-
7/27/2019 01. Drug Kidney
1/53
Obat pada ginjal
Prof M.A.Widodo PhD
THE KIDNEY IS A MAJOR ORGAN THAT DETERMINED
DRUG KINETIS AND IS A MAJOR SITE OF DRUG ACTION
RENAL FUNCTION MUST BE CONSIDERED IN THE
DEVELOPMENT OF MOST THERAPEUTIC STATEGIES
-
7/27/2019 01. Drug Kidney
2/53
Diuretics increase the rate of urine flow
and sodium excretion
used to adjust the volume and/or
composition of body fluids in a variety ofclinical situations,
including hypertension,
heart failure, renal failure, nephrotic
syndrome, and cirrhosis.
-
7/27/2019 01. Drug Kidney
3/53
-
7/27/2019 01. Drug Kidney
4/53
-
7/27/2019 01. Drug Kidney
5/53
-
7/27/2019 01. Drug Kidney
6/53
The basic urine-forming unit of the
kidney is the nephron, whichconsists of a filtering apparatus,
the
glomerulus, connected to a long
tubular portion that reabsorbs andconditions the glomerular
ultrafiltrate. Each human kidney is
composed of approximately onemillion nephrons.
-
7/27/2019 01. Drug Kidney
7/53
Glomerular Filtration. In the glomerular capillaries, a
portion
of the plasma water is forced through a filter that has
threebasic components: the fenestrated capillary endothelial cells,
a
basement membrane lying just beneath the endothelial cells,
and the filtration slit diaphragms formed by the epithelial
cells
that cover the basement membrane on its urinary space side.
Solutes of small size flow with filtered water (solvent drag)
into
the urinary (Bowman's) space, whereas formed elements and
macromolecules are retained by the filtration barrier. For
each
nephron unit, the rate of filtration [single-nephron
glomerular
filtration rate (SNGFR)] is a function of the hydrostatic
pressure in the glomerular capillaries the hydrostatic
pressure
in Bowman's space
-
7/27/2019 01. Drug Kidney
8/53
kidney is designed to filter large quantities of
plasma, reabsorb substances that the body must
conserve, and leave behind and/or secretesubstances that must be
eliminated. The two
kidneys in humans produce together
approximately 120 ml of ultrafiltrate, yet only 1
ml/min of urine is produced. Therefore, greater
than 99% of the glomerular ultrafiltrate is
reabsorbed at a staggering energy cost. The
kidneys consume 7% of total-body oxygen intakedespite the fact
that the kidneys make up only
0.5% of body weight.
-
7/27/2019 01. Drug Kidney
9/53
1, convective flow in which dissolved solutes are "dragged"by
bulk water flow; 2, simple diffusion of lipophilic solute
across membrane; 3, diffusion of solute through a pore; 4,
transport of solute by carrier protein down electrochemical
gradient; 5, transport of solute by carrier protein against
electrochemical gradient with ATP hydrolysis providing
driving force; 6 and 7, cotransport and countertransport,
respectively, of solutes, with one solute traveling uphill
against an electrochemical gradient and the other solute
traveling down an electrochemical gradient.
Seven basic mechanisms for t ransmembrane transpo r t of so
lutes.
-
7/27/2019 01. Drug Kidney
10/53
By definition, diuretics are drugs that increase the
rate of urine flow; however, clinically useful diuretics
also increase the rate of excretion of Na+(natriuresis) and of
an accompanying anion, usually
Cl-. NaCl in the body is the major determinant of
extracellular fluid volume, and most clinical
applications of diuretics are directed toward
reducing extracellular fluid volume by decreasing
total-body NaCl content.
-
7/27/2019 01. Drug Kidney
11/53
A sustained imbalance between dietary Na+ intake and Na+ loss
is
incompatible with life. A sustained positive Na+ balance would
result in
volume overload with pulmonary edema, and a sustained negative
Na+
balance would result in volume depletion and cardiovascular
collapse.
Although continued administration of a diuretic causes a
sustained net
deficit in total-body Na+, the time course of natriuresis is
finite because
renal compensatory mechanisms bring Na+ excretion in line with
Na+intake, a phenomenon known as diuretic braking. These
compensatory,
or braking, mechanisms include activation of the sympathetic
nervous
system, activation of the renin-angiotensin-aldosterone axis,
decreased
arterial blood pressure (which reduces pressure natriuresis),
hypertrophy
of renal epithelial cells, increased expression of renal
epithelialtransporters, and perhaps alterations in natriuretic
hormones such as
atrial natriuretic peptide
-
7/27/2019 01. Drug Kidney
12/53
INHIBITORS OF CARBONIC ANHYDRASE
Acetazolamide (DIAMOX) is the prototype of a class of agents
that
have limited usefulness as diuretics but have played a major
role in
the development of fundamental concepts of renal physiology
and
pharmacology
Mechanism and Site of Action. Proximal tubular epithelial
cells
are richly endowed with the zinc metalloenzyme carbonic
anhydrase, which is found in the luminal and basolateral
membranes (type IV carbonic anhydrase, an enzyme tethered to
the
membrane by a glycosylphosphatidylinositol linkage), as well as
in
the cytoplasm (type II carbonic anhydrase). Carbonic
anhydrase
plays a key role in NaHCO3 reabsorption and acid secretion.
-
7/27/2019 01. Drug Kidney
13/53
OSMOTIC DIURETICS
Osmotic diuretics are agents that are freely filtered at the
glomerulus, undergolimited reabsorption by the renal tubule, and
are relatively inert pharmacologically.
Osmotic diuretics are administered in large enough doses to
increase significantly
the osmolality of plasma and tubular fluid. gives the molecular
structures of the four
currently available osmotic diuretics glycerin (OSMOGLYN),
isosorbide
(ISMOTIC), mannitol(OSMITROL), and urea (UREAPHIL).
Mechanism and Site of Action. For many years it was thought that
osmotic
diuretics act primarily in the proximal tubule. By acting as
nonreabsorbable solutes,
it was reasoned that osmotic diuretics limit the osmosis of
water into the interstitial
space and thereby reduce luminal Na+ concentration to the point
that net Na+
reabsorption ceases. Although early micropuncture studies
supported this concept,
subsequent studies suggested that this mechanism, while
operative, may be of onlysecondary importance and that the major
site of action of osmotic diuretics is the
loop of Henle.
-
7/27/2019 01. Drug Kidney
14/53
INHIBITORS OF NA+-K+-2CL- SYMPORT (LOOP DIURETICS,
HIGH-CEILING
DIURETICS)
Drugs in this group of diuretics inhibit the activity of the
Na+-K+-2Cl- symporter in
the thick ascending limb of the loop of Henle; hence these
diuretics also are
referred to as loop diuretics. Although the proximal tubule
reabsorbs approximately
65% of the filtered Na+, diuretics acting only in the proximal
tubule have limited
efficacy because the thick ascending limb has a great
reabsorptive capacity and
reabsorbs most of the rejectate from the proximal tubule.
Diuretics actingpredominantly at sites past the thick ascending
limb also have limited efficacy
because only a small percentage of the filtered Na+ load reaches
these more distal
sites. I
In contrast, inhibitors of Na+-K+-2Cl-symport in the thick
ascending limb are highly
efficacious, and for this reason, they sometimes are called
high-ceiling diuretics.
The efficacy of inhibitors of Na+-K+-2Cl- symport in the thick
ascending limb of the
loop of Henle is due to a combination of two factors: (1)
Approximately 25% of the
filtered Na+ load normally is reabsorbed by the thick ascending
limb, and (2)
nephron segments past the thick ascending limb do not possess
the reabsorptive
capacity to rescue the flood of rejectate exiting the thick
ascending limb.
-
7/27/2019 01. Drug Kidney
15/53
Mechanism and Site of Action. Inhibitors of Na+-K+-2Cl-symport
act primarily in the thick ascending limb.
Micropuncture of the DCT demonstrates that loop diuretics
increase the delivery of solutes out of the loop of Henle.
Also,
in situ microperfusion of the loop of Henle and in
vitromicroperfusion of the CTAL indicate inhibition of transport
by
low concentrations of furosemide in the perfusate. Some
inhibitors of Na+-K+-2Cl- symport may have additional
effects
in the proximal tubule; however, the significance of these
effects is unclear
-
7/27/2019 01. Drug Kidney
16/53
INHIBITORS OF NA+-CL- SYMPORT (THIAZIDE AND THIAZIDELIKE
DIURETICS)
The benzothiadiazides were synthesized in an effort to enhance
thepotency of inhibitors of carbonic anhydrase. However, unlike
carbonic
anhydrase inhibitors, which primarily increase NaHCO3
excretion,
benzothiadiazides were found predominantly to increase NaCl
excretion,
an effect shown to be independent of carbonic anhydrase
inhibition.
Mechanism and Site of Action. Some studies using split-droplet
andstationary-microperfusion techniques have described reductions
in
proximal tubule reabsorption by thiazide diuretics; however,
free-flow
micropuncture studies have not consistently demonstrated
increased
solute delivery out of the proximal tubule following
administration of
thiazides. In contrast, micropuncture and in situ microperfusion
studies
clearly indicate that thiazide diuretics inhibit NaCl transport
in the DCT. TheDCT expresses thiazide binding sites and is accepted
as the primary site
of action of thiazide diuretics; the proximal tubule may
represent a
secondary site of action.
-
7/27/2019 01. Drug Kidney
17/53
INHIBITORS OF RENAL EPITHELIAL NA+ CHANNELS (K+-SPARING
DIURETICS)
Triamterene (DYRENIUM, MAXZIDE) and amiloride (MID-AMOR) are the
only
two drugs of this class in clinical use. Both drugs cause small
increases in NaCl
excretion and usually are employed for their antikaliuretic
actions to offset theeffects of other diuretics that increase K+
excretion. Consequently, triamterene
and amiloride, along with spironolactone (see next section),
often are classified
aspotassium (K+)-
Mechanism and Site of Action. Available data suggest that
triamterene andamiloride have similar mechanisms of action. Of the
two, amiloride has been
studied much more extensively, so its mechanism of action is
known with a
, principal cells in the late8-28Figurehigher degree of
certainty. As illustrated in
distal tubule and collecting duct have, in their luminal
membranes, epithelial
Na+ channels that provide a conductive pathway for the entry of
Na+ into the
cell down the electrochemical gradient created by the
basolateral Na+ pump
-
7/27/2019 01. Drug Kidney
18/53
ANTAGONISTS OF MINERALOCORTICOID RECEPTORS (ALDOSTERONE
ANTAGONISTS, K+-SPARING DIURETICS)
Mineralocorticoids cause retention of salt and water and
increase the excretion of
K+ and H+ by binding to specific mineralocorticoid receptors.
Early studies
indicated that some spirolactones block the effects of
mineralocorticoids; this
finding led to the synthesis of specific antagonists for the
mineralocorticoid
receptor (MR). Currently, two MR antagonists are available in
the United States,
spironolactone (a 17-spirolactone) and eplerenone; two others
are available).7-28Tableelsewhere (
Mechanism and Site of Action. Epithelial cells in the late
distal tubule and
collecting duct contain cytosolic MRs that have a high affinity
for aldosterone. This
receptor is a member of the superfamily of receptors for steroid
hormones, thyroid
). Aldosterone enters the1Chapterseehormones, vitamin D, and
retinoids (epithelial cell from the basolateral membrane and binds
to MRs; the MR-
aldosterone complex translocates to the nucleus, where it binds
to specific
sequences of DNA (hormone-responsive elements) and thereby
regulates the
expression of multiple gene products called aldosterone-induced
proteins (AIPs).
-
7/27/2019 01. Drug Kidney
19/53
-
7/27/2019 01. Drug Kidney
20/53
The Role of Diuretics in Clinical Medicine. Another implication
is that
three fundamental strategies exist for mobilizing edema fluid:
Correct
the underlying disease, restrict Na+ intake, or administer
diuretics. Themost desirable course of action would be to correct
the primary disease;
however, this often is impossible. For instance, the increased
hepatic
sinusoidal pressure in cirrhosis of the liver and the urinary
loss of
protein in nephrotic syndrome are due to structural alterations
in the
portal circulation and glomeruli, respectively, that may not
beremediable. Restriction of Na+ intake is the favored
nonpharmacologic
approach to the treatment of edema and hypertension and should
be
attempted; however, compliance is a major obstacle.
Diuretics,
therefore, remain the cornerstone for the treatment of edema or
volume
overload, particularly that owing to congestive heart failure,
ascites,
chronic renal failure, and nephrotic syndrome.
-
7/27/2019 01. Drug Kidney
21/53
Drug induced kidney disease
nephrotoxicity
-
7/27/2019 01. Drug Kidney
22/53
infeksi pada jaringan ginjal
penyakit imunologis
iskemia ginjal
batu obstruksi saluran gnjalobat bahan kimia
Penyakit sistemik
hiprertensi
diabetes
SLE
dll
Penyakit ginjal akut
Penyakit ginjal kronis
Gagal ginjal
Perubahan sruktur
Perubahan fungsi
Perubahan pada homeostais
Perubahan fungsi eskresi
Perubahan dosis obat
Anaemia
-
7/27/2019 01. Drug Kidney
23/53
Nephrotoxiity akibat obat tergantung pada
dosis
Interaksi dengan obat lain
Penyakit dan kondisi penderita
Pre-existing renal insufficiencyIncreased age
Poor nutrition
Shock
Gram-negative bacteremia
Liver disease
HypoalbuminemiaObstructive jaundice
Dehydration
Potassium or magnesium deficiencies
-
7/27/2019 01. Drug Kidney
24/53
Manifestations of DIN include acid-base abnormalities,
electrolyte
imbalances, urine sediment abnormalities, proteinuria, pyuria,
and/or
hematuria.
However, the most common manifestation of DIN is a decline
in the glomerular filtration rate (GFR), which results in a rise
inthe serum creatinine (Scr) and blood urea nitrogen (BUN).
This is consistent with the qualitative definition of acute
renal failure (ARF) or
an abrupt and sustained decrease in glomerular filtration, urine
output, or
both.
Diagnostic and therapeutic agents
Drug-induced kidney disease or nephrotoxicity (DIN)
-
7/27/2019 01. Drug Kidney
25/53
Aminoglycoside antibiotics,radiocontrast media,
nonsteroidal antiinflammatory drugs (NSAIDs),
amphotericin B, and
angiotensinconverting enzyme inhibitors (ACEIs) are frequently
implicated.
EPIDEMIOLOGY
Drug-induced nephrotoxicity occurs in all settings in which
drugs are
ingested or administered. It is a significant source of
morbidity and
mortality in the acute care hospital setting. DIN accounts for
nearly
7% of all drug toxicity and from 18% to 27% of all cases of
acuterenal failure in hospitals.
Overall, in-hospital drug use may contribute to 35% of all
cases
of acute tubular necrosis (ATN), most cases of allergic
interstitial
nephritis (AIN), as well as to nephropathy due to
alterations
in renal hemodynamics and postrenal obstruction.
-
7/27/2019 01. Drug Kidney
26/53
-
7/27/2019 01. Drug Kidney
27/53
Drug-Induced Renal
StructuralFunctional
Alterations and Examples
Tubular epithelial cell damage
Acute tubular necrosis
Aminoglycoside antibiotics
Radiographic contrast media
Cisplatin/carboplatin
Amphotericin B
Osmotic nephrosisMannitol
Dextran
Intravenous immunoglobulin
Hemodynamically-mediated
renal failureAngiotensin-converting
enzyme inhibitors
Angiotensin II receptor
antagonists
Nonsteroidal anti-inflammatory
drugs
Tubulointerstitial disease
Acute allergic interstitial nephritis
Penicillins
Ciprofloxacin
Nonsteroidal anti-inflammatory
drugs
Omeprazole
FurosemideChronic interstitial nephritis
Cyclosporine
Lithium
Aristolochic acid
Papillary necrosis
Combined phenacetin, aspirin,and caffeine analgesics
-
7/27/2019 01. Drug Kidney
28/53
Obstructive nephropathy
Intratubular obstruction
Acyclovir
SulfadiazineIndinavir
Foscarnet
Methotrexate
Extrarenal obstruction
Tricyclic antidepressants
IndinavirNephrolithiasis
Triamterene
Indinavir
Glomerular Disease
GoldNonsteroidal anti-inflammatory
drugs
Pamidronate
Renal vasculitis, thrombosis, and
cholesterol emboli
Vasculitis and thrombosis
HydralazinePropylthiouracil
Allopurinol
Penicillamine
Gemcitabine
Mitomycin C
Methamphetamines
Cholesterol emboli
Warfarin
Thrombolytic agents
Pseudo-renal failure
Corticosteroids
Trimethoprim
Cimetidine
-
7/27/2019 01. Drug Kidney
29/53
NSAIDs have an overall favorable safety profile resulting in OTC
availability in the
United States of ibuprofen, naproxen, and ketoprofen for
short-term therapy.
While potential adverse renal effects from OTC NSAIDs have been
a concern.
NSAIDs are unlikely to impair renal function in the absence of
renal ischemia or
excess renal vasoconstrictor activity. Nevertheless,given the
fact that 50 million
U.S. citizens report NSAID use, it has been estimated that
500,000 to 2.5 million
people will develop NSAID nephrotoxicity in this country
annually
ANALGESIC NEPHROPATHY
Classic analgesic nephropathy, characterized by chronic
tubulointerstitial
nephritis with papillary necrosis, was initially reported in
1953 and was
subsequently recognized as a worldwide public health concern.
Chronic
excessive consumption of combination analgesics, particularly
thosecontaining phenacetin, was believed to be the major cause and
led to the
removal of phenacetin and phenacetin mixtures from mostworld
markets.
Itwas subsequently thought, however, that abuse of
contemporary
analgesics, aspirin, acetaminophen, and NSAIDs, alone or in
combinations,
also results in analgesic nephropathy regardless of phenacetin
content
-
7/27/2019 01. Drug Kidney
30/53
EFEK SAMPING OBAT PADA FUNGSI GINJAL
HEMODINAMIK ACE INHB, NSAID, CYCLOSPORIN
GLOMERULUS
TOKSIK NSAID GOLD, PENICILINAMIN
IMUNOLOGIS SULFONAMIDE,DRUG INDUCED LUPUS
PELARUT ORGANIK
INTERSTITIALTOKSIK CYCLOSPORIN, ANALGESIK, LOGAM BERAT
IMUNOLOGIS PENICILLIN, SULFONAMIDE
COLLECTING SYSTEM SULFONAMIDE, OXYPURINOL,
TRIAMTERENE, PENINGKATAN EKSKRESI ASAM URAT
TUBULUS RENALIS BANYAKOBAT MEMPENGARUHI
HOMEOSTASIS CAIRAN DAN ELEKTROLIT Na, K Ca Mg
-
7/27/2019 01. Drug Kidney
31/53
-
7/27/2019 01. Drug Kidney
32/53
NEPHROTIC SYNDROM
-
7/27/2019 01. Drug Kidney
33/53
NEPHROTIC SYNDROME
Nephrotic syndrome is characterized by
proteinuria greater than 3.5 g/day per 1.73
m2,hypoproteinemia,
edema, and
hyperlipidemia.
A hypercoagulable state may also be present in some
patients.
Thesyndrome may be the result of primary diseases of the
glomerulus, orbe associated with systemic diseases such as diabetes
mellitus, lupus,
amyloidosis, and preeclampsia.
Hypoproteinemia, especially hypoalbuminemia, results from
increased urinary
loss of albumin and an increased rate of catabolism of filtered
albumin by
proximal tubular cells.
The compensatory increase in hepatic synthesis of albumin is
insufficient to replenish the protein loss, probably because of
malnutrition.
Mempengaruhi distribusi obat lebih banyak obat bebas.
-
7/27/2019 01. Drug Kidney
34/53
-
7/27/2019 01. Drug Kidney
35/53
The management of patients with glomerulonephritis
Specific pharmacologic therapy for the glomerular disease,
and supportif measures to prevent and/or treat the
pathophysiologic sequelae,
namely hypertension, edema, and progression of renal
disease.
In patients with nephrotic syndrome, supportive therapy should
alsoaddress the management of extrarenal complications of heavy
proteinuria,
namely hypoalbuminemia, hyperlipidemia, and thromboembolism.
Patients with significant proteinuria tend to have a more
rapid
decline of renal function. Thus reduction of proteinuria
becomes
critical in delaying the rate of progression towards end-stage
renaldisease.
Immunosuppressive agents, alone or in combination, are
commonly
used to alter the immune processes that are responsible for
the
glomerulonephritides.
Corticosteroids, in addition to their immunosuppressive effect,
also possess
anti-inflammatory activities. They reduce the production and/or
release of many
substances that mediate the inflammatory process, such as
prostaglandins,
leukotrienes,platelet-activating factors, tumor necrosis factors
(TNFs), and
interleukin-1 (IL-1)
-
7/27/2019 01. Drug Kidney
36/53
DRUG THERAPY INDIVIDUALIZATION FORPATIENTS WITH RENAL
INSUFFICIENCY
-
7/27/2019 01. Drug Kidney
37/53
Gagal ginjal
acute renal failure (hemodimik)
diuretik
chronic renal failure
pembatasan intake protein
eritropoetin
dialisapengaturan elektrolit
-
7/27/2019 01. Drug Kidney
38/53
-
7/27/2019 01. Drug Kidney
39/53
1.Chronic kidney disease can affect all aspects of drug
disposition, including
absorption, distribution, metabolism, and elimination.
2 Changes in protein binding induced by renal failure can alter
the relationship
between total drug concentration and response.
3 In addition to the expected changes in renal drug elimination,
nonrenal drug
clearance (i.e., hepatic drug metabolism) may also be decreased
in patients with
chronic kidney disease.
4 Individualization of a drug dosage regimen in a patient with
renal disease isbased on the pharmacokinetic characteristics of the
drug and the patients level of
renal function.
5 The effect of hemodialysis or chronic renal replacement
therapy on drug
elimination is dependent on the characteristics of the drug and
the dialysis
conditions.6.Acute renal failure (ARF) and chronic kidney
disease (CKD)
are often accompanied by alterations in several other organ
systems
and results in the development of anemia,
hyperparathyroidism,
bleeding abnormalities, hyperlipidemia, hypertension, and
changes
in gastrointestinal tract integrity
-
7/27/2019 01. Drug Kidney
40/53
Absorbtion : tidak ada data lengkap oleh karenaEvaluasi
bioavailability dlakukan pada pasien dengan gagal ginjal staium
5
Atau pada end-stage kidney disease (ESKD).
Penilaian bioavailability sulit oleh karena pasien menerima
berbagai macam
pengobatan dan sering drop out pada study.
Peningkatan bioavailability terjadi akibat penurunan metabolisme
obat di usus
Dan herpar seperti obat
-blockers (i.e., bufuralol,oxprenolol, propranolol, and
tolamolol),
dextropropoxyphene,
dihydrocodeine.
The volume of distribution of many drugs may be significantly
increased
or decreased in patients with renal insufficiency Alterations in
distribution
volume may result from increased or decreased protein
binding;
altered tissue binding; alterations in body composition
in addition to the expected decrease in renal drug elimination,
there is increasing
evidence that CKD also alters other elimination pathways, most
notably cytochrome
P450 (CYP450)-mediated metabolism in the liver and other
organ
-
7/27/2019 01. Drug Kidney
41/53
Gagal ginjal
Perubahan keseimbangan asam basa
Perubahan rasio obat terion dan non ion
Mempengaruhi distribusi obat dari plasma kejaringan
Salisilat pada pH asam menyebabkan leih banyak salislat non
ionYang masuk ke cns akibatnya timbul keracunan pada CNS
-
7/27/2019 01. Drug Kidney
42/53
Obat masuk tubuh
Metabolisme diusus/ hepar
Diconjugasi
Metabolit polar
Ekskresi ginjal
Ekskresi ginjal utuh
Gagal ginjal akumulasi
metabolit polar dan obat utuh
Dala tubuh
efek toksik
-
7/27/2019 01. Drug Kidney
43/53
Gagal ginjal
Penumpukan asam organik endogen
Menggantikan ikatan obat dengan protein
Penurunan ikatan protein dengan obat yang sifatnya asam
Obat bebas diplasma meningkat
Efek obat mengkat efek toksik
-
7/27/2019 01. Drug Kidney
44/53
Gagal ginjal
Penurunan fungsi
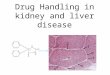
Metablisme di ginjal Tubulus proksimalis
Glukoronyl transferse
Sulfo transferaseCytochrome p 450 ksidase
Eliminasi obat berkurang
Insulin metabolisme diginjalKebutuhan insulin berkurang
-
7/27/2019 01. Drug Kidney
45/53
-
7/27/2019 01. Drug Kidney
46/53
Dose regimen
Pasien gagal ginjal
Ancaman akumulasi obat
Toksik efek
Dosis perlu disesuaikan
Terutama obat dengan terapeutik widow sempit
Dosis sama namun interval lebih jarang
(Variableinterval regimen)
Dosis dikurangi interval sama(vaiable-dose regimen)
Sebaiknya menggunakan infus apabila interval pendek
-
7/27/2019 01. Drug Kidney
47/53
-
7/27/2019 01. Drug Kidney
48/53
Erythropoietic Therapy
Pharmacology and Mechanism of Action.
Erythropoietic growth factors are required to stimulate division
and differentiationof erythroid progenitor cells and induce the
release of reticulocytes from
the bone marrow to the bloodstream where they mature into
erythrocytes
(red blood cells).
Available erythropoietic agents include epoetin alfa and
darbepoetin alfa and
Epoetin beta
These agents are glycoproteins manufactured by recombinant DNA
technology
that have the same biological activity as endogenous
erythropoietin. The amino
acid sequence of epoetin alfa is identical to the endogenous
protein; however, the
carbohydrate structure differs. Since 1989, epoetin alfa has
been the mainstay of
therapy for anemia of CKD and substantially reduced the
percentage of patientsdependent on transfusions for management of
anemia.
-
7/27/2019 01. Drug Kidney
49/53
Dosing and Administration.
Starting doses of epoetin alfa are 80to 120 units/kg per week
for SC administration and 120 to 180 units/
kg per week for IV administration divided in two to three doses
per
week (typically three times per week for hemodialysis
patients
receiving IV therapy).
If a patient is converted from IV to SC epoetin and is not at
the target
Hgb/Hct, the weekly SC dose should remain the same as the IV
dose.
The starting dose of darbepoetin alfa in patients not
previously
receiving erythropoietic therapy is 0.45 mcg/kg IV or SC
administered
once weekly.
-
7/27/2019 01. Drug Kidney
50/53
-
7/27/2019 01. Drug Kidney
51/53
TABLE 452. Advantages and Disadvantages of Peritoneal
Dialysis
Advantages
1. More hemodynamic stability (blood pressure) due to slow
ultrafiltration rate.2. Increased clearance of larger solutes,
which may explain good
clinical status in spite of lower urea clearance.
3. Better preservation of residual renal function.
4. Convenient intraperitoneal route of administration of drugs
such as
antibiotics and insulin.
5. Suitable for elderly and very young patients who may not
toleratehemodialysis well.
6. Freedom from the machine gives the patient a sense of
independence (for continuous ambulatory peritoneal
dialysis).
7. Less blood loss and iron deficiency, resulting in easier
management
of anemia or reduced requirements for erythropoietin and
parenteral
iron.
8. No systemic heparinization requirement.
9. Subcutaneous versus intravenous erythropoietin or darbepoetin
is
usual, which may reduce overall doses and be more
physiologic.
-
7/27/2019 01. Drug Kidney
52/53
Disadvantages
1. Protein and amino acid losses through peritoneum and
reducedappetite owing to continuous glucose load and sense of
abdominal
fullness predispose to malnutrition.
2. Risk of peritonitis.
3. Catheter malfunction, exit site, and tunnel infection.
4. Inadequate ultrafiltration and solute dialysis in patients
with a large
body size, unless large volumes and frequent exchanges
areemployed.
5. Patient burnout and high rate of technique failure.
6. Risk of obesity with excessive glucose absorption.
7. Mechanical problems such as hernias, dialysate leaks,
hemorrhoids,
or back pain may occur.
8. Extensive abdominal surgery may preclude peritoneal
dialysis.9. No convenient access for intravenous iron
administration.
-
7/27/2019 01. Drug Kidney
53/53
THE KIDNEY IS A MAJOR ORGAN THAT DETERMINED
DRUG KINETIS AND IS A MAJOR SITE OF DRUG ACTION
RENAL FUNCTION MUST BE CONSIDERED IN THE
DEVELOPMENT OF MOST THERAPEUTIC STATEGIES