8/7/2019 0310case1 GCA
1/4
C A S E O F M O N T H M A R C H 2 0 1 0 bpa_403 863..866
A 24-YEAR-OLD MALE WITH HEADACHES
Zhongchuan Will Chen, MDCM1; Sean P. Symons, MD2; Beverley
Young, RTC3; Juan M. Bilbao, MD4
1 Department of Pathology, Sunnybrook Health Sciences Centre,
University of Toronto, Toronto, Ontario.2 Department of Radiology,
Sunnybrook Health Sciences Centre, University of Toronto, Toronto,
Ontario.3 Department of Pathology, Sunnybrook Health Sciences
Centre, University of Toronto, Toronto, Ontario.4 Department of
Pathology, Sunnybrook Health Sciences Centre, University of
Toronto, Toronto, Ontario.
CLINICAL HISTORY
A 24-year-old Caucasian man was admitted following a 10-day
history of severe headache leading to collapse on the street.
On
presentation, he was confused and agitated with left-sided
weak-
ness and a positive left Babinski sign. His medical history
was
significant for asthma and non-Hodgkins lymphoma 10 years
pre-
viously treated with chemotherapy and radiation therapy with
no
recurrence.
Routine blood-work, hypercoagulability and autoimmune
workups including anti-neutrophil cytoplasmic antibodies
were
all normal. Serology was negative for Arbovirus, Bartonella,
Cryptococcus and the hepatitides. Consent for HIV testing
was not obtained. Blood, cerebrospinal fluid and urine
cultures
were all negative. Blood and urine toxicological screening
was
unremarkable.
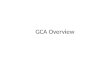
RADIOLOGY
CT perfusion suggested ischemia in both middle cerebral
artery
(MCA) and left anterior cerebral artery (ACA) territories and
inf-
arction in the left posterior cerebral artery (PCA) territory.
CT
angiography showed filling defects in these territories as
well
(Figures 1A, 1B, 1C). Treatment with intravenous tissue
plasmino-
gen activator (TPA) and intra-arterial thrombolysis was
attempted.
Initial anteroposterior angiogram confirmed occlusion of the
rightdistal M1 MCA and left A2 ACA (Figure 1D). Mechanical
throm-
bolysis and 4 mg of intra-arterial TPA were unsuccessful in
reopen-
ing the right MCA. The patient deteriorated and was declared
brain
dead 31 hours after arrival to hospital.
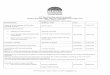
PATHOLOGY
On post-mortem examination, the fresh brain weighed 1560 g
and
showed edema with bilateral transtentorial herniation and
cerebel-
lar protrusion. Coronal sections showed thromboembolic
occlusion
of both ACAs beyond their A2 segments and the left MCA from
its
origin to its bifurcation (Figure 2). All posterior fossa
vessels were
normal. Both common carotid and internal carotid arteries
werepatent, but the right external carotid artery appeared
thickened with
a reduced lumen. Gross examination of the remainder of the
body
was unremarkable.
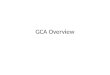
Hematoxylin phloxine saffron (HPS) stain-stained permanent
sections of the M1 and M2 segments of both MCAs, both ACAs
beyond the anterior communicating artery and the left P2 PCA
demonstrated a circumferential arteritic process composed of
multi-nucleated giant cells, lymphocytes and histiocytes
concen-
trated in the intima with fragmentation of the elastica interna
(rep-
resentative section; Figure 3).
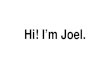
Elastica interna fragmentation by invading giant cells was
high-
lighted by Elastic Van Gieson staining (Figure 4A). CD68
staining
revealed a sandwich-like pattern of immunoreactive cells in
the
intima and adventitia with relative sparing of the media
(Figure 4B). A CD4/CD8-positive lymphocytic and mononuclear
cell infiltrate was present in the adventitia (CD4, Figure 4C;
CD8,
Figure 4D). Recent thrombosis in affected vessels caused
varying
degrees of corresponding neuronal ischemic change. There was
no
evidence of fibrinoid necrosis or previous healing lesions, but
a
A
B
C D
Figure 1.
doi:10.1111/j.1750-3639.2010.00403.x
863Brain Pathology 20 (2010) 863866
2010 The Authors; Journal Compilation 2010 International Society
of Neuropathology
8/7/2019 0310case1 GCA
4/4
DIAGNOSIS
Idiopathic disseminated giant cell arteritis (GCA).
DISCUSSION
GCA is extremely rare in young patients, such that onset above
age
49 is one of its American College of Rheumatology (ACR)
diag-nostic criteria. Due to the patients atypical presentation,
GCA was
not suspected and an erythrocyte sedimentation rate and
temporal
artery sampling were not performed. Although GCA classically
involves the temporal artery, it can involve other intracranial
and
extracranial arteries. The intracranial arteries most
commonly
affected are those of the vertebrobasilar system, but no
histologically-confirmed cases of GCA involving the cerebral
arteries have been reported.A rare form of GCA known as
dissemi-
nated visceral giant cell arteritis (DVGCA) has been reported
to
involve exclusively the extracranial organs (4), but
concurrent
intracranial and extracranial involvement in GCA has never
been
reported in patients under age 50. The few reports describing
con-
current involvement were all in older patients with
intracranial
involvement limited to the vertebrobasilar system (7, 9) or
theanterior inferior cerebellar artery (6). In fact, intracranial
GCA in
patients under age 50 is a rare occurrence in itself; to our
knowl-
edge, only two such cases with histological features similar to
ours
have been described, but both were associated with infectious
aeti-
ologies (1, 2). Most of the cases of intracranial GCA, DVGCA
and
GCA with concurrent involvement (including our case) share
the
textbook histology of classic GCA. Takayasu arteritis (TA),
which
can resemble GCA histologically, was also considered since one
of
its ACR diagnostic criteria is onset below age 40. However,
the
patient did not demonstrate history or physical examination
find-
ings fulfilling other TA criteria and the aorta was
uninvolved.
Moreover, direct involvement of intracranial arteries by TA
is
extremely rare, with only a few reports to date (5,
10).Granulomatous vasculitis of the CNS can be classified as
primary angiitis of the CNS (PACNS) or secondary to systemic
causes. By definition, PACNS is confined to the CNS and can
only
be established after ruling out secondary causes. It has
been
described to occur at any age, is male-predominant and lacks
sys-
temic symptoms (3). Histologically, small and medium leptom-
eningeal and cortical arteries are involved by a necrotizing
granu-
lomatous vasculitis. PACNS can also be indistinguishable
from
amyloidb peptide-related angiitis without the appropriate
immu-
nohistochemical workup (8). The dissimilar microscopic
picture,
presence of extracranial arteritis and negative b-amyloid
staining
rule out both diagnoses in our case. A secondary CNS
vasculitis
was also considered unlikely in our case as extensive workup
and
past medical history did not reveal any infection, systemic
vascu-litides, sarcoidosis or drugs.
We report the first occurrence of disseminated GCA with
extrac-
ranial and anterior, middle and posterior cerebral arterial
involve-
ment causing fatal cerebral infarction in an atypical age
group.
REFERENCES
1. Berger TM, Caduff JH, Gebbers JO (2000) Fatal
varicella-zoster virus
antigen-positive giant cell arteritis of the central nervous
system.
Pediatr Infect Dis J19(7):6536.
2. Browne L, Hardiman O, ODwyer H, Farrell M (2003)
Intracranial
giant cell arteritis with fatal middle cerebral artery territory
infarct.
Clin Neuropathol22(4):199203.
3. Hajj-Ali RA, Calabrese LH (2009) Central nervous system
vasculitis.Curr Opin Rheumatol21(1):108.
4. Kagata Y, Matsubara O, Ogata S, Lie JT, Mark EJ (1999)
Infantile
disseminated visceral giant cell arteritis presenting as sudden
infant
death. Pathol Int49(3):22630.
5. Magge SN, Chen HI, Stiefel MF, Ernst L, Cahill AM, Hurst R,
Storm
PB (2008) Multiple ruptured cerebral aneurysms in a child
with
Takayasu arteritis. J Neurosurg Pediatr 1(1):837.
6. McLean CA, Gonzales MF, Dowling JP (1993) Systemic giant
cell
arteritis and cerebellar infarction. Stroke 24(6):899902.
7. Save-Soderbergh J, Malmvall BE, Andersson R, Bengtsson BA
(1986) Giant cell arteritis as a cause of death. Report of nine
cases.
JAMA 255(4):4936.
8. Scolding NJ, Joseph F, Kirby PA, Mazanti I, Gray F, Mikol J,
Ellison
D, Hilton DA, Williams TL, MacKenzie JM, Xuereb JH, Love S
(2005) Abeta-related angiitis: primary angiitis of the central
nervoussystem associated with cerebral amyloid angiopathy. Brain
128(Pt
3):50015.
9. Sendino A, Barbado FJ, Gonzalez-Anglada I, Anton E,
Lopez-Barea
F, Vazquez JJ (1992) Temporal arteritis: a form of systemic
panarteritis. Ann Rheum Dis 51(9):10824.
10. Sikaroodi H, Motamedi M, Kahnooji H, Gholamrezanezhad A,
Yousefi N (2007) Stroke as the first manifestation of
Takayasu
arteritis. Acta Neurol Belg107(1):1821.
ABSTRACT
A 24-year-old man presented with a ten-day history of severe
head-
ache leading to collapse. CT studies showed filling defects
involv-
ing the anterior, middle and posterior cerebral arteries and
evidence
of ischemia and infarction. Post-mortem examination revealed
multiple cerebral infarcts secondary to an arteritic process
com-
posed of multi-nucleated giant cells, lymphocytes and
histiocytes
in both middle and anterior cerebral arteries and one
posterior
cerebral artery. Both carotid siphons and one renal artery
segment
were also involved. Extensive workup and stains for systemic
and
infectious causes were negative, leading to a diagnosis of
atypical
giant cell arteritis (GCA). Disseminated GCA involving
extracra-
nial arteries and the anterior, middle and posterior cerebral
arteries
leading to cerebral infarction has not been previously reported.
We
report this atypical case of disseminated GCA in a young
patient
with clinical features distinct from classic GCA (temporal
arteritis)
and discuss the differential diagnosis.
Correspondence
866 Brain Pathology 20 (2010) 863866
2010 The Authors; Journal Compilation 2010 International Society
of Neuropathology