Embed Size (px)
Citation preview
Pain Treatment in Children with Serious Illness and Intellectual Disability: From Myths, Morphine and Multimodal Analgesia Stefan J. Friedrichsdorf, MD, FAAPMedical Director, Department of Pain Medicine, Palliative Care & Integrative MedicineChildren's Hospitals and Clinics of Minnesota, Minneapolis/St. Paul, MNAssociate Professor of Pediatrics, University of Minnesota Medical School
Objectives• Evaluateassumptionsaboutopioiduseinchildren
• Discusshowmultipleagents,interventions,rehabilitation,psychologicalandintegrative(“non-pharmacologic”)therapiesactsynergisticallyformoreeffectivepediatricpaincontrolwithfewersideeffectsthanasingleanalgesicormodality
• Practiceformulatingatreatmentplanforacase-studyinsmallgroups
@NoNeedlessPain
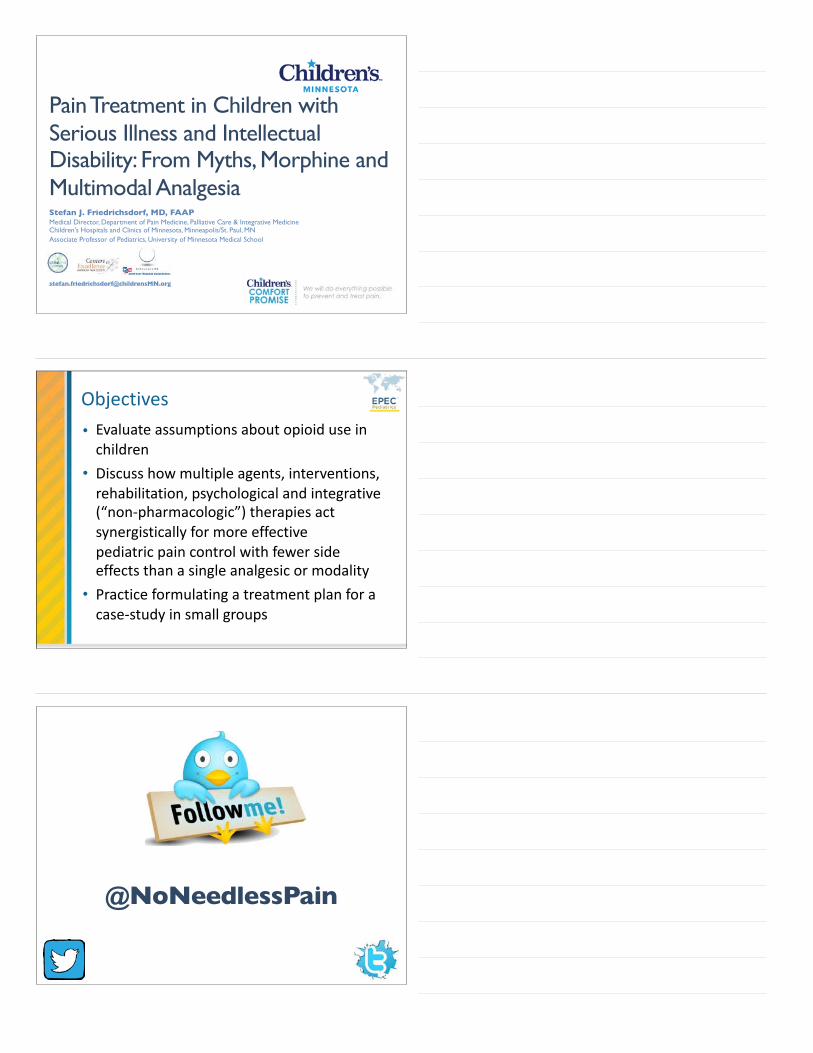
Causes of death in US children 2015 due to life-limiting conditions 0-24 years (n=11,933)
CongenitalAnomalies50%
MalignantNeoplasms23%
HeartDisease11%
ChronicLow.RespiratoryDisease7%
CirculatorySystemDisease4% Other
5%
NaSonalVitalStaSsScsSystem,NaSonalCenterforHealthStaSsScs,CDChUps://www.cdc.gov/injury/wisqars/pdf/leading_causes_of_death_by_age_group_2015-a.pdf
Wolfe J, Orellana L, Ullrich C et al Symptoms and Distress in Children with Advanced Cancer: Prospective Patient-Reported Outcomes from the PediQUEST Study, JCO 2015.
Distressing Symptoms = Common in PPC
Symptoms of PPC patients
FeudtnerC,KangTI,HexemKR,FriedrichsdorfSJ,OsengaK,SidenH,etal.Pediatricpalliativecarepatients:aprospectivemulticentercohortstudy.Pediatrics2011;127(6):1094-101.
• Symptom distress is strongly associated with health-related quality of life; Children with cancer: during the last 12 weeks of life, 11 distressing symptoms were associated with reductions in HRQOL Rosenberg AR, Orellana L, Ullrich C, Kang T, Geyer JR, Feudtner C, et al. Quality of Life in Children With Advanced Cancer: A Report From the PediQUEST Study. J Pain Symptom Manage. 2016;52(2):243-53.
Trigger Diagnoses for Consults
• UK: all PICU admissions over 15 months (n=89,127) Fraser LK, Parslow R. Children with life-limiting conditions in paediatric intensive care units: a national cohort, data linkage study. Arch Dis Child. 2017.
– Children with life-limiting conditions (LLC)• 57.6% (n=89,127) of PICU admissions • 72.90% (n=4,821) of deaths
• Pediatric Cancer: presence of “trigger diagnoses" increased likelihood of palliative principle introduction 3.41 times (p < 0.003) Weaver MS, Rosenberg AR, Tager J, Wichman CS, Wiener L. A Summary of Pediatric Palliative Care Team Structure and Services as Reported by Centers Caring for Children with Cancer. J Palliat Med. 2018;21(4):452-462.
"If you can't add life to my son's days, then don't add days to my
son's life"Father of a toddler to Dr. Sunny Anand on PICU
Outcomes Improve with PPC Involvement
• Parents of children with cancer report less distress from pain, dyspnea and anxiety at EOL Wolfe et al. J Clin Onc 2008
• Children who received PPC/Oncology more likely to have fun (70% versus 45%) and to experience events that added meaning to life (89% versus 63%) Friedrichsdorf SJ, Postier AC, Dreyfus J, Sencer S, Wolfe J: Improved Quality of Life in Children with Cancer at End of Life related to Home-based Palliative Care. J Pall Medicine 2015. 18(2):143-50
• Families who received PPC/Oncology report improved communication Kassam A, Skiadaresis J, Alexander S et al Differences in End-of-Life Communication for Children with Advanced Cancer who were Referred to a Palliative Care Team. Pediatr Blood Cancer, 2015. 62(8): p. 1409-13.
• Children receiving PPC experience shorter hospitalizations and fewer emergency department visits Ananth, P., et al., Hospital Use in the Last Year of Life for Children With Life-Threatening Complex Chronic Conditions. Pediatrics, 2015. 136(5): p. 938-46.
PPC = better clinical care?
• Integration of PPC inpatient team associated with fewer diagnostic /monitoring procedures and improved pain management documentation at end-of-life Osenga K, Postier A, Dreyfus J, Foster L, Teeple W, Friedrichsdorf SJ. A Comparison of Circumstances at the End of Life in a Hospital Setting for Children With Palliative Care Involvement Versus Those Without. J Pain Symptom Manage. 2016;52(5):673-80.
• Involvement of PPC team with adolescent and young adult oncology patients associated with the receipt of less intensive treatments Snaman JM, Kaye EC, Lu JJ, Sykes A, Baker JN. Palliative Care Involvement Is Associated with Less Intensive End-of-Life Care in Adolescent and Young Adult Oncology Patients. J Palliat Med. 2017;20(5):509-516.
– last month of life:• on ventilator: 34% vs 63%• invasive procedure 1 vs 3 • fewer deaths in the ICU (38% vs 68%)• DNR 2 days vs 6 days before death
So, how do we treat the individual pain patient in front of us ?
Hmhh...Spoiler Alert: Crystal-clear answer on 3rd last slide!
Alexis“Lexi• 7-year-oldgirl(20kg)• Progressiveneurologic,metabolicorchromosomallybasedconditionwithimpairmentofthecentralnervoussystem(e.g.mitochondrialdisease)
• Multiplelong-termhospitalizationsforcomplicationsofdisease&therapy
• Athome;“intractable”pain
Video
(1) Identify and treat underlying disease process
AdvancedmanagementofpaininPPC:Step1
Lexi
• AssumingPatienthasmixedpain…• Whatarethenextsteps?
What are we measuring...?
(1) Nociceptive Pain: arises from the activation of peripheral nerve endings (nociceptors) that respond to noxious stimulation [e.g. localized, sharp, squeezing, stabbing, or throbbing]
• Somatic (for example, muscles, joints)
• Chronic somatic pain typically well localized & often results from degenerative processes (such as arthritis)
(2) Visceral (internal organs) [poorly localized, dull, crampy, or achy]
(3) Psycho-social-spiritual-emotional Pain / Total Pain
(4) Persistant (Chronic) Pain
• Pain beyond expected time of healing
(5) Neuropathic Pain: resulting from injury to, or dysfunction of, the somatosensory system. [burning, shooting, electric, or tingling]
• Central pain: caused by a lesion or disease of the central somatosensory nervous system
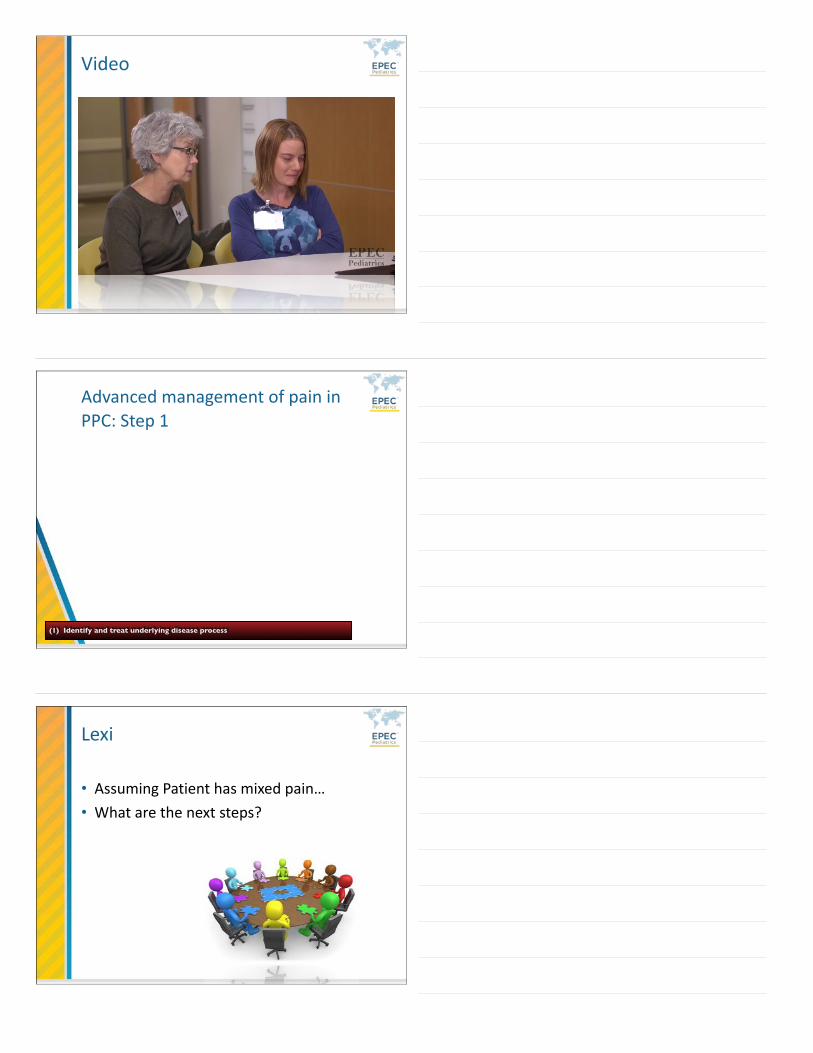
Pain Score 9/10
Somatic Pain
Somatic Pain
“Myhearthurts”
Visceral Pain
0
5
10 Child A Child B
What are we measuring...?
Neuropathic Pain
Validated Pinky Scale (PS) Pain Assessment
• Comprehensive Review Seers T, Derry S, Seers
K, Moore RA. Professionals underestimate patients' pain: a comprehensive review. Pain. 2018;159(5):811-818.
• High-quality studies (blind, comprehensive, or random sampling, >200 patients) consistently reported underestimation (10/11; 91%)
• Extent of underestimation tended to increase with pain severity
• Professionals consistently tend to underestimate pain compared with assessment by patients
• This tendency is more pronounced with more severe pain, and the extent of underestimation can be large
• It is likely that this contributes to undertreatment of pain
So how do clinicians do in pain assessment?
High specificity, low sensitivity…? Don’t forget:
• Withdrawal: WAT-1 score Franck, L et al, (2008) Ped Crit Care Med, Vol 9, no. 6 http://familynursing.ucsf.edu/research-and-clinical-tools Neonatal Abstinence Scoring Tool (Finnegan) Finnegan LP. Neonatal abstinence. In: Nelson NM, ed. Current Therapy in
Neonatal–Perinatal Medicine. 2nd ed. Toronto, Ontario: BC Decker Inc; 1990
• Delirium: CAPD Traube, C., et al., Cornell Assessment of Pediatric Delirium: a valid, rapid, observational tool for screening delirium in the
PICU. Crit Care Med, 2014. 42(3): p. 656-63.
• Sedation: SBS score Curley, M.A., et al., State Behavioral Scale: a sedation assessment instrument for infants and young children
supported on mechanical ventilation. Pediatr Crit Care Med, 2006. 7(2): p. 107-14.
Measuring pain alone…?
Is it Mixed Pain...?
• Children with CP: Daily pain 8.1% Houlihan CM, O’Donnell M, Conaway M, Stevenson RD: Bodyli pain and
health-related quality of life in children with cerebral palsy. Develop Med Child Neurol 2004, 46:305-10
• Cognitively impaired, non-communicating children: Daily pain 23.5 % Stallard P, Williams L, Lenton S, Velleman R: Pain in cognitively impaired, non-communicating children. Arch Dis Child 2001;85-460-2
• 275 children with progressive, non-curable genetic, metabolic, or neurological conditions: Pain 53% [Most of the time: 21.8 %] Friedrichsdorf SJ, Postier AC, Andrews GS, Hamre KES, Steele R, Siden H: Pain reporting and analgesia management in 270 children with a progressive neurologic metabolic or chromosomally based condition with impairment of the central nervous system cross sectional, baseline results from an observational longitudinal study. J Pain Research 2017 (10):1841-1852
HOT OFF THE
* PRESS *
Pain
Withdrawal
Delirium
Nociceptive Pain
Neuropathic Pain
Visceral Pain
Psychological pain
Anxiety
Depression
Spiritual Pain
Social Pain
Chronic Pain
Poor sleep hygiene
Mental Health
School absenteeism
Total Pain
Deconditioned
Racial Disparity
Multimodal AnalgesiaNo Needless Pain: The Children’s Comfort Promise
https://vimeo.com/20329079
(1) Identify and treat underlying disease process (radiation?) (corticosteroids?)
AdvancedmanagementofpaininPPC:Step2
(2) Integrative therapies & Rehabilitation: manage comorbidities (anxiety, sleep disturbances). Psychological Therapies.
Integrative, rehabilitative & supportive therapies
• Expected part of treatment protocol; Age-appropriate modalities include
• Physical (massage, TENS, comfort positioning, allowing family for close contact/touch)
• Rehabilitation (physical therapy, occupational therapy)
• Early increasing-intensity treadmill exercise reduces neuropathic pain (in rats) Lopez-Alvarez, V.M., et al., Early increasing-intensity treadmill exercise reduces neuropathic pain by preventing nociceptor collateral sprouting and disruption of chloride cotransporters homeostasis after peripheral nerve injury. Pain, 2015. 156(9): p. 1812-25.
• Behavioral (deep breathing, imagery, hypnosis, smart-phone/tablet “apps”)
• Acupressure, acupuncture, aromatherapy
Integrative modalities • Integrative modalities
effective in management of pediatric pain Hunt, K.; Ernst, E. The evidence-
base for complementary medicine in children: A critical overview of systematic reviews. Arch Dis Child 2011, 96, 769-776.; Friedrichsdorf, S.; Kuttner, L.; Westendorp, K.; McCarty, R. Integrative pediatric palliative care. In Integrative pediatrics, Culbert, T.; Olness, K., Eds. Oxford University Press: 2010. pp 569-93; Evans, S.; Tsao, J.C.; Zeltzer, L.K. Complementary and alternative medicine for acute procedural pain in children.
Alternative therapies in health and medicine 2008, 14, 52-56.
include• Hypnosis Kuttner, L.; Friedrichsdorf, S.J.
Hypnosis and palliative care. In Therapeutic hypnosis with children and adolescents., 2nd ed.; Crown House Publishing Limited: Bethel, 2013; pp 491-509.; Richardson, J.; Smith, J.E.; McCall, G.; Pilkington, K. Hypnosis for procedure-related pain and distress in pediatric cancer patients: A systematic review of effectiveness and methodology related to hypnosis interventions. J Pain Symptom Manage 2006, 31, 70-84.
• Guided imagery Dobson,
C.E.; Byrne, M.W. Original research: Using guided imagery to manage pain in young children with sickle cell disease. The American journal of nursing 2014, 114, 26-36; test 37, 47.
• Yoga Bussing, A.; Ostermann, T.; Ludtke, R.; Michalsen, A.
Effects of yoga interventions on pain and pain-associated disability: A meta-analysis. The journal of pain : official journal of the American Pain Society 2012, 13, 1-9.; Evans, S.; Moieni, M.; Taub, R.; Subramanian, S.K.; Tsao, J.C.; Sternlieb, B.; Zeltzer, L.K. Iyengar yoga for young adults with rheumatoid arthritis: Results from a mixed-methods pilot study. J Pain Symptom Manage 2010, 39, 904-913.
• Acupuncture Vas, J.; Santos-Rey, K.;
Navarro-Pablo, R.; Modesto, M.; Aguilar, I.; Campos, M.A.; Aguilar-Velasco, J.F.; Romero, M.; Parraga, P.; Hervas, V., et al. Acupuncture for fibromyalgia in primary care: A randomised controlled trial. Acupunct Med 2016.
• Massage Verkamp, E.K.; Flowers, S.R.; Lynch-
Jordan, A.M.; Taylor, J.; Ting, T.V.; Kashikar-Zuck, S. A survey of conventional
and complementary therapies used by youth with juvenile-onset fibromyalgia. Pain Manag Nurs 2013, 14, e244-250.
• Biofeedback Blume, H.K.; Brockman,
L.N.; Breuner, C.C. Biofeedback therapy for pediatric headache: Factors associated with response. Headache 2012, 52, 1377-1386
Integrative Pain & Symptom Management
• A Pediatrician’s Top 10 Apps for Distraction & Pain Management http://NoNeedlessPain.org
Aδ or C fiber
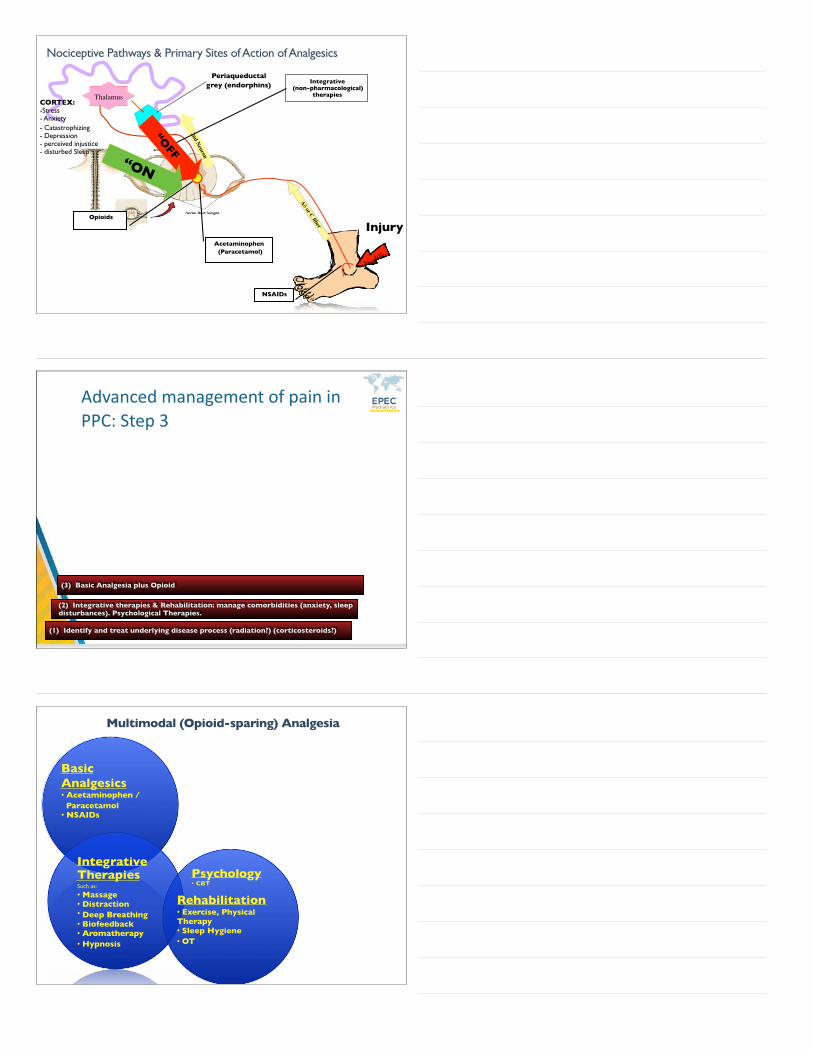
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Aδ or C fiber
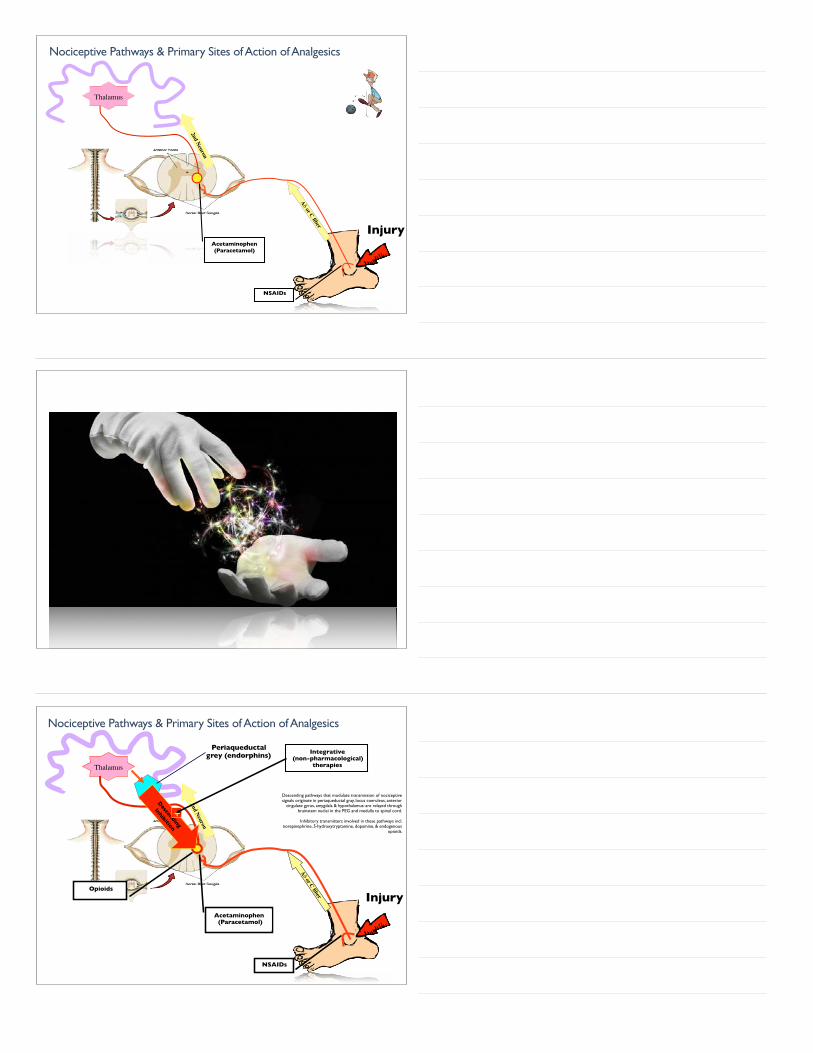
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Opioids
Periaqueductalgrey (endorphins)
Descending
Inhibition
+
Integrative (non-pharmacological)
therapies
Descending pathways that modulate transmission of nociceptive signals originate in periaqueductal gray, locus coeruleus, anterior
cingulate gyrus, amygdala & hypothalamus: are relayed through brainstem nuclei in the PEG and medulla to spinal cord.
Inhibitory transmitters involved in these pathways incl. norepinephrine, 5-hydroxytryptamine, dopamine, & endogenous
opioids.
Aδ or C fiber
Nociceptive Pathways & Primary Sites of Action of Analgesics
Injury
Thalamus
NSAIDs
Acetaminophen (Paracetamol)
2nd Neuron
Opioids
Periaqueductalgrey (endorphins)
“OFF
Integrative (non-pharmacological)
therapies
“ON
CORTEX:-Stress- Anxiety- Catastrophizing- Depression- perceived injustice- disturbed Sleep
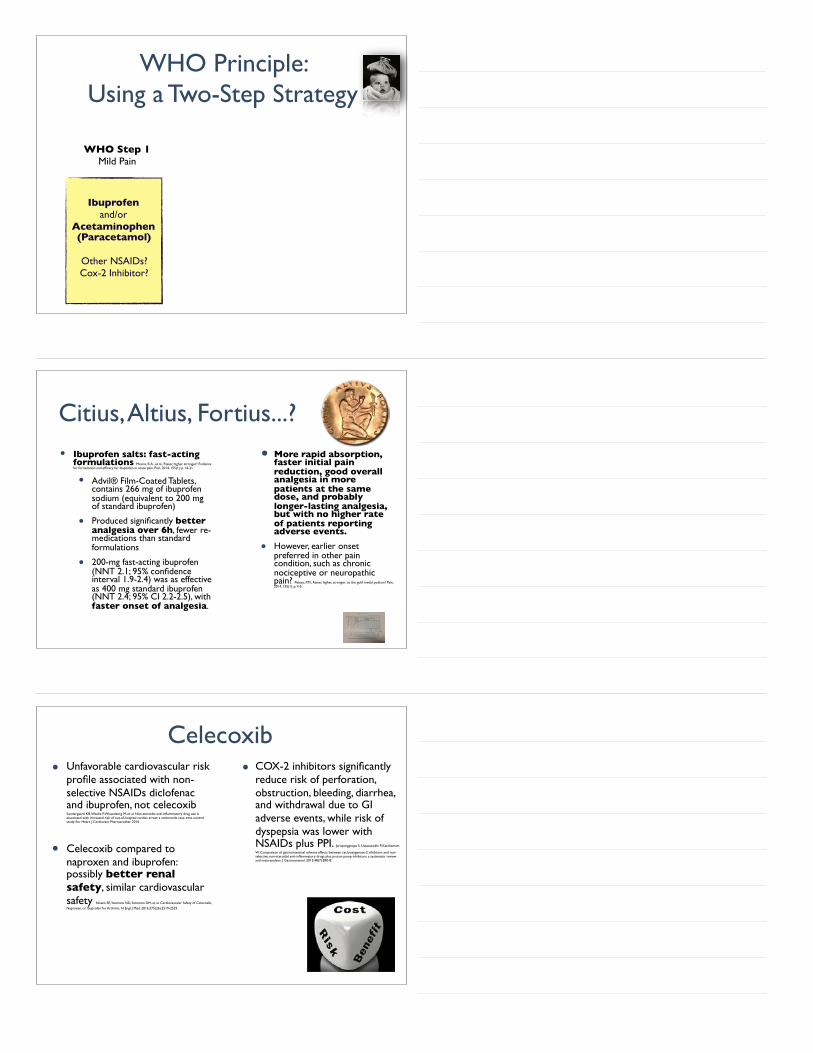
(1) Identify and treat underlying disease process (radiation?) (corticosteroids?)
AdvancedmanagementofpaininPPC:Step3
(2) Integrative therapies & Rehabilitation: manage comorbidities (anxiety, sleep disturbances). Psychological Therapies.
(3) Basic Analgesia plus Opioid
Multimodal (Opioid-sparing) Analgesia
Basic Analgesics• Acetaminophen / Paracetamol• NSAIDs
Integrative TherapiesSuch as:
• Massage• Distraction• Deep Breathing• Biofeedback• Aromatherapy• Hypnosis
Rehabilitation• Exercise, Physical Therapy• Sleep Hygiene• OT
Psychology• CBT
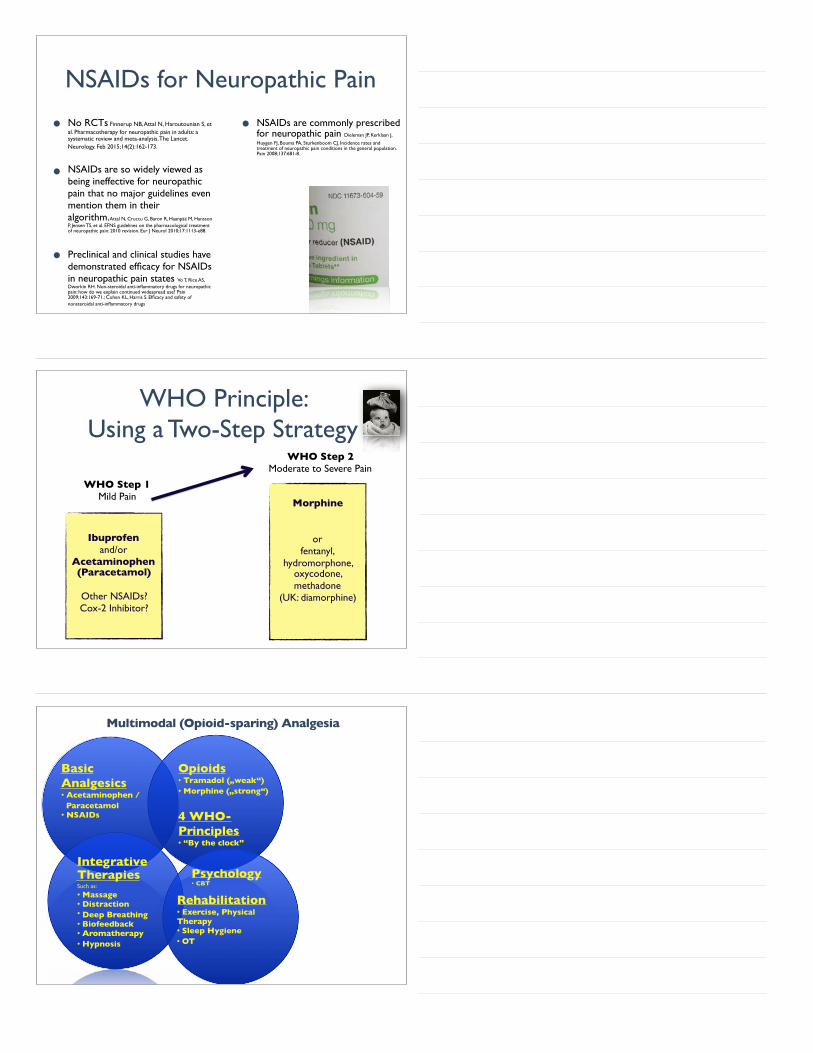
WHO Principle: Using a Two-Step Strategy
WHO Step 1Mild Pain
Ibuprofenand/or
Acetaminophen(Paracetamol)
Other NSAIDs?Cox-2 Inhibitor?
Citius, Altius, Fortius...?• Ibuprofen salts: fast-acting
formulations Moore, R.A., et al., Faster, higher, stronger? Evidence for formulation and efficacy for ibuprofen in acute pain. Pain, 2014. 155(1): p. 14-21.
• Advil® Film-Coated Tablets, contains 266 mg of ibuprofen sodium (equivalent to 200 mg of standard ibuprofen)
• Produced significantly better analgesia over 6h, fewer re-medications than standard formulations
• 200-mg fast-acting ibuprofen (NNT 2.1; 95% confidence interval 1.9-2.4) was as effective as 400 mg standard ibuprofen (NNT 2.4; 95% CI 2.2-2.5), with faster onset of analgesia.
• More rapid absorption, faster initial pain reduction, good overall analgesia in more patients at the same dose, and probably longer-lasting analgesia, but with no higher rate of patients reporting adverse events.
• However, earlier onset preferred in other pain condition, such as chronic nociceptive or neuropathic pain? Peloso, P.M., Faster, higher, stronger: to the gold medal podium? Pain, 2014. 155(1): p. 4-5.
Celecoxib• Unfavorable cardiovascular risk
profile associated with non-selective NSAIDs diclofenac and ibuprofen, not celecoxib Sondergaard KB, Weeke P, Wissenberg M, et al. Non-steroidal anti-inflammatory drug use is associated with increased risk of out-of-hospital cardiac arrest: a nationwide case-time-control study. Eur Heart J Cardiovasc Pharmacother. 2016.
• Celecoxib compared to naproxen and ibuprofen: possibly better renal safety, similar cardiovascular safety Nissen SE, Yeomans ND, Solomon DH, et al. Cardiovascular Safety of Celecoxib,
Naproxen, or Ibuprofen for Arthritis. N Engl J Med. 2016;375(26):2519-2529.
• COX-2 inhibitors significantly reduce risk of perforation, obstruction, bleeding, diarrhea, and withdrawal due to GI adverse events, while risk of dyspepsia was lower with NSAIDs plus PPI. Jarupongprapa S, Ussavasodhi P, Katchamart
W. Comparison of gastrointestinal adverse effects between cyclooxygenase-2 inhibitors and non-selective, non-steroidal anti-inflammatory drugs plus proton pump inhibitors: a systematic review and meta-analysis. J Gastroenterol. 2013;48(7):830-8.
NSAIDs for Neuropathic Pain
• No RCTs Finnerup NB, Attal N, Haroutounian S, et al. Pharmacotherapy for neuropathic pain in adults: a systematic review and meta-analysis. The Lancet. Neurology. Feb 2015;14(2):162-173.
• NSAIDs are so widely viewed as being ineffective for neuropathic pain that no major guidelines even mention them in their algorithm.Attal N, Cruccu G, Baron R, Haanpää M, Hansson P, Jensen TS, et al. EFNS guidelines on the pharmacological treatment of neuropathic pain: 2010 revision. Eur J Neurol 2010;17:1113-e88.
• Preclinical and clinical studies have demonstrated efficacy for NSAIDs in neuropathic pain states Vo T, Rice AS, Dworkin RH. Non-steroidal anti-inflammatory drugs for neuropathic pain: how do we explain continued widespread use? Pain 2009;143:169-71.; Cohen KL, Harris S. Efficacy and safety of nonsteroidal anti-inflammatory drugs
• NSAIDs are commonly prescribed for neuropathic pain Dieleman JP, Kerklaan J,
Huygen FJ, Bouma PA, Sturkenboom CJ. Incidence rates and treatment of neuropathic pain conditions in the general population. Pain 2008;137:681-8.
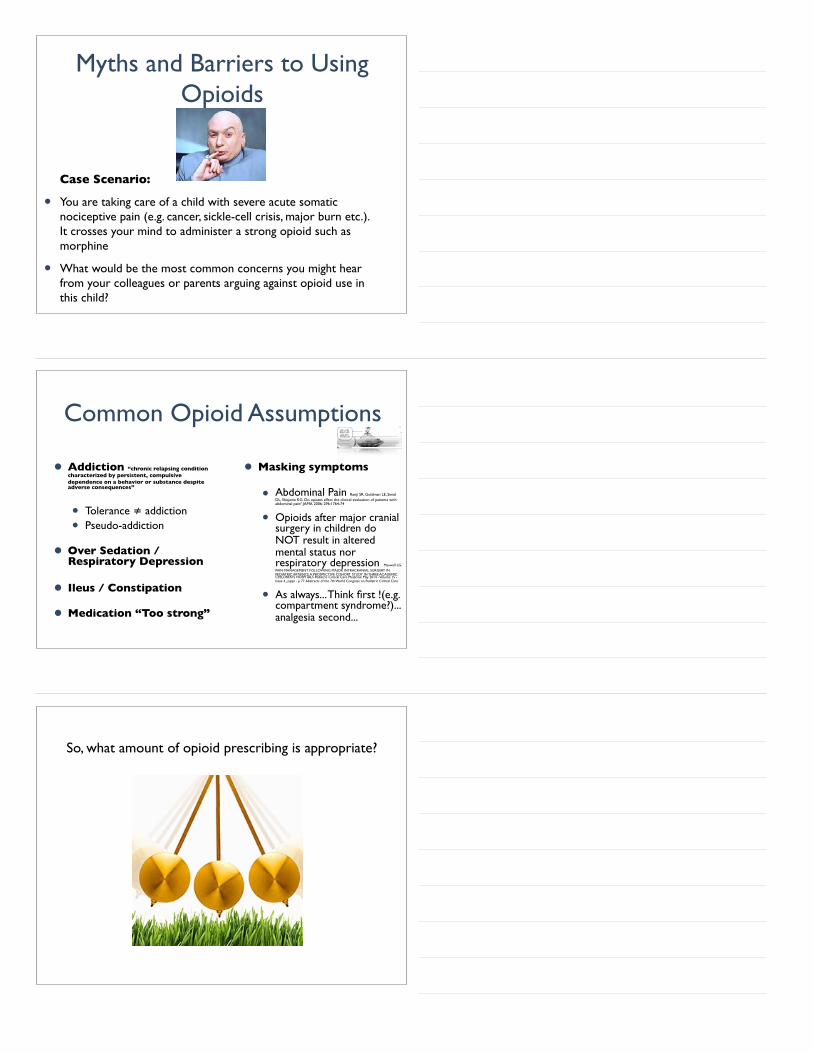
WHO Principle: Using a Two-Step Strategy
WHO Step 1Mild Pain
Ibuprofenand/or
Acetaminophen(Paracetamol)
Other NSAIDs?Cox-2 Inhibitor?
Morphine
or fentanyl,
hydromorphone, oxycodone, methadone
(UK: diamorphine)
WHO Step 2Moderate to Severe Pain
Opioids• Tramadol („weak“)• Morphine („strong“)
4 WHO-Principles• “By the clock”
Multimodal (Opioid-sparing) Analgesia
Basic Analgesics• Acetaminophen / Paracetamol• NSAIDs
Integrative TherapiesSuch as:
• Massage• Distraction• Deep Breathing• Biofeedback• Aromatherapy• Hypnosis
Rehabilitation• Exercise, Physical Therapy• Sleep Hygiene• OT
Psychology• CBT

Analgesic Response
• Patients differ in their response to opioid analgesics
• Even in well designed, successful clinical trials, as much as 40% of patients do not respond well to analgesic being studied Argoff CE, Yanni LM. Pharmacogenetics and pain. Prim Care Q 2010;1-8
• Unsurprising, patients may require trials of several opioids to find effective analgesia with acceptable tolerability
μ-Receptor Subtypes• Individuals display variety of
combinations of different mu-receptor subtypes
• Generated through “alternative splicing”, known to enhance protein diversity
• Binding profiles & resulting pharmacologic effects of opioid receptor subtypes vary among μ-opioids
• Contributing to individual variance in therapeutic response & incomplete cross-tolerance
• Review Brennan MJ. The clinical implications of cytochrome p450 interactions with opioids and strategies for pain management. Journal of Pain and Symptom Management. 2012 Dec;44(6 Suppl):S15-22.
dimer of μ receptors. Credit: Kobilka lab
Expect analgesic failure: pursue analgesic success
• Most analgesic drugs work well but in only a small percentage of people
• Pain relief not normally distributed but usually bimodal, being either very good (above 50%) or poor (below 15%)
• need to move away from focus on average response and seek out what works for each patient
Myths and Barriers to Using Opioids
Case Scenario:
• You are taking care of a child with severe acute somatic nociceptive pain (e.g. cancer, sickle-cell crisis, major burn etc.). It crosses your mind to administer a strong opioid such as morphine
• What would be the most common concerns you might hear from your colleagues or parents arguing against opioid use in this child?
Common Opioid Assumptions
• Addiction “chronic relapsing condition characterized by persistent, compulsive dependence on a behavior or substance despite adverse consequences”
• Tolerance ≠ addiction
• Pseudo-addiction
• Over Sedation / Respiratory Depression
• Ileus / Constipation
• Medication “Too strong”
• Masking symptoms
• Abdominal Pain Ranji SR, Goldman LE, Simel DL, Shojania KG. Do opiates affect the clinical evaluation of patients with abdominal pain? JAMA 2006: 296:1764-74
• Opioids after major cranial surgery in children do NOT result in altered mental status nor respiratory depression Maxwell LG.
PAIN MANAGEMENT FOLLOWING MAJOR INTRACRANIAL SURGERY IN PEDIATRIC PATIENTS: A PROSPECTIVE COHORT STUDY IN THREE ACADEMIC CHILDREN’S HOSPITALS Pediatric Critical Care Medicine: May 2014 - Volume 15 - Issue 4_suppl - p 77. Abstracts of the 7th World Congress on Pediatric Critical Care
• As always... Think first !(e.g. compartment syndrome?)... analgesia second...
So, what amount of opioid prescribing is appropriate?
Which Opioid to choose?Scrubs
Case Example “Lexi”
• 7-year-old girl in severe acute (!) pain; weight: 20 kg
• PCA pump currently not available
• Choice of opioid?
• Immediate release morphine
• ...unless...
Case Example Morphine
• Route of administration?
• Per kg dosing: Maximum 50 kg (!)
• Lean weight for obese children
• Please write the order (small group work)
Case Example Morphine (Immediate Release)
Scheduled (round-the-clock) dose
• IV: 0.1 mg x 15 kg = 2 mg Q4h (= 12 mg/day)
• PO: 0.3 mg x 15 kg = 6 mg Q4h (= 36 mg/day)
Breakthrough (rescue) dose = 1/10 - 1/6 of daily dose (Q1-2h)
• IV: (1.2 - 2 mg) 1.2 mg Q1h PRN
• PO: (3.6 - 6 mg) 3.6 mg Q1h PRN
if pain score > ...?..../10 and no signs of over sedation
Case Example Morphine
• 0300 hrs: Pain Score 10/10 -> 2 mg IV [or 6 mg PO]
• 0400 hrs: Pain Score 8/10) -> 1.2 mg IV [or 3.6 mg PO]
• 0500 hrs: Pain Score 7/10 -> 1.2 mg IV [or 3.6 mg PO]
• 0600 hrs: Pain Score 6/10 -> 1.2 mg IV [or 3.6 mg PO]
• 0700 hrs: Pain Score 5/10 .............???
• Do I need to increase the dose?
• Crystal clear answer:
Opioid Dose Escalation for Acute (!) Pain
• How to increase the dose?
Opioid Dose Escalation for Acute (!) Pain
• How to increase the dose?
• 50 per cent rule !
• ...However, depends on clinical scenario...
• 2 mg IV Q4h -> 3 mg IV Q4h
• 1.2 mg IV Q1 (-2)h PRN -> 1.8 mg IV Q1 (-2)h PRN
• or...add breakthrough dose to regular dose...? [not initial 12-24 hours]
Lexi, 3 Days Later….
• Scheduled oral immediate release morphine:
• 13 mg Q4h (= 78 mg/day)
• Breakthrough (rescue) dose for incidence pain (PT) only
• 10 mg x 3 / day
• She doesn’t like to be woken up Q4h...
• Change to extended-release morphine:
• 40 mg twice per day
• [occasionally end-of-dose failure: then Q8h]
• Continue breakthrough dose 10 mg Q1-2H PRN
Extended (Sustained) Release Opioids
• USA: Morphine, Oxycodone, Hydromorphone [oxymorphone, hydrocodone, tramadol]
• Do not cut nor crush tablets/capsules
• Do not store in liquids
• However, outside USA: Morphine extended-release “sachets” (powder) to be dissolved in liquid
Switching Opioids
Differences between opioids in the balance between analgesic cross-tolerance level and the level of cross-tolerance to adverse
effects can be exploited to clinical advantage.
Switching opioids can possibly achieve a more favorable balance between analgesia and adverse effects, hence the rationale for trial of a different opioid in the event of toxicity or inadequate
analgesia.Lawlor P (2001) Dose Ratios Among Different Opioids. In: Bruera E, Portenoy RK (ed) Topics in Palliative Care Vol 5; Oxford University Press, pp
247-76
Analgesia
Side effects Analgesia
Side effects
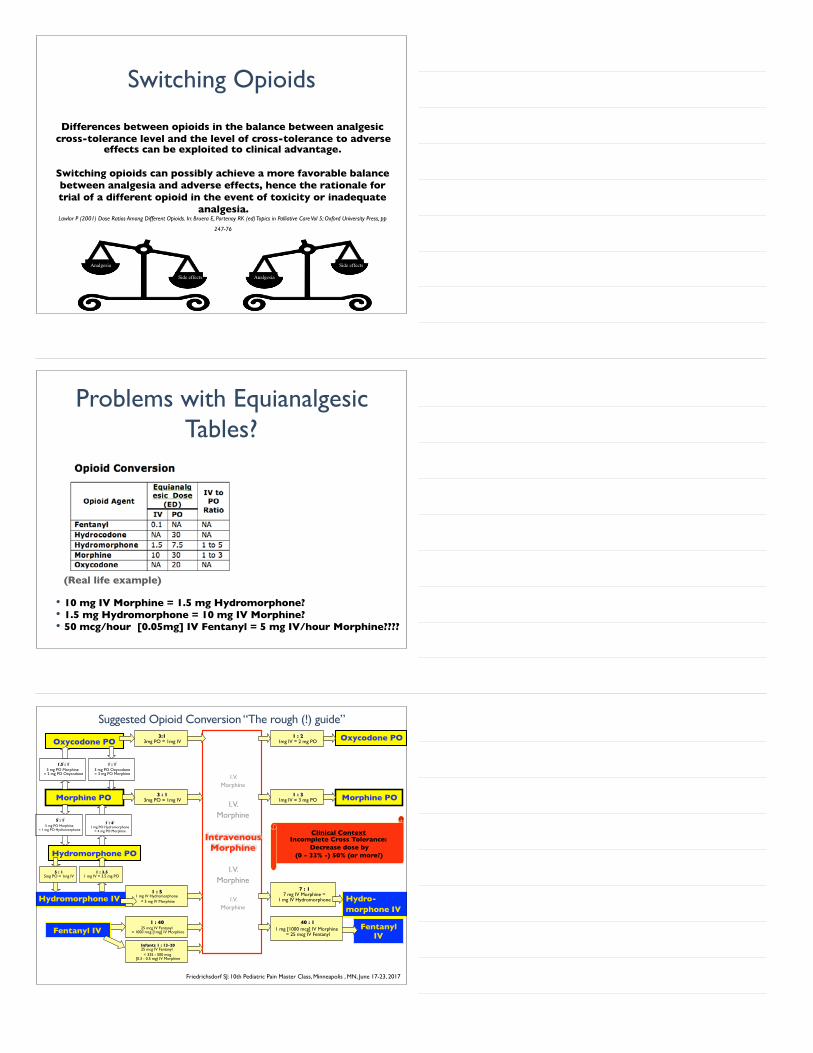
Problems with Equianalgesic Tables?
• 10 mg IV Morphine = 1.5 mg Hydromorphone?• 1.5 mg Hydromorphone = 10 mg IV Morphine?• 50 mcg/hour [0.05mg] IV Fentanyl = 5 mg IV/hour Morphine????
(Real life example)
I.V.Morphine
I.V.Morphine
IntravenousMorphine
I.V.Morphine
I.V.Morphine
Morphine PO
Oxycodone PO
Hydromorphone IV
Hydromorphone PO
Oxycodone PO
Morphine PO
Fentanyl IV
Friedrichsdorf SJ: 10th Pediatric Pain Master Class, Minneapolis , MN, June 17-23, 2017
3:13mg PO = 1mg IV
3 : 13mg PO = 1mg IV
1.5 : 13 mg PO Morphine
= 2 mg PO Oxycodone
5 : 15mg PO = 1mg IV
1 : 3.51 mg IV = 3.5 mg PO
1 : 51 mg IV Hydromorphone
= 5 mg IV Morphine
1 : 4025 mcg IV Fentanyl
= 1000 mcg [1mg] IV Morphine
Infants 1 : 13-2025 mcg IV Fentanyl
= 325 - 500 mcg[0.3 - 0.5 mg) IV Morphine
1 : 21mg IV = 2 mg PO
1 : 31mg IV = 3 mg PO
7 : 17 mg IV Morphine =
1 mg IV Hydromorphone Hydro-morphone IV
Fentanyl IV
40 : 11 mg [1000 mcg] IV Morphine
= 25 mcg IV Fentanyl
Clinical ContextIncomplete Cross Tolerance:
Decrease dose by (0 - 33% -) 50% (or more?)
1 : 13 mg PO Oxycodone= 3 mg PO Morphine
5 : 15 mg PO Morphine
= 1 mg PO Hydromorphone
1 : 41 mg PO Hydromorphone
= 4 mg PO Morphine
Suggested Opioid Conversion “The rough (!) guide”
• Starting Dose (Opioid Naïve): 0.05-0.1 mg/kg/dose [2.5 - 5 mg PO Q6-12]
Conversion Ratio:
Total Daily Oral Morphine Dose Gazelle G, Fine PG.
Methadone for the treatment of pain #75. J Palliat Med.
2003;6(4):620-1.
ROXANE LABORATORIES, INC. Columbus, OH 43216
http://www.accessdata.fda.gov/drugsatfda_docs/label/
2006/006134s028lbl.pdf
Toombs JD (2005) Americ Family Physician 71(7):1353-8
< 100 mg 3:1 20% - 30% 33 %
101mg - 300mg 5:1 10% - 20% 20 %
301mg - 600mg 10:1 8% - 12% 10 %
601mg - 800mg 12:1 5% - 10% 8 %
801mg - 1000mg 15:1 5% - 10% 7 %
> 1000mg 20:1 < 5 % 5 %
Estimated Daily Oral Methadone Requirement
Methadone Conversion- “The 30 mg Table” ... actually 60mg ... reduced by 50-75% for incomplete cross tolerance
Opioidsforneuropathicpain
• SimpleAnalgesia(NSAIDs)• Weakopioid:Tramadol– Dose:1-2mg/kgQ4-6hours,max8mg/kg/day(adult50-100mgq4-6h,max400mg/day)
– Notinchildrenwithseizuredisorder
• Strongopioids– morphine,fentanyl,hydromorphone,oxycodone,ormethadone
– (adult)NNT:4.3
Methadone as First Line Opioid
• Methadone may be effective as first-line drug in the management of cancer pain, providing analgesia and adverse effect profiles similar to those produced by other opioids Mercadante S, Bruera E. Methadone as a First-Line Opioid in Cancer Pain Management: A Systematic Review. J Pain Symptom Manage. 2018;55(3):998-1003
• doses tend to remain stable suggests that metabolic characteristics and extraopioid analgesic effects, as its well antihyperalgesic properties may be interesting potential advantages
• Starting Dose (Opioid Naïve): 0.05-0.1 mg/kg/dose [2.5 - 5 mg PO Q6-12]
HOT OFF THE
* PRESS *
Methadone • Cardiac Toxicity of Methadone:
Predictors of QTc prolongation: hypokalemia, rheumatologic disorders, use of medications with a known torsades de pointes risk, malignancy, hypocalcemia, and methadone doses >45 mg per day (Mild liver disease was protective) Juba KM, Khadem TM, Hutchinson DJ, Brown JE. Methadone and Corrected QT Prolongation in Pain and Palliative Care Patients: A Case-Control Study. J Palliat Med. 2017;20(7):722-728.
• case reports: Low-dose Methadone 0.03-0.04 mg/kg/dose BID effective to treat refractory neuropathic pain in 2 children with cancer. Madden K, Bruera E. Very-Low-Dose Methadone To Treat Refractory Neuropathic Pain in
Children with Cancer. J Palliat Med. 2017;20(11):1280-1283.
HOT OFF THE
* PRESS *
Twitter: @NoNeedlessPain
Stefan J. Friedrichsdorf, MD, FAAP Medical Director, Department of Pain Medicine, Palliative Care & Integrative Medicine
Associate Professor of Pediatrics, University of Minnesota Medical School
Children's Hospitals and Clinics of Minnesota2525 Chicago Ave S | Minneapolis, MN 55404 | USA
612.813.6450 phone | 612.813.7199 fax
[email protected]://www.childrensmn.org/painpalliativeintegrativemed
Further Training Contact: [email protected]
SAVE THE DATE:
• 12th International Symposium on Pediatric Pain (ISPP) in Basel, Switzerland, June 16-20, 2019 http://www.ispp2019.org
• Education in Palliative & End-of-life Care (EPEC) Pediatrics: Become an EPEC-Pediatrics Trainer Conference, Oct 2-4, 2019 plus optional EPEC-Pediatrics Professional Development Workshop: Oct 5, 2019
• 12th Pediatric Pain Master Class in Minneapolis, MN, June 13-19, 2020
Blog: http://NoNeedlessPain.org