Embed Size (px)
Citation preview

1
Barriers and Facilitators experienced while Barriers and Facilitators experienced while developing and implementing Athena-developing and implementing Athena-
Hypertension in VISN 1Hypertension in VISN 1
Views expressed are those of the speaker and not necessarily those of the Department of Veterans Affairs or other funding agencies or affiliated
institutions
Working with health care systems to translate research into practice
Mary K. Goldstein, MD Director, GRECC, VA Palo Alto Health Care SystemProfessor of Medicine (PCOR), Stanford University

2
Organizational Project TeamOrganizational Project Team
Acknowledgements– VA HSR&D and National Library of Medicine– Sociology colleagues for organizational component
• Ruth Cronkite, PhD; Dick Scott, PhD (and Grace Yeh)– The many participants in ATHENA development and
evaluation over years including• Co-PI Brian Hoffman, MD, VA Boston• Knowledge representation Samson Tu, Stanford Biomedical
Informatics Research (BMIR)• Site PI’s • Statistical consultants Phil Lavori, Alex Sox-Harris, Tyson
Holmes• Other team members at VAPAHCS Bob Coleman, Susana
Martins, and others

3
Translating Research into PracticeTranslating Research into Practice
Basic research
ClinicalEfficacy
trials
Change inRoutinepractice
Health ofpopulation
Animal studies,Single human,
Phase I trials, etc
Single-site;Multisite;
+/- meta study
“17 year”Translation
delay
TRIP I TRIP II

4
The “Quality Chasm”The “Quality Chasm”
Institute of Medicine (IOM) report on Crossing the Quality Chasm*Health care system must improve in– Patient safety, evidence-based practice
Improvability gaps between best practices and actual practiceInformation technology (IT) can support quality improvement– But IT is underutilized in clinical setting
* Crossing the Quality Chasm: A new health system for the 21st century. National Academy Press, 2001

5
VA HSR&D QUERIVA HSR&D QUERI
Quality Enhancement Research Inititative (QUERI)– “data-driven, outcomes-based, quality
improvement program…to achieve better health outcomes for veterans”
– “Particular emphasis is given to the documentation of best practices, implementation strategies, and dissemination”
– www.hsrd.research.va.gov/queri

6
QUERI ProcessQUERI Process
QUERI Steps1. identify high-risk/high volume disease or problems2. Identify best practices3. Define existing practice patterns and outcomes and
current variation from best practices4. Identify and implement interventions to promote
best practices5. Document that best practices improve outcomes6. Document that outcomes are associated with
improved health-related quality of life

7
Hypertension and QUERI StepsHypertension and QUERI Steps
We started pre-QUERI in 1997…can fit into the QUERI Steps retrospectively
We selected hypertension as a model for the study of guideline implementation becauseHypertension highly prevalent in adult medical practice (QUERI Step 1)Excellent evidence-based guidelines for management (QUERI Step 2)Evidence that the guidelines were not well-followed (QUERI Step 3)

8
Hypertension and Step 4Hypertension and Step 4
In 1997 when we started (pre-QUERI)– Known lack of impact of guidelines
• “Do Guidelines Guide Practice”
– Awareness to adherence model
Interventions first identified– Clinical reminders
First study in series implemented reminders (Step 4) and documents improved practice (Step 5) (next slide)

9
More “Diagnosis/Needs Assessment”More “Diagnosis/Needs Assessment”
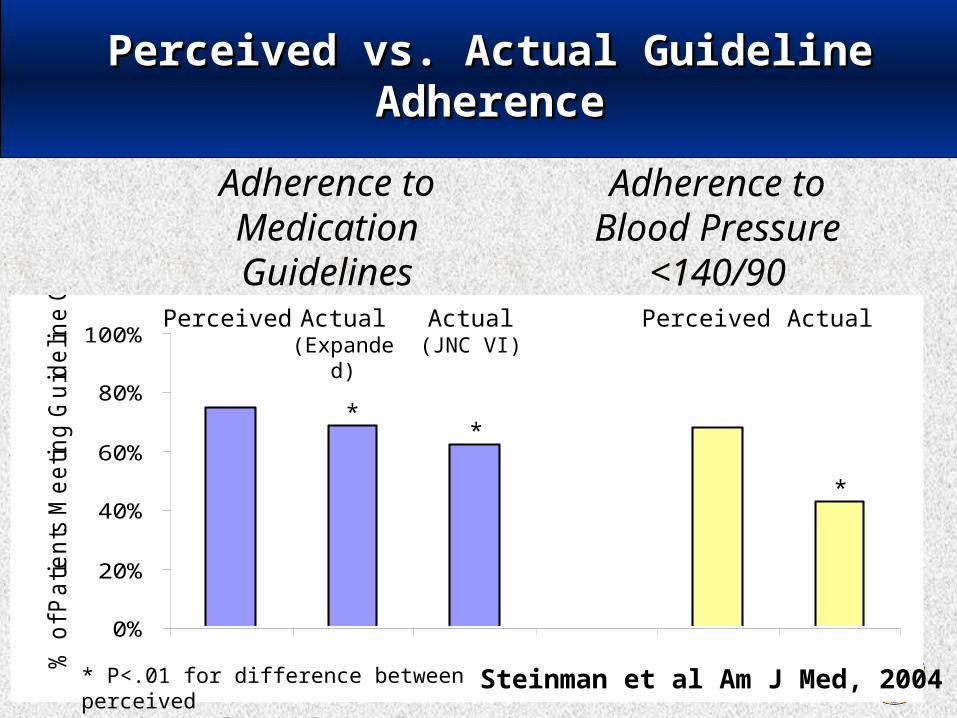
Are primary care clinicians aware of whether or not their own prescribing for hypertension adheres to guideline recommendations?
– Combined clinician questionnaire and patient data extracts to compare perceived with actual adherence to hypertension guidelines
10
0%
20%
40%
60%
80%
100%
% o
f P
atie
nts
Me
etin
g G
uid
elin
e G
oa
ls
Adherence to Medication Guidelines
Adherence toBlood Pressure
<140/90Perceived Actual
(Expanded)Actual
(JNC VI)Perceived Actual
Perceived vs. Actual Guideline Perceived vs. Actual Guideline AdherenceAdherence
**
*
* P<.01 for difference between perceived and actual guideline adherence
Steinman et al Am J Med, 2004

Change in % Guideline Change in % Guideline Concordance for CliniciansConcordance for Clinicians
Individualized Study Group
40%
50%
60%
70%
80%
90%
100%
Baseline After
General Study Group
40%
50%
60%
70%
80%
90%
100%
Baseline After
Perc
ent C
onco
rdan
t
General Individualized
GuidelineConcordanceIncreased11% in InterventionVs 3.8% in Control p<0.01)
Goldstein et al Am J Mgd Care 11:677-85;2005

Conceptualization of Impact of Conceptualization of Impact of Decision Support SystemDecision Support System
Clinician Prescribing
Treated Patients’ BP
Journals Peers
Pharmaceutical Marketing Guidelines
Clinical Decision Support System
Lifestyle choices: diet, exercise, smoking
Competing comorbidities
Medication adherence Individual
response to therapy

13
Desirable Features of Automated Decision SupportDesirable Features of Automated Decision Support
Integrated into clinical workflow
Requires access to separate system
Requires separate data entry
Uses existing electronic data
Transferable to diverse EMRs
Limited to single EMR
Presents explanation / evidence-base for recommendations
No explanation or evidence presented
Complex logic and reasoning
Limited to simple rules
Knowledge easy to browse/update
KnowledgeIn code

14
Decision Support for Common Decision Support for Common Chronic DiseasesChronic Diseases
The “Field of Dreams” approach to medical informatics implementations:
If you build it, they will come
The physician often seen as wondering about a clinical question and then seeking out decision support:

15

16
See also Goldstein and Hoffman, in AHA Hypertension Primer, J.L. Izzo, Jr and H.R. Black, Editors. 2003, Williams & Wilkins: Baltimore.

17
ACPACP
BMJ Clinical Evidence
Reprinted with permission BMJ Publishing
Group

18
Developing ATHENA-Hypertension Developing ATHENA-Hypertension Knowledge BaseKnowledge Base * *
Built with Protégé– open-source Java tool for creation of customized
knowledge-based applications• Developed at Stanford Medical Informatics (SMI)…
now Stanford Biomedical Informatics Research (BMIR)
– http://protege.stanford.edu/overview/
* Goldstein et al Proc AMIA 2000

ATHENA Protégé top levelATHENA Protégé top levelATHENA Hypertension
Drug classes
Patient riskcategories
Blood Pressure Targets
20
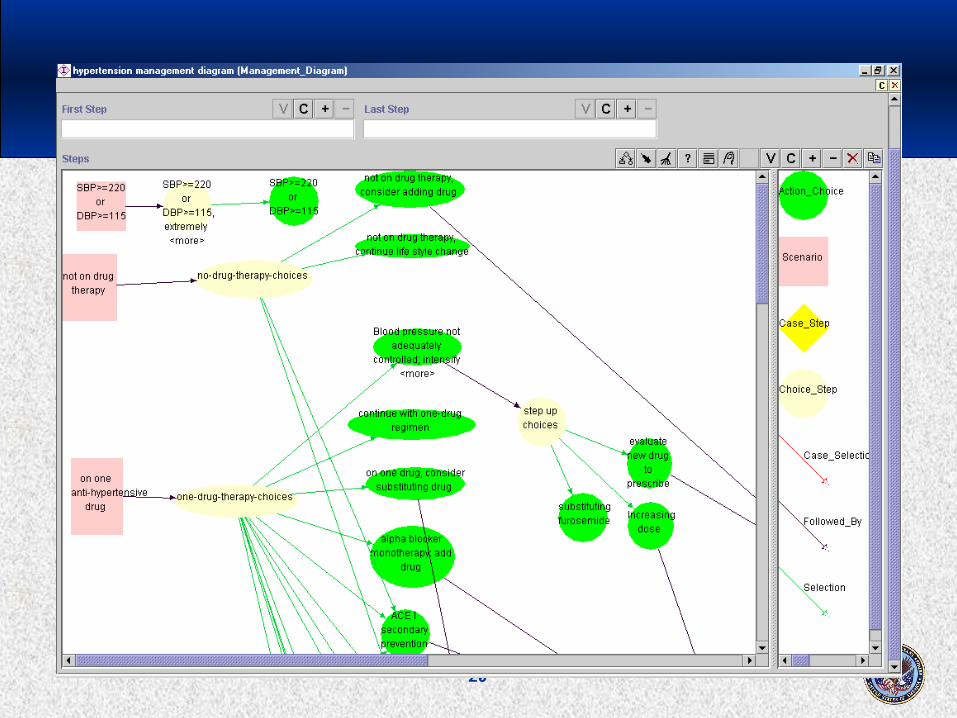
ATHENA Protégé ATHENA Protégé GL managementGL management
diagramdiagram

21
Electronic Medical RecordSystem Patient Data
ATHENA ArchitectureATHENA Architecture
VISTAhierarchical
Database in M
CPRS
ATHENA HTN Guideline
Knowledge Base
GuidelineInterpreter
Treatment Recommendation
SQL Server: Relational databaseData Mediator

22
Implementing in ClinicsImplementing in Clinics
VA as site for demonstration/implementation– Electronic health record in place (CPRS)– VA organizational interest in quality improvement
Established technique for generating popup windows within the CPRS-GUI windowDesigned system for extracting patient dataTime testing for popup windowAttention to organizational contextEarly deployments at remote sites rapid (eg Durham)
Goldstein et al Translating research into practice.
J AMIA 11:368-76; 2004.

23
Sites for First Clinical Trial 2002Sites for First Clinical Trial 2002
Palo Alto (in 7 cities), San Francisco, and Durham VAMC’s (total 9 separate sites)91 clinician-clusters – 47 ATHENA– 44 Active control
34,427 visits of 11,473 patients
San Francisco VA, San Francisco VA, CACA
Palo Alto VA, Palo Alto VA, CACA
Durham VAMC, Durham VAMC, North CarolinaNorth Carolina

24
Server-ClientServer-Clientnumber of client computers (n)number of client computers (n)
VA SF Clinics
VA Palo Alto Clinics
Server in Palo Alto, CA
Durham VA Clinics
Server in Durham, NC
n = 193
n = 40
n = 118

25
Organizational Context:Organizational Context:Working with StakeholdersWorking with Stakeholders
Primary CareProviders
Office of Information and Technology
Clinical Applications Coordinators
Admin/Clinical Mgrs
programming
networking
Clinic computerSupport staff

26
Next Step: VISN CollaborativeNext Step: VISN Collaborative
Three-site study did not establish Step 5– Improved processes but did not document
improved outcomes
Larger study with 5 medical centers– QUERI VISN collaborative funding mechanism
• link clinical with research• Required VISN leadership co-PI
•Track organizational activities– Part of project plan

27
Two Organizational Structures for Two Organizational Structures for the Studythe Study
As usual for clinical trials, a site-PI and structure for managing participants within sitesA second structure for the IT deployment– IT contacts
28
IT Deployment Steps IT Deployment Steps
To implement ATHENA, IT staff from each center installs:
– 1) The M program that extracts patient data. This program consists of the KIDSBUILD.
– 2) Connections to the ATHENA server on computers used in primary care.
29
ATHENA Extract
installed
FTP file transfers into
SQL database
ATHENA client starts
System Recognizes
user
Rich Client Computer Names
Obtained
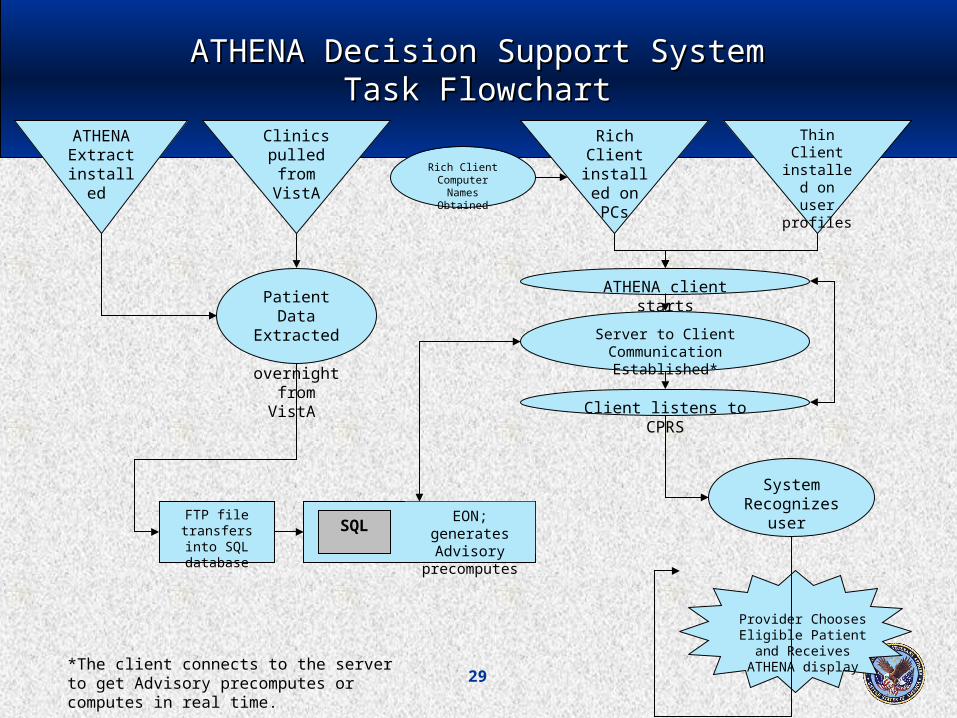
Patient Data Extracted overnight
from VistA
ATHENA Decision Support SystemATHENA Decision Support SystemTask FlowchartTask Flowchart
Thin Client installed on
user profiles
Rich Client
installed on PCs
Clinics pulled
from VistA
SQLEON; generates
Advisory precomputes
Server to Client Communication
Established*
Client listens to CPRS
*The client connects to the server to get Advisory precomputes or computes in real time.
Provider Chooses Eligible Patient and Receives ATHENA
display

30
Collaboration between research, CIO and Collaboration between research, CIO and IRMS programmer: Time to installIRMS programmer: Time to install
Task: Installing the ATHENA Extract The IRMS team at each medical center has to install the ATHENA extract program. An installation takes 6-8 hours to completeThe same ATHENA client installed in the start-up folder of rich client PCs is installed in the Start menu of the user’s profile on all the thin client servers.
0
5
10
15
20
25
Du
rati
on
(M
on
ths)
site1 site2 site3 site4 site5
install extract
install client
Site 5 has installed but still problems

31
Task: Obtaining correct computer Task: Obtaining correct computer names for rich clientsnames for rich clients
To install the shortcut on each computer, we needed computer namesSince there was no computer name list available to the ATHENA, an RA went to each site to collect all computer names in the primary care clinics This process took more than 1 year and several trips to each siteExample issue– Initial computer list developed but later a PC upgrade. Initial
list includes “a lot of neoware thin clients” no longer some other computers that are no longer there

32
Site computer changesSite computer changes
Site 1 thin clients rich clientsSite 2 thin clients rich clientsSite 3 rich clientsSite 4 mixture of thin and rich clientsSite 5 thin clients

33
Months to start trial from February 2006Months to start trial from February 2006
0
5
10
15
20
25
30
35
Du
rati
on
(M
on
ths)
site1 site2 site3 site4 site5
expected startdate
actual start
Site 5 has not started to date

34
No access to CPRS/VistA; resulting No access to CPRS/VistA; resulting effects on validation effortseffects on validation efforts
Groups involved in project
Site P.I.
Consultants
LabManagers
Their tasksATHENA Team Summary of Effects
•Prepare pt documents for Site P.I. to pull CPRS data•Validate pt data and f/up•Administer several rounds of validations when needed
•Access CPRS and update pt documents•Confirm differences between data sources
•Prepare pt documents for lab managers to verify LOINC codes•F/up once new LOINC codes were entered
•Direct technical questions to experts•Coordinate communication between various sites and consultants
•Validate LOINC codes and identify source of discrepancies
•Address questions with technical knowledge•Communicate with research team and sites
•Primary role of lab managers didn’t include our tasks and no funding provided•Time required to thoroughly validate lab discrepancies was increased
•Research team unable to act until response obtained from experts•Scheduling between sites and consultants resulted in slow responses to issues
•Delays up to 2 ½ months awaiting Site P.I. responses•Additional rounds of validations administered due to lapses in communication

35

36
Hiring a programmer: Hiring a programmer: New Features under DevelopmentNew Features under Development
• Write back capacity to VISTA:• Vitals• Notes
• Updated recommendations based on patient’s data
• Wish list: integration with computerized physician order entry

37
Reorganization of Research and OI&T: Reorganization of Research and OI&T: challenges to hire a Programmerchallenges to hire a Programmer
Dec 0
6 Pro
gram
mer
Inclu
ded
in IT
spe
ndin
g
plan
Sept 0
8, E
nd
of F
Y08
Meetings with high level official required for spending approval cancelled due to priorities. Official approved funds incorporating recommendations verbally in August meeting (4/07-8/07).
Initial request submitted to VA Central Office OI&T for programmer (1/07-3/07).
Funding approval stalled and FY07 funds were lost (9/07).
Begin
FY08
Requests for allocating IT funds for FY08 were redirected to various officials unsure who has authority to approve programmer (10/07-03/08).
Insufficient time to hire programmer even with approval prior to losing funds at end of FY08.
Approval of Project Modification providing IT funds to hire programmer (12/06).

38
Knowing and DoingKnowing and Doing
“If to do were as easy as to know what were good to do, chapels had been churches and poor men's cottages princes' palaces.”
Portia, Act I, Merchant of Venice, Shakespeare

39
The Team…early on…The Team…early on…
ATHENA Project Leadership– Mary Goldstein, MD, MSc and Brian Hoffman, MD (Co-PIs), VA Palo Alto
Health Care System and Stanford University Dept of Medicine• Brian now at Harvard Med Schl and VA West Roxbury/Boston
ATHENA Decision Support System Development– Stanford Medical Informatics EON Group
• Mark Musen, MD PhD; Samson Tu, MS; Ravi Shankar,MS; Martin O’Connor, MS; Aneel Advani, MD MPH
– ATHENA Group at VA Palo Alto and Stanford• Bob Coleman, MS Pharm; Susana Martins, MD, MSc; Parisa Gholami, MPH
Randomized Clinical Trial using ATHENA DSS as intervention– Phil Lavori, PhD, Biostatistician – Eugene Oddone, MD; Hayden Bosworth, PhD; and Michael Shlipak, MD:
investigators at VAMCs Durham and San Francisco

40
More of the Team…More of the Team…
Fellows/Resident– Patient Safety; computing active meds: Albert Chan, MD– Offline testing: S. Nicki Hastings, MD (former primary care chief
resident) – Accuracy of computer diagnoses related to HTN: Herb Szeto, MD– Clinician Questionnaire Study: Melissa Fischer, MD; Michael
Steinmann, MD (UCSF)– Provider barriers to GL adherence: Nancy Lin, ScD
Physician offline and clinic testing and monitoring– Lars Osterberg, MD; Howard Strasberg, MD; and others
Web pages for evidence displays– Emory Brock, MS
Assistance with Defining Knowledge Base – See Rules document for list of subspecialists
VISN 1 team (MAVERIC); Tyson Holmes statistics; et al!!
41
Funding SourcesFunding Sources
Development of ATHENA DSS– NLM LM05708 (PI: Musen) for development of EON architecture and
collaboration on building ATHENA DSS, built with EON Technology for guideline-based decision support systems
– VA HSR&D Career Development Award for Dr. Goldstein’s time; VA Palo Alto Health Care System for other staff time
Implementation and Clinical Trials– VA HSR&D CPI 99-275 (PI: Goldstein/Hoffman) – VA HSR&D IMV 04-062 VISN Collaborative for Improving Hypertension
Management with ATHENA-HTN.
Overall– VA support for staff

42
Stanford UniversitySchool of Medicine

43
Data SecurityData Security
Passwords must be changed in FTP every 90 days. We do not have full accessPassword changes must be coordinated with VISN1 so system does not go down.

44
END OF PRESENTATIONEND OF PRESENTATION
Following slides were removed from RIP presentation due to length of QUERI presentation
•These slides were placed at the end of the slideshow in the same order as they appear in the original slideshow. The Title of the slide that came before each group of slides is listed on the first slide of each group which is color coded by group.

45
Knowing and DoingKnowing and Doing
“If to do were as easy as to know what were good to do, chapels had been churches and poor men's cottages princes' palaces.”
Portia, Act I, Merchant of Venice, Shakespeare

46
Methods:Methods:Conceptual frameworkConceptual framework
Developed by Cabana et al (1999)
Knowledge Attitudes Behavior
Lack of familiarity
Lack of awareness
Lack of agreement
Belief that action will not lead to better outcomes
Inertia of previous practice
External factors Patient Environmental Other guidelines
Examplesof barriers

47
Conceptualization of Impact of Decision Conceptualization of Impact of Decision Support SystemSupport System
Clinician Prescribing
Treated Patients’ BP
Journals Peers
Pharmaceutical Marketing Guidelines
Clinical Decision Support System
Lifestyle choices: diet, exercise, smoking
Competing comorbidities
Medication adherence Individual
response to therapy

48
Public’s View of Public’s View of Why We Fund ResearchWhy We Fund Research
Basic research
Clinicaltrials
Change inroutinepractice
Health ofpopulation
Slide prior to this group - Organizational Project Team

49
Progression of Study TypesProgression of Study Types
Basic research
ClinicalEfficacy
trials
Change inRoutinepractice
Health ofpopulation
Animal studies,Single human,
Phase I trials, etc
Single-site;Multisite;
+/- meta study
“17 year”Translation
delay

50
Translating research into practice Translating research into practice (TRIP)(TRIP)
Two areas of translation in CTSA– TRIP I
• Process of applying discoveries generation during research in the laboratory and in preclinical studies
– TRIP II• Research aimed at enhancing the adoption of best
practices in the communityCost-effectiveness of prevention and treatment strategies is part of translational science

51
Clinical and Translational Science Clinical and Translational Science Awards (CTSA)Awards (CTSA)
NIH Roadmap for Medical ResearchCTSA Launched October 2006“Definable academic home for the discipline of clinical and translational science at institutions across the country”
• development of novel methods and approaches to clinical and translational research
• Informatics and technology resources• Improved training for new investigators to “navigate
the increasingly complex research system”

52
Two HTN ProjectsTwo HTN Projects
Automated clinical decision support– ATHENA-HTN
Group Visits (shared medical appointments)

53
Will it Be Used?Will it Be Used?
Once decision support is integrated technologically, will clinicians use it? Many clinical decision support systems are used only a tiny percent of time available
• For example, physicians viewed a hyperlipidemia guideline only 20 of 2610 visit opportunities (0.8%)
– Maviglia SM, Z.R., Paterno M, Teich JM, Bates DW, Kuperman GJ, Automating Complex Guidelines for Chronic Disease: Lessons Learned. J Am Med Inform Assoc, 2003. 10: p. 154-165.
– note that even infrequent use may still be beneficial, at very low cost

54
Clinician Interactions Clinician Interactions with ATHENA Advisorywith ATHENA Advisory
87/91 Clinicians interacted with 52% (10,740/20,524) of ATHENA AdvisoriesFocusing on survey responders:– 44/77 survey responders interacted with
60% (7,417/12,349) of ATHENA Advisories

55
Time Trend in Use at Visits: Time Trend in Use at Visits: New BP EnteredNew BP Entered
Percentage of ATHENA Hypertension Advisories with a Blood Pressure Update
0%
5%
10%
15%
20%
25%
30%
35%
40%
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Month
Pe
rce
nt
of
Ad
vis
ori
es
Dis
pla
ye
d t
ha
t h
ad
a
BP
Up
da
te

56
Evaluation of Clinician ReactionEvaluation of Clinician Reaction
Clinicians used the system extensively• Data logged by system
– Speaks to usability and usefulness
Clinicians reported ATHENA-HTN affected their prescribing decisions– Questionnaire data
57
Athena Survey ResultsAthena Survey Results
Response rate: 57% (44/77)
Ease of Navigation: 80% (35/44) good or excellent64% (28/44) reported they updated the blood pressure in the ATHENA advisory often or occasionally.

58
Group Medical Visits to Improve HypertensionChronic Disease Managment

59
Our Model of Group VisitsOur Model of Group Visits
Group visit conducted by the primary care provider (PCP) with patients from his/her own panel of patients
Patient-Centered– Recognizes that whatever physician prescribes it is
patient who follows the diet and exercise regimen, takes the medication
• Based in part on Bandura self-efficacy
– Aims to enhance patients’ self-efficacy for self-management of their chronic disease
60
Group Visit FindingsGroup Visit Findings
Group medical visits for patients with hypertension yielded higher rates of blood pressure control as compared with control groups– most apparent for patients whose BP was not
meeting target BP at baselinePatient satisfaction high in all groups – improved more among the Group Visits patients as
compared with the control groups

61
Knowing and DoingKnowing and Doing
When we move from knowing to doing, must study the effect (QUERI Steps 5 and 6):
does implementing the best practices improve outcomes?are the outcomes associated with improved HRQOL?are there unintended consequences?

62
Quality Improvement ApproachQuality Improvement Approach
Solution-Driven Approach– In contrast to D/NA, this approach often characterizes QI
• Identify an innovation or research finding• Work toward rapid diffusion
– Examples• Clinical practice guidelines• CQI
As evaluations of implementations are done– Greater appreciation of contribution of context to
successful implementation of QI

63
MVK ISO approval certificateMVK ISO approval certificate and re-push and re-push
After obtaining permission to push, we pushed to an old server.We had not obtained official permission to use the new server and, as a result, had to repush again to the computers in sites 1-3.












![[XLS]SimLEARN-VISN Programs, Department of Veterans · Web viewDatabase listing medical simulation training courses/classes available in each VA VISN](https://img.pdfslide.net/doc/110x75/5aac9d9d7f8b9a2e088d36f5/xlssimlearn-visn-programs-department-of-veterans-viewdatabase-listing-medical.jpg)














![ATHENA - Coordinate System Document...[RD02] ATHENA Mission Requirements Document (MRD), ATHENA-ESA-URD-0010 [RD03] ATHENA Product Tree, ATHENA-ESA-PT-0001 [RD04] Ariane 5 User’s](https://img.pdfslide.net/doc/110x75/5ff23cd84225de2c7f4f21b6/athena-coordinate-system-document-rd02-athena-mission-requirements-document.jpg)