Embed Size (px)
Citation preview

CMS Conditions of Participation (CoPs) for Critical Access Hospitals (CAHS):Ensuring Compliance
This is a 3-part series; each program can be taken independent of the others.
TELNET COURSE T2861 – PART 1 (WEBINAR)DATE: SEPTEMBER 12, 2013TIME: 9:00 – 10:30 A.M. CDT
TELNET COURSE T2864 – PART 2 (WEBINAR)DATE: SEPTEMBER 19, 2013TIME: 9:00 – 10:30 A.M. CDT
TELNET COURSE T2866 – PART 3 (WEBINAR)DATE: SEPTEMBER 26, 2013TIME: 9:00 – 10:30 A.M. CDT
CAHs must comply with CMS regulations and interpretive guidelines for the Conditions ofParticipation. Attendees will learn in detail the CoPs listed under program topics. Specificproblematic areas and recent changes will be addressed. Actions to take when a surveyor arrivesat the facility will also be discussed. Numerous changes to these regulations were made March15, 2013.
Target Audience: CEO, COO, CFO, CMO, CNO, Nursing Leadership, HIM Director, Pharmacist,Dietician, Social Worker, Infection Preventionist, Radiology Director, ED Director, OutpatientDirector, Ethicist, Director of Rehab, OT, PT, Speech Pathology and Audiology, OR Supervisor,Anesthesia Provider, Director of Swing Beds, Accreditation and Regulation Director, DepartmentDirector, The Joint Commission Coordinator, Performance Improvement Director, Risk Manager,Safety Officer, Compliance Officer, and Legal Counsel
Faculty: Sue Dill Calloway has been a nurse attorney and consultant for more than 30 years.Currently, she is President of Patient Safety and Healthcare Education and Consulting andpreviously the Chief Learning Officer for the Emergency Medicine Patient Safety Foundation. Priorto Sue’s current role, she was the Director of Hospital Patient Safety for The Doctors’ Companyand OHIC Insurance Company. She has conducted many educational programs for nurses,physicians, and other healthcare providers. Sue has authored over 100 books and numerousarticles. She is a frequent speaker and is well known across the country in the area of healthcarelaw, risk management, and patient safety. *The speaker has no real or perceived conflicts ofinterest that relate to this presentation.

PART 1
Program Topics:Introduction Changes: July 16, 2012 and March 15, 2013 CMS memos CAH problematic standards CAH resources Conditions of Participation CMS websites Copies of documents by surveyor How to locate changes Rehab or psych distinct unit standards CMS survey and certification website Visitation regulation Telemedicine standards
Survey Protocol Introduction Tasks in the survey protocol Survey team Task 1 – Off-site survey preparation Task 2 – Entrance activities Task 3 – Information gathering/investigation Task 4 – Preliminary decision making and
analysis of findings Task 5 – Exit conference Task 6 – Post-survey activities
Regulations and Interpretive Guidelines forCAHs Swing bed module Compliance with federal, state and local laws
and regulations Licensure of CAH Licensure, certification or registration of
personnel
Status and location Location in a rural area or treatment as
rural Location relative to other facilities or
necessary provider certification Compliance with CAH requirements at the
time of application agreements Agreements with network hospitals Agreements for credentialing and quality
assurance Emergency Services, respiratory policies ED staffing EMTALA Equipment, supplies, and medication Blood and Blood Products Staffing/Personnel Coordination with emergency response
systems Number of beds and length of stay Physical plant and environment Disposal of trash Storage of drugs Construction Maintenance Emergency procedures Life safety from fire Emergency fuel and water Emergency preparedness plan LSC waivers Fire inspections
Objectives:At the completion of this program, the participants will be able to:1. State that CMS requires the board to have a written agreement for telemedicine services.2. Discuss that CMS has a list of emergency drugs and emergency equipment that every CAH
must have.3. Recall that the length of stay in the CAH should not exceed 96 hours on an annual average
basis.4. Discuss recommendations to do a gap analysis to ensure compliance with all the hospital
CoPs.5. Recognize that hospitals must have a visitation policy and patients must be informed.

PART 2Program Topics:Introduction Governing body or responsible individual Nurse on duty Staff and physician responsibilities Physician supervision PA, NP, CNS responsibilities Provision of services Guidelines for medical management Services provided through agreements or
arrangements Nursing services Drugs and biologicals
Pharmacy Inspections/staff interviews Dispensing of drugs Pharmacist responsibilities Staffing Policies and procedures Medication therapy monitoring Pharmacy USP 797 regulations Emergency medicine kits Drug storage Nursing med carts/anesthesia carts Outdated drugs Survey of pharmacy Reporting adverse drug reactions (ADR) and
medication errors Near misses/good catches High alert medication Definition of medication error required Trigger/indicator drugs Monitoring medication errors Medication alerts Beers list (developed by Dr. Mark Beers) Do not use abbreviations Sound alike/look alike drugs Non-punitive policies
Infection Control Investigating and controlling infections’ Healthcare associated infections Policies Orientation for new employees Role of leaders Infection control officer
Dietary and Nutrition Policies Dietary compliance Qualified dietician Support staff Direct services
Outpatient Services Outpatient director
Rehab – removed in 2013LaboratoryRadiology Staff Scope of services Policies required
Regulations and Interpretive Guidelines Emergency procedures Contracted services Nursing care Observation of med passes/nursing care Changes in observation guidelines Nursing care plans RN for each patient RN supervising care Drugs and IVs Verbal orders Verbal order policy Culture of questioning Medication passes
Objectives:At the completion of this program, the participants will be able to:1. Explain the responsibilities of the pharmacists that include developing, supervising, and
coordinating activities of the pharmacy.2. Discuss the staff and physician responsibilities for infection control, dietary, outpatient services,
rehab, lab, and radiology.3. List the required polices for infection control, dietary, outpatient services, rehab, lab, and
radiology.

PART 3Program Topics:Medical Records Standards Identification of author Access to medical records Inpatient and outpatient requirements Records system Informed consent Procedures required for consent Medical necessity and the RACs History and physicals Discharge summaries Preventing unnecessary readmissions Response to treatment Confidentiality Retention Protection of record information
Surgical Services Policies required PACU OR register Operative report Surveyor in the OR Surgical privileges Designation of qualified practitioners
Anesthesia Services Anesthetic risk and evaluation Administration of anesthesia Pre- and post-anesthesia evaluation Discharge PI required Healthcare-associated infections State exemption of CRNAs Periodic evaluation
Organ, Tissue and Eye Procurement Definition of imminent death Tissue and eye bank Family notification Organ donation
Special Requirements for CAH Providers ofLong-Term Care Services (Swing beds) Eligibility Payment SNF services Resident rights Notice of rights and services Free choice Privacy and confidentiality Access and visitation rights Personal property Married couples Admission, transfer and discharge rights Transfer and discharge Payment of care Content of notice Resident behavior and facility practices Restraints Staff treatment of residents Hiring of employees Activities Social services Resident assessment Comprehensive care plans Discharge summary Nutrition Provision of services
Objectives:At the completion of this program, the participants will be able to:1. Explain the informed consent elements required by CMS.2. Describe the requirements for history and physicals for CAHs.3. List what must be contained in the operative report.4. Discuss what CAHs must do to comply with the requirements for notification of the organ
procurement (OPO) agency when a patient expires.5. Name some of the patient rights that are afforded to patients in swing beds.

Registration:There is a site fee of $175.00 for NDHA Member Hospitals and $300.00 for Non-members per
session for this course. NDHA member fee to attend all 3 sessions: $450.00 (a savings of$75.00). Member Hospital refers to an individual freestanding facility, not a hospital system. Theregistration fee provides you with one phone number, Web connection and a downloadablehandout. Numerous people at one physical site are encouraged to participate in the WebConference through one registration (utilizing the same telephone/Web connection). If anyadditional locations or facilities are added into your connection, additional registration fees will becharged. If participants at your site require more than one telephone/Web connection, additionalregistration fees will be charged.
Prior to the program you will receive an e-mail containing instructions on how to connect to theconference. This e-mail will also contain codes to access the conference call. Advanceregistration by August 29, 2013 is required to ensure delivery of instructional materials. A late feeof $25.00 will be charged for any registrations after this date. This fee is necessary, as we arebeing charged a late fee for any last minute registrations that require an overflow line on thebridge. If you do not receive an e-mail from Linda Simmons prior to the program with yourhandouts and dial-in information, please contact her at 701 224-9732.
Please contact Linda Simmons at 701 224-9732 or [email protected] for further information.You may register by fax (701) 224-9529, online at http://www.ndha.org under Education or by mailPO Box 7340, Bismarck ND 58507.
Registration fees are non-refundable unless notice of an individual’s cancellation is received atNDHA five working days prior to the event, in which case a cancellation fee of $50.00 will bededucted from your registration fee. If notice of cancellation is received after this date, there is norefund. You will be billed whether or not you attend the program.
Part I: September 12, 2013 CAH CoPs Part 1 ______
Part II: September 19, 2013 CAH CoPs Part 2 ______
Part III: September 26, 2013 CAH CoPs Part 3 ______
NDHA Members – attend all three sessions for $450.00 (a savings of $75.00)
Facility_____________________________________________________________________
Contact Name/Title ___________________________________________________________
E-Mail _____________________________________________________________________
Phone Number ______________________________________________________________

July 25, 2013
CMS Proposals for the Physician Quality Reporting System (PQRS) and Physician
Value-Based Payment Modifier (VM) under the Medicare Physician Fee Schedule 2014

www.cms.gov/NPC 2
• This MLN Connects™ National Provider Call (MLN Connects Call) is part of the Medicare Learning Network® (MLN), a registered trademark of the Centers for Medicare & Medicaid Services (CMS), and is the brand name for official information health care professionals can trust.
Medicare Learning Network®
www.cms.gov/NPC 3
This presentation was current at the time it was published or uploaded onto the web. Medicare policy changes frequently so links to the source documents have been provided within the document for your reference.
This presentation was prepared as a service to the public and is not intended to grant rights or impose obligations. This presentation may contain references or links to statutes, regulations, or other policy materials. The information provided is only intended to be a general summary. It is not intended to take the place of either the written law or regulations. We encourage readers to review the specific statutes, regulations, and other interpretive materials for a full and accurate statement of their contents.
Disclaimer

4 www.cms.gov/NPC
• Physician Fee Schedule (PFS) Proposed Rule – PQRS
• Changes to Individual Reporting Requirements • Changes to the Group Practice Reporting Option (GPRO) • Additional Program Changes
– Medicare Electronic Health Record (EHR) Incentive Program
– Physician Compare – Physician Value-Based Payment Modifier
• Application of the Value Modifier (VM) • VM and PQRS
Agenda

5 www.cms.gov/NPC
PQRS PROPOSALS RELATED TO REPORTING AS AN INDIVIDUAL
ELIGIBLE PROFESSIONAL (EP)

6 www.cms.gov/NPC
Proposed definition of a “qualified clinical data registry”: A CMS-approved entity (such as a registry, certification board, collaborative, etc.) that collects medical and/or clinical data for the purpose of patient and disease tracking to foster improvement in the quality of care furnished to patients. • Must be able to submit quality measures data or results to CMS for purposes of
demonstrating that, for a reporting period, its EPs have satisfactorily participated in PQRS
• Must submit quality measures data on multiple payers • Must provide timely feedback at least quarterly on the measures for which the
qualified clinical data registry would report on the individual EP’s behalf for purposes of the EP meeting the criteria for satisfactory participation under PQRS
• Must possess a method to benchmark the quality of care measures an EP provides with that of other EPs performing the same or similar functions
Qualified Clinical Data Registries

7 www.cms.gov/NPC
Proposals on how to become a qualified clinical data registry: • Meet minimum proposed characteristics • Self-nomination
– Deadline: January 31 – Submission method: Email
Qualified Clinical Data Registries (cont.)

www.cms.gov/NPC 8
Summary of Major Proposed Changes: • Measures group reporting only available via registry • For reporting individual measures via registry, propose a 50%
threshold • Increase the number of generally required measures to be reported
from 3 to 9 measures, covering at least 3 domains – Patient Safety – Person and Caregiver-Centered Experience and Outcomes – Communication and Care Coordination – Effective Clinical Care – Community/Population Health – Efficiency and Cost Reduction
2014 PQRS Incentive – Individual EPs

www.cms.gov/NPC 9
*Subject to Measure Applicability Validation (MAV)
Note: Additional reporting options were finalized in the 2013 PFS Final Rule
2014 Reporting Period
Measure Type Reporting Mechanism
Proposed Reporting Criteria
12-month (Jan 1 - Dec 31)
Individual Measures * Claims Report at least 9 measures covering at least 3 of the National Quality Strategy domains; OR If less than 9 measures apply to the EP, then the EP must report 1-8 measures for which there is Medicare patient data; AND Report each measure for at least 50% of the Medicare Part B FFS patients seen during the reporting period to which the measure applies.
12-month (Jan 1 - Dec 31)
Individual Measures Qualified Registry
Report at least 9 measures, covering at least 3 of the National Quality Strategy domains, AND Report each measure for at least 50% of the EP’s Medicare Part B FFS patients seen during the reporting period to which the measure applies.
12-month (Jan 1 - Dec 31)
Measures selected by Qualified Clinical Data Registry
Qualified Clinical Data Registry
Report at least 9 measures available for reporting under a qualified clinical data registry covering at least 3 of the National Quality Strategy domains, AND Report each measure for at least 50% of the EP’s patients. Of the measures reported via a clinical data registry, the EP must report on at least 1 outcome measure.
Proposed Changes to Criteria for Satisfactory Reporting/Participation
2014 PQRS Incentive – Individual EPs (cont.)

www.cms.gov/NPC 10
*Subject to Measure Applicability Validation (MAV)
Note: Additional reporting options were finalized in the 2013 PFS Final Rule
2014 Reporting Period
Measure Type Reporting Mechanism
Proposed Reporting Criteria
12-month (Jan 1 - Dec 31)
Individual Measures * Claims Report at least 9 measures covering at least 3 of the National Quality Strategy domains; OR If less than 9 measures apply to the EP, then the EP must report 1-8 measures for which there is Medicare patient data; AND Report each measure for at least 50% of the Medicare Part B FFS patients seen during the reporting period to which the measure applies. Measures with a 0% performance rate would not be counted.
12-month (Jan 1 - Dec 31)
Individual Measures Qualified Registry
Report at least 9 measures, covering at least 3 of the National Quality Strategy domains, AND Report each measure for at least 50% of the EP’s Medicare Part B FFS patients seen during the reporting period to which the measure applies. Measures with a 0% performance rate would not be counted.
12-month (Jan 1 - Dec 31)
Measures selected by Qualified Clinical Data Registry
Qualified Clinical Data Registry
Report at least 9 measures available for reporting under a qualified clinical data registry covering at least 3 of the National Quality Strategy domains; AND Report each measure for at least 50% of the EP’s patients. Of the measures reported via a clinical data registry, the EP must report on at least 1 outcome measure.
Proposed Changes to Criteria for Avoiding the 2016 PQRS Payment Adjustment
2016 PQRS Payment Adjustment – Individual EPs

12 www.cms.gov/NPC
Summary of Major Proposed Changes: • Eliminate the option for group practices of 25-99 to report PQRS measures
via the GPRO web interface • For reporting individual measures via registry, propose a 50% threshold,
which is also proposed for the individual satisfactory reporting criteria for the 2014 PQRS incentive
• Groups of 25 or more EPs will have the option to report the Clinician Group Consumer Assessment of Healthcare Providers and Systems (CG CAHPS)
• Group practices in the GPRO (including ACOs in the Medicare Shared Savings Program) must meet the criteria for the 2014 PQRS incentive to satisfactorily report to avoid the 2016 PQRS payment adjustment
• Registration: – New Proposed Deadline: September 30 – Same website where quality tiering is elected – If the group practice wishes to report the CG CAHPS, the group would be
required to indicate its intent to do so at self-nomination
Proposed Changes to the PQRS GPRO

13 www.cms.gov/NPC
Reporting the CG CAHPS Survey for group practices comprised of 25+ EPs: • 12 Survey Questions:
– Getting Timely Care, Appointments, and Information – How Well Providers Communicate – Patient’s Rating of Provider – Access to Specialists – Health Promotion & Education – Shared Decision Making – Health Status/Functional Status – Courteous and Helpful Office Staff – Care Coordination – Between Visit Communication – Helping Your to Take Medication as Directed, and – Stewardship of Patient Resources
• Must use a CMS-certified survey vendor • Please note that CMS will not bear the cost of administering the CG CAHPS survey
Proposed Changes to the PQRS GPRO (cont.)
14 www.cms.gov/NPC
Note: Additional reporting options were finalized in the 2013 PFS Final Rule
2014 Reporting Period
Reporting Mechanism Group Practice Size
Proposed Reporting Criteria
12-month (Jan 1 - Dec 31)
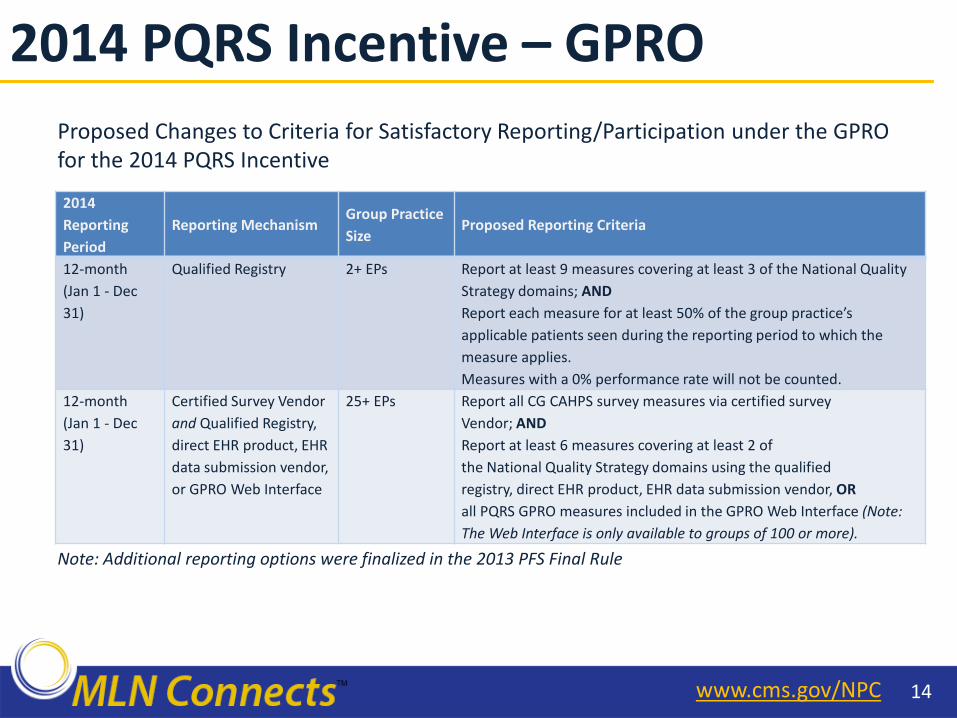
Qualified Registry 2+ EPs Report at least 9 measures covering at least 3 of the National Quality Strategy domains; AND Report each measure for at least 50% of the group practice’s applicable patients seen during the reporting period to which the measure applies. Measures with a 0% performance rate will not be counted.
12-month (Jan 1 - Dec 31)
Certified Survey Vendor and Qualified Registry, direct EHR product, EHR data submission vendor, or GPRO Web Interface
25+ EPs Report all CG CAHPS survey measures via certified survey Vendor; AND Report at least 6 measures covering at least 2 of the National Quality Strategy domains using the qualified registry, direct EHR product, EHR data submission vendor, OR all PQRS GPRO measures included in the GPRO Web Interface (Note: The Web Interface is only available to groups of 100 or more).
Proposed Changes to Criteria for Satisfactory Reporting/Participation under the GPRO for the 2014 PQRS Incentive
2014 PQRS Incentive – GPRO

15 www.cms.gov/NPC
Note: Additional reporting options were finalized in the 2013 PFS Final Rule
2014 Reporting Period
Reporting Mechanism Group Practice Size
Proposed Reporting Criteria
12-month (Jan 1 - Dec 31)
Qualified Registry 2+ EPs Report at least 9 measures covering at least 3 of the National Quality Strategy domains; AND Report each measure for at least 50% of the group practice’s applicable patients seen during the reporting period to which the measure applies. Measures with a 0% performance rate will not be counted.
12-month (Jan 1 - Dec 31)
Certified Survey Vendor and Qualified Registry, direct EHR product, EHR data submission vendor, or GPRO Web Interface
25+ EPs Report all CG CAHPS survey measures via certified survey Vendor; AND Report at least 6 measures covering at least 2 of the National Quality Strategy domains using the qualified registry, direct EHR product, EHR data submission vendor, OR all PQRS GPRO measures included in the GPRO Web Interface (Note: The Web Interface is only available to groups of 100 or more).
Proposed Changes to Criteria for Avoiding the 2016 PQRS Payment Adjustment Under the GPRO
2016 PQRS Payment Adjustment – GPRO
17 www.cms.gov/NPC
Summary of Proposed PQRS Measures • For 2014, we are proposing to add 47 new individual measures and
4 measures groups to fill existing measure gaps and retire a number of claims-based measures to encourage reporting via the registry and EHR-based reporting mechanisms
• Proposed deletion of 46 measures • Proposed addition of recommended core measures that align with
the EHR Incentive Program recommended core measures • Measures Groups:
– Proposed change to define a measures group as consisting of 6 or more measures
– 4 new measures groups: Total Knee Replacement, Optimizing Patient Exposure to Ionizing Radiation, General Surgery, and Gastrointestinal Surgery
Proposals Related to PQRS Measures

18 www.cms.gov/NPC
PQRS# NQF Measure Title 6 0067 Coronary Artery Disease (CAD): Antiplatelet Therapy 9 0105 Major Depressive Disorder (MDD): Antidepressant Medication During Acute Phase for Patients with MDD
39 0046 Screening or Therapy for Osteoporosis for Women Aged 65 Years and Older 47 0326 Advance Care Plan 48 0098 Urinary Incontinence: Assessment of Presence or Absence of Urinary Incontinence in Women Aged 65 Years and Older 53 0047 Asthma: Pharmacologic Therapy for Persistent Asthma - Ambulatory Care Setting 64 0001 Asthma: Assessment of Asthma Control – Ambulatory Care Setting 65 0069 Appropriate Treatment for Children with Upper Respiratory Infection (URI) 66 0002 Appropriate Testing for Children with Pharyngitis 84 0395 Hepatitis C: Ribonucleic Acid (RNA) Testing Before Initiating Treatment 85 0396 Hepatitis C: HCV Genotype Testing Prior to Treatment 87 0398 Hepatitis C: HCV Ribonucleic Acid (RNA) Testing at Week 12 of Treatment
107 0104 Major Depressive Disorder (MDD): Suicide Risk Assessment 116 0058 Antibiotic Treatment for Adults with Acute Bronchitis: Avoidance of Inappropriate Use 126 0417 Diabetes Mellitus: Diabetic Foot and Ankle Care, Peripheral Neuropathy – Neurological Evaluation 127 0416 Diabetes Mellitus: Diabetic Foot and Ankle Care, Ulcer Prevention – Evaluation of Footwear 130 0419 Documentation of Current Medications in the Medical Record 148 0322 Back Pain: Initial Visit 149 0319 Back Pain: Physical Exam 150 0314 Back Pain: Advice for Normal Activities 151 0313 Back Pain: Advice Against Bed Rest 176 AQA Adopted Rheumatoid Arthritis (RA): Tuberculosis Screening 177 AQA Adopted Rheumatoid Arthritis (RA): Periodic Assessment of Disease Activity 178 AQA Adopted Rheumatoid Arthritis (RA): Functional Status Assessment 179 AQA Adopted Rheumatoid Arthritis (RA): Assessment and Classification of Disease Prognosis 180 AQA Adopted Rheumatoid Arthritis (RA): Glucocorticoid Management 183 0399 Hepatitis C: Hepatitis A Vaccination in Patients with HCV 197 0074 Coronary Artery Disease (CAD): Lipid Control
2014 PQRS Measures with Reporting Method Update

19 www.cms.gov/NPC
Proposed Requirements for Measures Reported by Qualified Clinical Data Registries on behalf of Participating EPs: • The qualified clinical data registry must have at least 9 measures, covering at least 3 of the 6
National Quality Strategy domains, available for reporting.
• The qualified clinical data registry must have at least 1 outcome measure available for reporting, which is a measure that assesses the results of health care that are experienced by patients (that is, patients’ clinical events; patients’ recovery and health status; patients’ experiences in the health system; and efficiency/cost).
• The qualified clinical data registry may report on process measures, which are measures that focus on a process which leads to a certain outcome, meaning that a scientific basis exists for believing that the process, when executed well, will increase the probability of achieving a desired outcome.
• The outcome and process measures reported must contain denominator data. That is, the lower portion of a fraction used to calculate a rate, proportion, or ratio. The denominator must describe the population eligible (or episodes of care) to be evaluated by the measure. This should indicate age, condition, setting, and timeframe (when applicable). For example, “Patients aged 18 through 75 years with a diagnosis of diabetes.”
Measures Reported by Qualified Clinical Data Registries
20 www.cms.gov/NPC
Proposed Requirements for Measures Reported by Qualified Clinical Data Registries on behalf of Participating EPs: • The outcome and process measures reported must contain numerator data. That is, the upper portion of
a fraction used to calculate a rate, proportion, or ratio. The numerator must detail the quality clinical action expected that satisfies the condition(s) and is the focus of the measurement for each patient, procedure, or other unit of measurement established by the denominator (that is, patients who received a particular service or providers that completed a specific outcome/process).
• The qualified clinical data registry must provide denominator exceptions for the measures. That is, those conditions that should remove a patient, procedure or unit of measurement from the denominator of the performance rate only if the numerator criteria are not met. Denominator exceptions allow for adjustment of the calculated score for those providers with higher risk populations. Denominator exceptions allow for the exercise of clinical judgment and should be specifically defined where capturing the information in a structured manner fits the clinical workflow. Generic denominator exception reasons used in measures fall into three general categories: Medical, Patient, or System reasons.
• The qualified clinical data registry must provide denominator exclusions for the measures for which it will report to CMS. That is, those patients with conditions who should be removed from the measure population and denominator before determining if numerator criteria are met. (For example, Patients with bilateral lower extremity amputations would be listed as a denominator exclusion for a measure requiring foot exams.)
• The qualified clinical data registry must provide to CMS descriptions for the measures for which it will report to CMS by no later than March 31, 2014. The descriptions must include: name/title of measures, NQF # (if NQF endorsed), descriptions of the denominator, numerator, denominator exceptions and denominator exclusions of the measure.
Measures Reported by Qualified Clinical Data Registries (cont.)

21 www.cms.gov/NPC
• Future PQRS Reporting Periods • Plan for the Future of the PQRS GPRO • Future of Use of the Claims-based Reporting Mechanism in
PQRS • Future Submission Timelines for the Registry, EHR, GPRO Web
Interface and Qualified Clinical Data Registry Reporting Mechanisms
• Integration of Clinical Quality Measures Reported Under the Hospital Inpatient Quality Reporting (IQR) Program
• Feedback Reports
2017 PQRS Payment Adjustment and Beyond

22 www.cms.gov/NPC
2014 MEDICARE ELECTRONIC HEALTH RECORD (EHR) INCENTIVE PROGRAM

23 www.cms.gov/NPC
EHR Incentive Program CQM Reporting Using Clinical Data Registries: • The EHR Incentive Program is statutorily required to use Certified EHR Technology (CEHRT) as
a reporting requirement. The 2014 Edition certification criteria require certification of each individual electronic clinical quality measure (eCQM) that will be reported to CMS. We propose to allow CQM submission using clinical data registries, such as those established for PQRS, as long as the eCQMs are included in the Stage 2 final rule and use the same electronic specifications established for meaningful use (MU).
Comprehensive Primary Care Initiative – Proposed Additional Group Reporting Option: • The Comprehensive Primary Care Initiative (CPC), under the authority of Section 3021 of the
Affordable Care Act, is a multi-payer initiative fostering collaboration between public and private health care payers to strengthen primary care. The CPC program is already aligned with MU on the eCQMs finalized in the Stage 2 final rule. In a continuing effort to align quality reporting programs and innovation programs, we are proposing to add a group reporting option beginning in CY 2014 for EPs who are part of a CPC site that successfully submit according to their region’s CPC reporting requirements to also fulfill the CQM requirement for MU.
EHR Incentive Program

24 www.cms.gov/NPC
eCQM Reporting – Measure Versions: • Electronic reporting of eCQMs must use the most recent version of the measure (i.e., June
2013 release). In order to use any of the aligned options with MU, EPs must electronically report their CQMs. If the EP is not able to report the most recent version of the measure, then the CQM results must be submitted via attestation in the Registration & Attestation System. Attested data cannot be used for credit in any other quality reporting programs.
EHR Incentive Program (cont.)
26 www.cms.gov/NPC
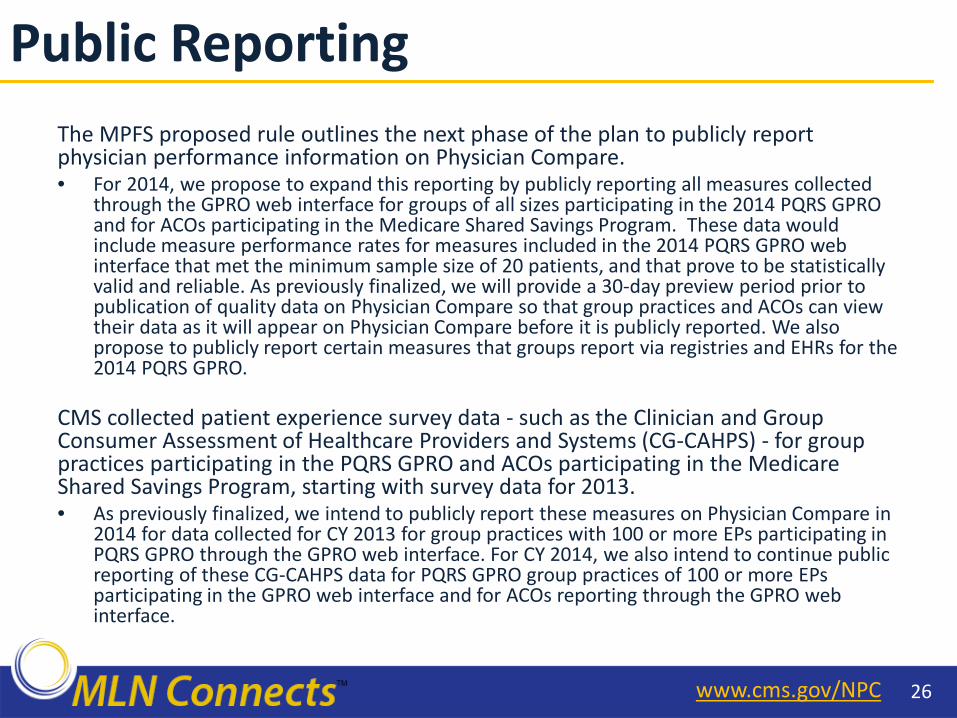
The MPFS proposed rule outlines the next phase of the plan to publicly report physician performance information on Physician Compare. • For 2014, we propose to expand this reporting by publicly reporting all measures collected
through the GPRO web interface for groups of all sizes participating in the 2014 PQRS GPRO and for ACOs participating in the Medicare Shared Savings Program. These data would include measure performance rates for measures included in the 2014 PQRS GPRO web interface that met the minimum sample size of 20 patients, and that prove to be statistically valid and reliable. As previously finalized, we will provide a 30-day preview period prior to publication of quality data on Physician Compare so that group practices and ACOs can view their data as it will appear on Physician Compare before it is publicly reported. We also propose to publicly report certain measures that groups report via registries and EHRs for the 2014 PQRS GPRO.
CMS collected patient experience survey data - such as the Clinician and Group Consumer Assessment of Healthcare Providers and Systems (CG-CAHPS) - for group practices participating in the PQRS GPRO and ACOs participating in the Medicare Shared Savings Program, starting with survey data for 2013. • As previously finalized, we intend to publicly report these measures on Physician Compare in
2014 for data collected for CY 2013 for group practices with 100 or more EPs participating in PQRS GPRO through the GPRO web interface. For CY 2014, we also intend to continue public reporting of these CG-CAHPS data for PQRS GPRO group practices of 100 or more EPs participating in the GPRO web interface and for ACOs reporting through the GPRO web interface.
Public Reporting

28 www.cms.gov/NPC
• VM assesses both quality of care furnished and the cost of that care under the Medicare Physician Fee Schedule
• Begin phase-in of VM in 2015, phase-in complete by 2017
• Implementation of the VM is based on participation in PQRS
• For CY 2015, we will apply the VM to groups of physicians with 100 or more EPs (EPs)
What is the Value-Based Modifier?

29 www.cms.gov/NPC
Value Modifier Components
2015 Finalized Policies
2016 Proposed Policies
Performance Year 2013 2014
Group Size 100+ 10+
Available Quality Reporting Mechanisms
GPRO-Web Interface, CMS Qualified Registries, Administrative Claims
GPRO-Web Interface, CMS Qualified Registries, EHRs, and 70% of EPs reporting individually
Outcome Measures
All Cause Readmission Composite of Acute Prevention Quality Indicators: (bacterial pneumonia, urinary tract infection, dehydration)
Composite of Chronic Prevention Quality Indicators: (chronic obstructive pulmonary disease (COPD), heart failure, diabetes)
Same as 2015
Patient Experience of Care Measures
N/A PQRS CAHPS: Option for groups of 25+ EPs
Value Modifier: 2015 Policies & 2016 Proposals
30 www.cms.gov/NPC
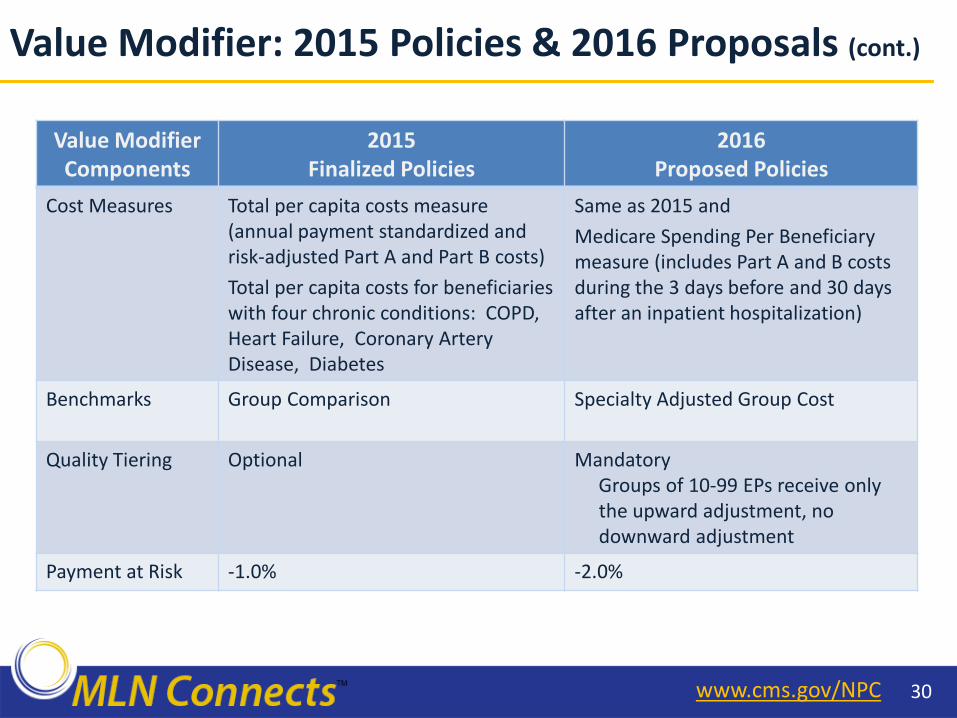
Value Modifier Components
2015 Finalized Policies
2016 Proposed Policies
Cost Measures Total per capita costs measure (annual payment standardized and risk-adjusted Part A and Part B costs) Total per capita costs for beneficiaries with four chronic conditions: COPD, Heart Failure, Coronary Artery Disease, Diabetes
Same as 2015 and Medicare Spending Per Beneficiary measure (includes Part A and B costs during the 3 days before and 30 days after an inpatient hospitalization)
Benchmarks Group Comparison
Specialty Adjusted Group Cost
Quality Tiering Optional Mandatory Groups of 10-99 EPs receive only
the upward adjustment, no downward adjustment
Payment at Risk -1.0% -2.0%
Value Modifier: 2015 Policies & 2016 Proposals (cont.)

32 www.cms.gov/NPC
PQRS Reporting Mechanism
Type of Measure
1. GPRO Web interface Measures focus on preventive care and care for chronic diseases (aligns with the Shared Savings Program)
2. GPRO using CMS-qualified registries
Groups select the quality measures that they will report through a PQRS-qualified registry.
3. GPRO using EHR Quality measures data extracted from a qualified EHR product for a subset of proposed 2014 Physician Quality Reporting System quality measures.
Groups with 10+ EPs may select one of the following PQRS GPRO quality reporting mechanisms and meet the criteria for the CY 2016 PQRS payment adjustment to avoid the 2.0% VM adjustment.
Reporting Quality Data at the Group Level for the VBM
33 www.cms.gov/NPC
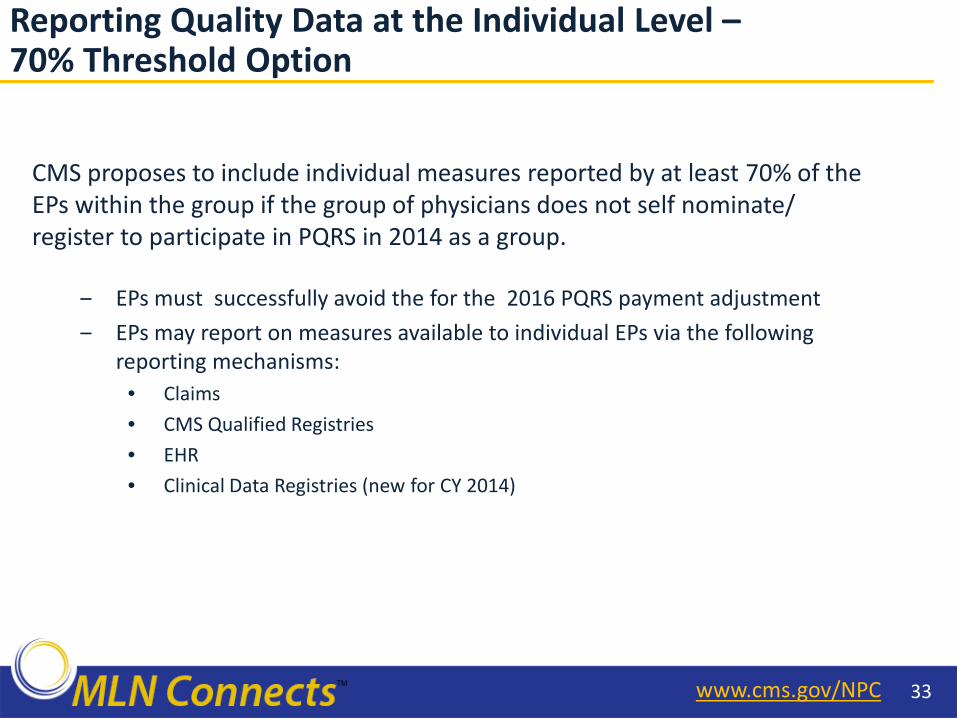
CMS proposes to include individual measures reported by at least 70% of the EPs within the group if the group of physicians does not self nominate/ register to participate in PQRS in 2014 as a group.
‒ EPs must successfully avoid the for the 2016 PQRS payment adjustment ‒ EPs may report on measures available to individual EPs via the following
reporting mechanisms: • Claims • CMS Qualified Registries • EHR • Clinical Data Registries (new for CY 2014)
Reporting Quality Data at the Individual Level – 70% Threshold Option
34 www.cms.gov/NPC
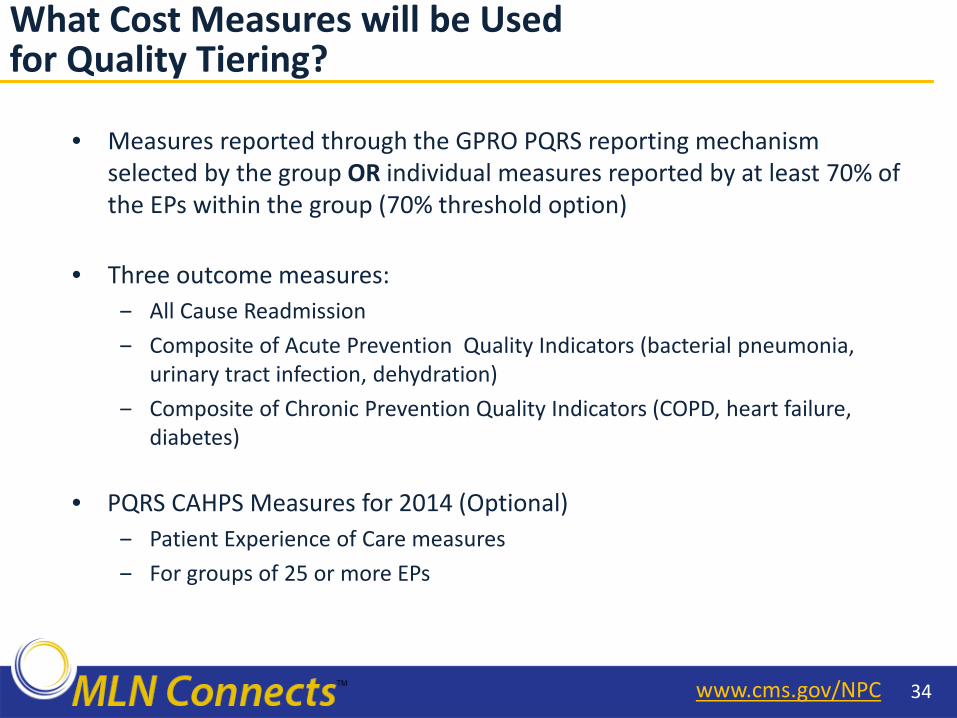
• Measures reported through the GPRO PQRS reporting mechanism selected by the group OR individual measures reported by at least 70% of the EPs within the group (70% threshold option)
• Three outcome measures: ‒ All Cause Readmission ‒ Composite of Acute Prevention Quality Indicators (bacterial pneumonia,
urinary tract infection, dehydration) ‒ Composite of Chronic Prevention Quality Indicators (COPD, heart failure,
diabetes)
• PQRS CAHPS Measures for 2014 (Optional) ‒ Patient Experience of Care measures ‒ For groups of 25 or more EPs
What Cost Measures will be Used for Quality Tiering?

35 www.cms.gov/NPC
• Total per capita costs measures (Parts A & B)
• Total per capita costs for beneficiaries with 4 chronic conditions: ‒ Chronic Obstructive Pulmonary Disease (COPD) ‒ Heart Failure ‒ Coronary Artery Disease ‒ Diabetes
• Medicare Spending Per Beneficiary measure (3 days prior and 30 days after an inpatient hospitalization) attributed to all groups providing a Part B service during hospitalization
• All cost measures are payment standardized and risk adjusted
• Each group’s cost measures adjusted for specialty mix of the EPs in the group
What Quality Measures will be Used for Quality Tiering?

36 www.cms.gov/NPC
Use domains to combine each quality measure into a quality composite and each cost measure into a cost composite
Quality Tiering Methodology

37 www.cms.gov/NPC
*Eligible for an additional +1.0x if reporting clinical data for quality measures and average beneficiary risk score in the top 25 percent of all beneficiary risk scores.
Quality/cost Low cost Average cost High cost
High quality +2.0x* +1.0x* +0.0%
Medium quality +1.0x* +0.0% -1.0%
Low quality +0.0% -1.0% -2.0%
• Each group receives two composite scores (quality of care; cost of care), based on the group’s standardized performance (e.g. how far away from the national mean).
• This approach identifies statistically significant outliers and assigns them to their respective cost and quality tiers.
Quality Tiering Approach

38 www.cms.gov/NPC
Timeline for VM that Applies to Payment Starting January 1, 2016

39 www.cms.gov/NPC
• Choose a PQRS Reporting Mechanism ‒ Web interface ‒ Qualified registry ‒ EHRs, OR ‒ Utilize the 70% option (70% of EPs in group must meet the criteria
for the CY 2016 PQRS payment adjustment)
• If group selects GPRO reporting mechanism, group must self-nominate/register (May 2014 – September 2014); no need to self-nominate or register for the 70% option
• Meet the satisfactory reporting criteria to avoid the CY 2016 payment adjustment for selected PQRS reporting mechanisms
Actions for Groups of 10+ EPs for the 2016 VM
40 www.cms.gov/NPC
• September 2013: Quality and Resource Use Reports for Groups of 25 or more EPs 2012 – Drill down table including beneficiaries attributed to the
group, their resource use, specific chronic diseases – Drill down table including all hospitalizations for attributed
beneficiaries – Drill down table of individual EP PQRS reporting
(December 2013)
• Late Summer 2014: QRURs for all Groups and Solo Practitioners
Physician Feedback Reports
42 www.cms.gov/NPC
• You may submit comments in one of four ways (please choose only one): – Electronically. You may submit electronic comments on this regulation to
http://www.regulations.gov. Follow the instructions for "submitting a comment.“ – By regular mail. You may mail written comments to the following address ONLY: Centers
for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1590-P, P.O. Box 8013, Baltimore, MD 21244-8013. Please allow sufficient time for mailed comments to be received before the close of the comment period.
– By express or overnight mail. You may send written comments to the following address ONLY: Centers for Medicare & Medicaid Services, Department of Health and Human Services, Attention: CMS-1590-P, Mail Stop C4-26-05, 7500 Security Boulevard, Baltimore, MD 21244-1850.
– By hand or courier. If you prefer, you may deliver (by hand or courier) your written comments before the close of the comment period to either of the following addresses:
• For delivery in Washington, DC -- CMS-1590-P, Centers for Medicare & Medicaid Services, Department of Health and Human Services, Room 445-G, Hubert H. Humphrey Building, 200 Independence Avenue, SW., Washington, DC 20201
• For delivery in Baltimore, MD -- Centers for Medicare & Medicaid Services, Department of Health and Human Services, 7500 Security Boulevard, Baltimore, MD 21244-1850
Comments mailed to the addresses indicated as appropriate for hand or courier delivery may be delayed and received after the comment period
How to Submit Comments on Proposals to the CY 2014 PFS Proposed Rule

43 www.cms.gov/NPC
• QualityNet Help Desk: – Portal password issues – PQRS/eRx feedback report availability and access – IACS registration questions – IACS login issues – PQRS and eRx Incentive Program questions
866-288-8912 (TTY 877-715-6222)
7:00 a.m.–7:00 p.m. CST M-F or [email protected] You will be asked to provide basic information such as
name, practice, address, phone, and e-mail
• Provider Contact Center: – Questions on status of 2012 PQRS/eRx Incentive Program incentive payment (during
distribution timeframe) – See Contact Center Directory at
http://www.cms.gov/MLNProducts/Downloads/CallCenterTollNumDirectory.zip
• EHR Incentive Program Information Center: 888-734-6433 (TTY 888-734-6563)
Where to Call for Help

44 www.cms.gov/NPC
• PFS Federal Regulation Notices http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/PhysicianFeeSched/PFS-Federal-Regulation-Notices.html
• CMS PQRS Website http://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/PQRS
• Medicare Shared Savings Program http://cms.gov/Medicare/Medicare-Fee-for-Service-
Payment/sharedsavingsprogram/Quality_Measures_Standards.html
• CMS Value-based Payment Modifier (VM) Website http://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/
PhysicianFeedbackProgram/ValueBasedPaymentModifier.html
• Medicare and Medicaid EHR Incentive Programs http://www.cms.gov/Regulations-and-Guidance/Legislation/ EHRIncentivePrograms
• Frequently Asked Questions (FAQs) https://questions.cms.gov/
• Physician Compare
http://www.medicare.gov/physiciancompare/search.html
Resources

45 www.cms.gov/NPC
Attention: Medicare-Enrolled Providers and Suppliers • Give CMS feedback about your experience with your Medicare
Administrative Contractor (MAC), the contractor that processes your Medicare claims
• Your feedback will help CMS monitor performance trends, improve
oversight, and increase efficiency of the Medicare program • Only providers and suppliers who register for the MSI will be
included in the random sample to rate their MAC • For more information and to register today for the 2013 MSI, go to
http://www.cms.gov/Medicare/Medicare-Contracting/MI/
Coming in Late Summer 2013 – The Medicare Administrative Contractor Satisfaction Indicator (MSI)

47 www.cms.gov/NPC
• Please help us continue to improve the MLN Connects National Provider Call Program by providing your feedback about today’s call.
• To complete the evaluation, visit http://npc.blhtech.com/ and select the title for today’s call.
• Evaluations are anonymous, confidential, and voluntary.
• All registrants will receive a reminder email about the evaluation for this call. Please disregard the email if you have already completed the evaluation.
• We appreciate your feedback.
Evaluate Your Experience
48 www.cms.gov/NPC
• For more information about the MLN Connects National Provider Call Program, please visit http://cms.gov/Outreach-and-Education/Outreach/NPC/index.html
• For more information about the Medicare Learning Network (MLN), please visit
http://cms.gov/Outreach-and-Education/Medicare-Learning-Network-MLN/MLNGenInfo/index.html
Thank You

N.D. Department of Human Services, 600 E. Boulevard Ave., Dept. 325, Bismarck, ND 58505-0250
701-328-2310, 800-472-2622, ND Relay TTY 800-366-6888 www.nd.gov/dhs
Mandatory Reporting – Community Abuse and Neglect of a Vulnerable Adult
Facilities
Congregate Care includes Assisted Living or Basic Care
Nursing Facilities also includes Swing Bed or Transitional Care Unit
Hospital
I want to report abuse, neglect, or exploitation of a:
Resident of a Nursing Facility, Basic Care, Swing Bed, or Hospital
Contact N.D. Health Department at 701-328-2352
o www.ndhealth.gov/HF/PDF_files/CNA%20Nurse%20Aide%20Abuse/Initial_Allegatio
n_of_Abuse_Form.pdf
I want to report abuse, neglect, exploitation, or financial exploitation of a:
Resident of an Assisted Living Facility
Contact local Adult Protective Services (contact information below)
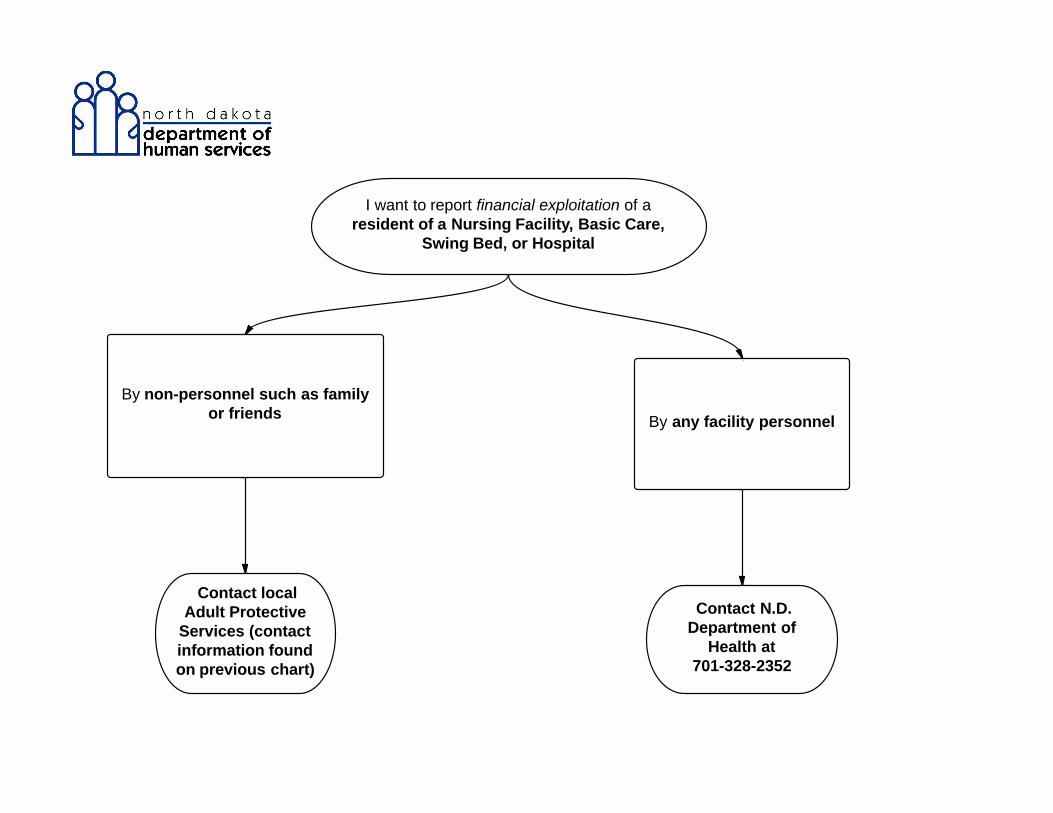
I want to report financial exploitation of a resident of a Nursing Facility, Basic Care, Swing Bed,
or Hospital by:
Non-personnel such as family or friends
Contact local Adult Protective Services (contact information below)
I want to report financial exploitation of a resident of a Nursing Facility, Basic Care, Swing Bed,
or Hospital by:
Any facility personnel
Contact N.D. Health Department at 701-328-2352 o www.ndhealth.gov/HF/PDF_files/CNA%20Nurse%20Aide%20Abuse/Initial_Allegatio
n_of_Abuse_Form.pdf

N.D. Department of Human Services, 600 E. Boulevard Ave., Dept. 325, Bismarck, ND 58505-0250
701-328-2310, 800-472-2622, ND Relay TTY 800-366-6888 www.nd.gov/dhs
Domestic Violence
I want to report domestic violence by an intimate partner (spouse, significant other, partner):
Contact a local domestic violence center
o www.ndcaws.org/resources/index.html
I want to report domestic violence by a relative caregiver including biological/adoptive, legal or
informal relationships:
Contact local Adult Protective Services (contact information below)
N.D. Protection & Advocacy Project
I want to report abuse, neglect, or exploitation of a person with a mental illness who is in:
An inpatient psychiatric ward, N.D. State Hospital, group home, geropsych unit,
transitional living facility
Contact N.D. Protection & Advocacy Project at 701-328-2950 or toll-free 800-472-2670
I want to report abuse, neglect, or exploitation of a person with a mental illness who is
receiving services from:
o Human Service Center
o Home and Community-Based Services or County Social Services
o Community Healthcare Association of the Dakotas (CHAD)
o Indian Health Services
o Public Health
o Guardianship
Contact N.D. Protection & Advocacy Project at 701-328-2950 or toll-free 800-472-2670
I want to report abuse, neglect, or exploitation of a person with a mental illness who is not
receiving services in the community:
Contact local Adult Protective Services (contact information below)
I want to report abuse, neglect, or exploitation of a person with a mental illness who is a
refugee:
Contact local Adult Protective Services (contact information below)
I want to report abuse, neglect, or exploitation of a person with developmental disabilities:
Contact N.D. Protection & Advocacy Project at 701-328-2950 or toll-free 800-472-2670

N.D. Department of Human Services, 600 E. Boulevard Ave., Dept. 325, Bismarck, ND 58505-0250
701-328-2310, 800-472-2622, ND Relay TTY 800-366-6888 www.nd.gov/dhs
Vulnerable Adult Protective Services
I want to report abuse, neglect, or exploitation of a vulnerable adult who does not fall into any of
the above categories:
Contact local Adult Protective Services (contact information below)
Contact Information
Region Contact Name Phone Toll-Free Fax E-mail
Bismarck Katie Schafer 701-328-8868 888-328-2662 701-328-8900 [email protected]
Devils Lake Kim Helten 701-665-2269 888-607-8610 701-665-2300 [email protected]
Dickinson Rene Schmidt 701-227-7582 888-227-7525 701-227-7575 [email protected]
Fargo Cass Co. Social
Services
701-241-5747
Option #3
701-239-6820
Grand Forks Bernie Hopman 701-795-3066 888-256-6742 701-795-3050 [email protected]
Jamestown Danelle Van Zinderen 701-253-6396 800-260-1310 701-253-6400 [email protected]
Minot Deb Kraft 701-857-8582 888-470-6968 701-857-8555 [email protected]
Williston Kayla Fenster 701-774-4685 800-231-7724 701-774-4620 [email protected]
If at any time you believe the adult is in immediate danger, please contact law enforcement right away.







Let’s talk about
HEALTH CARE REFORM AND ICD-10
Jamestown:Tue., Aug. 13 | 8 a.m. - 10 a.m. Jamestown Regional Medical CenterRSVP by Aug. 9
Bismarck:Wed., Aug. 14 | 8 a.m. - 9:45 a.m. Radisson Hotel Bismarck RSVP by Aug. 9
Dickinson:Tue., Aug. 20 | 1 p.m. - 3 p.m. St. Joseph’s HospitalRSVP by Aug. 16
Williston:Wed., Aug. 21 | 1 p.m. - 3 p.m. Mercy Medical CenterRSVP by Aug. 16
Rugby: Thur., Aug. 22 | 8 a.m. - 10 a.m. Heart of America Medical CenterRSVP by Aug. 16
Grand Forks:Tue., Aug. 27 | 8 a.m. - 10 a.m. Hilton Garden InnRSVP by Aug. 23
Fargo:Wed., Sep. 4 | 8 a.m. - 10 a.m. Blue Cross Blue Shield of North DakotaRSVP by Aug. 30
Join your colleagues for a FREE seminar hosted by Blue Cross Blue Shield of North Dakota.Discussion topics:
• Information about ACA
• Expansion of Medicaid
• Essential Health Benefits
• Risk Adjustment
• Accountable Care Organizations
• What is ICD-10?
• What are the benefits of ICD-10?
• As a provider, what do I need to do to prepare for ICD-10?
Aug. 27Grand Forks
Aug. 22Rugby
Aug. 21Williston
Aug. 20 Dickinson
Aug. 14Bismarck
Aug. 13Jamestown
Sep. 4Fargo
29317593 07-13
Register today! Please RSVP by email to [email protected] Indicate the location and number of people attending.
As you know, the Affordable Care Act (ACA) will influence how you care for your patients. We invite you to join us for a meaningful discussion about the impact of health care reform. We will also talk about the new ICD-10 updates and how it will affect you.




































