Embed Size (px)
Citation preview
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 1/24
ALLERGY TOPICS
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 2/24

8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 3/24
You have just assisted in the delivery of a 38-weekgestational age male infant who was born via cesarean
section to a 25-year-old woman. As you are completing theinfant's initial physical examination, the father mentions thathe and his wife have allergic rhinitis and asthma. He askswhether his son is at increased risk for allergies and howthey can reduce the boy's chance for developing suchallergic disorders.
Of the following, the MOST appropriate next step is:
A. explain that because both parents have asthma, breastfeeding will notreduce the risk of eczema
B. explain that breastfeeding or formula choices do not matter now becausethe mother did not restrict her diet during pregnancy
C. measure the cord blood immunoglobulin E concentration to help establishthe newborn's risk for atopic disorders
D. recommend exclusive breastfeeding for 4 months with the addition of ahypoallergenic formula if needed
E. start the newborn on a cow milk formula for the first month, then switch tostrict breastfeeding if he develops eczema
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 4/24
D. RECOMMEND EXCLUSIVE BREASTFEEDING FOR 4 MONTHS WITH THE
ADDITION OF A HYPOALLERGENIC FORMULA IF NEEDED
The incidence of atopy (allergic rhinitis, asthma, eczema) has increased significantly over the past few decades. Theability to intervene and either delay or prevent atopic disease in infants born to atopic parents has been the subject ofnumerous studies. Application of these studies to the population as a whole is difficult because the specific interventionsand endpoints for each study often differ. However, one aspect that is agreed on is that atopy risk for infants increases
significantly when both parents have a history of atopy (30% to 60%) compared with a history for just one parent (20% to40%) or neither parent (10% to 15%).
Prior to delivery, two prevention strategies have been studied: maternal diet restriction and supplementation withprobiotics. Currently, no evidence supports maternal dietary restriction to common allergenic foods. Some studies havesupported administration of probiotics (eg, Lactobacillus rhamnosus ) to the mother 2 to 4 weeks before delivery and to theinfant for 6 months after birth. One study demonstrated a reduction in eczema at 2 years but no reduction in asthma,immunoglobulin (Ig) E concentrations, or allergen sensitization. Further, the dose and type of probiotic has differed invarious investigations, making generalized recommendations difficult.
Even if both parents have atopy, as described in the vignette, breastfeeding or formula choices may affect atopy outcomes
for the infant. In "high-risk" newborns (ie, both parents have atopy or one parent and one sibling have atopy), the AmericanAcademy of Pediatrics Committee on Nutrition recommends exclusive breastfeeding for at least 4 months, withsupplementation of a hypoallergenic formula if needed. Although it is difficult to compare studies because the duration ofbreastfeeding and atopic outcome (ie, eczema, allergic rhinitis, asthma) differ, breastfeeding for at least 3 monthsreduces the risk for eczema. The protective benefit becomes more complex when controlling for the specific maternalatopic condition. For "high-risk" infants born to women who choose not to breastfeed, most studies and experts supportstarting an extensively hydrolyzed formula. Starting a cow or soy milk formula, compared with an extensively hydrolyzedformula, increases the risk for early eczema. Or note, interventions resulting in decreased atopy early in life may notpredict later atopic outcomes.
Cord IgE concentrations can be used to assess a newborn's risk for atopy, but its measurement currently is not
recommended as a routine screening tool. Furthermore, because both parents in the vignette have a history of atopy, thechild already is considered "high risk." The ability to predict atopy based on cord IgE concentrations also depends on thecutoff value used. In one study, 80% of newborns whose cord IgE concentrations were greater than 0.9 kU/L subsequentlydeveloped atopy by 5 years of age, but the specific IgE value did not correlate with atopy severity.
American Board of Pediatrics Content Specification:Know that breast-feeding for the first six months after birth with supplementation with a complete, nutritionally balancedhypoallergenic formula will decrease the severity and delay the onset of allergic disease

8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 5/24
PEARLS FOR BREASTFEEDING
Do not restrict maternal diet during pregnancy orlactation to prevent food allergy
Exclusive breast feeding for 4-6 months Maybe reduces risk of eczema, food allergy to CM,
wheezing If can’t breast feed – consider hydrolyzed infant
formula in *at-risk infants May reduce eczema, allergy to cow’s milk (not other
foods)
* biological parent or sibling with FA, AR, AD, Asthma
No conclusions on timing of introduction ofpotentially allergenic foods beyond 4-6 months
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 6/24
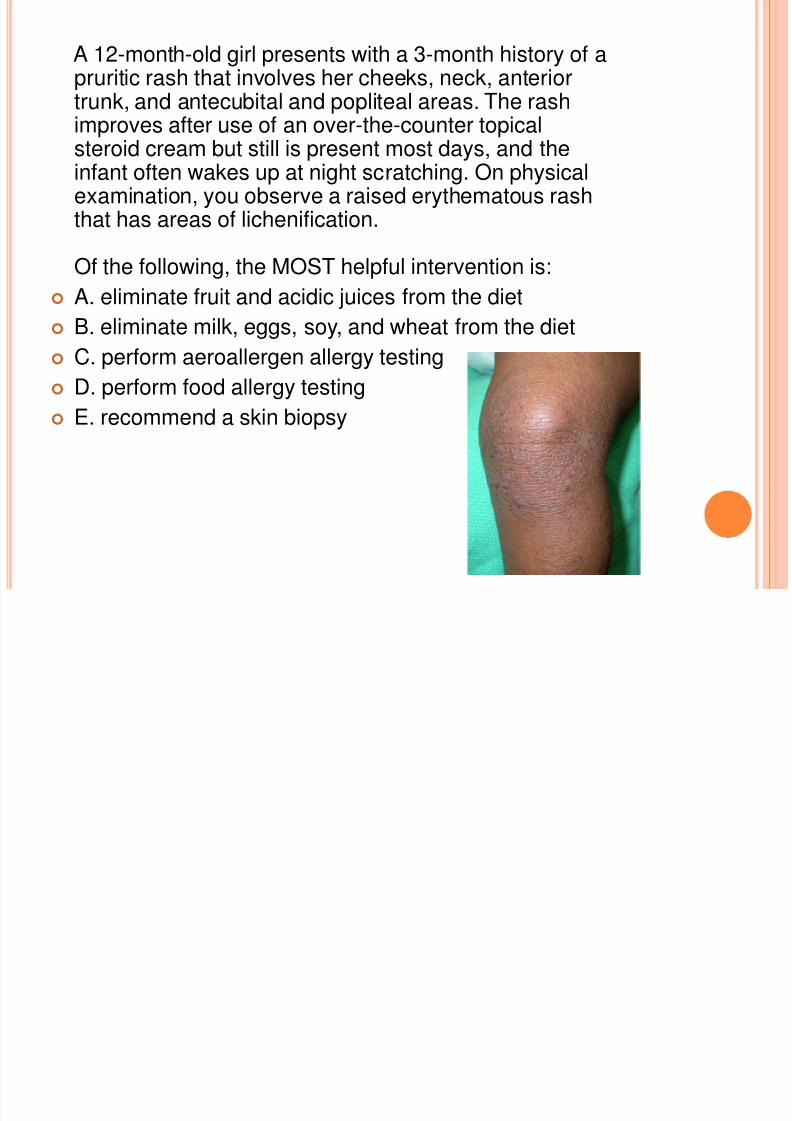
A 12-month-old girl presents with a 3-month history of apruritic rash that involves her cheeks, neck, anteriortrunk, and antecubital and popliteal areas. The rashimproves after use of an over-the-counter topicalsteroid cream but still is present most days, and theinfant often wakes up at night scratching. On physicalexamination, you observe a raised erythematous rashthat has areas of lichenification.
Of the following, the MOST helpful intervention is: A. eliminate fruit and acidic juices from the diet
B. eliminate milk, eggs, soy, and wheat from the diet
C. perform aeroallergen allergy testing
D. perform food allergy testing
E. recommend a skin biopsy
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 7/24
D. PERFORM FOOD ALLERGY TESTING
Some 30% to 40% of infants who have moderate-to-severe atopic dermatitis (AD), such as describedfor the infant in the vignette, may have an underlying immunoglobulin (Ig) E-mediated food allergyexacerbating the AD. For some infants, food ingestion may result in immediate worsening of AD severity,although most infants do not demonstrate this immediate reaction. Many foods have been implicated in AD,but five (milk, eggs, soy, wheat, and peanut) account for 90% of the causative allergens.
Both allergy skin testing and measurement of serum IgE concentrations to these foods can help to identifyand eliminate likely triggers. Either a negative IgE blood test (<0.35 kU/L) or a negative skin test for a specificfood provides a high negative predictive value. On the other hand, the positive predictive value for a skin orblood test may be only 50%.
Although the most commonly implicated foods often are eliminated from the diet, such an approach does notimprove symptoms in most (60% to 70%) children because they do not have IgE-mediated AD. Theunnecessary elimination of multiple foods can have an adverse effect on nutrition, and food avoidance shouldbe guided by the dietary history, eczema severity, and skin or blood testing.
Frequently, children experience perioral rashes after drinking fruit juice. Such rashes typically are nonpruritic,limited to the area of contact, and resolve within a few hours. The mechanism of such rashes is unknown, butchildren generally outgrow such reactions by age 4 years. In cases involving more widespread cutaneoussymptoms, such as described in the vignette, elimination of fruit or acidic juices is unnecessary.
Parents often request testing for environmental allergies. House dust mites have been implicated in somecases of AD, although they are less likely a cause for moderate-to-severe atopic dermatitis than foodallergies. Climate changes such as cold, dry air or hot, humid weather can worsen AD, but specific seasonal
allergens such as oak tree or ragweed are not associated with eczema in infants.
A skin biopsy can provide insight into the pathophysiology of chronic rashes or lesions. Generally, skinbiopsies neither are advised nor provide insight into the causes of typical AD manifestations in infants, butatypical presentations or lack of expected improvement with appropriate therapy should prompt considerationof a dermatology referral.
American Board of Pediatrics Content Specification:Understand the relationship of eczema and food allergies, and how to evaluate a patient with
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 8/24
PEARLS FOR ECZEMA
Presents by 2-6 months mostly, almost all by 5yo
Part of Atopic March Eczema/Food Allergy ->Asthma->Allergic Rhinitis
Major Features: Pruritis!!!!
Chronic/relapsing course
Personal/Family hx of atopy
Typical Distribution
Face and extensor surfaces < 2yo, trunk, face Flexural areas > 2 yo, Hands, feet
* SPARES nasolabial skin and diaper area
Dry skin is not a major feature
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 9/24
PEARLS FOR ECZEMA CONTINUED
Food allergies may trigger flares but is not a cause!!! Milk, egg, wheat, soy, peanut Only in children
< 5yo Moderate-severe persistent eczema despite optimum therapy
Child has a hx of worsening eczema after ingesting foods Complications associated with eczema
Infections S.aureus, HSV, Molluscum, Fungal infections
Eczema vaccinatum associated with smallpox vaccine
Treatment Moisturizing, bathing, topical steroids, oral antihistamines.
KNOW***** Eczema in patient with hx of severe infections and bloody
stools =====Wiscott Aldrich Syndrome Oto-sino-pulmonary infections initially. Get opportunistic infections
later.
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 10/24
A mother brings in her 11-month-old son after he brokeout in "hives" today during breakfast. The infant hadstayed home from child care with a low-grade fever, andthe mother had let him eat eggs for the first time.
Immediately after breakfast, the mother noted a diffuseerythematous, pruritic rash covering the boy's trunk andextremities. She is concerned that her son may have anegg allergy.
Of the following, the BEST statement regarding
immunoglobulin E-mediated egg food allergy is that: A. cooking the egg eliminates its allergic potential
B. egg is the most common food allergy in the firstpostnatal year
C. egg white is more allergenic than egg yolk
D. most children do not outgrow their egg allergy E. the measles-mumps-rubella vaccine is contraindicated
in children who have egg allergy
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 11/24
C. EGG WHITE IS MORE ALLERGENIC THAN EGG YOLK
Immunoglobulin (Ig) E-mediated egg allergy is one of the more common childhood food allergies, affectingapproximately 1% to 2% of children. As described in the vignette, cutaneous features are common,including atopic dermatitis, urticaria, and pruritus. Once the diagnosis of egg allergy is determined,
patients generally are advised to avoid all egg food products with the hope that most children will outgrowtheir egg allergy within 3 to 5 years.
The primary allergenic egg protein is ovomucoid, a protein predominantly in the egg white. Approximately50% of children may be able to tolerate small amounts of egg protein that has been heated extensively(eg, baked goods). Prolonged heating at high temperatures can denature proteins from a conformational formto a linear form. Some children who are allergic to eggs do not recognize the linear protein form as an allergenand, therefore, do not experience a reaction. Of note, the brief cooking used to make scrambled eggs will
not denature heat-stable proteins.
The relationship between egg allergy and vaccination is a common question. The measles-mumps-rubellavaccine is safe for children who have egg allergy and should be administered without special precautions.The trivalent influenza and live attenuated influenza vaccines contain small amounts of egg proteinand are contraindicated for patients who have egg allergy. However, studies have supported a two-doseprotocol for the administration of the influenza vaccine in egg-allergic patients. The two-dose protocol involvesadministering one tenth of the vaccine, observing the recipient for a period of time, and administering the restof the vaccine, followed by a similar observation period.
In westernized countries, milk generally is regarded as the most common food allergen in infants, with anincidence of 2.5%, compared with an incidence of 1.5% for egg allergy.
American Board of Pediatrics Content Specification:Know that most milk, egg, and soy allergies are outgrown by 5 years of age
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 12/24
PEARLS FOR FOOD ALLERGY
Non-immune reactions Toxic: food poisoning Intolerance (host dependent)
Lactase deficiency, galactosemia
Immune reactions IgE: hives, AE, GI sxs, resp sxs, anaphylaxis, OAS Mix: EE, eczema
Non-IgE: FPIES Prevalence of food allergy
Young Children Milk is most common (2.5%), egg (1.3%), Peanut (0.8%) Overall 6%
Adults Shellfish (2%), peanut (0.6%), Tree nuts (0.5%), fish (0.4%) Overall 3.7%
Diagnosis is based on hx, SPT/serum IgE, oral food challenges Testing offers very good NPV but poor PPV
Treatment: food avoidance, epipen, read labels, medicalert bracelet
Natural Hx: 85% outgrow milk, egg, wheat, soy by 5 yo 20% outgrow peanuts, 10% outgrow tree nuts, Shellfish, fish usually persist
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 13/24
An 18-year-old girl is admitted to the hospital for intravenous therapy for acomplicated urinary tract infection that failed to respond to outpatient therapy with
a sulfa-based antibiotic. Her urine culture shows more than 100,000 colony-forming units/mL of Pseudomonas aeruginosa that is sensitive to aztreonam andimipenem. As you take her medical history, she mentions she is "highly allergic" topenicillin.
Of the following, a TRUE statement regarding penicillin drug reactions is that:
A. a nonpruritic maculopapular rash that occurs in patients who receive amoxicillinduring mononucleosis is a contraindication for future penicillin therapy
B. aztreonam can be administered safely to patients who have a history ofimmunoglobulin E (IgE)-mediated penicillin allergy
C. desensitization can be used to administer penicillin safely to patients who haveexperienced Stevens-Johnson reactions to penicillin
D. skin testing to major and minor determinants of penicillin can exclude IgE-mediated and non-IgE-mediated reactions
E. a patient who can only recall a childhood history of penicillin allergy but does notremember the details is very likely to react to future penicillin courses
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 14/24
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 15/24
DRUG ALLERGY PEARLS
Type-1 reactions are IgE mediated
Atopy is not a risk factor for IgE drug allergy
Cross-Reactivity for PCN PCN 100% Cephalosporin variable – 2%
1st and 2nd G cause more allergic reactions
Carbapenems – imimpenem, meropenem is moderate – 0-10%
Aztreonam – does not cross-react with PCN
Only skin test reliably for PCN
Management + SPT to prepen: desensitization -SPT: administer normally or graded challenge
Cannot desensitize to non-IgE drug allergies SJS/TEN, Serum sickness, hepatitis, nephritis, hemolytic
anemia
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 16/24
A 10-year-old boy presents to the clinic complaining oftongue and mouth itching within a few minutes after eatingapples. His mother states that he has not experienced thesesymptoms with other foods, but they occur every time he eatsa fresh apple. He denies systemic symptoms, and the oralsymptoms resolve within a few minutes. Other than allergicrhinitis in the spring months, he is healthy.
Of the following, you are MOST likely to advise his motherthat:
A. allergy skin testing to fresh apples probably will havenegative results
B. cooking the apple will not alter its allergenicity
C. her son should avoid eating all fruits
D. her son should avoid milk products
E. her son's symptoms are related to his allergic rhinitis
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 17/24
E. HER SON'S SYMPTOMS ARE RELATED TO HIS ALLERGIC RHINITIS
The boy described in the vignette is exhibiting a common form of food allergy called food pollen syndromeor oral allergy syndrome (OAS). OAS is seen in 30% to 40% of children who have allergic rhinitis. Certainfoods contain proteins that are similar to airborne allergens, and patients who are allergic to an aeroallergen are atrisk of developing reactions to the cross-reacting food protein.
In most cases, symptoms are isolated to the oropharynx, where food comes in contact with a mucosal surface, andinclude lip, tongue, and oral mucosal pruritus; tingling; and occasionally angioedema. Interestingly, because thesefood proteins are heat-labile, cooking the food (eg, apple pie) negates its antigenic properties. Although symptomstypically are mild, there are reports of severe reactions. In one recent review involving 1,361 patients who had OAS,8.7% experienced systemic symptoms outside the gastrointestinal tract, 3% experienced symptoms other than oralsymptoms, and 1.7% experienced anaphylactic shock.
Because OAS is relatively specific to particular cross-reacting food(s), patients do not need to avoid otherfruits or vegetables to which they have not experienced reactions. Avoidance of unrelated foods (eg, milk, eggs)is not recommended unless the history suggests a previous reaction. The decision to avoid causative foods can bebased on the severity of reaction. Referral to an allergist typically is reserved for situations when skin testing isdesired or if the child has experienced systemic symptoms. Skin testing is performed using a commercial extractor the fresh fruit or vegetable. When using fresh food, the sensitivity of skin testing with a history ofreproducible reactions is close to 90%, while the negative predictive value is more than 90%. The skin prickdevice is pressed into the food and then pressed in the skin (so-called "prick-prick" skin test).
Other immunoglobulin (Ig) E food reactions include atopic dermatitis, eosinophilic esophagitis, and specific foodallergy. In the United States, 85% of specific food allergies are due to egg, milk, wheat, soy, peanuts, tree nuts, fish,and shellfish. Most children who have IgE food allergies react to only one or two causative foods, althoughchildren who have tree nut allergy, atopic dermatitis, and eosinophilic esophagitis often have IgE-mediated reactionsto multiple foods.
American Board of Pediatrics Content Specification:Know that more than 90% of food-allergic individuals demonstrate clinical responses to only 1 or 2 foods
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 18/24
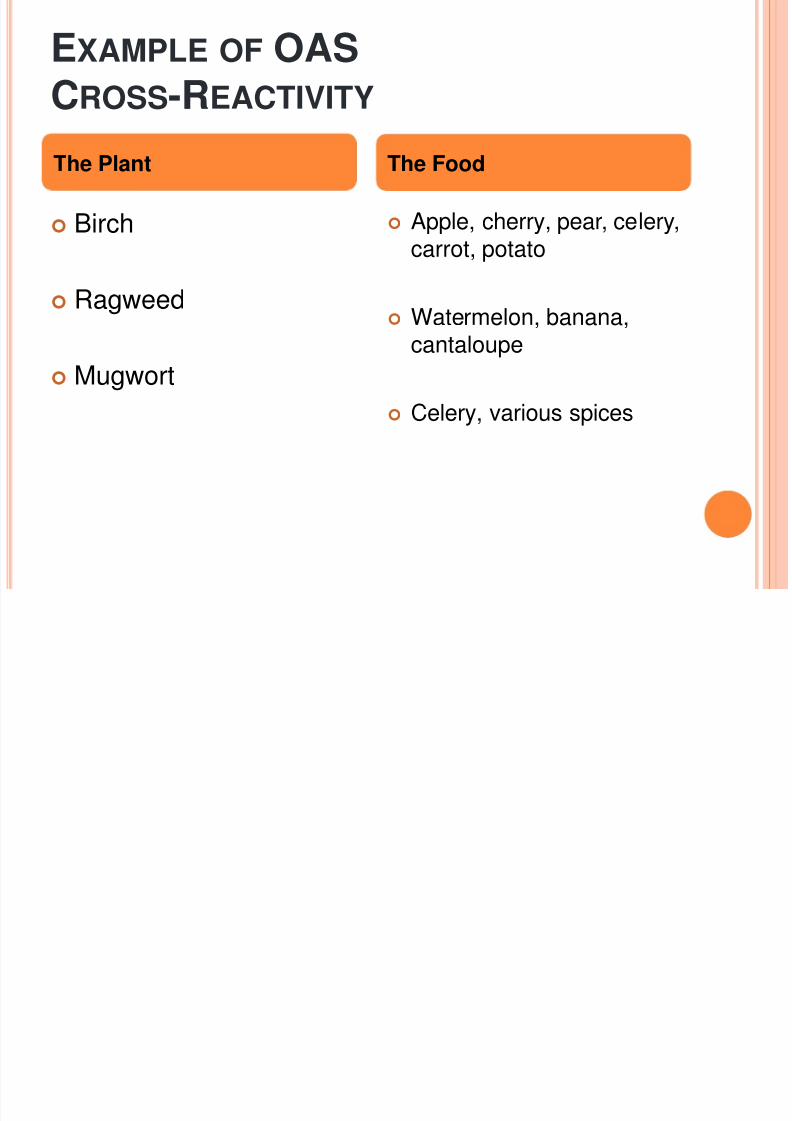
EXAMPLE OF OASCROSS-REACTIVITY
Birch
Ragweed
Mugwort
Apple, cherry, pear, celery,carrot, potato
Watermelon, banana,cantaloupe
Celery, various spices
The Plant The Food
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 19/24
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 20/24
The boy described in the vignette experienced a near-fatal reaction to a flying insect, with signs and symptomsconsistent with anaphylaxis. In the United States, stinging insects causing immunoglobulin (Ig) E-mediatedreactions include honeybees, yellow jackets, yellow hornets, white-faced hornets, paper wasps, and fire ants. Theidentification of an IgE-mediated allergic disorder involves identifying the allergen, estabishing a causalrelationship between the allergen and the reaction, and demonstrating the presence of specific IgE via immediatetype skin testing or in vitro testing.
Indications for immediate type skin testing include:
1. Identification of aeroallergen triggers in patients who have asthma2. Allergic rhinitis that is not controlled with usual medications or if specific avoidance (eg, pet dander) is desired3. Food allergy4. Insect sting allergy5. Vaccine, drug, or latex allergy6. Evaluation for moderate-to-severe atopic dermatitis7. Other conditions, including allergic fungal sinusitis, allergic bronchopulmonary aspergillosis, and eosinophilicesophagitis
The decision to perform skin or in vitro testing depends on the age of the patient, the desire to start allergenimmunotherapy, time since the reaction, and severity of the reaction.
Allergy skin testing can be performed at any age, but infants and toddlers generally do not tolerate intradermalskin testing well and may not be able to communicate to their parent/clinician if they are developing a reactionduring testing. In addition, clinicians may elect to start with in vitro testing in patients who have experienced life-threating reactions, as described in the vignette. Unfortunately, both skin testing and in vitro testing, when usedalone for assessment of insect sting allergy, may provide false-negative results in up to 25% of patients. In casesof anaphylaxis, if the results of the initial test (skin or in vitro) are negative, the second testing modality should beundertaken. If testing is performed too soon (ie, within 2 weeks of the reaction), results may be negative due todepletion of mast cell mediators. Generally, skin testing should be performed 4 to 6 weeks after a sting reaction.
Current guidelines recommend that patients who experience less severe reactions (eg, local or normal reactions,
large local reactions, or cutaneous-only symptoms in children younger than than 16 years of age) do not requiretesting because of their low risk for future anaphylaxis. Epidemiologic studies have demonstrated that 25% to 50%of individuals can develop specific IgE to stinging insects, even after a normal or local reaction. However, suchindividuals (local reaction only) should not be tested, based on their normal reactions, and no specific avoidancemeasures or immunotherapy are recommended.
Finally, when flying insect testing is performed, a complete set of the five Hymenoptera venoms (honey bee,yellow jacket, white-faced hornet, yellow hornet, wasp) should be used unless the specific insect is captured andidentified by an entomologist.
American Board of Pediatrics Content Specification:
Know the indications for immediate-type skin testing
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 21/24
PEARLS FOR STINGING INSECTS
6 different types of stinging insects Honeybee, yellow jacket, yellow hornet, WF-hornet and wasp
(also fire ants)
Risk of systemic reaction depends on previous reaction Systemic symptoms 20-50% future risk
With IT: < 5% When to skin test in children
LLR: no Cutaneous symptoms only – no (this is dif. Than adults) Systemic symptoms: yes!!
Test for all 5 flying insects – identification not reliable
Prevention No bright clothes Long sleeves Destroy nests Insect repellants don’t work
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 22/24
You have been asked by a local school to provide recommendationsabout the use of self-injectable epinephrine for anaphylaxis. The schoolsupervisor is concerned about the increased incidence of peanut and
tree nut food allergy. School officials have requested that each child whohas a diagnosis of "food allergy" have two self-injectable epinephrinedevices at the school nurse's office.
Of the following, the BEST response regarding anaphylaxis is that:
A. a patient should not receive a second dose of epinephrine unless aclinician is present
B. epinephrine reaches higher peak plasma concentrations if injectedinto the thigh rather than the arm
C. families should keep one epinephrine autoinjector in the car in case areaction occurs after school
D. skin manifestations (eg, flushing, itching, urticaria) are rare in severeanaphylaxis
E. subcutaneous injection of epinephrine is preferable to intramuscularinjection
8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 23/24
B. EPINEPHRINE REACHES HIGHER PEAK PLASMA CONCENTRATIONS IF INJECTED INTO THE
THIGH RATHER THAN THE ARM
The most common antigenic triggers of anaphylaxis are foods, drugs, insect venom, radiocontrast media, and latex.After exposure to an antigenic trigger, symptoms generally develop within 5 to 30 minutes, although symptomscan occur up to several hours after the exposure. Severe allergic reactions usually occur after binding of specificimmunoglobulin (Ig) E to the high-affinity IgE receptor, with subsequent cross-linking of receptors and mediator
release (eg, histamine, tryptase) from mast cells and basophils.
Cutaneous manifestations such as urticaria, flushing, pruritus, and angioedema are the most commonsymptoms in anaphylaxis, occurring in 80% to 90% of episodes . Respiratory symptoms such as dyspnea,wheezing, shortness of breath, and cough are the next most frequent symptoms. Cardiovascular symptoms includecardiovascular collapse, tachycardia or relative bradycardia, and arrhythmias. Among the gastrointestinalmanifestations are nausea, vomiting, diarrhea, abdominal pain, and cramping. Finally, many patients complain ofeither a metallic taste or "a sense of impending doom."
Appropriate treatment of anaphylaxis consists of early administration of epinephrine. Because anaphylaxis can occurin the absence of a health-care professional such as at school, home, or a birthday party, children at risk alwaysshould have self-injectable epinephrine nearby. Although parents or other adults may be reluctant to inject a child with
epinephrine, this agent, not an antihistamine, is the drug of choice for anaphylaxis. In the past, outpatientadministration of epinephrine was subcutaneous, but research has demonstrated that intramuscular injection,specifically in the thigh, is the preferred route and location due to higher and faster peak plasmaconcentration. If epinephrine is administered, parents or school personnel should follow an emergency action plan.This should involve calling emergency services to evaluate the child and transport him or her to the emergencydepartment for further evaluation. The effects of a single dose of epinephrine typically last for 5 to 15 minutes; upto 20% of individuals experiencing anaphylaxis may require a second epinephrine dose. When symptoms persist, asecond (or third) dose should be administered, even if the parent or school professional still is awaiting the ambulance.Although epinephrine always is the drug of choice in anaphylaxis, glucagon may be required in refractory cases forpatients using beta blockers.
Self-injectable epinephrine should be available for all locations (ie, the patient usually carries one to two
injectors), but leaving the device in the car is not recommended because extreme temperature changes candecrease the efficacy. Recommended storage temperatures are 20°to 25°C at home and 15°to 30°C during tripsoutside the home, school, or workplace.
Approximately 5% to 20% of patients who suffer initial anaphylactic events can experience a "late-phase"response 4 to 24 hours later in which symptoms such as flushing, pruritus, or airway obstruction recur. Suchlater symptoms result from the recruitment of inflammatory cells after the initial hypersensitivity response.
American Board of Pediatrics Content Specification:Know that IgE-mediated allergen challenge induces immediate obstruction, which resolves and is followed in 4 to 12hours by persistent late-phase obstruction

8/6/2019 08.01.2011 Allergy Topics
http://slidepdf.com/reader/full/08012011-allergy-topics 24/24
PEARLS FOR ANAPHYLAXIS
Definitions are confusing Unknown ingestion
Hives/swelling + resp or hypotension
Likely allergen ingestion: > 2 Resp, hypotension, skin, GI
Known allergen Hypotension only
RF for anaphylaxis
Atopy ( not venom or drugs) Gender (males > females < 15 yo) More severe with IM administration Time since reaction – longer the time, less likely
Be careful for biphasic reactions – (6-8 hrs after) RF = asthma, food, previous hx., delayed epi, no steroids
Diagnosis: can get total and fractionated tryptase =- have to get it 60-90 minutes after reaction
DDX: Flushing sxs (carcionoid), other forms of shock, mastocytosis, pheochromocytoma scrombroid
poisoning. Rx:
Don’t delay epi (epipen jr (<22 kg), regular epipen > 22 kg, dose is 0.01 mg/kg of 1:1000 ABCs, lie the patient down (prevent empty heart syndrome) IVF Benadryl, H2 blockers, Steroids, Bronchodilators. If on beta-blocker, consider glucagon