificate will be issued to registrants who attend 2 sessions or more.
CME Accreditation : Pending
Certificate Course on Sports Medicine
The HKMA Yau Tsim Mong Community Network
HKMA Yau Tsim Mong Community Network Fax: 2865 0943Certificate Course on Sports Medicine
I would like to register for the following session(s)*: Please “✓” as appropriate
16 June 2015 30 June 2015 7 July 2015
(*Certificate will be issued to registrants who attend 2 sessions or more).
Name: HKMA No.:
Mobile No.*: Fax No.:
*Please fill in your updated mobile number so that you can be notified of your application via SMS. If you do not have a mobile phone, the Secretariat will still issue a confirmation letter to you.
Practising location: In Yau Tsim Mong (Please specify *: )
Others (Please specify: )
* Null entry will be treated as non-Yau Tsim Mong member registration.
Signature: Date:
Data collected will be used and processed for the purposes related to this event only.
Organized by
CMEnotifications
32 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Meeting Highlights
HKMA Structured CME Programme with Hong Kong Sanatorium & Hospital 2015
Dr. YEUNG Yuk Pang (right) presenting a souvenir to the speaker, Dr. SIU Wing Tai (left).
The HKMA Central, Western and Southern Community Network (CW&SCN) ~ Dr. YIK Ping Yin
Dr. HO Kwan Lun (left, speaker) receiving a souvenir from Dr. YIK Ping Yin (moderator) during the lecture on 15 April 2015
Dr. HO Kwan Lun,
Specialist in Urology,
delivered a lecture
on “Management of
Erectile Dysfunction in
Primary Practice – An
Urologist’s Perspective”
on Wednesday, 15 April
2015.
Dr. SIU Wing Tai,
Specialist in General
Surgery, delivered a
luncheon lecture on
“What does a General
Surgeon Do Nowadays?”
on Thursday, 9 April
2015 at the HKMA
Central Premises. Dr.
YEUNG Yuk Pang kindly
acted as the moderator
for the event.
The HKMA Hong Kong East Community Network (HKECN) ~ Dr. CHAN Nim Tak, Douglas
The “Certificate Course on Neurology” began on Thursday, 16 April 2015 with
the first lecture entitled “Update on Stroke”, which was delivered by Dr. TSOI
Tak Hong, Specialist in Neurology.
Dr. LUK Kam Hung, Deputy Consultant in-charge (Primary Care) of Primary Care
Office of Department of Health, will deliver a talk on “Reference Framework for
Preventive Care for Older Adults in Primary Care Settings” on Thursday, 11 June
2015. Interested members please refer to the announcement on p.28 for details
and enrolment.
Group photo taken during the lecture on 16 April 2015From left: Dr. Kenneth YIP, Dr. Douglas CHAN, Dr. TSOI Tak Hong (speaker), Dr. TSANG Kin Lun and Dr. Dominic YOUNG (moderator)
The HKMA Kowloon West Community Network (KWCN) ~ Dr. TONG Kai SingThe Network and the Primary Care Office of the Department of Health will co-organize a lecture on “Reference Framework for
Preventive Care for Older Adults in Primary Care Settings” on Tuesday, 23 June 2015. Dr. MOK Chun Keung, Francis, Chief of
Service of the Department of Medicine and Geriatrics of Tuen Mun Hospital, is invited to be the speaker. Interested members
please refer to the announcement on p.29 for details and enrolment.
The HKMA New Territories West Community Network (NTWCN) ~ Dr. CHEUNG Kwok Wai, AlvinDr. CHAN Hoi Chung, Samuel, Family Doctor and Personal Physical Trainer, delivered
a lecture on “Management of Ketamine Abusers with Various Medical and Psychiatric
Complications” on Thursday, 23 April 2015.
The 2 remaining sessions of the “Certificate Course on Pain” will be organized in June
2015. Details are shown below:
Date (Thursdays) Topic Speaker
11 June 2015 A New Approach for Treating Elderly
Patients Suffering from Postherpetic
Neuralgia (PHN)
Dr. LO Man Wai
18 June 2015 Herpes Zoster and Post Herpetic
Neuralgia – Are They Related?
Dr. TONG Ka Fai,
HenryDr. Samuel CHAN (right, speaker) receiving a souvenir from Dr. TSANG Yat Fai (moderator) during the lecture on 23 April 2015
33HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Meeting Highlights
The HKMA Yau Tsim Mong Community Network (YTMCN) ~ Dr. LAM Tzit Yuen, DavidA lecture on “Treating Patient Present with Joint Pain” was delivered by Dr. SUNG Chi Keung, Specialist in Rheumatology, on Tuesday, 14 April 2015.
Dr. KO Wai Chin, Specialist in Cardiology, will present on “Diet and Chest Pain” on Tuesday, 9 June 2015. Dr. LEUNG Tat Chi, Godwin, Specialist in Cardiology, will present on “Update on the Management of Hypertension” on Friday, 26 June 2015. Interested members please refer to the announcement on p.27 for details and enrolment.
The 3-session “Certificate Course on Sports Medicine” will be organized on Tuesdays, 16 June, 30 June and 7 July 2015, each consists of two mini lectures. Details of the Course is as below. Interested members please refer to the announcement on p.30 for details and enrolment.
Date (Tuesdays) Topic Speaker
16 June 2015 Can we Prevent Sudden Cardiac Death during Sports Event? Dr. CHAN Wai Kwong, Andy
Common Sports Lower Limbs Injuries Dr. HO Hok Ming
30 June 2015 Exercises-Induced Asthma Dr. CHAN Ka Wing, Joseph
Common Sports Upper Limbs Injuries Dr. HO Hok Ming
7 July 2015 Musculoskeletal Ultrasound as a Point of Care for Diagnosing and Managing Common Musculoskeletal and Sports Injuries
Dr. LAM King Hei, Stanley
Fundamentals of Sports and Exercise Nutrition Ms. Sylvia LAM
Dr. HO Hok Ming (left, moderator) presenting a
souvenir to Dr. SUNG Chi Keung (speaker) during
the lecture on 14 April 2015
The HKMA Shatin Doctors Network (SDN) ~ Dr. FUNG Yee Leung, Wilson and Dr. MAK Wing KinDr. HO Ka Keung, Specialist in Dermatology & Venereology, presented on “Update in Management of Acne Vulgaris” on Wednesday, 15 April 2015.
The following lectures will be held in May:
Date Topic Speaker Registration/Enquiry
27 May 2015 (Wednesday) Cervical Myelopathy and it's Treatment Dr. HO Chin Hung Ms. Sharon LAMT: 8226 9582
29 May 2015 (Friday) An Insulin-Independent Approach to Managing Patients with Type 2 Diabetes
Dr. FUNG Lai Ming Mr. Johnson SHUMT: 8209 9667
Group photo taken during the lecture on 15 April 2015From left: Dr. MAK Wing Kin (moderator), Dr. HO Ka Keung (speaker) and Dr. WONG Tsz Kau
The HKMA Kowloon East Community Network (KECN) ~ Dr. AU Ka Kui, Gary
The first session of the “CME Course for Health
Personnel 2015” t it led “Update on Macular
Degeneration” was given by Dr. TANG Hoi Yau,
Heather, Associate Consultant of the Department
of Ophthalmology of United Christian Hospital,
on Saturday, 18 April 2015.
Dr. CHUNG Lap Yan, Kenneth, Specialist in
Paediatric Surgery, presented on “Update on
Management of Nocturnal Enuresis of Children”
on Thursday, 23 April 2015.
Dr. Kenneth CHUNG (left, speaker) receiving a souvenir from Dr. Danny MA (moderator) during the lecture on 23 April 2015
CMECalendar
35HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
# for whole function
May 2015
16 – 17 May 2015
(Sat-Sun)
Hong Kong University – Department of Medicine
20th Hong Kong Medical Forum
Room N101, 1/F (New Wing), Hong Kong Convention & Exhibition Centre
Administrative Assistant – Tel: 2255 4607
10#
17 May 2015
(Sun)
1:00 – 4:00 pm
Hong Kong Doctors Union
The 302nd HKDU Sunday Afternoon Symposium
Lecture Hall, 8/F, Block G, Princess Margaret Hospital, Kwai Chung, NT
Tel: 2388 2728
1.5
17 May 2015
(Sun)
3:30 – 5:30 pm
Hong Kong Doctors Union
The 303rd HKDU Sunday Afternoon Symposium
Lecture Hall, 8/F, Block G, Princess Margaret Hospital, Kwai Chung, NT
Tel: 2388 2728
1.5
18 May 2015
(Mon)
8:30 – 9:30 am
Union Hospital – Department of Paediatrics
Paediatrics Departmental Round
New Seminar Room 2, 2/F, Hospital Building, Union Hospital
Ms. Kay Ho – Tel: 2608 3800
1
18 May 2015
(Mon)
1:00 – 3:00 pm
Hong Kong Doctors Union
172nd Luncheon Meeting
Seminar Room, Hall 3F-3G, Level 3, Hong Kong Convention and
Exhibition Centre (Old Wing), 1 Harbour Road, Wanchai
Miss Cheng – Tel: 2388 2728
1
18 – 19 May 2015
(Mon-Tue)
Hospital Authority
Hospital Authority Convention
Theatre 1&2, Convention Hall, Hong Kong Convention and Exhibition Centre,
Wanchai
Mr. Banny Wong – Tel: 2300 6569
10#
19 May 2015
(Tue)
1:00 – 2:00 pm
Hong Kong College of Psychiatrists
Hospital Authority – United Christian Hospital – training centre
Balint Group
Conference Room, United Christian Hospital/Conference Room,
Yung Fung Shee Psychiatric Centre
Ms. Lucita Chan – Tel: 2871 8777
1
20 May 2015
(Wed)
9:30 – 12:30 pm
Hong Kong Poison Information Centre
Hong Kong College of Emergency Medicine
Certificate Program in Clinical Toxicology 2015 (Monthly Sessions)
Conference Room, 1/F, Block F, United Christian Hospital
Ms. Winnie Cheung – Tel: 3513 5096
3
20 May 2015
(Wed)
12:45 – 2:00 pm
Our Lady of Maryknoll Hospital
Grand Round/Journal Club (Wednesday Educational Meeting April-June 2015)
Conference Room A, 1/F, OPD Block, Our Lady of Maryknoll Hospital
Ms. Clara Tsang – Tel: 2354 2440
1
20 May 2015
(Wed)
1:00 – 2:00 pm
Castle Peak Hospital
Improvement of Schizophrenia Treatment and the Place of Asenapine
(Video Lecture)
Lecture Theatre, Block D, Castle Peak Hospital
Ms. Wong Suk Yee – Tel: 2456 7153
1
20 May 2015
(Wed)
2:00 – 4:00 pm
Hong Kong Academy of Medicine
Acute Shoulder Injuries and Non-acute Shoulder Disorders
Multi-function Room, G/F, Block D, Queen Elizabeth Hospital, Kowloon
Ms. Joanne Ho – Tel: 2871 8747
2
20 May 2015
(Wed)
4:15 – 5:15 pm
Hong Kong University – Department of Obstetrics & Gynaecology
Tumour Board Meeting – clinical-pathological conference on gynaecological
oncology cases
Rm 215, 2/F, Seminar Room, Clinical Pathology Building, Queen Mary Hospital
Ms. Phyllis Kwok – Tel: 2255 4518
1
21 May 2015
(Thu)
1:00 – 3:00 pm
Hospital Authority – United Christian Hospital
Hong Kong College of Family Physicians
Hong Kong Medical Association – Kowloon East Community Network
Certificate Course for GPs 2015 – Common ENT Problems in the Community
V Cuisine, 6/F, Holiday Inn Express Hong Kong Kowloon East, 3 Tong Tak Street,
Tseung Kwan O
Ms. Polly Tai – Tel: 3513 3430
1
21 May 2015
(Thu)
1:00 – 3:00 pm
Hong Kong Medical Association – New Territories West Community Network
Certificate Course on Pain
G/F, Marina Club House, Gold Coast Yacht and Country Club, 1 Castle Peak
Road, Castle Peak Bay, Hong Kong
Miss Hana Yeung – Tel: 2527 8285
1
22 May 2015
(Fri)
1:00 – 2:00 pm
Tuen Mun Hospital – Department of Obstetrics & Gynaecology
CME Programme for January-June 2015
Room SB1034 A&B, Conference Room, 1/F, Special Block, Tuen Mun Hospital
Ms. Angela Cheung – Tel: 2468 5404
1
23 May 2015
(Sat)
9:30 – 11:30 am
Hospital Authority
Hong Kong College of Community Medicine
Case presentations and Journal presentations in areas related to Administrative
Medicine
Room 524N, 5/F, Hospital Authority Building, 147B Argyle Street, Kowloon
Ms. Yandy Ho – Tel: 2871 8745
2
26 May 2015
(Tue)
1:00 – 3:00 pm
Hong Kong Medical Association – Kowloon West Community Network
Psoriatic Arthritis: Does Early Diagnosis Make A Difference?
Crystal Room I-III, 30/F, Panda Hotel, 3 Tsuen Wah Street, Tsuen Wan, NT
Miss Hana Yeung – Tel: 2527 8285
1
26 May 2015
(Tue)
5:30 – 6:30 pm
Hospital Authority – Hong Kong East Cluster – Cluster Trauma Service
Committee
HKEC Trauma Audit
Lecture Theatre, 1/F, Pathology Block, Pamela Youde Nethersole Eastern
Hospital, 3 Lok Man Road, Chai Wan, Hong Kong
Ms. Natalie Choi – Tel: 2595 7312
1
26 – 27 May 2015
(Tue-Wed)
Hong Kong College of Emergency Medicine
American Heart Association (AHA) Pediatric Advanced Life Support
(PALS) Courses
HKEC Training Centre for Healthcare Management & Clinical Technology,
Pamela Youde Nethersole Eastern Hospital
Ms. Cherry Kwok – Tel: 2871 8877
10#
27 May 2015
(Wed)
12:45 – 2:00 pm
Our Lady of Maryknoll Hospital
Grand Round/Journal Club (Wednesday Educational Meeting April-June 2015)
Conference Room A, 1/F, OPD Block, Our Lady of Maryknoll Hospital
Ms. Clara Tsang – Tel: 2354 2440
1
27 May 2015
(Wed)
1:00 – 3:00 pm
Hong Kong Medical Association – Central, Western & Southern Community
Network
Advances in Diagnosis and Management of Male Pattern Hair Loss
HKMA Central Premises, Dr. Li Shu Pui Professional Education Centre, 2/F,
Chinese Club Building, 21-22 Connaught Road, Central, Hong Kong
Miss Hana Yeung – Tel: 2527 8285
1
27 May 2015
(Wed)
1:00 – 3:00 pm
Hong Kong Medical Association – Shatin Doctors Network
Cervical Myelopathy & it’s Treatment
Chairman Room, Level 2, Royal Park Hotel, 8 Pak Hok Ting Street, Shatin, NT
Ms. Sharon Lam – Tel: 8226 9582
1
27 May 2015
(Wed)
4:15 – 5:15 pm
Hong Kong University – Department of Obstetrics & Gynaecology
Tumour Board Meeting – clinical-pathological conference on gynaecological
oncology cases
Rm 215, 2/F, Seminar Room, Clinical Pathology Building, Queen Mary Hospital
Ms. Phyllis Kwok – Tel: 2255 4518
1
28 May 2015
(Thu)
8:30 – 10:30 am
Hong Kong Sanatorium & Hospital – Orthopaedic & Sports Medicine Centre
Academic Professional Development Meeting 2015 of OSMC HKSH
(Every Fourth Thursday of the Month)
Hong Kong Sanatorium & Hospital
Ms. Cheng Hoi Yan – Tel: 2835 7890
2
28 May 2015
(Thu)
1:00 – 3:00 pm
Hong Kong Medical Association – Hong Kong East Community Network
Certificate Course on Neurology
Session 4: Parkinsonism: First Encounter and Subsequent Management
5/F, Duke of Windsor Social Service Building, 15 Hennessy Road, Wanchai,
Hong Kong
Ms. Candice Tong – Tel: 2527 8285
1
28 May 2015
(Thu)
1:00 – 3:00 pm
Hong Kong Medical Association – Kowloon East Community Network
Treatment Options in DM Treatment
V Cuisine, 6/F, Holiday Inn Express Hong Kong Kowloon East,
3 Tong Tak Street, Tseung Kwan O
Miss Hana Yeung – Tel: 2527 8285
1
28 May 2015
(Thu)
1:00 – 3:00 pm
HKDU – Tsimshatsui Study Group
Advance Treatment Strategy for Atrial Fibrillation
Nathan Room 3-Hall, 1st Floor, Eaton Hong Kong, 380 Nathan Road, Kowloon
Miss Cheng – Tel: 2388 2728
1
28 May 2015
(Thu)
6:00 – 7:00 pm
Queen Mary Hospital – Department of Neurosurgery
Neuroscience Working Group Meeting (4th Thursday of every month)
Lecture Theatre, 5th Professorial Block, Queen Mary Hospital
Ms. Sherla Yu – Tel: 2255 3368
1
28 – 29 May 2015
(Thu-Fri)
Hong Kong College of Emergency Medicine
American Heart Association (AHA) Advanced Cardiovascular Life Support (ACLS)
HKEC Training Centre for Healthcare Management & Clinical Technology,
Pamela Youde Nethersole Eastern Hospital
Ms. Cherry Kwok – Tel: 2871 8877
10
29 May 2015
(Fri)
1:00 – 3:00 pm
Hong Kong Medical Association – Yau Tsim Mong Community Network
Male LUTS: Beyond BPH Management
Diamond Room V-Hall, Level B1, Eaton, Hong Kong, 380 Nathan Road, Kowloon
Ms. Candice Tong – Tel: 2527 8285
1
31 May 2015
(Sun)
1:30 – 3:00 pm
Association of Licentiates of Medical Council of Hong Kong
1) The Overview of Asthma Treatment
2) Update on Management in Dementia
九龍亞皆老街147B號醫院管理局大樓M/F研討室ALMCHK – Tel: 2327 2869
3
CMECalendar
36 HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
Jun 2015
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kwai Chung Hospital
Level 1 Topic 18: Rehabilitation & Social Psychiatry – Explain antipsychotic treatment
Meeting Room, 1/F, Admin Block, Kwai Chung Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kwai Chung Hospital
Level 2 Topic 18: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (part 1)
Seminar Room, 1/F, Admin Block, Kwai Chung Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Pamela Youde Nethersole Eastern Hospital
Queen Mary Hospital
Level 1 Topic 18: Rehabilitation & Social Psychiatry – Explain antipsychotic treatment
J2 Seminar Room, Queen Mary Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kowloon Hospital
United Christian Hospital
Level 1 Topic 18: Rehabilitation & Social Psychiatry – Explain antipsychotic
treatment
Conference Room, 13/F, Block S, Untied Christian Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kowloon Hospital
United Christian Hospital
Level 2 Topic 18: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (part 1)
Conference Room 2, Kowloon Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Pamela Youde Nethersole Eastern Hospital
Queen Mary Hospital
Level 2 Topic 18: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (part 1)
Room 36, 1/F, East Block, Pamela Youde Nethersole Eastern Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
HA-NT East Cluster
Level 1 Topic 18: Rehabilitation & Social Psychiatry – Explain antipsychotic treatment
Multicentre Seminar Room, Tai Po Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
HA-NT East Cluster
Level 2 Topic 18: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (part 1)
Multicentre Seminar Room, Tai Po Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Castle Peak Hospital
Level 1 Topic 18: Rehabilitation & Social Psychiatry – Explain antipsychotic
treatment
Kaizen Room, Block D, Castle Peak Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Castle Peak Hospital
Level 2 Topic 18: Rehabilitation & Social Psychiatry – Explain rehabilitation plans to
patients (part 1)
Seminar Room 4, Block F, Castle Peak Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
2 Jun 2015
(Tue)
6:00 – 8:00 pm
Hong Kong College of Physicians
Palliative Medicine Grand Round
Conference Room 118, 1/F, Wai Shun Block, Caritas Medical Centre
Ms. Kathy Wong – Tel: 2991 1348
2
3 Jun 2015
(Wed)
1:30 – 3:30 pm
Hong Kong Medical Association
Medical Protection Society
Mastering Adverse Outcomes – 2 hours
Eaton, Hong Kong, 380 Nathan Road, Kowloon
HKMA CME Dept. – Tel: 2527 8452
2
3 Jun 2015
(Wed)
2:00 – 4:00 pm
Hong Kong Academy of Medicine
1) Infant and Young Child Feeding Approach to Increase Vegetable and
Fruit Intake and Weaning from Bottle;
2) Urogynaecology for Non-urogynaecologists
Lecture Theatre, G/F, Block M, Queen Elizabeth Hospital, Kowloon
Ms. Joanne Ho – Tel: 2871 8747
2
3 Jun 2015
(Wed)
4:15 – 5:15 pm
Hong Kong University – Department of Obstetrics & Gynaecology
Tumour Board Meeting – clinical-pathological conference on gynaecological
oncology cases
Rm 215, 2/F, Seminar Room, Clinical Pathology Building, Queen Mary Hospital
Ms. Phyllis Kwok – Tel: 2255 4518
1
3 Jun 2015
(Wed)
5:00 – 7:30 pm
Hong Kong College of Emergency Medicine
Joint Clinical Meeting & Didactic Lecture (JCM)
Lecture Theatre, G/F, Block M; Multi-Function Room, G/F, Block D; Seminar
Room, G/F, Block A, 12/F, Block R, Lecture Theatre, Queen Elizabeth Hospital
Ms. Cherry Kwok – Tel: 2871 8877
2
4 Jun 2015
(Thu)
8:30 – 9:30 am
Hong Kong Sanatorium & Hospital-Neurology Centre
Joint neurology – neurosurgery clinical meeting
4/F, Function Room, Hong Kong Sanatorium & Hospital
Ms. Linda Chan – Tel: 2835 7287
1
5 Jun 2015
(Fri)
1:00 – 2:00 pm
Tuen Mun Hospital – Department of Obstetrics & Gynaecology
Mortality and Morbidity Meeting – Obstetrics
Room SB1034 A&B, Conference Room, Special Block, Tuen Mun Hospital
Ms. Angela Cheung – Tel: 2468 5404
1
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kwai Chung Hospital
Level 1 Topic 19: Forensic Psychiatry – Assess violent risk, with subsequent
verbal report to a consultant
Meeting Room, 1/F, Admin Block, Kwai Chung Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kowloon Hospital
United Christian Hospital
Level 1 Topic 19: Forensic Psychiatry – Assess violent risk, with subsequent
verbal report to a consultant
Conference Room, Room 2080, 2/F, PYPC
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kowloon Hospital
United Christian Hospital
Level 2 Topic 19: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (Part II)
Conference Room 2, Kowloon Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kwai Chung Hospital
Level 2 Topic 19: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (Part II)
Seminar Room, 1/F, Admin Block, Kwai Chung Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Pamela Youde Nethersole Eastern Hospital
Queen Mary Hospital
Level 1 Topic 19: Forensic Psychiatry – Assess violent risk, with subsequent
verbal report to a consultant
J2 Seminar Room, Queen Mary Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Pamela Youde Nethersole Eastern Hospital
Queen Mary Hospital
Level 2 Topic 19: Rehabilitation & Social Psychiatry – Explain rehabilitation plans to
patients (Part II)
Room 36, 1/F, East Block, Pamela Youde Nethersole Eastern Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
HA-NT East Cluster
Level 1 Topic 19: Forensic Psychiatry – Assess violent risk, with subsequent
verbal report to a consultant
Multicentre Seminar Room, Tai Po Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
HA-NT East Cluster
Level 2 Topic 19: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (Part II)
Multicentre Seminar Room, Tai Po Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Castle Peak Hospital
Level 1 Topic 19: Forensic Psychiatry – Assess violent risk, with subsequent
verbal report to a consultant
Kaizen Room, Block D, Castle Peak Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
9 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Castle Peak Hospital
Level 2 Topic 19: Rehabilitation & Social Psychiatry – Explain rehabilitation
plans to patients (Part II)
Seminar Room 4, Block F, Castle Peak Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
10 Jun 2015
(Wed)
8:30 – 9:30 am
Union Hospital
Mortality and Morbidity Meeting (Regular Meeting 2015)
Training Room, MIC, 8/F, Hospital Building, Union Hospital
Ms. Penny Fok – Tel: 2608 3287
1
10 Jun 2015
(Wed)
12:45 – 2:00 pm
Our Lady of Maryknoll Hospital
Grand Round/Journal Club (Wednesday Educational Meeting April-June 2015)
Conference Room A, 1/F, OPD Block, Our Lady of Maryknoll Hospital
Ms. Clara Tsang – Tel: 2354 2440
1
CMECalendar
37HKMA CME Bulletin 持續醫學進修專訊 May 2015www.hkmacme.org
10 Jun 2015
(Wed)
2:00 – 4:00 pm
Hong Kong Academy of Medicine
1) Updates on DM Nephropathy; 2) Nuclear Medicine & Molecular Imaging-An
Evolution from “Unclear Medicine”
Lecture Theatre, G/F, Block M, Queen Elizabeth Hospital, Kowloon
Ms. Joanne Ho – Tel: 2871 8747
2
10 Jun 2015
(Wed)
4:15 – 5:15 pm
Hong Kong University – Department of Obstetrics & Gynaecology
Tumour Board Meeting – clinical-pathological conference on gynaecological
oncology cases
Rm 215, 2/F, Seminar Room, Clinical Pathology Building, Queen Mary Hospital
Ms. Phyllis Kwok – Tel: 2255 4518
1
10 Jun 2015
(Wed)
5:00 – 7:00 pm
Hong Kong Poison Information Centre
Hospital Authority – United Christian Hospital
Monthly Meeting of HKPIC (Presentation and discussion on interesting cases
of the month)
Lecture Theatre, Block F, United Christian Hospital
Ms. Winnie Cheung – Tel: 3949 5096
2
10 Jun 2015
(Wed)
6:30 – 9:30 pm
Hong Kong Medical Association
Medical Protection Society
Mastering Professional Interactions
HKMA Dr. Li Shu Pui Professional Education Centre, 2/F, Chinese Club
Building, 21-22 Connaught Road, Central, Hong Kong
HKMA CME Dept. – Tel: 2527 8452
2.5
11 Jun 2015
(Thu)
1:00 – 3:00 pm
Hong Kong Medical Association – New Territories West Community Network
Certificate Course on Pain
G/F, Marina Club House, Gold Coast Yacht and Country Club, 1 Castle Peak
Road, Castle Peak Bay, Hong Kong
Miss Hana Yeung – Tel: 2527 8285
1
11 Jun 2015
(Thu)
1:00 – 3:00 pm
Hong Kong Medical Association – Hong Kong East Community Network
Reference Framework for Preventive Care for Older Adults in Primary
Care Settings
5/F, Duke of Windsor Social Service Building, 15 Hennessy Road, Wanchai,
Hong Kong
Ms. Candice Tong – Tel: 2527 8285
1
11 Jun 2015
(Thu)
1:15 – 3:00 pm
Hong Kong Medical Association
Hong Kong Sanatorium & Hospital
HKMA Structured CME Programme with HKS&H Session 8: Ultrasound for
Head & Neck Disease
Function Room A, HKMA Dr. Li Shu Pui Professional Education Centre, 2/F,
Chinese Club Building, 21-22 Connaught Road Central, Hong Kong
HKMA CME Dept. – Tel: 2527 8452
1
11 Jun 2015
(Thu)
8:30 – 10:30 pm
Union Hospital
Association of Private Orthopaedic Surgeons
Hong Kong Sanatorium & Hospital – Orthopaedic & Sports Medicine Centre
Orthopaedic Clinical Meeting – Teleconference (Every Second Thursday of the
Month)
Hong Kong Sanatorium & Hospital/Union Hospital
Ms. Cheng Hoi Yan – Tel: 2835 7890
2
12 Jun 2015
(Fri)
1:00 – 2:00 pm
Tuen Mun Hospital – Department of Obstetrics & Gynaecology
CME Programme for January-June 2015
Room SB1034 A&B, Conference Room, 1/F, Special Block, Tuen Mun Hospital
Ms. Angela Cheung – Tel: 2468 5404
1
13 Jun 2015
(Sat)
2:15 – 4:15 pm
Hong Kong Medical Association
Hong Kong College of Family Physicians
Our Lady of Maryknoll Hospital
Refresher Course for Health Care Providers 2014/2015
– Primary care rheumatology
Training Room II, 1/F, OPD Block, Our Lady of Maryknoll Hospital, 118 Shatin
Pass Road, Wong Tai Sin, Kowloon
Ms. Clara Tsang – Tel: 2354 2440
2
13 Jun 2015
(Sat)
2:30 – 5:30 pm
Hong Kong Medical Association
Medical Protection Society
Mastering Difficult Interactions with Patients
HKMA Dr. Li Shu Pui Professional Education Centre, 2/F, Chinese Club Building,
21-22 Connaught Road, Central, Hong Kong
HKMA CME Dept. – Tel: 2527 8452
2.5
15 Jun 2015
(Mon)
8:30 – 9:30 am
Union Hospital – Department of Paediatrics
Paediatrics Departmental Round
New Seminar Room 2, 2/F, Hospital Building, Union Hospital
Ms. Kay Ho – Tel: 2608 3800
1
15 Jun 2015
(Mon)
1:00 – 2:00 pm
Hong Kong University – Family Medicine and Primary Care
Department of Family Medicine and Primary Care Research Meetings
Department of Family Medicine and Primary Care, 3/F, Ap Lei Chau Clinic,
161 Main Street, Ap Lei Chau, Hong Kong
Ms. Crystal Wong – Tel: 2518 5654
1
16 Jun 2015
(Tue)
1:00 – 2:45 pm
Hong Kong Medical Association – Yau Tsim Mong Community Network
Certificate Course on Sports Medicine
Session 1A: Can We Prevent Sudden Cardiac Death during Sports Event?
Session 1B: Common Sports Lower Limbs Injuries
Jade Ballroom, Level 2, Eaton, Hong Kong, 380 Nathan Road, Kowloon
Ms. Candice Tong – Tel: 2527 8285
1
16 Jun 2015
(Tue)
1:00 – 5:00 pm
Matilda International Hospital
Certificate course on incident/accident reporting and documentation for hospital
staff
Lecture Hall, 4/F, Matilda International Hospital
Ms. Bonita Lam – Tel: 2849 0358
3
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kwai Chung Hospital
Level 1 Topic 20: Forensic Psychiatry – Interview a patient with schizophrenia who
has committed an offence for the purpose of writing a medical report
Meeting Room, 1/F, Admin Block, Kwai Chung Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kwai Chung Hospital
Level 2 Topic 20: Substance Misuse & Addiction Psychiatry – Assessment of
substance abuse (Part 1)
Seminar Room, 1/F, Admin Block, Kwai Chung Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Pamela Youde Nethersole Eastern Hospital
Queen Mary Hospital
Level 1 Topic 20: Forensic Psychiatry – Interview a patient with schizophrenia who
has committed an offence for the purpose of writing a medical report
J2 Seminar Room, Queen Mary Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kowloon Hospital
United Christian Hospital
Level 1 Topic 20: Forensic Psychiatry – Interview a patient with schizophrenia who
has committed an offence for the purpose of writing a medical report
Conference Room, Room 2096, CPS Office, 2/F, PYPC
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Kowloon Hospital
United Christian Hospital
Level 2 Topic 20: Substance Misuse & Addiction Psychiatry – Assessment of
substance abuse (Part 1)
Conference Room 2, Kowloon Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Pamela Youde Nethersole Eastern Hospital
Queen Mary Hospital
Level 2 Topic 20: Substance Misuse & Addiction Psychiatry – Assessment of
substance abuse (Part 1)
Room 36, 1/F, East Block, Pamela Youde Nethersole Eastern Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
HA-NT East Cluster
Level 1 Topic 20: Forensic Psychiatry – Interview a patient with schizophrenia who
has committed an offence for the purpose of writing a medical report
Multicentre Seminar Room, Tai Po Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
HA-NT East Cluster
Level 2 Topic 20: Substance Misuse & Addiction Psychiatry – Assessment of
substance abuse (Part 1)
Multicentre Seminar Room, Tai Po Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Castle Peak Hospital
Level 1 Topic 20: Forensic Psychiatry – Interview a patient with schizophrenia who
has committed an offence for the purpose of writing a medical report
Kaizen Room, Block D, Castle Peak Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
16 Jun 2015
(Tue)
3:30 – 5:30 pm
Hong Kong College of Psychiatrists
Castle Peak Hospital
Level 2 Topic 20: Substance Misuse & Addiction Psychiatry – Assessment of
substance abuse (Part 1)
Seminar Room 4, Block F, Castle Peak Hospital
Ms. Kaman Chan – Tel: 2871 8717
2
17 Jun 2015
(Wed)
9:30 – 12:30 pm
Hong Kong Poison Information Centre
Hong Kong College of Emergency Medicine
Certificate Program in Clinical Toxicology 2015 (Monthly Sessions)
Conference Room, 1/F, Block F, United Christian Hospital
Ms. Winnie Cheung – Tel: 3513 5096
3
17 Jun 2015
(Wed)
12:45 – 2:00 pm
Our Lady of Maryknoll Hospital
Grand Round/Journal Club (Wednesday Educational Meeting April-June 2015)
Conference Room A, 1/F, OPD Block, Our Lady of Maryknoll Hospital
Ms. Clara Tsang – Tel: 2354 2440
1
17 Jun 2015
(Wed)
2:00 – 4:00 pm
Hong Kong Academy of Medicine
1) Pitfalls in Interpreting Chemical Pathology Laboratory Results;
2) Management of Thyroid Nodule
Lecture Theatre, G/F, Block M, Queen Elizabeth Hospital, Kowloon
Ms. Joanne Ho – Tel: 2871 8747
2
17 Jun 2015
(Wed)
4:15 – 5:15 pm
Hong Kong University – Department of Obstetrics & Gynaecology
Tumour Board Meeting – clinical-pathological conference on gynaecological
oncology cases
Rm 215, 2/F, Seminar Room, Clinical Pathology Building, Queen Mary Hospital
Ms. Phyllis Kwok – Tel: 2255 4518
1