Embed Size (px)
Citation preview
1
胸壁和胸膜疾病
Disorders of the chest wall and pleura
天津医科大学总医院 心胸外科 刘毅梅 Yimei Liu
Department of Cardiothoracic Surgery General Hospital, Tianjin Medical University
2
Quick Review: Anatomy
Chest wall
soft tissue & bony thorax cage
Pleura
visceral and parietal pleura
Pleural space
a potential space between the visceral and parietal pleura
3
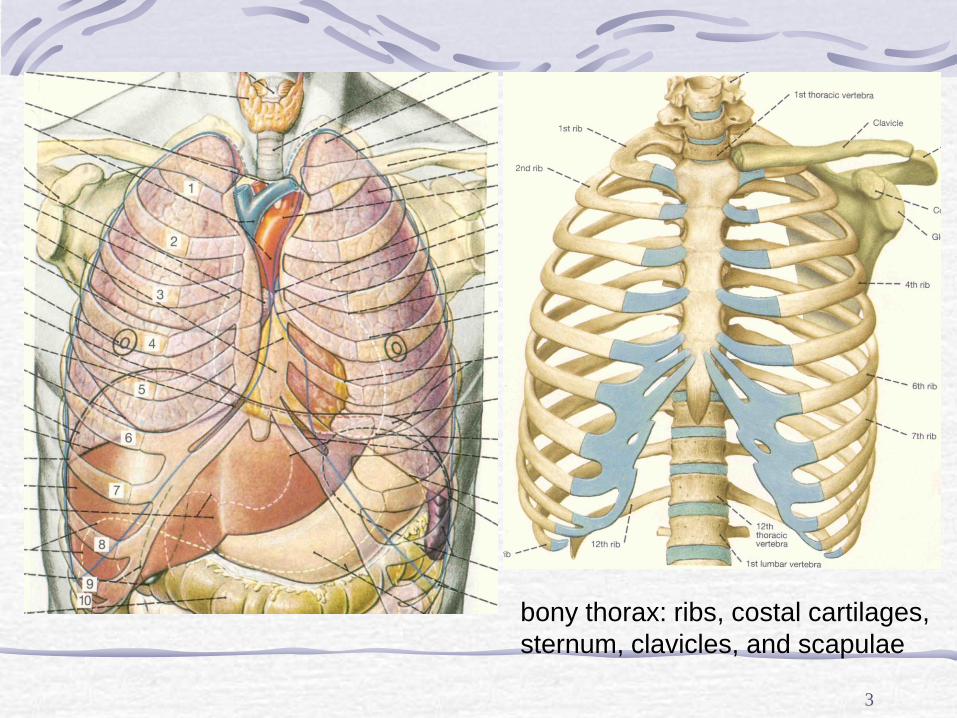
bony thorax: ribs, costal cartilages,
sternum, clavicles, and scapulae
4
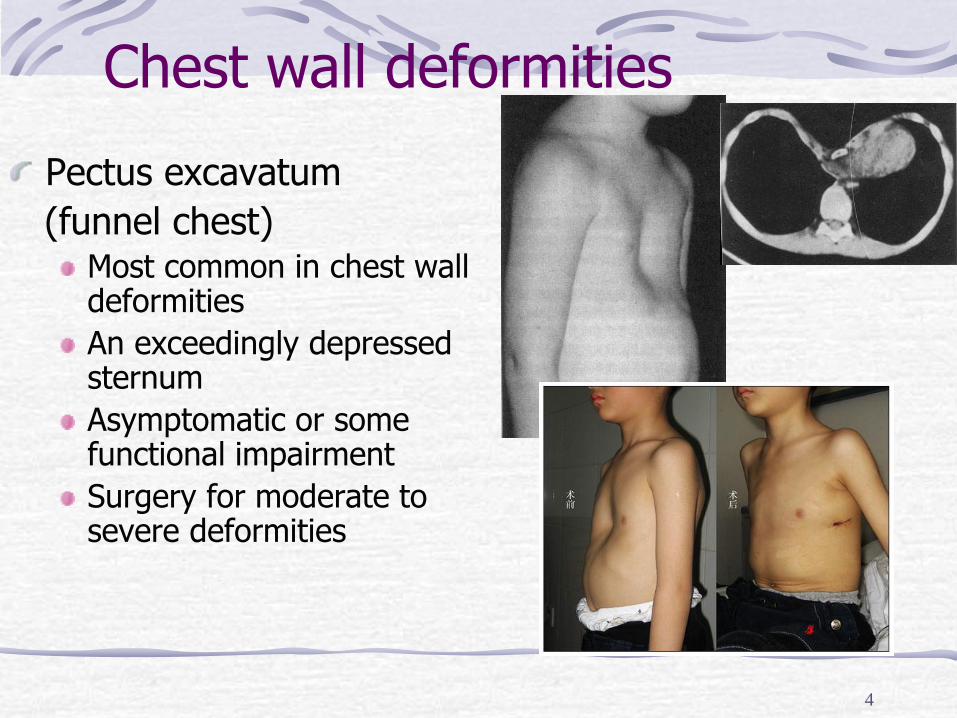
Chest wall deformities
Pectus excavatum
(funnel chest) Most common in chest wall deformities
An exceedingly depressed sternum
Asymptomatic or some functional impairment
Surgery for moderate to severe deformities
5
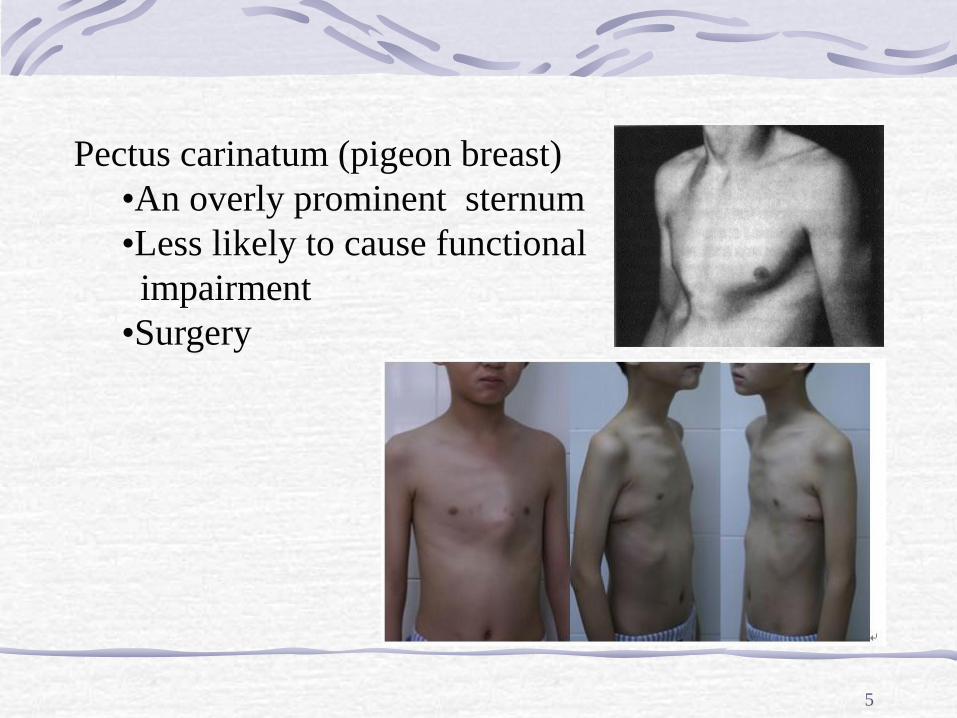
Pectus carinatum (pigeon breast)
•An overly prominent sternum
•Less likely to cause functional
impairment
•Surgery
Chest wall tumors
Tumors of the chest wall encompass a variety
of bone and soft tissue disorders.
Chest wall tumors generally present as slowly
enlarging, asymptomatic masses. With
continued growth, pain invariably occurs.
6
7
Chest wall tumors Benign tumors
Fibrous dysplasia of the rib
Chondroma—most common
Osteochondroma
Malignant tumors
Fibrosarcoma, chondrosarcoma, osteogenic
sarcoma, myeloma, and Ewing's sarcoma
Treatment—wide excision and reconstruction
8
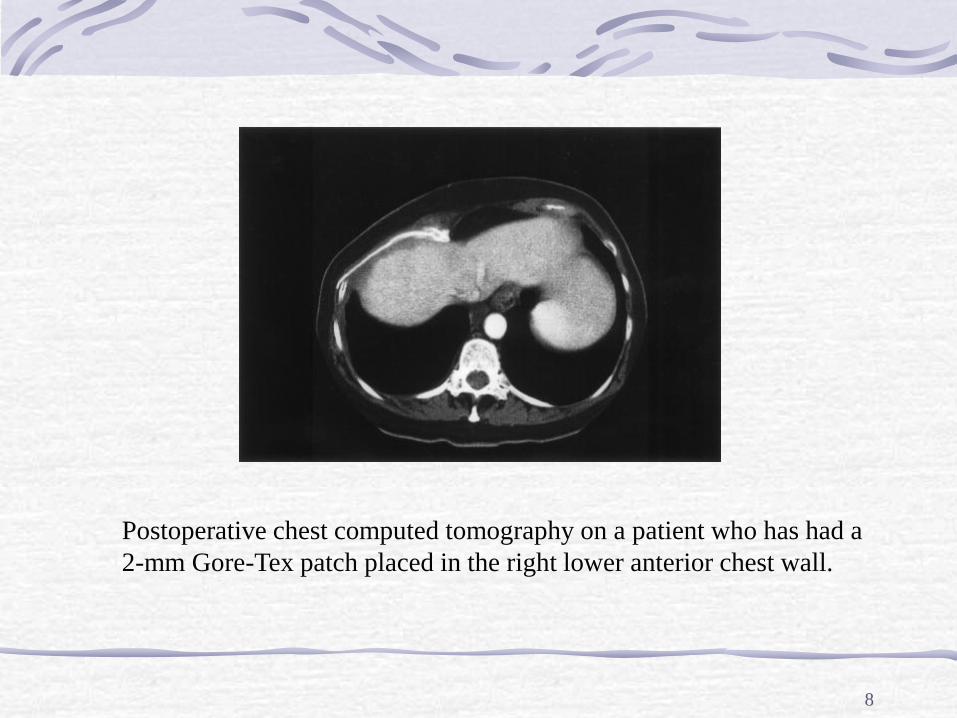
Postoperative chest computed tomography on a patient who has had a
2-mm Gore-Tex patch placed in the right lower anterior chest wall.
Primary Chest Wall Neoplasm Malignant
Malignant fibrous histiocytoma
Chondrosarcoma
Rhabdomyosarcoma
Myeloma
Ewing’s sarcoma
Liposarcoma
Neurofibrosarcoma
Osteogenic sarcoma
Hemangiosarcoma
Leiomyosarcoma
Lymphoma 9
Benign
Osteochondroma
Chondroma
Desmoid
Lipoma
Fibroma
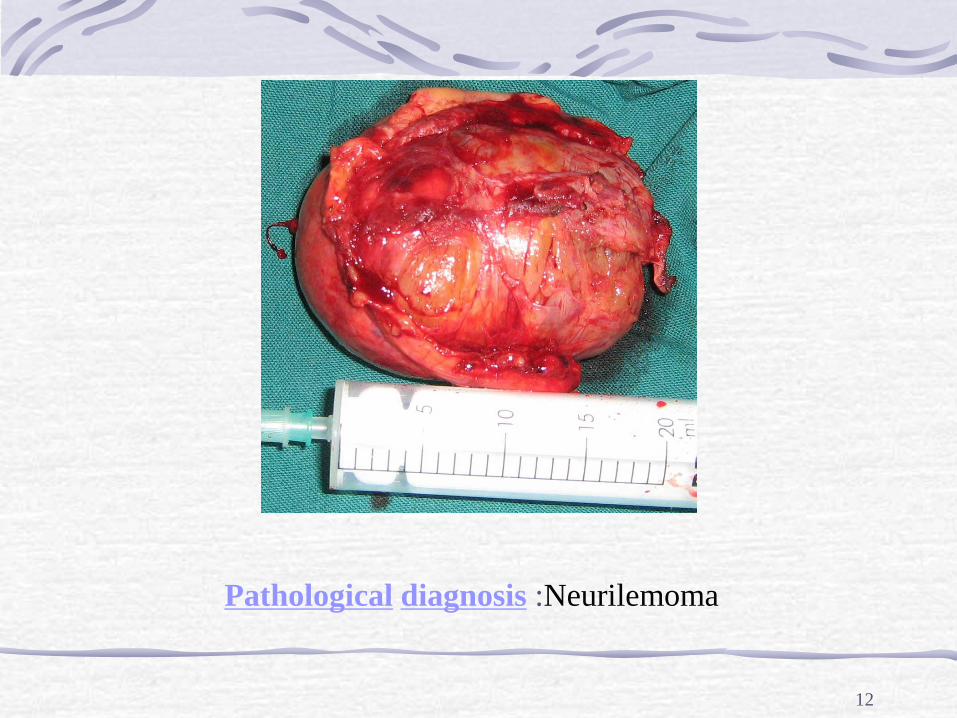
Neurilemoma
10

11
13
Pleural effusions Most common causes
Congestive heart failure
Infection
Neoplasm
Management Treatment of the underlying disease
Thoracentesis
Pleural drainage (tube thoracostomy)
14
Pleural neoplasm benign or malignant
Focal pleural masses Localized fibrous neoplasm pleura Thoracic lipoma Local invasion from a bronchogenic carcinoma and metastatic spread from thymoma Very rarely melanoma and certain sarcomas (leiomyosarcoma, liposarcoma, rhabdosarcoma and fibrous histiocytoma)
extensive pleural involvement Mesothelioma Pulmonary adenocarcinoma Lymphoma
15
Mesothelioma Related to asbestos exposure
Localized mesothelioma Usually arise from the visceral pleura
Treated by local incision
Malignant mesothelioma Fatal
Presents with a pleural effusion
May require palliative decortication
Chemotherapy :Pemetrexed
16
17
18
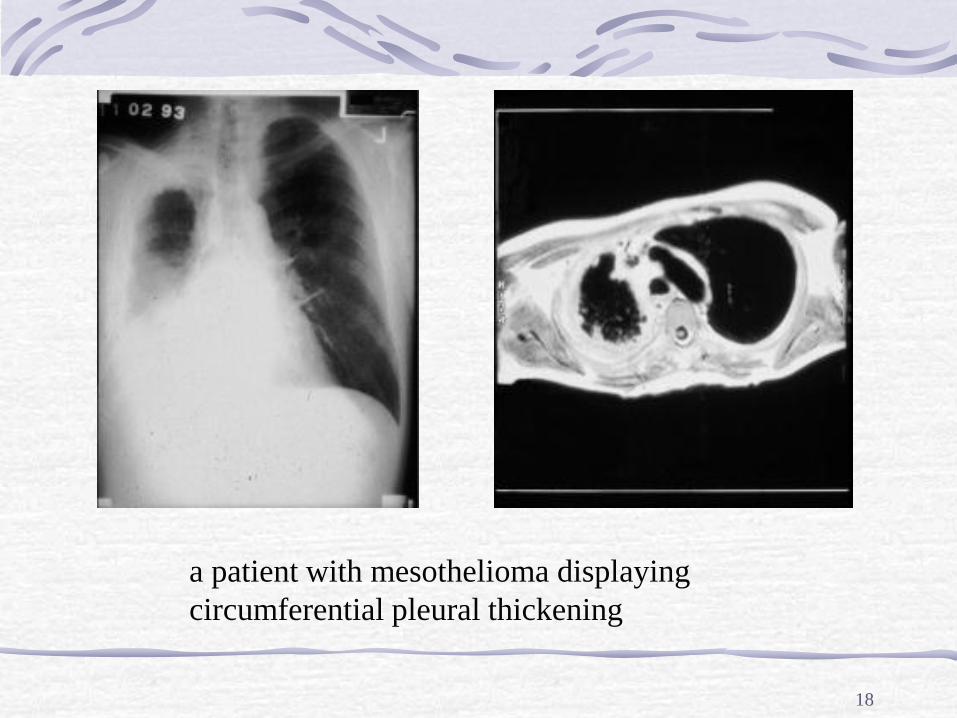
a patient with mesothelioma displaying
circumferential pleural thickening
19
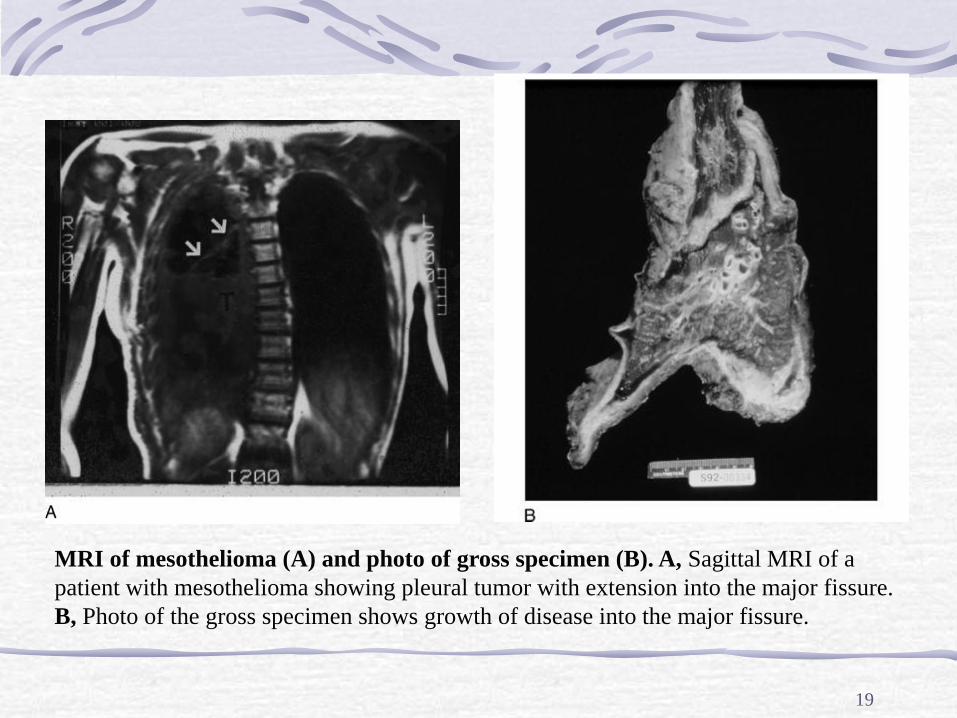
MRI of mesothelioma (A) and photo of gross specimen (B). A, Sagittal MRI of a
patient with mesothelioma showing pleural tumor with extension into the major fissure.
B, Photo of the gross specimen shows growth of disease into the major fissure.
20
脓胸 Empyema Definition: is inflammatory fluid and
debris collected in the pleural space
Associated infections
Tuberculosis
Anerobe lung infection
Staphylococcus pneumonia
Streptococcus pneumonia
Gram-negative bacteria lung infection
21
Causes Bacterial pneumonia, septic pulmonary
embolism, lung abscess or bronchopleural
fistula
Spread of infection from adjacent structures
such as chest wall, ribs, liver or subphrenic
area
Thoracic trauma or Esophageal tear
Iatrogenic introduction or indwelling catheter
22
Natural history
The formation of an empyema has 3
stages:
1.Exudative stage
2.Fibrinopurulent stage
3.Organizing stage
23
Natural history (1)
The formation of an empyema has 3 stages:
1.Exudative stage: Protein-rich pleural fluid
remains free-flowing. The number of
neutrophils is rapidly increasing. Glucose and
pH levels are normal. Drainage of the
effusion and appropriate antimicrobial
therapy are normally sufficient for treatment.
24
Natural history (2)
2. Fibrinopurulent stage: Viscosity of the
pleural fluid is increasing. Coagulation
factors are activated, and fibroblast activity
begins coating the pleural membrane with
an adhesive meshwork. Glucose and pH
levels are lower than normal.
25
Natural history (3)
3. Organizing stage: Loculations are forming. Fibroblast activity causes adherence to the visceral and parietal pleura. This activity may progress with the formation of pleural peels in which the pleural layers are indistinguishable. Pus, which is a protein-rich fluid with inflammatory cells and debris, is present in the pleural space. Surgical intervention is often required at this stage.
26
Symptoms Pulmonary symptoms (e.g. cough, tachypnea,
sputum production, desaturations)
Systemic symptoms
a fever and chills
excessive sweating, especially night sweats
general discomfort, uneasiness, or ill feeling (malaise)
weight loss
leukocytosis
chest pain, worse on deep inspiration (inhalation)
27
Signs and tests Abnormal findings
friction rub when auscultation
same as hydrothorax
Tests include:
thoracentesis, pleural fluid gram stain and culture
chest X-ray
computed tomography
ultrasonography
28
Pleural space fluid
Early/acute stage, one or more of:
pH < 7.2, glucose < 40 mg/dL, LDH >1000IU/dL, protein > 2.5 g/dL, WBC > 500/µL, specific gravity greater than 1.018
Thin serous or cloudy fluid, generally sterile
Fibrinopurulent/intermediate stage
Thicker, opaque fluid or fluid with positive cultures
Organizing/late stage
An organizing peel with entrapment of the lung
29
Differential diagnosis
Between an empyema and a lung abscess
The presence of air in an empyema may be due to
the development of a bronchopleural fistula
CT scanning is useful under this circumstance
An empyema tends to have a thinner, smoother
wall than a lung abscess, is lentiform in shape and
forms an obtuse angle with the chest wall.
30
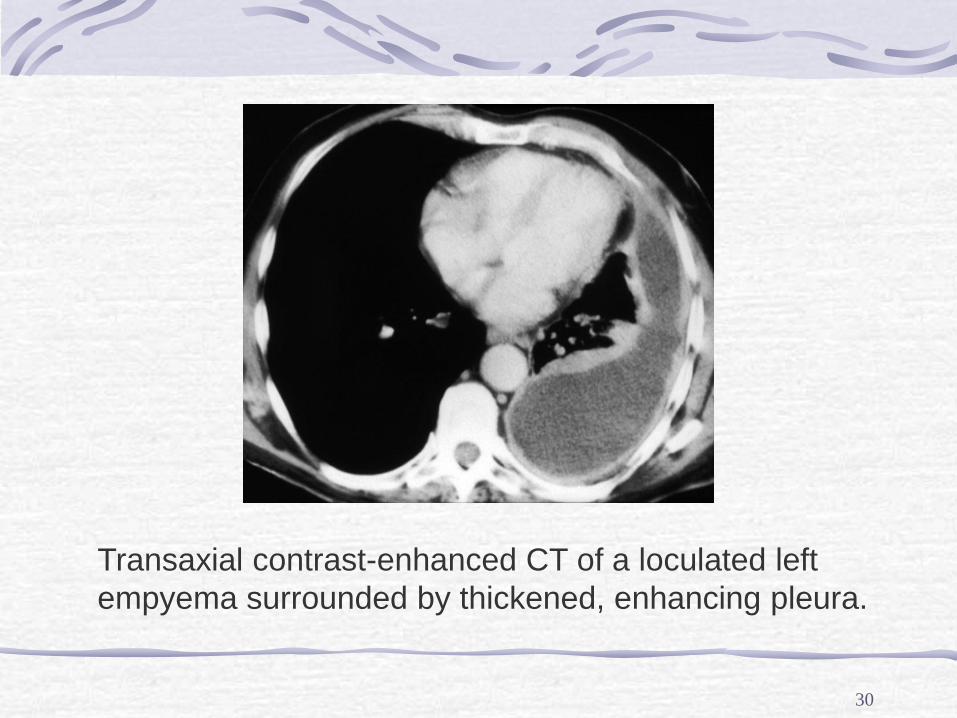
Transaxial contrast-enhanced CT of a loculated left
empyema surrounded by thickened, enhancing pleura.
31
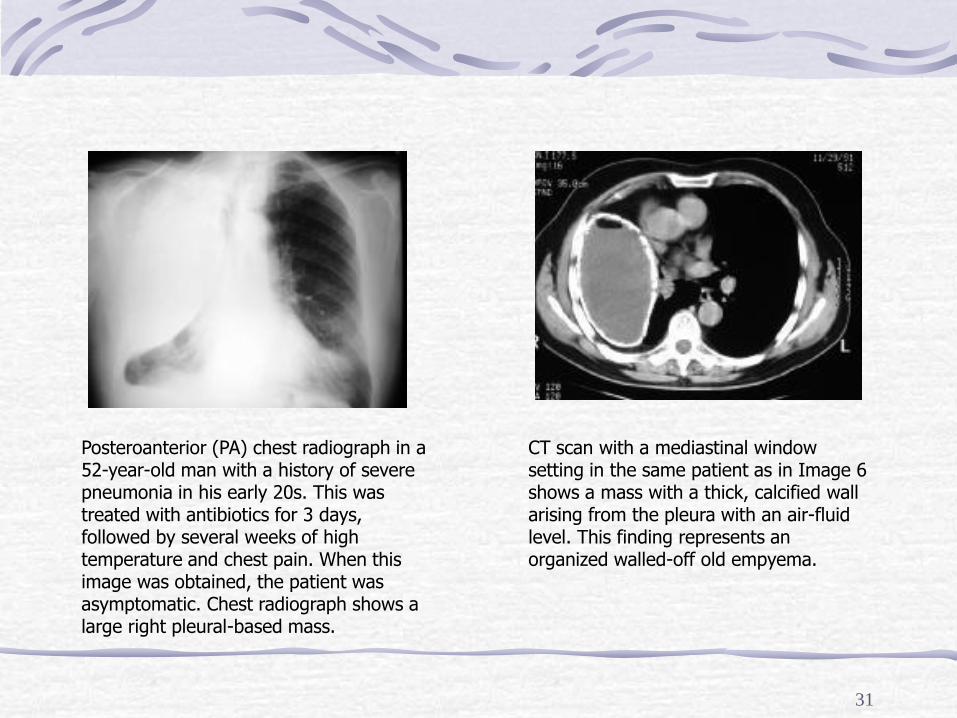
Posteroanterior (PA) chest radiograph in a 52-year-old man with a history of severe pneumonia in his early 20s. This was treated with antibiotics for 3 days, followed by several weeks of high temperature and chest pain. When this image was obtained, the patient was asymptomatic. Chest radiograph shows a large right pleural-based mass.
CT scan with a mediastinal window setting in the same patient as in Image 6 shows a mass with a thick, calcified wall arising from the pleura with an air-fluid level. This finding represents an organized walled-off old empyema.
32
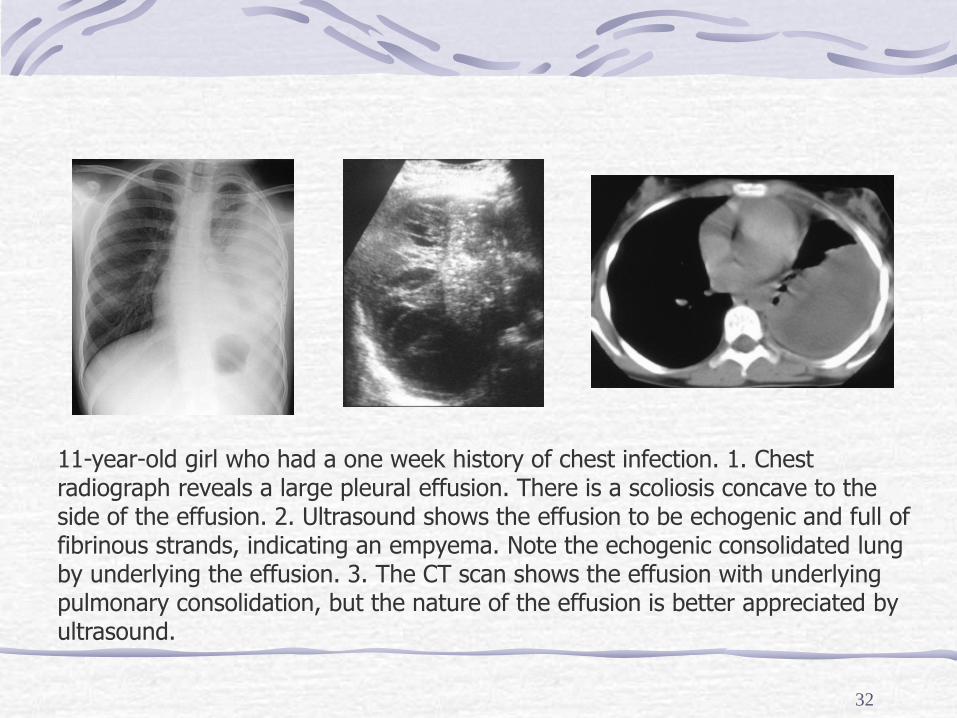
11-year-old girl who had a one week history of chest infection. 1. Chest radiograph reveals a large pleural effusion. There is a scoliosis concave to the side of the effusion. 2. Ultrasound shows the effusion to be echogenic and full of fibrinous strands, indicating an empyema. Note the echogenic consolidated lung by underlying the effusion. 3. The CT scan shows the effusion with underlying pulmonary consolidation, but the nature of the effusion is better appreciated by ultrasound.
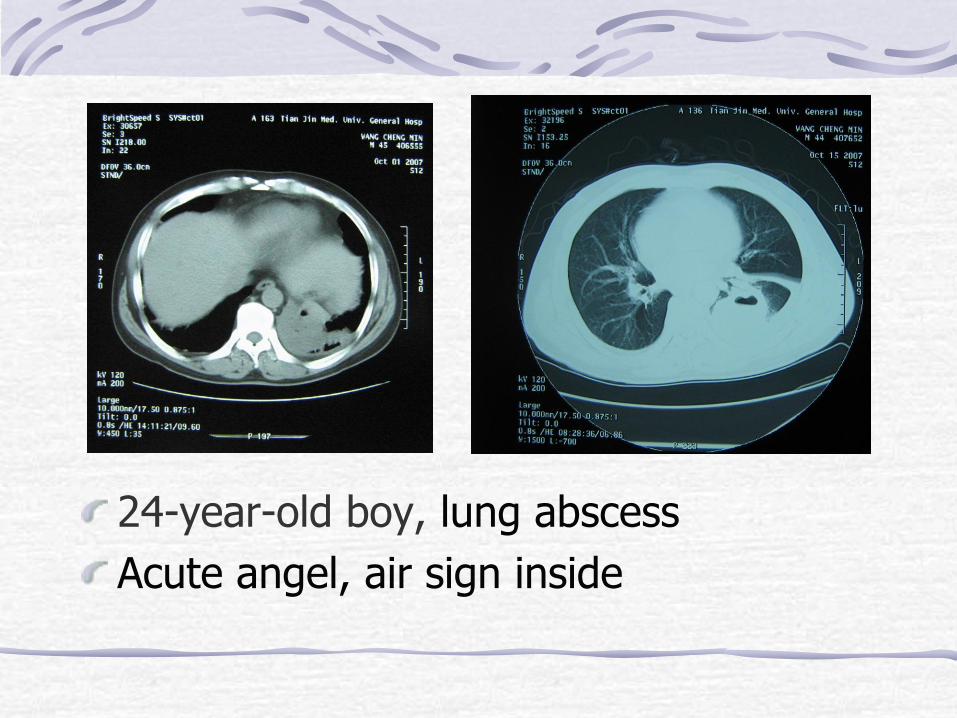
24-year-old boy, lung abscess
Acute angel, air sign inside
34
Management (1)
The goal of treatment is to cure the infection
and remove the collection of pus from the
lung.
Three core principles
prompt initiation of appropriate antibiotics
the complete evacuation of suppurative pleural
fluid
the preservation or restoration of lung expansion
35
Management (2)
Thoracentesis (maybe under ultrasonography or CT
guidance) and antibiotics alone have been
successful in treatment of empyema in 6 to 20% of
patients, particularly with early stage disease
If the effusion recurs, placement of a chest tube or
small-bore catheter for continuous drainage is the
next step
36
Management (3)
Large closed-tube thoracostomy with or without
the adjunctive use of fibrinolytics has been the
traditional management with the fibrinopurulent
stage of the empyema process
Appropriate time to drain the empyema: a large free-
flowing effusion (at least half of a hemithorax), a
loculated effusion or effusion with thickened parietal
pleura, positive culture or Gram stain results, parietal
pus, and pH less than 7.20
37
Management (4)
Surgical intervention is required in
effusions with multiple loculations that are
difficult to drain and effusions that have not
responded to catheter drainage
The organizing phase of empyema requires
direct removal of the restrictive coagulum
(decortication) with open or thoracoscopic
technique
38
Management (5)
Surgical interventions may include the
following:
Thoracoscopic debridement
Video-assisted thoracoscopic surgery (VATS)
Open thoracotomy for debridement
Open surgical decortication
39
Management (6)
Indications for Surgery
fail to respond to intravenous antibiotics with defervescence
and improving pulmonary symptoms
pleural fluid does not aspirate with needle or tube
thoracostomy
responded more quickly with earlier decortication
Caution in associated necrotizing pneumonias and
lung abscesses for fear of the development of
prolonged air leaks and bronchopleural fistulae
40
Expectations(prognosis)
Usually empyema does not result in
permanent pulmonary damage

41
纵隔疾病
Disorders of the Mediastinum
42
Anatomy (1)
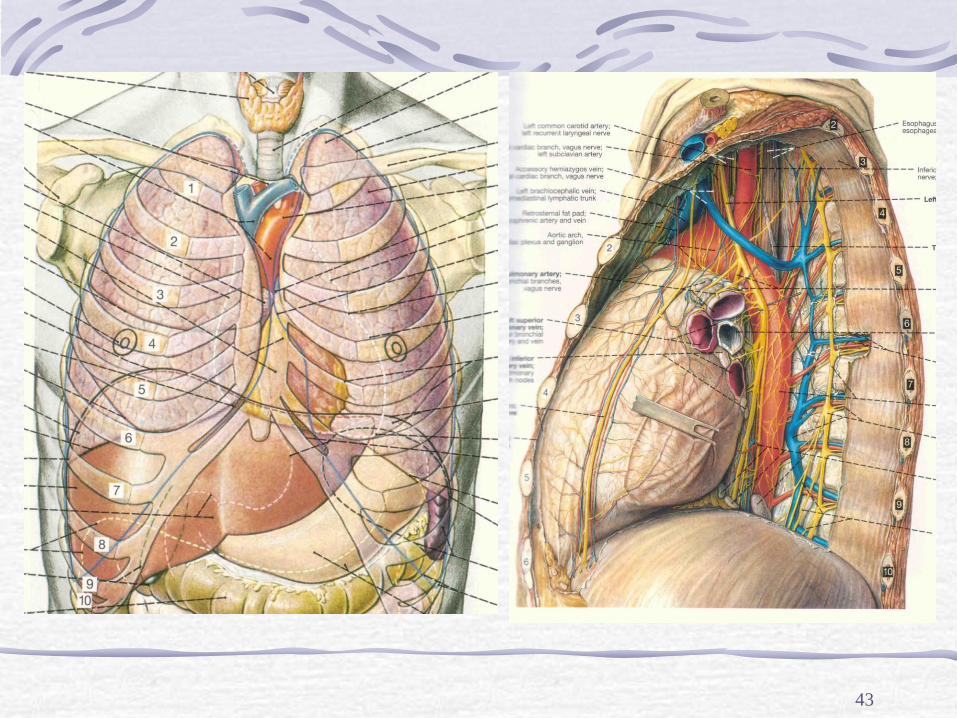
The mediastinum is the region of the thoracic cavity bounded by:
posteriorly: thoracic spine
anteriorly: sternum and costal cartilages
laterally: mediastinal pleura bounding the pleural cavities
superiorly: thoracic inlet
inferiorly: diaphragm
43
44
Anatomy (2)
The mediastinum is subdivided into
various regions :
Anterior mediastinum
Middle mediastinum
Posterior mediastinum
Anatomy (3)
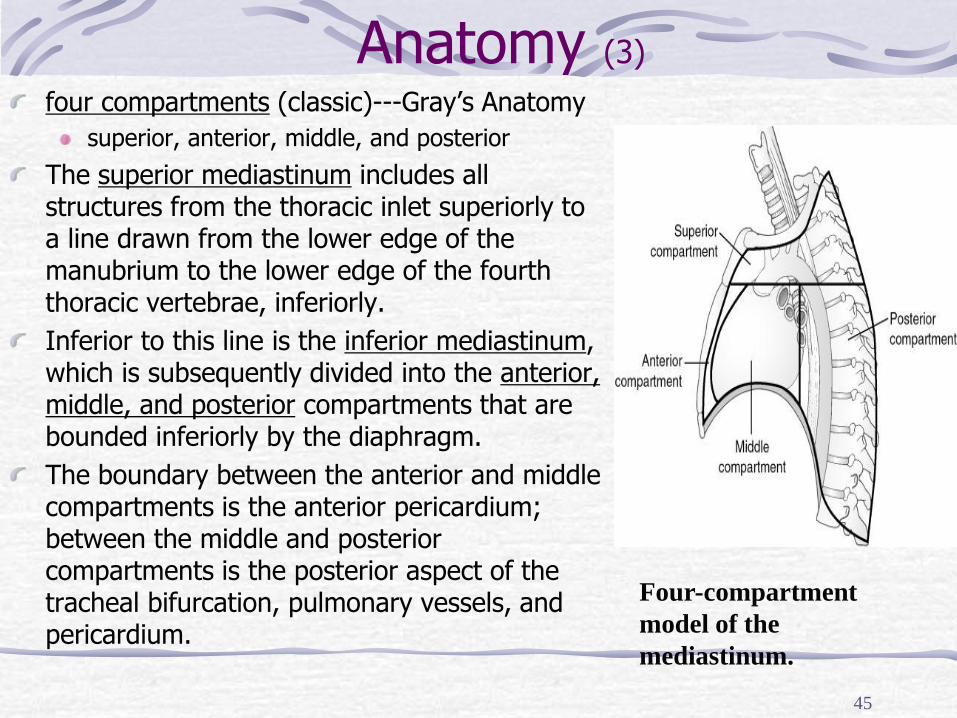
four compartments (classic)---Gray’s Anatomy
superior, anterior, middle, and posterior
The superior mediastinum includes all structures from the thoracic inlet superiorly to a line drawn from the lower edge of the manubrium to the lower edge of the fourth thoracic vertebrae, inferiorly.
Inferior to this line is the inferior mediastinum, which is subsequently divided into the anterior, middle, and posterior compartments that are bounded inferiorly by the diaphragm.
The boundary between the anterior and middle compartments is the anterior pericardium; between the middle and posterior compartments is the posterior aspect of the tracheal bifurcation, pulmonary vessels, and pericardium.
45
Four-compartment
model of the
mediastinum.
Anatomy (4)
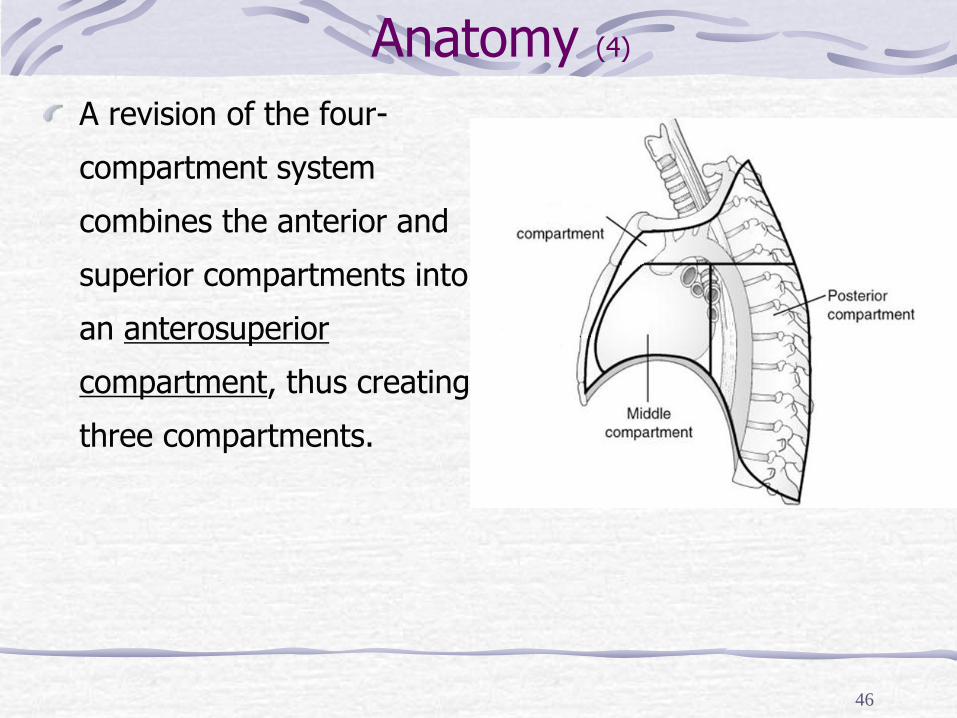
A revision of the four-
compartment system
combines the anterior and
superior compartments into
an anterosuperior
compartment, thus creating
three compartments.
46
Anatomy (5)
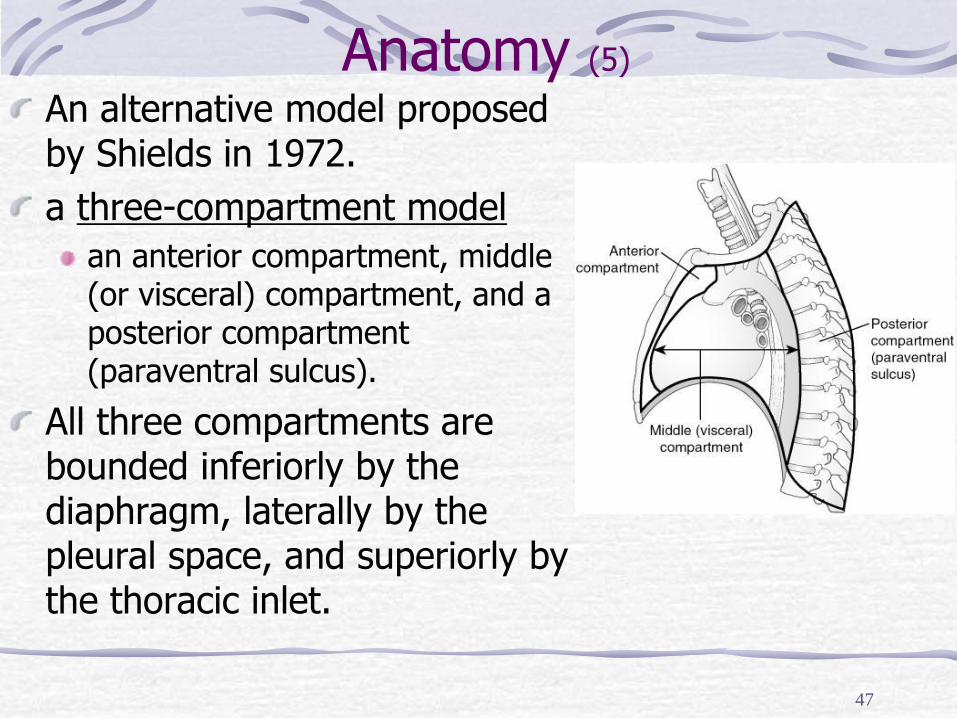
An alternative model proposed by Shields in 1972.
a three-compartment model
an anterior compartment, middle (or visceral) compartment, and a posterior compartment (paraventral sulcus).
All three compartments are bounded inferiorly by the diaphragm, laterally by the pleural space, and superiorly by the thoracic inlet.
47
Anatomy (6)
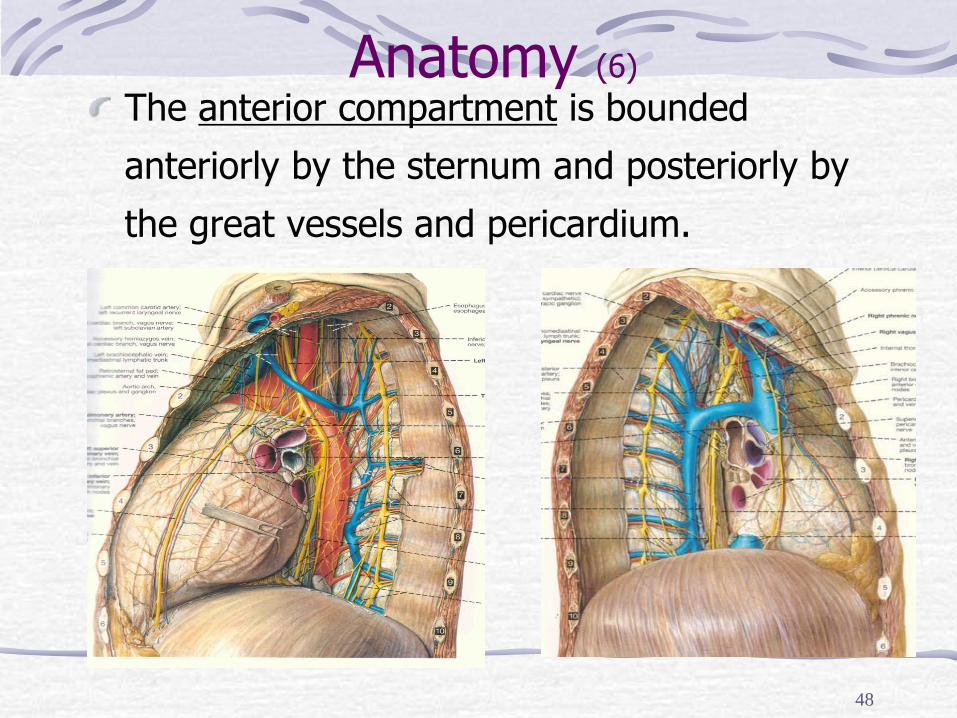
The anterior compartment is bounded
anteriorly by the sternum and posteriorly by
the great vessels and pericardium.
48
49
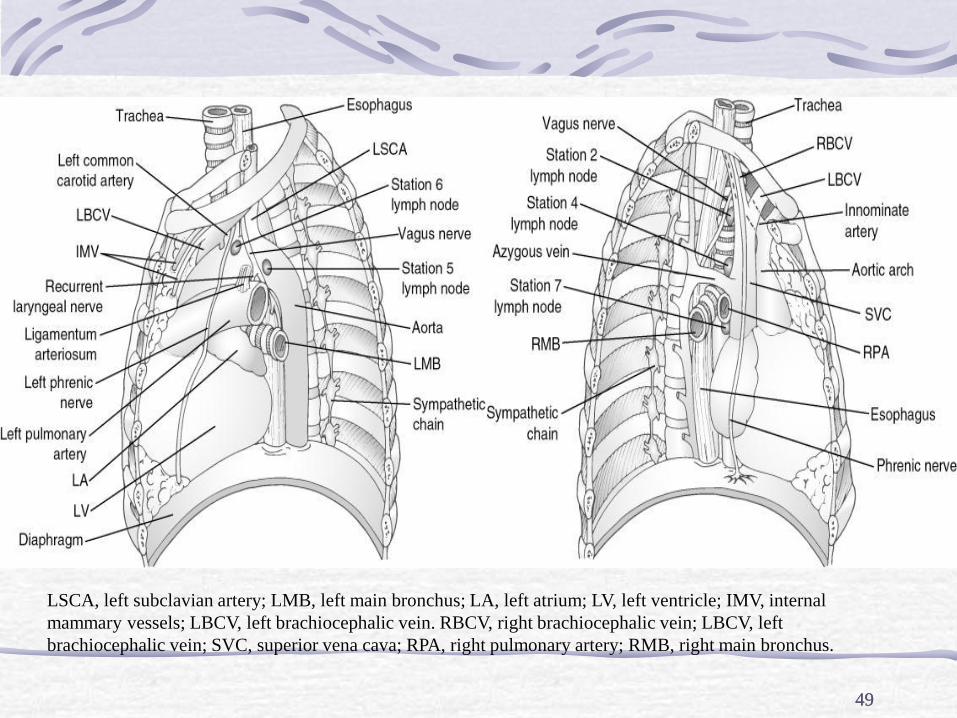
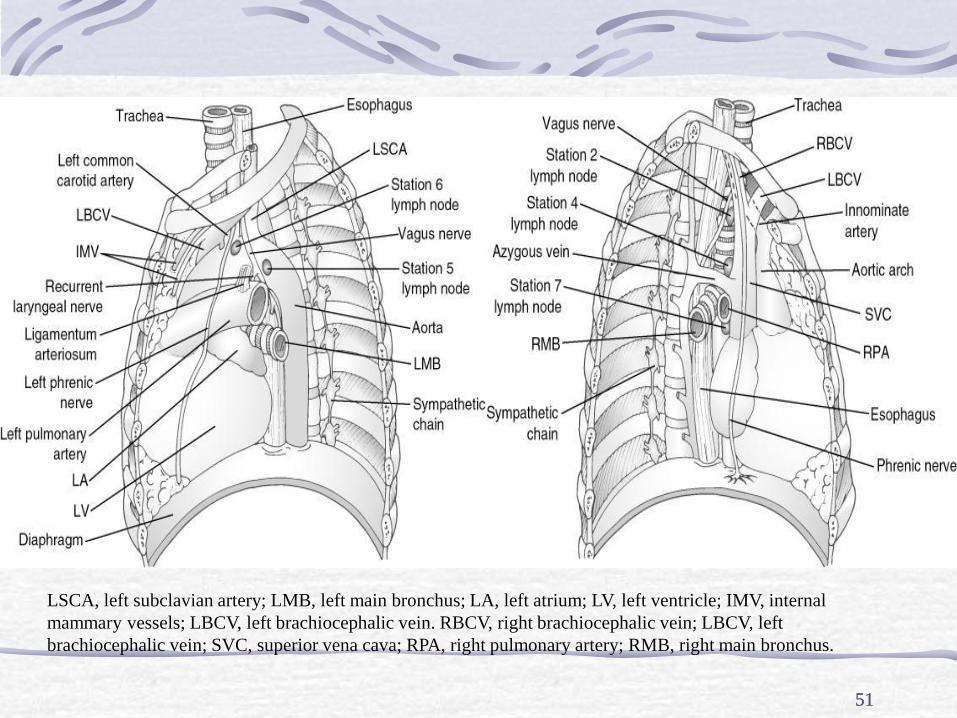
LSCA, left subclavian artery; LMB, left main bronchus; LA, left atrium; LV, left ventricle; IMV, internal
mammary vessels; LBCV, left brachiocephalic vein. RBCV, right brachiocephalic vein; LBCV, left
brachiocephalic vein; SVC, superior vena cava; RPA, right pulmonary artery; RMB, right main bronchus.
49
Anatomy (7)
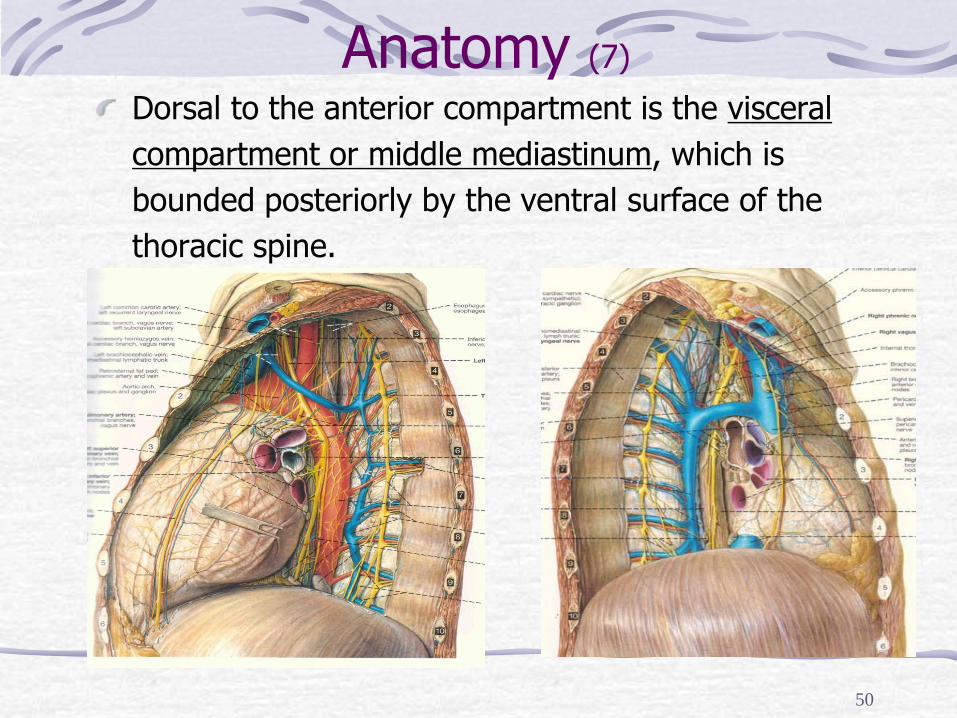
Dorsal to the anterior compartment is the visceral
compartment or middle mediastinum, which is
bounded posteriorly by the ventral surface of the
thoracic spine.
50
51
LSCA, left subclavian artery; LMB, left main bronchus; LA, left atrium; LV, left ventricle; IMV, internal
mammary vessels; LBCV, left brachiocephalic vein. RBCV, right brachiocephalic vein; LBCV, left
brachiocephalic vein; SVC, superior vena cava; RPA, right pulmonary artery; RMB, right main bronchus.
51
Anatomy (8)
The posterior compartment of the mediastinum or paraventral sulcus consists of potential spaces along the thoracic vertebrae that contain the sympathetic chain, proximal portions of the intercostal neurovascular bundles, thoracic spinal ganglia, and the distal azygous vein.
The paraventral sulci are not technically in the mediastinum but contain structures that give rise to pathology that is classically considered in the posterior mediastinum (neurogenic tumors).
52
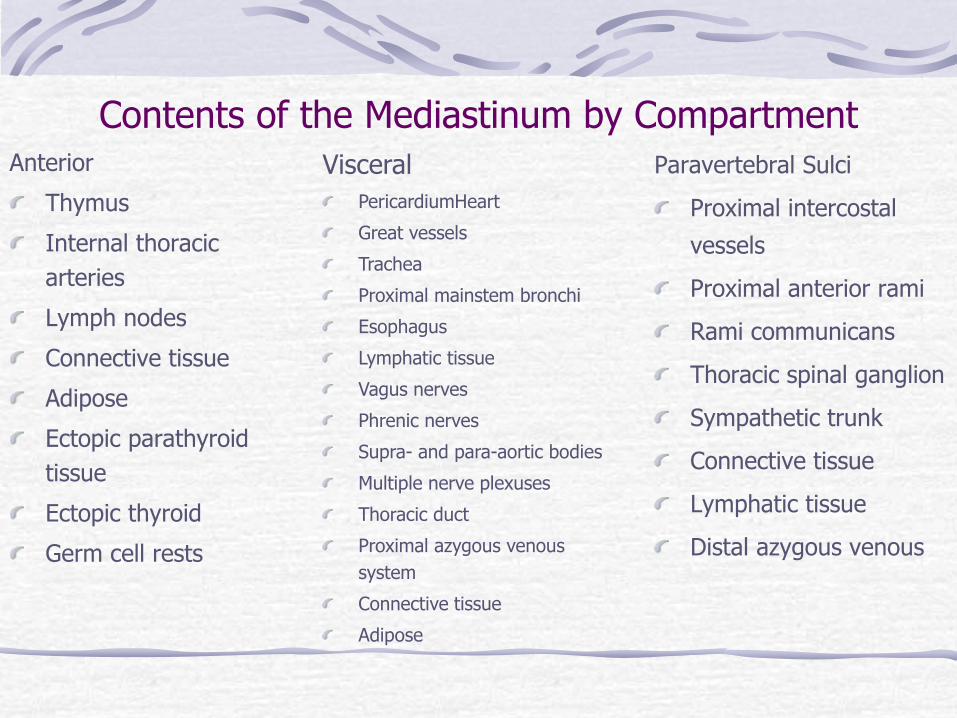
Contents of the Mediastinum by Compartment Anterior
Thymus
Internal thoracic
arteries
Lymph nodes
Connective tissue
Adipose
Ectopic parathyroid
tissue
Ectopic thyroid
Germ cell rests
Paravertebral Sulci
Proximal intercostal
vessels
Proximal anterior rami
Rami communicans
Thoracic spinal ganglion
Sympathetic trunk
Connective tissue
Lymphatic tissue
Distal azygous venous
Visceral
PericardiumHeart
Great vessels
Trachea
Proximal mainstem bronchi
Esophagus
Lymphatic tissue
Vagus nerves
Phrenic nerves
Supra- and para-aortic bodies
Multiple nerve plexuses
Thoracic duct
Proximal azygous venous
system
Connective tissue
Adipose
54
Anatomy (9)
Different division
Four parts
Superior
Inferior: Anterior, Middle, Posterior
Six parts
Superior: Anterior, Middle, Posterior
Inferior: Anterior, Middle, Posterior
Nine parts
Superior: Anterior, Middle, Posterior
Middle : Anterior, Middle, Posterior
Inferior: Anterior, Middle, Posterior
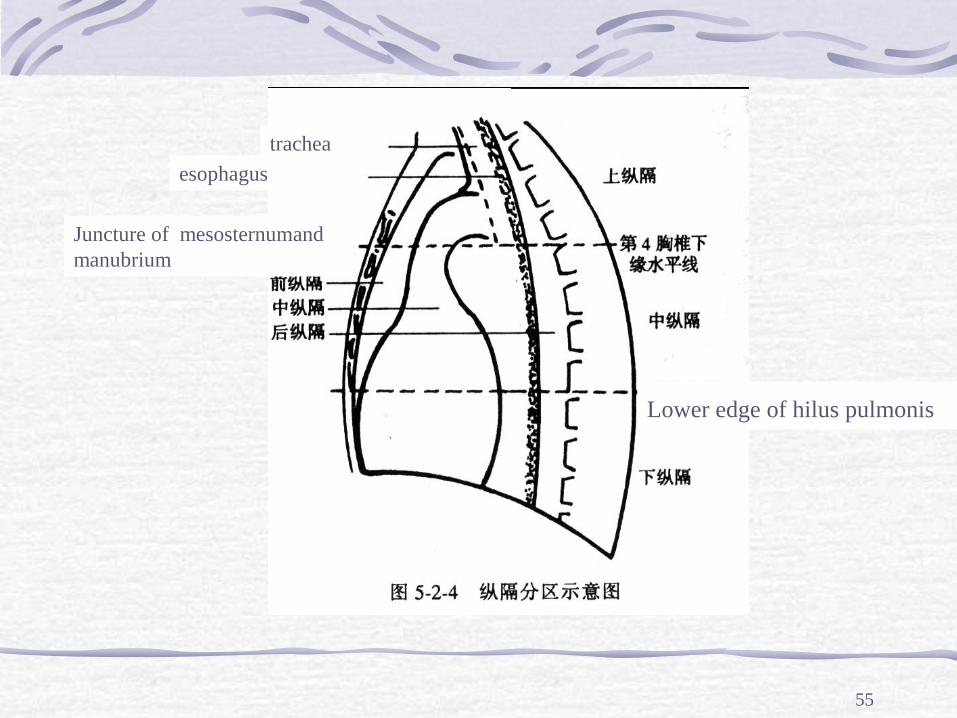
55
trachea
esophagus
Juncture of mesosternumand
manubrium
Lower edge of hilus pulmonis
56
Mediastinal mass (1)
Anterior mediastinum
Thymoma
Lymphoma
Teratoma
Thyroid mass
Germ cell neoplasm
Thymic cyst
57
Mediastinal mass (2)
Middle mediastinum
Bronchogenic cyst
Lymphadenopathy
Pericardial cyst
Tracheal tumours
Vascular abnormalities including aortic aneurysm,
aortic dissection, vascular variants
Esophageal abnormalities (achalasia, neoplasm,
hiatal hernia), esophageal varices
58
Mediastinal mass (3)
Posterior mediastinum
Extramedullary hematopoiesis
Lymphadenopathy
Neuroenteric cyst
Neurogenic neoplasm
Paravertebral abnormalies (infectious, malignant
and traumatic abnormalities of the thoracic spine)
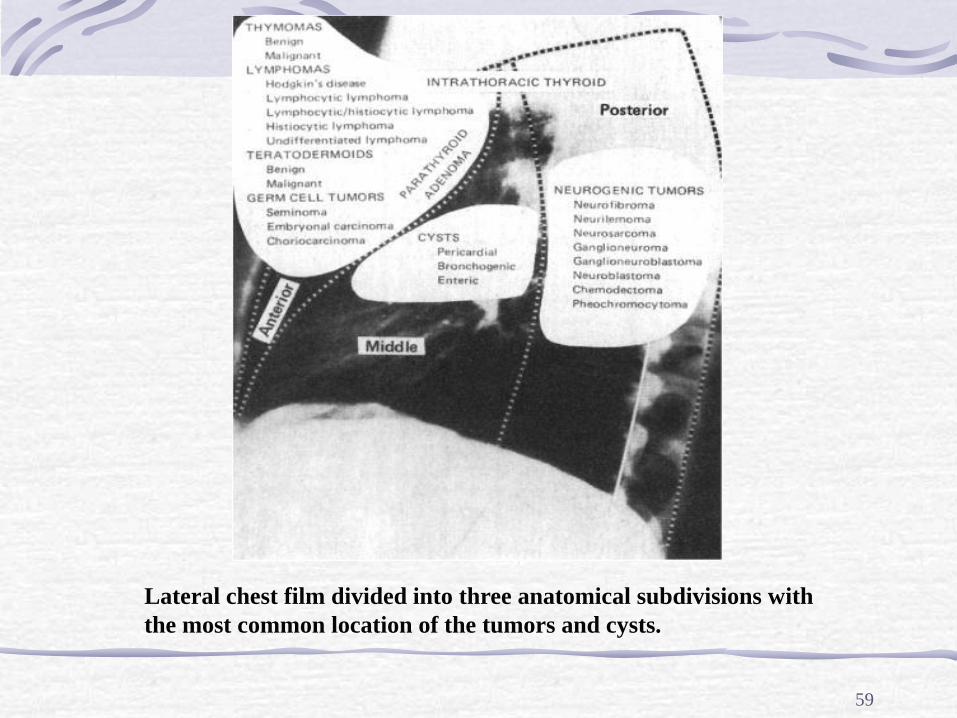
59
Lateral chest film divided into three anatomical subdivisions with
the most common location of the tumors and cysts.
60
Clinical features
Asymptomatic: in more than 50% of cases,
the lesion being detected as an incidental
finding.
Symptomatic: pressure effects on the
surrounding structures. Features may include
insidious onset of restrosternal chest pain,
dysphagia or dyspnea.
61
Investigations (1)
Over 50% as incidental findings on a chest X-ray
Further information from:
CT scan
barium swallow - if esophageal disease is suspected
doppler sonography or venography of brachiocephalic veins
or superior vena cava
Arteriography
MRI - when results of CT scan are equivocal
biopsy - if suspected neoplasm
62
Investigations (2)
advantages of MRI over CT:
distinguishes vessels and masses
contrast media unnecessary
imaging in multiple planes
good delineation of hilar structures
63
sagittal plane sagittal plane
64
sagittal plane coronal plane
65
Management (1)
thoracotomy may be considered for diagnosis
and removal
radiotherapy may be indicated for the
primary tumour or for any tumour residue -
this may be curative in neuroblastoma and
thymoma; it may achieve long-term control in
malignant teratoma
66
Management (2)
combination chemotherapy may be required
for neuroblastoma
note that treatment with radiotherapy may
cause dysphagia and an irritant cough during
and immediately after treatment. Occasionally
there may be later symptoms of pulmonary
fibrosis and pericardial fibrosis
67
CASES
68
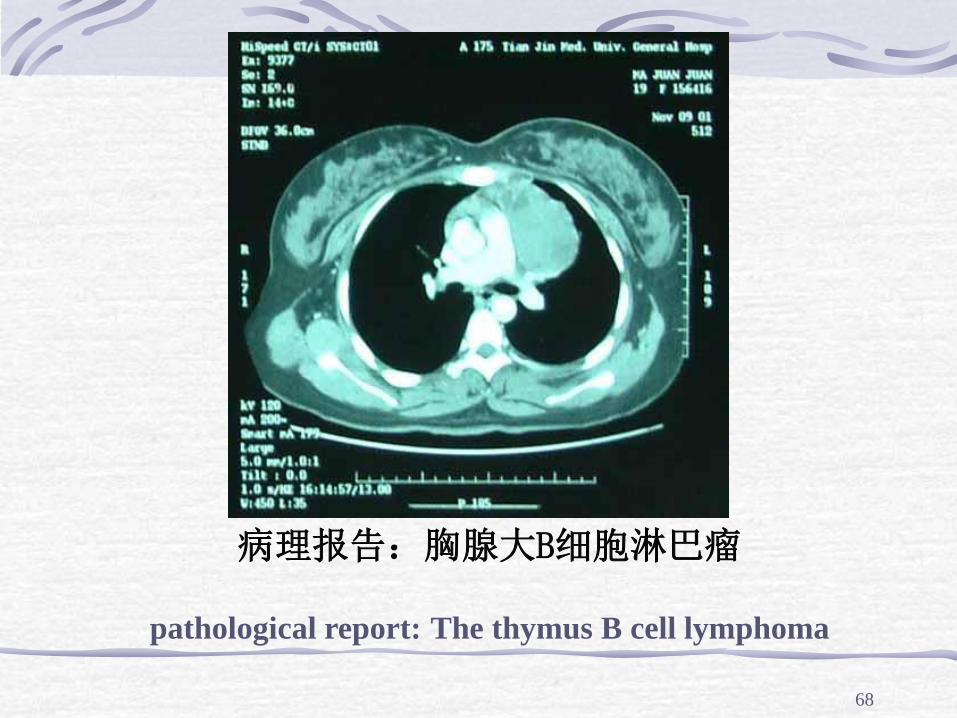
病理报告:胸腺大B细胞淋巴瘤
pathological report: The thymus B cell lymphoma
69
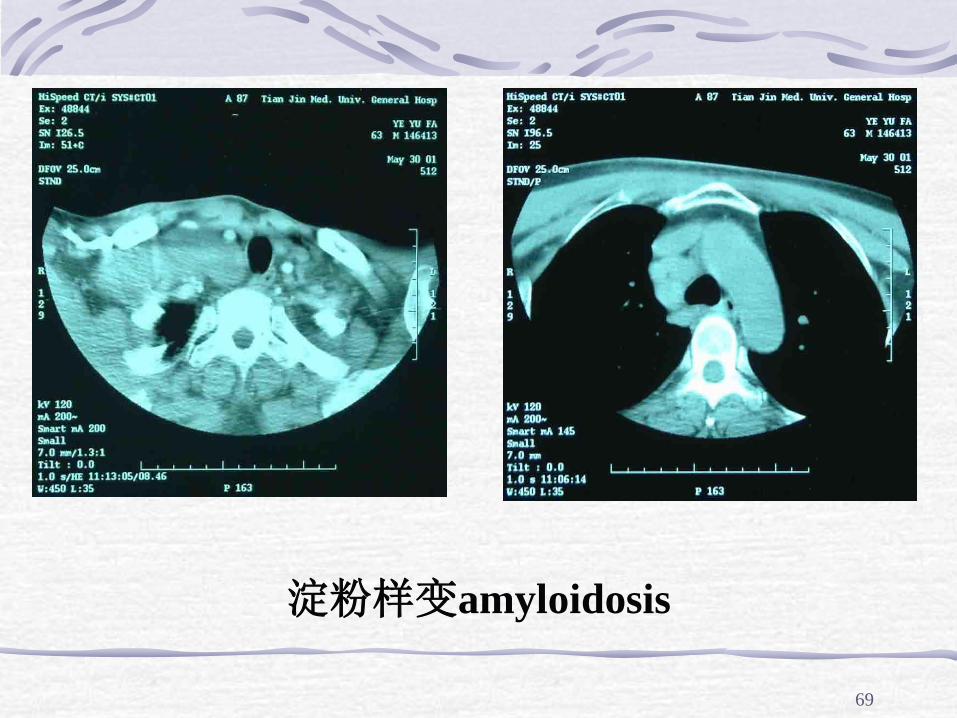
淀粉样变amyloidosis
70
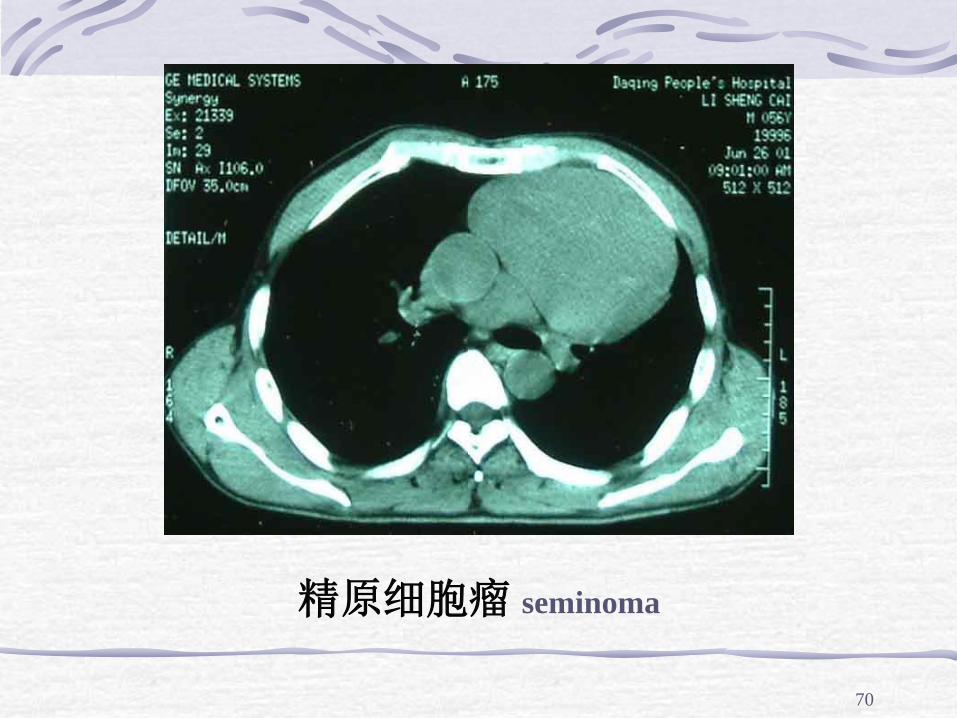
精原细胞瘤 seminoma
71
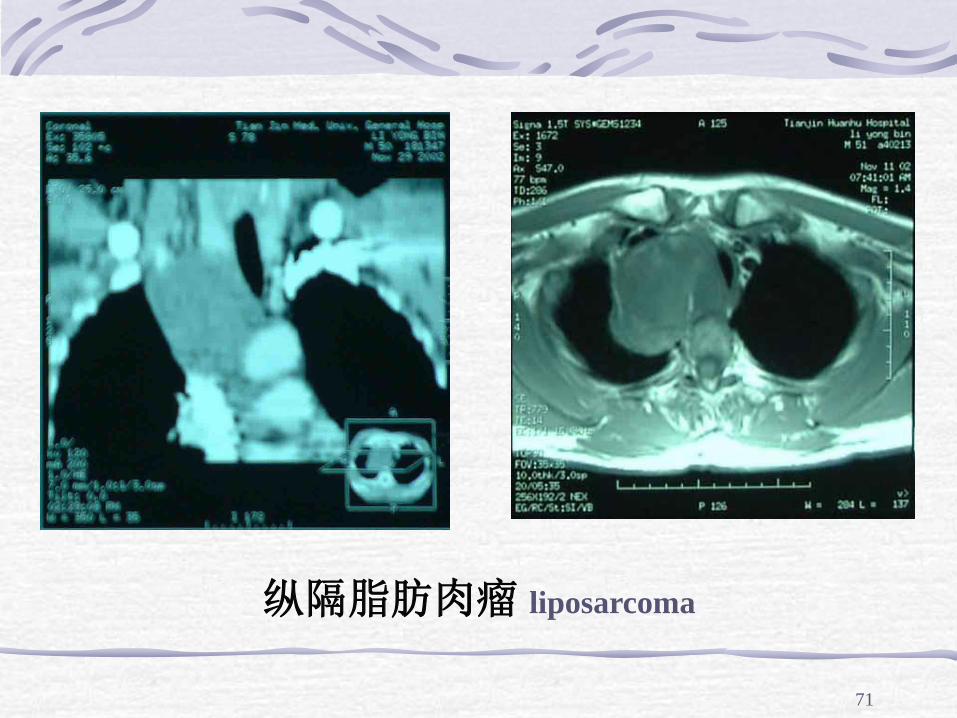
纵隔脂肪肉瘤 liposarcoma
72
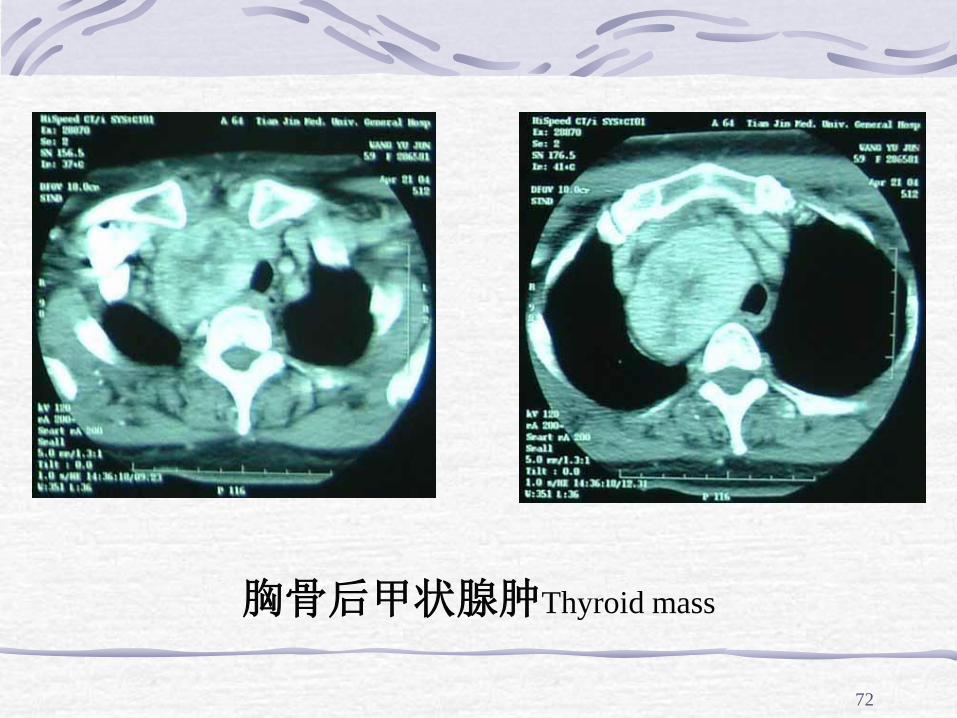
胸骨后甲状腺肿Thyroid mass
73
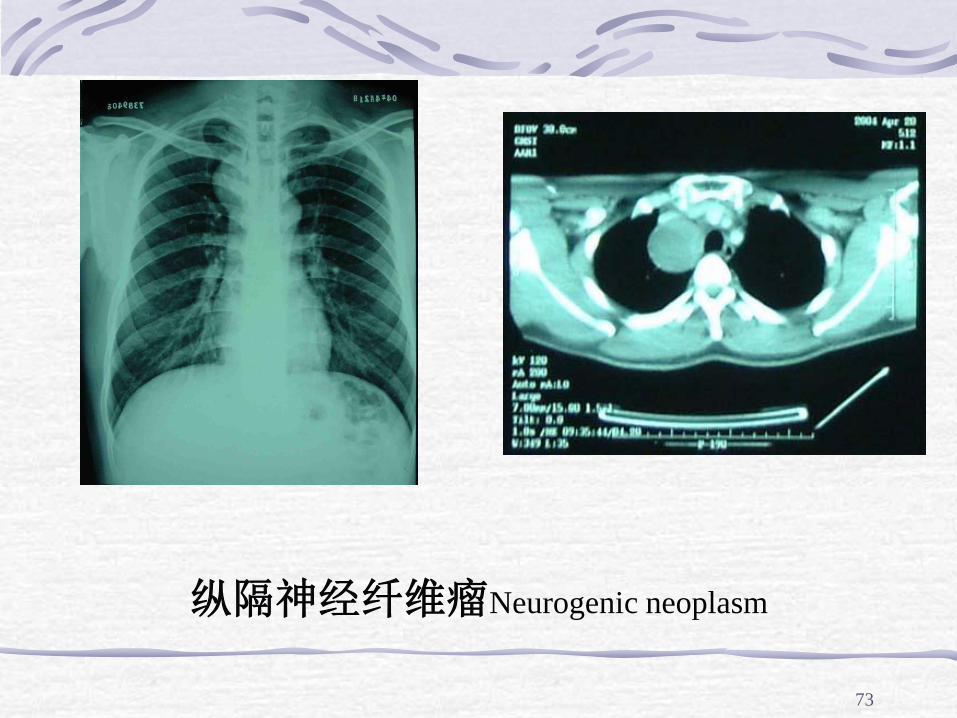
纵隔神经纤维瘤Neurogenic neoplasm
74
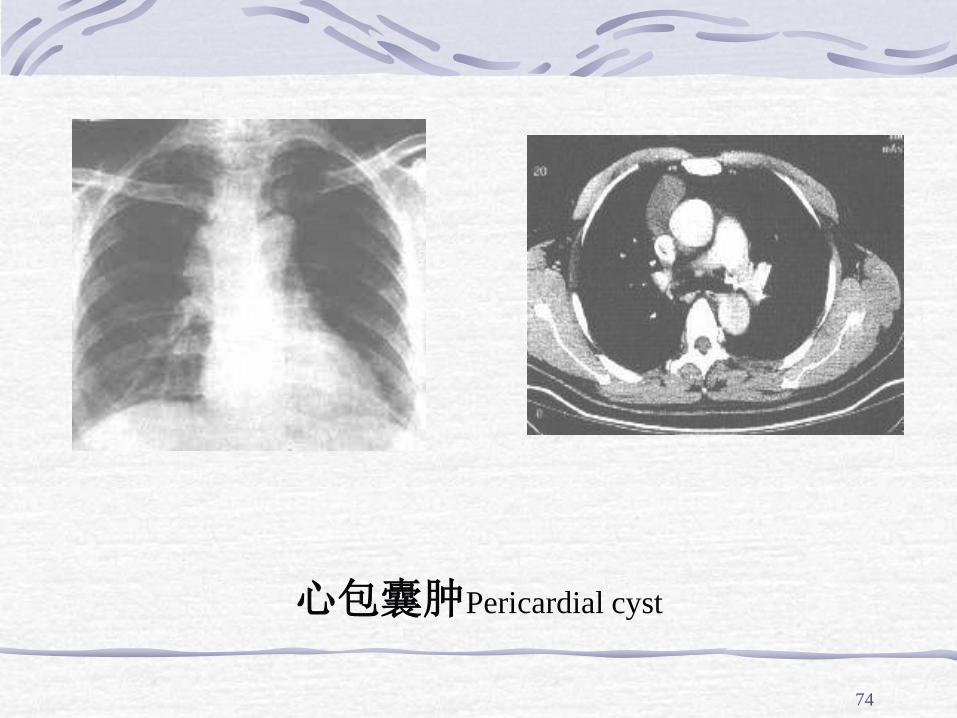
心包囊肿Pericardial cyst
75
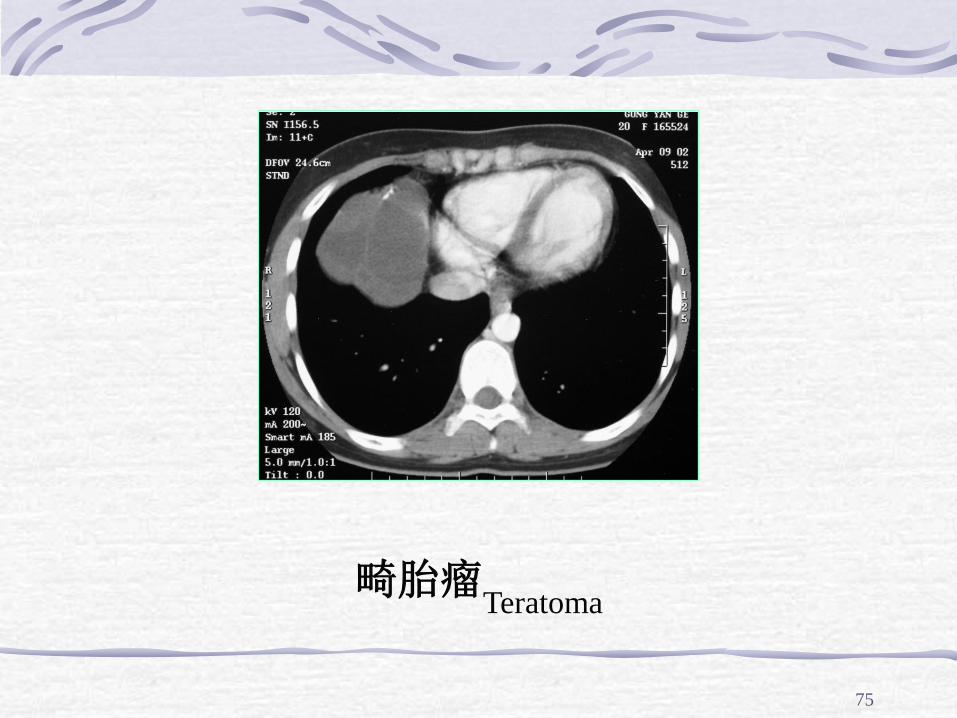
畸胎瘤Teratoma
76
胸腺瘤 Thymoma
Thymomas are one of the most common mediastinal
neoplasms - 90% are benign.
Association with a number of systemic disorders,
notably myasthenia gravis, hematologic cytopenias,
hypogamma-globulinemia, various collagen-vascular
diseases, and nonthymic cancers
77
78
79
Histological classification
Histological type via cell composition
Lymphocytic: More than two-thirds lymphocytic
Epithelial: Less than one-third lymphocytic
Lymphoepithelial (mixed): Neither more than
two-thirds nor less than one-third lymphocytic
80
Histological Classification of Thymoma
Cell Composition
细胞构成
Histological Type
组织学类型
>2/3 lymphocytic Lymphocytic
<1/3 lymphocytic Epithelial
>1/3, <2/3lymphocytic Lymphoepithelial (mixed)
81
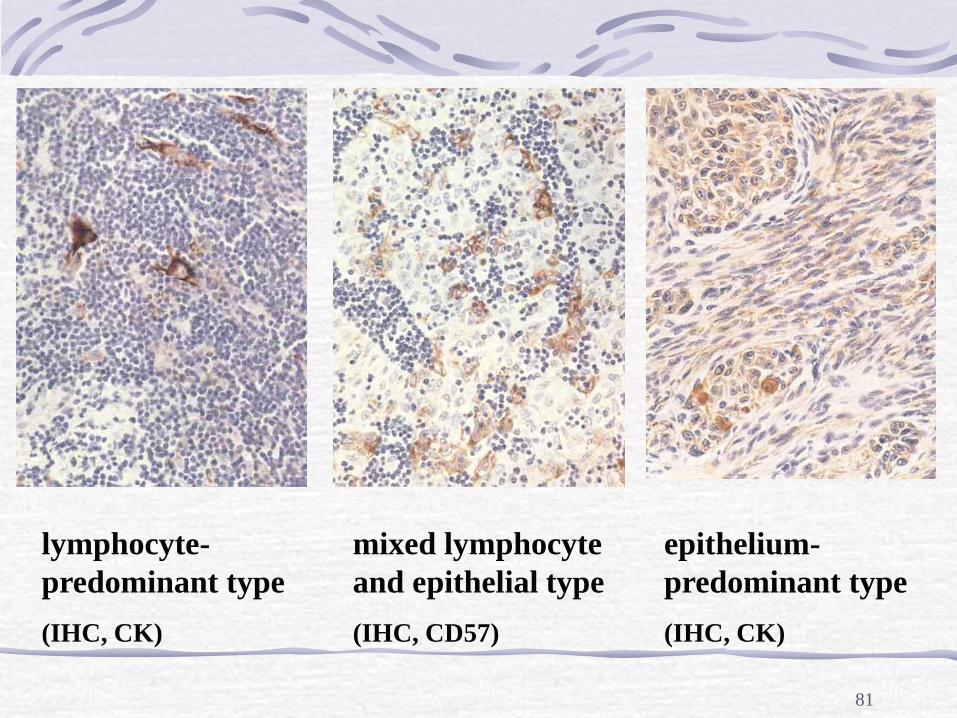
lymphocyte-
predominant type
(IHC, CK)
mixed lymphocyte
and epithelial type
(IHC, CD57)
epithelium-
predominant type
(IHC, CK)
82
Types Three main types are recognised
benign - the most common, accounting for 80-90% of thymomas. Characterized by a diffuse proliferation of neoplastic thymic epithelial cells and an abundance of lymphocytes. There is no capsular invasion.
malignant type I - cytologic features are identical to the benign thymoma but with additional invasion of the capsule. Occasionally, there may be metastases to the lungs and bone.
malignant type II - known as thymic carcinoma. There is capsular invasion and cytologic pleomorphism. The tumour often resembles a squamous cell carcinoma.
83
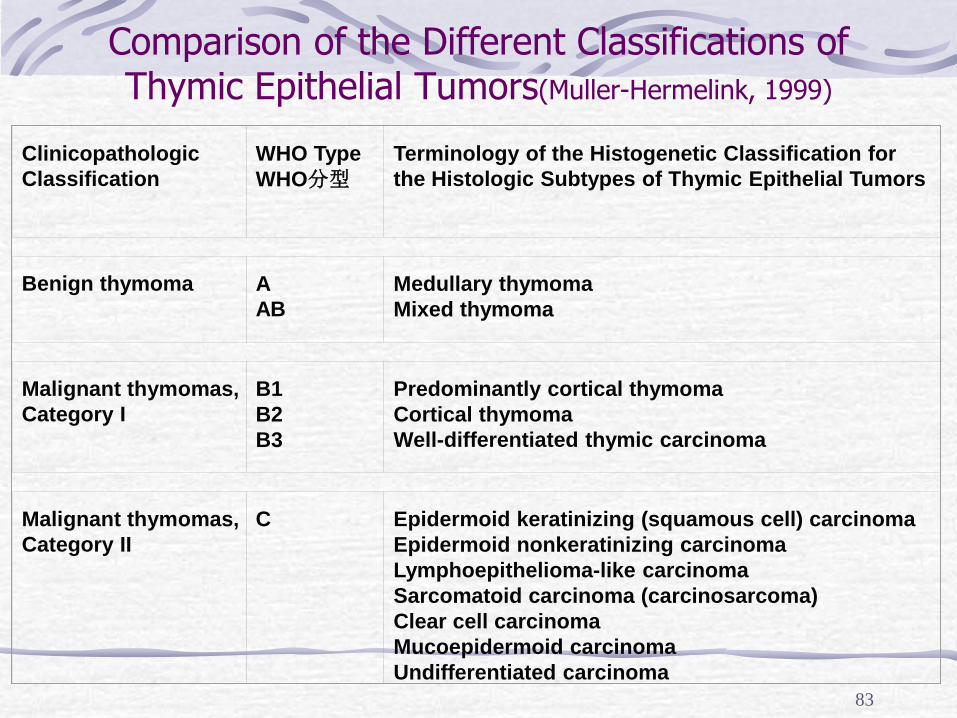
Comparison of the Different Classifications of Thymic Epithelial Tumors(Muller-Hermelink, 1999)
Clinicopathologic
Classification
WHO Type
WHO分型
Terminology of the Histogenetic Classification for
the Histologic Subtypes of Thymic Epithelial Tumors
Benign thymoma A
AB
Medullary thymoma
Mixed thymoma
Malignant thymomas,
Category I
B1
B2
B3
Predominantly cortical thymoma
Cortical thymoma
Well-differentiated thymic carcinoma
Malignant thymomas,
Category II
C Epidermoid keratinizing (squamous cell) carcinoma
Epidermoid nonkeratinizing carcinoma
Lymphoepithelioma-like carcinoma
Sarcomatoid carcinoma (carcinosarcoma)
Clear cell carcinoma
Mucoepidermoid carcinoma
Undifferentiated carcinoma
84
Clinical features (1)
Mean age of patients with thymomas is 50
years; rare in children where they are
associated with a poor prognosis
Males and females equally affected
Radiographic mass - most common in
anterosuperior mediastinum
85
Clinical features (2)
Variable clinical presentation dependent upon
the aggressiveness of the lesion include:
asymptomatic
features attributable to local pressure effects e.g.
cough, dyspnoea, dysphagia and superior venal
caval obstruction
associated systemic disorders (see associated
conditions)
86
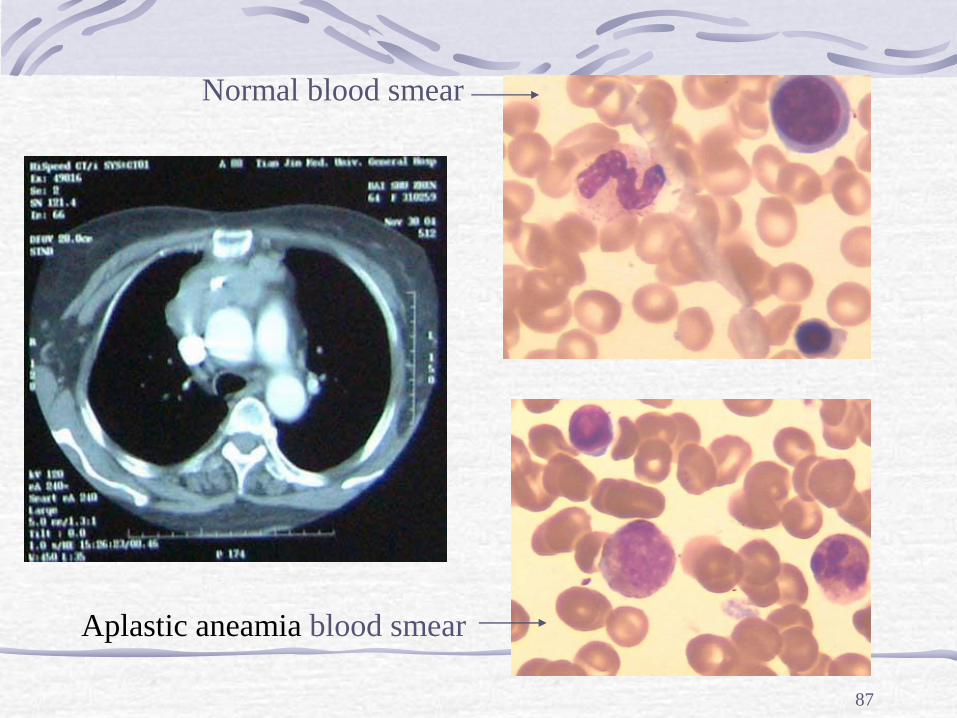
Associated conditions Thymomas may occur in association with a variety of
autoimmune and hematologic phenomena including:
myasthenia gravis - the most common association but less
often associated with more aggressive thymomas
hematologic cytopenias e.g. aplastic aneamia
Hypogammaglobulinemia
collagen vascular diseases e.g. systemic lupus erythematous
non-thymic malignancies
87
Aplastic aneamia blood smear
Normal blood smear
88
Diagnostic procedures Imaging Studies
PA and lateral chest radiographs
CT scan
CT scan with intravenous contrast dye
Biopsy: limited anterior mediastinotomy
or thoracoscopic approach
Fine-needle aspiration
89
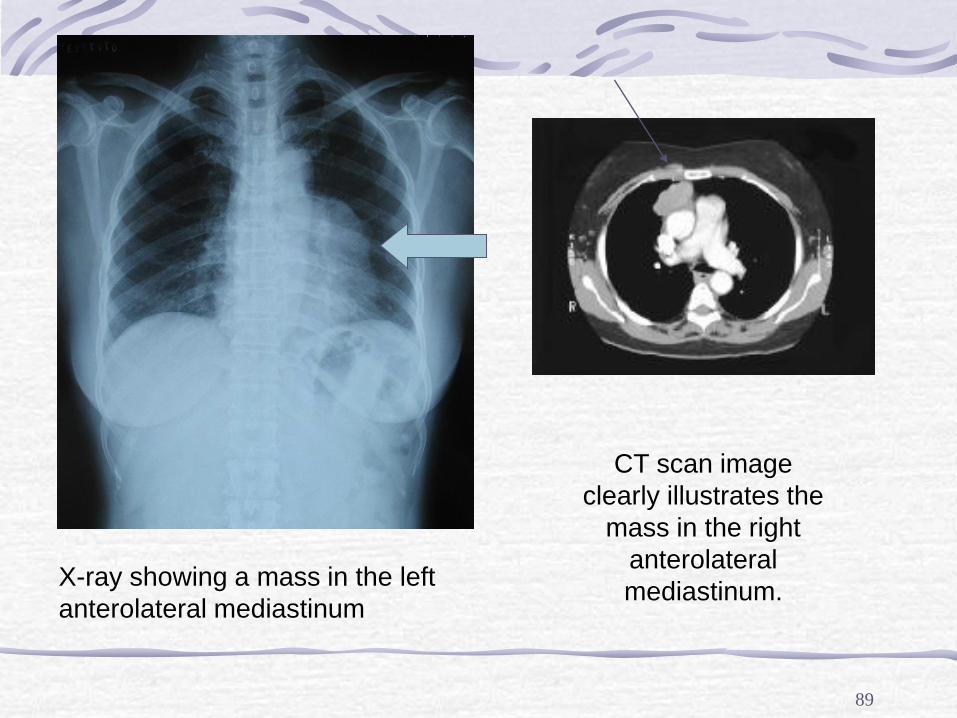
CT scan image
clearly illustrates the
mass in the right
anterolateral
mediastinum. X-ray showing a mass in the left
anterolateral mediastinum
90
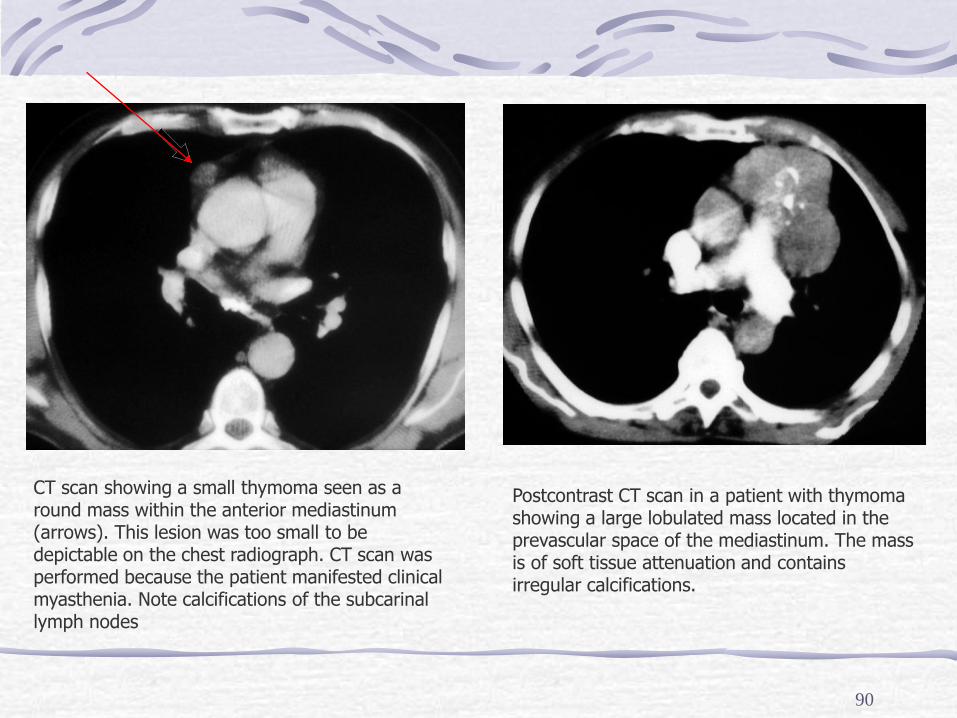
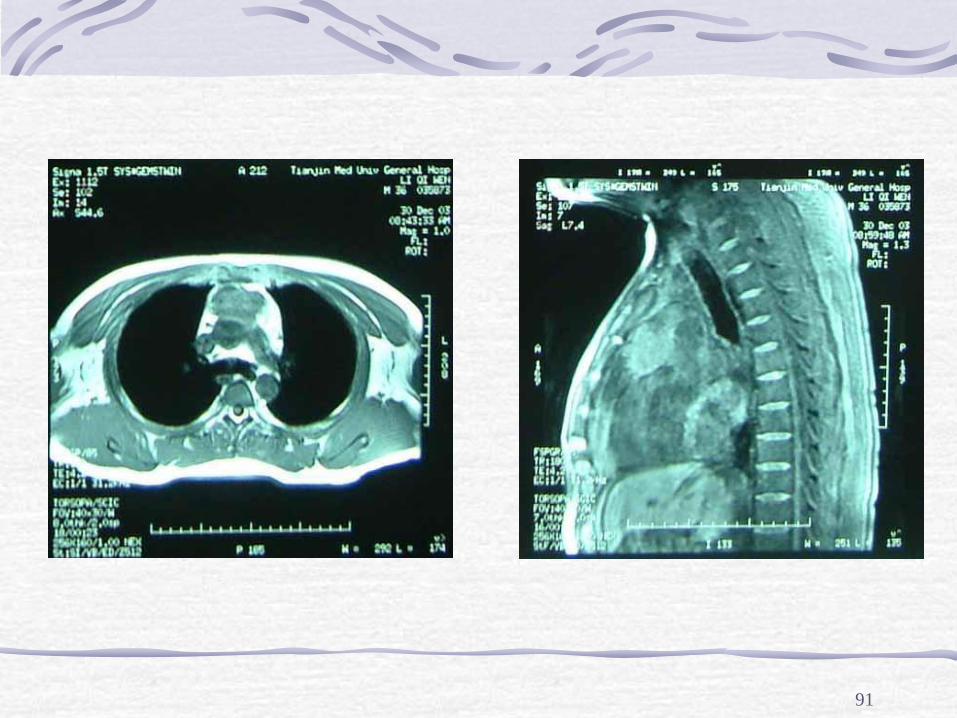
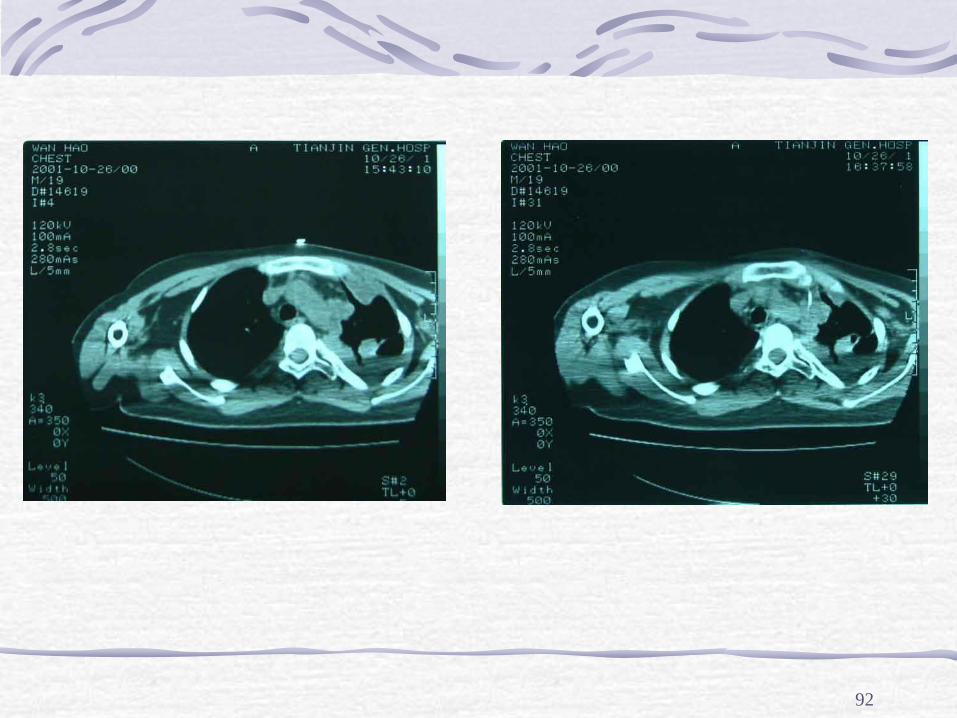
CT scan showing a small thymoma seen as a round mass within the anterior mediastinum (arrows). This lesion was too small to be depictable on the chest radiograph. CT scan was performed because the patient manifested clinical myasthenia. Note calcifications of the subcarinal lymph nodes
Postcontrast CT scan in a patient with thymoma showing a large lobulated mass located in the prevascular space of the mediastinum. The mass is of soft tissue attenuation and contains irregular calcifications.
91
92
93
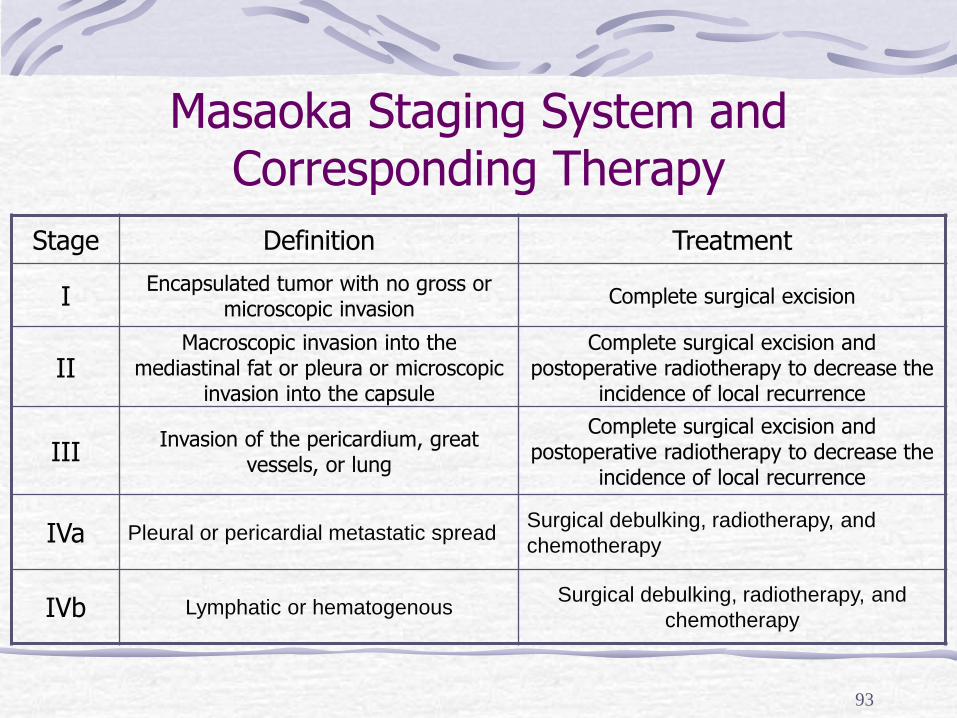
Masaoka Staging System and Corresponding Therapy
Stage Definition Treatment
I Encapsulated tumor with no gross or
microscopic invasion Complete surgical excision
II Macroscopic invasion into the
mediastinal fat or pleura or microscopic invasion into the capsule
Complete surgical excision and postoperative radiotherapy to decrease the
incidence of local recurrence
III Invasion of the pericardium, great
vessels, or lung
Complete surgical excision and postoperative radiotherapy to decrease the
incidence of local recurrence
IVa Pleural or pericardial metastatic spread Surgical debulking, radiotherapy, and
chemotherapy
IVb Lymphatic or hematogenous Surgical debulking, radiotherapy, and
chemotherapy
Surgical approaches for thynoma depend on the mass’s size, extraesophageal extension of the primary tumor .
95
Classical approach: median sternotomy
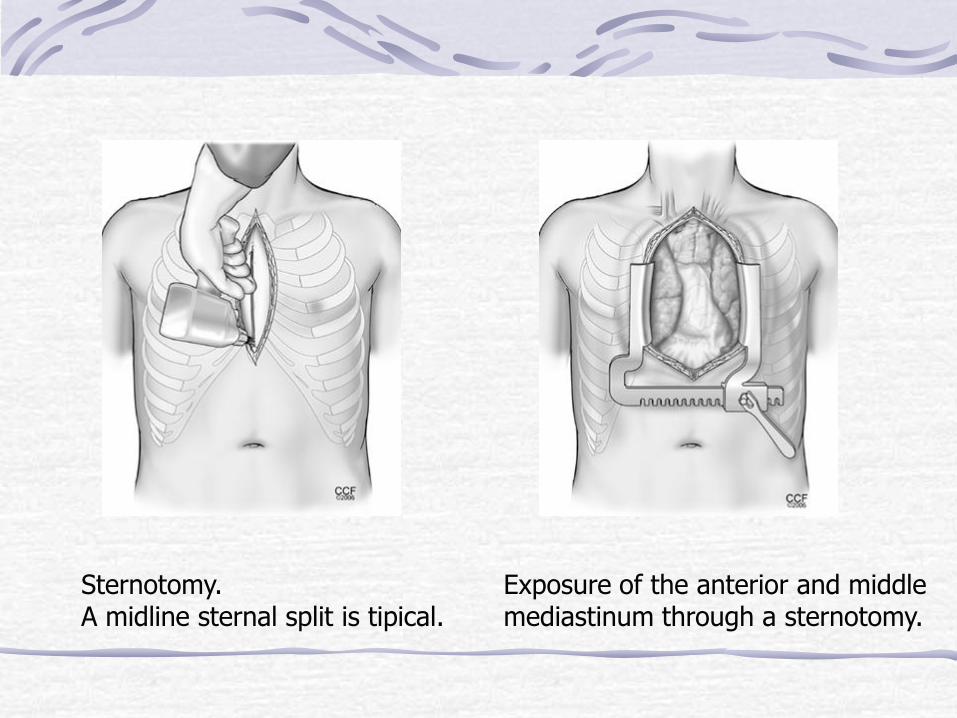
Sternotomy. A midline sternal split is tipical.
Exposure of the anterior and middle mediastinum through a sternotomy.
97
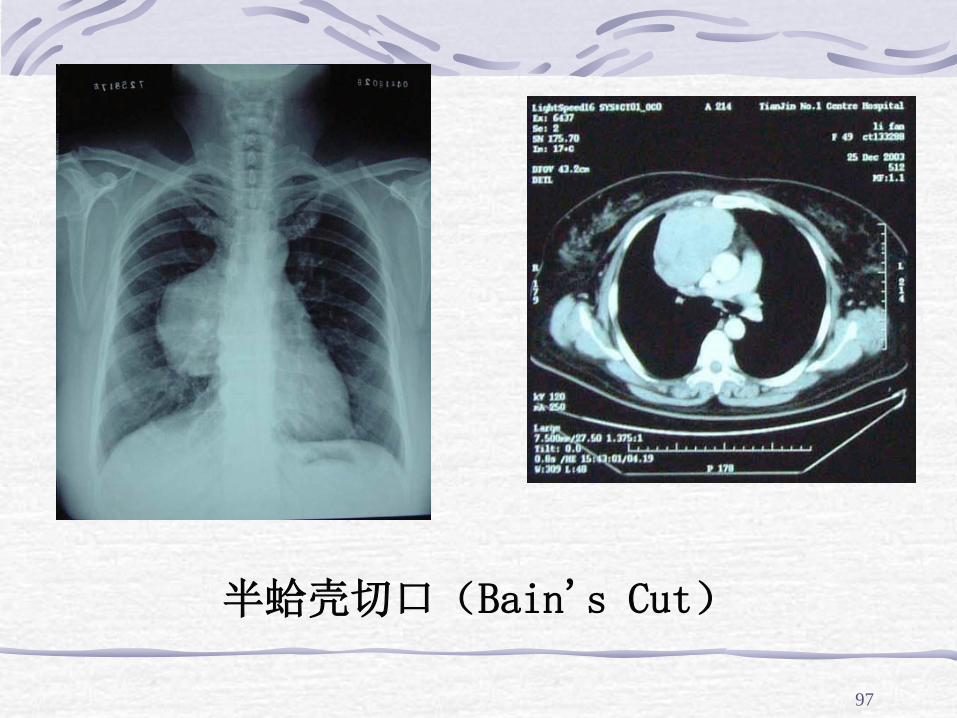
半蛤壳切口(Bain's Cut)
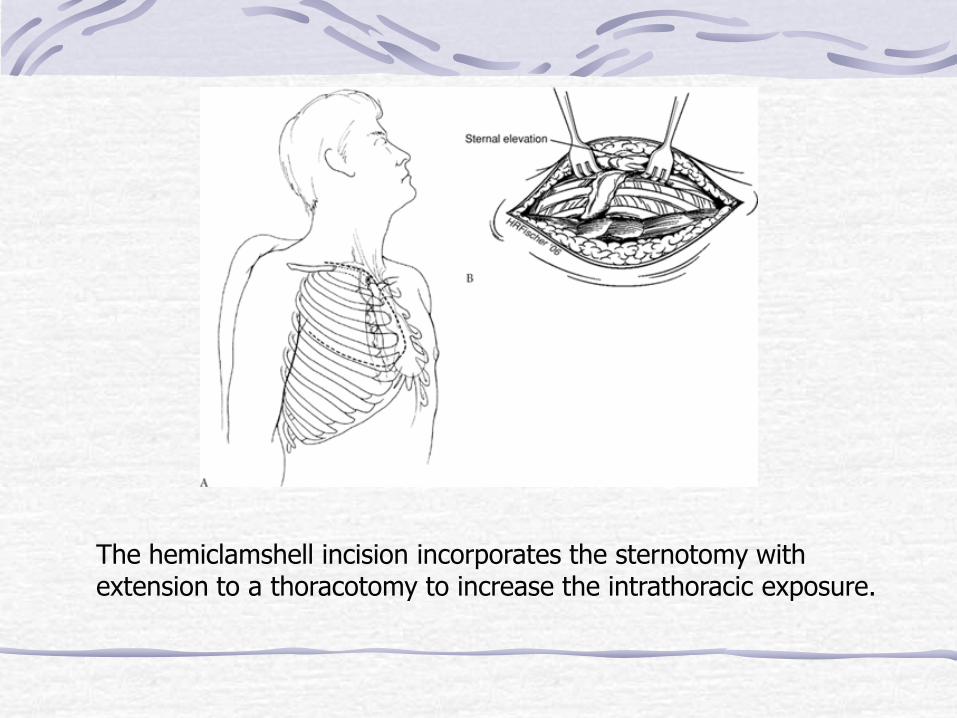
The hemiclamshell incision incorporates the sternotomy with extension to a thoracotomy to increase the intrathoracic exposure.
99
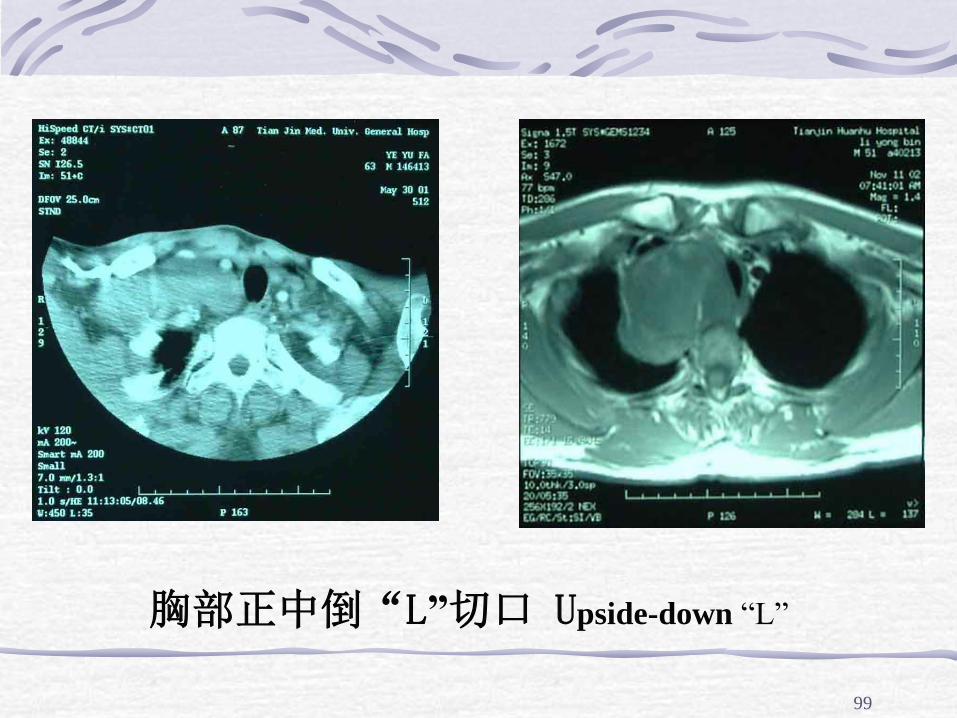
胸部正中倒“L”切口 Upside-down “L”
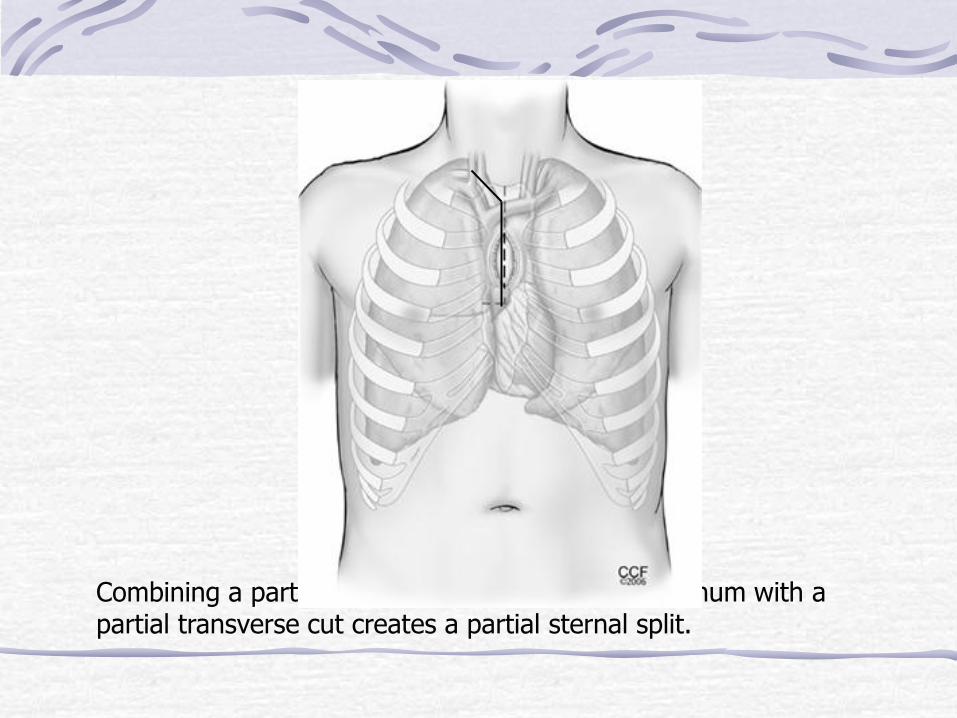
Combining a partial longitudinal division of the sternum with a partial transverse cut creates a partial sternal split.
101
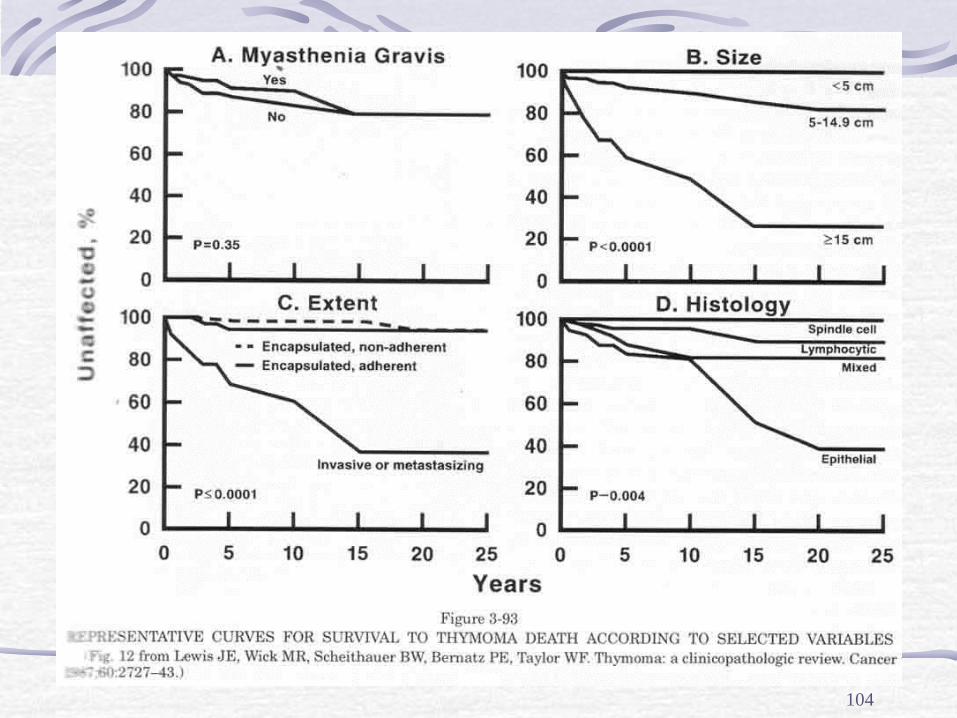
Prognosis
benign - excellent prognosis but there is a
2% recurrence rate if excision is incomplete
malignant type I - excellent prognosis if
resection is complete
malignant type II - approximate 20% 5-year
survival after treatment.
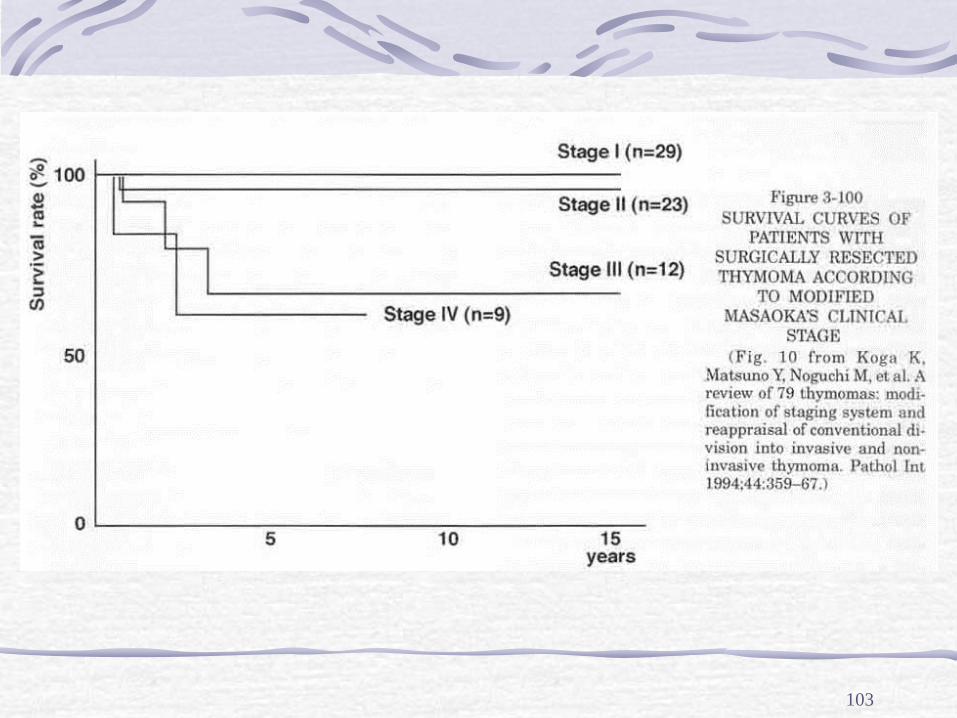
102
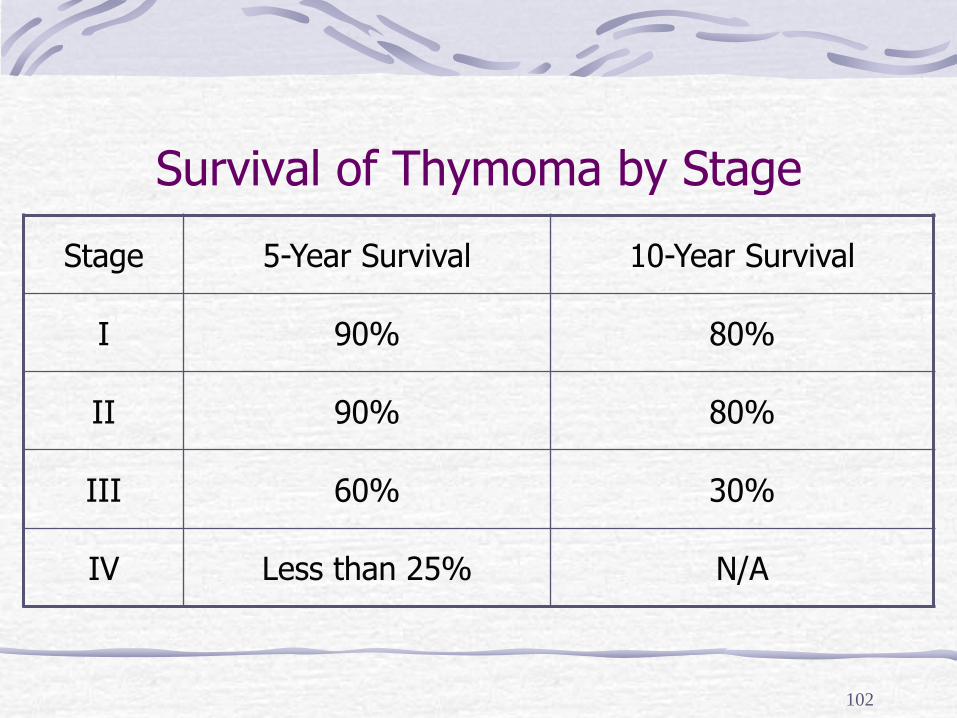
Survival of Thymoma by Stage
Stage 5-Year Survival 10-Year Survival
I 90% 80%
II 90% 80%
III 60% 30%
IV Less than 25% N/A
103
104
105
CASES

106
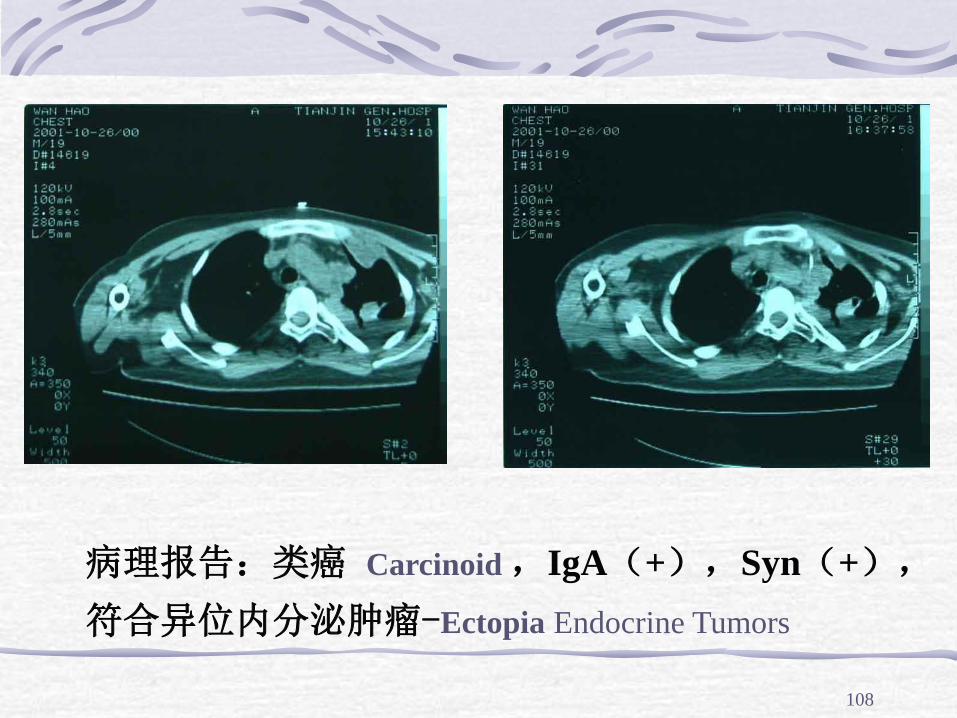
实验室检查:血糖(Blood sugar)12.2mmol/L↑,24小时尿糖(24hUrine sugar) 67.8g↑,血钾 K+ 1.7 mmol/L↓,空腹血浆皮质醇(Cortisol )>50μg/ml↑,血浆促肾上腺皮质激素(ACTH)>1250ng/ml,尿皮质醇>1100μg/24h↑,大小剂量地塞米松抑制试验(dexamethasone suppression test)均不被抑制
Cushing's syndrome
107
108
病理报告:类癌 Carcinoid ,IgA(+),Syn(+),
符合异位内分泌肿瘤-Ectopia Endocrine Tumors
109
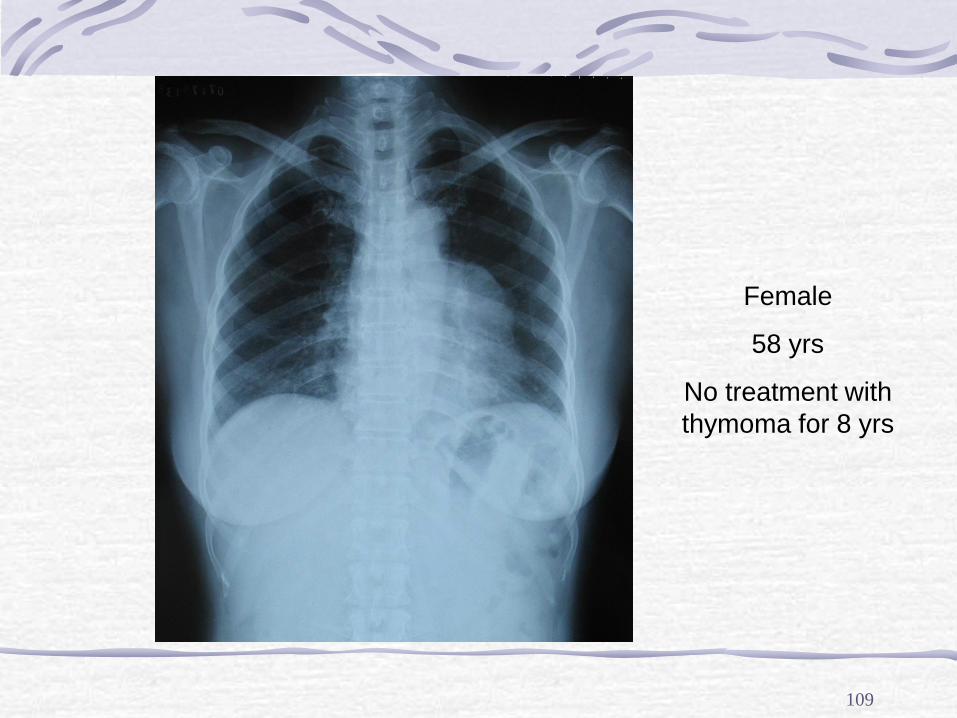
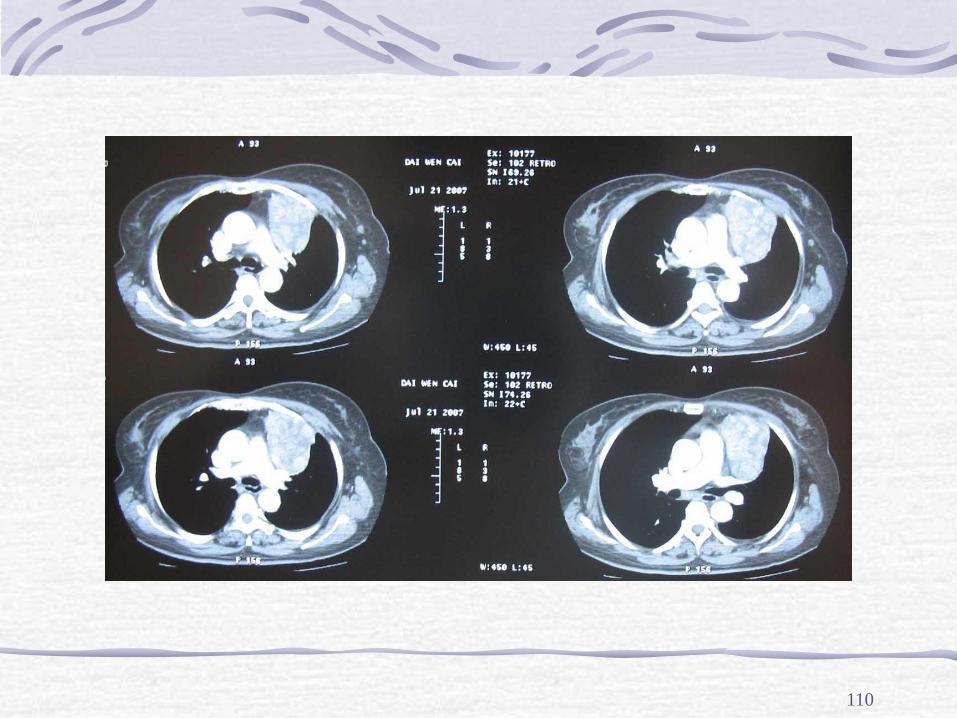
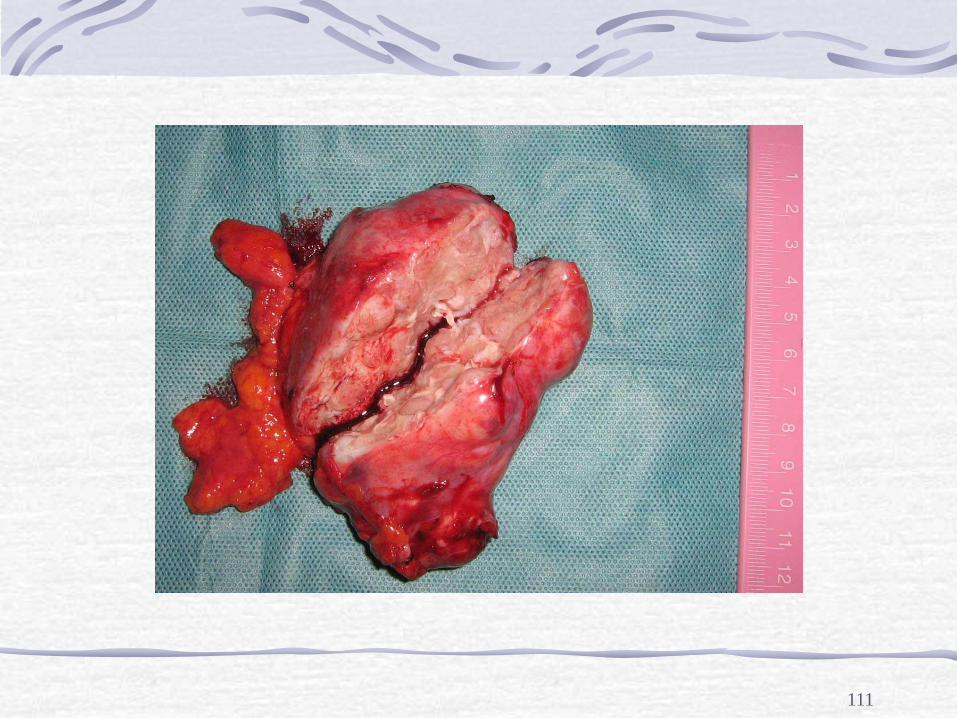
Female
58 yrs
No treatment with
thymoma for 8 yrs
110
111
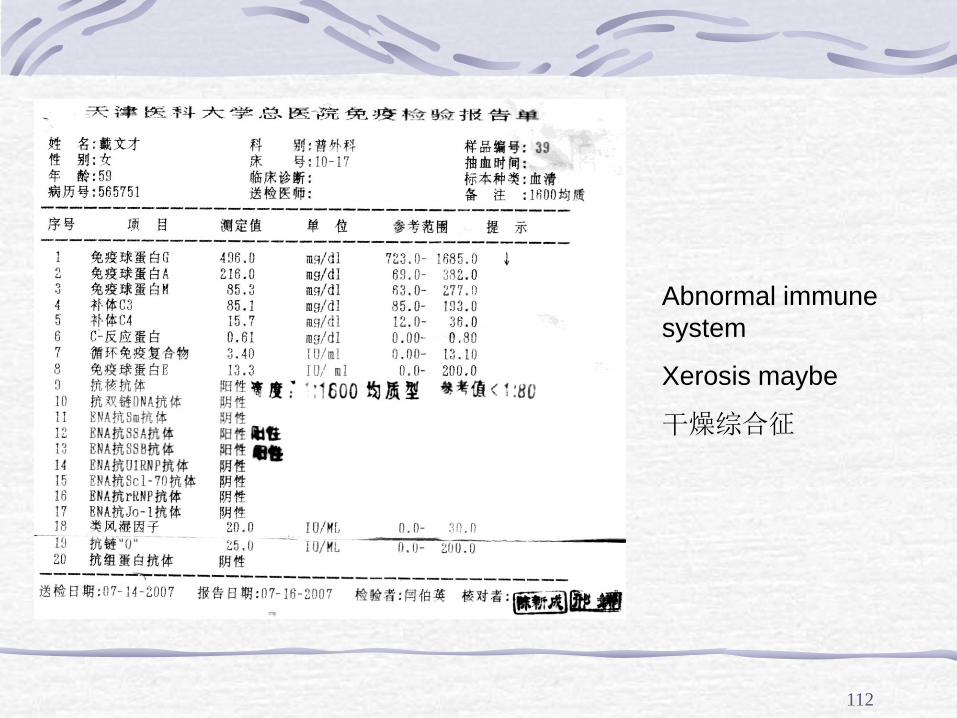
112
Abnormal immune
system
Xerosis maybe
干燥综合征
113
Questions Term
Empyema
Blank
Natural history of empyema(3 stages)
3 anatomy regions of mediastinum
Simple answer
Core principles of empyema management
Types of anterior mediastinal masses(4 or more)
2009-3-18 114