Embed Size (px)
Citation preview

CONTENTS | SCOPE
SCOPE | SEPTEMBER 08 | 03
THIS ISSUE
COVER FEATURE46
08
19
32
40
ULTRASONIC DETECTION Invention of ultrasounddevices to detectunderwater objects, suchas icebergs andsubmarines, and theresulting patent war
08 SCIENTIFIC EXCELLENCEA programme to collaborate on research in brain imaging in a consortium of six Scottish universities
19 TRAVEL REPORTA fun and timely seminar tour of the UK from the recipient of the 2007 AAPM–IPEM Medical Physics Travel Grant
45 65TH ANNIVERSARY OF THE HPATo mark this historic event, meeting notes from the inaugural meeting of the Hospital Physicists Association are reproduced
04 PRESIDENT’S LETTER Our modern healthcare system05 EDITORIAL An image issue06 NEWS A summary of recent innovations and studies40 MEMBER’S NEWS IPEM member wins the UK’s biggest engineering prize40 EXAM RESULTS For clinical scientists41 DIARY OF MEETINGS Events for 2008–200942 BOOK REVIEWS A packed issue with lots of newly published books
REGULARS
23 CAN OPEN SOURCE SOFTWARE BE USED FOR CLINICAL WORK?Dom Withers
24 ADVANCED NEUROLOGICAL MR: CLINICAL APPLICATIONS UPDATEJohn Thornton
26 RADIATION PROTECTION IN NUCLEAR MEDICINEMF Dempsey
29 ICMP 2008: CURRENT AND FUTURE SCIENCES IN RADIATION MEDICINEDavid and Rosemary Eaton
32 SOUTH WEST IPEM MEETING: REGIONAL UPDATESPenny Latimer and Amanda Brason
35 CLINICAL TRIALS IN RADIOTHERAPY: OVERVIEW OF THE RATIONALECatharine Clark
38 VOICE OF YOUNG SCIENCE: STANDING UP FOR SCIENCE WORKSHOPConstantinos Zervides
MEETING REPORTS
11 IMAGE REGISTRATION FOR MEDICAL IMAGING Past, present and future16 LETTER TO THE EDITOR Comments on Publishing Professional Writing (2)
TUTORIALS

SCOPE | FEATURE
08 | SEPTEMBER 08 | SCOPE
INAPSE (ScottishImaging Network – APlatform for ScientificExcellence) is aconsortium of sixScottish universities
(Aberdeen, Dundee, Edinburgh,Glasgow, St Andrews and Stirling)that has been established withfunding from the Scottish FundingCouncil, the Chief Scientific Officeand the universities. The aim of theconsortium is to create a strongdynamic network for a sharedenvironment that leads to thedevelopment of brain imagingresearch. The focus is primarily onthe technologies of magneticresonance imaging (MRI), positronemission tomography (PET), singlephoton emission computedtomography (SPECT),electrophysiology (EEG) and eventrelated potentials (ERPs).
The network is already gainingsignificant strength, with keyresearch staff appointments beingmade in the areas of imageacquisition, fMRI paradigm designand image analysis. A key area is thedevelopment of Scottish molecularimaging, where expertise has beenincreased by appointing staff inradiochemistry at Glasgow,Edinburgh and Aberdeen to furtherthe development of novel tracers in
PET brain imaging. To follow this, inthe near future, strategicappointments to five ProfessorialChairs will be made, covering allareas of brain imaging, includingimage analysis, brain imagingphysics, functional imaging,oncology and vascular imaging.
One of the most exciting parts ofSINAPSE for early career researchscientists is that this first-rateresearch base will have its capacityenhanced by the appointment of 24postgraduate studentships over thenext few years. Two PhD calls havealready been completed, with twostudents currently active and moredue to start in October 2008. TheSINAPSE network will provide thesestudents with a strong cohesivedoctoral training programmebetween universities, allowing themto develop their careers, andeffectively establishing a futuregeneration of imaging researchers inScotland. Below is the view on theground from a selection of theSINAPSE centres.
SINAPSE – A VIEW FROM EDINBURGHOne of the aims of SINAPSE is tofacilitate all the Scottish imagingcentres working together as a singleimaging lab, thereby allowing thedata acquired from subjects scanned
at each site to be pooled together inone analysis. Clearly, with themixture of make, model and fieldstrength of the SINAPSE MRIscanners, preferred local protocolsand coils, this is no easy task!Another complicating factor isscanner performance, particularly inlongitudinal studies providing datafor quantitative analyses – hence it isso important to develop anappropriate quality assurance (QA)protocol.
Through our work for ‘Calibrain:multicentre structural and functionalMRI in Scotland’, funded by theScottish Government and a pre-curser to SINAPSE, involving theUniversities of Edinburgh, Aberdeenand Glasgow, we have realised theimportance of QA in determining thereproducibility of the acquired data.In a multi-centre environment, QA isparticularly important as it ensuresthat any change in the subject’simages can be attributed to genuine,patient-specific changes and notchanges in the scanner or associatedprotocols.
Building on this experience, we’reworking with medical physicistsfrom each SINAPSE centre to reviewand optimise our QA for our multi-centre work. As well as including thestandard QA tests for our sMRI andfMRI, we hope to address specific
Oneof theaims is tofacilitateall theimagingcentres asa singleimaginglab
“
”
SCIENTIFICEXCELLENCE Dr Janet De Wilde (Heriot-Watt University, Edinburgh)explains more about SINAPSE, a programme to collaborateon research in brain imaging across Scottish universities
S

SCOPE | SEPTEMBER 08 | 09
QA issues in some of the moreadvanced modalities such as DTI,with the development of dedicatedtest objects and protocols through ourSINAPSE-funded PhD studentships.
THOUGHTS FROM THE GRANITE CITYAberdeen has an internationalreputation in neuroimaging research,particularly in ageing brain research,that includes multimodality imaging,such as PET, SPECT and structuraland functional MRI. We are, however,a small group of researchers. We seeSINAPSE as being the perfect route togenerating a critical mass ofresearchers to allow us to competemore successfully on theinternational stage. The inclusion of24 part-funded PhD studentships inthe initial SINAPSE bid will alsoallow Scotland to develop the nextgeneration of neuroimagingresearchers, and with the firstappointment made in Aberdeen inOctober 2007 we are already takingthe first steps.
As mentioned above, our workwith the Calibrain project introducedthree of the six universitiescollaborating in SINAPSE to theadvantages of pooling expertise anddata. We know that the addition ofDundee, St Andrews and Stirling willadd to the experience, making
Scotland a major player in the arenaof neuroimaging.
From a more personal view,although we all know that Scotland isrelatively small geographically we, asresearchers, have all been guilty of‘re-inventing the wheel’ rather thanasking our neighbours for help.Hopefully we will be a bit morewilling to ask for help.
PRE-SINAPTIC THOUGHTSFROM GLASGOWIt is clear that Scotland has tofunction as a coordinated unit to beinternationally competitive in clinicalresearch, particularly in those fieldsthat involve technologies of highcomplexity. Neuroimaging is a primeexample. In recent years Glasgowneuroimaging researchers have mademodest contributions to research inmany clinical fields, have taken eightcompounds from the experimentallaboratory setting and developedthem into SPECT tracers that havebeen used in clinical studies in manydifferent centres around the UK, andhave won a Proof of Concept awardto develop a patented MRI contrasttechnique. It would have been easyfor us to have delusions of adequacy,yet we struggle to recruit staff withappropriate skills.
The Wyeth/TMRC partnership hasenabled us to embark on joint
neuroimaging studies with Aberdeenon SPECT and PET tracerdevelopment, and with Edinburghand Aberdeen on stroke. This is astart in promoting joint working, butdoes not address the long-term issueof developing skills and optimisingthe use of facilities across the wholeof Scotland. This is what we expectwill be achieved through SINAPSE.Early signs are encouraging. Post-doctoral researchers and PhDstudents are being recruited.Importantly, each PhD student will beco-supervised by experiencedacademics from two centres and willwork on projects of interest to theSINAPSE partnership.
At a recent meeting of the NewYork Academy of Science in London,the Chairman made a plea to theUniversities in the south-east ofEngland to learn from theUniversities of New York and work inpartnership. By comparison SINAPSEwill be small, but hopefully perfectlyformed.
A STIRLING APPROACH TOIMAGINGBrain imaging at the University ofStirling has always played somethingof a back-seat role to the biggeruniversities in Scotland, largelybecause Stirling has no Department ofMedicine. There is, however, an active
TOP LEFT.Dr Gordon Waiter(physicist)standing next tothe MRI systembased inAberdeen.
�
TOP RIGHT.FDG PET inAlzheimer’s,courtesy of DrAlison Murray,Aberdeen.
�
FEATURE | SCOPE
�

SCOPE | FEATURE
10 | SEPTEMBER 08 | SCOPE
brain imaging laboratory within theDepartment of Psychology – whereresearch is carried out to investigatethe neural basis of basic mentalabilities such as memory andlanguage. The development ofSINAPSE is a major plus for Stirlingbecause it provides a greatopportunity for the integration ofdifferent methods and approachesacross the participating universities.
The Stirling approach has been touse event-related potentials (ERPs) toinvestigate the brain – a measure ofneural activity recorded fromelectrodes placed on a subject’s scalp.ERPs provide a powerful means ofassessing brain activity in real time,revealing the changing patterns ofbrain activity that occur duringmental processing.
In fact, ERP laboratories exist in allof the participating universities thatare part of the SINAPSE network,and the scientists in theselaboratories have often worked inrelative isolation from one another.The coordination of brain imagingacross Scotland that is at the heart ofthe SINAPSE network looks certain
to enhance the interaction betweenbrain scientists and, as a result, leadto better research.
DUNDEE DEVELOPMENTSIn Dundee, a new Clinical ResearchCentre (CRC) has been built and astate-of-the-art 3 Tesla MRI scanner isvery soon to be installed solely forresearch use. There is also space inthe building for PET/CT and thereare ambitious plans to install acyclotron in the adjacent MedicalPhysics building. Hence Dundeeplans to contribute fully to theSINAPSE network with academicappointments also pending. The MRIscanner will be set up for fMRIstudies and it is expected thatDundee and St Andrewspsychologists will make full use ofthis facility.
BUILDING ON REPUTATION ATST ANDREWS The School of Psychology at StAndrews has a well-establishedreputation for cutting-edge researchinto brain function and humanbehaviour. This includes a tradition
of brain imaging research from theestablishment of the first EEGlaboratory in the School in the late1970s, which spawned a generation ofmemory researchers, many of whomare still working in Scotland. EEGresearch continues to thrive in theSchool where it is currently used toinvestigate a range of cognitiveprocesses. SINAPSE represents a newway of working and cooperating notonly between institutions but alsodisciplines. Multidisciplinarity maybe SINAPSE’s greatest strength andalso its greatest appeal to both theresearch and clinical communities.The opportunity for involvement in anetwork of leading scientists fromsuch a broad range of disciplines whoshare a common interest in furtheringknowledge about the brain is quiteunique. SINAPSE will provide aplatform for an exchange of ideas andknowledge that will benefit theresearch community and the Scottishpopulation through the co-operationand collaboration of researchers andclinicians. This is a truly excitingdevelopment that we are delighted tobe part of. �
TheSINAPSEnetworklookscertain toenhanceinteractionbetweenbrainscientists
“
”
�
CT-MR. CT-PET. IGRT.
but you’re not sure how to test ...
of your image registration algorithm
Accuracy? Limitations? Results?
Provides the what, and the how to test.
Without the scanner
Without the hard phantom
15 software phantoms
Deformable & 4D phantoms
CT, MR & PET images computer generated
NEW Image Fusion Test Protocol included
So, you’re performing Image Fusion..?
ImSimQA
tel: +44 (0)1743 462 694 [email protected] Oncology Systems Limited

2007 AAPM–IPEM MEDICAL TRAVEL GRANT AWARD REPORT | SCOPE
SCOPE | SEPTEMBER 08 | 19
ow, what aride! I’dtaken asabbaticalleave yearfromPurdue
University starting at the beginningof July 2007 and spent most of thattime on opposite sides of the globe;England and Australia. It seemedthat fitting in 2 weeks for a seminartour of the UK as part of the honourfor receiving the 2007 AAPM–IPEMMedical Physics Travel Grant wasgoing to be easy. After all,everything was leaning my way. I’moriginally from Liverpool, England,a city that is home to the Beatles,world class soccer teams and apeculiar local accent known as‘Scouse’. All my siblings, myparents, and about half a millionother souls still reside in this 2008European Capital of Culture plus Ihave friends abounding in the cityand on the island at large. Yes, easyas eating pie, except life comes at
you hard, fast and without warningsometimes. A family crisis,encountering sick parents and acareer-related opportunity allcolluded to force a change in myaward travel plans from Fall 2007 toSpring 2008. Nevertheless, all wentsmoothly in the end and the tourwas a great success.
PROTON THERAPY ATCLATTERBRIDGEI’ve had an interest in protontherapy for a long time and thisinterest has recently been focusedon problems concerning thetreatment of lung cancer using thismodality. How should we be doingtrue 4D proton therapy and may wetake advantage of the timedimension to improve optimisedintensity modulated therapy?Aspects of this question, togetherwith scattered neutron dose to afetus and prostate cryosurgery,comprised the six seminars given inpart fulfillment of the awardrequirements.
First I visited the ClatterbridgeCentre for Oncology (CCO) inBebington, which is the secondlargest dedicated cancer centre inEngland. There I was hosted byProfessor Alan Nahum to deliverthe seminar entitled ‘ProtonTherapy in Motion?’. This wasobviously a pleasant experiencejudging by the big smile on my facein the picture shown in figure 1!Clatterbridge has the only protontherapy treatment centre in the UK,a low energy facility that treats eyesexclusively. However there is greatinterest in acquiring funding for ahigh energy proton treatmentfacility by Clatterbridge and I metwith the centre’s Chief ExecutiveOfficer, Mr Darren Hurrell, todiscuss the opportunities presentlyavailable. The CEO attended myseminar and I hope he waseducated as to the potential of thismodality and the cutting edgeresearch that would be translatedinto the clinic by the time theirproton facility is built.
RADIOBIOLOGICALMODELLING COURSEAlan is an expert in Monte Carlocalculations and radiationdosimetry who has an increasingprofile in biological modelling ofradiation therapy treatment. In factI arrived a few days before theannual international course heorganises on RadiobiologicalModelling in Radiotherapy at theCCO (see www.ccotrust.nhs.uk orcontact Alan directly for details onthe 2009 course,[email protected]). Notonly did Alan host me for theseminar at one of his busiest timesof the year but he had kindly beenmy sponsor for a long stay atClatterbridge in 2007 as part of mysabbatical. Alan’s boss and Directorof the Medical Physics Departmentat Clatterbridge is Dr Philip Mayles.Somewhat coincidentally, I had twoprior connections with Philip but Ihad never spoken with him
W
A FUN AND TIMELY SEMINAR TOUR OFTHE UK – IT’S SUCH A SMALL WORLD!PROFESSOR GEORGE SANDISON School of Health Sciences, Purdue University
FIGURE 1.Delivering theseminar ‘ProtonTherapy inMotion?’ at theClatterbridgeCentre forOncology.
�
�

20 | SEPTEMBER 08 | SCOPE
mountainside views of splendidvalleys and lakes unravelling beforeme with each turn of the road. Ittaught me to get lost more oftenaround Sheffield and then enjoy thetrip. I’d started out early and sofortunately arrived only a fewminutes late for my meeting withJohn. Actually this was quite amiraculous feat since gettingaround hospital buildings in the UKis now a high security event withelectronic keys cutting off non-patient areas from visitors. Johngave me a tour of the clinic, treatedme to lunch, and hustled so theseminar was well attended by alarge cross section of staff.
THE OLD AND NEW INRESEARCH IN OXFORDNext was a trip to Oxford where Iwas hosted by Ms ElizabethMacaulay (figure 3) to deliver aseminar entitled ‘SecondaryNeutron Dose to the Fetus fromProton Radiotherapy of theMother’. Interestingly, there are nospecified radiation dose limits to thefetus of a mother undergoingradiation therapy treatment. Icompared the scattered neutrondose equivalent between protonbeam passive scattering systemsand scanning systems to each otherand to high energy x-ray treatments.Elizabeth took me on a tour of theChurchill Hospital’s radiationtherapy facilities and over the plansfor the new facilities at the OxfordCancer Centre in the process ofbeing built as part of a new hospitalcomplex costing over £200 million.Courtesy of Dr Chris Gibson,Director of Medical Physics andClinical Engineering, we three thenate lunch at the University ofOxford’s old observatory buildinglocated within the grounds of thenewest of the Oxford colleges,Green College. This very attractiveCollege was established in 1979 andis 730 years younger than the first,University College, established in1249. Green is devoted to studentsin the medical disciplines andboasted Regis Professor of MedicineSir Richard Doll as its first Warden.He, along with another MedicalResearch Council scientist SirAustin Bradford Hill, published in1950 the first article describing anepidemiological study linking lungcancer with a major causative agent,smoking.
SCOPE | 2007 AAPM–IPEM MEDICAL TRAVEL GRANT AWARD REPORT
FIGURE 2 .(TOP)Dr John Conway,possibly beingover affectionatewith his newlyacquired model.
FIGURE 3 .(BOTTOM)Ms ElizabethMacaulay, DrChris Gibson andyours trulyoutside the OxfordUniversity oldobservatory aftera fine lunch. Thephotographerwas a Cambridgeman and thoughtthe shot mightlook better fromthat town.
until my stay. First, his wife Helenand I completed our MS degreestogether in radiation physics asapplied to medicine back in 1978–9at St Bartholomew’s MedicalCollege, University of London.Second, Dr Paul Mobit became oneof my post-doctoral researchassociates after completing his PhDunder Philip’s and Alan’s co-mentorship when they were allemployed at the Royal MarsdenHospital. Yes, the world of medicalphysics is a small one!
TRAVELLING OFF THE BEATENTRACK TO SHEFFIELDMy second seminar entitled ‘4D-CTfor Proton Therapy’ was deliveredto the Radiotherapy Department ofWeston Park Hospital, Sheffield.There I was hosted by the Head of
Radiotherapy Physics Dr JohnConway (figure 2). Sheffield isbeautifully situated in the Penninemountain range that is the backboneof Britain. It was famous for its steelfrom the 14th century until thatindustry declined in the 1970s andnow boasts education and medicineas its major employment industries.The ancient Pennines have only twopasses to be negotiated close toSheffield, Snake Road Pass andWoodhead Road Pass. I took thewrong one, Woodhead, that swungme far to the north of my target.There is no turning back on thisnarrow road. Worse still, there areno sign postings; why waste moneyposting a sign when there is noturning off? Dazzling naturalbeauty was the salve to my irritatedmental state and I soon relaxed into
� �
�

2007 AAPM–IPEM MEDICAL TRAVEL GRANT AWARD REPORT | SCOPE
SCOPE | SEPTEMBER 08 | 21
SIGHTSEEING IN OXFORDA well-deserved rest day saw mespending my leisure time in theoldest British museum, the OxfordAshmolean Museum. Initially basedon a private collection of EliasAshmole it was opened to the publicin 1683, and now contains incrediblyrare and incomparable works of artand craft including two Stradaveriviolins and a guitar among themaster musical instrumentcollection. Then later I toured theBodleian Library complex whichhouses an astounding number ofancient medieval books andmanuscripts in its oldest part. Thispart of the library was finalised in1488 as a gift to Oxford Universityby Humphrey, Duke of Gloucester,who was younger brother to KingHenry V. The Bodleian, named afterSir Thomas Bodley, a Fellow ofMerton College in the late 16thcentury, is Oxford University’soldest and main research library.The inside will be familiar to manyas it is featured in several scenes ofthe Harry Potter movies as theHogwarts library.
DISCUSSING FUTUREPROSPECTS WITH STUDENTSFrom Oxford I travelled to theUniversity of Surrey, Guildford, tojoin my host Dr David Bradley inthe Centre for Nuclear andRadiation Physics, Department ofPhysics. I arrived just in time todeliver my seminar on‘Contemporary Problems in ProtonTherapy’ to the graduate medicalphysics students and faculty. Then Ispent another hour chatting in afreestyle format with the studentsanswering any questions they had.Mostly their interests lay in jobs,clinical training and furthereducation at the PhD level. Somewere interested in my thoughts onthe best medical physicsprogrammes to apply for in theUSA. Later I was treated to lunch atthe faculty club by David and wewere joined by Emeritus ProfessorNikolas Spyrou and ProfessorAndrew Nisbet, Head of MedicalPhysics at the Royal Surrey CountyHospital. We chatted about theexciting and ground-breakingresearch being pursued at Surrey
University including plasticradiation detectors, protonmicrobeam tomography,determination of trace elementanalysis using neutron activation,and the use of proton induced x-rayexcitation (PIXE) for determiningthe metabolism and pathology ofdisease. Proton work is carried outat the university’s ion beamanalysis and accelerator facility andfollowing lunch David took me on agrand tour. One of the highlights ofthis tour for me was the ongoingconstruction of an £11 millionnanobeam charged particle facilitythat is to be dedicated in part tocellular radiation damage studieslooking at mechanisms for thebystander effect. David and I alsostumbled across a mutual friendand colleague in our conversations,Dr Suprakash Roy. He is an Indianscientist based in Calcutta who is anexpert in neutron bubble detectorsand had previously spent twosummers on Visiting Professorshipswith me doing the work onscattered neutron dose equivalentto a fetus from x-ray and �
[email protected] tel:(+44) 01743 462694
IMRT / TomoTherapy / VMAT / Rapid Arc™ Pre-treatment Dose Verification
a
®
®
Wechattedabout theexcitingandground-breakingresearchbeingpursued atSurreyUniversity
“
”

SCOPE | 2007 AAPM–IPEM MEDICAL TRAVEL GRANT AWARD REPORT
22 | SEPTEMBER 08 | SCOPE
proton radiation beams. David hadalso worked with him several timesin Calcutta. Yes, the world ofmedical physics is a small one!
TIME AND MOTION, ANDMUSIC!My visit to the prestigious Instituteof Cancer Research and RoyalMarsden Hospital was hosted byProfessor Steve Webb. Steve is notonly an outstanding andaccomplished medical physicist butalso a serious artisan and musician.He has built copies of renaissancestringed instruments includingcopies of the Sellas guitars in theAshmolean Museum. In thephotograph in figure 4 he is playingone of several renaissance copyguitars that he built himself, thisone being quite a lot smaller thanthe 180 cm string lengthTieffenbrucker copy he built toexact scale from the design of theoriginal bicycle-sized one housed inthe Royal College of Music. Steveorganised a full day of meetingswith various leadership teams and a‘meet the professor’ session forgraduate students as well as mylunchtime seminar entitled ‘Time
and Motion – Enemy and Friend’.The Institute of Cancer Researchand the department led by Steve isthe home of British expertise indynamic therapy and 4Dprocedures so I was happy toprovide in detail some of mythoughts on the topic relating toproton therapy and also coveredthe most recent work of Zhao Liand Ryan McMahon, PhDcandidates in the School of HealthSciences at Purdue University. Thisseminar was very well receivedand, I learned, an appropriateprecursor to the visit of Dr ThomasBortfeld, MGH and HarvardMedical School, an acquaintancewho was also to speak on the topicof proton radiation therapy thefollowing week since he wasinvited to give the Institute’s 2008Haddow Lecture in recognition ofhis many scientific contributions toradiation therapy physics research.Yes, the world of medical physics isa small one!
BACK TO MY ROOTS INLONDONThe last seminar of this seriesentitled ‘Treatment of Prostate
Cancer Using CryosurgicalFreezing’ was delivered to theDepartment of Medical Physics andBioengineering, University ofLondon, and I was hosted by theHead of the Department ProfessorAndrew Todd-Pokropek. Thisdepartment is strongly focused onimaging problems related tomedicine and I felt members wouldbe interested in the imagingproblems of ultrasound forcryosurgical procedures and thebenefits of using x-ray CT guidedprocedures instead. I am analumnus of the University ofLondon and upon touring andmeeting with various facultymembers to discuss their research Ilearned several were intimatelyfamiliar with the medical physicsprogramme from which I hadgraduated. It felt good to have afeeling of belonging and I evenreminisced with Andrew aboutspending time writing up my MSproject around the corner in mygirlfriend’s apartment on GowerStreet. This project centred on theevaluation of the first commercialSPECT machine (J and PEngineering, manufacturer).Andrew shocked me when herevealed that he was the designer ofthe first prototype for that machine.Yes, the world of medical physics isa small one!
ACKNOWLEDGEMENTS TO ALL INVOLVEDI’d like to thank the AAPM andIPEM for the financial support andopportunity to interact with some ofthe most prominent medicalphysicists in the UK. Hopefully thisexperience will result in somefuture collaborations reachingacross the Atlantic. I’d also like tothank all my hosts for theirgraciousness and kindness whileparticipating in this event. Finally,I’d like to thank my many pastgraduate students, post-docs andscientific collaborators whose workand role in the research presentedwas formally recognised at thebeginning of each seminar. Eventhough the world of medicalphysics is a small one, it is abeautiful one filled with some of thefinest people one could ever hope tomeet. My wish is that the 2008award recipient of the AAPM–IPEMTravel Grant has as much fun as Idid. �
FIGURE 4.Professor SteveWebb building hisown version ofstring theory!
� �

FEATURE | SCOPE
SCOPE | SEPTEMBER 08 | 45
s well as being the60th anniversary ofthe NHS, 2008 marksthe 65th anniversaryof the formation ofthe Hospital
Physicists Association. The HPA wasthe first national organisation formedical physicists and medicalphysics in the world. Its inauguralmeeting, during wartime inSeptember 1943, had been precededby a meeting of 11 physicists inLeeds in May 1943, when Bill Spiershad organised the launch meeting ofthe Northern Group of MedicalPhysicists, which became the firstregional group of HPA.
The minutes of the first cycle ofmeetings of HPA, held on Friday24th and Saturday 25th September1943, are reproduced here to markthis historic event.
FRIDAY 24TH SEPTEMBERInaugural meeting held at 2.30pmFriday 24th September 1943 in theBritish Institute of RadiologyAbout 30 present
The meeting; after somediscussion, resolved that the bodyformed should interest itself in, anddiscuss, all matters arising out of themutual interests of those engaged inhospital physics.
It was decided that membershipis to be open to physicists attached tohospitals, medical schools, medical
should be ‘The Hospital PhysicistsAssociation’. The motion wasseconded by Dr L.H. Clark andcarried unanimously by the meeting.
It was resolved unanimously thata Governing Committee should beelected and that its constitutionshould be discussed at the nextmeeting which should take place inLondon during the week-end beforeChristmas 1943.
In connection with the scope ofour future meetings Professor Russexpressed the opinion that we hadbeen too ambitious that morning inproviding three hospitals formembers to visit and that in futureone hospital would be sufficient. Themeeting endorsed this view.
Dr H.J. Flint read a paper on‘Technique with Radium GrammeUnits’ in which he stressed the factthat our Association could be usefulin educating radio-therapists in theneed for the fullest application ofphysical information to theirtherapy.
Professor F.L. Hopwood read apaper on ‘The Betatron’ whichemphasised the potentialities of thisnew physical tool in the future workof hospital physicists and gaveconsiderable encouragement to theyounger members of ourAssociation.
In a paper on ‘Teaching for theDiploma’ Professor G. Stead gave amost interesting account of thehistory of radiological teaching inthis country up to the present time,and pointed out that it seemsnecessary in the future to provideseparate courses for diagnostic andtherapeutic radiologists.
In the final paper on ‘TheEquipment of a Hospital Physicist’,Professor Russ dealt with the kind ofknowledge a hospital physicist mustacquire, outside his own science, ifhe is to be of maximum service tomedicine, and so indicated, thatanother line of future work for theAssociation, would be to arrangefacilities for the acquirement of thisknowledge.
After some discussion on thepapers the meeting closed when ithad expressed its thanks to theconveners. �
or biological research departmentswho have had one years’ experience.
The meeting agreed that thereshould be a chairman who wouldhold office for one year only and asecretary who would hold office forone year in the first instance, butwho should be eligible for re-election for a maximum period ofthree years.
Professor F.L. Hopwoodproposed that Professor S. Russ(picture) should be the firstChairman of the body. This motionwas seconded by Professor W.V.Mayneord and carried by themeeting unanimously.
Drs J.E. Roberts and C.W. Wilsonwere nominated for the office ofsecretary and the latter was elected.
Finally it was resolved that thebody should hold three ordinarymeetings of its members each year,at least one of these to take placeoutside London.
Before he left, Mr Phillipsproposed that Birmingham shouldbe the place of our first meetingoutside London, the provisionaltime of this meeting being May 1944.
A message of goodwill to ournew body was received through DrL.H. Clark from the NationalRadium Commission.Saturday morning 25th September1943 10.30am – 12.30pm
Visits were paid by groups ofmembers to The Royal CancerHospital, The Middlesex Hospitaland The Westminster Hospitalwhere comprehensive exhibitsdealing with the work were shown.
SATURDAY 25TH SEPTEMBERMeeting held at 2.30pm Saturday25th September 1943 in the BritishInstitute of RadiologyIn the Chair: Professor Sidney RussAbout 30 present
Professor Russ read to themeeting a letter received from theBritish Institute of Radiologywelcoming the formation of ourAssociation, in particular, the factthat we desired its formation to takeplace within the framework of theInstitute if this could be so arranged.
Professor F.L. Hopwoodproposed that the name of our body
Meeting notes from the inauguration of the Hospital Physicists Association
65th Anniversary of the HPA
Professor S. Ross, firstchairman of theHPA.
�
A

Francis Duck provides thefascinating story of howunderwater detection wasdeveloped using ultrasoundand the resulting patentwars across the globe
ICEBERGS ANDSUBMARINESTHE GENESIS OF ULTRASONIC DETECTION

FEATURE | SCOPE
just inside the ship’ within whichthere would be a parabolic mirror withthe whistle at its focus.
However brilliant in concept,Richardson’s apparatus was neverbuilt. It was left to the impetus ofsubmarine warfare to cause thedevelopment of the first operationalultrasound pulse-echo locationsystem. At the start of the warGermany had just 30 submarines. Thesinking of three British cruisers inSeptember 1914, by submarine-launched torpedoes, served toemphasise the huge threat they posedto allied shipping. At that time, thereexisted no practical device fordetecting undersea obstacles. Depthmeasurement had barely developedsince the Greeks first used lead-loadedlines to determine the sea depth. So itis not surprising to find several reportsof new underwater detection systemsat this time. In the USA, RA Fessendenbuilt and tested the first practicalecho-locating device, albeit working ata much lower frequency, about 1 kHz.This system measured the time takenfor an echo to return from an object todetermine its range, and on 27th April1914 an iceberg was detected at adistance of 2 miles. During the nextdecade a number of prototype echo-location systems were developed andtested, both in Europe and America.Some systems used explosive charges,bullets or detonators fired into thewater to generate the pulse of sound.Concerned about the safety of thesetechniques, the British Admiraltydeveloped a mechanical system. Asteel diaphragm sounder, 5 inches indiameter, was fixed to the hull of the
ltrasonic waves over100 kHz, well above thelimit to human hearing,were being explored bythe early 20th centuryusing tiny tuning forks,
whistles and spark generators assources. But no practical use had beenmade of this knowledge until twoevents triggered the developments tobe described. First, on 15th April 1912,the Titanic collided with an icebergand sank with a huge loss of life(figure 1). And, secondly, 2 years later,war broke out in Europe.
RICHARDSON’S PATENTSFive days after the Titanic disaster,Lewis F. Richardson filed the first oftwo echo-ranging patents with theBritish Patent Office. Richardson wasborn in Newcastle, educated in Yorkand Cambridge, and worked briefly atthe NPL. He recognised the potentialoffered by ultrasound for underwaterdetection, specifically the ability tocreate a directional acoustic beam. Inhis second patent, filed on 10th May1912, he proposed an underwaterpulse-echo system instead of theairborne system of the first patent. Thepurpose of the apparatus was to warna ship of its nearness to an objectahead. Richardson declared that thebest frequency ‘will probably be of theorder of 100,000 complete vibrationsper second’, and imagined that thesound would be ‘produced bywhistles or reeds, blown with water orother liquid’. The sender would be ‘abody somewhat resembling in shapean enormous motor car lamp 85 cmdiameter and about 1 m long placed
U
SCOPE | SEPTEMBER 08 | 47
FIGURE 1. The sinking of the Titanic.
�

SCOPE | FEATURE
48 | SEPTEMBER 08 | SCOPE
vessel and was thumped by anelectromechanical hammer twice asecond, emitting a sound pulse with acentre frequency about 1.25 kHz. Thereceiving hydrophone, also fixed onthe hull, was a microphone mountedin rubber. An insulating segment onthe receiving drum, which could berotated by hand, allowed an estimateof the pulse–echo transmission timeand hence the target range.
PROGRESS DURING THE WARAll these acoustic echo-locators,however, suffered from the deficiencyrecognised by Richardson. They wereinherently omni-directional, becauseboth source and detector weresignificantly smaller than thewavelength, λ, at the frequency used.Richardson’s second patent explicitlyforesaw the need for directional sourcewith ‘an aperture of at least 3λ’, sodefining the technical challenge ofcreating appropriate ultrasonicsources and receivers. This challengewas taken up by a young Russianelectrical engineer, ConstantinChilowsky. His proposal was, likeRichardson’s, to use high-frequencysound but using a magnetically-drivendiaphragm as a source. This proposaleventually (February 1915) reachedthe desk of Paul Langevin in Paris.Langevin, by then in his early 40s anda dominant figure in French science,had been requested by his formerstudent, Maurice de Broglie, to find away of detecting enemy submarines.Langevin understood the potential inChilowsky’s proposal, but was unsurethat a magnetically-driven diaphragm,similar to a telephone, would becapable of giving sufficient acousticpower in water at 100 kHz. Havingalso considered magneto-striction andpiezoelectricity, he finally opted for a‘singing condenser’ as the preferredoption. By July 1915 his team wereable to generate ultrasonic intensitiesaround 100 mW cm−2, using anexperimental arc transmitter designedfor wireless telegraphy for the Frenchnavy to drive a mica capacitor. (Thepower was estimated from a measureof radiation force on a target, thestandard method still used today.)One-way transmission tests across theRiver Seine in early 1916, using acarbon microphone as a receiver, weresufficiently encouraging for a firstpatent application to be prepared. Aselection of diagrams from this patent(figure 2) show some ideas formounting the transmitter and receiver
in a pod on the bow of the vessel, andvarious forms for the construction ofthe condenser source. Shortlythereafter, Chilowsky (who wasdescribed as brilliant but volatile) andLangevin parted company, atLangevin’s request, and the fieldexperiments were transferred to thenaval sea base at Toulon. There,practical problems dogged theprogramme. Spark discharges oftenoccurred across the singingcondensers because they were beingworked at the limits of their electricalstrength, the carbon microphoneswere unstable underwater, and seawater kept leaking into the apparatus.
Meanwhile, in London, theAdmiralty set up a committee – theBoard of Inventions Research – toconsider methods that could shortenthe war. The Board was supported byan advisory panel of which ErnestRutherford was the Secretary. Initiallythe preferred option for submarinedetection was some sort of passivesensor. The team was soon joined byRobert Boyle, from Canada. Boyle wasfrom Newfoundland originally, andhad studied electrical engineering inMontreal, where he had metRutherford. By autumn 1916, deBroglie had informed the BritishAdmiralty of progress in Paris, andChilowsky had visited London to givea first-hand account of theirexperiments. Boyle was assigned thetask to reproduce and test theChilowsky system, working in alaboratory in South Acton. At thesame time Rutherford and Boyle wereexperimenting with quartzpiezoelectric transducers, but werestruggling to make any significantprogress towards achieving adequatesensitivity. The piezoelectricity ofquartz was well understood at thistime, having been established byJacques and Pierre Curie, working inParis 30 years earlier, but it had neverpreviously been exploited for soundgeneration or reception. Both theAdmiralty committee and Langevinwere aware of Rutherford’s view that‘it is a pity that the effect is so small’.There was clearly much formal andinformal communication betweenlaboratories at this stage and, byMarch 1917, Langevin was able to letthe British group know that his teamhad succeeded in making significantimprovement to the sensitivity of hisquartz piezoelectric transducers.Shortly thereafter, Boyle spent 2months in Toulon (figure 3).
IMPROVEMENTS BY LANGEVINLangevin was initially put off the useof quartz transducers because ofRutherford’s pessimistic view.However he must have reconsideredthis judgement following thesignificant practical problems thatwere being experienced with thecondenser/microphone system. Histeam initially made two significantpractical advances. The first was toreplace the carbon microphone with aquartz plate as the receiver ofultrasound, amplifying the smallsignal using a multi-stage high-frequency triode amplifier which hadjust become available as part of aseparate French research programme.Secondly, he started to make progressin obtaining quartz plates of sufficientsize to act as directional sources. Thefirst was a slice, 10 x 10 x 1.6 cm,which he persuaded an optician inParis to cut from a showpiece in hisshop window. It was the initial results,obtained in February 1917, using thiscrystal as a receiver, which Langevinshared with the British group duringhis visit in March.
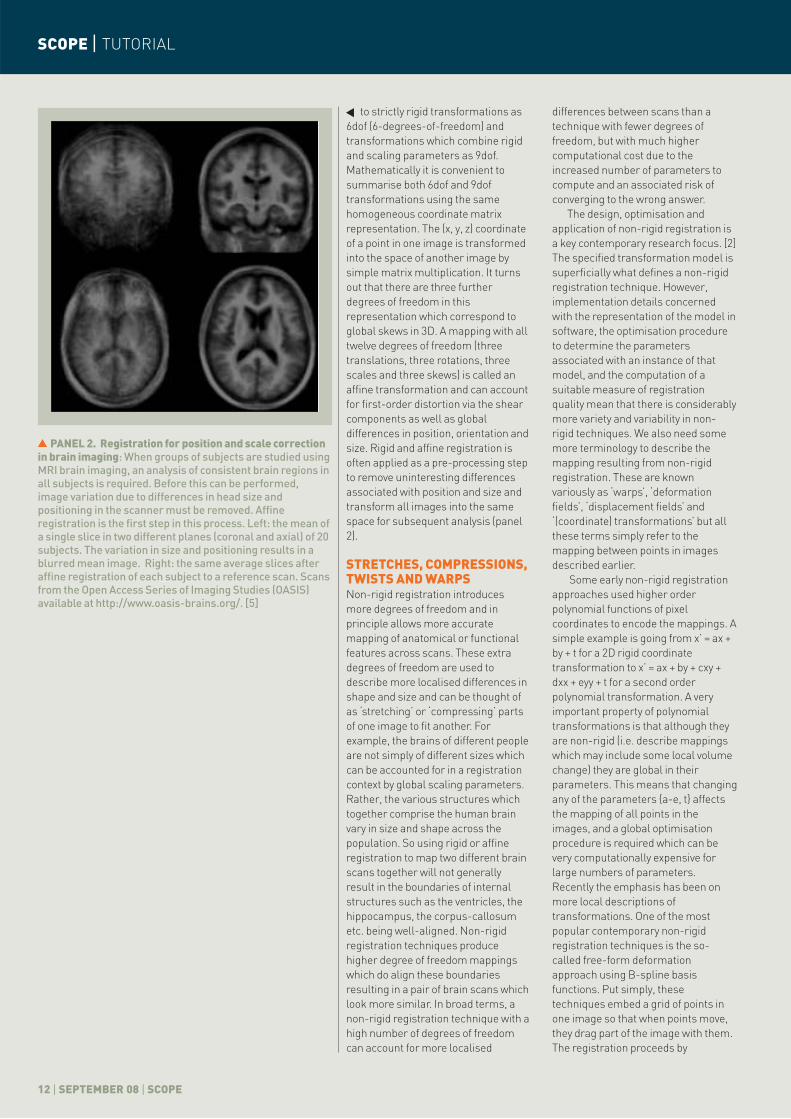
Meanwhile, spectacular successhad been achieved using the samecrystal as a transmitter. The key to thissuccess was that the drive voltage wastuned to the resonant frequency of thequartz, which in this case was about150 kHz. Driven at 12 kV, Langevinestimated that the transducergenerated about 1 kW acoustic outputpower, a result that immediatelyplaced a practical system within thebounds of possibility. Langevinreported that any ‘fish in theneighbourhood of the beam werekilled immediately’, and Robert Wood,one of the visitors from the USA at thistime, recalled later that ‘if the handwas held in the water near the plate analmost insupportable pain was felt’:these reports can probably be creditedas the first observations of ultrasoundbioeffects. No matter how successfulthese initial experiments were,however, there remained two finalchallenges. 12 kV was viewed as toohigh a voltage for practical use; andthere was little prospect of findingenough large quartz crystals. The finalinnovation from Langevin’s laboratorydealt with both with a single designchange. The quartz plate was reducedin thickness to a few millimetres, andsandwiched between two thickerplates of steel. Such an arrangementamplifies the piezoelectricresponse allowing a much lower
FIGURE 2.(TOP)Detail from theChilowsky andLangevin patent,1917, showingproposedmounting of theultrasonic sourceand receiver onthe bow of theship, andalternativedesigns for thesingingcondenser.
FIGURE 3. (MIDDLE LEFT)A photographtaken in Toulonduring Boyle’svisit in 1917. Fromleft to right:Capitaine deFrégate Colin,LieutenantSaville, PaulLangevin, RobertBoyle and MarcelTournier.
FIGURE 4. (MIDDLE RIGHT)A diagram of theLangevin‘sandwich’transducer (fromA.B. Wood: ATextbook ofSound, 1932).
TABLE 1.Chronology of thedevelopment ofunderwaterultrasonic pulse-echo detection.
��
��
�
�
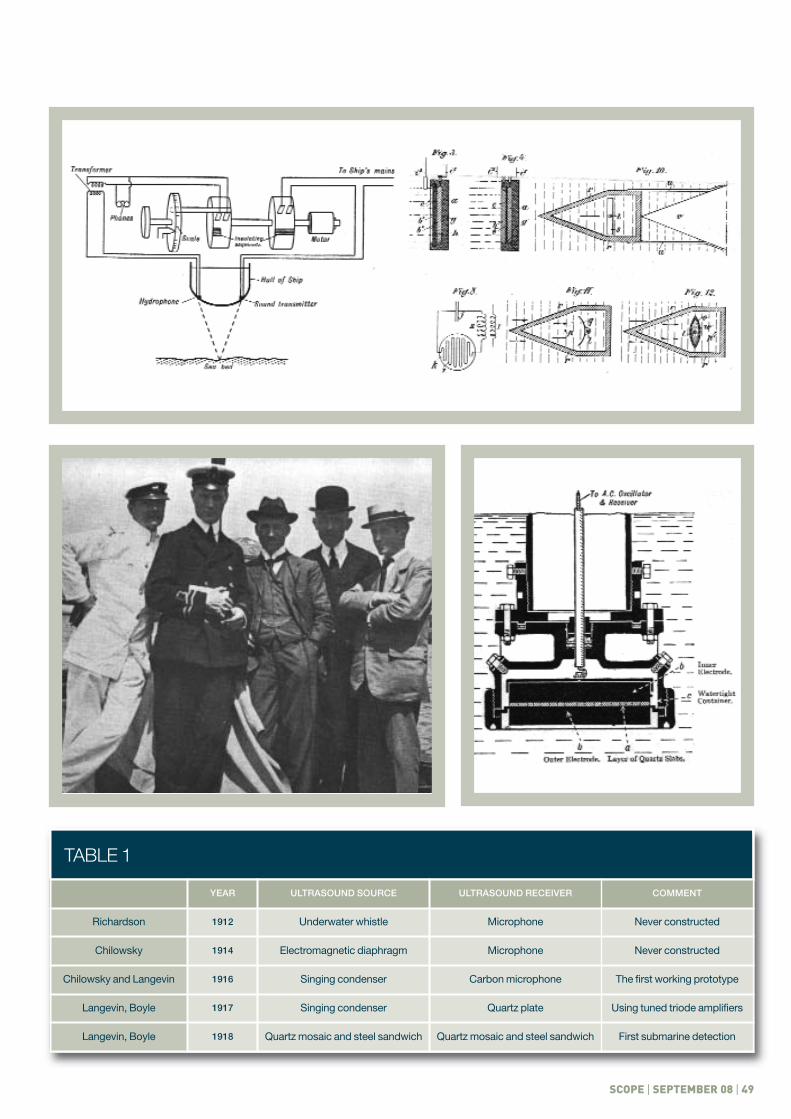
TABLE 1
SCOPE | SEPTEMBER 08 | 49
TABLE 1
YEAR ULTRASOUND SOURCE ULTRASOUND RECEIVER COMMENT
Richardson 1912 Underwater whistle Microphone Never constructed
Chilowsky 1914 Electromagnetic diaphragm Microphone Never constructed
Chilowsky and Langevin 1916 Singing condenser Carbon microphone The first working prototype
Langevin, Boyle 1917 Singing condenser Quartz plate Using tuned triode amplifiers
Langevin, Boyle 1918 Quartz mosaic and steel sandwich Quartz mosaic and steel sandwich First submarine detection

SCOPE | FEATURE
50 | SEPTEMBER 08 | SCOPE
drive voltage to be used. The resonantfrequency is defined by the thicknessof the whole sandwich, allowing muchthinner quartz to be used. And finally,instead of a single crystal, the quartzplate was made up from a mosaic ofsmall pieces. The relative thickness ofsteel and quartz layers can be seen infigure 4, a diagram of the finaltransducer assembly. By mid 1918, theFrench system had demonstratedsubmarine detection with a rangeextending occasionally to 1,500 m.Table 1 shows a summary of the stepsfrom Richardson’s 1912 patent to theoperational prototype in 1918.
SOURCING SUFFICIENT QUARTZ CRYSTALSCo-operation between the French andBritish groups was sufficient at thisstage for Langevin to supply one ofthe 10 x 10 cm crystals to Boyle, whoby then was working at the AdmiraltyExperimental Station at ParkestonQuay, Harwich. The British group alsobuilt a quartz mosaic transducer,bonded to a single steel sheet with aresonance at 75 kHz, with which, bythe end of 1917, they had transmittedsignals for nearly a mile. By March1918, Boyle had successfully detectedechoes from a submarine at a distanceof 500 yards, within a month of thefirst submarine detection in France.Boyle was particularly conscious of thedifficulty that would be encounteredin finding enough quartz crystals,even those suitable for mosaics. Hisfirst source was an opticalmanufacturer, Culver and Co. inLondon, and he arranged for thecrystals to be cut by Farmer & Brinlay,tombstone-makers of Lambeth. Later,a determined search even threatened
to requisition all the quartz specimensin British geological museums. Hefinally tracked down a French supplierof chandelier pendants in Bordeauxwhere he was astonished to find, in awarehouse, a huge mound of naturalquartz crystals piled up like coal.
During the final successful testing,the news was communicated to navallaboratories of other allied countries.The combined progress of French andBritish programmes was presented inWashington on 15th June 1917 duringa visit of a Franco–BritishCommission to the USA, whichincluded Rutherford and Fabry.Shortly thereafter, work started at theNaval Experimental Station inConnecticut. Once war was over,however, the period of generous co-operation between the allies seems tohave ended and a rather silly debateemerged over prior rights. Langevinfiled a French patent on 17thSeptember 1918 describing the steel-quartz-steel transducer for echo-ranging. The equivalent British patentwas challenged by the Admiralty, whoasserted that it should be filed jointlyin the names of Langevin, Boyle andRutherford. This caused Rutherfordconsiderable embarrassment. Quotingin Rutherford’s biography, A.S. Evegives his short and final comment: ‘IfLangevin says that the idea was his,then the idea was Langevin’s’. Thedebate rambled on ratheracrimoniously and was not closeduntil 1925. Rutherford said at the timethat he was ‘surprised anddisappointed by the attitude of theAdmiralty, and that it would be agrave injustice to Langevin if theservices given to the Admiraltyduring a very difficult period were
not generously recognised’. Patentchallenges in the United States werenot finally resolved until 1946, shortlybefore Langevin’s death. It seems clearthat Langevin must have consideredpiezoelectric methods at an early stagein this development. As a student hewas supervised by Pierre Curie, theco-discoverer of the piezoelectricity ofquartz. He was close friends with theCuries, and would have undoubtedlyunderstood the function of ‘quartzpiézo-électrique’ with which theyquantified the radioactivity of radium.He remained very close to Marie Curieand her family after Pierre’s death,and later ensured that 10 per cent ofthe income associated with his patentswas shared between their daughters,Irène and Ève, and Jacques Curie.
SUBSEQUENT WORK OF THEINVENTORSBoyle returned to Alberta in 1919, andcommenced a research programmeinto acoustic cavitation. Langevincontinued to work to improvepiezoelectric pulse-echo systems,working with C.L. Florisson todevelop depth-sounding equipment at40 kHz. He became a convincedpacifist and internationalist who tooka strongly anti-fascist positionbetween the wars, activelyparticipating in campaigns aimed atsecuring peace. He was imprisonedafter the capitulation of France andsubsequently held under house arrestuntil May 1944. After the war, hedevoted his efforts to educationalreform, and supported the CommunistParty in the hope of encouraging abrotherhood that he judged capitalismhad failed to establish. Paul Langevindied in 1946 after a short illness. �
TheequivalentBritishpatent waschallengedby theAdmiralty,whoassertedthat itshould befiled jointly
“
”
REFERENCES BIOGRAPHIES AND TECHNICAL DETAILS
1 Arshadi R, Cobbold RSC. A pioneer in the development ofmodern ultrasound: Robert William Boyle (1883–1955).Ultrasound Med Biol 2007; 33: 3–14.
2 Eve AS. Rutherford. Cambridge: Cambridge UniversityPress, 1939.
3 Bensuade-Vincent B. Langevin – Science et Vigilance.Paris: Belin, 1987.
4 Anon. Echo sounding. Hydrographic Review 1924; 2: 51–91.
5 Chilowsky C, Langevin P. Improvements In and ConnectedWith the Production of Submarine Signals and the Locationof Submarine Objects. British Patent 125122. Applied for
29th May 1916, granted 17th April 1919.
6 Hunt FV. Electroacoustics. The Analysis of Transductionand its Historical Background. New York: AmericanInstitute of Physics, 1954 (paperback 1982), 44–53.
7 Langevin P. Discloses Steel-Quartz-Steel Transducer.French Patent 505703. Applied for 17th September 1918,granted 14th May 1920. British Patent 145691.
8 Richardson LF. Apparatus for Warning a Ship at Sea of itsNearness to Large Objects Wholly or Partly Under Water.British Patent 11,125. Applied for 10th May 1912, granted27th March 1913.
�
IMAGE REGISTRATION FOR MEDICAL IMAGING:PAST, PRESENT AND FUTUREWilliam R. Crum explains image registration; mapping between images obtainedfrom medical imaging equipment
PANEL 1.A conceptual viewof registration:Registration isabout determiningthe correctgeometrictransformation tomatch images. Theprocess isanalogous toensuring a key isof the right size, atthe correctorientation and inthe correctposition to engagewith a lock. Thepanel shows theprogressiverecovery ofmismatches inscale, orientationand translationbetween a key andlock correspondingto a 9dofregistrationproblem – see textfor further details.Knowing thecorrect parameterswhich describethis transformationallows the key tocorrectly fit thelock. Note thatregistrationdetermines theparameters whichdefine thetransformationwhich must thenbe applied to thekey to guide it intothe lock.
WHAT IS IMAGE REGISTRATION?Image registration is a technique formapping corresponding pixel positionsacross images, which has been appliedin medical imaging for at least twodecades. By mapping between images,scans acquired on different imagingequipment, at different times, or ofdifferent people can be accuratelycompared and analysed. [4] The imagesare most often derived from medicalimaging equipment such as MagneticResonance Imaging (MRI), X-rayComputed Tomography (CT), UltraSound(US), Positron Emission Tomography(PET) etc., but may also come from video,microscopy or endoscopy, or be derivedfrom digital models of prosthetics andsurgical implants. Medical imagingapplications of registration includeassociating structure with function bygiving nuclear medicine images astructural context from MRI or CT,correcting for patient motion duringdynamic processes such as dynamiccontrast enhanced MRI, and exploringpopulation variation in anatomical shapeand function by registering a group ofsubjects to a common template.Registration is fundamental totechniques like functional-MRI of thebrain which are susceptible to subtlepatient movement. Left uncorrected thismovement can at best preventactivations being detected, and at worstcorrelate with a functional task in such away as to create apparent activationwhere none really exists.
It quickly becomes apparent that thecatch-all term ‘registration’ actuallyencompasses a variety of applicationswhich have specific demands onrobustness, user intervention andcompute-time. For instance an off-linefusion of 3D MRI and CT volumes can beperformed at a relatively leisurely pacecompared with registration of pre-operative and intra-operative imagingwhich must be near real time. Similarly,registration accuracy requirements maybe different in radiotherapy treatmentplanning compared with image-guidedneurosurgery because of the treatment
margins built into the former and theimportance of avoiding eloquent areasin the latter. In this tutorial we reviewthe key concepts underlyingregistration in medical imaging,highlight some recent advances andrisk ridicule by trying to second-guessfuture developments.
COMPONENTS OF AREGISTRATION ALGORITHMImage registration relies on threerelated concepts: (i) the transformationmodel which defines the class ofallowed mappings between images, (ii)a measure of registration quality, and(iii) an optimisation procedure forchoosing the best allowed mapping bymaximising the registration quality. Themost common distinction inregistration is between so-called ‘rigid’and ‘non-rigid’ techniques. Rigidregistration is defined by atransformation model where onlyglobal translation and global rotation isallowed. These are the same operationsused to guide a key into a key-hole (seepanel 1). The key must have the correct3D orientation and be translated intothe correct position to fit the lock. Rigidregistration is most-often used whenimages are of the same objects but withdifferent positions and orientations.One example is someone who has a CTand MRI brain scan on the same day butof course in different scanners; thepositioning of the head may be similarbut will never be the same in two scans.MRI and CT are 3D scanning techniqueswhich generate a stack of 2D slices;these slices will be inconsistent, evenbetween scans of the same person, dueto positioning differences and may be ofdifferent thicknesses or orientations.Rigid registration can correct for thesedifferences.
There is sometimes confusion aboutterminology. Usually one image isdefined as a ‘reference’ (or ‘target’ or‘template’) image and the mappingsbetween this image and other ‘floating’(or ‘source’) images are determined byregistration. Unfortunately there is still
some inconsistency in the literatureabout how these terms are used. Theregistration result is the set ofparameters which define thetransformations (mappings) betweenimages. These transformations can beapplied to the floating images togenerate new images which have been‘transformed’ (or ‘realigned’ or‘resliced’) into the space of thereference. In the key and lock exampleabove, the transformation parametersdescribe the distance the key has totravel and the angle it has to rotate byto fit into the lock. If I actually pick upthe key and translate and rotate it intoplace then I am applying thattransformation.
ROTATIONS, TRANSLATIONS,SCALES AND SKEWSFor 3D rigid registration, sixparameters (translation along threeorthogonal directions and rotationaround three orthogonal axes)completely specify the problem. In 2Donly three parameters are required(translation in x- and y-directions androtation around the z-axis). In manypractical applications, global scalingin three orthogonal directions is alsorequired which adds three moreparameters to determine. In theexample above this would allow us tochange the size of the key (but not itsshape) to fit the key-hole. Scalingparameters can account forcalibration variation when registeringimages from more than one scanner,or size differences when comparingscans of different individuals. Acommon short-hand is to refer
SCOPE | SEPTEMBER 08 | 11
TUTORIAL | SCOPE
�
�
SCOPE | TUTORIAL
12 | SEPTEMBER 08 | SCOPE
differences between scans than atechnique with fewer degrees offreedom, but with much highercomputational cost due to theincreased number of parameters tocompute and an associated risk ofconverging to the wrong answer.
The design, optimisation andapplication of non-rigid registration isa key contemporary research focus. [2]The specified transformation model issuperficially what defines a non-rigidregistration technique. However,implementation details concernedwith the representation of the model insoftware, the optimisation procedureto determine the parametersassociated with an instance of thatmodel, and the computation of asuitable measure of registrationquality mean that there is considerablymore variety and variability in non-rigid techniques. We also need somemore terminology to describe themapping resulting from non-rigidregistration. These are knownvariously as ‘warps’, ‘deformationfields’, ‘displacement fields’ and‘(coordinate) transformations’ but allthese terms simply refer to themapping between points in imagesdescribed earlier.
Some early non-rigid registrationapproaches used higher orderpolynomial functions of pixelcoordinates to encode the mappings. Asimple example is going from x’ = ax +by + t for a 2D rigid coordinatetransformation to x’ = ax + by + cxy +dxx + eyy + t for a second orderpolynomial transformation. A veryimportant property of polynomialtransformations is that although theyare non-rigid (i.e. describe mappingswhich may include some local volumechange) they are global in theirparameters. This means that changingany of the parameters {a-e, t} affectsthe mapping of all points in theimages, and a global optimisationprocedure is required which can bevery computationally expensive forlarge numbers of parameters.Recently the emphasis has been onmore local descriptions oftransformations. One of the mostpopular contemporary non-rigidregistration techniques is the so-called free-form deformationapproach using B-spline basisfunctions. Put simply, thesetechniques embed a grid of points inone image so that when points move,they drag part of the image with them.The registration proceeds by
to strictly rigid transformations as6dof (6-degrees-of-freedom) andtransformations which combine rigidand scaling parameters as 9dof.Mathematically it is convenient tosummarise both 6dof and 9doftransformations using the samehomogeneous coordinate matrixrepresentation. The (x, y, z) coordinateof a point in one image is transformedinto the space of another image bysimple matrix multiplication. It turnsout that there are three furtherdegrees of freedom in thisrepresentation which correspond toglobal skews in 3D. A mapping with alltwelve degrees of freedom (threetranslations, three rotations, threescales and three skews) is called anaffine transformation and can accountfor first-order distortion via the shearcomponents as well as globaldifferences in position, orientation andsize. Rigid and affine registration isoften applied as a pre-processing stepto remove uninteresting differencesassociated with position and size andtransform all images into the samespace for subsequent analysis (panel2).
STRETCHES, COMPRESSIONS,TWISTS AND WARPSNon-rigid registration introducesmore degrees of freedom and inprinciple allows more accuratemapping of anatomical or functionalfeatures across scans. These extradegrees of freedom are used todescribe more localised differences inshape and size and can be thought ofas ‘stretching’ or ‘compressing’ partsof one image to fit another. Forexample, the brains of different peopleare not simply of different sizes whichcan be accounted for in a registrationcontext by global scaling parameters.Rather, the various structures whichtogether comprise the human brainvary in size and shape across thepopulation. So using rigid or affineregistration to map two different brainscans together will not generallyresult in the boundaries of internalstructures such as the ventricles, thehippocampus, the corpus-callosumetc. being well-aligned. Non-rigidregistration techniques producehigher degree of freedom mappingswhich do align these boundariesresulting in a pair of brain scans whichlook more similar. In broad terms, anon-rigid registration technique with ahigh number of degrees of freedomcan account for more localised
�PANEL 2. Registration for position and scale correction
in brain imaging: When groups of subjects are studied usingMRI brain imaging, an analysis of consistent brain regions inall subjects is required. Before this can be performed,image variation due to differences in head size andpositioning in the scanner must be removed. Affineregistration is the first step in this process. Left: the mean ofa single slice in two different planes (coronal and axial) of 20subjects. The variation in size and positioning results in ablurred mean image. Right: the same average slices afteraffine registration of each subject to a reference scan. Scansfrom the Open Access Series of Imaging Studies (OASIS)available at http://www.oasis-brains.org/. [5]
�

SCOPE | SEPTEMBER 08 | 13
systematically moving points to mapthe floating image to the reference. Bycontrast with the polynomialapproaches above, this is a localtechnique because the functions whichdescribe the positions of each grid-point (the B-splines) have compact-support. This means that changing theparameters which describe thedisplacement of a grid-point has only alocal effect on the mapping rather thanthe global effect of the polynomialapproaches. This localisation becomesvery important when trying todetermine many thousands oftransformation parameters (panel 3).
Another very important class ofnon-rigid transformations originatesfrom applying physics-based models ofelastic solids and viscous fluids.Modelling the mapping betweenimages using the theory of elasticityleads immediately to a pleasing mentalimage of the floating image beingstretched like a sheet of rubber tomatch the reference image. Oneunfortunate consequence of elastictransformations being one of theearliest non-rigid transformationmodels is that many scientific papersuse ‘elastic’ to describe any non-rigidtransformation model. Elastictransformations are intuitive andrelatively straightforward to compute.Their main disadvantage is that therestoring force of an elastic medium isproportional to the local displacement.Therefore registration using purelyelastic models will tend to reach someequilibrium point dictated by themanner in which the elastic forcesdriving the registration are applied.More recently, attention has turned totransformations based on viscous fluidflow which can be imagined as thefloating image slowly flowing intoregistration over the reference image.Fluid transformations are morecomplicated to compute than elastictransformations but have severaladvantages. The main one is that therestoring forces relax over time whichmeans that fluid transformations cansuccessfully model large magnitudelocalised displacements. Anotheradvantage is that they produce so-called ‘diffeomorphic’ transformationswhich, loosely speaking, have theproperty that every point in thereference image is uniquely associatedwith a single point in the floating image.This property prevents parts of thefloating image ‘turning inside-out’which is a common problem for highlylocalised non-rigid transformations –
these inversions are generally notphysically meaningful. Thedisadvantage of fluid transformations isthat with such flexibility, optimising forthe best – in an application sense –transformation instance is difficult.
SURROGATE MEASURES OFREGISTRATION QUALITYTo determine the correcttransformation parameters requires ameasurement of correspondence toquantify how successfully a registrationtransformation maps points acrossimages. For example in brainregistration, if a candidatetransformation maps ventricles ontohippocampus it is low quality in termsof correspondence. The correcttransformation is assumed to be theone that maximises thecorrespondence measure. In practicethe true correspondence is rarelyknown (this is why registration isrequired!) so surrogate measures ofcorrespondence are used. Historicallythese were derived in two ways: bycomparing geometric features and bycomparing voxel (3D pixels) intensities.
Geometric features can be as simpleas point landmarks but also includelines, curves, ridges, corners, surfacesetc. Identifying the same set ofgeometric features in a pair of imagesin terms of their location, orientationand size allows a mapping to becomputed. Modern feature registrationtechniques account for errors inherentin taking measurements from noisydigital images and can select the bestpairs of features to use for registrationfrom larger sets identified on eachimage. Much recent research hasfocused on automating both theidentification and pairing of meaningfulfeatures and the best way to usesparsely defined feature-sets in non-rigid registration. The caveats withfeature-based methods are that theyoften still require considerable userinput to identify the feature sets and bydefinition the mappings computed bymatching individual features are notnecessarily correct for image regionswhere identified features do not exist.
These drawbacks have lead to thewide-spread adoption of voxel-intensitybased registration where a surrogatemeasure of correspondence is definedas a function of the intensities of pairsof voxels in the reference and floatingimages. The assumption is that whenthe correct transformation parametersare found, the so-called image-similarity will be maximised. Different �
TUTORIAL | SCOPE
PANEL 3. Registration applied in dynamic lungimaging: Rigid and non-rigid image registration of lung CTimages has been used to analyse the chest motionassociated with regular breathing. A floating image is firstacquired in a single breath hold i.e. with the chest and lungsstatic. Then a series of reference images are collecteddynamically while the patient is freely breathing.Registration enables the anatomy to be tracked in space asthe lungs fill and empty. The goal is to track this motion inreal time in a radiotherapy application to improve thetargetting of tumours. This will in turn increase theradiation dose which can safely be delivered to the tumourwhile reducing the dose received by unaffected tissue. Thefirst column of the figure shows a floating image (top) andreference image (bottom) before registration. The nextthree columns show the floating image (top) after noregistration, rigid registration and non-rigid registration,respectively. The corresponding images on the bottom rowshow the reference image for each case with coloursindicating regions where structures do not match properly.Before registration there are large regions of colour butafter rigid and non-rigid registration there is virtually noregistration error within the chest cavity. Technical details:the floating image was acquired at breath-hold, and coversthe entire lungs. The reference image was acquired whilethe patient was freely breathing with the scanner operatingin cine mode, and so only covers a thin 'slab' of data (16slices). The non-rigid registration used a free-formdeformation algorithm with B-spline basis functions. Thegrid-points defining the mapping were defined at 20 mmintervals in all directions. This work concerned registrationof CT images of the same subject so a simple imagesimilarity measure based on the difference in intensitybetween each point in the reference and floating imagecould be used. Images courtesy of Dr Jamie McClelland ofthe Centre for Medical Image Computing, UniversityCollege London. [6]
�

measures of registration quality whichare commonly quoted: accuracy,robustness and consistency. Accuracy(in terms of mm) measures the extentto which corresponding features arecorrectly mapped by registration.Measuring accuracy relies onknowledge of the true, underlying,mapping. The accuracy of registrationdriven by geometrical features can bemeasured directly at those featuresand, for rigid transformations,computed elsewhere. The accuracy ofregistration driven by voxel intensitiesmust usually be assessed usingadditional information. Methods toobtain this information for evaluationpurposes include scanning artificialtest objects (‘phantoms’), usingsynthetic, computer-generated objects(‘digital phantoms’), generating newsynthetic images from existing realscans (e.g. to simulate patient-positioning differences or the impact ofdisease), adding artificial features tosubjects being scanned (e.g. markersattached to the skin), and askingclinicians to manually identifymappings between anatomicalfeatures on a series of test scans. All ofthese methods can be used to measureaccuracy in specific image-pairs andprovided these are chosen to berepresentative of the data collected inthe chosen application, accuracy canbe associated with the registrationmethod when applied to new scans.
Robustness describes the extent towhich mappings can be recoveredunder challenging or non-idealconditions including noisy or restrictedfield of view, differences in patientpositioning, differences in scan typeand differences between subjects.Robustness to positioning differencesis often quoted in terms of a ‘capturerange’ which reports how much initialmisregistration can exist before theregistration procedure fails to convergeto the correct result. In non-rigidregistration applications, robustnessmay not simply refer to positioningdifferences, but also to how variable theanatomy is before registration fails.Applications where this is importanttend to involve parts of the body whichare highly variable even in theindividual, e.g. the abdomen (and itscontents!) imaged on different days, thebreast imaged by digitalmammography over several years, orchanging due to growth or disease. Anydifferences within subjects are usuallymagnified when comparing one personwith another. In some applications it is
SCOPE | TUTORIAL
14 | SEPTEMBER 08 | SCOPE
similarity measures make differentassumptions about the intensityrelationships between registeredimages. Common examples of thesemeasures include normalised crosscorrelation (appropriate whenintensities in one image are linearlyrelated to those in another, e.g. two MRIimages) and mutual information (whereonly a probabilistic relationship existsbetween intensities, e.g. MRI and PET).Intensity-based methods are attractiveas they are largely automatic and makeuse of all the information available inthe images; however they can besensitive to intensity-related artifacts,particularly with an inappropriatechoice of similarity measure. As theunderlying assumption is that atregistration both images contain thesame information, intensity methodsmust also be used with caution whenregistering scans which contain largeage-related or disease-relatedstructural or textural differences. [3]
COMBINING FEATURES ANDINTENSITIESIt has long been recognised that thedistinction between feature-based andintensity-based methods is somewhatartificial and that more powerfulmethods might result if they could becombined. Intensity-based similaritymeasures defined throughout theimages can provide continuity in regionswhich lack features. Features, on theother hand, are a way of injecting priorknowledge about the spatial location,orientation and correspondence ofspecific localised regions which canimprove robustness. Many methodsdefine a composite surrogatecorrespondence measure which is afunction of both feature correspondenceand intensity similarity. Thesecomposite measures must be carefullycrafted and there is usually a parameterchoice to determine the relativeimportance of features over intensities.There are also issues of noisy,artifactual image intensities andfeatures measured by processessubject to error to contend with. Aslightly different approach, typified bythe HAMMER (Hierarchical AttributeMatching Mechanism for ElasticRegistration) method of Shen andDavatizkos, constructs features fromthe intensities themselves. [7] Theseapproaches try and capture the uniqueimage environment at a point bycomputing various intensity-basedmeasures which are functions of thelocal image structure at a number of
different scales; the result is a vectordefined at each point summarising thelocal image content. The underlyingassumption is that points which arebiologically or functionally similar willhave similar local image environmentsand that these image environments willbe substantially different to most otherpoints in the images. The challenges areto define appropriate ways of compactlycapturing this information and toseparate the wheat from the chaff byidentifying so-called ‘salient’ points.These are biologically or functionallysignificant, uncommon but consistent,and therefore reproducibly identifiable interms of their vector description, fromone image to another.
IT LOOKS GOOD BUT IS IT RIGHT?Testing and evaluation of registration isgenerally difficult. The bottom line is thatit is hard to characterise registrationerrors for arbitrary applications inadvance and there are many subtleties inestimating and measuring registrationerror. One of the main ones is thedistinction between optimisationproblems, correspondence problemsand degrees of freedom problems. If thesimilarity measure being used trulymeasures the correspondence betweentwo images then the only thing to worryabout is whether or not a globalmaximum has been found. This is astandard optimisation task (whichdoesn’t mean that it is necessarily astraight-forward task). However, usuallythe similarity measure is anapproximation to the correspondence sowe have to consider whether a globalmaximum necessarily corresponds tothe ‘correct’ registration. To rigorouslydetermine whether a registrationalgorithm has determined the correctcorrespondences between imagesrequires an evaluation procedure whichis independent from the process used bythe algorithm and will usually be morecostly in terms of operator time, imagingtime or computing time. An additionalconfound is that if the transformationclass or the number of allowed degreesof freedom within that class are notsufficient to accurately map thedifferences between two images, thenthe maxima of the similarity measuresare likely to be poorly defined. Inapplications involving clinical imageswhere there may be noise and scanner-induced artifacts in addition tophysiological, population and disease-related differences between scans,evaluation is particularly challenging.
There are a number of different
Geometricfeaturescan be assimple aspointlandmarksbut alsoincludelines,curves,ridges,corners,surfacesetc.
“
”
�

SCOPE | SEPTEMBER 08 | 15
Oneclassicexampleoccurswhenthreescans A, Band C of asubjecthave beencollectedover aperiod oftime
“
”
TUTORIAL | SCOPE
possible to simulate these complicatedvariations using computer models of theanatomy and its response to variousexternal mechanical stimuli includinggravity.
Sometimes consistencymeasurements, again in terms of mm,are reported. The simplest case is whena registration is run twice with theimages designated as reference andfloating swapped between runs. It isdesirable for the obtained mapping to beindependent of the choice of referenceand a measure of inverse-consistencycaptures the extent to which this is true.Many emerging registration methodsare inherently inverse-consistent, atleast to some specified tolerance. Otherconsistency measurements come intoplay when there are several concurrentregistrations. One classic exampleoccurs when three scans A, B and C of asubject have been collected over aperiod of time. It is desirable thatregistering C →A should result in thesame overall mapping as combining themapping from C→B with B→A. Again,some contemporary registrationalgorithms attempt to solve the three-way problem directly to enforce thisconsistency.
CHOOSING THE RIGHTREGISTRATION ALGORITHM Rigid and affine registration is nowreadily available but there remain trapsfor the unwary. The bottom-line inregistration is that it relies on theimages being inherently similar byvirtue of being scans of the samesubject acquired in different ways or ofthe same anatomy in different subjects.Errors can creep in when theseassumptions are violated, usuallybecause of combinations of effectswhich cannot be separated byregistration. For instance, (i) changes intissue morphology (shape) combinedwith distortions introduced by the imageacquisition, (ii) changes in tissue texture(intensity) combined with intensity-related imaging artefacts, (iii) a diseaseprocess which causes changes in bothshape and texture of normal anatomy.Similar problems can occur when aninappropriate correspondence measureor transformation model is chosen.Often, several registration approachesmay need to be trialled for a newapplication. The use of highly non-rigidregistration changes the way analysis isperformed. Some techniques can makeeven very different images highly similarby locally stretching and compressingthe floating image. When rigid
registration is used to align two scans, itis usually just correcting for positionaldifferences. Non-rigid registration isalso correcting for structural differencesfundamental to the scans. After rigidregistration, significant differences inscans are often detected by examiningthe registered images. After non-rigidregistration, significant differences inscans may have been removed by thevery act of registration but thatinformation is encoded in thetransformation parameters used to mapthe images. Therefore after non-rigidregistration, analysis may be performedon the transformation parametersthemselves rather than the registeredimages. In practice, non-rigidregistration is imperfect and there maybe useful information in both theregistered scans and the transformationparameters. In these cases, a hybridanalysis which includes informationfrom both domains may be performed.This is typified by the voxel-basedmorphometry approach to brain scananalysis. [1]
THE PRESENT AND THE FUTUREThere has been immense progress inmedical image registration and it hasdeveloped from early borrowings fromcomputer vision and remote-sensing toa research area in its own right.Registration is a generic problem whichcrops up in many branches of sciencebut applications in medical imaging areparticularly challenging. Three reasonsfor this are the diversity of image types,the diversity of image content and thediversity of application requirements.Related challenges include the relativelyuncontrolled environment in which manyimages are acquired, the inability to testregistration against the ‘truth’ in themajority of every-day applications, andthe critical importance of the registrationbeing correct. If there is a subtle mis-registration in a neuroimaging studyinvestigating normal ageing processes itis potentially damaging to the researcherbut not life-threatening to theparticipants. If there is an undetectedmis-registration between MRI, CT andthe operating environment in image-guided neurosurgery it is potentiallymuch more serious. Hence the relativelyslow transition of registration technologyto front-line clinical applications.
There are many computationalchallenges to address, particularly innon-rigid registration, concerning thepracticalities of optimising a largenumber of transformation parametersover a pair (or a larger number) of
images. Fast registration solutions areparticularly important for intra-operative applications including image-guided interventions. Of moreintellectual interest are fundamentalchallenges related to choice anddefinition of appropriate similaritymeasures and transformation modelsand in particular the potential forinformation from multiple sources to beincorporated into the registrationproblem. The latter can include scansfrom different sources, operator-defined labels, biomechanicaldeformation models, 1D signals such asECG in cardiac applications andstatistical models of the ‘expected’results. A gradual move away from pair-wise registration to the consistentregistration of ensembles of images willcontinue.
There is also evidence to suggestthat registration should not beresearched as an isolated technique.Most basic processing tasks in medicalimaging rely on one or more of threecore technologies: image registration,image segmentation (region labelling)and statistical modelling of images.Knowledge from one of these processescan often strengthen the others. Forinstance, consistently labelled regionson a group of images provide additionalinformation for registration.Registration across the group can beused to generate a statistical model ofpopulation intensity and shapevariation. Such a statistical model canbe used to improve region labelling.Researchers are starting to tackle thesecombined problems directly. The mostcommon example is combining regionlabelling across two or more imageswith image registration. It is thoughtthese combined approaches, whilesuperficially more complicated thanperforming registration or labelling inisolation, are actually more elegant,more robust and make the best use ofall the available information. Combinedapproaches are likely to grow inimportance.
All these advances will rely ondevelopments in maths, numericalanalysis, computer science, physics andmedicine. With the continued expansionof imaging in modern medicine, medicalimage registration and its relatedtechnologies and applications willremain a rich and fertile area for futureresearch. Image registration has thepotential to transform the way we usemedical images and maximise theirvalue for both medical research andpatient care.

SCOPE | TUTORIAL
16 | SEPTEMBER 08 | SCOPE
REFERENCES
1 Ashburner J, Friston KJ. Voxel-based morphometry – themethods. NeuroImage 2000; 11: 805–21.
2 Crum WR, Hartkens T, Hill DLG. Non-rigid registration,theory and practice. Brit J Radiol 2004; 77: S140–53.
3 Crum WR, Griffin LD, Hill DLG, Hawkes DJ. Zen and the artof medical image registration: correspondence, homologyand quality. NeuroImage 2003; 20: 1425–37.
4 Hill DLG, Batchelor PG, Holden M, Hawkes DJ. Medicalimage registration. Phys Med Biol 2001; 46: R1–45.
5 Marcus DS, Wang TH, Parker J, Csernansky JG, Morris JC,
Buckner RL. Open Access Series of Imaging Studies(OASIS): cross-sectional MRI data in young, middle aged,nondemented, and demented older adults. J CognitiveNeurosci 2007; 19: 1498–507.
6 McClelland JR, Chandler AG, Blackall JM, Tarte S, HughesS, Ahmad S, Landau D, Hawkes DJ. A continuous 4D motionmodel from multiple respiratory cycles for use in lungradiotherapy. Med Phys 2006; 33: 3348–58.
7 Shen D, Davatzikos C. HAMMER: hierarchical attributematching mechanism for elastic registration. IEEE T MedImaging 2002; 21: 421–39.
LETTER TO THE EDITORMARC E. MIQUEL
Mark McJury et al.'s article‘Publishing Professional Writing (2)‘contained a lot of good advice.
Although it's certainlyconventional to restrict Resultssections in the way suggested, I'vealways felt it was a disservice to thereader. By its very nature, researchtends to be unpredictable: the resultof an initial experiment oftensuggests a change in design or theaddition of other steps ormeasurements. When you thencome to writing up the Resultssection, it's helpful to the reader ifyou provide a little interpretation tolead them through it. Interpretationin the broader context of currentknowledge should, of course, beconfined to the Discussion.
When I'm refereeing a paper, Iwill allow this sort of latitude, but Isometimes find those refereeing myown submitted work more rigid intheir application of this ‘rule’. Myview is that papers are forcommunication, and if deviatingfrom the accepted straitjacket forpresentations helps communication,I'm all for it.
Of course the guidance in thisarticle will be read by newcomers topublishing, and it's right and properthat they should learn the rules beforebending them.
I could list a few more ‘dos anddon'ts’. Do read the Guide to Authorsand submit in the format requested bythe journal. This is especiallyimportant in the way references arecited and the bibliography isformatted. (Don't assume the endnotestyle is correct either – it often isn't.)Don't repeat the same information inthe text, in tables and in figures. Don'tquote a mean to more decimal placesthan are justified by the standarderror. Believe your own statistics: if Pis greater than 0.5, it's not significantat that level, so try not to be temptedto talk about a ‘trend’. And if P is 0.2for one comparison and 0.7 foranother, it doesn't mean that the firstdifference is ‘more significant’ thanthe second! Remember that theabstract is the only section that will beread by a lot of people, so beresponsible and conservative in theconclusions drawn there.
Finally, I can't resist remarking
that the trouble with writing aboutwriting is that the same standardswill be applied to you. I'm afraid allfour of the authors missed ‘loose’instead of ‘lose’ (p. 20, column 1) and‘very’ instead of ‘vary’ (p. 21, column3)! Perhaps the last word should be:don't rely on spell checkers...
Whoops!
Best wishes
Stanley Salmons, EmeritusProfessor, Department of HumanAnatomy & Cell Biology, Universityof Liverpool
Following the second part of the PublishingProfessional Writing tutorial (Scope 17(2):19-21) Prof. Salmons sent me the following letter:
Letters for publication should be sent to: [email protected]
Always consultreference guidesfor the correctstyles to be used.
�

TUTORIAL | SCOPE
SCOPE | SEPTEMBER 08 | 17
Thank you for letting me have sight ofProfessor Salmons' letter, the pointshe makes are most helpful.Examining the structure and contentof articles published in a broad rangeof professional and scientific journalswould help would-be writersunderstand options available in orderto express themselves and bestrepresent their information / data.Consequently, depending upon thejournal, there can be a wide range ofacceptable ways in which the workmight be presented. Instructions toAuthors can help in elucidating this.
I would like to comment upontypographical errors (and alsostandard of English). I have been theeditor of an international journal for 6years and have listened to theexperiences of many other editors too.On reading published texts, it iscommon to see mistakes, no matterhow minor. Mistakes are fairlycommon in tabloids and fiction / non-fiction books too. Professional andscientific journals are no different andthe level of [minor] errors in some canbe quite high. Some 'financially rich'(and usually eminent) journals andprofessional magazines employ copyeditors to help address theseproblems. These editors are trainedand then employed solely to proof readarticles, to make corrections, pickingup particularly on typographical andgrammatical deficiencies. The [final]published article, as such, is highlypolished. The majority of journals andprofessional magazines cannot affordthe luxury of being able to employ copyeditors. Consequently publishedarticles will be variable in their quality;their quality will be down to the abilityof the author(s) and the editor. In thisscenario the editor is normally aprofessional drawn from the field
Finally, I'd like to add a few comments regarding Scope and proof reading. When we first receive the articles, members of theeditorial team will do some editing (the level of which varies greatly with the editor and the piece itself). The manuscripts arethen sent to the publishers. Century One employs a sub-editor, Karen, who carries out major editing and proof reading;believe me she does a great job. We usually do not send the proofs to the authors as our schedule is very tight, instead Gemmaand I go through the entire set of proofs; it is a time-consuming and ungrateful job as you will always miss something. Forsome features and tutorials, and if the author(s) specifically asks for it, I make an exception and also send them the proofs.This was the case for this tutorial which means it went through seven pairs of eyes before being published and two errors stillsurvived our scrutiny. You might consider it is a lot (well, I do) but I really think only a very small percentage of errors are stillthere when the magazine arrives at the printer.
Proof readingis essential priorto articlepublication.
A reply from Prof. Hogg, co-author
A reply from Marc Miquel
represented by the journal /professional magazine, they might be ascientist or clinical practitioner. It isunlikely their professional backgroundwould be in journalism or editing. I fallinto this category. Given that manyjournals and professional magazinesoperate upon this basis the onus placedupon the author(s) to get it rightbecomes critical. Proof readingimmediately prior to article submissionis essential and should not be treatedlightly. In our case, in spite of givingsight of the final version to all authorsfor comment we still managed to missone grammatical error and onetypographical error. I am really pleasedthat Professor Salmons spotted theseerrors as it gave us another chance tohighlight the importance of proofreading prior to submission. Let this bean important lesson to us all, no matterhow experienced or inexperienced wethink we are.
Finally, on the theme of standard ofEnglish, we are told that the[contemporary] spoken word is poorlyrepresented too. Only yesterday
morning, during BBC’s Breakfast TVprogramme, an expert in English wascommenting that the standards ofnewsreaders had slipped to aparticularly low level. He claimed thatgrammar was poor. He also claimedthat there was often an inappropriatechoice of words.
What is the solution if one is notparticularly gifted at spoken or writtenEnglish? I would suggest that you getadvice from somebody who is. Thiswould be done prior to submitting thework to a journal or giving a paper at aconference. Consequently, during theproof reading phase consider gettinghelp from somebody who is good at[written] English and has an eye fordetail.
Yours sincerely,
Professor Peter Hogg, University ofSalford
PS. Would you mind proof reading thisletter carefully, because I am certainthere will be a mistake or three!
�

MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 23
CAN OPEN SOURCE SOFTWARE BE USED FOR CLINICAL WORK?
KING’S FUND, LONDON 7th November 2007
DOM WITHERS Formerly Guy’s & St Thomas’, now at Computerized Medical Systems
IN NOVEMBER 2006 INFORMATICS and ComputingSIG (ICSIG) considered the idea of a meeting to discussthe possibility of writing an open-source MU (monitorunit) check program; many hospitals write their own, socollaboration seems sensible to produce a programdeveloped and tested by many different centres. Thismeeting idea evolved to a more general title, to addresspractical and legal aspects of sharing software inhealthcare.
In the introduction, Dom Withers (Guy’s & StThomas’ Hospital, London) gave some definitions: theOpen Source Initiative (www.opensource.org) says:‘Open Source is a development method for software thatharnesses the power of distributed peer review’; the FreeSoftware Foundation (FSF, www.fsf.org) is quitedefensive in its definition of free software, listing fourfundamental freedoms that must be complied with inorder for software to be ‘free’: the oft-used phrase is ‘freeas in speech, rather than free as in beer’.
LEGAL IMPLICATIONSPhil Cosgriff (Pilgrim Hospital, Boston, Lincolnshire)gave a useful overview of the issues, with the disclaimer‘I am not a lawyer’. Phil's four reasons for a perceiveddecline of in-house software were: commercial softwarehas improved; physicists have less time to spend writingsoftware; there are questions about competency, andlegal liability presents worries. If your software is amedical device you can use it yourself and the MedicalDevice Regulations do not apply. If you give it away orsell it to another legal entity, then the regulations apply.There is room for manoeuvre in the interpretation ofwhat constitutes a medical device.
Most open source software used in healthcare wouldnot be considered a medical device. Talks were givenwhich showed such successful and useful applications.
Dudley Ibbett (Derby Hospitals, Derby) describedapplications used in his nuclear medicine department,including packages that monitored QC readings onradionuclide calibrators and gamma cameras and kepttrack of radioactive waste. Dudley also talked about thevalidity of disclaimers in licences, and quoted from theUnfair Contract Terms Act of 1977: ‘Liability for death orpersonal injury resulting from negligence cannot beexcluded or restricted by any contract term or notice’.This seems to suggest that software authors cannotdisclaim responsibility for the use of their software.
James Moggridge (St George's Hospital, London)uses JDICOM and the dcm4che DICOM toolkit to createworklists for use with a PACS system. This has reducederrors in demographic data entry and increasedworkflow efficiency.
Gunaranjan Bose (Queen Elizabeth Hospital,Birmingham) described a web-based system to facilitatemovement of radiotherapy and diagnostic images
between different hospital systems. The medical physicsdepartment has a dedicated computing section whichprovides such software. Another database system for QAwas described by Lindsay Cherry (Edinburgh CancerCentre) which used Visual C#.NET and featured a GUIthat could be used to add and retrieve records.
Invited speaker Matt Lee (GNU Project,www.gnu.org) spoke on ‘Examining freedom – freesoftware in healthcare’. He emphasised the differencesbetween the Open Source Movement and the FreeSoftware Foundation from his viewpoint; in particular,not all open source software can be described as ‘free’.The FSF wants users to have these freedoms: to run theprogram, for any purpose; to study how the programworks, and adapt it to their needs; to redistribute copiesso they can help their neighbours; to improve theprogram, and release their improvements to the public,so that the whole community benefits.
Matt pointed out the social and philosophicalsimilarities of the FSF and the NHS – a desire to offerservices free to all. It is obvious that this radicalism hasbeen diminished in today’s NHS, where Trusts areseparate legal entities, encouraged to protect and profitfrom their intellectual property rather than share for thebenefit of all.
EXAMPLES OF SOFTWAREEd McDonagh (Royal Marsden Hospital, London)presented IQWorks – a collaboration between the RMHand NHS Lothian in Edinburgh, developing a softwarepackage for automating CT QC procedures. IQWorksuses 11 packages, all issued under different licences. As atool specifically designed for measuring a medicaldevice, IQWorks can be considered a medical deviceitself.
More obviously, a radiotherapy treatment planningsystem (TPS) is a medical device, and Henry Lawrence(Bristol Haematolology and Oncology Centre, Bristol)talked about open source TPSs developed in the UK andabroad, including a project he worked on calledEuroplan, designed to work on affordable PC hardwarefor developing countries. Henry also described accidentsin radiotherapy due to errors in the implementation anduse of TPSs: open source development could help usersunderstand their algorithms more thoroughly, and allowtesting by third parties to limit the likelihood of errors.
Alan J. Green (Centre for Professional Ethics,University of Keele) examined ethical considerations in atalk entitled ‘Trust me, I’m a geek’. He emphasised thatthe chain of trust has a loose end when using opensource software, and that chain ‘must be anchored onyour desk’, as Alan put it – the responsibility will liewith the person implementing it.
Concluding roundtable discussion was extensive.With no definite legal answer to the meeting’s title, it �

two fronts: firstly, to produce guidelines for thedevelopment of in-house software, building on guidelinesproduced by the British Computer Society and others;and secondly, by creating example case studies indicatinghow open source software could be used in healthcare, tocirculate to interested parties such as the National PatientSafety Agency, the NHS Litigation Agency, MHRA andCfH (Connecting for Health).
If you would like to take part in either of theseprojects, please contact ICSIG Chair Ed McDonagh([email protected]). �
SCOPE | MEETING REPORTS
24 | SEPTEMBER 08 | SCOPE
ADVANCED NEUROLOGICAL MR: CLINICAL APPLICATIONS UPDATE
THE UCL INSTITUTE OF CHILD HEALTH, LONDON 13th February 2008
JOHN THORNTON The National Hospital for Neurology and Neurosurgery, London
MAGNETIC RESONANCE (MR) IMAGING of the brainhas continued to progress markedly in the last 15 years,exciting developments precipitating new insights into thestructure, function and physiology of the nervous system.More recently, advanced quantitative neurological MRmethods, originally developed in a neuroscience-researchcontext, have begun to find application in hospitalimaging departments, contributing directly to patientdiagnosis, monitoring and treatment.
Close to 50 participants attended this one-day meetingorganised by the MR SIG, co-sponsored by the BritishAssociation of MR Radiographers, and supported by theBritish Chapter of the International Society of MagneticResonance in Medicine. Speakers, including a number ofthe UK’s leading authorities on neuro-MR physics,addressed an audience comprising a multi-disciplinarycross-section of hospital physicists, academic researchers,clinicians and MR radiographers.
Gareth Barker (King’s College London) began themorning session with a comprehensive overview ofquantitative MR, starting with the premise that the MRscanner may be usefully treated as an instrument forscientific measurement, rather than simply an imageformation device. In this invited talk, Gareth provided asummary of the underlying physics, acquisitionrequirements, analysis strategies and clinical applicationsof a variety of methods, including high-resolutionmorphometry, relaxometry, magnetisation transferimaging and diffusion tensor imaging (DTI).
DIFFUSION TENSOR IMAGINGThe theme of diffusion tensor imaging was furtherdeveloped by the next two invited speakers, Derek Jones(University of Cardiff) and Chris Clark (UniversityCollege London). Derek provided an in-depthintroduction to the physics of DTI and the metricsavailable to quantify aspects of nervous tissuemicrostructure and geometric organisation, including thetechnique of ‘diffusion tractography’, a method with thepotential to non-invasively trace specific white mattertracts in the human brain. A number of clinicalapplications were reviewed, as well as the advantages
and potential pitfalls of the various approaches to dataanalysis. Chris Clark reviewed the applications of DTI inthe specific area of neurosurgical planning, where theability to delineate white matter tracts may providesurgeons with information vital in planning their surgicalapproach to, for example, tumour resection. While dataanalysis methods are not yet mature, and the technique ispresently limited to specialist research centres, initialcorroborative comparisons with intra-operative corticalstimulation data, and successful neurosurgical outcomes,are very encouraging.
ADVANCED NEURO-MR IN PAEDIATRICSAfter coffee two speakers explored paediatricapplications of advanced MR techniques. In his invitedpresentation, David Gadian (UCL Institute of ChildHealth, London) described work addressing therelationships between focal brain abnormalities, asdetermined by MR methods such as voxel-basedmorphometry, volumetry and T2 relaxometry, andcognitive function as measured on neuropsychologicaltesting. Fascinating examples illustrated the success ofthis approach in children with temporal lobe epilepsy, astudy in an extended family with an inheritedneurodevelopmental condition, and cases ofdevelopmental amnesia. Ernest Cady (UCLH NHSFoundation Trust, London) next described applications ofMR imaging and particularly MR spectroscopy, a methodproviding a non-invasive window into brainbiochemistry, to the detection of brain injury in newborninfants. These techniques can provide vital prognosticinformation in the first few days of life, and informationinvaluable in the clinical management perinatalencephalopathy, especially with the recent availability forthe first time of cerebroprotective therapies such ascerebral hypothermia.
CEREBRAL BLOOD FLOWThe afternoon session commenced with an overview ofclinical cerebral perfusion MRI provided by IainWilkinson (University of Sheffield). Assessment of thelocal blood supply to the brain is important in patients �
was suggested that a tried case may be required toestablish precedent. Medical device directives preventsharing software between hospitals. As physicists andengineers, we would like the freedom to choose whattools we want to use, accepting that we have theprofessional responsibility to go through an acceptanceand commissioning process – much as we already do forcommercially-bought medical devices. The benefits of theopen source model are obvious but require, in ourcommunity, willing developers with time available.
Further action is required, and ICSIG is working on

MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 25
FIGURE 1.Functional MRimaging resultsobtained duringpreparation forsurgical resectionof a brain tumourvisible in the lowerright-hand cornerof the images. Thehighlighted areasrepresent regionsof brain activityassociated withvarious motorfunctions. Thedata are useful inneurosurgicalplanning whereminimisingdamage to theseregions, therebyreducing post-surgical functionalimpairment, is apriority.Slide provided byDr Laura Mancini,National Hospitalfor Neurology andNeurosurgery,London, andreproduced bypermission.
�
FIGURE 2.Images producedwith a number ofcomplementaryMR imagingtechniques in apatient with anacute strokeshowinganatomicalimages (top row)and imagesdepicting changesin the diffusionproperties oftissue water,cerebral bloodflow and an MRIangiogram(bottom row).Slide provided byDr Iain Wilkinson,University ofSheffield, andreproduced bypermission.
�

SCOPE | MEETING REPORTS
26 | SEPTEMBER 08 | SCOPE
RADIATION PROTECTION IN NUCLEAR MEDICINE
BRITISH INSTITUTE OF RADIOLOGY 27th February 2008
DR MF DEMPSEY West of Scotland PET-CT Centre
THIS MEETING WAS JOINTLY organised by the NuclearMedicine and Radiation Protection Special InterestGroups (SIGs). Wendy Waddington (UCL Hospitals NHSFoundation Trust, London) and Michaela Moore(Newcastle General Hospital, Newcastle) were thescientific organisers representing each SIG, respectively.Recent expansion and diversification of nuclear medicineservices has provided us with significant radiationprotection challenges. Consequently, there was littlesurprise that this one-day meeting offered a packedprogramme to a packed lecture theatre – the BritishInstitute of Radiology was full to capacity with manymore expressions of interest but unfortunately, despiteIPEM’s efforts, an alternative larger venue could not beidentified.
Wendy Waddington opened the day by highlightinghow the significant interest shown in this meetingreflected how timely it was for the SIGs to co-host such anevent and perhaps organisation of joint meetings by theseSIGs is something that should be re-visited moreregularly.
PET ISSUESWith the recent rapid growth in the use of PET imagingin the UK, the first session of the morning was dedicatedto this theme. Deborah Tout (Christie Hospital,Manchester) provided a review of extremity dosemonitoring at the Christie Hospital Manchester andillustrated how this work was used to improve design oftheir new dispensary area. In a similar vein, MatthewGuy (Royal Surrey County Hospital, Guildford)presented on how his team had employed a review ofvideo monitoring data in combination with extremitydose monitoring to minimise staff extremity doses.
Following this, Debbie Peet (Royal Surrey CountyHospital, Guildford) presented on the RPA’s perspectiveon radiation protection challenges for mobile PET/CTwith ‘challenges’ being the operative word. By virtue ofbeing mobile, the shielding and physical space of theseunits is limited (as illustrated in figure 1) with seriousimplications for radiation doses to staff and potentiallymembers of the public using the car park or working innearby buildings. Facility design has to consider patient
�
with a number of conditions such as transient ischaemicattacks, disabling stroke, fits and headache, and haspotential for staging and grading tumours. There arecurrently two complementary MR perfusion methods:dynamic susceptibility-contrast imaging, wherein thepassage of an injected bolus of paramagnetic tracerthrough the vascular bed may be followed, and arterialspin labelling (ASL), in which blood magnetisation ismanipulated to provide an entirely non-invasiveendogenous contrast label. While both methods presentdifferent challenges in terms of absolute quantificationand sensitivity, the clinical assessment of cerebralperfusion by MRI is set to expand as the methodologiesimprove and new applications emerge. Iain’s invitedoverview was followed by a presentation of anexperimental study of methodological aspects of ASL,presented by Marta Varela (HammersmithHospital/Imperial College London). Marta described herwork in determining the T1-relaxation time of blood andpresented encouraging results from both adults andnewborn infants, which may significantly improve theaccuracy of ASL perfusion measurements.
In a sharp change of subject matter, DavidCarmichael (UCL Institute of Neurology, London) nextpresented experimental work addressing the safety ofusing MR imaging to accurately determine intracranialelectrode locations during the presurgical work-up ofpatients with temporal lobe epilepsy. Computersimulations were presented depicting theelectromagnetic interactions between the MR scannerand the conducting electrode implants, suggesting thatwith suitable precautions electrode-associated tissue
heating during MR imaging should remain within safelimits.
FMRI AND NEUROSURGICAL PLANNINGAfter a tea break, the final two speakers presented clinicalapplications of functional MR imaging (fMRI), in whichactive brain regions may be detected due to localisedblood-oxygenation changes which modify the MRproperties of tissue. Laura Mancini (National Hospital,Queen Square, London) gave an overview of how fMRImay be useful in identifying areas of eloquent cerebralcortex in the presurgical planning stages of tumourresection, in order that damage to areas directlyimplicated in for example motor or speech function maybe minimised. This approach complements, and isincreasingly used in conjunction with, the diffusiontractography method described by the morning speakers.Finally, Sarah Peel (Southampton University HospitalsTrust) addressed the tricky issue of the reliable presurgicaldetermination of language lateralisation by fMRI usingjust an auditory prompt, in the absence of a sophisticated(and expensive) visual projection system. Thepresentation prompted a lively discussion of variousmethodological alternatives to providing patients withshouted instructions to ‘stop thinking!’ during the restperiods of fMRI acquisitions, and provided an excellentillustration of the value of meetings such as this inbringing together members of the academic researchcommunity with clinical practitioners to exchangemethodological expertise on the one hand, andknowledge of important real-world clinical applicationson the other. �
�

MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 27
FIGURE 1.Diagram showingplan of mobile PETunit (courtesy ofDr Debbie Peet).
�
FIGURE 2.Table showingpeptide receptorradioligands indevelopment(courtesy of DrGlenn Flux).
�

SCOPE | MEETING REPORTS
28 | SEPTEMBER 08 | SCOPE
clerking, dose preparation, administration and uptake,toilets and scanning. There are many RSA93 issues to beovercome which ultimately require cooperationbetween employers, RPAs and estates departments.Furthermore, risk assessments/training requirementsmust be considered for work in such a newenvironment in addition to working through all thelogistical issues regarding deliveries, QC testing etc.and potentially dealing with radioactive spills indifficult locations. As if these RPA radiation protectionissues are not challenging enough, Debbie indicatedthat the MPE with responsibility for resolving the manysite and equipment specific IRMER and ARSACconsiderations does not have an easy task either!
RADIONUCLIDE THERAPYFollowing a coffee break, the first invited speaker of theday, Glenn Flux (Royal Marsden Hospital, Sutton),gave us food for thought by presenting on the manynew products that could be making their way to nuclearmedicine departments in the UK in the near future(some examples are shown in figure 2). Of course suchdevelopments in patient care are always welcome butthe intrinsic radiation protection challenges need someattention. For example, with the new alpha emittingagent of Ra-223, are we prepared for its arrival? Havewe considered RSA93 issues (waste disposal) andlicences? Do we know how we would deal with spills?With an imminent phase 3 multicentre trial involvingseveral UK sites, will we be expected to resolve all theseradiation protection issues in a short time? Glennsuggested that a systematic and supported introductionof this and other new agents would be hugelybeneficial.
Philip Anderson (Queen Elizabeth Hospital,Birmingham) then presented the results of a multicentrestudy on internal radiation dose to families ofthyrotoxic patients treated with I-131. It was reassuringto hear that although transfer of contamination canoccur to family members (thought to be primarilythrough salivary routes), internal dose to familymembers is low. Combining this with a previous studyon external dose to family members, findings suggestthat most families can comply with EU recommendeddose limits/constraints. Fred Wickham (Royal FreeHampstead NHS Trust, London) then discussed twodifferent techniques on calculating restriction periodsfor patients discharged following I-131 therapy forthyroid cancer before Richard Fernandez (Guy’s & StThomas’ Hospital, London) illustrated how periodicenvironmental monitoring to check areas remainadequately designated can prove hugely worthwhile –he demonstrated that sometimes a small change topractice can significantly affect designation of nearbyareas. Fionnuala Barker (St Luke’s Hospital, Dublin)then showed how in-patient treatment of thyroid cancerpatients with significant physical disabilities is possibledespite what may seem like daunting radiationprotection issues. This session was brought to an end byHamish Richardson (King’s College Hospital, London)discussing nurse training in radio-iodine therapy.
CT IMAGING IN NUCLEAR MEDICINEBe it as part of the explosive growth of SPECT/CT orPET/CT systems in nuclear medicine, an increasing
number of nuclear medicine staff have to get to gripswith CT. The first presentation after lunch was by DavidPlatten (King’s College Hospital, London), the secondinvited speaker of the day, talking about radiationprotection in CT. David provided a very comprehensivereview of shielding issues, scanning protocols, imagequality parameters, single vs. multi-slice and doseoptimisation. Shielding requirements really depend onthe current and planned use of the facility, e.g. will theCT be used diagnostically or for anatomical localisationand attenuation correction purposes? Regarding imagequality parameters, he stressed that unlike doseadministration in nuclear medicine, there is not alwaysa linear relationship between image quality parametersand effective dose, e.g. changing from 80 kVp to 100kVp with all other parameters constant could effectivelydouble the patient’s dose.
On a similar theme, Dudley Ibbett (DerbyshireRoyal Infirmary, Derby) then presented on lookinginside the dosimetry black box of SPECT-CT. Thisinvolved consideration of calculating effective dosefrom DLP, pregnancy issues and IRMER trainingrequirements to minimise risk if incorrect exposure.
AND SOME OTHER STUFFOf course there are always other radiation protectionissues affecting nuclear medicine departments. The firstpresentation to fall under this umbrella was by BenJohnson (Guy’s & St Thomas’, London), whose reporton the recent experiences at Guy’s and St Thomas’ oftransport inspections of both the old and new transportregulations. Richard Peace (Royal Victoria Infirmary,Newcastle) then presented on the issues of nuclearmedicine patients at UK ports and airports and therecent ARSAC guidance on this – some discussion post-presentation led to the suggestion that a credit card typedocument should be given to patients for thesepurposes – several departments already do this andadvocate the practice. Mike Haddaway (Robert Jones &Agnes Hunt Orthopaedic & District Hospital,Oswestry) then presented on the incidence andimplications of extravasation of bone scans suggestingthat the incidence is probably greater than we think asextravasation dissipates with time. Dr Ibbett thenreturned to the floor for his second presentation of theday about improving compliance with an RSA93Accumulation and Disposal of Radioactive WasteAuthorisation Certificate. He discussed the introductionof best practicable means into these certificates andsubsequent implications. The final presentation of theday was by Hugh Wilkins (Royal Devon & Exeter NHSTrust, Exeter) on using wristbands to identifyradioactive in-patients. With the National Patient SafetyAgency standardising the wristbands nationally,making use of this system to identify nuclear medicinepatients returning to wards may not be feasible formuch longer.
IN SUMMARYThis was a well-organised, well-attended interactivemeeting with a good complement of invited speakersand proffered papers. For those who didn’t get a spacebecause it was such a rapid sell-out, the good news isthat a re-run has been organised for 4th November 2008(further details to be posted shortly). �
�

MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 29
ICMP 2008: CURRENT AND FUTURESCIENCES IN RADIATION MEDICINE
DUBAI, UNITED ARAB EMIRATES 14th–16th April 2008
DAVID1 AND ROSEMARY2 EATON 1Royal Free and 2Guy’s & St Thomas’ Hospitals, London
BRIEF HISTORY IN 1894, SHEIKH Maktoum bin Hasher al-Maktoumexempted foreign traders from paying tax in a smallfishing settlement on the Arabian peninsula. A century ofexponential growth later and Dubai is an internationalhub of industry, commerce and tourism. Contrary topopular belief, only 10 per cent of Dubai’s income isderived from oil, but generous investment by a series ofambitious rulers has provided the infrastructure andiconic buildings to match the booming economy. Theemirate is currently home to the world’s only 7-star hotel(the scale was extended specially after construction), theBurj al-Arab, and the world’s tallest building, the BurjDubai. Construction on an unprecedented scale isproceeding apace (figure 1), including extension of theexisting coastline with an artificial marina and series ofislands in the shape of palm trees and the entire world.The Health City district aims to attract internationalclinics into setting up outposts there, making Dubai a‘world hub in curative tourism’.
Although medical physics had been practised in the
United Arab Emirates (UAE) for more than two decades, itwas only in 2005 that the profession became officiallyestablished. A physics department was created at theDubai Hospital and the Emirates Medical Physics Society(EMPS) was inaugurated. The following year the societyjoined the International Organisation of Medical Physics(IOMP). Through this connection, and in recognition ofdevelopment throughout the Middle East in healthcarescience, the International Conference on Medical Physics(ICMP) was hosted by Dubai in 2008. The 350 delegatescame from all over the world, but the Middle East, Africaand Asia were particularly well represented.
INFORMATION AND COLLABORATIONThe title of the conference was ‘Current and FutureSciences in Radiation Medicine’, and it had two mainaims: the first was to inform and educate participants inthe latest developments around the world. For thispurpose invited presentations were given by a host ofinternationally renowned speakers in plenary sessions andeducational streams. The second aim was to provide a
FIGURE 1.Outside theconferencecentre, theworld’s tallestbuilding loomslarge in thedistance.
�
�

SCOPE | MEETING REPORTS
30 | SEPTEMBER 08 | SCOPE
FIGURE 2.The keynotepresentation onIGRT given by afamous Canadian(at heart) medicalphysicist.
�
forum for local departments to present their own researchand share ideas.
In the opening ceremony, Barry Allen (Centre forExperimental Radiation Oncology, University NSW,Australia and IOMP chairman) challenged delegates toconsider ‘what is the greatest benefit to the most people inyour country?’ when weighing up all the technologiesand techniques on offer. He also reminded us that ‘scienceis international, beyond national boundaries’ and thiscollaborative spirit could be clearly seen during the week.‘People to people contact is the most important [aspects ofthe meeting]’, said one Pakistani physicist over lunch.With over 150 proffered oral and poster presentations,from more than 35 countries, there was plenty to talkabout.
PRESENT AND FUTURETwo symposia book-ending the first day described thecurrent and potential future state of radiation therapy.William Hendee (Medical College of Wisconsin, USA)described how image-guided radiotherapy (IGRT) isbringing together diagnostic and therapeutic disciplinesonce again. As with image-guided ablation, or surgery,‘precise [physical] delivery requires precise [biological]knowledge’. In the future, we can expect a shift frommargins to molecular differentiation with greaterhybridisation of modalities broadening the physicist’sremit like never before. However, the responsibilities ofthe profession remain unchanged:� expansion of knowledge;� contribution of research;� involvement in patients;� assurance of quality;
� excellence of teaching;� accountability of performance.
The keynote address continued the topic of IGRT andwas given by Rockwell Mackie (University ofWisconsin, USA). He described the benefits of dailyimaging in greatly reducing setup errors greater than 3per cent and visualising tumour shrinkage. He alsodescribed progress in deformable registration andadaptive planning. In the future, radiotherapy mayexpand its remit into the realms of surgery andchemotherapy, with increasing precision and ability totreat metastatic disease (figure 2).
The ever-present concerns of risk and staffing levelswere addressed by Cari Borrás (Washington, DC, USA)who described work by AAPM task group 100 onrevising guidelines for quality assurance inradiotherapy. Their report will contain detailed processtrees with failure mode and effect analysis to allowdepartments to quantify risks and focus on the greatestones. In the ensuing discussion, it was suggested by onespeaker that the greatest risk in radiotherapy isunderdosing from lack of clinical aggression, or sideeffects from denial of the latest technologies. However,the take home point for these authors was howadvanced the UK is to have staffing levels supported bylegislature and an established formal training scheme. Italso became clear during the week that UK publicationsare often taken as a benchmark for many countriesdeveloping their own reference systems. For example,IPEM Reports, dose survey data published by theformer NRPB and ImPACT’s CT Dosimetry Calculatorwere all mentioned during the conference, with littleneed for explanation.
�
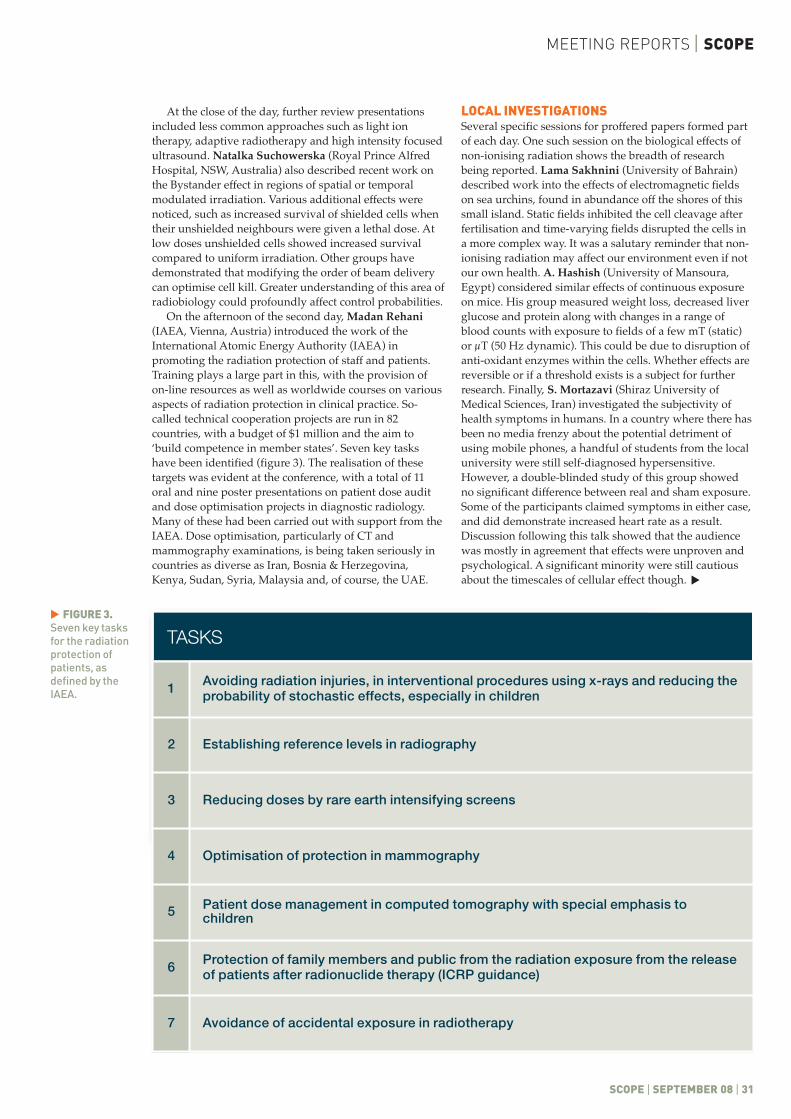
MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 31
At the close of the day, further review presentationsincluded less common approaches such as light iontherapy, adaptive radiotherapy and high intensity focusedultrasound. Natalka Suchowerska (Royal Prince AlfredHospital, NSW, Australia) also described recent work onthe Bystander effect in regions of spatial or temporalmodulated irradiation. Various additional effects werenoticed, such as increased survival of shielded cells whentheir unshielded neighbours were given a lethal dose. Atlow doses unshielded cells showed increased survivalcompared to uniform irradiation. Other groups havedemonstrated that modifying the order of beam deliverycan optimise cell kill. Greater understanding of this area ofradiobiology could profoundly affect control probabilities.
On the afternoon of the second day, Madan Rehani(IAEA, Vienna, Austria) introduced the work of theInternational Atomic Energy Authority (IAEA) inpromoting the radiation protection of staff and patients.Training plays a large part in this, with the provision ofon-line resources as well as worldwide courses on variousaspects of radiation protection in clinical practice. So-called technical cooperation projects are run in 82countries, with a budget of $1 million and the aim to‘build competence in member states’. Seven key taskshave been identified (figure 3). The realisation of thesetargets was evident at the conference, with a total of 11oral and nine poster presentations on patient dose auditand dose optimisation projects in diagnostic radiology.Many of these had been carried out with support from theIAEA. Dose optimisation, particularly of CT andmammography examinations, is being taken seriously incountries as diverse as Iran, Bosnia & Herzegovina,Kenya, Sudan, Syria, Malaysia and, of course, the UAE.
LOCAL INVESTIGATIONSSeveral specific sessions for proffered papers formed partof each day. One such session on the biological effects ofnon-ionising radiation shows the breadth of researchbeing reported. Lama Sakhnini (University of Bahrain)described work into the effects of electromagnetic fieldson sea urchins, found in abundance off the shores of thissmall island. Static fields inhibited the cell cleavage afterfertilisation and time-varying fields disrupted the cells ina more complex way. It was a salutary reminder that non-ionising radiation may affect our environment even if notour own health. A. Hashish (University of Mansoura,Egypt) considered similar effects of continuous exposureon mice. His group measured weight loss, decreased liverglucose and protein along with changes in a range ofblood counts with exposure to fields of a few mT (static)or µT (50 Hz dynamic). This could be due to disruption ofanti-oxidant enzymes within the cells. Whether effects arereversible or if a threshold exists is a subject for furtherresearch. Finally, S. Mortazavi (Shiraz University ofMedical Sciences, Iran) investigated the subjectivity ofhealth symptoms in humans. In a country where there hasbeen no media frenzy about the potential detriment ofusing mobile phones, a handful of students from the localuniversity were still self-diagnosed hypersensitive.However, a double-blinded study of this group showedno significant difference between real and sham exposure.Some of the participants claimed symptoms in either case,and did demonstrate increased heart rate as a result.Discussion following this talk showed that the audiencewas mostly in agreement that effects were unproven andpsychological. A significant minority were still cautiousabout the timescales of cellular effect though.
FIGURE 3.Seven key tasksfor the radiationprotection ofpatients, asdefined by theIAEA.
�
TABLE 1TASKS
1 Avoiding radiation injuries, in interventional procedures using x-rays and reducing theprobability of stochastic effects, especially in children
2 Establishing reference levels in radiography
3 Reducing doses by rare earth intensifying screens
4 Optimisation of protection in mammography
5 Patient dose management in computed tomography with special emphasis tochildren
6 Protection of family members and public from the radiation exposure from the releaseof patients after radionuclide therapy (ICRP guidance)
7 Avoidance of accidental exposure in radiotherapy
�

SCOPE | MEETING REPORTS
32 | SEPTEMBER 08 | SCOPE
SOUTH WEST IPEM MEETING:REGIONAL UPDATES
CHELTENHAM GENERAL HOSPITAL 9th–10th May 2008
PENNY LATIMER AND AMANDA BRASON Gloucestershire Hospitals NHS Trust
THIS YEAR THE SOUTH WEST IPEM meeting washosted by Gloucestershire Hospitals NHS Trust(GHNHST) (figure 1). While many conferences focus on aparticular topic, regional meetings offer an opportunity tohear about some of the varied work being carried out inengineering and physics groups locally. Some talks covertopics that are applicable to many departments such astraining and competency assessments, by MoradToussand (Medical Equipment ManagementOrganisation, MEMO, Bristol) or risk assessmenttechniques, by Nick Powell (Royal Cornwall HospitalsNHS Trust, Truro). Others offer a reminder that there islife outside one’s own speciality!
NEW SOUTH WEST REPRESENTATIVEThe programme started on Friday afternoon with a headsof department meeting. In the evening delegates had aguided tour of Gloucester cathedral followed by a mealand the first talk of the meeting. This was given by BrianWitcombe (GHNHST), a winner of the Ig Nobel Prize forhis paper on ‘Sword swallowing and its side effects’.
The main meeting started the next day in Cheltenhamand began with an introduction to the developments and
structural changes taking place at the IPEM. It was anopportunity for the new IPEM South West representativeLiz Pitcher (Bristol General Hospital) to introduce herselfand request feedback so that she could accuratelyrepresent the members from the region at meetings.
During the first session, Dominic Nolan (SalisburyDistrict Hospital) talked about the work to developtechnology to support a teenager with a C1 spinal cordbreak. The engineering challenge was to find and developappropriate methods of access to everyday activities, inparticular communicating through different media, andusing equipment such as television and a PC. Part of thesolution was to adapt an eye tracking computer system.Dominic described the system used for this patient(MyTobii) and how the complexity of access was tailoredto meet the patient’s needs. In addition they havedeveloped an EMG switch which is worn on the patient’sforehead. As a result of the work, this patient now hasaccess to email, text messaging and internet along withcomputer games and music.
John Archer (Gloucester Royal Hospital) presented hisPhD research work on the application of Ramanspectroscopy to cerebral tissue as a potential tool to
Poster presentations were on a similar breadth oftopics. Highlights for these authors included:� Design and fabrication of a prototype add-on
multileaf collimator (Avicenna Research Institute,Mashhad, Iran);
� Effects of natural radiation on neural function inBrazil (Dawnesh Research Institute, Barcelona,Spain);
� Assessment of gamma background in outdoor andindoor areas in Zanjan province (Zanjan University ofMedical Sciences, Iran).
UK INVOLVEMENTIn addition to the handful of UK delegates, several of theinvited speakers were from Britain and a number ofIPEM members serve on the committees of IOMP.
Martin Leach (Institute of Cancer Research and RoyalMarsden Hospital, Sutton) described current progress inthe use of magnetic resonance techniques in cancerbiology; in particular, how dynamic contrastenhancement, diffusion-weighting and spectroscopy canbe used to visualise cell vasculature, death andmetabolism, respectively. He also related theestablishment of MR screening for women at high risk ofdeveloping breast cancer, and NICE guidelines for itsuse alongside mammography in a cost-effective manner.
Richard Bowtell (University of Nottingham)presented the latest results from the UK’s only 7Tscanner, weighing the advantages and disadvantages ofa high field system. Features resulting from shorter T2*,
longer T1, increased signal-to-noise and so on weredescribed. One area of detailed investigation was use ofthe phase information available from increasedsusceptibility effects. After some complex processing, itwas possible to construct susceptibility maps, givingeffectively susceptibility-weighted images.
The EMITEL project, an online encyclopaedia andmultilingual dictionary of medical physics, wasdescribed by Peter Smith (Northern Ireland MedicalPhysics Agency, Belfast). It will contain several thousandpeer-reviewed articles at MSc level and above, with 1,200currently written. Translation of key terms between 20languages, including Arabic, will be possible. The projectis aiming for an official launch at the World Congressnext year. In the meantime, further details can be foundat http://www.emerald2.eu.
The ICMP was an eye-opening chance for theseauthors to gain a better understanding of how far andhow fast medical physics has developed around theworld. However, it is also apparent that the UK hasmuch to offer the wider medical physics communityfrom our own experiences. The next internationalmeeting to be hosted by the IOMP will be the 2009 WorldCongress on Medical Physics and BiomedicalEngineering. This will be held a little closer to home inMunich, so why not start writing that abstract now? �
FOR MORE INFORMATIONEducational presentations can be found on the conferencewebsite (http://www.icmpdubai.com/sp/default.asp) along withabstracts for all talks and posters.
�
�
MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 33
FIGURE 1.Gloucester RoyalHospital (left) andCheltenhamGeneral Hospital.
�
FIGURE 2.Image derivedfrom an artcollaboration atGloucestershireHospitals NHSTrust.
�

SCOPE | MEETING REPORTS
34 | SEPTEMBER 08 | SCOPE
FIGURE 4.Several speakersdiscussed dosesin diagnosticradiology.
�
FIGURE 3.The new OxfordCancer andHaematologyCentre.
�

MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 35
diagnose dementias. The work hopes to aid moreaccurate diagnosis of Alzheimer’s disease, which iscurrently identified using the patient’s symptoms. Theuse of drugs to treat this disease is expensive and adefinitive test is needed to establish who would benefit.John’s research used ethically-approved post-mortembrain tissue from patients that had either Huntington’sdisease, Alzheimer’s disease or were a normal control.By using multivariate analysis and processing hedisplayed results that could identify the differentpathologies. The research will be used to find outwhether other less invasive tissue could be used andother neurodegenerative diseases could be identified.
Later in the session, Belinda Christie (GHNHST)gave a presentation on the experiences that the NuclearMedicine Department in Gloucester had with an artist inresidence. The project aimed to promote the profile oflesser-known departments to the public through art. Theartist, Simon Ryder, developed his ideas over 6 monthsand kept a blog of his experiences as a non-scientificperson in this environment. One interesting idea thatSimon and Belinda developed was to image nature usingradio-isotope Tc99m. This led to various flowers andleaves being applied with radioactive material. As wellas being a useful training exercise on the uptake andimaging of radioisotopes, it also generated somestunning images. They concluded that rhubarb leaveswere the best at taking up the radioisotope and beingimaged. The final art presentation is displayed to thepublic in the entrance atrium of Gloucestershire RoyalHospital (figure 2).
Two talks in this session mentioned the consequencesof unforeseen water in a radiotherapy department. In thefirst Rosemary Belton (Churchill Hospital, Oxford)spoke about the planning and commissioning of the newOxford Cancer and Haematology Centre (figure 3). Aftera lot of planning, it is becoming a reality and Rosemarydescribed the commissioning of four new linacs andother equipment. One unexpected setback was flooding
due to leaking heating pipes. Impressively, despite thissetback and all the extra workload that commissioningentails on top of maintaining the current service, theproject is progressing well.
VARIED RESEARCH INTERESTSIn contrast, the unexpected water in Gloucestershire wasexternal to the department – the severe floodsexperienced in July 2007. Jason Brimelow (CheltenhamGeneral Hospital) spoke about the impact and thechallenges of continuing to treat patients when theCheltenham water supply was cut off and access forpatients and staff was restricted. The contingency planswere severely tested during both the initial flooding andin the weeks that followed.
Other talks throughout the day discussed manydifferent subjects, including a recent visit to the protonfacility in Houston by Tony Bedford (Derriford Hospital,Plymouth), and an insight into the role of an IR(ME)Rinspector by Carol Scott (Cheltenham General Hospital).Three of the speakers discussed different aspects ofpatient doses in diagnostic radiology: CT qualityassurance, Trevelyan Foy (Truro Hospital); estimationand measurement of CBCT (cone beam computedtomograpy) doses, Edward Matthews (Royal UnitedHospital, Bath); and the ICRP 103 report, Pravin Mistri(GHNHST) (figure 4).
In addition to hearing the talks, the SW meeting is agood occasion to catch up with old friends andcolleagues from neighbouring hospitals as well asmeeting new faces.
During the breaks there was a welcome opportunityto talk to the companies who kindly sponsored themeeting and to find out about their latest products anddevelopments. �
SPONSORSThe meeting was sponsored by Bentham Ltd, Clifden HealthcareLtd, Imaging Systems Ltd, Oncura Ltd, Oncology Systems Ltd,Qados and Southern Scientific Ltd.
CLINICAL TRIALS IN RADIOTHERAPY:OVERVIEW OF THE RATIONALE
SOCIETY OF CHEMICAL INDUSTRY, LONDON 13th May 2008
CATHARINE CLARK Royal Marsden Foundation NHS Trust, Sutton, Surrey
THE CLINICAL TRIALS IN Radiotherapy meeting washeld at The Society of Chemical Industry in the heart ofBelgravia, aiming to provide an overview of therationale behind radiotherapy clinical trials and theirQA entry requirements. Physicists, radiographers,clinicians and trials management staff attended.
Neil Richmond (James Cook University Hospital,Middlesbrough) opened the day by welcomingeveryone and explaining that the day would includespeakers from trials, quality assurance (QA) groups andindividual radiotherapy departments.
TRIALS IN EARLY BREAST CANCER John Yarnold (Royal Marsden Hospital, Sutton) opened
the one-day meeting by giving an overview of the resultsfrom the very successful START (STAndardisation ofbreast RadioTherapy) breast trial. In total STARTrecruited 4,451 patients and both parts of the trial aresuggesting that fewer larger fractions give better normaltissue sparing whilst maintaining the same localrecurrence rates as the control arm. He then went on toexplain how the IMPORT (Intensity Modulated andPartial Organ RadioTherapy) LOW and IMPORT HIGHtrials have been designed to question whether IMRT(intensity modulated radiation therapy) can be used tomodulate fraction size and thus gain normal tissuetolerance by reducing the dose to the tissue surroundingthe tumour.
�
�

SCOPE | MEETING REPORTS
36 | SEPTEMBER 08 | SCOPE
FIGURE 1.The QA processesfor radiotherapytrials.
�
FIGURE 2.Different levelsof QA forradiotherapytrials.
�

MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 37
EFFECTS OF RADIOTHERAPY ON NORMALTISSUES IN EARLY BREAST CANCERThis talk was followed by Penny Hopwood (ChristieHospital, Manchester) who explained some of thequality of life endpoints in START and pointed out thatthe shorter treatment times suggested should alsoimprove resource allocation.
WHY PARTICIPATE IN CLINICAL TRIALS? A PHYSICIST’S PERPECTIVEKaren Venables (Mount Vernon Hospital, Northwood)was up next and spoke on behalf of the RadiotherapyTrials QA team (RTTQA) at Mount Vernon to describethe philosophy behind quality assurance programmes intrials. She explained that the RTTQA team iscoordinating and streamlining the QA process (as can beseen in figure 1) between the different trials to try toreduce the QA burden on individual centres. One aspectof this is the baseline questionnaire which is filled inonce by each department and the information is sharedbetween all the trials. It only needs updating every 2years or after a major upgrade has taken place. She alsoexplained that each trial is assessed at the time ofprotocol writing to ascertain the appropriate QA level(see chart in figure 2). Finally Karen gave the pros andcons of joining a trial to implement a new technique (seethe slide used in figure 3) and concluded that theadvantages of the external audit and supportoutweighed the extra work required to undertake theQA exercises.
RADIOTHERAPY CLINICAL TRIALS –RESOURCE IMPLICATIONSGill Lawrence (Newcastle General Hospital) then spokeabout what it is like to be in a department which iscurrently contributing to eight radiotherapy trials. Sheshowed some tables of how much time each trial hadtaken to set up and support. It was interesting to see thelarge discrepancy in staff time and input across thedifferent trials.
AN IMRT CREDENTIALING PROGRAMME FOR CLINICAL TRIALS IN THE UKJust before lunch there were presentations from two ofthe posters which were on display in the exhibition.Catharine Clark (Royal Marsden Hospital, Sutton)spoke about the IMRT credentialing programme whichis being run by the RTTQA team(http://rttrialsqa.org.uk). The aim of the programme isto provide any centre which joins an IMRT trial with afull audit on all aspects of the IMRT process for theirfirst trial. The programme includes outlining andplanning exercises, TPS (Treatment Planning System)verification and field and point dose measurements, aswell as an assessment of the processes in the patientpathway. For subsequent IMRT trials the QA can then besubstantially reduced with streamlining of the QAbetween the different IMRT trials. Laura Ciurlionis(Mount Vernon Hospital, Northwood) then describedthe design and implementation of IMPORT LOW in thesecond of the presentations from the posters.
FIGURE 3.Are trials thedriving force forchange?
�
�
�

SCOPE | MEETING REPORTS
38 | SEPTEMBER 08 | SCOPE
�
EVOLVING QUALITY ASSURANCEPROGRAMMES IN CLINICAL TRIALSAfter lunch Annette Haworth (Peter MacallumHospital, Melbourne, Australia) gave an overview ofradiotherapy trials down under. They are also startingup several IMRT trials and are developing their ownIMRT credentialing system. She proposed that the UKand Australia QA groups join forces to develop theirrespective programmes such that the two countriescould have a reciprocal agreement for the QA requiredby centres joining each other’s trials.
TRIBULATIONS OF A TRIAL PHYSICISTThe day concluded with Stuart McNee (Beatson CancerCentre, Glasgow) describing his experiences inundertaking the role of QA physicist for the SOCCAR(Sequential Or Concurrent Chemotherapy AndRadiotherapy in non-small cell lung cancer) trial, whichinvolved standard 3D conformal therapy, although itwas a trial to determine the best chemotherapy practice.
He joined the trial once it was already established andfound that acting as a trial physicist was a rewardingrole, especially as it gives an insight into the wholeradiotherapy process. He stated that he would like to seemore physicists being involved at the early stages of trialproposal and organisation.
There is currently some conflict between, on the onehand, the need for high standards of compliance and QAand, on the other hand, the costs of time and effortrequired by organisers and participating centres.Approaches to trial recruitment and QA need to bedeveloped in order that clinical trials can be runsuccessfully in the UK. This is certainly food for thoughtgiven the government requirements we are facing forincreased trial recruitment in each centre.
Overall this was an excellent meeting with points ofview from both the trials teams and radiotherapycentres. It was a great opportunity to get an overview ofwhich trials are currently recruiting and to hear some ofthe impressive results from previous trials. �
VOICE OF YOUNG SCIENCE: STANDING UP FOR SCIENCE MEDIA WORKSHOP
INSTITUTE OF BIOLOGY, LONDON 6th June 2008
CONSTANTINOS ZERVIDES University College London
THE WORKSHOP, ORGANISED by Sense AboutScience (a registered charity that works with scientistspromoting good science and evidence for the public),was focused on helping individuals identify the issuesof representing science in the media. Furthermore, itprovided guidelines for helping early career scientistsin getting involved in public debates about science andparticularly when those debates are on controversialissues.
The workshop was divided into three distinctsessions. Session one, Science and the Media, involved adiscussion on the changing image and role of scienceand scientists in the public domain. It was led by threescientists, Prof R Lovell-Badge (MRC National Institutefor Medical Research), Dr S. Keevil (King’s CollegeLondon) and Prof A.C.Ghani (Imperial College)- whoall had in the past dealt with the media. Of particularinterest to medical physicists and engineers was the talkgiven by Dr S. Keevil, who became involved in the MRIcommunity’s campaign about the impact of thePhysical Agents (EMF) Directive on MRI. He explainedhow he approached and used the influence of the mediato accomplish his goals regarding this campaign.Moreover all of the panel members discussed theirsuccesses and the difficulties experienced whenspeaking to the media and concluded that given thechance, talking about science is worthwhile andscientists should get involved.
The second session, What journalists are lookingfor?, introduced a panel of journalists, Mr. Mike Swain(The Mirror), Mr Tom Feilden (Science & EnvironmentCorrespondent BBC Radio) and Lewis Smith (TheTimes). The explained how the media works and how
they approach stories, trying to balance news andentertainment with reporting science. They defendedtheir profession by trying to respond to accusations thatthey misrepresent the facts and they polarize debates.All three indicated that the media do not intentionallymake mistakes and use scare tactics to sell more sincethis will dampen their reputation and people will not bewilling to work with them in the future. They finallyconcluded that when speaking to the media it is best tospeak with a science reporter and try to establish agood working relationship with him/her based ontrust.
The third and final session, Standing up for science –the nuts and bolts, had a more informal attitude.Representatives from Sense About Science, Voice ofYoung Science and the Science Media Center, took it inturns to inform the participants on what is available forearly career researchers and how they can encouragegood science and evidence in the public domain. Theyoffered practical advice in getting your opinions heardin debates regarding science and how to respond to badscience when you see it. They concluded by giving tipson how to respond to journalists if you are contacted bythem and also how to handle a face to face interview,experience.
All in all it was a very lively and informative dayand after speaking to the majority of the participants, itwas well received. The next workshop will be held inEdinburgh on Friday 21st November 2008. �
FOR MORE INFORMATIONFor more information regarding the organizers, the workshop andhow you can help protect science or get involved visit:www.senseaboutscience.org/VoYS.
MEETING REPORTS | SCOPE
SCOPE | SEPTEMBER 08 | 39
FIGURE 1.The first sessionpanel.
�
FIGURE 2.The workshopparticipants.
�

SCOPE | PRESIDENT’S LETTER
04 | SEPTEMBER 08 | SCOPE
s we get older, mostof us accumulatewisdom and loseflexibility.Organisations canhowever be different.
The NHS, that great health systemsurvivor, is now 60 years old. Can itsexperiences teach us anything aboutthe future of healthcare in Britainand internationally?
FOUNDATION OF THE NHSThe roots of the NHS go back manyyears before its foundation but apivotal moment was the publicationof the Beveridge Report in 1942. Thisreport recommended creating a freenational health service whileobserving that the state of medicalprovision in Britain ‘fell seriouslyshort’ compared with other countriesof the world. Even with this analysis,it faced strong opposition fromgovernment and from professionalswith vested interests. However, just 6years later, opposition was overcomeand the NHS came into being, togreat popular acclaim. Why wasthis?
Crucially, the Beveridge Reportprovided a vision. Its proposals for aunited health and social care systemhit the popular mood. It became thebest-selling UK government reportever (635,000 copies) and was widelydiscussed. It offered a positive aimfor the war against Britain’s enemies.Over 90 per cent of the populationwere in favour of implementing thereport, and it could not be ignored.After heated debate and prolongednegotiations through the war andafterwards, the NHS became a realityin July 1948.
The unifying and caring vision setout in the Beveridge Report alsomotivated the 53 founding membersof the Hospital PhysicistsAssociation. ‘Hospital physics’ haddeveloped steadily, following theappointment of academic physicistSydney Russ to the first hospital postat the Middlesex Hospital in 1913.Twenty-five physicists came togetherin 1943 at the first meeting called byRuss, to build the science andsubsequently its professionalpractice, including growingengineering and technology. Theinfluence of these pioneers still
Aresonates through IPEM. My firsthead of department was a foundermember of the HPA, as concerned touse engineering and physics in thepursuit of patient care as he was toencourage academic endeavour andinvolvement with industry.
WHAT IS THE FUTURE?Looking back over the last 65 years,it is hard to appreciate the battlesneeded to make Beveridge’s vision areality. What has provedextraordinary is the lasting natureand influence of that vision. In 1942Britain was fighting a war it mightnot win, hospitals were strugglingdue to lack of funds, and access tohealthcare for the poor depended oncharity. Fast forward to today andwe face similar problems, exceptthat in the developed world patchyaccess to healthcare has replaced noaccess at all. The achievements oftechnologists, engineers andscientists in healthcare have beenphenomenal, and yet when lookedat on a global scale there is far moreyet to be done.
Looking to the future, medicineseems to be losing its way. Ten yearsago, Professor Roy Porter wrote thatmedical consumerism – the fantasy
Keith IsonPresident
OUR MODERN HEALTHCARE SYSTEM
It faced strongopposition fromgovernment and fromprofessionals withvested interests
that everyone and everything can becured – was leading to inflated andunfulfillable expectations. Medicineneeds to define its limits, he said,even as it extends its capabilites. Heasked the question: what is the priceof extending life if it leads todegrading neglect, as resources growoverstretched?
DECIDING ON PRIORITIESSo in an interconnected world facingcommon problems, what visionmight we develop in IPEM to servethe NHS and other healthcaresystems over the next 65 years? Asinternational trends start to bringtogether leading academicinstitutions and health serviceproviders, remember that theBeveridge Report was about bothhealth and social care. The twocannot be separated in modernsocieties, where difficult decisionsneed to be made on priorities andallocations. In a resource-limitedfuture, the NHS is seeking to changeemphasis from sickness to healthwhile improving delivery to all. Willits original twin values of unity andcaring be sustained? And are thesethe ones on which IPEM shouldbuild its future?
”“
Access to healthcareshould be available to all

COMMENT | SCOPE
SCOPE | SEPTEMBER 08 | 05
MARC E MIQUEL EDITOR-IN-CHIEF
Scope is the quarterlymagazine of the Institute ofPhysics and Engineering inMedicineIPEM Fairmount House, 230 Tadcaster Road, York YO24 1EST 01904 610821F 01904 612279E [email protected] www.ipem.ac.uk
EDITOR-IN-CHIEFMarc E. MiquelDepartment of ClinicalPhysics, The Royal LondonHospital, 56–76 AshfieldStreet, London E1 2BLT +44 (0)207 377 7000
extension 2201F +44 (0)207 377 7100E [email protected]
ASSISTANT EDITORGemma WhitelawRadiotherapy Physics, St.Bartholomew’s Hospital, 25 Bartholomew Close,West Smithfield, London EC1A 7BEE [email protected]
MEETING REPORTS EDITORAngela CottonHead of Non-IonisingRadiation Support, MedicalPhysics & Bioengineering,Southampton GeneralHospital, SouthamptonSO16 3DRE angela.cotton@suht.
swest.nhs.uk
NEWS EDITORChristie McCombMRI/SPECT, Institute ofNeurological Science,Southern General Hospital,1345 Govan Road, GlasgowG51 4TFT 0141 201 2120E [email protected]
ENGINEERING EDITORDonna CowanHead of RehabilitationEngineering Service, ChaileyHeritage Clinical Service,Beggars Wood Road, EastSussex BN8 4JNT 01825 724706E donna.cowan@southdowns
.nhs.uk
BOOK REVIEW EDITORSarah Misson-YatesRadiotherapy PhysicsSouthampton OncologyCentre, SouthamptonGeneral, Mailpoint 301SO16 6YD
T 0238 079 8503E [email protected].
nhs.uk
Published on behalf of theInstitute of Physics andEngineering in Medicine byCENTURY ONEPUBLISHING LTD.Arquen House, 4–6 SpicerStreet, St Albans, Herts AL3 4PQT 01727 893 894F 01727 893 895E enquiries@centuryone
publishing.ltd.ukW www.centuryone
publishing.ltd.uk
MANAGING DIRECTORNick SimpsonT 01727 893 894E nick@centuryone
publishing.ltd.uk
ADVERTISING MANAGER Oliver KirkmanT 01727 739 184E ollie@centuryone
publishing.ltd.uk
SUB EDITORKaren MclarenE karen@centuryone
publishing.ltd.uk
DESIGN & PRODUCTIONHeena GudkaE studio@centuryone
publishing.ltd.uk
PRINTED BY Visa Press Ltd.
Scope is published quarterlyby the Institute of Physicsand Engineering in Medicinebut the views expressed arenot necessarily the officialviews of the Institute.Authors instructions andcopyright agreement can befound on the IPEM website.Articles should be sent to theappropriate member of theeditorial team. By submittingto Scope, you agree totransfer copyright to IPEM.We reserve the right to edityour article. Proofs are notsent to contributors. Theintegrity of advertisingmaterial cannot beguaranteed.
CopyrightReproduction in whole orpart by any means withoutwritten permission of thepublisher is strictly forbidden.
© IPEM 2008ISSN 0964-9565
hile shadowing Mark McJury, I enquiredabout comments and feedback. It did nottake me long to realise they wereinfrequent. It also seems that onlydispleased readers found the time towrite. I was therefore happy when finallysome positive and some constructive
messages landed in my inbox. The first email praised thephotographs in Iain Chambers’ report (March); nothing to dowith my work but still pleasing. The second message was aconstructive comment on Mark McJury’s recent PublishingProfessional Writing tutorial (June). The letter by ProfessorSalmons is re-printed in this issue with the answer from one ofthe tutorial co-authors, Professor Hogg.
One thing that has puzzled me since taking over is that thebulk of the questions and comments I have faced are neitherpositive nor negative (although some were cheeky) but have todo with the disappearance of the editor’s photograph. In animage-obsessed society, I was naively expecting scientists to beimmune and have an interest in images limited to acquisitionand quality assurance! Well, if you are that interested (andfrankly I cannot understand why), rest assured that thephotograph will come back; but only with the next editor. Forthis one, I hardly see the point as only the fastest CPU andlargest memory would allow you to morph me into GeorgeClooney. To achieve this small miracle you will also need to bean expert in image processing and to help you along the way Iam kindly providing you with an excellent tutorial on imageregistration. This field is nowadays not limited to research buttakes an increasingly important place in our professional lifefrom new imaging modalities like PET/CT to MRI/CT fusion inradiotherapy planning. This is a vast and often complex subjectand this substantial tutorial covers both the basics and advancedexamples. The article was written by Dr William Crum of theInstitute of Psychiatry (KC L). Bill not only is an expert in thefield, he has the ability to make it accessible to most as I am sureyou will agree when reading his article.
In the remainder of the issue you will find your usual itemsincluding meeting reports, book reviews and news. The news isnow edited by Christie McComb (Glasgow); I would like to takethis opportunity to welcome her and thank her predecessor, JohnMcLean, for his sterling job. Christie is an MRI physicist and shedid not hesitate to go in the scanner to illustrate one of her items.
In the features, you will discover why it has been an excitingtime for a lot of imaging physicists in Scotland with the creationof SINAPSE, a consortium of six universities with an interest inneuro-imaging. This year marks the 65th anniversary of the HPAcreation and the York office managed to unearth the originalmeeting notes.
To finish in style, we travel further back in time with FrancisDuck's riveting article on the early days of ultrasonic detection.
Hope you’ll enjoy this issue.
WAN IMAGE ISSUE

SCOPE | NEWS BY CHRISTIE MCCOMB
06 | SEPTEMBER 08 | SCOPE
However we need to bear in mindthat the magnetic fields producedby the machines are quitesubstantial and that these fieldsare increasing in order to achieveimproved clarity of image. Theexposures to patients and medical
staff from the magnetic fields canbe high and there is a shortage ofinformation on possible adverselong term health effects. TheAgency’s Board thereforeconsiders more research isneeded in this area.’
The view that there is a need formore epidemiological research onpeople exposed to MRI is shared bythe World Health Organization,which has suggested that aninternational collaborative studymay be the most effective way toproceed, as it would ensure thereare sufficient numbers of exposedcases in the study to drawaccurate conclusions. The Agencywill now examine the feasibility ofsuch a study with specialists hereand abroad, with the aim oflaunching such a study as soon aspossible.
More information can be foundusing the following link:http://www.hpa.org.uk/webw/HPAweb&HPAwebStandard/HPAweb_C/1211354081861?p=1204186170287
effects from high static fieldMagnetic Resonance Imaging(MRI) scanners.
Sir William said: ‘MRI scanninghas some undoubted benefits inmedicine, especially as an aid toaccurate clinical diagnosis.
The news editor goes for a scan at the Institute of Neurological Sciences, Glasgow.
PET probe image in a mouse.Image courtesy of Professor Caius Radu,University of California, Los Angeles, at theInstitute of Neurological Sciences, Glasgow.
Study into adverse health effects ofMagnetic Resonance Imaging (MRI)
PET probe images of immune system activationThe ability to monitor immunesystem function could have aconsiderable impact on thediagnosis and treatment ofimmunological disorders andtherapeutic immune response. Atechnical report published onlineon 8th June in Nature Medicine(doi:10.1038/nm1724) describes anew PET probe which has beendeveloped to achieve this purpose.
The concept behind the probeinvolves a fundamental processcalled the DNA salvage pathway.This is essentially a recyclingpathway that immune cells use toquickly and efficiently producenew cells in the event of infection.The probe consists of a moleculecalled FAC (fluoroarabinofurano-syl cytosine), which is effective atentering immune cells. In the
presence of a particular enzymeinvolved in the first step of DNArecycling, FAC is phosphorylatedand retained within the cell. It islabelled with 18F, a commonly usedPET radionuclide, which allows itsdistribution to be imaged.
Experiments were conductedin mice to determine theeffectiveness of 18F-FAC imaging inimmune activation and systemicautoimmunity. In one suchexperiment, the mice wereinjected with an oncogenic virus,causing a tumour to develop, of atype which is quickly recognisedand attacked by the immunesystem. An injection of the probewas administered, followed byrepeated PET scans.
PET scans obtained 15 dayspost-injection, which corresponds
to the peak anti-tumour immuneresponse, showed an increasedaccumulation of 18F-FAC in thespleen and tumour draining lymphnodes with reduced retention inthe tumour site, which suggeststhat 18F-FAC has good specificityfor imaging immune rejection ofvirally-induced tumours.
Studies are currently underwayto translate the use of the newprobe into human subjects, and toevaluate its potential formonitoring autoimmunity,inflammation and cancer.
This story was reported onTechnology Review on 9th June,and more can be found at:http://www.technologyreview.com/Biotech/20876/page1/http://www.nature.com/nm/index.html
On 21st May, the Chairman of theHealth Protection Agency, SirWilliam Stewart, issued a pressrelease stating that the Agency’sboard had approved in principlethe need for an epidemiologicalstudy of possible adverse health

Benefits of dose modulation inneuroradiology CT confirmed
NEWS BY CHRISTIE MCCOMB | SCOPE
SCOPE | SEPTEMBER 08 | 07
IN BRIEF
MOBILE IMAGINGA simple data acquisitiondevice can communicatewith a central imageprocessing centre viamobile phone, allowingaccess to medical imagingtechnology forpopulations who do nothave the expertise orfinancial ability tomaintain conventionalimaging systems. The rawdata from a scan can besent from the phone to beprocessed, and theresulting image sent backfor local analysis.
CT DOSEMODULATIONA study has confirmedsignificant reductions indose when applying dosemodulation techniques tocommonly-usedneuroradiology CTprotocols. The use of dosemodulation has no effecton image quality.
HEALTHEFFECTS OF MRIThe HPA has approved inprinciple the need for anepidemiological study ofpossible adverse healtheffects from high staticfield Magnetic ResonanceImaging (MRI) scanners.Fields used are becomingstronger and their longterm effects on patientsand staff need to beunderstood.
PET PROBE FORIMMUNE SYSTEMA new PET probe hasbeen developed whichallows imaging ofimmune system responsein mice, and has thepotential to monitorautoimmunity,inflammation and cancerin human subjects. Theprobe enters and isretained in immune cellsso can be labelled and itsdistribution imaged.
Mobile imaging gets a new meaningAccording to World HealthOrganization reports, aroundthree-quarters of the world’spopulation currently has no accessto medical imaging technologies,often because the systems are toocostly to maintain or there is a lackof staff with the expertise tooperate them. In a paper publishedon the PLoS ONE website in April2008, researchers describe amethod to overcome this byexploiting the prevalence of mobilephone networks, which are oftenavailable even in remote locations.
Conventional medical imagingsystems usually consist of threecomponents – the data acquisitionhardware, the image processingsystem and an image display unit.In the new system, the componentsare physically separated, with themost complicated component – theimage processing system – at acentral location that could serveseveral remote sites. Only theacquisition device used to collectthe raw data needs to be at thepatient site, which reduces the costand allows it to be operated by staffwith basic technical training. Theunprocessed raw data are
transmitted via mobile phone to thecentral server, which processes thedata and sends the resulting imageback to the patient location. Theimage can then be viewed on themobile phone screen and analysedby local physicians.
Its feasibility was tested usingElectrical Impedance Tomography(EIT) to image a simulated tumour.A simple acquisition device wasconstructed using 32 stainlesssteel electrodes, 15 of whichserved as current sources and oneas a current sink, with theremaining 16 electrodes used forvoltage measurements. The devicewas connected to a gel-filledcontainer that simulated breasttissue with a tumour and used torecord 225 voltage measurements.The measurements were uploadedto a mobile phone, which sent theraw data to the central facility forprocessing. The resulting imagewas viewed on the mobile phonescreen, and clearly showed thesimulated tumour. According to theresearchers, the system shouldwork for any mobile phone that iscapable of sending and receivingmultimedia images.
This story was reported onMedical Physics Web on 2nd May,and more can be found at:http://medicalphysicsweb.org/cws/article/research/34046http://www.plosone.org/article/fetchArticle.action?articleURI=info:doi/10.1371/journal.pone.0002075
Studies in the United States andEurope have revealed thatcomputed tomography (CT)examinations account for up to 15per cent of all imagingexaminations, but contribute up to75 per cent of the total dose to thepopulation. One possible methodof dose reduction available onmost modern CT scanners is dosemodulation, in which tube currentis adjusted separately for each CTsection according to patientattenuation. However, there islittle documented evidence on theoverall effect of using dosemodulation.
A study published in Radiology(2008; 247(2): 499) investigated theeffect of dose modulation on fourcommonly-used CT protocols –
unenhanced brain CT in adults,unenhanced brain CT inpaediatrics, adult cervical spine CTand adult cervical and intracranialCT angiography. For each protocol,scans which had been performedwith and without dose modulationwere reviewed, and the weightedvolume CT dose index (CTDI) anddose length product (DLP) whichhad been recorded by the scannerwere compared. The image qualitywas also rated subjectively by aneuroradiologist who was blindedto the use of dose modulation.
The results showed a significantdecrease in dose when dosemodulation was used, with areduction in CTDI and DLP duringunenhanced brain CT in adults of57.9 per cent and 55.4 per cent
respectively with z-axis dosemodulation, and 52.6 per cent and25.8 per cent with x-y-z-axis dosemodulation. The use of dosemodulation had no effect on imagequality.
The researchers recommendthe use of dose modulation inneuroradiology CT procedures, andwill be expanding their study toinvestigate the effect of dosemodulation on CT protocols forother parts of the body.
This story was reported onMedical Physics Web on 29th April,and more information can be foundusing the following links:http://medicalphysicsweb.org/cws/article/research/33987http://radiology.rsnajnls.org/cgi/reprint/247/2/499
Image courtesy of Professor Boris Rubinsky,University of California, Berkeley.
Congratulations to the following members who were recently elected to Fellowship of IPEM.Dr Panayiotis Kyriacou, London (elected March 2008); Dr David Brettle, Leeds (elected May 2008); Mrs Anne Walker, Manchester (elected May 2008)
Congratulations to the following who have recently been successful in the IPEM Viva Voce examinations for the Clinical Science Diploma of IPEM[DipIPEM(S)].
IPEM EXAM RESULTS
NEW FIPEMS
IPEM EXAM RESULTS CLINICAL SCIENTISTS
Name Training Centre Result
Jennifer DobsonAlison HandDebbie HolmesElaine KennedyClara Marquez-MorenoSarah NaylorBarry O’ConnellGregory Stevens
Julian AllanPeter AustinPaul CallaghanGordon MitchellPaul MusgraveDerek PonsonbyJames ScobieLeah Speirs
MerseysideSheffieldOxfordNorthernLondon NorthEast MidlandsWalesSurrey and South West
GlasgowEssexGlasgowEdinburghCumbriaGlasgowGlasgowGlasgow
PassPassPassPassPassPass with MeritPassPass
PassPassPassPassPass with MeritPass with MeritPassPass with Merit
Congratulations also go to the following students who have successfully completed the Clinical Technology Diploma of IPEM [DipIPEM(T)].
SCOPE | MEMBER’S NEWS
40 | SEPTEMBER 08 | SCOPE
Touch Bionics of Livingston hasbeen awarded the 2008 RoyalAcademy of EngineeringMacRobert Award for the world'sfirst commercially available hand.Stuart Mead (chief executive),David Gow (director of research,founder and MIPEM), Stewart Hill(project manager), Hugh Gill(director of technology andoperations), Phil Newman(director of marketing) and NickyHolt (project coordinator) werepresented the £50,000 prize andthe solid gold MacRobert Awardmedal by HRH the Duke ofEdinburgh.
The Touch Bionics i-LIMB Handis a prosthetic device that looksand acts like a real human handwith five individually poweredfingers. The project started in 1963
as part of a research programmeat Edinburgh's Princess MargaretRose Hospital to help childrenaffected by Thalidomide. The handcontrol system uses the electricalsignal generated by the musclesin the remaining portion of thepatient’s limb. The myoelectricsignal is picked up by electrodeson the surface of the skin. Thesystem is very intuitive andpatients master the functionalityof the device within minutes. Theprosthetic device is manufacturedusing high-strength plasticmaking it lightweight, robust andhighly realistic.
Since its launch in 2007 over200 patients have benefited fromthis revolutionary device. Onesuch patient is Ray Edwards(photographed). For Ray the new
prosthetic is more than addedfunctionality: ‘i-LIMB has helpedme more psychologically thanphysically. That was the first timein 21 years that I had seen a handopening there – it made me feel Iwas just Ray again. You can do somuch with technology but it's gotto make the user happy – and i-LIMB does!’ Ray also noticedimprovement within 4 weeks ofhaving the prosthetic and nowfeels it is part of him.
You can watch Ray's interviewand David explaining how the handworks on the BBC website(http://news.bbc.co.uk/1/hi/sci/tech/7443866.stm). When you readthis you will still be able to see itfor a few more days in the LondonScience Museum .M.E.M.
Member wins big engineering prize
Ray Edwards demonstrating useof the i-LIMB prosthetic hand

MEMBER’S NEWS | SCOPE
SCOPE | SEPTEMBER 08 | 41
PLANNED MEETINGS
DIARY OF MEETINGS 2008
Meeting Dates Venue
Beyond Improvement:Can EnablingTechnology MaximisePerformance
Practical DICOM:Radiology,Radiotherapy andBeyond!
Working LikeClockwork – theEquipmentManagement Database
Radiation Protection inNuclear Medicine
NeurophysiologicalIntra OperativeMonitoring
Challenges in MedicalEquipment Design andDevelopment
UKRO 2009
30th September
7th October
21st October
4th November
6th November
2nd December
6th–8th April2009
York
Assistive technology has made it possible to augment individuals beyond improvement tosuper performance. This meeting will provide an inspirational insight into the use of enablingtechnology to surpass boundaries in sport, rehabilitation and life achievement. Jointpresentations with user experiences, technical explanation and research and development willbe given.
Birmingham
This meeting is aimed at people who need to understand the technical issues behind thecommunication of electronic data around a department using DICOM.
Birmingham
The equipment management database is one of the most important tools in any EBMEdepartment. The aim of this conference is to stimulate greater utilisation of this valuableresource.
London
This meeting will bring together nuclear medicine and radiation protection professionals toshare experiences in managing new radiation protection concerns and challenges.
York
This one-day meeting aims to focus on new developments within the speciality along withreviewing the standard practices.
Coventry
Framework topics addressed by the meeting will include how innovation is handled within theNHS, the importance of industrial design and also how to climb the ethical mountain.
Cardiff
A multidisciplinary conference for clinical oncologists, therapy radiograhers, radiotherapyphysicists, clinical radiobiologists and oncology nurses.For further details visit www.ukro.org.uk
DIARY OF MEETINGS 2009
Clinical Science in Physiological Measurement, Managing Motion in Radiotherapy, Mammography Physics Training meeting, Radiographer QAtraining day, Risk and Maintenance, A code of practice study day
OTHER MEETINGS COMING SOON IN 2008/2009...
The meetings department of IPEM is delighted to announce its upcoming programme of meetings. Our programme is regularly updated so please visit ourwebsite at www.ipem.ac.uk for the latest details. Abstract submission instructions, programmes and registration forms can be downloaded for each meeting.

SCOPE | BOOK REVIEWS
42 | SEPTEMBER 08 | SCOPE
n this packed issue we have bookreviews of Digital Radiography andPACS and The Physics ofRadiotherapy X-Rays andElectrons.
Following the successful launchof our ‘Popular Science’ section in
the last issue, this time we have a reviewof The Oxford Book Of Modern ScienceWriting.
Our regular ‘Just published!’ sectiontakes a look at the books that are due forpublication over the next few months.
If you are interesting in reviewing anyof these, please contact the book revieweditors.
Gemma Whitelaw and Sarah Misson-Yates
Towards SaferRadiotherapyTowards Safer Radiotherapy has recentlybeen published as a joint venture betweenIPEM, the British Institute of Radiology,the NHS Patient Safety Agency, theSociety and College of Radiographers andthe Royal College of Radiologists.
The document recognises thatradiotherapy incidents in the UK are fewbut cites their impact as devastating to thepatient, the staff and the integrity of theprofession. It therefore addresses andoutlines ways in which to minimise errorsin radiotherapy. This is achieved in anumber of ways; the main text exploresthe type of errors, the frequency of them,ways in which to detect them and thingsthat can be learned from past incidents. Italso looks at ways in which to deal withconsequences of errors. The report alsoprovides the reader with a list ofrecommendations in order to improvetheir own practice.
The report is aimed at radiotherapyprofessionals, patients and otherinterested individuals; for this reason it iswritten in a readable style that isapproachable for those who are not from a
radiotherapy background. This is essential reading for those in a
radiotherapy setting and is available as aPDF through a link on the IPEM websiteand from www.rcr.ac.uk.
Digital Radiographyand PACSThis 240-page book is intended forradiography students. However, traineephysicists, technologists and anyone whois unfamiliar with digital radiography andPACS may find this book a useful primer.The book was written by Americanauthors. A mixture of metric and non-metric units is used.
The book is organised into five parts,with a useful glossary and abbreviationtable at the end. Each part contains one ormore chapters. The chapters are structured,with the topics that will be discussed, theobjectives and key terms listed up front.At the end of each chapter, there is asummary in bullet point form, followed bychapter review questions. There is anabundance of pictures, diagrams andtabulated summaries throughout. It is avery ‘visual’ book which is helpful inmany instances, but the brief treatment ofsome topics may leave the reader feelingrather lacking in depth or intellectualsatisfaction.
Part I is the Introduction, whichcontains a tabulated comparison ofconventional, computed and digitalradiography. Part II is Basic Principles,which contains basic computer principleswhich some readers may find elementary.It should be considered up-to-date,although in the section on operatingsystems only Windows 95, 98, 2000, ME,XP and NT are mentioned, not WindowsVista.
The chapter on networking andcommunication basics contains a brief butuseful description of network classes,DICOM and HL-7. The major sections ofthe book are in Part III and Part IV. Part IIIis Digital Radiographic Image Acquisition
and Processing. It goes through theprinciples and mechanics of computedradiography (CR) and direct digitalradiography in a descriptive way.
There are brief explanations of topicssuch as exposure indicator, imagesampling, processing and manipulation.Topics such as modulation transferfunction, detective quantum efficiency andaliasing are given a brief descriptiveexplanation, rather than mathematicaldefinitions or scientific explanation. Thereis a conspicuous absence of equations.More emphasis is put on the practical side,such as collimation, technical factor andequipment selection and artefacts.
The section on artefacts encountered incomputed radiography is well worthreading. It contains many high qualityimages of different types of artefacts, withclear explanation of the problems in theattending captions.
Part IV is PACS Fundamentals. PACSdesign, workflow, system architecture andtypes of display workstations aredescribed and illustrated. There are one ormore photographs or diagrams on mostpages to show the reader what things looklike.
There is a chapter on PACS archivingand a chapter on digitisers, imagers(printers) and CD/DVD burners. Thesechapters serve to give useful backgroundinformation to the reader. Part V is QualityControl (QC) and Quality Management.There is a good section on radiographer’sQC of workstation monitors, rejectanalysis and other duties, but very little onQC of CR readers.
In summary, anyone who wants aneasy-to-read and well-illustrated primeron digital radiography and PACS may findthis book helpful.
Ruby FongBarts and The London NHS Trust
I
DIGITAL RADIOGRAPHY AND PACSCHRISTI E. CARTER AND BETH L. VEALEPublished by Mosby Elsevier US (2008)Language: EnglishISBN: 978-0-323-04444-8Paperback, 240 pages
The chapters arestructured, with the topicsthat will be discussed, theobjectives and key termslisted up front. At the end ofeach chapter is a summaryin bullet point form
”“

BOOK REVIEWS | SCOPE
SCOPE | SEPTEMBER 08 | 43
The Physics ofRadiotherapy X-Raysand ElectronsThis is without doubt an all-in-one book ofradiotherapy physics, and even more. Thetitle, which refers to the physics of X-raysand electrons, does not describe the wholecontent of the book, as the authors felt theneed to top-up with extra subjects, likeproton physics and radiobiology. Thelatter is added in the last chapter (14)probably for a supposed completeness, butit could have been very well omitted basedon the book’s subject.
The book is well presented; the layoutis clear and follows logically through thesubject. The text practically covers allimportant aspects in connection withradiotherapy. It starts with medical linacsand, although not complex, theinformation in this chapter is enough tounderstand the science behind them, theirconstruction and functional parts. It isfollowed by a chapter regarding theinteraction of radiation with matter, wherephysics is properly explained using asuitable proportion of mathematics andconcepts. The authors provide acomprehensive description of all thedosimetric techniques of interest in thethird chapter, while the calibration ofbeams, including several codes of practice,is placed in Chapter 8. The codes ofpractice mainly discussed are IAEA TRS398 and AAPM TG 51, but others, like TG21 NACP or early HPA protocols, are alsopart of the subject. I must say I find usefulthe comparison between some of theprotocols, which is provided in a sub-chapter.
The beam properties of X-rays andelectrons and their related fundamentalquantities are also suitably presented overtwo chapters, with good illustrations andjust enough equations to keep the subjectsimple but clear. I was pleased to find agood and thorough presentation of beamand brachytherapy models, together with
the concepts, physics and also themathematics behind them, their strengthsand weaknesses. There is quite a detaileddiscussion about the influence ofinhomogeneities on dose distributions,and the characteristics of the variouscorrection methods used. The inclusion ofthe Monte Carlo (MC) codes is a positiveinitiative, as this method becomes morepopular in commercial software. It isdisappointing though that the Macro MCis limited to one page, whilst this is animportant and modern implementation ofMC in terms of computational efficiency.
This edition is updated with moderntechniques, including robotic radiosurgeryand tomotherapy. A whole chapter isdedicated to these advanced procedures,where one can find a brief but plaindescription of their principles, technologyand applications.
Another two chapters cover qualityassurance and radiation protection of thetreatment machines and bunkers, topicsthat could not be missed from thecomplete structure of the book.
Patient immobilisation, setupverification and treatment delivery are notforgotten, as they are fundamentallyimportant for the accuracy aimed byradiation physicists.
Overall, the graphs, tables and picturesare well balanced. It is worth a mentionhere that the authors illustrated most oftheir discussion about radiation transportand interaction concepts using graphicalMonte Carlo tracks, which I consider agreat idea. Unfortunately, there are a fewmistakes in the text, formulas andillustrations. One that I found quiteamusing is where the abbreviation ESQ,which should mean equivalent square, isaffirmed to be electrostatic quadrupoles!
To sum up, the book is a usefulreference for the radiotherapy physicist –both junior and experienced. It iscomplete, up-to-date, and there is anadequate balance of graphics,mathematics, concepts and descriptivetext.
Apart from to radiotherapy physicists, Iwould recommend it, even if not as awhole, to other radiotherapy professionalslike radiographers or technologists.
Dr Virgiliu CraciunSouthampton Oncology Centre
The Oxford Book ofModern ScienceWritingFor his latest book, and the last as CharlesSimonyi Professor of the PublicUnderstanding of Science, Richard Dawkinsputs on his editor’s hat and tackles thedifficult exercise of the popular sciencewriting anthology. Unlike John Carey’sspectacular Faber Book of Science, this bookonly focuses on writings from the lastcentury (hence ‘Modern Science’). It is alsolimited to pieces written by scientists and,with some rare exceptions (like the greatPrimo Levi), to original English texts.
The book is divided into four sections –‘What scientists study’, ‘What scientiststhink’, ‘Who scientists are’ and ‘Whatscientists delight in’. Those categories arequite fuzzy, and as scientists often delight inwhat they study (and vice versa) and whatthey think is linked or derived from whatthey study, a lot of pieces could easily bemoved around. However, this has the clearadvantage of giving some structure to thebook. All the pieces are short extracts frombooks, articles, magazine columns or talks.Sometimes shorter than a page and hardlyever exceeding eight, the texts are ideal forfragmented reading during your dailycommute or before going to sleep.
Dawkins’ didactic and literary talents arenot only apparent through his choices, veryfew texts are hard to read and even theextract from the notoriously hard A BriefHistory of Time is accessible to all, but also inhis extremely well-written introductions toeach author. In only a few lines, he deliversfirst hand anecdotes or details on theauthor’s life, work and field that instantlygive you a sense of familiarity.
The volume starts with a short piece byJames Jeans which looks towards theimmensity of the Universe and theinsignificance of Earth in space. Like anecho, it finishes with an extract from CarlSagan’s Pale Blue Dot looking down on oursmall and fragile planet from the immensity
THE PHYSICS OF RADIOTHERAPY X-RAYS AND ELECTRONSPETER METCALFE, TOMAS KRON AND PETER HOBANPublished by Medical Physics Publishing US (3rdEdn) (2007)Language: EnglishISBN: 1930524366List price: £60 �

SCOPE | BOOK REVIEWS
44 | SEPTEMBER 08 | SCOPE
of the Universe. In between, you can find afurther 88 texts from 77 other authorscovering most fields of science (excludinghuman sciences that is) from evolution tocosmology, theoretical physics to zoology orchemistry to mathematics. The selection iswell balanced with only a slight (and to beexpected) biology bias. Out of such anabundance of texts, it would be impossiblefor a reader not to find a few to dislike or toadmire. Within the scope of this review, thehardest thing was to limit my examples andI could have picked many others like OliverSacks’ touching Uncle Tungsten or the pieceon flight by John Maynard Smith.
A few did particularly resonate with mypast. Growing up spending days in fieldsand reading J. H. Fabre, I particularlyenjoyed the extract from Curious Naturaliston the solitary wasp Philanthus triangulum.There is something both simple andbeautiful in the experiments, observationsand joys of a young Niko Tinlergen, futureNobel Laureate, spending his days alone insand dunes.
As a teenager Les Fleurs du Mal was oftenon my bedside table. Rectal carcinoma, thesubject of Cancer is a Funny Thing, would nothave looked out-of-place in Baudelaire’smasterpiece between poems on wine anddecaying carcasses. The use of technicalwords, by essence hard and non-poetical,brings an almost Neruda feel to the poem.Unlike most of Baudelaire’s work, whattranspires through this poem is thecontagious optimism of J.B.S. Haldane;cancer is tamed, it becomes poetry, a simplematter of life, not just a sentence to death.This made it my favourite selection; thispoem should be pinned in hospital waitingrooms throughout the country.
By nature, no anthology can ever becomplete, authors will always have to beexcluded, choices can always be altered.Dawkins also decided not to include himselfwhich I think was a wise decision (for thosenot familiar with his work I wouldrecommend that you start with A Devil’sChaplain, a fantastic collection of shortessays). However, this collection is in myopinion as good as any that could beassembled. This book is a startling reminderthat some great scientists, even some Nobellaureates, do also write beautiful prose (andoccasionally poetry). It is one of the bestintroductions to popular science writing anddeserves to become a classic in its own right.
Marc Miquel
THE OXFORD BOOK OF MODERN SCIENCEWRITINGPublished by Oxford University PressLanguage: EnglishISBN-13: 978-0199216802Hardback: 448 pages
Just Published!This quarter we have a range of new booksthat have just been or are about to bepublished.
If you are interested in them or wouldlike to try your hand at reviewing themplease contact the book review editors fordetails.
Diagnostic Imaging for PhysicalTherapists by James Swain, Kenneth W.Bush, and Juliette Brosing (Elsevier).This book is aimed at giving the reader theknowledge to understand the basicprinciples of imaging in practice. There isan accompanying DVD with interactiveactivities to consolidate the readers’understanding of the topic.
Advances in Medical Physics: 2008 byAnthony B. Wolbarst, Kenneth L. Mossmanand Willam R. Hendee (Medical PhysicsPublishing US).This is the second book in the series (thefirst was published in 2006) that intends tokeep practicing medical physicists,technical staff and physicians up to datewith the current advances in the field. Thebook covers all the recent developments inmedical physics including computer-aideddiagnosis (CAD), advances in quantitativeMRT and image guided radiotherapy(IGRT).
Fundamentals of MRI: An InteractiveLearning Approach by Elizabeth Berry andAndrew J. Bulpitt (Taylor and Francis).This is an interactive book withaccompanying CD-ROM on anintroduction to the principles of MRI. Itprovides animations and exercises (withsolutions) to help the reader to develop adeeper understanding of the topic.
Advances in Biomedical Engineering byPascal Verdonck (Elsevier).This book is a review of all the currentresearch advances in the field ofbiomedical engineering from visualisationtechnology through to cardiovascularmedical devices and is aimed at educatingstudents and professionals.
Medical Devices into Healthcare by AlexFaulkner et al. (Palgrave Macmillan).This work explores the world of medicaldevice innovation and regulationincluding five technology case studiesfrom orthopaedic surgery, intensive carenursing, haematology, cancer detectionand regenerative medicine.
Sarah MissonSouthampton General
REVIEWERSWANTED!
Being a Scope book review editor is a funnyold business. One minute you have nobooks on your desk and you’re worryingabout where your next copy is coming from.Next minute there is an avalanche; youreceive a package of books every day andthe tower on your desk becomes higher andhigher.
A way to make the whole process a biteasier is to have a good group of reviewersready and waiting. We have recently been inconsultation with the IPEM special interestgroups, and they are willing to help us createa group of keen reviewers who we may referbooks on to.
We need more than this however and thisis where you come in. If you have seen abook in Just Published! that you might like toreview, please drop us a line and we will tryand get a copy for you, likewise with anyrecent book in print. You may also decidethat you would like to be a reviewer but areunsure what to review. Please contact usand we could match you with a book. Eitherway, as a thank you, you get to keep thebook. We don’t operate short deadlines,therefore allowing you to review at your ownpace.
Popular Science is our newly launchedcolumn, and again we are on the lookout forreviewers. This time we cannot call on theSIGs for help so this is where volunteers likeyou are especially needed. Popular Sciencebooks are generally shorter and easier toread in one go, making them ideal for time-short reviewers, and again you would get tokeep the book.
There are advantages to doing bookreviews for Scope; in addition to increasingyour library, it counts towards valuable CPD,and as a more junior member of IPEM it maybe a good addition to your CV.
So please, we ask you to considerbecoming a Scope book review editor, ittakes little time, there are clear benefits and itwould make our lives easier!
�





























