-
8/21/2019 01 Initial Patient Assessment.pdf
1/13
KEY
POIN
TS
Open questions rather than
closed ones should be used
to encourage each patient to
provide as much information
as possible
All aspects of the subjective
and objective questioning
and examination should be
conducted with a clear idea
of how the information will
either assist in the choice
of lens or help in the future
monitoring of the contact
lens wearer
Throughout the examination,
the patent should be kept
informed of the proceduresbeing conducted and the
reasons for any decisions.
An informed patient is a
better patient
KEY POINTS
1
Public awareness of the benefits of contact
lens correction is arguably higher today than at
any time in history, thanks largely to advertising
and public relations. And significant advanc-
es in contact lens technology, materials and
design mean that more patients can comfortably
wear contact lenses. Yet despite these factors,
the number of contact lens wearers in Europe
remains significantly less than in the US, Japan
or much of the Pacific Rim. There are two main
factors keeping this penetration to the low levels.
Firstly, there is a lack of proactive recommendation
by eye care practitioners and, secondly, there
is a high incidence of contact lens drop-outs.
Correct patient selection and pre-screening is a
key element in addressing both these issues.
InitialPatient
Assessment
Essential Contact Lens Practice
-
8/21/2019 01 Initial Patient Assessment.pdf
2/13
E N V I R O N M E N T L E N S T Y P E
S O F T H A R D
Metal splinters ++ -
Burning grit particle s ++ -
Particl e contamination, moderate + -
Particl e contamination, heavy - -
Strong infra-re d radiation - ?
Underwa ter, splashes +- +-
Dry environments +- +-
Extreme cold + +
Solvents, gases, short exposure ++ ++
Solvent s, gases, long exposur e ? ?
Acids, strong, splashes ++ ++
Acids, weaker, splashes ++ ++Alkalis, strong, splashes +- ?
Alkalis, weaker, splashes +- ++
T
ABLE
1
Influence of contact lenses in different environments5
Initial Patient Assessment
2
he initial patient selection for contact lenses must bemade in
conjunction with the patient in the contextof explaining to them
that contact lenses could be a
viable vision correction option. Several studies conrm that
proactive contact lens prescribing introduces contact lens
wearto patients who previously assumed they were unsuitable.
1,2
Market research continues to show the number one concernof most
patients is the perceived discomfort/fear of having alens on the
eye. The challenge facing practitioners is to matchthese
physiological and emotional needs to products.
Although ocular topography is rarely a barrier to moderncontact
lenses, ocular anomalies, pathology and patientmotivation remain
signicant factors restricting the numberof contact lens wearers.
Many of the factors should, and can, be
screened for at the initial tting. Beyond the desire to
increasethe number of patients successfully wearing contact
lenses,the practitioner has ethical and legal obligations.
Patientsmust be oered the most suitable and safe correction for
theirneeds and practitioners must ensure their records clearly
notepre-assessment and assessmentbaseline measurements of
thecontact lens wearer. The need to communicate with the patientis
heightened with the increasing choice in materials, designsand
replacement frequencies available. The practitioner hasan ethical
obligation to inform patients of any new material,
modality or lens design that could improve their wearingsuccess.
Failure to do so could result in legal issues shouldthe patient
later have problems with their lenses. It alsoensures that
practitioners are seen to be up to date with newdevelopments.
T
++ certain protection
+ makes no differ ence+- possibly unfavourable
- unfavourabl e
? not fully studied
-
8/21/2019 01 Initial Patient Assessment.pdf
3/13
3
Essential Contact Lens Practice
Aftercare begins before the rst contact lens is even placed
onthe eye. Patient selection and pre-screening thus become partof
the aftercare process.
InstrumentationPre-screening contact lens wearers requires three
basictechniques: observation, measurement and communication.The key
instruments the slit lamp and the keratometer are discussed in
detail in other articles in this series. However, afew pertinent
points relating to pre-assessment are mentionedhere.
Ideally, the slit lamp should be tted with an eyepiecegraticule,
or at least have an adjustable slit height to assist in
recording both the size of lesions in the anterior segment
andmeasurements of horizontal visible iris diameter (HVID) andpupil
size. Measurement using the graticule is ideal as it iseasy and
accurate. The crude technique of using a hand-heldruler is not to
be recommended. Problems of parallax, vertexdistance and lack of
divisions on the millimetre scale reduceaccuracy and
reliability.
Baseline measurements and initial assessment of ocular
tissueappearance can be more accurate and repeatable by using
grading scales such as the IER (Figure 1), or Efron grading
scale.3
The increased accessibility of digital photographyshould also be
considered in taking base line measurements.Use of a photographic
slit lamp enables the practitionerto photograph any pre-existing
lesion so that this can becompared with any subsequent changes.
Consideration mustalso be given to the keratometer as more than an
instrumentsolely for measuring corneal radius. The keratometer can
beused to measure non-invasive break-up time (NIBUT) of thetear lm,
well established as a more accurate record of tearlm stability than
the use of uorescein.
TechniquesAs in refraction, it is important that a standard
routine isfollowed during the contact lens screening
examination.Developing a routine ensures a full procedure is
carried outeciently. While there are no hard and fast rules as to
theorder of a routine, it is customary to start with the
patientdiscussion before moving on to the preliminary
examination.
Patient discussion
Initial discussions with the patient are arguably the singlemost
important aspect of a preliminary examination. Acorrect
understanding of the patients working environmentand lifestyle is
important, as well as an understanding of thepatients vision
requirements and expectations.
FIGURE 1 Institute for Eye Research(IER) photographic scales
FIGURE 2Corneal desiccationsecondary to incomplete blinking
-
8/21/2019 01 Initial Patient Assessment.pdf
4/13
Initial Patient Assessment
4
With presbyopic vision correction any option will have
itslimitations, so an informal discussion about the patientsneeds
will assist in choosing the most suitable option. Forexample, the
benets of gaze independent vision oered by
simultaneous vision contact lenses may outweigh any
smallreduction in vision clarity. Establishing this before
tting
will save both practitioner and patient considerable time
andmoney. Each piece of information gathered at this stage shouldbe
collected with a purpose and should help the practitionerdecide
which contact lens is best for the patient.
Before considering individual aspects of the history
andsymptoms, it is worth underlining the importance ofquestioning
technique. Questions can be dened as openor closed. A closed
question for example, Is your general
health good? is less likely to get a comprehensive responsethan
an open question such as: Tell me about your generalhealth. The
second question invites the patient to divulgeinformation, whereas
a negative answer to the rst requiresmore probing by the
practitioner.
An even better approach would be: How would you describeyour
general health? This is important to help me decidewhich lenses are
most suitable for your eyes. This explainswhy the practitioner
needs the information and is more likelyto prompt a full
answer.
Eective communication also relies on responsive listeningand
appropriate body language on the part of the practitioner.It is
critical that the practitioner looks interested in hearing
what the patient has to say. Studies have shown that, onaverage,
it takes a patient 90 seconds to fully explain whythey are visiting
a surgeon. On average, the surgeon interruptsafter just 18.4 The
practitioner should maintain eye contact
whenever possible. Notes should be made in a deliberate
andconsidered manner, and if there is ambiguity about a pointthen
the practitioner needs to stop the patient and make surethat the
point is understood by both parties.
In a medical environment patients remember just 30 per centof
what they hear. The practitioner must make sure that allimportant
and salient points are understood by the patient.
The main areas for consideration in patient discussions areas
follows.
Occupation
In some occupations contact lens wear is not permitted, inothers
it may be contraindicated. Occupational requirementscan be found
from various organisations and the prospectivecontact lens wearer
should be made aware of any occupationalrestrictions. Contact
lenses may be contraindicated for
-
8/21/2019 01 Initial Patient Assessment.pdf
5/13
5
Essential Contact Lens Practice
patients working in dusty environments or environments inwhich
toxic fumes are present. Consideration should also begiven to
patients working long hours at computer screens.Studies have shown
the blink rate reduces during computer
use, which can lead to corneal desiccation. The increase
inair-conditioned oces is a further exacerbating element incontact
lens dryness often associated with long term computerscreen
work.
While computer use is usually not a contraindication forlens
wear, the practitioner will want to ensure this doesnot become a
problem by alerting users to the importanceof blinking. Many
patients will put up with the discomfortassociated with oce work in
the belief that there is littlethat can be done to remedy the
situation. Traditionally the
options to the practitioner were largely limited to
re-wettingdrops, but today the increase in choice of materials,
some of
which include wetting agents, means that there are multipleways
to manage contact lens dryness. Signicant dierence inpatient
comfort exist when dierent lens types are used forcomputer
activities.6
Recreational activities
The desire to wear contact lenses for playing sport may be
animportant motivation for the potential contact lens wearer.
There are certain simple points which should be taken
intoconsideration when tting a patient who wants to wear lensesfor
sport.
Soft lenses are usually the rst choice for most sports
andcontact sports in particular. However, while all contactlenses
have some protective eect on the eye, they are not asecient as
protective eyewear for some high-risk sports, suchas squash.
For water sports, the patient must be made aware of the
need for high levels of hygiene due to the potential for
theincreased risk of infection. Swimming in contact lensesmay carry
a higher risk of microbial keratitis and the risk
ofAcanthameobakeratitis is highly associated with swimming
incontact lenses. In both cases the accommodation of microbeson the
lens surface during swimming is a likely cause of theinfection.7
Patients must be warned about the increasedrisk when swimming and
should be advised, if they still
wish to swim in lenses, to wear tight tting goggles and
payparticular attention to their lens cleaning regime or
advisedaily disposable lens wear. The onus is on the practitionerto
provide the patient with the information required andall patients
should be informed that swimming pools, andjacuzzis in particular
are higher risk environments. Contactlenses have been successfully
worn for sub-aqua pursuits.8
-
8/21/2019 01 Initial Patient Assessment.pdf
6/13
TABLE
2O C C U L A R C H A N G E S V I S U A L P E R F O M A N C E
Decreased tonus of upper
and lower eyelids
Reduced palpebral aperture
Decreased lacrimal secretion
Reduced tear stability
Corneal changes
- decreased sensitivity
- increased fragility
Ocular media changes
Decreased pupil diameter
Effects of increased intake
of systemic drugs
Increased incidence of corneal
age-related disorders
The effects of ageing on the eye (adapted from Woods9,10)
Decrease in visual acuity (reduction
greater for low contrast targe ts andunder low luminance)
Reduction in contrast sensitivity
for higher spatial and temporal
frequencies
Potential reduction in stereo acuity
Increased glare sensitivity
Initial Patient Assessment
6
There is increasing evidence to suggest that UV radiationcan be
harmful to ocular tissues. UV-blocking contactlenses help provide
additional protection to the cornea,lens and retina, especially
against entry of UV light at the
temporal l imbus. However, in pursuits involving exposure tohigh
concentrations of ultraviolet light, such as skiing, thepatient
should be advised to wear wrap-around sunglasses or
goggles to oer glare protection and to prevent damage to
theconjunctiva, lid margins and surrounding skin.
Patients ageWhile there is no maximum age, or indeed minimum
age, at
which a patient can wear contact lenses, the practitioner has
toappreciate the changes that take place in the ageing eye. The
physiological changes that occur with ageing are summarised
inTable 2. The presbyopic patient will require special
management.However, the practitioner should also consider the eect
changingfrom spectacles to contact lenses would have on all contact
lens
wearers. Most myopes of more than 4.00D will notice theincreased
accommodation and convergence needed for close
work with contact lenses and should be forewarned of this.
Fitting contact lenses to children can be especially
rewarding,and most commonly considered from the age of eight
upwards.When considering tting children with contact lenses the
practitioner needs to assess the maturity and ability of
thechild to look after the lenses. This discussion needs to
takeplace with the childs parents. Patient dexterity also needs to
beconsidered, but deciencies can often be overcome by
greaterattention to the teaching of patient handling
techniques.
-
8/21/2019 01 Initial Patient Assessment.pdf
7/13
7
Essential Contact Lens Practice
Complexion
Patients with auburn hair and freckled skin have
increasedcorneal sensitivity. Blue-eyed and fair-skinned patients
alsohave relatively sensitive corneas and are more likely to
have
problems adapting to lenses, especially rigid lenses.
Motivation
Assessment of a patients needs and degree of motivation
forcontact lenses must be made. Nelson and West11 concludedfrom a
small study that stable, well-adjusted extroverted people
were more likely to adapt to contact lenses without dicultythan
anxious, introverted and less stable personalities.
Patients who are highly motivated and comply with
instructions
have an increased probability of success. Discussions should
takeplace to allow the practitioner to assess the expectations of
thepatient with regard to contact lens wear. Part of the
discussionshould also include the opportunity to discuss refractive
surgery.Many patients who have had problems with contact lenses
inthe past might register an interest in surgery without
realisinghow much contact lenses have changed. It is important that
thepatient be given a balanced and objective perspective of all
the
vision correction options that are open to them.
Unrealistic expectations need to be discussed and the
limitations of any chosen lens type and wear modalityexplained.
Patient expectations are a key factor in the successor failure of
contact lens wear.
Financial considerations
Practitioners should not pre-judge a patients ability to pay.The
main focus should be on the prospective wearers visualneeds. The
practitioner should present the most suitable lensto the patient,
but it is the patient who should make a decision
with regard to the nancial commitment.
Never assume nancial status. Patients must be made awareof the
ongoing costs of contact lens wear and care.
Smoking
Studies show that smokers are more likely than non-smokersto
develop microbial keratitis.12Patients who smoke should be
warned of this.
Ocular pathology
Contact lens tting is indicated in the management of
severalocular conditions keratoconus and monocular aphakia,
forexample. Fitting in the presence of active pathology should
neverbe undertaken without the prior approval of an
ophthalmologist.
-
8/21/2019 01 Initial Patient Assessment.pdf
8/13
TAB
LE
3
Possible effects of systemic medications and general health
status on contact lens wear
C O N D I T I O N P O T E N T I A L P R O B L E M M E D I C AT I
O N P O T E N T I A L P RO B L E M A D V I C E
Allergies Preservative reactions
Atopic reactionto deposit build-up
Antihistamines Atopic conjunctivitis
Contact lens associatedpapillary conjunctivitis
Reduced contactlens tolerance
One-day disposable
contact lenseor non-preservedsystems with frequentreplacements
lenses
Monitor check fordry eyes
Skin condition(eg eczema)
Excessive deposits
Lid irritationsBlepharitis
Punctate keratitis
One-day disposableor frequentreplacement lens
Thin edge design
Avoid contact lenswear until clear
Monitor do not fitif clinically significant
Diabetes Reduced epithelialhealing
Close monitoring
Thyroid dysfunction Tear deficiencyand poor blinking
Avoid contactlens wear
Vitamin A deficiency Mucus deficiencydeposit build up
Monitor possible softfrequent replacement
Systemichypertension
-blockers,diuretics
Dry eye Monitor
Psychosis Contact lens adaptation Psychotics Dry eye Monitor
contactlens wear possiblycontraindicated
Hormone changeseg birth control,pregnancy,menopause
Dry eyeCorneal contour changesChanges in cornealsensitivity
Oralcontraception
Dry eye Monitor
Initial Patient Assessment
8
Previous contact lens wearThe high number of contact lens
dropouts in Europe means ahigh likelihood of previous contact lens
wearers presenting tothe practitioner. In many cases these patients
will not broach the
subject of contact lens wear as they will feel that, having
failedonce, they are not suitable. It is important for the
practitionerto probe the reasons why the lens wear was discontinued
andsee if, assuming that these reasons could be overcome,
thepatient would be interested in resuming lens wear. The
mostcommon reasons for contact lens drop-out include
discomfort,dryness and poor vision. In many cases these conditions
can beaddressed with new materials, for example, silicone
hydrogel,or updated replacement frequencies, such as daily
disposables,or modern toric lens designs.13
-
8/21/2019 01 Initial Patient Assessment.pdf
9/13
9
Essential Contact Lens Practice
Dry eyes
Possibly one of the most common reasons for failure to
wearcontact lenses is dry eye. Much debate remains as to the
best
way to assess the dry eye. The use of specic questionnaires
hasreceived some validation in the literature and is recommendedas
a way of screening for potential dry-eyed patients.
TheMcMonnies14questionnaire and the Dry Eye15questionnaire
areexamples widely used in dry eye research. Key areas to
exploreare the frequency of the symptom, the presence of
discomfortand whether the patients lifestyle is aected.
Overall health and medication
As well as considering general health and the eects of
systemicmedications on overall ocular performance,
practitioners
should be aware of conditions and medications which mayhave a
direct impact on a patients ability to wear contactlenses. Table 3
outlines some of these conditions and suggestsmanagement
options.
Allergies
Approximately 25 per cent of the population suer allergies
atsome time in their life. This number varies as a function of
theclimate and will also be complicated seasonally with around
10per cent who report they suer from hay fever. It is important
for the practitioner to understand the atopic history of
thepatient as this can impact lens and care product selection.Daily
disposable lenses should be the rst choice for patients
who have ocular symptoms associated with allergies.16
Ocular history
Full consideration should be given to a patients ocularhistory
as well as to pathology, dry eye and motivation giventhe degree of
ametropia. Potential problems due to muscleimbalance should be
considered, given the lack of prismatic
eect (assisting or not) in contact lens correction. Any
previouscontact lens-wearing history should be fully explored,
andany reasons for past failures noted. Details of any
previousrefractive surgery should be investigated.
-
8/21/2019 01 Initial Patient Assessment.pdf
10/13
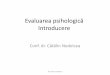
-5.00/-2.00x180 @ 10 mm
transposes to:
-5.00x90/-7.00x180 @ 10 mm
which from vertex correc tion
tables becomes:
-4.76x90/-6.54x180
and then
-4.75/-1.75x180
FOR EXAMPLE:
FIGURE
3 A method of recording the position ofthe lids with respect to
the limbus
x
y
Initial Patient Assessment
10
Patient examinationBefore examining the anterior segment, the
practitioner mustobtain a baseline refraction, perform a binocular
assessmentand undertake an ophthalmological examination of
thepatients eye. Refraction must be recorded as the
ocularrefraction, taken as the spectacle refraction with
compensationfor back vertex distance. It is important that in an
astigmaticcorrection both meridians are treated independently in
crosscylinder form (see example at left).
This becomes particularly important in the ordering of softtoric
lenses and calculation of tear lm powers in rigid gas-permeable
(RGP) lenses.
Anterior segment measurementsThe improved accuracy of
measurements with the slit-lamp graticule has already been
discussed. The followingmeasurements should be recorded.
Horizontal visible iris diameter (HVID)The horizontal visible
iris diameter underestimates thehorizontal cornea by just under
1mm. Its value lies only inensuring that a soft lens total diameter
is sucient to maintainfull corneal coverage.
Vertical palpebral apertureThe measurement of palpebral aperture
is of questionablevalue in contact lens tting other than in the
monitoring ofits size longitudinally. Of more relevance, especially
for RGPand bifocal lens tting, is the position of the lids with
respectto the limbus. This can be recorded as shown in Figure
3.
Superior x mm
Inferior y mm
Corneal coverage =
-ve, corneal exposure +ve
-
8/21/2019 01 Initial Patient Assessment.pdf
11/13
FIGUR
E
4
Preliminary contact lens examination
P A T I E N T D I S C U S S I O N
Personal details
Name, address
Age
Dexterity
Complexion
Occupation, recreation
Contact Lens specific
Expectations
Motivation
General History
Systemic disease history
Familial disorders
Motivation
Ocular history
Refraction correction past
Ocular disease history
Ocular symptoms
P A T I E N T E X A M I N A T I O N
Full eye examination
Vision
Refraction
Binocular assessment
Ophthalmoscopy
Measurements
Corneal curvature
Corneal diameter
Pupil size
Palpebral aperture
Examination of anterior
segment
Lids and lashes
Conjunctiva
Tears
Cornea
epithelium
stroma
endothelium
A S S E S S M E N T O F S U I T A B I L I T Y
11
Essential Contact Lens Practice
Pupil size
Pupil size measurement allows the practitioner to predict,and
manage, any likely are from a misalignment of the pupildiameter
with the back optic zone diameter of a rigid lens. Itis also an
important variable in predicting rigid bifocal contactlens success.
An estimation of maximum pupil diameter may bemade by viewing with
the Burton lamp in a darkened room.
Tear prism height
The height of the inferior tear meniscus gives a useful guideto
the volume of tears on the eye. The slit-lamp graticule orslit
height can be used to judge the height of the tear meniscusformed
at the margin of the lower lid. A normal value wouldbe around
0.4mm.
Keratometry
While keratometry values have no correlation to soft lenstting
performance, it is nevertheless important that theseshould be
recorded, whatever the type of lens to be tted.K-readings should be
monitored on a regular basis throughoutthe aftercare. They should
be compared to baseline values takenat the initial tting. As well
as the values, the clarity of themires must also be recorded. This
gives an indication of cornealclarity and is a sensitive monitor of
early corneal distortion.
-
8/21/2019 01 Initial Patient Assessment.pdf
12/13
TABLE
4
Variations from the norm that need to be considered in the
initial slit-lamp examination
S T R U C T U R E VA R I AT I O N F R O M T H E N O R M M A N A
G E M E N T O P T I O N S
Eyelashes Blepharitis
Stye
Resolve condition before fitting,be aware of atopic
reactions
Usually limiting wait until cleared up
Eyelid margin Meibomian gland dysfunction
Meibomian gland cyst
Treat with hot compress before fitting
Refer for removal before fitting
Palpebral conjunctiva Hyperaemia
Follicle and/or papillae
Ascertain cause prior to fitting
Depending on severity fit with RGP lens withintensive cleaning
or soft one-day disposable orfrequent replacement and nonpreserved
care system
Bulbar conjunctiva Hyperaemia
Pinguecula/pterygium
Ascertain cause prior to fitting
Ensure minimum mechanical stimulus on area
Limbus Vascularisation Record for baseline, if physiological
loops
fit as normal if neovascularisation fit higher Dk/tmaterial and
monitor closely
Cornea Staining
Opacities
Oedema
Ascertain cause prior to fitting
Ascertain cause, record for baseline information
Fit high-Dk RGP lenses or high Dk/t siliconehydrogel lenses
Initial Patient Assessment
12
Non-invasive break-up time(NIBUT)/tear thinning time (TT T)
As well as its use in measuring corneal radius and
assessingcorneal contour, keratometry may also be used to
measuretear lm stability. The technique involves recording the
timetaken for the reected mire image (the rst catoptric image)
todistort (TTT) and/or break up after a blink (NIBUT).
Tolerantcontact lens wearers average a NIBUT of around 20
seconds.
The advantages of this technique, as opposed to uorescein,
areits accuracy and repeatability. Instillation of uorescein into
theeye causes disruption of the lipid layer and, as well as
stimulatingreex tearing, decreases the stability of the tear
lm.
Anterior segment examinationThe slit-lamp examination is
probably the most importantprocedure in both preassessment and
aftercare of the contactlens wearer. It is sucient to stress here
that a full slit-lampexamination should be conducted and the
results recorded infull. Use of a grading scheme will enable the
practitioner toquantify the results and should be routinely used.
Table 4 liststhe main structures to be examined. The table also
suggestshow variations from the norm may be considered to help
thepractitioner identify the most suitable lens.
-
8/21/2019 01 Initial Patient Assessment.pdf
13/13
Essential Contact Lens Practice
R E F E R E N C E S
1. Jones L, Jones, D, Langley C andHoulford M. Reactive or
proactivecontact lens fitting does it make adifference?JBCLA, 1996;
19: 2 4143.
2. Morgan SL and Efron, NE Thebenefits of a proactive approach
tocontact lens fitting.JBCLA, 1996; 19: 397101.
3. Efron, N. (2000) Efron GradingScale for Contact Lens
Complications.Millennium Edition, January 1, 2000.Biocompatibles
Hydron
4. Panting G. Cited in Euro Times,February, 2000.
5. Nilsson SEG Contact lenses and thework environment.In: Ruben
M, Guillon M, eds. ContactLens Practice. Chapman & Hall
Medical,1994; 917-930.
6. Ruston D, Meyler J. A newsilicone hydrogel lens for
contact
lens-related dryness. Subjectiveclinical performance. Optician,
2005October 7th.
7. Choo J, Vuu K, Bergenske P BurnhamK Smythe, J, Caroline P.
Bacterialpopulations on silicone hydrogeland hydrogel contact
lenses afterswimming in a chlorinated pool. Optom& Vis Science,
2005; 82:2 134-137.
8. Josephson JE and Caffery BC Contactlens considerations in
surface andsubsurface aqueous environments.
Optom & Vis Science, 1991; 68:1 211.
9. Woods RL. The ageing eye andcontact lenses a review of
ocularcharacteristics.JBCLA, 1991; 14:3115127.
10. Woods RL. The ageing eye andcontact lenses a review of
visualperformance.JBCLA, 1992; 15:1 3143.
11. Nelson DM. and West L. Adapting tolenses: the personality of
success andfailure.JBCLA, 1987; 10:1 3637.
12. Stapleton F. Contact lensRelatedMicrobial Keratitis: What
canepidemiologic studies tell us? Eye &Contact Lens, 2003;
29(15): 585-589
13. Young G. Veys J. Pritchard N.Coleman S. A multi-centre study
oflapsed contact lens wearers. OpthalPhys Opt, 2002; 22:
516-527.
14. McMonnies CW. Key questions ina dry eye history.J Am Optom
Assoc,2006; 57:7 512517.
15. Begley Cet al. Use of the dry eyequestionnaire to measure
symptomsof ocular irritation in patients withaqueous tear deficient
dry eye. Cornea.2002; 21: 664-70
16. Hayes VY. Schnider CM. Veys J. Anevaluation of 1-day
dipsosable contactlens wear in a population of allergysufferers.
Contact Lens & Anterior Eye,2003; 28: 85-93
Patient informationOnce the decision as to the type of contact
lens has beenmade, the practitioner must take responsibility for
explainingthe reasons. The discussion should include information
onthe benets and risks of the particular wear modality andtype of
contact lens chosen, as well as advice on the likelyongoing
maintenance costs, the importance of regularaftercare, emergency
procedures and the need for patientself-monitoring. This is made
easier by the use of a patientinstruction book and acknowledgement
form.
SummaryContact lens aftercare begins with the preassessment of
theprospective wearer. By considering patient
requirements,motivation, history and symptoms, and the
physiological stateof the eye as parts of a jigsaw, the
practitioner can compile apicture of the best management option for
an individual patient.
Time spent at this stage helps avoid unnecessary failures.
Figure4 is a ow chart, showing how objective and subjective
ndingsare considered in turn to reach the nal decision.
The Vision Care Instituteis a trademark of Johnson & Johnson
Medical Ltd. Johnson & Johnson Medical Ltd. 2008
Jane VeysMSc MCOptomFBCLA FAAO, Education Director,
The Vision Care InstituteJohnson & Johnson Vision
Care,Europe, Middle East & Africa.Formerly in contact lens
research,optometric education andindependent practice.
John MeylerBSc FCOptomDipCLP Senior DirectorProfessional
Affairs, Johnson& Johnson Vision Care, Europe,Middle East &
Africa. Formerly inindependent optometric practice.
Ian DaviesBSc MCOptom DipCLP
FAAO, Vice President, TheVision Care Institute Johnson&
Johnson Vision Care, Europe,Middle East & Africa. Formerlyin
contact lens research andindependent optometric practice.
AUTHORS