8/7/2019 0209 Case 1
1/4
C O M F E B R U A R Y C A S E 1 b p a _3 0 1 5 3 1 ..5 3 3
5-YEAR OLD MALE WITH AN INTERHEMISPHERIC FRONTAL
MASSbpa_301 531..534Laura An Bertolino, MD2; Pa Lpore, MD2;
Mnica Carassai, MD2; Roberto Gonzlez, MD3;
Gustavo Sevlever, MD, PhD1; Miguel A. Riudavets, MD1
1 Department of Neuropathology. Institute for Neurological
Research, FLENI. Buenos Aires, Argentina.2 Departments of
Pathology, and 3 Neurosurgery. Hospital Churruca-Visca. Buenos
Aires, Argentina.
CLINICAL HISTORY
A 1-year old male (with no significant past medical history)
pre-
sented to the Department of Plastic Surgery for evaluation
and
eventual resection of a subcutaneous frontal mass. Imaging of
the
head revealed a second intracranial mass and he was referred to
the
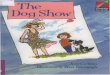
Department of Neurosurgery. Subsequently, Magnetic Resonance
Imaging (MRI) detected two T-1-hyperintense masses. One was
the
extra-cranial frontal mass noted clinically and the other was
an
intra-axial, interhemispheric frontal mass. Additionally,
partial
agenesis of posterior corpus callosum was found. (Figure 1)At
that
time, only the subcutaneous mass was resected and physical
exami-
nation was normal. Four years later a follow-up MRI revealedthat
the intracranial lesion had doubled in size (Figure 2). It was
hyperintense on bothT1 and T2 (Figures 2 and 3). Craniotomy
was
performed and a soft yellow mass was partially resected.
Focal
attachment to the cingulate gyri was appreciated.
GROSS AND MICROSCOPICPATHOLOGY
Macroscopically, surgical fragments from both specimens were
yellow, lobulated and soft. Permanent sections from the
extracra-
nial frontal mass are shown in Figure 4. Sections from the
intracra-
nial lesion are shown in Figures 5, 6, 7 & 8. No normal
cortex was
appreciated. Some areas were positive for GFAP (glial
fibrillaryacidic protein). (Figure 9)
Figure 1.
Figure 2.
doi:10.1111/j.1750-3639.2009.00301.x
531Brain Pathology 19 (2009) 531534
2009 The Authors; Journal Compilation 2009 International Society
of Neuropathology
8/7/2019 0209 Case 1
4/4
DIAGNOSIS
Encephalic Lipoma (tubulonodular type) with neuroglial
compo-
nent associated with partial agenesis of the Corpus Callosum.
The
patient was discharged home without further deficit.
Follow-up
MRI displayed remaining tumor in the location. The patient
remains under clinical observation for mass re-growth and
other
systemic lesions.
DISCUSSION
Intracranial lipomas are infrequent Central Nervous System
(CNS)
lesions with an incidence that ranges between 0.08 to 0.2%
of
autopsied cases and between 0.06 to 0.3% among those found
during imaging, (3) but according to others this frequency can
raise
up to 0.4%. (12) Although these lesions are considered grade
I
mesenchymal, non-meningothelial tumors according to the
World
Health Organization, (12) their origin is not clear and the idea
of a
primary malformation is still accepted. In fact, their origin
may
arise in the abnormal persistence and abnormal
differentiation
of the primitive meninx. (5) These kind of lesions are more
fre-
quently detected as a single entity, however, they can also be
acomponent of encephalocraniocutaneous lipomatosis a rare neu-
rocutaneous syndrome. (7)
By imaging studies intracranial lipomas are frequently located
in
the midline, usually in the supratentorial compartment, and
more
precisely they tend to be interhemispheric in the anterior
corpus
callosum. (9, 12, 15) In fact, pericallosal lipomas as a single
entity
are usually divided into two groups: curvilinear and
tubulonodular;
(1, 2, 14, 15). The former are thin, posteriorly located in the
corpus
callosum, and have low incidence of associated anomalies;
(2,14).
On the other hand, tubulonodular lipomas are located
anteriorly,
and are associated with a high incidence of facial defects
and/or
encephaloceles. (14) On MRI, characteristically these lesions
are
homogenous, and show hyperintensity on T1-weighted images
andhypo or isointensity on T2. (5)
Clinically patients can be asymptomatic, present with
recurrent
headaches, (3) show mental retardation (8) or can present
with
focal or generalized epilepsy, (4, 6) which has been regarded
by
some as the most frequent presentation, (11) but this has
more
recently been challenged. (13)
In our case, the patientpresented with three lesions: a
subcutane-
ous frontal lipoma independent of the cranial vault, an
intracranial
tubulonodular lipoma mixed with neuroglial tissues arising in
the
interhemisphericfissure, and partialagenesis of the posterior
corpus
callosum.There was no history of mental retardation or
epilepsy.
In terms of the histological assessment, this case showed
typical
features of a mature lipoma intermingled with neuroglial
tissue
imparted by the presence of neuropil showing reactive
astrocytesand mature neurons with glial satellitosis. Reports of
lipomas
arising in that location with or without agenesis of the
corpus
callosum are not abundant and most of the lesions described
are
composed only of typical mature lipomatous tissue; (12) and
these
lesions are usually sharply demarcated from cortex, (10) or
but
others may show myelo-lipomatous differentiation (i.e., with
hematopoietic elements).
In conclusion, we report a case of an asymptomatic child
with
partial agenesis of the corpus callosum and two lipomas, an
extrac-
ranial one with mature lipomatous tissues only and a second
intrac-
ranial interhemispheric frontal mass with a mixture of
mature
lipomatous and neuroglial tissues.
REFERENCES
1. Alzoum M, Alorainy IA, Husain M, Al Ruhainmi K (2002)
Multiple
pericallosal lipomas in two siblings with frontonasal dysplasia.
Am J
Neuroradiol23:7301.
2. Demaerel P, Van de Gaer P, Wilms G, Baert AL
(1996)Interhemispheric lipoma with variable callosal
dysgenesis:
relationship between embryology, morphology, and
symptomatology.
Eur Radiol6(6):9049.
3. Donati F, Vassella F, Kaiser G, Blumberg A (1992)
Intracranial
lipomas. Neuropediatrics 23(1):328.
4. Gastaut H, Regis H, Gastaut JL, Yermenos E, Low MD (1980)
Lipomas of the corpus callosum and epilepsy. Neurology
30(2):1328.
5. Gmez-Goslvez F, Menor-Serrano F, Tllez de Meneses-Lorenzo
M,
AleuPrez-Gramunt M, Sala-Snchez AG, Rubio-SorianoA,
Carbonell-Nadal J, Mulas F (2003) Lipomas intracraneales en
pedi-
atra: estudio retrospectivo de 20 pacientes.Rev
Neurol37(6):51521.
6. Guye M, Gastaut JL, Bartolomei F (1999) Epilepsy and
perisylvian
lipoma/cortical dysplasia complex. Epileptic
Disord1(1):6973.
7. Haberland C, Perou M (1970) Encephalocraniocutaneous
lipomatosis.Arch Neurol22:14455.
8. Hayashi T, Shojima K, Yamamoto M, Hashimoto T, Fukuzumi
A,
Honda E (1983) Intracranial lipomasreport of six cases. No
To
Shinkei 35(3):25768.
9. Ichikawa T, Kumazaki T, Mizumura S, Kijima T, Motohashi
S,
Gocho G (2000) Intracranial lipomas: demonstration by
computed
tomography and magnetic resonance imaging. J Nippon Med Sch
67(5):38891.
10. Kakita A, Inenaga C, Kameyama S, Masuda H, Ueno T, Honma
J,
Shimohata M, Takahashi H (2005) Cerebral lipoma and the
underlying cortex of the temporal lobe: pathological
features
associated with the malformation. Acta
Neuropathol109(3):33945.
11. Kazner E, Stochdorph O, Wende S, Grumme T (1980)
Intracranial
lipoma. Diagnostic and therapeutic considerations. J
Neurosurg
52(2):23445.12. Kleihues P, Cavenee WK (2000) Pathology and
Genetics of Tumours
of the Nervous System, IARCPress: Lyon.
13. Loddenkemper T, Morris HH 3rd, Diehl B, Lachhwani DK.
(2006)
Intracranial lipomas and epilepsy. J Neurol253(5):5903.
14. Tart R, Quisling RG (1991) Curvilinear and tubulonodular
varieties of
lipoma of the corpus callosum: an MR and CT study. J Comput
Assist
Tomogr 15(5):80510.
15. Truwit C, Barkovich AJ (1990) Pathogenesis of intracranial
lipoma:
an MR study in 42 patients. AJR Am J Roentgenol155(4):85564.
ABSTRACT
We describe a 1 year-old male infant who presented to the
Depart-
ment of Plastic Surgery with a subcutaneous frontal mass.
Radio-
logical studies showed this to be an extracranial mass, but
imagingalso demonstrated a second interhemispheric mass in the
frontal
lobe as well as partial agenesis of the corpus callosum. Only
the
frontal mass was resected at that time and it was a lipoma. At
the
age of five, surgical excision of the second lesion was
performed
since it had increased in size. The child had no history of
seizures.
It showed lipomatous tissue with hyalinized connective areas
inter-
mingled with a neuroglial component. The lesion was diagnosed
as
an encephalic lipoma (tubulonodular type) associated with
partial
agenesis of the corpus callosum.The patient is under clinical
obser-
vation for mass re-growth and other systemic lesions.
Correspondence
534 Brain Pathology 19 (2009) 531534
2009 The Authors; Journal Compilation 2009 International Society
of Neuropathology






















![[20대연구소]주간뉴스클리핑(20140203 0209)](https://img.pdfslide.net/doc/110x75/55912cde1a28ab1c028b4596/2020140203-0209.jpg)




