Upload
equality-case-files
View
226
Download
0
Embed Size (px)
Citation preview
8/3/2019 09-80173 #31
1/110
SUBMITTED UNDER THE PROCEDURES OF THEEMPLOYMENT DISPUTE RESOLUTION PLAN FOR THE
UNITED STATES COURT OF APPEALS FOR THE NINTH CIRCUIT
In re Karen Golinski et ux.No. 09-80173
DECLARATION OF DARLENE PULLEN IN SUPPORT OF KARENGOLINSKI'S REQUEST FOR BACK PAY AND ATTORNEY'S FEES
MORRISON & FOERSTER LLPJAMES R. MCGUIRE (SBN 189275)RITA F. LIN (SBN 236220)SARAH E. GRISWOLD (SBN 240326)425 Market StreetSan Francisco, California 94105-2482Telephone: 415.268.7000Facsimile: 415.268.7522Attorneys forKaren Golinski
DECLARATION OF DARLENE PULLEN ISO KAREN GOLINSKI'S REQUEST FOR BACK PAY AND Any 'S FEES5f-2793962
Case: 09-80173 01/25/2010 Page: 1 of 5 ID: 7206864 DktEntry: 31-1
8/3/2019 09-80173 #31
2/110
I, Darlene Pullen, hereby declare and state as follows:1. I submit this declaration in support ofKaren Golinski's request for an
award of back pay, pursuant to the Back Pay Act, 5 U.S.C. 5595 et seq., and theu.s. Court ofAppeals for the Ninth Circuit Employment Dispute Resolution Plan.I am an insurance broker licensed in the state ofCalifornia and employed by MikeKenney Insurance Agency. I make this declaration ofmy own personalknowledge, and if called as a witness could and would testify competently to the
matters stated herein.2. I have been an insurance broker licensed in the state ofCalifornia
since 1999. As an insurance broker, I assist clients in purchasing insurance. Thisincludes evaluating the relative health coverage offered by different healthinsurance plans with different prices.
3. I reviewed the summary of benefits for Karen Golinski's familycoverage under the Blue Cross and Blue Shield Service Benefit Plan.
4. I searched for individual health plans with coverage similar toMs. Golinski's family coverage for a woman ofMs. Golinski's spouse's and zipcode. Group plans, such as the plan under which Ms. Golinski get coverage, areset up quite differently from individual plans. It can be difficult to identifycomparable coverage.
DECLARAnON OF DARLENE PULLEN ISO KAREN GOLINSKI'S REQUEST FOR BACK PAY AND ATTY'S FEES 1sf-2793962
Case: 09-80173 01/25/2010 Page: 2 of 5 ID: 7206864 DktEntry: 31-1
8/3/2019 09-80173 #31
3/110
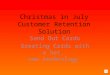
5. I identified six individual health plans that provide similar coverage tothat ofMs. Golinski's family plan. I identified these plans by comparing theannual deductible, annual out ofpocket, office visit copay(s), hospital/outpatientservices, and prescriptions to the summary of benefit for Ms. Golinski's plan.
6. These plans compare to Ms. Golinski's within reasonable range ofcopays, out-of-pocket maximum, and prescription drug coverage. The benefitstructure ofgroup to individual benefits cannot be duplicated in the individualmarketplace, but I feel these best fit those parameters, and her total annual cost formedical benefits.
7. I prepared a spreadsheet summarizing the benefits and costs ofMs. Golinski's family plan and the six similar plans for a woman of her spouse'sage and zip code for the years 2008, 2009, and 2010. A true and correct copy ofthat spreadsheet is attached hereto as Exhibit 1.
8. Ms. Golinski's plan is described in Column B ofExhibit 1, and istitled BC/BC Basic Option. Columns C through H ofExhibit 1 set forthdescriptions ofBlue Shield Balance Plan 1000, Anthem RightPlan 40Comprehensive, Anthem SmartSense 500 Full Rx, Health NetFirst Rx Plus, BlueShield Active Start 25, and Blue Shield Spectrum $750, respectively. A true andcorrect benefits summary for the Blue Shield Balance Plan 1000 is attached heretoas Exhibit 2. A true and correct copy of the summary of benefits for Anthem
DECLARATIONOF DARLENE PULLEN ISO KAREN GOLINSKI'S REQUEST FOR BACK PAY ANDATrY'S FEES 25f-2793962
Case: 09-80173 01/25/2010 Page: 3 of 5 ID: 7206864 DktEntry: 31-1
8/3/2019 09-80173 #31
4/110
01/22/2010 13:28 FAX 8054941363 }lIKE KENNEY INSURANCE l4l 005/005
RightPlan 40 Comprehensive and Anthem SmartSense 500 Full Rx is attachedhereto as Exhibit 3. A true and correct copy of the summaryof benefits for HealthNetFirst Rx Plus is attached hereto as Exhibit 4. A true and correct copy of thepolicy for the Blue ShieldActive Start 25 is attached hereto as Exhibit 5. A trueand correct copy of the summary ofbenefits for Blue Shield Spectrum $750 isattached hereto as Exhibit 6.
9. I declare under penalty ofpeIjuryunder the laws of the United StatesofAmerica that the foregoing is true and correct.
Executed t b i ~ day of January 2010, at Thousand Oaks, California.
DFI.ARATION OFDARLENE PULLEN ISO KAREN GoLINSKI'S REQUFST FOR BACK PAY ANDATTY'S FEES 3sf-2793962
Case: 09-80173 01/25/2010 Page: 4 of 5 ID: 7206864 DktEntry: 31-1
8/3/2019 09-80173 #31
5/110
1sf-2775152
CERTIFICATE OF SERVICE
I hereby certify that on January 25, 2010, I filed the foregoing with the Clerk of the
Court for the United States Court of Appeals for the Ninth Circuit:
DECLARATION OF DARLENE PULLEN IN SUPPORT OF KAREN
GOLINSKIS REQUEST FOR BACK PAY AND ATTORNEYS FEES
I further certify that I have mailed the foregoing document by U.S. mail, postage
prepaid, to the following:
Elaine Kaplan, Esq.
General Counsel
Office of Personnel Management
1900 E Street NW
Washington, D.C. 20415
Robert Loesche, Esq.
Deputy General Counsel
Administrative Office of the U.S. Courts
One Columbus Circle NE
Washington, D.C. 20544
/s/Janie Fogel
Janie Fogel
Case: 09-80173 01/25/2010 Page: 5 of 5 ID: 7206864 DktEntry: 31-1
8/3/2019 09-80173 #31
6/110
EXHIBIT 1
Case: 09-80173 01/25/2010 Page: 1 of 3 ID: 7206864 DktEntry: 31-2
8/3/2019 09-80173 #31
7/110
BLUE SHIELD ANTHEM ANTHEM HEALTH BLUE SHIELD
BC/BS BALANCE RIGHTPLAN 40 SMARTSENSE 500 NETFIRST ACTIVE
BENEFIT SUMMARY Basic Option PLAN 1000 COMPREHENSIVE FULL RX RX PLUS START 25
Annual Deductible $0 1000.00 $0 $500 $0 $0
Annual Out of Pocket Max. $5,000 $5,500 7500.00 $3,000 $7,500 $6,000
Offfice Visit Copay $20 30.00 40.00 $30/3 Visits $35 $25then 30%
Hospital Copay/ $100/day 30% after $500/day; 30% after 35% after $500 40% afterAdmissions $500 Max. deductible max $2,000 deductible per day/max. 4 day $500 admission
Out-Patient Procedures $40/day $250/visit 40% after $500; 30% after 35% after 40% afterthen 30% max 4-day deductible $500 copay $500 admission
Preventive Care $0 30.00 $40 OV; 40% 30% after $35 copay 25related services deductible
Chiropractic Care/ 50% up to 40% negotiated 30% after 35%/max 40% up to
Phys. Therapy 15 visits fee deductible $500/year 12 visits
Prescriptions $10/generic $10/generic $15/generic $15 or 40% $10/generic $10/generic$30/brand $35 after $35 after $15 or 40% $35/brand $35/brand after
50% Non-Form $500 ded. $500 ded. after $500 ded. $500 ded.
MONTHLY PREMIUMS
2010 362.00 422.00 $398.00 $382.00 $506.00
2009 307.00 317.00 $337.00 $357.00 420.00
2008 254.00 241.00 $232.00 Not Available $308.00
FEMALE, 47 YEARS OF AGE, PPO MEDICAL OPTIONS
Case: 09-80173 01/25/2010 Page: 2 of 3 ID: 7206864 DktEntry: 31-2
8/3/2019 09-80173 #31
8/110
BLUE SHIELD
SPECTRUM
$750
$750
$4,000
$35
30% after$250 admission
30% after$250 admission
$35
30% after
deductible
$10/generic$35 after$250 ded.
$681.00
$635.00
$500.00
Case: 09-80173 01/25/2010 Page: 3 of 3 ID: 7206864 DktEntry: 31-2
8/3/2019 09-80173 #31
9/110
EXHIBIT 2
Case: 09-80173 01/25/2010 Page: 1 of 5 ID: 7206864 DktEntry: 31-3
8/3/2019 09-80173 #31
10/110
Case: 09-80173 01/25/2010 Page: 2 of 5 ID: 7206864 DktEntry: 31-3
8/3/2019 09-80173 #31
11/110
Case: 09-80173 01/25/2010 Page: 3 of 5 ID: 7206864 DktEntry: 31-3
8/3/2019 09-80173 #31
12/110
Case: 09-80173 01/25/2010 Page: 4 of 5 ID: 7206864 DktEntry: 31-3
8/3/2019 09-80173 #31
13/110
Case: 09-80173 01/25/2010 Page: 5 of 5 ID: 7206864 DktEntry: 31-3
8/3/2019 09-80173 #31
14/110
EXHIBIT 3
Case: 09-80173 01/25/2010 Page: 1 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
15/110
Case: 09-80173 01/25/2010 Page: 2 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
16/110
Case: 09-80173 01/25/2010 Page: 3 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
17/110
Case: 09-80173 01/25/2010 Page: 4 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
18/110
Case: 09-80173 01/25/2010 Page: 5 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
19/110
Case: 09-80173 01/25/2010 Page: 6 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
20/110
Case: 09-80173 01/25/2010 Page: 7 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
21/110
Case: 09-80173 01/25/2010 Page: 8 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
22/110
Case: 09-80173 01/25/2010 Page: 9 of 9 ID: 7206864 DktEntry: 31-4
8/3/2019 09-80173 #31
23/110
EXHIBIT 4
Case: 09-80173 01/25/2010 Page: 1 of 3 ID: 7206864 DktEntry: 31-5
8/3/2019 09-80173 #31
24/110
Case: 09-80173 01/25/2010 Page: 2 of 3 ID: 7206864 DktEntry: 31-5
8/3/2019 09-80173 #31
25/110
Case: 09-80173 01/25/2010 Page: 3 of 3 ID: 7206864 DktEntry: 31-5
8/3/2019 09-80173 #31
26/110
EXHIBIT 5
Case: 09-80173 01/25/2010 Page: 1 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
27/110
Active Start Plan 25Policy for Individuals
This Policy is issued by Blue Shield of California Life & Health Insurance Company ("Blue Shield Life"), to the Insuredwhose identification cards are issued with this Policy. In consideration of statements made in the application and timely pay-ment of Premiums, Blue Shield Life agrees to provide the benefits of this Policy.
NOTICE TO NEW SUBSCRIBERS
Please read this Policy carefully. If you have questions, contact Blue Shield Life. You may surrender this Policy by deliver-
ing or mailing it with the Identification Cards, within ten (10) days from the date it is received by you, to BLUE SHIELDLIFE, 50 BEALE STREET, SAN FRANCISCO, CA 94105. Immediately upon such delivery or mailing, the Policy shall bedeemed void from the beginning, and Premiums paid will be refunded.
PLEASE NOTE
Some hospitals and other providers do not provide one or more of the following services that maybe covered under your policy and that you might need: family planning; contraceptive services,including emergency contraception; sterilization, including tubal ligation at the time of labor anddelivery; infertility treatments; or abortion. You should obtain more information before you be-
come a policyholder or select a network provider. Call your prospective doctor or clinic, or callthe health plan at Blue Shield Life's Customer Service telephone number provided on the lastpages of this booklet to ensure that you can obtain the health care services that you need.
IMPORTANT!
No Insured has the right to receive the benefits of this Plan for Services or supplies furnished following termination of cov-erage. Benefits of this Plan are available only for Services and supplies furnished during the term it is in effect and whilethe individual claiming benefits is actually covered by this Policy. Benefits may be modified during the term of this Plan asspecifically provided under the terms of this Policy or upon renewal. If benefits are modified, the revised benefits (includ-
ing any reduction in benefits or the elimination of benefits) apply for Services or supplies furnished on or after the effectivedate of the modification. There is no vested right to receive the benefits of this Plan.
IFP-DOIAS-000 (1-10)
IFP-AS025-000 (1-10)
Case: 09-80173 01/25/2010 Page: 2 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
28/110
The Blue Shield Life Active Start Plan 25
Subscriber Bill of Rights
As a Blue Shield Life Active Start Plan 25 Subscriber, you have the right to:
1. Receive considerate and courteous care, with respect foryour right to personal privacy and dignity.
2. Receive information about all health Services availableto you, including a clear explanation of how to obtainthem.
3. Receive information about your rights and responsibili-ties.
4. Receive information about your Blue Shield Life ActiveStart Plan 25, the Services we offer you, the Physicians,and other practitioners available to care for you.
5. Have reasonable access to appropriate medical services.6. Participate actively with your Physician in decisions
regarding your medical care. To the extent permitted bylaw, you also have the right to refuse treatment.
7. A candid discussion of appropriate or Medically Neces-sary treatment options for your condition, regardless ofcost or benefit coverage.
8. Receive from your Physician an understanding of yourmedical condition and any proposed appropriate orMedically Necessary treatment alternatives, including
available success/outcomes information, regardless of costor benefit coverage, so you can make an informed decisionbefore you receive treatment.
9. Receive preventive health Services.10. Know and understand your medical condition, treatment
plan, expected outcome, and the effects these have onyour daily living.
11. Have confidential health records, except when disclo-sure is required by law or permitted in writing by you.With adequate notice, you have the right to review yourmedical record with your Physician.
12. Communicate with and receive information from Cus-tomer Service in a language that you can understand.
13. Know about any transfer to another Hospital, includinginformation as to why the transfer is necessary and anyalternatives available.
14. Be fully informed about the Blue Shield Life grievanceprocedure and understand how to use it without fear ofinterruption of health care.
15. Voice complaints or grievances about the Blue ShieldLife Active Start Plan 25 or the care provided to you.
Case: 09-80173 01/25/2010 Page: 3 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
29/110
The Blue Shield Life Active Start Plan 25
Subscriber Responsibilities
As a Blue Shield Life Active Start Plan 25 Subscriber, you have the responsibility to:
1. Carefully read all Blue Shield Life Active Start Plan 25materials immediately after you are enrolled so you un-derstand how to use your Benefits and how to minimizeyour out of pocket costs. Ask questions when neces-sary. You have the responsibility to follow the provi-sions of your Blue Shield Life Active Start Plan 25membership as explained in the Policy.
2. Maintain your good health and prevent illness by mak-ing positive health choices and seeking appropriate carewhen it is needed.
3. Provide, to the extent possible, information that yourPhysician, and/or the Plan need to provide appropriate
care for you.
4. Follow the treatment plans and instructions you andyour Physician have agreed to and consider the potentialconsequences if you refuse to comply with treatmentplans or recommendations.
5. Ask questions about your medical condition and makecertain that you understand the explanations and instruc-tions you are given.
6. Make and keep medical appointments and inform yourPhysician ahead of time when you must cancel.
7. Communicate openly with the Physician you choose soyou can develop a strong partnership based on trust andcooperation.
8. Offer suggestions to improve the Blue Shield Life Ac-tive Start Plan 25.
9. Help Blue Shield Life to maintain accurate and currentmedical records by providing timely information regard-ing changes in address, family status and other healthplan coverage.
10. Notify Blue Shield Life as soon as possible if you arebilled inappropriately or if you have any complaints.
11. Treat all Plan personnel respectfully and courteously aspartners in good health care.
12. Pay your Premiums, Copayment, Coinsurance, andcharges for non-covered Services on time.
13. For all Mental Health and substance abuse Services,follow the treatment plans and instructions agreed to byyou and the Mental Health Service Administrator(MHSA) and obtain prior authorization for all Non-Emergency Inpatient Mental Health and substanceabuse Services.
14. Follow the provisions of the Blue Shield Life BenefitsManagement Program.
Case: 09-80173 01/25/2010 Page: 4 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
30/110
TABLE OF CONTENTSPART PAGESUMMARY OF BENEFITS...............................................................................................................................................................1YOUR BLUE SHIELD LIFE ACTIVE START PLAN 25 AND HOW TO USE IT -....................................................................23
BLUE SHIELD LIFE NETWORK OF PREFERRED PROVIDERS...............................................................................................................24
CONTINUITY OF CARE BY A TERMINATED PROVIDER ......................................................................................................................24FINANCIAL RESPONSIBILITY FOR CONTINUITY OF CARE SERVICES .................................................................................................24PREMIUMS.......................................................................................................................................................................................24PLAN CHANGES .............................................................................................................................................................................25CONDITIONS OF COVERAGE.....................................................................................................................................................25
ENROLLMENT AND LIMITATION OF ENROLLMENT ...........................................................................................................................25DURATION OF THE POLICY...............................................................................................................................................................25TERMINATION/CANCELLATION/REINSTATEMENT OF THE POLICY ................................................................................................25TRANSFER OF COVERAGE ................................................................................................................................................................26RENEWAL OF THE POLICY................................................................................................................................................................27
MAXIMUM AGGREGATE PAYMENT .......................................................................................................................................27MEDICAL NECESSITY..................................................................................................................................................................27SECOND MEDICAL OPINION POLICY .....................................................................................................................................28
UTILIZATION REVIEW ................................................................................................................................................................28HEALTH EDUCATION AND HEALTH PROMOTION.............................................................................................................28RETAIL-BASED HEALTH CLINICS............................................................................................................................................28NURSEHELP 24/7 AND LIFEREFERRALS 24/7 ........................................................................................................................28BENEFITS MANAGEMENT PROGRAM ....................................................................................................................................28
PRIOR AUTHORIZATION...................................................................................................................................................................29PRE-ADMISSION REVIEW.................................................................................................................................................................30HOSPITAL AND SKILLED NURSING FACILITY ADMISSIONS ..............................................................................................................30PRIOR AUTHORIZATION FOR OTHER THAN MENTAL HEALTH OR SUBSTANCE ABUSE ADMISSIONS ................................................30PRIOR AUTHORIZATION FOR INPATIENT MENTAL HEALTH OR SUBSTANCE ABUSE SERVICES, AND OUTPATIENT PARTIAL
HOSPITALIZATIONSERVICES AND OUTPATIENT ECT...............................................................................................................31EMERGENCY ADMISSION NOTIFICATION .........................................................................................................................................31HOSPITAL INPATIENT REVIEW .........................................................................................................................................................31
DISCHARGE PLANNING....................................................................................................................................................................31CASE MANAGEMENT .......................................................................................................................................................................31ADDITIONAL AND REDUCED PAYMENTS FOR FAILURE TO USE THE BENEFITS MANAGEMENT PROGRAM.............................................................................................................................................................................................................31DEDUCTIBLE...................................................................................................................................................................................32PAYMENT.........................................................................................................................................................................................32
OUT-OF-AREA PROGRAM:THE BLUECARDPROGRAM..................................................................................................................32MAXIMUM PER INSURED CALENDAR YEAR COPAYMENT/COINSURANCE RESPONSIBILITY .............................................................34
PRINCIPAL BENEFITS AND COVERAGES (COVERED SERVICES)..................................................................................34ACUPUNCTURE BENEFITS ................................................................................................................................................................35AMBULANCE BENEFITS ...................................................................................................................................................................35AMBULATORY SURGERY CENTER BENEFITS ...................................................................................................................................35BARIATRIC SURGERY BENEFITS ......................................................................................................................................................35
CHIROPRACTIC BENEFITS ................................................................................................................................................................36CLINICAL TRIAL FOR CANCER BENEFITS .........................................................................................................................................37DIABETES CARE BENEFITS ..............................................................................................................................................................37DIALYSIS BENEFITS .........................................................................................................................................................................37DURABLE MEDICAL EQUIPMENT BENEFITS .....................................................................................................................................38EMERGENCY ROOM BENEFITS .........................................................................................................................................................38FAMILY PLANNING SERVICE BENEFITS............................................................................................................................................38HOME HEALTH CARE BENEFITS ......................................................................................................................................................38HOME INFUSION/HOME INJECTABLE THERAPY BENEFITS..............................................................................................................39HOSPICE PROGRAM BENEFITS .........................................................................................................................................................39
Case: 09-80173 01/25/2010 Page: 5 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
31/110
HOSPITAL BENEFITS (FACILITY SERVICES)......................................................................................................................................41MEDICAL TREATMENT OF THE TEETH,GUMS, OR JAW JOINTS AND JAW BONES BENEFITS..............................................................43MENTAL HEALTH AND SUBSTANCE ABUSE BENEFITS .....................................................................................................................44ORTHOSES BENEFITS .......................................................................................................................................................................45OUTPATIENT OR OUT-OF-HOSPITAL X-RAY,PATHOLOGY, AND/OR LABORATORY BENEFITS .........................................................45OUTPATIENT REHABILITATION BENEFITS ........................................................................................................................................45
OUTPATIENT PRESCRIPTION DRUG BENEFITS ..................................................................................................................................46PKURELATED FORMULAS AND SPECIAL FOOD BENEFITS ..............................................................................................................50PREGNANCY BENEFITS ....................................................................................................................................................................51PODIATRIC BENEFITS.......................................................................................................................................................................51PREVENTIVE HEALTH BENEFITS ......................................................................................................................................................51PROFESSIONAL (PHYSICIAN)BENEFITS............................................................................................................................................52PROSTHETIC APPLIANCE BENEFITS..................................................................................................................................................53RADIOLOGICAL PROCEDURES BENEFITS (REQUIRING PRIOR AUTHORIZATION) ..............................................................................54SKILLED NURSING FACILITY BENEFITS ...........................................................................................................................................54SPEECH THERAPY BENEFITS............................................................................................................................................................54TRANSPLANT BENEFITS ...................................................................................................................................................................54
PRINCIPAL LIMITATIONS, EXCEPTIONS, EXCLUSIONS, AND REDUCTIONS ............................................................55GENERAL EXCLUSIONS....................................................................................................................................................................55
MEDICAL
NECESSITY
EXCLUSION
...................................................................................................................................................58PRE-EXISTING CONDITIONS.............................................................................................................................................................59LIMITATIONS FOR DUPLICATE COVERAGE.......................................................................................................................................59EXCEPTION FOR OTHER COVERAGE.................................................................................................................................................60CLAIMS REVIEW ..............................................................................................................................................................................60REDUCTIONS -ACTS OF THIRD PARTIES ..........................................................................................................................................60
GENERAL PROVISIONS ...............................................................................................................................................................60NON-ASSIGNABILITY.......................................................................................................................................................................60PLAN INTERPRETATION ...................................................................................................................................................................61CONFIDENTIALITY OF PERSONAL AND HEALTH INFORMATION........................................................................................................61ACCESS TO INFORMATION ...............................................................................................................................................................61INDEPENDENT CONTRACTORS .........................................................................................................................................................61ENTIRE POLICY:CHANGES ..............................................................................................................................................................61TIME LIMIT ON CERTAIN DEFENSES ................................................................................................................................................61
GRACE PERIOD ................................................................................................................................................................................61NOTICE AND PROOF OF CLAIM ........................................................................................................................................................62PAYMENT OF BENEFITS ...................................................................................................................................................................62COMMENCEMENT OF LEGAL ACTION...............................................................................................................................................62ORGAN AND TISSUE DONATION.......................................................................................................................................................62CHOICE OF PROVIDERS ....................................................................................................................................................................62ENDORSEMENTS AND APPENDICES ..................................................................................................................................................63NOTICES ..........................................................................................................................................................................................63COMMENCEMENT OR TERMINATION OF COVERAGE.........................................................................................................................63IDENTIFICATION CARDS...................................................................................................................................................................63LEGAL PROCESS ..............................................................................................................................................................................63NOTICE ............................................................................................................................................................................................63
CUSTOMER SERVICE ...................................................................................................................................................................63FOR ALL SERVICES OTHER THAN MENTAL HEALTH AND SUBSTANCE ABUSE -.................................................................................63FOR ALL MENTAL HEALTH AND SUBSTANCE ABUSE SERVICES - .....................................................................................................63
GRIEVANCE PROCESS .................................................................................................................................................................64FOR ALL SERVICES OTHER THAN MENTAL HEALTH AND SUBSTANCE ABUSE -.................................................................................64FOR ALL MENTAL HEALTH AND SUBSTANCE ABUSE SERVICES - .....................................................................................................64CALIFORNIA DEPARTMENT OF INSURANCE REVIEW ........................................................................................................................65
DEFINITIONS...................................................................................................................................................................................65PLAN PROVIDER DEFINITIONS .........................................................................................................................................................65ALL OTHER DEFINITIONS ................................................................................................................................................................67
NOTICE OF THE AVAILABILITY OF LANGUAGE ASSISTANCE SERVICES .................................................................72
Case: 09-80173 01/25/2010 Page: 6 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
32/110
Page 1IFP-DOISOB-001 (1-10)
Summary of BenefitsPreferred Provider Plan
Note: The SUMMARY OF BENEFITS represents only a brief description of the Benefits. Please read this Policy carefully for acomplete description of provisions, benefits, exclusions, and other important information pertaining to this Plan.
For Benefits that have a visit maximum, all visits count toward the visit maximum, regardless of whether the Calendar Year De-ductible has been satisfied, or you have reached the Maximum Calendar Year Copayment/Coinsurance Responsibility.
Note that certain services are covered only if rendered by a Preferred Provider. Using a Non-Preferred Provider could result in no payment by Blue Shield Life for services. Please read this Sum-mary of Benefits and the section entitled Covered Services so you will know from which providershealth care may be obtained. The Preferred Provider Directory can be located online atwww.blueshielca.com or by calling Customer Service at the telephone number provided on the lastpage of this Policy.
Calendar Year Deductibleper Insured Deductible
(Medical Plan Deductible)
Deductible Responsibility
The Calendar Year deductible is as indicated. $0 per Insured
There is no Calendar Year deductible (Medical Plan Deductible).
Calendar Year Brand Name Drug Deductible1 Deductible Responsibility
The Calendar Year Brand Name Drug deductible isas indicated.
$500 per Insured
The Brand Name Drug deductible applies to all covered Brand Name Drugs Incurred during a Calendar Year.
Charges for Brand Name Drugs in excess of the Participating Pharmacy contracted rate do not apply to the Calendar Year BrandName Drug deductible.
The Brand Name Drug deductible must be satisfied once during each Calendar Year by or on behalf of the Insured.
1 The Calendar Year Brand Name Drug deductible does not count towards the Calendar Year deductible nor toward the Insureds
maximum Calendar Year Copayment / Coinsurance responsibility.
Case: 09-80173 01/25/2010 Page: 7 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
33/110
Page 2IFP-DOISOB-001 (1-10)
Maximum per Insured Calendar YearCopayment/Coinsurance Responsibility
Copayment/CoinsuranceResponsibility 1
The maximum Calendar Year Copayment/Coinsurance responsibility for applicable cov-ered Services * rendered by any combinations of Preferred Providers, Participating Pro-
viders, MHSA Participating Providers, and/or Other Providers.
$6,000 per Insured
The maximum Calendar Year Copayment/Coinsurance responsibility for applicable cov-ered Services * rendered by any combination of eligible providers.
$8,000 per Insured
* Once you have reached the maximum responsibility as indicated, the Plan will pay 100% of your covered medical Services forthe remainder of the Calendar Year except as noted below.
1 The following are not included in the maximum Calendar Year Copayment amount:
The Calendar Year Brand Name Drug deductible;
Charges in excess of the benefit maximum;Any additional payment Incurred as described in the Benefits Management Program;Charges for Services which are not covered and charges by non-Preferred and MHSA Non-Participating Providers in excess
of the amounts covered by this Policy;Outpatient prescription Drugs including mail service prescription Drugs;Outpatient visits for other than Severe Mental Illnesses or Serious Emotional Disturbances of a Child;Inpatient Hospital Facility Services for Mental Illness when Services are received from MHSA Non-Participating Providers;Services by a Non-Preferred Hospital-based Skilled Nursing Facility;Internet Based Consultations;Non-Emergency Services from a Non-Participating Hospital;Partial hospitalization Services for Mental Illnesses from a MHSA Non-Participating Provider;Outpatient Surgery from a Non-Participating Ambulatory Surgery Center;Family Planning injectable contraceptives administered by a Physician;
Diabetes self-management training from a non-participating Physician;Dialysis services from a non-preferred Dialysis Center;Covered travel expenses for bariatric surgery Services;Outpatient routine newborn circumcision in the outpatient department of a Hospital; andProfessional Services for Reconstructive Surgery from Non-Preferred Physicians;
Note that Copayments, Coinsurance, and charges for Services not accruing to the maximum Calendar Year Copay-ment/Coinsurance responsibility continue to be the Insureds payment responsibility after the maximum Calendar Year Copay-ment/Coinsurance responsibility is reached.
Case: 09-80173 01/25/2010 Page: 8 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
34/110
Page 3IFP-DOISOB-001 (1-10)
Additional Payments
Additional payments for failure to utilize the Benefit Management Program.
Please refer to the Benefits Management Programs section for additional information.
Maximum Aggregate Payment Maximum Blue ShieldLife Payment
The maximum aggregate payment amount is determined by totaling all covered Benefits pro-vided to you whether covered under the Plan as a Subscriber or Dependent while coveredunder this Plan or while covered under any prior or subsequent health Plan with Blue Shieldof California or any of its affiliated companies, including Blue Shield Life. Benefits in excessof this amount are not covered under this Plan.
$6,000,000 per Insured
Case: 09-80173 01/25/2010 Page: 9 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
35/110
Page 4IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Acupuncture Benefits
Covered Services by a Doctor of Medicine or a certified acupuncturist up to aBenefit maximum of 12 visits per Insured, per Calendar Year.
50% of up to $50per visit
50% of up to $50per visit
Ambulance Benefits
Covered Services by ambulance companies
40% of billed charges 40% of billed charges
Ambulatory Surgical Benefits
Covered Services by Ambulatory Surgery Centers
Note: Participating Ambulatory Surgery Centers may not be available in allareas. Outpatient ambulatory surgery Services may also be obtained from aHospital or an ambulatory surgery center that is affiliated with a Hospital.Ambulatory surgery Services obtained from a Hospital or a Hospital affiliatedambulatory surgery center will be paid at the Preferred or Non-Preferred levelas specified in the Hospital section of this Summary of Benefits.
40% 50% of up to$300 per visit
Allowable Amount
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
Case: 09-80173 01/25/2010 Page: 10 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
36/110
Page 5IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred Bariatric
Surgery ServiceProviders 1
Services byNon-Preferred and
Non-ParticipatingProviders 1
Bariatric Surgery Benefits for Residents of Designated Counties inCalifornia 2
Facility Bariatric Surgery Services
Hospital Inpatient Services
Hospital Outpatient Services
Physician Bariatric Surgery Services
Note: Bariatric surgery Services for residents of non-designated counties 1 willbe paid as any other covered surgery as described elsewhere in this Summary ofBenefits.
All bariatric surgery Services must be prior authorized in writing, from thePlans Medical Director. Prior authorization is required for all Insureds, whetherresidents of designated or a non-designated county.
A per admissionCopayment of $500
and then 40%
$500 per Surgeryplus 40%
40%
Not covered 1
Not covered
1
Not covered 1
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
1 Bariatric Surgery Services for residents of designated counties must be provided by a Preferred Bariatric Surgery Services Pro-vider. See the Bariatric Surgery Services Benefits and Definitions sections for additional information.
2 See the Bariatric Surgery Services Benefits section for a list of designated counties.
Case: 09-80173 01/25/2010 Page: 11 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
37/110
Page 6IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services by
Preferred,Participating, andOther Providers **
Services by
Non-Preferred andNon-ParticipatingProviders ***
Chiropractic Benefits 1
Benefits are limited to a combined Benefit maximum of 12 visits per Insured,per Calendar Year for chiropractic Services, Outpatient Rehabilitation Ser-vices, and Speech Therapy Services.
40% Not covered
Clinical Trials for Cancer Benefits
Covered Services for the Insured who has been accepted into an approvedclinical trial for cancer when prior authorized by the Plan.
Services for routine patient care will be paid on the same basis and at the sameBenefit levels as other covered Services shown in the Summary of Benefits.
No charge No charge
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 No benefits are provided for Chiropractic Services by Non-Preferred or Non-participating Providers.
Case: 09-80173 01/25/2010 Page: 12 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
38/110
Page 7IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Diabetes Care Benefits
Covered Services and supplies
Outpatient self-management training
40%
$25 per visit 1
50%
$25 per visit 1
Dialysis Center Benefits 2
40% 50% of up to$300 per day
Durable Medical Equipment Benefits
There is a combined Benefit maximum of $2,000 per Insured, per CalendarYear for prosthetic appliances, orthotic Services, and Durable Medical Equip-ment. This maximum does not apply to Services covered under the DiabeticCare benefit. The maximum does not apply to Medically Necessary oxygencovered under this section.
40% 50%
Emergency Room Benefits
Emergency room Physician Services
Emergency room Services not resulting in an admission
Emergency room Services resulting in an admission (billed as part of InpatientHospital Services)
$25
$100 per visitplus 40%
$500 per admissionplus 40%
$25
$100 per visitplus 40%
$500 per admissionplus 40% 3
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the Allowable
Amount.
1 If billed by your provider, you will also be responsible for an office visit Copayment.
2 Prior authorization by Blue Shield Life is required for all dialysis Services.
3 For emergency room Services directly resulting in an admission as an Inpatient to a Non-Preferred Hospital which Blue ShieldLife determines are not an emergency, your Copayment/Coinsurance will be the Non-Preferred Hospital Inpatient Services Co-payment/Coinsurance.
Case: 09-80173 01/25/2010 Page: 13 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
39/110
Page 8IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Family Planning Service Benefits 1
Counseling and Consultation Services
Injectable Contraceptives when administered by a Physician during an OfficeVisit
Tubal ligation, vasectomy, and elective abortion
40%
$25 2
40%
Not covered
Not covered
Not covered
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 No benefits are provided for Family Planning Services by Non-Preferred or Non-Participating Providers.
2 Copayment for injectable contraceptives is in addition to any Copayment for the Office Visit.
Case: 09-80173 01/25/2010 Page: 14 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
40/110
Page 9IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Home Health Care Benefits
Home health agency Services including home visits by a nurse, home healthaide, medical social worker, physician therapist, speech therapist, or occupa-tional therapist
Medical supplies and related laboratory Services to the extent the Benefitswould have been provided had the Insured remained in the Hospital or SkilledNursing Facility.
Note: There is a combined Benefit maximum of 90 visits per Insured, per Cal-endar Year for all Home Health and Home Infusion/Home Injectable Services.
40%
40%
Not covered 1
Not covered 1
Home Infusion /Home Injectable Therapy Benefits
Home infusion/home injectable therapy and infusion nursing visits provided bya Home Infusion Agency
Note: There is a combined Benefits maximum of 90 visits per Insured, per Cal-endar Year for all Home Health and Home Infusion/Home Injectable Services.
40% Not Covered 1
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 Services by Non-Participating Home Health Care/Home Infusion Agencies are not covered unless prior authorized by the Plan.When authorized by the Plan, these Non-Participating Agencies will be reimbursed at a rate determined by the Plan and the agencyand your Copayment/Coinsurance will be at the Participating Agency Copayment/Coinsurance.
Case: 09-80173 01/25/2010 Page: 15 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
41/110
Page 10IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Hospice Program Benefits
Covered Services for Insureds who have been accepted into an approvedHospice Program.
Continuous home care during a period of crisis
General Inpatient care
Inpatient respite care
Routine home care
Pre-hospice consultative visit
40%
40%
No charge
No charge
No charge
Not covered 1
Not covered 1
Not covered
1
Not covered 1
Not covered 1
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 Services by Non-Participating Hospice Agencies are not covered unless prior authorized by the Plan. When authorized by thePlan, these Non-Participating Agencies will be reimbursed at a rate determined by the Plan and the agency and your Coinsurancewill be at the Participating Provider level.
Case: 09-80173 01/25/2010 Page: 16 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
42/110
Page 11IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Hospital Benefits (Facility Services)
Inpatient Services
Emergency Facility Services
Non-Emergency Facility Services
$500 per admissionplus 40%
$500 per admissionplus 40%
$500 per admission
plus 40% 1
50% of up to$500 per day
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 For Emergency Services by Non-Preferred Hospitals, your Copayment/Coinsurance will be at the Preferred Hospital Copay-ment/Coinsurance.
Case: 09-80173 01/25/2010 Page: 17 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
43/110
Page 12IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Hospital Benefits (Facility Services)continued
Outpatient Services
Services for Illness or Injury
Surgery Services
Dialysis Services 2
40%
$500 per Surgeryplus 40%
40%
50% of up to
$500 per day 1
50% of up to
$500 per day 1
50% of up to$300 per day
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 For Emergency Services by Non-Preferred Hospitals, your Copayment/Coinsurance will be at the Preferred Hospital Copay-ment/Coinsurance.
2 Prior authorization by Blue Shield Life is required for all dialysis Services.
Case: 09-80173 01/25/2010 Page: 18 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
44/110
Page 13IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Medical Treatment for the Teeth, Gums, Jaw Joints, or Jaw BonesBenefits
Office Visit
Services with the office visit
$25
40%
50%
50%
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
Case: 09-80173 01/25/2010 Page: 19 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
45/110
Page 14IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Mental Health and Substance Abuse Benefits
(All Services provided through the Plans Mental Health ServiceAdministrator [MHSA])
Services byMHSA
ParticipatingProviders *
Services byMHSA
Non-ParticipatingProviders **
Inpatient Mental Health Services 1
Hospital Services
Partial Hospitalization 3
Professional (Physician Services)
Outpatient Facility & Office Mental Health Services for Severe Mental
Illnesses or Serious Emotional Disturbances of a Child 4
Hospital Outpatient department Services (including intensive Outpatientcare and electroconvulsive therapy [ECT])
Office Services
$500 per admissionplus 40%
40% per
episode of care 3
40%
$25
$25
50% of up to$500 per day 2
50% of up to$500 per day
50%
50%
50%
* Unless otherwise specified, Copayments are calculated based on the Allowable Amount.
** For Services by MHSA Non-Participating Providers you are responsible for all charges above the Allowable Amount.
1 All Inpatient Mental Health Services and Outpatient Partial Hospitalization and Outpatient electroconvulsive therapy Services(except for Emergency and urgent Services) must be prior authorized by the MHSA.
2 For Emergency Services by MHSA Non-Participating Hospitals your Copayment/Coinsurance will be the MHSA ParticipatingHospital Copayment/Coinsurance based on billed charges.
3 For Partial Hospitalization Services, an episode of care is the date from which the patient is admitted to the Partial Hospitaliza-tion Program to the date the patient is discharged or leaves the Partial Hospitalization Program. Any Services received betweenthese two dates would constitute the episode of care. If the patient needs to be readmitted at a later date, this would constitute an-other episode of care.
4 This Copayment/Coinsurance includes both Outpatient facility and Professional (Physician) Services.
Case: 09-80173 01/25/2010 Page: 20 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
46/110
Page 15IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Mental Health and Substance Abuse Benefits (continued)
(All Services provided through the Plans Mental Health ServiceAdministrator [MHSA])
Services byMHSA
ParticipatingProviders *
Services byMHSA
Non-ParticipatingProviders **
Outpatient Facility & Office Mental Health Services for other than SevereMental Illnesses or Serious Emotional Disturbances of a Child
Note: Services are limited to a combined Benefit maximum of 20 visits perInsured, per Calendar Year. No Benefits are provided for Outpatient or out-of-Hospital Mental Health Services & substance abuse care from MHSA Non-
Participating Providers, except for the initial visit. 1
Psychological Testing
Psychosocial support through LifeReferrals 24/7
40%
40%
No charge
Not covered 1
50%
N/A
* Unless otherwise specified, Copayments are calculated based on the Allowable Amount.
** For Services by MHSA Non-Participating Providers you are responsible for all charges above the Allowable Amount.
1 For the initial Mental Health Service or substance abuse care visit to determine the condition and diagnosis of the Insured, Bene-fits will be provided and paid as if the condition was a Severe Mental Illness or a Serious Emotional Disturbances of a Child asshown above.
Case: 09-80173 01/25/2010 Page: 21 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
47/110
Page 16IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Orthoses Benefits
Benefits are limited to a combined Benefit maximum of $2,000 per Insured,per Calendar Year for prosthetic appliances, orthotic Services, and DurableMedical Equipment.
40% 50%
Outpatient or Out-of-Hospital X-Ray, Pathology, and Laboratory Benefits
40% 1 50% 1
Outpatient Rehabilitation Benefits
Benefits are limited to a combined Benefit maximum of 12 visits per Insured,per Calendar Year for chiropractic Services, Outpatient Rehabilitation Ser-vices, and Speech Therapy Services.
40%2, 3
50% of up to$50 per visit 2, 3
PKU Related Formulas & Special Food Products Benefits
PKU related formulas & special food products
The above Services must be prior authorized by the Plan.
40% of billed charges Not covered 4
Podiatric Benefits $25 per visit 50%
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1
Coinsurance will be assessed per provider and per date of Service.
2 If billed by your provider, you will also be responsible for an office visit Copayment.
3 For Services by certified occupational therapists and certified respiratory therapists, which are Other Providers, you are responsi-ble for all charges above the Allowable Amount.
4 Services by Non-Participating Home Health Care/Home Infusion Agencies are not covered unless prior authorized by the Plan.When authorized by the Plan, these Non-Participating Agencies will be reimbursed at a rate determined by the Plan and the agencyand your Copayment/Coinsurance will be at the Participating Agency Copayment/Coinsurance.
Case: 09-80173 01/25/2010 Page: 22 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
48/110
Page 17IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Prescriptions filledby a Participating
Retail or Mail OrderPharmacy
Prescriptions filledby a
Non-ParticipatingPharmacy 3
Outpatient Prescription Drug Benefits 1, 2, 3, 4, 5, & 6
Retail prescriptionsFormulary Generic Drugs
Formulary Brand Name Drugs
Non-Formulary Brand Name Drugs
Mail services prescriptionsFormulary Generic Drugs
Formulary Brand Name Drugs
Non-Formulary Brand Name Drugs
Home Self-Administered Injectables
$10
$35
The greater of $50or 50% of Blue Shield
Lifes contracted rate
$20
$70
The greater of $100or 50% of Blue ShieldLifes contracted rate
30%
Not covered
Not covered
Not covered
Not covered
Not covered
Not covered
Not covered
* Copayment/Coinsurance is calculated based on the contracted rate for covered prescriptions between Blue Shield Life and theParticipating Pharmacy, including Specialty Pharmacies, or the Participating Mail Order Pharmacy.
1 The Insureds Maximum Calendar Year Copayment/Coinsurance responsibility does not apply to the Outpatient PrescriptionDrug benefit.
2 Except for covered emergencies and Drugs for emergency contraception, no benefits are provided for Drugs received from Non-Participating Pharmacies.
3 Copayment / Coinsurance apply per prescription or refill.
4
Benefits for covered Brand Name Drugs are subject to a per Insured, per Calendar Year $500 Brand Name Drug deductible.5 The Outpatient Prescription Drug benefit is separate from the Active Start Plan 25.
6 There is a maximum Blue Shield Life payment of $2,000 per Insured, per Calendar Year for Brand Name Drugs.
Case: 09-80173 01/25/2010 Page: 23 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
49/110
Page 18IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Pregnancy Benefits No Coverage No Coverage
Preventive Care Benefits 1
Annual Physical Examination including only the annual routine physical ex-amination office visit; urinalysis; eye and ear screening; and pediatric and adultimmunizations and the immunizing agent
Annual Gynecological Examination including only the annual gynecologicalexamination office visit; mammography; routine Papanicolaou (Pap) test orother Food and Drug Administration (FDA) approved cervical cancer screen-ing test; and the human papillomavirus (HPV) screening test
Well Baby Examinations including only the well baby examination office visit;tuberculin test; and pediatric immunizations and the immunizing agent
Colorectal Cancer Screening Services
Osteoporosis Screening Services
NurseHelp 24/7
$25
$25
$25
40%
40%
No charge
Not covered
Not covered
Not covered
Not covered
Not covered
N/A
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 No benefits are provided for Preventive Care Services when rendered by Non-Preferred or Non-Participating Providers.
Case: 09-80173 01/25/2010 Page: 24 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
50/110
Page 19IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Professional (Physician) Benefits
Office visits except for Allergy testing and treatment
Services with the office visit including allergy testing and treatment
Visits to the home, Hospital except for those rendered in the Emergency Room,skilled nursing facility, and Ambulatory Surgery Center, including surgery,chemotherapy, and kidney dialysis
Internet Based Consultations
$25
40%
40%
$10
50%
50%
50%
Not covered
Prosthetic Appliance Benefits
Benefits are limited to a combined Benefit maximum of $2,000 per Insured,per Calendar Year for prosthetic appliances, orthotic Services, and DurableMedical Equipment.
40% 50%
Radiological Procedure Benefits (Requiring Prior Authorization)
Outpatient, non-Emergency radiological procedures including CT scans, MRIs,MRAs. PET scans, and cardiac diagnostic procedures utilizing nuclear medi-cine
Note: Blue Shield Life requires prior authorization for all these Services.
40% 50%
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
Case: 09-80173 01/25/2010 Page: 25 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
51/110
Page 20IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Skilled Nursing Facility Benefits
Services by a Skilled Nursing Facility Unit of a Hospital
Services by a freestanding Skilled Nursing Facility
Note: There is a combined Benefit maximum of 100 days per Insured, perCalendar Year for all skilled nursing Services.
40%
40% 1
50%
40% 1
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 For Services by free-standing skilled nursing facilities (nursing homes), which are Other Providers, you are responsible for allcharges above the Allowable Amount.
Case: 09-80173 01/25/2010 Page: 26 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
52/110
Page 21IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, andOther Providers **
Services byNon-Preferred and
Non-ParticipatingProviders ***
Speech Therapy Benefits
Note: All Outpatient speech therapy Services require prior authorization fromthe Plan.
Outpatient Services
Benefits are limited to a combined Benefit maximum of 12 visits per Insured,per Calendar Year for chiropractic Services, Outpatient Rehabilitation Ser-
vices, and Speech Therapy Services.
40% 1, 2 50%
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for acomplete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 For Services by licensed speech therapists, which are Other Providers, you are responsible for all charges above the Allowable
Amount.2 If billed by your provider, you will also be responsible for an office visit Copayment/Coinsurance.
Case: 09-80173 01/25/2010 Page: 27 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
53/110
Page 22IFP-DOISOB-001 (1-10)
Benefit Copayment/CoinsuranceResponsibility *
Services byPreferred,
Participating, &Other Providers **
Services byNon-Preferred &Non-Participating
Providers ***
Transplant Benefits
Organ Transplants
Hospital Services
Professional (Physician) Services
Special Transplant Benefits 1
Facilities Services in a Special Transplant Facility
Professional (Physician) Services
Note: The Plan requires prior authorization for all Special Transplant Ser-vices. Also, all Services must be provided at a Special Transplant Facilitydesignated by Blue Shield Life.
$500 per admissionand then 40%
40%
$500 per admissionand then 40%
40%
50% of up to$500 per day
50%
Not covered
Not covered
* Unless otherwise specified, Copayments/Coinsurance are calculated on the Allowable Amount.
** Other Providers are not preferred Providers and so for Services from Other Providers you are responsible for all charges abovethe Allowable Amount. Other Providers include acupuncturists, ambulance companies, nursing homes, and certain labs (for a com-plete list of Other Providers see the Definitions section).
*** For Services by Non-Preferred and Non-Participating Providers you are responsible for all charges above the AllowableAmount.
1 Special Transplant Benefits are limited to the procedures listed in the Covered Services section. See the Special Transplant Bene-fits Covered Services section for information on Services and requirements.
Case: 09-80173 01/25/2010 Page: 28 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
54/110
Page 23IFP-DOIAS-000 (1-10)
Your Blue Shield Life Active Start Plan 25 andHow to Use It -PLEASE READ THE FOLLOWING SO YOU WILLKNOW FROM WHOM OR WHAT GROUP OFPROVIDERS, HEALTH CARE MAY BE PROVIDED.
The Blue Shield Life Active Start Plan 25 has a commongoal with you and with health care professionals - qualityhealth care coverage at a reasonable cost. You can controlyour out-of-pocket costs by carefully choosing the providersfrom whom you receive covered Services.
This Plan has two different payment levels depending on thePhysician or Hospital from which you receive covered Ser-vices. Blue Shield Life has a statewide network of nearly50,000 Physician Members and contracted Hospitals knownas Preferred Providers. Many other health care profession-als, including optometrists and podiatrists are also PreferredProviders.
The highest benefits of the Active Start Plan 25 are providedwhen you receive covered Services from a Preferred Pro-vider. You will Incur higher out-of-pocket costs when youreceive covered Services from a Non-Preferred Provider.
Note: choosing a Preferred Provider will assure the lowestlevel of Insureds payments available under this Plan. Seethe Definitions section for more information.
Preferred Providers have agreed to accept the Plans pay-ment, plus payment of any applicable deductibles, the In-sureds Copayments and Coinsurances, or amounts in excess
of specified benefit maximums as payment-in-full for cov-ered Services, except as provided under the section entitledActs of Third Parties. This is not true of Non-Preferred Pro-viders. If you receive Services from a Non-Preferred Pro-vider, the Plans payment may be substantially less than theamount the provider bills. You are responsible for the dif-ference between the amount the Non-Preferred Provider billsand the amount the Plan pays.
In addition, certain services are not covered when receivedfrom Non-Preferred Providers. It is therefore to your advan-tage to obtain medical and Hospital Services from PreferredProviders.
Failure to meet these responsibilities may result in your In-curring a substantial financial liability. Some services maynot be covered unless prior review and other requirementsare met.
Blue Shield Life, or the MHSA, will render a decision on allrequests for prior authorization, and pre-admission reviewwithin five (5) business days from receipt of the request.The treating provider will be notified of the decision within
24 hours followed by written notice to the provider and Sub-scriber within two (2) business days of the decision. Forurgent Services in situations in which the routine decisionmaking process might seriously jeopardize the life or healthof an Insured, or when the Insured is experiencing severepain, Blue Shield Life, or the MHSA, will respond as soon as
possible to accommodate the Insureds condition not to ex-ceed 72 hours from receipt of the request.
Preferred Providers submit claims for payment after theirServices have been received. You or your Non-PreferredProviders also submit claims for payment after Services havebeen received.
Providers do not receive financial incentives or bonuses fromthe Plan.
When you need health care, present your Blue Shield LifeIdentification Card to your Physician, Hospital or other li-
censed health care provider. Your Identification Card hasyour Subscriber and group number on it. Be sure to includeyour Insured and group numbers on all claims you submit toBlue Shield Life. Preferred Providers usually bill the Plandirectly. See section on Notice and Proof of Claim in thisPolicy for information on filing a claim if a provider has notbilled the Plan directly. Blue Shield Life will notify you ofits determination within thirty (30) days after receipt of theclaim.
The Blue Shield Life Active Start Plan 25 is specifically de-signed for you to use the Blue Shield Life Provider Networkof Preferred Providers. Refer to the Covered Services sec-tion of this Policy for Copayment and Coinsurance informa-tion. Preferred Providers are listed in the Preferred ProviderDirectories.
If you wish to obtain a copy of the Preferred Provider Direc-tory, you may request a copy by contacting the Plans Cus-tomer Service Department at 1-800-431-2809. You may alsoverify this information by accessing Blue Shield Lifes Inter-net site located at http://www.blueshieldca.com.
Note: A Preferred Providers status may change. It is yourobligation to verify whether the Physician, Hospital, or Al-ternate Care Services provider you choose is a Preferred Pro-vider in case there have been any changes since your Pre-ferred Provider Directory has been published.
Insureds who reasonably believe that they have an emer-gency medical condition which requires an emergency re-sponse are encouraged to appropriately use the 911 emer-gency response system where available.
For all Mental Health and substance abuse Services: TheMHSA is a specialized health care service plan that will un-
Case: 09-80173 01/25/2010 Page: 29 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
55/110
Page 24IFP-DOIAS-000 (1-10)
derwrite and deliver the Plans Mental Health and substanceabuse Services through a separate network of Mental HealthService Administrator (MHSA) Participating Providers.
Note that MHSA Participating Providers are only those Pro-viders who participate in the MHSA network and have con-
tracted with the MHSA to provide Mental Health and sub-stance abuse Services to Insureds. A Blue Shield Life ProviderNetwork Preferred/Participating Provider may not be anMHSA Participating Provider. MHSA Participating Providersagree to accept the MHSAs payment, plus your payment ofCopayment, Coinsurance or amounts in excess of benefitmaximums specified, as payment-in-full for covered MentalHealth and substance abuse Services. This is not true ofMHSA Non-Participating Providers; therefore, it is to youradvantage to obtain Mental Health and substance abuse Ser-vices from MHSA Participating Providers.
It is your responsibility to ensure that the Provider you select
for Mental Health and substance abuse Services is an MHSAParticipating Provider. MHSA Participating Providers areindicated in the Behavioral Health Provider Directory. Addi-tionally, Insureds may contact the MHSA directly for informa-tion on, and to select an MHSA Participating Provider by call-ing 1-877-214-2928. You may also search for an MHSAParticipating Provider by accessing Blue Shield Life's Internetsite located at http://www.blueshieldca.com.
Blue Shield Life Network of Preferred ProvidersPLEASE READ THE FOLLOWING SO YOU WILLKNOW FROM WHOM OR WHAT GROUP OFPROVIDERS, HEALTH CARE MAY BE OBTAINED.
The California Department of Insurance has regulations thatestablish access standards for a plans provider network inCalifornia. For purposes of these provide network accessstandards, the service area for this Plan is the State of Cali-fornia.
This Plan is most effective and advantageous when coveredServices are received from Preferred Providers. You receivethe maximum benefits of the Plan when you receive Servicesfrom these providers.
Insureds are paid directly by Blue Shield Life if Services arereceived from a Non-Preferred Provider. Payments to Insur-eds for Services are in amounts identical to those made di-rectly to providers. See the section entitled NOTICE ANDPROOF OF CLAIM in this Policy for information on filing aclaim if a provider has not billed the Plan directly. BlueShield Life will notify you of its determination within thirty(30) days after receipt of the claim.
Insureds are not responsible to Preferred Providers for pay-ment for covered Services, except for payment of any appli-
cable deductibles, Copayments, Coinsurances, or amounts inexcess of specified benefit maximums, except as providedunder the section entitled Acts of Third Parties.
Payment for Emergency Services rendered by a physician orhospital who is not a Preferred Provider will be based on the
Allowable Amount but will be paid at the Preferred level ofbenefits. You are responsible for notifying the Plan within24 hours, or by the end of the first business day, following anemergency admission at a Non-Preferred Hospital, or as soonas is reasonably possible to do so.
Continuity of Care by a Terminated ProviderInsureds who are being treated for acute conditions, seriouschronic conditions, pregnancies (including immediate post-partum care), or terminal illness; or who are children frombirth to 36 months of age; or who have received authoriza-tion from a now-terminated provider for surgery or anotherprocedure as part of a documented course of treatment can
request completion of care in certain situations with a pro-vider who is leaving the Blue Shield Life provider network.Contact Customer Service to receive information regardingeligibility criteria and the policy and procedure for request-ing continuity of care from a terminated provider.
Financial Responsibility for Continuity of Care ServicesIf an Insured is entitled to receive Services from a terminatedprovider under the preceding Continuity of Care provision,the responsibility of the Insured to that provider for Servicesrendered under the Continuity of Care provision shall be nogreater than for the same Services rendered by a PreferredProvider in the same geographic area.
PremiumsMonthly Premiums are as stated in the Appendix. BlueShield Life offers a variety of options and methods by whichyou may pay your Premiums. Please call Customer Serviceat 1-800-431-2809 to discuss these options or visit the BlueShield Life internet site at http://www.blueshieldca.com.
Payments by mail are to be sent to:
Blue Shield LifeP.O. Box 51827
Los Angeles, CA 90051-6127
Additional Premiums may be charged in the event that a stateor any other taxing authority imposes upon Blue Shield Lifea tax or license fee, which is calculated upon, base Premiumsor Blue Shield Life's gross receipts or any portion of either.Premiums increase according to the Subscriber's age, asstated in the Appendix. Premiums may also increase fromtime to time as determined by Blue Shield Life. You willreceive thirty (30) days written notice of any changes in themonthly Premiums for this Plan.
Case: 09-80173 01/25/2010 Page: 30 of 80 ID: 7206864 DktEntry: 31-6
8/3/2019 09-80173 #31
56/110
Page 25IFP-DOIAS-000 (1-10)
Plan ChangesThe benefits of this Plan, including but not limitedto Covered Services, deductible, Copayment, Co-insurance, and annual copayment/coinsurancemaximum amounts, are subject to change at any
time. Blue Shield will provide at least 30 dayswritten notice of any such change.
Benefits for Services or supplies furnished afterthe Effective Date of any change in benefits willbe based on the change. There is no vested right toobtain benefits.
Conditions of Coverage
Enrollment and Limitation of Enrollment1. Enrollment in this Plan is limited to the individual Sub-
scriber only. The Plan does not provide family coveragefor any Dependent of the Subscriber, including coveragefor newborns.
2. Enrollment of the Subscriber is not effective until BlueShield Life approves an application and accepts the ap-plicable Premiums. Only Blue Shield Life's Underwrit-ing Department can approve an application.
3. An applicant, upon completion and approval by BlueShield Life of the application, is entitled to the benefitsof this Policy upon the Effective Date.
4. By completing an application, the Subscriber agrees tocooperate with Blue Shield Life by providing, or provid-ing access to, documents and other information that thePlan may request to corroborate the information for cov-erage. If the Subscriber fails or refuses to provide thesedocuments or information to Blue Shield Life, coverageunder this plan may be cancelled.
5. The Subscriber must be a Resident of California. Uponchange of residence to another jurisdiction, this Policywill terminate. Coverage may be transferred to a BlueCross or Blue Shield Plan for that jurisdiction, if any.Please see the section entitled Transfer of Coverage for
additional information.
Duration of the PolicyThis Policy shall be renewed upon receipt of prepaid Premi-ums unless otherwise terminated as described herein. Re-newal is subject to Blue Shield Lifes right to amend thisPolicy. Any change in Premiums or benefits, are effectiveafter 30 days notice from date of mailing to the Subscriber'saddress of record with Blue Shield Life.
Termination / Cancellation / Reinstatement ofthe Policy1. Blue Shield Life may terminate this Policy to-
gether with all like Policies by giving 90 dayswritten notice. No Insured shall be terminated
individually by Blue Shield Life for any causeother than as provided under this Section. ASubscriber desiring to terminate this Policyshall give Blue Shield Life 30 days written no-tice.
This Policy may be cancelled by Blue ShieldLife for false representations to, or conceal-ment of material facts from, Blue Shield Life inany health statement, application, or any writ-ten instruction furnished to Blue Shield Life by
the Insured at any time before or after issuanceof this Policy, or fraud or deception in enroll-ment. The Policy may also be cancelled if theSubscriber fails or refuses to provide access todocuments and other information that was pro-vided in the application for coverage. Cancel-lation in such instances shall be effective as ofthe original Effective Date of coverage, with-out prior notice to the Subscriber.
Blue Shield Life may terminate this Policy for
cause immediately upon written notice for thefollowing:
a. Material information that is false or misrep-resented information provided on the en-rollment application or given to the Plan;
b. Permitting use of your Insured identifica-tion card by someone other than yourself toobtain Services;
c. Obtaining or attempting to obtain Servicesunder this Policy by means of false, materi-ally misleading, or fraudulent information,acts or omissions; or
d. Abusive or disruptive behavior