Embed Size (px)
Citation preview

TherapyAN OVERVIEW OF TREATMENTWhy Do People Seek Therapy?Who Provides Psychotherapeutic Services?The Therapeutic Relationship
MEASURING SUCCESS IN PSYCHOTHERAPYObjectifying and Quantifying ChangeWould Change Occur Anyway?Can Therapy Be Harmful?
WHAT THERAPEUTIC APPROACHESSHOULD BE USED?Evidence-Based TreatmentsMedication or Psychotherapy?Combined Treatments
PHARMACOLOGICAL APPROACHESTO TREATMENTAntipsychotic DrugsAntidepressant Drugs
Antianxiety DrugsLithium and Other Mood-Stabilizing DrugsElectroconvulsive TherapyNeurosurgery
PSYCHOLOGICAL APPROACHES TO TREATMENTBehavior TherapyCognitive and Cognitive-Behavioral TherapyHumap:stic-Experiential TherapiesPsychodynamic TherapiesMarital and Family TherapyEclecticism and Integration
PSYCHOTHERAPY AND SOCIETYSocial Values and PsychotherapyPsychotherapy and Cultural Diversity
UNRESOLVED ISSUES:Is There Bias in the Reporting of Drug Trials?

ost of ~s hav.e experienced a time or situation when we were dramatically helpedby talking things over with a relative or friend. Most therapists, like all good lis-teners, rely on receptiveness, warmth, and empathy and take a nonjudgmentalapproach to the problems their clients present.
But there is more to therapy than just giving someone an opportunity to talk.Therapists also introduce into the relationship psychological interventions thatare designed to promote new understandings, behaviors, or both, on the client'spart. The fact that these interventions are deliberately planned and systematicallyguided by certain theoretical preconceptions is what distinguishes professionaltherapy from more informal helping relationships.
AN OVERVIEW OFTREATMENTThe belief that people with psychological problems canchange-can learn more adaptive ways of perceiving, eval-uating, and behaving-is the conviction underlying allpsychotherapy. Achieving these changes is by no meanseasy. Sometimes a person's view of the world and her or hisself-concept are distorted from pathological early relation-ships reinforced by years of negative life experiences. Inother instances, environmental factors such as an unsatis-fying job, an unhappy marriage, or financial stresses mustbe a focus of attention in addition to psychotherapy.Because change can be hard, people sometimes find iteasier to bear their present problems than to challengethemselves to chart a different life course. Therapy alsotakes time. Even a highly skilled and experienced therapistcannot undo a person's entire past history and prepare himor her to cope adequately with difficult life situations withina short time. Therapy offers no magical transformations.Nevertheless, it holds promise even for the most severemental disorders. Moreover, contrary to common opinion,psychotherapy can be less expensive in the long run thanalternative modes of intervention (Gabbard et al., 1997).
It has been estimated that several hundred therapeuticapproaches exist, ranging from psychoanalysis to Zenmeditation. However, the era of managed care hasprompted new and increasingly stringent demands thatthe efficacy of treatments be empirically demonstrated.This chapter will explore some of the most widely acceptedpharmacological and psychological treatment approachesin use today. Although we recognize that different groupsof mental health professionals often have their own prefer-ences with respect to the use of the terms client and patient,in this chapter we use the terms interchangeably.
Why Do People Seek Therapy?STRESSFUL CURRENT LIFE CIRCUMSTANCES Peoplewho seek therapy vary widely in their problems and in
their motivations to solve them. Perhaps the most obviouscandidates for psychological treatment are people experi-encing sudden and highly stressful situations such as adivorce or unemployment-people who feel so over-whelmed by a crisis that they cannot manage on their own.These people often feel quite vulnerable and tend to beopen to psychological treatment because they are moti-vated to alter their present intolerable mental states. Insuch situations, clients may gain considerably, in a brieftime, from the perspective provided by their therapist.
PEOPLE WITH LONG-STANDING PROBLEMS Otherpeople entering therapy have experienced long-term psy-chological distress and have lengthy histories of maladjust-ment. They may have had interpersonal problems such asan inability to be comfortable with intimacy, or they mayhave felt susceptible to low moods that are difficult forthem to shake. Chronic unhappiness and the inability tofeel confident and secure may finally prompt them to seekoutside help. These people seek psychological assistanceout of dissatisfaction and despair. They may enter treat-ment with a high degree of motivation, but as therapy pro-ceeds, their persistent patterns of maladaptive behaviormay generate resistance with which a therapist must con-tend. For example, a narcissistic client who expects to bepraised by his or her therapist may become disenchantedand hostile when such "strokes" are not forthcoming.
RELUCTANT CLIENTS Some people enter therapy by amore indirect route. Perhaps they had consulted a physi-cian for their headaches or stomach pains, only to be toldthat nothing was physically wrong with them. After theyare referred to a therapist, they may at first resist the ideathat their physical symptoms are emotionally based. Moti-vation to enter treatment differs widely among psy-chotherapy clients. Reluctant clients may come from manysources-for example, an alcoholic whose spouse threat-ens "either therapy or divorce," or a suspected felon whoseattorney advises that things will go better at trial if it can beannounced that the suspect has "entered therapy." In gen-eral, males are more reluctant to enter therapy than

17.1
Compared to women, men are much more likelyto resist seeking treatment from health profes-sionals when they are experiencing difficulties.For example, they visit their primary physi-cians less frequently; they also visit mental
health specialists less often, and they are less likely toenter psychotherapy or counseling than women are. In thecase of depression, far more men than women say thatthey would never consider seeing a therapist; when menare depressed they are even reluctant to seek informalhelp from their friends. Moreover, when men do seek pro-fessional help, they tend to ask fewer questions thanwomen do (see Addis & Mahalik, 2003).
Why is the average man, regardless of age, socialbackground, and ethnicity, so much more reluctant thanthe average woman to utilize health services? One answeris that men are less able than women to recognize andlabel feelings of distress and to identify these feelings asemotional problems. In addition, men who subscribe tomasculine stereotypes emphasizing self-reliance and lackof emotionality also tend to experience more gender-roleconflict when they consider traditional counseling, with itsfocus on emotions and emotional disclosure. For a manwho prides himself on being emotionally stoic, seeking
females are (see The World Around Us 17.1). A substantialnumber of angry parents bring their children to therapistswith demands that their child's "uncontrollable behavior,"which they view as independent of the family context, be"fixed." These parents may be surprised and reluctant torecognize their own role in shaping their child's behaviorpatterns.
PEOPLE WHO SEEK PERSONAL GROWTH A finalgroup of people who enter therapy have problems thatwould be considered relatively normal. That is, they appearto have achieved success, have financial stability, have gen-erally accepting and loving families, and have accom-plished many of their life goals. They enter therapy not outof personal despair or impossible interpersonal involve-ments, but out of a sense that they have not lived up totheir own expectations and realized their own potential.These people, partly because their problems are moremanageable than the problems of others, may make sub-stantial gains in personal growth.
Psychotherapy, however, is not just for people whohave clearly defined problems, high levels of motivation,and an ability to gain ready insight into their behavior.Psychotherapeutic interventions have been applied to a
Why Are Men So Reluctant toEnter Therapy?
help for a problem like depression may present a majorthreat to his self-esteem. Seeking help also requires givingup some control. and may run counter to the ideology that" a real man helps himself."
How can men be encouraged to seek help when theyhave difficulties? One basic problem is that the kinds of ser-vices that are available may not be the kinds of servicesthat men who endorse traditional masculine roles can read-ily accept. In other words, for some men, there may be amismatch between what is available and what they can psy-chologically tolerate. Part of the solution may be to developtreatment approaches that are based on theories of howmen are socialized and that provide a better fit for men whoare constrained by gender-role expectations. Another strat-egy is to use more creative approaches to encourage mento seek help and support. For example, television commer-cials for erectile dysfunction use professional basketballplayers and football coaches to encourage men with similarproblems to "step up to the plate" and talk to their doctors.Making men more aware of other "masculine men" whohave been "man enough" to go for help when they neededit may be an important step toward educating those whoseadherence to masculine gender roles makes it difficult forthem to acknowledge and seek help for their problems.
wide variety of chronic problems. Even a severely dis-turbed, psychotic client may profit from a therapeuticrelationship that takes into account his or her level of func-tioning and maintains therapeutic subgoals that are withinthe client's present capabilities (e.g., see Hogarty et al.,1997a, 1997b; Kendler, 1999b).
It should be clear from these brief descriptions thatthere is no "typical" client. Neither is there a "model" ther-apy. No currently used form of therapy is applicable to alltypes of clients, and all of the standard therapies can docu-ment some successes. Most authorities agree that clientvariables such as motivation to change and the severity ofsymptoms are exceedingly important to the outcome oftherapy (Clarkin & Levy, 2004). As we will see, the varioustherapies have relatively greater success when a therapisttakes the characteristics of a particular client into accountin determining treatment approaches.
Who ProvidesPsychotherapeutic Services?Members of many different professions have traditionallyprovided advice and counsel to individuals in emotionaldistress. Physicians, in addition to caring for their patients'

Many clients with psychological problems can be helped bytalking with a skilled, empathetic, and nonjudgmental therapist.
physical problems, often become trusted advisers in emo-tional matters as well. Many physicians are trained to rec-ognize psychological problems that are beyond theirexpertise and to refer patients to psychological specialistsor to psychiatrists.
Another professional group who deals extensivelywith emotional problems is the clergy. A minister, priest,or rabbi is frequently the first professional to encounter aperson experiencing an emotional crisis. Although someclergy are trained mental health counselors, most limittheir counseling to religious matters and spiritual sup-port and do not attempt to provide psychotherapy.Rather, like ~eneral-practice physicians, they are trainedto recognize problems that require professional manage-ment and to refer seriously disturbed people to mentalhealth specialists.
The three types of mental health professionals whomost often administer psychological treatment in mentalhealth settings are clinical psychologists, psychiatrists, andpsychiatric social workers. These professions were brieflydescribed in Chapter 1 (see The World Around Us 1.3). Inaddition to their providing psychotherapy, the medical
training and licensure qualifications of psychiatrists enablethem to prescribe psychoactive medications and also toadminister other forms of medical treatment such as elec-troconvulsive therapy. In some states, appropriately super-vised psychologists and other clinical specialists may nowprescribe medications if they have received additionaltraining. Although every mental health professional differsto some degree in his or her training and approach to treat-ment, generally, psychiatrists differ from psychologists intheir predilection for treating mental disorders with a bio-logical approach (i.e., medications), whereas psychologistsgenerally treat patients' psychopathology by examiningand in some cases changing their patients' behaviors andthought patterns.
In a clinic or hospital (as opposed to an individualpractice), a wide range of treatment approaches may beused. These range from the use of drugs, to individual orgroup psychotherapy, to home, school, or job visits aimedat modifying adverse conditions in a client's life-forexample, helping a teacher become more understandingand supportive of a child-client's needs. Often the latter isas important as treatment directed toward modifying theclient's personality, behavior, or both.
This willingness to use a variety of procedures isreflected in the frequent use of a team approach to assess-ment and treatment, particularly in group practice andinstitutional settings. This approach ideally involves thecoordinated efforts of medical, psychological, social work,and other mental health personnel working together as theneeds of each case warrant. Also of key importance is thecurrent practice of providing treatment facilities in thecommunity. Instead of considering maladjustment to bean individual's private misery, which in the past oftenrequired confinement in a distant mental hospital, thisapproach integrates family and community resources inthe total treatment approach.
The Therapeutic RelationshipThe therapeutic relationship evolves out of what bothclient and therapist bring to the therapeutic situation. Theoutcome of psychotherapy normally depends on whetherthe client and therapist are successful in achieving a pro-ductive working alliance. The client's major contribution ishis or her motivation. Clients who are pessimistic abouttheir chances of recovery or who are ambivalent aboutdealing with their problems and symptoms respond lesswell to treatment (e.g., Mussell et aI., 2000).
THE THERAPEUTIC ALLIANCE The establishment of aneffective "working alliance" between client and therapist isseen by most investigators and practitioners as essential topsychotherapeutic gain. Our experiences as therapistsaffirm this basic observation, as does the research litera-ture. In a very real sense, the relationship with the therapistis therapeutic in its own right.

There is much evidence that therapists' personal char-acteristics help determine therapeutic outcome (e.g., seeBeutler et al., 2004; Blatt et al., 1996; Moyers et al., 2005).How well clients do in treatment is related to the strength ofthe alliance they have with their therapists (Barber et al.,2000; Kazdin et al., 2005; Martin et al., 2000). However, peo-ple who have a lot of problems often have very troubledinterpersonal relationships. An important skill for any ther-apist therefore is the ability to foster good relationships withclients who may present some challenges in this regard.
Other factors such as the level of expertise and experi-ence of the therapist also appear to be important, althoughthere is considerable variability across studies (e.g., Beutleret al., 2004; Huppert et al., 2001; Lambert & Ogles, 2004)and more research is warranted. Expert therapists havebeen shown to be better than either experienced or novicetherapists in such skills as the ability to provide a clear,coherent, and succinct account of a patient's problems(that is, to make a case formulation) and to develop anappropriate treatment plan (Eells et al., 2005).
Although definitions of the therapeutic alliance vary,its key elements are (1) a sense of working collaborativelyon the problem, (2) agreement between patient and ther-apist about the goals and tasks of therapy, and (3) an affec-tive bond between patient and therapist (see Constantinoet al., 2001; Martin et al., 2000). Clear communication isalso important. This is no doubt facilitated by the degreeof shared experience in the backgrounds of client andtherapist.
OTHER QUALITIES THAT ENHANCE THERAPY Asalready noted, the client's motivation to change is a crucialelement in determining the quality of the therapeuticalliance and hence the level of success likely to be achievedin the therapeutic effort. A wise therapist is appropriatelycautious about accepting an unmotivated client. Not allprospective clients, regardless of their need for treatment,are ready for the temporary discomfort that effective ther-apy may entail. As already described, many men, in partic-ular, have trouble accepting the conditions that therapymay impose such as the need to report their innermostfeelings. Even the motivation of self-referred clients maydissipate in the face of the painful confrontations with selfand past experiences that good therapy may require.
Almost as important as motivation is a client's expec-tation of receiving help. This expectancy is often sufficientin itself to bring about substantial improvement (Fisher &Greenberg, 1997; Lambert et al., 1986); this may be becausepatients who expect therapy to be effective engage more inthe process (Meyer et al., 2002). Just as a placebo oftenlessens pain for someone who believes it will do so, a personwho expects to be helped by therapy is likely to be helped,almost regardless of the particular methods used by a ther-apist. The downside of this fact is that if a therapy or thera-pist fails for whatever reason to inspire client confidence,the effectiveness of treatment is likely to be compromised.
To the art of therapy, a therapist brings a variety ofprofessional skills and methods intended to help peoplesee themselves and their situations more objectively-thatis, to gain a different perspective. Besides helping provide anew perspective, most therapy situations also offer a clienta safe setting in which he or she is encouraged to practicenew ways of feeling and acting, gradually developing boththe courage and the ability to take responsibility for actingin more effective and satisfying ways.
To bring about such changes, an effective psychother-apist must help the client give up old and dysfunctionalbehavior patterns and replace them with new, functionalones. Because clients will present varying challenges in thisregard, the therapist must be flexible enough to use a vari-ety of interactive styles. Effective therapy depends, at leastto some extent, on a good match between client and thera-pist. For this reason, a therapist's own personality is animportant factor in determining therapeutic outcomes,quite aside from his or her background and training or theparticular formal treatment plan adopted (Beutler et al.,2004; Blatt et al., 1996; Lambert, 1989). For example, atherapist who inadvertently but unfailingly takes charge infinding solutions for clients' problems will have consider-able difficulty helping people who are experiencing inhib-ited autonomy, as in dependent personality disorder.
In ReVIew~ What kinds of professionals provide help to
people in psychological distress? In whatkinds of settings does treatment occur?
~ What factors are important in determininghow well patients do in therapy?
MEASURING SUCCESS INPSYCHOTHERAPYEvaluating treatment success is not always as easy as itmight seem (Hill & Lambert, 2004). Attempts at estimat-ing clients' gains in therapy generally depend on one ormore of the following sources of information: (1) a thera-pist's impression of changes that have occurred, (2) aclient's reports of change, (3) reports from the client'sfamily or friends, (4) comparison of pretreatment andpost-treatment scores on personality tests or on otherinstruments designed to measure relevant facets of psy-chological functioning, and (5) measures of change inselected overt behaviors. Unfortunately, each of thesesources has its own limitations.

A therapist may not be the best judge of a client'sprogress, because any therapist is likely to be biased in favorof seeing himself or herself as competent and successful(after all, therapists are only human). In addition, the ther-apist typically has only a limited observational sample (theclient's in-session behavior) from which to make judg-ments of overall change. Furthermore, therapists can inflateimprovement averages by deliberately or subtly encourag-ing difficult clients to discontinue therapy. The problem ofhow to deal with early dropouts from treatment furthercomplicates many studies of therapy outcomes. Shouldthese patients be excluded from analyses of outcome? (Afterall, they have received little or none of the therapy beingevaluated.) Or should they be included and counted astreatment failures? These issues have been at the heart ofmuch debate and discussion.
Also, a client is not necessarily a reliable source ofinformation on therapeutic outcomes. Not only mayclients want to believe for various personal reasons thatthey are getting better, but in an attempt to please the ther-apist, they may report that they are being helped. In addi-tion, because therapy often requires a considerableinvestment of time, money, and sometimes emotional dis-tress, the idea that it has been useless is a dissonant one.Relatives of the client may also be inclined to "see" theimprovement they had hoped for, although they oftenseem to be more realistic than either the therapist or theclient in their evaluations of outcome.
Clinical ratings by an outside, independent observerare sometimes used in research on psychotherapy out-comes to evaluate the progress of a client; these ratingsmay be more objective than ratings by those directlyinvolved in the therapy. Another widely used objectivemeasure of client change is perfor-mance on various psychological tests. Aclient evaluated in this way takes a bat-tery of tests before and after therapy,and the differences in scores are assumedto reflect progress, or lack of progress, oroccasionally even deterioration. How-ever, some of the changes that suchtests show may be artifactual, as withregression to the mean (Speer, 1992),wherein very high (0r very low) scorestend on repeated measurement to drifttoward the average of their own distri-butions, yielding a false impression thatsome real change has been documented.Also, the particular tests selected arelikely to focus on the theoretical pre-dictions of the therapist or researcher.They are not necessarily valid predic-tors of the changes, if any, that the ther-apy actually induces, or of how theclient will behave in real life. And without follow-up
assessment, they provide little information on howenduring any change is likely to be.
Objectifying and Quantifying ChangeGeneralized terms such as recovery, marked improvement,and moderate improvement, which were often used inoutcome research in the past, are open to considerabledifferences in interpretation. Today the emphasis is onusing more quantitative methods of measuring change.For example, the Beck Depression Inventory (a self-report measure of depression severity) and the HamiltonRating Scale for Depression (a set of rating scales used byclinicians to measure the same thing) both yield sum-mary scores and have become almost standard in the pre-and post-therapy assessment of depression. Changes inpreselected and specifically denoted behaviors that are sys-tematically monitored, such as how many times a clientwith obsessions about contamination washes his hands,are often highly valid measures of outcome. Such tech-niques, including client self-monitoring, have been widelyand effectively used, mainly by behavior and cognitive-behavioral therapists. In research settings, one new devel-opment is using functional magnetic resonance imaging(fMRI) to examine brain activity before and after treat-ment (see Developments in Research 17.2).
Would Change Occur Anyway?What happens to disturbed people who do not obtain for-mal treatment? In view of the many ways in which peoplecan help each other, it is not surprising that improvementoften occurs without professional intervention. Relevant
here is the observation that treatmentoffered by therapists has not alwaysbeen clearly demonstrated to be supe-rior in outcome to nonprofessionallyadministered therapies (Christensen &Jacobson, 1994). Moreover, some formsof psychopathology such as depressiveepisodes or brief psychotic disordersometimes run a fairly short coursewith or without treatment. In otherinstances, disturbed people improveover time for reasons that are notapparent.
Even if many emotionally dis-turbed persons tend to improve overtime without psychotherapy, psy-chotherapy can often accelerateimprovement or bring about desiredbehavior change that might not other-wise occur. Most researchers todaywould agree that psychotherapy is more
effective than no treatment (see Shadish et al., 2000), and
This reflects the statistical tendencyfor extreme scores (e.g., very highor very low scores) on a givenmeasure to look less extreme at asecond assessment (as occurs ina repeated-measures design).Because of this statistical artifact,people whose scores are furthestaway from the group mean to beginwith (e.g., people who have thehighest anxiety scores or the lowestscores on self-esteem) will tend toscore closer to the group mean atthe second assessment, even if noreal clinical change has occurred.

7.2 Using Brain Activationto Measure TherapeuticChange
17unctional magnetic resonance imaging(fMRI) is an exciting technique that can beused to measure changes in activation in thehuman brain. When certain areas of thebrain are active and in use, it is believed that
they require more oxygen. By measuring the amount ofblood flow and oxygen in a given region of the brain, scien-tists can begin to learn what is happening in the humanmind.
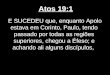
Research using neuroimaging to explore the changesthat occur in psychotherapy is still in its infancy. However,clinical scientists are using fMRI to measure clinical changein patient populations. Nakao and colleagues (2005) stud-ied ten outpatients with obsessive-compulsive disorder(OCO). At the start of the study, all the patients received abrain scan while they were engaged in a task that requiredthem to think about words (e.g., sweat, urine, feces) thattriggered their obsessions and compulsions. Patients werethen treated for 12 weeks either with the SSRI fluvoxamine(Luvox) or with behavior therapy. At the end of this treat-ment period, the brain scanning was repeated.
The results showed that, before treatment, certainareas of the brain thought to be involved in OeD (forexample, a brain region in the frontal lobe called the"orbitofrontal cortex") were activated during the symptom-provocation task. However, after therapy, these sameregions showed much less activation when the patients
Researchers are now using functional magnetic resonanceimaging {fMRt} to look at brain activity before and aftertreatment.
were challenged to think about the provocative triggerwords. Several methodological problems limit the conclu-sions that can be drawn from this study (e.g., small num-ber of subjects). However, research studies of this typehighlight the potential of neuroimaging in treatmentresearch and suggest that physiological changes mayaccompany the clinical gains that occur in psychotherapy.
Treatment changes the patterns of brain activation ofOCD patients during an experimental task. After receiving treatment,patients' brain activation patterns look similar to those of normal controls when they perform the same task. This suggeststhat OCDsymptoms might suppress activity in key brain areas involved in cognitive performance and that treatment mayhelp to correct this.Source: Nakao et aI., 2005.

indeed the pertinent evidence, widely cited throughoutthis entire text, confirms this strongly. The chances of anaverage client benefiting significantly from psychologicaltreatment are, overall, impressive (Lambert & Ogles,2004). Research suggests that about 50 percent of patientsshow clinically significant change after 21 therapy ses-sions. After 40 sessions, about 75 percent of patients haveimproved (Lambert et aI., 2001).
Progress in therapy is not always smooth and linear,however. Tang and his colleagues have shown that "suddengains" can occur between one therapy session and another(Tang & DeRubeis, 1999; Tang et aI., 2002). These clinicalleaps appear to be triggered by cognitive changes or by psy-chodynamic insights that patients experience in certaincritical sessions.
Can Therapy Be Harmful?The outcomes of psychotherapy are not invariably eitherneutral (no effect) or positive. Some clients are actuallyharmed by their encounters with psychotherapists (Lam-bert & Ogles, 2004; Mays & Franks, 1985; Strupp et al.,1977). According to one estimate, somewhere between 5and 10 percent of clients deteriorate during treatment(Lambert & Ogles, 2004). Patients suffering from border-line personality disorder and from obsessive-compulsivedisorder typically have higher rates of negative treatmentoutcomes than patients with other problems (Mohr, 1995).
Obvious ruptures of the therapeutic alliance-whatBinder and Strupp (1997) refer to as "negative process"(p. 121) in which client and therapist become embroiledin a mutually antagonistic and downwardly spiralingcourse-account for only a portion of the failures. Inother instances an idiosyncratic array of factors operatetogether (for example, the mismatch of therapist andclient personality characteristics) to produce deteriorat-ing outcomes. Our impression, supported by some evi-dence (see Beutler et aI., 2004), is that certain therapists,probably for reasons of personality, just do not do wellwith certain types of client problems. In light of theseintangible factors, it is ethically required of all therapists(1) to monitor their work with various types of clients todiscover any such deficiencies, and (2) to refer to othertherapists those clients with whom they may be ill-equipped to work (APA, 2002).
A special case of therapeutic harm is the problem ofsex between therapist and client, typically seduction of aclient (or former client) by a therapist. This is highlyunethical conduct. Given the frequently intense and inti-mate quality of therapeutic relationships, it is not sur-prising that sexual attraction arises. What is distressing isthe apparent frequency with which it is manifested inexploitive and unprofessional behavior on the part of ther-apists-all the more so in light of the fact that virtually allauthorities agree that such liaisons are nearly always
destructive of good client functioning in the long run(Pope et a1., 1993). A prospective client seeking therapyneeds to be sufficiently wary to determine that the thera-pist chosen is one of the large majority who are committedto high ethical and professional standards.
~ What approaches can be used to evaluatetreatment success?What are the advantagesand limitations of these approaches?
~ Do people who receive psychologicaltreatment always show a clinical benefit?
WHAT THERAPEUTICApPROACHES SHOULDBE USED?
When a pharmaceutical company develops a new drug, itmust obtain approval of the drug from the federal Foodand Drug Administration (FDA) before that drug can bemarketed. This involves, among other things, demon-strating through research on human subjects that thedrug has efficacy-that is, that it does what it is supposedto do in curing or relieving some target condition. Thesetests, using voluntary and informed patients as subjects,are called randomized clinical trials (RCTs) or, more sim-ply, efficacy trials. Although these trials may become quiteelaborate, the basic design is one of randomly assigning(e.g., by the flip of a coin) half the patients to the suppos-edly "active" drug and the other half to a visually identicalbut physiologically inactive placebo. Usually, neither thepatient nor the prescriber is informed which is to beadministered; that information is recorded in code by athird party. This double-blind procedure is an effort toensure that expectations on the part of the patient and pre-scriber play no role in the study. After a predeterminedtreatment interval, the code is broken and the active orplacebo status of all subjects is revealed. If subjects on theactive drug have improved in health significantly morethan subjects on the placebo, the investigator has evidenceof the drug's efficacy. Obviously, the same design could bemodified to compare the efficacy of two or more activedrugs, with the option of adding a placebo condition.Thousands of such studies are in progress daily across thecountry. They usually take place in academic medical set-

tings and many are financially supported by the pharma-ceutical industry.
Investigators of psychotherapy outcomes haveattempted to apply this research design to their own fieldof inquiry, with necessary modifications (see Chambless& Ollendick, 200l). A source of persistent frustration hasbeen the difficulty of concocting a credible placebo condi-tion. Most such research has thus adopted the strategy ofeither competitively comparing two or more purportedly"active" therapies or using a no-treatment ("wait list")control of the same duration as the active treatment.Another problem is that therapists, even those with thesame theoretical orientations, often differ markedly in themanner in which they deliver therapy. (In contrast, pills ofthe same chemical compound and dosage do not vary.) Totest a given therapy, it therefore becomes necessary todevelop a treatment manual to specify just how the ther-apy under examination will be delivered. Therapists in theresearch trial are then trained (and monitored) to makesure that their therapy sessions do not deviate significantlyfrom the procedures outlined in the manual (e.g., seeSanderson & Woody, 1995).
Efforts to "manualize" therapy represent one way thatresearchers have tried to minimize the variability inpatients' clinical outcomes that might result from charac-teristics of the therapist themselves (such as "personalcharisma"). Although manualized therapies originatedprincipally to standardize psychosocial treatments to fitthe randomized clinical trial (RCT) paradigm, some ther-apists recommend extending these manualized therapies'use to routine clinical practice after efficacy for particulardisorders has been established (e.g., see Wilson, 1998).Practicing clinicians, however, vary in their attitudestoward treatment manuals (Addis & Krasnow, 2000).
Efficacy or RCT studies of psychosocial treatments areincreasingly common. These time-limited studies typicallyfocus on patients who have a single DSM -IV-TR diagnosis(patients with comorbid diagnoses are sometimes excluded)and involve two or more treatment or control (e.g., wait list)conditions where at least one of the treatment conditions isa psychosocial one (another could be some biological ther-apy, such as a particular drug). Client -subjects are randomlyassigned to these conditions, whose effects, if any, are evalu-ated systematically with a common battery of assessmentinstruments, usually administered both before and aftertreatment.
Efficacy studies of the outcomes of specific psychoso-cial treatment procedures are considered the most rigor-ous type of evaluation we have for establishing that a giventherapy "works" for clients with a given DSM -IV-TR diag-nosis. Treatments that meet this standard are oftendescribed as "empirically validated" or "empirically sup-ported," and various lists of such treatments are now rou-tinely published and updated (e.g., Chambless et al., 1998;Nathan & Gorman, 1998; Roth & Fonagy, 1996).
Medication or Psychotherapy?Modern psychopharmacology has helped many individ-uals who would otherwise require hospitalization to func-tion in their family and community settings. It has also ledto the earlier discharge of those who do require hospital-ization and made restraints and locked wards largelyobsolete. In short, medication has led to a much morefavorable hospital climate for patients and staff alike.
Nevertheless, certain issues arise in the use of psy-chotropic drugs. Aside from possible unwanted sideeffects, there is the complexity of matching drug and drugdosage to the needs of the specific patient. It is also some-times necessary for patients to change medication in thecourse of treatment. In addition, the use of medications inisolation from other treatment methods may not be idealfor some disorders, because drugs themselves do not gen-erally cure disorders. As many investigators have pointedout, drugs tend to alleviate symptoms by inducing bio-chemical changes, not by helping the individual under-stand and change the personal or situational factors thatmay be creating or reinforcing maladaptive behaviors.Moreover, when drugs are discontinued, patients may be'at risk of relapsing. For many disorders, a variety ofevidence-based forms of psychotherapy may producemore long-lasting benefits than medications alone unlessthe medications are continued indefinitely.
On the other hand, for some disorders for which thereare known effective medications, the failure to incorporatemedication into a psychotherapeutic treatment programcan also lead to very serious problems. The World AroundUs 17.3 on page 608 well illustrates this point.
In the past, it was believed that medication and psychother-apy were incompatible approaches and so should not beadministered together (see Gabbard & Kay, 2001). How-ever, for many disorders the integration of medication andpsychotherapy is now common in clinical practice (Thase& Jindal, 2004). One survey suggests that 55 percent ofpatients receive both medications and psychotherapy fortheir problems (Pincus et al., 1999). This integrativeapproach is a good example of the biopsychosocial perspec-tive that best describes current thinking about mental dis-orders and that is reflected throughout this book.
Medications can be combined with a broad range ofpsychological approaches. In some cases, they can helppatients benefit more fully from psychotherapy and canserve to reduce noncompliant behavior in therapy. In othercases, psychotherapy may be directed at the family of thepatient, as, for example, in psychosocial interventions,which are designed to reduce high levels of expressed emo-tion and thus decrease patients' relapse rates, with the fami-lies of patients who have schizophrenia (see Chapter 14).

17.3
O sherhoff, a physician, was severelydepressed and functioning so ineffectivelythat his family hospitalized him at ChestnutLodge, which at the time was a largely psy-choanalytically oriented treatment facility.
Osherhoff received intensive psychoanalytic treatment fourtimes a week. He did not receive any medications.
After several months, Osherhoff's family became con-cerned over his lack of progress. He had lost 40 pounds, hewas experiencing severe sleep disturbance, and he hadsuch marked psychomotor agitation that his feet hadbecome swollen and blistered from pacing. The familysought a reevaluation of his case. The staff, in a case confer-ence, decided to continue the treatment program that hadbeen initiated. When Dr.Osherhoffs condition worsened
Overall, there is some cause to be optimistic about thecombined use of drugs and psychosocial approaches, espe-cially in the more severe disorders such as schizophreniaand bipolar disorder, although in these cases the psy-chotherapy often cannot start until a psychotic episode hasat least begun to subside. Such integrated approaches arealso appreciated and regarded as essential by the patientsthemselves. Here is the description of one patient withbipolar disorder, who also happens to be a prominent clin-ical scientist, highlighting her need for both medicationand psychotherapy:
Medications andPsychotherapy
At this point in my existence, I cannot imagine leading anormal life without both taking lithium and having hadthe benefits of psychotherapy. Lithium prevents myseductive but disastrous highs, diminishes my depres-sions, clears out the wool and webbing from my disor-dered thinking, slows me down, gentles me out, keepsme from ruining my career and relationships, keeps meout of a hospital, alive, and makes psychotherapy possi-ble. But ineffably, psychotherapy heals. It makes somesense of the confusion, reins in the terrifying thoughtsand feelings, returns some control and hope and possi-bility of learning from it all. Pills cannot, do not, ease oneback into reality; they only bring one back headlong,
further, his family had him discharged and admitted toanother facility,where he was treated with a combination ofphenothiazines and tricyclic antidepressants. He improvedmarkedly and was discharged in 3 months. Later he filed asuit claiming that Chestnut Lodge had not administered theproper treatment, drug therapy-an error that had causedhim to lose a year of employment in his medical practice.
Preliminary court arbitration indicated an initial awardof damages to Dr.Osherhoff, but the case was settled outof court before a final judgment was rendered. Anumber ofcomplicated issues were involved in this case, which isdescribed in Klerman (1990). However, it serves as animportant reminder that therapists may be liable for failingto provide medication to patients with certain disorders forwhich medications known to be effective are available.
careening, and faster than can be endured at times. Psy-chotherapy is a sanctuary; it is a battleground; it is aplace I have been psychotic, neurotic, elated, confused,and despairing beyond belief. But, always, it is where Ihave believed -or learned to believe-that Imight some-day be able to contend with all of this.
No pill can help me deal with the problem of notwanting to take pills; likewise, no amount of psycho-therapy alone can prevent my manias and depressions. Ineed both. It is an odd thing, owing life to pills, one's ownquirks and tenacities, and this unique, strange, and ulti-mately profound relationship called psychotherapy. (Fromthe autobiography of KayJamison, An Unquiet Mind, 1995,pp.88-89·)
Source: FromANUNQUIETMINDby KayRedfieldJamison,copyright© 1995 by KayRedfieldJamison. Used by permissionofAlfredA.Knopf,a divisionof RandomHouse, Inc.
In addition to combined treatments being wellreceived by patients, research suggests that there are clin-ical benefits to this approach, especially for patients withsevere disorders (see Gabbard & Kay, 2001). For example,Keller and colleagues (2000) compared the outcomes of519 depressed patients who were treated with an antide-pressant (nefazodone), with psychotherapy (cognitive-behavioral), or with a combination of both of thesetreatments. In the medication-alone condition, 55 per-cent of patients did well. In the psychotherapy-alonecondition, 52 percent of patients responded to treat-ment. However, patients for whom the two treatments

were combined did even better, with an overall positiveresponse rate of 85 percent. These findings echo theresults ofThase et al. (1997), who conducted a large-scaleanalysis of single and combined treatments for patientswith depression and found that the combination of med-ication and psychotherapy was particularly beneficial forpatients with more severe and recurrent depressions.Similar clinical advantages for combining cognitive-behavioral therapy (CBT) and medications have alsobeen reported in the treatment of panic disorder (Barlowet aI., 2000), although in this study the long-term bene-fits of CBT were somewhat reduced for patients in thecombined-treatment condition. Quite possibly, com-bined treatment is effective because medications andpsychotherapy may target different symptoms and workat different rates. As Hollon and Fawcett (1995) noteafter reviewing this literature, "Pharmacotherapy appearsto provide rapid, reliable relief from acute distress, andpsychotherapy appears to provide broad and enduringchange, with combined treatment retaining the specificbenefits of each" (p. 1232).
In ReVIew~ What are the advantages and drawbacks of
using a "manualized" therapy?~ What is the difference between an
effectiveness study and an efficacy study?~ What does it mean to describe a treatment as
"evidence-based"?~ Why is the integration of medication and
psychotherapy becoming increasinglycommon in clinical practice?
PHARMACOLOGICALApPROACHES TOTREATMENTThe field of psychopharmacology is characterized by rapidand exciting progress. Clinical breakthroughs are occur-ring on a regular basis, and there is now real hope forpatients previously considered to be beyond help. In thefollowing sections we discuss some of the major classes ofmedications that are now routinely used to help patientswith a variety of mental disorders, as well as some addi-tional treatment approaches (such as electroconvulsivetherapy) that are less widely used but highly effective, espe-cially for patients who fail to show a good clinical responseto other treatments.
These drugs are sometimes referred to as "psychoac-tive" (literally, "mind-altering") medications, indicatingthat their major effects are on the brain. As we examinethese medications, it is important to remember that peo-ple differ in how rapidly they metabolize drugs-that is,in how quickly their bodies break down the drugs onceingested. For example, many African-Americans metabo-lize antidepressant and antipsychotic medications moreslowly than whites. What this means is that African-Americans sometimes show a more rapid and greaterresponse to these medications but also experience moreside effects (see U.S. Department of Health and HumanServices, 2001, p. 67). Determining the correct dosage iscritical, because too little of a drug can be ineffective; onthe other hand, too much medication can cause toxicitythat may be life-threatening, depending on the individualand the medication concerned.
Antipsychotic DrugsAs their name suggests, antipsychotic drugs are used totreat psychotic disorders such as schizophrenia and psy-chotic mood disorders. You have already read about thesemedications in Chapter 14. The key therapeutic benefit ofanti psychotics derives from their ability to alleviate orreduce the intensity of delusions and hallucinations. Theydo this by blocking dopamine receptors.
Table 17.1 on page 610 lists some of the more com-monly used neuroleptic drugs as well as information abouttypical dose ranges and the half-life of each drug. The half-life is the time it takes for the level of active drug in thebody to be reduced by 50 percent (due to the drug beingmetabolized and excreted). Advantages of a long half-lifeinclude the need for less frequent dosing, less variation inthe concentration of the drug in the plasma, and less severewithdrawal. Disadvantages include the risk of the drugaccumulating in the body, as well as increased sedation andpsychomotor impairment during the day.
Studies have found that approximately 60 percent ofpatients with schizophrenia who are treated with tradi-tional antipsychotic medication have a resolution of theirpositive symptoms within 6 weeks, compared to onlyabout 20 percent of those treated with placebo (see Brad-ford et aI., 2002). These drugs are also useful in treatingother disorders with psychotic symptoms such as mania,psychotic depression, and schizoaffective disorder, andthey are occasionally used to treat transient psychoticsymptoms when these occur in people with borderlinepersonality disorder and schizotypal personality disorder(Koenigsberg et aI., 2002). Finally, they are useful in treat-ing Tourette's syndrome and delirium (see Chapter 15)and are sometimes used in the treatment of the delusions,hallucinations, paranoia, and agitation that can occur withAlzheimer's disease (Gitlin, 1996).
Antipsychotic medications are usually administereddaily by mouth. However, some patients, particularly those

Drug ClassSecondGeneration(Atypical)
FirstGeneration(Conventional)
Commonly Prescribed Anlip~ycholic;Drug~-' " , ' '
Generic Name Trade Name Dose Range (mg) Half-Life (hrs)clozapine Clozaril 300-900 5-16risperidone Risperdal 1-8 20-24olanzapine Zyprexa 5-20 21-54quetiapine Seroquel 100-750 6-7ziprasidone Geodon 80-160 6.6aripiprazole Abilify 15-30 75chlorpromazine Thorazine 75-900 16-30perphenazine Trilafon 12-64 9-21molindone Moban 50-200 6.5thiothixene Navane 15-60 34trifluroperazine Stelazine 6-40 13haloperidol Haldol 2-100 12-36fluphenazine Prolixin 2-20 13-58
with chronic schizophrenia, are often not able to remem-ber to take their medications each day. In such cases, depotneuroleptics can be very helpful. These are neurolepticsthat can be administered in a long-acting, injectable form.The clinical benefits of one injection can last for up to 4weeks, which makes depot neuroleptics very valuable forpatients, like the one in the following case, who need med-ication but are unwilling or unable to take drugs every day.
He Forgets to Take HisMedications
A45-year-old male patient with chronic schizophrenia hasa history of recurrent delusions of persecution and ideasof reference as well as auditory persecutory hallucina-tions. He has a history of 19 inpatient psychiatric admis-sions. He will generally keep outpatient appointments,but he forgets to take his antipsychotic medications andusually relapses within 2 weeks of discontinuing them.While in the hospital, he has an alleviation of his psychoticsymptoms when he is given 20 mg per day of fluphenazinehydrochloride (Prolixin)orally. Because he responds wellto medication but is not compliant, his psychiatristdecides to treat him with a biweekly injection of a depotneuroleptic. (Adapted from Janowsky et aI., 1987.)
One very problematic side effect that can result fromtreatment with conventional antipsychotic medicationssuch as chlorpromazine is tardive dyskinesia (see Chapter14). Tardive (from tardy) dyskinesia is a movement abnor-mality that is a delayed result of taking antipsychotic med-
ications. The problem of tardive dyskinesia is well illus-trated in the following case. Because movement-relatedside effects are much less common with atypical antipsy-chotic medications such as clozapine (Clozaril) and olan-zapine (Zyprexa), these medications are now generallypreferred in the clinical management of schizophrenia.Clozapine also seems to be especially beneficial for psy-chotic patients at high risk of suicide (Meltzer et al., 2003).
Suffering from TardiveDyskinesia
A62-year-old woman with chronic schizophrenia who hasbeen a 2o-year inpatient in a state mental hospital isnoted to manifest bizarre repetitive movements of hermouth, tongue, hands, and feet. Her mouth involuntarilygrimaces, and her tongue intermittently protrudes. Herfingers repetitively flex and she is often noted to rockback and forth. Her hand and feet movements appearchoreiform (pronounced chor-ray-if-form; means "jerkyand flowing"). The patient has a history of paranoid delu-sions and hallucinations, beginning 25 years previously.She has not manifested these symptoms of schizophre-nia for 6 years. She has been treated with a progressionof antipsychotic drugs in moderate doses for the past 18years. (Adapted from Janowsky et aI., 1987.)
In addition to having a lower risk of producingmovement-related side effects, atypical antipsychoticssuch as clozapine (Clozaril), risperidone (Risperdal), olan-zapine (Zyprexa), quetiapine (Seroquel), ziprasidone

(Geodon), and the more recently introduced aripiprazole(Abilify) have other treatment advantages. Specifically,there is evidence that atypical antipsychotics may effec-tively treat both the positive and the negative symptoms ofschizophrenia, whereas the older, traditional neurolepticsworked mainly on the positive symptoms. This representsa major treatment advance. However, even the atypicalneuroleptics have side effects, weight gain being very com-mon and diabetes also being a clinical concern (Sernyaket aI., 2002).You may recall that a more serious side effectof clozapine is a potentially life-threatening drop in whiteblood cells called "agranulocytosis:' which occurs in 0.5 to2 percent of patients (Stahl, 2002). Accordingly, patientsmust have their blood tested every week for the first 6months of treatment and then every 2 weeks thereafterfor as long as they are on the medication. Because of this,clozapine is best regarded as a medication to consider afterother medications (e.g., some of the other atypical anti-psychotic medications) have proved ineffective. Currentthinking is that the atypical antipsychotics described above(with the exception of clozapine) are the first-choice treat-ments for psychosis and that clozapine and conventional
antipsychotics (e.g., Haldol) are best considered as second-line therapies.
Antidepressant DrugsSELECTIVE SEROTONIN RE-UPTAKE INHIBITORS(SSRIS) As is the case for antipsychotic medications, thedrugs that were discovered first (so-called "classical antide-pressants" such as monoamine oxidase inhibitors and tri-cyclic antidepressants) have now been replaced in routineclinical practice by "second-generation" treatments such asthe SSRIs. In 1988 fluoxetine (Prozac) became the firstSSRI to be released in the United States. It is now the mostwidely prescribed antidepressant in the world (Sadock &Sadock, 2003). Its pharmacological cousins include sertra-line (Zoloft) and paroxetine (Paxil). Recent additions tothe SSRI family are fluvoxamine (Luvox), which is used inthe treatment of obsessive-compulsive disorder; citalo-pram (Celexa), which was introduced to the U.S. market in1998; and escitalopram (Lexapro), which became availablein 2002. Table 17.2lists some of the most widely used anti-depressant medications.
•• '~.' .,'-.T·Commonly Prescnbed Antidepressant Drugs ',,::~'"
~ t-~ .•~~~
Drug ClassSSRI
Generic Name Trade Name Dose Range (mg) Half-life (hrs)fluoxetine Prozac 10-80 4-6 dayssertraline Zoloft 50-200 26paroxetine Paxil 10-60 21fluvoxamine Luvox 50-300 15citalopram Celexa 10-60 33escitalopram Lexapro 10-20 27-32venlafaxine Effexor 75-375 3-13reboxetine Vestra 8-20 13amitriptyline Elavil 75-300 10-46clomipramine Anafranil 75-300 17-37desipramine Norpramin 75-300 12-76doxepin Sinequan 75-300 8-36Imlpramme Tofranil 75-300 4-34nortriptyline Aventyl 40-200 13-88trimipramine Surmontil 75-300 7-30phenelzine Nardil 45-90 1.5-4tranylcypromine Parnate 20-60 2.4isocarboxazid Marplan 30-50 N/A
nefazodone Serzone 100-600 2-5trazodone Desyrel 150-600 4-9mirtazapine Remeron 15-60 20-40bupropion Wellbutrin 225-450 10-14

SSRIs are chemically unrelated to the older tricyclic:mtidepressants and to the monoamine oxidase inhibitors(see Chapter 7). However, most antidepressants work byincreasing the availability of serotonin, norepinephrine,
ROOTS
InStyle
The actress Brooke Shields is one of many public figures whohave been open with the public about their experiences withdepression.
Normalmood
or both. As their name implies, the SSRIs serve to inhibitthe reuptake of the neurotransmitter serotonin followingits release into the synapse. Unlike the tricyclics (whichinhibit the reuptake of both serotonin and norepineph-rine), the SSRIs selectively inhibit the reuptake of sero-tonin. They have become the preferred antidepressantdrugs because they are thought to be relatively "safe":They are easier to use, have fewer side effects, and are gen-erally not found to be fatal in overdose as the tricyclics canbe. However, it should be noted that they are generally notconsidered more effective than the classic tricyclic antide-pressants-they are simply more acceptable and bettertolerated by many patients. In many cases, they are nowbeing used by people who are not clinically depressed butjust want a "pharmacological lift" (see The World AroundUs 17.4).
Another widely used antidepressant in this drug fam-ily is venlafaxine (Effexor). This medication blocks reup-take of both norepinephrine and serotonin and is part of anew category of medications called "SNRIs" (serotoninand norepinephrine reuptake inhibitors; see Stahl, 2000).Its side effect profile resembles that of the SSRIs, and it isrelatively safe in overdose. This drug seems to help a signif-icant number of patients who have not responded well toother antidepressants, and it appears more effective thanthe SSRIs in the treatment of severe major depression(Thase, Entsuah, & Rudolph, 2001). Other SNRI drugs arecurrently in development and are expected to become clin-ically available in the near future.
Clinical trials with the SSRIs indicate that patientstend to improve after about 3 to 5 weeks of treatment.Patients who show at least a 50 percent improvement intheir symptoms are considered to have had a positiveresponse to treatment (see Figure 17.1). However,although considerably better, such patients are not fullywell. When treatment removes all of a patient's symptoms,patients are considered to be in a period of remission (seeFigure 17.2). If this remission is sustained for 6 to 12
When treatment of depressionresults in at least 50 percentimprovement in symptoms, it iscalled a response. Such patientsare better, but not well.
Source: From Essential Psychopharma-cology: Neuroscientific Basis andPractical Applications, 2E, p. 143, byStephen M. Stahl, copyright © Cam-bridge University Press, 2000.
Reprinted with the permission ofCambridge University Press.

17.4The drug Prozac and others that are pharmaco-
logically similar to it (such as Paxil and Zoloft)are now among the drugs most prescribed byphysicians. Originally recommended for thetreatment of relatively severe mood disorders,
they are now widely prescribed by many physicians, eventhose who are not psychiatrists, to ease patients' com-plaints of just feeling unhappy. In this respect they havecome to occupy a role not unlike that of the benzodi-azepines (antianxiety agents such as Valium) during the1970S and 1980s. The pharmacological message appears tobe that many people feel "better" when they have moreserotonin available in the neuronal synapses of their brains.
What is the nature of this "feeling better"? Psychia-trist Peter Kramer (1993), in his popular book Listening toProzac, argues that Prozac does more than amelioratedepressive states; in many instances it transforms person-ality, usually in a very positive, self-esteem-enhancingway. Kramer describes cases in which people claim to befunctioning far better than they were before becomingdepressed -literally "better than well" -or to have dis-covered, while on the drug, a "true" self different from and
months or more, the patient is considered to have recov-ered. In other words, he or she is fully well again.
Side effects of the SSRIs include nausea, diarrhea, ner-vousness, insomnia, and sexual problems such as dimin-ished sexual interest and difficulty with orgasm (Gitlin,1996; Nemeroff & Schatzberg, 2002). Although SSRIs help
Normalmood I
IIIIIIIIIIIIIIIIIII
6-12 weeks I
Time
Continuation4-9 months
more satisfying than their previous self. In light of theseeffects on subjective well-being, patients are often under-standably reluctant to stop taking the drug. That aspect,too, is reminiscent of the serious problems the overuse ofbenzodiazepines eventually caused.
Kramer suggests that the person taking Prozac experi-ences a diminished sensitivity to disapproval, criticism, andrejection by others. Obviously, such effects would be of con-siderable benefit to many people, not only people who sufferfrom major depression. Kramer addresses forthrightly thedisturbing questions raised by the availability of a prescrip-tion drug that seems not only to ameliorate disorder butalso, for many individuals, to alter their personalities, mostlyin ways they find pleasing. Moreover, Kramer is undoubtedlycorrect when he says that Prozac is only among the first of alarge number of "legitimate" drugs with comparable person-ality-altering properties that willeventually become avail-able. Willthese drugs be given only to people who reallyneed them? Orare we on the verge of entering an era of"cosmetic psychopharmacology," where people may evenget to choose major aspects of their personalities, just assome now choose the shapes of their noses?
many people, as the following case study illustrates, somepeople have side effects that are so extreme that they areunable to continue to take their medication as prescribed.Contrary to earlier reports (e.g., Cole & Bodkin, 1990;Papp & Gorman, 1990), Prozac is no more associatedwith suicide than other antidepressants are (Gitlin, 1996;
Maintenance1or more years
When treatment of depressionresults in removal of essentially allsymptoms, it is called remission forthe first several months, and thenrecovery if it is sustained for longerthan 6 to 12 months. Such patientsare not just better - they are well.Source: From Essential Psychopharma-cology: Neuroscientific Basis and Practi-cal Applications, 2E, p. 143, by StephenM. Stahl, copyright © Cambridge Uni-versity Press, 2000. Reprinted with thepermission of Cambridge UniversityPress.

Jick et aI., 2004). Because they have fewer side effects andare safer and easier to use, prescriptions for antidepres-sants have increased substantially in recent years.
A Psychiatrist Gets a Tasteof Her Own Medicine
Dr.G. had been a psychiatrist for many years when, dur-ing a consultation with a patient, she broke into a sweat,started to shake, and felt as if she were disintegrating. Aclose friend was dying of cancer and she felt weigheddown and depressed. Her partner, also a psychiatrist, rec-ommended that she take buproprion (Wellbutrin). Thiswas an antidepressant that Dr.G. had often prescribed toher own patients, with favorable results. She began totake it herself.
Within 10 days she developed insomnia, agitation,and tremors. She lost the ability to distinguish betweensadness and the side effects of the drug. She began todevelop panic attacks and could barely function at work.Evenso, she was terrified that she might feel worse ifshestopped taking the buproprion or started taking a newdrug. Determined to keep taking the medication despiteher deteriorating physical and mental health, she tried tofollow the advice she had given to hundreds of her ownpatients to stick things out. She forced herself to eat butlost 10 pounds. Sometimes she felt paranoid and won-dered if she was delusional. When she wasn't working,she curled up in a fetal position and wondered if sheshould hospitalize herself.
After 4 weeks she had had enough. She began totaper the medication, although her symptoms, insomnia,lack of appetite, agitation, and panic attacks continued for3 weeks after she had taken the last tablet. For a monthshe felt weak, as if she had just recovered from the flu.
After her experiences with buproprion, Dr. G. nowdescribes potential side effects to her patients in muchgreater detail than she did before. Although she contin-ues to prescribe the medication, she is vigilant aboutsigns of distress in her patients. Whereas in the past shewould have encouraged patients with side effects to stickit out, anticipating that these would eventually pass, shenow switches her patients to a new medication at the firstsign of problems. Ataste of her own medicine has madeher a more attentive and aware physician. (Adapted fromGartrell,2oo4·)
MONOAMINE OXIDASE (MAO) INHIBITORS Althoughthey are used infrequently now, these were the first antide-pressant medications to be developed in the 1950s. Thesedrugs were being studied for the treatment of tuberculosiswhen they were found to elevate the mood of patients
(Gitlin, 1996). They were later shown to be effective intreating depression. Monoamine oxidase (MAO) inhibitorsinclude isocarboxazid (Marplan), phenelzine (Nardil),tranylcypromine (Parnate), and selegiline (Eldepryl; seeChapter 7). They inhibit the activity of monoamine oxi-dase, an enzyme present in the synaptic cleft that helpsbreak down the monoamine neurotransmitters (such asserotonin and norepinephrine) that have been releasedinto the cleft. Patients taking MAO inhibitors must avoidfoods rich in the amino acid tyramine (such as salami andStilton cheese). This limits the drugs' clinical usefulness.Nevertheless, they are used in certain cases of atypicaldepression that are characterized by hypersomnia andovereating and do not respond well to other classes of anti-depressant medication (Nemeroff & Schatzberg, 2002).
TRICYCLIC ANTIDEPRESSANTS The tricyclic antide-pressants (TCAs) operate to inhibit the reuptake of norep-inephrine and (to a lesser extent) serotonin once thesehave been released into the synapse. Their discovery wasalso serendipitous in that the first TCA-imipramine-was being studied as a possible treatment for schizophreniawhen it was found to elevate mood. As discussed inChapter 7, the theory that these drugs work by increasingnorepinephrine activity is now known to be oversimpli-fied. It is also known that when the tricyclics are taken forseveral weeks, they alter a number of other aspects of cel-lular functioning including how receptors function andhow cells respond to the activation of receptors and thesynthesis of neurotransmitters. Because these alterationsin cellular functioning parallel the time course for thesedrugs to exert their antidepressant effects, one or more ofthese changes are likely to be involved in mediating theirantidepressant effects (see Figure 17.3).
OTHER ANTIDEPRESSANTS Trazodone (Desyrel) wasthe first antidepressant to be introduced in the United Statesthat was not lethal when taken in overdose. It specificallyinhibits the reuptake of serotonin. Trazodone has heavysedating properties that limit its usefulness. It is sometimesused in combination with SSRls and taken at night to helpcounter the adverse effects the SSRls often have on sleep. Inrare cases, it can produce a condition in men called priapism(Nemeroff & Schatzberg, 2002). Priapism is prolonged erec-tion in the absence of any sexual stimulation.
Bupropion (Wellbutrin) is an antidepressant that isnot structurally related to other antidepressants. It does notblock reuptake of either serotonin or norepinephrine, but itdoes seem to increase noradrenegic function through othermechanisms (Gitlin, 1996). One clinical advantage ofbupropion is that, unlike some of the SSRls, it does notinhibit sexual functioning (Nemeroff & Schatzberg, 2002).
Released in 1995, nefazodone (Serzone) is structurallyrelated to trazodone. It inhibits the reuptake of both sero-tonin and norepinephrine and has other effects on sero-

Synaptic Receptor sites
C;left .~1- Po,lsy.,plk .,.ro.
• •
TricyclicADblocking reuptake
\
Synaptic vesicles(packets ofneu rotransm itters)
tonin as well. One of the major advantages of nefazodoneis that (compared to the SSRls) it does not reduce sexualresponsiveness and does not produce insomnia. However,patients taking this medication need regular monitoring toensure that the drug is not causing any liver damage.
Other drugs that facilitate serotonin and norepineph-rine neurotransmission are mirtazapine (Remeron) andthe newly introduced duloxetine hydrochloride, which ismarketed as Cymbalta. A major side effect of Remeron isweight gain; Cymbalta, on the other hand, has been associ-ated with decreased appetite and weight loss. As new med-ications are developed, they further increase the therapeuticoptions available to patients suffering from depression.
USING ANTIDEPRESSANTS TO TREAT ANXIETY DIS-ORDERS, BULIMIA, AND PERSONALITY DISORDERSIn addition to their usefulness in treating depression, theantidepressant drugs are also widely used in the treatmentof various other disorders. As discussed in Chapter 6, SSRIsare widely used in the treatment of panic disorder, socialphobia, and generalized anxiety disorder, as well asobsessive-compulsive disorder (Dougherty et al., 2002;Gitlin, 1996; Wolfe & Maser, 1994; Roy-Byrne & Cowley,2002). However, some people with panic disorder aregreatly bothered by the side effects of these drugs (whichcreate some of the symptoms to which panic patients arehypersensitive), so they quickly discontinue the medica-tion. SSRIs and tricyclic antidepressants are also used inthe treatment of bulimia (see Chapter 9). Many, but not all,studies have shown that these antidepressants are useful inreducing binge eating and purging (Gitlin, 1996; Wilson &Fairburn, 2002). Patients with Cluster B personality disor-ders such as borderline personality disorder may show adecrease in certain symptoms, most notably mood lability,if they take SSRIs (Rinne et al., 2002).
Tricyclic Antidepressants asReuptake Blockers
Adapted from Gitlin, 1996, p. 287.
Antianxiety DrugsBENZODIAZEPINES The most important and widelyused class of antianxiety (or anxiolytic) drugs are the ben-zodiazepines. (Another class of drugs, the barbiturates[e.g., phenobarbitol], are seldom used today except to con-trol seizures or as anesthetics during electroconvulsive ther-apy.) The first benzodiazepines were released in the early1960s. They are now the drugs of choice for the treatmentof acute anxiety and agitation. They are rapidly absorbedfrom the digestive tract and start to work very quickly. Atlow doses they help quell anxiety; at higher doses they act assleep-inducing agents and can be used to treat insomnia.For this reason, people taking these medications are cau-tioned about driving or operating machinery.
One problem with benzodiazepines is that patientscan become psychologically and physiologically depen-dent on them (Gitlin, 1996; Roy-Byrne & Cowley, 2002).Patients taking these medications must be "weaned" fromthem gradually because of the risk of withdrawal symp-toms, which include seizures in some cases. Moreover,relapse rates following discontinuation of these drugs areextremely high (Roy-Byrne & Cowley, 2002). For example,as many as 60 to 80 percent of panic patients relapse fol-lowing discontinuation of Xanax (McNally, 1994). Benzo-diazepine drugs include diazepam (Valium), oxazepam(Serax), clonazepam (Klonopin), alprazolam (Xanax), andlorazepam (Ativan). Table 17.3 on page 616 provides amore comprehensive list of antianxiety medications.
Benzodiazepines and related anxiolytic medicationsare believed to work by enhancing the activity of GABAreceptors (Gitlin, 1996; Roy-Byrne & Cowley, 2002).GABA (gamma aminobutyric acid) is an inhibitory neuro-transmitter that plays an important role in the way ourbrain inhibits anxiety in stressful situations. The benzodi-azepines appear to enhance GABA activity in certain parts

~ < Commonly Prescribed Antianxiety Drugs < :
Drug Class Generic Name Trade Name Dose Range (mg) Half-Life (hrs)Benzodiazepines alprazolam Xanax 0.5-10 9-20
clonazepam Klonopin 1-6 19-60diazepam Valium 4-40 30-200lorazepam Ativan 1-6 8-24oxazepam Serax 30-120 3-25clorazepate Tranxene 15-60 120chlordiazepoxide Librium 10-150 28-100
Other buspirone Buspar 5-30 1-11
Sources: Bezchlibnyk-Butler & Jeffries (2003); Buckley & Waddington (2001); and Sadock & Sadock (2003).
Anti-anxiety medications are widely prescribed. However,patients can become psychologically and physiologicallydependent on them.
of the brain known to be implicated in anxiety such as thelimbic system.
The range of applications of antianxiety drugs is quitebroad. They are used in all manner of conditions in whichtension and anxiety may be significant components, includ-ing anxiety-based and psychophysiological disorders. Theyare also used as supplementary treatment in certain neuro-logical disorders to control such symptoms as convulsiveseizures, but they have little place in the treatment of psy-chosis. They are among the most widely prescribed drugs, afact that has caused concern among some leaders in themedical and psychiatric fields because of these drugs' addic-tive potential and sedating effects.
OTHER ANTI-ANXIETY MEDICATIONS The only newclass of antianxiety medication that has been released since
the early 1960s is buspirone (Buspar), which is completelyunrelated to the benzodiazepines and is thought to act incomplex ways on serotonergic functioning rather than onGABA. It has been shown to be as effective as the benzodi-azepines in treating generalized anxiety disorder (Gitlin,1996; Roy-Byrne & Cowley, 2002), although patients whohave previously taken benzodiazepines tend not to respondas well as patients who have never taken them. Buspar has alow potential for abuse, probably because it has no sedativeor muscle-relaxing properties and so is less pleasurable forpatients. It also does not cause any withdrawal effects. Theprimary drawback to the use of buspirone is that it takes2 to 4 weeks to exert any anxiolytic effects. It is thereforenot useful in acute situations. Because it is nonsedating, itcannot be used to treat insomnia.
Lithium and Other Mood-StabilizingDrugsIn the late 1940s John Cade in Australia discovered thatlithium salts such as lithium carbonate were effective intreating manic disorders. One of Cade's (1949) own casesserves well as an illustration of the effects of lithiumtreatment.
Lithium Helps a DifficultPatient
Mr.W.B. was a 51-year-old man who had been in a stateof chronic manic excitement for 5 years. So obnoxiousand destructive was his behavior that he had long beenregarded as the most difficult patient on his ward in thehospital.
He was started on treatment with a lithium com-pound, and within 3 weeks his behavior had improved so

much that transfer to the convalescent ward was deemedappropriate. He remained in the hospital for another 2
months, during which time his behavior continued to beessentially normal. Prior to discharge, he was switched toanother form of lithium salts because the one he hadbeen taking had caused stomach upset.
Hewas soon back at his job and living a happy andproductive life. In fact, he felt so good that, contrary toinstructions, he stopped taking his lithium. Thereafter hesteadily became more irritable and erratic; some 6months following his discharge, he had to cease work. Inanother 5 weeks he was back at the hospital in an acutemanic state.
Lithium therapy was immediately reestablished,with prompt positive results. In another month Mr.W.B.was pronounced ready to return to home and work, pro-vided that he not fail to continue taking a prescribeddosage of lithium.
It was about 20 years before lithium treatment wasintroduced, around 1970, in the United States. There wereat least two reasons for this delay. First, lithium had beenused as a salt substitute for patients with hypertension inthe 1940s and 1950s when its toxic side effects wereunknown. Some tragic deaths resulted, making the med-ical community very wary of using it for any reason. Sec-ond, because it is a naturally occurring compound, it isunpatentable. This meant that drug companies did notfind it profitable to investigate its effects. Nevertheless, bythe mid-1970s it was regarded as a wonder drug in psychi-atry (Gitlin, 1996). It is still widely used for the treatmentof bipolar disorder and is marketed as Eskalith.
The biochemical basis oflithium's therapeutic effect isunknown. One hypothesis is that lithium, being a mineralsalt, may affect electrolyte balances that may alter the activ-ities of many neurotransmitter systems in the brain, whichis consistent with its diverse clinical effects (Gitlin, 1996).So far, however, this connection remains largely specula-tive. Clearly, the riddle of exactly what occurs will be solvedonly by more and better research.
Even though we still do not know exactly how itworks, there is no doubt about the effectiveness oflithium.As many as 70 to 80 percent of patients in a clear manicstate show marked improvement after 2 to 3 weeks of tak-ing lithium (Keck & McElroy, 2002b; Sadock & Sadock,2003). In addition, as we saw in Chapter 7, lithium some-times relieves depression, although probably mainly inpatients with bipolar depression. Nevertheless, there maybe a subclass of unipolar depressive patients who benefitfrom lithium treatment (Abou-Saleh, 1992; Gitlin, 1996).
There is increasing evidence that lithium mainte-nance treatment may be less reliable at preventing futureepisodes of mania than was once thought. For example,several studies of bipolar patients maintained on lithium
for 5 years or more found that only just over one-thirdremained in remission. Nevertheless, discontinuation oflithium is also very risky. The probability of relapse is esti-mated to be 28 times higher after withdrawal than whenthe patient is on lithium, with about 50 percent relapsingwithin 6 months (Keck & McElroy, 2002b).
Side effects of lithium include increased thirst, gas-trointestinal difficulties, weight gain, tremor, and fatigue.In addition, lithium can be toxic if the recommended doseis exceeded or if the kidneys fail to excrete it from the bodyat a normal rate. Lithium toxicity is a serious medical con-dition. If not treated swiftly and appropriately, it can causeneuronal damage or even death.
Despite the clinical benefits oflithium, not all patientswith bipolar disorder take it exactly as prescribed. Manyseem to miss the "highs" and the abundance of energyassociated with their hypomanic episodes, so when facedwith unpleasant side effects and the loss of these highs,they may stop taking the drug.
Even though I was a clinician and a scientist, and eventhough I could read the research literature and see theinevitable, bleak consequences of not taking lithium, formany years after my initial diagnosis I was reluctant totake my medications as prescribed. Whywas I so unwill-ing? Why did I have to go through more episodes ofmania, followed by long suicidal depressions, before Iwould take lithium in a medically sensible way?
Some of my reluctance, no doubt, stemmed from afundamental denial that what I had was a real disease.This is a common reaction that follows, rather counterin-tuitively, in the wake of early episodes of manic-depres-sive illness. Moods are such an essential part of thesubstance of life, of one's notion of oneself, that evenpsychotic extremes in mood and behavior somehow canbe seen as temporary, even understandable reactions towhat life has dealt. ... It was difficult to give up the highflights of mind and mood, even though the depressionsthat inevitably followed nearly cost me my life.
Myfamilyand friends expected that Iwould welcomebeing "normal," be appreciative of lithium, and take instride having normal energy and sleep. But ifyou have hadstars at your feet and rings of planets through your hands,are used to sleeping only 4 or 5 hours a night and nowsleep 8, are used to staying up all night for days andweeks ina rowand now cannot, it is a very real adjustmentto blend into a three-piece-suit schedule, which, thoughcomfortable to many, is new, restrictive, seemingly lessproductive, and maddeningly less intoxicating. People
(continued)

say, when I complain of being less lively, less energetic,less high-spirited, "Well, now you're just like the rest ofus," intending, among other things, to be reassuring. But Icompare myself with my former self, not with others. Notonly that, I tend to compare my current self with the best Ihave been, which is when I have been mildly manic.(Adapted from Jamison,1995, pp. 91-93, 167.)
Source: From AN UNQUIET MIND by Kay Redfield Jamison,copyright © 1995 by Kay Redfield Jamison. Used by permissionof Alfred A. Knopf, a division of Random House, Inc.
OTHER MOOD-STABILIZING DRUGS Although lith-ium is still widely used, other drugs are also consideredfirst-line treatments for bipolar disorder (see Table 17.4).These include divalproic acid (Depakote) and carba-mazepine (Tegretol). Other drugs that are currently beingresearched and used clinically as treatments for rapidcycling bipolar disorders are gabapentin (Neurontin), lam-otrigine (Lamictal), and topiramate (Topamax). Many ofthese drugs are used in the treatment of epilepsy and areanticonvulsant agents (Keck & McElroy, 2002a, 2002b).Carbamazepine has been associated with significant sideeffects including blood problems, hepatitis, and seriousskin conditions (Sadock & Sadock, 2003). As with lithium,careful blood monitoring of patients is required. Valpro ateprobably has the fewest and mildest side effects, which caninclude nausea, diarrhea, sedation, tremor, and weightgain. Abilify, an antipsychotic medication, is also nowbeing marketed as a treatment for bipolar disorder.
Electroconvulsive TherapyUsing convulsions to treat mental disorders dates back tothe Swiss physician/alchemist Paracelsus (1493-1591),who induced a patient with "lunacy" to drink camphoruntil he experienced convulsions (Abrams, 2002; Mow-bray, 1959). However, Ladislas von Meduna, a Hungarianphysician, is generally regarded as the modern originatorof this treatment approach. Von Meduna noted-erro-neously, as it turned out-that schizophrenia rarely
A patient who receives electroconvulsive therapy (ECT) today isgiven sedative and muscle-relaxant medication prior to theprocedure to prevent violent contractions. In the days before suchmedication was available, the initial seizure was sometimes soviolent as to fracture vertebrae.
occurred in people with epilepsy. This observation causedhim to infer that schizophrenia and epilepsy were some-how incompatible and to speculate that one might be ableto cure schizophrenia by inducing convulsions. In an earlytreatment effort, von Meduna used camphor to induceconvulsions in a patient with schizophrenia, who relativelyquickly regained lucidity after the convulsive therapy.Later, von Meduna began to use a drug called Metrazol toinduce convulsions because it operated more rapidly.
Another early approach, adopted by Sakel in the1930s, was to cause convulsions by injecting patients withinsulin (see Fink, 2003). However, these chemical methodsgave physicians no control over the induction and timingof the seizures. Then, in 1938, the Italian physicians UgoCerletti and Lucio Bini tried the simplest method of all-passing an electric current through a patient's head. Thismethod. which became known as electroconvulsive ther-apy (ECT), is still used today. In the United States, about100,000 patients are treated with ECT each year (Sadock &Sadock,2003).
The general public often views ECT as a horrific andprimitive form of treatment. Indeed, a number of mal-
If:~~:~mmonlyPrescribed Mood-Stabilizing Medications
Drug Class Generic Name Trade Name Dose Range (mg) Half-Life (hrs)Lithium lithium Eskalith 400-1200 24
Anticonvulsants carbamazepine Tegretol 300-1600 16-24divalproex Depakote 750-3000 6-16lamotrigine Lamictal 100-500 25gabapentin Neurontin 900-3600 5-9topiramate Topamax 50-1300 21

practice lawsuits have been brought against psychiatristswho use ECT, primarily over the failure to obtain appro-priate patient consent, which can be very difficult whenpatients may not be legally competent to give such con-sent due to their illness (Abrams, 2002; Leong & Eth,1991). However, despite the distaste with which some peo-ple regard ECT, it is a safe, effective, and important formof treatment. In fact, it is the only way of dealing withsome severely depressed and suicidal patients-patientswho may have failed to respond to other forms of treat-ment. In addition, it is often the treatment of choice forseverely depressed women who are pregnant, for whomtaking antidepressants may be problematic, as well as forthe elderly, who may have medical conditions that maketaking antidepressant drugs dangerous (Gitlin, 1996).Properly administered, ECT does not do any structuraldamage to the brain (Devanand et aI., 1994; Gitlin, 1996).Moreover, numerous reviews evaluating the research onECT over the past 50 years have concluded that ECT isalso an effective treatment for patients with manic disor-ders who have not responded to pharmacotherapy (it is 80percent effective overall with difficult-to-treat patients;e.g., Abrams, 2002; Mukherjee et aI., 1994). For example,Husain and colleagues (1993) reported on the use of along-term (2-year) treatment of an elderly woman withrecurring mania. The authors pointed out that the ECT(81 sessions in all) was the only effective means of con-trolling her manic episodes and proved to be both safe andcost -effective.
Virtually every neurotransmitter system is affected byECT. ECT is known to downregulate the receptors for nor-epinephrine, increasing the functional availability of thisneurotransmitter. However, exactly how ECT works is stillnot fully clear (Abrams, 2002; Gitlin, 1996).
ECT can be administered in one of two ways. Inbilateral ECT, electrodes are placed on either side of thepatient's head (see Figure 17.4), and constant-current briefelectrical pulses of either high or low intensity are passedfrom one side of the head to the other for up to about 1.5seconds. In contrast, unilateral ECT (see Figure 17.4)involves limiting current flow to one side of the brain, typ-ically the non dominant side (right side, for most people).Anesthetics allow the patient to sleep through the proce-dure, and muscle relaxants are used to prevent the violentcontractions that, in the early days of ECT, could be sosevere as to cause the patient to fracture bones. Today, ifyou were to observe someone receiving ECT, all you mightsee would be a small twitch of the hand, perhaps, as theconvulsions occurred.
After the ECT is over, the patient has amnesia for theperiod immediately preceding the therapy and is usuallysomewhat confused for the next hour or so. Normally, atreatment series consists of fewer than a dozen sessions,although occasionally more are needed (Gitlin, 1996).With repeated treatments, usually administered threetimes weekly, the patient gradually becomes disoriented, astate that usually clears after termination of the treatments.
Unilateral and bilateral electrode placement for fer.Adapted from Sadock & Sadock, 2003, p. 1142.
Empirical evidence suggests that bilateral ECT is moreeffective than unilateral ECT (Sackheim et aI., 1993).Unfortunately, bilateral ECT is also associated with moresevere cognitive side effects and memory problems.Patients often have difficulty forming new memories(anterograde amnesia) for about 3 months after ECT ends.Physicians must therefore weigh the greater clinical bene-fits of bilateral ECT against its tendency to cause greatercognitive side effects. Some clinicians recommend startingwith unilateral ECT and switching to bilateral after five orsix treatments if no improvement is seen (Abrams, 2002;Gitlin, 1996).
A dramatic early example of successful ECT treat-ments is provided in the autobiographical account ofLenore McCall (1947/1961), who suffered a severe depres-sive disorder in her middle years.
Using ECTto Treat SevereDepression
Ms. McCall, a well-educated woman of affluent circum-stances and the mother of three children, noticed a feel-ing of persistent fatigue as the first sign of her impendingdescent into depression. Too fearful to seek help, she atfirst attempted to fight off her increasingly profound apa-thy by engaging in excessive activity, a defensive strategythat accomplished little but the depletion of her remain-ing strength and emotional reserves.
Indue course, she noticed that her mental processesseemed to be deteriorating- her memory appearedimpaired and she could concentrate only with great diffi-culty. Emotionally,she felt an enormous loneliness, bleak-
(continued)

ness of experience, and increasingly intense fear aboutwhat was happening to her mind. She came to view herpast small errors of commission and omission as the mostheinous of crimes and increasingly withdrew from contactwith her husband and children. Eventually, at her hus-band's and her physician's insistence, she was hospital-ized despite her own vigorous resistance. She feltbetrayed and shortly thereafter attempted suicide byshattering a drinking glass and ingesting its fragments. Toher great disappointment, she survived.
Ms. McCallthen spent nearly 4 years continuously intwo separate mental hospitals, during which time shedeteriorated further. She was silent and withdrawn,behaved in a mechanical fashion,lost an alarming amountof weight, and underwent a seemingly premature agingprocess. She felt that she emitted an offensive odor. Atthis time, ECTwas introduced into the therapeutic proce-dures in use at her hospital.
A series of ECTtreatments was given to Ms. McCallover about a 3-month period. Then one day, she woke upin the morning with a totally changed outlook: "I sat upsuddenly, my heart pounding. I looked around the roomand a sweep of wonder surged over me. God in heaven,I'mwell. I'm myself. ... " After a brief period of convales-cence, she went home to her husband and children.
NeurosurgeryAlthough neurosurgery was used occasionally in thenineteenth century to treat mental disorders by relievingpressure in the brain (Berrios, 1990), it was not consid-ered a treatment for psychological problems until thiscentury. In 1935 in Portugal, Antonio Moniz introduceda neurosurgical procedure in which the frontal lobes ofthe brain were severed from the deeper centers under-lying them. This technique eventually evolved into anoperation known as "prefrontal lobotomy," which stands
17.5One ofthe victimsof the zeal to performpre-
frontal lobotomiesto alleviatebehaviorprob-lemswas RosemaryKennedy,the sister offormerpresident John F. Kennedyand sena-tors Robertand EdwardKennedy.Rosemary
was the third childofJoseph and RoseKennedy.Bornduringthe height of the influenzaepidemicof 1918, she was a beau-
as a dubious tribute to the extremes to which profession-als have sometimes been driven in their search for effec-tive treatments for the psychoses. In retrospect, it is ironicthat this procedure-which results in permanent struc-tural changes in the brain of the patient and has beenhighly criticized by many within the profession-wonMoniz the 1949 Nobel Prize in medicine (although hewas later shot by a former patient who was, presumedly,less than grateful).
From 1935 to 1955 (when antipsychotic drugs becameavailable), tens of thousands of mental patients in this coun-try and abroad were subjected to prefrontal lobotomies andrelated neurosurgical procedures. In some settings, as manyas 50 patients were treated in a single day (Freeman, 1959).Initial reports of results tended to be enthusiastic, down-playing complications (which included a 1 to 4 percentdeath rate) and undesirable side effects. It was eventuallyrecognized, however, that the "side effects" of psychosurgerycould be very undesirable indeed. In some instances theyincluded a permanent inability to inhibit impulses, in othersan unnatural "tranquility" with undesirable shallowness orabsence of feeling. The World Around Us 17.5 describes thetragic results of the lobotomy performed on RosemaryKennedy, sister of former president John F.Kennedy.
The introduction of the major antipsychotic drugscaused an immediate decrease in the widespread use ofpsychosurgery, especially prefrontal lobotomy. Such oper-ations are rare today and are used only as a last resort forpatients who have not responded to all other forms oftreatment for a period of 5 years and who are experiencingextreme and disabling symptoms. Modern surgical tech-niques involve the selective destruction of minute areas ofthe brain. Psychosurgery is sometimes used for patientswith debilitating obsessive-compulsive disorders (seeRauch & Jenike, 1998; Sachdev et a1., 2001) or treatment-resistant severe self-mutilation (Price et a1.,2001). Morganand Crisp (2000) have also reported long-term follow-updata on four patients with intractable anorexia nervosawho were treated with leukotomy.
The Tragedy ofRosemary Kennedy
tifulbaby,witha sweet temperament. Overtime, however,her mother became increasinglyconcernedabout Rose-mary'sslowdevelopment comparedto her brothers and sis-ters. Whenthe familyfinallyconcludedthat Rosemarywasretarded, the best experts inthe countryat the time couldofferno guidanceand told the familythat nothingcould bedone except to place Rosemaryinan institution.

Rose Kennedy and the family rebelled againstthis suggestion. Instead of being institutionalized,Rosemary was kept at home. She had a special gov-erness and many private tutors. She participatedfully in the Kennedy family's activities, and shemade considerable progress. By the age of 18,Rosemary was performing at a fifth-grade level inEnglish and at a fourth-grade level in math.
Because of the considerable stigma associ-ated with mental retardation at the time, Rose-mary's parents kept her condition hidden fromthose outside the family, a major task because ofthe scrutiny the family was subjected to by thepress. Although her parents and siblings werealways nearby to protect her, Rosemary developedthe social skills needed to be presented success-fully as a debutante and later to the king and queenof England at Buckingham Palace.
Unfortunately, Rosemary's behavior deterio-rated when, around the beginning of World War II,the family returned to the United States from Eng-land, where Joseph Kennedy had been ambas-sador. Some of her deterioration may have beencaused by her increasing frustration at not being able todo all the things her siblings were able to do, as well ashaving to leave the school in England where she had feltsuccessful. The 21-year-old Rosemary became quite vio-lent and frequently ran away from home or her conventschool, and there was considerable concern for hersafety. Her father turned to the medical experts of thetime, searching for a solution.
These experts convinced Joseph Kennedy that themiracle treatment he sought lay in prefrontal lobotomy.Rosemary Kennedy became one of the thousands submit-
Although not enough controlled studies of these newpsychosurgery techniques have been published to warrantfirm conclusions, research has been encouraging for atleast one disorder. Mindus and colleagues (1993, 1994)described an overall satisfactory result of psychosurgery in253 severely obsessive-compulsive patients. About half ofthese patients were found to show at least a 35 percentreduction in intensity of symptoms after surgery. Thisexperimental procedure is associated with relatively fewnegative side effects (although occasionally patients experi-ence seizures or transient headaches). However, effects oncognition or personality are rare (Dougherty et al., 2002).
Deep brain stimulation is a new treatment approachthat involves surgery but does not result in a permanentlesion being made in the brain. As Developments inResearch 17.6 on page 622 illustrates, this innovative formof therapy is now being used to help patients get somerelief from their unrelenting symptoms of depression.
The tragic failure of Rosemary Kennedy's prefrontal lobotomy is areminder that brain surgery can permanently alter personality.Rosemary is shown here in foreground, with her sister Kathleen(left) and mother Rose (center},before the surgery.
ted to that "desperate" cure. In Rosemary's case, thesurgery was a tragic failure-all her previous accomplish-ments were wiped out, leaving little of her former person-ality and adaptive ability intact: "They knew right awaythat it wasn't successful. You could see by looking at herthat something was wrong, for her head was tilted andher capacity to speak was almost entirely gone. Therewas no question now that she could no longer take careof herself and that the only answer was an institution."(Ann Gargan King, a cousin, as reported by Goodwin,1988, p. 744.)
~ What kinds of disorders can be treated withantipsychotic drugs? How do these drugshelp patients? What are their drawbacks?
~ Why have the SSRls largely replaced tricyclicantidepressants in routine clinical practice?What kinds of conditions can be treated withantidepressants?
~ What kinds of medications can be used totreat acute anxiety and agitation? How arethese medications believed to work?
~ Do the clinical advantages of ECToutweighits disadvantages?

7. Treating DepressedPatients with Deep BrainStimulation
21 new development in the treatmentof patients with severe and chronicmental health problems is deepbrain stimulation. This involves stim-ulating patients' brains electrically
over a period of several months. In one study, sur-geons drilled holes into the brains of six severelydepressed patients and implanted small electrodes(see Mayberg et aI., 2005). Because this procedurewas done under local anesthetic, the patients wereable to talk to the doctors about what was happeningto them and tell the doctors about the changes theyexperienced when the voltage through the electrodeswas gradually increased. Although the patients hadno cues to tell them when current was being passedthrough the electrodes or when the current was off, allof them reported a response to the electrical stimula-tion. When current was flowing into an area of thebrain that is thought to be metabolically overactive indepression (the cingulate region), patients reportedfeelings of "sudden calmness or lightness," "connect-edness", or "disappearance of the void" (p. 652).Patients also reported feeling better during theseperiods of stimulation.
In the days after the operation, the researchersgave patients short sessions of deep brain stimulationin which current was passed through the implantedelectrodes. Using the reports of the patients as a guide,the researchers then selected the settings that wouldbe used after the patients left the hospital to providestimulation through an implanted pulse device.
Over the next few months, four of the six patientswho received treatment with deep brain stimulationshowed clinical improvement, and two patients wereactually depression-free after 6 months.
Of course, from a research perspective, there aremany limitations to this study. The treatment technique isalso invasive. However, this innovative approach may be
PSYCHOLOGICALApPROACHES TOTREATMENT
Behavior TherapyBehavior therapy is a direct and active treatment that rec-ognizes the primacy of behavior, acknowledges the role oflearning, and includes thorough assessment and evalua-tion (see Kazdin, 1984). Instead of exploring past trau-
In deep brain stimulation, electrodes are implanted into the brain.These are stimulated by pulse generators implanted into the chestregion.Sou ree: http://www. cleve land cIInie.0rgIn eu rosc Ience Itreatlmove me n t/imageslmedtronicman.gl{
able to provide relief to depressed patients who have failedto show improvement with other forms of therapy withoutpermanent lesions being made in their brains.
matic events or inner conflicts, behavior therapists focuson the presenting problem-the problem or symptom thatis causing the patient great distress. A major assumption ofbehavior therapy is that abnormal behavior is acquired inthe same way as normal behavior-that is, by learning. Avariety of behavioral techniques have therefore been devel-oped to help patients "unlearn" maladaptive behaviors byone means or another.
EXPOSURE THERAPY A behavior therapy techniquethat is widely used in the treatment of anxiety disorders isexposure (see Chapter 6). If anxiety is learned, then, from

the behavior therapy perspective, it can be unlearned. Thisis accomplished through guided exposure to anxiety-provoking stimuli. During exposure therapy, the patientor client is confronted with the fear-producing stimulus ina therapeutic manner. This can be accomplished in a verycontrolled, slow, and gradual way, as in systematicdesensitization, or in a more extreme manner, as inflooding, where the patient directly confronts the fearedstimulus at full strength. (An example is a houseboundpatient with agoraphobia being accompanied outdoors bythe therapist). Moreover, the form of the exposure can bereal (also known as in vivo exposure) or imaginary(imaginal exposure).
The rationale behind systematic desensitization isquite simple: Find a behavior that is incompatible withbeing anxious (such as being relaxed or experiencingsomething pleasant) and repeatedly pair this with thestimulus that provokes anxiety in the patient. Because it isdifficult if not impossible to feel both pleasant and anxiousat the same time, systematic desensitization is aimed atteaching a person, while in the presence (real or imagined)of the anxiety-producing stimulus, to relax or behave insome other way that is inconsistent with anxiety. It maytherefore be considered a type of counter-conditioningprocedure. The term systematic refers to the carefully grad-uated manner in which the person is exposed to the fearedstimulus.
The prototype of systematic desensitization is theclassic experiment of Mary Cover Jones (1924), in whichshe successfully eliminated a small boy's fears of a whiterabbit and other furry animals. She began by bringing therabbit just inside the door at the far end of the room whilethe boy, Peter, was eating. On successive days, the rabbitwas gradually brought closer until Peter could pat it withone hand while eating with the other.
Joseph Wolpe (1958; Rachman & Hodgson, 1980)elaborated on the procedure developed by Jones andcoined the phrase systematic desensitization to refer to it.On the assumption that most anxiety-based patterns are,fundamentally, conditioned responses, Wolpe worked outa way to train a client to remain calm and relaxed in situa-tions that formerly produced anxiety. Wolpe's approach iselegant in its simplicity, and his method is equallystraightforward.
A client is first taught to enter a state of relaxation,typically by progressive concentration on relaxing variousmuscle groups. Meanwhile, patient and therapist collabo-rate in constructing an anxiety hierarchy that consists ofimagined scenes graded as to their capacity to elicit anxi-ety. For example, for a dog-phobic patient, a low-anxietystep might be imagining a small dog in the distance beingwalked on a leash by its owner. In contrast, a high-anxietystep might be imagining a large and exuberant dog run-ning toward oneself. Therapy sessions consist of thepatient's repeatedly imagining, under conditions of deeprelaxation, the scenes in the hierarchy, beginning with low-anxiety images and gradually working toward those in the
more extreme ranges. Treatment continues until all itemsin the hierarchy can be imagined without notable discom-fort, at which point the client's real-life difficulties typicallyhave shown substantial improvement.
Imaginal procedures have some limitations, an obvi-ous one being that not everybody is capable of vividlyimagining the required scenes. In an early study of clientswith agoraphobia, Emmelkamp and Wessels (1975) con-cluded that prolonged exposure in vivo was superior toimaginal exposure. Since then, therapists have sought touse in vivo exposure whenever this is practical, encourag-ing clients to confront anxiety-provoking situations directly(Barlow, 1988, 1993). Obviously, however, this cannot beaccomplished for all stimuli. In addition, an occasionalclient is so fearful that he or she cannot be induced to con-front the anxiety-arousing situation directly (Emmelkamp& Wessels, 1975). Imaginal procedures are therefore a vitalpart of the therapeutic exposure repertoire. A recent devel-opment in behavior therapy is the use of virtual reality tohelp patients overcome their fears and phobias (e.g.,Emmelkamp, 2004; Rothbaum, Hodges, et aI., 2000). Suchapproaches are obviously helpful when the source of thepatient's anxiety is something that is not easily reproducedin real life.
When a therapist has a choice, in vivo procedures seemto have an edge in efficiency, and possibly in ultimate effi-cacy, over those employing imagery as the mode of con-frontation (Emmelkamp, 1994). Overall, the outcomerecord for exposure treatments is impressive (Barlow et al.,2002; Emmelkamp, 2004; Roth & Fonagy, 1996).
AVERSION THERAPY Aversion therapy involves modi-fying undesirable behavior by the old-fashioned method ofpunishment. Probably the most commonly used aversivestimuli today are drugs that have noxious effects, such asAntabuse, which induces nausea and vomiting when a per-son who has taken it ingests alcohol (see Chapter 12). Inanother variant, the client is instructed to wear a substan-tial elastic band on the wrist and to "snap" it when tempta-tion arises, thus administering self-punishment.
In the past, painful electric shock was commonlyemployed in programs that paired it with the occurrence ofthe undesirable behavior, a practice that certainly con-tributed to aversion therapy's "negative image" amongsome segments of the public. Although aversive condition-ing has been used to treat a wide range of maladaptivebehaviors including smoking, drinking, overeating, drugdependence, gambling, sexual deviance, and bizarre psy-chotic behavior, interest in this approach is now on thedecline (see Emmelkamp, 2004).
MODELING As the name implies, in modeling the clientlearns new skills by imitating another person, such as aparent or therapist, who performs the behavior to beacquired. A younger client may be exposed to behaviors orroles in peers who act as assistants to the therapist and thenbe encouraged to imitate and practice the desired new

responses. For example, modeling may be used to promotethe learning of simple skills such as self-feeding for a pro-foundly mentally retarded child, or more complex skillssuch as being more effective in social situations for a shy,withdrawn adolescent. In work with children especially,effective decision making and problem solving may bemodeled when the therapist "thinks out loud" about every-day choices that present themselves in the course of ther-apy (Kendall, 1990; Kendall & Braswell, 1985).
Modeling and imitation are adjunctive aspects of var-ious forms of behavior therapy as well as other types oftherapy. For example, in an early classic work, Bandura(1964) found that live modeling offearlessness, combinedwith instruction and guided exposure, was the most effec-tive treatment for snake phobia, resulting in the elimina-tion of phobic reactions in over 90 percent of the casestreated. The photographs taken during the treatment ofspider phobia on page 189 of this text provide a graphicexample of a similar combined approach.
SYSTEMATIC USE OF REINFORCEMENT Often referredto as "contingency management;' systematic programsthat manage through reinforcement to suppress (extin-guish) unwanted behavior or to elicit and maintain effec-tive behavior have achieved notable success, particularlybut by no means exclusively in institutional settings.
Suppressing problematic behavior may be as simple asremoving the reinforcements that support it, provided, ofcourse, that they can be identified. Sometimes identifica-tion is relatively easy, as in the following case. In otherinstances, it may require extremely careful and detailedobservation and analysis for the therapist to learn what ismaintaining the maladaptive behavior.
Billy,a 6-year-old first grader, was brought to a psycho-logical clinic by his parents because he hated school andbecause his teacher had told them that his showing offwas disrupting the class and making him unpopular. Itbecame apparent, in observing Billyand his parents dur-ing the initial interview, that both his mother and hisfather were noncritical and approving of everything Billydid. After further assessment, a three-phase program oftherapy was undertaken: (1) The parents were helped todiscriminate between showing-off behavior and appro-priate behavior on Billy's part. (2) The parents wereinstructed to show a loss of interest and attention whenBillyengaged in showing-off behavior, while continuingto show their approval of appropriate behavior. (3) Billy'steacher was instructed to ignore Billy,insofar as it was
feasible, when he engaged in showing-off behavior andto devote her attention at those times to children whowere behaving more appropriately.
Although Billy's showing off in class increased dur-ing the first few days of this behavior therapy program, itdiminished markedly after his parents and teacher nolonger reinforced it. As his maladaptive behavior dimin-ished, he was better accepted by his classmates, which,in turn, helped reinforce more appropriate behavior pat-terns and changed his negative attitude toward school.
Billy's was a case in which unwanted behavior waseliminated by eliminating its reinforcers. On other occa-sions, therapy is administered to establish desired behav-iors that are missing. Examples of such approaches areresponse shaping and use of token economies. In responseshaping, positive reinforcement is often used to establish,by gradual approximation, a response that is activelyresisted or is not initially in an individual's behavioralrepertoire. This technique has been used extensively inworking with children's behavior problems.
TOKEN ECONOMIES Years ago, when behavior therapywas in its infancy, token economies based on the principlesof operant conditioning were developed for use withchronic psychiatric inpatients. When they behaved appro-priately on the hospital ward, patients earned tokens thatthey could later use to receive rewards or privileges (Paul,1982; Paul & Lentz, 1977).
Token economies have been used to establish adaptivebehaviors ranging from elementary responses such as eat-ing and making one's bed, to the daily performance ofresponsible hospital jobs. In the latter instance, the tokeneconomy resembles the outside world, where an individualis paid for his or her work in tokens (money) that can laterbe exchanged for desired objects and activities. Althoughsometimes the subject of criticism and controversy, tokeneconomies remain a relevant treatment approach for theseriously mentally ill and those with developmental dis-abilities (see Corrigan, 1995; Higgins et aI., 2001; Le Blancet aI., 2000; Morisse et aI., 1996).
Similar reinforcement-based methods are now beingused to treat substance abuse. In one study, people beingtreated for cocaine dependence were rewarded withvouchers worth 25 cents if their urine test came back neg-ative (see Higgins, Wong, et al., 2000). Patients could thenask a staff member to purchase for them items from thecommunity with the vouchers they had accumulated.Patients who received the incentive vouchers based ontheir abstinence from cocaine had better clinical outcomesthan a comparison group of patients who also receivedvouchers but whose vouchers were not contingent on theirabstinent behavior.

EVALUATING BEHAVIOR THERAPY Compared withsome other forms of therapy, behavior therapy has somedistinct advantages. Behavior therapy usually achievesresults in a short period of time because it is generallydirected to specific symptoms, leading to faster relief of aclient's distress and to lower costs. The methods to be usedare also clearly delineated, and the results can be readilyevaluated (Marks, 1982). Overall, the outcomes achievedwith behavior therapy compare very favorably with thoseof other approaches (Emmelkamp, 2004; Nathan & Gor-man, 2002; Roth & Fonagy, 1996).
As with other approaches, behavior therapy worksbetter with certain kinds of problems than with others.Generally, the more pervasive and vaguely defined theclient's problem, the less likely behavior therapy is to beuseful. For example, it appears to be only rarely employedto treat complex personality disorders, although dialecticalbehavior therapy for patients with borderline personalitydisorder (see Chapter 11) is an exception. On the otherhand, behavioral techniques are the backbone of modernapproaches to treating sexual dysfunctions, as discussed inChapter 13. Moreover, quantitative reviews of therapeuticoutcomes confirm the expectation that behavior therapy isespecially effective in the treatment of anxiety disorders,where the powerful exposure techniques can be broughtto bear (Andrews & Harvey, 1981; Chambless et aI., 1998;Clum et al., 1993; Nathan & Gorman, 2002). Behaviortherapy can even be used with psychotic patients. Althoughbehavior therapy is far from a cure-all, it has a highlyrespected place among the available psychosocial treat-ment approaches.
Cognitive and Cognitive-BehavioralTherapyEarly behavior therapists focused on observable behaviorand regarded the inner thoughts of their clients as unim-portant. Because of this, these therapists were often viewedas mechanistic technicians who simply manipulated theirclients without considering them as people. Starting in the1970s, a number of behavior therapists began to reappraisethe importance of "private events"-thoughts, percep-tions, evaluations, and self-statements-and started to seethem as processes that mediate the effects of objectivestimulus conditions and thus help determine behavior andemotions (Borkovec, 1985; Mahoney & Arnkoff, 1978).
Cognitive and cognitive-behavioral therapy (termsfor the most part used interchangeably) stem from bothcognitive psychology (with its emphasis on the effects ofthoughts on behavior) and behaviorism (with its rigorousmethodology and performance-oriented focus). At thepresent time, no single set of techniques defines cognitivelyoriented treatment approaches. Two main themes areimportant, however: (1) the conviction that cognitiveprocesses influence emotion, motivation, and behavior,and (2) the use of cognitive and behavior-change tech-
niques in a pragmatic (hypothesis-testing) manner. In ourdiscussion we briefly describe the rational emotive behav-ior therapy of Albert Ellis and then focus in more detail onthe cognitive therapy approach of Aaron Beck.
RATIONAL EMOTIVE BEHAVIOR THERAPY One of theearliest developed of the behaviorally oriented cognitivetherapies is the rational emotive therapy (now calledrational emotive behavior therapy-REBT) of AlbertEllis (see Ellis & Dryden, 1997). REBT attempts to changea client's maladaptive thought processes, on which mal-adaptive emotional responses, and thus behavior, are pre-sumed to depend.
Ellis posited that a well-functioning individual behavesrationally and in tune with empirical reality. Unfortunately,however, many of us have learned unrealistic beliefs andperfectionistic values that cause us to expect too much ofourselves, leading us to behave irrationally and then to feelthat we are worthless failures. For example, a person maycontinually think, "I should be able to win everyone's loveand approval" or "I should be thoroughly adequate andcompetent in everything I do." Such unrealistic assump-tions and self-demands inevitably spell problems.
The task of REBT is to restructure an individual'sbelief system and self-evaluation, especially with respect tothe irrational "shoulds," "oughts;' and "musts" that are pre-venting the individual from having a more positive senseof self-worth and an emotionally satisfying, fulfilling life.Several methods are used. One method is to dispute a per-son's false beliefs through rational confrontation ("Whyshould your failure to get the promotion you wanted meanthat you are worthless?").
REBT therapists also use behaviorally oriented tech-niques. For example, homework assignments might begiven to encourage clients to have new experiences and tobreak negative chains of behavior. Although the techniquesdiffer dramatically, the philosophy underlying REBT hassomething in common with that underlying humanistictherapy (discussed later) because both take a clear stand onpersonal worth and human values. Rational emotivebehavior therapy aims at increasing an individual's feelingsof self-worth and clearing the way for self-actualization byremoving the false beliefs that have been stumbling blocksto personal growth.
BECK'S COGNITIVE THERAPIES Beck's cognitive ther-apy approach was originally developed for the treatment ofdepression (see Chapter 7) and was later extended to anxi-ety disorders, eating disorders and obesity, conduct disor-der in children, personality disorders, and substance abuse(Beck, 2005; Beck & Emery, 1985; Beck et aI., 1990, 1993;Hollon & Beck, 2004). The cognitive model is basically aninformation-processing model of psychopathology. Abasic assumption of the cognitive model is that problemsresult from biased processing of external events or internalstimuli. These biases distort the way that a person makes

sense of the experiences that she or he has in the world,leading to cognitive errors.
But why do people make cognitive errors at all?According to Beck (2005), underlying these biases is a rela-tively stable set of cognitive structures or schemas thatcontain dysfunctional beliefs. When these schemasbecome activated (by external or internal triggers), theybias how people process information. In the case of depres-sion, people become inclined to make negatively biasedinterpretations of themselves, their world, and their future.
In the initial phase of cognitive therapy, clients aremade aware of the connection between their patterns ofthinking and their emotional responses. They are firsttaught simply to identify their own automatic thoughts(such as, "This event is a total disaster") and to keeprecords of their thought content and their emotional reac-tions (e.g., see Clark, 1997). With the therapist's help, theythen identify the logical errors in their thinking and learnto challenge the validity of these automatic thoughts. Theerrors in the logic behind their thinking lead them (1) toperceive the world selectively as harmful while ignoringevidence to the contrary; (2) to overgeneralize on the basisof limited examples-for example, seeing themselves astotally worthless because they were laid off from work;(3) to magnify the significance of undesirable events-forexample, seeing the job loss as the end of the worldfor them; and (4) to engage in absolutistic thinking-forexample, exaggerating the importance of someone's mildlycritical comment and perceiving it as proof of their instantdescent from goodness to worthlessness. In the followingcase study, the therapist describes some of these errors inthinking to a depressed patient.
THERAPIST: You have described many instances todaywhere your interpretations led to particularfeelings. Youremember when you were cryinga little while ago and I asked you what wasgoing through your mind? You told me thatyou thought that I considered you patheticand that I wouldn't want to see you for ther-apy. I said you were reading my mind andputting negative thoughts in my mind thatwere not, in fact, correct. Youwere making anarbitrary inference, or jumping to conclusionswithout evidence. This is what often happenswhen one is depressed. One tends to put themost negative interpretations on things, evensometimes when the evidence is contrary, andthis makes one even more depressed. Doyourecognize what Imean?
PATIENT: You mean even my thoughts are wrong?THERAPIST: No, not your thoughts in general, and Iam not
talking about right and wrong. As I wasexplaining before, interpretations are notfacts. They can be more or less accurate, butthey cannot be right or wrong. What Imean isthat some of your interpretations, in particularthose relating to yourself, are biased nega-tively. The thoughts you attributed to mecould have been accurate. But there were alsomany other conclusions you could havereached that might have been less depressingfor you, in that they would reflect less badly onyou. Forexample, you could have thought thatsince I was spending time with you, thatmeant Iwas interested and that Iwanted to tryand help. If this had been your conclusion,how do you think that you would have felt? Doyou think that you would have felt like crying?
PATIENT: Well, Iguess Imight have felt less depressed,more hopeful.
THERAPIST: Good. That's the point I was trying to make.We feel what we think. Unfortunately, thesebiased interpretations tend to occur automat-ically.They just pop into one's head and onebelieves them. What you and Iwill do in ther-apy is to try and catch these thoughts andexamine them. Together we will look at theevidence and correct the biases to make thethoughts more realistic. Does this sound allright with you?
PATIENT: Yes.
Source: From Cognitive Therapy for Depression and Anxiety:A Practitioner's Guide by Ivy-Marie Blackburn and Kate M.Davidson, copyright © 1995. Blackwell Science.
Much of the content of the therapy sessions and home-work assignments is analogous to experiments in which atherapist and a client apply learning principles to alter theclient's biased and dysfunctional cognitions, and continu-ously evaluate the effects that these changes have on subse-quent thoughts, feelings, and overt behavior. It is importantto note, however, that in Beck's cognitive therapy, clients donot change their beliefs by debate and persuasion as is com-mon in REBT. Rather, they are encouraged to gather infor-mation about themselves. For example, a young man whobelieves that his interest will be rebuffed by any woman heapproaches would be led into a searching analysis of thereasons why he holds this belief. The client might then beassigned the task of "testing" this dysfunctional "hypothe-sis" by actually approaching seemingly appropriate womenwhom he admires. The results of the "test" would then be

According to the cognitive model, how we think about situationsis closely linked to our emotional responses to them. If this youngman is having automatic thoughts such as, "I'llnever get to play.I'm such a loser," he is likely to be more emotionally distressedabout waiting on the sideline than if he has a thought such as,"There's a lot I can learn from watching how this game is going."
thoroughly analyzed with the cognitive therapist, and anycognitive "errors" that may have interfered with a skillfulperformance would be discussed and corrected.
In addition, the client is encouraged to discover thefaulty assumptions or dysfunctional schemas that may beleading to problem behaviors and self-defeating tenden-cies. These generally become evident over the course oftherapy as the client and the therapist examine the themesof the client's automatic thoughts. Because these dysfunc-tional schemas are seen as making the person vulnerable(e.g., to depression), this phase of treatment is consideredessential in ensuring resistance to relapse when the clientfaces stressful life events in the future. That is, if the under-lying cognitive vulnerability factors are not changed, theclient may show short-term improvement but will still besubject to recurrent depression.
For disorders other than depression, the generalapproach is quite similar. However, the nature of thepatient's automatic thoughts and underlying beliefs isobviously quite different across disorders. In panic disor-der, for example, the focus is on identifying the automaticthoughts about feared bodily sensations and on teachingthe client to "decatastrophize" the experience of panic(Clark, 1986; Clark, Salkovskis, et aI., 1994). In bulimia, thecognitive approach centers on the person's overvaluedideas about body weight and shape, which are often fueledby low self-esteem and fears of being unattractive. In addi-tion, faulty cognitions about which foods are "safe" andwhich "dangerous" are explored (Agras, 1993; Fairburn,Marcus, et aI., 1993; Wilson, 2005).
EVALUATING COGNITIVE-BEHAVIORAL THERAPIESIn spite of the widespread attention that Ellis's REBT has
enjoyed, little research attests to its efficacy, especially forcarefully diagnosed clinical populations. It appears to beinferior to exposure-based therapies in the treatment ofanxiety disorders such as agoraphobia, social phobia(Haaga & Davison, 1989, 1992), and probably obsessive-compulsive disorder (Franklin & Foa, 1998). In general, itmay be most useful in helping basically healthy people tocope better with everyday stress and perhaps in preventingthem from developing full-blown anxiety or depressivedisorders (Haaga & Davison, 1989, 1992).
In contrast, the efficacy of Beck's cognitive treatmentmethods has been well documented. Research suggeststhat these approaches are extremely beneficial in alleviat-ing many different types of disorders (see Hollon & Beck,2004). For depression, cognitive-behavioral therapy is atleast comparable to drug treatment for all but the mostsevere cases (e.g., psychotic depression). It also offers long-term advantages, especially with regard to the preventionof relapse (Craighead et al., 2002). Cognitive therapy pro-duces dramatic results in the treatment of panic disorderand generalized anxiety disorder (Hollon & Beck, 2004),and cognitive-behavioral therapy is now the treatment ofchoice for bulimia (Wilson & Fairburn, 2002; Wilson,2005). Finally, cognitive approaches have promise in thetreatment of conduct disorder in children (Hollon & Beck,2004), substance abuse (Beck et aI., 1993), and certain per-sonality disorders (Beck et aI., 1990; Linehan, 1993).
The combined use of cognitive and behavior therapyapproaches is now quite routine. Some disagreementremains about whether the effects of cognitive treatmentsare actually the result of cognitive changes, as the cognitivetheorists propose (Hollon & Beck, 2004; Jacobson et aI.,1996). At least for depression and panic disorder, it doesappear that cognitive change is the best predictor of long-term outcome, just as cognitive theory maintains (Hollonet aI., 1990). Exactly what the active ingredients of cogni-tive treatments really are, however, is now a focus of debateand research (e.g., Teasdale et aI., 2001; see also the Fall1997 issue of Behavior Therapy [vol. 28, no. 4]).
Humanistic-Experiential TherapiesThe humanistic-experiential therapies emerged as sig-nificant treatment approaches after World War II. In asociety dominated by self-interest, mechanization, com-puterization, mass deception, and mindless bureaucracy,proponents of the humanistic-experiential therapies seepsychopathology as stemming in many cases from prob-lems of alienation, depersonalization, loneliness, and afailure to find meaning and genuine fulfillment. Prob-lems of this sort, it is held, are not likely to be solvedeither by delving into forgotten memories or by correct-ing specific maladaptive behaviors.
The humanistic-experiential therapies are based onthe assumption that we have both the freedom and theresponsibility to control our own behavior-that we can

7.7 MotivationalInterviewing
~
s anyone who has considered therapyknows, people tend to be ambivalent aboutmaking changes in their lives. They want tochange, but they also don't want to change.Motivational Interviewing (MI;see Hettema
et aI., 2005) is a brief form of therapy that can be delivered inone or two sessions. Itwas developed as a way to help peo-ple resolve their ambivalence about change and make a com-mitment to treatment (Miller,1983). At its center is asupportive and empathic style of relating to the client thathas its origins in the work of Carl Rogers. However, MIdiffersfrom client-centered counseling because it also employs amore direct approach that explores the client's own reasonsfor wanting to change. The therapist encourages this "changetalk" by asking the client to discuss his or her desire, ability,reasons, and need for change. These are reflected back bythe therapist, thus exposing the client to periodic summariesof his or her own motivational statements and thoughtsabout change. The result is that clients can develop andstrengthen their commitment to change in an active, accept-ing, and supportive atmosphere.
Motivational Interviewing is most often used in theareas of substance abuse and addiction. When added tothe beginning of a treatment program, it appears to benefitpatients, perhaps because it facilitates patients' staying intreatment and following the treatment plan. Hettema andcolleagues' (2005) meta-analysis of the MI literature hasalso shown that MI has a large effect when it is used withethnic minorities. In one alcoholism-treatment trial, NativeAmerican participants did better if they received four ses-sions of MI than if they received 12 sessions of cognitive-behavior therapy or else participated in a 12-step program(Villanueva et aI., 2003). Quite possibly, the supportive andnonconfrontational style of MI may be more congruent withthe typical and culturally sanctioned communication styleof Native Americans and thus represent a culturally appro-priate intervention. As research continues, we will learnmore about the efficacy of this increasingly popular thera-peutic technique and gain knowledge about the kinds ofclients for whom it is most appropriate.
reflect on our problems, make choices, and take positiveaction. Humanistic-experiential therapists feel that a clientmust take most of the responsibility for the direction andsuccess of therapy, with the therapist serving merely ascounselor, guide, and facilitator. Although humanistic-experiential therapies differ in their details, their centralfocus is always expanding a client's "awareness."
CLIENT-CENTERED THERAPY The client-centered(person-centered) therapy of Carl Rogers (1902-1987)focuses on the natural power of the organism to heal itself(Rogers, 1951, 1961). Rogers saw therapy as a process ofremoving the constraints and restrictions that grow out ofunrealistic demands that people tend to place on them-selves when they believe, as a condition of self-worth, thatthey should not have certain kinds of feelings such as hos-tility. By denying that they do in fact have such feelings,they become unaware of their actual "gut" reactions. Asthey lose touch with their own genuine experience, theresult is lowered integration, impaired personal relation-ships, and various forms of maladjustment.
The primary objective of Rogerian therapy is toresolve this incongruence-to help clients become able toaccept and be themselves. To this end, client-centered ther-apists establish a psychological climate in which clients canfeel unconditionally accepted, understood, and valued aspeople. Within this context, the therapist employs non-
directive techniques such as empathic reflecting, or restate-ment of the client's descriptions of life difficulties. If allgoes well, clients begin to feel free, for perhaps the firsttime, to explore their real feelings and thoughts and toaccept hates and angers and ugly feelings as parts of them-selves. As their self-concept becomes more congruent withtheir actual experience, they become more self-acceptingand more open to new experiences and new perspectives;in short, they become better-integrated people.
In contrast to most other forms of therapy, the client-centered therapist does not give answers, interpret what aclient says, probe for unconscious conflicts, or even steerthe client toward certain topics. Rather, he or she simply lis-tens attentively and acceptingly to what the client wants totalk about, interrupting only to restate in different wordswhat the client is saying. Such restatements, devoid of anyjudgment or interpretation by the therapist, help the clientto clarify further the feelings and ideas that he or she isexploring-really to look at them and acknowledge them.
Pure client-centered psychotherapy, as originallypracticed, is rarely used today in North America, althoughit is still relatively popular in Europe. Motivational Inter-viewing is a new form of therapy that is based on thisempathic style (see Developments in Practice 17.7). Thefollowing excerpt from a therapist's second interview witha young woman will serve to illustrate these techniques ofreflection and clarification.

ALICE: I was thinking about this business of stan-dards. I somehow developed a sort of aknack, I guess, of-well-habit-of tryingto make people feel at ease around me, orto make things go along smoothly....
COUNSELOR: In other words, what you did was always inthe direction of trying to keep things smoothand to make other people feel better and tosmooth the situation.
ALICE: Yes. I think that's what it was. Nowthe rea-son why I did it probably was-I mean, notthat I was a good little Samaritan goingaround making other people happy, but thatwas probably the role that felt easiest forme to play. I'd been doing it around home somuch. Ijust didn't stand up for my own con-victions, until I don't know whether I haveany convictions to stand up for.
COUNSELOR: You feel that for a long time you've beenplaying the role of kind of smoothing out thefrictions or differences or what not.
ALICE: M-hm.COUNSELOR: Rather than having any opinion or reaction
of your own in the situation. Is that it?ALICE: That's it. Or that I haven't been really hon-
estly being myself, or actually knowing whatmy real self is, and that I've been just play-ing a sort of a false role. Whatever role noone else was playing, and that needed to beplayed at the time, I'd try to fill it in.
(FromRogers, 1951, pp. 152-53.)
GESTALT THERAPY In German, the term gestalt means"whole," and gestalt therapy emphasizes the unity of mindand body-placing strong emphasis on the need to inte-grate thought, feeling, and action. Gestalt therapy wasdeveloped by Frederick (Fritz) Perls (1969) as a means ofteaching clients to recognize the bodily processes and emo-tions they had been blocking off from awareness. As withthe client-centered and humanistic approaches, the maingoal of gestalt therapy is to increase the individual's self-awareness and self-acceptance.
Although gestalt therapy is commonly used in a groupsetting, the emphasis is on one person at a time, with whoma therapist works intensively, trying to help identify aspectsof the individual's self or world that are not being acknowl-edged in awareness. The individual may be asked to act outfantasies concerning feelings and conflicts or to representone side of a conflict while sitting in one chair and thenswitch chairs to take the part of the adversary. Often the
therapist or other group members will ask such questionsas, "What are you aware of in your body now?" and "Whatdoes it feel like in your gut when you think of that?"
In Perls' approach to therapy, a good deal of attentionis also paid to dreams, but with an emphasis very differentfrom that of classical psychoanalysis. In gestalt theory, allelements of a dream, including seemingly inconsequen-tial, impersonal objects, are considered to be representa-tions of unacknowledged aspects of the dreamer's self.The therapist urges the client to suspend normal criticaljudgment, to "be" the object in the dream, and then toreport on the experience. This is illustrated in the follow-ing case study.
A college professor and therapist was preoccupied withhis academic promotion and tenure and found himselfunable to experience any joy.Hesought the assistance ofa friend who was a gestalt therapist. She asked him toconjure up a daydream, rather than a dream. The day-dream that emerged spontaneously was one of skiing.The therapist asked him to be the mountain, and hebegan to experience how warm he was when he was athis base. As he got closer to the top, what looked sobeautiful was also very cold and frozen. The therapistasked the professor to be the snow, and he experiencedhow hard and icy he could be near the top. But near thebottom, people ran over him easily and wore him out.When the session was finished, the professor did not feellike crying or shouting; he felt like skiing. So he went,leaving articles and books behind. In the sparkle of thesnow and sun, he realized that joy in living emergesthrough deeds and not through words. In his rush to suc-ceed, he had committed one of the cardinal sins againsthimself-the sin of not being active. (Adapted from Pro-chaska & Norcross, 2003, p. 183.)
PROCESS-EXPERIENTIAL THERAPY Process-experi-ential (PE) therapy is a relatively new treatment approachthat combines client-centered therapy and gestalt therapy.Developed by Greenberg and his colleagues, (see Green-berg, 2004) this treatment emphasizes the experiencing ofemotions during therapy. Clients are also asked to reflecton their emotions and are encouraged to create meaningfrom them (see Elliot et al., 2004). The therapist plays amore active role than in pure client-centered therapy andmay work to guide the patient to experience emotionsmore vividly through a variety of different techniques. Likeother humanistic-experiential therapies, the relationshipwith the therapist is regarded as extremely important andthe vehicle through which progress in treatment is made.

EVALUATING HUMANISTIC-EXPERIENTIAL THERA-PIES Many of the humanistic-experiential concepts-the uniqueness of each individual, the importance oftherapist genuineness, the satisfaction that comes fromrealizing one's potential, the importance of the search formeaning and fulfillment, and the human capacity forchoice and self-direction-have had a major impact on ourcontemporary views of both human nature and the natureof good psychotherapy.
However, humanistic-experiential therapies have beencriticized for their lack of agreed-upon therapeutic proce-dures, and their vagueness about what is supposed to hap-pen between client and therapist. In response, proponentsof such approaches argue against reducing people toabstractions, which can diminish their perceived worthand deny their uniqueness. Because people are so different,they argue, we should expect different techniques to beappropriate for different cases.
Controlled research on the outcomes achieved bymany forms of humanistic-existential therapy was lackingin the past. However, research in this area is now on theincrease. As the number of controlled-outcome studiesgrows, there is evidence to suggest that these treatmentapproaches are helpful for patients with a variety of prob-lems including depression, anxiety, trauma, and maritaldifficulties (Elliot et aI., 2004).
Psychodynamic TherapiesPsychodynamic therapy is a treatment approach thatfocuses on individual personality dynamics, usually from apsychoanalytic or some psychoanalytically derived per-spective (see Chapter 3). Psychoanalytic therapy is the old-est form of psychological therapy and began with SigmundFreud. The therapy is mainly practiced in two basic forms:classical psychoanalysis and psychoanalytically orientedpsychotherapy. As developed by Freud and his immediatefollowers, classical psychoanalysis is an intensive (at leastthree sessions per week), long-term procedure for uncov-ering repressed memories, thoughts, fears, and conflictspresumably stemming from problems in-early psychosex-ual development-and helping individuals come to termswith them in light of the realities of adult life. For example,excessive orderliness and a grim and humorless focus onrigorous self-control would probably be viewed as derivingfrom difficulties in early toilet training.
In psychoanalytically oriented psychotherapy, thetreatment and the ideas guiding it may depart substantiallyfrom the principles and procedures laid out by orthodoxFreudian theory, yet the therapy is still loosely based onpsychoanalytic concepts. For example, many psychoana-lytically oriented therapists schedule less frequent sessions(e.g., once per week) and sit face-to-face with the clientinstead of having the latter recline on a couch with the ana-lyst out of sight behind him or her. Likewise, the relativelypassive stance of the analyst (primarily listening to the
client's "free associations" and rarely offering "interpreta-tions") is replaced with an active conversational style inwhich the therapist attempts to clarify distortions and gapsin the client's construction of the origins and conse-quences of his or her problems, thus challenging client"defenses" as they present themselves. It is widely believedthat this more direct approach significantly shortens totaltreatment time. We will first examine Freud's originaltreatment methods, in part because of their historical sig-nificance and enormous influence; we will then lookbriefly at some of the contemporary modifications of psy-chodynamic therapy, which for the most part focus oninterpersonal processes. Before we do so, however, let'sconsider the case of Karen.
Karen was about to be terminated from her nursing pro-gram if her problems were not resolved. She had alwaysbeen a competent student who seemed to get along wellwith peers and patients. Now, since the beginning of herrotation on 3 South, a surgical ward, she was plagued byheadaches and dizzy spells. Of more serious consequencewere the two medical errors she had made when dispens-ing medications to patients. She realized that these errorscould have proved fatal, and she was as concerned as hernursing faculty about why such problems had begun inthis final year of her education. Karen knew she had manynegative feelings toward the head nurse on 3 South, butshe did not believe these feelings could account for hercurrent dilemma. She entered psychotherapy.
After a few weeks of psychotherapy, the therapistrealized that one of Karen's important conflicts revolvedaround the death of her father when she was 12 years old.Karen had just gone to live with her father after being withher mother for 7 years. She remembered how upset shewas when her father had a heart attack and had to berushed to the hospital. For a while it looked as though herfather was going to pull through, and Karen began enjoy-ing her daily visits to see him. During one of these visits,her father clutched his chest in obvious pain and toldKaren to get a nurse. She remembered how helpless shefelt when she could not find a nurse, although she did notrecall why this was so difficult. Her search seemed end-less, and by the time she finally found a nurse, her fatherwas dead.
The therapist asked Karen the name of the ward onwhich her father had died. She paused and thought, andthen she blurted out, "3 South." She cried at length asshe told how confused she was and how angry she felttoward the nurses on the ward for not being more readilyavailable, although she thought they might have been

involved with another emergency. After weeping andshaking and expressing her resentment, Karen felt calmand relaxed for the first time in months. Her symptomsdisappeared, and her problems in the nursing programwere relieved. (Adapted from Prochaska & Norcross,2003, p. 28.)
FREUDIAN PSYCHOANALYSIS Psychoanalysis is a sys-tem of therapy that evolved over a period of years duringFreud's long career. Psychoanalysis is not easy to describe,and the problem is complicated by the fact that many peo-ple have inaccurate conceptions of it based on cartoonsand other forms of caricature. The best way to begin ourdiscussion is to describe the four basic techniques of thisform of therapy: (1) free association, (2) analysis ofdreams, (3) analysis of resistance, and (4) analysis of trans-ference. Then we will note some of the most importantchanges that have taken place in psychodynamic therapysince Freud's time.
Free Association The basic rule of free association isthat an individual must say whatever comes into his or hermind, regardless of how personal, painful, or seeminglyirrelevant it may be. Usually a client lies in a relaxed posi-tion on a couch and gives a running account of all thethoughts, feelings, and desires that come to mind as oneidea leads to another. The therapist normally takes a posi-tion behind the client so as not to disrupt the free flow ofassociations in any way.
Although such a running account of whatever comesinto one's mind may seem random, Freud did not view it assuch; rather, he believed that associations are determinedjust like other events. The purpose of free association is toexplore thoroughly the contents of the preconscious-thatpart of the mind considered subject to conscious attentionbut largely ignored. Analytic interpretation involves a ther-apist's tying together a client's often disconnected ideas,beliefs, and actions into a meaningful explanation to helpthe client gain insight into the relationship between his orher maladaptive behavior and the repressed (unconscious)events and fantasies that drive it.
Analysis of Dreams Another important, related proce-dure for uncovering unconscious material is the analysis ofdreams. When a person is asleep, repressive defenses aresaid to be lowered, and forbidden desires and feelings mayfind an outlet in dreams. For this reason, dreams have beenreferred to as the "royal road to the unconscious." Somemotives, however, are so unacceptable to an individual thateven in dreams they are not revealed openly but areexpressed in disguised or symbolic form. Thus a dream hastwo kinds of content: (1) manifest content, which is thedream as it appears to the dreamer, and (2) latent content,
which consists of the actual motives that are seekingexpression but that are so painful or unacceptable that theyare disguised.
It is a therapist's task, in conjunction with the associa-tions of the patient, to uncover these disguised meaningsby studying the images that appear in the manifest contentof a client's dream and in the client's associations to them.For example, a client's dream of being engulfed in a tidalwave may be interpreted by a therapist as indicating thatthe client feels in danger of being overwhelmed by inade-quately repressed fears and/or hostilities.
Analysis of Resistance During the process of free asso-ciation or of associating to dreams, an individual may evi-dence resistance-an unwillingness or inability to talkabout certain thoughts, motives, or experiences (Strean,1985). For example, a client may be talking about animportant childhood experience and then suddenly switchtopics, perhaps stating, "It really isn't that important" or "Itis too absurd to discuss." Resistance may also be evidencedby the client's giving a too-glib interpretation of someassociation, or coming late to an appointment, or even"forgetting" an appointment altogether. Because resistanceprevents painful and threatening material from enteringawareness, its sources must be sought if an individual is toface the problem and learn to deal with it in a realisticmanner.
Analysis of Transference As client and therapist inter-act, the relationship between them may become complexand emotionally involved. Often people carryover, andunconsciously apply to their therapist, attitudes and feel-ings that they had in their relations with a parent or otherperson close to them in the past, a process known astransference. Thus clients may react to their analyst asthey did to that earlier person and feel the same love, hos-tility, or rejection that they felt long ago. If the analyst isoperating according to the prescribed role of maintainingan impersonal stance of detached attention, the oftenaffect-laden reactions of the client can be interpreted, it isheld, as a type of projection-inappropriate to the presentsituation, yet highly revealing of central issues in theclient's life. For example, should the client vehemently (butinaccurately) condemn the therapist for a lack of caringand attention to the client's needs, this would be seen as a"transference" to the therapist of attitudes acquired (possi-bly on valid grounds) in childhood interactions with par-ents or other key individuals.
In helping the client to understand and acknowledgethe transference relationship, a therapist may provide theclient with insight into the meaning of his or her reactionsto others. In doing so, the therapist may also introduce acorrective emotional experience by refusing to engage theperson on the basis of his or her unwarranted assump-tions about the nature of the therapeutic relationship. Ifthe client expects rejection and criticism, for example, the

therapist is careful to maintain a neutral manner. Or con-trarily, the therapist may express positive emotions at apoint where the client feels particularly vulnerable,thereby encouraging the client to reframe and rethink heror his view of the situation. In this way it may be possiblefor the individual to recognize these assumptions and to"work through" the conflict in feelings about the real par-ent or perhaps to overcome feelings of hostility and self-devaluation that stemmed from the earlier parentalrejection. In essence, the negative effects of an undesirableearly relationship are counteracted by working through asimilar emotional conflict with the therapist in a thera-peutic setting. A person's reliving of a pathogenic pastrelationship in a sense re-creates the neurosis in real life,and therefore this experience is often referred to as atransference neurosis.
It is not possible here to consider at length the com-plexities of transference relationships, but a client's atti-tudes toward his or her therapist usually do not followsuch simple patterns as our examples suggest. Often theclient is ambivalent-distrusting the therapist and feelinghostile toward him or her as a symbol of authority, but atthe same time seeking acceptance and love. In addition, theproblems of transference are not confined to the client, forthe therapist may also have a mixture of feelings towardthe client. This counter-transference, wherein the thera-pist reacts in accord with the client's transferred attribu-tions rather than objectively, must be recognized andhandled properly by the therapist. For this reason, it is con-sidered important that therapists have a thorough under-standing of their own motives, conflicts, and "weak spots";in fact, all psychoanalysts undergo psychoanalysis them-selves before they begin independent practice.
The resolution of the transference neurosis is said to bethe key element in effecting a psychoanalytic "cure." Suchresolution can occur only if an analyst successfully avoidsthe pitfalls of counter-transference. That is, the analystneeds to keep track of his or her own transference or reac-tion to a client's behavior. Failure to do so risks merelyrepeating, in the therapy relationship, the typical relation-ship difficulties characterizing the client's adult life.Analysisof transference and the phenomenon of counter-transfer-ence are also part of most psychodynamic derivatives ofclassical psychoanalysis, to which we now turn.
Psychodynamic Therapy since Freud The originalversion of psychoanalysis is practiced only rarely today.Arduous and costly in time, money, and emotional com-mitment, it may take several years before all major issues inthe client's life have been satisfactorily resolved. In light ofthese heavy demands, psychoanalytic/psychodynamictherapists have worked out modifications in proceduredesigned to shorten the time and expense required. A goodreview of some of these approaches can be found in Pro-chaska and Norcross (2003).
INTERPERSONAL THERAPY (lPT) Contemporary psy-chodynamic approaches to therapy tend to have a stronglyinterpersonal focus. They emphasize, in other words, whattraditional Freudians would consider transferential andcounter-transferential phenomena, extending these con-cepts to virtually all of a disturbed person's relationships,rather than considering them only in the treatment situa-tion. Interpersonal therapy was first articulated in thiscountry by Harry Stack Sullivan (see Chapter 3). Its centralidea is that all of us, at all times, involuntarily invokeschemas acquired from our earliest interactions with oth-ers, such as our parents, in interpreting what is going on inour current relationships. Where those earlier relation-ships have had problematic features such as rejection orabuse, the "introjected" characteristics of those earlierinteraction partners may distort in various ways the indi-vidual's ability to process accurately and objectively theinformation contained in current interpersonal transac-tions. Thus the formerly abused or rejected person maycome to operate under the implicit (unconscious) assump-tion that the world is generally rejecting and/or abusive.The mistrust stemming from this belief is bound to affectcurrent relationships negatively. In the worst instances itmay even lead (because of the reactions of others to theclient's wariness, reticence, or counteraggression) to a fur-ther confirmation that the world is a nasty if not a danger-ous place-an instance of self-fulfilling prophecy (e.g., seeCarson, 1982; Wachtel, 1993).
OBJECT RELATIONS, SELF-PSYCHOLOGY, AND OTHERINTERPERSONAL VARIATIONS The most extensiverevisions of classical psychoanalytic theory undertakenwithin recent decades have been related to the object-relations perspective (in psychoanalytic jargon, "objects"are other people) and, to a lesser extent, the attachmentand self-psychology perspectives (see Chapter 3; also seeProchaska & Norcross, 2003). Whether or not psychother-apy investigators and clinicians use the term object rela-tions (or attachment or self-psychology) to denote theirapproach, increasing numbers of them describe proce-dures that focus on interpersonal relationship issues, par-ticularly as they play themselves out in the client-therapistrelationship (e.g., Benjamin, 1996; Frank & Spanier, 1995;Kiesler, 1996; Klerman et aI., 1984; Strupp & Binder, 1984).
The greatest contribution of the interpersonalapproach may be its role in the developing movementtoward "integration" of the various forms of therapy.Numerous contemporary investigators and clinicians (e.g.,Beutler, 1992; Blatt et aI., 1996; Lazarus, 1997a, 1997b;Linehan, 1993; Safran, 1990a, 1990b; Wachtel, 1997) havepointed to the many ways in which interpersonal issuesplaya central role in psychodynamic, behavioral, cogni-tive, and even psychopharmacological therapies.
Interpersonally oriented psychodynamic therapistsvary considerably in their time focus: whether they concen-

trate on remote events of the past, on current interpersonalsituations and impasses (including those of the therapyitself), or on some balance of the two. Most seek to expose,bring to awareness, and modify the effects of the remotedevelopmental sources of the difficulties the client is cur-rently experiencing. These therapies generally retain, then,the classical psychoanalytic goal of understanding the pres-ent in terms of the past. What they ignore are the psycho-analytic notions of staged libidinal energy transformationsand of entirely internal (and impersonal) drives that arechanneled into psychopathological symptom formation.
EVALUATING PSYCHODYNAMIC THERAPY Classicalpsychoanalysis is routinely criticized by outsiders for beingrelatively time-consuming and expensive; for being basedon a questionable, stultified, and sometimes cult-likeapproach to human nature; for neglecting a client's imme-diate problems in the search for unconscious conflicts inthe remote past; and for there being no adequate proof ofits general effectiveness. Concerning this, we note thatthere have been no rigorous, controlled outcome studies ofclassical psychoanalysis. This is understandable, given theintensive and long-term nature of the treatment and themethodological difficulties inherent in testing such anapproach. Nonetheless, there are some promising but pre-liminary hints that this treatment approach has some value(Gabbard et aI., 2002). Psychoanalysts also argue that man-ualized treatments unduly limit treatment for a disorder.They note that simply because a treatment cannot bestandardized does not mean that it is invalid or unhelp-ful.Whether the clinical benefits justify the time andexpense of psychoanalysis, however, remains uncertain.
In contrast, there is much more research on some ofthe newer psychodynamically oriented approaches,although research showing that this form of therapy worksfor specific diagnoses is still generally lacking. Andersonand Lambert (1995) have published a useful summary,involving quantitative analysis, of 26 efficacy studies ofbrief psychodynamic psychotherapy. In general, thedemonstrated results of this type of therapy are quiteimpressive. We would single out in particular the interper-sonal therapy model developed by Klerman and associates(1984), originally targeted for the problem of depression,where it has demonstrable value (de Mello et aI., 2005). Ithas also been shown to be a promising treatment forbulimia nervosa (Fairburn, Jones, et aI., 1993).
Marital and Family TherapyMany problems brought to practitioners are explicitly rela-tionship problems. A common example is couples or mar-ital distress. The maladaptive behavior in these instances isshared between the members of the relationship. Extend-ing the focus even further, a family systems approachreflects the assumption that the within-family behavior of
any particular family member is subject to the influence ofthe behaviors and communication patterns of other familymembers. It is, in other words, the product of a "system"that may be amenable to both understanding and change.Addressing problems deriving from the in-place systemthus requires therapeutic techniques that focus on rela-tionships as much as, or more than, on individuals.
MARITAL THERAPY The large numbers of couples seek-ing help with relationship problems have made couplescounseling a growing field of therapy. Typically the coupleis seen together, and improving communication skills anddeveloping more adaptive problem-solving styles are botha major focus of clinical attention. Although it is quite rou-tine at the start of couples therapy for each partner secretlyto harbor the idea that only the other will have to do thechanging (e.g., Cordova & Jacobson, 1993), it is nearlyalways necessary for both partners to alter their reactionsto the other.
For many years the gold standard of marital therapyhas been traditional behavioral couple therapy (TBCT;see Christensen & Heavey, 1999). TBCT is based on asocial-learning model and views marital satisfaction andmarital distress in terms of reinforcement. The treatmentis usually short-term (10 to 26 sessions) and is guided by amanual. The goal of TBCT is to increase caring behaviorsin the relationship and to teach partners to resolve theirconflicts in a more constructive way through training incommunication skills and adaptive problem solving.
Research has established TBCT as an empirically sup-ported treatment for marital distress (for a review ofnumerous outcome studies, see Christensen & Heavey,1999). Approximately two-thirds of couples do well andshow improvement in relationship satisfaction (Jacobsonet aI., 1987). However, this form of treatment does not workfor all couples (Jacobson & Addis, 1993). Moreover, evenamong couples who show an improvement in relationship
Marital therapists try to help couples improve theircommunication skills and develop more adaptive ways ofsolving their problems.

satisfaction, the improvement may not be maintained overtime (Jacobson et al., 1987).
The limitations of TBCT have led researchers to con-clude that a change-focused treatment approach is notappropriate for all couples. This, in turn, has led to thedevelopment of integrative behavioral couple therapy(IBCT; see Jacobson et aI., 2000; Wheeler et aI., 2001).Instead of emphasizing change (which sometimes has theparadoxical effect of making people not want to change),IBCT focuses on acceptance and includes strategies thathelp each member of the couple come to terms with andaccept some of the limitations of his or her partner. Ofcourse, change is not forbidden. Rather, within IBCT,acceptance strategies are integrated with change strategiesto provide a form of therapy that is more tailored to indi-vidual characteristics and the needs of the couple.
Although this is a new development in the maritaltherapy field, the preliminary findings are quite promising.In one study, improvement rates were 80 percent in thecouples treated with IBCT versus 64 percent in couplesreceiving TBCT (Jacobson et aI., 2000).
FAMILY THERAPY Therapy for a family obviously over-laps with couples and marital therapy but has somewhatdifferent roots. Whereas marital therapy developed inresponse to the large number of clients who came for assis-tance with couples problems, family therapy began withthe finding that many people who had shown markedimprovement in individual therapy-often in institutionalsettings-had a relapse when they returned home. As youhave already learned from Chapters 7 and 14, family-basedtreatment approaches designed to reduce high levels ofcriticism and family tension have been successful in reduc-ing relapse rates in patients with schizophrenia and mooddisorders (Miklowitz, 2002; Pilling et aI., 2002).
Another approach to resolving family disturbances iscalled structural family therapy (Minuchin, 1974). Thisapproach, which is based on systems theory, holds that ifthe family context can be changed, then the individualmembers will have altered experiences in the family andwill behave differently in accordance with the changedrequirements of the new family context. Thus an impor-tant goal of structural family therapy is changing the orga-nization of the family in such a way that the familymembers will behave more supportively and less patho-genically toward each other.
Structural family therapy is focused on present inter-actions and requires an active but not directive approachon the part of a therapist. Initially, the therapist gathersinformation about the family-a structural map of thetypical family interaction patterns-by acting like one ofthe family members and participating in the family inter-actions as an insider. In this way, the therapist discoverswhether the family system has rigid or flexible boundaries,who dominates the power structure, who gets blamedwhen things go wrong, and so on. Armed with this under-
standing, the therapist then operates as an agent for alter-ing the interaction among the members, which often hastransactional characteristics of enmeshment (overinvolve-ment), overprotectiveness, rigidity, and poor conflict reso-lution skills. The "identified client" is often found to playan important role in the family's mode of conflict avoid-ance. As discussed in Chapter 9, structural family therapyhas quite a good record of success in the treatment ofanorexia nervosa (see Lock et aI., 2001).
Eclecticism and IntegrationThe various "schools" of psychotherapy that we have justdescribed used to stand more in opposition to one anotherthan they do now. Today, clinical practice is characterized bya relaxation of boundaries and a willingness on the part oftherapists to explore differing ways of approaching clinicalproblems (see Castonguay et aI., 2003, for a discussion), aprocess sometimes called multimodal therapy (Lazarus,1981, 1985, 1997a). When asked what their orientation is,most psychotherapists today reply "eclectic;' which usuallymeans that they try to borrow and combine concepts andtechniques from various schools, depending on what seemsbest for the individual case. This inclusiveness even extendsto efforts to combine individual and family therapies (e.g.,Feldman, 1992; E.Wachtel, 1994) and to combine biologicaland psychosocial approaches (e.g., Feldman & Feldman,1997; KIerman et aI., 1994; Pinsof, 1995).
In ReVIew~ Describe the different techniques that can be
used to provide anxious patients withexposure to the stimuli they fear.
~ In what ways are RESTand cognitive therapysimilar? In what ways are they different?
~ Explain the concepts of transference andcounter-transference.
~ What special difficulties do clinicians facewhen they work with couples? How havetechniques of marital therapy evolved overrecent years?
PSYCHOTHERAPY ANDSOCIETYThe criticism has been raised-from both inside and out-side the mental health professions-that psychotherapycan be viewed as an attempt to get people adjusted to a

"sick" society rather than to encourage them to worktoward its improvement. As a consequence, psychother-apy has often been considered the guardian of the statusquo. This issue is perhaps easier for us to place in perspec-tive by looking at other cultures. For example, there hadbeen frequent allegations that psychiatry was used as ameans of political control in the former Soviet Union, anabuse that was eventually officially acknowledged (seeSchizophrenia Bulletin, 1990, vol. 16, no. 4). Although fewwould claim that psychiatry in most industrialized soci-eties is used to gain control over social critics, there is nev-ertheless the possibility that therapists in some ways playthe role of "gatekeepers" of social values. Such charges, ofcourse, bring us back to the question we raised in Chapter1:What do we mean by "abnormal"? That question can beanswered only in the light of our values.
Social Values and PsychotherapyIn a broader perspective, there is the complex and con-troversial issue of the role of values in science. Psy-chotherapy is not, or at least should not be, a system ofethics; it is a set of tools to be used at the discretion of atherapist in pursuit of a client's welfare. Thus mentalhealth professionals are confronted with the same kindsof questions that confront scientists in general: Should aphysical scientist who helps develop weapons of massdestruction be morally concerned about how they areused? Similarly, should a psychologist or behavioral sci-entist who develops powerful techniques to influence orcontrol how people behave be concerned about howthose techniques are used?
Many psychologists and other scientists try to sidestepthis issue by insisting that science is value-free-that it isconcerned only with gathering facts, not with how they areapplied. Each time therapists decide that one behaviorshould be eliminated or substituted for another, however,they are making a value judgment. For example, is a thera-pist to assume that the depression of a young mother whois abused by an alcoholic husband is an internally baseddisorder requiring "treatment," as once would have beenthe routine interpretation? Or does the therapist have alarger responsibility to look beyond individual pathologyand confront the abnormality of the marital relationship?Therapy takes place in a context that involves the values ofthe therapist, the client, and the society in which they live.There are strong pressures on a therapist-from parents,schools, courts, and other social institutions-to help peo-ple adjust to the world as it is. At the same time, there aremany counterpressures, particularly from young peoplewho are seeking support in their (sometimes overdone)attempts to become authentic people rather than blindconformists.
The dilemma in which contemporary therapistsmay find themselves is illustrated by the following casestudy.
;-j Who Needs Therapy?
A ls-year-old high school sophomore is sent to a thera-pist because her parents have discovered that she hasbeen having sexual intercourse with her boyfriend. Thegirl tells the therapist that she thoroughly enjoys suchrelations and feels no guilt or remorse over her behavior,even though her parents strongly disapprove. In addition,she reports that she is quite aware of the danger ofbecoming pregnant and is careful to take contraceptivemeasures.
What is the role of the therapist in such a case? Shouldthe girl be encouraged to conform to her parents' expecta-tions and postpone sexual activity until she is older andmore mature? Or should the parents be helped to adjust tothe pattern of sexual behavior their daughter has chosen?What should be the therapist's goal? As we noted earlier, itis not unusual for individuals to be referred for psycholog-ical treatment because their behavior, though not particu-larly destructive or disturbing, has caused concern amongfamily members, who want the therapist to "fix" them.
Psychotherapy and Cultural DiversityAs we have seen, the establishment and maintenance of aneffective psychotherapeutic "working alliance" betweenclient and therapist is generally regarded as a crucial andindispensable element in determining the success of theoutcome. What does this mean for a client whose back-ground is considerably different from that of the therapist?
As yet, there is little or no solid evidence that psy-chotherapeutic outcomes are diminished when client andtherapist differ in race or ethnicity (Beutler et al., 2004; Sueet aI., 1994)_ However, members of minority groups areseriously underrepresented in treatment research studies,and this makes it difficult to fully assess their needs andoutcomes (Miranda et aI., 2005; Nagayama Hall, 2001).Moreover, racial and ethnic minorities are clearly under-served by the mental health system (Snowden & Yamada,2005; U.S. Department of Health and Human Services,2001). However, the factors that are behind these dispari-ties are complex and not well understood.
Many minorities are economically disadvantagedand simply do not have the health insurance they need toseek treatment. It is also difficult for patients to find thekind of therapists they want. In general, minority patientstend to prefer ethnically similar therapists over European-American therapists (Coleman, et aI., 1995). Mexican-Americans state a strong preference for therapists whoshare their ethnic background and express the view that

such therapists are more "credible" than Anglo therapistswould be (Lopez et al., 1991; Ponce & Atkinson, 1989).However, finding an ethnically matched therapist may pre-sent difficulties. In one survey, for example, only 2 percentof psychiatrists, 2 percent of psychologists, and 4 percentof social workers said they were African-Americans(Holzer et al., 1998). The number of mental health profes-sionals who are representative of other minority groups isno better (US. Department of Health and Human Ser-vices, 2001). The lack of trained therapists familiar withthe issues important to different ethnic groups is a seriousdrawback, given the unique problems often associatedwith certain groups. This is illustrated in the followingcase, which concerns a Southeast Asian refugee woman inher mid-forties who was relocated to the United States.
"I lost my husband, I lost my country, I lost every prop-erty/fortune we owned. And coming over here, I can'tlearn to speak English and the way of life here is different;my mother and oldest son are very sick: I feel crippled,I can do nothing. I can't control what's going on. I don'tknow what I'm going to do once my public assistanceexpires. 1may feel safe in a way-there is no war here, noCommunist to kill or torture you-but deep down insideme, I still don't feel safe or secure. I get scared. I getscared so easily." (From Rumbaut, 1985, p. 475.)
When specialized, ethnically focused mental healthprograms are made available in community settings,minority clients are less likely to drop out of treatment andoften do well (Snowden & Yamada, 2005). However, suchprograms are still lacking in many comm unities. Also lack-ing are research investigations designed to understandhow culture and ethnicity affect a person's ability to accessand receive psychiatric and psychological treatments.Although special funding initiatives do exist, this is still anarea of research in need of much more attention andactivity.
IIIReVIeW~ Can psychotherapy ever be value-free? Why
or why not?
~ What special issues do racial and ethnicminorities face when they seek therapy?

any researchers, especially those whoconduct clinical trials of drugs, receivemoney, directly from the pharmaceuticalindustry, to conduct their studies. Someacademic researchers in medical schools
and universities receive grants from drug companies. Otherclinical investigators are actually employed by the drug com-panies themselves. Clinical investigators often also haveother links to the pharmaceutical industry. For example, theymay own stock in the company whose drug they are studying.They may also serve as consultants for drug companies orreceive speaking fees from them.
Do such financial conflicts of interest have any implica-tions for the results of the clinical trials that these researchersconduct? Interest in this issue escalated after Jesse Gelsinger, ateenager, died after he participated in a University of Pennsyl-vania study that was led by a researcher with a financial inter-est in the company that was sponsoring the research (seeBodeneheimer, 2000). Although some argue that researcherswith financial ties to drug companies remain independent andobjective collectors of data, others believe that such ties maysubtly influence scientific judgment, leading to bias in the find-ings that are reported (Angell, 2000; Stossel, 2005).
In an examination of this issue, Perlis and colleagues(2005) looked at all the clinical drug trials that were reportedin four of the most prestigious psychiatry journals betweenJanuary 2001 and December 2003. They noted who fundedthe study and also determined whether authors reportedfinancial conflicts of interest such as being employed by thedrug company or owning stock in it. They then looked at theresults of the clinical trials that were published.
It is noteworthy that the majority (60 percent) of the clin-ical trials were funded by the pharmaceutical industry. Finan-cial conflicts of interest were also quite common (47 percentof studies). The central question, however, is whether either
~ Psychological treatment is aimed at reducingabnormal behavior in individuals throughpsychological means. The goals of psychotherapyinclude changing maladaptive behavior, minimizingor eliminating stressful environmental conditions,reducing negative affect, improving interpersonalcompetencies, resolving personal conflicts, modifyingpeople's inaccurate assumptions about themselves,and fostering a more positive self-image.
of these factors was associated with the likelihood that theauthors reported a positive finding (Le., drug better thanplacebo) for their study.
Perlis and colleagues' findings (2005) showed that thechances of a positive finding were not associated with whofunded the clinical trial. In other words, receiving financial sup-port from a drug company to do the study did not make it morelikely that the drug would be reported as performing betterthan the placebo. However, there was an association betweenauthor conflict of interest and positive results. Specifically,when at least one author had a financial interest in the com-pany, the odds of positive findings being reported were 4.9times greater than when there was no conflict of interest.
How can the link between author conflict of interest andthe outcome of the clinical trial be explained? One possibilityis that the most senior and experienced investigators werealso those who served as consultants for the drug compa-nies, and perhaps these senior investigators also designedbetter clinical trials that yielded positive findings. But thenagain, perhaps authors with an interest in the company mighthave been more inclined to use research designs that couldhave favored the drug produced by their sponsors. Authorswith financial conflicts of interest might also have been lessinclined to publish negative findings that did not show thedrug of their sponsors to be superior to placebo.
What are the implications here? At the very least, thesefindings validate the current practice of journals' requiringauthors to disclose any financial links they have with indus-try. The findings also support calls for all clinical trials to beregistered so that the results have to be reported regardlessof whether they are positive or negative (Meier, 2004).
Finally, these results raise the possibility that there may besubtle factors operating to undermine the objectivity of sci-entific researchers, perhaps even without them being fullyaware of this.
~ Although these goals are by no means easy toachieve, psychological treatment methods have beenshown to be generally effective in promoting adaptivepsychological functioning in many troubled people.
~ Medications are also important in the treatment ofmany disorders. It is now common clinical practiceto combine medication and psychologicaltreatments.

~ Some of the earlier antidepressant medications (e.g.,tricyclics and monoamine oxidase inhibitors) havenow been replaced by SSRls and SNRls. In general,antidepressants work through their influence on theserotonin and norepinephrine neurotransmittersystems.
~ The most commonly used antipsychotic medicationsare the atypical neuroleptics. These improve bothpositive and negative symptoms and have fewerextrapyramidal symptoms (unwanted side effectsinvolving movement) than conventional (firstgeneration) anti psychotics.
~ Although not frequently used, ECTis a safe andeffective treatment for depression and otherdisorders. It causes some short-term cognitiveside effects, especially when administered bilaterally.
~ Anxiolytic medications work via their effect on theGABAsystem to decrease anxiety. They are widelyprescribed.
~ Lithium is an important medication in thetreatment of mania. However, some of the newermood-stabilizing drugs (which are also used to treatepilepsy) are now more frequently prescribed.
~ Many approaches to psychological treatmenthave been developed to treat individuals withpsychological disorders. One of the oldestapproaches to psychological treatment, classicalpsychoanalysis, was originated a century ago bySigmund Freud. It is rarely practiced today, andthere is little empirical support for its efficacy.
~ Several variants of therapy have developed out ofthe psychoanalytic tradition. These diverge fromclassical psychoanalysis on matters such as theduration of therapy and the role of primitivepsychosexual drives in personality dynamics. Manyof the newer psychodynamic forms of treatmentemphasize the way interpersonal processes are
affected by early interactions with parents and otherfamily members.
~ Behavior therapy is extensively used to treat manyclinical problems. Behavior therapy approachesinclude exposure, aversion therapy, modeling, andreinforcement approaches.
~ Cognitive or cognitive-behavioral therapy attempts tomodify a person's self-statements and construal ofevents in order to change his or her behavior.Cognitive-behavioral methods have been used for awide variety of clinical problems-from depression toanger control-and with a range of clinicalpopulations. Much research attests to the efficacy ofcognitive and cognitive-behavioral approaches.
~ Other psychological treatment approaches includehumanistic-experiential therapies and gestalttherapy.
~ In addition to their use in treating individuals, somepsychological treatment methods are applied toproblematic relationships through marital or familytherapy. These approaches typically assume that aperson's problems lie partly in his or her interactionswith others. Consequently, the focus of treatment ison changing the ways in which members of the socialor family unit interact.
~ A key element in all therapies is the development ofan effective "working alliance." A principal socialissue in psychotherapy is ensuring the developmentof a good therapeutic working alliance between clientand therapist, even when they differ widely incultural, ethnic, and/or socioeconomic backgrounds.
~ Evaluation of the success of psychotherapy inproducing desired changes in clients is difficult. Twocriteria for doing so have evolved: efficacy andeffectiveness. Research on psychotherapy, however,has shown that most treatment approaches are moreeffective than no treatment at all.

antianxiety drugs (P. 616)
antidepressant drugs (P. 612)
antipsychotic drugs (P. 609)
behavior therapy (P. 622)
client-centered therapy (P. 628)
cogn itive/ cognitive-behavioraltherapy (P. 625)
counter-transference (P. 632)
double-blind (P. 606)
efficacy (P. 606)
electroconvulsive therapy (ECT)(p.618)
family therapy (P. 634)
free association (P. 631)
half-life (P. 609)
imaginal exposure (P. 623)
integrative behavioral coupletherapy (P. 634)
in vivo exposure (P. 623)
latent content (P. 631)
manifest content (P. 631)
manualized therapy (P. 607)
marital therapy (P. 633)
modeling (P. 623)
neurosurgery (P. 620)
placebo (P. 606)
psychodynamic therapy (P. 630)
psychopharmacology (P. 607)
psychotherapy (P. 600)
randomized clinical trials (RCTs)(p.606)
rational emotive behavior therapy(REBT) (P. 625)
resistance (P. 631)
response shaping (P. 624)
structural family therapy (P. 634)
systematic desensitization (P. 623)
tardive dyskinesia (P. 610)
token economy (P. 624)
traditional behavioral coupletherapy (P. 633)
transference (P. 631)








![Improved light therapy system and methods of use · IMPROVED LIGHT THERAPY SYSTEM AND METHODS O F USE CROSS-REFERENCE T O RELATED APPLICATIONS [0001] This application claims benefit](https://img.pdfslide.net/doc/110x75/5edafbd209ac2c67fa689f4c/improved-light-therapy-system-and-methods-of-use-improved-light-therapy-system-and.jpg)



![7HPHW I|OGHN 6]i]KDORPEDWWD · 2017-07-06 · 022 a b a b sz 7 019/94 L a b 019/95 019/98 L L L L 019/99 L 019/100 019/101 019/102 019/103 019/87 019/96 019/88 019/89 019/90 019/91](https://img.pdfslide.net/doc/110x75/5e4940c49568aa74b4721e0b/7hphw-ioghn-6i-2017-07-06-022-a-b-a-b-sz-7-01994-l-a-b-01995-01998-l-l-l.jpg)