Embed Size (px)
Citation preview

خدا نام به

• The patient was a 38-year-old woman who presented with shortness of breath.
• She claimed to be an active woman who used to worked actively until she began to notice progressive dyspnea while working 1 year ago.
• Her symptoms had progressed to the point that she was symptomatic while climbing a flight of stairs.
Case history

• At the time of the initial visit, her symptoms were so severe that she was breathless with activities of daily living.
• She denied any symptoms of cough, fevers, chills, and syncope, but she did complain of mild, dull, midsternal chest pain.
• She had hemoptysis and hoarseness 2w prior first visit.
• She also reported occasional palpitations.
Case history

• There was no history of venous thromboembolism, diet medication use, risk factors for HIV, and use of any illegal drugs.
• The patient hadn’t history of smoking.
• She did, however, complain of occasional muscle aches and joint pains but has not noted any other symptoms suggestive of collagen vascular disease.
• Her past medical history:not diabet ,not HTN , not IHD
Case history

Physical Exam• The patient was well developed, well
nourished, and in no acute distress.• Vitals: weight: 69 kg, height: 166 cm.pulse: 87
beats/min, SaO2: 96%, BP: 160/100 mmHg. T=37 axillary
• Head &neck: There was no scleral icterus. The nasal passages are narrow but patent.
• thyriod gland NL.• The oropharynx reveals a moderate-sized
tongue. There is no retrognathia.

• There weren’t cervical lymphadenopathy.• Skin: There were no rashes or nodules.• The heart had a regular rate and rhythm with a
normal S1 but a fixed, split S2. • There were no cardiac murmurs, rubs, or
gallops.• Pulmonary: Lungs were normal to auscultation
and percussion. There were no wheezes, rhonchi, or rales.
• Abdomen: The abdomen was soft and non tender without evidence of hepatosplenomegaly

Physical Exam
• Extremities: There was clubbing , no cyanosis, or edema.
• Neurologic: The cranial nerves were intact. Muscle strength was normal, and her gait was normal.
Lab test
• WBC (×10E3/uL):5.9• Hemoglobin (g/dL):12.4• Hematocrit (%):36.2• Platelets (×10E3/uL):267• Albumin, bilirubin, Alkaline phosphatase,
AST, ALT:nl

Chest X Rey

Latral X Rey

اول سوال
شواهد گرافی قفسه سینه به نفع کدام •نوع درگیری است؟
- لنفادنوپاتی مدیاستن1•- برجستگی شریانهای پولمونر2•

Chest X Rey

Echocardiogram• Normal left ventricular size with an ejection
fraction of 60–65%.• There is left ventricular diastolic dysfunction.• There is a flattened ventricular septum, consistent
with right ventricular pressure and volume overload.
• The right ventricle is dilated and diffusely hypokinetic with moderate to severe right ventricular systolic dysfunction.
• There is mild right ventricular hypertrophy.

Echocardiogram
• The estimated pulmonary arterial pressure is 90–95 mmHg.
• The right atrium is dilated. • The mitral and aortic valves appear normal.

دوم سوال
فشار شریان ریوی اندازه گیری شده •در اکوکاردیوگرافی:
- فشار سیستولیک1•- فشار دیاستولیک2•- فشار متوسط شریانی3•

• A ???? pulmonary artery pressure (PAP) > 25 mmHg at rest or >30 mmHg with exercise in the presence of a normal pulmonary capillary wedge pressure (<15 mmHg).
• The exercise criterion was removed from the definition of PH due to the wide variation in pulmonary artery pressures during exercise in normal, healthy individuals as well as the increases that occur with aging.

سوم سوال
منظور از این فشار کدامست؟•
- فشار سیستولیک1•- فشار دیاستولیک2•- فشار متوسط شریانی3•

چهارم سوال
با توجه به ابتال به هیپرتانسون پولمونر •اولین اقدام تشخیصی :
PFT1.CT scan2.
Perfusion scan3.PSG4.

PFT
•FEV1= 1.97 L (78 % of Ref)•FVC= 2.51 L (84% of Ref)•FEV1/FVC (%) 90•FEF25–75% (L/s) 1.85 (76 % of Ref)

پنج سوال
پترن درگیری در •اسپیرومتری؟
-تحدیدی1•- انسدادی2•-مخلوط3•
• FEV1= 1.97 L (78 % of Ref)• FVC= 2.51 L (84% of Ref)• FEV1/FVC (%) 90• FEF25–75% (L/s) 1.85 (70 % of Ref)
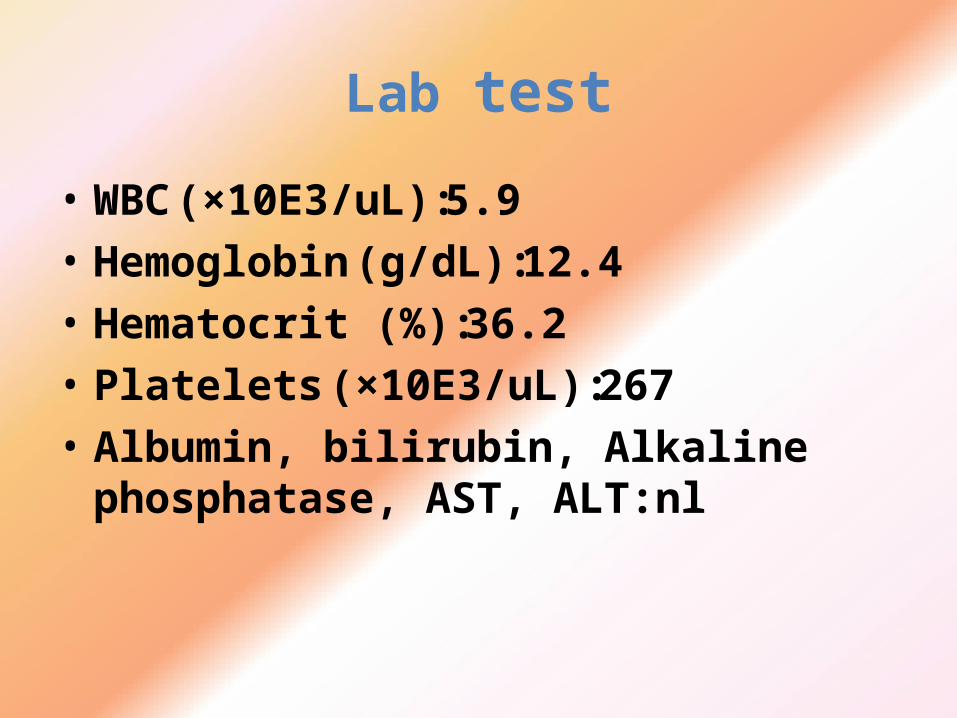
ششم سوال
با توجه به اسپیرومتری بعمل امده •اقدام بعدی شما؟
•1 -HRCT•2-perfusion scan•3 -PSG•4 -TEE
?

هفتم سوال
•HRCT بیمار نرمال بدون درگیری پارانشیم ریه .اقدام بعدی ؟
- اسکن پرفیوژن ریه1••2 -PSG- انجام ازمایشات بیوشیمی3•- تست ورزش4•
?

Lab test
• TSH=4.6• ESR=6• ANA: negative, RF: negative, ANCA: negative,
HIV: negative

• Perfusion scan:There are no segmental or subsegmental perfusion defects.


Pulmonary HTN
• Pulmonary HTN is characterized by elevated pulmonary arterial pressure and secondry right ventricular failure.
• Pulmonary HTN primary ,idiopathic & secondry

Epidemiology
• PPHTN a disease of young women• Femal to male ratio 1/7 : 1• Infrequency over the next 60 year
• However PPHTN has been reported in both sexes within a wide age range of 1 to 81 years
• Mean age: 36 • Incidece : 5 to 15 cases per million

Pathogenesis
• Mutation in bone morphogenic protein receptor 2(BMPR2) gene that contributes to apoptotic process. PPHTN =cacer of pulmonary of artery
• Defect in spesific voltage gated potassium ion channel excessive ca to inter cell promote cell concentration
• Defect in vasodilatory ( NO ,Prostacycline) in lung • An excess in lung and circulating level of endothelin 1

pathophysiology
1. Medial hypertrophy vasoconstricture2. intimal proliferation ,intimal fibrosis 3. progressive obstruction4. Vascular dilation in present of high pressure5. Some of dilated area evolved into
microaneurysms in situ thrombosis6. Necrotizing arteritis neutrophil
inflammation

Clinical manifestation
Non spesificInitialy exertional dyspnea(95%), breathlessness(60%)fatigue and weaknessexertional Chest pain, syncopeLess commen symptom: cough,hemoptysis,hoarsness(ortner syndrom)

Ph/EX
• Initial ph/Ex:increase of intensity of pulmonic S2• S2 is narrowly split or single in patient with
preserved right ventricular function• Right ventricular failure :wide S2 /systolic murmur• Sever RV failure :jvp increase ,hepatomegaly,ascitis,
pleural effusion• Cyanosis during exercise is a late phenomen• Clubbing is not usual sign

Assesment
• CBC polycytemia • Chest x Rey paranchymal lung
disease ,protrusion of main pulmonary artery• ECG right ventricular hypertrophy• Echo ruling out condition such as MVD ,
Left ventricular failure and measurment PAP• PFT ruling out obstructive disease ,if
FEV1<25% increase PAP
Assesment
• ABG low PCO2 respiratory alkalosis• PFT normal or restrictive pattern• Lung scan segmental defect
(thromboemboli) , no defect( exclusively PPHTN) , multiple subsegmental defect ( maybe ppHTN )

Diagnostic criteria
• Mean pumonary artery pressure is >25 mmhg at rest and artery pressure >30 on exercise
• Mean pulmonary capillary wedge pressure <15mmhg
• Chronich lung disease are mild or absent• Venous thromboemboli is absent• Certain miscellaneous disorder are absent

Cardiac Catheterization
Cardiac catheterization is mandatory to document PAH, R/O cardiac disease and determine vasoreactivity to drug.
It is recommended that patients with pulmonary arterial hypertension undergo drug testing with a short-acting pulmonary vasodilator to determine the extent of pulmonary vasodilator reactivity. Inhaled nitric oxide, adenosine, and intravenous prostacycline
Respons a fall in mean pulmonary arterial pressure 10 mmHg and a final mean pressure <40 mmHg .

Treatment: Pulmonary Arterial Hypertension
• Because the pulmonary artery pressure in PAH increases with exercise, patients should be cautioned against participating in activities that impose physical stress.
• Diuretic therapy relieves peripheral edema and may be useful in reducing RV volume overload.
• Pulse oximetry should be monitored, as O2 supplementation helps alleviate dyspnea and RV ischemia in patients whose arterial O2 saturation is reduced

Treatment
• Anticoagulant therapy is advocated for all patients with PAH based on studies demonstrating that warfarin increases survival of patients with PAH. The dose of warfarin generally is titrated to achieve an international normalized ratio (INR) of 2–3 times control.

Principle of drug treatment

هشتم سوال
IPAHاز عالیم ذکر شده کدام یک با •همخوانی ندارد؟
- خشونت صدا1•- کالبینگ2•- هموپتزی3•- درد رترواسترنال4•

Ca Cannel Blocker
• High doses• Diltiazem 120mg/d ,long actin nifedipin 30
mg/d ,Amlodipin 20 mg /d
• No response vasoreactive : Ca cannal Blocker therapy may cause significant morbidity and mortality

Endothelin Receptor Antagonists
• The endothelin receptor antagonists bosentan and ambrisentan .
• bosentan is initiated at 62.5 mg bid for the first month and increased to 125 mg bid thereafter. Ambrisentan is initiated as 5 mg once daily and can be increased to 10 mg daily.
• Because of the high frequency of abnormal hepatic function tests associated with these drugs, primarily an increase in transaminases, it is recommended that liver function be monitored monthly .
• Bosentan is contraindicated in patients who are on cyclosporine or glyburide concurrently.

Phosphodiesterase-5 Inhibitors
• Sildenafil and tadalafil, phosphodiesterase-5 inhibitor. Phosphodiesterase-5 is responsible for the hydrolysis of cyclic GMP in pulmonary vascular smooth muscle, the mediator through which nitric oxide lowers pulmonary artery pressure and inhibits pulmonary vascular growth.
• The effective dose for sildenafil is 20–80 mg tid. The effective dose for tadalafil is 40 mg once daily.
• The most common side effect is headache. Neither drug should be given to patients who are taking nitrovasodilators.

Prostacyclin analogus
• The intravenous prostacyclins have the greatest efficacy as treatments for PAH and are often effective in patients who have failed all other treatments. The optimal doses of these drugs have not been determined, but the typical doses of epoprostenol range from 25 to 40 ng/kg per min.
• The major problem with intravenous therapy is infection related to the indwelling venous catheter, which requires close monitoring . In addition, abrupt discontinuation of intravenous prostacyclins can lead to a rebound increase in pulmonary pressure
• Side effects include flushing, jaw pain, and diarrhea, which are tolerated by most patients.

Lung Transplantation
• Lung transplantation is considered for patients who, while on an intravenous prostacyclin, continue to manifest right heart failure.
• complication :opportunistic infection , graft
rejection ,obliterative bronchiolitis

Thank you