Embed Size (px)
Citation preview

1
Componentsof a Learning Health Care System
Denis A. Cortese, MD
BPC Health Care Reform EventApril 24, 2008

2
Pay for value
Value*
Individ-
ualized
Medicine
Science
of Health
Care Delivery
Integration and coordination
*Value = Quality/Cost = Outcomes, Safety, Service/Cost Over Time

3
Pay for Value
• Pay for results, outcomes, value,not process compliance
• Purpose for process is to achievebetter value
(outcomes, safety, service)(outcomes, safety, service)
Value =Value =
Cost over a span of careCost over a span of care
QualityQuality

Translational
Research
Translational
Research
Basic
Research
Basic
Research
Clinical
Practice
Clinical
Practice
New
Clinical
Practice
New
Clinical
Practice
Innovation
(New Idea, Old Idea,
New Way)
Innovation
(New Idea, Old Idea,
New Way)
Time, people and capital
Val
ue
Translational EducationTranslational Education
Increasing Value in Health Care
4

Translational
Research
Translational
Research
Basic
Research
Basic
Research
Clinical
Practice
Clinical
Practice
New
Clinical
Practice
New
Clinical
Practice
Innovation
(New Idea, Old Idea,
New Way)
Innovation
(New Idea, Old Idea,
New Way)
Time, people and capital
Val
ue
Translational EducationTranslational Education
En
terp
rise
Lea
rnin
g
Sy
ste
m
En
terp
rise
Lea
rnin
g
Sy
ste
m
Individualized Medicine
Science of Health Care Delivery
Integration
Increasing Value in Health Care
5

6
Pay for value
Insurance for all
Value*
Individ-
ualized
Medicine
Science
of Health
Care Delivery
Integration and coordination
*Value = Quality/Cost = Outcomes, Safety, Service/Cost Over Time

7
Mayo Clinic Health Policy Center
Goal
Influence stakeholders to implementsubstantive health care reform before 2011that will enhance quality and availabilityof health care for all patients
Role
Convening body

8
Mayo Clinic Health Policy Center• 10 sectors
• 800 people
• 400 patient comments – 9-city tour
• 1000 patients surveyed

9
MCHPC Cornerstones
Coordinated care Value
Insurance
for all: FEHBP
model
Payment reform

10
Health Policy Center Action Steps:Public Sector• Insurance for all
• Ensure/mandate insurance coverage for all
• Interoperable EMR• Require all providers to have interoperable EMRs within
a certain time (5 years) with patient accessibility
• Federal Health Board/Reserve• Implement an independent board to set rules/standards
to promote value in health care
• Care coordination • Reward care coordination
• Pay for value• Direct Medicare to pay for value/outcomes/prevention
using innovative payment models

11
Insurance for All
• FEHBP – Model• All people own insurance; All participate• Employers can purchase all or some• Government help finance in sliding scale• All insurers take All patients• No pre-existing condition exclusions• Adjust for initial conditions• Sunset Medicare and Medicaid

12
If Medicare Continues…Mayo Clinic Calls for Major Changes:• Congress must be out as BOD
• Stop price controls in exchange for provider pricing transparency on a set of common visits/procedures/tests and quality
• Pay for value• Focus on results ▫ O,S,S, and Cost over span of care• UHC ▫ Dartmouth Atlas ▫ NQF ▫ Leapfrog ▫ AHRQ
• Let patients pay more if they chose
• Coverage with evidence development
• Allow comparative effectiveness considerationsin benefit design and coverage decisions

13
Pay For Value: Concepts
• FFS with reward for good outcomes
• FFS with shared savings
• Shared decision making
• Episode based payments
• Chronic disease coordinator payment

14
Role for President
• Learning Organization
• Value: O,S,S, / Cost over Time
• Insurance for all
• Pay for value

15

16
5,500 6,000 6,500 7,000 7,500 8,000 8,500 9,00020
30
40
50
60
70
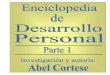
Medicare Spending** and Quality of Care*
*Quality from “National Health Quality Report, 2006” by AHRQ
**Cost from Medicare Health Expenditures by State 2004, CMS website (www.cms.hhs.gov)
Medicare personal health care spending per enrollee
Quality
score
LA
MS
OK
TX FL
AR
VA
ID
CT
MA
MDNJ
CO
NE
MNWI
NH
ME
SD ND
HI IA VT
UT
Best quality – Lowest cost
Lowest quality – Highest cost

17
0.4
0.6
0.8
1.0
1.2
1.4
1.6
1.8
0 10 20 30 40 50 60
Teaching Hospital Variability in Value
Good
Effectiveness
Good
Efficiency
Good
Effectiveness
Good
Efficiency
Good
Effectiveness
Poor
Efficiency
Good
Effectiveness
Poor
Efficiency
Poor
Effectiveness
Good
Efficiency
Poor
Effectiveness
Good
Efficiency
Poor
Effectiveness
Poor
Efficiency
Poor
Effectiveness
Poor
Efficiency
Cost in last 6 months of life ($000s)Cost in last 6 months of life ($000s)
Case mix
adjusted
mortality
(>1 is better)
Case mix
adjusted
mortality
(>1 is better)
AA BB
CC DD
RewardReward
Incent
to move
to upper left
Incent
to move
to upper left