Embed Size (px)
Citation preview

Br Heart J 1990;63:122-8
Abnormalities of the spleen in relation tocongenital malformations of the heart: a survey ofnecropsy findings in children
Christine Anderson, William A Devine, Robert H Anderson, Diane E Debich,James R Zuberbuhler
Department ofPediatric Cardiology,Children's Hospital ofPittsburgh,Pittsburgh,Pennsylvania, USAC AndersonR H AndersonJ R ZuberbuhlerDepartment ofPathology, Children'sHospital ofPittsburgh,Pittsburgh,Pennsylvania, USAW A DevineD E DebichCorrespondence toProfessor Robert HAnderson, Department ofPaediatrics, National Heartand Lung Institute,Dovehouse Street, LondonSW3 6LY.Accepted for publication21 September 1989
AbstractA series of 1042 reports of necropsies onchildren dying at Children's Hospital ofPittsburgh was reviewed. In each case,note was taken of the status of the spleen,the lobation of the lungs, the arrange-ment of the bronchi, the morphology ofthe atrial appendages, and the presence ofany congenital malformations of theheart and great vessels and ofany malfor-mations of the abdominal organs. Therewas isomerism of the left atrial appen-dages in eight (0-77%), 13 (1-25%) showedisomerism of the right appendages, andseven (0 67%) had multiple spleens with-out having isomerism ofthe atrial appen-dages. Unexpectedly, a normal spleen wasfound in one patient with isomerism ofthe right appendages and also in a patientwith isomerism of the left appendages. Inone patient with isomeric left atrialappendages there was no spleen. Thereview showed that the morphology oftheatrial appendages, and hence thearrangement of the atria, is notaccurately predicted by the type ofspleen. The arrangement of the atrialappendages is the most reliable guide tothe recognised combinations of congen-ital cardiac malformations previously
I
described as "splenic syndromes".Because there is no certain way ofpredic-ting all the malformations in patientswith complex congenital heart disease, itis advisable to record separately for eachpatient the details oflobation ofthe lungs,the bronchial and atrial arrangement,anomalies of the heart and great vessels,the type of spleen, and any abnormalarrangement of the abdominal organs.
It is now well recognised that complex con-genital malformations of the heart areassociated with abnormalities of the spleen andabnormal arrangement of the other thoracoab-dominal organs.`' Although it became fashion-able to call these cardiac syndromes "asplenia"and "polysplenia",4 it has since become clearthat these are imperfect terms to describe theheart and its contained anomalies. This isbecause some patients without spleens have theconstellation of lesions expected in "poly-splenia", whereas the malformations expectedin "asplenia" can be found in patients withsingle or multiple spleens."6 The presence ofright or left isomerism of the atrial appen-dages' is a much more accurate guide to thecharacteristic syndromes. Furthermore, somepatients with multiple spleens and left isomer-
*t~~~~~~~~
..6..! .' 9S' 'SS*\.:::.:*
p*:...Xs-tet.
.,I,
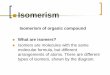
Figure I The arrangements of the bronchi are shownfrom behind in (a) a normal heart, (b) a heart with isomerism of the right bronchi, and (c) aheart with left bronchial isomerism. The left bronchus (L) is longer than the right (R). The morphologically left bronchus is below the pulmonaryartery (hyparterial) while the morphologically right bronchus is above the artery (eparterial). Black star = bronchus; white star = pulmonaryartery.
122
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from

Abnormalities of the spleen in relation to congenital malformations of the heart:a survey of necropsy findings in children
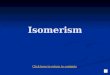
Figure 2 The normal heart is opened out to show the internal structures of themorphologically left and right atria. The tubular left atrial appendage has a narrow
junction with the venous component of the atrium whereas the triangular right atrialappendage has a broadjunction (dotted lines).
ism of the thoracic organs can have normallyconstructed hearts with the atria in their nor-
mal position.'9 But how common is this find-ing? And how frequently are accessory, as
opposed to multiple, spleens encountered bythe paediatric pathologist? These questions are
vital for those who try to understand andcategorise congenital malformations of theheart.'0°" To answer them, we have reviewedthe necropsy records from Children's Hospitalof Pittsburgh over an 11 year period to ascer-
tain the frequency and relation ofabnormalitiesof the heart and thoracoabdominal organs.
Patients and methodsWe examined the detailed reports on the 1158necropsies carried out on children who died atthe Children's Hospital of Pittsburgh from1976 to 1986 inclusive. Of these reports, 116were not included in the final analyses because
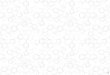
Figure 3 Multiplespleens.
the necropsy had either been exclusivelythoracic or abdominal. We did not include twocases of conjoined twins because their heartswere fused.We took information on the arrangement of
the lungs, bronchi (fig 1), and atrial appendages(fig 2) from each report and noted any con-genital abnormalities of the heart and greatvessels. These structures were assumed to benormal if not specifically described to thecontrary. The state of the spleen was recorded,as well as any evidence of abnormal arrange-ment of the other abdominal organs. Thespleen was designated to be normal, absent,multiple (fig 3), or accompanied by accessorysplenules (fig 4). Multiple spleens were recor-ded only when specifically described as such bythe reporting pathologist. It was more commonfor additional splenic tissue, when noted, to bereported as accessory. The hearts of all thepatients with isomerism of the atrial appen-dages had been retained in the Heart Museum.We re-examined these in sequential segmentalfashion, making particular note of the veno-atrial connections and any associated malfor-mations (fig 5).
ResultsTable 1 shows the general findings from thesurvey of the 1042 cases, broken down accord-ing to splenic morphology. According to themorphology of the atrial appendages, a total ofeight patients (0 77%) in the overall seriesshowed morphologically left isomerism (table2) while 13 (1*25%) showed morphologicallyright isomerism (table 3). Another seven cases(0 67%) were discovered to have multiplespleens without any evidence of isomerism ofthe atrial appendages (table 4). There were noinstances of complete absence of the spleenwithout left or right isomerism of the atrialappendages, but four cases had hypoplasticspleens (weighing, on average, 1-6 g). Thespleen in one weighed only 0 6 g.
Five of the 116 incomplete reports areworthy of mention. Two were described ashaving "polysplenia", but a postmortemexamination of the thoracic organs had notbeen performed to confirm the presence (orabsence) of isomerism of the appendages.Another patient showed isomerism of the leftatrial appendages and one isomerism of theright appendages, but no abdominal inspectionhad been carried out to record the state ofthe spleen. A fifth example of isomerism of theright appendages was noted in one of theconjoined twins. It is probable, therefore, thatthese cases would have increased the incidenceof isomerism of the left and right appendages inthe overall population.Two of the 1042 cases had a mirror image
atrial arrangement. Because the position of thelungs, bronchi, and abdominal organs showedappropriate mirror imagery these were allincluded in the category of those having normalspleens and lungs with attendant congenitalheart disease.There were 11 reports (1 .06Oo) of accessory
spleens accompanied by malrotation of the gut.
123
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from

Anderson, Devine, Anderson, Debich, Zuberbuhler
Figure 4 An accessory spleen.
One of these also had bilaterally bilobed lungsand hyparterial bronchi but all showed theusual atrial arrangement. Ten had diaphrag-matic hernias, chromosomal disorders, orbiliary atresia. Four cases had congenital heartdisease, but not in the combinations expectedfor isomerism of the atrial appendages.
Isolated malrotation of the gut with a normalspleen was noted in 19 necropsies (1 .820 ). In13 of these there were either diaphragmatichernias or chromosomal disorders. Atrialarrangement was usual in all instances, withnine patients having some form of congenitalheart disease. Abnormal lung lobation was
mentioned twice, but neither patient had an
isomeric arrangement of the bronchi.Abnormalities of lobation of the lungs were
reported in 80 cases (768%o). Thirteen (125%/ )of these had bilaterally trilobed lungs (one case
also having bilaterally eparterial bronchi). Thespleen was normal in nine of these patients andthe other four had accessory spleens. None hadeither form of isomerism of the atrial appen-dages or their cardiac manifestations. Fortyfour (4 22%) reports noted bilaterally bilobedlungs (four with accompanying bilaterally
Table 1 Summary offindingsfrom 1042 necropsies
Categories No
Cases of normal spleen:Normal lungs and normal heartNormal lungs and abnormal heartAbnormal lungs and normal heartAbnormal lungs and abnormal heart*
Cases of accessory spleens:Normal lungs and normal heartNormal lungs and abnormal heartAbnormal lungs and normal heartAbnormal lungs and abnormal heart
Cases of multiple spleens:Usual atrial arrangementLeft atrial isomerism
Cases of absent spleen:Right atrial isomerismLeft atrial iosomerism
5621933437
Total 826
11650816
Total I90
7
6Total 13
121
Total -13
% of total
53.9318-523-263-55
79-26
11-134-800771-541824
0-670-581-25
1-150-101 25
*One case had right atrial isomerism.
hyparterial bronchi). The spleen was normal in35 of these patients, eight had accessoryspleens, and the remaining patient had multiplespleens. None of these patients, however, hadeither isomerism of the left atrial appendages orthe expected cardiac lesions.
DiscussionOur review of a large series of paediatricnecropsies confirms our earlier predictions.35It is no longer reasonable to attempt to describeor diagnose congenital malformations of theheart in terms of abnormalities of the spleen.The attention given to the "splenic syn-dromes" has served its purpose in drawingattention to the cardiac malformations knownto accompany them.Our findings emphasise the relative con-
stancy of the cardiac lesions themselves. Thuson the one hand there are hearts characterisedby bilateral atrial appendages of right mor-phology. These hearts have bilateral superiorcaval veins, totally anomalous pulmonaryvenous connection, a common atrioventricularvalve, and a high proportion of double inletatrioventricular connection and an abnormalventriculoarterial connection, usually with pul-monary stenosis or atresia.' On the other handthere are hearts with bilateral appendages ofleft morphology. These hearts characteris-tically have bilateral superior venae cavae(caval veins) and a common atrioventricularvalve, but they have a relatively normalarrangement of their ventricular mass, coarc-tation rather than pulmonary atresia, and ananomalous connection of the inferior vena cava(caval vein), usually with azygos contin-uation.28 The most accurate guide to thepresence of these cardiac lesions is neitherabsence of the spleen nor the presence ofmultiple spleens. It is the existence of iso-merism of the atrial appendages.6When we describe "atrial isomerism", it
should not be presumed that each atrium, alongwith its venous connections, is an isomer of theother. Far from it. The isomerism affects onlythe appendages, and these structures are trulyisomeric. In this respect, it is the appendagesthat fulfil the criteria established by VanPraagh and his colleagues for determining themorphology of any cardiac chamber.'2 Theprinciple they established'2 is called the mor-phologic method. In essence, it states thatchambers within the heart should be identifiedaccording to their most constant components.It had been suggested that the inferior venacava (caval vein) was the most constant atrialcomponent, serving in this way to identify themorphologically right atrium.'3 The analysis ofthe present patients shows that this is not thecase.In our patients with abnormal arrangement
of the abdominal organs, where it is mostnecessary accurately to determine atrial mor-phology, presence or absence of the inferiorvena cava (caval vein) provides an ineffectivemarker of the morphologically right atrium. Incontrast, all patients with the constellation ofcardiac lesions previously known as "splenicsyndromes" would have been correctly iden-
124
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from

Abnormalities of the spleen in relation to congenital malformations of the heart:a survey of necropsy findings in children
Figure 5 The top panelsshow a heart withisomerism of the rightatrial appendages: (a)right sided atrium, (b) leftsided atrium. Note thepresence of bilateral venaecavae and terminal crests.The lower panels show theinternal arrangement ofthe atria in the presence ofisomerism of the left atrialappendages: (c) rightsided atrium, (d) left sidedatrium. Note the presenceof bilateral superior venaecavae and pulmonaryveins connecting directly tothe atria. MRAA,morphologically rightatrial appendage; RAA,right atrial appendage;morph, morphologically;MLAA, morphologicalleft atrial appendage;pulm, pulmonary.
tified on the basis of isomerism of their atrialappendages. Thus the anatomy of the appen-dage and the arrangement of its junction withthe venous atrial component provide anaccurate means of distinguishing the mor-phologically right and left atria even in thepresence of the most complex malformations ofthe heart. It is this criterion that best deter-mines the arrangement of the atria. Further-more, when the atria are abnormally formed in
association with congenital cardiac anomalies,it is more accurate to describe them in terms ofatrial isomerism rather than invoking con-siderations of malformations of the spleen.Determining the arrangement of the atria is
relatively easy for the pathologist, who holdsthe heart in his hands, and also for the cardiacsurgeon, who can readily recognise the struc-ture of the appendages as seen in the operatingroom. But what of the clinician, who is often
125
.... IS00A
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from

126 Anderson, Devine, Anderson, Debich, Zuberbuhler
Table 2 Details of eight cases of isomerism of the left atrial appendages
Feature 1 2 3 4 S 6 7 8
Right/leftilung lobation 2 2 2 2 2 2 2 2 2 2 2 2 1 2 2 2Bronchial arrangement BH BH BH BH BH RH BH RHSpleen Multiple 5 Multiple 9 Multiple 15 Multiple 12 Multiple 4 Multiple 7 Normal AbsentLiver Sym L Sym Sym L Sym Sym RGallbladder R L Mid Mid Mid Mid Mid NKPancreas Short mid Glob mid Glob Glob mid Short mid Short mid Glob GlobStomach R L L L L L R RGut Mal Mal Mal Mal Mal Mal Mal MalSuperior venae cavae Bilateral Bilateral L to Bilateral Bilateral L to Bilateral Bilateral atretic L to L-sided R to R-sided
CS to R-sided L-sided atrium left atrium atriumatrium atretic R
Inferior vena cava Bilateral SVCs Right to R- Azy cont to Azy cont to Azy cont to Azy cont to Azy cont to Azy cont to& azy veins sided atrium RSVC LSVC LSVC RSVC LSVC RSVC
Hepatic veins Confl to R- Bilateral 2 veins to R- Bilateral Bilateral Confl to L- Confl to R- Confl to R-sided atrium sided atrium sided atrium sided atrium sided atrium
Pulmonary veins To L-sided To R-sided Bilateral Bilateral To L-sided To L-sided To R-sided To L-sidedatrium atrium atrium atrium atrium atrium
Positionofheart L L L L L L R LApex ofheart L L L L L L R LArterial relations Normal Normnal Normal Normal Normal Normal Mirror image NormalAtrial defects Common Common Common Common Common Common Common Common
atrium atrium atrium atrium atrium atrium atrium atriumAtrioventricular septal defect Yes Yes Yes Yes Yes Yes Yes YesAtrioventricular valves Common valve Common valve Common valve 2 valves Common valve Common valve Common valve Common valveVentricular septal defect Yes Yes Yes No Yes Yes Yes YesAtrioventricular connection Ambig Ambig Ambig Ambig Ambig Ambig Ambig AmbigVentricular topology' RH RH RH LH RH RH LH RHVentricular arterial connection Concordant Concordant DORV 'DORV Concordant Concordant Concordant ConcordantPulmonary outflow tract Patent Patent Musc subpulm Patent Valvar pulmon Patent Musc stenosis Patent
stenosis stenosisAortic outflow tract Subaortic Stenosis Patent Subaortic Patent Stenosis Patent Patent
stenosis -obstruct bytissue tag
Coarctation Nil Shelf Nil Isthmal hypo Nil Isthmal hypo Nil Isthmal hypoArterial duct Ligament Patent Ligamnent Patent Ligament Patent Patent LigamentAorticarch L L L L L L R LLeft ventricle Normal Hypo Normal Normal Normal Normal Normal NormalOther malformations Nil Nil R juxta atrial Nil Nil Nil RV hypo Nil
append
Ambig, ambiguous; append, appendages; azy cont, azygos continuation; RH, bilaterally hyparterial; Confl, confluent; CS, coronary sinus; DORV, double outletright ventricle; Glob, globular; Hypo, hypoplasia; L, left; LH, left-hand; Ligament, ligamentous; LSVC, left superior vena cava; Mal, malrotation; Mid, midline;Musc, muscular; NK, not known; Obstruct, obstruction; Pulmon, pulmonary; R, right; RH, right-hand; R juxta, right juxtaposition of; RSVC, right superior venacava; Subpulm, subpulmonary; Sym, symmetrical.
Table 3 Details of thirteen cases of isomerism of the right atrial appendages
Feature 1 2 3 4 S 6 7 8
Right/leftlung lobation 3 3 3 3 3 3 3 3 3 3 3 3 2 2 3 2Bronchial arrangement BE BE BE BE BE BE BE BESpleen Absent Absent Absent Normal Absent Absent Absent AbsentLiver Sym Sym L Sym Sym R Sym SymGallbladder R Mid Mid NK NK R L RPancreas Short mid Short mid Glob mid L NK R R ElongStomach Mid R R LNK R R NKGut Mal Mal Mal Normal Mal Mal Mal MalSuperior venae cavae Bilateral atretic L to L-sided Bilateral Bilateral; L to Bilateral Bilateral Bilateral atretic Bilateral
right atrium L-sided A; leftatretic R
Inferior vena cava To L-sided To R-sided To L-sided To L-sided To L-sided To R-sided To R-sided To L-sidedatrium atrium atrium atrium atrium atrium atrium atrium
Hepatic veins Bilateral To IVC Bilateral To IVC To IVC To IVC To IVC To IVCPulmonary veins TAPVC TAPVC to TAPVC to 'TAPVC to TAPVC to TAPVC R to TAPVC to R- TAPVC to R-
Infradia portal vein RSVC RSVC portal vein portal L to sided A sided ALSVC
Positionofheart R R L L L L R RApexofheart R R L L L L R RArterial relations Aorta ant Aorta to R Aorta ant & Aorta ant Aorta ant Aorta to R side Aorta ant Aorta ant
right by sideAtrial defects Oval fossa Septal strand Primum Oval fossa Oval fossa & Commnon Oval fossa Septal strand
defect (AVSD) defect primum atrium defect(AVSD)
Atrioventricular septal defect Yes Nil Yes Nil Yes Nil Nil NilAtrioventricular valves Common valve Common valve Commnon valve Common valve Common valve Common valve Common valve Common valveVentricular septal defect Yes (AVSD) Yes Nil Nil Yes Nil Yes NilAtrioventricular connection Ambiguous DIRV Ambiguous DIRV Ambiguous DILV DILV DIIVVentricular topology LH RH RH RH RH LH LH NAVentricular arterial connection Discordant DORV DORV Single outlet Single outlet Concordant Single outlet Single outlet
Ao from RV Ao from RV Ao from RV Ao from IVPulmonary outflow tract PA Subpulm Subpulmn PA PA PA PA PA
Aortic outflow tract Patent Patent Patent Patent Patent Patent Patent PatentCoarctation Nil Nil Nil Nil Nil Nil Nil NilDuctus arteriosus Patent to confl Patent Ligament R-sided patent R-sided patent R-sided patent R-sided patent Ligament
PAsAortic arch R R R L L L R RLeft ventricle Hypo Slit-like Hypo Slit-like Normal Dominant NormalOther malformations Nil Nil ImperfLAVV Nil Nil RV grossly Rudimentary Solitary IV
hypo RV
Ant, anterior; Ao, aorta; AVSD, atrial or ventricular component of atrioventricular septal defect; BE, bilaterally hyparterial; DIIV, double inlet indeterminateventricle; DILV, double inlet left ventricle; DIRV, double inlet right ventricle; Elong, elongated; IVC, inferior vena cava; Imperf LAVV, imperforate leftatrioventricular valve; Infradia, infradiaphragmatic; IV, solitary and indeterminate ventricle; L-sided A, left-sided atrium; NA, not applicable; PA, pulmonaryatresia; PAs, pulmonary arteries; R-sided A, right-sided atrium; RV, right ventricle; TAPVC, totally anomalous pulmonary venous connection.
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from

Abnormalities of the spleen in relation to congenital malformations of the heart:a survey of necropsy findings in children
Table 4 Details of seven cases of multiple spleens and usual atrial arrangement
AzygosCase Right lung Left lung Bronchial No of Abnormal continuation of OtherNo lobation lobation arrangement spleens abdominal organs Heart defects inferior vena cava malformations
1 3 2 Usual 6 Globular pancreas, absent Nil No Biliary atresiagallbladder
2 3 2 Usual 7 Globular midline pancreas, ASD, Ao-pulmonary No Biliary atresiamalrotated gut window
3 3 2 Usual 6 Malrotated gut Nil No Pneumococcalsepticaemia
4 3 + Acc 2 + Acc Usual 4 Malformed stomach and POF, ductus arteriosus, Yes Diaphragmatic herniapancreas LSVC to CS
5 2 2 Usual 17 Absent gallbladder, short Nil No Biliary atresiapancreas, malrotated gut
6 2 2 Bilat hypart 5 Globular midlint pancreas, Nil Yes Biliary atresiapartially malrotated gut
7 2 1 Usual 9 Malformed pancreas, POF No Arnold-Chiarimalrotated gut malformation
Acc, accessory lobe; ASD, atrial septal defect; Ao-pulmonary, Aorto-pulmonary; Bilat hypart, bilaterally hyparterial; LSVC to CS, left superior vena cava tocoronary sinus; POF, patent oval foramen.
unable accurately to distinguish the mor-phology of the appendages and the nature oftheir junctions with the venous components. Itis recognised that inferences must be made inthese circumstances to permit the paediatriccardiologist to assess atrial arrangement, al-though it has been suggested that cross sec-tional echocardiography may, in skilled hands,permit direct recognition of the appendages.Similarly, if injections of contrast material aremade into the atrial appendages, cineangio-graphy permits direct diagnosis of atrialisomerism. None the less, if inferences are to bemade, our analysis shows that bronchial mor-phology'4 is the best guide to the existence ofisomerism of the atrial appendages. All but onecase with atrial isomerism also had bronchialisomerism. The exception was a case of rightatrial isomerism with usual bronchial
9 10 11 12 13
3 3 2 3 3 2 1 1 3 2BE Mirror image BE BE BEAbsent Absent Absent Absent AbsentSym Sym L Sym SymL L L NK LNK R R NK RL R R NK LMal Mal Mal Normal MalBilateral Right to R-sided Bilateral Bilateral Left to L-sided
atrium atrium
To L-sided L to L-sided To L-sided To R-sided To L-sidedatrium atrium atrium atrium atriumBilateral To IVC Bilateral To IVC To IVCTAPVC to portal TAPVC to portal TAPVC to TAPVC to TAPVC to R-vein vein R-sided A R-sided A sided A
R R R R RR R R R RAorta ant & left Aorta ant & left Aorta ant & left Aorta ant & left Aorta ant
Primum (DIRV) Septal strand Primum (DILV) Septal strand Common atrium
Nil Yes Nil Nil NilCommon valve Common valve Common valve Common valve Common valveNil Yes Yes Yes YesDIRV Ambiguous DILV DILV DILVLH LH LH LH LHDORV DORV Discordant Single outlet Ao Single outlet Ao
from RV from RVSubpulm stenosis Subpulm stenosis Severe subpulm PA PA
stenosisPatent Patent Patent Patent PatentNil Nil Nil Nil NilR-sided patent R-sided patent Patent Patent R-sided patent
R R R L RSlit-like Normal Normal Normal NormalNil Nil RV hypo RV hypo RV hypo
arrangement. Five patients, however, werereported to have isomeric bronchi with usualatrial arrangement in the absence of any severecardiac lesions. One of these cases was recentlyhighlighted by Devine et al,'5 but our presentanalysis shows them to be more frequent thanwe thought. Despite these "false positives",bronchial anatomy remains by far the bestinferential guide to the existence of the cardiacsyndromes previously linked with (and namedaccording to) splenic malformations. We foundas many patients with multiple spleens withnormal hearts as with isomerism of the leftatrial appendages (previously described as"polysplenia"). Those with multiple spleensand usual atrial arrangement were usuallyexamples of a syndrome known to exist withbiliary atresia.9 Their presence in such num-bers in our series may reflect Pittsburgh's roleas a major centre for liver transplantation.That, however, does not diminish the findingthat multiple spleens can no longer be regardedas an accurate pointer to the presence of aspecific syndrome of congenital heart disease.Although no patients without cardiac lesionshad no spleen, four had such gross hypoplasiaof splenic tissue that it was questionablewhether the organ would have been demon-strable by clinical diagnostic techniques.Furthermore, one patient with isomeric rightappendages had a normal spleen while anotherpatient with isomeric left appendages had nospleen.The lesions previously correlated with
splenic malformations are best diagnosed interms of isomerism ofthe atrial appendages.6 Ifdiagnosis has to be made by inference, this willbe achieved most accurately by referring to thepattern of bronchial morphology.'4 Splenicmalformations are insufficiently wellcorrelated with anomalies of the heart to justifytheir use either as an inferential guide or as aplatform for nomenclature.
We thank Dr E Yunis, Director of Pediatric Pathology, whoplaced all the facilities of his department at our disposal, andthe many pathologists who performed the initial necropsies,notably, Dr R Jaffe, Dr J Hubbard, Dr Y Hashida, and Dr STaylor. During the course of their investigation, CA and RHAwere on study leave from the National Heart and Lung Institute,University of London, and were supported by the Patrick DickMemorial Fund, the British Heart Foundation, and the JosephLevy Foundation.
127
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from

Anderson, Devine, Anderson, Debich, Zuberbuhler
1 Van Mierop LHS, Gessner IH, Schiebler GL. Asplenia andpolysplenia syndromes. Birth Defects 1972;VHI (no 5):36-44.
2 Peoples WM, Moller JH, Edwards JE. Polysplenia: a reviewof 146 cases. Pediatr Cardiol 1983;4:129-37.
3 Macartney FJ, Zuberbuhler JR, Anderson RH. Mor-phological considerations pertaining to recognition ofatrial isomerism. Consequences for sequential chamberlocalisation. Br Heart J 1980;44:657-67.
4 Van Praagh R, Van Praagh S, Vlad P, Keith JD. Anatomictypes of congenital dextrocardia. Diagnostic andembryologic implications. Am J Cardiol 1964;13:510-31.
5 Anderson RH, Sharma S, Ho SY, Zuberbuhler JR, Macart-ney FJ. Splenic syndromes, "situs ambiguus" and atrialisomerism. Rev Latina de Card Inf 1986;2:97-1 10.
6 Sharma S, Devine W, Anderson RH, Zuberbuhler JR. Thedetermination of atrial arrangement by examination ofappendage morphology in 1842 heart specimens. Br HeartJ 1988;60:227-31.
7 Van Mierop LHS, Wiglesworth FW. Isomerism of thecardiac atria in the asplenia syndrome. Lab Invest1962;11:1303-15.
8 Sharma S, Devine W, Anderson RH, Zuberbuhler JR.
Identification and analysis of left atrial isomerism. Am JCardiol 1987;60:1 157-60.
9 Chandra RS. Biliary atresia and other structural anomalies incongenital polysplenia syndrome. J Pediatr 1974;85:649-55.
10 Van Praagh R. The segmental approach to diagnosis incongenital heart disease. Birth Defects 1972;VIII (no 5):4-23.
11 Anderson RH, Becker AE, Freedom RM, et al. Sequentialsegmental analysis of congenital heart disease. PaediatrCardiol 1984;5:281-8.
12 Van Praagh R, David I, Van Praagh S. What is a ventricle?The single ventricle trap. Pediatr Cardiol 1982;2:79-84.
13 Brandt PWT, Calder AL. Cardiac connections: the segmen-tal approach to radiologic diagnosis in congenital heartdisease. Curr Probl Diagn Radiol 1977;7:1-35.
14 Deanfield JE, Leanage R, Stroobant J, Chrispin AR, TaylorJEN, Macartney FJ. Use of high kilovoltage filtered beamradiographs for detection of bronchial situs in infants andyoung children. Br Heart J 1980;44:577-83.
15 DevineWA, Debich DE, Taylor SR. Symmetrical bronchialpattern with normal atrial morphology. Int J Cardiol1988;20:395-8.
128
on August 7, 2021 by guest. P
rotected by copyright.http://heart.bm
j.com/
Br H
eart J: first published as 10.1136/hrt.63.2.122 on 1 February 1990. D
ownloaded from