Embed Size (px)
Citation preview

A r q u i v o s b r a s i l e i r o s d e
77 02publicação oficial do conselho brasileiro de oftalmologia
março/abril 2014
issn 0004-2749versão impressa
Novel refractive toric multifocal IOL
Corneal sensitivity and cross-linking
Adaptive optics of ICL and
femtosecond LAsIk
keratectasia in benign joint
hypermobility syndrome
In vivo ultrathin DsAEk with
femtosecond laser
indexada nas bases de dados
MEDLINE | EMBASE | ISI | SciELO

Frequency of publication: Bimonthly Arq Bras Oftalmol. São Paulo, v. 77, issue 2, pages 71-138, Mar./Apr. 2014
Continuous publication since 1938
Publisher: Ipsis Gráfica e Editora S.A. Divulgation: Brazilian Council of OphthalmologyCirculation: 8.600 copies
CODEN - AQBOAP
PUBLICAÇÃO OFICIAL DOCONSELHO BRASILEIRO
DE OFTALMOLOGIA
OFFICIAL PUBLICATION OF THE BRAZILIAN COUNCIL OF OPHTHALMOLOGY (CBO)
&ýĂčĈċĂúą�#Ĉúċý/účĂĈćúąAna Luísa Höfling-Lima (São Paulo-SP)André Augusto Homsi Jorge (Ribeirão Preto-SP)André Messias (Ribeirão Preto-SP)Andrea Zin (Rio de Janeiro-RJ)Antonio Augusto Velasco e Cruz (Ribeirão Preto-SP)Ayrton Roberto B. Ramos (Florianópolis-SC)Cristina Muccioli (São Paulo-SP)Denise de Freitas (São Paulo-SP)Eduardo Cunha de Souza (São Paulo-SP)Eduardo Ferrari Marback (Salvador-BA)Érika Hoyama (Londrina-PR)Fábio Ejzenbaum (São Paulo-SP)Flávio Jaime da Rocha (Uberlândia-MG)João Antonio Prata Jr. (Uberaba-MG)João Borges Fortes Filho (Porto Alegre-RS)João J. Nassaralla Jr. (Goiânia-GO)João Luiz Lobo Ferreira (Florianópolis-SC)José Beniz Neto (Goiânia-GO)José Paulo Cabral Vasconcellos (Campinas-SP)Keila Monteiro de Carvalho (Campinas-SP)Lisandro Sakata (Curitiba-PR)Luiz V. Rizzo (São Paulo-SP)Marcelo Francisco Gaal Vadas (São Paulo-SP)Marcelo Hatanaka (São Paulo-SP)
Marcelo Vieira Netto (São Paulo-SP)Marcony Santhiago (Rio de Janeiro-RJ)Maria Cristina Nishiwaki Dantas (São Paulo-SP)Maria de Lourdes V. Rodrigues (Ribeirão Preto-SP)Martha Maria Motono Chojniak (São Paulo-SP)Maurício Maia (Assis-SP)Mauro Campos (São Paulo-SP)Mauro Goldchmit (São Paulo-SP)Midori Hentona Osaki (São Paulo-SP)Milton Ruiz Alves (São Paulo-SP)Mônica Alves (Campinas-SP)Mônica Fialho Cronemberger (São Paulo-SP)Newton Kara-José Júnior (São Paulo-SP)Norma Helen Medina (São Paulo-SP)Paulo E. Correa Dantas (São Paulo-SP)Procópio Miguel dos Santos (Brasília-RJ)Ramon Ghanem (Joinvile-SC)Remo Susanna Jr. (São Paulo-SP)Roberto L. Marback (Salvador-BA)Roberto Pinto Coelho (Ribeirão Preto-SP)Rosane da Cruz Ferreira (Porto Alegre-RS)Rubens Belfort Jr. (São Paulo-SP)Sebastião Cronemberger (Belo Horizonte-MG)Sérgio Kwitko (Porto Alegre-RS)Sidney Júlio de Faria e Souza (Ribeirão Preto-SP)Silvana Artioli Schellini (Botucatu-SP)
Tiago Prata (São Paulo-SP)Vital Paulino Costa (São Paulo-SP)Walter Yukihiko Takahashi (São Paulo-SP)
*ćčþċćúčĂĈćúąAlan B. Scott (E.U.A.)Andrew Lee (E.U.A.)Baruch D. Kuppermann (E.U.A.)Bradley Straatsma (E.U.A.)Careen Lowder (E.U.A.)Cristian Luco (Chile)Emílio Dodds (Argentina)Fernando M. M. Falcão-Reis (Portugal)Fernando Prieto Díaz (Argentina)James Augsburger (E.U.A.)José Carlos Cunha Vaz (Portugal)José C. Pastor Jimeno (Espanha)Marcelo Teixeira Nicolela (Canadá)Maria Amélia Ferreira (Portugal)Maria Estela Arroyo-Illanes (México)Miguel N. Burnier Jr. (Canadá)Pilar Gomez de Liaño (Espanha)Richard L. Abbott (E.U.A.)Zélia Maria da Silva Corrêa (E.U.A.)
ISSN 0004-2749(Printed version)
ISSN 1678-2925(Electronic version)
SUBSCRIPTIONS - BRASIL: CBO Members: Free Distribuiton
Non-members: Annual Subscription: R$ 630.00 Single issue: R$ 95.00
Foreign: Annual Subscription: US$ 200.00 Single issue: US$ 40.00
Chief-editor: Wallace Chamon
Commercial Manager: Mauro Nishi
Executive Secretary: Claudete N. Moral Claudia Moral
Final Review: Paulo Mitsuru Imamura
Technical Editorship: Edna Terezinha Rother Maria Elisa Rangel Braga
Cover: Ipsis
"ýĆĂćĂČčċúčĂďþ�#ĈúċýHarley E. A. Bicas Milton Ruiz Alves Roberto Lorens Marback Rubens Belfort Jr. Wallace Chamon
$āĂþÿ�&ýĂčĈċWallace Chamon
'ĈċĆþċ�&ýĂčĈċČWaldemar Belfort MattosRubens Belfort MattosRubens Belfort Jr.Harley E. A. Bicas
"ČČĈüĂúčþ�&ýĂčĈċČAugusto Paranhos Jr. José Álvaro Pereira GomesBruno Machado Fontes Karolinne Maia RochaEduardo Melani Rocha Luiz Alberto S. Melo Jr.Eduardo Sone Soriano Mário Luiz Ribeiro MonteiroGalton Carvalho Vasconcelos Michel Eid FarahHaroldo Vieira de Moraes Jr. Norma AllemannIvan Maynart Tavares Rodrigo Pessoa Cavalcanti LiraJayter Silva de Paula Suzana Matayoshi
Cover: Retinography of a patient with angioid streaks. Photographer: Laércio da Silva Gonçalves (Department of Ophthalmology-UNIFESP).
ABO – ARQUIVOS BRASILEIROS DE OFTALMOLOGIAEditorial Office: R. Casa do Ator, 1.117 - 2nd Floor - São Paulo - SP - Brazil - 04546-004
Phone: +55 (11) 3266-4000 - Fax: +55 (11) 3171-0953 - E-mail: [email protected] - www.scielo.br/abo

OFFICIAL PUBLICATION OF THE BRAZILIAN COUNCIL OF OPHTHALMOLOGY (CBO)PUBLICAÇÃO OFICIAL DOCONSELHO BRASILEIRO
DE OFTALMOLOGIAISSN 0004-2749(Printed version)
ISSN 1678-2925(Electronic version)
Support:
www.freemedicaljournals.com
www.scielo.org
www.periodicos.capes.gov.br
(SM)
$#0�#Ĉúċý�Ĉÿ�%ĂċþüčĈċČ������������Milton Ruiz Alves (President)
Renato Ambrósio Jr. (Vice-President)
Leonardo Mariano Reis (First Secretary)
(General Secretary)
Mauro Nishi (Treasurer)
4ĈüĂþčĂþČ�"ÿÿĂąĂúčþý�čĈ�čāþ�#ċúēĂąĂúć�$ĈĎćüĂą�Ĉÿ�0ĉāčāúąĆĈąĈĀĒ�úćý�5āþĂċ�1ċþČĂýþćčČ
Centro Brasileiro de Estrabismo Marcelo Francisco Gaal Vadas
Sociedade Brasileira de Administração em Oftalmologia Flávio Rezende Dias
Sociedade Brasileira de Catarata e Implantes Intra-Oculares Armando Stefano Crema
Sociedade Brasileira de Cirurgia Plástica Ocular Guilherme Herzog
Sociedade Brasileira de Cirurgia Refrativa Renato Ambrósio Júnior
Sociedade Brasileira de Ecografia em Oftalmologia Norma Allemann
Sociedade Brasileira de Glaucoma Francisco Eduardo Lopes de Lima
Sociedade Brasileira de Laser e Cirurgia em Oftalmologia Caio Vinicius Saito Regatieri
Sociedade Brasileira de Lentes de Contato, Córnea e Refratometria Newton Kara José
Sociedade Brasileira de Oftalmologia Pediátrica João Borges Fortes Filho
Sociedade Brasileira de Oncologia em Oftalmologia Virgínia Laura Lucas
Sociedade Brasileira de Retina e Vítreo Walter Yukihiko Takahashi
Sociedade Brasileira de Trauma Ocular André Barbosa Castelo Branco
Sociedade Brasileira de Uveítes Áisa Haidar Lani
Sociedade Brasileira de Visão Subnormal Maria de Fátima Neri Góes
www.scirus.com Arquivos Brasileiros de Oftalmologia www.abonet.com.br
www.copernicusmarketing.com
Literatura Latino-americana em Ciências da Saúde

Contents
OFFICIAL PUBLICATION OF THE BRAZILIAN COUNCIL OF OPHTHALMOLOGY (CBO) ISSN 0004-2749(Printed version)
ISSN 1678-2925(Electronic version)
Frequency of publication: Bimonthly Arq Bras Oftalmol. São Paulo, v. 77, issue 2, pages 71-138, Mar./Apr. 2014
PUBLICAÇÃO OFICIAL DOCONSELHO BRASILEIRO
DE OFTALMOLOGIA
� &ýĂčĈċĂúąV Endorsement of reporting guidelines is our next step O endosso das diretrizes de publicação é o nosso próximo passo Rodrigo Pessoa Cavalcanti Lira
� 0ċĂĀĂćúą�"ċčĂüąþČ71 Visual outcomes after implantation of a novel refractive toric multifocal intraocular lens Resultado visual após implante de uma nova lente intraocular multifocal refrativa tórica Talita Shimoda, Gilberto Shimoda, Wilson Takashi Hida, Celso Takashi Nakano, Antônio Francisco Motta, Aline Silva Guimarães, Patrick Frensel M. Tzelikis
76 Artificial pupil versus contralateral balanced contact lens fit for presbyopia correction Pupila artificial vs adaptação contralateral equilibrada de lentes de contato para correção da presbiopia Santiago García-Lázaro, Teresa Ferrer-Blasco, Hema Radhakrishnan, César Albarrán-Diego, Robert Montés-Micó
81 Metallic corneal foreign bodies: an occupational health hazard Corpos estranhos metálicos na córnea: um problema de saúde ocupacional Zeynep Gursel Ozkurt, Harun Yuksel, Gunay Saka, Hande Guclu, Sina Evsen, Selahattin Balsak
84 Changes in corneal sensitivity following cross-linking for progressive early-stage keratoconus Alterações da sensibilidade corneana após cross-linking para ceratocone progressivo em estágio inicial Anelise de Medeiros Lago, Belquiz R. do Amaral Nassaralla, Larissa Rossana Souza Stival, João Jorge Nassaralla Junior
88 The influence of body position on Bielschowsky’s test A influência da posição corporal sobre o teste de Bielschowsky Carlos R. Souza-Dias, Mauro Goldchmit, Fabio P. Moraes, Arthur Jampolsky
91 Optical and nonoptical aids for reading and writing in individuals with acquired low vision Auxílios ópticos e não ópticos na leitura e escrita de pessoas com baixa visão adquirida Mayla Myrina Bianchim Monteiro, Rita de Cássia Ietto Montilha, Keila Miriam Monteiro de Carvalho, Maria Elisabete Rodrigues Freire Gasparetto
95 Vision-related quality of life in patients after ocular penetrating injuries Qualidade de vida relacionada à visão em pacientes após ferimentos oculares penetrantes Harun Yüksel, Fatih M. Türkcü, Muhammed Şahin, Yasin Çinar, Abdullah K. Cingü, Zeynep Özkurt, Yasin Bez, İhsan Çaça
99 Artificial tears alone versus 0.45% ketorolac tromethamine with artificial tears for the treatment of acute viral conjunctivitis Lágrima artificial versus cetorolaco de trometamina 0,45% associado à lagrima artificial no tratamento da conjuntivite viral aguda Adriana Falcão Veloso Lyra, Lílian Correia Bastos, Raquel Coelho de Souza Lima, Lúcio de Vieira Leite Maranhão, Tiago Eugênio Arantes
103 Implantable collamer lens and femtosecond laser for myopia: comparison using an adaptive optics visual simulator Lente implantável de collamer e laser de femtosegundo para miopia: comparação usando um simulador visual de óptica adaptativa Cari Pérez-Vives, César Albarrán-Diego, Santiago García-Lázaro, Teresa Ferrer-Blasco, Robert Montés-Micó

110 Quality of life of patients with strabismus Qualidade de vida em pacientes estrábicos Geraldo de Barros Ribeiro, Ana Gabriela Zum Bach, Camila Maia Faria, Suze Anastásia, Henderson Celestino de Almeida
� $úČþ�3þĉĈċčČ114 Congenital simple hamartoma of the retinal pigment epithelium: a case report Hamartoma congênito simples do epitéilo pigmentado da retina: relato de caso Mariana Rossi Thorell, Vinicius Ferreira Kniggendorf, Luis Augusto Arana, Alexandre Achille Grandinetti
116 Medial rectus muscle myositis as an atypical presentation of mucosa-associated lymphatic tissue lymphoma: a case report Miosite do músculo reto medial como forma atípica de apresentação de linfoma tipo MALT: relato de caso Juliana Sá Freire Medrado Dias, Mirtha Alicia Ramirez Dittrich, Jacqueline Martins de Sousa, Luiz Fernando Teixeira, Paulo Gois Manso
119 Ectasia corneana após ceratomileuse a laser in situ em um paciente com baixo risco e apresentando síndrome de hipermobilidade articular benigna Gustavo Galperin, Martin Berra, Alejandro Berra
122 In vivo ultrathin Descemet stripping automated endothelial keratoplasty with a low-energy and high-frequency femtosecond laser
In vivo Descemet stripping automated endothelial keratoplasty ultrafina com laser de femtosegundo de baixa energia e alta frequência Gustavo Victor, Walton Nosé, Sidney Júlio de Faria e Sousa, Adriana dos Santos Forseto, Milton Ruiz Alves
� 3þďĂþĐ�"ċčĂüąþČ125 Surgical management of astigmatism with toric intraocular lenses Uso de lentes intraoculares tóricas no tratamento cirúrgico de astigmatismo Bruna V. Ventura, Li Wang, Mitchell P. Weikert, Shaun B. Robinson, Douglas D. Koch1
� -þččþċČ�čĈ�čāþ�&ýĂčĈċ132 Use of the Iowa Satisfaction with Anesthesia Scale in Portuguese Franklin Dexter
132 Reply Manuela Bezerril Cipiao Fernandes
133 Plagiarism and misconduct in research Beuy Joob, Viroj Wiwanitkit
135� *ćČčċĎüčĂĈćČ�čĈ�"ĎčāĈċČ

V
&ýĂčĈċĂúą
Endorsement of reporting guidelines is our next step
O endosso das diretrizes de publicação é o nosso próximo passo
RodRigo Pessoa CavalCanti liRa1
Submitted for publication: April 25, 2014 Accepted for publication: April 25, 20141 Departamento de Oftalmologia, Universidade Federal de Pernambuco (UFPE), Recife, PE, Brazil.
Departamento de Oftalmologia, Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil.
Funding: No specific financial support was available for this study.
Disclosure: The author has any potential conflicts of interest to disclose.
Correspondence author: Rodrigo P. C. Lira. Rua Irmã Maria David, 200/1.302 - Recife (PE) - 52061-070 - Brazil
Training means learning to follow rules, experience is recognizing exceptions(1). Unfortunately the latter is provided exclusively by the time, however initiatives such as the EQUATOR (Enhancing the QUality And Trans-parency Of health Research) Network and its reporting guidelines may help with the former. The purpose of this international initiative (launched in June 2008) is to improve the value and reliability of the research literature by promoting accurate and transparent reporting(2).
Poorly designed reports lead to a waste of money in research. The lack of training and knowledge of existing tools by authors, editors and peer reviewers is the main reason(3). Moreover, the public expects that research is conducted and reported to the highest standards(4,5).
Editors noted that in the 1970-1980s many of the published studies lacked transparent methodological rigor. It was estimated that blinding was reported in only 30% of trials from major journals, primary end points were described in 27%, sample size was provided in only 43% of trials and <5% trials were truly randomized(6). Use to be a hard task to the reviewer or readers of the research identify the good from the bad.
The challenge was to provide a framework for authors to ensure they reported the essential information needed to enable critical analysis by reviewers and readers. To deal with this objective there were developed checklists of essential items to be reported for each specific study design. The most popular are the CONSORT (CONsolidated Standards Of Reporting Trials), the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology), and the PRISMA (Preferred Reporting Items of Systematic reviews and Meta-Analyses).
CONSORT, STROBE and PRISMA are now standard requirements for most major journals and are widely suppor ted by the major editorial groups. In those journals adopting these checklists, an improvement in repor-ting of the critical elements has been observed(7).
The main mechanism for dissemination and acceptance of reporting guidelines among authors and re-viewers has been its endorsement by journals. Such endorsement is usually done by a statement of support in a journal’s “Instructions for Authors”, encouraging authors to adopt a checklist when submitting their manuscript(3).
In conclusion, the reporting guidelines will not be an additional obstacle for publication. Advantages of its use for authors include the supply of a structure by which to upgrade the transparency and clarity of report writing; for reviewers and readers benefits include a method by which to critically analyze an article. From the 1st number of 2015, the Arquivos Brasileiros de Oftalmologia will endorse these guidelines and will employ them within the review process. We hope the implementation of those checklists, as a condition of submission for most of research designs by our journal, will induce an improvement in the quality of papers published.
REFERENCES 1. Wagoner K. Ao mestre com carinho, 365 reflexões sobre a arte de ensinar. São Paulo:
Publifolha; 2002. 2. The EQUATOR Network. Enhancing the QUAlity and Transparency Of Health Research
[Internet]. Oxford; Centre for Statistics in Medicina [cited 2014 Feb 20] Available from:: http://www.equator-network.org/
3. Shamseer L, Galipeau J, Turner L, Moher D. Improving the reporting and usability of research studies. Can J Anaesth. 2013;60(4):337-44.
4. Moher D. Reporting research results: a moral obligation for all researchers. Can J Anaesth. 2007;54(5):331-5.
5. Groves T. Enhancing the quality and transparency of health research. BMJ. 2008; 337:a718.
6. Altman DG, Schulz KF, Moher D, Egger M, Davidoff F, Elbourne D, et al. The revised CONSORT statement for reporting randomized trials: explanation and elaboration. Ann Intern Med. 2001;134(8):663-94. Comment in: Aust Occup Ther J. 2009; 56(1):72-3; Med Clin (Barc). 2005; 124(11):439; Ann Intern Med. 2002; 136(12):926-7; author reply 926-7.
7. Hopewell S, Dutton S, Yu LM, Chan AW, Altman DG. The quality of reports of rando-mised trials in 2000 and 2006: comparative study of articles indexed in PubMed. BMJ. 2010;340:c723. Comment in: BMJ. 2010;340:c1432.

71"SR�#SBT�0GUBMNPM���������������
0ċĂĀĂćúą�"ċčĂüąþ�
Visual outcomes after implantation of a novel refractive toric multifocal intraocular lens
Resultado visual após implante de uma nova lente intraocular multifocal refrativa tórica
talita shimoda1, gilbeRto shimoda1, Wilson takashi hida1,2, Celso takashi nakano1, antônio FRanCisCo motta1, aline silva guimaRães2, PatRiCk FRensel m. tzelikis2
Submitted for publication: August 15, 2013 Accepted for publication: December 1, 2013
Study conducted at Centro de Microcirurgia Ocular Atibaia (CEMOA), Atibaia, São Paulo, SP, Brazil.1 Ophthalmology Department, Faculdade de Medicina, Universidade de São Paulo (USP), São Paulo,
SP, Brazil.2 Brasília Ophthalmologic Hospital (HOB), Brasília, DF, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Patrick F. M. Tzelikis. SQN 203, Bloco G - Apto. 405 - Brasília (DF) - 70833-070 - Brazil - E-mail: [email protected]
ClinicalTrials.gov Identifier: NCT01505816
INTRODUCTIONThe goal of modern cataract surgery is to gain spectacle inde-
pendence for distance, intermediate, and near vision, which can be achieved with the implantation of multifocal intraocular lenses (IOLs). However, approximately 15%-29% cataract patients have more than 1.50 diopters (D) of corneal or refractive astigmatism(1-3). A residual astigmatism error of 1.50 to 3.0 D after cataract surgery may decrease uncorrected visual acuity (UCVA) to 20/70 or 20/100 and may inter-fere with spectacle independence after multifocal IOL implantation(4).
To overcome this problem, various surgical options to control astigmatism during cataract surgery are available(4,5). Patients with a considerable amount of corneal astigmatism who wish to undergo multifocal IOL implantation have several options, including a clear corneal cataract incision along the steep meridian(5), astigmatic ke-ratotomy (AK)(6,7), opposite clear corneal incisions(8), limbal relaxing
ABSTRACTPurpose: To assess the postoperative outcomes of a novel toric multifocal in-traocular lens (IOL) in patients with cataract and corneal astigmatism.Methods: This prospective nonrandomized study included patients with cata-ract, corneal astigmatism, and a motivation for spectacle independence. In all patients, a Rayner M-flex® T toric IOL was implanted in the capsular bag. Three months after surgery, the distance, intermediate, and near visual acuities; spherical equivalent; residual refractive astigmatism; defocus curve; and contrast sensitivity were evaluated. A patient satisfaction and visual phenomena questionnaire was administered to all patients. Results: Thirty-four eyes of 18 patients were included in this study. Three months after surgery, the mean corrected distance visual acuity (logMAR) was 0.00 ± 0.08 at 6 m, 0.20 ± 0.09 at 70 cm, and 0.08 ± 0.11 at 40 cm. Uncorrected distance vision acuity was 20/40 or better in 100% eyes. The preoperative mean refractive cylinder (RC) was -2.19 (SD: ± 0.53). After a 3-month follow-up, the average RC was -0.44 D (SD: ± 0.27; p<0.001). Contrast sensitivity levels were high. At the last follow-up, 87.5% patients were spectacle-independent for near, intermediate, and distance vision, and approximately 44% patients reported halos and glare. Conclusion: Toric multifocal IOL implantation in patients with cataract and cor neal astigmatism using the Rayner M-flex® T toric IOL was a simple, safe, and accurate option. This technology provides surgeons with a feasible option for meeting patient expectations of an enhanced lifestyle resulting from decreased spectacle dependence.
Keywords: Astigmatism/surgery; Lens implantation, intraocular; Lenses, intraocu-lar; Phacoemulsification; Polymethyl methacrylate; Refraction ocular; Visual acuity
RESUMOObjetivo: Avaliar o resultado pós-operatório de uma nova lente intraocular (LIO) multifocal tórica implantada em pacientes com catarata e astigmatismo corneano.Métodos: Estudo prospectivo não randomizado envolvendo pacientes com catarata, astigmatismo corneano, e motivação para eliminar a dependência dos óculos. Em todos os casos, a lente intraocular tórica Rayner M-flex® T foi implantada dentro do saco capsular. Três meses pós-operatório foram avaliados: acuidade visual para longe, intermediário e perto; equivalente esférico; astigmatismo refracional residual; curva de defocus e sensibilidade ao contraste. Ao final do estudo um questionário referente à satisfação visual foi aplicado.Resultados: Trinta e quatro olhos de 18 pacientes foram incluídos no estudo. Após 3 meses de pós-operatório, a acuidade visual corrigida para longe (logMAR) era de 0,00 ± 0,08 a 6 m, 0,20 ± 0,09 a 70 cm e 0,08 ± 0,11 a 40 cm. A acuidade visual sem correcão foi de 20/40, ou melhor, em 100% dos olhos. A média do cilindro refracional pré-operatório era de -2,19 (DP: ± 0,53). Após o seguimento de 3 meses a média do cilindro refracional era de -0,44 D (DP: ± 0,27) (p<0,001). Os níveis de sensibilidade ao contraste foram elevados. Ao final do seguimento, 87,5% dos pacientes estavam independentes dos óculos para perto, intermediário e para longe, e aproximadamente 44% dos pacientes relatavam halos e glare. Conclusão: O implante de uma lente intraocular multifocal em pacientes com catarata e astigmatismo corneano utilizando a lente intraocular tórica Rayner M-flex® T foi uma opção simples, segura e acurada. Essa nova tecnologia oferece ao cirurgião uma maneira passível de se atingir as expectativas dos pacientes em relação a qualidade de vida em razão de uma menor dependência dos óculos.
Descritores: Astigmatismo/cirurgia; Implante de lente intraocular; Lentes intraocu-lares; Facoemulsificação; Polimetil metacrilato; Refração ocular; Acuidade visual
incisions(9), and, of late, toric multifocal IOL implantation to decrease astigmatism after cataract surgery(10).
Toric multifocal IOLs offer the opportunity to correct astigmatism and achieve spectacle independence at all distances in patients with corneal astigmatism with only one procedure. This study assessed the visual function after cataract surgery and implantation of a toric multifocal IOL (Rayner M-flex® T toric) in a small single-site series of 34 eyes in 18 patients.
METHODSThis prospective study included patients with age-related cata-
ract, corneal astigmatism of at least 1.00 D (measured by keratome-try), normal findings in ophthalmological examination besides senile cataract, an unsatisfactory correction with glasses, and a motivation

7ĂČĎúą�ĈĎčüĈĆþČ�úÿčþċ�ĂĆĉąúćčúčĂĈć�Ĉÿ�ú�ćĈďþą�ċþÿċúüčĂďþ�čĈċĂü�ĆĎąčĂÿĈüúą�ĂćčċúĈüĎąúċ�ąþćČ
72 "SR�#SBT�0GUBMNPM���������������
for spectacle independence. Written informed consent was obtained from all patients before surgery, and the study was approved by the local ethics committee. All the procedures were in accordance with the ethical standards of the responsible committee on human expe-rimentation and the Helsinki Declaration of 1975. Exclusion criteria were previous ocular surgery and irregular corneal astigmatism.
Before surgery, patients underwent extensive ophthalmological examination, including the measurement of uncorrected distance visual acuity (UDVA), corrected distance visual acuity (CDVA), re-fraction, slit-lamp examination, fundoscopy, corneal topography (EyeSys unit, version 3.03; EyeSys Technologies, Houston, Texas), and biometry with the IOLMaster partial coherence interferometry device (Carl Zeiss Meditec AG, Jena, Germany). The targeted postoperative refractive error was the closest to 0.0 D.
IOLAll patients received a Rayner M-flex® toric IOL (model 638F M-flex®
T, Rayner IOLs, Ltd., UK). This multifocal aspheric IOL is made of hydrophilic acrylate. It is a multizoned, refractive, aspheric IOL with either 4 or 5 annular zones (depending on IOL base power). The optic diameter is 6.25 mm and the overall diameter is 12.5 mm. Available spherical powers range from +14.0 D to +32.0 D in 0.50-D increments and include a near addition (add) of +3.00 D. Cylinder powers range from +1.00 to +6.00 D in 0.50-D increments. The IOL power was cal-culated using an online calculator.
SURGICAL TECHNIQUE All patients were operated upon by the same surgeon using
iden tical procedures. Before surgery, corneal reference marks were placed at 0° and 180° using a toric reference marker, with the patient sitting upright to correct for cyclotorsion. Next, the desired alignment axis for the toric IOL was intraoperatively marked with an angular graduation instrument. Phacoemulsification was performed using the Infinite (Alcon Surgical) Vision system. All IOLs were inserted in the capsular bag with the injector system. The toric IOL was implan-ted and rotated until the IOL markings agreed with the alignment marking. Postoperative follow-up was at 1 day and 1 and 3 months after surgery.
OUTCOME MEASURES
Postoperative evaluation was performed at 3 months. UDVA and CDVA were assessed using the 100% contrast Early Treatment Diabe-tic Retinopathy Study chart. Uncorrected intermediate visual acuity (UIVA) for intermediate vision was assessed at 70 cm, and the un-corrected near visual acuity (UNVA) for near vision was assessed at 40 cm (Near reading chart, Presby Corp.). A binocular defocus curve was constructed using the Early Treatment of Diabetic Retinopathy Study (ETDRS) chart at 4 m. The cylinder axis of the IOL was measured at the slit lamp using the beam protractor after full mydriasis. The mean of the absolute IOL degrees that were off-axis was determined.
Contrast sensitivity was measured using the CSV-1000 HGT ins-trument (VectorVision, Inc. Greenville, OH, USA), which presents a translucent chart divided into 4 cycles with spatial frequencies of 3, 6, 12, and 18 cycles per degree (cpd). All measurements were obtained under mesopic (5 cd/m2) and photopic (85 cd/m2) conditions. Exami-nations were unilaterally performed at a distance of 2.5 m, with the corrected visual acuity (BCVA) and an undilated pupil.
Patient satisfaction and quality of life were assessed by a simple questionnaire. All patients were interviewed 3 months after surgery. Patients were asked about visual disturbances, visual lifestyle activi-ties, spectacle use, and procedural satisfaction.
All data analyses were performed using SPSSX statistical programs (SPSS Inc, Chicago, IL, USA). The normality of all data samples was first checked using the Kolmogorov-Smirnov test. When parametric analysis was possible, Student’s t-test for paired data was used for all parameter comparisons between pre- and postoperative examina-tions. When parametric analysis was not possible, the Wilcoxon rank-sum
test was applied. Any differences showing a p-value of <0.05 (i.e., at the 5% level) were considered statistically significant.
RESULTSThe study enrolled 18 patients (34 eyes). Sixteen patients had
bilateral Rayner M-flex® T toric multifocal IOL implantation; the other 2 received a Rayner M-flex® multifocal IOL because they had mild astigmatism (<1.0 D). Three patients were men (16.7%) and 15 were women (83.3%), with a mean age of 69.44 years (range, 52-86 years; SD, ±8.9). All patients had mild cataract at presentation. The mean sphe-rical power of the implanted toric multifocal IOLs was +20.32 ± 3.1 D (range, 14.00-25.00 D). The mean preoperative axial length (AL) was 23.22 ± 0.8 mm (range, 21.39-26.19 mm). All patients were followed-up for 3 months.
VISUAL ACUITY AND REFRACTION
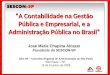
Table 1 shows the distance, intermediate, and near visual acuities. The postoperative UDVA was 20/40 (0.3 logMAR) or better in 34 eyes (100%), 20/30 (0.18 logMAR) or better in 31 eyes (91.2%), and 20/25 (0.10 logMAR) or better in 30 eyes (88.2%), while CDVA was 20/40 or better in 34 eyes (100%) and 20/25 or better in 32 eyes (94.1%). Figure 1 shows the binocular defocus curve with 2 peaks of optimum CDVA at 0.00 D and -2.75 D.
Table 1. Mean preoperative and postoperative visual acuity and refraction (logMAR)
Mean ± SDPreop Postop p-value
UDVA 0.51 ± 0.33 0.03 ± 0.09 <0.001
CDVA 0.13 ± 0.13 0.00 ± 0.08 <0.001
UIVA - 0.22 ± 0.09 -
DCIVA - 0.20 ± 0.09 -
UNVA - 0.10 ± 0.13 -
DCNVA - 0.08 ± 0.11 -
SE (D) -0.24 ± 1.59 0.11 ± 0.40 0.21
Refractive cylinder (D)
Mean -2.19 ± 0.53 -0.44 ± 0.27 <0.001
Range -1.25 to -3.25 0.00 to -1.00
UDVA= uncorrected distance visual acuity, CDVA= corrected distance visual acuity, UIVA= uncorrected intermediate visual acuity, DCIVA= distance-corrected intermediate visual acuity, UNVA= uncorrected near visual acuity, DCNVA= distance-corrected near visual acuity, SE= spherical equivalent.
Figure 1. Defocus curve (mean binocular CDVA as a function of diopters of defocus).CDVA= corrected distance visual acuity.

4āĂĆĈýú�5 �þč�úą�
73"SR�#SBT�0GUBMNPM���������������
The average SE of these eyes was -0.24 D (range, -2.75 – +3.00 D; SD, ±1.59) at referral and 0.11 (range, -1.00 – +1.25 D; SD, ±0.40; p=0.21) at 3 months after surgery. The average refractive cylinder of these eyes was -2.19 D (range, -1.25 – -3.25 D; SD, ±0.53) at referral and -0.44 D (range, 0.00 – -1.00 D; SD, ±0.27; p<0.001) at 3 months. Almost 95% eyes had a postoperative residual refractive astigmatism of -0.75 D or less.
Corneal topography values at presentation were recorded for all eyes. The average flatter corneal meridian topography was 43.21 D (range, 40.40-45.96 D; SD, ±1.20), and the average steeper corneal meridian topography was 45.57 D (range, 42.74-47.74 D; SD, ±1.27). The average topographic astigmatism was 2.29 D (range, 1.36-3.19 D; SD, ±0.52), which increased to 43.25 D (range, 40.32-45.93 D; SD, ±1.25) at 3 months after surgery. The average steeper corneal me-ridian topography was 45.51 D (range, 42.64-47.74 D; SD, ±1.26), and the average topographic astigmatism was 2.16 D (range, 1.38-3.16 D; SD, ±0.54; p>0.05).
MISALIGNMENT
Three months after surgery, the mean error in IOL alignment was 2.34 ± 2.33° (range, 0-9°). The mean error in IOL alignment was more than 5° in 5 eyes (17.6%). No IOL was misaligned by 10° or more.
CONTRAST SENSITIVITY
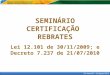
Figure 2 shows the mean log monocular contrast sensitivity va lues under photopic and mesopic conditions at 3 months after surgery. The mean contrast sensitivity levels in photopic and mesopic conditions were 1.60 ± 0.11 and 1.39 ± 0.16, respectively, at 3 cpd, 1.69 ± 0.12 and 1.44 ± 0.21, respectively, at 6 cpd, 1.12 ± 0.36 and 0.93 ± 0.41, respectively, at 12 cpd, and 0.57 ± 0.42 and 0.37 ± 0.41, respectively, at 18 cpd.
PATIENT SATISFACTION AND SPECTACLE DEPENDENCY
All 16 patients with bilateral Rayner M-flex® T toric IOLs completed the questionnaire. Table 2 shows patient-reported spectacle depen-dence; satisfaction with distance, intermediate, and near vision; and the incidence of halos and glare. Three months after cataract surgery, no eye required a second procedure. At the last follow up, 14 patients (87.5%) were spectacle-independent for near, intermediate, and distance vision and were very satisfied with their quality of vision without glasses. Good distance and near vision were reported by all patients.
DISCUSSIONClinical trials evaluating the clinical, optical, functional, and
quality-of-life outcomes after implantation of these new-generation IOLs found that the participants had improved near vision and
good distance vision(10-13). Although patients with these IOLs report less limitation in visual function and less spectacle dependency compa red with patients with monofocal IOLs(14), some have reported dis sa tis faction with the outcomes that are mostly related to visual aberrations such as halos, glare, and dysphotopsia(15).
After cataract surgery, even a relatively low amount of uncorrected astigmatism can significantly decrease visual acuity in eyes with mul tifocal IOLs, which will further decrease the ability to perform low-contrast tasks(16,17). However, today’s cataract patients are more demanding, and they usually seek total visual rehabilitation and total independence from spectacles. These requirements have been the motivating factor in the development of toric multifocal IOLs. These IOLs were designed to compensate for corneal astigmatism and the loss of accommodative ability after cataract extraction.
In the current study, we evaluated visual and refractive outcomes, contrast sensitivity, and patient satisfaction after Rayner M-flex toric multifocal IOL implantation. At present, there are only 4 types of toric multifocal IOL models available: diffractive ReSTOR IQ toric IOL (Alcon Laboratories, Inc.), diffractive AT Lisa toric IOL (Carl Zeiss Meditec AG), Lentis Mplus toric IOL (Oculentis GmbH), and refractive M-flex T IOL (Rayner Intraocular Lens Ltd.)(18). So far, to our knowledge, no study of the Rayner M-flex T IOL has been published.
Nontoric Rayner multifocal IOL implantation has been evaluated in a few studies(19). This IOL has the same platform as the Rayner M-flex T IOL. Cezón Prieto and Bautista(19) studied the Rayner M-flex 630F +3.00 D IOL and found a mean monocular CDVA of 0.03 logMAR (ap-proximately 20/20) 12 months after surgery; 100% eyes had a CDVA of 0.30 logMAR (20/40) or better, while 100% eyes had a CDVA of 0.00 logMAR (20/20) or better. The toric Rayner monofocal IOL has also been evaluated in a few studies(20). In a study of the Rayner T-flex 623T toric IOL, some authors(20) found a mean CDVA of 0.19 logMAR (approximately 20/30) 4 months after surgery; 96.6% eyes had a CDVA of 0.30 logMAR (20/40) or better, 81.8% eyes had a CDVA of 0.18 logMAR (20/30) or better, and 21.1% eyes had a CDVA of 0.00 logMAR (20/20) or better. Our study found a good CDVA (mean 0.00 logMAR), with all patients having a CDVA of 20/25 or better at 3 months. There are few published studies describing refractive Figure 2. Mean log contrast sensitivity values at 3 months.
Table 2. Subjective symptoms and spectacle-dependence 3 months after surgery
Parameter Mean score ± SD
Satisfaction with distance vision (from 0 to 10) 9.28 ± 1.37
Satisfaction with intermediate vision (from 0 to 10) 8.97 ± 2.41
Satisfaction with near vision (from 0 to 10) 8.44 ± 2.06
Spectacle dependence (number of patients) Number of patients (%)
Never 16 (88.9%)
Sometimes 02 (11.1%)
Always 00 (00.0%)
Halos Number of patients (%)
None 10 (55.6%)
Mild 05 (27.7%)
Moderate 03 (16.7%)
Severe 00 (00.0%)
Glare Number of patients (%)
None 10 (55.6%)
Mild 04 (22.2%)
Moderate 03 (16.7%)
Severe 01 (05.5%)
Overall satisfaction, range from 0 (least satisfied) to 10 (most satisfied).

7ĂČĎúą�ĈĎčüĈĆþČ�úÿčþċ�ĂĆĉąúćčúčĂĈć�Ĉÿ�ú�ćĈďþą�ċþÿċúüčĂďþ�čĈċĂü�ĆĎąčĂÿĈüúą�ĂćčċúĈüĎąúċ�ąþćČ
�� "SR�#SBT�0GUBMNPM���������������
outcomes after toric multifocal IOL implantation(10,13,21). Other au-thors(10,13) reported a binocular logMAR CDVA of -0.06 and 0.05 after 3 months of follow-up using the AT Lisa toric multifocal IOL.
Uncorrected outcomes were also good, with 90% patients achie ving a UDVA of 20/25 or better in our study. Cezón Prieto and Bautista(19) found a mean UDVA of 0.09 logMAR (approximately 20/25) 12 months after surgery using the Rayner M-flex 630F IOL, with 100% eyes achieving a UDVA of 0.30 logMAR (20/40) or better and 75% eyes achieving a UDVA of 0.00 logMAR (20/20) or better. Similar results were reported by Viesser et al.(10) using the AT Lisa toric multifocal IOL with a mean monocular logMAR UDVA of 0.04 3 months after surgery; 98% eyes had a UDVA of 0.30 logMAR (20/40) or better and 71% eyes had a UDVA of 0.10 logMAR (20/25) or better.
Recently, there has been a trend toward decreasing the power of the near add (from +4.00 D to +3.00 D) in some models of multifocal IOLs to improve intermediate vision or expand reading distance(19,21-23). At 3 months, the mean monocular UIVA and distance-corrected inter-mediate visual acuity (DCIVA) in our study were 0.22 logMAR and 0.20 logMAR, respectively. These findings are slightly better than those of Viesser et al.(10), who reported a 3-month monocular intermediate vision (at 60 cm) with toric multifocal IOL of 0.40 logMAR with and without correction. For intermediate distances, different models of multifocal IOL with a +3.00-D add power have shown similar results. Alfonso et al.(22), in a study of the AcrySof ReSTOR SN6AD1, found mean binocular UIVA and DCIVA logMAR values of 0.165 and 0.147 at 70 cm after 6 months of follow-up. Muñoz et al.(23) studied the Lentis Mplus LS-312 multifocal IOL and found a logMAR UIVA and DCIVA of 0.13 and 0.14 at 1 m 6 months after surgery. Cezón Prieto and Bautista(19) reported a mean UIVA and DCIVA value of 0.15 logMAR in eyes with Rayner M-flex IOL. This was consistent with our finding that the majority of patients did not use spectacles for intermediate vision because of the excellent visual acuity between 50 and 70 cm.
In our study, the Rayner M-flex T IOL with +3.00 D add provided high performance for near vision; the mean monocular UNVA was 0.10 logMAR and the mean DCNVA was 0.08 logMAR at 3 months. The near vision achieved with the Rayner M-flex T IOL was comparable to that with other multifocal IOLs(10,12,13,22,23). In the study by Viesser et al.(10), the mean UNVA was 0.20 logMAR. In another study of toric mul-tifocal IOL by Alió et al.(13) the mean postoperative UNVA and CDNVA was 0.24 and 0.24 logMAR, respectively, at 3 months. Cezón Prieto and Bautista(19) reported a UNVA value of 0.28 logMAR in eyes implan-ted with Rayner M-flex IOL. Similar results (binocular logMAR DCNVA, approximately 0.10) were reported by Fujimoto et al.(24), who used the multifocal refractive Array SA40N IOL (Abbott Medical Optics, Inc.) and by Alió et al.(25), who used the multifocal refracti ve-diffractive Acri.LISA 366D (Carl Zeiss Meditec AG) and the AcrySof ReSTOR SN6AD3 (Alcon Laboratories, Inc.).
The defocus curve for the Rayner M-flex T IOL was consistent with the above findings, with a V-shaped curve with 2 peaks of ma-ximum vision, 1 at distance (around a 0.00-D defocus level) and 1 at near (approximately -2.75 D defocus level). Between these 2 peaks, acceptable vision was maintained, resulting in acceptable interme-diate vision. IOL performance for distance was similar to that with a monofocal IOL, with a logMAR acuity of approximately 0.00. The IOL provided a logMAR intermediate acuity of approximately 0.20-0.30 between 50 cm and 70 cm and had the best logMAR near vision between 33 cm and 40 cm. When considering the defocus curve for other multifocal IOLs, the range of focus for functional vision exten-ded approximately from +1.0 D to -3.5 for +3.0-D IOL(10,22).
According to slit-lamp examination, the mean misalignment of Rayner M-flex T IOL was 2.34 ± 2.33°, with no IOL off-axis by more than 10° at 3 months. We found the Rayner M-flex T IOL to be stable once positioned in the capsular bag. The amount of rotation of different toric IOL models is reported to be between 0° and 20°(26). The FDA trial of the AcrySof SA60T toric IOL compared 244 patients with a control group of 250 patients who received the nontoric AcrySof SA60AT
IOL. The former exhibited excellent rotation stability, with a mean rotation of less than 4° from the initial alignment at 12 months after surgery. Rotation misalignment was 10° or less in 97% patients and 5° or less in 81% patients. Zuberbuhler et al.(27) subsequently repor-ted a large series of AcrySof SN60T toric IOLs in 44 eyes. The mean toric IOL axis rotation was 2.2 ± 2.2°, and 95%IOL were within 5° of the targeted axis. The current study of the rotational stability of the Rayner M-flex T toric IOL showed nearly identical results; the mean rotation was less than 4°, with 100% IOL showing a rotation of 10° or less. Our results were comparable with those in studies of the AcrySof toric IOL. Intraoperative positioning of toric IOLs with grea-ter accuracy was necessary to achieve the most optimum cylinder correction in all patients(21,26,27).
The Rayner M-flex T is a refractive toric multifocal IOL with a mul-tizone design that can cause loss of contrast sensitivity because of the distribution of total available light between several focal points. Patients with multifocal IOLs may therefore be more sensitive to changes in contrast and have been reported to have lower contrast sensitivity compared with the normal population(28). Several stu-dies(22,23,25,28) have reported lower photopic contrast sensitivity with a multifocal IOL than with a monofocal IOL; however, the contrast sen-sitivity was still in the normal range. The results in our study confir med these results. We obtained contrast sensitivity values under mesopic and photopic conditions that were similar to those obtained by Cezón Prieto and Bautista(19), Montés-Micó et al.(28), and de Vries et al.(29). In a normal population, contrast sensitivity levels measured with the CSV-1000 system were 1.56 ± 0.15 at 3 cpd, 1.80 ± 0.16 at 6 cpd, 1.50 ± 0.15 at 12 cpd, and 0.93 ± 0.25 at 18 cpd(30). This indicated that the contrast sensitivity after Rayner M-flex T implantation was compa-rable with that in the normal population at 2 spatial frequencies (3 and 6 cpd) and decreased at high spatial frequencies (12 and 18 cpd) under photopic and mesopic conditions.
CONCLUSIONSThe results of our study showed that implantation of the Rayner
M-flex T IOL effectively decreased visually significant keratometric astigmatism and spectacle-dependence after cataract surgery, with acceptable low rates of IOL misalignment. Further studies on the effi-cacy of this toric multifocal IOL in cataract surgery are recommended with larger sample sizes and longer follow-ups.
REFERENCES 1. Hoffmann PC, Hütz W. Analysis of biometry and prevalence data for corneal astigmatism
in 23239 eyes. J Cataract Refract Surg. 2010;36(9):1479-85. Comment in: J Cataract Refract Surg. 2010;36(9):1447-8; J Cataract Refract Surg. 2011;37(3):621; author reply 621.
2. Hoffer KJ. Biometry of 7,500 cataractous eyes. Am J Ophthalmol. 1980;90(3):360-8. 3. Grabow HB. Intraocular correction of refractive errors. In: Kershner RM, editor. Refracti-
ve keratotomy for cataract surgery and the correction of astigmatism. New Jersey: Slack Thorofare; 1994. p.79-115.
4. Frohn A, Dick HB, Thiel HJ. Implantation of a toric poly(methylmethacrylate) intrao-cular lens to correct high astigmatism. J Cataract Refract Surg. 1999;25(12):1675-8.
5. Koch D, Lindstrom RL. Controlling astigmatism in cataract surgery. Sem Ophthalmol. 1992;7:224-33.
6. Shepherd JR. Correction of preexisting astigmatism at the time of small incision cataract surgery. J Cataract Refract Surg. 1989;15(1):55-7.
7. Osher RH. Paired transverse relaxing keratotomy: a combined technique for reducing astigmatism. J Cataract Refract Surg. 1989;15(1):32-7.
8. Lever J, Dahan E. Opposite clear corneal incisions to correct pre-existing astigmatism in cataract surgery. J Cataract Refract Surg. 2000;26(6):803-5. Comment in: J Cataract Refract Surg. 2000;26(6):789-90; J Cataract Refract Surg. 2001;27(1):7-8; J Cataract Refract Surg. 2000;26(12):1697-8.
9. Müller-Jensen K, Fisher P, Slepe U. Limbal relaxing incision to correct astigmatism in clear corneal cataract surgery. J Refract Surg. 1999;15(5):586-9.
10. Viesser N, Nuijts RM, de Vries NE, Bauer NJ. Visual outcomes and patient satisfaction after cataract surgery with toric multifocal intraocular lens implantation. J Cataract Refract Surg. 2011;37(11):2034-42.
11. Chang DF. Prospective functional and clinical comparison of bilateral ReZoom and ReSTOR intraocular lenses in patients 70 years or younger. J Cataract Refract Surg. 2008;34(6):934-41.

4āĂĆĈýú�5 �þč�úą�
��"SR�#SBT�0GUBMNPM���������������
VII Congresso Baiano de Oftalmologia
10 e 11 de outubro de 2014Hotel Sheraton
Salvador - BA
Informações: Site: www.sofba.com..br
12. Pepose JS, Qazi MA, Davies J, Doane JF, Loden JC, Sivalingham V, et al. Visual perfor-mance of patients with bilateral vs combination Crystalens, ReZoom, and ReSTOR in traocular lens implants. Am J Ophthalmol. 2007;144(3):347-57. Comment in: Am J Ophthalmol. 2008;145(4):593-4.
13. Alió JL, Piñero DP, Tomás J, Plaza AB. Vector analysis of astigmatism changes after ca-taract surgery with implantation of a new toric multifocal intraocular lens. J Cataract Refract Surg. 2011;37(7):1217-29.
14. Souza CE, Mucciolli C, Soriano ES, Chalita MR, Oliveira F, Freitas LL, et al. Visual perfor-mance of AcrySof ReSTOR apodized diffractive IOL: a prospective comparative trial. Am J Ophthalmol. 2006;141(5):827-32.
15. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992-7.
16. Hayashi K, Manabe S, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with diffractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8): 1323-9.
17. Wolffsohn JS, Bhogal G, Shah S. Effect of uncorrected astigmatism on vision. J Cata-ract Refract Surg. 2011;37(3):454-60.
18. Lane SS, Morris M, Nordan L, Packer M, Tarantino N, Wallace RB 3rd. Multifocal intra-ocular lenses. Ophthalmol Clin North Am. 2006;19(1):89-105.
19. Cezón Prieto J, Bautista MJ. Visual outcomes after implantation of a refractive multi-focal intraocular lens +3.00 D addition. J Cataract Refract Surg. 2010;36(9):1508-16.
20. Entabi M, Harman F, Lee N, Bloom PA. Injectable 1-piece hydrophilic acrylic toric intraocular lens for cataract surgery: efficacy and stability. J Cataract Refract Surg. 2011;37(2):235-40.
21. Liekfeld A, Torun N, Friederici L. [A new toric diffractive multifocal lens for refractive surgery]. Ophthalmologe. 2010;107(3):256;258-61. German.
22. Alfonso JF, Fernández-Vega L, Amhaz H, Montés-Mico R, Valcárcel B, Ferrer-Blasco T. Visual function after implantation of an aspheric bifocal intraocular lens. J Cataract Refract Surg. 2009;35(5):885-92.
23. Muñoz G, Albarrán-Diego C, Ferrer-Blasco T, Sakla HF, García-Lázaro S. Visual function after bilateral implantation of a new zonal refractive aspheric multifocal intraocular lens. J Cataract Refract Surg. 2011;37(11):2043-52.
24. Fujimoto K, Honda K, Wada YR, Tanaka M, Irie T. Four-year experience with a silicone refractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8):1330-5.
25. Alió JL, Plaza-Puche AB, Piñero DP, Amparo F, Rodríguez-Pratas JL, Ayala MJ. Quality of life evaluation after implantation of 2 multifocal intraocular lens models and a monofocal model. J Cataract Refract Surg. 2011;37(4):638-48.
26. Viestenz A, Seitz B, Langenbucher A. Evaluating the eye’s rotational stability during standard photography: effect on determining the axial orientation of toric intraocular lenses. J Cataract Refract Surg. 2005;31(3):557-61.
27. Zuberbuhler B, Signer T, Gale R, Haeflinger E. Rotational stability of the AcrySof SA60TT toric intraocular lenses: a cohort study. BMC Ophthalmology. 2008;8:8.
28. Montés-Micó R, España E, Bueno I, Charman WN, Menezo JL. Visual performance with multifocal intraocular lenses; mesopic contrast sensitivity under distance and near conditions. Ophthalmology. 2004;111:85-96.
29. de Vries NE, Webers CAB, Montés-Micó R, Ferrer-Blasco T, Nuijts RM. Visual outcomes after cataract surgery with implantation of a +3.00 D or +4.00 D aspheric diffractive multifocal intraocular lens. Comparative study. J Cataract Refract Surg. 2010;36(8): 1316-22.
30. Pomerance GN, Evans DW. Test-retest reliability of the CSV-1000 contrast test and its relationship to glaucoma therapy. Invest Ophthalmol Vis Sci. 1994;35(9):3357-61.

76 "SR�#SBT�0GUBMNPM����������������
0ċĂĀĂćúą�"ċčĂüąþ�
Artificial pupil versus contralateral balanced contact lens fit for presbyopia correction
������ȱ����ę����ȱ��ȱ������³¨�ȱ�������������ȱ�����������ȱ��ȱ������ȱ��ȱ�������ȱ����ȱ�����³¨�ȱ��ȱ����������
santiago gaRCía-lázaRo1, teResa FeRReR-blasCo1, hema RadhakRishnan2, CésaR albaRRán-diego3, RobeRt montés-miCó1
Submitted for publication: May 20, 2013 Accepted for publication: October 23, 2013
Study conducted at University of Valencia, Spain.1 Optics Department, University of Valencia, Spain.2 University of Manchester, Manchester, United Kingdom.3 Optics Department, Faculty of Physics, University of Valencia, Spain.
Funding: This research was supported in part by a Ministerio de Ciencia e Innovación Research Grant to Robert Montés-Micó (#SAF2009-13342-E#).
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Santiago García-Lázaro. Optics Department, Faculty of Physics. Univer sity of Valencia - C/ Dr. Moliner, 50. 46100. Burjassot (Valencia). SPAIN
E-mail: [email protected]
INTRODUCTIONPresbyopia is the natural decrease in accommodative ability
caused by loss of elasticity of the lens of the eye. It occurs normally with aging and is first observed between 40 and 45 years of age, with a peak onset between 42 and 44 years of age(1,2). Without optical cor-rection, presbyopia results in the inability to perform once-effortless tasks at a customary working distance without experiencing visual symptoms(3)..
A possible solution to presbyopia is wearing contact lenses. Among the different options for correcting the refractive error with contact lenses in presbyopic patients, simultaneous vision is the preferred choice for most contact lens wearers(4,5). In simultaneous vision, the contact lens has multiple powers positioned within the pupil at the same time: a multiconcentric surface with different rings for distance and near vision, a near-center aspheric geometry, and a distance-center aspheric geometry. It is possible to combine a near-center and distance-center aspheric geometry contact lens in the same patient to emphasize the distance vision in one eye and
ABSTRACTPurpose: To assess and compare the effects of contact lens-based artificial pupil design and contralateral balanced multifocal contact lens combination (CBMCLC) on visual performance.Methods: This randomized crossover study conducted at the University of Valen-cia, Spain included 38 presbyopic patients using an artificial pupil contact lens in the nondominant eye and a CBMCLC. After a month of lens wear, the binocular distance visual acuity (BDVA), binocular near visual acuity (BNVA), defocus curve, binocular distance, and near contrast sensitivity and near stereoacuity (NSA) were measured under photopic conditions (85 cd/m2). Moreover, BDVA and binocular distance contrast sensitivity were examined under mesopic conditions (5 cd/m2). Results: Visual acuity at an intermediate distance and near vision was better with the CBMCLC than with the artificial pupil (p<0.05). Statistically significant differences were found in contrast sensitivity between the two types of correction for distance (under mesopic conditions) and for near vision, with the CBMCLC exhibiting better results in both cases (p<0.05). The mean NSA values obtained for the artificial pupil contact lens were significantly worse than those for the CBMCLC (p=0.001). Conclusion: The CBMCLC provided greater visual performance in terms of inter-mediate and near vision compared with the artificial pupil contact lens.
Keywords: Contact lenses; Presbyopia/rehabilitation; Pupil; Prosthesis fitting do -minance, ocular
RESUMOObjetivo: Avaliar e comparar os efeitos da pupila artificial baseada em lentes de contato e a combinação equilibrada de lente de contato multifocal contralateral (CBMCLC) sobre o desempenho visual. Métodos: Estudo realizado na Universidade de Valência, Espanha. Em um projeto de estudo do tipo “cross-over”, 38 pacientes présbitas foram avaliados utilizando uma lente de contato com pupila artificial no olho não-dominante e CBMCLC. Após 1 mês, foram avaliadas, em condições fotópicas (85 cd/m2), a acuidade visual binocular para distância (BDVA), a acuidade visual binocular para perto (BNVA), a curva de desfoca-gem, a sensibilidade ao contraste binocular para distância e para perto, assim como a acuidade estereoscópica para perto (NSA). Além disso, a BDVA e a sensibilidade ao contraste binocular para distância foram avaliadas em condições mesópicas (5 cd/m2). Resultados: A acuidade visual em distâncias intermediárias e para perto foram melhores com CBMCLC do que com pupila artificial (p<0,05). Foram encontradas diferenças estatisticamente significativas entre a sensibilidade ao contraste com os dois tipos de correção para distância (em condições mesópicas) e para perto, com CBMCLC ser melhor em ambos os casos (p<0,05). Os valores médios da NSA obtidos com as lentes de contato das pupilas artificiais foram significativamente piores do que com CBMCLC (p=0,001). Conclusão: CBMCLC proporciona melhor desempenho visual para visão intermediária e para perto do que a lente de contato com pupila artificial.
Descritores: Lentes de contato; Presbiopia/reabilitação; Pupila; Ajuste de prótese; Dominância ocular
near vision in the other. This technique, which combines multifocal optics with monovision, is known as the contralateral balanced mul-tifocal contact lens combination (CBMCLC).
In a recent research study, García-Lázaro et al.(6) compared 4 diffe-rent designs of artificial pupil contact lenses that were fitted in the nondominant eye. This study reported good visual acuity for distance and functional intermediate vision, with no significant differences between the aperture diameters examined (from 1.6 to 3.5 mm). However, it would be interesting to compare the possible benefits of the artificial pupil on visual acuity and depth-of-field for presbyopia correction with those of other techniques such as CBMCLC.
This study aimed to assess and compare the visual performance of patients fitted with the artificial pupil contact lens and CBMCLC by evaluating the binocular visual acuity, defocus curve, binocular con-trast sensitivity, and near stereoacuity (NSA) measurements obtained under different illumination levels for both distance and near vision. To the best of our knowledge, this is the first study to compare the vi-sual performance of a contact lens-based artificial pupil and CBMCLC.

(úċüIJú�-ĦēúċĈ�4 �þč�úą�
77"SR�#SBT�0GUBMNPM����������������
METHODSThis study was conducted in accordance with the tenets of the
Declaration of Helsinki. Informed consent was obtained from all patients after the nature and possible consequences of the study had been explained. This study was approved by the institutional review board.
PATIENTS AND LENSES
Thirty-eight presbyopic patients (25 females and 13 males) aged 48-62 years (54.2 ± 5.1 years) participated in this randomized crosso-ver study. Inclusion criteria were as follows: age between 45 and 65 years, emmetropia [cycloplegic spherical equivalent (SE), ±0.25 D; astigmatism, ≤0.50 D], monocular best spectacle-corrected distance visual acuity ≥20/20, and normal binocularity. Exclusion criteria were as follows: subjects with photopic (85 cd/m2) distance pupil size ≥4.00 mm, anterior segment pathology, previous intraocular or cor-neal surgery, cataracts, corneal abnormalities (including endothelial dystrophy, guttata, or recurrent corneal erosion), and a history of chronic dry eye, macular degeneration, retinal detachment, and/or any other fundus pathology.
Patients were randomized to be fitted with the artificial pupil or Biofinity multifocal (CooperVision, Fairport, NY) contact lenses for the first month. After a month of wear, patients returned to be refitted with the other lenses. The afocal artificial pupil contact lens was manufactured from a silicone hydrogel material with two base curve radii (8.40 and 8.80 mm) and a 14.00-mm lens diameter. The lens design included a 1.6-mm central aperture in a 4-mm diameter opa-que zone (see Figure 1). The artificial pupil systems were developed to provide functional near and intermediate vision by increasing the depth-of-field in the eye. Depth-of-field is defined as the distance in front of and beyond the object of regard that appears to be in focus. The depth-of-focus of the eye may be increased by decreasing the pupil diameter. In these patients, the dominant eye was not fitted with any contact lenses, while the nondominant eye was fitted with the artificial pupil.
The Biofinity multifocal lens is a simultaneous multifocal contact lens. This design combines spherical and aspheric optics and unique zone sizes to produce a “D” lens (center-distance design), which em-phasizes distance vision, and an “N” lens (center-near design), which optimizes near vision. The “D” lens has a spherical central zone that is 2.3 mm in diameter and is dedicated to distance vision, followed by an annular aspheric zone of 5.0 mm and a spherical annular zone of 8.5 mm, with both increasing the add power. In contrast, the “N” lens has a spherical central zone that is 1.7 mm and is dedicated to
near vision, followed by an aspheric annular zone of 5.0 mm and an annular spheric zone of 8.5 mm, with both decreasing the add power. Each “D” and “N” design is available from +6.00 to -6.00 D in 0.25-D increments and from -6.00 to -8.00 D in 0.50-D increments, as well as in 4 different add powers (+1.00, +1.50, +2.00, +2.50). The lens is manufactured from Comfilcon A that has a water content of 48%. The lens has a total diameter of 14.00 mm and a base curve of 8.60 mm. Following the fitting nomogram suggested by CooperVision for initial lens selection, we used the “D” design in the dominant eye and the “N” design in the nondominant eye for all patients included in this study.
MEASUREMENTS
The near add power and eye dominance were determined following the clinical protocol from the study by García-Lázaro et al.(7). The do-minant eye was identified using the “plus acceptance to blur” and confirmed with the Ogle’s eye dominancy test. When the two tests yielded conflicting results, a subjective approach was followed, and the lenses were fitted according to the conditions under which the subject reported the most comfortable vision. The near add power was selected on the basis of near spectacle addition [minimum spectacle addition to reach logMAR 0.0 at 40 cm (distance preferred by patients for reading)] and subject age (the amplitude of accom-modation changes with age are predictable)(8-10).
After completion of a month of wear, the subjects returned for the assessment of visual function. The latter involved clinical assessment of visual function; the binocular distance visual acuity (BDVA), bino-cular near visual acuity (BNVA), defocus curve, binocular distance con trast sensitivity, binocular near contrast sensitivity, and NSA were all measured in each patient under photopic conditions (85 cd/m2). Moreover, BDVA and binocular distance contrast sensitivity were also examined under mesopic conditions (5 cd/m2).
BDVA was measured using the Early Treatment Diabetic Retino-pathy Study (ETDRS) high-contrast logMAR chart with the Functional Vision Analyzer (FVA, Stereo Optical Company, Inc., Chicago, IL). BNVA was determined using the Precision Vision Logarithmic Visual Acuity Chart 2000 New ETDRS at 40 cm. The through focus binocular logMAR visual acuity (defocus curve; range, -5.00 -+1.50 D in 0.50-D increments), with randomized letter sequences and randomized lens presentations to decrease the effect of memory(11), was also evaluated with the ETDRS high-contrast logMAR chart. NSA was determined using the Howard-Dolman system(12-14). For the calculation of NSA values, the interpupillary distance (IPD) was measured for near vision using the Pupill´on pupillometer (Essilor Co., Ltd., France).
All near measurements were made at a distance of 40 cm. All described procedures were then repeated for the second lens type.
DATA ANALYSIS
The normality of data distribution was assessed by the Shapiro-Wilk test. The null hypothesis that data came from a normally distributed population was not rejected; therefore, parametric tests were applied. Data analysis was performed using the SPSS Statistics software v.12.0 (SPSS, Chicago, IL). Paired sample t-tests were applied to test for differences between both types of correction and each of the different illumination levels. Differences were considered to be statistically signi ficant when the p-value was <0.05.
RESULTSThe mean SE refractive error was +0.04 ± 0.10 D (range, +0.25
to -0.25 D), while the mean near spectacle addition was +2.26 ± 0.36 D (range, 2 to 3 D). The difference between the values obtained by minimum spectacle addition to reach logMAR 0.0 at 40 cm and those reported by the guidelines for presbyopia(8-10) were ≤0.25 D in all patients. The pupil size was measured using the Colvard pupillo-meter (Oasis Medical, Inc., Glendora, CA). The mean pupil diameter Figure 1. Design of the artificial pupil fitted.

"ċčĂÿĂüĂúą�ĉĎĉĂą�ďþċČĎČ�üĈćčċúąúčþċúą�ûúąúćüþý�üĈćčúüč�ąþćČ�ÿĂč�ÿĈċ�ĉċþČûĒĈĉĂú�üĈċċþüčĂĈć
�� "SR�#SBT�0GUBMNPM����������������
was 3.55 ± 0.23 mm and 4.36 ± 0.21 mm under photopic (85 cd/m2) and mesopic conditions (5 cd/m2), respectively, for distance vision, and 3.07 ± 0.25 mm and 4.02 ± 0.18 mm under photopic (85 cd/m2) and mesopic conditions (5 cd/m2), respectively, for near vision. The near IPD at distance showed a mean value of 62.9 ± 2.9 mm, with a range of 58-66 mm.
All results comparing visual acuity with the artificial pupil contact lens to that with CBMCLC are summarized in table 1. Figures 2 and 3 represent the binocular distance contrast sensitivity values obtained with both types of correction under photopic and mesopic binocu-lar conditions, respectively. Statistically significant differences were not found between the two techniques at any spatial frequency for distance under photopic conditions (p>0.05); however, binocular dis tance contrast sensitivity revealed better performance for CBMCLC than for the artificial pupil under mesopic conditions (p<0.05) [statis-tically significant differences for 6 cycles per degree (cpd), 12 cpd and 18 cpd]. Figure 4 displays the contrast sensitivity values obtained for binocular near vision under photopic conditions. CBMCLC showed significantly better contrast sensitivity values for this distance. Statis-tically significant differences were found between the two types of correction for contrast sensitivity for near vision at all spatial frequen-cies tested (p<0.05), except for 1.5 cpd (p=0.48).
Figure 5 shows the mean binocular visual acuity measurements as a function of defocus for the artificial pupil contact lens and CBMCLC. The defocus curve showed a peak of optimum distance vision, 0.00 ± 0.05 and -0.03 ± 0.07 logMAR, for the artificial pupil contact lens and CBMCLC, respectively, at the vergence of 0 D. Statistical analysis sho-
wed no significant differences between both systems at this ver gence (p=0.08). When negative lenses were introduced from a vergence of 0 D, a continuous deterioration was observed with both techniques at all steps. The defocus curve showed that CBMCLC was significantly better than the artificial pupil contact lens for intermediate and near distance vision. Significant differences between both corrections of presbyopia for intermediate distance vision (lens power, from -1.00 D to -2.00 D, corresponding to optical distances between 50 cm and 100 cm; p<0.05) and near vision (lens power, -2.50 D; p<0.05). In all patients, when statistically significant differences were found for the negative values of defocus, the mean visual acuities values were better with CBMCLC.
The average NSA values were significantly better with CBMCLC than with the artificial pupil contact lens (235 ± 28 and 147 ± 41 sec arc, respectively; p<0.01).
DISCUSSIONIn this study, we evaluated two possible solutions for presbyo-
pia through contact lenses. These two techniques were based on different monocular optical principles to achieve focus at different distances (aspheric design for CBMCLC and increasing the depth of focus for artificial pupil contact lens); however, both solutions further emphasized distance vision in the dominant eye and near vision in the nondominant eye for binocular vision. This selection that emphasized distance vision for binocular conditions can explain the favorable results in distance vision because the best monocular
Table 1. Summary of visual acuity between artificial pupil design and contralateral balanced multifocal contact lens combination. In each case the mean and standard deviation of all subjects is given
Mean ± standard deviation by type of contact lens correction
Artificial pupil Contralateral balanced multifocal contact lens combination p-value
BDVA photopic (logMAR) 0.01 ± 0.06 -0.03 ± 0.07 0.11
BDVA mesopic (logMAR) 0.16 ± 0.08 -0.12 ± 0.06 0.07
BNVA photopic (logMAR) 0.33 ± 0.16 -0.19 ± 0.10 000.001*
BDVA= binocular distance visual acuity; BNVA= binocular near visual acuity.*= statistically significant difference.
CBMCLC= contralateral balanced multifocal contact lens combination.Figure 2. Binocular photopic log contrast sensitivity function (85 cd/m2) for distance for the artificial pupil design and the balanced presbyopic contact lens. The y-axis shows the log contrast sensitivity and the x-axis shows the spatial frequencies in cycles per degree (cpd). Error bars represent the standard deviation from the means. Gray lines are the age-correlated norm values.
*= statistically significant differences between both systems.CBMCLC= contralateral balanced multifocal contact lens combination.
Figure 3. Binocular mesopic log contrast sensitivity function (5 cd/m2) for distance vision for the artificial pupil design and the balanced presbyopic contact lens. The y-axis shows the log contrast sensitivity and the x-axis shows the spatial frequencies in cycles per degree (cpd). Error bars represent the standard deviation from the means. Gray lines are the age-correlated norm values.

(úċüIJú�-ĦēúċĈ�4 �þč�úą�
79"SR�#SBT�0GUBMNPM����������������
input would be responsible for conducting binocular visual acuity tasks. The BDVA values obtained in this study were coincident with those previously reported in patients fitted with CBMCLC(13,15) (Pro-clear Multifocal of Cooper Vision) or those fitted with artificial pupil contact lenses(7). Moreover, our results were consistent with those of research conducted in patients implanted with a artificial pupil in a corneal inlay for correcting presbyopia(16,17) or simulated pinholes using adaptive optics(18) under photopic conditions.
The add power in the aspheric multifocal contact lenses and the near-center design of lenses placed in the nondominant eye pro-vided better performance compared with the monocular increased depth-of-field in the artificial pupil contact lenses in near vision. The results for the artificial pupil contact lens reported here are in agreement with the results of recently reported studies that com-pared pinhole contact lenses(6) and artificial pupil contact lenses (1.6-mm central aperture in a 4-mm diameter opaque zone) with monovision(7) or using adaptive optics(18). In contrast, at least 3 studies using intracorneal inlays reported better BNVA values compared with those found in our study(16,17,19). These differences may be due to the increased transmission of visible light because of the 1.600 small holes (25-µm diameter) arranged in a randomized pattern of small perforations in the intracorneal inlay (Kamra intracorneal inlay). These holes allowed the light to pass, with an average light transmission of 7.1% through the annulus of the inlay(16). This disagreement also occurred in previous studies performed with CBMCLC(13) or simulta-neous vision multifocal contact lenses(5,12,20,21). Probably, this disparity in results was related to the different techniques, design of lenses, and adaptation criteria.
Contrast sensitivity is a very important measurement for patients fitted with contact lenses for presbyopia and allows for the detec-tion of subtle changes in visual quality that may not be detected by any other measurement. Our results, in terms of binocular contrast sensitivity, were consistent with those reported previously using the artificial pupil contact lens(6,7). Unfortunately, no previous studies ana lyzed contrast sensitivity in patients with CBMCLC; therefore, a direct comparison with other reports was not possible. Nevertheless, we can compare our results with those for other simultaneous vision multifocal lenses (with other surface designs). The CBMCLC results re-ported here were in agreement with those reported by other authors
CBMCLC= contralateral balanced multifocal contact lens combination.*= statistically significant differences between both systems.
Figure 4. Binocular photopic log contrast sensitivity function (85 cd/m2) for near vision for the artificial pupil design and the balanced presbyopic contact lens. The y-axis shows the log contrast sensitivity and the x-axis shows the spatial frequencies in cycles per degree (cpd). Error bars represent the standard deviation of the means.
CBMCLC= contralateral balanced multifocal contact lens combination.*= statistically significant differences between both systems.
Figure 5. Defocus curve for the artificial pupil design and the contralateral balanced multifocal contact lens combination. The y-axis shows visual acuity (logMAR) and the x-axis shows vergence (top, diopters; bottom, cm). Error bars represent the standard deviation of the means.
using simultaneous vision contact lenses with a center-near design (PureVision multifocal)(20-22). The differences in binocular contrast sensitivity between the artificial pupil and CBMCLC strategies in our study may be due to the greater effect of increased retinal blur from the defocus in the artificial pupil contact lens compared with that from the superimposed images in CBMCLC.
Intermediate vision can be crucial (for example, most of the tasks performed with a computer require good intermediate vision) because of the current lifestyles of presbyopic patients. Therefore, any presbyopic solution should give the patients a wide range of vision. In order to do that, previous studies have shown that the de focus curve may be an effective method to assess the clear range of vision in patients with simultaneous vision multifocal contact lenses(21). In the present research, the visual acuity from -1.00 to -4.00 D (these vergences are equivalent to a distance from 100 to 25 cm) was significantly better with CBMCLC than with the artificial pupil contact lens (Figure 5). These results obtained with pinhole contact lenses were consistent with the outcomes reported previously with artificial pupil contact lenses(6,7) or after intracorneal implantation(16,17). There are no previous studies on the defocus curve of the CBMCLC technique in presbyopic patients for comparison with our results. With regard to simultaneous vision multifocal contact lenses, Gupta et al.(21) had reported visual acuity values of 0.30 ± 0.10 logMAR at 80 cm with the PureVision multifocal contact lens, while in the pre-sent study, the acuities were approximately 0.03 logMAR with CBMCLC for the same distance. This difference between both multi-focal studies could be due to the use of a center-distance and cen-ter-near design in the dominant and nondominant eyes, respectively, with CBMCLC, as opposed to the use of a center-near design in both eyes with PureVision multifocal contact lenses.
The NSA may be measured using different tests, and the prac -ti tioner must select the one that is appropriate for each situation. The Howard-Dolman apparatus accurately analyzes the stereosco-pic threshold in contrast to more commercial and clinically used vecto graphic tests such as the Titmus and Random Dot. The Titmus and Random Dot stereotests provide fixed disparities; therefore, the accuracy of the outcomes depends on the number of steps and their disparity levels. Instead, the Howard-Dolman method gives a continuous measure of NSA with high accuracy. The differences

"ċčĂÿĂüĂúą�ĉĎĉĂą�ďþċČĎČ�üĈćčċúąúčþċúą�ûúąúćüþý�üĈćčúüč�ąþćČ�ÿĂč�ÿĈċ�ĉċþČûĒĈĉĂú�üĈċċþüčĂĈć
�� "SR�#SBT�0GUBMNPM����������������
between the two systems were consistent with those obtained in terms of visual acuity and contrast sensitivity in patients with near vision. Previous studies have analyzed the effects of artificial pupils placed in one eye at the NSA threshold under binocular conditions and have shown similar outcomes(6,7). The CBMCLC results reported here were in disagreement with those reported by the only study that analyzed NSA in patients fitted with CBMCLC(13). Ferrer-Blasco et al.(13)
found 22.40 ± 8.23, 56.40 ± 18.00, and 54.80 ± 20.23 sec of arc in 25 patients fitted with Proclear multifocal lenses from Cooper Vision using the Howard-Dolman, Titmus, and Random Dot sterereotests, respectively. Previous studies have analyzed NSA in patients fitted with different models of multifocal contact lenses with the same(12,22) or different stereotests(5,21,23-25). Considering all these previous studies, there has been some variability among results. The use of different stereotests and the design of the lenses (concentric or aspheric and add power) with the consequent image created on the retina made these differences plausible.
In summary, the present study assessed and compared the effects of the contact lens-based artificial pupil design and CBMCLC on visual performance. The results of this study suggested that for presbyopes, CBMCLC provided better performance in terms of inter-mediate and near vision compared with the artificial pupil contact lens. The combined design of multifocal optics with monovision may be more appropriate than contact lenses based on the depth-of-field under real-life conditions.
REFERENCES 1. Kleinstein RN. Epidemiology of presbyopia. In: Stark L, Obrecht G, editors. Presbyopia.
New York: Professional Press; 1987. p.12-8. 2. Ferrer-Blasco T, González-Méijome JM, Montés-Micó R. Age-related changes in the
human visual system and prevalence of refractive conditions in patients attending an eye clinic. J Cataract Refract Surg. 2008;34(3):424-32.
3. Patorgis CJ. Presbyopia. In: Amos JF, editor. Diagnosis and management in vision care. Boston: Butterworths; 1987. p.203-38.
4. Morgan PB, Efron N, Woods CA; International Contact Lens Prescribing Survey Con-sortium. An international survey of contact lens prescribing for presbyopia. Clin Exp Optom. 2011;94(1):87-92.
5. Richdale K, Mitchell GL, Zadnik K. Comparison of multifocal and monovision soft contact lens corrections in patients with low-astigmatic presbyopia. Optom Vis Sci. 2006;83(5):266-73.
6. García-Lázaro S, Ferrer-Blasco T, Radhakrishnan H, Cerviño A, Charman WN, Montés-Micó R. Visual function through 4 different contact-lens based pinhole systems for pres-byopia. J Cataract Refract Surg. 2012;38(5):858-65.
7. García-Lázaro S, Ferrer-Blasco T, Radhakrishnan H, Albarrán-Diego C, Montés-Micó R. Visual comparison of an artificial pupil contact lens to monovisión. Optom Vis Sci. 89(7):E1022-9
8. Borish IM. Clinical Refraction. Chicago: Professional Press; 1970. p.355. 9. Hanlon SD, Nakabayashi L Shigezawa G. A critical review of presbyopic add determi-
nation. J Am Optom Assoc. 1987;58(6):468-72. 10. Woo GC, Sivak IG. A comparison of three methods for determining the reading
addition. Am J Optom Pnysiot Opt. 1979;56(2):75-7. 11. Gupta N, Naroo SA, Wolffsohn JS. Is randomisation necessary for measuring defocus
curves in pre-presbyopes? Cont Lens Anterior Eye. 2007;30(2):119-24. 12. Ferrer-Blasco T, Madrid-Costa D. Stereoacuity with simultaneous vision multifocal
contact lenses. Optom Vis Sci. 2010;87(9):E663-8. 13. Ferrer-Blasco T, Madrid-Costa D. Stereoacuity with balanced presbyopic contact
lenses. Clin Exp Optom. 2011;94(1):76-81. 14. Ferrer-Blasco T, Madrid-Costa D, García-Lázaro S, Cerviño A, Montés-Micó R. Stereopsis
in bilaterally multifocal pseudophakic patients. Graefes Arch Clin Exp Ophthalmol. 2011;249(2):245-51.
15. Sanders E, Wagner H, Reich LN. Visual acuity and balanced progressive simultaneous vision multifocal contact lenses. Eye Contact Lens. 2008;34(5):293-6.
16. Yilmaz OF, Bayraktar S, Agca A, Yilmaz B, McDonald MB, van de Pol C. Intracorneal inlay for the surgical correction of presbyopia. J Cataract Refract Surg. 2008;34(11):1921-7.
17. Seyeddain O, Riha W, Hohensinn M, Nix G, Dexl AK, Grabner G. Refractive surgical correction of presbyopia with the AcuFocus small aperture corneal inlay: two-year follow-up. J Refract Surg. 2010;26(10):707-15.
18. Tabernero J, Schwarz C, Fernández EJ, Artal P. Binocular visual simulation of a corneal inlay to increase depth of focus. Invest Ophthalmol Vis Sci. 2011;52(8):5273-7.
19. Yılmaz OF, Alagöz N, Pekel G, Azman E, Aksoy EF, Cakır H, Bozkurt E, Demirok A. Intra-corneal inlay to correct presbyopia: Long-term results. J Cataract Refract Surg. 2011; 37(7):1275-81.
20. Llorente A, García-Lázaro S, Ferrer-Blasco T, Pérez -Cambrodí RJ, Cerviño A. Visual performance with simultaneous vision multifocal contact lenses. Clin Exp Optom. 2011,95(1):54-9.
21. Gupta N, Naroo SA, Wolffsohn JS. Visual comparison of multifocal contact lens to monovision. Optom Vis Sci. 2009;86(2):98-105.
22. García-Lázaro S, Ferrer-Blasco T, Radhakrishnan H, Albarrán-Diego C, Montés-Micó R. Visual performance comparison between contact-lens based pinhole and simulta-neous vision contact lenses. Clin Exp Optom. 2013;96(1):46-52.
23. Back A, Grant T, Hine N. Comparative visual performance of three presbyopic contact lens corrections. Optom Vis Sci. 1992;69(6):474-80.
24. Woods J, Woods CA, Fonn D. Early symptomatic presbyopes-what correction moda-lity works best? Eye Contact Lens. 2009;35(5):221-6.
25. Kirschen DG, Hung CC, Nakano TR. Comparison of suppression, stereoacuity, and interocular differences in visual acuity in monovision and acuvue bifocal contact lenses. Optom Vis Sci. 1999;76(12):832-7.

��"SR�#SBT�0GUBMNPM���������������
0ċĂĀĂćúą�"ċčĂüąþ�
Metallic corneal foreign bodies: an occupational health hazard
Corpos estranhos metálicos na córnea: um problema de saúde ocupacional
zeyneP guRsel ozkuRt1, haRun yuksel1, gunay saka1, hande guClu2, sina evsen2, selahattin balsak2
INTRODUCTIONA superficial corneal foreign body (FB) is the most common and
preventable eye injury(1). Metallic corneal FBs resulting from occupa-tional accidents are often seen in construction and metal industry workers(2). FBs can decrease the quality of vision by causing scars on the visual axis and secondary infections ranging from keratitis to en-dophthalmitis(3,4). The health care costs for these injuries are another problem as they create an economic burden(5).
Prevention of FB accidents and their potentially serious conse-quences are certainly possible, and the investment in their preven-tion is easily justified. Wearing appropriate protective goggles pre-vents about two-thirds of these accidents(6). In addition to the use of personal protective measures, it is important to improve workplace standards and provide appropriate training for supervisors(7).
Approximately 36% workers in Turkey are unregistered(8). Unre-gistered workers do not qualify for government-funded health care
Submitted for publication: November 22, 2013 Accepted for publication: December 6, 2013
Study conducted at Dicle University Faculty of Medicine, Diyarbakir, Turkey.1 Department of Ophthalmology, Dicle University of Medicine, Diyarbakir, Turkey.2�'L\DUEDNLU�(GXFDWLRQ�DQG�5HVHDUFK�+RVSLWDO��'L\DUEDN×U��7XUNH\�
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Zeynep Gursel Ozkurt. Dicle University Medical. Faculty Ophthalmology Department Diyarbakir, Diyarbakir 21280 - Turkey - E-mail: [email protected]
This study was approved by Dicle University Medical Faculty Ethics Committee Hospital.
ABSTRACTPurpose: To analyze the risk factors, outcomes, demographic characteristics, and attitudes of workers with metallic corneal foreign body (FB) injury. Methods: One hundred consecutive patients who presented with a metallic cor neal FB to the eye clinic at Diyarbakir Training and Research Hospital were eva -luated. The patients completed a questionnaire and were examined to determine features of the injury. Results: All patients were male. The mean age was 32.46 ± 1.03 years. Fifty-five percent of the patients were unregistered workers, 59% were working in the metal industry sector, and 65% injuries resulted from metal cutting. Protective goggles were available in the workplace of 64% patients. However, 57% patients were not wearing goggles when the accident occurred, and 43% were injured despite goggle use. Most patients (52%) attempted to remove FBs by themselves. FBs were located in the central zone of the cornea in 16% patients. Rust marks remained after FB removal in 26% patients. Corneal scars from previous FB injuries were present in 58% patients. Only 8% workplaces provided compensation for physician visits for occupation-related illnesses. Conclusions: Workplaces with a high risk for eye injuries should increase their protective measures, and educational programs should be implemented for both workers and occupational physicians. The government should enforce laws regarding unregistered workers in a better manner.
Keywords: Corneal injuries; Ocular foreign bodies; Eye injuries; Occupational health; Accidents, occupational
RESUMOObjetivo: Analisar os fatores de risco, resultados, características demográficas dos trabalhadores e atitudes em relação à lesão por corpo estranho metálico na córnea. Métodos: Foram avaliados cem pacientes consecutivos que se apresentaram com corpo estranho metálico na córnea à clínica oftalmológica do Diyarbakir Training and Research Hospital. Um questionário foi respondido e as características da lesão foram anotadas. Resultados: Todos os pacientes eram do sexo masculino. A idade média foi de 32,46 ± 1,03 anos. Cinquenta e cinco por cento dos pacientes eram trabalhadores não registrados. Cinquenta e nove por cento dos pacientes estavam trabalhando no setor da indústria metal, 65% das lesões resultaram de corte de metal. A presença de óculos de proteção no local de trabalho foi de 64%. Cinquenta e sete por cento dos pacientes não estavam usando óculos de proteção no momento do acidente, e 43% sofreram a lesão, apesar do uso óculos de proteção. Cinquenta e dois por cento dos pacientes tentaram remover o corpo estranho por si só. Dezesseis por cento dos corpos estranhos foram na zona central da córnea. Um depósito de ferrugem permaneceu após a remoção do corpo estranho em 26% dos pacientes. Cinquenta e oito por cento dos pacientes tinham cicatrizes na córnea por causa de lesões por corpo estranho anteriores. Os locais de trabalho que proporcionaram remuneração por visita médica relacionada à ocupação foram de apenas 8%. Conclusões: Locais de trabalho de alto risco devem ser detectados e medidas de pro-teção devem ser aumentadas. Os programas educacionais devem ser implementados para os trabalhadores e médicos do trabalho. As leis sobre trabalhadores sem carteira assinada deve ser melhor fiscalizadas pelo governo.
Descritores: Córnea/lesões; Corpos estranhos oculares; Lesões oculares; Saúde ocu-pacional; Acidentes de trabalho
after an occupational accident nor do they take advantage of their legal rights. In this study, we investigated the demographic characte-ristics, eye protection measures, approaches to FBs, and the level of knowledge about corneal FBs in a working population in Turkey.
METHODSThis study was approved by the hospital’s institutional review
board and adhered to the tenets of the Declaration of Helsinki. This prospective study evaluated 100 consecutive patients who presen-ted with metallic corneal FBs to the eye clinic at Diyarbakir Training and Research Hospital between December 2012 and May 2013. Ver-bal consent was obtained from the patients before they completed the questionnaire.
Patients were evaluated with a silt-lamp biomicroscope. FBs and rust rings were removed using a 26-gauge needle under topical anes thesia. A topical antibiotic treatment (Tobramycin, four times

.þčúąąĂü�üĈċćþúą�ÿĈċþĂĀć�ûĈýĂþČ��úć�ĈüüĎĉúčĂĈćúą�āþúąčā�āúēúċý�
�� "SR�#SBT�0GUBMNPM���������������
a day) was prescribed after FBs were removed. The locations of the removed FB, rust marks, and any existing corneal scars from previous FBs were noted.
We recorded demographic information for each patient, which included age, gender, education, and type of social insurance. The following data also were obtained through our questionnaire: busi-ness sector and occupation at the time of incident, number of years of work in the present sector, time between the incident and first visit to an ophthalmologist, number of previous similar eye injuries, availa-bility of protective goggles at work, protective goggle use during the incident, attempted FB removal by the patient, technique used if self-removal was attempted, the number of workers in the workplace, and presence of an occupational physician. To determine a worker’s level of knowledge about corneal FB injuries, we asked whether they understood that repetitive FB injuries can cause serious visual impair-ment and FB removal by themselves can cause serious and infection.
Statistical analyses were performed with Statistical Program for Social Science (SPSS) version 15 (SPSS, Chicago, Illinois, USA). The sta -tistical calculations included descriptive statistics, chi-square test, and Spearman-Brown correlation. The data are presented as the mean ± standard deviation.
RESULTSWe examined 100 patients who were diagnosed with a metallic
corneal FB. All patients were male and had a mean age of 32.46 ± 1.03 years (age range: 14-57 years; Table 1). Six percent of patients had not received formal education, 56% had completed primary school, 23% had completed secondary school, 15% had graduated from high school or an equivalent institution. Forty-eight percent of the pa-tients had a green card (a document given to low-income individuals without social insurance to allow them to use the public health care service in Turkey) and 7% had no social insurance; thus, 55% patients were unregistered workers, whereas only 45% were registered.
Most patients (59%) were working in the metal industry sector, 25% were working in the construction sector, and 8% were working in automotive repair sector (Table 2). Most injuries (65%) occurred when the patient was cutting metal (65%), 22% occurred with welding, and 13% had an unknown origin (Table 3). The number of FB injuries increa sed significantly with number of years at work in the metal industry and construction sectors (p<0.001, p=0.005). Sixty-four per-cent of the patients reported that protective goggles were available in their workplace; however, 57% were not wearing goggles at the time the accident occurred, and 43% were injured despite goggle use. There was no significant correlation between the education level and goggle use (p=0.470).
We examined the patient’s knowledge about corneal FBs and his approach to treatment. The mean duration between the injury and the first visit to an ophthalmologist was 2.16 (±0.26) days and ranged between 0 and 21 days. We found that 52% patients attempted FB removal by themselves. The materials used for the removal were currency notes (31%), napkins (7%), a cloth (4%), and miscellaneous items (10%) such as a needle or toothpick, which can cause further in-jury (Table 4). One patient presented with a deep central corneal scar that caused a secondary infection after he had removed the FB by himself. There was no significant correlation between the education level and whether patients attempted to remove FBs by themselves, or between understanding the potential harm in self-removal and understanding repetitive FB injuries can harm visual acuity (p=0.079, p=0.435, p=0.329).
Only 8% workplaces provided an occupational physician service; however, the presence of an occupational physician in the workplace did not affect the availability of protective goggles (p=0.580), the workers’ attitudes about wearing goggles (p=0.341), whether workers attempted to remove FBs by themselves (p=0.284), or understanding the harm of self-removal of FBs p=0.764).
The locations of the FBs were central (16%), paracentral (61%), and peripheral (23%). Rust marks were present in 26% patients after FBs were removed. Corneal scars due to previous FB injuries were pre-sent in 58% patients and were located in the central (5%), paracentral (42%), and peripheral (11%) regions.
DISCUSSIONCorneal injury due to a metallic FB is a common occupational
health injury in Turkey and worldwide. Occupational injury by corneal FB comprises 35%-58% of all ocular trauma(9,10), and more frequently affects young men(11). These preventable injuries cause additional bur den on the national economy, adjustment problems, and psycho-logical morbidity(5,12).
In a study conducted in Turkey, metal fragments caused 37% of all superficial corneal FB injuries, but the occupational injury ratio and the causes of injury were not defined in that study(13). In our study, occupational injuries occurred during metal cutting (65%) or welding (22%), whereas 13% had an unknown origin. Metal cutting and welding are frequent tasks in the metal industry; hence, most FB eye injuries occurred in this sector (59%), which was followed by the construction sector. In a similar study, 70% corneal FB injuries occur red in the metal cutting industry(14). In a Canadian study, 21% eye injuries occurred during welding(15). Thus, the people working in these sectors comprise the largest risk group.
In our patient population, 52% patients attempted to remove the FBs themselves using materials that can damage and infect the
Table 4. Materials used for self-removal
Material Percentage
Paper money 31%
Napkins 07%
A piece of cloth 04%
Other 10%
Table 1. Distribution of patients by age group in 15-year age intervals
Age group (years) Percentage
14-29 42%
30-44 42%
45-60 16%
Table 2. Occupation sectors
Sector Percentage
Metal industry 59%
Construction industry 25%
Automotive repair 08%
Other 08%
Table 3. İnjury mechanisms
İnjury mechanism Percentage
Metal cutting 65%
Welding 22%
Unknown origin 13%

0ēĄĎċč�;( �þč�úą�
��"SR�#SBT�0GUBMNPM���������������
cornea. In a study conducted by Filho et al., several microorganisms apart from the normal conjunctival flora were isolated from 20% conjunctival swabs of patients with corneal FBs(4). In a similar study, 14% positive bacteria cultures were obtained from patients with corneal FBs(5). Corneal FBs themselves can spread infections, and self-removal of an FB with contaminated and potentially traumatic materials can increase the risk of corneal infections. These secondary corneal infections affect the quality of vision and can cause corneal scarring. In one of our patients, a deep corneal scar caused vision loss that resulted from a corneal abscess that formed after self-removal of an FB. In an Australian study that included 100 patients with metallic corneal FBs, one patient presented with bacterial keratitis, although it was not indicated whether the patient attempted FB removal(11).
Metallic FBs usually leaves a rust ring in the cornea often causes a white scar to form that can decrease visual quality. The appearance of a rust ring indicates an FB was embedded in the cornea for >12-24 h(16). Therefore, visiting an ophthalmologist after an injury as soon as possi-ble is crucial. Among our patients, the mean duration between the injury and their first visit to an ophthalmologist was 2.16 (±0.26) days after the injury. A rust ring remained in 26% patients and a corneal white scar attributed to a previous FB was observed in 58% patients. The high frequency of scarring observed in our patients likely resul-ted from the delay in seeking treatment from an ophthalmologist and the attempt of removing the FB with traumatic materials.
Using protective goggles, especially those with top and side shields, may have prevented two-thirds of these FB injuries(6). Despite wearing goggles, 43% patients sustained injuries. In a similar study, 45% patients sustained an eye injury while wearing some form of eye protection(11). In this context, new designs should be implemented and workplace standards should be adjusted to increase the protecti-ve capabilities of goggles(7).
According to the current occupational health and safety board re -gulations in Turkey, an occupational physician is necessary in sectors that employ at least 50 workers. The workplaces of only 8% patients in the present study had an occupational physician. The dominance of small-scale workplaces and 55% workers being unregistered might explain this low ratio. Unfortunately, the presence of an occupational physician has not been effective for the procurement of protective goggles at workplaces or the attitudes of workers toward goggle use. In addition, the presence of an occupational physician has not increa-sed the workers’ level of knowledge about ocular safety. In addition, no correlation was found between education and the knowledge of the subject. According to these data, occupational physicians should be informed about the importance of preventative measures against eye injuries, and they should inform workers about the subject without considering the workers education status.
In Turkey, approximately 36% employees are unregistered(8). In the present study, this percentage was even higher at 55%. These
unregistered workers are unable to take advantage of legal rights for accidents occurring at work. In addition, workers do not have social insurance and are ineligible for free health care. This situation can force workers to remove the FBs by themselves rather than seek care from an ophthalmologist.
CONCLUSIONWorkplaces with a high risk for corneal injury should be identified,
occupational physicians and workers should be educated about such eye injuries, and eye protective measures should be increased. Furthermore, the necessary legal arrangements should be made to decrease the number of unregistered workers.
ACKNOWLEDGMENTWe are grateful to Dicle University DUBAP for their sponsorship
of the English editing of this manuscript.
REFERENCES 1. Woo JH, Sundar G. Eye injuries in Singapore-Don’t risk it. Do more. A prospective study.
Ann Acad Med Singapore. 2006;35(10):706-18. 2. Welch LS, Hunting KL, Mawudeku A. Injury surveillance in construction: eye injuries.
Appl Occup Environ Hyg. 2001;16(7):755-62. 3. DeBroff BM, Donahue SP, Caputo BJ, Azar MJ, Kowalski RP, Karenchak LM. Clinical cha-
racteristics of corneal foreign bodies and their associated culture results. CLAO J. 1994; 20(2):128-30.
4. Macedo Filho ET, Lago A, Duarte K, Liang SJ, Lima AL, Freitas D. Superficial corneal foreign body: laboratory and epidemiologic aspects. Arq Bras Oftalmol. 2005;68(6):821-3.
5. Fong LP. Eye injuries in Victoria, Australia. Med J Aust. 1995;162(2):64-8. 6. Gumus K, Karakucuk S, Mirza E. Corneal ınjury from a metallic foreign body: an occu-
pational hazard. Eye Contact Lens. 2007;33(5):259-60. 7. Lipscomb HJ, Dement JM, McDougall V, Kalat J. Work-related eye injuries among union
carpenters. Appl Occup Environ Hyg. 1999;14(10):665-76. 8. Turkiey Istatistik Kurumu. [cited 2013 Sep 6]. Available from: http://www.tuik.gov.tr/
PreHaberBultenleri.do?id=13483 9. Nicaeus T, Erb C, Rohrbach M, Thiel HJ. [An analysis of 148 outpatient treated occupa-
tional accidents]. Klin Monatsbl Augenheilkd. 1996;209(4):A7-11. German. 10. Voon LW, See J, Wong TY. The epidemiology of ocular trauma in Singapore: perspective
from the emergency service. Eye (Lond). 2001;15(Pt 1):75-81. 11. Ramakrishnan T, Constantinou M, Jhanji V, Vajpayee RB. Corneal metallic foreign body
injuries due to suboptimal ocular protection. Arch Environ Occup Health. 2012;67(1):48-50. 12. Alexander DA, Kemp RV, Klein S, Forrester JV. Psychiatric sequelae and psychosocial
adjustment following ocular trauma: a retrospective pilot study. Br J Ophthalmol. 2001; 85(5):560-2.
13. Yiğit O, Yürüktümen A, Arslan S. Foreign body traumas of the eye managed in an emer-gency department of a single-institution. Ulus Travma Acil Cerrahi Derg. 2012;18(1):75-9.
14. Nepp J, Rainer G, Krepler K, Stolba U, Wedrich A. [Etiology of non-penetrating corneal injuries]. Klin Monatsbl Augenheilkd. 1999;215(6):334-7. German
15. Reesal MR, Dufresne RM, Suggett D, Alleyne BC. Welder eye injuries. J Occup Med. 1989;31(12):1003-6.
16. Casser L, Fingeret M, Woodcome H. Atlas of primary eyecare procedures. New York: Appleton Lange; 1990.

�� "SR�#SBT�0GUBMNPM���������������
0ċĂĀĂćúą�"ċčĂüąþ�
Changes in corneal sensitivity following cross-linking for progressive early-stage keratoconus
Alterações da sensibilidade corneana após cross-linking para ceratocone progressivo em estágio inicial
anelise de medeiRos lago1, belquiz R. do amaRal nassaRalla2, laRissa Rossana souza stival1, João JoRge nassaRalla JunioR3,4
Submitted for publication: June 20, 2013 Accepted for publication: October 25, 2013
Study conducted at Goiania Eye Institute, Goiânia, GO, Brazil.1 Goiania Eye Institute, Goiânia, GO, Brazil.2 Department of Cornea and Refractive Surgery, Goiania Eye Institute, Goiânia, GO, Brazil.3 Department of Retina & Vitreous, Goiania Eye Institute, Goiânia, GO, Brazil.4 Faculty of Health Sciences, University of Brasília, Brasília, DF, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Corresponding address: Anelise de Medeiros Lago. Rua Soledade, 1.268 - Apto. 405 - Edifício Re sidencial Petrópolis - Esteio (RS) - 793260-150 - Brazil - E-mail: [email protected]
ClinicalTrials.gov ID: NCT01743443
Research Ethics Committee: Goiânia Eye Institute, Goiânia, Goiás, Brazil.
INTRODUCTIONKeratoconus is a corneal ectatic disease where the cornea assu-
mes a conical shape because of thinning, inducing irregular astigma-tism and leading to marked impairment of vision. Keratoconus typi-cally initiates at puberty and may progress, depending on individual characteristics, until the third or fourth decade of life; alternatively, it may commence later and arrest at any age. The disease is associated with several conditions, particularly those that encourage eye rubbing. This theory is supported by the fact that patients with keratoconus frequently have itchy eyes and ocular irritation. An autosomal domi-nant inheritance is reported in approximately 10% patients(1).
Keratoconus occurs in virtually every ethnic group. There is no gen der predominance, and it almost always presents bilaterally, alth ough the clinical features are frequently asymmetrical. The rate of progression varies between individuals and also between the two eyes. The severity at the stop of progression is also highly variable and can range from mild irregular astigmatism to severe thinning, scarring, and protrusion(1,2).
ABSTRACTPurpose: To evaluate changes in corneal sensitivity following corneal cross-linking (CXL) in patients with progressive earlier stage keratoconus.Methods: Thirty-eight eyes of 19 patients (11 women, 8 men) were included in a prospective, nonrandomized clinical study. The mean patient age was 22 years (range, 18-26 years). Inclusion criteria were early stage bilateral progressive kera-toconus, a transparent cornea, and a thickness of ≥440 µm in the thinnest area of the cornea. Using the Cochet-Bonnet esthesiometer, central corneal sensitivity was measured before surgery, 7 days after surgery, and once a month thereafter until recovery of baseline preoperative levels. Central corneal sensitivity >40 mm was considered normal. Results: Corneal sensitivity gradually returned to preoperative levels in all trea-ted eyes. The mean central corneal sensitivity was 52.2, 24.0, 38.2, 42.5, 50.0, and 52.5 mm before surgery, 7 days after surgery, and at 1, 2, 3, and 4 months after surgery, respectively. Normal levels of corneal sensation, but not baseline (preo-perative) levels, were observed 2 months after surgery. The preoperative levels were obser ved 3 months after surgery. Conclusions: Our results suggest that central corneal sensitivity can be decrea sed for as long as 3 months after CXL for progressive earlier stage keratoconus.
Keywords: Keratoconus/therapy; Collagen/radiation effects; Riboflavin/therapeu-tic use; Ultraviolet therapy; Cross-linking reagents; Corneal sensitivity
RESUMOObjetivo: Avaliar as alterações da sensibilidade corneana após cross-linking (CXL) da córnea em pacientes com ceratocone progressivo em estágio inicial. Métodos: Trinta e oito olhos de 19 pacientes (11 mulheres, 8 homens) foram incluídos em um estudo clínico prospectivo, não randomizado. A média de idade dos pacientes era de 22 anos (variação, 18-26 anos). Os critérios de inclusão foram ceratocone progressivo bilateral em estágio inicial, córnea transparente e espessura da córnea ≥440 µm usando o estesiômetro de Cochet-Bonnet, mediu-se a sensibilidade da córnea no pré-operatório, após 7 dias, e uma vez por mês até a recuperação dos níveis pré-operatórios. Foram considerados normais, valores de sensibilidade corneana superiores a 40 mm. Resultados: A sensibilidade da córnea retornou gradualmente aos níveis pré-ope-ratórios em todos os olhos tratados. A média de sensibilidade corneana central foi de 52,2, 24,0, 38,2, 42,5, 50,0 e 52,5 mm, antes da cirurgia, aos 7 dias, e em 1, 2, 3 e 4 meses após a cirurgia, respectivamente. Níveis normais de sensibilidade, mas não os níveis pré-operatórios basais, foram observados dois meses após a cirurgia. Níveis pré-operatórios foram observados três meses após a cirurgia. Conclusão: Nossos resultados sugerem que após CXL para ceratocone progressivo em estágio inicial, a sensibilidade corneana permanece diminuída por até 3 meses.
Descritores: Ceratocone/terapia; Colágeno/efeitos de radiação; Riboflavina/uso terapêutico; Terapia ultravioleta; Reagentes para ligações cruzadas; Sensibilidade da córnea
Several possible alternatives to manage keratoconic corneas have been reported in the literature, including gas-permeable contact lenses, intracorneal ring segment implantation, and corneal transplantation. However, these options have been limited to the treatment of the consequences of progressive corneal weakening, without any effect on the cause of the disease(2).
Corneal collagen cross-linking (CXL) has been established as an effective surgical treatment for increasing the biomechanical stability of the cornea to prevent the progression of corneal ectasia that occurs in keratoconus(3-5) or after laser refractive surgery(6,7). This te chni que uses a combination of riboflavin (vitamin B2) and ultraviolet A (UVA) light to induce cross-linking in the stromal collagen. There are two roles of riboflavin in this method. It works as a photosensitizer for the induction of cross-links and protects the underlying tissues from the deleterious influence of UVA irradiation(3-5). It is the only the-rapeutic approach designed to arrest the progression of disease(3,4).
The cornea is one of the most sensitive tissues of the body be cause it is densely innervated with sensory nerve fibers via the

-úĀĈ�". �þč�úą�
��"SR�#SBT�0GUBMNPM���������������
ophthalmic division of the trigeminal nerve through 70-80 long and short ciliary nerves. Apart from the important sensory functions, corneal nerves help in maintaining the functional integrity of the ocular surface by releasing trophic substances to promote epithelial homeostasis through activation of brain circuits that stimulate tear production and the blinking reflex(8). Given the crucial role of the cor neal nerve in maintaining normal corneal structure and function, impaired corneal innervation may challenge the ability of the cornea to withstand surgical challenges, thus leading to a significantly in -crea sed risk of complications(9).
Evaluation of corneal sensitivity after corneal CXL with UVA irra-diation is important to assess the efficacy and long-term effects of this treatment. In this prospective study, we evaluated the changes in corneal sensitivity after corneal CXL in patients with progressive early-stage keratoconus.
METHODSThirty-eight eyes of 19 patients (11 men and 8 women) with pro -
gressive early-stage keratoconus, transparent corneas, and a corneal thickness of ≥440 µm in the thinnest area were enrolled in a pros-pective, nonrandomized clinical study. According to the Amsler-Kru-meich classification(10) of keratoconus, all eyes were considered to be in the early stages of keratoconus: 32 eyes (84.2%) were in stage I and 6 eyes (15.8%) were in stage II. An increase of 1.00 diopter (D) in maxi-mum topographic K-value (Kmax) and a decrease in corneal thickness with or without changes in uncorrected visual acuity (UCVA) and best spectacle-corrected visual acuity (BSCVA) within the last year were considered as indications of progression. The mean patient age was 22 ± 2.7 years (range, 18-26 years). All procedures were performed by a single surgeon (BAN) at the Goiania Eye Institute, Goiania, GO, Brazil from January to December 2011.
Patients who fulfilled one of the following criteria after preope-rative examination were excluded: age <16 or >35 years; presence of corneal scars or opacities, pregnancy or lactation, active anterior segment pathologic features, systemic connective tissue disease, ocular or systemic disease that can affect epithelial healing, and/or dry eye syndrome; and a history of corneal or anterior segment surgery. Patients using contact lenses were asked to discontinue lens use for at least 3 weeks before each examination.
Preoperative and postoperative examinations included the following: UCVA, BSCVA, slit-lamp biomicroscopy, Goldmann tono-metry (Haag Streit, Bern, Swiss), fundus examination (Sigma 150K, Heine, Germany), specular microscopy (Konan, Hyogo, Japan), ul -tra sound pachymetry (CompuScanTM P, Storz, St. Louis, MO, USA), cor neal sensitivity testing (Cochet-Bonnet® esthesiometer, Luneau, Paris, France), and corneal topography (Orbscan IIz, Technolas Perfect Vision GmbH).
The institutional ethics committee approved the study. All patients provided written informed consent in accordance with the Declara-tion of Helsinki after receiving a detailed description of the nature and risks of the procedure.
TREATMENT
Corneal CXL was conducted under sterile conditions in an opera-ting room. All patients received a mild oral sedative (diazepam, 5 mg) 30 min before surgery and two drops of topical 0.5% proximetacaine 2 to 5 min before surgery. A wire eyelid speculum was placed for exposure. Corneal epithelium was removed by mechanical scraping over the central cornea (9.0 mm) with a blunt Paton spatula (Storz Ophthalmic Instruments, St Louis, USA).
The lid speculum was removed. Iso-osmolar 0.1% riboflavin solu-tion (402.7 mOsmol/L), which was prepared by diluting 0.5% vitamin B2-riboflavin-5-phosphate with 20% dextran T500, was instilled into the cornea every 3 min for 30 min. Slit-lamp examination using a blue filter ensured the presence of riboflavin in the anterior chamber.
The lid speculum was replaced before irradiation. Fixation during irradiation was achieved by instructing the patient to focus on the light-emitting diode on the UVA emitter. The surgeon’s thorough control ensured the patient’s centration. UVA irradiation was perfor-med for 30 min using a commercially available UVA system (UV-X, Peschke Meditrade) at a working distance of 5 cm, with an irradiance of 3 mW/cm2 corresponding to a surface dose of 5.4 J/cm2. During irra diation, iso-osmolar 0.1% riboflavin drops were applied every 5 min to ensure saturation of the cornea with riboflavin. A topical anes-thetic agent (0.5% proximetacaine) was applied as required.
After this treatment, the patients were medicated with 0.3% to pical moxifloxacin drops 4 times a day for 5 days and ketorolac trometha-mine 3 times a day for 3 days. A soft therapeutic lens was applied until complete re-epithelialization of the cornea was achieved. Un preserved artificial tears were recommended for mild irritation. Paracetamol-codeine pain medication was also prescribed as needed for the first 2 to 3 days. Fluorometholone eye drops were then applied 3 times a day for 2 weeks.
Using the Cochet-Bonnet® esthesiometer, central corneal sensi-tivity was measured before surgery, 7 days after surgery, and once a month after surgery until recovery of the baseline (preoperative) sen sitivity level. A central corneal sensitivity of >40 mm was consi-de red normal(11). Full recovery was considered as the recovery of the preoperative level of corneal sensitivity. The Cochet-Bonnet® es thesiometer comprises a nylon filament measuring 60.0 mm in length and 0.12 mm in diameter. The force exerted by the filament when it touches the cornea is inversely proportional to its length. All measurements were obtained by the same experienced observer. Patients lay in the supine position looking straight ahead, and they were asked to indicate when the stimulus was felt. The filament was moved toward the cornea smoothly at a perpendicular angle, guided by its corneal reflection. Contact was detected by a slight bending in the filament. If there was no patient response to the first contact, the length of the filament was decreased by 5.0 mm to increase its rigidity, and the procedure was repeated until the patient reported the feeling of corneal contact. The mean filament length from a mini-mum of 3 stimulus applications that elicited a positive response from the patient was considered to be the corneal touch threshold(11,12).
Statistical analysis was performed using SPSS 17.0 (SPSS, Inc.) software. The paired t-test was used to check the significance of the difference between two dependent groups in every continuous variable. A p-value of <0.05 was considered statistically significant.
RESULTS After treatment, complete re-epithelialization was observed wi thin
4 days in all patients. Corneal sensitivity gradually returned to preoperative levels in all
treated eyes. The mean central corneal sensitivity was 52.24 (±6.44) mm before surgery, 24.08 (±7.78) mm 7 days after surgery, and 38.29 (±4.23), 42.50 (±3.02), 50.00 (±3.07), and 52.50 (±2.78) mm 1, 2, 3, and 4 months after CXL, respectively. Normal levels of corneal sensation, but not a return to baseline (preoperative) levels, were noted 2 months after surgery (p=0.000). Statistical analysis showed a signifi-cant decrease in corneal sensitivity for up to 3 months after surgery. Preoperative levels were observed at 3 (p=0.081) and 4 months after surgery (p=0.817; Figure 1).
Four months after corneal CXL, 3 eyes (7.9%) experienced 1-line improvement in postoperative BSCVA. It did not change in 33 eyes (86.84%) and decreased by 1 line in 2 eyes (5.2%). No statistically signi-ficant difference was noted between preoperative and postoperative BSCVA values (p=0.571).
Sixteen eyes (42.2%) experienced a 1-line improvement in pos-toperative UCVA. One eye lost 1 line and another lost 2 lines in UCVA. No statistically significant improvement was observed between pre-operative and 4-month postoperative results (p=0.092).

$āúćĀþČ�Ăć�üĈċćþúą�ČþćČĂčĂďĂčĒ�ÿĈąąĈĐĂćĀ�üċĈČČ�ąĂćĄĂćĀ�ÿĈċ�ĉċĈĀċþČČĂďþ�þúċąĒ�ČčúĀþ�ĄþċúčĈüĈćĎČ�
�� "SR�#SBT�0GUBMNPM���������������
Figure 1. Changes in corneal sensitivity over time.
Table 1. Mean corneal pachymetry values, spherical equivalents, topo-graphic K-readings (Kmax and Kmin), intraocular pressure, and endothelial cell counts before and after corneal cross-linking
Before corneal CXL
Four months after surgery p-value
Pachymetry values 478 ± 24.8 µm (440-508 µm)
454 ± 29.06 µm (420-488 µm)
0.00
Spherical equivalents -2.08 (±0.85) D -1.92 (±0.84) D 0.00
Kmax 51.45 ± 1.77 D 50.18 ± 1.64 D 0.00
Kmin 45.49 ± 1.79 D 45.48 ± 1,81 D 0.860
Intraocular pressure 11.66 ± 1.23 mmHg 11.50 ± 1.24 mmHg 0.279
Endothelial cell counts 2280.26 ± 258 mm2 2287 ± 270 mm2 0.549
Four months after surgery, comparison of preoperative and posto-perative results showed a statistically significant difference between some of them. The mean thickness as assessed by central corneal pa chymetry decreased from 478 ± 24.8 µm to 454 ± 29.06 µm (p=0.00). The mean spherical equivalent decreased from -2.08 ± 0.85 D to -1.92 ± 0.84 D (p=0.00), and the mean maximum topographic K-readings (Kmax) dropped from 51.45 ± 1.77 D to 50.18 ± 1.64 D (p=0.00). No other data showed significant differences before and after surgery. The mean minimum topographic K-readings (Kmin) chan ged from 45.49 ± 1.79 D to 45.48 ± 1.81 D (p=0.860). The mean intraocular pressure changed from 11.66 ± 1.23 mmHg to 11.50 ± 1.24 mmHg (p=0.279), and the endothelial cell counts changed form 2280.26 ± 258 to 2287 ± 270 cells/mm2 (p=0.549). The mean patient data before and after cross-linking are shown in table 1.
No intraoperative, early postoperative, or late postoperative com-plications were observed in this series of patients. After 4 months, all corneas remained transparent, without any scar in the stroma.
DISCUSSIONMany corneal surgical procedures have been associated with a
tem porary decrease in corneal sensitivity due to amputation or laser ablation of the corneal nerves. This damage may contribute to the development of dry eye, impaired epithelial wound healing, increa-sed epithelial permeability, and ocular surface changes after the pro -cedure. In such cases, the corneal sensitivity usually returns to nor mal within 3-12 months after surgery(9,13).
Increased visibility of nerve fibers by slit lamp biomicroscopy has been demonstrated in patients with keratoconus. Corneal nerves pass between the stroma and epithelium at sites of early degradative change. The keratocytes wrap around the nerves as they pass through an otherwise acellular Bowman’s layer. Localized nerve thickening develops in the epithelium and stresses the epithelial architecture(14). In vivo laser scanning confocal microscopy has revealed decreased innervation and decreased cell density in all layers of the keratoco-nic cornea(15). The sub-basal nerve plexus architecture isaltered with fragmentation of the plexus, increased sub-basal nerve tortuosity, decreased central nerve fiber density, and a correlation between the decrease in nerve density decrease and severity of disease(16-18). Ano-ther study(19) reported decreased sensitivity in all corneal zones of pa-tients with keratoconus, and the decrease depended on the severity of the condition. Injured nerve fibers may quickly regenerate and may exhibit abnormal responses because of the altered expression of ion channel proteins in the regenerating nerve terminals(20). In the current study group, according to the Amsler-Krumeich classification(10) of ke ratoconus disease, all eyes were considered to be in early-stage keratoconus: 32 eyes (84.2%) were in stage I and 6 eyes (15.8%) were in stage II. Therefore, faster corneal sensitivity recovery was expected.
Corneal CXL with riboflavin and UVA irradiation is a technique of a minimally invasive nature that is used for the stabilization of diffe-rent types of corneal ectatic disorders. This technique augments the mechanical rigidity of the cornea by inducing cross-links at the corneal stroma(3-5). Removal of the epithelium has been recommended as an initial step in the CXL procedure because its lipophilic nature decreased the diffusion of riboflavin into the corneal stroma(4,5). Moreover, the epithelium may block the UV rays(3). The photosensitizer riboflavin is applied to the de-epithelialized surface of the cornea and is allowed to penetrate the corneal stroma(3-6). Subsequent exposure of the cornea to UVA light is believed to result in photodynamic cross-linking when riboflavin, excited by UVA, creates free radicals leading to collagen cross-linking(4,5).
An in vivo confocal laser scanning microscopy study(16) has de-mons trated that the anterior subepithelial stroma was recolonized by ner ve fibers, with the restoration of corneal sensitivity, 6 months after CXL using the epithelium-off technique. An animal study(17) of corneal sensitivity and innervation after CXL in rabbits has also shown that corneal sensitivity was significantly decreased 3 days after UVA irra-diation with de-epithelialization treatment. Corneal sensitivity in the central region of the cornea decreased to the lowest level 7 days after treatment and returned to normal 3 months after the procedure; the corneal nerve fiber density appeared normal after 6 months. A recent prospective, interventional case series(21) evaluated the effects of CXL on corneal innervation, sensitivity, and tear function in patients with progressive early-stage keratoconus. The study detected prominent hypoesthesia 1 month after surgery, which gradually recovered by 9 months after surgery; the time course was similar for both sensi-tivity restoration and corneal nerve regeneration. Another study(22) evaluated the changes in corneal tactile sensitivity following corneal collagen cross-linking in patients with progressive keratoconus and concluded that corneal CXL performed in keratoconus patients in-duced a considerable decrease in corneal sensitivity. This decrease was greater in the first week after the procedure, with progressive recovery for up to 6 months of follow-up. Our results demonstrated that normal levels of corneal sensation that were not yet baseline (preoperative) levels were observed two months after surgery, and significant transient hypoesthesia was observed for as long as 3 months after CXL. The difference in the time of corneal sensation recovery between the different studies may be related to other factors such as the degree of ectasia, contact lens use, and systemic disease that can affect epithelial healing or corneal sensitivity.
Contact lens wear decreases corneal sensitivity(23). To minimize any effect on measurements, patients using contact lenses have been asked to discontinue lens use for at least 3 weeks before each examination.

-úĀĈ�". �þč�úą�
��"SR�#SBT�0GUBMNPM���������������
Corneal sensation is also decreased in patients with diabetes and mild to moderate somatic neuropathy, and it progresses with the severity of neuropathy. These findings have important clinical im pli-cations with regard to the development of corneal abnormalities in patients with diabetes(24). Therefore, patients with systemic di sease that can affect epithelial healing and corneal sensitivity, such as dia-betes, were excluded from our study.
An important finding of this study was a significant decrease in corneal thickness after corneal CXL, which may also have contributed to the decrease in corneal sensitivity. Our group(25) recently described transient corneal thinning after corneal CXL with UVA irradiation and a hypo-osmolar riboflavin solution in thin corneas (<400 µm) for pro-gressive keratoconus. In our analysis of changes in corneal thickness over time, pachymetric values decreased until 1 month after surgery and appeared to increase thereafter. Six months after treatment, no statistically significant difference was found between postoperative and baseline values. The physiology of this initial thinning and subse-quent rethickening remains unclear. Epithelial removal may increase the rate of water evaporation from the stroma and renders the cornea vulnerable to thinning because the stroma has no dehydration resis-tance(26). Epithelial remodeling, anatomical and structural changes in corneal collagen fibrils(27), and keratocyte apoptosis(28) may also be im plicated. Surgeons must be aware about postoperative thinning of the cornea after CXL, particularly in thinner corneas. Ours results suggest that further studies are necessary to evaluate the relationship between the decrease in corneal thickness and transient corneal hy -poesthesia after CXL.
A few potential limitations were apparent in this study, with the small sample of studied eyes and the absence of a control group of patients being the major ones. However, because all patients pre -sented with bilateral progressive keratoconus, it was considered une thical to leave the disease untreated in one eye. Esthesiometry is a reproducibly accurate measure of corneal sensation. The most popular device for this purpose is the Cochet-Bonnet esthesiometer, which comprises a calibrated nylon filament for mechanical stimula-tion(11). It has limitations in its sensitivity as a test, but it is the most prac tical method available(12). The conclusions of this study should be interpreted within the limits of this method of evaluation.
Touching the cornea triggers one of the most sensitive protective reflexes of the human body. The threshold of sensitivity, particularly in the center of the cornea, is exceedingly low; therefore, pathological changes can be diagnosed early and precisely and can be used for diagnosis and follow-up and to assess the prognosis of various cor-neal disorders. The loss of normal corneal sensation may compromise the protective blink reflex, delay epithelial wound healing, decrease tear flow, and show an association with neurotrophic keratitis, sterile corneal melts, and infectious keratitis(11,28).
CONCLUSIONSThe results of this study emphasized the slow and gradual reco-
very of corneal sensitivity after CXL, as observed in other studies pu -blished in the literature. These observations can help to direct studies to better define the risk and management of persistent epitheliopa-thy and dry eye symptoms after CXL.
REFERENCES 1. Rabinowitz YS. Keratoconus. Surv Ophthalmol. 1998;42(4):297-319. 2. Romero-Jiménez M, Santodomingo-Rubido J, Wolffsohn JS. Keratoconus: a review.
Cont Lens Anterior Eye. 2010;33(4):157-66. 3. Wollensak G, Spoerl E, Seiler T. Ribofloavin/ultraviolet-A-induced collagen cosslinking
for the treatment of keratoconus. Am J Ophthalmol. 2003;135(5):620-27. 4 Spoerl E, Huhle M, Seiler T. Induction of cross-links in corneal tissue. Exp Eye Res. 1998;
66(1):97-103. 5. Wollensak G, Spoerl E, Seiler T. Stress-strain measurements of human and porcine
corneas after riboflavin-ultraviolet-A-induced cross-linking. J Cataract Refract Surg. 2003;29(9):1780-5.
6. Hafezi F, Kanellopoulos J, Wiltfang R, Seiler T. Corneal collagen cross-linking with ribo-flavin and ultraviolet A to treat induced keratectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2007;33(12):2035-40.
7. Salgado J, Khoramnia R, Lohmann C, Winkler von Mohrenfels C. Corneal collagen cross linking in post-LASIK keratectasia. Br J Ophthalmol. 2011;95(4):493-7.
8. Marfurt CF, Cox J, Deek S, Dvorscak, L. Anatomy of the human corneal innervation. Exp Eye Res. 2010;90(4):478-92.
9. Erie JC, McLaren JW, Hodge DO, Bourne WM. Recovery of corneal subbasal nerve density after PRK and LASIK. Am J Ophthalmol. 2005;140(6):1059-64.
10. Alió JL, Shabayek MH. Corneal higher order aberrations: a method to grade kerato-conus. J Refract Surg. 2006;22(6):539-45.
11. Cochet P, Bonnet R, L’ésthésie cornéenne. Sa mesure clinique. Ses variations physio-logiques et pathologiques. Clin Ophtalmol. 1960;4(1):3-27.
12. Murphy PJ, Lawrenson JG, Patel S, Marshall J. Reliability of the non-contact cor-neal aesthesiometer and its comparison with the Cochet–Bonnet aesthesiometer. Ophthal Physiol Opt. 1998;18(6):532-9.
13. Nassaralla BA, McLeod SD, Boteon JE, Nassaralla JJ. The effect of hinge position and depth plate on the rate of recovery of corneal sensation following LASIK. Am J Ophthalmol. 2005;139(1):118-24.
14. Dogru M, Karakaya H, Ozçetin H, Erturk H, Yucel A, Ozmen A, et al. Tear function and ocualr surface changes in keratoconus. Ophthalmology. 2003;110(6):1110-8.
15. Niederer RL, Perumal D, Sherwin T, McGhee NJ. Laser scanning in vivo confocal microscopy reveals reduced innervation and reduction in cell density in all layers of the keratoconic cornea. Invest Ophthalmol Vis Sci. 2013;49(7):2964-70.
16. Mazzotta C, Traversi C, Baiocchi S, Caporossi O, Bovone C, Sparamo M, et al. Corneal healing after riboflavin ultraviolet-A collagen cross-linking determined by confocal laser scanning microscopy in vivo: early and late modifications. Am J Ophthalmol. 2008;146(4):527-3.
17. Xia Y, Chai X, Zhou C, Ren Q. Corneal nerve morphology and sensitivity changes after ultraviolet A/riboflavin treatment. Exp Eye Res. 2011;93(4):541-7.
18. Kymionis GD, Diakonis VF, Kalyvianaki M, Pallikaris IG. One-year follow-up of corneal confocal microscopy after corneal cross-linking in patients with post laser in situ keratomileusis ectasia and keratoconus. Am J Ophthalmol. 2009;147(5):774-8.
19. Bleshoy H. Corneal sensitivity in keratoconus. J Br Contact Lens Assoc. 1986;9:9-12. 20. Belmonte C, Acosta MC, Gallar J. Neural basis of sensation in intact and injured
corneas. Exp Eye Res. 2004;78(3):513-25. 21. Kontadakis GA, Kymionis GD, Kankariya VP, Pallikaris AI. Effect of corneal collagen
cross-linking on corneal innervation, corneal sensitivity, and tear function of patients with keratoconus. Ophthalmology. 2013;120(5):917-22.
22. Wasilewski D, Mello HR, Moreira H. Impact of collagen crosslinking on corneal sensi-tivity in keratoconus patients. Cornea 2013;(7):899-902.
23. Martin XD, Safran AB. Corneal hypoesthesia. Surv Ophtalmol. 1988;33(1):28-40; erratum p.217.
24. Mitra T, Panagiotis A, Kallinikos NE, Andrew JM, Boulton RA. Corneal sensitivity is reduced and relates to the severity of neuropathy in patients with diabetes. Diabetes Care. 2007;(30):1895-7.
25. Nassaralla BA, Vieira DM, Machado ML, Figueiredo MN, Nassaralla JJ Jr. Corneal thickness changes during corneal collagen cross-linking with UV-A irradiation and hypo-osmolar riboflavin in thin corneas. Arq Bras Oftalmol. 2013;76(3):155-8.
26. Wollensak G, Aurich H, Pham D-T, Wirbelauer C. Hydration behavior of porcine cornea cross-linked with riboflavin and ultraviolet A. J Cataract Refract Surg. 2007;33(3):516-21.
27. Hafezi F, Mrochen M, Iseli HP, Seiler T. Collagen cross linking with ultraviolet-A and hypo-osmolar riboflavin solution in thin corneas. J Cataract Refract Surg. 2009;35(4): 621-24.
28. Wollensak G, Spoerl E, Reber F, Seiler T. Keratocyte cytotoxicity of riboflavin/UVA-treat-ment in vitro. Eye. 2004;18(7):718-22.

�� "SR�#SBT�0GUBMNPM����������������
0ċĂĀĂćúą�"ċčĂüąþ�
The influence of body position on Bielschowsky’s test
�ȱ��Ě�¹����ȱ��ȱ����³¨�ȱ��������ȱ�����ȱ�ȱ�����ȱ��ȱ�������� ��¢
CaRlos R. souza-dias1, mauRo goldChmit1,2, Fabio P. moRaes2, aRthuR JamPolsky3
INTRODUCTION The compensatory head tilt during certain oculomotor anomalies
has the goal of reducing hypertropia, avoiding diplopia, and main-taining fusion(1).
The forced head tilt difference means the difference in the magni-tude of vertical deviations when hypertropia is measured with the head tilted toward both shoulders; this primarily occurs in patients with superior oblique paresis and superior rectus contracture (Jam-polsky’s syndrome(2)). In 1985, David Robinson(3), after a mathematical analysis of his Robinson’s model of the oculomotor plant with regard to large vertical deviations in the head tilt test, concluded that only a contractured superior rectus muscle could account for such a large forced tilt difference in some patients with superior oblique palsy.
The conventional mechanical explanation for Bieslschowsky’s test(4) is based on the otolith static reflex, which is responsible for the counter-rolling of eyes induced by head tilting toward the shoulders. When the head is tilted toward the right shoulder, for instance, the right eye tends to incycloduct, which is induced by the otolith system,
ABSTRACTPurpose: To investigate the veracity of Jampolsky’s statement that Bielschowsky’s head tilt test is inverted if performed with the patient in the upside-down position and to interpret its neuromuscular mechanism.Methods: We present a series of 10 patients selected from a referred sample who were diagnosed with superior oblique paresis. Hypertropia was measured in the primary position, with the head erect and tilted toward both shoulders with the patient in the erect, supine, and upside-down positions. The last position was achieved by hanging the patient upside-down. Results: As expected, our results showed the veracity of Jampolsky’s statement. The forced head tilt difference was inverted or significantly decreased when the test was performed in the upside-down position. Moreover, in all patients, Bielschowsky’s phenomenon was neutralized in the supine body position, in which hypertropia with the head erect tended to vanish. In 3 patients, it disappeared completely. Conclusions: This study showed that, in patients with superior oblique paresis, differences in the extent of hypertropia in Bielschowsky’s test tended to vanish when the test was performed with the patient in the supine position and invert when it was performed with the patient in the upside-down position.
Keywords: Strabismus; Body positioning; Troclear nerve; Ophthalmoplegia
RESUMOObjetivo: Investigar a veracidade da suposição de Jampolsky de que o teste de in-clinação da cabeça de Bielschowsky inverte-se caso seja realizado com o paciente de cabeça para baixo, e tentar interpretar o mecanismo neuromuscular envolvido. Métodos: Apresentamos uma série de 10 pacientes portadores de paresia do oblíquo superior. Foi medida a hipertropia dos pacientes na posição primária do olhar e com a cabeça inclinada para cada um dos lados nas posições ereta, supina e de cabeça para baixo. Resultados: Como esperado, nossos resultados confirmaram a suposição de Jampolsky; além disso, e em todos os pacientes, o fenômeno de Bielschowsky foi neutralizado em posição supina. As diferenças da magnitude da hipertropia ao teste de Bielschowsky diminuiram significativamente ou inverteram-se quando o paciente foi testado de cabeça para baixo. Conclusões: Este estudo demonstrou que, nos pacientes com paresia do oblíquo superior, a hipertropia evidenciada pelo teste de Bielschowsky tende a desaparecer com o paciente na posição supina e a se inverter quando o teste é realizado com o paciente de cabeça para baixo.
Descritores: Estrabismo; Posicionamento do paciente; Nervo troclear; Oftal mo plegia
through the innervation of its intorsional muscles, namely the su-perior rectus and superior oblique muscles. These muscles are antagonists in vertical and horizontal actions; therefore, when they are simultaneously innervated, they compensate for each other and result in no vertical or horizontal eye movement. However, they are synergistic when it comes to torsion. When they are simultaneously innervated by right head tilting, as in the case of right superior oblique palsy, the superior rectus muscle overcomes the depressor action of the weakened superior oblique muscle and elevates the eye(5).
Jampolsky stated, in 1994(6), that if Bielschowsky’s test is perfor-med with the patient in an upside-down position, the forced tilt difference would give a mirror image, that is, an inverted one. This led to inte-resting speculations about the otolith mechanism and the muscular mechanics of the forced head tilt difference.
This study aimed to investigate the veracity of this statement and interpret the underlying neuromuscular mechanism. Patients with superior oblique paresis were selected, and the deviation with the head tilted to both sides was measured with the patient in the erect, supine, and upside-down positions.
Submitted for publication: May 29, 2013 Accepted for publication: October 23, 2013
Study conducted at Faculdade de Ciências Médicas da Santa Casa de Misericórdia de São Paulo, São Paulo, SP, Brazil.
1 Department of Ophthalmology, Faculdade de Ciências Médicas da Santa Casa de Misericórdia de São Paulo, São Paulo, SP, Brazil.
2 Instituto Cema, São Paulo, SP, Brazil.3 Smith-Kettlewell Eye Research Institute, San Francisco, California, United States of America.
Funding: This study was supported by a grant from the Smith Kettlewell Eye Research Institute.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Carlos R. Souza-Dia. Rua Cincinato Braga, 59 - Cj. 5 B2 - São Paulo (SP) - 01333-011 - Brazil - E-mail: [email protected]
Research Ethics Committee: Approved by the Comitê de Ética e Pesquisa of the Santa Casa de Misericórdia de São Paulo under the number 364/11.

4ĈĎēú�%ĂúČ�$3 �þč�úą�
��"SR�#SBT�0GUBMNPM����������������
METHODS This work was approved by the Ethics Committee of the Faculty
of Medical Sciences of the Santa Casa de Misericórdia of São Paulo under the number 364/11. After the procedure was explained to the subjects (or legal guardians for minors) and accepted by free will, informed consent was obtained.
Ten patients [8 unilateral and two asymmetric bilateral (Patients 7 and 10), Table 1] consecutively examined in the Santa Casa and CEMA hospitals who presented with the clinical picture of superior oblique paresis were prospectively examined. The mean age was 31.4 ± 15.3 years (9–52 years).
The data necessary for diagnosing unilateral superior oblique paresis included the following: hypertropia of the affected eye that increased on the contralateral side with the head tilted toward the ipsilateral shoulder and decreased on ipsilateral side with the head tilted toward the contralateral shoulder (Bielschowsky’s test), ex-cyclotropia, and a V-anisotropia. Asymmetric superior oblique paresis was diagnosed according to the criteria discussed by Souza-Dias in another paper(7).
For this research, we measured the deviations in the primary po sition with the head erect and maximally tilted to both shoulders, with the patient in the erect, supine, and upside-down positions. Ipsilateral superior rectus contracture was investigated during sur-gery with the forced duction test (“knife-edge” maneuver, proposed by Jampolsky in 1978(8)).
After external, anterior segment, and fundus examinations and refractometry, a thorough ocular motility examination was perfor-med, with special attention to the alternate prism and cover test in all positions of gaze and in the primary position with the head tilted toward both shoulders. All patients possessed 40” to 50” of stereoa-cuity, which was assessed using the Titmus Fly Test® (Titmus Optical, Petersburg, VI, USA), or were able to recognize the 3 figures on Lang’s test. All patients showed extorsion of the affected eye as diagnosed by the double Maddox test and, in some of them, fundoscopy.
The upside-down position was achieved in the 2 young patients by an adult hanging them by the legs and in the remaining 8 adults by utilizing a special slanting bed that was specifically built for this investigation (Figure 1).
In order to avoid misunderstanding, let us define 2 terms. Hyper-tropia of an eye indicates that the affected eye is deviated toward the top of the head, and hypotropia of an eye indicates that the affected eye is deviated toward the feet, regardless of the patient’s body position.
RESULTSIn all patients, the forced head tilt difference was neutralized or
tended to vanish when the test was performed with the patient in the supine position, while it was inverted or significantly decreased in magnitude when the patient was in the upside-down position.
As seen in table 1, there was a complete inversion (Patient 2) or an almost complete inversion (Patient 3) of the forced head tilt difference when the test was repeated with the patient in the upside-down position. In all the other patients, there was a clear tendency for inver-sion. In Patient 1, for instance, the left hypertropia with the head tilted toward the right shoulder increased from 8∆ to 25∆, thus increasing by 17∆, while that with the head tilted toward the left shoulder decrea-sed from 35∆ to 15∆, thus decreasing by 20∆. The forced tilt difference that measured 27∆ was reduced to 10∆, but in the opposite sense (it was inverted). Therefore, the total change was 37∆. In Patient 10, the hypertropia disappeared in the supine and upside-down positions.
When the test was repeated with the patients in the supine posi-tion, the forced head tilt difference tended to disappear in all patients. It was noteworthy that the hypertropia in the primary position ten-ded to vanish when tested with the head erect and the body in the supine position. In Patients 3 and 10, the hypertropia disappeared. In Patient 9, in these body and head positions, there was a tendency for inversion of Bielschowsky’s test, but the hypertropia in the primary position remained (it was only decreased).
The measurement of the forced head tilt difference in the 10 pa tients in the primary position; with the body erect, supine, and upside-down; and with the head erect and tilted toward both shoulders are listed in table 1.
DISCUSSIONIf the otolith mechanism is considered as the explanation for the
forced head tilt difference, it is not difficult to explain the disappearan-ce of the hypertropia when the patient is in the supine position. A probable explanation is that if the head is tilted toward the shoulders with the patient in this position, the hypertropia does not appear because the otoliths stimulate other areas inside the utricule; fur-thermore, the force G vector (gravity) does not change its relative di rection within the utricle with the change in head position. It is more difficult to explain the tendency for the decrease in the magni-tude of the hypertropia in the primary position with the patient in the supine position. Till date, no study regarding this phenomenon has been published. A possible mechanism is relaxation of all the
Figure 1. The method for measuring hypertropia with the patients in the upsidedown position. The boy is hung from the legs by an adult, while the adult is strapped in a slant stretcher designed for this purpose.

5āþ�ĂćÿąĎþćüþ�Ĉÿ�ûĈýĒ�ĉĈČĂčĂĈć�Ĉć�#ĂþąČüāĈĐČĄĒ�Č�čþČč
90 "SR�#SBT�0GUBMNPM����������������
cyclovertical muscles in this position. Its permanence, with only a small decrease in Patient 9, was probably caused by an ipsilateral superior rectus contracture.
However, in the upside-down position, the sense of the force G vector into the utriculi is inverted, and it is not known if there is such an inversion mechanism in the utriculi. The otoliths stimulate an opposite area. Furthermore, considering the mechanical reasoning for the forced head tilt difference described above, with the patient in the upside-down position, for the right eye to move toward the, the case of a right superior oblique palsy, there would have to be an imbalance of the vertical forces between the ipsilateral inferior rectus and inferior oblique of this eye (a weakness of the inferior oblique), for the inferior rectus to overcome its elevating action, and depress the eye, which did not exist in this case. On the contrary, in patients with superior oblique palsy, there is generally an ipsilateral inferior oblique overaction that can elevate the eye (to move toward the top of the head) instead of depressing it (to move toward the feet).
It is noteworthy that Wong et al.(9) found different data. In patients diagnosed with skew deviation, hypertropia decreased by >50% when measurements performed with the head erect and in the su-pine position were compared. This was in contrast with the findings
Table 1. Measurement of hypertropia in the 3 head positions of Bielschowsky’s test (erect and tilted toward each of the shoulders), with the patients in the erect, supine, and upside-down positions
Patients
Bielschowsky’s test
Body position
Erect Supine Upside-down
Head position
Right Erect Left Right Erect Left Right Erect Left
01 -8 -25 -35 -25 -15
02 -3 -25 -5 0 +25 -3
03 +25 +5 0 0 0 0 0 +20
04 0 -10 -12 -2 -6 -12 -3 -5
05 +25 +25 +6 +3 +3 +3 +12 +20 +20
06 -3 -4 -15 -6 -5 -5 -12 -10 -13
07 +15 +8 -6 +5 0 +7 0 +2 +5
08 -4 -15 -15 -6 -5 -5 -12 -12 -3
09 0 -22 -40 -12 -15 -25 -15 -12 0
10 +15 +8 -4 0 0 0 0 0 0
The measurements are in prism diopters. The symbol “+” indicates right hypertropia, while the symbol “-” means left hypertropia. The affected eye is indicated by the side of the larger hypertropia in Bielschowsky’s test in the erect body position.
for patients with superior oblique palsy, in whom this decrease was smaller or absent. In all 8 patients who underwent measurements in the supine position, there was a decrease or disappearance in the forced head tilt difference; the hypertropia in the primary position disappeared in 3 and decreased in the remaining, except in Patient 9 (Table 1).
In conclusion, the behavior of the cyclovertical extraocular mus-cles during static head tilt toward the shoulders with the patient in the upside-down and supine positions remains to be elucidated. This lack of knowledge suggests, as pointed out by Jampolsky in 1994(6), that the neurophysiology of the static vestibulo-ocular reflexes and clinical head tilt test interpretations should be re-examined. The findings also explain the fact that the so-called Parks’ test frequently fails to diagnose diseases of the other cyclovertical muscles other than superior oblique palsy, as pointed out by Bicas & De Sordi(10), Prieto-Díaz & Souza-Dias(11), and Souza-Dias & Goldchmit(12).
ACKNOWLEDGEMENT The authors acknowledge Dr. Roberto Mitiaki Endo for his assis-
tance in the submission of this work to the Ethics Committee.
REFERENCES 1. Khawan E, Scott AB, Jampolsky A. Acquired superior oblique palsy. Arch Ophthalmol.
1967;77(6):761-8. 2. Khawam E, Ghazi N, Salti H. “Jampolsky Syndrome”: superior rectus overaction-con-
tracture syndrome: prevalence, characteristics, etiology and management. Binocul Vis Strabismus Q. 2000;15(4):331-42.
3. Robinson D. Bielschowsky head tilt test II – Quantitative mechanics of the Bielschowsky head tilt test. Vis Rev. 1985;25(12):1983-8.
4. Bielschowsky A. Lectures on motor anomalies. Hannover: Dartmouth College Public; 1943. p.73.
5. von Noorden GK, Campos E. Binocular vision and ocular motility. 6th ed. St. Louis: Mosby; 2002. p.417.
6. Jampolsky A. A new look at the head tilt test. In: Fuchs AF, Brandt TH, Buttner U, Zee DS editors. Contemporary ocular motor and vestibular research: a tribute to David A. Robinson. Stuttgart, Ger: Thieme Verlag; 1994. p.432-9.
7. Souza-Dias C. Asymmetrical bilateral paresis of the superior oblique muscle. J-AAPOS. 2007;11(1):12-6.
8. Jampolsky AS. Surgical leashes and reverse leashes in strabismus surgical manage-ment. In: Symposium on Strabismus. Transactions of the New Orleans Academy of Ophthalmol. St. Louis: Mosby; 1978. p.244.
9. Wong AM, Colpa L, Chandrakumar M. Ability of an upright-supine test to differen-tiate skew deviation from other vertical strabismus causes. Arch Ophthalmol. 2011; 129(12):1570-5.
10. Bicas HE, De Sordi GB. Contradições nos resultados de testes diagnósticos de dese-quilíbrios verticais. In: Anais do XVI Congresso Brasileiro de Oftalmologia, Campinas (SP); 1971. Conselho Brasileiro de Oftalmologia; 1971. p.132.
11. Prieto-Díaz J, Souza-Dias C. Estrabismo. Buenos Aires, Ediciones Científicas Argenti-nas; 2005. p.324.
12. Souza-Dias C, Goldchmit M. Os estrabismos: teoria e casos comentados. Rio de Janeiro: Cultura Médica; 2011. p.289-91.

91"SR�#SBT�0GUBMNPM���������������
0ċĂĀĂćúą�"ċčĂüąþ�
Optical and nonoptical aids for reading and writing in individuals with acquired low vision
��¡Ç����ȱà������ȱ�ȱ�¨�ȱà������ȱ��ȱ�������ȱ�ȱ�������ȱ��ȱ�������ȱ���ȱ���¡�ȱ���¨�ȱ���������
mayla myRina bianChim monteiRo1, Rita de Cássia ietto montilha1, keila miRiam monteiRo de CaRvalho1, maRia elisabete RodRigues FReiRe gasPaRetto1
INTRODUCTIONVision plays an important role in human development because
it stimulates and directs human movements and actions. It is the agent’s motivation to trigger the acquisition of skills, and it allows capture of the environment quickly and efficiently. Vision is the sense that rapidly unifies sensations (tactile and auditory) and sets a direction in relation to the other part(1).
The relationship with the outside world is accomplished primarily through vision; therefore, ocular problems can cause serious adverse effects on learning and socialization(2).
According to the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10) by the World Health Organization (WHO), an individual is considered to have low vision if the visual acuity with optical correction in the better eye is <20/70 (0.3) and >20/400 (0.05) or if the visual field is less than 20° in the better eye with the best optical correction possible(3).
Low vision is characterized by a significant change in the functio-nal capacity of vision that results in isolation and is caused by a single
ABSTRACTPurpose: To evaluate the use of optical and nonoptical aids during reading and writing activities in individuals with acquired low vision. Methods: This study was performed using descriptive and cross-sectional surveys. The data collection instrument was created with structured questions that were developed from an exploratory study and a previous test based on interviews, and it evaluated the following variables: personal characteristics, use of optical and nonoptical aids, and activities that required the use of optical and nonoptical aids. Results: The study population included 30 subjects with acquired low vision and visual acuities of 20/200-20/400. Most subjects reported the use of some optical aids (60.0%). Of these 60.0%, the majority (83.3%) cited spectacles as the most widely used optical aid. The majority (63.3%) of subjects also reported the use of nonoptical aids, the most frequent ones being letter magnification (68.4%), followed by bringing the objects closer to the eyes (57.8%). Subjects often used more than one nonoptical aid. Conclusions: The majority of participants reported the use of optical and nonopti-cal aids during reading activities, highlighting the use of spectacles, magnifying glasses, and letter magnification; however, even after the use of these aids, we found that the subjects often needed to read the text more than once to understand it. During writing activities, all subjects reported the use of optical aids, while most stated that they did not use nonoptical aids for such activities.
Keywords: Vision, low/rehabilitation; Reading; Visually impaired individuals; Lan-guage; Handwriting; Audiovisual aids
RESUMOObjetivo: Avaliar o uso de auxílios ópticos e não ópticos na leitura e na escrita de pessoas com baixa visão adquirida. Métodos: Realizou-se estudo descritivo, tipo transversal. O instrumento de coleta de dados continha questões estruturadas, desenvolvidas em estudo exploratório e teste prévio e foi aplicado por entrevista, onde foram investigadas as seguintes variáveis: características pessoais, uso de auxílios ópticos e não ópticos, atividades para as quais utiliza auxílios ópticos e não ópticos. Resultados: A população foi composta por 30 sujeitos com baixa visão adquirida, com acuidade visual entre 20/200 a 20/400. A maioria dos sujeitos declarou fazer uso de algum tipo de auxílio óptico (60,0%). Desses 60,0%, a maioria (83,3%) citou os óculos como o auxílio óptico mais usado. A maioria (63,3%) dos sujeitos relatou fazer uso de auxílios não ópticos e os mais citados foram a ampliação de letras (68,4%), seguidos da aproximação dos objetos aos olhos (57,8%). Os sujeitos ressaltaram o uso de mais de um auxílio não óptico. Conclusão: A maioria informou utilizar os auxílios ópticos e não ópticos nas atividades de leitura, evidenciando o uso de óculos e da lupa manual, assim como da ampliação de letras, mas mesmo utilizando tais auxílios verificou-se que os sujeitos necessitavam ler o texto mais de uma vez para terem a compreensão do mesmo. Para a realização das atividades de escrita, a totalidade dos sujeitos declarou utilizar os auxílios ópticos, enquanto que a maioria declarou não utilizar auxílios não ópticos nessas atividades.
Descritores: Baixa visão/reabilitação; Leitura; Pessoas com deficiência visual; Lin-guagem; Escrita manual; Recursos audiovisuais
or multiple factors such as significant visual impairment, a significant decrease in the visual field, and changes in color vision and/or con-trast sensitivity that interfere with or limit visual performance(4). It also can be described as any degree of visual impairment that causes disability and a decrease in visual performance(5).
While performing activities of daily living, there is a need to utilize reading and writing; these activities can be greatly affected by visual loss because the eyes are necessary to perform these.
Improvement in the visual performance of an individual with low vision can be achieved through the use of resources such as assistive te-chnology. Assistive technology is an interdisciplinary area of knowledge that includes products, resources, methodologies, strategies, practi-ces, and services that work to promote the functionality related to the activity and participation of individuals with disabilities, inabilities, or decreased mobility, and it can help those that are seeking autonomy, independence, quality of life, and social inclusion(6).
Assistive technology resources may be optical, nonoptical, or electronic. These resources can lead to a decrease in functional losses in patients with low vision(7).
Submitted for publication: June 12, 2012 Accepted for publication: October 23, 2013
Study conducted at Center of Studies and Researches in Rehabilitation (CEPRE), College of Me dical Sciences (FCM), University of Campinas (UNICAMP), Campinas, SP, Brazil.
1 Faculdade de Ciências Médicas, Universidade Estadual de Campinas (UNICAMP), Campinas, SP, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Mayla M. B. Monteiro. Av. Adolfo Lutz, s/n - Campinas (SP) - 13083-887 - Brazil - E-mail: [email protected]
Dissertação de Mestrado. O projeto foi aprovado pelo Comitê de Ética em Pesquisa da Faculdade de Ciência Médicas da Universidade Estadual de Campinas (Protocolo de Projeto: 091/2008).

0ĉčĂüúą�úćý�ćĈćĈĉčĂüúą�úĂýČ�ÿĈċ�ċþúýĂćĀ�úćý�ĐċĂčĂćĀ�Ăć�ĂćýĂďĂýĎúąČ�ĐĂčā�úüĊĎĂċþý�ąĈĐ�ďĂČĂĈć
92 "SR�#SBT�0GUBMNPM���������������
Optical aids include one or more lenses that are placed between the eyes and the object to promote the magnification or enlarge-ment of the retinal image. The optical aids can be as simple as a glass lens to better see the details of a figure or as complex as a sophistica-ted telescope that can be used for far and near vision(8).
Nonoptical aids are simple features that can increase visual reso-lution. These features do not involve the use of a magnifying lens to improve visual function, but they can be used in addition to optical devices or may possibly replace them in some instances. Some exam-ples include filter lenses, lighting, marker pens, magnification of ma-terials, and changes in contrast (dark background and light object)(5).
Language is a way to communicate and express feelings, ideas, and actions. It is a process of dialogue that takes place in the social practices of different groups at different times in their history and an activity and a mental operation that involves the construction of meaning(9).
This emphasizes the importance of the use of optical and no -noptical aids to help individuals with low vision in performing reading and writing activities.
This study aimed to verify the use of optical and nonoptical aids to assist in the performance of reading and writing activities by indi-viduals with low vision.
METHODSThis was a descriptive and cross-sectional study. To construct the
data collection instrument, we used features of exploratory research that presented qualitative and contextual results(10).
The population comprised 30 subjects with acquired low vision who attended the Rehabilitation Program for Adolescents and Adults with Visual Impairment conducted by the Center of Studies and Re-searches in Rehabilitation (CEPRE), College of Medical Sciences (FCM), University of Campinas (UNICAMP), Brazil. The inclusion criteria were as follows: subjects aged >18 years who were divided into young adults (18-39 years), adults (40-59 years), and elderly (>60 years); literacy; acquired low vision; and participation in the Rehabilitation Group of CEPRE during the period between June and December 2008.
The variables selected were personal characteristics, the use of optical and nonoptical aids, and participation in activities that requi-red the use of optical and nonoptical aids.
The data collection instrument was created using structured questions developed from an exploratory study, a previous test based on interviews, and reading and writing activities associated with the use of optical and nonoptical aids.
During the planning stage, this study provided data that reflected the knowledge and opinions of individuals with acquired low vi-sion with regard to reading and writing activities. Therefore, it was possible to adjust the perceptions of the researcher to match the perceptions of the subjects.
The first phase of the exploratory study involved individual inter-views with 3 subjects with acquired low vision, which included open questions based on the above variables, and reading and writing activities.
On the basis of the results obtained in the first exploratory stage, the second phase involved the construction of a semistructured measuring instrument. The questions were organized to respect the order of content and grouped according to the study variables, while maintaining fidelity to the language used by the subjects. With the data obtained in this second phase, it was possible to build the instrument with structured questions.
The previous test was intended to improve the instrument and gradually integrate stepwise information into the exploratory study. Proof was needed to ensure the reliability and validity of data obtai-ned during the research(11).
The previous test was performed by applying the structured questionnaire to 3 subjects with acquired low vision who had not participated in the previous steps (the third phase of the exploratory study). At the end of this phase, the questions in the quiz needed to be reviewed and answered.
The researchers applied the previous test to subjects with low vision included in CEPRE. This population was similar to the popula-tion that was involved in the exploratory study, which was excluded from the final population.
The fourth and final stage of the exploratory study was comple-ted by re-applying the questionnaire to 2 other subjects with acquired low vision. No changes were required; therefore, the instrument for data collection was complete.
Data collection was performed using the structured questionnaire administered to subjects who agreed to participate in the study by signing an informed consent statement.
After collecting the data, the open questions were categorized and grouped and the closed questions were quantified and tabulated. The responses were statistically analyzed using EPI INFO version 6.0.
RESULTSThe study population comprised 30 subjects with acquired low
vision and visual acuities of 20/80-20/1000. All subjects were conside-red to have severe visual impairment, and 60% were males. The age range was 18-73 years, with an average age of 38 years.
With regard to educational qualification, 33.5% subjects had re-ceived primary education, 23.3% had completed elementary school, 20.0% had completed secondary school, 16.6% had completed high school, and 6.6% had received university education.
The age of onset of the eye problems ranged from 10 to 69 years, and the average age of onset was 29 years. The duration of participa-tion in the Group Rehabilitation CEPRE ranged from 1 to 8 months, with an average duration of 4.5 months.
Table 1 shows that the majority (60.0%) of subjects reported the use of some optical aids. Of this 60.0%, the majority (83.3%) cited that lenses (regular spectacles) were the most commonly used. It also shows the activities during which the subjects used these optical aids, highlighting the activities of reading, cleaning, cooking, and shopping (50.0%).
Table 1. Use of optical aids by subjects included in the rehabi litation program for adolescents and adults with visual impairment (CEPRE-FCM-UNICAMP; Campinas, 2008)Optical aids N %
N=30
Declare use 18 60.0
Claim ignorance 12 40.0
Types of optical aids* N=18
Spectacles 15 83.3
Telescope system 04 22.1
Manual magnifier 01 05.3
Sun glasses 01 05.3
Activities using optical aids* N=18
Reading 09 50.0
Cleaning, cooking, shopping 09 50.0
Watching TV 05 27.7
Writing 01 05.3
Orientation and mobility 01 05.3
*= multiple answers.N= number of subjects; %= percent.

.ĈćčþĂċĈ�..# �þč�úą�
93"SR�#SBT�0GUBMNPM���������������
Table 2 shows that the majority (63.3%) of subjects reported the use of nonoptical aids. The most frequent nonoptical aids were letter magnification (68.4%), followed by bringing objects closer to the eyes (57.8%). The subjects often used more than one nonoptical aid.
The activities during which the participants reported the use of nonoptical aids have been listed In table 2, including reading (73.6%), writing (21.0%), and watching television (10.5%).
Table 3 shows that the majority (55.5%) of subjects used optical aids for easier reading. The most common aids used were spectacles (90.0%), followed by manual magnifying lenses (10.0%).
DISCUSSIONThe study of the characteristics of visual impairment, featuring
individuals with blindness or low vision and their opinions and ex-pectations during the rehabilitation process, is fundamental to plan-ning their rehabilitation and making it compatible with the patient’s condition(11).
Researchers believe that the cognitive science of reading and writing has much to contribute to research in the field of visual im-pairment because both reading and writing utilize the eyes(12).
This study verified that the prevalence of low vision was greater among men (60.0%) than among women. Other authors have also found larger populations of men with low vision(13,14).
The age of onset of visual impairment varied between 10 and 69 years in this study, with the mean age of onset being 29 years. In a study by Montilha(15) conducted in CEPRE/FCM/UNICAMP the mean age of patients was 27.9 years, which was close to that in our study. Both studies were conducted in CEPRE; this probably affected the age of the populations.
Most subjects (60.0%) reported the use of some optical aids to perform near and far activities, and the activities that were most often cited were reading, cleaning, cooking, and shopping. Of those 60.0%, the majority (88.8%) reported the use of spectacles and lenses to perform close manual activities (Table 1). Carvalho et al.(16) reported similar findings in their study, where 60% subjects reported the use of optical aids. These patients achieved considerable improvement in visual acuity when they used prescriptions for near distance vision in accordance with their visual needs.
Spectacles allow for better vision during near tasks by providing a greater visual field, thus facilitating the performance of activities of daily living (ADL) and ambient visual processing (AVP). Telescope systems can assist with distance tasks such as watching television, orientation, mobility and shopping, locating industries and stores, and finding boxes. Manual loupes are designed to help subjects with low vision to perform close, short-term tasks.
The selection of such aids is based on the patient’s visual status and the visual and activity needs of the individual with low vision. After the selection of optical aids, adaptation is very important. If the patient is trained, the aids will be used appropriately(17).
For the activities of cleaning and cooking, the manual magnifying glass can be used to identify a product or a food; however, the subject would need to be careful when approaching the stove for safety.
According to Bonatti el al.(18), optical aids can assist and improve the vision quality in subjects and can make the more commonly performed activities (reading, cleaning, cooking, shopping) easier. The findings of these authors agreed with those of our research; reading, cleaning, cooking, and shopping (50.0%) were cited as the activities during which the subjects used optical aids. In this study, we also determined that the use of optical aids made it easier to perform such activities.
Overall, the experiences with daily life activities showed that most subjects with visual impairment experienced difficulties before the visual practice of ADL/AVPs. The use of optical aids is effective in conducting these activities and can improve the visual performance of subjects with their use.
To facilitate and promote the frequent use of optical aids, sub-jects should always use them for tasks; the periods of use must be serialized and short in order to avoid visual and physical fatigue. It is important for the physician or the rehabilitation team to explain the purposes of the aids to enable the patient to make the best use of his or her residual vision(16).
Sacks(19) mentioned that the use of optical aids can increase the self-esteem of subjects with low vision. The benefits of using these aids include the development of a sense of independence (when the subject can have access to reading materials printed in the daily envi-ronment, he or she becomes independent), an increase in the sense of responsibility (in purchasing real visual information, he or she realizes their potential and feels safe and responsible in other situations), an improvement in identification of the environment, the development of a sense of competence (because the subject has visual control over the environment), and the feeling of great pleasure with their vision quality.
The use of optical aids does more than improving visual function. It also impacts the emotional side of the subject. This is very impor-tant for effective participation in the rehabilitation process and can improve the quality of life and social inclusion. The use of optical aids allows patients to use their residual vision and preserve their visual function(16).
Table 2. Use of nonoptical aids by subjects included in the rehabilitation program for adolescents and adults with visual impairment (CEPRE-FCM-UNICAMP; Campinas, 2008)Nonoptical Aids N %
N=30
Declare use 19 63.3
Claim ignorance 11 37.6
Types of nonoptical aids* N=19
Letter magnification 13 83.3
Bring the objects closer to the eyes 11 58.0
Lighting 06 31.5
Telescope 04 21.0
Contrast 03 15.7
Support for reading and writing 01 05.3
Activities using nonoptical aids* N=19
Reading 14 73.6
Writing 04 21.0
Watch TV 02 10.5
Computer use 01 05.3
Crochet, sewing 01 05.3
*= multiple answers.N= number of subjects; %= percent.
Table 3. Use of optical aids for easier reading by subjects included in the rehabilitation program for adolescents and adults with visual impairment (CEPRE-FCM-UNICAMP; Campinas-SP, 2008)Optical aids N %
N=18
Use 10 55.5
No use 08 44.5
Type of optical aids* N=10
Spectacles 09 90.0
Handheld magnifier 01 10.0
*= multiple answers.N= number of subjects; %= percent.

0ĉčĂüúą�úćý�ćĈćĈĉčĂüúą�úĂýČ�ÿĈċ�ċþúýĂćĀ�úćý�ĐċĂčĂćĀ�Ăć�ĂćýĂďĂýĎúąČ�ĐĂčā�úüĊĎĂċþý�ąĈĐ�ďĂČĂĈć
�� "SR�#SBT�0GUBMNPM���������������
In a study, conducted in rehabilitation programs, that determined rehabilitation strategies that were most suitable for each subject, Lu-cas et al.(15) found that the most frequent goal of the use of optical aids was to improve performance of reading and writing activities (44.5%).
The prescription of optical aids depends to the subject’s visual status and can generally improve visual performance, depending on the eye disease, level of visual acuity, and beliefs of the subject in relation to eye health. A study conducted in England showed the follow-up of 168 patients who were prescribed optical aids for low vision, received orientation for the use of nonoptical aids, and were followed for 6 consecutive months. The level of performance in their reading activities improved significantly, with 88.0% subjects beginning to read letters printed in newspapers after receiving the treatment mentioned(20).
Most (63.3%) subjects in this study reported the use of nonoptical aids. The nonoptical aids most frequently used were letter magnifi-cation (68.4%), followed by bringing the objects closer to the eyes (57.8%). Reading activities (73.6%) were the most frequently mentio-ned activities during which nonoptical aids were used, followed by writing activities (21.0%; Table 2).
The nonoptical aids mentioned in this study (magnification, bringing the object closer to the eyes, lighting, telescope systems, contrast, support for reading and writing) were largely used for the most frequently cited activities of reading and writing. Nonoptical aids are easy to use; however, some can be expensive. These aids were available for most subjects who participated in this study.
Nonoptical aids can be used alone or in conjunction with optical aids in order to promote the best adaptation and functional use(21). As a matter of fact, the combination used is often indicated in activities such as reading and writing because the use of all available resources can make it easier for the subject(22).
Table 1 shows that 60% subjects reported the use of optical aids for these activities. Of these, 55.5% reported the use of these aids for easier reading. Of the 55.5% who used optical aids for easier reading, 90.0% reported the use of spectacles and 10.0% reported the use of manual magnifiers.
The spectacles are used with a high frequency because of their convenience. After placing them on the face, the subject needs to find the best position for reading; spectacles can also be used in con-junction with nonoptical aids. With aids such as manual magnifying lenses, the speed of reading can be slowed down because the subject can explore only a small piece of text at a time; the subject also has to use one hand to hold the lens itself(22). With handheld magni fiers, the subject needs to do two things at the same time: hold the handheld magnifier and focus the eyes on what he or she is reading.
Reading involves the integration of multiple factors such as the previous experience of the subject, skill, and neurological functioning. During reading, different eye movements are required; the saccades that bring the eyes from left to right and the oblique saccades that lead the eye from one line of the text to the next. Additionally, the angle of vergence of the two optical axes must be adjusted to the distance from the reading material(23).
According to Cagliari(24), the skill of writing in adults is so inte-grated into everyday life that most of the time, its importance and usefulness in life maintenance and survival may not be recognized. In a world built by the written word, individuals who can see may not reflect on the difficulties faced by individuals with visual impairments who are exposed daily to reading and writing tasks.
It was found that, despite the use of nonoptical aids by all subjects during writing activities, they reported the use of letter magnification and bringing the objects closer to their eyes to better perform their activities (Table 2). Individuals with low vision can write even without the use of optical and nonoptical aids, although they most often do not read what they write. This difficulty can be mini-mized by the use of nonoptical aids such as the expansion of (own) words and bringing objects closer to the eyes.
The most important way to acquire knowledge, even during this era of the internet and in this virtual world, is still the written
language. Reading and writing is an essential requirement for an in-dividual to participate effectively in the society they live in and to be a conscientious citizen.
CONCLUSIONSThe majority of subjects reported the use of optical and no-
noptical aids during reading activities and highlighted the use of spectacles, magnifying lenses, and the manual expansion of words.
To perform the activities of writing, all subjects reported the use of optical aids, while most said that they did not use nonoptical aids during such activities
Even while using these aids, it was found that the subjects needed to read the text more than once to understand it.
REFERENCES 1. Sanches PA. Deficiências visuales y psicomotricidade: teoria y pratica. Organización
Nacional de Ciegos Españoles. 1994. p.255. 2. Alves MR, Kara-Jose N. O olho e a visão: o que fazer pela saúde ocular das nossas
crianças. Rio de Janeiro: Vozes; 1996. 3. World Health Organization. Consultation on development of standards for characteriza-
tion for vision loss and visual functioning [Internet]. Geneva: WHO/PBL; 2003. [cited 2013 Dec 21]. Available from: http://whqlibdoc.who.int/hq/2003/WHO_PBL_03.91.pdf?ua=1
4. Bruno MM. A inclusão da criança com baixa visão na educação infantil. In: Masini EF, Gasparetto ME. Visão subnormal: um enfoque educacional. São Paulo: Vetor; 2007. p.84.
6. Montilha RC, Temporini ER, Nobre MI, Gasparetto ME, Kara-Jose N. Utilização de recur-sos ópticos e equipamentos por escolares com deficiência visual. Arq Bras Oftalmol. 2006;69(2):207-11.
7. Brasil. Ministério da Justiça. CORDE. Comitê de Ajudas Técnicas. Ata VII. Brasília: MJ. [citado 2009 Ago 5]. Disponível em: http://www.mj.gov.br/sedh/ct/corde/dpdh/corde/comite_at.asp
8. Brito PR, Veitzman S. Causas de cegueira e baixa visão em craianças. Arq Bras Oftalmol. 2000:63(1):49-54.
9. Thylefors B, Négrel AD, Pararajasegaram R, Dadzie Ky. Global date on blindness. Bull World Health Organ. 1995;73(1):115-20.
10. Oliveira LL. Uma possibilidade de intervenção psicopedagógica no processo dialéti-co de mediação entre o sujeito que aprende e o objeto do conhecimento. In: Santos MT, Navas AL. Distúrbios de leitura e escrita: teoria e prática. São Paulo: Manole; 2002. p.169-90.
11. Piovesan A, Temporini ER. Pesquisa exploratória: procedimento metodológico para o estudo de fatores humanos no campo da saúde pública. Rev Saúde Pública. 1995; 29(4):318-25.
12. Temporini ER. Pesquisa de oftalmologia em saúde pública: considerações metodo-lógicas sobre fatores humanos. Arq Bras Oftalmol. 1991;54(6):279-81.
13. Corn Al, Wall RS, Jose RT, Bell JK, Wilcox K, Perez A. An initial study of reading and comprehension rates for students who received optical devices. J Vis Impair Blind. 2002;96(5):322-33.
14. Montilha RC. O atendimento de terapia ocupacional com o adulto portador de cegueira adquirida. Sinopse de Oftalmologia. 2000;2(1):24-5.
15. Lucas MB, Leal MO, Tavares SS, Barros EA, Aranha ST. Condutas reabilitacionais em pacientes com baixa visão. Arq Bras Oftalmol. 2003;66(1): 77-82.
16. Montilha RC, Temporini ER, Kara-Jose N, Nobre MI. Deficiência visual: características e expectativas da clientela de serviço de reabilitação. Rev Ciênc Méd (Campinas). 2000;9(3):123-8.
17. Carvalho KM, Monteiro GB, Isaac CR, Shiroma LO, Amaral MS. Causes of low vision and use of optical aids in the elderly. Rev Hosp Clin Fac Med Sao Paulo. 2004;59(4):157-60.
18. Burman-Lindelow P. Magnificação e auxílios ópticos em baixa visão. In: Veitzman S. Visão subnormal. Rio de Janeiro, Cultura Médica; 2000. p.111-22.
19. Bonatti FAS, Bonatti JA, Sampaio MW, Haddad MA, Souza PR, Kara-Jose N. [Evaluation of patients using an innovative low-vison aid]. Arq Bras Oftalmol. 2008;71(3):385-8. Portuguese.
20. Sacks SZ. Psychological and social implications of low vision. In: Corn AL, Koenig AJ. Foundation of low vision: clinical and functional perspective. New York: American Foundation for the Blind press; 1966. p.26-42.
21. Margrain TH. Helping blind and partially sighted people to read: the effectiveness of low vision aids. Br J Ophthalmol. 2000;84(8):919-21.
22. Haddad MAO, Sampaio MW. Estudo da acuidade visual e da velocidade de leitura na baixa visão. In: Sampaio MW, Haddad MA, Filho HA, Siaulys MO, organizadores. Baixa visão e cegueira: os caminhos para a reabilitação, a educação e a inclusão. Rio de Janeiro: Cultura Médica; 2010. p.79-96.
23. Monteiro MM, Montilha RC, Gasparetto ME. Atenção fonoaudiológica e a linguagem escrita de pessoa com baixa visão: estudo exploratório. Rev Bras Educ Esp. 2011;17(1):121-36.
24. Castro CT. Método de avaliação da acuidade e velocidade de leitura- Tabela MNREAD. In: Ventura OL, Travassos SB, Silva AO, Dolan MA. Dislexia e distúrbios de Aprendiza-gem. Rio de janeiro: Cultura Medica; 2012. p.175-82.
25. Cagliari CL. Alfabetização & Lingüística. 10a ed. São Paulo: Sapione; 2001.

��"SR�#SBT�0GUBMNPM���������������
0ċĂĀĂćúą�"ċčĂüąþ�
Vision-related quality of life in patients after ocular penetrating injuries
Qualidade de vida relacionada à visão em pacientes após ferimentos oculares penetrantes
haRun yüksel1, Fatih m. tüRkCü1��08+$00('�û$+,11, yasin ÇinaR1, abdullah k. Cingü1, zeyneP ÖzkuRt1, yasin bez2��ú+6$1�d$d$1
INTRODUCTIONOcular trauma, one of the most common causes of visual loss and
impairment, can contribute considerably to a decreased quality of life (QOL). Among the types of ocular trauma, ocular penetrating injuries (OPI) are the leading cause of unilateral vision loss. In the United Sta-tes, the incidence of OPI was reported to be 3.81 per 100,000 persons. Many of these injuries are preventable(1).
OPI lead to varying degrees of vision loss, depending on the complications, location, and size of the injury. The majority of people who suffer OPI are young individuals(2). Therefore, loss of vision and visual prognosis is more important for a longer life expectancy. Ocular pathology in young patients does not only affect visual acuity (VA) but also affects occupational and social functions(3). In the practice of ophthalmology, visual function tests, such as visual field analysis, do not provide information about the psychological consequences of decreased vision and QOL(4,5). To the best of our knowledge, no published study has examined the impact of OPI on QOL.
In our study, we used the National Eye Institute 25-Item Visual Function Questionnaire (NEI VFQ-25) and the 36-Item Short Form Health Survey (SF 36) to better understand the impact of OPI on QOL. In previous studies, decreases in visual acuity affected NEI VFQ-25
ABSTRACTPurpose: To measure and investigate visual functioning and health-related quality of life (QOL) in patients after ocular penetrating injuries (OPI). Methods: Fifty-four adult patients with OPI and 26 healthy control subjects were enrolled in the study. The National Eye Institute Visual Functioning Questionnaire (NEI VFQ-25) and the 36-Item Short Form Health Survey (SF 36) were administered. Sociodemographic and clinical data also were collected. The primary outcome measures were comparisons and multivariate analysis among groups for the NEI VFQ-25 and SF 36 subscale scores. Results: All NEI VFQ-25 scores, except general health, were significantly lower in the OPI group than those in the control group. All SF 36 scores were significantly lower in the OPI group than in the control group. The NEI VFQ-25 subscale item scores showed no significant differences with respect to age, educational level, or visual acuity in the injured eye. The SF 36 subscale item scores revealed no significant differences according to gender or educational level. Conclusions: Patients with OPI have increased psychological symptoms and lower levels of QOL than healthy control subjects have. Deteriorations in QOL should be kept in mind when managing patients with OPI.
Keywords: Eye injuries, penetrating; Quality of life; Questionnaires
RESUMOObjetivo: Medir e investigar a função visual e a qualidade de vida relacionada à saúde (QOL) em pacientes após ferimentos ocular penetrantes (OPI). Método: Cinquenta e quatro pacientes adultos com OPI e 26 indivíduos saudáveis (controles) foram incluídos no estudo. O questionário de função visual do National Eye Institute (NEI VFQ-25) e a avaliação curta de 36 itens (Short Form Health Survey - SF 36) foram administrados. Dados sociais, demográficos e clínicos também foram coletados. As comparações e análise multivariada entre os grupos para as subescalas do NEI VFQ-25 e do SF 36 foram consideradas como resultados primários. Resultados: Todos os índices do NEI VFQ-25, exceto saúde geral, foram significati-vamente menores no grupo OPI do que aqueles no grupo controle. Todos os índices do SF 36 foram significativamente menores no grupo OPI do que no grupo controle. Os índices das subescalas do NEI VFQ-25 não apresentaram diferenças significativas em relação à idade, escolaridade, ou acuidade visual no olho ferido. Os índices das subescalas do SF 36 não revelaram diferenças significativas de acordo com o nível de escolaridade ou sexo. Conclusões: Pacientes com OPI apresentaram sintomas psicológicos aumentados e níveis mais baixos de qualidade de vida que os indivíduos saudáveis. Deteriorações na qualidade de vida devem ser consideradas ao gerenciar pacientes com OPI.
Descritores: Ferimentos oculares penetrantes; Qualidade de vida; Questionários
and SF 36 scores(6). NEI VFQ-25 was developed to assess a patient’s perception of QOL and visual function, and has been used to assess the quality of vision in retinal vein occlusion(7), diabetic retinopathy(8), glaucoma(9), and after ocular surgery(4,5). SF 36 evaluates the effect of overall health on QOL(10).
Here, we report vision-related QOL (VR-QOL) and health-related QOL (HR-QOL) in a population of patients with OPI using NEI VFQ-25 and SF 36 questionnaires. To the best of our knowledge, this is the first study to measure VR-QOL and HR-QOL in patients with OPI.
METHODSInstitutional review board approval was obtained through the
university ethics committee, and the study was conducted in com-pliance with the Declaration of Helsinki. Written informed consent was obtained from the participants. This prospective study enrolled 54 patients with OPI who were scheduled for vision care at the De-partment of Ophthalmology. Patients were enrolled in the study if they were aged ≥18 years, at least 6 months into the clinical course after the injury (to achieve relatively stable results of visual outcomes), and had no other systemic or ocular disease that could affect vision.
Submitted for publication: November 19, 2013 Accepted for publication: January 3, 2014
Study conducted at Dicle University Faculty of Medicine, Diyarbakir, Turkey.1 Department of Ophthalmology, Dicle University Faculty of Medicine, Diyarbakir, Turkey.2 Department of Psychiatry, Dicle University Faculty of Medicine, Diyarbakir, Turkey.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: +DUXQ�<�NVHO��'LFOH�hQLYHUVLWHVL�7×S�)DN�OWHVL���6XU�'L\DUEDN×U��7XUNH\�� E-mail: [email protected]

7ĂČĂĈć�ċþąúčþý�ĊĎúąĂčĒ�Ĉÿ�ąĂÿþ�Ăć�ĉúčĂþćčČ�úÿčþċ�ĈüĎąúċ�ĉþćþčċúčĂćĀ�ĂćăĎċĂþČ
96 "SR�#SBT�0GUBMNPM���������������
A complete ophthalmological examination, including visual acuity, intraocular pressure measurements, and biomicroscopic evalua-tion of the anterior segment and fundus was performed for all participants. To correlate visual acuity with subscale responses, the Snellen visual acuity of the affected eye was converted to a logMar equivalent.
Data, including age, gender, and best-corrected visual acuity, of all participants were recorded. All participants completed the SF 36 and VFQ-25 questionnaires to evaluate their HR-QOL and VR-QOL, respectively. The control group consisted of age, gender, and edu-cation level matched patients who were admitted to our clinic for examination with no pathology that affected visual function.
MEASUREMENTS OF PSYCHOLOGICAL STATE AND QOL SF 36SF 36 is the most widely used self-report scale that measures
HR-QOL. It successfully measures the HR-QOL of patients with medical or psychological disorders, as well as healthy subjects. The scale can assess the positive and negative aspects of health, and it is considered sensitive to small changes in disability status. It was first developed by Ware and Sherbourne in 1992(10). It provides scores ranging between 0 and 100 that represent QOL in eight dimensions of health (physical functioning, physical role difficulty, bodily pain, general health perception, vitality, social functioning, emotional role difficulty, and mental health). Higher scores reflect a better QOL. The validity and reliability of the Turkish version of the SF 36 was demons-trated by Kocyigit et al. in 1999(11).
NEI VFQ-25NEI VFQ-25 was used to assess VR-QOL in our participants. It is
a validated and reliable instrument that assesses the dimensions of self-reported and vision-targeted health status, which are most im -portant for persons with chronic eye disease.
The NEI VFQ-25 has been translated into Turkish, and its reliability and validity have been established. This version, which was used in previous studies, was administered to all subjects(12). VR-QOL, which measures visual functioning level in 12 dimensions, was assessed using NEI VFQ-25. It generates subscales for the following 12 dimensions of VR-QOL: general health, general vision, ocular pain, near activities, distance activities, vision-specific social functioning, vision-specific mental health, vision-specific role difficulties, vision-specific depen-dency, driving, color vision, and peripheral vision. Finally, an overall composite score is calculated that serves as an average of all subscales, excluding the general health subscale. Scores range from 0 to 100, with higher scores indicating a better QOL(13).
STATISTICAL ANALYSIS
Statistical analysis were performed with Statistical Program for So cial Science version 15 (SPSS, Chicago, Illinois, USA). Independent sample t-tests, one-way analysis of variance (ANOVA), correlational analysis, and linear regression were used in the statistical analysis. The data are presented as the mean ± standard deviation.
RESULTSThe study participants included 54 patients who had undergone
surgery because of OPI occurring at least 6 months before the study began. In addition, we examined 26 healthy control subjects. There were no differences between groups in terms of age, gender, or edu-cation level. The demographic characteristics of the patients and the control group are given in table 1.
SF 36 and NEI VFQ-25 scores are presented in table 2. All NEI VFQ-25 scores, except general health, were significantly lower in the OPI group than in the control group. The study participants answered all questions, except driving-related questions. Driving-related questions were answered by only 6 (11%) patients in the OPI group and 13 (50%) subjects in the control group. All SF 36 scores were
significantly lower in the OPI group than in the control group. All patients with OPI had sustained an injury in only one eye. The mean follow-up for patients after surgery was 8.4 ± 3.1 (6-19) months. Male and female patients in the OPI group showed no difference in NEI VFQ-25 and SF 36 scores.
A correlation analysis of the NEI VFQ-25 and SF 36 scores, age, visual acuity, and gender are presented in table 3. A linear regression analysis was performed with the variables that showed a significant correlation. In the regression analysis, the NEI VFQ-25 composite
Table 1. Demographic characteristics of the ocular penetrating injury patients and control subjects
OPI n (%) Control n (%) p
Sex
Female 12 (22.2) 09 (34.6)
Male 42 (77.8) 17 (65.4) 0.238
Duration 8.4 ± 3.1 (6-19) month
Educational level
Elementary school 02 (03.7) 02 (07.7)
Junior high school 09 (16.7) 04 (15.4) 0.564
High school 40 (74.1) 20 (76.9)
logMar VA 0.76 ± 0.89 0.0 ± 0.0 p<0.001
Type of the injury
Corneal 32 (59.3)
Corneoscleral 09 (16.7)
Scleral 13 (24.1)
Age 30.5 ± 8.2 33.0 ± 4.6 0.158
Table 2. Test result of NEI VFQ-25 and SF 36 tests
Subscale OPI group Control group p value
NEI VFQ-25 (mean ± SD) (mean ± SD)
General health 80.1 ± 25.4 091.7 ± 11.7 <0.092
General vision 50.4 ± 18.1 095.4 ± 8.6 <0.001
Ocular pain 58.7 ± 13.6 098.1 ± 6.8 <0.001
Near activity 54.8 ± 12.3 099.0 ± 3.4 <0.001
Distance activity 56.5 ± 15.5 097.1 ± 7.0 <0.001
Social function 63.0 ± 19.9 100.0 ± 0 <0.001
Mental health 53.3 ± 11.4 100.0 ± 0 <0.001
Role difficulties 52.5 ± 12.9 100.0 ± 0 <0.001
Dependency 66.8 ± 17.6 100.0 ± 0 <0.001
Driving (6/13) 56.9 ± 3.4 093.6 ± 7.0 <0.001
Color vision 70.8 ± 17.3 100.0 ± 0 <0.001
Peripheral vision 58.2 ± 21.3 100.0 ± 0 <0.001
Composite score 58.1 ± 21.3 099.8 ± 0.7 <0.001
SF 36 (mean ± SD) (mean ± SD)
Physical functioning 98.2407 ± 3.2443 100.0000 ± 0 <0.001
Social functioning 73.3796 ± 21.3139 94.7115 ± 7.2224 <0.001
Physical problems 53.3704 ± 44.1478 97.1154 ± 8.1453 <0.001
Pain 66.3889 ± 21.9454 87.8462 ± 4.6276 <0.001
Emotional problems 55.5557 ± 46.2426 100.0000 ± 0 <0.001
Mental health 65.5556 ± 13.1043 85.2308 ± 5.7432 <0.001
Energy and vitality 59.0741 ± 12.4033 83.2692 ± 5.6466 <0.001
General perception of health 48.5556 ± 17.8997 89.1923 ± 8.3331 <0.001

:ŁĄČþą�) �þč�úą�
97"SR�#SBT�0GUBMNPM���������������
score was affected by the final visual acuity, social function, and emo-tional status sub-scores of the SF 36 (Table 4). In addition, the final visual acuity was affected by the NEI VFQ-25 composite score and initial visual acuity (Table 5). Gender and education level were not related to the NEI VFQ-25 composite score or the final visual acuity.
DISCUSSIONTo our knowledge, the present study is the first to compare the
psychological status and QOL of patients with OPI to those of healthy control subjects. The results of the current study demonstrate that OPI patients have increased psychological symptoms and lower levels of QOL than healthy control subjects.
OPI, which are usually observed in young individuals, is the lea-ding cause of unilateral vision loss; men are more often affected than women(2). In our study, the male/female ratio was consistent with those reported in the literature. However, there was no significant effect of gender on QOL.
Many studies have found the size and location of the wound are important indicators for the visual prognosis(2,14). Corneoscleral OPI has a poorer prognosis in terms of visual acuity(14,15). In our study, there was no relationship between OPI location and NEI VFQ-25 or SF 36
scores. Schareder et al.(16) evaluated patients with open eye injuries and examined how the trauma affected their work life, QOL, and emo-tional well-being. They reported that QOL was negatively affected in patients with an ocular injury. However, in that study they, did not report information about their questionnaire; therefore, it is uncertain if a standard questionnaire was used. In our study, the effect of OPI on QOL was analyzed with standard questionnaires and compared with the QOL of healthy controls.
Patients with vision loss due to ocular trauma not only suffer vision impairments, they also experience deterioration in social functioning that can decrease labor in the workplace. Many patients with vision loss cannot continue their employment and need to change their occupation or obtain disability status(13). Therefore, QOL of those indi-viduals is seriously affected. In our study, the overall health of patients in the OPI group was affected and the SF 36 scores, which determine the HR-QOL, were significantly lower in the group than in the con-trol group. Rofail et al. compared QOL in patients who underwent primary or secondary enucleation because of OPI(17). They reported that QOL was more affected in patients who underwent primary enu-cleation than in those who underwent secondary enucleation. They suggested that, if possible, the eyeball should not be removed during the primary repair. However, in that study, QOL was not compared between patients with OPI and control subjects.
The NEI VFQ-25 composite scores observed in the present study were lower than those reported for patients with PDR, SMD, or Behçet’s disease in other studies(8,18,19). Our patients were younger than those in other studies; therefore, young individuals may experience a greater impact on their QOL with permanent vision loss due to trauma than with other diseases. The NEI VFQ-25 scores for a younger patient group with ocular chemical burns reported in a study(13) were similar to those observed in our study. In that study, patients with bilateral in juries had severely decreased composite scores in NEI VFQ-25(16). No patient had bilateral trauma in our study.
Using NEI VFQ-25, Onal et al. reported that general health was more influenced than general vision in patients with Behçet’s disea-se(18). In contrast, the present study found that OPI affected vision more than general health. We suggest that this difference is based on the systemic involvement of the Behçet’s disease, whereas OPI is usually localized to one eye.
Previous reports indicated that QOL is affected by ocular disea-ses(18,20,21). In this study, SF 36, a widely known instrument, was used to assess HR-QOL. Using the same questionnaire, QOL changes were reported with central serous chorioretinopathy, age-related macular degeneration, and Behçet’s disease(8,18,20). In our patients’ first VA exam, the composite score of NEI VFQ-25 and the mental health score of SF 36 affected the final VA. Level of education, age, and gender had no effect on the final VA. In contrast to Onal et al., who reported that education level and age affected the visual prognosis in Behçet’s disease(15); another study found that education, general vision, near vision, and social functioning scores decreased. They suggested that a high level of education increases the patient’s awareness and knowledge of their disease.
In this study, we showed that OPI patients showed poorer vision and health-related QOL than healthy subjects. In addition, general vision was more affected than general health in patients with OPI. Furthermore, deterioration in QOL should be considered in patients with OPI. Deterioration in QOL may lead to psychiatric disorders. Pa-tients should be evaluated in this aspect and psychiatric help should be given when necessary.
ACKNOWLEDGMENTWe are grateful to Dicle University DUBAP for their sponsorship
about English editing of this manuscript.
Table 3. The correlations between visual acuity, age duration of OPI with the NEI VFQ-25* scores
Test scoresVisual acuity Age
r pr p
General health -0.507 <0.001 -0.271 0.279
General vision -0.582 <0.001 -0.311 0.122
Ocular pain -0.224 0.103 -0.224 0.271
Near activity -0.386 0.004 -0.200 0.327
Distance activity -0.496 <0.001 -0.353 0.077
Social function -0.468 <0.001 -0.433 0.027
Mental health -0.443 0.001 -0.296 0.141
Role difficulties -0.437 0.001 -0.240 0.238
Dependency -0.477 <0.001 -0.171 0.403
Color vision -0.402 0.430 -0.097 0.637
Peripheral vision -0.178 0.197 -0.111 0.591
Composite score -0.574 <0.001 -0.393 0.047
*NEI VFQ-25= National Eye Institute Visual Functioning Questionnaire.
Table 4. Regression analysis of the factors that were found to be effective on composite score of NEI VFQ-25* in a univariate analysis
Beta t p value
Social function 0.850 11.64 0.000
Final visual acuity 0.555 06.09 0.000
Emotional score of SF 36 0.273 02.28 0.027
Dependent variable= composite score of VFQ 25 r2=0.81.*NEI VFQ-25= The National Eye Institute Visual Functioning Questionnaire.
Table 5. Regression analysis of the factors that were found to be effective on final visual acuity in a univariate analysis
Beta t p valueComposite score of NEI VFQ-25* -0.810 -9.942 0.000
First visual acuity -0.231 -2.404 0.020
Dependent variable is final visual accuity. r2=0.66.*NEI VFQ-25= The National Eye Institute Visual Functioning Questionnaire.

7ĂČĂĈć�ċþąúčþý�ĊĎúąĂčĒ�Ĉÿ�ąĂÿþ�Ăć�ĉúčĂþćčČ�úÿčþċ�ĈüĎąúċ�ĉþćþčċúčĂćĀ�ĂćăĎċĂþČ
�� "SR�#SBT�0GUBMNPM���������������
REFERENCE 1. Kuhn F, Morris, R, Witherspoon CD, Mann L. Epidemiology of blinding trauma in the
United States Eye Injury Registry. Ophthalmic Epidemiol. 2006;13(3):209-6. 2. Yalcin Tök O, Tok L, Eraslan E, Ozkaya D, Ornek F, Bardak Y. Prognostic factors influen-
cing final visual acuity in open globe injuries. J Trauma. 2011;71(6):1794-800. 3. Le Q, Chen Y, Wang X, Li Y, Hong J, Xu J. Vision-related quality of life in patients with
ocular chemical burns. Invest. Ophthalmol Vis Sci. 2011;52(12):8951-6. 4. Massof RW, Rubin GS. Visual function assessment questionnaires. Surv Ophthalmol.
2001;45(6):531-48. 5. Vitale S, Schein OD. Qualitative research in functional vision. Int Ophthalmol Clin.
2003;43(2):17-30. 6. Chia EM, Mitchell P, Ojaimi E, Rochtchina E, Wang JJ. Unilateral visual impairment and
health related quality of life: the Blue Mountains Eye Study. Br J Ophthalmol. 2003; 87(4):392-5.
7. Awdeh RM, Elsing SH, Deramo VA, Stinnett S, Lee PP, Fekrat S. Vision-related quality of life in persons with unilateral branch retinal vein occlusion using the 25-item National Eye Institute Visual Function Questionnaire. Br J Ophthalmol. 2010;94(3):319-23.
8. Klein R, Moss SE, Klein BE, Gutierrez P, Mangione CM. The NEI-VFQ-25 in people with long-term type 1 diabetes mellitus: the Wisconsin Epidemiologic Study of Diabetic Retinopathy. Arch Ophthalmol. 2001;119(5):733-40.
9. Wren PA, Musch DC, Janz NK, Niziol LM, Guire KE, Gillespie BW; CIGTS Study Group. Contrasting the use of 2 vision-specific quality of life questionnaires in subjects with open-angle glaucoma. J Glaucoma. 2009;18(5):403-11.
10. Ware J, Sherbourne E. Donald C. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30(6):473-83.
11. Koçyiğit H, Aydemir Ö, Fişek G, Ölmez N, Memiş A. Validity and reliability of Turkish version of Short Form-36 (SF-36). J Drug Treat. 1999;12:102-6.
12. Toprak AB, Eser E, Guler C, Baser FE, Mayali H. Cross-validation of the Turkish version of the 25-item National Eye Institute Visual Functioning Questionnaire (NEI-VFQ 25). Ophthalmic Epidemiol. 2005;12(4):259-69.
13. Mangione CM, Lee PP, Gutierrez PR, Spritzer K, Berry S, Hays RD. National Eye Ins-titute Visual Function Questionnaire Field Test Investigators. Development of the 25-item National Eye Institute Visual Function e Questionnaire. Arch Ophthalmol. 2001;119(7):1050-8.
14. Agrawal R, Rao G, Naigaonkar R, Ou X, Desai SS. Prognostic factors for vision outcome after surgical repair of open globe injuries. Indian J Ophthalmol. 2011;59(6):465-70.
15. Soylu M, Sizmaz S, Cayli S. Eye injury (ocular trauma) in southern Turkey: epidemio-logy, ocular survival, and visual outcome. Int Ophthalmol. 2010;30(2):143-8.
16. Schrader WF. Open globe injuries: epidemiological study of two eye clinics in Ger-many, 1981-1999. Croat Med J. 2004;45(3):268-74.
17. Rofail M, Lee G. A, O’Rourke P. Quality of life after open-globe injury. Ophthalmology. 2006;13:(6)1057.e1-3.
18. Onal S, Savar F, Akman M, Kazokoglu H. Vision- and health-related quality of life in patients with Behçet uveitis. Arch Ophthalmol. 2010;128(10):1265-71.
19. Leys A, Zlateva G, Shah SN, Patel M. Quality of life in patients with age-related macular degeneration: results from the VISION study. Eye (Lond). 2008;22(6):792-8.
20. Sahin A, Bez Y, Kaya MC, Türkcü FM, Sahin M, Yüksel H. Psychological distress and poor quality of life in patients with central serous chorioretinopathy. Semin Ophthalmol. 2014;29(2):73-6.
21. Türkcü FM, Sahin A, Bez Y, Yüksel H, Cinar Y, Kürşat Cingü A, et al. Vision-related quality of life in patients with chronic central serous chorioretinopathy. Semin Ophthalmol. 2013 Oct 28; doi:10.3109/08820538.2013.839818.
17o Congresso de Oftalmologia USP
16o Congresso de Auxiliar de Oftalmologia USP
28 e 29 de julho de 2014 Centro de Convenções Rebouças
São Paulo - SP
Informações: Tels.: (11) 5084-9174/5082-3030
E-mail: [email protected]: www.oftalmologiausp.com.br

99"SR�#SBT�0GUBMNPM�����������������
0ċĂĀĂćúą�"ċčĂüąþ�
Artificial tears alone versus 0.45% ketorolac tromethamine with artificial tears for the
treatment of acute viral conjunctivitis
�¤�����ȱ����ę����ȱ������ȱ����������ȱ��ȱ�����������ȱŖǰŚśƖȱ���������ȱ¥ȱ�������ȱ����ę����ȱ��ȱ����������ȱda conjuntivite viral aguda
adRiana FalCão veloso lyRa1, lílian CoRReia bastos1, Raquel Coelho de souza lima1, lúCio de vieiRa leite maRanhão1,2, tiago eugênio aRantes1,2
INTRODUCTIONInfectious conjunctivitis accounts for approximately 25% consul-
tations in ophthalmology emergency services(1,2) and 1%-2% of fa mily-medicine consultations(3). Among the types of infectious con-junctivitis, viral etiologies are the most common, and the adenovirus is responsible for approximately 60% cases(4).
Symptoms associated with viral conjunctivitis include redness, tearing, swelling, and irritation that often last from 1 to 3 weeks, and, in general, the management of this condition comprises symptoma-tic treatment(3). Despite standard treatment with artificial tears, cold compresses, and topical vasoconstrictors, patients still suffer from great discomfort until the disease resolves completely(5).
Anti-inflammatory drugs, including topical steroids, may be used for the treatment of viral conjunctivitis. Generally, these medications
ABSTRACTPurpose: To evaluate the effects of preservative-free 0.45% ketorolac trome-thamine and artificial tears (carboxymethylcellulose) compared with those of preservative-free artificial tears alone on the symptoms and signs of acute viral conjunctivitis. Methods: This was a randomized, double-masked clinical trial that included 50 patients who were diagnosed with acute viral conjunctivitis and distributed into two groups (Group 0: artificial tears and Group 1: 0.45% ketorolac tromethamine + carboxymethylcellulose). The patients were instructed to use the medication 4 times daily. Signs (conjunctival hyperemia, chemosis, follicles, and secretion) and symptoms (general ocular discomfort, itching, foreign body sensation, tearing, redness, and swelling of the eyelids) were scored at baseline and on the third and seventh days of treatment using a standardized questionnaire and slit-lamp anterior segment examination. Results: Both groups showed an improvement in the signs and symptoms of con-junctivitis in their follow-up visits. There was no significant difference in symptom and sign scores between Group 0 and Group 1 in the study visits (p>0.05). The frequency of side effects during treatment was similar between groups (p>0.05).Conclusions: Our findings indicate that 0.45% ketorolac tromethamine was not superior to the use of artificial tears in relieving the signs and symptoms of viral conjunctivitis.
Keywords: Conjunctivitis, viral/drug therapy; Ketorolac tromethamine/therapeutic use; Ophthalmic solutions
RESUMOObjetivo: Avaliar o efeito do colírio de cetorolaco de trometamina 0,45% associado à carboximetilcelulose sem conservante em comparação ao uso isolado de lágrimas artificiais sem conservantes nos sinais e sintomas da conjuntivite viral aguda. Métodos: Ensaio clínico duplo-mascarado randomizado incluindo 50 pacientes com diagnóstico de conjuntivite viral aguda, distribuídos em dois grupos (Grupo 0: lágrimas artificiais e Grupo 1: cetorolaco 0,45% + carboximetilcelulose). Os pacientes foram orientados a utilizar a medicação quatro vezes ao dia. Sinais (hiperemia conjuntival, quemose, folículos e secreção) e sintomas (desconforto ocular geral, prurido, sensa-ção de corpo estranho, lacrimejamento, vermelhidão e inchaço de pálpebras) foram avaliados na consulta inicial, no terceiro e no sétimo dia de tratamento utilizando um questionário padronizado e biomicroscopia de segmento anterior. Resultados: Ambos os grupos apresentaram melhora dos sinais e sintomas de con -juntivite nas visitas de reavaliação. Não foi observado diferença estatística na mudança dos escores dos sinais e sintomas entre o Grupo 0 e o Grupo 1 durante as visitas do estudo (p>0.05). A frequência de efeitos colaterais durante o tratamento foi similar entre os dois grupos (p>0.05). Conclusão: O uso do cetorolaco de trometamina 0,45% não se mostrou superior ao uso isolado de lágrimas artificiais no alívio dos sinais e sintomas da conjuntivite viral.
Descritores: Conjuntivite viral/quimioterapia; Cetorolaco de trometamina/uso te -rapêutico; Soluções oftálmicas
are indicated in severe cases, such as those with appearance of su-bepithelial corneal opacities and conjunctival membranes. Beneficial effects have been demonstrated with topical steroids(6); however, side effects such as ocular hypertension, cataract formation, delayed wound healing, and secondary infection limit their use(5). Some stu-dies have also shown that topical steroids can enhance virus replica-tion and prolong the duration of virus shedding(7).
Ketorolac tromethamine is a topical nonsteroidal anti-inflamma-tory drug (NSAID) that blocks the cyclooxygenase enzyme, which catalyzes the conversion of arachidonic acid into prostaglandins. Several studies have demonstrated the effectiveness of 0.4% and 0.5% formulations of this drug in relieving inflammation and ocular pain and the prevention and treatment of cystoid macular edema in patients who undergo ocular surgery(8,9). This topical medication has also been used with good results for the symptomatic treatment of
Submitted for publication: October 9, 2013 Accepted for publication: December 1, 2013
Study conducted at Fundação Altino Ventura, Recife, PE, Brazil.1 Fundação Altino Ventura, Recife, PE, Brazil.2 Hospital de Olhos de Pernambuco, Recife, PE, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflict of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence adress: Adriana Falcão Veloso Lyra. Fundação Altino Ventura. Rua da Soledade, 170 - Recife (PE) - 50070-040 - Brazil - E-mail: [email protected]
Registration number on clinicaltrials.gov: NCT01799863
Research project approved by the Ethics Committee of Fundação Altino Ventura (no 011/2012).

"ċčĂÿĂüĂúą�čþúċČ�úąĈćþ�ďþċČĎČ�Ō�Őő��ĄþčĈċĈąúü�čċĈĆþčāúĆĂćþ�ĐĂčā�úċčĂÿĂüĂúą�čþúċČ�ÿĈċ�čāþ�čċþúčĆþćč�Ĉÿ�úüĎčþ�ďĂċúą�üĈćăĎćüčĂďĂčĂČ
100 "SR�#SBT�0GUBMNPM�����������������
seasonal allergic conjunctivitis(10). In viral conjunctivitis associated with varicella, 0.5% ketorolac was more effective in decreasing con-junctival hyperemia compared with artificial tears(11). In adenoviral conjunctivitis, 0.5% ketorolac showed results similar to those of arti-ficial tears in terms of providing symptomatic relief, but there were frequent stinging and burning sensations upon eyedrop instillation(5).
Currently, a formulation of 0.45% ketorolac tromethamine asso-ciated with carboxymethylcellulose (CMC), with a better tolerability profile and bioavailability, is commercially available and is indicated for the treatment of pain and inflammation in patients undergoing cataract surgery(8,9,12).
This study aimed to evaluate the effects of preservative-free 0.45% ketorolac tromethamine and carboxymethylcellulose com-pared with those of preservative-free artificial tears alone on the symptoms and signs of acute viral conjunctivitis.
METHODSThis prospective, double-masked, randomized study included 50
patients divided into 2 treatment groups: Group 1, who received the formulation of preservative-free 0.45% ketorolac tromethamine with CMC (Acular CMC®, Allergan, Irvine, USA), and Group 0, who received only preservative-free artificial tears (Optive UD®, Allergan, Irvine, USA). Patients were recruited from the emergency service of Funda-ção Altino Ventura, Recife, Pernambuco, between June and Septem-ber 2012. Eligible patients were required to have acute unilateral or bilateral conjunctivitis of less than 2 weeks duration. In addition, they were required to have at least one of the following features compa-tible with viral conjunctivitis: preauricular lymphadenopathy, upper respiratory tract infection (URTI), or recent contact with individuals with conjunctivitis.
Exclusion criteria included a history of seasonal allergic conjuncti-vitis, herpetic eye disease, ocular surgery, and/or chronic ocular disease other than refractive error; use of any ocular medication after the beginning of symptoms; contact lens wear; allergy to NSAIDs; pregnancy; age of less than 18 years; presence of a bleeding disorder; corneal epithelial staining with fluorescein; and intraocular inflammation.
Each patient was randomly assigned a sealed envelope contai-ning vials of unidentified 0.45% ketorolac tromethamine with CMC or artificial tears. Both patients and examiners were blinded to the medication. Patients were instructed to place one drop into each symptomatic eye 4 times daily for 7 days and were reassessed after 3-7 days from the first visit. At the end of follow-up for the 50th patient, the randomization code was revealed for data analysis.
In all evaluations, the patients completed a standardized ques-tionnaire where they were asked about the following symptoms: overall discomfort, itching, foreign body sensation, tearing, redness, and lid swelling. Each of the symptoms was rated by the patient at presentation and at follow-up on a 4-point scale: none (0), mild (1), moderate (2), and severe (3). During re-evaluation, the patients were asked about the proper use of medications, side effects, and dis-comfort with the use of medications. Patients were also asked about the improvement in symptoms after the use of eye drops.
Clinical examination comprised anterior segment slit-lamp bio-microscopy, and all re-evaluations for each patient were performed by the same examiner from the initial consultation. Four signs were assessed on physical examination: conjunctival hyperemia, conjunc-tival chemosis, conjunctival mucus, and the presence of follicles in the lower tarsal conjunctiva. The signs were classified as none (0), mild (1), moderate (2), and severe (3). For conjunctival hyperemia, grade 0 indicated no detectable hyperemia, grade 1 indicated con-junctival hyperemia that was barely detectable, grade 2 indicated conjunctival hyperemia that was readily detectable, and 3 indicated intense conjunctival hyperemia that could be mistaken for subcon-junctival hemorrhage without slit-lamp examination. Only patients
with a conjunctival hyperemia score of >1 were included in the study. For the sign of chemosis, grade 0 indicated no detectable conjuncti-val edema, grade 1 indicated conjunctival edema that was barely detectable, grade 2 indicated conjunctival edema that was rea dily detectable, and grade 3 indicated conjunctival edema sufficient to cause the protrusion of swollen redundant conjunctiva through closed lids. For the sign of conjunctival mucus, grade 0 indicated no detectable mucus discharge, grade 1 indicated mucus discharge that was barely detectable, grade 2 indicated mucus discharge that was readily detectable, and grade 3 indicated mucus discharge asso-ciated with an inflammatory conjunctival pseudomembrane or true membrane. For the sign of follicles, grade 0 indicated no detectable follicles, grade 1 indicated barely detectable follicles, grade 2 indi-cated readily detectable follicles, and grade 3 indicated an intense follicular reaction.
The study was initiated after approval from the institutional ethics committee. All patients were included in the study after agreement and signature of the study informed consent form, and they were ins-tructed to contact one of the investigators if they were experiencing any significant side effects from the study medication.
The likelihood ratio test was used to evaluate differences in fre-quencies between categorical variables. Student’s t test was used to evaluate differences between means. A p-value of <0.05 was used to indicate statistical significance.
RESULTS A total of 50 patients met the eligibility criteria and were enrolled
in the study. Twenty-six were included in Group 0 (artificial tears) and 24 in Group 1 (0.45% ketorolac tromethamine + CMC). During follow-up, 6 patients missed their re-evaluation appointments (3 in each group; 12% dropout rate during follow-up).
The general characteristics of the patients enrolled in the study are presented in table 1. There were no statistical differences in age, distribution of sex, and symptoms suggestive of viral conjunctivitis between the studied groups (p>0.05).
The patient’s perception of general improvement in symptoms after 3 and 7 days of treatment is shown in table 2. There was no statistical difference between groups in relation to the general im-provement in symptoms after the use of the medications (p>0.05).
The evolution of conjunctivitis symptoms on the 3rd and 7th days of re-evaluation are shown in tables 3 and 4, respectively. Tables 5 and 6 present the evolution of signs on the 3rd and 7th days of treatment, respectively. As noted in the tables, there was no statistical difference in sign and symptom scores between the 2 groups during follow-up (p>0.05).
Side effects that comprised mild symptoms of burning, itching, and stinging upon eyedrop instillation were reported (64% in Group 0; 57% in Group 1); however, no significant difference was observed (p=0.764).
During follow-up, 6 patients (12%) developed tarsal conjunctival membranes (3 patients from Group 0 and 3 patients from Group 1). These membranes were removed, and a combination of 0.3% cipro-floxacin + 0.1% dexamethasone was added to the initial regimen.
DISCUSSIONViral conjunctivitis, despite being a self-limiting disease, is asso-
ciated with high morbidity because of its symptoms and the risk of contagion. Currently, there are no effective treatments to decrease disease duration and contagion, and only symptomatic treatment is indicated(3). Novel treatment options are being studied, including antiviral drugs such as ganciclovir and povidone-iodine(13-16).
In experimental and in vitro studies, ketorolac tromethamine did not lead to prolonged adenoviral replication as opposed to predni-solone, proving a safer alternative when compared with corticos-

-Ēċú�"'7 �þč�úą�
101"SR�#SBT�0GUBMNPM�����������������
Table 1. General characteristics of the studied patientsTotal (n=50) Group 0 (n=26) Group 1 (n=24) p
Age (mean ± standard deviation) 31.6 ± 10.7 30.4 ± 8.6 32.8 ± 12.7 0.432a
Male [n (%)] 34 (68%) 30.18 (69%) 016 (67%) 0.999b
Unilateral involvement 36 (72%) 00.21 (81%) 015 (63%) 0.211b
Association with URTIc 31 (62%) 30.16 (62%) 015 (63%) 0.999b
Preauricular lymphadenopathy 12 (24%) 330.6 (23%) 006 (25%) 0.999b
Recent contact with conjunctivitis 37 (74%) 3018 (69%) 019 (79%) 0.526b
a= Student t test; b= Fisher exact test; c= URTI upper tract respiratory infection.
Table 2. Perception of treatment benefit in the 3rd and 7th follow-up days in patients with viral conjunctivitis
3th day 7th day
Evolution of symptoms with treatment Group 0 (n=25) Group 1 (n=21) Group 0 (n=23) Group 1 (n=19)
Considerable improvement 15 (60%) 09 (43%) 20 (87%) 019 (100%)
Slight improvement 07 (28%) 10 (48%) 00 (00%) 00 (00%)
Not helped 03 (12%) 02 (09%) 03 (13%) 00 (00%)
pa 0.388 0.239 a= likelihood ratio test.
Table 3. Evolution of symptoms reported by the patient on the 3rd day of treatment compared to the initial consultation
3th day
Symptoms on 3th day Group 0 (n=25) Group 1 (n=21) pa
General symptoms
Worsening 01 (04%) 00 (00%) 0.844
Unchanged 04 (16%) 05 (24%)
Improvement 20 (80%) 16 (76%)
Itching
Worsening 03 (12%) 05 (24%) 0.303
Unchanged 06 (24%) 07 (33%)
Improvement 16 (64%) 09 (43%)
Foreign body sensation
Worsening 02 (08%) 01 (05%) 1.000
Unchanged 09 (36%) 07 (33%)
Improvement 14 (56%) 13 (62%)
Tearing
Worsening 01 (04%) 02 (10%) 0.870
Unchanged 04 (16%) 03 (14%)
Improvement 20 (80%) 16 (76%)
Redness
Worsening 01 (04%) 00 (00%) 0.163
Unchanged 01 (04%) 04 (19%)
Improvement 23 (92%) 17 (81%)
Eyelid swelling
Worsening 02 (08%) 02 (09%) 0.617
Unchanged 03 (12%) 05 (24%)
Improvement 20 (80%) 14 (67%)a= likelihood ratio test.
Table 4. Evolution of symptoms reported by the patient on the 7th day of treatment compared to the initial consultation
Symptoms on 7th day
7th day
Group 0 (n=23) Group 1 (n=19) pa
General symptoms
Worsening 02 (09%) 00 (00%) 0.495
Unchanged 01 (04%) 00 (00%)
Improvement 20 (87%) 019 (100%)
Itching
Worsening 01 (04%) 00 (00%) 1.000
Unchanged 04 (18%) 04 (21%)
Improvement 18 (78%) 15 (79%)
Foreign body sensation
Worsening 03 (13%) 00 (00%) 0.322
Unchanged 04 (17%) 04 (21%)
Improvement 16 (70%) 15 (79%)
Tearing
Worsening 01 (04%) 00 (00%) 1.000
Unchanged 02 (09%) 02 (11%)
Improvement 20 (87%) 17 (89%)
Redness
Worsening 02 (09%) 00 (00%) 0.495
Unchanged 01 (04%) 02 (11%)
Improvement 20 (87%) 17 (89%)
Eyelid swelling
Worsening 02 (09%) 00 (00%) 0.133
Unchanged 02 (09%) 06 (32%)
Improvement 19 (82%) 13 (68%)a= likelihood ratio test.

"ċčĂÿĂüĂúą�čþúċČ�úąĈćþ�ďþċČĎČ�Ō�Őő��ĄþčĈċĈąúü�čċĈĆþčāúĆĂćþ�ĐĂčā�úċčĂÿĂüĂúą�čþúċČ�ÿĈċ�čāþ�čċþúčĆþćč�Ĉÿ�úüĎčþ�ďĂċúą�üĈćăĎćüčĂďĂčĂČ
102 "SR�#SBT�0GUBMNPM�����������������
Table 5. Evolution of signs presented by patients on the 3rd day of treatment compared to the initial consultation
Signs on 3th day
3th day
paGroup 0 (n=25) Group 1 (n=21)
Hyperemia
Worsening 00 (00%) 02 (10%) 0.192
Unchanged 07 (28%) 04 (19%)
Improvement 18 (72%) 15 (71%)
Follicles
Worsening 00 (00%) 02 (09%) 0.175
Unchanged 09 (36%) 05 (24%)
Improvement 16 (64%) 14 (67%)
Chemosis
Worsening 01 (04%) 02 (10%) 1.000
Unchanged 03 (12%) 04 (19%)
Improvement 21 (84%) 15 (71%)
Secretion
Worsening 02 (08%) 03 (14%) 1.000
Unchanged 08 (32%) 08 (38%)
Improvement 15 (60%) 10 (48%)a= likelihood ratio test.
Table 6. Evolution of the signs presented by patients on the 7th day of treatment compared to the initial consultation
Signs on 7th day
7th day
p-valueaGroup 0 (n=23) Group 1 (n=19)
Hyperemia
Worsening 01 (04%) 02 (11%) 0.486
Unchanged 03 (13%) 01 (05%)
Improvement 19 (83%) 16 (84%)
Follicles
Worsening 01 (04%) 00 (00%) 1.000
Unchanged 03 (13%) 02 (11%)
Improvement 19 (83%) 17 (89%)
Chemosis
Worsening 00 (00%) 00 (00%) 1.000
Unchanged 03 (13%) 02 (11%)
Improvement 20 (87%) 17 (89%)
Secretion
Worsening 01 (04%) 03 (16%) 0.206
Unchanged 04 (18%) 01 (05%)
Improvement 18 (78%) 15 (79%)a= likelihood ratio test.
teroids(17). Because of their good response in patients with allergic conjunctivitis(10), 0.5% ketorolac was proposed for the treatment of adenoviral conjunctivitis. However, it was not superior to artificial tears in relieving itching, redness, foreign body sensation, tearing, and eyelid edema and was associated with discomfort (stinging and burning) upon instillation(5). Such discomfort is associated with the preservative benzalkonium chloride (BAK), the surfactant octoxy-nol-40, and the metal-chelating agent sodium edetate(8,9). Therefore, in this study, we evaluated a preservative-free formulation of 0.45% ketorolac with artificial tears (CMC), which presents a better tolerabi-lity profile and penetration into ocular tissues(8.9).
Evaluation of a patient’s perception of overall improvement on the 3rd and 7th days of treatment showed no significant differences between the 2 studied groups, suggesting that both eye drops had similar effects. This finding was similar to those in previous reports on the use of 0.5% ketorolac tromethamine solution with preservati-ves(5). No significant difference was found when the symptoms were individually evaluated or when the signs observed on ophthalmo-logic examinations were analyzed. In contrast to a previous study eva luating 0.5% ketorolac with preservatives(5), treatment with pre-servative-free 0.45% ketorolac was not associated with the worsening of ocular hyperemia or stinging upon instillation. The frequency of reported side effects was similar in both groups.
CONCLUSIONSIn conclusion, 0.45% ketorolac tromethamine was not superior to
artificial tears in relieving the signs and symptoms of viral conjuncti-vitis. Further research studies to evaluate safe and effective therapies for this common eye disease are required.
ACKNOWLEDGMENTSThe authors thank Leandro Lucena for assistance with statistical
analysis.
REFERENCES 1. Vieira GM. Um mês em um pronto-socorro de oftalmologia em Brasília. Arq Bras
Oftal mol. 2007;70(5):797-802. 1. Carvalho R de S, José NK. Ophthalmology emergency room at the University of São
Paulo General Hospital: a tertiary hospital providing primary and secondary level care. Clinics (Sao Paulo). 2007;62(3):301-8.
2. Visscher KL, Hutnik CM, Thomas M. Evidence-based treatment of acute infective conjunctivitis: breaking the cycle of antibiotic prescribing. Can Fam Physician. 2009; 55(11):1071-5. Comment in: Can Fam Physician. 2010;56(1):18.
3. Sambursky RP, Fram N, Cohen EJ. The prevalence of adenoviral conjunctivitis at the Wills Eye Hospital Emergency Room. Optometry. 2007;78(5):236-9.
4. Shiuey Y, Ambati BK, Adamis AP. A randomized, double-masked trial of topical keto-rolac versus artificial tears for treatment of viral conjunctivitis. Ophthalmology. 2000; 107(8):1512-7.
5. Wilkins MR, Khan S, Bunce C, Khawaja A, Siriwardena D, Larkin DF. A randomised pla cebo-controlled trial of topical steroid in presumed viral conjunctivitis. Br J Ophthalmol. 2011;95(9):1299-303. Comment in: Br J Ophthalmol. 2012;96(7):1040-1.
6. Romanowski EG, Roba LA, Wiley L, Araullo-Cruz T, Gordon YJ. The effects of corticos-teroids of adenoviral replication. Arch Ophthalmol. 1996;114(5):581-5.
7. McCormack PL. Ketorolac 0.45% ophthalmic solution. Drugs Aging. 2011;28(7):583-9. 8. Attar M, Schiffman R, Borbridge L, Farnes Q, Welty D. Ocular pharmacokinetics of
0.45% ketorolac tromethamine. Clin Ophthalmol. 2010;4:1403-8. 9. Schechter BA. Ketorolac tromethamine 0.4% as a treatment for allergic conjuctivitis.
Expert Opin Drug Metab Toxicol. 2008;4(4):507-11. 10. Toker MI, Erdem H, Erdogan H, Arici MK, Topalkara A, Arslan OS, et al. The effects of
topical ketorolac and indomethacin on measles conjunctivitis: randomized controlled trial. Am J Ophthalmol. 2006;141(5):902-5.
11. Xu K, McDermott M, Villanueva L, Schiffman RM, Hollander DA. Ex vivo corneal epithe-lial wound healing following exposure to ophthalmic nonsteroidal anti-inflammatory drugs. Clin Ophthalmol. 2011;5:269-74.
12. Kaufman HE. Adenovirus advances: new diagnostic and therapeutic options. Curr Opin Ophthalmol. 2011;22(4):290-3. Review
13. Trinavarat A, Atchaneeyasakul LO. Treatment of epidemic keratoconjunctivitis with 2% povidone-iodine: a pilot study. J Ocul Pharmacol Ther. 2012;28(1):53-8.
14. Pelletier JS, Stewart K, Trattler W, Ritterband DC, Braverman S, Samson CM, et al. A combination povidone-iodine 0.4%/dexamethasone 0.1% ophthalmic suspension in the treatment of adenoviral conjunctivitis. Adv Ther. 2009;26(8):776-83.
15. Yabiku ST, Yabiku MM, Bottós KM, Araújo AL, Freitas Dd, Belfort Jr R. Uso de ganciclovir 0,15% gel para tratamento de ceratoconjuntivite adenoviral. Arq Bras Oftalmol. 2011; 74(6):417-21.

103"SR�#SBT�0GUBMNPM����������������
0ċĂĀĂćúą�"ċčĂüąþ�
Implantable collamer lens and femtosecond laser for myopia: comparison using an
adaptive optics visual simulator
Lente implantável de collamer e laser de femtosegundo para miopia: comparação usando um
simulador visual de óptica adaptativa
CaRi PéRez-vives1, CésaR albaRRán-diego1, santiago gaRCía-lázaRo1, teResa FeRReR-blasCo1, RobeRt montés-miCó1
Submitted for publication: December 16, 2013 Accepted for publication: January 3, 2014
Study conducted at Optics Department, Faculty of Physics, University of Valencia, Spain.1 Optics Department, Faculty of Physics, University of Valencia, Spain.
Funding: This research was supported in part by the VALi+D research scholarship to Cari Pérez-Vives (ACIF/2012/099; GeneralitatValenciana).
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Cari Pérez-Vives. Optics Department. University of Valencia C/ Dr. Moliner 50 - 46100 Valencia (Spain) - E-mail: [email protected]
INTRODUCTIONThe femtosecond laser (FS) is the most interesting technical
de velopment in laser refractive surgery during the last few years(1,2). This technique was developed to create flaps for laser in situ kerato-mileusis (LASIK)(3,4). The FS is a focusable infrared (1053 nm) laser that uses ultrafast pulses in the 100-femtosecond (100 x 10-15 second) range. The laser delivers closely spaced spots that can be focused at a preset depth to photodisrupt tissue within the corneal stroma, while causing minimal inflammation and collateral tissue damage. In the recent meta-analysis by Zhang et al.(5) that compared femtosecond LASIK (F-LASIK) with mechanical microkeratome LASIK for myopia, no
ABSTRACTPurpose: To compare optical and visual quality of implantable collamer lens (ICL) implantation and femtosecond laser in situ keratomileusis (F-LASIK) for myopia.Methods: The CRX1 adaptive optics visual simulator (Imagine Eyes, Orsay, France) was used to simulate the wavefront aberration pattern after the two surgical procedures for -3-diopter (D) and -6-D myopia. Visual acuity at different contrasts and contrast sensitivities at 10, 20, and 25 cycles/degree (cpd) were measured for 3-mm and 5-mm pupils. The modulation transfer function (MTF) and point spread function (PSF) were calculated for 5-mm pupils. Results: F-LASIK MTF was worse than ICL MTF, which was close to diffraction-limited MTF. ICL cases showed less spread out of PSF than F-LASIK cases. ICL cases showed better visual acuity values than F-LASIK cases for all pupils, contrasts, and myopic treatments (p<0.05). No statistically significant differences were found in contrast sensitivities between ICL and F-LASIK cases with -3-D myopia for both pupils for all evaluated spatial frequencies (p>0.05). For -6-D myopia, however, statistically significant differences in contrast sensitivities were found for both pupils for all evaluated spatial frequencies (p<0.05). Contrast sensitivities were better after ICL implantation than after F-LASIK. Conclusions: ICL implantation and F-LASIK provide good optical and visual qua-lity, although the former provides better outcomes of MTF, PSF, visual acuity, and contrast sensitivity, especially for cases with large refractive errors and pupil sizes. These outcomes are related to the F-LASIK producing larger high-order aberrations.
Keywords: Myopia/surgery; Lasers, excimer/therapeutic use; Keratomileusis, laser in situ/methods; Lenses, intraocular; Contrast sensitivity; Visual acuity
RESUMOObjetivo: Comparar a qualidade óptica e visual da lente implantável de collamer (ICL) e da ceratomileuse in situ com laser de femtosegundo (F-LASIK) na correção de miopia.Métodos: O simulador visual de óptica adaptativa CRX1 (Imagine Eyes, Orsay, França) foi usado para simular o padrão de aberração de frentes de onda, depois de dois procedimentos cirúrgicos: implante de ICL e tratamento F-LASIK para -3 e -6 D. A acuidade visual em diferentes contrastes e sensibilidade ao contraste em 10, 20 e 25 ciclos/grau (cpd) foram medidos para pupilas de 3 e 5 mm. A função de transferência de modulação (MTF) e a função de espalhamento de ponto (PSF) foram calculados para a pupila de 5 mm. Resultados: A MTF do F-LASIK foi pior do que a do ICL, que estava perto da MTF do limite de difração. A ICL apresentou menor espalhamento do PSF do que o F-LASIK. ICL apresentou melhores valores da acuidade visual do que F-LASIK para todas as pu-pilas, contrastes e tratamentos miópicos (p<0,05). Não foram encontradas diferenças estatisticamente significantes na sensibilidade ao contraste entre ICL e F-LASIK de -3 D, para ambas as pupilas e quaisquer frequências espaciais avaliadas (p>0,05). Por outro lado, para -6 D, diferenças estatisticamente significativas na sensibilidade ao contraste foram encontrados para ambas as pupilas e todas as frequências espaciais avaliadas (p<0,05). Sensibilidade ao contraste foi melhor após o implante da ICL que após o F-LASIK. Conclusões: ICL e F-LASIK proporcionam uma boa qualidade óptica e visual, em-bora a ICL oferece melhores resultados de MTF, PSF, acuidade visual e sensibilidade ao contraste, especialmente para grandes erros de refração e tamanhos de pupila. Estes resultados estão relacionados ao procedimento F-LASIK que induz maiores aberrações de alta ordem.
Descritores: Miopia/cirurgia; Laser de excimer; Ceratomileuse assistida por excimer laser in situ/métodos; Lentes intraoculares; Sensibilidade de contraste; Acuidade visual
differences in efficacy, accuracy, or safety measures were observed between the two techniques, although F-LASIK was found to induce fewer aberrations. Other studies(6,7) comparing these techniques report a better contrast sensitivity (CS) at high frequencies used in F-LASIK, subsequently resulting in a better optical quality.
The Visian Implantable Collamer lens (ICL, STAAR Surgical, Nidau, Switzerland) is a posterior chamber phakic intraocular lens approved for myopia correction by the United States Food and Drug Adminis-tration (US FDA). Previous studies, including the multicenter US FDA ICL(8,9) and others(10), have confirmed both the safety and effectiveness of ICL implantation in correcting moderate to high levels of myopia

*Ćĉąúćčúûąþ�üĈąąúĆþċ�ąþćČ�úćý�ÿþĆčĈČþüĈćý�ąúČþċ�ÿĈċ�ĆĒĈĉĂú��üĈĆĉúċĂČĈć�ĎČĂćĀ�úć�úýúĉčĂďþ�ĈĉčĂüČ�ďĂČĎúą�ČĂĆĎąúčĈċ
��� "SR�#SBT�0GUBMNPM����������������
with 3(9) and 5(10) years of follow-up. Other studies have also shown the high optical and visual quality of these lenses(11,12). Outcomes of these studies have demonstrated the viability of the Visian ICL as an alternative to current refractive laser surgical treatment options.
Previous reports(13-15) have compared ICL implantation with me-chanical microkeratome LASIK and found better outcomes for safety, efficacy, predictability, and stability with ICL implantation, even in eyes with low myopia. Using an adaptive optics visual simulator, Pérez-Vives et al.(16) compared optical and visual quality after ICL im -plan tation and LASIK and obtained better outcomes after the former. However, to our knowledge, there are no studies comparing the outcomes of ICL implantation and F-LASIK.
The goal of this study was to compare optical and visual quality after ICL implantation and F-LASIK for -3-diopter (D) and -6-D of myopia. We used an adaptive visual simulation to simulate ICL and F-LASIK’s aberration patterns. Visual acuity (VA) for different contrasts and CS for 3-mm and 5-mm pupils also were evaluated.
METHODSSUBJECTS
Twenty individuals (20 eyes) aged 19-35 years who had experien-ce in psychophysical experiments participated in this study. Spherical refractive errors ranged between -2.50 and +1.50 D with astigmatism <0.50 D. The patients had clear intraocular media and no known ocu-lar pathology. Wavefront aberrations were measured with the natural pupil. The pupil diameter was usually >5 mm as the room light was off during the experiments.
The tenets of the Declaration of Helsinki were followed. Informed consent was obtained from each participant after verbal and written explanations of the nature and possible consequences of the study were provided. The study protocol received institutional review board approval.
INTRAOCULAR LENS
The Visian ICL is a plate-haptic single-piece lens designed to be implanted in the posterior chamber with support on the ciliary sul-cus. It is made of Collamer, a flexible, hydrophilic, and biocompatible material. The optic diameter of these lenses is 6 mm and they come in five sizes with different overall diameters (11.0, 11.5, 12.0, 12.5, and 13.0 mm). The lens has a central convex-concave optic zone with a diameter of 4.5-5.5 mm, depending on the dioptric power. The design of ICLs has been modified many times. In this study, we used the ICM V4 model.
ADAPTIVE OPTICS VISUAL SIMULATOR
We used the CRX1 adaptive optics system (Imagine Eyes, Orsay, France), which comprises two basic elements: a wavefront sensor and a correcting device. The system optically conjugates the exit pupil plane of the individual with the correcting device, the wavefront sensor, and an artificial pupil. The Shack-Hartmann wavefront sensor has a square array of 1024 lenslets. The wavefront aberration measu-rements are made at 850 nm. The deformable mirror is a correcting system composed of 52 independent magnetic actuators used to either partially or totally correct the aberrations up to the 5th order(17) (18 Zernike coefficients) and to add different values of aberrations (up to 4th order). Control of the deformable mirror surface is accom-plished by a commercially available program (HASO; Imagine Eyes), which reshapes the deformable mirror from its normally flat surface to the desired shape. The observer viewed visual tests generated on a microdisplay system through the adaptive optics system and an artificial pupil. The microdisplay system subtended a visual angle of 114 x 86 arcmin with a resolution of 800 x 600 pixels (pixel size=0.143 arcmin). The luminance conditions during the experiments were manually adjusted.
The adaptive optics system optically introduces predefined wavefront corrections using an internal closed-loop system that mo-difies the electromagnetic deformable mirror surface to the desired shape. Ideally, the adaptive optics simulator software continuously displays the residual wavefront value of the wavefront generated by the deformable mirror, compared with the wavefront defined by the examiner, to control the reliability of the system during measu-rements. The device’s software calculates the difference between the wavefront measured by the Shack-Hartmann sensor and the expected wavefront outcome; it then displays the residual wavefront correction as the RMS error at the level of the deformable mirror. The most accurate retinal images of the visual performance tests were provided by these dynamically adjusting wavefronts, which enabled the compensation of small eye decentration and aberration varia-tions due to the tear film or accommodation.
The adaptive optics system required precise alignment of the individual’s pupil with the optical axis set-up (with the wavefront sensor and the deformable mirror). The pupil’s size and position were monitored using a charge-coupled device camera. The control hand wheel of the CRX1 system enabled the pupil’s position to be main-tained with a quick, smooth, and fine adjustment.
EXPERIMENTAL PROCEDURE
The IRX3 Hartmann-Shack wavefront aberrometer (Imagine Eyes, Orsay, France), together with a custom-made wet cell, was used to de-termine the in vitro wavefront of ICL (ICL + wet cell). The aberrations of the wet cell alone were also measured and subtracted from ICL + wet cell aberrations following previously published methods(11,16,18-20). Two ICL powers were analyzed: -3 D and -6 D. All measurements were repeated 10 times for each lens and computed for 3-mm and 5-mm pupil diameters.
Once we obtained the aberration pattern of ICLs, we measured each eye’s wavefronts using the CRX1 visual simulator. The natural pu-pil diameter was checked for each eye (≥5 mm). The pupil’s size was controlled using the simulator artificial pupil. Then, CRX1 was pro-grammed to compensate for the eye’s wavefront error up to the 5th order and the refractive error by the Basal system. In order to simulate vision in each individual that underwent ICL implantation surgery, the eye’s wavefront was measured, compensated for with the defor-mable mirror, and then the wavefront pattern of ICLs was induced by adding the wavefront pattern of the myopic eye. The same procedure was followed to simulate vision after F-LASIK, but the wavefront pattern of the laser surgery was induced. The wavefront aberration used for the patients where those obtained by Montés-Micó et al.(7) with F-LASIK for low (-2.50 to -3.50 D) and medium (-5.50 to -6.50 D) myo-pia. Montés-Micó’s study compared F-LASIK with standard LASIK for myopia. They evaluated 100 eyes that underwent F-LASIK (mean age: 30.1 ± 5.71) and 100 eyes that underwent standard LASIK (mean age: 31.8 ± 4.22). Postoperative examinations were performed 1, 3, and 6 months after surgery; all patients completed a 6-month follow-up. Topographic data were obtained with a TMS-2N instrument (Tomey Corp., Nagoya, Japan). Corneal videokeratographic data were then digitally downloaded in ASCII files, which contained information about corneal elevation, curvature, power, and pupil position. The videokeratographic data were fitted with Zernike polynomials up to the 6th order to determine the aberration coefficients.
Figure 1 shows the Zernike coefficients of ICL implantation and the Zernike coefficients obtained with F-LASIK (aberrations after surgery - aberrations before surgery) for both pupils.
OPTICAL QUALITY EVALUATION
To evaluate the optical quality of both procedures, we analyzed the modulation transfer function (MTF)(21) and the point spread function (PSF). In the present study, the mean one-dimensional MTF was calcu-lated as the average over all orientations of the two-dimensional MTF.

1Įċþē�7ĂďþČ�$ �þč�úą�
���"SR�#SBT�0GUBMNPM����������������
We computed these metrics using a custom-made MATLAB program (Mathworks, Nantick, MA) from the wavefront data obtained with the IRX3 Hartmann-Shack sensor(22).
VISUAL QUALITY MEASUREMENT
High-contrast (100%), medium-contrast (50%), and low-contrast (10%) VA was measured using Freiburg Visual Acuity Test (FrACT) software(23) with a white background and luminance of 51 cd/m2. The acuity threshold was determined using the best parameter estimation by sequential testing (PEST) method(24) based on 30 pre-sentations. It was an eight-alternative, forced-choice method. The individual’s task was to identify the Landolt-C gap position using a keypad. The VA value was determined from the average of three measurements. We followed the same methodology used by Rocha et al.(25,26) and Pérez-Vives et al.(11,16) in their studies using CRX1.
The CS was measured for three spatial frequencies: 10, 20, and 25 cycles/degree (cpd). Oriented sinusoidal gratings (0°, 45°, 90°, and 135°) were randomly generated and displayed on the microdisplay using a 4-alternative, forced-choice method. A modified best PEST method based on 30 presentations was used to determine the contrast thresholds. Each individual was asked to indicate the gra-ting orientation by pressing the appropriate button on a numerical keypad. Three CS measurements were performed at each spatial frequency and the average was recorded.
DATA ANALYSIS
Student’s t-test for unpaired data was used to compare different surgical procedures regarding VA and CS. Results are presented as the mean ± SD and the statistical significance was set at p values of <0.05.
RESULTSOPTICAL QUALITY
Figure 1 shows the Zernike coefficients expressed as the root mean square (RMS) for -3-D and -6-D ICL implantation and F-LASIK at 3-m and 5-mm pupil diameters. The ICL implantation induced fewer aberrations than LASIK, especially when it increased the refractive error and pupil diameter. We found statistically significant differences in spherical aberration between the two procedures for -3-D and -6-D for both pupil diameters (p<0.05).
Figure 2 shows the normalized MTF for ICL implantation and F-LASIK for -6 D with a 5-mm pupil. ICL-MTF was near the diffraction- limited MTF, but F-LASIK-MTF was worse and deviated away from both curves. Note that differences between MTFs come from the higher-order aberrations (HOAs) effect that decreases the eye’s opti-cal quality. Figure 2 also sho ws the retinal contrast threshold curve at a retinal illuminance of 500 td. Figure 3 shows the images of PSF for ICL implantation and F-LASIK for -3-D and -6-D with a 5-mm pupil. When compared with ICL implantation, we observed a broad range of PSFs corresponding to F-LASIK for both -3-D and -6-D.
VISUAL QUALITY
Figures 4 and 5 show VA for the -3-D and -6-D ICL implantation and F-LASIK at 3-mm and 5-mm pupil diameters, respectively. For both pupil diameters, we found statistically significant differences between the procedures at -3 D and -6 D and all contrast evaluated (p<0.05), thus showing better VA values for ICL implantation.
Figures 6 and 7 show the mean log10 CS values for the -3 D and -6 D ICL implantation and F-LASIK for 3-mm and 5-mm-diameter pupils, respectively. For both pupil diameters, no statistically significant differences were found between procedures at -3 D for any spatial frequency (p>0.05). In contrast, we found statistical significant diffe-rences between both procedures at -6 D for both pupil diameters and all spatial frequencies (p<0.05). ICL implantation showed better outcomes than F-LASIK.
DISCUSSIONOPTICAL QUALITY
We found statistically significant differences in spherical aberra-tion between the procedures (Figure 1). This difference was due to increases in LASIK HOAs, especially spherical aberration, during laser ablation in the central cornea(27). In contrast, ICL implantation does not require surgical tissue ablation and leaves the central cornea untouched; therefore, it produces significantly lower HOAs than
Figure 1. Zernike coefficients expressed in root mean square (RMS) of ICL implantation (black bars) and RMS provoked by femtosecond laser in situ keratomileusis (F-LASIK; gray bars) for 3-mm (top images) and 5-mm pupils (bottom images).
Figure 2. Radial projection, averaged over all orientations, of the two-dimensional mo-dulation transfer function (MTF) for 780 nm versus spatial frequency (cycles/deg) for a 5-mm pupil and -6 D with ICL implantation (black dashed line) and with femtosecond laser in situ keratomileusis (F-LASIK) (gray dashed line). Diffraction-limited (black line) and retinal contrast threshold curves at a retinal illuminance of 500 td are included (gray line). Error bars are omitted for clarity; the deviation of the modulation transfer at any spatial frequency was typically 10% of the mean value.

*Ćĉąúćčúûąþ�üĈąąúĆþċ�ąþćČ�úćý�ÿþĆčĈČþüĈćý�ąúČþċ�ÿĈċ�ĆĒĈĉĂú��üĈĆĉúċĂČĈć�ĎČĂćĀ�úć�úýúĉčĂďþ�ĈĉčĂüČ�ďĂČĎúą�ČĂĆĎąúčĈċ
106 "SR�#SBT�0GUBMNPM����������������
LASIK and offers a better retinal image quality(28). However, an ICL im plantation may induce HOAs after its implantation by the innate optical properties of the lens (i.e., spherical aberration increases with ICL power) or by the incision type performed during the surgical pro-cedure(29). Despite that F-LASIK induces less HOAs than mechanical microkeratome LASIK(5), these values are higher than those found in patients who underwent ICL implantation for myopia(28).
MTF shows how the optical system transmitted spatial frequen-cies. The loss of high frequencies indicates a loss of information regarding the details of an object, thus decreasing the image quality and VA. For -6-D, F-LASIK-MTF was worse than ICL-MTF, which was close to the diffraction-limited MTF, and therefore provides a better optical quality (Figure 2). These results agree with the calculated RMS values of the Zernike coefficients and PSF images (Figure 3). The PSF
images after F-LASIK were worse than those after ICL implantation for both -3 D and -6 D. Note in the F-LASIK PSF images that the increase in spherical aberration is nicely illustrated.
Sarver et al.(28) compared the image quality following LASIK and ICL implantation performed to correct high myopia. They found higher HOAs after LASIK than after ICL implantation. They represented the two-dimensional PSFs and observed the PSFs corresponding to the LASIK aberration values were more spread out than the ICL aberration values. These findings are in agreement with our findings in which we found more HOAs after F-LASIK than after ICL implantation (note the spread of the PSFs shown in Figure 3). Uozato et al.(30) obtained MTFs for different myopic ICL powers using a model eye at various pupil diameters. The outcomes reported by these authors for the -5-D ICL model with a 5-mm pupil were quite similar with those obtained in
Figure 3. Point spread function (PSF) for a 5-mm pupil for -3 D and -6 D with ICL implanta-tion (top images) and femtosecond laser in situ keratomileusis (F-LASIK) (bottom images).
Figure 4. Visual acuity (VA) logMAR and fraction Snellen at high (100%), medium (50%), and low (10%) contrast, with ICL implantation (black bars) and femtosecond laser in situ keratomileusis (F-LASIK) (gray bars) for-3 D and -6 D and a 3-mm pupil. Errors bars represent the standard deviation (SD).
(*) Statistically significant differences (p<0.05).

1Įċþē�7ĂďþČ�$ �þč�úą�
107"SR�#SBT�0GUBMNPM����������������
Figure 5. Visual acuity (VA) logMAR and fraction Snellen at high (100%), medium (50%), and low (10%) contrast, with ICL implantation (black bars) and femtosecond laser in situ keratomileusis (F-LASIK) (gray bars) for -3 D and -6 D and a 5-mm pupil. Errors bars represent the standard deviation (SD).
Figure 6. Mean log contrast sensitivities (CS) at three spatial frequencies: 10, 20, and 25 cycles/degree (cpd) for -3 D and -6 D and a 3-mm pupil with ICL implantation (black points) and femtosecond laser in situ keratomileusis (F-LASIK) (gray squares). Error bars have been omitted for clarity.
Figure 7. Mean log contrast sensitivities (CS) at three spatial frequencies: 10, 20, and 25 cycles/degree (cpd) for -3 D and -6 D with ICL implantation (black points) and femtosecond laser in situ keratomileusis (F-LASIK) (gray squares) with a 5-mm pupil. Error bars have been omitted for clarity.
(*) Statistically significant differences (p<0.05).
(*) Statistically significant differences (p<0.05).
(*) Statistically significant differences (p<0.05).

*Ćĉąúćčúûąþ�üĈąąúĆþċ�ąþćČ�úćý�ÿþĆčĈČþüĈćý�ąúČþċ�ÿĈċ�ĆĒĈĉĂú��üĈĆĉúċĂČĈć�ĎČĂćĀ�úć�úýúĉčĂďþ�ĈĉčĂüČ�ďĂČĎúą�ČĂĆĎąúčĈċ
��� "SR�#SBT�0GUBMNPM����������������
our study. Pérez-Vives et al.(16) recently compared optical and visual quality after ICL implantation and LASIK using an adaptive optics simulator. They found better MTF and PSF images after ICL implanta-tion than after LASIK. They concluded that these outcomes were due to LASIK producing larger HOAs.
VISUAL QUALITY
With a 3-mm pupil, VA values were sufficient for both procedures, achieving values above 20/20 at high and medium contrasts for -3 D and -6 D (Figure 4). At low contrast, VA decreased for both treatments. We found statistically significant differences between ICL implanta-tion and F-LASIK for -3 D and -6 D at all contrasts evaluated (p<0.05). For ICL implantation with a 5-mm pupil, VA values for -3 D and -6 D were above 20/20 at high and medium contrasts and above 20/40 for low contrast (Figure 5). These values decreased for F-LASIK, which had VA values for both powers below 20/20 at high and medium contrasts and below 20/40 for low contrast. We found statistically significant differences between both procedures for -3 D and -6 D and all contrasts evaluated (p<0.05). In all cases, VA values were better after ICL implantation than after F-LASIK.
Several studies compared mechanical microkeratome LASIK and ICL treatments(13-16). These studies were in agreement that the eyes that underwent ICL implantation had the best spectacle correction visual acuity (BSCVA) and uncorrected visual acuity (UCVA) compa-red with eyes that underwent LASIK. Sanders et al.(13) compared the outcomes after LASIK and ICL treatments in eyes between -8 and -12 D of myopia. One year after surgery, 90% ICL patients showed 20/20 or better BSCVA, in contrast 82% LASIK patients showed these VA values. With regard to UCVA, ICL patients also showed a large percentage of eyes with 20/20 or better UCVA (36% LASIK and 52% ICL). More recently, Sanders obtained similar outcomes(15) by compa-ring ICL implantation and LASIK for myopia of -3.00 to -7.88 D. After 6 months, Sanders found better results in the ICL group: 85% patients in the LASIK group and 95% in the ICL group obtained a BSCVA ≥20/20. Pérez-Vives et al.(16) compared optical and visual quality after ICL implantation and LASIK for -3 D and -6 D using an adaptive optics visual simulation. Regarding VA values, they found better outcomes after ICL implantation: 100% eyes had 20/20 or better VA for both ICL powers. In contrast, with LASIK, they found 91.6% and 83.3% eyes with 20/20 or better VA values for -3 D and -6 D, respectively. Despite that we compared ICL implantation with F-LASIK, our findings agree with those reported by those studies, as we found better optical and visual quality outcomes with ICL implantation than those found with F-LASIK. With ICL implantation, VA was 20/20 or better in 100% eyes for -3 D and 93.3% eyes for -6 D. In contrast, with F-LASIK, VA was 20/20 or better in 91.6% eyes for -3 D and 86.6% eyes for -6 D.
Regarding CS outcomes, CS values were good after ICL implanta-tion and F-LASIK (Figures 6 and 7). For -3 D, we found no statistically significant differences between surgeries at any spatial frequency and for both 3-mm and 5-mm pupils (p>0.05). In contrast, for -6 D, the effect of the aberrations was apparent by finding statistically signifi-cant differences for both pupils and all spatial frequencies evaluated (p<0.05). In all cases, CS values were better with ICL implantation than with F-LASIK. Pérez-Vives et al.(16) also evaluated CS values in their comparison study between ICL implantation and LASIK; their outcomes are in agreement with those obtained in the present study.
Although F-LASIK induces fewer aberrations than microkeratome LASIK(5), the differences in VA and CS between the techniques are minimal when we compare our results with other studies that used microkeratome instead of the femtosecond laser(13-16). However, some studies(7) reported statistically significant differences in CS between the techniques at high frequencies.
The visual optics simulator allows us to compare the impact of different surgical techniques on visual quality in the same patient before surgery. In this study, we did not considered factors regarding the surgeon, lens decentrations, or postoperative changes(31), which may affect the visual outcomes of ICL.
In summary, ICL implantation and F- LASIK provide good optical and visual quality, although ICL provides better outcomes than F-LASIK for MTF, PSF, VA, and CS, especially for higher refractive errors and pupil sizes. These outcomes are due to F-LASIK producing larger HOAs than ICL implantation.
REFERENCES 1. Vogel A, Günther T, Asiyo-Vogel M, Birngruber R. Factors determining the refractive
effects of intrastromal photorefractive keratectomy with the picoseconds laser. J Cataract Refract Surg. 1997;23(9):1301-10.
2. Kurtz RM, Horvath C, Liu HH, Krueger RR, Juhasz T. Lamellar refractive surgery with scanned intrastromal picosecond and femtosecond laser pulses in animal eyes. J Refract Surg. 1998;14(5):541-8.
3. Juhasz T, Loesel FH, Kurtz RM, Horvath C, Bille JF, Mourou G. Corneal refractive surgery with femtosecond lasers. IEEE J Selected Topics Quantum Electron. 1999;5(4):902-10.
4. Ratkay-Taub I, Juhasz T, Horvath C, Suarez C, Kiss K, Ferincz I, Kurtz R. Ultra-short pulse (femtosecond) laser surgery: initial use in LASIK flap creation. Ophthalmol Clin North Am. 2001;14(2):347-55.
5. Zhang ZH, Jin HY, Suo Y, Patel SV, Montés-Micó R, Manche EE, Xu X. Femtosecond laser versus mechanical microkeratome laser in situ keratomileusis for myopia: Me-taanalysis of randomized controlled trials. J Cataract Refract Surg. 2011;37(12):2151-9.
6. Montés-Micó R, Rodríguez-Galiero A, Alió JL. Contrast sensitivity after LASIK flap cre-ation with femtosecond laser and mechanical microkeratome. J Refract Surg. 2007; 23(2):188-92.
7. Montés-Micó R, Rodríguez-Galiero A, Alió JL. Femtosecond laser versus mechanical ke ratome LASIK for myopia. Ophthalmology. 2007;114(1):62-8.
8. Sanders DR, Vukich JA, Doney K, Gaston M; Implantable Contact Lens in Treatment of Myopia Study Group. U.S. Food and Drug Administration clinical trial of the implanta-ble contact lens for moderate to high myopia. Ophthalmology. 2003;110(2):255-66.
9. Sanders DR, Doney K, Poco M; ICL in Treatment of Myopia Study Group. United States Food and Drug Administration clinical trial of the Implantable Collamer Lens (ICL) for moderate to high myopia; three-year follow up. Ophthalmology. 2004;111(9):1683-92.
10. Alfonso JF, Baamonde B, Fernández-Vega L, Fernandes P, González-Méijome JM, Montés-Micó R. Posterior chamber collagen copolymer phakic intraocular lenses to correct myopia: Five-year follow-up. J Cataract Refract Surg. 2011;37(5):873-80.
11. Pérez-Vives C, Ferrer-Blasco T, Domínguez-Vicent A, García-Lázaro S, Montés-Micó R. Optical and visual quality of the visian implantable collamer lens using an adaptive-optics visual simulator. Am J Ophthalmol. 2013;155(3):499-507.
12. Pérez-Vives C, Domínguez-Vicent A, Ferrer-Blasco T, Pons AM, Montés-Micó R. Optical quality of the visian implantable collamer lens for different refractive powers. Graefes Arch Clin Exp Ophthalmol. 2013;251(5):1423-9.
13. Sanders DR, Vukich JA. Comparison of implantable contact lens and laser assisted in situ keratomileusis for moderate to high myopia. Cornea. 2003;22(4):324-31.
14. Sanders DR, Vukich JA. Comparison of implantable collamer lens (ICL) and laser-assisted in situ keratomileusis (LASIK) for low myopia. Cornea. 2006;25(10):1139-46.
15. Sanders DR. Matched population comparison of the Visian implantable collamer lens and standard LASIK for myopia of -3.00 to -7.88 diopters. J Refract Surg. 2007;23(6): 537-53.
16. Pérez-Vives C, Dominguez-Vicent A, García-Lázaro S, Ferrer-Blasco T, Montés-Micó R. Optical and visual quality comparison of implantable Collamer lens and laser in situ keratomileusis for myopia using an adaptive optics visual simulator. Eur J Ophthal-mol. 2012, Jul 30; DOI:10.5301/ejo.5000188.
17. Fernandez EJ, Vabre L, Hermann B, Unterhuber A, Povazay B, Drexler W. Adaptive optics with a magnetic deformable mirror: applications in the human eye. Optics Express. 2006;14(20):8900-17.
18. Madrid-Costa D, Ruiz-Alcocer J, Pérez-Vives C, Ferrer-Blasco T, López-Gil N, Montés-Micó R. Visual simulation through different intraocular lenses using adaptive optics: effect of tilt and decentration. J Cataract Refract Surg. 2012;38(6):947-58.
19. Madrid-Costa D, Pérez-Vives C, Ruiz-Alcocer J, Albarrán-Diego C, Montés-Micó R. Visual simulation through different intraocular lenses in patients with previous myopic cor neal ablation using adaptive optics: impact of tilt and decentration. J Cataract Refract Surg. 2012;38(5):774-86.
20. Ruiz-Alcocer J, Pérez-Vives C, Madrid-Costa D, López-Gil N, Montés-Micó R. Effect of simulated IOL tilt and decentration on spherical aberration after hyperopic LASIK for different intraocular lenses. J Refract Surg. 2012;28(5):327-34.
21. Meeteren AV. Calculations on the optical modulation transfer function of the human eye for white light. Opt Acta. 1974;21:395-412.
22. Marsack JD, Thibos LN, Applegate RA. Metrics of optical quality derived from wave aberrations predict visual performance. Journal of Vision. 2004;4(4):322-8.
23. Bach M. The “Freiburg Visual Acuity Test”- automatic measurement of visual acuity. Optom Vis Sci. 1996;73(1):49-53.
24. Lieberman HR, Pentland AP. Microcomputer-based estimation of psychophysical threshol-ds: the best PEST. Behavior Research Methods & Instrumentation. 1982;14(1):21-5.
25. Rocha KM, Vabre L, Harms F, Chateau N, Krueger RR. Effects of Zernike wavefront aber-rations on visual acuity measured using electromagnetic adaptive optics technology. J Refract Surg. 2007;23(9):953-9.
26. Rocha KM, Vabre L, Chateau N, Krueger RR. Enhanced visual acuity and image per-ception following correction of highly aberrated eyes using an adaptive optics visual simulator. J Refract Surg. 2010;26(1):52-6.

1Įċþē�7ĂďþČ�$ �þč�úą�
109"SR�#SBT�0GUBMNPM����������������
27. Gatinel D, Adam PA, Chaabouni S, et al. Comparison of corneal and total ocular aber-ra tions before and after myopic LASIK. J Refract Surg. 2010;26(5):333-40.
28. Sarver EJ, Sanders DR, Vukich JA. Image quality in myopic eyes corrected with laser in situ keratomileusis and phakic intraocular lens. J Refract Surg. 2003;19(4):397-404.
29. Kim SW, Yang H, Yoon G, et al. Higher-order aberration changes after implantable collamer lens implantation for myopia. Am J Ophthalmol. 2011;151(4):653-62.
30. Uozato H, Shimizu K, Kawamorita T, Ohmoto F. Modulation transfer function of intrao-cular collamer lens with a central artificial hole. Graefes Arch Clin Exp Ophthalmol. 2011; 249(7):1081-5.
31. Fernandes P, González-Méijome JM, Madrid-Costa D, Ferrer-Blasco T, Jorge J, Montés-Micó R. Implantable collamer posterior chamber intraocular lenses: a review of potential complications. J Refract Surg. 2011;27(10):765-76.
XXI Congresso Brasileiro de Prevenção da Cegueira e Reabilitação Visual
II Congresso de Oftalmologia de Língua Portuguesa
3 a 6 de setembro de 2014 Centro de Convenções de Pernambuco
Recife (PE)
Informações: ASSESSOR - Assessoria e Marketing
Tels.: (81) 3423-1300 / 9172-7580 E-mail: [email protected]
MAIS EventosTels.: (81) 3033-5147 / 81 8129-4354 E-mail: [email protected]
Site: http://www.congressocbo.com.br/cbo2014/

110 "SR�#SBT�0GUBMNPM����������������
0ċĂĀĂćúą�"ċčĂüąþ�
Quality of life of patients with strabismus
Qualidade de vida em pacientes estrábicos
geRaldo de baRRos RibeiRo1, ana gabRiela zum baCh1, Camila maia FaRia1, suze anastásia1, hendeRson Celestino de almeida1
Submitted for publication: May 21, 2013 Accepted for publication: November 7, 2013
Study conducted at Strabismus Sector, Hospital São Geraldo, Federal University of Minas Gerais (UFMG), Belo Horizonte, MG, Brazil.
1 Hospital São Geraldo, Federal University of Minas Gerais (UFMG), Belo Horizonte, MG, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Geraldo de Barros Ribeiro. Av. Silviano Brandão, 1600 - Belo Horizonte (MG) - 31015-015 - Brazil - E-mail: [email protected]
Approved by the Research Ethics Committee of the Hospital das Clínicas at UFMG on 09/28/2011
INTRODUCTION Strabismus is one of the ophthalmological problems that can
affect the quality of life of individuals. The quantitative assessment of the quality of life of patients with strabismus may be an impor-tant addition to clinical examination because it allows for a greater understanding of the condition and a proper assessment of the effectiveness of treatment(1).
The main purpose of strabismus treatment is the alignment of the visual axes in order to achieve single binocular vision with good image fusion. Other advantages of strabismus correction include the improvement of any abnormal head posture, expansion of the visual field, restoration of stereoscopic acuity, centralization of the
ABSTRACT Purpose: To evaluate the impact of strabismus on quality of life.Methods: This cross-sectional study included 101 individuals aged 7-67 years with strabismus. They were interviewed and made to answer a questionnaire with 20 questions intended to assess the individual’s interaction with their social and working environment, sensory perception, and limitations in their daily lives. There were five types of possible responses for each question: never, rarely or very few times, sometimes, frequently, and always. The questionnaire was based on the AS-20 and contained 11 questions assessing psychosocial aspects and 9 questions assessing functional aspects. Among those who were interviewed, 24.8% had undergone surgical correction of strabismus. Results: We observed a significant impact of strabismus on the quality of life of the interviewed individuals. Feelings of sadness and inferiority because of stra-bismus were reported by 74.2% and 58.4% respondents, respectively. In terms of functionality, 12.1% reported difficulty in reading, 14% said they had difficulty in depth perception (stereopsis), and 17.8% frequently or always associated pain or burning sensation in the eyes to strabismus. A significant difference was detected in the quality of life scores for the psychosocial aspect among patients who had and had not undergone surgery (Wilcoxon test, 158; p<0.001). Individuals who had undergone surgery had a better quality of life from the psychosocial perspective.Conclusions: In this evaluation, we found a significant negative interference of strabismus on quality of life from both the functional and psychosocial perspecti-ves. This demonstrated the importance of treatment for strabismus, regardless of age, because it can interfere with the functional well-being of the individual.
Keywords: Strabismus/physiopathology; Social behavior; Quality of life; Ques-tionnaires
RESUMOObjetivo: Avaliar a interferência do estrabismo na qualidade de vida em indivíduos estrábicos.Métodos: Estudo transversal envolvendo 101 indivíduos estrábicos entre 7 e 67 anos. Eles foram entrevistados e responderam um questionário com 20 perguntas aplica-das pelos pesquisadores. As perguntas tinham como objetivo avaliar a interação do indivíduo com o seu meio social, de trabalho, percepção sensorial e limitações na sua vida diária, com cinco tipos de respostas para cada pergunta: nunca, raramente ou muito pouco, algumas vezes, frequentemente e sempre. O questionário foi baseado no AS-20 e contendo 11 questões avaliando aspectos psicossociais e 9 questões avaliando aspectos funcionais. Entre os indivíduos entrevistados, 24,8% haviam sido submetidos a correção cirúrgica do estrabismo.Resultados: Observou-se impacto significativo do estrabismo sobre a qualidade de vida dos indivíduos avaliados. Sentir-se incomodado ou inferiorizado em decorrência do estrabismo foram relatados por 74,2% e 58,4% dos entrevistados respectivamente. No quesito de funcionalidade, 12,1% relataram dificuldade para ler, 14% disseram ter dificuldade na percepção de profundidade (estereopsia) e 17,8% associaram dor ou ardor nos olhos ao estrabismo frequentemente ou sempre. Diferença significativa foi detectada com respeito ao escore de qualidade de vida no aspecto psicossocial entre indivíduos que realizaram e não realizaram cirurgia (teste de Wilcoxon = 158, p-valor <0,001). Indivíduos que realizaram cirurgia possuíam melhor qualidade de vida no aspecto psicossocial. Conclusões: Nessa avaliação, percebe-se uma interferência negativa muito signi-ficativa do estrabismo na qualidade de vida, tanto funcional como psicossocial nos indivíduos pesquisados. Isso demonstra a importância do tratamento do estrabismo, independente da idade, pois ele pode interferir muito na qualidade de vida e bem estar psicossocial e funcional do indivíduo.
Descritores: Estrabismo/fisiopatologia; comportamento social; Qualidade de vida; Questionários
visual field, elimination of diplopia, improvement in ocular motility, improvement in psychomotor development, and restoration of nor-mal appearance(2-7).
Both children and adults with strabismus suffer frequently from various psychosocial and emotional problems such as low self-esteem, negative social prejudice, school bullying, increased social anxiety, fragile interpersonal relations, and job opportunity issues. Strabismus is known by the lay population only as a physiognomic esthetic de-fect that causes damaged self-esteem and hinders relationships and psychosocial relations. Many authors condemn the use of the terms esthetic or cosmetic for the treatment of strabismus because these terms mean “something made to improve or embellish.” However,

3ĂûþĂċĈ�(# �þč�úą�
111"SR�#SBT�0GUBMNPM����������������
strabismus is a pathological state caused by a process from an un-derlying disease associated with abnormal binocular vision that leads to a change in the normal appearance of an individual and can affect the quality of life(8-12).
In recent years, many studies have evaluated the strabismus-re-lated quality of life (SRQOL). There are some specific instruments for SRQOL assessment, which were elaborated on the basis of interviews with patients and their relatives. Feelings and expressions have been thus collected and used by doctors and researchers for the de velopment of more objective and efficient questionnaires for mea-suring the impact of strabismus on the patients’ quality of life(13-17).
In 2009, the AS-20 questionnaire was developed for the assessment of SRQOL. It can be used in everyday clinical practice or as a research tool and can be filled out by the patient without supervision. The full version is available with no restrictions as long as it is identified by quoting its original description(13). On this basis, we developed a similar questionnaire with small changes caused by cultural diffe-rences and forms of expression in our country. The questionnaire established by our department was conducted by the researchers instead of being filled out by the patient alone. With this, we could better explain the purpose of the research and the questions, making it possible for use in children aged >8 years. The purpose of this study was to assess and compare the psychosocial, emotional, and functional consequences of strabismus in a portion of the Bra-zilian population.
METHODS This study was approved by the Research Ethics Committee of
the Hospital das Clínicas at Universidade Federal de Minas Gerais (UFMG) on 09/28/2011. It was conducted in the Strabismus Sector of Hospital São Geraldo at UFMG. A semistructured interview was conducted with individuals aged >7 years old after their parents provided written informed consent. The patients underwent iden-tification and complete eye examination. A questionnaire assessing
strabismus was filled out by the researchers. In addition, the patients completed a specific questionnaire with 20 questions about quality of life (Annex) that was performed specifically for the study. This ques-tionnaire was created by the researchers on the basis of AS-20(13). Its purpose was to assess patient interaction within social and working environments, sensory perception, and daily life limitations, with five types of answers for each question: never, rarely or very few times, sometimes, frequently, or always. This strategy aimed to facilitate the patient’s understanding, make the answering of questions easier, and allow for fewer false-negative answers.
RESULTSTotally, 101 individuals aged 7-67 years were interviewed. The
ave rage age of patients was 22.7 years, with the majority being ≤18 years (53.4%). With regard to the subgroups, a relative predomi-nance of women (61.4%) was observed. With regard to the type of strabismus, 58.4% respondents had esotropia, 37.6% had exotropia, 2% had dissociated vertical deviation (DVD), 1% had left eye hypotro-pia, and 1% did not have any deviations because he had previously undergone corrective surgery. At the time of the study, the patients were interviewed in the strabismus outpatient department; 75.2% had not undergone strabismus correction surgery and 24.8% had already undergone surgery an average of 2.7 years before the inter-view. The number of answers for each question and the respective percentages are shown in table 1.
For the first question in the quality of life questionnaire, 68.3% pa-tients always noticed that they had strabismus, and when added to-gether with the answers of “frequently” and “sometimes”, this number increased to 83.1%. When asked how frequently strabismus bothered them, 49.5% reported that it always did, and when combined toge-ther with the answers “frequently” and “sometimes”, this percentage increased to 74.2%. The majority of the patients (54.4%) thought that people were always staring at their eyes, and only 15.8% thought that people never noticed their strabismus. When asked if they felt
Annex. Questionnaire on the impact of strabismus on patient quality of life
Questions NeverRarely or very
few times Sometimes Frequently Always
01- Do you notice you have strabismus (crossed eyes or lazy eyes)?
02- Does strabismus bother you?
03- When you interact with other people, do you feel they notice your strabismus?
04- Do you feel different (inferior) because of strabismus?
05- Do you feel that strabismus hinders your performance (at school or at work)?
06- Do you feel that strabismus affects your relations with other people?
07- Do you feel that your opportunities (social interaction or at work) are fewer because of strabismus?
08- Do you imagine what other people are thinking about your eyes?
09- Do you have more difficulty in making friends because of strabismus?
10- Do you feel uncomfortable if someone asks something about your eyes?
11- Do you feel that people avoid looking at you because of strabismus?
12- Does strabismus hinder your vision?
13- Do you have difficulty in reading because of strabismus?
14- Do you feel more stressed out (anxious) because of strabismus?
15- Do you have difficulty in depth perception (assess the distance of objects)?
16- Do you feel any discomfort such as pain or burning sensation in the eyes because of strabismus?
17- Do you have to close one of your eyes to read?
18- Do you have diplopia (double vision)?
19- Do you feel eye strain because of strabismus?
20- Do you think about your strabismus so frequently that it hinders your concentration?

2ĎúąĂčĒ�Ĉÿ�ąĂÿþ�Ĉÿ�ĉúčĂþćčČ�ĐĂčā�ČčċúûĂČĆĎČ
112 "SR�#SBT�0GUBMNPM����������������
Table 1. Answers for the 20 questions (Q1 to Q20) with absolute numbers and the percentage for each one of them in brackets
Never Rarely or very few times Sometimes Frequently Always
Q1 16 (15.84) 01 (00.99) 12 (11.88) 3 (2.97) 69 (68.32)
Q2 18 (17.82) 08 (07.92) 21 (20.79) 4 (3.96) 50 (49.50)
Q3 16 (15.84) 04 (03.96) 20 (19.80) 6 (5.94) 55 (54.46)
Q4 38 (37.62) 04 (03.96) 14 (13.86) 3 (2.97) 42 (41.58)
Q5 52 (51.49) 07 (06.93) 14 (13.86) 5 (4.95) 23 (22.77)
Q6 48 (47.52) 10 (09.90) 18 (17.82) 3 (2.97) 22 (21.78)
Q7 52 (51.49) 04 (03.96) 19 (18.81) 7 (6.93) 19 (18.81)
Q8 29 (28.71) 05 (04.95) 26 (25.74) 6 (5.94) 35 (34.65)
Q9 63 (62.38) 02 (01.98) 17 (16.83) 2 (1.98) 17 (16.83)
Q10 36 (35.64) 02 (01.98) 27 (26.73) 3 (2.97) 33 (32.67)
Q11 59 (58.42) 07 (06.93) 18 (17.82) 2 (1.98) 15 (14.85)
Q12 58 (57.43) 08 (07.92) 12 (11.88) 5 (4.95) 18 (17.82)
Q13 69 (68.31) 05 (04.95) 15 (14.85) 3 (2.97) 09 (08.91)
Q14 52 (51.49) 05 (04.95) 16 (15.84) 7 (6.93) 21 (20.79)
Q15 69 (69.00) 05 (05.00) 12 (12.00) 3 (3.00) 11 (11.00)
Q16 43 (42.57) 08 (07.92) 32 (31.68) 6 (5.94) 12 (11.88)
Q17 84 (83.16) 02 (01.98) 09 (08.91) 0 (0.00) 06 (05.94)
Q18 83 (82.18) 03 (02.97) 09 (08.91) 1 (0.99) 05 (04.95)
Q19 52 (51.49) 03 (02.97) 27 (26.73) 6 (5.94) 13 (12.87)
Q20 52 (51.49) 02 (01.98) 18 (17.82) 9 (8.91) 20 (19.80)
inferior because of the strabismus, 41.5% reported that they always did. If we considered the answers “sometimes” and “frequently”, this percentage increased to 58.4%. Of all the interviewed patients, 22.7% felt that strabismus affected their performance at school or work.
In terms of their relationships with other people, 53% patients felt that strabismus affected their interpersonal relationships at some point in their lives. Of those patients, 22% felt that this was a constant problem. They were asked if social interaction and job opportunities were diminished because of strabismus, and 44.5% answered that it always, frequently, or sometimes happened in their lives.
The majority of patients (71.2%) imagined what other people thought about their eyes, and 34.6% observed the same. The majority of the patients (62.3%) answered that strabismus never prevented them from making friends, but 16.8% felt that it always interfered. The majority of patients (62.3%) always, frequently, or sometimes felt upset when somebody asked them about their eyes, and 16.8% felt that people frequently or always avoided looking at them.
When asked if strabismus hindered their vision, 22.7% answered that they were frequently or always impaired by their problem, and 12.1% said that they had difficulty in reading because of strabismus. With regard to an increase in anxiety related to strabismus, 27.7% were always or frequently anxious. When asked about their assess-ment of depth perception or the evaluation of the distance between objects, 11% patients reported that they always faced this difficulty. Pain or burning sensation in the eyes was also associated with strabis-mus; 57.4% patients felt some kind of discomfort. Of all the patients interviewed, 84% reported that they never had to close one eye while reading. The majority of patients (82.1%) did not complain of double vision, but this always happened to 4.9%. Many patients related eye strain with strabismus, 26.7% sometimes felt eye strain, and 18.8% always or frequently felt eye strain. In addition, many patients repor-ted attention deficits related to the problem: 19.8% always experien-ced them and 26.7% sometimes or frequently experienced them.
A significant difference was detected in quality of life scores for the psychosocial aspect between patients who had and had not undergone surgery (Wilcoxon test, 158; p<0.001). Individuals who
underwent surgery had a better quality of life from the psychosocial aspect (the median value for individuals who did not undergo sur-gery was -0.467, while that for those who underwent surgery was 1.095). The same difference was detected for the total quality of life score (Wilcoxon test, 169; p<0.001). Individuals who underwent sur-gery had a better total quality of life (the median value for individuals who did not undergo surgery was -0.475, while that for individuals who underwent surgery was 1.21). No significant difference was detected at the 5% level in the functional aspect of the quality of life score between individuals who had and had not undergone surgery.
DISCUSSIONSome quality of life studies have demonstrated that strabismus
may have a more harmful effect than diabetic retinopathy, macular degeneration, or a mild cerebrovascular accident(18). This study de-monstrated that strabismus in adults was associated not only with functional effects but also with psychosocial negative effects; both can have a great influence on all aspects of the patient’s life.
Reports of the psychosocial negative effects of strabismus in adults were published in 1993; the patients said that every aspect of their lives was affected by strabismus, such as self-esteem, employment prospects, interpersonal relationships, education, and playing sports(19). More severe manifestations have been observed, including an increa-se in the occurrence of psychiatric disorders in young adults with strabismus, particularly exotropia. A study determined that 41.3% patients with strabismus developed mental health problems compa-red with 30.7% from the control group(20,21)
In order to assess the quality of life, it is necessary to focus on the problems associated with the disease of interest. Therefore, it is im-portant to develop specific assessment tools. Previous studies have quantified the negative effects of strabismus using a variety of ge-neric questionnaires that were nonspecific for strabismus, such as the Time Trade-Off (TTO) (how much time of their life they would use to achieve perfect vision) or the Standard Gamble (SG: what would they risk in order to achieve perfect vision). According to the former, there was a 3.7% decrease in quality of life(20,22,23).

3ĂûþĂċĈ�(# �þč�úą�
113"SR�#SBT�0GUBMNPM����������������
CONCLUSIONSIn our study, we managed to capture the perception of younger
individuals aged >7 years, which is the age at which a child can recognize the interference of strabismus with the functional and psychosocial aspects of his or her life. Our study demonstrated that strabismus interfered with patient quality of life. A significant variation was observed in the psychosocial aspect of quality of life between patients who had and had not undergone surgical treat-ment. With this information, new studies can be conducted for the assessment of quality of life before and after surgical treatment in patients with strabismus.
REFERENCES 1. Leske DA, Hatt SR, Holmes JM. Test-retest reliability of health-related quality-of-life
questionnaires in adults with strabismus. Am J Ophthalmol. 2010;149(4):672-6. 2. Assaf AA. The sensitive period: transfer of fixation after occlusion for strabismic am-
blyopia. Br J Ophthalmol. 1982;66(1):64-70. 3. Von Noorden GK. Binocular vision and ocular motility. 4th ed. St Louis: Mosby; 1990. 4. Pediatric Eye Disease Investigator Group. A randomized trial of atropine vs. patching
for treatment of moderate amblyopia in children. Arch Ophthalmol. 2002;120(3):268-78. Comment in: Arch Ophthalmol. 2002;120(3):387-8.
5. Van Leeuwen R, Eijkemans MJ, Vingerling JR, Hofman A, de Jong PT, Simonsz HJ. Risk of bilateral visual impairment in individuals with amblyopia: the Rotterdam study. Br J Ophthalmol. 2007;91(11):1450-1. Comment in: Br J Ophthalmol. 2007;91(11):1417-8.
6. Rahi J, Logan S, Timms C, Russell-Eggitt I, Taylor D. Risk, causes, and outcomes of visual impairment after loss of vision in the non-amblyopic eye: A population-based study. Lancet. 2002;360(9333):597-602.
7. Packwood EA, Cruz OA, Rychwalski PJ, Keech RV. The psychosocial effects of amblyo-pia study. J AAPOS. 1999;3(1):15-7.
8. Chua B, Mitchell P. Consequences of amblyopia on education, occupation, and long term vision loss. Br J Ophthalmol. 2004;88(9):1119-21. Comment in: Br J Ophthalmol. 2004;88(9):1105-6.
9. van de Graaf ES, van Kempen-du Saar H, Looman CW, Simonsz HJ. Utility analysis of disability caused by amblyopia and/or strabismus in a population-based, historic cohort. Graefes Arch Clin Exp Ophthalmol. 2010;248(12):1803-7.
10. Kothari M, Balankhes S, Gawade R, Toshnival S. Comparison of psychosocial and emotional consequences of childhood strabismus on the families from rural and urban India. Indian J Ophthalmol. 2009;57(4):285-8. Comment in: Indian J Ophthalmol. 2010; 58(3):257-8; author reply 258-9.
11. Jackson S, Harrad RA, Morris M, Rumsey N. The psychosocial benefits of corrective surgery for adults with strabismus. Br J Ophthalmol. 2006;90(7):883-8.
12. Beauchamp GR, Felius J, Stager DR, Beauchamp CL. The utility of strabismus in adults. Trans Am Ophthalmol Soc. 2005;103:164-71; discussion 171-2.
13. Hatt SR, Leske DA, Bradley EA, Cole SR, Holmes JM. Comparison of quality-of-life instruments in adults with strabismus. Am J Ophthalmol. 2009;148(4):558-62.
14. van de Graaf ES, Felius J, van Kempen-du Saar H, Looman CW, Passchier J, Kelderman H, et al. Construct validation of the Amblyopia and Strabismus Questionnaire (A&SQ) by factor analysis. Graefes Arch Clin Exp Ophthalmol. 2009;247(9):1263-8.
15. Hatt SR, Leske DA, Bradley EA, Cole SR, Holmes JM. Development of a quality-of-life questionnaire for adults with strabismus. Ophthalmology. 2009;116(1):139-44.
16. Hatt SR, Leske DA, Adams WE, Kirgis PA, Bradley EA, Holmes JM. Quality of life in inter-mittent exotropia: child and parent concerns. Arch Ophthalmol. 2008;126(11):1525-9.
17. Hatt SR, Leske DA, Kirgis PA, Bradley EA, Holmes JM. The effects of strabismus on quality of life in adults. Am J Ophthalmol. 2007;144(5):643-7.
18. Beauchamp CL, Beauchamp GR, Stager DR Sr, Brown MM, Brown GC, Felius J. The cost utility of strabismus surgery in adults. J AAPOS. 2006;10(5):394-9.
19. Satterfield D, Keltner JL, Morrison TL. Psychosocial aspects of strabismus study. Arch Ophthalmol. 1993;111(8):1100-5. Comment in: Arch Ophthalmol. 1994; 112(3):302.
20. Bez Y, Coskun E, Erol K, Cingu AK, Eren Z, Topçuoglu V, et al. Adult strabismus and social phobia: a case-controlled study. J AAPOS. 2009;13(3):249-52.
21. Mohney BG, McKenzie JA, Capo JA, Nusz KJ, Mrazek D, Diehl NN. Mental illness in young adults who had strabismus as children. Pediatrics. 2008;122(5):1033-8.
22. Chua B, Mitchell P. Consequences of amblyopia on education, occupation, and long term vision loss. Br J Ophthalmol. 2004;88(9):1119-21. Comment in: Br J Ophthalmol. 2004;88(9):1105-6.
23. Archer SM, Musch DC, Wren PA, Guire KE, Del Monte MA. Social and emotional impact of strabismus surgery on quality of life in children. J AAPOS. 2005;9(2):148-51.
12o Congresso SOTRIM - Sociedade de Oftalmologia do Triângulo Mineiro
6 a 8 de novembro de 2014Universidade Federal do Triângulo Mineiro (CEA)
Uberaba - MG
Informações: Tels.: (34) 3338-5343/3312-0657

��� "SR�#SBT�0GUBMNPM����������������
$úČþ�3þĉĈċč
INTRODUCTIONCongenital simple hamartoma of the retinal pigment epithelium
(CSHRPE) is an uncommon condition, and few cases have been des-cribed in the literature(1,2). It was first discussed by Laqua in 1981(3), and Gass reported three similar cases that he later published in a review of focal congenital anomalies of the retinal pigment epithelium (RPE)(4). This lesion has particular features on fundoscopic examination, fluo-rescein angiography (FA), and optical coherence tomography (OCT)(5,6).
Tumors of the RPE include congenital hamartoma, congenital hypertrophy, combined hamartoma of the retina and RPE, and ade -noma or adenocarcinoma(7,8). In one study, several authors(9) reported on five cases classified as CSHRPE according to their clinical fea tu res; all of these lesions maintained a stable pattern during the follow-up period.
Here we describe a case of an asymptomatic 56-year-old woman with a unilateral circumscribed and pigmented fundus lesion sugges-tive of CSHRPE on clinical examination and confirmed by FA and OCT.
CASE REPORTA 56-year-old woman was referred for a routine ophthalmic exa -
mination to our institution because of a 20-year history of type 2 diabetes treated with insulin. The Snellen best-corrected visual acuity was 20/20 in both eyes, which did not require correction in the right eye and was corrected with a prescription of +0.75 -0.25 X 130° in
the left. Biomicroscopy examination was normal, and the intraocular pressure corresponded to 12 mmHg and 10 mmHg in her right and left eyes, respectively. Indirect ophthalmoscopy in the right eye was normal, and in the left eye, there was a circumscribed black pos terior pole tumor that was inferotemporal to the fovea. There was no evidence of macular edema, traction, retinal exudation, or subretinal fluid.
Fluorescein angiography and OCT were performed. Angiography revealed a nonfluorescent lesion during all the phases of the exami-nation, including the late phases (Figure 1). OCT revealed an abruptly elevated hyper-reflective mass with deep optical shadowing (Figure 2). The diagnosis was compatible with CSHRPE, and the patient was followed by observation.
DISCUSSIONCSHRPE is a benign tumor that is incidentally diagnosed and in -
volves all layers of the retina. This hamartoma is presumed to be a congenital lesion. It is a rare tumor that can be detected during rou-tine fundus ocular examination. On clinical examination, it appears as a solitary macular lesion that is darkly pigmented, well-defined, and involves the full thickness of the retina. Although FA findings were unremarkable in the present case, hyperfluorescence is occasionally observed in the late phases(1,2). OCT typically shows a complete blocka ge of optical transmission.
Congenital simple hamartoma of the retinal pigment epithelium: a case report
��������ȱ����¹����ȱ�������ȱ��ȱ����·���ȱ����������ȱ��ȱ������DZȱ������ȱ��ȱ����
maRiana Rossi thoRell1, viniCius FeRReiRa kniggendoRF2, luis augusto aRana3, alexandRe aChille gRandinetti2
Submitted for publication: September 23, 2013 Accepted for publication: November 27, 2013
Study conducted at Departamento de Oftalmologia e Otorrinolaringologia do Hospital das Clínicas da Universidade Federal do Paraná (UFPR), Curitiba, PR, Brazil.
1 Bascom Palmer Eye Institute, University of Miami, United States of America.2 Department of Ophthalmology, Universidade Federal do Paraná (UFPR), Curitiba, PR, Brazil.3 Hospital de Olhos do Paraná (HOP), Curitiba, PR, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Alexandre Achille Grandinetti. Av. Vicente Machado, 1.171 - Curitiba (PR) - 80420-011 - Brazil - E-mail: [email protected]
ABSTRACTWe report the case of a 56-year-old woman who presented for a routine ophthal-mological examination without visual symptoms and had a unilateral black retinal lesion that was detected by clinical examination. Fluorescein angiography and optical coherence tomography findings were compatible with a congenital simple hamartoma of the retinal pigment epithelium. It is very important to de tect this tumor and differentiate it from other pigmented fundus lesions that can com-promise visual function or result in systemic conditions such as those caused by malignant tumors.
Keywords: Hamartoma/pathology; Retinal pigment epithelium; Retinal diseases; Congenital abnormalities; Tomography, optical coherence; Case report
RESUMORelato de um caso de paciente feminina de 56 anos que compareceu a uma consulta oftalmológica de rotina sem sintomas visuais e apresentando uma lesão retiniana preta, unilateral, detectada ao exame clínico. As características da angiografia fluo-resceínica e da tomografia de coerência óptica foram compatíveis com ha mar toma congênito simples do epitélio pigmentado da retina. É muito importante detectar este tumor e diferenciá-lo de outras lesões fundoscópicas pigmentadas que podem comprometer a função visual ou, além disso, afetar o paciente sistemicamente como em tumores malignos.
Descritores: Hamartoma; Epitélio pigmentado da retina; Doenças retinianas; Anor-malidades congênitas; Doenças retinianas; Tomografia de coerência óptica; Relato de caso

5āĈċþąą�.3 �þč�úą�
���"SR�#SBT�0GUBMNPM����������������
A
B
Figure 1. Fluorescein angiography of the left eye. A well-circumscribed lesion located inferotemporal to the fovea shows the absence of leakage and the presence of fluo-rescence blockage.
Figure 2. Optical coherence tomography. Slight elevation of the retina is observed at the location of the lesion, which is protruding into the vitreous cavity and shows increased optical reflectivity on its inner surface, with deep optical shadowing of the remaining retina and the entire choroid.
As noted in other reported cases, in this patient, CSHRPE remai-ned stable in size and clinical aspects during the 12 months of fol-low-up, and the patient remains asymptomatic and without changes in visual acuity. Because of these features, adults are generally diag-nosed at an advanced age.
Differential diagnoses include the following: combined hamarto-ma of the retina and RPE, congenital hypertrophy of the RPE (CHRPE), adenoma or adenocarcinoma of the RPE, hyperplasia of the RPE, intra-retinal foreign body, and retinal invasion from an underlying cho roidal nevus (melanocytoma) or choroidal melanoma(2). All these can be ruled out by clinical and complementary examinations, as observed in the described patient.
OCT is a useful noninvasive examination that can help in diag-nosis and provide information about additional features such as vi treoretinal adhesion(10).
In conclusion, it is very important to identify congenital simple hamartomas of the RPE and follow these patients over the long-term to rule out tumor growth and suspicious malignant features.
REFERENCES 1. Lopez JM, Guerrero P. Congenital simple hamartoma of the retinal pigment epithe-
lium: optical coherence tomography and angiography features. Retina. 2006;26(6): 704-6.
2. Shields CL, Materin MA, Shields JA. Review of optical coherence tomography for intraocular tumors. Curr Opin Ophthalmol. 2005;16(3):141-54.
3. Laqua H. Tumors and tumor-like lesions of the retinal pigment epithelium. Ophthal-mologica. 1981;183(1):34-8.
4. Gass JD. Focal congenital anomalies of the retinal pigment epithelium. Eye (Lond). 1989;3(Pt 1):1-18.
5. Madgula IM, Adatia FA, Sagoo MS, Wescott M. Simple hamartoma of the retinal pigment epithelium in a man of African descent. Can J Ophthalmol. 2009;44(4):35-6.
6. Shields CL, Materin MA, Karatza EC, Shields JA. Optical coherence tomography of con-genital simple hamartoma of the retinal pigment epithelium. Retina. 2004;24(2):327-8.
7. Souissi K, El Afrit MA, Kraiem A. Congenital retinal arterial macrovessel and congenital hamartoma of the retinal pigment epithelium. J Pediatr Ophthalmol Strabismus. 2006; 43(3):181-2.
8. Shields JA, Shields CL. Atlas of intraocular tumors. Philadelphia: Lippincott Williams & Wilkins; 1999.
9. Shields CL, Shields JA, Marr BP, Sperber DE, Gass JDM. Congenital simple hamarto-ma of the retinal pigment epithelium - a study of five cases. Ophthalmology. 2003; 110(5):1005-11.
10. Shukla D, Ambatkar S, Jethani J, Kim R. Optical coherence tomography in presumed congenital simple hamartoma of the retinal pigment epithelium. Am J Ophthalmol. 2005;139(5):945-7.

116 "SR�#SBT�0GUBMNPM����������������
$úČþ�3þĉĈċč
INTRODUCTIONExtraocular muscle disease is typically associated with thyroid di -
sease. However, other rarer etiologies such as neoplasms and infec-tion should also be considered(1-4).
Lymphomas are the most common malignant tumors of the orbit in adults, and the majority of these are secondary to other systemic findings(5,6). On the basis of the classification of the World Health Or-ganization (WHO), and with some modifications from the Revised European and American Lymphoma (REAL) classification, the most common histological type is B-cell lymphoma(6-9). Jakobiec recom-mended the term B-cell lymphoma of the extranodal marginal zone to indicate the histological subtype of soft tissue tumors located in the orbit. He also suggested that the designation of mucosa-associa-ted lymphoma (MALT) was not appropriate for cases of muscle invol-vement and should be used only for cases of conjunctival, lacrimal gland, and lacrimal sac area involvement(6).
Certain specific areas such as the conjunctiva, infraorbital tissues, lacrimal system, and extraocular muscles show a good response to treatment and a better prognosis (63%, 58%, 28%, and 13%, respecti-vely)(1,6,9). Eyelid involvement is related to a worse prognosis(6).
Here we describe the case of a 55-year-old man with orbital non-Hodgkin B-cell MALT lymphoma and emphasize its atypical presentation as medial rectus muscle myositis.
CASE REPORTA 55-year-old presented with progressive eye pain and low visual
acuity in the right eye since 2 years. His past medical history was unremarkable, and he denied the use of any medications. He had pre-viously undergone treatment for glaucoma in both eyes with trava-prost and brimonidine. During the ophthalmologic examination, his visual acuity was 20/70 in the right eye and counting fingers at 1.5 m in the left eye. The right eye exhibited proptosis (exophthalmometry base 100 = 31 mm in the right eye and 14 mm in the left eye), which was associated with chemosis, conjunctival hyperemia, lower eyelid retraction, exotropia, and ocular motility limitation (Figure 1). There was no palpable regional lymphadenopathy. According to Goldmann tonometry, his intraocular pressure was 32 mmHg in the right eye and 30 mmHg in the left eye. Fundoscopy revealed a cup-to-disc ratio of 0.9 × total in the right eye and 0.7 × 0.8 in the left eye, with no other changes. Computed tomography (CT) and magnetic resonance ima-ging (MRI) of the orbit showed a significantly larger fusiform medial rectus muscle in the right eye, with tendon involvement (Figure 2).
The patient’s routine laboratory tests were normal, including thyroid hormones and antibodies. The Mantoux test (purified pro-tein derivative; PPD) was strongly reactive (22 mm). A biopsy was scheduled, and the hematoxylin-eosin staining of the biopsied tissue showed a relatively homogeneous small cell population with slight
Medial rectus muscle myositis as an atypical presentation of mucosa-associated
lymphatic tissue lymphoma: a case report
Miosite do músculo reto medial como forma atípica de apresentação de linfoma tipo MALT: relato de caso
Juliana sá FReiRe medRado dias1, miRtha aliCia RamiRez dittRiCh1, JaCqueline maRtins de sousa1, luiz FeRnando teixeiRa1, Paulo gois manso1
Submitted for publication: October 29, 2013 Accepted for publication: November 7, 2013
Study conducted at Department of Ophthalmology, Universidade Federal de São Paulo (UNIFESP), São Paulo, SP, Brazil.
1 Department of Ophthalmology, Universidade Federal de São Paulo (UNIFESP), São Paulo, SP, Brazil.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Jacqueline M. Sousa. Rua Botucatu, 821 - São Paulo (SP) - 04023-062 - Brazil - E-mail: [email protected]
ABSTRACT Here we describe the rare case of a 55-year-old man with medial rectus muscle myositis as an atypical presentation of non-Hodgkin B-cell mucosa-associated lymphoma (MALT). Pathology and immunohistochemistry of the affected muscle confirmed the diagnosis of a neoplasm. The primary etiology of orbital myositis is Graves’ ophthalmopathy, but several other diseases may cause this clinical pre -sentation. Therefore, the neoplastic causes must be eliminated from the differential diagnoses. Non-Hodgkin B-cell mucosa-associated lymphoma is the most common histological type of lymphoma in the orbit, with the conjunctiva and lacrimal glands being the most commonly affected sites. However, it may also present in atypical forms involving others sites and tissues.
Keywords: Orbital neoplasms; Orbital myositis; Oculomotor muscles/pathology; Muscle neoplasms; Orbital neoplasms; Lymphoma, B-Cell, marginal zone; Humans; Male; Middle-aged; Case report
RESUMODescrevemos um raro caso de miosite do músculo reto medial como forma atípica de apresentação de linfoma não-Hodgkin de células B tipo MALT. A anatomia patológica e imuno-histoquímica do músculo afetado confirmaram o diagnóstico definitivo do caráter neoplásico da doença. As miosites orbitárias têm como principal etiologia a oftalmopatia de Graves, porém diversas outras causas podem apresentar-se dessa forma. Sendo assim, as causas neoplásicas devem ser descartadas. O linfoma não-Hodgkin de células B tipo MALT é o tipo histológico mais comum de linfoma orbitário, as regiões mais frequentemente acometidas são a conjuntiva e glândula lacrimal. No entanto, pode apresentar-se com formas clínicas atípicas, acometendo outras regiões e tecidos.
Descritores: Neoplasias orbitárias; Miosite orbital; Músculos oculomotores; Neoplasias musculares; Linfoma de zona marginal tipo células B; Humanos; Masculino; Adulto; Meia-idade; Relato de caso

%ĂúČ�+4'. �þč�úą�
117"SR�#SBT�0GUBMNPM����������������
nuclear irregularity, inconspicuous nucleoli, and scant cytoplasm (Fi -gure 3). Immunohistochemistry confirmed non-Hodgkin B-cell MALT lymphoma that was CD20 (+), CD3 (+), cyclin D1 (−), CD5 (−), CD10 (−), CD23 (−), and BCL2 (−) (Figure 4). The patient was referred to the hematology department for systemic staging and treatment.
DISCUSSIONThe extraocular muscles may be involved in several systemic
di sea ses, initially manifesting as orbital myositis. The most common etiology of this pathology in the orbit is Graves’ ophthalmopathy, whi-ch is an organ-specific autoimmune process with inflammation, ede-ma, and secondary fibrosis. Bilateral symmetric muscle involvement is observed in 70% patients. The usual pattern of clinical involvement in decreasing order of frequency is as follows: inferior, medial, superior, and lateral muscles(3).
In our patient, Graves’ ophthalmopathy was the first diagnostic hypothesis according to the history and clinical findings. Therefore, we requested laboratory tests and imaging studies to confirm this hypothesis. Because the thyroid profile and antithyroid antibodies were normal and CT and MRI findings were unremarkable, the hy-pothesis of Graves’ ophthalmopathy became less likely. During our search for the specific etiology, we also considered infectious causes, which are very common in our country. Then, we asked for several serologies and a PPD, which was the only positive test. At that time, our diagnosis was tuberculosis myositis. To confirm this hypothesis and initiate specific treatment, we performed an incisional biopsy, which, to our surprise, revealed non-Hodgkin B-cell MALT lymphoma.
The causes of nonthyroid-related enlargement of the extrinsic muscles are diverse and include inflammatory (idiopathic, sarcoido-
Figure 1. Ectoscopy showing chemosis, conjunctival hyperemia, lower eyelid retraction, exotropia, and limited ocular motility in the right eye.
Figure 3. Hematoxylin-eosin staining of the affected rectus muscle shows a relatively homogenous small cell population with slight nuclear irregularity, inconspicuous nu-cleoli, and scant cytoplasm.
Figure 4. Immunohistochemistry of the biopsied muscle shows CD20 positivity and cyclin D1, CD5, and CD10 negativity.
Figure 2. Computed tomography (two photos above) and magnetic resonance imaging (four photos below) of the orbit show that the optic nerve is deflected upward and to the side, with fusiform enlargement of the right medial rectus muscle in full extension, tendon involvement, no damage to the bones of the orbital wall, and no signs of cortical erosion.

.þýĂúą�ċþüčĎČ�ĆĎČüąþ�ĆĒĈČĂčĂČ�úČ�úć�účĒĉĂüúą�ĉċþČþćčúčĂĈć�Ĉÿ�ĆĎüĈČú�úČČĈüĂúčþý�ąĒĆĉāúčĂü�čĂČČĎþ�ąĒĆĉāĈĆú��ú�üúČþ�ċþĉĈċč
��� "SR�#SBT�0GUBMNPM����������������
sis, Crohn’s disease, systemic lupus erythematosus, rheumatoid ar-thritis, and Wegener’s granulomatosis), vascular (carotid-cavernous fistula and arteriovenous malformation), neoplastic (metastatic, se condary or primary), infectious (secondary to orbital cellulitis or pri mary), deposition-related (amyloid), traumatic, and iatrogenic causes(3). Despite its rare occurrence, orbital lymphomas should be considered in the differential diagnosis of this type of condition(3). Another rare etiology that should be considered, particularly in en -de mic regions such as Brazil, is myositis caused by tuberculosis(4).
Lymphomas with the presentation of myositis and no other sym p toms are very rare in the scientific literature. The largest series of ocular adnexal lymphomas described in the scientific literature (353 cases) do not describe this type of clinical presentation. There have been few revisions or only isolated case reports(1,2,5,7-9). Different authors have mentioned diplopia, periorbital inflammation, restric-tion of motility, and proptosis as the main clinical findings(1,5,7-9). Such sym ptomatology may suggest the impairment of ocular muscles. Watkins et al. and Lacey et al. mention that the upper muscles are more frequently involved, particularly the superior rectus and the su perior oblique muscles, respectively(1,3). Lacey et al. also determined that the disease is usually unilateral, describing only one patient with symmetrical bilateral infiltration(3). In our patient, there was unilateral involvement of the medial rectus muscle, as observed in the case described by Rossman et al.(2). Histologically, the muscle involvement is mainly nodular and does not spare the tendons(1,3).
The clinical presentation of non-Hodgkin B-cell MALT lymphoma or extranodal marginal zone lymphoma in the orbit is indolent with a low risk of progression in the bone marrow, indicating a good prog-nosis in most cases(2,3). Our patient was symptomatic for 2 years and had no metastasis, emphasizing the indolent course of the disease.
Imaging studies such as CT and MRI allow for the observation of the increased thickness of the affected muscle and tendon involve-ment. This information, together with the clinical signs and patholo-gy, can confirm the diagnosis. In our patient, imaging studies revea-led tendon involvement, which suggested a differential diagnosis of Graves’ ophthalmopathy. In imaging studies, other characteristics of thyroid ophthalmopathy that may be observed include well-defined fusiform enlargement of the muscle (especially posteriorly) with smooth borders, no tendon enlargement, normal orbital fat, presep-tal edema, and lacrimal gland prolapse(3).
Confirmation of the diagnostic biopsy with immunohistochemis-try is essential, and the usual findings are as follows: CD 20 (+), CD 43
(+), BCL 6 (−) MUM1 (−), p16 (+), p21 (−), pRB (−) p53 (−), and cyclin D1 (−)(3). Our patient was CD 20 (+), CD 10 (−), CD 23 (−), BCL2 (−), and cyclin D1 (−) in B-cells and CD3 (+) and CD 5 (+) in T-lymphocytes. Ge-netically, the translocations most frequently encountered are t (3;14)(p14.1;q32) involving FOXP1 and IgH and t(14;18)(q32;q21) involving IgH and MALT1(6,10).
When the diagnosis of non-Hodgkin B-cell MALT lymphoma was established, we immediately sent the patient to the Hematology de partment of UNIFESP for treatment. Multidisciplinary evaluation and systemic staging was mandatory because of good response to treatment and good prognosis.
In conclusion, the findings from our case indicate that it is impor-tant to consider lymphoma as one of the differential diagnoses in cases of isolated myositis, although Graves’ ophthalmopathy should continue to be the first diagnosis to be considered.
REFERENCES 1. Watkins LM, Carter KD, Nerad JA. Ocular adnexal lymphoma of the extraocular mus-
cles: case series of the University of Iowa and review of the literature. Ophthal Plast Reconstr Surg. 2011;27(6):471-6.
2. Rossman D, Michel R, Codere F. A case of an enlarged medial rectus muscle. Int Ophthalmol. 2009;29(4):319-21.
3. Lacey B, Chang W, Rootman J. Nonthyroid causes of extraocular muscle disease. Surv Ophthalmol. 1999;44(3):187-213.
4. Wang JY, Lee LN, Hsueh PR, Shih JY, Chang YL, Yang PC, et al. Tuberculous myositis rare but existing clinical entity. Rheumatology (Oxford). 2003;42(7):836-40.
5. Ferry JA, Fung CY, Zukerberg L, Lucarelli MJ, Hasserijan RP, Preffer FI, et al. Lymphoma of the ocular adnexa: a study of 353 cases. Am J Surg Pathol. 2007;31(2):170-84.
6. Jakobiec FA. Ocular adnexal lymphoid tumors: progress in need of clarification. Am J Ophthalmol. 2008;145(6):941-50. Comment on: Am J Ophthalmol. 2008;145(6):1002-6.
7. Coupland SE, Hellmich M, Auw- Haedrich C, Lee WR, Stein H. Prognostic value of cell-cycle markers in ocular adnexal lymphoma: an assessment of 230 cases. Arch Clin Exp Ophtalmol. 2004;242(2):130-45.
8. Coupland SE, Krause L, Delecluse HJ, Anagnostopoulos I, Foss HD, Hummel M, et al. Lymphoproliferative lesions of the ocular adnexal: analysis of 112 cases. Ophthalmo-logy. 1998;105(8):1430-41.
9. Lagoo AS, Haggerty C, Kim Y, Hammons M, Neufeld K, Redher C, et al. Morphologic features of 115 lymphomas of the orbit and ocular adnexa categorized according to the WHO classification: are marginal zone lymphomas in the orbic mucosa-associa-ted lymphoid tissue type lymphomas? Arch Pathol Lab Med. 2008;132(9):1405-16.
10. Takada S, Yoshino T, Taniwaki M, Nakamura N, Nakamine H, Oshima K, et al. Involve-ment of the chromosomal translocation t (11;18) in some mucosa-associated lym phoid tissue lymphomas and diffuse large B-cell lymphomas of the ocular adnexa: evidence from multiplex reverse transcriptase-polymerase chain reaction and fluorescence in situ hybridization on using formalin-fixed, paraffin-embedded specimens. Mod Pathol. 2003;16(5):445-52.

119"SR�#SBT�0GUBMNPM�����������������
$úČþ�3þĉĈċč
INTRODUCTIONKeratectasia is a well-documented complication of laser in situ ke-
ratomileusis (LASIK) and photorefractive keratectomy (PRK), although it is more common after LASIK(1-4). Potential risk factors include, but are not limited to, high attempted correction, thin residual corneal thickness, flap creation, irregular corneal topography, clinical kerato-conus, and undiagnosed subclinical keratoconus(1).
Benign joint hypermobility syndrome (BJHS) is a connective tis-sue disorder with hypermobility in which musculoskeletal symptoms occur in the absence of systemic rheumatological disease(5). This syn-drome is considered to be an inherited connective tissue disorder(6). The primary clinical manifestations of BJHS are hypermobility and pain in multiple joints. It is different from other disorders that cause local joint hypermobility and generalized joint laxity, such as Marfan syndrome and Ehlers-Danlos syndrome (EDS).
Hypermobility that is not associated with systemic disease occurs in 4% -13% of the population(6). The hypermobility diminishes as one ages, and it also appears to be related to sex and race6. Individuals of African, Asian, and Middle Eastern descent also have increased joint laxity(7-9).
Here we describe the case of a 27-year-old woman with BJHS who keratectasia after LASIK (Figures 1, 2).
CASE REPORTA 27-year-old woman with BJHS presented for a refractive sur-
gery evaluation in August 2000. Her corrected distance visual acuity
(CDVA) was 20/20 with a manifest refraction of -4.50 -0.75 × 180 in the right eye and 20/20 with a manifest refraction of -4.00 -1.25 × 180 in the left eye. There was no significant history of ocular trauma or a family history of keratoconus, and she had no eye rubbing habit or other ocular issues. The patient had been wearing soft contact lenses for several years without incident.
She fulfilled the Beighton score(5). Her medical history revealed arthralgia in two joints (right elbow and right wrist) for more than 6 months, two episodes of shoulder dislocation, a marfanoid habitus, myopia, and mitral valve prolapse.
At the time of consultation, her refraction had been stable for more than 3 years, and both topography and pachymetry findings appeared normal. Topography revealed symmetric bow-tie patterns in both eyes. Central ultrasonic pachymetry revealed a corneal thi ckness of 515 µm and 513 µm in the right and left eyes, respec-tively. Central keratometry revealed a corneal surface curvature of 42.99/42.24 diopters (D) in the right eye and 42.77/42.18 D in the left eye, representing a topographical cylinder (0.75 and 0.59, respectively; Figures 3 A and 3 B). According to the Randleman customized ectasia risk score, each eye represented a low risk for the development of excimer keratectasia.
Uneventful LASIK was performed in November 2000 on both eyes, with a 1-week interval between surgeries. The Automated Cor-neal Shaper microkeratome (Bausch & Lomb) with a 160-µm plate and a Meditec MEL-60 excimer laser was used. In both eyes, the optic ablation zone was 6 mm, and the estimated ablation depth was 43 µm. The intended correction was the manifest refraction in both eyes.
Keratectasia following laser in situ keratomileusis in a low-risk patient with benign
joint hypermobility syndrome
Ectasia corneana após ceratomileuse a laser in situ em um paciente com baixo risco e apresentando
síndrome de hipermobilidade articular benigna
gustavo galPeRin1,2, maRtin beRRa1,2, aleJandRo beRRa2
ABSTRACTHere we present the case of a 27-year-old woman with benign joint hypermobility (BJHS) syndrome who developed keratectasia after laser in situ keratomileusis (LASIK) in both eyes. Both eyes had identical low Randleman risk factor scores. To our knowledge, this is the first report of such a complication in a patient with BJHS. It highlights our incomplete knowledge of the risk factors for kera-tectasia following LASIK and suggests that BJHS should be considered as a risk factor for keratectasia.
Keywords: Cornea/pathology; Corneal diseases/keratomileusis; Laser in situ/adverse effects; Joint instability; Case report
RESUMO Apresentamos um caso de estasia corneana em um paciente submetido à cirurgia refrativa a laser. Ceratomileuse a laser in situ (LASIK) foi realizada em ambos os olhos. Ambos os olhos apresentavam idênticos escores baixos na avaliação de fatores de risco de Randleman. Acreditamos que este é o primeiro caso desta complicação em um paciente com síndrome de hipermobilidade articular benigna relatado na litera-tura. Ele destaca o nosso conhecimento incompleto dos fatores de risco para ectasia corneana após LASIK e sugere que a síndrome de hipermobilidade articular benigna deve ser considerada um fator de risco para ectasia corneana.
Descritores: Córnea/patologia; Ceratomileuse assistida pro excimer laser in situ/efeitos adversos; Instabilidade articular; Relato de caso
Submitted for publication: November 27, 2013 Accepted for publication: December 9, 2013
Study conducted at Laboratorio de Investigaciones Oculares, Universidad de Buenos Aires, Argentina.1 Hospital Oftalmológico Pedro Lagleyze, Buenos Aires, Argentina.2 Laboratorio de Investigaciones Oculares, Universidad de Buenos Aires, Argentina.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Martín Berra. Laboratorio de Investigaciones Oculares. Departamento de Patología, Facultad de Medicina. Universidad de Buenos Aires. José E. Uriburu 950, entre piso (1114) Buenos Aires, Argentina - E-mail: [email protected]

,þċúčþüčúČĂú�ÿĈąąĈĐĂćĀ�ąúČþċ�Ăć�ČĂčĎ�ĄþċúčĈĆĂąþĎČĂČ�Ăć�ú�ąĈĐ�ċĂČĄ�ĉúčĂþćč�ĐĂčā�ûþćĂĀć�ăĈĂćč�āĒĉþċĆĈûĂąĂčĒ�ČĒćýċĈĆþ
120 "SR�#SBT�0GUBMNPM�����������������
Figure 1. Apposition of the thumb to the flexor aspect of the forearm. Figure 2. Hyperextension of the elbow beyond 90 degrees (neutral).
Three months after surgery, the uncorrected distance visual acuity (UDVA) was 20/20 in the right eye and 20/20 in the left. Biomicrosco-py was clear, and the patient was discharged from the clinic. In May 2006, she returned, reporting that the visual acuity in the right eye had deteriorated over the past 6 months; she reported no problems with the left eye. The UDVA was 20/200 in the right eye and 20/20 in the left eye. The CDVA was 20/25, with a refraction of -4.00 × 70° in the right eye. The intraocular pressure remained normal before and after surgery. With the OCT Visante, the LASIK interface was not visible. The Reichert Ocular Response Analyzer (ORA) showed low values for cor-
neal hysteresis (CH; right eye, 7.4; left eye, 8.5) and corneal resistance factor (CRF; right eye, 6.3; left eye, 6.9). Topography (Orbscan, Bausch & Lomb) of the right eye showed an irregular pattern, suggestive of corneal ectasia (Figure 3 C). Pachymetry revealed a thickness of 402 µm at the thinnest point. The posterior float was 125 µm.
Topography (Orbscan, Bausch & Lomb) of the left eye appeared normal. Pachymetry revealed a thickness of 408 µm at the thinnest point. The posterior float was 42 µm (Figure 3 D).
Because the surgeon believed that it was important to minimize the possible progression of keratectasia while the patient was away, corneal collagen cross-linking with riboflavin and ultraviolet A (IROC, Zurich, Switzerland) irradiation was performed in 2007. Both eyes re-mained stable during 5 years of follow-up.
DISCUSSIONCorneal ectasia is a serious complication of laser refractive sur ge-
ry. Progressive distortion of the cornea can lead to a significant de-
Figure 3. A) Preoperative right topography. B) Preoperative left topography. C) Postoperative right topography. D) Postoperative left topography.
A
C D
B

(úąĉþċĂć�( �þč�úą�
121"SR�#SBT�0GUBMNPM�����������������
crease in CDVA and may ultimately require transplantation for visual rehabilitation. Although several risk factors have been well outlined, the pathogenesis of the condition is not clearly understood(3). Various authors have attributed age, preoperative corneal pachymetry, resi-dual stromal bed thickness, high preoperative correction, number of enhancements, flap creation, the presence of subclinical corneal disease, or high posterior float on topography to be related to the onset or progression of ectasia(1-3). Our patient’s preoperative and intraoperative assessments with no known risk factors suggest that the patient was at a low risk of developing ectasia. Before surgery, CDVA was 20/20 in both eyes. Her refraction was not high and had been stable for several years. Preoperative corneal topography and pachymetry findings appeared normal in both eyes.
Because of the retrospective nature of the case, the preoperative topography maps were not available for further review, and no fur-ther comment on the same is possible.
BJHS may be a sign of biomechanical weakness and a possible risk factor for keratectasia.
In conclusion, we described the first case, to the best of our knowledge, of keratectasia after LASIK in both eyes in a patient with BJHS. The right eye developed late-onset ectasia despite the relative absence of presurgical risk factors. We suggest that screening for BJHS
as a possible risk factor will limit the incidence of ectasia in these pa-tients and support the decision to proceed with an alternative to LASIK surgery. Alternative surgical options, including surface ablation and phakic intraocular lenses, should be considered patients with BJHS.
REFERENCES 1. Randleman JB, Russell B, Ward MA, Thompson KP, Stulting RD. Risk factors and prog-
nosis for corneal ectasia after LASIK. Ophthalmology. 2003;110(2):267-75. 2. Comaish IF, Lawless MA. Progressive post-LASIK keratectasia; biomechanical instabi-
lity or chronic disease process? J Cataract Refract Surg. 2002;28(12):2206-13. 3. Chan CC, Hodge C, Sutton G. External analysis of the Randleman Ectasia Risk Factor
Score System: a review of 36 cases of post LASIK ectasia. Clin Exp Ophthalmol. 2010; 38(4):335-40.
4. Randleman JB, Caster AI, Banning CS, Stulting RD. Corneal ectasia after photorefrac-tive keratectomy. J Cataract Refract Surg. 2006;32(8):1395-8.
5. Grahame R. The revised (Brighton 1998) criteria for the diagnosis of benign joint hy permobility syndrome (BJHS). J Rheumatol. 2000;27(7):1777-9.
6. Biro F, Gewanter HL, Baum J. The hypermobility syndrome. Pediatrics. 1983;72(5):701-6. 7. Engelbert R, Uiterwaal C, Van de Putte E, Helders P, Sakkers R, Van Tintelen P, et al.
Pediatric generalized joint hypomobility and musculoskeletal complaints: a new en-tity? Clinical, biochemical, and osseal characteristics. Pediatrics. 2004;113(4):714-9.
8. Everman DB, Robin NH. Hypermobility syndrome. Pediatr Rev. 1998;19(4):111-7. 9. Finsterbush A, Pogrund H. The hypermobility syndrome. Clin Orthop Relat Res. 1982;
168:124-7.
XVII Congresso Internacional da Sociedade Brasileira de Oftalmologia
23 a 26 de julho de 2014Hotel Windsor Barra
Rio de Janeiro - RJ
Informações: Tel.: (21) 2554-7000 (Sandra Regina)
E-mail: [email protected] Site: www.congressosbo.com.br

122 "SR�#SBT�0GUBMNPM����������������
$úČþ�3þĉĈċč
INTRODUCTIONDescemet stripping automated endothelial keratoplasty (DSAEK)
is the standard surgical treatment for endothelial failure. Its efficacy is indicated by a spectacle-corrected acuity of 20/40 or better in most patients(1,2). The microkeratome coupled to the artificial chamber can produce an endothelial donor lamella (EDL); however, the cutting irregularities and the unpredictability of the depth of the cut are major impediments to the visual outcome of lamellar transplanta-tion(3,4). New models of femtosecond lasers (FS) produce a better corneal lamella quality than the microkeratome(5-9). Lasers with a high frequen cy and low energy tend to make a corneal cut smoother, more homogeneous, accurate, and reproducible, as smaller intrastro-mal bubbles are produced, creating smaller cavities in the cornea(5-9). Cell necrosis and inflammation in the cornea increase as the energy used by FS increases(5-9). There is a direct relationship between the frequency and amount of energy required to form a shooting corneal lamella. With a lower frequency, more energy is required to manu-facture the lamella. In addition, with more energy, the size of the intrastromal bubbles and cavities generated by each shot increases, which decreases the laser’s precision(5-9). Theoretically, a better visual outcome can be achieved with a thinner and more regular corneal donor lamella produced by a low-energy and high-frequency FS. The objective of this report is to describe, for the first time in Brazil, the creation of an EDL with a low energy and high frequency FS and its subsequent use in vivo.
CASE REPORTA 59-year-old female presented with an endothelial failure in the
left eye (LE) after phacoemulsification and intraocular lens implanta-tion performed 9 years previously. Figure 1 presents a preoperative photograph of her LE. Her best-corrected visual acuity (BCVA, with glasses) was a finger count at 1 m. The central corneal thickness (CCT) was 730 µm, as measured by ultrasonic pachymetry (P55, Paradigm®, USA). Following the preoperative examinations, she was subjected to DSAEK.
An EDL was prepared with a low energy and high frequency FS (LDV®, Ziemer® Ophthalmic System AG, Port, Switzerland). This laser operates with a pulse frequency in the megahertz range, with hi gh- aperture optics, with a per pulse time exposure of 250 fs, and a spot diameter of 2 µm. The shots were overlapped to avoid leaving un-treated areas. The energy per pulse was 30 nJ(5).
For proper laser application, the donor cornea was first attached to the Ziemer® anterior chamber, the epithelium was removed, and CCT was measured by ultrasonic pachymetry. The donor cornea was then flattened using the head of the laser. The preoperative donor endothelium cell count was 2835 cells/mm2, and the intraoperative CCT was 590 µm. The anterior donor lamella was planned to have a 10-mm diameter and a 500-µm thickness, theoretically leaving a 90-µm EDL. After laser treatment, the cornea was manually trephined from the endothelial side using an 8-mm trephine blade (Katena® Products, Denville, NJ, USA). Next, the posterior and anterior lamellae
In vivo ultrathin Descemet stripping automated endothelial keratoplasty with a
low-energy and high-frequency femtosecond laser
In vivoȱ��������ȱ���������ȱ���������ȱ�����������ȱ�����������¢ȱ�����ę��ȱ���ȱ�����ȱ��ȱ������������ȱ ��ȱ���¡�ȱ�������ȱ�ȱ����ȱ�����¹����
gustavo viCtoR1, Walton nosé2, sidney Júlio de FaRia e sousa3, adRiana dos santos FoRseto2, milton Ruiz alves1
ABSTRACTThis case report describes the production of an ultrathin endothelial donor cor-neal lamella using a femtosecond laser with low energy and a high frequency. In addition, we report its use in vivo in an eye with pseudophakic bullous keratopa-thy. The outcomes were observed 3 months after surgery in terms of the change in endothelial donor lamella and full cornea thickness (including pachymetric mapping), visual acuity, and endothelial cell count.
Keywords: Descemet stripping endothelial keratoplasty; Laser therapy, low-level/methods; Endothelium corneal; Tomography, optical coherence; Case report
RESUMOEste relato de caso mostra a confecção de uma lamela corneana doadora endotelial ultrafina com o uso de um laser de femtosegundo de baixa energia e alta taxa de repetição, e sua utilização in vivo em um paciente com ceratopatia bolhosa do pseu-dofácico. O resultado final foi observado quanto a evolução da espessura da lamela endotelial doadora e de toda a córnea (incluindo mapa paquimétrico), da acuidade visual, e da contagem endotelial ao final de 3 meses de pós-operatório.
Descritores: Ceratoplastia endotelial com remoção da lâmina limitante posterior; Terapia a laser de baixa intensidade; Endotélio da córnea; Tomografia de coerência óptica; Relato de caso
Submitted for publication: November 4, 2013 Accepted for publication: November 7, 2013
Study conducted at Universidade de São Paulo, São Paulo, SP, Brazil.1 Department of Ophthalmology, School of Medicine, Universidade de São Paulo, São Paulo, SP, Brazil.2 Department of Ophthalmology, Universidade Federal de São Paulo, São Paulo, SP, Brazil.3 Department of Ophthalmology, School of Medicine, Universidade de São Paulo, Ribeirão Preto, SP,
Brazil.
Funding: This study was support by the Foundation for Research Support of the State of São Paulo (FAPESP).
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose.
Correspondence address: Gustavo Victor. Av. República do Líbano, 1.034 - São Paulo (SP) - 04002-001 - Brazil - E-mail: [email protected]

7ĂüčĈċ�( �þč�úą�
123"SR�#SBT�0GUBMNPM����������������
The surgeon (WN) performed a standard DSAEK procedure in the receptor eye after peribulbar anesthesia, as described previously(2). In brief, the anterior chamber was filled with air through the paracente-sis and a reverse Sinskey hook was used to remove an approximately 8-mm diameter section of the central endothelium and Descemet membrane, previously marked on the host epithelium, through the main 2.4-mm clear corneal incision. Afterwards, the main incision was enlarged with a 5.2-mm surgical blade to insert the endothelial lamella with a Busin® glide (Moria®, France). The anterior chamber was maintained with air throughout the procedure. The EDL was positioned over the receptor corneal epithelium using a cannula with smooth movements. The main incision was sutured with a single 10-0 mononylon stitch. The patient remained in the supine position for 2 h to promote proper EDL adhesion when the air was partially removed and the anterior chamber was filled with balanced saline solution.
After surgery, topical moxifloxacin hydrochloride 0.5% (Vigamox®, Alcon®, Brazil) was prescribed four times per day for 1 week and pred-nisolone acetate 1% (Predfort®, Allergan®, Brazil) every 3 h for 1 week, then six times per day for 1 week, which was decreased thereafter by one application per day each week.
On the first postoperative day, the patient had an uncorrected visual acuity (UCVA) of 20/400 in LE. After 1 month, her BCVA was 20/150 (+1.50 -2.50 × 15°). In the third postoperative month, she had an UCVA of 20/150 and her BCVA improved to 20/30 with a refraction of +075 -2.75 × 120°. The central and paracentral endothelial lamella thickness was measured with the Visante® OCT (Zeiss®, Germany) at 158 µm in the first postoperative month and 62 µm after the third postoperative month. Figure 3 A and 3 B show the Visante® OCT after 1 month whereas figure 3 C and 3 D show the same after 3 months. Figure 4 presents the global pachymetric map and endothelial cell count in the third postoperative month. Global pachymetric measu-rements with the Visante® OCT were within the normal range, with 521 µm for CCT (Figure 4). The endothelial cell count in the third postoperative month was 1036 cells/mm2 (Figure 4).
DISCUSSION Bullous keratopathy remains one of the leading causes worldwide
for corneal transplantation(10). Many surgeons consider DSAEK as the treatment of choice for this condition(1,2). According to the potential
Figure 1. Preoperative photograph of the patient’s left eye.
Figure 3. Postoperative Visante OCT® of the left eye. A) Anterior segment and B) High resolution cornea: Postoperative examination after 1 month. C) Anterior segment and D) High resolution cornea: postoperative examination in the third postoperative month.
A B
C
were separated by holding the edge of the posterior lamella with forceps and gently sliding off the anterior lamella using the tip of a Merocel® sponge (Figure 2).
Figure 2. Deep anterior donor cornea lamellae (thicker) being removed. Endothelial donor lamellae (thinner), from same cornea, remains on the bottom with the endothelium side up after cutting with an LDV® femtosecond laser.
D

In vIvo�ĎąčċúčāĂć�%þČüþĆþč�ČčċĂĉĉĂćĀ�úĎčĈĆúčþý�þćýĈčāþąĂúą�ĄþċúčĈĉąúČčĒ�ĐĂčā�ú�ąĈĐ�þćþċĀĒ�úćý�āĂĀā�ÿċþĊĎþćüĒ�ÿþĆčĈČþüĈćý�ąúČþċ
��� "SR�#SBT�0GUBMNPM����������������
Figure 4. Visante OCT® global pachymetry map and endothelial cell count in the third postoperative month.
vision of the eye, a thinner EDL will result in a better final visual acuity. The endothelial cell count declined significantly, but could maintain a viable tissue. The EDL was set to 90 µm without epithelium, and the effective EDL was 62 µm. The desired thinner thickness was calculated on the basis of the full thickness of the central cornea after removing it from the Optisol® and placing it in the artificial an terior chamber, which certainly had edema. This shows a certain predictability for this technique using this laser. The primary reasons for this small difference may be the influence of pressure within the artificial anterior chamber at the time of preoperative measurements, pachymetric measure after flattening the cornea with the laser to construct the EDL, and the preoperative corneal edema and laser safety margin. These factors should be considered by the surgeon and examined in future studies. In another in vitro study(9) that used the same FS used in the present study, 5 corneas were cut to produce EDLs with a 70-μm thickness and the mean central posterior stromal thickness of the cut corneas was 60.6 μm (range, 43-72 μm). FS can help spread DSAEK when creating an automated ultrafine EDL and facilitate DSAEK, especially if eye banks can send a pre-cut EDL. The disadvantage is the high cost of FS.
Here, we report the production of an ultrathin EDL using a low energy and high frequency FS. We also report its use in vitro and the outcomes observed 3 months after surgery in terms of the evolution of EDL, the total corneal thickness (including the global pachymetric mapping), the visual acuity, and the endothelial cell count.
REFERENCES 1. Bahar I, Kaiserman I, McAllum P, Slomovic A, Rootman D. Comparison of posterior
la mellar keratoplasty techniques to penetrating keratoplasty. Ophthalmology. 2008; 115(9):1525-33.
2. Price MO, Price FW Jr. Descemet’s stripping with endothelial keratoplasty: compara-tive outcomes with microkeratome-dissected and manually dissected donor tissue. Ophthalmology. 2006;113(11):1936-42.
3. Kang PC, McEntire MW, Thompson CJ, Moshirfar M. Preparation of donor lamellar tissue for deep lamellar endothelial keratoplasty using a microkeratome and artificial anterior chamber system: endothelial cell loss and predictability of lamellar thickness. Ophthalmic Surg Lasers Imaging. 2005;36(5):381-5.
4. Thiel MA, Kaufmann C, Dedes W, Bochmann F, Becht CN, Schipper I. Predictability of microkeratome-dependent flap thickness for DSAEK. Klin Monbl Augenheilkd. 2009; 226(4):230-3.
1. Lubatschowski H. Overview of commercially available Femtosecond lasers in refracti-ve surgery. J Refract Surg. 2008;24(1):S102-107.
5. Salomão MQ, Wilson SE. Femtosecond laser in laser in situ keratomileusis. J Cataract Refract Surg. 2010;36(6):1024-32.
6. Ahn H, Kim JK, Kim CK, Han GH, Seo KY, Kim EK, et al. Comparison of laser in situ ke-ratomileusis flaps created by 3 femtosecond lasers and a microkeratome. J Cataract Refract Surg. 2011;37(2):349-57.
7. Medeiros FW, Kaur H, Agrawal V, Chaurasia SS, Hammel J, Dupps WJ Jr, et al. Effect of femtosecond laser energy level on corneal stromal cell death and inflammation. J Refract Surg. 2009;25(10):869-74.
8. Phillips PM, Phillips LJ, Saad HA, Terry MA, Stolz DB, Stoeger C, et al. “Ultrathin” DSAEK tissue prepared with a low-pulse energy, high-frequency femtosecond laser. Cornea. 2013;32(1):81-6.
9. Zhang C, Xu J. Indications for penetrating keratoplasty in East China, 1994-2003. Graefes Arch Clin Exp Ophthalmol. 2005;243(10):1005-9.

���"SR�#SBT�0GUBMNPM�����������������
3þďĂþĐ�"ċčĂüąþ
Surgical management of astigmatism with toric intraocular lenses
Uso de lentes intraoculares tóricas no tratamento cirúrgico de astigmatismo
bRuna v. ventuRa1,2,3, li Wang1, mitChell P. WeikeRt1, shaun b. Robinson1, douglas d. koCh1
Submitted for publication: January 17, 2014 Accepted for publication: March 13, 20141 Department of Ophthalmology, Cullen Eye Institute, Baylor College of Medicine, Houston, Texas,
United States of America.2 Fundação Altino Ventura, Recife, PE, Brazil. 3 Department of Ophthalmology, Universidade Federal de São Paulo, São Paulo, SP, Brazil.
Funding: This study was supported by Research to Prevent Blindness.
Disclosure of potential conflicts of interest: B.V.Ventura, None; L.Wang, Consultant of Ziemer; M.P.Weikert, Consultant for Ziemer; S.B.Robinson, None; D.R.Koch, Consultant for Ziemer, AMO, Alcon and I-Optics.
Correspondence address: Bruna Vieira Ventura. Fundação Altino Ventura. Rua da Soledade, 170 - Recife (PE) - 50070-040 - Brazil - E-mail: [email protected]
INTRODUCTIONIn the last 3 decades, advances in cataract surgery have drama-
tically improved patients’ outcomes, increasing expectations regar-ding visual results. Simultaneously, some key factors associated with good visual outcomes were identified. It has been estimated that 30% of cataract patients have more than 0.75 diopters (D) of corneal astigmatism, that 22% have more than 1.50 D, and that 8% have more than 2.00 D(1,2). Since post-surgical residual astigmatism can compro-mise uncorrected distance visual acuity (UDVA), correction of corneal astigmatism is a critical element of modern cataract surgery.
Corneal astigmatism can be surgically treated with adjustment of wound size and location, peripheral corneal relaxing incisions, additional clear corneal cataract incision along the steep meridian, laser refractive surgery, or toric intraocular lenses (IOLs). Toric IOLs correct corneal astigmatism at the time of cataract surgery and are a predictable treatment in general(3-18). Monofocal toric IOLs can be used to correct the patient’s vision for distance, for near or for both (this latter being attained via monovision)(3-10), while multifocal toric IOLs aim at providing good uncorrected vision for near, intermediate and far(14-16,19). Moreover, toric phakic IOLs are a largely reversible treatment option for pre-cataractous patients who are not good candidates for corneal refractive surgery and have clinically signifi-cant astigmatism(20-22).
ABSTRACTCorrection of corneal astigmatism is a key element of cataract surgery, since post-surgical residual astigmatism can compromise the patient’s uncorrected visual acuity. Toric intraocular lenses (IOLs) compensate for corneal astigmatism at the time of surgery, correcting ocular astigmatism. They are a predictable treat ment. However, accurate measurement of corneal astigmatism is mandatory for choosing the correct toric IOL power and for planning optimal alignment. When calculating the power of toric IOLs, it is important to consider anterior and posterior corneal astigmatism, along with the surgically induced astigmatism. Accurate toric lens alignment along the calculated meridian is also crucial to achieve effective as tigmatism correction. There are several techniques to guide IOL alignment, in-cluding the traditional manual marking technique and automated systems based on anatomic and topographic landmarks. The aim of this review is to provide an overview on astigmatism management with toric IOLs, including relevant patient selection criteria, corneal astigmatism measurement, toric IOL power calculation, toric IOL alignment, clinical outcomes and complications.
Keywords: Astigmatism; Toric intraocular lenses; Refractive errors; Corneal topo-graphy; Complications
RESUMOO tratamento do astigmatismo corneal é um fator importante na cirurgia de cata-rata, uma vez que o astigmatismo residual pode comprometer a acuidade visual não corrigida do paciente após a cirurgia. Lentes intraoculares (LIOs) tóricas compensam o astigmatismo corneal no momento da cirurgia, corrigindo o astigmatismo ocular. Ademais, constituem um tratamento previsível. Entretanto, é necessário obter uma medida precisa do astigmatismo corneal para selecionar o poder correto da LIO tórica e para planejar o melhor alinhamento da mesma. No cálculo do poder da LIO tórica, é importante considerar o astigmatismo das superfícies anterior e posterior da córnea, além do astigmatismo induzido na cirurgia. O alinhamento da lente tórica no meridiano planejado é essencial para se obter uma correção efetiva do astigmatismo. Há várias técnicas para guiar o alinhamento da LIO, incluindo a técnica de marcação manual tradicional e sistemas que se baseiam em pontos de referência anatômicos e topográficos. O objetivo desse artigo de revisão é discutir o uso de LIOs tóricas no tratamento de astigmatismo corneal, incluindo os critérios de seleção dos pacientes, a medida do astigmatismo corneal, o cálculo do poder da LIO tórica, o alinhamento da LIO tórica, os resultados clínicos e as complicações.
Descritores: Astigmatismo; Implante de lente intraocular; Planejamento cirúrgico; Topografia da córnea; Complicações
The final visual outcomes attained with toric IOLs depend on several factors, including the visual potential of the eye. The ideal patients for toric IOL implantation are those with regular astigmatism, although previous papers have also shown good outcomes in cases of stable, mild central irregular astigmatism, such as patients with mild to moderate stable keratoconus(23), pellucid marginal degene-ration(24) and post-corneal transplant(25). In these cases, it is important to have a fairly symmetrical power and alignment of the astigmatism within the cornea’s central 4 mm. Toric phakic IOLs can be used in adults and in children. Although there is no consensus regarding the use of toric phakic IOLs in children, many authors consider implan-ting them in patients with high anisometropia or high isometropia with an astigmatic component, and in those with neurobehavioral disorders and visually significant astigmatism. In these cases, the IOL is usually considered as a treatment option when the patient is non-compliant to medical treatment, including spectacles and contact lenses(20,21). Multifocal toric lenses should be considered in patients who want good near and distance uncorrected visual acuity postoperatively and who have approximately 0.50 D of corneal astig-matism or more(19,26).
Toric IOLs should be avoided in patients with corneal dystrophies that might need a corneal transplant in the future and should be used with caution in patients with potential capsular bag instability. Phakic

4ĎċĀĂüúą�ĆúćúĀþĆþćč�Ĉÿ�úČčĂĀĆúčĂČĆ�ĐĂčā�čĈċĂü�ĂćčċúĈüĎąúċ�ąþćČþČ�
126 "SR�#SBT�0GUBMNPM�����������������
toric IOLs should not be implanted in eyes with shallow anterior cham bers and low endothelial cell counts(22). In addition, as multifocal toric IOLs split the available light between the distance and near foci, they should not be implanted in patients with ocular comorbidities that affect the visual acuity or the quality of vision, such as amblyopia, maculopathy, glaucoma, and uveitis(27).
MEASURING CORNEAL ASTIGMATISM AND CALCULATING TORIC IOLS
Devices
The anterior and posterior corneal surfaces contribute to the total corneal astigmatism. Accurate measurement of corneal astigmatism is mandatory for choosing toric IOL power and planning optimal alignment. Various measuring methods are available, including manual keratometry, automated keratometry, corneal topography, slit-scanning technology, optical coherence tomography, and Scheim pflug imaging. The first three methods measure the anterior corneal surface only. Using a standardized corneal refractive index, most commonly 1.3375, they assume a fixed posterior:anterior cor-neal curvature ratio to calculate total corneal power and astigmatism. On the other hand, slit-scanning technology, optical coherence tomography and Scheimpflug imaging measure the anterior and posterior corneal surface. Therefore, they provide total corneal po-wer and astigmatism based on the measured anterior and posterior corneal data.
No single method has been identified as being the best for measuring corneal astigmatism. Previous studies have shown that manual keratometry, automated keratometry, simulated keratometry of Placido-based corneal topography, and simulated keratometry of Scheimpflug imaging provide similar values for anterior corneal curvature(28-30), although significant disagreement in axis location has been reported(29). Contrarily, anterior corneal astigmatism mea-surements differed significantly when comparing values derived from total corneal power and equivalent keratometry to that of au-tomated, manual, and simulated keratometry(30,31). These three later measurements are based only on the anterior corneal surface data, while the total corneal power and equivalent keratometry are based on the measurements of both the anterior and posterior corneal curvatures. Total corneal power is calculated by tracking the path of incident light rays through the anterior and posterior corneal surface using a ray-tracing method and Snell’s law with the true refractive indices to calculate the anterior and posterior corneal powers (1.376 for cornea and 1.336 for aqueous)(32).
The role of the posterior cornea
Recent studies(15-17) have shown the importance of considering the posterior corneal surface when determining total corneal astigma tism and planning astigmatism correction. The posterior cornea acts as a minus lens. It generally has a steeper vertical meridian, and remains steeper vertically with increasing age. The anterior corneal steeper meridian is also commonly oriented vertically in younger individuals, but shifts towards the horizontal meridian as patients get older. Thus, in general, posterior corneal astigmatism partially compensates for anterior corneal astigmatism in young adults and increases total corneal astigmatism in older individuals(33).
The mean magnitude of posterior corneal astigmatism is - 0.30 D. Koch et al.(33) have shown that one cannot accurately predict the posterior corneal astigmatism based only on anterior corneal mea-surements. They found maximal values of posterior corneal astigma-tism of over 0.8 D in corneas that had with-the-rule astigmatism on the anterior corneal surface and of over 0.5 D in corneas that had against-the-rule corneal astigmatism on the anterior corneal surface. The correlation between anterior and posterior corneal astigmatism was moderate when the steep anterior meridian was aligned verti-cally, weak when it was oriented obliquely, and absent when it was aligned horizontally(33).
A second study by Koch et al.(35) reported in pseudophakic eyes the mean corneal astigmatism prediction error of four devices that calculate total corneal astigmatism based only on anterior surface measurements. The corneal astigmatism prediction error (the de-viation from the actual total corneal astigmatism) was obtained by subtracting the actual corneal astigmatism (which is the difference between the postoperative manifest refraction corrected to the corneal plane and the effective toric IOL power calculated with the Holladay IOL Consultant Program (Holladay Consulting, Inc., Bell Air, USA) from the corneal astigmatism measured by each device. Their results confirmed the findings in the above-noted study. They found an overestimation of with-the-rule astigmatism of 1) 0.5 to 0.6 D in eyes that had with-the-rule astigmatism on the anterior corneal surface and 2) 0.2 to 0.3 D in eyes that had against-the-rule corneal astigmatism on the anterior corneal surface. Posterior corneal as-tigmatism can be measured directly using devices such as the dual Scheimpflug analyzer, although the accuracy on an individual basis is still uncertain. Alternatively, one can account for posterior corneal astigmatism using nomograms such as the Baylor Toric IOL Nomo-gram (Table 1). Although this nomogram derived from the findings of previous studies(33,35), further validation would be beneficial.
Surgically induced astigmatism
When calculating the power of toric IOLs, it is also important to consider the surgically induced astigmatism (SIA). The SIA is a result of flattening in the meridian of incision and steepening 90o away(36). The amount of SIA depends on several factors, including the size, sha-pe, and location of the incision, suture use, and the response of the patient’s cornea. As an incision is placed further from the optical axis, it may progressively have a bigger width and still remain astigma-tically neutral. Thus, a longer scleral tunnel incision can induce as much SIA as a shorter clear corneal incision(37). With regards to shape of the scleral tunnel incision, various authors have investigated the SIA associated with straight, curved (parallel to the limbus), reverse curved (frown incision), and V-shaped incisions. However, none of these shapes have been clearly shown to induce less astigma-tism(38,39). Conversely, previous papers have shown that incision loca-tion plays an important role in the amount of SIA. Nasal, superonasal and superior incisions induce more astigmatism than temporal and superotemporal incisions(40-43). Each surgeon should calculate his/her own SIA, which can be done using a standard astigmatism vector analysis(44). One of the websites that can be used for this purpose is http://www.doctor-hill.com/(45).
Table 1. Baylor Toric IOL Nomogram* (postoperative target: up to 0.40 D WTR astigmatism)
Effective IOL cylinder power at corneal plane (D) WTR (D) ATR (D)
0 ≤1.69 (PCRI if >1.00) <0.39
1.00 1.70 - 2.19 0.40* - 0.79
1.50 2.20 - 2.69 0.80* - 1.29
2.00 2.70 - 3.19 1.30* - 1.79
2.50 3.20 - 3.69 1.80* - 2.29
3.00 3.70 - 4.19 2.30* - 2.79
3.50 4.20 - 4.69 2.80* - 3.29
4.00 4.70 - 5.19 3.30* - 3.79
WTR= with-the-rule astigmatism; ATR= against-the-rule astigmatism; D= diopter; PCRI= peripheral corneal relaxing incision.*= values in the table are the vector sum of the anterior corneal and surgically induced as ti gmatism If an SN6AT2 is available, consider implanting it in WTR astigmatism of 1.40 - 1.69 D, and in ATR of 0.30 - 0.49 D (in this latter case, T3 would be implanted in astigmatism ranging from 0.50 to 0.79 D).

7þćčĎċú�#7 �þč�úą�
127"SR�#SBT�0GUBMNPM�����������������
Calculating toric IOL power
Determination of the optimal IOL toricity can be performed using a calculation program provided by the manufacturer, calculation me-thods described in the literature(46), or nomograms, such as the Baylor Toric IOL Nomogram (Table 1). The cylindrical power of the toric IOL should be chosen based on the total corneal astigmatism, taking into consideration anterior corneal astigmatism, posterior corneal as-tig matism, and SIA. Another factor to consider is the impact of effective lens position and of the spheroequivalent power of the IOL on the effective cylinder power of the IOL at the corneal plane. Effective toricity of the IOL diminishes with increasing anterior chamber depth and lower IOL spherical power. The Holladay IOL Consultant Program and the Tecnis Toric Calculator (Abbott Laboratories Inc., Santa Ana, USA)(47) take this into account in its calculation of toric IOL power. Furthermore, when choosing the IOL toricity, it is desirable to leave patients with slight with-the-rule astigmatism, due to the normal tendency for astigmatism to drift against-the-rule with advancing age. Thus, leaving this slight with-the-rule astigmatism prolongs the period of time in which the patient’s corneal astigmatism is compen-sated by the toric IOL(15,23,33,48).
TORIC IOL ALIGNMENT AND EYE MARKING TECHNIQUES
During surgery, the marks on the toric IOL should be aligned with the previously marked meridian of alignment. The marks on the IOL indicate the flat meridian (plus cylinder axis) of the toric lens. Accurate toric lens alignment at the calculated meridian is crucial to achieve effective astigmatism correction. When a toric IOL is misaligned, there is a reduction in the cylinder correction along the desired meridian and induction of cylinder at a new meridian. For any given eye, the magnitude of residual cylinder power and the site of the new cylinder axis depend on the cylinder power of the toric IOL and the degree of misalignment. The precise relation between residual cylinder and meridional misalignment is sinusoidal, although, within 15 degrees of misalignment, the amount of residual cylinder is approximately 3.5% per degree. A 30o misalignment induces an estimated residual cylinder of 100% of the toric IOL cylinder power, again with the new astigmatic meridian far away from the original steep meridian(49). Im-portantly, the residual cylinder can be large and visually disturbing to the patient.
Preoperatively, the eye should be marked with the patient in an upright position to compensate for cyclotorsion. When the patient goes from the upright to the supine position, a cyclotorsion of appro -xi mately 2o to 3o usually occurs, with some patients having up to 14o of cyclotorsion(50,51). Also, the marking procedure should be performed with the patient fixating with the contralateral eye at a distant target at head height to avoid cyclotorsion from near-fixation.
There are several eye marking techniques. The most commonly described is a 3-step procedure: 1) preoperatively marking the eye at the horizontal meridian, which can be done using a coaxial thin slit beam of the slit-lamp turned to the 3- and 9-o’clock position, a bubble marker, a pendular marker, or a tonometer marker, (2) intraoperatively aligning to these marks a secondary device with angular graduations, such as the Mendez gauge, and (3) then marking the limbus or the cornea at the desired angle of alignment using a surgical marking pen or a needle(49,52). A previous study evaluating the accuracy of the 3-step procedure using a bubble marker in the first step found a mean error in axis marking of 2.4o ± 0.8o, and a total error in toric IOL alignment of 4.9o ± 2.1o. Even though the slit-lamp marker and the pendular marker seem to be more accurate than the bubble marker and the tonometer marker(52), the eye marking procedure is a potential source of error for toric IOL alignment, and should be done carefully, independently of the instruments used.
A 1-step technique has been described using a slit-lamp eyepiece with an embedded angle-measuring reticule or using a slit-lamp that allows measurement of the angle in which the slit beam is rotated(49).
Another technique uses a preoperative anterior segment photograph of the cornea and limbal vessels together with imaging software to determine the distance from two reference limbal vessels to the desi-red alignment meridian(53). Intraoperatively, the surgeon uses calipers to apply the distances calculated from the photograph to the reference vessels and to mark the desired meridian for IOL alignment. This later technique had a mean meridional marking error of 2.29o ± 1.06°(53).
An iris fingerprinting technique is another option for marking the eye(54). A preoperative detailed image of the eye is obtained, the desired alignment meridian is drawn, and the image is printed and used in the operating room to align the toric lens based on iris cha-racteristics.
Several imaging modalities for toric IOL alignment have been developed, including the Callisto Eye with Z-Align (Carl Zeiss Medi-tec AG, Jena, Germany), the iTrace with Zaldivar Toric Caliper (Tracey Technologies, Houston, USA), the TrueGuide software (TrueVision 3D Surgical, Inc., Santa Barbara, USA), and the VERION Digital Marker (Alcon Laboratories, Ft. Worth, USA).
Zeiss’ Callisto Eye with Z-align integrates with the OPMI Lumera 700 microscope (Carl Zeiss Meditec AG, Jena, Germany) and overlays graphical data onto real-time video images in the operating room. The original version requires preoperative manual marking of the 0° and 180° axis with the patient seated. The horizontal axis serves as a reference axis, being automatically detected by the Callisto system intraoperatively. Using this reference axis, the intended toric IOL axis (entered into the Callisto interface preoperatively) is digitally displayed to the surgeon as three parallel lines superimposed on the patient’s eye within the oculars of the operative microscope. Active eye tracking software using the inkpen marks and software recogni-tion of the limbus maintains alignment of the digitally overlaid axis lines with the position of the eye in real-time. This graphical overlay serves as a visible guide to the surgeon for toric IOL alignment along the appropriate axis. A newer version of Callisto Eye is available; this imports a high contrast digital reference image obtained by the IOLMaster 500 biometer (Carl Zeiss Meditec., Jena, Germany) to de-termine the reference axis and provide intraoperative eye-tracking, based on limbal and scleral vessels(55).
Tracey’s iTrace preoperatively measures the patient’s corneal to -pography and keratometry, displaying the corneal topography data and a reticule superimposed on a photograph of the patient’s cornea and limbus (Figure 1). The Zaldivar Toric Caliper tool can be used to calculate the angle difference in degrees between the steep meridian (intended toric IOL axis) and iris or limbal landmarks, both nasally and temporally. This information is printed and taken to the operating room for intraoperative guidance during toric IOL alignment (Figure 1).
The TrueGuide software uses a preoperative photograph and in traoperative registration to enable digital intraoperative surgical guidance and alignment of toric IOLs, without the need for preo-perative ocular marking. The i-Optics Cassini topographer (i-Optics, The Hague, Netherlands) is used to obtain a high-resolution image of the patient’s eye preoperatively (Figure 2). This source image is then uploaded to the TrueVision system in the operating room for intraoperative registration of the patient’s eye based on iris landmarks, scleral/limbal vessels, and scleral pigmentation. When combined with the system’s active tracking software, the intended toric IOL axis and a protractor along the limbus can be digitally aligned on a live view of the eye and tracked in real-time on a HD monitor to aid in IOL alignment.
Alcon’s VERION Digital Marker also uses a high-resolution preope-rative image and intraoperative registration to guide toric IOL alignment without the need of preoperative ocular marking. The VERION system matches the preoperative photograph with the eye intraoperatively using scleral vessels, limbal vessels, and iris features. This facilitates proper reference alignment and tracking of the eye in real-time throughout the case. The intended toric IOL axis along

4ĎċĀĂüúą�ĆúćúĀþĆþćč�Ĉÿ�úČčĂĀĆúčĂČĆ�ĐĂčā�čĈċĂü�ĂćčċúĈüĎąúċ�ąþćČþČ�
��� "SR�#SBT�0GUBMNPM�����������������
with a limbal protractor is graphically aligned on a live view of the eye, being displayed on an external monitor or through the oculars of compatible microscopes. The toric IOL can then be aligned along the appropriate axis, guided by the digital overlay (Figure 3).
All of these automated systems using anatomic or topographic landmarks to guide toric IOL alignment seek to decrease the inherent error associated with preoperative manual marking alone. However, there is still a need for clinical studies to assess the efficacy of each of these systems.
CLINICAL OUTCOMES
The correction of less than 0.50 D of corneal astigmatism does not seem to improve visual performance(56). However, in patients with cor-neal astigmatism above 0.75 D, implantation of toric IOLs is associated with better visual outcomes than monofocal IOLs: significantly more patients achieve an UDVA better than 20/40 and better than 20/25, are spectacle-independent, and have a lower absolute residual refractive cylinder(3). In peer-reviewed papers, the reported percentage of pa-tients achieving an UDVA better than 20/40 after toric IOL implantation
ranges from 70% to 100%(4,5,32,33). Spectacle-independence for distance vision was reported by 60% to 85% of patients with unilateral toric IOL(3,6,31,34) and by 69% to 97% of patients with bilateral toric IOLs(7,8,35,36). Reported percentages of patients with residual refractive astigmatism lower than 0.50 D range from 25% to 100%(9,10,37,38). In addition, patients with forme fruste keratoconus and mild non-progressive keratoconus generally have a meaningful reduction in ocular astigmatism and improved uncorrected visual acuity after toric IOL implantation(11-13).
Toric multifocal IOLs are also associated with good visual outco-mes. In the literature, an UDVA better than 20/40 has been reported in 97% to 100% of patients, while 100% of patients had an uncorrected near visual acuity better than 20/40(14,15,42,43). Spectacle-independence was achieved by 79% to 100% of patients(15,16,43,44). The percentage of patients with a residual refractive astigmatism lower than 0.50 D ranged from 38% to 79%(15,16). However, some patients had symptoms that are typically associated with multifocal lenses, such as glare and halos(16). Thus, when considering the implantation of a toric multifocal IOL, it is important to explain to the patient the possible benefits, but also the potential of having disturbing visual symptoms inherent to the current models of multifocal IOLs.
Figure 1. Image from iTrace to guide intraocular (IOL) lens alignment in a patient’s right eye. A reticule is superimposed on a photograph of the patient’s cornea and limbus. In this case the IOL should be aligned at 62°. The Zaldivar Toric Caliper tool is used to calculate the angle difference in degrees between the intended meridian for toric IOL alignment and a limbal vessel temporally (118°). This image is printed and used intraoperatively to guide IOL alignment.
Age Eye Steep axis (deg) white (mm)
Pachymetry 1 (µm)
Pachymetry 2 (µm)(yrs) (D) (D)
69 Right (OD) 45.45 46.31 19.00 11.22 0 0
Incision axis (deg)
Paracentesis 1 (deg)
Paracentesis 2 (deg)
IOL cylinder Toric axis (deg)
LRI arc length (deg)
LRI axis LRI diameter(D) (deg) (mm)
172.00 112.00 232.00 37.00 0 37.00 10.10
Residual astigmatism 0.01
Figure 2. Two screenshots of the Cassini topographer, which provide the data to the TrueVision system in the operating room for intraoperative registration of the patient’s eye based on iris landmarks, scleral/limbal vessels, and scleral pigmentation. A) Cassini topography superimposed on a photograph of the patient’s cornea and limbus. The red line corresponds to the corneal steep meridian, in this case at 19°, and the blue line corresponds to the flat meridian B) Surgical plan provided by the Cassini. During surgery, the intended toric intraocu lar lens axis of alignment is digitally superimposed on the patient’s eye in real-time.
A B

7þćčĎċú�#7 �þč�úą�
129"SR�#SBT�0GUBMNPM�����������������
Previous studies have shown the efficacy, predictability, safety and stability of toric phakic IOLs in adults(17,18,36,45,46). In a series of 42 eyes, Muñoz et al.(17) reported that 78.6% of eyes had UDVA of 20/25 or better one year after surgery, equal to the percentage of eyes with a CDVA of 20/25 or better preoperatively. Seventy to 81% of eyes with toric phakic IOLs achieved a spherical equivalent within ± 0.50 D range of the preoperative target, and 93% to 99% attained a spherical equivalent within ± 1.00 D range(17,18,45,46). There are no large prospective clinical studies of toric phakic lens implantation in patients with neu robehavioral disorders or in children with high anisometropia or high isometropia and a significant astigmatic component. However, published current case series have reported encouraging results, with a clinically significant decrease in spherical equivalent and im -provement in visual acuity and vision-related quality of life(20,21).
COMPLICATIONS
Toric lens misalignment is a concern, because the lens alignment is intrinsically related to its efficacy in correcting corneal astigmatism. Postoperatively, IOL misalignment from its intended position can be assessed using a slit-lamp with a rotating slit and rotational gauge. This method requires sufficient mydriasis to see the marks on the IOL optic. An obvious limitation in accuracy is the 10-degree steps on the slit-lamp’s measuring reticule.
Errors produced by some combination of misalignment or in-correct toric IOL power can be evaluated using the postoperative as tigmatic refraction and keratometry value(57), postoperative as-tigmatic refraction and power and axis of the toric IOL (Figure 4)(49) or wavefront aberrometry(58). Using vector analysis, postoperative resi-dual refractive astigmatism and keratometry can be used to calculate the angle of lens misalignment. This angle is the angle between the target astigmatism vector and the surgically-induced astigmatism vector (vector of the astigmatism achieved after surgery)(57). Vector analysis can also be used to calculate the angle of lens misalignment based on postoperative astigmatic refraction, and power and axis of toric IOL(49). An online calculator is available for this approach: Berdahl & Hardten Toric IOL Calculator (www.astigmatismfix.com)(59). Another method for determining lens misalignment is wavefront aberro-metry. Based on the internal ocular aberrations, it determines the orientation of the toric IOL, without requiring a dilated pupil(58). Note that all of these methods determine the misalignment of the IOL from an ideal orientation, which may not be the same as the surgically planned orientation due to errors in measuring preoperative corneal astigmatism and the corneal astigmatism induced by the surgery.
There are at least three causes of toric IOL misalignment. One is inaccurate prediction of the ideal IOL alignment, as noted above. A second cause is inaccurate alignment during surgery. Hence, the eye marking procedure is a key factor to achieve correct lens position.
A promising new technology to evaluate toric IOL alignment is in-traoperative wavefront aberrometry. The WaveTec Vision Systems (Aliso Viejo, CA) first introduced the intraoperative wavefront aberrometer called ORange, and then substituted it by the Optiwave Refractive Analysis (ORA) system. The aberrometer is directly attached to the operating microscope and is connected to a monitor. After cataract extraction, it measures the aphakic refraction, and suggests a lens power and the axis of toric IOL alignment. After toric lens placement, it detects the need for IOL rotation (Figure 5). Another intraoperative aberrometer that was recently developed is the Holos (Clarity Me-dical Systems, Pleasanton, California), which provides a continuous video readout of the refractive data during surgery. Unfortunately, intraoperative wavefront aberrometry is still influenced by several factors, such as eyelid speculum pressure and corneal hydration. However, it is a promising technology that can play an important role in toric IOL calculation and alignment.
Figure 3. A screenshot of the VERION Digital Marker showing an overlay of the intended toric intraocular lens axis with adjacent limbal protractor on a live view of the patient’s eye.
Figure 4. An example of an online vector analysis calculator (Berdahl & Hardten Toric IOL Calculator [www.astigmatismfix.com])49 that determines at which axis a toric intraocu lar lens (IOL) should be aligned to minimize the postoperative residual refractive astigma-tism. In this case, the vector analysis is based on the patient’s postoperative astigmatic refraction and power and axis of the implanted toric IOL. By rotating the toric IOL from the 27° axis to the 8° axis, the residual astigmatism would decrease from 1.00 diopter (D) x 52° to 0.02 D x 100°.
Figure 5. Screen of the Optiwave Refractive Analysis (ORA) system showing the results of a pseudophakic measurement. The anticipated residual cylinder with the specified toric IOL power and meridian of alignment was 0.31 diopter (D) x 44o. The residual cylin-der measured after lens placement and alignment was of 0.14 D x 13o, and the device suggested no rotation of the lens.

4ĎċĀĂüúą�ĆúćúĀþĆþćč�Ĉÿ�úČčĂĀĆúčĂČĆ�ĐĂčā�čĈċĂü�ĂćčċúĈüĎąúċ�ąþćČþČ�
130 "SR�#SBT�0GUBMNPM�����������������
A third cause of IOL misalignment is postoperative rotation, which presumably is influenced by the IOL’s architecture and biomaterial and/or ocular anatomy. After lens implantation, the fusion of the anterior and posterior capsules with the lens haptics and border of the optic play an important role in preventing IOL rotation(60). Thus, we would expect that it would be helpful for the anterior capsulorhe-xis to be smaller than the diameter of the lens’ optic to provide a 360o-overlap. The strength of IOL adhesion to the bag varies: hy drophobic acrylic IOLs have the highest adhesive properties, followed by the hydrophilic acrylic IOLs, then the PMMA IOLs, and, finally, the silicone IOLs(61). It is estimated that hydrophobic acrylic lenses rotate less than 1o postoperatively(27). In addition, the lens design also influences its postoperative rotation. IOLs with smaller diameters misalign more frequently(62). Silicone IOLs with loop haptics have a higher incidence of rotation than those with plate haptics(63), but there are reports of more than 5o of rotation in over 27% of sili-cone plate-haptic lenses(64). One study found that acrylic plate- and loop-haptic lenses have similar rotational stability(65). Another factor associated with postoperative toric IOL rotation is axial myopia. Pre-sumably, the capsular bag is larger in axial myopes, slightly increasing the risk of IOL rotation.
Realignment of a significantly misaligned toric IOL should be done within the first few weeks of surgery, because the adhesions that form between the capsular bag and the lens can pose difficulties to the second intervention(66). When the IOL is correctly aligned but there is still residual astigmatism, a corneal relaxing incision or laser refractive surgery can be done.
Other complications associated with toric IOL implantation are those related to the cataract surgery itself, such as posterior capsule opacification, cystoid macular edema, and retinal detachment. Re-garding toric phakic IOLs, possible complications include cataract, significant loss of endothelial cells, pupil ovalization, and pupillary block glaucoma(17).
CONCLUSIONToric IOLs are an effective and safe tool to treat corneal astigmatism in
patients who undergo cataract surgery. However, patients’ outcomes depend on accurate corneal astigmatism measurement, accurate marking of corneal meridians and angle of alignment, and accurate and stable IOL alignment.
REFERENCES 1. Hoffmann PC, Hutz WW. Analysis of biometry and prevalence data for corneal astigma-
tism in 23,239 eyes. J Cataract Refract Surg. 2010;36(9):1479-85. 2. Ferrer-Blasco T, Montés-Micó R, Peixoto-de-Matos SC, González-Méijome JM, Cerviño
A. Prevalence of corneal astigmatism before cataract surgery. J Cataract Refract Surg. 2009;35(1):70-5.
3. Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller KM. The AcrySof Toric intraocular lens in subjects with cataracts and corneal astigmatism: a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010;117(11):2104-11.
4. Entabi M, Harman F, Lee N, Bloom PA. Injectable 1-piece hydrophilic acrylic toric intraocular lens for cataract surgery: efficacy and stability. J Cataract Refract Surg. 2011;37(2):235-40.
5. Cervantes-Coste G, Garcia-Ramirez L, Mendoza-Schuster E, Velasco-Barona C. High-cylinder acrylic toric intraocular lenses: a case series of eyes with cataracts and large amounts of corneal astigmatism. J Refract Surg. 2012;28(4):302-4.
6. Mingo-Botín D, Muñoz-Negrete FJ, Won Kim HR, Morcillo-Laiz R, Rebolleda G, Oblanca N. Comparison of toric intraocular lenses and peripheral corneal relaxing incisions to treat astigmatism during cataract surgery. J Cataract Refract Surg. 2010;36(10):1700-8.
7. Ahmed, II, Rocha G, Slomovic AR, Climenhaga H, Gohill J, Grégoire A, et al. Visual function and patient experience after bilateral implantation of toric intraocular lenses. J Cata-ract Refract Surg. 2010;36(4):609-16.
8. Lane SS, Ernest P, Miller KM, Hileman KS, Harris B, Waycaster CR. Comparison of clini-cal and patient-reported outcomes with bilateral AcrySof toric or spherical control intraocular lenses. J Refract Surg. 2009;25(10):899-901.
9. Dick HB, Krummenauer F, Tröber L. [Compensation of corneal astigmatism with toric intraocular lens: results of a multicentre study]. Klin Monbl Augenheilkd. 2006;223(7): 593-608. German.
10. Lichtinger A, Sandstedt CA, Schwartz DM, Chayet AS. Correction of astigmatism after cataract surgery using the light adjustable lens: a 1-year follow-up pilot study. J Refract Surg. 2011;27(9):639-42.
11. Jaimes M, Xacur-García F, Alvarez-Melloni D, Graue-Hernández EO, Ramirez-Luquin T, Navas A. Refractive lens exchange with toric intraocular lenses in keratoconus. J Refract Surg. 2011;27(9):658-64.
12. Visser N, Gast ST, Bauer NJ, Nuijts RM. Cataract surgery with toric intraocular lens implantation in keratoconus: a case report. Cornea. 2011;30(6):720-3.
13. Navas A, Suárez R. One-year follow-up of toric intraocular lens implantation in forme fruste keratoconus. J Cataract Refract Surg. 2009;35(11):2024-7.
14. Venter J, Pelouskova M. Outcomes and complications of a multifocal toric intraocular lens with a surface-embedded near section. J Cataract Refract Surg. 2013;39(6):859-66.
15. Ferreira TB, Marques EF, Rodrigues A, Montés-Micó R. Visual and optical outcomes of a diffractive multifocal toric intraocular lens. J Cataract Refract Surg. 2013;39(7):1029-35.
16. Visser N, Nuijts RM, de Vries NE, Bauer NJ. Visual outcomes and patient satisfaction after cataract surgery with toric multifocal intraocular lens implantation. J Cataract Refract Surg. 2011;37(11):2034-42.
17. Muñoz G, Cardoner A, Albarrán-Diego C, Ferrer-Blasco T, Belda-Salmeron L. Iris-fixa ted toric phakic intraocular lens for myopic astigmatism. J Cataract Refract Surg. 2012;38(7): 1166-75.
18. Doors M, Budo CJ, Christiaans BJ, Luger M, Marinho AA, Dick HB, et al. Artiflex Toric foldable phakic intraocular lens: short-term results of a prospective European multi-center study. Am J Ophthalmol. 2012;154(4):730-9 e2.
19. Crema AS, Walsh A, Ventura BV, Santhiago MR. Visual outcomes of eyes implanted with the new toric multifocal intraocular lens. J Refract Surg. 2014; in press.
20. Althomali TA. Posterior chamber toric phakic IOL implantation for the management of pediatric anisometropic amblyopia. J Refract Surg. 2013;29(6):396-400.
21. Ryan A, Hartnett C, Lanigan B, O’Keefe M. Foldable iris-fixated intraocular lens implan-tation in children. Acta ophthalmol. 2012;90(6):e458-62.
22. Sedaghat M, Ansari-Astaneh MR, Zarei-Ghanavati M, Davis SW, Sikder S. Artisan iris-sup-ported phakic IOL implantation in patients with keratoconus: a review of 16 eyes. J Refract Surg. 2011;27(7):489-93.
23. Nanavaty MA, Lake DB, Daya SM. Outcomes of pseudophakic toric intraocular lens im-plantation in Keratoconic eyes with cataract. J Refract Surg. 2012;28(12):884-9.
24. Luck J. Customized ultra-high-power toric intraocular lens implantation for pellucid mar ginal degeneration and cataract. J Cataract Refract Surg. 2010;36(7):1235-8.
25. Stewart CM, McAlister JC. Comparison of grafted and non-grafted patients with corneal astigmatism undergoing cataract extraction with a toric intraocular lens implant. Clin Experiment Ophthalmol. 2010;38(8):747-57.
26. Hayashi K, Manabe S, Yoshida M, Hayashi H. Effect of astigmatism on visual acuity in eyes with a diffractive multifocal intraocular lens. J Cataract Refract Surg. 2010;36(8): 1323-9.
27. Visser N, Bauer NJ, Nuijts RM. Toric intraocular lenses: historical overview, patient se-lec tion, IOL calculation, surgical techniques, clinical outcomes, and complications. J Cataract Refract Surg. 2013;39(4):624-37.
28. Shirayama M, Wang L, Weikert MP, Koch DD. Comparison of corneal powers obtained from 4 different devices. Am J Ophthalmol. 2009;148(4):528-35 e1.
29. Kobashi H, Kamiya K, Igarashi A, Ishii R, Sato N, Wang G, et al. Comparison of corneal power, corneal astigmatism, and axis location in normal eyes obtained from an auto-keratometer and a corneal topographer. J Cataract Refract Surg. 2012;38(4):648-54.
30. Visser N, Berendschot TT, Verbakel F, de Brabander J, Nuijts RM. Comparability and repeatability of corneal astigmatism measurements using different measurement technologies. J Cataract Refract Surg. 2012;38(10):1764-70.
31. Srivannaboon S, Soeharnila, Chirapapaisan C, Chonpimai P. Comparison of corneal astig ma tism and axis location in cataract patients measured by total corneal power, automa ted keratometry, and simulated keratometry. J Cataract Refract Surg. 2012; 38(12):2088-93.
32. Wang L, Mahmoud AM, Anderson BL, Koch DD, Roberts CJ. Total corneal power estimation: ray tracing method versus gaussian optics formula. Invest Ophthalmol Vis Sci. 2011;52(3):1716-22.
33. Koch DD, Ali SF, Weikert MP, Shirayama M, Jenkins R, Wang L. Contribution of poste-rior corneal astigmatism to total corneal astigmatism. J Cataract Refract Surg. 2012; 38(12):2080-7.
34. Ho JD, Tsai CY, Tsai RJ, Kuo LL, Tsai IL, Liou SW. Validity of the keratometric index: evaluation by the Pentacam rotating Scheimpflug camera. J Cataract Refract Surg. 2008;34(1):137-45.
35. Koch DD, Jenkins R, Weikert MP, Yeu E, Wang L. Correcting astigmatism with toric intraocular lenses: the effect of posterior corneal astigmatism. J Cataract Refract Surg. 2013;39(12):1803-9.
36. Visser N, Berendschot TT, Bauer NJ, Nuijts RM. Vector analysis of corneal and refractive astigmatism changes following toric pseudophakic and toric phakic IOL implanta-tion. Invest Ophthalmol Vis Sci. 2012;53(4):1865-73.
37 Koch PS. Structural analysis of cataract incision construction. J Cataract Refract Surg. 1991;17:661-7.
38. Vass C, Menapace R, Rainer G. Corneal topographic changes after frown and straight sclerocorneal incisions. J Cataract Refract Surg. 1997;23(6):913-22.
39. Wollensak J, Pham DT, Seiler T. [Effect of incision form and tunnel length on induced as-tigmatism with the no-stitch technique.] Ophthalmologe. 1994;91(4):439-41. German.

7þćčĎċú�#7 �þč�úą�
131"SR�#SBT�0GUBMNPM�����������������
VII Congresso Brasileiro da SOBLEC
10 a 12 de março de 2015 Maksoud Plaza Hotel
São Paulo - SP
Informações: E-mail: [email protected]
Site: www.congressosoblec.com.br
40. Altan-Yaycioglu R, Akova YA, Akca S, Gur S, Oktem C. Effect on astigmatism of the location of clear corneal incision in phacoemulsification of cataract. J Refract Surg. 2007;23(5):515-8.
41. Mallik VK, Kumar S, Kamboj R, Jain C, Jain K, Kumar S. Comparison of astigmatism following manual small incision cataract surgery: superior versus temporal approach. Nepal J Ophthalmol. 2012;4(1):54-8.
42. Pakravan M, Nikkhah H, Yazdani S, Shahabi C, Sedigh-Rahimabadi M. Astigmatic outcomes of temporal versus nasal clear corneal phacoemulsification. J Ophthalmic Vis Res. 2009;4(2):79-83.
43. Anders N, Pham DT, Antoni HJ, Wollensak J. Postoperative astigmatism and relative strength of tunnel incisions: a prospective clinical trial. J Cataract Refract Surg. 1997; 23(3):332-6.
44. Holladay JT, Moran JR, Kezirian GM. Analysis of aggregate surgically induced refracti ve change, prediction error, and intraocular astigmatism. J Cataract Refract Surg. 2001; 27(1):61-79.
45. East Valley Ophthalmology. [Internet]. IOL power calculations: surgically induced astig-matism calculator. [cited 2014 Jan 5]. Available from: http://www.doctor-hill.com/.
46. Langenbucher A, Viestenz A, Szentmary N, Behrens-Baumann W, Viestenz A. Toric intraocular lenses--theory, matrix calculations, and clinical practice. J Refract Surg. 2009;25(7):611-22.
47. Tecnis. Toric aspheric IOL. [Internet]. Tecnis toric calculator. [cited 2014 Jan 5]. Availa-ble from: http://www.tecnistoriciol.com/tecnis-toric-iol-calculator/.
48. Hayashi K, Hirata A, Manabe S, Hayashi H. Long-term change in corneal astigmatism after sutureless cataract surgery. Am J Ophthalmol. 2011;151(5):858-65.
49. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631-6.
50. Chang J. Cyclotorsion during laser in situ keratomileusis. J Cataract Refract Surg. 2008; 34(10):1720-6.
51. Febbraro JL, Koch DD, Khan HN, Saad A, Gatinel D. Detection of static cyclotorsion and compensation for dynamic cyclotorsion in laser in situ keratomileusis. J Cataract Refract Surg. 2010;36(10):1718-23.
52. Popp N, Hirnschall N, Maedel S, Findl O. Evaluation of 4 corneal astigmatic marking methods. J Cataract Refract Surg. 2012;38(12):2094-9.
53. Cha D, Kang SY, Kim SH, Song JS, Kim HM. New axis-marking method for a toric intraocular lens: mapping method. J Refract Surg. 2011;27(5):375-9.
54. Osher RH. Iris fingerprinting: new method for improving accuracy in toric lens orien-tation. J Cataract Refract Surg. 2010;36(2):351-2.
55. Hill WE, Lackerbauer C, Olsen T, Shah S. Diagnostic technologies for enhanced cataract surgery outcomes: surgeons discuss their preferred tools for achieving superior results. Cataract & Refractive Surgery Today Europe [Internet]. 2013 mar [cited 2014 Jan 5];20-7. Available from: http://bmctoday.net/crstodayeurope/pdfs/0313CRSTEuro_bf3_ Diagnostics.pdf
56. Villegas EA, Alcón E, Artal P. Minimum amount of astigmatism that should be cor re cted. J Cataract Refract Surg. 2014;40(1):13-9.
57. Alpins NA, Goggin M. Practical astigmatism analysis for refractive outcomes in cata-ract and refractive surgery. Surv Ophthalmol. 2004;49(1):109-22.
58. Carey PJ, Leccisotti A, McGilligan VE, Goodall EA, Moore CB. Assessment of toric in-traocular lens alignment by a refractive power/corneal analyzer system and slit lamp observation. J Cataract Refract Surg. 2010;36(2):222-9.
59. Toric results analyzer. [Internet]. [cited 2014 Jan 5]. Available from: http://www.astig-matismfix.com.
60. Linnola RJ, Werner L, Pandey SK, Escobar-Gomez M, Znoiko SL, Apple DJ. Adhesion of fibronectin, vitronectin, laminin, and collagen type IV to intraocular lens materials in pseudophakic human autopsy eyes. Part 1: histological sections. J Cataract Refract Surg. 2000;26(12):1792-806.
61. Lombardo M, Carbone G, Lombardo G, De Santo MP, Barberi R. Analysis of intraocu-lar lens surface adhesiveness by atomic force microscopy. J Cataract Refract Surg. 2009;35(7):1266-72.
62. Chang DF. Early rotational stability of the longer Staar toric intraocular lens: fifty consecutive cases. J Cataract Refract Surg. 2003;29(5):935-40.
63. Patel CK, Ormonde S, Rosen PH, Bron AJ. Postoperative intraocular lens rotation: a randomized comparison of plate and loop haptic implants. Ophthalmology. 1999; 106(11):2190-5; discussion 2196.
64. Chang DF. Comparative rotational stability of single-piece open-loop acrylic and pla-te-haptic silicone toric intraocular lenses. J Cataract Refract Surg. 2008;34(11):1842-7.
65. Prinz A, Neumayer T, Buehl W, Vock L, Menapace R, Findl O, et al. Rotational stability and posterior capsule opacification of a plate-haptic and an open-loop-haptic intra-ocular lens. J Cataract Refract Surg. 2011;37(2):251-7.
66. Chang DF. Repositioning technique and rate for toric intraocular lenses. J Cataract Refract Surg. 2009;35(7):1315-6.

132 "SR�#SBT�0GUBMNPM��������������
-þččþċČ�čĈ�čāþ�&ýĂčĈċ
Use of the Iowa Satisfaction with
Anesthesia Scale in Portuguese
Fernandes et al.(1) used the Iowa Satisfaction with Anesthesia Scale (ISAS) to measure patient satisfaction after cataract surgery. The ISAS generally is appropriate for cataract surgery and has content validity for monitored anesthesia care(1-3). Fung et al.(4) showed that the ISAS can be used to measure patient satisfaction with cataract care under topical local anesthesia and monitored sedation.
However, the three previous studies that assessed the reliability and validity of ISAS were performed in English. There is a clear dis-tinction in English between the somatic “I felt pain” and the emotive “I hurt.” The authors’ Methods section does not state that the study was limited to patients who speak and write English at a 4th grade level or higher, as applicable. The authors’ Discussion does not men-tion language. Was the instrument used in English or Portuguese? If Portuguese, what systematic processes were used for translation? What percentage of respondents answered these two questions differently? What was the internal consistency (Cronbach alpha) of the instrument? A Portuguese version of the instrument would be very helpful for future investigations.
In addition, ISAS is copyrighted by Franklin Dexter and the Uni-versity of Iowa Research Foundation. This is stated in each table of the original paper, throughout the second paper, and in each related table of the Fung et al. paper(2-4). Performing a web search with either Google or Bing (performed February 14, 2014) using the term “Iowa Satisfaction with Anesthesia Scale” returned the authorization form for use as the first entry. What steps did the authors follow to use ISAS, and what changes do the authors recommend for the authorization process described at www.FranklinDexter.net/FAQ/FAQ_a32.htm.
Franklin Dexter
Department of Anesthesia, University of Iowa, Iowa City.
Disclosure of potential conflicts of interest: Please refer to www.FranklinDexter.net/FAQ/FAQ_a1.htm. The Iowa Satisfaction with Anesthesia Scale is copyrighted by Franklin Dexter and the University of Iowa Research Foundation. Income from the Division’s consulting work, including the Iowa Satisfaction with Anesthesia Scale scores, is used to fund Division research.
Correspondence author: Franklin Dexter. Division of Management Consulting. Department of Anes-thesia University of Iowa - 200 Hawkins Dr 6JCP - Iowa City, IA 52246 USA. +1 (319) 621-6360 - E-mail: [email protected]
Submitted for publication: February 17, 2014Accepted for publication: February 27, 2014
REFERENCES 1. Fernandes MB, de Souza RV, Vasconcelos GC, Ribeiro KG, Andrade BB, Fernandes CR.
Assessing patient satisfaction with cataract surgery under topical anesthesia supple-mented by intracameral lidocaine combined with sedation. Arq Bras Oftalmol. 2013; 76(6):345-9.
2. Dexter F, Aker J, Wright WA. Development of a measure of patient satisfaction with monitored anesthesia care: the Iowa Satisfaction with Anesthesia Scale. Anesthesio-logy. 1997;87(4):865-73.
3. Dexter F, Candiotti KA. Multicenter assessment of the Iowa Satisfaction with Anesthe-sia Scale, an instrument that measures patient satisfaction with monitored anesthesia care. Anesth Analg. 2011;113(2):364-8.
4. Fung D, Cohen M, Stewart S, Davies A. Can the Iowa Satisfaction with Anesthesia Scale be used to measure patient satisfaction with cataract care under topical local anesthesia and monitored sedation at a community hospital? Anesth Analg. 2005;100(6):1637-43.
Reply
The authors appreciate the thoughtful comments expressed in the letter. Authors have applied published grading system that has been used in the medical field for several situations, including tumor grading, graft rejection grading, heart failure grading (NYHSA score), criteria for diagnosing rheumatological conditions, and many other published guidelines.
We consider the Iowa Satisfaction with Anesthesia Scale (ISAS) scale as a very interesting and useful method to measure patient sa tisfaction after cataract surgery. As stated in letter, ISAS is generally appropriate for cataract surgery. The ISAS had content validity for monitored anesthesia care(1,2) and Fung et al., showed “…ISAS can be used to measure patient satisfaction with cataract care under topical local anesthesia and monitored sedation”(3).
The internal consistency was not measured because this was an exploratory pilot study. All patients were Brazilian and spoke Por-tuguese. The instrument was applied in Portuguese and our group translated it. All authors speak Portuguese as their native language and English higher than a fourth grade level. The translation was evaluated before its submission by the company American Journal Experts. “I felt pain” was translated exactly as “I felt pain,” and “I hurt” was translated as “I hurt.” All patients who had answered that they felt pain had answered they did not hurt, and most patients had no pain and had not hurt themselves.
We are glad to know there is interest in validating ISAS in Por-tuguese. The data obtained herein would be useful for a future pilot study that might examine the reliability and validity of ISAS in Portuguese. Knowing how to best use ISAS would help investigators in future studies.
Manuela Bezerril Cipiao Fernandes
TSA, Sociedade Brasileira de Anestesia, BA, Hospital Geral de Fortaleza.
Correspondence author: Manuela Fernandes. Department of Anesthesiology. Hospital Geral de Fortaleza. Rua José Vilar, 300/1300 - Fortaleza (CE) - 60125-000 - Brazil.E-mail: [email protected]
REFERENCES 1. Dexter F, Aker J, Wright WA. Development of a measure of patient satisfaction with
mo nitored anesthesia care: the Iowa Satisfaction with Anesthesia Scale. Anesthesio-logy. 1997;87(4):865-73.
2. Dexter F, Candiotti KA. Multicenter assessment of the Iowa Satisfaction with Anesthe-sia Scale, an instrument that measures patient satisfaction with monitored anesthesia care. Anesth Analg. 2011;113(2):364-8.
3. Fung D, Cohen M, Stewart S, Davies A. Can the Iowa Satisfaction with Anesthesia Scale be used to measure patient satisfaction with cataract care under topical local anes thesia and monitored sedation at a community hospital? Anesth Analg. 2005; 100(6):1637-43.

133"SR�#SBT�0GUBMNPM��������������
-þččþċČ�čĈ�čāþ�&ýĂčĈċ
Plagiarism and misconduct in research
Sir, the article on “plagiarism and misconduct in research”(1) is very interesting. Chamon reported the use of the computational tool for help detect the plagiarism(1). In fact, the detection of plagiarism in submitted manuscript should be the requirement for all biomedical journals. The pre-submission screening should be encouraged for all contributors(2). Of interest, although there are several attempts the pro blems can still be detected. The use of computational tool might be a solution but it still has the limitations. First, the computational program might not be possible to detect the problem of figure pla-giarism as well as conceptual plagiarism(3), which are also common problems in the present day. Second, when the problem is detected and reported, the response and action from the plagiarist’s institute might not appropriate(4). As Chamon mentioned for “where we are and what we can do”(1), it seems that it is still a long way to successfully manage the problem. Re-evaluation on the success of the implemen-
tation of the computation tool for detection of plagiarism should be continuously done.
Beuy Joob1, Viroj Wiwanitkit2
1 Sanitation Medical Academic Center, Bangkok, Thailand.2 Joseph Ayobabalola University, Nigeria.
Funding: No specific financial support was available for this study.
Disclosure of potential conflicts of interest: None of the authors have any potential conflicts of interest to disclose
Correspondence author: Beuy Joob. Sanitation Medical Academic Center, Bangkok, Thailand - E-mail: [email protected]
Submitted for publication: February 18, 2014Accepted for publication: February 18, 2014
REFERENCES 1. Chamon W. Plagiarism and misconduct in research: where we are and what we can
do. Arq Bras Oftalmol. 2013;76(6):V-VI. 2. Wiwanitkit V. Plagiarism: pre-submission screening. Perspect Clin Res. 2011;2(4):149-50. 3. Wiwanitkit V. Plagiarism, beyond crosscheck, figure and conceptual theft. Sci Eng
Ethics. 2013 Sep 18. [Epub ahead of print] 4. Wiwanitkit V. Plagiarism, management, journal retraction and response by author’s
institute. Saudi J Anaesth. 2013;7(2):223.

���"SR�#SBT�0GUBMNPM����������������
*ćČčċĎüčĂĈćČ�"ĎčāĈċČ
INSTRUCTIONS TO AUTHORS
ABO-ARQUIVOS BRASILEIROS DE OFTALMOLOGIA (ABO, ISSN 0004-2749 - printed version and ISSN 1678-2925 - online version) is the official bimonthly publication of the Brazilian Council of Ophthal-mology (Conselho Brasileiro de Oftalmologia - CBO). The purpose of the journal is to publish scientific studies in Ophthalmology, Visual Sciences, and Public Health, encouraging research, as well as qualifi-cation and updating of the professionals involved in this field.
METHODSOriginal manuscripts are accepted in Portuguese or English. All
ma nuscripts submitted in Portuguese will be translated to English before publishing. Authors will cover translation costs. Manuscripts are grouped into one of the following categories based on the me-thodology used:
CLINICAL STUDIES
Descriptive or analytical studies involving humans or evaluating the literature relevant to humans.
EPIDEMIOLOGICAL STUDIES
Analytical studies involving results from human populations.
LABORATORY EXPERIMENTAL STUDIES
Descriptive or analytical studies involving animal models or other biological, physical or chemical techniques.
THEORETICAL STUDIES
Descriptive studies involving description and theoretical analysis of new hypotheses based on the knowledge available in the literatu-re. Theoretical results must add new information to literature.
TYPES OF MANUSCRIPTSManuscripts submitted to ABO should fit into one of the follo-
wing categories according to their format. The maximum number of words, figures, tables and, references for each type of manuscript are in parentheses at the end of the description for each category. The word count of the manuscript includes the text from the beginning of the introduction up to the end of the discussion; therefore, the following items are not included: title page, abstract, references, acknowledgments, tables and figures, including legends.
EDITORIALS
Editorials are contributed by invitation and should be related to to pics of current interest, preferentially related to articles published in the same issue of ABO (title, maximum of 1,000 words, 2 figures or tables, and 10 references).
ORIGINAL ARTICLES
Original articles present complete experiments with results that have never been published before (title, structured abstract, maxi-mum of 3,000 words, 7 figures or tables, and 30 references). The eva-luation of the manuscripts will be based on the following priorities:
1. New and relevant information confirmed in a study using appro-priate methodology.
2. Repetition of information available in the literature, but not previously confirmed locally, based on a study using appropriate methodology.
3. Repetition of information available in the literature and previously confirmed locally, based on a study using appropriate methodology.
* Manuscripts containing speculative conclusions, unsubstantiated by the results or based on a study with inappropriate methodology will not be accepted.
CASE REPORTS AND CASE SERIES
Case reports or case series will be considered for publication when describing rare and original findings that have not been internatio-nally confirmed, or when presenting clinical or surgical responses that can contribute to elucidate the pathophysiology of a disease (ti tle, unstructured abstract, maximum of 1,000 words, 4 figures or tables, and 10 references).
LETTERS TO THE EDITOR
Letters to the editor are considered for publication if they contain comments related to manuscripts previously published in ABO or, exceptionally, the results of original studies with insufficient content to be submitted as Original Article. These letters should present new information or new interpretation of existing information. When the content of the letter refers to an article previously published in ABO, such article should be mentioned in the first paragraph of the letter and included in its reference list. In these cases, the letters will be linked to the article, and the authors of the article will have their right of reply guaranteed in the same issue. Congratulation letters will not be published (title, maximum of 700 words, 2 figures or tables, and 5 references).
REVIEW ARTICLES
Review articles follow the editorial line and are accepted only by invitation from the editor. Suggestions of topics for review articles should be sent directly to the editor, but manuscripts cannot be sent without an invitation (title, unstructured abstract, maximum of 4,000 words, 8 figures or tables, and 100 references).
EDITORIAL PROCESSManuscripts will only be considered for publication if they meet
all the journal’s requirements. The editorial office will inform the authors if their manuscript fails to meet such requirements. Upon notification, the corresponding author will have 30 days to make the necessary changes in the manuscript. If the deadline is not met, the manuscript will be excluded from the editorial process.
The manuscripts submitted to ABO are initially evaluated by the editors to check for content compliance with the editorial line of the journal. After this assessment, all manuscripts are sent for peer review. The anonymity of reviewers is preserved throughout the whole process. However, the authors of manuscripts do not remain anonymous.
After the initial editorial evaluation, the reviewers’ comments can be sent to the authors to guide the changes to be implemented in the text. After implementing the changes suggested by the revie-wers, the revised manuscript should be resubmitted along with a letter (which is sent as a supplementary document) with specific in dications of all changes made to the manuscript or the reasons why the suggested changes were not made. Manuscripts that are resubmitted without a letter will be withheld until the editorial office receives the letter. The deadline to submit the new version of the ma-

136 "SR�#SBT�0GUBMNPM����������������
nuscript is 30 days after the authors are informed of the need to make changes in their manuscript. Manuscripts will be excluded from the process if authors fail to meet this deadline. The ultimate publication will be based on the final approval of the editors.
Manuscripts submitted to ABO should not be simultaneously considered for publication by other journals. In addition, total or par-tial publication or translation for publication in another language of the manuscripts submitted to ABO should not be considered without the permission of the editors of ABO.
AUTHORSHIPThe criteria for authorship of manuscripts in medical journals are
well established. Individuals who have contributed in a concrete way during the following three phases of manuscript preparation should be considered authors: I. Conception and design, acquisition of data, or analysis and
interpretation of data. II. Draft or critical revision of the article for important intellectual
content. III. Final approval of the version to be published.
The authors of manuscripts submitted to ABO should make sure that all authors meet the criteria mentioned above and that all per -sons who meet these criteria are listed. Individuals who hold head-ship positions cannot be considered authors of manuscripts based only on their positions. ABO does not accept the participation of honorary authors.
The corresponding author should complete and submit the Au-thor Contribution Statement as a supplementary document.
GUIDELINES FOR EXCELLENT RESEARCHIt is recommended that authors follow the appropriate guideline
bellow before submitting your work:CONSORT (Controlled and randomized clinical trials)STARD (Diagnostic instruments or techniques)PRISMA (Systematic reviews and meta-analyses) STROBE (Observational studies)
MANUSCRIPT PREPARATIONManuscripts should only be submitted online using the appro-
priate interface of ABO. The following guidelines were based on the format suggested by the International Committee of Medical Journal Editors (ICMJE) and published in the document: Uniform Require-ments for Manuscripts Submitted to Biomedical Journals.
Only the manuscripts complying with these guidelines will be considered for analysis.
The text should be sent as a digital file. Only the following formats are accepted: .doc or .rtf. The text should be typed double-spaced, in 12 point font. The pages should be numbered in Arabic numerals, starting each section on a new page.
The sections should be presented according to the following se-quence: Title page (as a separate document); Abstract and Keywords; Introduction; Methods; Results; Discussion; Acknowledgements (if any); References; Tables (optional) and Figures (optional) including legends.
1. Title Page. It should contain: a) title (no more than 135 characters with spaces); b) running title to be used as a page heading (no more than 60 characters with spaces); c) authors’ names as they should appear in print; d) each author’s affiliation* (city, state, country and, if applicable, department, school, university); e) corresponding author’s, name, address, phone number, and email; f ) sources of fi-
nancial support (if any); g) project number and institution responsible for the approval of the Research Ethics Committee; h) statement of conflicts of interests of all authors; i) clinical trial registration number on a public trials registry.* Professional or academic degrees, as well as job position will not be published.
Approval of the Institutional Review Board (IRB). All retrospec-tive, cross-sectional, or prospective studies involving primary data collection or clinical and surgical reports should include the project number and name of the institution that provided the approval of the IRB on the title page. Studies involving humans should be compliant with the Declaration of Helsinki, whereas studies involving animals should be in accordance with the principles suggested by the Asso-ciation for Research in Vision and Ophthalmology (ARVO).
As a supplementary document, the corresponding author should send the IRB approval or its report stating that the evaluation of the project by the Committee is not necessary. The author cannot decide on the need for evaluation by the Research Ethics Committee.
Statement of Conflicts of Interest. The title page should contain the statement of conflicts of interest of all authors (even if there is no conflict of interest). For more information about potential conflicts of interest, refer to: World Association of Medical Editors: Conflict of interest in peer-reviewed medical journals.
All authors should send the Form for Disclosure of Potential Con-flicts of Interest as supplementary documents.
Clinical Trials. All Clinical Trials shall include on the title page the registration number in an international registry that allows free ac-cess to trial information (examples: U.S. National Institutes of Health, Australian and New Zealand Clinical Trials Registry, International Standard Randomised Controlled Trial Number - ISRCTN, University Hospital Medical Information Network Clinical Trials Registry - UMIN CTR, Nederlands Trial Register).
2. Abstract and Keywords. Structured abstract (Objective, Metho-ds, Results, Conclusions) with no more than 300 words. Unstructured abstract with no more than 150 words. Five keywords in English listed by the National Library of Medicine (MeSH - Medical Subject Headings).
3. Abstract and Keywords in Portuguese. Structured abstract (Objective, Methods, Results, Conclusions) with no more than 300 words. Unstructured abstract with no more than 150 words. Five keywords in Portuguese listed by BIREME (DeCS - Descritores em Ciências da Saúde). Portuguese translation may be provided by ABO at publication.
4. Introduction, Methods, Results, and Discussion. Citations in the text should be numbered sequentially in superscript Arabic numerals and in parentheses. The names of the authors should not be cited in the text.
5. Acknowledgements. This section should include the colla-boration of people, groups or institutions that deserve to be ack-nowledged but do not meet the criteria for authorship. Statisticians and medical editors may meet the criteria for authorship and, in this case, should be acknowledged as authors. When they do not meet the criteria for authorship, they should be mentioned in this section. Writers who are not identified in the manuscript cannot be accepted as authors; therefore, professional writers should be acknowledged in this section.
6. References. Citations (references) of authors in the text should be numbered sequentially in the same order as they are cited and identified using superscript Arabic numerals. References should be in accordance with the format suggested by the International

137"SR�#SBT�0GUBMNPM����������������
Committee of Medical Journal Editors (ICMJE), based on the exam-ples below.
The titles of the journals should be abbreviated according to the style provided by the List of Journal Indexed in Index Medicus of the National Library of Medicine.
The names of all authors should be cited for references with up to six authors. For studies with seven or more authors, cite only the first six authors followed by et al.
Examples of references:Journal ArticlesCosta VP, Vasconcellos JP, Comegno PEC, José NK. O uso da mitomi cina C em cirurgia combinada. Arq Bras Oftalmol. 1999;62(5):577-80.BooksBicas HEA. Oftalmologia: fundamentos. São Paulo: Contexto; 1991.Book ChaptersGómez de Liaño F, Gómez de Liaño P, Gómez de Liaño R. Exploración del niño estrábico. In: Horta-Barbosa P, editor. Estrabismo. Rio de Janeiro: Cultura Médica; 1997. p. 47-72.AnnalsHöfling-Lima AL, Belfort R Jr. Infecção herpética do recém-nascido. In: IV Congresso Brasileiro de Prevenção da Cegueira; 1980 Jul 28-30, Belo Horizonte, Brasil. Anais. Belo Horizonte; 1980. v.2. p. 205-12.DissertationsSchor P. Idealização, desenho, construção e teste de um ceratômetro cirúrgico quantitativo [dissertation]. São Paulo: Universidade Federal de São Paulo; 1997.Electronic DocumentsMonteiro MLR, Scapolan HB. Constrição campimétrica causada por vigabatrin. Arq Bras Oftalmol. [online journal]. 2000 [cited 2005 Jan 31]; 63(5): [about 4 p.]. Available at:http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0004-27492000000500012&lng=pt&nrm=iso
7. Tables. Tables should be numbered sequentially using Arabic nu-merals in the order they are mentioned in the text. All tables should have a title and a heading for all columns. Their format should be simple, with no vertical lines or color in the background. All ab-breviations (even if previously defined in the text) and sta tistical tests should be explained below the table. The bibliographical source of the table should also be informed when the table is extracted from another study.Do not include tables in the main document of the manuscript, they should be uploaded as supplementary documents
8. Figures (graphs, photos, illustrations, charts). Figures should be numbered sequentially using Arabic numerals in the order they are mentioned in the text. ABO will publish the figures in black and white at no cost to the authors. Manuscripts with color figures will be published only after the authors pay a publication fee of R$ 500.00 per manuscript.
Graphs should preferably be in shades of gray, on a white background and without three-dimensional or depth effects. Instead of using pie charts, the data should be included in tables or described in the text.Photos and illustrations should have a minimum resolution of 300 DPI for the size of the publication (about 2,500 x 3,300 pixels for a full page). The quality of the images is considered in the evaluation of the manuscript.
The main document should contain all figure legends, typed dou ble-spaced and numbered using Arabic numerals.
Do not include figures in the main document of the manuscript; they should be uploaded as supplementary documents.
Supplemental files can have the following extensions: JPG, BMP, TIF, GIF, EPS, PSD, WMF, EMF or PDF.
9. Abbreviations and Acronyms. Abbreviations and acronyms should be preceded by the spelled-out abbreviation on first mention and in the legends of tables and figures (even if they have been pre-viously mentioned in the text). Titles and abstracts should not contain abbreviations and acronyms.
10. Units of Measurement: Values of physical quantities should be used in accordance with the standards of the International System of Units.
11. Language. Texts should be clear to be considered appropriate for publication in a scientific journal. Use short sentences, written in a direct and active voice. Foreign words should be in italics. Thera-peutic agents should be mentioned by their generic names with the following information in parentheses: trade name, manufacturer’s name, city, state and country of origin. All instruments or apparatus should be mentioned including their trade name, manufacturer’s name, city, state and country of origin. The superscript symbol of trademark ® or™ should be used in all names of instruments or trade names of drugs. Whenever there are doubts about style, terminology, units of measurement and related issues, refer to the AMA Manual of Style 10th edition.
12. Original Documents. Corresponding authors should keep the original documents and the letter of approval from the Research Ethics Committee for studies involving humans or animals, the con-sent form signed by all patients involved, the statement of agreement with the full content of the study signed by all authors and the state-ment of conflict of interest of all authors, as well as the records of the data collected for the study results.
13. Corrections and Retractions. Errors may be noted in published manuscripts that require the publication of a correction. However, some errors pointed out by any reader may invalidate the results or the authorship of a manuscript. If substantial doubt arises about the honesty or integrity of a submitted manuscript, it is the editor’s responsibility to exclude the possibility of fraud. In these situations, the editor will inform the institutions involved and the funding agen-cies about the suspicion and wait for their final decision. If there is confirmation of a fraudulent publication in ABO, the editor will act in compliance with the protocols suggested by the International Com-mittee of Medical Journal Editors (ICMJE) and by the Committee on Publication Ethics (COPE).
CHECKLISTBefore submitting their manuscript, authors should make sure
that all the following items are available:� Ƒ�Manuscript prepared in accordance with the instructions to
authors.� Ƒ�Maximum number of words, tables, figures, and references
according to the type of manuscript.� Ƒ� Title page including the clinical trial registration number is not
included in the main document� Ƒ� No figures and tables are included in the main document of
the manuscript.� Ƒ� All figures and tables were uploaded separately as supple-
mentary documents.� Ƒ� Author Contribution Statement completed and saved as a
digital file to be sent as a supplementary document.� Ƒ� Form for Disclosure of Potential Conflicts of Interest of all
authors completed and saved as digital files to be sent as supplementary documents.
� Ƒ� Digital version of the report provided by the Institutional Re-view Board containing the approval of the project to be sent as a supplementary document.

��� "SR�#SBT�0GUBMNPM����������������
Chief Executive Officer: Fernando Steven Ullmann;Commercial Director: Helen Suzana Perlmann; Art Director: Elza Rudolf;
Publishing, Printing and CTP: Ipsis Gráfica e Editora S.A.Frequency of publication: Bimonthly; Circulation: 8.600 copies
Edited byIPSIS GRÁFICA E EDITORA S.A.
Rua Vereador José Nanci, 151 - Parque Jaçatuba 09290-415 - Santo André - SP - Brazil
Phone: (5511) 2172-0511 - Fax (5511) 2273-1557
Advertising
OFTALMOLOGIA
R. Casa do Ator, 1.117 - 2nd Floor - São Paulo - SP - Brazil - 04546-004
Contact: Fabrício LacerdaPhone: (5511) 3266-4000 - Fax: (5511) 3171-0953E-mail: [email protected]
LIST OF WEBITESOnline interface for submission of manuscripts to ABOhttp://www.scielo.br/ABO
Authors’ Participation Formhttp://www.cbo.com.br/site/files/Formulario Contribuicao dos Auto-res.pdf
International Committee of Medical Journal Editors (ICMJE) http://www.icmje.org/
Uniform requirements for manuscripts submitted to biomedical journalshttp://www.icmje.org/urm_full.pdf
Declaration of Helsinkihttp://www.wma.net/en/30publications/10policies/b3/index.html
Principles of the Association for Research in Vision and Ophthalmology (ARVO)http://www.arvo.org/eweb/dynamicpage.aspx?site=arvo2&webcode=AnimalsResearch
World Association of Medical Editors: Conflict of interest in peer-reviewed medical journals.http://www.wame.org/conflict-of-interest-in-peer-reviewed-medical-journals
Authorship Principles according to the ICMJEhttp://www.icmje.org/ethical_1author.html
Form for Disclosure of Potential Conflicts of Interesthttp://www.icmje.org/coi_disclosure.pdf
CONSORT (Consolidated Standards of Reporting Trials)http://www.consort-statement.org/consort-statement/
STARD (Standards for the Reporting of Diagnostic accuracy studies)http://www.stard-statement.org/
PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) http://www.prisma-statement.org/index.htm
STROBE (Strengthening the Reporting of Observational studies in Epidemiology)http://www.strobe-statement.org/
U.S. National Institutes of Healthhttp://www.clinicaltrials.gov
Australian and New Zealand Clinical Trials Registryhttp://www.anzctr.org.au
International Standard Randomised Controlled Trial Number - ISRCTNhttp://isrctn.org/
University Hospital Medical Information Network Clinical Trials Registry - UMIN CTRhttp://www.umin.ac.jp/ctr/index/htm
Nederlands Trial Registerhttp://www.trialregister.nl/trialreg/index.asp
MeSH - Medical Subject Headingshttp://www.ncbi.nlm.nih.gov/sites/entrez?db=mesh&term=
DeCS - Health Sciences Keywords in Portuguesehttp://decs.bvs.br/
Format suggested by the International Committee of Medical Journal Editors (ICMJE)http://www.nlm.nih.gov/bsd/uniform_requirements.html
List of Journal Indexed in Index Medicushttp://www.ncbi.nlm.nih.gov/journals
AMA Manual of Style 10th editionhttp://www.amamanualofstyle.com/
Protocols of the International Committee of Medical Journal Editors (ICMJE) http://www.icmje.org/publishing_2corrections.html
Protocols of the Committee on Publication Ethics (COPE)http://publicationethics.org/flowcharts