Embed Size (px)
Citation preview

HIV PathogenesisLecture 18
Virology W3310/W4310Spring 2012
Nature is not human-‐heartedLAO TZUTao Te Ching
1

2

HIV is a len0virus
• First isolated in 1983 from the lymph node of a paBent with lymphadenopathy in Paris
• Subsequently isolated at NIH and UCSF
• Electron microscopy and sequence analysis revealed them to be lenBviruses, a known group of retroviruses
3

Retroviridae• Orthoretrovirinae
-‐ Alpharetrovirus
-‐ Betaretrovirus
-‐ Gammaretrovirus
-‐ Deltaretrovirus
‣ HTLV-‐1, HTLV-‐2, HTLV-‐3
-‐ Epsilonretrovirus
-‐ LenBvirus
‣ HIV-‐1, HIV-‐24

5

Two evolu0onarily dis0nct groups of human retroviruses
• The lymphotropic viruses: HTLV 1, 2, 3, 4
• The immunodeficiency viruses: HIV-‐1, HIV-‐2
-‐ LenBviruses, not new or unique to humans
-‐ Equine infecBous anemia virus, causes fatal immunodeficiency of horses, isolated early 1900s
6

HIV and AIDS: Acquired ImmunoDeficiency Syndrome
• Syndrome: the occurrence together of a characterisBc group or paXern of symptoms
• HIV-‐1 is the eBological agent of epidemic AIDS
• AIDS denialists: the hypothesis that HIV causes AIDS has been tested by inadvertent infecBon of people with HIV-‐contaminated blood
7

HIV/AIDS pandemic
• In the US, HIV has killed over 600,000, exceeding all US combat-‐related deaths in all wars fought in the 20th century
• >1 million in the US are infected; 25% unaware
• 40,000 new infecBons each year; 70% men, 30% women
• Half of all new infecBons in US occur in people 25 or younger
8

9

Total: 34.0 million [31.6 million – 35.2 million]
Western & Central Europe
840 000[770 000 – 930 000]
Middle East & North Africa470 000
[350 000 – 570 000]
Sub-Saharan Africa22.9 million
[21.6 million – 24.1 million]
Eastern Europe & Central Asia
1.5 million [1.3 million – 1.7 million]
South & South-East Asia 4.0 million
[3.6 million – 4.5 million]
Oceania54 000
[48 000 – 62 000]
North America1.3 million
[1.0 million – 1.9 million]
Latin America1.5 million
[1.2 million – 1.7 million]
East Asia790 000
[580 000 – 1.1 million]Caribbean200 000
[170 000 – 220 000]
Adults and children estimated to be living with HIV | 2010
10

Estimated number of adults and children newly infected with HIV | 2010
Western & Central Europe
30 000[22 000 – 39 000]
Middle East & North Africa59 000
[40 000 – 73 000]
Sub-Saharan Africa1.9 million
[1.7 million – 2.1 million]
Eastern Europe & Central Asia
160 000 [110 000 – 200 000]
South & South-East Asia270 000
[230 000 – 340 000]
Oceania3300
[2400 – 4200]
North America58 000
[24 000 – 130 000]
Latin America100 000
[73 000 – 140 000]
East Asia88 000
[48 000 – 160 000]
Caribbean12 000
[9400 – 17 000]
Total: 2.7 million [2.4 million – 2.9 million]
11

Estimated adult and child deaths from AIDS | 2010
Western & Central Europe
9900[8900 – 11 000]
Middle East & North Africa35 000
[25 000 – 42 000]
Sub-Saharan Africa1.2 million
[1.1 million – 1.4 million]
Eastern Europe & Central Asia
90 000 [74 000 – 110 000]
South & South-East Asia250 000
[210 000 – 280 000]
Oceania1600
[1200 – 2000]
North America20 000
[16 000 – 27 000]
Latin America67 000
[45 000 – 92 000]
East Asia56 000
[40 000 – 76 000]Caribbean
9000[6900 – 12 000]
Total: 1.8 million [1.6 million – 1.9 million]
12

Western & Central Europe
1400[<1000 – 1800]
Middle East & North Africa40 000
[27 000 – 52 000]
Sub-Saharan Africa3.1 million
[2.8 million – 3.5 million]
Eastern Europe & Central Asia
17 000 [14 000 – 23 000]
South & South-East Asia160 000
[110 000 – 210 000]
Oceania4600
[3600 – 5800]
North America4500
[4000 – 5800]
Latin America42 000
[30 000 – 54 000]
East Asia16 000
[11 000 – 21 000]Caribbean
16 000[12 000 – 19 000]
Children (<15 years) estimated to be living with HIV | 2010
Total: 3.4 million [3.0 million – 3.8 million]
13

Western & Central Europe
<100[<200]
Middle East & North Africa6800
[4800 – 8800]
Sub-Saharan Africa350 000
[300 000 – 410 000]
Eastern Europe & Central Asia
2200 [1700 – 2900]
South & South-East Asia 20 000
[14 000 – 28 000]
Oceania<1000
[<500 – <1000]
North America<100[<200]
Latin America3500
[2100 – 5000]
East Asia2100
[<1000 – 3800]Caribbean
1200[<1000 – 1700]
Estimated number of children (<15 years) newly infected with HIV | 2010
Total: 390 000 [340 000 – 450 000]
14

Western & Central Europe
<100[<200]
Middle East & North Africa3900
[2700 – 5000]
Sub-Saharan Africa230 000
[200 000 – 260 000]
Eastern Europe & Central Asia
1200 [<1000 – 1800]
South & South-East Asia 14 000
[8300 – 20 000]
Oceania<500
[<500 – <500]
North America<100[<200]
Latin America2400
[1300 – 3500]
East Asia1100
[<1000 – 1700]Caribbean
1000[<1000 – 1300]
Estimated deaths in children (<15 years) from AIDS | 2010
Total: 250 000 [220 000 – 290 000]
15

Over 7000 new HIV infections a day in 2010
§ About 97% are in low and middle income countries
§ About 1000 are in children under 15 years of age
§ About 6000 are in adults aged 15 years and older, of whom:─ almost 48% are among women─ about 42% are among young people (15-24)
16

17

Control of AIDS
• Triple-‐drug therapy has slowed the pandemic in countries with money
18

But...• There is as yet no cure-‐ Can’t clear virus from an infected individual
• There is no vaccine-‐ Can’t block primary infecBon
• Can’t stop taking anBviral drugs-‐ Reservoirs: latently infected hematopoieBc progenitor cells
(TWiV 133: The HIV hideout)
• Drug resistant viruses appear
• Drugs are expensive
• AIDS is becoming a Third World disease-‐ Spreading unabated in sub-‐Saharan Africa
19

HIV-‐2
• Restricted primarily to populaBons in West Africa
• Less virulent, transmissible than HIV-‐1
• HIV-‐2 membrane proteins share homology with those of SIV
• Humans infected with HIV-‐2 have anBbodies that cross-‐react with SIV
• SIV causes AIDS-‐like disease in macaques, but is not pathogenic in some species like African green monkeys
20

Primate len0viruses and the origin of HIV
21

Origin of HIV
• Current thinking, based on sequence analysis, is that HIV-‐1 and HIV-‐2 came from separate colonizaBon events of simian lenBviruses in humans
22

HIV-‐1 clades or subtypes
• Four groups (four separate colonizaBons of humans with SIV)
• Group M: at least 9 disBnct clades
• Assignment based on sequence of ENV and GAG genes
23

•Clades A, C, D, E predominate in areas with highest rates of infec9on
-‐Most clades are found in central Africa
•Elsewhere, one or two clades predominate
-‐Clade B predominates in the US and Western Europe
•HIV spread changing with 9me
-‐Spread of the C-‐clade in Africa
24

Sequence comparisons provide insight on HIV origins
• Chimpanzee (SIV CPZ) and Mandrill (SIV MND) viruses: closely related to HIV-‐1
• Sooty mangabey virus group (SIV SM): closely related to HIV-‐2
25
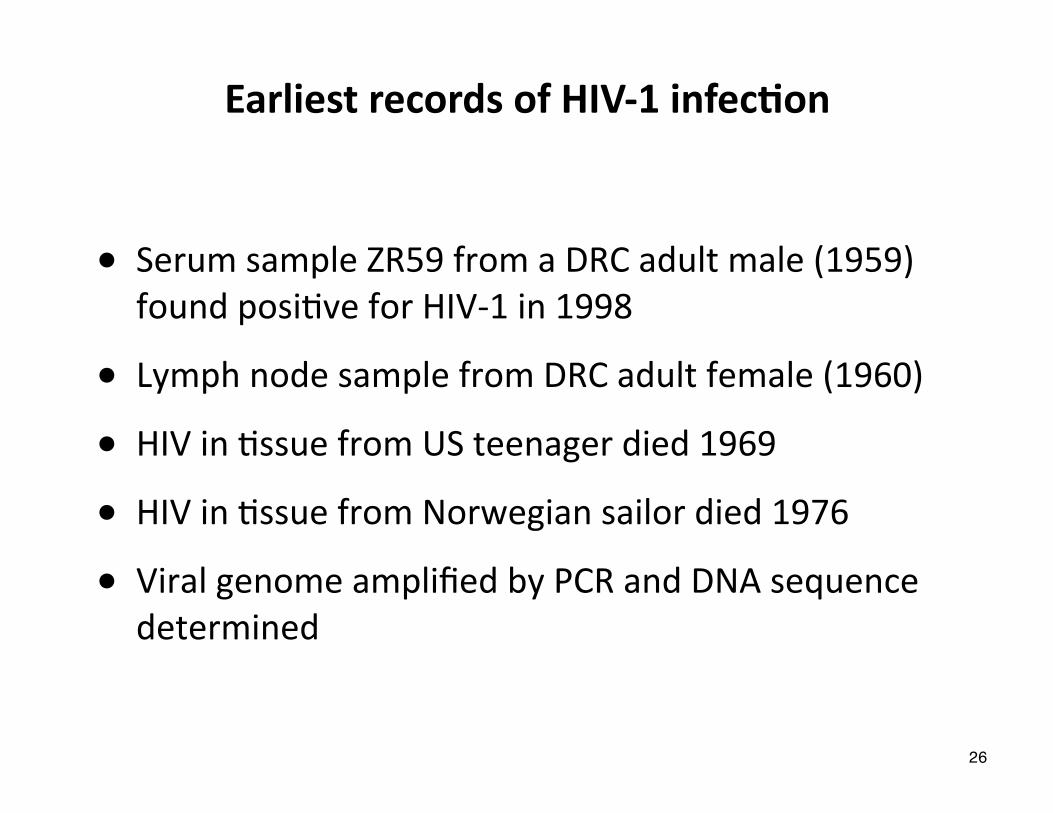
Earliest records of HIV-‐1 infec0on
• Serum sample ZR59 from a DRC adult male (1959) found posiBve for HIV-‐1 in 1998
• Lymph node sample from DRC adult female (1960)
• HIV in Bssue from US teenager died 1969
• HIV in Bssue from Norwegian sailor died 1976
• Viral genome amplified by PCR and DNA sequence determined
26

When did SIV infect humans?
• 1931 (+/-‐ 15 yr)
• 1884 -‐ 1924, comparing 1959 and 1960 sequences
• Suggested that Kinshasa was epicenter, early spread concurrent with development of colonial ciBes
• Hunter, colonialism, contaminated needle theories
27

Transmission
• HIV is not a parBcularly infecBous virus, not contagious like measles virus
• Not spread by respiratory, alimentary, or vector routes
28

29

30

Transmission
• HIV-‐1 infecBvity reduced by air drying (99%/24 hr)
• By heaBng (56°C/30 min)
• By 10% bleach or 70% alcohol
• By pH extremes (<6 or >10)
31
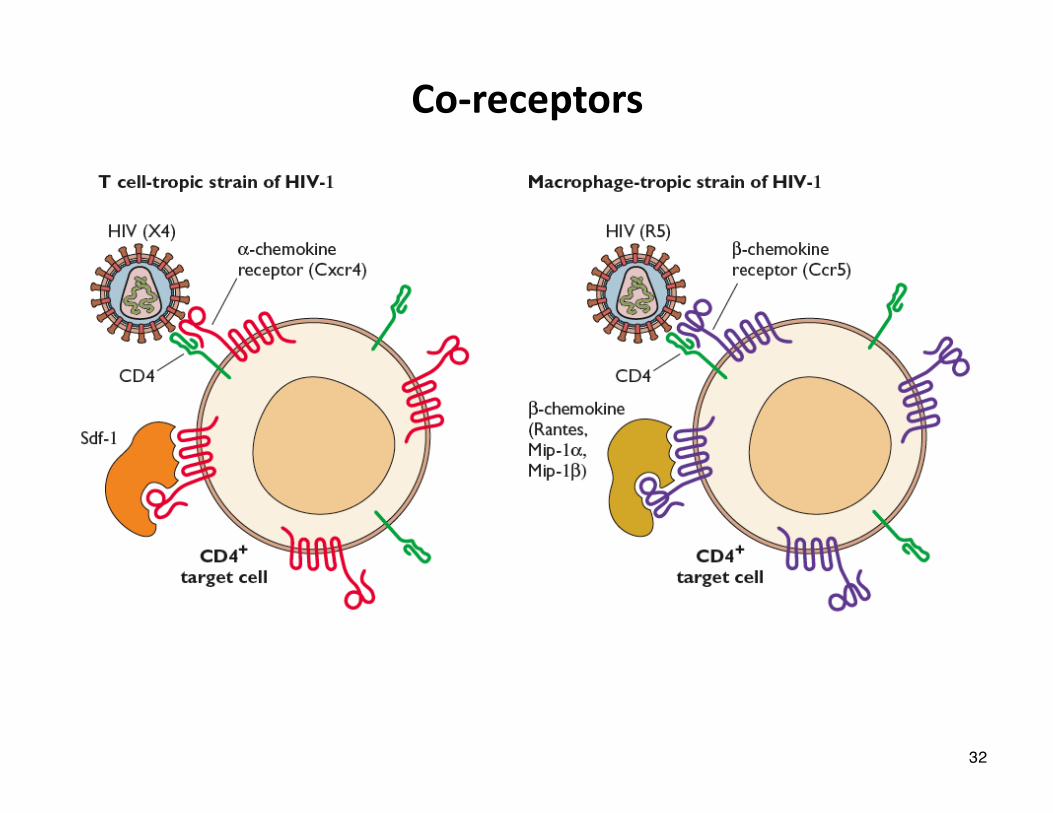
Co-‐receptors
32

Primary HIV Infec0on
• Virus-‐dendriBc cell interacBon
- InfecBon is typically with CCR5 (M-‐tropic) strains
- Importance of DC-‐SIGN (dendriBc cell-‐specific, Icam-‐3 grabbind nonintegrin)
• Delivery of virus to lymph nodes
• AcBve replicaBon in lymphoid Bssue
• High levels of viremia and disseminaBon
• DownregulaBon of virus replicaBon by immune response
• Viral set point reached aker ~6 months33

Primary HIV Infec0on: Clinical Characteris0cs
• 50-‐90% of infecBons are symptomaBc
• Symptoms generally occur 5-‐30 days aker exposure
• Symptoms and signs
- Fever, faBgue, malaise, arthralgias, headache, nausea, vomiBng, diarrhea
- Adenopathy, pharyngiBs, rash, weight loss, mucocutaneous ulceraBons, asepBc meningiBs
- Leukopenia, thrombocytopenia, elevated liver enzymes
• Median duraBon of symptoms: 14 days
34

GI associated lymphoid 0ssue following acute infec0on
Absence of lymphoid cell aggregates in terminal Ileum
35

36

Established HIV Infec0on
• AcBve viral replicaBon throughout course of disease
• Major reservoirs of infecBon exist outside of blood
-‐ LymphoreBcular Bssues (GastrointesBnal tract -‐ GALT)
-‐ Central nervous system
-‐ Genital tract
• At least 10 x 109 virions produced and destroyed each day
• T1/2 of HIV in plasma is <6 h and may be as short as 30 min
37

mulBpotent hematopoieBc progenitor cells -‐ latent reservoir38

years
yearsyearsmonths
months
?
months
Primary HIVInfec0on AIDS
Viral Rep
lica0
on
The Variable Course of HIV-‐1 Infec>on
Typical Progressor Rapid Progressor
CD4 Level
Clinical Latency
A Viral Rep
lica0
on
CD4 Level
Primary HIVInfec0on AIDS
BViral Rep
lica0
onCD
4 Level
Primary HIVInfec0on Clinical Latency
C
Nonprogressor
39

Immune cell dysfunc0on in AIDS
40

AIDS• <200 CD4+ T cells/ml
• Protozoal: Pneumocys@s, Toxoplasma, Isospora, Cryptosporidium, microsporidia
• Bacterial: Mycobacterium, Treponema
• Fungal: Candida, Cryptococcus, Histoplasma
• Viral: CMV, HSV
• Malignancies: EBV lymphoma, Kaposi’s sarcoma, anogenital carcinoma
• Neurological symptoms: asepBc meningiBs, myelopathies, neuropathies, AIDS demenBa complex
41

Neurological symptoms
42

HIV and cancer
• HIV-‐1 infecBon leads to increase incidence of malignancy: 40% of infected individuals
• An indirect effect of dysregulaBon of the immune system
-‐ Absence of proper immune surveillance
-‐ High levels of cytokines leads to inappropriate cell proliferaBon, replicaBon of oncogenic viruses, angiogenesis
43

Kaposi’s sarcoma
• Described 1872 by Hungarian physician
• Pre-‐AIDS: mainly in older Mediterranean men
• Occurs in 20% of HIV-‐1 infected homosexual men, 2% of HIV-‐1 infected women, transfusion recipients
• InfecBon with human herpesvirus 8 is necessary for development of KS
44

B-‐cell lymphomas
• 60-‐100 Bmes more common in AIDS paBents than general populaBon
• Tumors in lymph nodes, intesBne, CNS, liver
• Oken associated with infecBon by HHV-‐8 or Epstein-‐Barr virus
45

46

Is an HIV-‐1 vaccine possible?
Viral Load
AnBviral Immunity
How does HIV-‐1 persist despite effecBve anB-‐viral immunity?
How does it eventually outstrip immune control?
47

HIV-‐1 escape from neutralizing an0body
48

Broadly neutralizing an0bodies
• Have been idenBfied in some HIV-‐1 infected individuals
• Neutralize broadly across clades
• Recognize conserved epitopes on Env glycoprotein
49

CD8+ CTL are important for control of HIV-‐1
• KineBcs of early CTL response peak as early viremia falls
• Adverse effect of removing CD8+ T cells in SIV-‐infected macaques
50

Elite HIV Controllers
• Individuals who maintain normal CD4 counts and undetectable viral loads (<50 copies HIV RNA/ml of plasma) for >10 years in the absence of anBretroviral therapy
-‐ EsBmated at 1/300 infected persons
• Associated with favorable HLA types (esp HLA B57 and B27) and T-‐cell responses (CD4 and CD8) to Gag
• Persistent viremia (1-‐30 copies of RNA/ml) demonstrable
• Not associated with aXenuated viruses
hXp://www.twiv.tv/2010/05/16/twiv-‐82-‐immunology-‐in-‐silico/51