Embed Size (px)
Citation preview

11
Hospital Pricing Behavior for Hospital Pricing Behavior for the Uninsured: the Uninsured: Are Safety-Net Hospitals Are Safety-Net Hospitals Different?Different?
This study is funded in part by This study is funded in part by Robert Wood Johnson Foundation Robert Wood Johnson Foundation under the HCFO Programunder the HCFO Program
Katya Fonkych, MPhilGlenn Melnick, PhD
RAND Corporation
June 27, 2006

22
Background Background Rapid increase in hospital charges (list prices)Rapid increase in hospital charges (list prices)
Charges per day doubled from 2000 to 2004Charges per day doubled from 2000 to 2004
Growing billed chargesGrowing billed charges were ignored: were ignored: Managed care allowed for steep discounts Managed care allowed for steep discounts PPS fixed the real prices for governmentPPS fixed the real prices for government
Self-pay (SP) patients receive bills based on list Self-pay (SP) patients receive bills based on list prices (charges) and many are expected to pay prices (charges) and many are expected to pay themthem Media coverageMedia coverage

33
Research QuestionsResearch Questions
1.1. Do hospitals collect higher proportion of Do hospitals collect higher proportion of charges from self-pay patients than from charges from self-pay patients than from insured patients? insured patients?
2.2. Do safety net hospitals give more or less of a Do safety net hospitals give more or less of a discount for self pay patients compared to non-discount for self pay patients compared to non-safety net hospitals?safety net hospitals? Which safety-net Which safety-net dimensions matter for pricing:dimensions matter for pricing:
• Government subsidies for safety-net providersGovernment subsidies for safety-net providers• Hospitals that treat the largest uninsured populationHospitals that treat the largest uninsured population• Non-profit statusNon-profit status

44
Data and MethodsData and Methods Hospital data for descriptive and multivariate Hospital data for descriptive and multivariate
analysesanalyses California annual financial reports on acute-care hospitals:California annual financial reports on acute-care hospitals:
• Gross charges and net (received) revenue by payor class Gross charges and net (received) revenue by payor class Non-comparable hospitals excluded: Non-comparable hospitals excluded:
• CountyCounty, State, Psychiatric and Kaiser hospitals, hospitals with < 50 , State, Psychiatric and Kaiser hospitals, hospitals with < 50 uninsured patients uninsured patients
Key dependent variables Key dependent variables Collection percentageCollection percentage by payor class, within a hospital: by payor class, within a hospital:
Difference in collection percentageDifference in collection percentage bw self pay and insured bw self pay and insured
~ discount or relative price for SP patients, because:~ discount or relative price for SP patients, because:Gross charges are about the same for patients in same hospital Gross charges are about the same for patients in same hospital regardless of their payor (we checked top 20 DRG category )regardless of their payor (we checked top 20 DRG category )
% Paid (payor)= % Paid (payor)= Net Revenue (payor) / Gross Charges (payor)Net Revenue (payor) / Gross Charges (payor)
Δ Paid (com. insured) = Δ Paid (com. insured) = %Paid (self-pay) - %Paid (com. insured)%Paid (self-pay) - %Paid (com. insured)

55
Measurement of Self-Pay versus Measurement of Self-Pay versus Low Income UninsuredLow Income Uninsured
Ideally we would like to identify low-income, uninsured, Ideally we would like to identify low-income, uninsured, self pay patients, but our SP data may include:self pay patients, but our SP data may include:
1.1. International or out of state high-income patientsInternational or out of state high-income patients• 0.6% of self-paid come out of US, vs. 0.1% among all payors0.6% of self-paid come out of US, vs. 0.1% among all payors
2.2. High income patients seeking elective procedures, not High income patients seeking elective procedures, not covered by their insurancecovered by their insurance
Self-paid patients are mostly admitted through ER, unlike Self-paid patients are mostly admitted through ER, unlike commercially insured (ER is unlikely to be elective): 70% vs 40%commercially insured (ER is unlikely to be elective): 70% vs 40%
3.3. Misclassified auto accident patients, who pay their bill from Misclassified auto accident patients, who pay their bill from auto insurance coverageauto insurance coverage
However only 12% of all accidents are self-paidHowever only 12% of all accidents are self-paid
4.4. Insured patients whose charges are misclassified as SP Insured patients whose charges are misclassified as SP initially or SP patients that are misclassified as insured initially or SP patients that are misclassified as insured

66
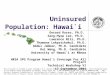
About One in 20 Patients About One in 20 Patients Is Self-Pay (CA, 2004)Is Self-Pay (CA, 2004)
4.0%
8.1%
3.9%
5.3%
0% 2% 4% 6% 8% 10%
Discharges
Visits
Days
Adjusted Days
794 thousand
135 thousand
3.42 million
1.36 million
All acute-care Californian hospitals, excluding psychiatric
Adjusted days = inpatient days and outpatient care, weighted by their relative charges

77
By 2004 SP Patients Paid Less Than By 2004 SP Patients Paid Less Than Insured But More Than GovernmentInsured But More Than Government
% Paid = Net Revenue / Gross Chargesin a given hospital (hospital-level, not patient-level)
48%
34%
0%
10%
20%
30%
40%
50%
60%
2000 2004
All self paid
Third party
MedicareMedical

88
Difference in Collection Rates BW Self Difference in Collection Rates BW Self Pay and Commercially Insured, 2004Pay and Commercially Insured, 2004
Mean ΔPaid -5.4%
1/3 of hospitals that treat 1/3 of self-pays on average collect from them more than from their commercially insured patients
0%
5%
10%
15%
20%
25%
< -30 -20 -30
-10 -20
0 -10 0+10 +10 +20
+20 +30
>+30
ΔPaid (commercial) = % Paid (self-pay) - % Paid (commercial)
% hospitals
% patients

99
Dimensions of Safety Net: Dimensions of Safety Net: Disproportionate Share HospitalsDisproportionate Share Hospitals
Hospitals that qualify for “Disproportionate Share” Hospitals that qualify for “Disproportionate Share” payment from Medicaid treat high share of low-income payment from Medicaid treat high share of low-income patients patients
Whether or not qualifyWhether or not qualify % revenue from DSH payments % revenue from DSH payments
In CA DSH hospitals must have > 25% of care provided In CA DSH hospitals must have > 25% of care provided for low-income patients, defined as indigent and Medical for low-income patients, defined as indigent and Medical
weighted towards Medicalweighted towards Medical In CA 29% of hospitals receive DSH payments (county In CA 29% of hospitals receive DSH payments (county
excluded), account for only 25% of care for self-pay excluded), account for only 25% of care for self-pay patientspatients
Profit status is another dimension of safety net: Profit status is another dimension of safety net: Non-profit hospitals are supposed to provide indigent care to Non-profit hospitals are supposed to provide indigent care to
justify their non-profit status and fulfill their missionjustify their non-profit status and fulfill their mission

1010
Dimensions of Safety Net: Dimensions of Safety Net: Hospitals with Most Self-Pay PatientsHospitals with Most Self-Pay Patients
Defined Safety-Net hospitals for Self-Pay, as those that provide most Defined Safety-Net hospitals for Self-Pay, as those that provide most access to care for uninsured (top 25% of adjusted days)access to care for uninsured (top 25% of adjusted days)
Top 25% of hospitals (82 hospitals) provide 70% of SP careTop 25% of hospitals (82 hospitals) provide 70% of SP care Only a third of top 25% hospitals (29 hospitals) are DSH => Only a third of top 25% hospitals (29 hospitals) are DSH =>
little overlaplittle overlap
Cumulative Distribution of Uninsured Patients by Hospitals
0%10%20%30%40%50%60%70%80%90%
100%
0% 25% 50% 75% 100%
% hospitals
% p
ati
en
ts
Safety Net for Self-pays

1111
Safety-Net Hospitals Safety-Net Hospitals Do NotDo Not Provide Provide Greater Discounts for SP PatientsGreater Discounts for SP Patients
AverageAverageAcrossAcross
HospitalsHospitalsNon-Non-DSHDSH DSHDSH
BottomBottom 75%75%
Top Top 25%25%
Top 25%Top 25%andand
DSHDSHFor-For-
ProfitProfitNon-Non-ProfitProfit
% Paid –% Paid –self paidself paid 35%35% 32%32% 34%34% 35%35% 34%34% 32%32% 35%35%
% Paid - % Paid - commercialcommercial 41%41% 36%36% 40%40% 36%36% 35%35% 29%29% 43%43%
Δ Paid -Δ Paid -commercialcommercial -5.9%-5.9% -3.9%-3.9% -5.8%-5.8% -4.0%-4.0% -1.4%-1.4% 3%3% -8%-8%
But non-profits do

1212
Multivariate ModelMultivariate ModelSN hospitals have different characteristics, which might be SN hospitals have different characteristics, which might be responsible for the difference in responsible for the difference in ΔPaidΔPaid : patient distribution, profit : patient distribution, profit and teaching status etc. and teaching status etc.
Dependent Variable:Dependent Variable: ΔPaid (insured) = %Paid (self-pay) - %Paid (insured)ΔPaid (insured) = %Paid (self-pay) - %Paid (insured)
Independent VariablesIndependent Variables Safety net measures (Safety net measures (DSH hospital & % revenues from DSH, DSH hospital & % revenues from DSH,
Top 25% SP, For-Profit, DSH*For-Profit) Top 25% SP, For-Profit, DSH*For-Profit) SP adjustments: % homeless, % SP accidents, % out of stateSP adjustments: % homeless, % SP accidents, % out of state Patient distribution: Outpatient SP Share, Share of commercial Patient distribution: Outpatient SP Share, Share of commercial
patientspatients Hospital characteristics: Bed Size, Rural, Teaching, Profit Margin Hospital characteristics: Bed Size, Rural, Teaching, Profit Margin
from previous yearfrom previous year

1313
Estimated Effects on ΔPaidEstimated Effects on ΔPaid (Relative Price to Self-Pay Patients)(Relative Price to Self-Pay Patients)
Safety-Net MeasuresSafety-Net Measures CoefficientCoefficient
DSH hospitalDSH hospital 0.0740.074
DSH & for-profitDSH & for-profit 0.0480.048
% Revenues from DSH% Revenues from DSH -0.875*-0.875*
Top 25% SP HospitalTop 25% SP Hospital 0.092**0.092**
For-profitFor-profit 0.108**0.108**
Other significant Other significant variablesvariables CoefficientCoefficient
% commercial patients% commercial patients 0.236*0.236*
% Homeless% Homeless -6.558*-6.558*
% Out of California% Out of California -0.282*-0.282*
Profit margin 2003Profit margin 2003 -0.280**-0.280**
SN Hospitals did not offer higher discounts to SP compared to non-SN SN Hospitals did not offer higher discounts to SP compared to non-SN hospitals (CA, 2004, county hospitals excluded)hospitals (CA, 2004, county hospitals excluded)
* significant at 10%* significant at 10%
** significant at 5%** significant at 5%

1414
Subsidy Doesn’t Help to Reduce Subsidy Doesn’t Help to Reduce “Relative Price” for SP Patients“Relative Price” for SP Patients
Difference in % Paid bw Self-paid and Commercial is higher in Difference in % Paid bw Self-paid and Commercial is higher in DSH hospitals (for av. DSH payment of 6%) than in non-DSH, DSH hospitals (for av. DSH payment of 6%) than in non-DSH, for both for-profit and non-profit hospitalsfor both for-profit and non-profit hospitals
-35%-30%-25%-20%-15%-10%
-5%0%5%
10%15%20%
0% 10% 20% 30%
% revenue from DSH payments
Δ P
aid
For-profit
Non-DSH
DSH
Non-profit
DSH
Non-DSH 8.5%
14%
6%

1515
Summary of FindingsSummary of Findings
Self-pays used to pay the highest average % of gross Self-pays used to pay the highest average % of gross charges in 2000, but in 2004:charges in 2000, but in 2004:
On average SP paid a bit less than commercially insured (-5.4%)On average SP paid a bit less than commercially insured (-5.4%) But in a third of hospitals, self-pays still pay on average more But in a third of hospitals, self-pays still pay on average more
than commercially insured patients. than commercially insured patients. SN providers do not provide bigger discounts to SP SN providers do not provide bigger discounts to SP
patients compared to other hospitals; patients compared to other hospitals; An average SN hospital have smaller discount than non-SNAn average SN hospital have smaller discount than non-SN This includes DSH and Top SP hospitalsThis includes DSH and Top SP hospitals
But non-profits do provide discounts (additional 11% of But non-profits do provide discounts (additional 11% of charges)charges)
Hospitals that provide most care for self-pays rarely get Hospitals that provide most care for self-pays rarely get government DSH subsidy government DSH subsidy
official “safety net” is hardly a safety net for self-paysofficial “safety net” is hardly a safety net for self-pays

1616
Policy IssuesPolicy Issues
Should we expect DSH provider to offer bigger Should we expect DSH provider to offer bigger discounts for uninsured in return for getting a discounts for uninsured in return for getting a subsidy?subsidy?
The hospitals where most SP patients receive The hospitals where most SP patients receive their care have higher relative prices than the their care have higher relative prices than the rest of the hospitalsrest of the hospitals Should those hospitals receive additional financial Should those hospitals receive additional financial
support for caring for uninsured, as DSH often doesn’t support for caring for uninsured, as DSH often doesn’t target them?target them?
Should there be regulatory or social pressure to limit Should there be regulatory or social pressure to limit prices to the uninsured?prices to the uninsured?