Embed Size (px)
Citation preview

S
Therapy Considerations for the Radial Nerve
Sybil Hedrick, OTR/L, CHT, CSCSAugust 23, 2014

Radial Nerve Innervation

EtiologyTrauma Internal Forces External Forces Other
Laceration Radial Tunnel Syndrome*b/t head of radius and supinatorWartenberg Syndrome
Tourniquet Ischemia
Gunshot Wound
Synovitis “Crutch Palsy” Traction
Fracture/Dislocation*mid/distal 1/3 of humerus
TumorCallus
Saturday Night Palsy
X-radiation
Electrical Injury
InjectionThe regional anatomy of the nerve and its adjacent structures, as well as the nerve’s proximity to underlying bone and unyielding fascial bands, must be considered.

Muscle Loss:Axilla or Proximal Humerus
Weakness/paralysis of: Tricep Aconeous Brachioradialis All the muscles distal to
brachioradialis

“Wrist Drop” Rests in a position of: Forearm pronation Wrist flexion Thumb flexion &
abduction Slight MCP flexion IP extension (some flexion
if flexors are tight)
Unable to: Extend wrist/fingers Abduct/extend thumb
Muscle Loss: Distal Humerus

Muscle Loss:Forearm: Posterior Interosseous Nerve
Isolated involvement of the deep motor branch of the radial nerve
Present with strong radial deviation with extension of the wrist
Lack MP extension Splinting is similar as for
radial nerve palsy

Sensory Loss
Sensory loss in Radial Nerve Palsy is not as much of a concern as compared to median/ulnar, address as applicable

Functional Loss
Cannot reach out with open hand to obtain objects
No stability at wrist for stable prehension
Difficult to write, type

Pre-Operative TherapyAnd/Or Conservative
Management
Prevent deformity
Maintain tissue pliability
Promote neural regeneration and reorganization
Maintain function
Objectives
Radial Nerve Palsy often recovers spontaneously and will often not be rushed into tendon/nerve transfers so conservative management is key

Pre-Operative TherapyAnd/Or Conservative
Management
Evaluation History
Sympathetic Function
Sensibility (tho not of a huge concern with radial nerve)
Motor Function ROM: active and passive Manual Muscle Testing
Be aware of substitution patterns
Dexterity

Splinting for Function
Goal to maximize current functional use of the hand/UE
Goal to harness wrist motion while allowing full finger flexion/extension
Try to recreate natural tenodesis motion to allow normal grasp/release of the hand
* Note: a static wrist immobilization orthosis does not allow for functional grasp/release, covers palmar sensation and in the end, is not functional for the patient.

Splinting for Function

Splinting for Function

VanLede Radial Nerve Palsy Splint
Improved functional dexterity
Lower profile
Easier to get on/off for patient
Can use Delta Cast or Thermoplastic
Instructions for thermoplastic version can be found @ pattersonmedical.com search for Extension Assist Splint

Splinting to Prevent or Correct Deformity
Keep deneravated muscles from resting in an overstretched position
Prevent joint contractures
Enhance returning muscle function instead of allowing substitution patterns

Adaptations/Modifications
Cold intolerance frequently accompanies peripheral nerve injuries (PNI): neoprene mittens, gloves

Interventions: After Splinting
Modalities: Heat NMES
Nerve glides
Manual work
Home program
Repeated assessment to assist tracking of nerve recovery
Strengthening Gravity eliminated Aquatic therapy Progressive resistance
(PRE)

Preparation for Tendon Transfer
Ideal, full if possible, PROM at joints which will be involved
Idea, full if possible, AROM as well
Proximal muscle strength should be at least 4/5 or better
The muscle to be transferred should have strength at least 4/5 or better

Motor Learning & Cortical Re-Mapping
Motor Learning
Motor Leaning aptitude should be assessed on the non-involved limb
Acquisition
Retention (consistency)
Transfer (flexibility)
Efficiency
Cortical Re-Mapping

Post-Operative TherapyRadial Nerve Tendon Transfer
Psychosocial Issues: client roles, motivation and compliance, cognition, past and current abilities/interests
Diminished success from transfer surgery can result with: Denial Frustration Lack of trust in therapy program Finances Time
Must work closely with patient and Physician to eliminate and/or minimize or ease these factors

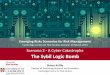
Post-Operative TherapyRadial Nerve Tendon Transfers
Pronator Teres to the ECRB for wrist extension
Palmaris Longus to rerouted EPL for thumb extension (if no PL, FDS (IV))
FCR to EDC for finger extension (sometimes FCU is used)
emedicine.medscape.com

Tendon Transfer Precautions
Common complications from tendon transfer include: Excessive radial deviation
at the wrist Bowstringing of transferred
tendons (EPL in particular) Incomplete extension of 1
or more fingers Incomplete finger flexion
with simultaneous wrist flexion
Complete Rupture Tendon adhesion
Therapist can play a key role in preventing some of these issues: Careful monitoring of
active motion, retrain movement patterns
Gradual progression out of splint
Ensure tendon gliding Education, education,
education every visit on stage of healing, phase of rehab

Post-Operative TherapyRadial Nerve Tendon Transfers
Phase Goal Method
1 (weeks 0-3)Immobilization
Protect repair site Good fitting orthosis positioned per physician/therapist to minimize tension at wrist, fingers, thumbEnsure freedom of motion of joints allowed to move
Manage Edema & incision/scar care
Elevation (overhead hook fisting)Compression (coban, Game ready)Wound care, silicone gel
Active motion of non-involved joints
ShoulderPIP and DIP of fingersLegs/core

Post-Operative TherapyRadial Nerve Tendon Transfers
Splint picture
Splint out of surgery: ultimately depends on your surgeon! Sources vary between surgical and therapy resources. Usually 2-3 weeks
Elbow included, held in a position of pronation
wrist 30-50 deg of extension and 10-15 deg of UD
MCP’s at 0deg or 0-15 deg of flexion, finger IP’s free
Thumb fully abducted with IP in full extension

Post-Operative TherapyRadial Nerve Tendon Transfers
Phase Goal Method
2Weeks3-6
ActivationOf the transfer
Regain AROM & maintain PROM
Elbow extension and flexionProtected: supination, wrist flexion, finger flexion, thumb adduction/flexionPronation, wrist extension, finger extension, thumb abduction/extensionPROM, myofascial release, scar massage
Activation of tendon transfer
Muscle retraining:Pronation for wrist extensionWrist flexion for finger extensionPalm contraction for thumb abd/ext
Enhance sensorimotor control
Grasping lightweight objects of various shapes, sizes, manipulation
Enhance function while maintaining good biomechanics
Ensure normal movement patterns as much as possible using verbal/nonverbal feedbackIn clinic and with basic ADL tasks at home

Motor Re-Education
Start with both the original motion combined with new motion
Start in gravity eliminated position and/or place and hold
Some resources say to use the opposite limb, however the wiring is now different??
Slow, short session at a non-extreme force
Tips for specifics:
Wrist extension Resist pronation to help
facilitate wrist ext
Finger extension Resist wrist flexion to help
facilitate finger ext Caution to NOT flex forcefully
past neutral as this can stress the repair site
Thumb abduction/extension

Post-Operative TherapyRadial Nerve Tendon Transfers
Phase Goal Method
3Weeks6-12
Improve strength Usual suspects: weights, therabandHammer, Dynaflex*
Strengthening& return to priorfunction
Enhance aerobic capacity
UBE, aquatic, general conditioning
Return to prior level of function
Work hardening, sport specific training, don’t forget leisure!
Ongoing assessment Capacity for continuing improvementNeeds for further surgical consult/issuesLong-term adaptive equipment/techniques

Ther Ex Pearls
Hammer Dynaflex

The Cube

Post-Operative Therapy Nerve Transfer for Radial Nerve
Paralysis Pre-operatively: Therapist should work on motor retraining
using contralateral arm and normal movement patterns
Radial Nerve specific? Typing, reaching and grasping, playing instrument, etc. Tasks for wrist/finger extension, thumb abd/ex

Post-Operative Therapy Nerve Transfer for Radial Nerve
Paralysis
Post-operative pain management
Edema control
Immobilization 7-10 days
Early ROM Shoulder, trunk 3-4 weeks: elbow, forearm, wrist and hand

Motor Re-Education
Must learn to coordinate new pathways for target muscle activation
Cortical command is now different and new
Motor reeducation with tasks that are normal for elbow flexion are instituted to relearn: normal movement
patterns muscle recruitment reestablish muscle
balance
1st: wrist/finger extension and thumb abduction muscle “contraction” combined with contraction from donor nerve: FDS, FCR, PL
Want most synergistic action based on original motor pattern
Bimanual tasks

Strengthening
Utilize reinnervated muscle physiology and biomechanics 1) short duration exercise sessions (<5-10min)
Slow onset contractions begin in mid-range (place and hold) or gravity
eliminated 2) Multi-angle isometrics 3) Concentric strengthening 4) Eccentric strengthening