Embed Size (px)
Citation preview

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 1/61
.1 HEPATIC AMOEBIASIS, GENERAL
If amoebae are transported with the venous blood from the intestinal wall to theliver, an abscess in the liver may be formed: hepatic amoebiasis. If the abscess is
located adjacent to the fibrous capsule of the liver, adhesions are formed. Asubphrenic abscess is less frequent than direct perforation of the diaphragm withempyema or fistula formation to the bronchi. Perforation to the peritoneum israre. Perforations of the intestine, biliary ducts or navel with secondaryphagedenic ulceration of the skin are more frequent than generalised peritonitis.Abscesses of the left hepatic lobe may perforate the pericardium in a life-threatening manner. [The term "abscess" is not actually correct here in thestrictest sense, because this is not a collection of pus cells (white blood cells). It islocal cytolysis of liver tissue.]
6.2 HEPATIC AMOEBIASIS, CLINICAL ASPECTS
Upon physical examination there is fever and pain in the liver region (pain uponpalpation or percussion). The pain increases during deep inspiration or coughing.If the volume of the abscess is significant, the liver will be enlarged and the jdiaphragm will be elevated (percussion, auscultation, chest X-ray). The patientmay develop pain in the right shoulder (referred pain). Dullness upon percussionof the base of the right lung may be due to the elevation of the diaphragm, to
Liver amoebiasis withperforation of the abscess
through the abdominal skin.Photo Prof. Gigase. CopyrightITM
Liver amoebiasis withperforation of the abscess
through the abdominal skin.Photo Prof. Gigase. Copyright
ITM

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 2/61
reactive pleural fluid or breakthrough to the pleura, or to atelectasis of the lung.Jaundice is only a very late symptom. The abscess continues to spread until thereis breakthrough to the surroundings: the pleura (empyema), the lung, thepericardium or the skin. If fistulisation to the skin occurs, there may be swiftprogression of a painful skin ulcer. Death follows if not treated.
6.3 HEPATIC AMOEBIASIS, DIAGNOSIS
The diagnosis of a hepatic abscess may be suspected from clinical findings.Leukocytosis will be high. Ultrasound and serology (ELISA, Latex agglutination)can confirm the diagnosis, but are often not available. Antibodies will remainpresent for a long time -often years- after infection. An amoebic abscess of theliver will contain necrotic liver tissue at its centre. Upon aspiration this often has adark brownish red colour called "anchovy " or "chocolate" pus, but the pus may
also be yellow, grey or greenish. The pus has no offensive odour, unlike mostbacterial (anaerobic) abscesses, which is an important difference. The wall of theabscess contains trophozoites, but the necrotic liver tissue itself does not. Thepresence of local oedema or bulging of the skin with or without fluctuation,indicates the proximity of the abscess and the site where a puncture can becarried out. In case of doubt a trial therapy quickly produces a spectacularimprovement. Fewer than 20 % of people with a hepatic abscess have Entamoeba
histolytica in the faeces. The absence of amoebae in the stools is therefore not astrong argument against the diagnosis.
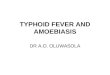
Entamoeba histolytica.Echography liver showing an
amoebic liver abscess.Copyright ITM
Liver abscess due toinfection with Entamoebahistolytica. CT-scan of the
liver shows a circular necroticarea. Copyright ITM
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 3/61
6.4 HEPATIC AMOEBIASIS, DIFFERENTIAL DIAGNOSIS
Pyogenic anaerobic hepatic abscess: stinking pus, poor general condition,often icterus, negative serology, sometimes portal-of-entry in the intestine(e.g. colon tumour).Subphrenic abscess: sometimes a history of peritonitis or surgery, possiblypleural fluid, negative serology.Hydatid cyst: slow development, no fever, no toxaemia, serology positive forEchinococcus, sometimes calcifications on abdominal X-ray, no leukocytosis.Ultrasound may show daughter cysts.Biliary cysts: ultrasound shows a thin wall and the content is anechoic,otherwise asymptomatic.Haemangioma: hyperreflective on ultrasound, otherwise asymptomatic. OnCT scan with dynamic sequences there is a centripetal staining with a delayedisodense appearance to the surrounding liver tissue. On MRI a haemangioma is
extremely hyperreflective on T2-weighted images (T2 = "water images").Metastases: ultrasound shows generally (but not necessarily) irregular andhyperreflective structure, central necrosis may occur. Frequently peripheraloedema.Hepatoma: no fever or toxaemia, no response to trial therapy, elevatedalpha-foeto protein, negative serology, biopsy is diagnostic.
6.5 HEPATIC AMOEBIASIS, TREATMENT
An amoebic abscess of the liver is treated with metronidazole for 10 days (ofteninitially IV), followed by diloxanide furoate for 10 days. The latter is to destroyany amoebae in the lumen of the intestines. Chloroquine is moderately active onliver abscesses and may in some cases be administered. If the diagnosis isknown, aspiration is only carried out for very large abscesses or if there is a riskof breakthrough. Surgery is indicated if the abscess ruptures (e.g. into theperitoneum). If a relapse of the abscess occurs this will usually happen within twomonths.
*
In case of resistance to metronidazole the quite toxic drug emetine may beused. Emetine is administered by deep intramuscular or subcutaneous route: 1mg/kg/day with maximum of 60 mg/day. Emetine has been used since 1912 inthe treatment of amoebiasis. It is an alkaloid from the roots and rhizomes of ipecac (Cephaelis ipecacuanha (Brazil) and C. acuminata (Central America andColombia). These shrubs belong to the plant family of Rubiaceae and are alsoknown as Uragoga ipecacuanha or Psychotria ip. The plant was known in earlier
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 4/61
times. In 1682 the son of the French king Louis XIV recovered from severedysentery after taking extracts of this plant. The active alkaloid was identified in1817.
Emetine induces nausea and vomiting, from which it has its name, and is only
rarely administered orally. After parenteral administration absorption is rapid, butexcretion is slow. Traces of emetine can still be recovered in tissues up to 60 daysafter a treatment.
Tachycardia and dizziness after a single administration are signs of hypersensitivity to the drug. Emetine is cytotoxic, including for the myocardium.Signs of intoxication are as follows:
Nausea, vomiting and diarrhoea, although occurrence of these does not meanthat the treatment has failed.Palpitations, tachycardia, retrosternal pain, hypotension, dyspnoea, ECG
changes (ST depression, QT prolongation, T-wave inversion). The ECG returnsto normal 1 to 2 weeks after discontinuation of the injections.Asthenia, tremor, myasthenia and paralysis including respiratory paralysis.
Treatment must not be repeated within six weeks following the initial treatment.Emetine must not be combined with other drugs which are toxic for themyocardium. The drug is preferably administered by deep subcutaneous injectionand this is painful. IM administration may result in muscle necrosis which healsslowly and may lead to formation of fistulae and permanent scars. The drug is notadministered IV. Contraindications are organic heart disease and conditions of
advanced asthenia. The treatment is not without risk in children and the elderly,and in debilitated or undernourished patients. Admission and strict bed rest arenecessary. Emetine is very effective in amoebic dysentery and amoebic abscess of the liver, but contact amoebicides should be used to supplement the treatment.
*
Dehydroemetine is better than emetine. Dehydroemetine is a semi-syntheticproduct with is more rapidly eliminated and has fewer side-effects. Recommended
Chemical structure of dehydro-emetine. Used insecond line treatment of amoebiasis (Entamoeba
histolytica) and fasciolasis(Fasciola hepatica). Copyright
ITM

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 5/61
doses are between 1 mg/kg/day IM for 5 days and 2 mg/kg/day (maximum 90mg/day) for not more than 15 days (two injections daily). Oral administration issometimes recommended
tsetse fly
Help us provide free content to the world by donating today!
Tsetse fly
FROM WIKIPEDIA, THE FREE ENCYCLOPEDIA
Jump to: navigation, searchThis page is about the insect. For other meanings, see Tsetse (disambiguation). Tsetse fly (Glossina)

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 6/61
Scientific classification
Kingdom: Animalia
Phylum: Arthropoda
Subphylum: HexapodaClass: InsectaSubclass: Pterygota
Infraclass: Neoptera
Superorder: Endopterygota
Order: Diptera
Suborder: BrachyceraSubsection: Calyptratae
Superfamily: Hippoboscoidea
Family: GlossinidaeTheobald, 1903
Genus: GlossinaWiedemann, 1830
Species groups
• morsitans ("savannah"species)
• fusca ("forest" species)
• palpalis ("riverine" species)Tsetse (pronounced /ts/e-/ts/e, teet-SEE, or set-see, alternatively spelled tzetze
or tsetze) are large biting flies from Africa which live by feeding on the blood of vertebrate animals. Tsetse include all the species in the genus Glossina, whichare generally placed in their own family, Glossinidae.
Tsetse have been extensively studied because they are biological vectors of theAfrican trypanosomiases, deadly diseases that include sleeping sickness in peopleand nagana in cattle.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 7/61
Tsetse are crudely similar to other large flies, such as the housefly, but can bedistinguished by four characteristics of their anatomy, two of which are easy toobserve. Tsetse fold their wings completely when they are resting so that onewing rests directly on top of the other over their abdomen. Tsetse also have along proboscis which extends directly forward and is attached by a distinct bulb to
the bottom of their head.
Tsetse have existed in the modern morphological form for at least 34 millionyears since fossil tsetse have been recovered from the Florissant Fossil Beds inColorado[1] .
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 8/61
Contents
[hide]
• 1 Systematicso 1.1 Species
• 2 Trypanosomiasiso 2.1 Human trypanosomiasiso 2.2 Animal trypanosomiasis
• 3 Controlo 3.1 Control techniques
3.1.1 Slaughter of wild animals 3.1.2 Land clearing 3.1.3 Pesticide campaigns 3.1.4 Trapping 3.1.5 Releases of irradiated males
• 4 Etymology• 5 See also• 6 References• 7 External links• 8 Resources
o 8.1 Fiction
o 8.2 Scientific books on tsetse and trypanosomiasis
[ edit ] Systematics
Glossina palpalis and G. morsitans from a 1920 lexiconTsetse include up to thirty four species and sub-species depending on theparticular classification used.
Tsetse are sufficiently different in appearance and behavior to have been placed intheir own distinct branch of the flies. This placement is controversial. The scienceof systematics is currently struggling to reconcile the traditional form of biological

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 9/61
classification with the modern understanding of genomic evolution and speciation.The controversy surrounding the placement of tsetse is therefore likely tocontinue into the future.
All current classifications place all the tsetse species in a single genus named
Glossina. Most classifications place this genus as the sole member of the familyGlossinidae. The Glossinidae are generally placed within the superfamilyHippoboscoidea, which contains other hematophagous families. This superfamilyis in the subsection Calyptratae which includes the housefly and the blowfly due tothe similarity of their developmental biology. This infraorder in turn, is part of thesub-order Brachycera, the stubby flies with reduced antenna.
[EDIT] SPECIES
The tsetse genus is generally split into three groups of species based on acombination of distributional, behavioral, molecular and morphologicalcharacteristics. The genus includes [2][3]:
• The savannah flies:(Subgenus Morsitans,occasionally namedGlossina):
o Glossina austeni(Newstead, 1912)
o Glossina
longipalpis(Wiedemann, 1830)
o Glossina morsitanscentralis (Machado,1970)
o Glossina morsitans
morsitans(Wiedemann, 1850)
o Glossina morsitans
submorsitans(Newstead, 1911)
o Glossina pallidipes(Austen, 1903)
o Glossina swynnertoni (Austen,1923)
• The forest flies: (Subgenus Fusca, previously named Austenia):
o Glossina
brevipalpis(Newstead, 1911)
o Glossina fusca
congolensis(Newstead and Evans,
1921) o Glossina fusca
fusca (Walker, 1849) o Glossina
fuscipleuris (Austen,1911)
o Glossina frezili
(Gouteux, 1987)[4] o Glossina
haningtoni(Newstead and Evans,1922)
o Glossinalongipennis (Corti,1895)
o Glossina
medicorum (Austen,1911)
o Glossina nashi(Potts,1955)
• The riverine flies: (Subgenus Palpalis, previounamed Nemorhina):
o Glossina caligin(Austen, 1911)
o Glossina fuscip
fuscipes (Newste1911)
o Glossina fuscip
martinii (Zumpt,1935) o Glossina fuscip
quanzensis (Pire1948)
o Glossina pallic
pallicera (Bigot,1891)
o Glossina pallic
newsteadi (Aust1929)
o Glossina palpal
palpalis (RobineDesvoidy, 1830)
o Glossina palpal
gambiensis(Vanderplank, 191
o Glossina
tachinoides

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 10/61
o Glossina
nigrofusca hopkinsi(Van Emden, 1944)
o Glossina
nigrofusca
nigrofusca(Newstead, 1911) o Glossina severini
(Newstead, 1913) o Glossina schwetzi
(Newstead and Evans,1921)
o Glossina
tabaniformis(Westwood, 1850)
o Glossina vanhoofi
(Henrard, 1952)
(Westwood, 1850)
[ edit ] Trypanosomiasis
Tsetse are biological vectors of trypanosomes meaning that tsetse, in the processof feeding, acquire and then transmit small, single-celled organisms calledtrypanosomes from infected vertebrate hosts to uninfected animals. Some tsetsetransmitted trypanosome species cause trypanosomiasis, an infectious disease. Inhumans, tsetse transmitted trypanosomiasis is called sleeping sickness. Inanimals, tsetse vectored trypanosomiases include nagana, souma, and surra according to the animal infected and the trypanosome species involved, althoughthe usage is not strict and nagana is occasionally used for any form of animaltrypanosomiasis.
Trypanosomes are animal parasites, specifically protozoa of the genusTrypanosoma. These organisms are approximately the size of red blood cells.Different species of trypanosomes infect different hosts as can be seen in thetable attached to this section. Trypanosomes range widely in their effects on thevertebrate hosts. Some species, such as Trypanosoma theileri , do not seem tocause any health problems except perhaps in animals which are already quitesick [5].
Some strains are much more virulent. Tsetse seem to be unaffected by theinfection of trypanosomes but it is entirely possible that the parasites alter tsetsebehavior or have other effects which improve the chances of transmission andsurvival. These trypanosomes have become highly evolved and developed a lifecycle which requires periods in both the vertebrate and tsetse hosts.
Tsetse transmit trypanosomes in two ways, mechanical and biological
transmission.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 11/61
• Mechanical transmission involves the direct transmission of the same individualtrypanosomes taken from an infected host into an uninfected host. The namemechanical reflects the similarity of this mode of transmission to the transmissionwhich could be caused mechanically with a syringe. Mechanical transmissionrequires that tsetse feed on an infected host and acquire trypanosomes in the
bloodmeal, and then, within in a relatively short period, for tsetse to feed on anuninfected host and regurgitate some of the infected blood from the first bloodmeal into the tissue of the uninfected animal. This type of transmissionoccurs most frequently when tsetse are interrupted during a bloodmeal andattempt to satiate themselves with another meal. Other flies, such as horse-flies,also can cause mechanical transmission of trypanosomes [6].
• Biological transmission requires a period of incubation of the trypanosomeswithin the tsetse host. The term biological is used because trypanosomes mustreproduce through several generations inside the tsetse host during the period of incubation, which requires extreme adaptation of the trypanosomes to their tsetsehost. In this mode of transmission, trypanosomes reproduce through several
generations, changing in morphology at certain periods. This mode of transmission also includes the sexual phase of the trypanosomes. Tsetse are believed to be more likely to become infected by trypanosomes during their firstfew bloodmeals. Tsetse infected by trypanosomes are thought to remain infectedfor the remainder of their lives. Because of the adaptations required for biologicaltransmission, trypanosomes which are transmitted biologically by tsetse cannot betransmitted in this manner by other insects.
The relative importance of these two modes of transmission for the propagation of tsetse-vectored trypanosomiases is not yet well understood. However, since thesexual phase of the trypanosome lifecycle occurs within the tsetse host, biological
transmission is a required step in the life cycle of the tsetse vectoredtrypanosomes.
The cycle of biological transmission of trypanosomiasis involves two phases, oneinside the tsetse host and the other inside the vertebrate host. Trypanosomes arenot passed between a pregnant tsetse and her offspring so all newly emergedtsetse adults are free of infection. An uninfected fly which feeds upon an infectedvertebrate animal may acquire trypanosomes in its proboscis or gut. Thesetrypanosomes, depending on the species, may remain in place, move to adifferent part of the digestive tract, or migrate through the tsetse body into thesalivary glands. When an infected tsetse bites a susceptible host, the fly mayregurgitate part of a previous bloodmeal which contains trypanosomes or mayinject trypanosomes contained within its saliva. It is believed that the inoculationmust contain a minimum of 300 to 450 individual trypanosomes to be successful,and may contain up to 40,000 individuals [5].
The trypanosomes are injected into vertebrate muscle tissue but make their way,first into the lymphatic system, then into the bloodstream, and eventually into the

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 12/61
brain. The disease causes the swelling of the lymph glands, emaciation of thebody, and eventually leads to death. Uninfected tsetse may bite the infectedanimal prior to its death and acquire the disease, thereby closing the transmissioncycle.
The tsetse vectored trypanosomiases affect various vertebrate species includinghumans, antelopes, bovine cattle, camels, horses, sheep, goats, and pigs. Thesediseases are caused by several different trypanosome species which may alsosurvive in wild animals such as crocodiles and monitor lizards. The diseases havedifferent distributions across the African continent and are therefore transmittedby different species of tsetse. The following table summarizes this information [5]
[7]:
Disease Species affectedTrypanosoma
agentsDistribution
Glossina
vectors
Sleeping
sickness — chronic form
humansT. brucei
gambiense
WesternAfrica
G. palpalis
G. tachinoides
G. fuscipesG. morsitans
Sleeping
sickness — acute
form
humansT. brucei
rhodesiense
Eastern Africa
G. morsitans
G. swynnertoni
G. pallidipesG. fuscipes
Nagana — acuteform
antelopecattlecamelshorses
T. brucei brucei Africa
G. morsitans
G.
swynnertoniG. pallidipes
G. palpalis
G. tachinoides
G. fuscipes
Nagana — chronic form
cattlecamelshorses
T. congolense Africa G. palpalis
G. morsitans
G. austeniG.
swynnertoni

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 13/61
G. pallidipesG. longipalpis
G. tachinoides
G. brevipalpis
Nagana — acuteform
domestic pigscattlecamelshorses
T. simiae Africa
G. palpalis
G. fuscipes
G. morsitansG. tachinoides
G. longipalpis
G. fuscaG.
tabaniformis
G. brevipalpis
G. vanhoofiG. austeni
Nagana — acuteform
cattlecamelshorses
T. vivax Africa
G. morsitans
G. palpalisG. tachinoides
G.
swynnertoniG. pallidipes
G. austeni
G. vanhoofiG. longipalpis
Surra — chronicform
domestic pigswarthog ( Phacochoerusaethiopicus)forest hogs( Hylochoerus spp.)
T. suis Africa
G. palpalis
G. fuscipesG. morsitans
G. tachinoides
G. longipalpis
G. fuscaG.
tabaniformisG. brevipalpisG. vanhoofi
G. austeni

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 14/61
[EDIT] HUMAN TRYPANOSOMIASIS
Main article: sleeping sickness
Human African trypanosomiasis, also called sleeping sickness, is caused bytrypanosomes of the Trypanosoma brucei species. This disease is invariably fatal
unless treated but can almost always be cured with current medicines, if thedisease is diagnosed early enough.
Sleeping sickness begins with a tsetse bite leading to an inoculation in the sub-cutaneous tissue. The infection moves into the lymphatic system leading to acharacteristic swelling of the lymph glands which is called Winterbottoms's
sign[1]. The infection progresses into the blood stream and eventually crossesinto the central nervous system and invades the brain leading to extreme lethargyand eventually to death.
The Trypanosoma brucei species, which causes the disease, has often been
subdivided into three sub-genera which were identified based either on thevertebrate hosts which the strain could infect or on the virulence of the disease inhumans. The trypanosomes infectious to animals and not to humans were namedTrypanosoma brucei brucei . The strains which infected humans were divided intotwo sub-species based on their different virulences: Trypanosoma brucei
gambiense was thought to have a slower onset and Trypanosoma brucei
rhodesiense refers to strains with a more rapid, virulent onset. Thischaracterization has always been problematic but was the best that could be donegiven the knowledge of the time and the tools available for identification. A recentmolecular study using restriction fragment length polymorphism analysis suggests
that the three sub-genera are polyphyletic
[8]
, so the elucidation of the strains of T. brucei infective to humans will require a more complex explanation.
Other forms of human trypanosomiasis also exist but are not transmitted bytsetse. The most notable is American trypanosomiasis, known as Chagas disease,which occurs in South America, caused by Trypanosoma cruzi , and transmitted bycertain species of the Reduviidae, members of the Hemiptera.
[EDIT] ANIMAL TRYPANOSOMIASIS
Animal trypanosomiasis, also called nagana when it occurs in bovine cattle or
horses or sura when it occurs in domestic pigs, is caused by several trypanosomespecies. These diseases reduce the growth rate, milk productivity, and strength of farm animals, generally leading to the eventually death of the infected animals.Certain species of cattle are called trypanotolerant because they can survive andgrow even when infected with trypanosomes although they also have lowerproductivity rates when infected.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 15/61
The course of the disease in animals is similar to the course of sleeping sickness in humans.
Trypanosoma congolense and Trypanosoma vivax are the two most importantspecies infecting bovine cattle in sub-saharan Africa. Trypanosoma simiae causes
a virulent disease in swine.
Other forms of animal trypanosomiasis are also known from other areas of theglobe, caused by different species of trypanosomes and transmitted without theintervention of the tsetse fly.
Tsetse vector ranges mostly in the central part of Africa.
[ edit ] Control
Tsetse control has been undertaken in order to reduce the incidence of thediseases which the flies transmit. Two alternative strategies have been used in
the attempts to reduce this African trypanosomiasis. One tactic is primarilymedical or veterinary and targets the disease directly using monitoring,prophylaxis, treatment, and surveillance to reduce the number of organismswhich carry the disease. The second strategy is generally entomological andintends to disrupt the cycle of transmission by reducing the number of flies.
The idea of tsetse control implies a change in the relationship between people andthese insects. Prior to the twentieth century, people in Africa had largely adaptedto the presence of tsetse. Human settlement patterns and agricultural practiceshad adapted to the presence of the fly. For example, in Ethiopia draft poweredfarming was restricted to the highland areas where the flies were absent, whereaslowland areas where tsetse are present were more sparsely populated by peopleliving a nomadic, less agriculturally intensive lifestyle. Tsetse control is a responseto changing conditions. Tsetse control has been proposed as a way of reducingthe incidence of the disease in the populations living in tsetse regions, of allowingthe expansion of human settlement and agriculture into new areas, and of helpingpeople previously relocated either in forced transfers or due to migration.
Tsetse control efforts have been undertaken throughout the African continent butlong-term, sustainable control has rarely been achieved. Tsetse control effortsinvariably are tied to the complex problems of poverty, health, politics, and
violence which have proved such a disaster for the African people.
The reduction of fly numbers has generally been attempted with two differentaims, either eradication which intends to completely eliminate tsetse from thearea or control which aims simply to reduce the numbers. Eradication is an ideawhich has often been imagined, has repeatedly been attempted, and is stillproposed but many reasons suggest that control is a safer, cheaper, morerealistic, and sustainable approach. Eradication refers to the successful killing of

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 16/61
every tsetse either in a region or, under more grandiose proposals, from theentire African continent. Local eradication efforts have repeatedly beenundertaken and have achieved temporary success only to fail in the long termbecause tsetse were able to re-invade (Zanzibar).
All of the economic, ecological, political, and environmental justifications foreradication have been called into question. The economic justification foreradication offsets the immense costs of the eradication campaign against themedical and veterinary benefits which are considered to accrue in perpetuity.
However, eradication campaigns may have unintended social consequences, as asuccessful campaign may open up lands for agriculture which have previouslybeen populated by nomadic hunters, resulting in the displacement of the originalpopulation with its attendant consequences.
[EDIT] CONTROL TECHNIQUES
Many techniques have been used to reduce tsetse populations with earlier crudemethods being replaced in more recent times by methods which are cheaper,more directed, and ecologically better considered.
[edit] Slaughter of wild animals
One early technique involved the slaughter of all the wild animals on which tsetsefed. For example, the island of Principé off the west coast of Africa, was entirelycleared of feral pigs in the 1930s which led to the extirpation of the fly. While the
fly eventually re-invaded in the 1950s, the new population of tsetse was free fromthe disease.
[edit] Land clearing
Another early technique involved the complete removal of any brush or woodyvegetation from an area. Tsetse tend to rest on the trunks of trees so the removalof woody vegetation made the area inhospitable to the flies. However, thetechnique has not been widely used and has been abandoned in more recenttimes. Preventing the regrowth of woody vegetation requires continuous clearingefforts which is only practicable where large human populations are present. The
clearing of woody vegetation has come to be seen as an environmental problemmore than a benefit.
[edit] Pesticide campaigns
Pesticides have been used to control tsetse starting initially during the early partof the twentieth century in localized efforts using the inorganic metal based

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 17/61
pesticides, expanding after the Second World war into massive aerial and groundbased campaigns (with organochlorine pesticides such as DDT applied as aerosol sprays at Ultra-Low Volume rates. Later, more targeted techniques used pour-on
formulations in which advanced organic pesticides were applied directly to thebacks of cattle.
[edit] Trapping
Tsetse trapTsetse populations can be monitored and effectively controlled using simple,inexpensive traps. These often use electric blue cloth, since this colour attractsthe flies. Early traps mimicked the form of cattle but this seems unnecessary andrecent traps are simple sheets or have a biconical form. The traps can kill bychanneling the flies into a collection chamber or by exposing the flies toinsecticide sprayed on the cloth.
The use of chemicals as attractants to lure tsetse to the traps has been studiedextensively in the late 20th century, but this has mostly been of interest toscientists rather than as an economically reasonable solution. The attractantsstudied have been those which might be used by tsetse to find their food, likecarbon dioxide and acetone, which are given off in the animals' breath anddistributed downwind to form an 'odour plume'. Synthetic versions of thesechemicals can be used to create artificial odour plumes. A cheaper approach is toplace some cattle urine in a half gourd near the trap. For large trapping efforts,the use of additional traps is generally cheaper than the use of expensive artificialattractants.
A special trapping method is applied in Ethiopia, where the BioFarm Consortium(ICIPE, BioVision Foundation, BEA, Helvetas, DLCO-EA, Praxis Ethiopia) applies
the traps in a sustainable agriculture and rural development context (SARD). Thetraps are just the entry point, followed by improved farming, human health andmarketing inputs. This method is in the final stage of testing (as per 2006).
[edit] Releases of irradiated males
The sterile insect technique has been used to reduce tsetse populations. Thistechnique involves the rearing of large numbers of tsetse, separation of the

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 18/61
males, irradiation of these flies with large doses of gamma rays to make themsterile and then release into to the wild. Since females only mate a few times intheir life, generally only once, any mating with a sterile male will prevent thatfemale from giving birth to any offspring.
The Sterile Insect Technique has recently been used on Zanzibar, an island off thecoast of East Africa. Like other eradication efforts, early indications are that thefly numbers have been decimated with the fly possibly extirpated (locallyeradicated) from the island. A number of traps are in place to monitor the islandand repress any resurgence.
Additionally, using the parasite refractory strains is another method to control thetsetse, that means providing the blood meal containing the trypanocide beforereleasing the sterilised males. Also we can consider to use the cytoplasmicincompatibility strategy to control the population of tsetse. With the developmentof genetic engineering, the releasing of engineered parasite refractory
counterparts is another strategy to control the population of tsetse.
[ edit ] Etymology
The word 'tsetse' comes from Tswana, a language of southern Africa, and, in thatlanguage, the word means fly[9]. Recently 'tsetse' without the 'fly' has becomemore common in English, particularly in the scientific and developmentcommunities.
The pronunuciation of the word differs in different regions. Many Africanlanguages have an ejective ts sound and so a common pronunciation of the word
involves two identical syllables both having this ts sound and a shorter sound of the vowel, as ts-eh-ts-eh. The British pronunciation of the word uses two differentsounds for the two different syllables, generally tee-tsee. In Zimbabwe, it isgenerally pronounced tseh-tsee.
Your continued donations keep Wikipedia running!
Sleeping sickness
FROM WIKIPEDIA, THE FREE ENCYCLOPEDIA
Jump to: navigation, searchThis article is about the African trypanosomiasis. For the encephalitis epidemic of 1917–
1928, see encephalitis lethargica.
Sleeping sickness
Classification and external resources

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 19/61
Trypanosoma forms in a bloodsmear.
ICD-10 B56.
ICD-9 086.5DiseasesDB 29277 13400
MedlinePlus 001362
eMedicine med/2140
MeSH D014353
Sleeping sickness or human African trypanosomiasis is a parasitic disease of people and animals, caused by protozoa of species Trypanosoma brucei andtransmitted by the tsetse fly.[1] The disease is endemic in certain regions of Sub-Saharan Africa, covering about 36 countries and 60 million people. It is estimated
that 50,000 to 70,000 people are currently infected, the number having declinedsomewhat in recent years.[2] Three major epidemics have occurred in recenthistory, one lasting from 1896–1906 and the other two in 1920 and 1970. In2008 there was an epidemic in Uganda.[3]

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 20/61
Contents
[hide]
• 1 Clinical features• 2 History• 3 Geographic distribution and epidemiology• 4 Life cycle• 5 Laboratory diagnosis• 6 Treatment
o 6.1 History of treatment for sleeping sickness• 7 Drug targets and drug discovery• 8 Prevention and control• 9 See also• 10 References
• 11 External links
[ edit ] Clinical features
Winterbottom's sign - Swollen lymph nodes along back of neck in child with earlytrypanosomiasis
Symptoms begin with fever, headaches, and joint pains. As the parasites enterthrough both the blood and lymph systems, lymph nodes often swell up to
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 21/61

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 22/61
T. b. rhodesiense, is the acute form of the disease but has a much more limitedrange. It is found in southern and eastern Africa; its infection emerges in a fewweeks and is more virulent and faster developing. According to recent estimates,the disability adjusted life years (9 to 10 years) (DALYs) lost due to sleepingsickness are 2.0 million.[6] Recent estimates indicate that over 60 million people
living in some 250 foci are at risk of contracting the disease, and there are about300,000 new cases each year.[7] The disease has been recorded as occurring in 36countries, all in sub-Saharan Africa. It is endemic in southeast Uganda andwestern Kenya and kills more than 40,000 Africans a year.[8]
Humans are the main reservoir for Trypanosoma brucei gambiense, but thisspecies can also be found in pigs and other animals. Wild game animals and cattleare the main reservoir of T. b. rhodesiense.
Horse-flies (Tabanidae) and Stomoxydinae possibly could play a role bymechanical transmission (in special situations) not only of Nagana (the animal
form of sleeping sickness) but also of the human disease form.[9]
[ edit ] Life cycle
Life cycle of the Trypanosoma brucei parasites. Source: CDCThe tsetse fly is large, brown and stealthy. While taking blood from a mammalianhost, an infected tsetse fly (genus Glossina) injects metacyclic trypomastigotesinto skin tissue. The parasites enter the lymphatic system and pass into the
bloodstream (1). Inside the host, they transform into bloodstreamtrypomastigotes (2), are carried to other sites throughout the body, reach otherblood fluids (e.g., lymph, spinal fluid), and continue the replication by binaryfission (3). The entire life cycle of African Trypanosomes is represented byextracellular stages. A tsetse fly becomes infected with bloodstreamtrypomastigotes when taking a blood meal on an infected mammalian host (4,5).In the fly's midgut, the parasites transform into procyclic trypomastigotes,

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 23/61
multiply by binary fission (6), leave the midgut, and transform into epimastigotes(7). The epimastigotes reach the fly's salivary glands and continue multiplicationby binary fission (8). The cycle in the fly takes approximately 3 weeks toprogress.
[ edit ] Laboratory diagnosis
Two areas from a blood smear from a patient with African trypanosomiasis. Thin bloodsmear stained with Giemsa. Typical trypomastigote stages (the only stages found in patients), with a posterior kinetoplast, a centrally located nucleus, an undulatingmembrane, and an anterior flagellum. The two Trypanosoma brucei species that cause
human trypanosomiasis, T. b. gambiense and T. b. rhodesiense, are indistinguishablemorphologically. The trypanosomes length range is 14 to 33 µm, Source: CDCThe diagnosis rests upon demonstrating trypanosomes by microscopicexamination of chancre fluid, lymph node aspirates, blood, bone marrow, or, inthe late stages of infection, cerebrospinal fluid. A wet preparation should beexamined for the motile trypanosomes, and in addition a smear should be fixed,stained with Giemsa (or Field), and examined. Concentration techniques can beused prior to microscopic examination. For blood samples, these includecentrifugation followed by examination of the buffy coat; mini anion-exchange/centrifugation; and the Quantitative Buffy Coat (QBC) technique. Forother samples such as spinal fluid, concentration techniques include centrifugationfollowed by examination of the sediment. Isolation of the parasite by inoculationof rats or mice is a sensitive method, but its use is limited to T. b. rhodesiense.Antibody detection has sensitivity and specificity that are too variable for clinicaldecisions. In addition, in infections with T. b. rhodesiense, seroconversion occursafter the onset of clinical symptoms and thus is of limited use.
Three similar serological tests are available for detection of the parasite; themicro-CATT, wb-CATT, and wb-LATEX. The first uses dried blood while the othertwo use whole blood samples. A 2002 study found the wb-CATT to be the mostefficient for diagnosis, while the wb-LATEX is a better exam for situations where
greater sensitivity is required. PMID 12481210
[ edit ] Treatment
The current standard treatment for first stage disease is:
• Intravenous pentamidine (for T.b. gambiense); or • Intravenous suramin (for T.b. rhodesiense)

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 24/61
However, the drug Eflornithine was found safe as first-line sleeping sicknesstreatment in 2008, according to the Science and Development Network's Sub-Saharan Africa news updates. [1] The drug eflornithine — previously used only asan alternative treatment for sleeping sickness due to its labour-intensiveadministration — was found to be safe and effective as a first-line treatment for
the disease. Researchers tracked over 1,000 adults and children at a centre inIbba, Southern Sudan — the first use of eflornithine on a large scale.
The current standard treatment for second stage (later stage) disease is:
• Intravenous melarsoprol 2.2 mg/kg daily for 10 consecutive days.[10]
Alternative first line therapies include:
• Intravenous melarsoprol 0.6 mg/kg on day 1, 1.2 mg/kg iv melarsoprol on day 2,and 1.2 mg/kg/day iv melarsoprol combined with oral 7.5 mg/kg nifurtimox twice
a day on days 3 to 10;[11] or • Intravenous eflornithine 50 mg/kg every six hours for 14 days.[12]
In areas with melarsoprol resistance or in patients who have relapsed aftermelarsoprol monotherapy, the treatment should be:
• melarsoprol and nifurtimox, or • eflornithine
The following traditional regimens should no longer be used:
• (old "standard" 26-day melarsoprol therapy) Intravenous melarsoprol therapy (3series of 3.6 mg/kg/day intravenously for 3 days, with 7-day breaks between theseries) (this regimen is less convenient and patients are less likely to completetherapy);[13]
• (incremental melarsoprol therapy) 10-day incremental-dose melarsoprol therapy(0.6 mg/kg iv on day 1, 1.2 mg/kg iv on day 2, and 1.8 mg/kg iv on days 3–10)(previously thought to reduce the risk of treatment-induced encephalopathy, butnow known to be associated with an increased risk of relapse and a higher incidence of encephalopathy)[11][13];
According to a treatment study of Trypanosoma gambiense caused human Africantrypanosomiasis, use of eflornithine (DMFO) resulted in fewer adverse events thantreatment with melarsoprol. [14]
All patients should be followed up for two years with lumbar punctures every sixmonths to look for relapse.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 25/61
[EDIT] HISTORY OF TREATMENT FOR SLEEPING SICKNESS
Suramin was introduced in 1920 to treat the first stage of the disease. By 1922,Suramin was generally combined with Tryparsamide (another pentavalent organo-arsenic drug) in the treatment of the second stage of the gambiense form. It was
used during the grand epidemic in West and Central Africa in millions of peopleand was the mainstay of therapy until 1969.
Pentamidine, a highly effective drug for the first stage of the disease, has beenused since 1939. During the fifties, it was widely used as a prophylactic agent inWestern Africa, leading to a sharp decline in infection rates. At the time, it wasthought that eradication of the disease was at hand.
The organo-arsenical melarsoprol (Arsobal) was developed in the 1940s, and iseffective for patients with second stage sleeping sickness. However, 3 - 10% of those injected have reactive encephalopathy (convulsions, progressive coma, or
psychotic reactions), and 10 - 70% of such cases result in death; it can causebrain damage in those who survive the encephalopathy. However, due to itseffectiveness, melarsoprol is still used today. Resistance to melarsoprol isincreasing, and combination therapy with nifurtimox is currently under research.
Eflornithine (difluoromethylornithine or DFMO), the most modern treatment, wasdeveloped in the 1970s by Albert Sjoerdsmanot and underwent clinical trials inthe 1980s. The drug was approved by the United States Food and DrugAdministration in 1990, but Aventis, the company responsible for its manufacture,halted production in 1999. In 2001, however, Aventis, in association withMédecins Sans Frontières and the World Health Organization, signed a long-termagreement to manufacture and donate the drug.
An international research team working in the Democratic Republic of the Congo,New Sudan and Angola involving Immtech International and University of NorthCarolina at Chapel Hill have completed a Phase IIb clinical trial and commenced aPhase III trial in 2005 testing the efficacy of the first oral treatment for SleepingSickness, known at this point as "DB289". [15] [16]
[ edit ] Drug targets and drug discovery
The genome of the parasite has been decoded and several proteins have been
identified as potential targets for drug treatment. The decoded DNA also revealedthe reason why generating a vaccine for this disease has been so difficult. T.
brucei has over 800 genes that manufacture proteins that the disease mixes andmatches to evade immune system detection.[17]
Recent findings indicate that the parasite is unable to survive in the bloodstreamwithout its flagellum. This insight gives researchers a new angle with which toattack the parasite.[18]
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 26/61
A new treatment based on a truncated version of the apolipoprotein L-1 of highdensity lipoprotein and a nanobody has recently been found to work in mice, buthas not been tested in humans.[19]
The cover story of the August 25, 2006 issue of Cell journal describes an
advance; Dr. Lee Soo Hee and colleagues, working at Johns Hopkins, haveinvestigated the pathway by which the organism makes myristate, a 14-carbonlength fatty acid. Myristate is a component of the variant surface glycoprotein(VSG), the molecule that makes up the trypanosome's outer layer. This outersurface coat of VSG is vital to the trypanosome's avoidance of immunologicalcapture. Dr. Lee and colleagues discovered trypanosomes use a novel fatty acidsynthesis pathway involving fatty acid elongases to make myristate and otherfatty acids.
[ edit ] Prevention and control
For in depth information on prevention of the disease via tsetse fly control seeTsetse fly control .
Prevention and control focus on, where it is possible, the eradication of theparasitic host, the tsetse fly. Two alternative strategies have been used in theattempts to reduce the African trypanosomiases. One tactic is primarily medical orveterinary and targets the disease directly using monitoring, prophylaxis,treatment, and surveillance to reduce the number of organisms which carry thedisease. The second strategy is generally entomological and intends to disrupt thecycle of transmission by reducing the number of flies. Instances of sleepingsickness are being reduced by the use of the sterile insect technique.
Regular active surveillance, involving case detection and treatment, in addition totsetse fly control, is the backbone of the strategy for control of sleeping sickness.Systematic screening of communities in identified foci is the best approach ascase-by-case screening is not practically possible in highly endemic regions.Systematic screening may be in the form of mobile clinics or fixed screeningcentres where teams travel daily to the foci. The nature of gambiense disease issuch that patients do not seek treatment early enough because the symptoms atthat stage are not evident or serious enough to warrant seeking medicalattention, considering the remoteness of some affected areas. Also, diagnosis of
the disease is difficult and most health workers may not be able to detect it.Systematic screening allows early-stage disease to be detected and treated beforethe disease progresses, and removes the potential human reservoir.[20]
There is a single case report of sexual transmission of West African sleepingsickness.[21] This is not believed to be an important route of transmission. A caseof sexually transmitted sleeping sickness was the focus of an episode of thetelevision program House.
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 27/61
[ edit ] See also
• Drugs for Neglected Diseases Initiative• David Bruce (microbiologist)• Sleep disorder
• The other important human tropical disease caused by Trypanosomes is Chagas-disease, occurring in America.
Make a donation to Wikipedia and give the gift of knowledge!
Malaria
FROM WIKIPEDIA, THE FREE ENCYCLOPEDIA
Jump to: navigation, search
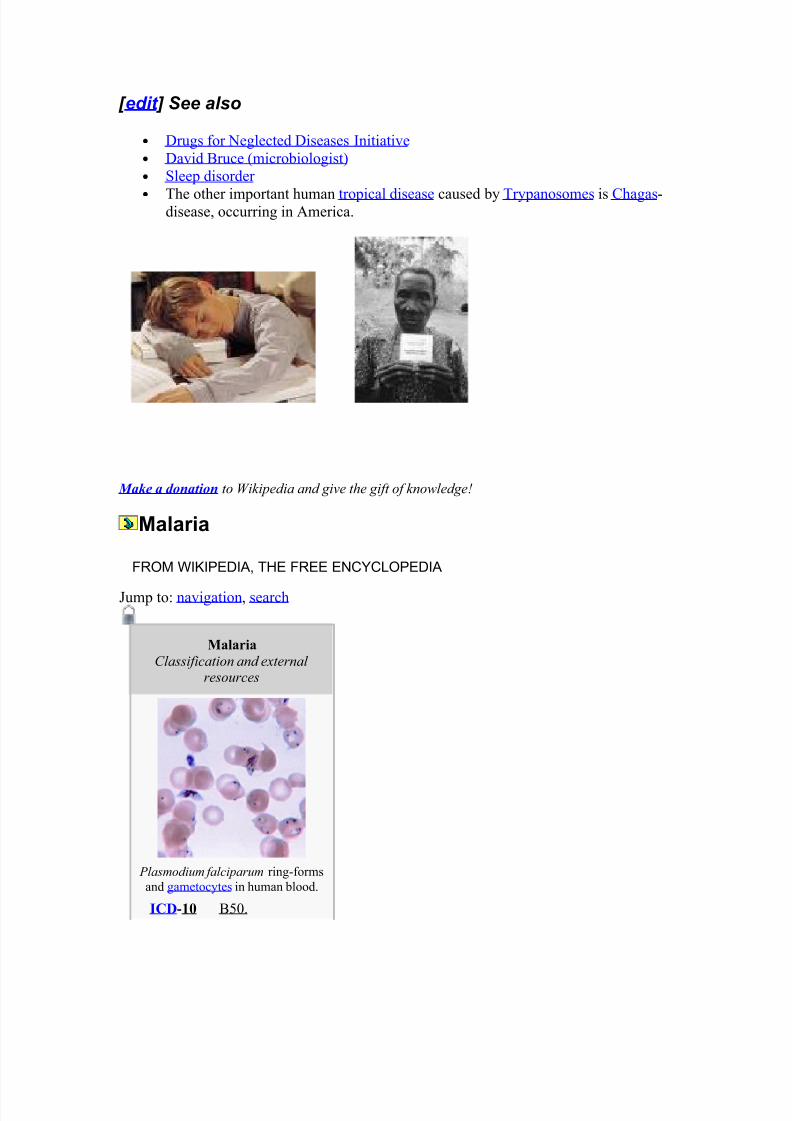
Malaria
Classification and external resources
Plasmodium falciparum ring-formsand gametocytes in human blood.
ICD-10 B50.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 28/61
ICD-9 084
OMIM 248310
DiseasesDB 7728
MedlinePlus 000621
eMedicine med/1385 emerg/305 ped/1357
MeSH C03.752.250.552
Malaria is a vector-borne infectious disease caused by protozoan parasites. It iswidespread in tropical and subtropical regions, including parts of the Americas,Asia, and Africa. Each year, there are approximately 515 million cases of malaria,killing between one and three million people, the majority of whom are youngchildren in Sub-Saharan Africa.[1] Malaria is commonly associated with poverty,but is also a cause of poverty and a major hindrance to economic development.
Malaria is one of the most common infectious diseases and an enormous publichealth problem. The disease is caused by protozoan parasites of the genus Plasmodium. Only four types of the plasmodium parasite can infect humans; themost serious forms of the disease are caused by Plasmodium falciparum andPlasmodium vivax , but other related species (Plasmodium ovale, Plasmodium
malariae) can also affect humans. This group of human-pathogenic Plasmodium
species is usually referred to as malaria parasites.
Malaria parasites are transmitted by female Anopheles mosquitoes. The parasitesmultiply within red blood cells, causing symptoms that include symptoms of
anemia (light headedness, shortness of breath, tachycardia etc.), as well as othergeneral symptoms such as fever, chills, nausea, flu-like illness, and in severecases, coma and death. Malaria transmission can be reduced by preventingmosquito bites with mosquito nets and insect repellents, or by mosquito controlmeasures such as spraying insecticides inside houses and draining standing waterwhere mosquitoes lay their eggs.
Although some are under development, no vaccine is currently available formalaria; preventative drugs must be taken continuously to reduce the risk of infection. These prophylactic drug treatments are often too expensive for most
people living in endemic areas. Most adults from endemic areas have a degree of long-term infection, which tends to recur and also possess partial immunity (resistance); the resistance reduces with time and such adults may becomesusceptible to severe malaria if they have spent a significant amount of time innon-endemic areas. They are strongly recommended to take full precautions if they return to an endemic area. Malaria infections are treated through the use of antimalarial drugs, such as quinine or artemisinin derivatives, although drugresistance is increasingly common.
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 29/61
Contents
[hide]
• 1 History• 2 Distribution and impact
o 2.1 Socio-economic effects• 3 Symptoms• 4 Causes
o 4.1 Malaria parasites• 5 Mosquito vectors and the Plasmodium life cycle• 6 Pathogenesis• 7 Evolutionary pressure of malaria on human genes
o 7.1 Sickle-cell diseaseo 7.2 Thalassaemiaso 7.3 Duffy antigenso 7.4 G6PDo 7.5 HLA and interleukin-4
• 8 Diagnosiso 8.1 Symptomatic diagnosiso 8.2 Microscopic examination of blood filmso 8.3 Field testso 8.4 Molecular methodso 8.5 Laboratory tests
• 9 Treatmento 9.1 Antimalarial drugso 9.2 Counterfeit drugs
• 10 Prevention and disease controlo 10.1 Vector controlo 10.2 Prophylactic drugso 10.3 Indoor residual sprayingo 10.4 Mosquito nets and bedclotheso 10.5 Vaccinationo 10.6 Other methods
• 11 See also• 12 References
• 13 External links
History
Further information: History of malaria
Charles Louis Alphonse LaveranMalaria has infected humans for over 50,000 years, and may have been a humanpathogen for the entire history of our species.[2] Indeed, close relatives of the

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 30/61
human malaria parasites remain common in chimpanzees, our closest relatives.[3]
References to the unique periodic fevers of malaria are found throughout recordedhistory, beginning in 2700 BC in China.[4] The term malaria originates fromMedieval Italian: mala aria — "bad air"; and the disease was formerly called ague
or marsh fever due to its association with swamps.
Scientific studies on malaria made their first significant advance in 1880, when aFrench army doctor working in the military hospital of Constantine in Algeria named Charles Louis Alphonse Laveran observed parasites for the first time,inside the red blood cells of people suffering from malaria. He therefore proposedthat malaria was caused by this protozoan, the first time protozoa were identifiedas causing disease.[5] For this and later discoveries, he was awarded the 1907Nobel Prize for Physiology or Medicine. The protozoan was called Plasmodium bythe Italian scientists Ettore Marchiafava and Angelo Celli.[6] A year later, CarlosFinlay, a Cuban doctor treating patients with yellow fever in Havana, provided
strong evidence that mosquitoes were transmitting disease to and from humans.[7]
This work followed earlier suggestions by Josiah C. Nott,[8] and work by PatrickManson on the transmission of filariasis.[9]
However, it was Britain's Sir Ronald Ross working in the Presidency GeneralHospital in Calcutta who finally proved in 1898 that malaria is transmitted bymosquitoes. He did this by showing that certain mosquito species transmitmalaria to birds and isolating malaria parasites from the salivary glands of mosquitoes that had fed on infected birds.[10] For this work Ross received the 1902Nobel Prize in Medicine. After resigning from the Indian Medical Service, Rossworked at the newly-established Liverpool School of Tropical Medicine and
directed malaria-control efforts in Egypt, Panama, Greece and Mauritius.[11] Thefindings of Finlay and Ross were later confirmed by a medical board headed byWalter Reed in 1900, and its recommendations implemented by William C. Gorgas in the health measures undertaken during construction of the Panama Canal. Thispublic-health work saved the lives of thousands of workers and helped developthe methods used in future public-health campaigns against this disease.
The first effective treatment for malaria was the bark of cinchona tree, whichcontains quinine. This tree grows on the slopes of the Andes, mainly in Peru. Thisnatural product was used by the inhabitants of Peru to control malaria, and the
Jesuits introduced this practice to Europe during the 1640s where it was rapidlyaccepted.[12] However, it was not until 1820 that the active ingredient quinine wasextracted from the bark, isolated and named by the French chemists PierreJoseph Pelletier and Joseph Bienaimé Caventou.[13]
In the early twentieth century, before antibiotics, patients with syphilis wereintentionally infected with malaria to create a fever, following the work of JuliusWagner-Jauregg. By accurately controlling the fever with quinine, the effects of

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 31/61
both syphilis and malaria could be minimized. Although some patients died frommalaria, this was preferable to the almost-certain death from syphilis.[14]
Although the blood stage and mosquito stages of the malaria life cycle wereidentified in the 19th and early 20th centuries, it was not until the 1980s that the
latent liver form of the parasite was observed.[15][16]
The discovery of this latentform of the parasite finally explained why people could appear to be cured of malaria but still relapse years after the parasite had disappeared from theirbloodstreams.
Distribution and impact
Further information: Diseases of poverty , Tropical disease
Areas of the world where malaria is endemic as of 2003 (coloured yellow).[17]
Malaria causes about 250 million cases of fever and approximately one milliondeaths annually.[18] The vast majority of cases occur in children under the age of 5years;[19] pregnant women are also especially vulnerable. Despite efforts to reducetransmission and increase treatment, there has been little change in which areas
are at risk of this disease since 1992.[20] Indeed, if the prevalence of malaria stayson its present upwards course, the death rate could double in the next twentyyears.[21] Precise statistics are unknown because many cases occur in rural areaswhere people do not have access to hospitals or the means to afford health care.Consequently, the majority of cases are undocumented.[21]
Although co-infection with HIV and malaria does cause increased mortality, this isless of a problem than with HIV/tuberculosis co-infection, due to the two diseasesusually attacking different age-ranges, with malaria being most common in theyoung and active tuberculosis most common in the old.[22] Although HIV/malariaco-infection produces less severe symptoms than the interaction between HIV andTB, HIV and malaria do contribute to each other's spread. This effect comes frommalaria increasing viral load and HIV infection increasing a person's susceptibilityto malaria infection.[23]
Malaria is presently endemic in a broad band around the equator, in areas of theAmericas, many parts of Asia, and much of Africa; however, it is in sub-SaharanAfrica where 85– 90% of malaria fatalities occur.[24] The geographic distribution of
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 32/61
malaria within large regions is complex, and malaria-afflicted and malaria-freeareas are often found close to each other.[25] In drier areas, outbreaks of malariacan be predicted with reasonable accuracy by mapping rainfall.[26] Malaria is morecommon in rural areas than in cities; this is in contrast to dengue fever whereurban areas present the greater risk.[27] For example, the cities of Vietnam, Laos
and Cambodia are essentially malaria-free, but the disease is present in manyrural regions.[28] By contrast, in Africa malaria is present in both rural and urbanareas, though the risk is lower in the larger cities.[29] The global endemic levels of malaria have not been mapped since the 1960s. However, the Wellcome Trust,UK, has funded the Malaria Atlas Project[30] to rectify this, providing a morecontemporary and robust means with which to assess current and future malariadisease burden.
SOCIO-ECONOMIC EFFECTS
Malaria is not just a disease commonly associated with poverty, but is also acause of poverty and a major hindrance to economic development. The diseasehas been associated with major negative economic effects on regions where it iswidespread. A comparison of average per capita GDP in 1995, adjusted to giveparity of purchasing power, between malarious and non-malarious countriesdemonstrates a fivefold difference ($1,526 USD versus $8,268 USD). Moreover, incountries where malaria is common, average per capita GDP has risen (between1965 and 1990) only 0.4% per year, compared to 2.4% per year in othercountries.[31] However, correlation does not demonstrate causation, and theprevalence is at least partly because these regions do not have the financial
capacities to prevent malaria. In its entirety, the economic impact of malaria hasbeen estimated to cost Africa $12 billion USD every year. The economic impactincludes costs of health care, working days lost due to sickness, days lost ineducation, decreased productivity due to brain damage from cerebral malaria, andloss of investment and tourism.[19] In some countries with a heavy malariaburden, the disease may account for as much as 40% of public healthexpenditure, 30-50% of inpatient admissions, and up to 50% of outpatient visits.[32]
Symptoms
Symptoms of malaria include fever, shivering, arthralgia (joint pain), vomiting,anemia (caused by hemolysis), hemoglobinuria, and convulsions. There may be afeeling of tingling in the skin, particularly with malaria caused by P. falciparum.[citation needed ] The classic symptom of malaria is cyclical occurrence of suddencoldness followed by rigor and then fever and sweating lasting four to six hours,occurring every two days in P. vivax and P. ovale infections, while every three forP. malariae.[33] P. falciparum can have recurrent fever every 36-48 hours or a lesspronounced and almost continuous fever. For reasons that are poorly understood,

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 33/61
but which may be related to high intracranial pressure, children with malariafrequently exhibit abnormal posturing, a sign indicating severe brain damage.[34]
Malaria has been found to cause cognitive impairments, especially in children. Itcauses widespread anemia during a period of rapid brain development and alsodirect brain damage. This neurologic damage results from cerebral malaria to
which children are more vulnerable.[35][36]
Severe malaria is almost exclusively caused by P. falciparum infection and usuallyarises 6-14 days after infection.[37] Consequences of severe malaria include coma and death if untreated—young children and pregnant women are especiallyvulnerable. Splenomegaly (enlarged spleen), severe headache, cerebral ischemia,hepatomegaly (enlarged liver), hypoglycemia, and hemoglobinuria with renalfailure may occur. Renal failure may cause blackwater fever, where hemoglobinfrom lysed red blood cells leaks into the urine. Severe malaria can progressextremely rapidly and cause death within hours or days.[37] In the most severe
cases of the disease fatality rates can exceed 20%, even with intensive care andtreatment.[38] In endemic areas, treatment is often less satisfactory and theoverall fatality rate for all cases of malaria can be as high as one in ten.[39] Overthe longer term, developmental impairments have been documented in childrenwho have suffered episodes of severe malaria.[40]
Chronic malaria is seen in both P. vivax and P. ovale, but not in P. falciparum.Here, the disease can relapse months or years after exposure, due to thepresence of latent parasites in the liver. Describing a case of malaria as cured byobserving the disappearance of parasites from the bloodstream can therefore bedeceptive. The longest incubation period reported for a P. vivax infection is 30
years.[37] Approximately one in five of P. vivax malaria cases in temperate areasinvolve overwintering by hypnozoites (i.e., relapses begin the year after themosquito bite).[41]

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 34/61
Causes
A Plasmodium sporozoite traverses the cytoplasm of a mosquito midgut epithelial cell inthis false-color electron micrograph.
MALARIA PARASITES
Malaria is caused by protozoan parasites of the genus Plasmodium (phylumApicomplexa). In humans malaria is caused by P. falciparum, P. malariae, P.
ovale, P. vivax and P. knowlesi . P. falciparum is the most common cause of infection and is responsible for about 80% of all malaria cases, and is alsoresponsible for about 90% of the deaths from malaria.[42] Parasitic Plasmodium
species also infect birds, reptiles, monkeys, chimpanzees and rodents.[43] Therehave been documented human infections with several simian species of malaria,namely P. knowlesi , P. inui , P. cynomolgi ,[44] P. simiovale, P. brazilianum, P.
schwetzi and P. simium; however, with the exception of P. knowlesi, these aremostly of limited public health importance. Although avian malaria can killchickens and turkeys, this disease does not cause serious economic losses topoultry farmers.[45] However, since being accidentally introduced by humans it hasdecimated the endemic birds of Hawaii, which evolved in its absence and lack anyresistance to it.[46]
Mosquito vectors and the Plasmodium life cycle
The parasite's primary (definitive) hosts and transmission vectors are femalemosquitoes of the Anopheles genus. Young mosquitoes first ingest the malaria
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 35/61
parasite by feeding on an infected human carrier and the infected Anopheles
mosquitoes carry Plasmodium sporozoites in their salivary glands. A mosquitobecomes infected when it takes a blood meal from an infected human. Onceingested, the parasite gametocytes taken up in the blood will further differentiateinto male or female gametes and then fuse in the mosquito gut. This produces an
ookinete that penetrates the gut lining and produces an oocyst in the gut wall.When the oocyst ruptures, it releases sporozoites that migrate through themosquito's body to the salivary glands, where they are then ready to infect a newhuman host. This type of transmission is occasionally referred to as anteriorstation transfer.[47] The sporozoites are injected into the skin, alongside saliva,when the mosquito takes a subsequent blood meal.
Only female mosquitoes feed on blood, thus males do not transmit the disease.The females of the Anopheles genus of mosquito prefer to feed at night. Theyusually start searching for a meal at dusk, and will continue throughout the night
until taking a meal. Malaria parasites can also be transmitted by bloodtransfusions, although this is rare.[48]
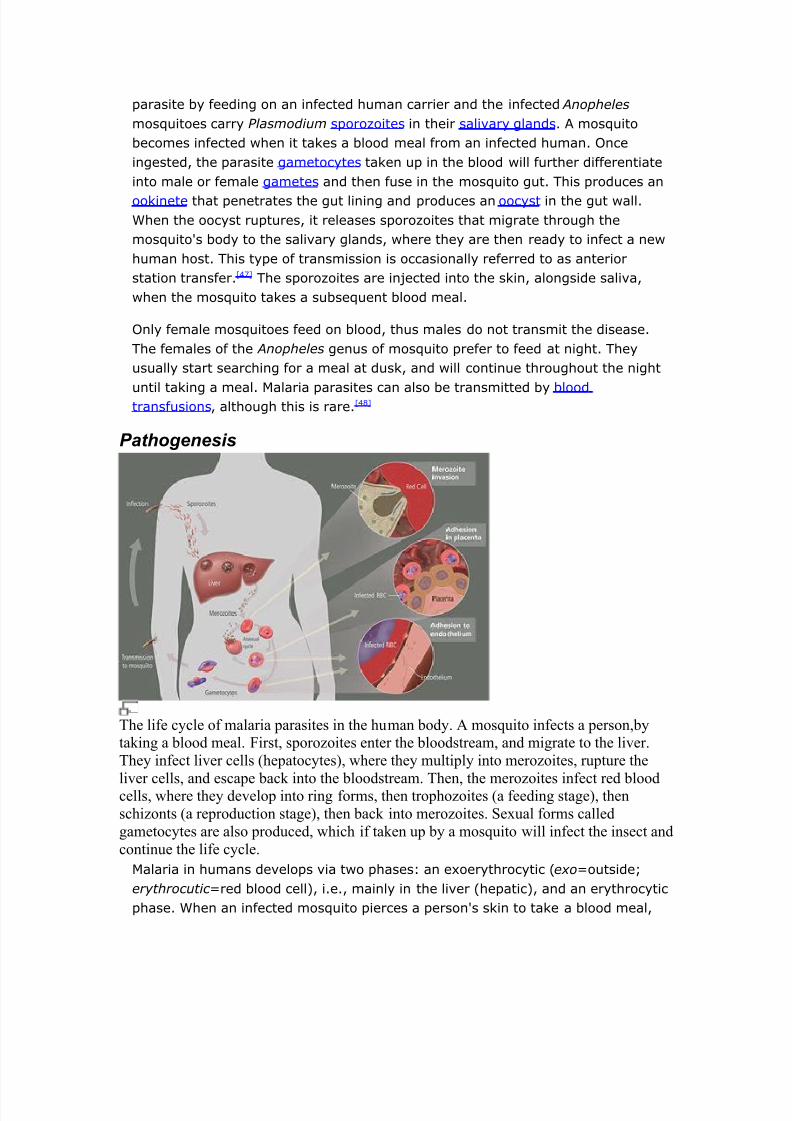
Pathogenesis
The life cycle of malaria parasites in the human body. A mosquito infects a person,bytaking a blood meal. First, sporozoites enter the bloodstream, and migrate to the liver.They infect liver cells (hepatocytes), where they multiply into merozoites, rupture the
liver cells, and escape back into the bloodstream. Then, the merozoites infect red bloodcells, where they develop into ring forms, then trophozoites (a feeding stage), thenschizonts (a reproduction stage), then back into merozoites. Sexual forms calledgametocytes are also produced, which if taken up by a mosquito will infect the insect andcontinue the life cycle.
Malaria in humans develops via two phases: an exoerythrocytic (exo=outside;erythrocutic =red blood cell), i.e., mainly in the liver (hepatic), and an erythrocyticphase. When an infected mosquito pierces a person's skin to take a blood meal,

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 36/61
sporozoites in the mosquito's saliva enter the bloodstream and migrate to theliver. Within 30 minutes of being introduced into the human host, they infecthepatocytes, multiplying asexually and asymptomatically for a period of 6–15days. Once in the liver these organisms differentiate to yield thousands of merozoites which, following rupture of their host cells, escape into the blood and
infect red blood cells, thus beginning the erythrocytic stage of the life cycle.[49]
The parasite escapes from the liver undetected by wrapping itself in the cellmembrane of the infected host liver cell.[50]
Within the red blood cells the parasites multiply further, again asexually,periodically breaking out of their hosts to invade fresh red blood cells. Severalsuch amplification cycles occur. Thus, classical descriptions of waves of fever arisefrom simultaneous waves of merozoites escaping and infecting red blood cells.
Some P. vivax and P. ovale sporozoites do not immediately develop intoexoerythrocytic-phase merozoites, but instead produce hypnozoites that remain
dormant for periods ranging from several months (6–12 months is typical) to aslong as three years. After a period of dormancy, they reactivate and producemerozoites. Hypnozoites are responsible for long incubation and late relapses inthese two species of malaria.[51]
The parasite is relatively protected from attack by the body's immune system because for most of its human life cycle it resides within the liver and blood cellsand is relatively invisible to immune surveillance. However, circulating infectedblood cells are destroyed in the spleen. To avoid this fate, the P. falciparum
parasite displays adhesive proteins on the surface of the infected blood cells,
causing the blood cells to stick to the walls of small blood vessels, therebysequestering the parasite from passage through the general circulation and thespleen.[52] This "stickiness" is the main factor giving rise to hemorrhagic complications of malaria. High endothelial venules (the smallest branches of thecirculatory system) can be blocked by the attachment of masses of these infectedred blood cells. The blockage of these vessels causes symptoms such as inplacental and cerebral malaria. In cerebral malaria the sequestrated red bloodcells can breach the blood brain barrier possibly leading to coma.[53]
Although the red blood cell surface adhesive proteins (called PfEMP1, forPlasmodium falciparum erythrocyte membrane protein 1) are exposed to the
immune system they do not serve as good immune targets because of theirextreme diversity; there are at least 60 variations of the protein within a singleparasite and perhaps limitless versions within parasite populations.[52] Like a thief changing disguises or a spy with multiple passports, the parasite switchesbetween a broad repertoire of PfEMP1 surface proteins, thus staying one stepahead of the pursuing immune system.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 37/61
Some merozoites turn into male and female gametocytes. If a mosquito piercesthe skin of an infected person, it potentially picks up gametocytes within theblood. Fertilization and sexual recombination of the parasite occurs in themosquito's gut, thereby defining the mosquito as the definitive host of thedisease. New sporozoites develop and travel to the mosquito's salivary gland,
completing the cycle. Pregnant women are especially attractive to the mosquitoes,[54] and malaria in pregnant women is an important cause of stillbirths, infantmortality and low birth weight,[55] particularly in P. falciparum infection, but also inother species infection, such as P. vivax .[56]
Evolutionary pressure of malaria on human genes
Further information: Evolution , Natural selection Malaria is thought to have been the greatest selective pressure on the humangenome in recent history.[57] This is due to the high levels of mortality andmorbidity caused by malaria, especially the P. falciparum species.
SICKLE-CELL DISEASE
Distribution of the sickle cell trait.
Distribution of malaria.The best-studied influence of the malaria parasite upon the human genome is theblood disease, sickle-cell disease. In sickle-cell disease, there is a mutation in theHBB gene, which encodes the beta globin subunit of haemoglobin. The normalallele encodes a glutamate at position six of the beta globin protein, while thesickle-cell allele encodes a valine. This change from a hydrophilic to a hydrophobic

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 38/61
amino acid encourages binding between haemoglobin molecules, withpolymerization of haemoglobin deforming red blood cells into a "sickle" shape.Such deformed cells are cleared rapidly from the blood, mainly in the spleen, fordestruction and recycling.
In the merozoite stage of its life cycle the malaria parasite lives inside red bloodcells, and its metabolism changes the internal chemistry of the red blood cell.Infected cells normally survive until the parasite reproduces, but if the red cellcontains a mixture of sickle and normal haemoglobin, it is likely to becomedeformed and be destroyed before the daughter parasites emerge. Thus,individuals heterozygous for the mutated allele, known as sickle-cell trait, mayhave a low and usually unimportant level of anaemia, but also have a greatlyreduced chance of serious malaria infection. This is a classic example of heterozygote advantage.
Individuals homozygous for the mutation have full sickle-cell disease and in
traditional societies rarely live beyond adolescence. However, in populationswhere malaria is endemic, the frequency of sickle-cell genes is around 10%. Theexistence of four haplotypes of sickle-type hemoglobin suggests that thismutation has emerged independently at least four times in malaria-endemicareas, further demonstrating its evolutionary advantage in such affected regions.There are also other mutations of the HBB gene that produce haemoglobinmolecules capable of conferring similar resistance to malaria infection. Thesemutations produce haemoglobin types HbE and HbC which are common inSoutheast Asia and Western Africa, respectively.
THALASSAEMIAS
Another well documented set of mutations found in the human genome associatedwith malaria are those involved in causing blood disorders known asthalassaemias. Studies in Sardinia and Papua New Guinea have found that thegene frequency of β-thalassaemias is related to the level of malarial endemicity ina given population. A study on more than 500 children in Liberia found that thosewith β-thalassaemia had a 50% decreased chance of getting clinical malaria.Similar studies have found links between gene frequency and malaria endemicityin the α+ form of α-thalassaemia. Presumably these genes have also been
selected in the course of human evolution.
DUFFY ANTIGENS
The Duffy antigens are antigens expressed on red blood cells and other cells inthe body acting as a chemokine receptor. The expression of Duffy antigens onblood cells is encoded by Fy genes (Fya, Fyb, Fyc etc.). Plasmodium vivax malariauses the Duffy antigen to enter blood cells. However, it is possible to express no

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 39/61
Duffy antigen on red blood cells (Fy-/Fy-). This genotype confers completeresistance to P. vivax infection. The genotype is very rare in European, Asian andAmerican populations, but is found in almost all of the indigenous population of West and Central Africa.[58] This is thought to be due to very high exposure to P.
vivax in Africa in the last few thousand years.
G6PD
Glucose-6-phosphate dehydrogenase (G6PD) is an enzyme which normallyprotects from the effects of oxidative stress in red blood cells. However, a geneticdeficiency in this enzyme results in increased protection against severe malaria.
HLA AND INTERLEUKIN-4
HLA-B53 is associated with low risk of severe malaria. This MHC class I moleculepresents liver stage and sporozoite antigens to T-Cells. Interleukin-4, encoded byIL4, is produced by activated T cells and promotes proliferation and differentiationof antibody-producing B cells. A study of the Fulani of Burkina Faso, who haveboth fewer malaria attacks and higher levels of antimalarial antibodies than doneighboring ethnic groups, found that the IL4-524 T allele was associated withelevated antibody levels against malaria antigens, which raises the possibility thatthis might be a factor in increased resistance to malaria.[59]
Diagnosis
Further information: Blood film
Blood smear from a P. falciparum culture (K1 strain). Several red blood cells have ringstages inside them. Close to the center there is a schizont and on the left a trophozoite.
Severe malaria is commonly misdiagnosed in Africa, leading to a failure to treatother life-threatening illnesses. In malaria-endemic areas, parasitemia does notensure a diagnosis of severe malaria because parasitemia can be incidental toother concurrent disease. Recent investigations suggest that malarial retinopathy
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 40/61
is better (collective sensitivity of 95% and specificity of 90%) than any otherclinical or laboratory feature in distinguishing malarial from non-malarial coma.[60]
SYMPTOMATIC DIAGNOSIS
Areas that cannot afford even simple laboratory diagnostic tests often use only ahistory of subjective fever as the indication to treat for malaria. Using Giemsa-stained blood smears from children in Malawi, one study showed that unnecessarytreatment for malaria was significantly decreased when clinical predictors (rectaltemperature, nailbed pallor, and splenomegaly) were used as treatmentindications, rather than the current national policy of using only a history of subjective fevers (sensitivity increased from 21% to 41%).[61]
MICROSCOPIC EXAMINATION OF BLOOD FILMS
For more details on individual parasites, see P. falciparum, P. vivax, P. ovale, P.malariae.
The most economic, preferred, and reliable diagnosis of malaria is microscopicexamination of blood films because each of the four major parasite species hasdistinguishing characteristics. Two sorts of blood film are traditionally used. Thinfilms are similar to usual blood films and allow species identification because theparasite's appearance is best preserved in this preparation. Thick films allow themicroscopist to screen a larger volume of blood and are about eleven times moresensitive than the thin film, so picking up low levels of infection is easier on thethick film, but the appearance of the parasite is much more distorted andtherefore distinguishing between the different species can be much more difficult.
With the pros and cons of both thick and thin smears taken into consideration, itis imperative to utilize both smears while attempting to make a definitivediagnosis.[62]
From the thick film, an experienced microscopist can detect parasite levels (orparasitemia) down to as low as 0.0000001% of red blood cells. Diagnosis of species can be difficult because the early trophozoites ("ring form") of all fourspecies look identical and it is never possible to diagnose species on the basis of asingle ring form; species identification is always based on several trophozoites.
FIELD TESTS
In areas where microscopy is not available, or where laboratory staff are notexperienced at malaria diagnosis, there are antigen detection tests that requireonly a drop of blood.[63] Immunochromatographic tests (also called: Malaria RapidDiagnostic Tests, Antigen-Capture Assay or "Dipsticks") have been developed,distributed and fieldtested. These tests use finger-stick or venous blood, thecompleted test takes a total of 15-20 minutes, and a laboratory is not needed.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 41/61
The threshold of detection by these rapid diagnostic tests is in the range of 100parasites/µl of blood compared to 5 by thick film microscopy. The first rapiddiagnostic tests were using P. falciparum glutamate dehydrogenase as antigen.[64]
PGluDH was soon replaced by P.falciparum lactate dehydrogenase, a 33 kDaoxidoreductase [EC 1.1.1.27]. It is the last enzyme of the glycolytic pathway,
essential for ATP generation and one of the most abundant enzymes expressed byP.falciparum. PLDH does not persist in the blood but clears about the same timeas the parasites following successful treatment. The lack of antigen persistenceafter treatment makes the pLDH test useful in predicting treatment failure. In thisrespect, pLDH is similar to pGluDH. The OptiMAL-IT assay can distinguish betweenP. falciparum and P. vivax because of antigenic differences between their pLDHisoenzymes. OptiMAL-IT will reliably detect falciparum down to 0.01% parasitemia and non-falciparum down to 0.1%. Paracheck-Pf will detect parasitemias down to0.002% but will not distinguish between falciparum and non-falciparum malaria.Parasite nucleic acids are detected using polymerase chain reaction. This
technique is more accurate than microscopy. However, it is expensive, andrequires a specialized laboratory. Moreover, levels of parasitemia are notnecessarily correlative with the progression of disease, particularly when theparasite is able to adhere to blood vessel walls. Therefore more sensitive, low-tech diagnosis tools need to be developed in order to detect low levels of parasitaemia in the field. Areas that cannot afford even simple laboratorydiagnostic tests often use only a history of subjective fever as the indication totreat for malaria. Using Giemsa-stained blood smears from children in Malawi, onestudy showed that unnecessary treatment for malaria was significantly decreasedwhen clinical predictors (rectal temperature, nailbed pallor, and splenomegaly)
were used as treatment indications, rather than the current national policy of using only a history of subjective fevers (sensitivity increased from 21% to 41%).[65]
MOLECULAR METHODS
Molecular methods are available in some clinical laboratories and rapid real-timeassays (for example, QT-NASBA based on the polymerase chain reaction)[66] arebeing developed with the hope of being able to deploy them in endemic areas.
LABORATORY TESTS
OptiMAL-IT will reliably detect falciparum down to 0.01% parasitemia and non-falciparum down to 0.1%. Paracheck-Pf will detect parasitemias down to 0.002%but will not distinguish between falciparum and non-falciparum malaria. Parasitenucleic acids are detected using polymerase chain reaction. This technique ismore accurate than microscopy. However, it is expensive, and requires aspecialized laboratory. Moreover, levels of parasitemia are not necessarily

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 42/61
correlative with the progression of disease, particularly when the parasite is ableto adhere to blood vessel walls. Therefore more sensitive, low-tech diagnosis toolsneed to be developed in order to detect low levels of parasitaemia in the field. [67]
Treatment
Active malaria infection with P. falciparum is a medical emergency requiringhospitalization. Infection with P. vivax , P. ovale or P. malariae can often betreated on an outpatient basis. Treatment of malaria involves supportivemeasures as well as specific antimalarial drugs. When properly treated, someonewith malaria can expect a complete recovery.[68]
ANTIMALARIAL DRUGS
Further information: Antimalarial drugs There are several families of drugs used to treat malaria. Chloroquine is very
cheap and, until recently, was very effective, which made it the antimalarial drugof choice for many years in most parts of the world. However, resistance of Plasmodium falciparum to chloroquine has spread recently from Asia to Africa,making the drug ineffective against the most dangerous Plasmodium strain inmany affected regions of the world. In those areas where chloroquine is stilleffective it remains the first choice. Unfortunately, chloroquine-resistance isassociated with reduced sensitivity to other drugs such as quinine andamodiaquine.[69]
There are several other substances which are used for treatment and, partially,for prevention (prophylaxis). Many drugs may be used for both purposes; larger
doses are used to treat cases of malaria. Their deployment depends mainly on thefrequency of resistant parasites in the area where the drug is used. One drugcurrently being investigated for possible use as an anti-malarial, especially fortreatment of drug-resistant strains, is the beta blocker propranolol. Propranololhas been shown to block both Plasmodium' s ability to enter red blood cell andestablish an infection, as well as parasite replication. A December 2006 study byNorthwestern University researchers suggested that propranolol may reduce thedosages required for existing drugs to be effective against P. falciparum by 5- to10-fold, suggesting a role in combination therapies.[70]
Currently available anti-malarial drugs include:[71]
• Artemether -lumefantrine (Therapy only, commercial names Coartem and Riamet )• Artesunate-amodiaquine (Therapy only)• Artesunate-mefloquine (Therapy only)• Artesunate-Sulfadoxine/ pyrimethamine (Therapy only)• Atovaquone- proguanil, trade name Malarone (Therapy and prophylaxis)• Quinine (Therapy only)

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 43/61
• Chloroquine (Therapy and prophylaxis; usefulness now reduced due to resistance)• Cotrifazid (Therapy and prophylaxis)• Doxycycline (Therapy and prophylaxis)• Mefloquine, trade name Lariam (Therapy and prophylaxis)• Primaquine (Therapy in P. vivax and P. ovale only; not for prophylaxis)•
Proguanil (Prophylaxis only)• Sulfadoxine- pyrimethamine (Therapy; prophylaxis for semi-immune pregnantwomen in endemic countries as "Intermittent Preventive Treatment" - IPT)
• Hydroxychloroquine, trade name Plaquenil (Therapy and prophylaxis)
The development of drugs was facilitated when Plasmodium falciparum wassuccessfully cultured.[72] This allowed in vitro testing of new drug candidates.
Extracts of the plant Artemisia annua, containing the compound artemisinin orsemi-synthetic derivatives (a substance unrelated to quinine), offer over 90%efficacy rates, but their supply is not meeting demand.[73] In 2007, the Bill &
Melinda Gates Foundation contributed $13.6m to support research at theUniversity of York to develop fast and high-yield strains of artemisia, withresearchers predicting an increase in yield of up to 1000% compared to currentvarieties.[74] One study in Rwanda showed that children with uncomplicated P.falciparum malaria demonstrated fewer clinical and parasitological failures onpost-treatment day 28 when amodiaquine was combined with artesunate, ratherthan administered alone (OR = 0.34). However, increased resistance toamodiaquine during this study period was also noted.[75] Since 2001 the WorldHealth Organization has recommended using artemisinin-based combinationtherapy (ACT) as first-line treatment for uncomplicated malaria in areas
experiencing resistance to older medications. The most recent WHO treatmentguidelines for malaria recommend four different ACTs. While numerous countries,including most African nations, have adopted the change in their official malariatreatment policies, cost remains a major barrier to ACT implementation. BecauseACTs cost up to twenty times as much as older medications, they remainunaffordable in many malaria-endemic countries. The molecular target of artemisinin is controversial, although recent studies suggest that SERCA, acalcium pump in the endoplasmic reticulum may be associated with artemisininresistance.[76] Malaria parasites can develop resistance to artemisinin andresistance can be produced by mutation of SERCA.[77] However, other studiessuggest the mitochondrion is the major target for artemisinin and its analogs.[78]
In February 2002, the journal Science and other press outlets[79] announcedprogress on a new treatment for infected individuals. A team of French and SouthAfrican researchers had identified a new drug they were calling "G25".[80] It curedmalaria in test primates by blocking the ability of the parasite to copy itself withinthe red blood cells of its victims. In 2005 the same team of researchers publishedtheir research on achieving an oral form, which they refer to as "TE3" or "te3".[81]

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 44/61
As of early 2006, there is no information in the mainstream press as to when thisfamily of drugs will become commercially available.
In 1996, Professor Geoff McFadden stumbled upon the work of British biologistIan Wilson, who had discovered that the plasmodia responsible for causing
malaria retained parts of chloroplasts,[82]
an organelle usually found in plants,complete with their own functioning genomes. This led Professor McFadden to therealisation that any number of herbicides may in fact be successful in the fightagainst malaria, and so he set about trialing large numbers of them, and enjoyeda 75% success rate.
These "apicoplasts" are thought to have originated through the endosymbiosis of algae[83] and play a crucial role in fatty acid bio-synthesis in plasmodia.[84] To date,466 proteins have been found to be produced by apicoplasts[85] and these are nowbeing looked at as possible targets for novel anti-malarial drugs.
Although effective anti-malarial drugs are on the market, the disease remains athreat to people living in endemic areas who have no proper and prompt access toeffective drugs. Access to pharmacies and health facilities, as well as drug costs,are major obstacles. Médecins Sans Frontières estimates that the cost of treatinga malaria-infected person in an endemic country was between US$0.25 and $2.40per dose in 2002.[86]
COUNTERFEIT DRUGS
Sophisticated counterfeits have been found in several Asian countries such as
Cambodia,
[87]
China,
[88]
Indonesia, Laos, Thailand, Vietnam and are an importantcause of avoidable death in these countries.[89] WHO have said that studiesindicate that up to 40% of artesunate based malaria medications are counterfeit,especially in the Greater Mekong region and have established a rapid alert systemto enable information about counterfeit drugs to be rapidly reported to therelevant authorities in participating countries.[90] There is no reliable way fordoctors or lay people to detect counterfeit drugs without help from a laboratory.Companies are attempting to combat the persistence of counterfeit drugs by usingnew technology to provide security from source to distribution.
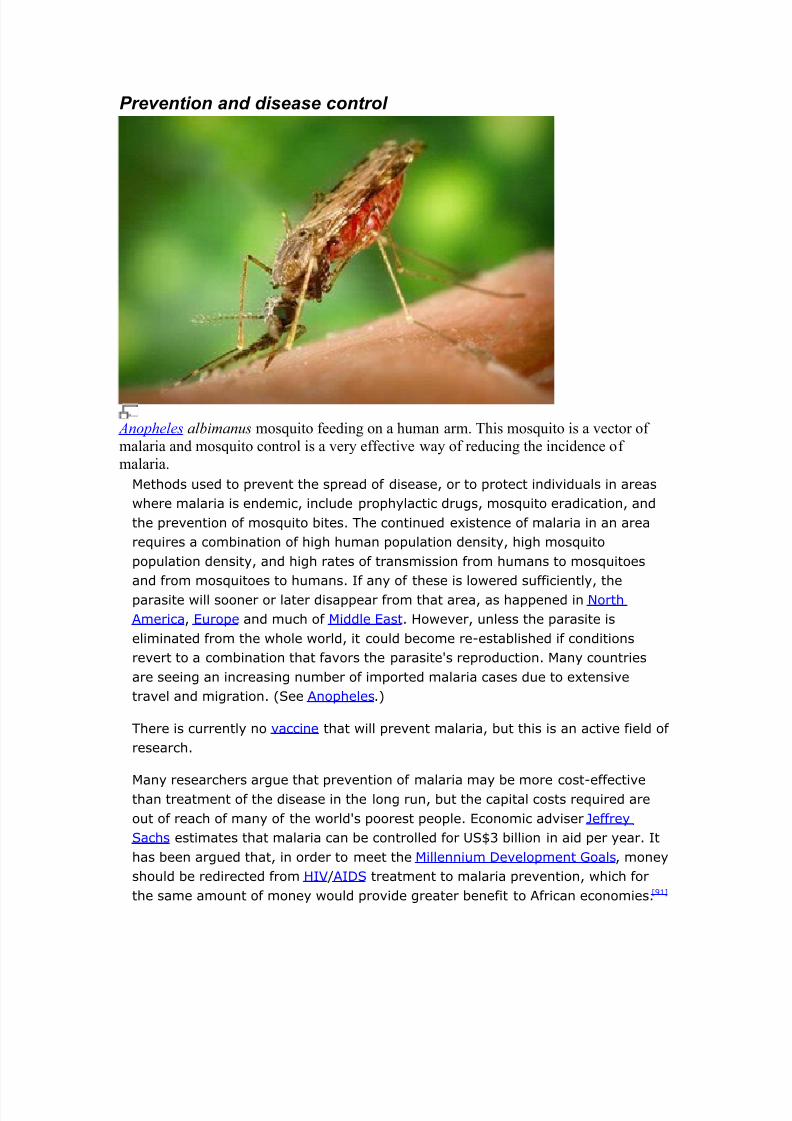
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 45/61
Prevention and disease control
Anopheles albimanus mosquito feeding on a human arm. This mosquito is a vector of malaria and mosquito control is a very effective way of reducing the incidence of malaria.
Methods used to prevent the spread of disease, or to protect individuals in areaswhere malaria is endemic, include prophylactic drugs, mosquito eradication, andthe prevention of mosquito bites. The continued existence of malaria in an arearequires a combination of high human population density, high mosquitopopulation density, and high rates of transmission from humans to mosquitoesand from mosquitoes to humans. If any of these is lowered sufficiently, theparasite will sooner or later disappear from that area, as happened in NorthAmerica, Europe and much of Middle East. However, unless the parasite iseliminated from the whole world, it could become re-established if conditionsrevert to a combination that favors the parasite's reproduction. Many countriesare seeing an increasing number of imported malaria cases due to extensivetravel and migration. (See Anopheles.)
There is currently no vaccine that will prevent malaria, but this is an active field of research.
Many researchers argue that prevention of malaria may be more cost-effectivethan treatment of the disease in the long run, but the capital costs required areout of reach of many of the world's poorest people. Economic adviser JeffreySachs estimates that malaria can be controlled for US$3 billion in aid per year. Ithas been argued that, in order to meet the Millennium Development Goals, moneyshould be redirected from HIV /AIDS treatment to malaria prevention, which forthe same amount of money would provide greater benefit to African economies.[91]

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 46/61
Brazil, Eritrea, India, and Vietnam have, unlike many other developing nations,successfully reduced the malaria burden. Common success factors includedconducive country conditions, a targeted technical approach using a package of effective tools, data-driven decision-making, active leadership at all levels of government, involvement of communities, decentralized implementation and
control of finances, skilled technical and managerial capacity at national and sub-national levels, hands-on technical and programmatic support from partneragencies, and sufficient and flexible financing.[92]
VECTOR CONTROL
Further information: Mosquito control Before DDT, malaria was successfully eradicated or controlled also in severaltropical areas by removing or poisoning the breeding grounds of the mosquitoesor the aquatic habitats of the larva stages, for example by filling or applying oil to
places with standing water. These methods have seen little application in Africafor more than half a century.[93]
Efforts to eradicate malaria by eliminating mosquitoes have been successful insome areas. Malaria was once common in the United States and southern Europe,but the draining of wetland breeding grounds and better sanitation, in conjunctionwith the monitoring and treatment of infected humans, eliminated it from affluentregions. In 2002, there were 1,059 cases of malaria reported in the US, includingeight deaths. In five of those cases, the disease was contracted in the UnitedStates. Malaria was eliminated from the northern parts of the USA in the earlytwentieth century, and the use of the pesticide DDT eliminated it from the South
by 1951. In the 1950s and 1960s, there was a major public health effort toeradicate malaria worldwide by selectively targeting mosquitoes in areas wheremalaria was rampant.[94] However, these efforts have so far failed to eradicatemalaria in many parts of the developing world - the problem is most prevalent inAfrica.
Sterile insect technique is emerging as a potential mosquito control method.Progress towards transgenic, or genetically modified, insects suggest that wildmosquito populations could be made malaria-resistant. Researchers at ImperialCollege London created the world's first transgenic malaria mosquito,[95] with the
first plasmodium-resistant species announced by a team at Case Western ReserveUniversity in Ohio in 2002.[96] Successful replacement of existent populations withgenetically modified populations, relies upon a drive mechanism, such astransposable elements to allow for non-Mendelian inheritance of the gene of interest.
On December 21, 2007, a study published in PLoS Pathogens found that thehemolytic C-type lectin CEL-III from Cucumaria echinata, a sea cucumber found

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 47/61
in the Bay of Bengal, impaired the development of the malaria parasite whenproduced by transgenic mosquitoes.[97][98] This could potentially be used one dayto control malaria by using genetically modified mosquitoes refractory to theparasites, although the authors of the study recognize that there are numerousscientific and ethical problems to be overcome before such a control strategy
could be implemented.
PROPHYLACTIC DRUGS
Main article: Malaria prophylaxis
Several drugs, most of which are also used for treatment of malaria, can be takenpreventively. Generally, these drugs are taken daily or weekly, at a lower dosethan would be used for treatment of a person who had actually contracted thedisease. Use of prophylactic drugs is seldom practical for full-time residents of malaria-endemic areas, and their use is usually restricted to short-term visitors
and travelers to malarial regions. This is due to the cost of purchasing the drugs,negative side effects from long-term use, and because some effective anti-malarial drugs are difficult to obtain outside of wealthy nations.
Quinine was used starting in the seventeenth century as a prophylactic againstmalaria. The development of more effective alternatives such as quinacrine,chloroquine, and primaquine in the twentieth century reduced the reliance onquinine. Today, quinine is still used to treat chloroquine resistant Plasmodium
falciparum, as well as severe and cerebral stages of malaria, but is not generallyused for prophylaxis. Of interesting historical note is the observation by SamuelHahnemann in the late 18th century that over-dosing of quinine leads to a
symptomatic state very similar to that of malaria itself. This lead Hahnemann todevelop the medical Law of Similars, and the subsequent medical system of Homeopathy.
Modern drugs used preventively include mefloquine (Lariam), doxycycline (available generically), and the combination of atovaquone and proguanil hydrochloride (Malarone). The choice of which drug to use depends on whichdrugs the parasites in the area are resistant to, as well as side-effects and otherconsiderations. The prophylactic effect does not begin immediately upon startingtaking the drugs, so people temporarily visiting malaria-endemic areas usually
begin taking the drugs one to two weeks before arriving and must continue takingthem for 4 weeks after leaving (with the exception of atovaquone proguanil thatonly needs be started 2 days prior and continued for 7 days afterwards).
INDOOR RESIDUAL SPRAYING
Indoor residual spraying (IRS) is the practice of spraying insecticides on theinterior walls of homes in malaria effected areas. After feeding, many mosquito

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 48/61
species rest on a nearby surface while digesting the bloodmeal, so if the walls of dwellings have been coated with insecticides, the resting mosquitos will be killedbefore they can bite another victim, transferring the malaria parasite.
The first and historically the most popular insecticide used for IRS is DDT. While it
was initially used to exclusively to combat malaria, its use quickly spread toagriculture. In time, pest-control, rather than disease-control, came to dominateDDT use, and this large-scale agricultural use led to the evolution of resistantmosquitoes in many regions. During the 1960s, awareness of the negativeconsequences of its indiscriminate use increased ultimately leading to bans onagricultural applications of DDT in many countries in the 1970s.
Though DDT has never been banned for use in malaria control and there areseveral other insecticides suitable for IRS, some advocates have claimed thatbans are responsible for tens of millions of deaths in tropical countries where DDThad once been effective in controlling malaria. Furthermore, most of the problems
associated with DDT use stem specifically from its industrial-scale application inagriculture, rather than its use in public health.[99]
The World Health Organization (WHO) currently advises the use of 12 differentinsecticides in IRS operations. These include DDT and a series of alternativeinsecticides (such as the pyrethroids permethrin and deltamethrin) to bothcombat malaria in areas where mosquitoes are DDT-resistant, and to slow theevolution of resistance.[100] This public health use of small amounts of DDT ispermitted under the Stockholm Convention on Persistent Organic Pollutants (POPs), which prohibits the agricultural use of DDT.[101] However, because of its
legacy, many developed countries discourage DDT use even in small quantities.[102]
MOSQUITO NETS AND BEDCLOTHES
Mosquito nets help keep mosquitoes away from people, and thus greatly reducethe infection and transmission of malaria. The nets are not a perfect barrier, sothey are often treated with an insecticide designed to kill the mosquito before ithas time to search for a way past the net. Insecticide-treated nets (ITN) areestimated to be twice as effective as untreated nets,[91] and offer greater than70% protection compared with no net.[103] Since the Anopheles mosquitoes feed atnight, the preferred method is to hang a large "bed net" above the center of a bedsuch that it drapes down and covers the bed completely.
The distribution of mosquito nets impregnated with insecticide (often permethrin or deltamethrin) has been shown to be an extremely effective method of malariaprevention, and it is also one of the most cost-effective methods of prevention.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 49/61
These nets can often be obtained for around US$2.50 - $3.50 (2-3 euro) from theUnited Nations, the World Health Organization, and others.
For maximum effectiveness, the nets should be re-impregnated with insecticideevery six months. This process poses a significant logistical problem in rural
areas. New technologies like Olyset or DawaPlus allow for production of long-lasting insecticidal mosquito nets (LLINs), which release insecticide forapproximately 5 years,[104] and cost about US$5.50. ITNs have the advantage of protecting people sleeping under the net and simultaneously killing mosquitoesthat contact the net. This has the effect of killing the most dangerous mosquitoes.Some protection is also provided to others, including people sleeping in the sameroom but not under the net.
Unfortunately, the cost of treating malaria is high relative to income, and theillness results in lost wages. Consequently, the financial burden means that thecost of a mosquito net is often unaffordable to people in developing countries,
especially for those most at risk. Only 1 out of 20 people in Africa own a bed net.[91] Although shipped into Africa mainly from Europe as free development help, thenets quickly become expensive trade goods. They are mainly used for fishing, andby combining hundreds of donated mosquito nets, whole river sections can becompletely shut off, catching even the smallest fish.[105]
A study among Afghan refugees in Pakistan found that treating top-sheets andchaddars (head coverings) with permethrin has similar effectiveness to using atreated net, but is much cheaper.[106]
A new approach, announced in Science on June 10, 2005, uses spores of thefungus Beauveria bassiana, sprayed on walls and bed nets, to kill mosquitoes.While some mosquitoes have developed resistance to chemicals, they have notbeen found to develop a resistance to fungal infections.[107]
VACCINATION
Further information: Malaria vaccine Vaccines for malaria are under development, with no completely effective vaccineyet available. The first promising studies demonstrating the potential for a malariavaccine were performed in 1967 by immunizing mice with live, radiation-
attenuated sporozoites, providing protection to about 60% of the mice uponsubsequent injection with normal, viable sporozoites.[108] Since the 1970s, therehas been a considerable effort to develop similar vaccination strategies withinhumans. It was determined that an individual can be protected from a P.
falciparum infection if they receive over 1000 bites from infected, irradiatedmosquitoes.[109]

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 50/61
It has been generally accepted that it is impractical to provide at-risk individualswith this vaccination strategy, but that has been recently challenged with workbeing done by Dr. Stephen Hoffman of Sanaria, one of the key researchers whooriginally sequenced the genome of Plasmodium falciparum. His work mostrecently has revolved around solving the logistical problem of isolating and
preparing the parasites equivalent to a 1000 irradiated mosquitoes for massstorage and inoculation of human beings. The company has recently receivedseveral multi-million dollar grants from the Bill & Melinda Gates Foundation andthe U.S. government to begin early clinical studies in 2007 and 2008.[110] TheSeattle Biomedical Research Institute (SBRI), funded by the Malaria VaccineInitiative, assures potential volunteers that "the [2009] clinical trials won't be alife-threatening experience. While many volunteers [in Seattle] will actuallycontract malaria, the cloned strain used in the experiments can be quickly cured,and does not cause a recurring form of the disease." "Some participants will getexperimental drugs or vaccines, while others will get placebo."[111]
Instead, much work has been performed to try and understand the immunological processes that provide protection after immunization with irradiated sporozoites.After the mouse vaccination study in 1967,[108] it was hypothesized that theinjected sporozoites themselves were being recognized by the immune system,which was in turn creating antibodies against the parasite. It was determined thatthe immune system was creating antibodies against the circumsporozoite protein(CSP) which coated the sporozoite.[112] Moreover, antibodies against CSPprevented the sporozoite from invading hepatocytes.[113] CSP was thereforechosen as the most promising protein on which to develop a vaccine against themalaria sporozoite. It is for these historical reasons that vaccines based on CSPare the most numerous of all malaria vaccines.
Presently, there is a huge variety of vaccine candidates on the table. Pre-erythrocytic vaccines (vaccines that target the parasite before it reaches theblood), in particular vaccines based on CSP, make up the largest group of research for the malaria vaccine. Other vaccine candidates include: those thatseek to induce immunity to the blood stages of the infection; those that seek toavoid more severe pathologies of malaria by preventing adherence of the parasiteto blood venules and placenta; and transmission-blocking vaccines that wouldstop the development of the parasite in the mosquito right after the mosquito has
taken a bloodmeal from an infected person.[114] It is hoped that the sequencing of the P. falciparum genome will provide targets for new drugs or vaccines.[115]
The first vaccine developed that has undergone field trials, is the SPf66,developed by Manuel Elkin Patarroyo in 1987. It presents a combination of antigens from the sporozoite (using CS repeats) and merozoite parasites. Duringphase I trials a 75% efficacy rate was demonstrated and the vaccine appeared tobe well tolerated by subjects and immunogenic. The phase IIb and III trials were

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 51/61
less promising, with the efficacy falling to between 38.8% and 60.2%. A trial wascarried out in Tanzania in 1993 demonstrating the efficacy to be 31% after ayears follow up, however the most recent (though controversial) study in theGambia did not show any effect. Despite the relatively long trial periods and thenumber of studies carried out, it is still not known how the SPf66 vaccine confers
immunity; it therefore remains an unlikely solution to malaria. The CSP was thenext vaccine developed that initially appeared promising enough to undergo trials.It is also based on the circumsporoziote protein, but additionally has therecombinant (Asn-Ala-Pro15Asn-Val-Asp-Pro)2-Leu-Arg(R32LR) protein covalentlybound to a purified Pseudomonas aeruginosa toxin (A9). However at an earlystage a complete lack of protective immunity was demonstrated in thoseinoculated. The study group used in Kenya had an 82% incidence of parasitaemiawhilst the control group only had an 89% incidence. The vaccine intended tocause an increased T-lymphocyte response in those exposed, this was also notobserved.
The efficacy of Patarroyo's vaccine has been disputed with some US scientistsconcluding in The Lancet (1997) that "the vaccine was not effective and should bedropped" while the Colombian accused them of "arrogance" putting down theirassertions to the fact that he came from a developing country.
The RTS,S/AS02A vaccine is the candidate furthest along in vaccine trials. It isbeing developed by a partnership between the PATH Malaria Vaccine Initiative (agrantee of the Gates Foundation), the pharmaceutical company, GlaxoSmithKline,and the Walter Reed Army Institute of Research[116] In the vaccine, a portion of CSP has been fused to the immunogenic "S antigen" of the hepatitis B virus; this
recombinant protein is injected alongside the potent AS02A adjuvant.[114] InOctober 2004, the RTS,S/AS02A researchers announced results of a Phase IIbtrial, indicating the vaccine reduced infection risk by approximately 30% andseverity of infection by over 50%. The study looked at over 2,000 Mozambican children.[117] More recent testing of the RTS,S/AS02A vaccine has focused on thesafety and efficacy of administering it earlier in infancy: In October 2007, theresearchers announced results of a phase I/IIb trial conducted on 214Mozambican infants between the ages of 10 and 18 months in which the fullthree-dose course of the vaccine led to a 62% reduction of infection with noserious side-effects save some pain at the point of injection.[118] Further research
will delay this vaccine from commercial release until around 2011.[119]
OTHER METHODS
Education in recognising the symptoms of malaria has reduced the number of cases in some areas of the developing world by as much as 20%. Recognising thedisease in the early stages can also stop the disease from becoming a killer.Education can also inform people to cover over areas of stagnant, still water eg

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 52/61
Water Tanks which are ideal breeding grounds for the parasite and mosquito thus,cutting down the risk of the transmission between people. This is most put inpractice in urban areas where there is large centres of population in a confinedspace and transmission would be most likely in these areas.
The Malaria Control Project is currently using downtime computing power donatedby individual volunteers around the world (see Volunteer computing and BOINC)to simulate models of the health effects and transmission dynamics in order tofind the best method or combination of methods for malaria control. Thismodeling is extremely computer intensive due to the simulations of large humanpopulations with a vast range of parameters related to biological and social factorsthat influence the spread of the disease. It is expected to take a few months usingvolunteered computing power compared to the 40 years it would have taken withthe current resources available to the scientists who developed the program.[120]
An example of the importance of computer modelling in planning malaria
eradication programs is shown in the paper by Águas and others. They showedthat eradication of malaria is crucially dependent on finding and treating the largenumber of people in endemic areas with asymptomatic malaria, who act as areservoir for infection.[121] The malaria parasites do not affect animal species andtherefore eradication of the disease from the human population would beexpected to be effective.
See also
• The Global Fund to Fight AIDS, Tuberculosis and Malaria
References
1. ^ Snow RW, Guerra CA, Noor AM, Myint HY, Hay SI (2005). "The global distributionof clinical episodes of Plasmodium falciparum malaria". Nature 434 (7030): 214–7.doi:10.1038/nature03342. PMID 15759000.
2. ^ Joy D, Feng X, Mu J, et al (2003). "Early origin and recent expansion of Plasmodiumfalciparum". Science 300 (5617): 318–21. doi:10.1126/science.1081449. PMID 12690197.
3. ^ Escalante A, Freeland D, Collins W, Lal A (1998). "The evolution of primate malaria parasites based on the gene encoding cytochrome b from the linear mitochondrialgenome". Proc Natl Acad Sci USA 95 (14): 8124–9. doi:10.1073/pnas.95.14.8124. PMID9653151.
4. ^ Cox F (2002). "History of human parasitology". Clin Microbiol Rev 15 (4): 595–612.doi:10.1128/CMR.15.4.595-612.2002. PMID 12364371.
5. ^ "Biography of Alphonse Laveran". The Nobel Foundation. Retrieved on 2007-06-15. ] Nobel foundation. Accessed 25 Oct 2006
6. ^ "Ettore Marchiafava". Retrieved on 2007-06-15.7. ^ Tan SY, Sung H (May 2008). "Carlos Juan Finlay (1833-1915): of mosquitoes and yellow
fever ". Singapore Med J 49 (5): 370–1. PMID 18465043.
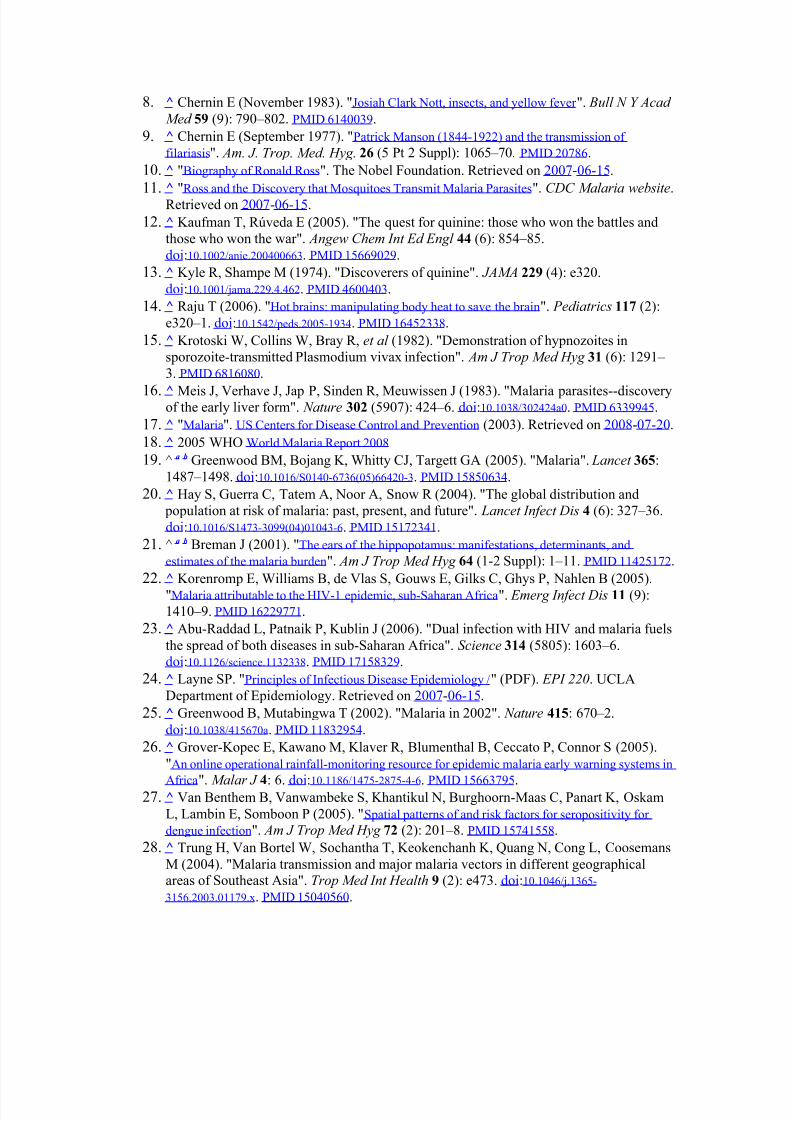
8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 53/61
8. ^ Chernin E (November 1983). "Josiah Clark Nott, insects, and yellow fever ". Bull N Y Acad
Med 59 (9): 790–802. PMID 6140039. 9. ^ Chernin E (September 1977). "Patrick Manson (1844-1922) and the transmission of
filariasis". Am. J. Trop. Med. Hyg. 26 (5 Pt 2 Suppl): 1065–70. PMID 20786. 10. ^ "Biography of Ronald Ross". The Nobel Foundation. Retrieved on 2007-06-15.11. ^ "Ross and the Discovery that Mosquitoes Transmit Malaria Parasites". CDC Malaria website.
Retrieved on 2007-06-15.12. ^ Kaufman T, Rúveda E (2005). "The quest for quinine: those who won the battles and
those who won the war". Angew Chem Int Ed Engl 44 (6): 854–85.doi:10.1002/anie.200400663. PMID 15669029.
13. ^ Kyle R, Shampe M (1974). "Discoverers of quinine". JAMA 229 (4): e320.doi:10.1001/jama.229.4.462. PMID 4600403.
14. ^ Raju T (2006). "Hot brains: manipulating body heat to save the brain". Pediatrics 117 (2):e320–1. doi:10.1542/peds.2005-1934. PMID 16452338.
15. ^ Krotoski W, Collins W, Bray R, et al (1982). "Demonstration of hypnozoites insporozoite-transmitted Plasmodium vivax infection". Am J Trop Med Hyg 31 (6): 1291– 3. PMID 6816080.
16. ^ Meis J, Verhave J, Jap P, Sinden R, Meuwissen J (1983). "Malaria parasites--discoveryof the early liver form". Nature 302 (5907): 424–6. doi:10.1038/302424a0. PMID 6339945. 17. ^ "Malaria". US Centers for Disease Control and Prevention (2003). Retrieved on 2008-07-20. 18. ^ 2005 WHO World Malaria Report 2008 19. ^ a b Greenwood BM, Bojang K, Whitty CJ, Targett GA (2005). "Malaria". Lancet 365:
1487–1498. doi:10.1016/S0140-6736(05)66420-3. PMID 15850634.20. ^ Hay S, Guerra C, Tatem A, Noor A, Snow R (2004). "The global distribution and
population at risk of malaria: past, present, and future". Lancet Infect Dis 4 (6): 327–36.doi:10.1016/S1473-3099(04)01043-6. PMID 15172341.
21. ^ a b Breman J (2001). "The ears of the hippopotamus: manifestations, determinants, andestimates of the malaria burden". Am J Trop Med Hyg 64 (1-2 Suppl): 1–11. PMID 11425172.
22. ^ Korenromp E, Williams B, de Vlas S, Gouws E, Gilks C, Ghys P, Nahlen B (2005)."Malaria attributable to the HIV-1 epidemic, sub-Saharan Africa". Emerg Infect Dis 11 (9):1410–9. PMID 16229771.
23. ^ Abu-Raddad L, Patnaik P, Kublin J (2006). "Dual infection with HIV and malaria fuelsthe spread of both diseases in sub-Saharan Africa". Science 314 (5805): 1603–6.doi:10.1126/science.1132338. PMID 17158329.
24. ^ Layne SP. "Principles of Infectious Disease Epidemiology /" (PDF). EPI 220. UCLADepartment of Epidemiology. Retrieved on 2007-06-15.
25. ^ Greenwood B, Mutabingwa T (2002). "Malaria in 2002". Nature 415: 670–2.doi:10.1038/415670a. PMID 11832954.
26. ^ Grover-Kopec E, Kawano M, Klaver R, Blumenthal B, Ceccato P, Connor S (2005)."An online operational rainfall-monitoring resource for epidemic malaria early warning systems in
Africa". Malar J 4: 6. doi:10.1186/1475-2875-4-6. PMID 15663795.27. ^ Van Benthem B, Vanwambeke S, Khantikul N, Burghoorn-Maas C, Panart K, OskamL, Lambin E, Somboon P (2005). "Spatial patterns of and risk factors for seropositivity for dengue infection". Am J Trop Med Hyg 72 (2): 201–8. PMID 15741558.
28. ^ Trung H, Van Bortel W, Sochantha T, Keokenchanh K, Quang N, Cong L, CoosemansM (2004). "Malaria transmission and major malaria vectors in different geographicalareas of Southeast Asia". Trop Med Int Health 9 (2): e473. doi:10.1046/j.1365-
3156.2003.01179.x. PMID 15040560.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 54/61
29. ^ Keiser J, Utzinger J, Caldas de Castro M, Smith T, Tanner M, Singer B (2004)."Urbanization in sub-saharan Africa and implication for malaria control". Am J Trop Med Hyg 71 (2 Suppl): 118–27. PMID 15331827.
30. ^ Hay SI, Snow RW (2006). "The Malaria Atlas Project: Developing Global Maps of MalariaRisk ". PLoS Medicine 3 (12): e473. doi:10.1371/journal.pmed.0030473. PMID 17147467.
31. ^ Sachs J, Malaney P (2002). "The economic and social burden of malaria". Nature 415:680–5. doi:10.1038/415680a. PMID 11832956.
32. ^ Roll Back Malaria. "Economic costs of malaria". WHO. Retrieved on 2006-09-21.33. ^ Malaria life cycle & pathogenesis. Malaria in Armenia. Accessed October 31, 2006.34. ^ Idro, R; Otieno G, White S, Kahindi A, Fegan G, Ogutu B, Mithwani S, Maitland K,
Neville BG, Newton CR. "Decorticate, decerebrate and opisthotonic posturing and seizures inKenyan children with cerebral malaria". Malaria Journal 4 (57): 57. doi:10.1186/1475-2875-4-
57. PMID 16336645. Retrieved on 2007-01-21. 35. ^ Boivin MJ (October 2002). "Effects of early cerebral malaria on cognitive ability in
Senegalese children". J Dev Behav Pediatr 23 (5): 353–64. PMID 12394524. 36. ^ Holding PA, Snow RW (2001). "Impact of Plasmodium falciparum malaria on performance
and learning: review of the evidence". Am. J. Trop. Med. Hyg. 64 (1-2 Suppl): 68–75. PMID
11425179.37. ^ a b c Trampuz A, Jereb M, Muzlovic I, Prabhu R (2003). "Clinical review: Severe malaria".Crit Care 7 (4): 315–23. doi:10.1186/cc2183. PMID 12930555.
38. ^ Kain K, Harrington M, Tennyson S, Keystone J (1998). "Imported malaria: prospectiveanalysis of problems in diagnosis and management". Clin Infect Dis 27 (1): 142–9.doi:10.1086/514616. PMID 9675468.
39. ^ Mockenhaupt F, Ehrhardt S, Burkhardt J, Bosomtwe S, Laryea S, Anemana S,Otchwemah R, Cramer J, Dietz E, Gellert S, Bienzle U (2004). "Manifestation andoutcome of severe malaria in children in northern Ghana". Am J Trop Med Hyg 71 (2):167–72. PMID 15306705.
40. ^ Carter JA, Ross AJ, Neville BG, Obiero E, Katana K, Mung'ala-Odera V, Lees JA, Newton CR (2005). "Developmental impairments following severe falciparum malaria in
children". Trop Med Int Health 10: 3–10. doi:10.1111/j.1365-3156.2004.01345.x. PMID15655008.
41. ^ Adak T, Sharma V, Orlov V (1998). "Studies on the Plasmodium vivax relapse patternin Delhi, India". Am J Trop Med Hyg 59 (1): 175–9. PMID 9684649.
42. ^ Mendis K, Sina B, Marchesini P, Carter R (2001). "The neglected burden of Plasmodiumvivax malaria" (PDF). Am J Trop Med Hyg 64 (1-2 Suppl): 97–106. PMID 11425182.
43. ^ Escalante A, Ayala F (1994). "Phylogeny of the malarial genus Plasmodium, derivedfrom rRNA gene sequences". Proc Natl Acad Sci USA 91 (24): 11373–7.doi:10.1073/pnas.91.24.11373. PMID 7972067.
44. ^ Garnham, PCC (1966). Malaria parasites and other haemosporidia. Blackwell ScientificPublications.
45. ^ Investing in Animal Health Research to Alleviate Poverty. International Livestock Research Institute. Permin A. and Madsen M. (2001) Appendix 2: review on diseaseoccurrence and impact (smallholder poultry). Accessed 29 Oct 2006
46. ^ Atkinson CT, Woods KL, Dusek RJ, Sileo LS, Iko WM (1995). "Wildlife disease andconservation in Hawaii: pathogenicity of avian malaria ( Plasmodium relictum) inexperimentally infected iiwi (Vestiaria coccinea)". Parasitology 111 Suppl: S59–69.PMID 8632925.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 55/61
47. ^ Talman A, Domarle O, McKenzie F, Ariey F, Robert V (2004). "Gametocytogenesis:the puberty of Plasmodium falciparum". Malar J 3: 24. doi:10.1186/1475-2875-3-24. PMID15253774.
48. ^ Marcucci C, Madjdpour C, Spahn D (2004). "Allogeneic blood transfusions: benefit,risks and clinical indications in countries with a low or high human development index". Br Med Bull 70: 15–28. doi:10.1093/bmb/ldh023. PMID 15339855.
49. ^ Bledsoe, G. H. (December 2005) "Malaria primer for clinicians in the United States" Southern Medical Journal 98(12): pp. 1197-204, (PMID: 16440920) ;
50. ^ Sturm A, Amino R, van de Sand C, Regen T, Retzlaff S, Rennenberg A, Krueger A,Pollok JM, Menard R, Heussler VT (2006). "Manipulation of host hepatocytes by themalaria parasite for delivery into liver sinusoids". Science 313: 1287–1490.doi:10.1126/science.1129720. PMID 16888102.
51. ^ Cogswell FB (January 1992). "The hypnozoite and relapse in primate malaria". Clin.
Microbiol. Rev. 5 (1): 26–35. PMID 1735093. PMC:358221.52. ^ a b Chen Q, Schlichtherle M, Wahlgren M (2000). "Molecular aspects of severe malaria".
Clin Microbiol Rev 13 (3): 439–50. doi:10.1128/CMR.13.3.439-450.2000. PMID 10885986.53. ^ Adams S, Brown H, Turner G (2002). "Breaking down the blood-brain barrier:
signaling a path to cerebral malaria?". Trends Parasitol 18 (8): 360–6. doi:10.1016/S1471-4922(02)02353-X. PMID 12377286.54. ^ Lindsay S, Ansell J, Selman C, Cox V, Hamilton K, Walraven G (2000). "Effect of
pregnancy on exposure to malaria mosquitoes". Lancet 355 (9219): 1972.doi:10.1016/S0140-6736(00)02334-5. PMID 10859048.
55. ^ van Geertruyden J, Thomas F, Erhart A, D'Alessandro U (2004). "The contribution of malaria in pregnancy to perinatal mortality". Am J Trop Med Hyg 71 (2 Suppl): 35–40. PMID15331817.
56. ^ Rodriguez-Morales AJ, Sanchez E, Vargas M, Piccolo C, Colina R, Arria M, Franco-Paredes C (2006). "Pregnancy outcomes associated with Plasmodium vivax malaria innortheastern Venezuela". Am J Trop Med Hyg 74: 755–757. PMID 16687675.
57. ^ Kwiatkowski, DP (2005). "How Malaria Has Affected the Human Genome and What Human
Genetics Can Teach Us about Malaria". Am J Hum Genet 77: 171–92. doi:10.1086/432519.PMID 16001361.
58. ^ Carter R, Mendis KN (2002). "Evolutionary and historical aspects of the burden of malaria".Clin. Microbiol. Rev. 15 (4): 564–94. doi:10.1128/CMR.15.4.564-594.2002. PMID 12364370.
59. ^ Verra F, Luoni G, Calissano C, Troye-Blomberg M, Perlmann P, Perlmann H, Arcà B,Sirima B, Konaté A, Coluzzi M, Kwiatkowski D, Modiano D (2004). "IL4-589C/T polymorphism and IgE levels in severe malaria". Acta Trop. 90 (2): 205–9.doi:10.1016/j.actatropica.2003.11.014. PMID 15177147.
60. ^ Beare NA, Taylor TE, Harding SP, Lewallen S, Molyneux ME (November 2006)."Malarial retinopathy: a newly established diagnostic sign in severe malaria". Am. J. Trop. Med. Hyg. 75 (5): 790–7. PMID 17123967. PMC:2367432.
61. ^ Redd S, Kazembe P, Luby S, Nwanyanwu O, Hightower A, Ziba C, Wirima J, Chitsulo
L, Franco C, Olivar M (2006). "Clinical algorithm for treatment of Plasmodiumfalciparum malaria in children". Lancet 347 (8996): 80. doi:10.1016/S0140-6736(96)90404-3.PMID 8551881..
62. ^ Warhurst DC, Williams JE (1996). "Laboratory diagnosis of malaria". J Clin Pathol
49: 533–38. doi:10.1136/jcp.49.7.533. PMID 8813948.63. ^ Pattanasin S, Proux S, Chompasuk D, Luwiradaj K, Jacquier P, Looareesuwan S,
Nosten F (2003). "Evaluation of a new Plasmodium lactate dehydrogenase assay

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 56/61
(OptiMAL-IT®) for the detection of malaria". Transact Royal Soc Trop Med 97: 672–4.doi:10.1016/S0035-9203(03)80100-1. PMID 16117960.
64. ^ Ling IT., Cooksley S., Bates PA., Hempelmann E., Wilson RJM. (1986). "Antibodiesto the glutamate dehydrogenase of Plasmodium falciparum". Parasitology 92,: 313–24.PMID 3086819.
65. ^ Redd S, Kazembe P, Luby S, Nwanyanwu O, Hightower A, Ziba C, Wirima J, ChitsuloL, Franco C, Olivar M (2006). "Clinical algorithm for treatment of Plasmodiumfalciparum malaria in children". Lancet 347 (8996): 80. doi:10.1016/S0140-6736(96)90404-3.PMID 8551881..
66. ^ Mens PF, Schoone GJ, Kager PA, Schallig HDFH. (2006). "Detection andidentification of human Plasmodium species with real-time quantitative nucleic acidsequence-based amplification". Malaria Journal 5 (80): 80. doi:10.1186/1475-2875-5-80.
67. ^ Redd S, Kazembe P, Luby S, Nwanyanwu O, Hightower A, Ziba C, Wirima J, ChitsuloL, Franco C, Olivar M (2006). "Clinical algorithm for treatment of Plasmodiumfalciparum malaria in children". Lancet 347 (8996): 80. doi:10.1016/S0140-6736(96)90404-3.PMID 8551881..
68. ^ If I get malaria, will I have it for the rest of my life? CDC publication, Accessed 14 Nov2006
69. ^ Tinto H, Rwagacondo C, Karema C, et al. (2006). "In-vitro susceptibility of Plasmodium falciparum to monodesethylamodiaquine, dihydroartemsinin and quinine inan area of high chloroquine resistance in Rwanda". Trans R Soc Trop Med Hyg 100 (6):509–14. doi:10.1016/j.trstmh.2005.09.018.
70. ^ Murphy S, Harrison T, Hamm H, Lomasney J, Mohandas N, Haldar K (Dec 2006)."Erythrocyte G protein as a novel target for malarial chemotherapy". PLoS Med 3 (12):e528. doi:10.1371/journal.pmed.0030528. PMID 17194200.
71. ^ Prescription drugs for malaria Retrieved February 27, 2007.72. ^ Trager W, Jensen JB. (1976). "Human malaria parasites in continuous culture". Science
193(4254): 673–5. doi:10.1126/science.781840. PMID 781840. 73. ^ Senior K (2005). "Shortfall in front-line antimalarial drug likely in 2005". Lancet Infect
Dis 5 (2): 75. PMID 15702504.74. ^ York CNAP Artemisia Project Retrieved August 30, 2008 75. ^ Rwagacondo C, Karema C, Mugisha V, Erhart A, Dujardin J, Van Overmeir C,
Ringwald P, D'Alessandro U (2004). "Is amodiaquine failing in Rwanda? Efficacy of amodiaquine alone and combined with artesunate in children with uncomplicatedmalaria". Trop Med Int Health 9 (10): 1091–8. doi:10.1111/j.1365-3156.2004.01316.x. PMID15482401..
76. ^ Eckstein-Ludwig U, Webb R, Van Goethem I, East J, Lee A, Kimura M, O'Neill P,Bray P, Ward S, Krishna S (2003). "Artemisinins target the SERCA of Plasmodiumfalciparum". Nature 424 (6951): 957–61. doi:10.1038/nature01813. PMID 12931192.
77. ^ Uhlemann A, Cameron A, Eckstein-Ludwig U, Fischbarg J, Iserovich P, Zuniga F, EastM, Lee A, Brady L, Haynes R, Krishna S (2005). "A single amino acid residue may
determine the sensitivity of SER`CAs to artemisinins". Nat Struct Mol Biol 12 (7): 628–9.doi:10.1038/nsmb947. PMID 15937493.
78. ^ Li W, Mo W, Shen D, Sun L, Wang J, Lu S, Gitschier J, Zhou B (2005). "Yeast modeluncovers dual roles of mitochondria in action of artemisinin". PLoS Genet 1 (3): e36.doi:10.1371/journal.pgen.0010036. PMID 16170412.
79. ^ Malaria drug offers new hope. BBC News 2002-02-15.80. ^ One step closer to conquering malaria

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 57/61
81. ^ Salom-Roig, X. et al . (2005) Dual molecules as new antimalarials. Combinatorial
Chemistry & High Throughput Screening 8:49-62.82. ^ "Herbicides as a treatment for malaria". Retrieved on 2007-09-25. 83. ^ Khöler, Sabine (March 1997). "A Plastid of Probable Green Algal Origin in
Apicomplexan Parasites". Science 275 (5305): 1485–1489.doi:10.1126/science.275.5305.1485. PMID 9045615.
84. ^ Gardner, Malcom (November 1998). "Chromosome 2 Sequence of the Human MalariaParasite Plasmodium falciparum". Science 282 (5391): 1126–1132.doi:10.1126/science.282.5391.1126. PMID 9804551.
85. ^ Foth, Bernado (January 2003). "Dissecting Apicoplast Targeting in the Malaria ParasitePlasmodium falciparum". Science 299 (5607): 705–708. doi:10.1126/science.1078599. PMID12560551.
86. ^ Medecins Sans Frontieres, "What is the Cost and Who Will Pay?"87. ^ Lon CT, Tsuyuoka R, Phanouvong S, et al. (2006). "Counterfeit and substandard
antimalarial drugs in Cambodia". Trans R Soc Trop Med Hyg 100 (11): 1019–24.doi:10.1016/j.trstmh.2006.01.003. PMID 16765399.
88. ^ U. S. Pharmacopeia (2004). "Fake antimalarials found in Yunan province, China" (PDF).
Retrieved on 2006-10-06.89. ^ Newton PN Green MD, Fernández FM, Day NPJ, White NJ. (2006). "Counterfeit anti-infective drugs". Lancet Infect Dis 6 (9): 602–13. doi:10.1016/S1473-3099(06)70581-3. PMID16931411.
90. ^ Jane Parry (2005). "WHO combats counterfeit malaria drugs in Asia". Retrieved on 2008-07-19.
91. ^ a b c Hull, Kevin. (2006) "Malaria: Fever Wars". PBS Documentary 92. ^ Barat L (2006). "Four malaria success stories: how malaria burden was successfully
reduced in Brazil, Eritrea, India, and Vietnam". Am J Trop Med Hyg 74 (1): 12–6. PMID16407339.
93. ^ Killeen G, Fillinger U, Kiche I, Gouagna L, Knols B (2002). "Eradication of Anophelesgambiae from Brazil: lessons for malaria control in Africa?". Lancet Infect Dis 2 (10):
e192. doi:10.1016/S1473-3099(02)00397-3. PMID 12383612.94. ^ Gladwell, Malcolm. (2001-07-02). "The Mosquito Killer ", The New Yorker.95. ^ Imperial College, London, "Scientists create first transgenic malaria mosquito", 2000-06-
22.96. ^ Ito J, Ghosh A, Moreira LA, Wimmer EA, Jacobs-Lorena M (2002). "Transgenic
anopheline mosquitoes impaired in transmission of a malaria parasite". Nature 417: 387– 8. doi:10.1038/417452a. PMID 12024215.
97. ^ BBC NEWS, Sea cucumber 'new malaria weapon' 98. ^ Yoshida S, Shimada Y, Kondoh D, et al (2007). "Hemolytic C-type lectin CEL-III from
sea cucumber expressed in transgenic mosquitoes impairs malaria parasite development". PLoS Pathog. 3 (12): e192. doi:10.1371/journal.ppat.0030192. PMID 18159942.
99. ^ Tia E, Akogbeto M, Koffi A, et al (2006). "[Pyrethroid and DDT resistance of Anopheles gambiae s.s. (Diptera: Culicidae) in five agricultural ecosystems from Côte-d'Ivoire]" (in French). Bulletin de la Société de pathologie exotique (1990) 99 (4): 278– 82. PMID 17111979.
100. ^ Indoor Residual Spraying: Use of Indoor Residual Spraying for Scaling Up GlobalMalaria Control and Elimination. World Health Organization, 2006.
101. ^ 10 Things You Need to Know about DDT Use under The Stockholm Convention 102. ^ The Stockholm Convention on persistent organic pollutants

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 58/61
103. ^ Bachou H, Tylleskär T, Kaddu-Mulindwa DH, Tumwine JK (2006)."Bacteraemia among severely malnourished children infected and uninfected with the humanimmunodeficiency virus-1 in Kampala, Uganda". BMC Infect. Dis. 6: 160. doi:10.1186/1471-
2334-6-160. PMID 17090299.104. ^ New Mosquito Nets Could Help Fight Malaria in Africa 105. ^ The Economist. "Traditional Economy of the Kavango", Economist Documentary.106. ^ Rowland M, Durrani N, Hewitt S, Mohammed N, Bouma M, Carneiro I,
Rozendaal J, Schapira A (1999). "Permethrin-treated chaddars and top-sheets:appropriate technology for protection against malaria in Afghanistan and other complexemergencies". Trans R Soc Trop Med Hyg 93 (5): 465–72. doi:10.1016/S0035-9203(99)90341-
3. PMID 10696399. 107. ^ "Fungus 'may help malaria fight'", BBC News, 2005-06-09 108. ^ a b Nussenzweig R, Vanderberg J, Most H, Orton C (1967). "Protective
immunity produced by the injection of x-irradiated sporozoites of plasmodium berghei". Nature 216 (5111): 160–2. doi:10.1038/216160a0. PMID 6057225.
109. ^ Hoffman SL, Goh LM, Luke TC, et al (2002). "Protection of humans againstmalaria by immunization with radiation-attenuated Plasmodium falciparum sporozoites".
J. Infect. Dis. 185 (8): 1155–64. doi:10.1086/339409. PMID 11930326. 110. ^ Sanaria Press and Publications 111. ^ Health | You can get paid to catch malaria | Seattle Times Newspaper 112. ^ Zavala F, Cochrane A, Nardin E, Nussenzweig R, Nussenzweig V (1983).
"Circumsporozoite proteins of malaria parasites contain a single immunodominant regionwith two or more identical epitopes". J Exp Med 157 (6): 1947–57.doi:10.1084/jem.157.6.1947.
113. ^ Hollingdale M, Nardin E, Tharavanij S, Schwartz A, Nussenzweig R (1984)."Inhibition of entry of Plasmodium falciparum and P. vivax sporozoites into culturedcells; an in vitro assay of protective antibodies". J Immunol 132 (2): 909–13. PMID6317752.
114. ^ a b Matuschewski K (2006). "Vaccine development against malaria". Curr Opin
Immunol 18 (4): 449–57. doi:10.1016/j.coi.2006.05.004. PMID 16765576.115. ^ Gardner M, Hall N, Fung E, et al (2002). "Genome sequence of the human
malaria parasite Plasmodium falciparum". Nature 370 (6906): 1543.doi:10.1038/nature01097. PMID 12368864.
116. ^ Heppner DG, Kester KE, Ockenhouse CF, et al (2005). "Towards an RTS,S- based, multi-stage, multi-antigen vaccine against falciparum malaria: progress at theWalter Reed Army Institute of Research". Vaccine 23 (17-18): 2243–50.doi:10.1016/j.vaccine.2005.01.142. PMID 15755604.
117. ^ Alonso PL, Sacarlal J, Aponte JJ, et al (2004). "Efficacy of the RTS,S/AS02Avaccine against Plasmodium falciparum infection and disease in young African children:randomised controlled trial". Lancet 364 (9443): 1411–20. doi:10.1016/S0140-6736(04)17223-
1. PMID 15488216.
118. ^ Aponte JJ, Aide P, Renom M, et al (November 2007). "Safety of theRTS,S/AS02D candidate malaria vaccine in infants living in a highly endemic area of Mozambique: a double blind randomised controlled phase I/IIb trial". Lancet 370 (9598):1543–51. doi:10.1016/S0140-6736(07)61542-6. PMID 17949807.
119. ^ Africa: Malaria - Vaccine Expected in 2011. Accra Mail. 9 January 2007. Accessed15 January 2007.
120. ^ "What is Malariacontrol.net". AFRICA@home. Retrieved on 2007-03-11.

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 59/61
121. ^ Águas R, White LJ, Snow RW, Gomes MG (2008). "Prospects for malariaeradication in sub-Saharan Africa". PLoS ONE 3 (3): e1767. doi:10.1371/journal.pone.0001767. PMID 18335042.
External links
External links[hide]General information
• Siward's Overview of Malaria An in-depth and somewhat comprehensive overviewof malaria, suitable for those starting to study it seriously.• National Geographic July 2007 Issue on Malaria
• WHO site on malariao 2006 WHO Guidelines for the Treatment of Malaria• Johns Hopkins Malariology Open Courseware
o World Malaria Report 2005• United States Centers for Disease Control - Malaria information pages
• Doctors Without Borders/Medecins Sans Frontieres - Malaria information pages• HRC/Eldis Health Resource Guide - Malaria research and resources on health in
developing countries• Medline Plus - Malaria
• Interview with Dr Andrew Speilman, Harvard malaria specialist• GlobalHealthFacts.org Malaria Cases and Deaths by Country
• Survey article: History of malaria around the North Sea• DriveAgainstMalaria.org, "World's longest journey to fight the biggest killer of
children"• Malaria Atlas Project
• UNITAID, International Facility for the Purchase of Drugs (Wikipedia Article)• World Malaria Reported Cases Map by SHOW®/World.
Vaccine and other research
• BBC - Hopes of Malaria Vaccine by 2010 15 October 2004 • BBC - Science shows how malaria hides 8 April 2005
• History of discoveries in malaria• Malaria. The UNICEF-UNDP-World Bank-WHO Special Programme for Research
and Training in Tropical Diseases • Malaria Vaccine Initiative
• Story of the discovery of the vector of the malarial parasite• Wellcome Trust against Malaria
• "Vaccines for Development" - Blog on vaccine research and production for developing countries
• Malaria and Mosquitoes - questions and answers• JoVE (Journal of Visualized Experiments): Malaria-related Experiments
Charities
• Against Malaria Foundation• Nothing But Nets

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 60/61
Mosquito Netting as Prevention
• Call for Increased Production of Long-Lasting Insecticidal Nets as Part of the U.N. Millennium Campaign
• Providing everyone with a LLIN in Sahn Malen, a small village in Sierra Leone• OnEarth Magazine » Bad Blood
DDT
• DDT and malaria vector control• WHO Position on DDT Use
• The DDT Ban Myth
Animations, images and photos
• Burden of Malaria, BBC pictures relating to malaria in northern Uganda • Malaria: Cooperation among Parasite, Vector, and Host (Animation)
• Malaria Blog from the Johns Hopkins Bloomberg School of Public Health Center for Communications Programs
• [1] Buzz and Bite Malaria Prevention Campaign
[hide] v • d • e
Infectious diseases - Parasitic disease: protozoan infection (A06-A07, B50-B64)
Apicomplexa
Coccidia (Cryptosporidiosis, Isosporiasis, Cyclosporiasis, Toxoplasmosis)
Malaria (Blackwater fever )
Babesiosis
Sarcomastigophora
Excavata/Mastigophora
Trypanosomiasis (Sleeping sickness, Chagas disease)
Leishmaniasis (Cutaneous leishmaniasis, Visceralleishmaniasis) - Trichomoniasis
Giardia lamblia (Giardiasis)
Sarcodina
Entamoeba histolytica (Amoebiasis) - Dientamoeba fragilis (Dientamoebiasis) - Naegleria fowleri (Primary
amoebic meningoencephalitis)

8/4/2019 1 Hepatic Amoebiasis
http://slidepdf.com/reader/full/1-hepatic-amoebiasis 61/61
Other
Blastocystis (Blastocystosis)
Balantidium coli (Balantidiasis)
Zygomycota , Microsporidia (Microsporidiosis)
Mesomycetozoea , Rhinosporidium seeberi (Rhinosporidiosis)
Retrieved from "http://en.wikipedia.org/wiki/Malaria"Categories: Apicomplexa | Insect-borne diseases | Malaria | Medical emergencies |Parasitic diseases | Tropical diseases | Deaths from malaria | Neglected diseasesHidden categories: Semi-protected against vandalism | All articles with unsourcedstatements | Articles with unsourced statements since July 2008
Views
• Article• Discussion• View source• History
Personal tools







![Amoebiasis: A 10 Year Retrospective Study at the ...eprints.um.edu.my/4204/1/Amoebiasis-_a_10_year... · at the University Hospital, Kuala Lumpur I ]amaiah, (M. Se) and K C Shekhar,](https://img.pdfslide.net/doc/110x75/60c53cb34796b1007f254985/amoebiasis-a-10-year-retrospective-study-at-the-at-the-university-hospital.jpg)