-
7/29/2019 1. IHD
1/73
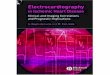
This is the external appearance of anormal heart.The epicardial
surface
is smooth and glistening.The
amount of epicardial fat is
usual.The left anterior descending
coronary artery extends down from
the aortic root to the apex.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV002.html
-
7/29/2019 1. IHD
2/73
The anterior surface of the heart
demonstrates an opened left anteriordescending coronary
artery.Within the
lumen of the coronary can be seen a dark
red recent coronary thrombosis. The dull
red color to the myocardium as seen below
the glistening epicardium to the lower right
of the thrombus is consistent with
underlying myocardial infarction.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV108.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV018.html
-
7/29/2019 1. IHD
3/73
-
7/29/2019 1. IHD
4/73
-
7/29/2019 1. IHD
5/73
-
7/29/2019 1. IHD
6/73
-
7/29/2019 1. IHD
7/73
-
7/29/2019 1. IHD
8/73
-
7/29/2019 1. IHD
9/73
-
7/29/2019 1. IHD
10/73
-
7/29/2019 1. IHD
11/73
RISK FACTORS
The prevalence and severity of the disease
among individuals and groups are related to a
number of factors,
uncontrollable,
potentially capable of control.
-
7/29/2019 1. IHD
12/73
NonModifiable Risk Factors
Age
Sex
Family History
Genetics abnormalities
-
7/29/2019 1. IHD
13/73
Potentially Controllable Major
Risk Factors,
Diabetes
Hypertension
Smoking
Hyperlipidemia
-
7/29/2019 1. IHD
14/73
Other risk factors
Stress
Physical inactivity
Obesity
Postmenopausal estrogen deficiency
High carbohydrate intake
Lipoproteins
Chlamydia pneumoinae
-
7/29/2019 1. IHD
15/73
Reduction ( 75%) in the lumen of coronary artery
Acute plaque changes
Fissuring
Hemorrhages
Rupture
Markedly eccentric
Large soft core of necrotic debries
Macrophages metalloproteases
-
7/29/2019 1. IHD
16/73
Coronary artery thrombosis
Exposure of sub-endothelial collagen
Platelet aggregation
Thrombus formation
Complete occlusion
Partial occlusion
-
7/29/2019 1. IHD
17/73
Coronary artery spasm
Exact mechanism is not clear
Thromboxane A2 vasospastic mediater
Platelet aggregates
Endothelial dysfunction
reduced relaxing factor NO
Increased adrenergic activity
Smoking
-
7/29/2019 1. IHD
18/73
-
7/29/2019 1. IHD
19/73
-
7/29/2019 1. IHD
20/73
LCA
Anterior descending
-
7/29/2019 1. IHD
21/73
RCA (posterior wall)
-
7/29/2019 1. IHD
22/73
LCA - circumflex (lateral wall)
-
7/29/2019 1. IHD
23/73
Acute occlusion (on minimal stenosis)
-
7/29/2019 1. IHD
24/73
-
7/29/2019 1. IHD
25/73
-
7/29/2019 1. IHD
26/73
-
7/29/2019 1. IHD
27/73
M I at 08 hours
-
7/29/2019 1. IHD
28/73
M I at 824 hours
-
7/29/2019 1. IHD
29/73
M I at 24 hours3 days
-
7/29/2019 1. IHD
30/73
M I at 310 days
-
7/29/2019 1. IHD
31/73
M I after 10 days
-
7/29/2019 1. IHD
32/73
After weeks and months
-
7/29/2019 1. IHD
33/73
Sequence of changes in MI
S f h i MI
-
7/29/2019 1. IHD
34/73
Sequence of changes in MI
-
7/29/2019 1. IHD
35/73
Complications
Cardiac arrhythmias (7590 %)
Left ventriculer failure (60 %)
Cardiogenic shock (10 %)
Rupture of wall , papillary muscle (4
8%)
Thromboembolism (1549 %)
Acute pericarditis ( 15%)
-
7/29/2019 1. IHD
36/73
-
7/29/2019 1. IHD
37/73
-
7/29/2019 1. IHD
38/73
Lab.diagnosis
Creatine kinase
CK
MB
Troponins
SGOT
Lactate dehydrogenase
-
7/29/2019 1. IHD
39/73
This is the external appearance of anormal heart.The epicardial
surface
is smooth and glistening.The
amount of epicardial fat is
usual.The left anterior descendingcoronary artery extends down
from
the aortic root to the apex.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV002.html
-
7/29/2019 1. IHD
40/73
This is the normal appearance of myocardial
fibers in longitudinal section. Note the centralnuclei and the
syncytial arrangement of the
fibers, some of which have pale pink
intercalated disks.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV004.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV005.html
-
7/29/2019 1. IHD
41/73
This is the tricuspid valve. The leaflets and thin anddelicate.
Just like the mitral valve, the leaflets have
thin chordae tendineae that attach the leaflet margins
to the papillary muscles of the ventricular wall below.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV002.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV004.html
-
7/29/2019 1. IHD
42/73
The coronary artery shown here has narrowingof the lumen due to
build up of atherosclerotic
plaque. Severe narrowing can lead to angina,
ischemia, and infarction.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV171.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV006.html
-
7/29/2019 1. IHD
43/73
At high magnification, the dark red thrombus is
apparent in the lumen of the coronary. Theyellow tan plaques of
atheroma narrow this
coronary significantly, and the thrombus
occludes it completely.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV019.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV124.html
-
7/29/2019 1. IHD
44/73
A thrombosis of a coronary artery is shown here in
cross section. This acute thrombosis diminishes blood
flow and leads to ischemia and/or infarction, marked
clinically by the sudden onset of chest pain.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV018.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV020.html
-
7/29/2019 1. IHD
45/73
This section of coronary artery demonstrates
remote thrombosis with recanalization to leave
only two small, narrow channels.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV005.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV007.html
-
7/29/2019 1. IHD
46/73
There is a pink to red recent thrombosis in this
narrowed coronary artery. The open, needle-like
spaces in the atheromatous plaque are
cholesterol clefts.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CV009.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV007.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV009.html
-
7/29/2019 1. IHD
47/73
A coronary artery has been opened longitudinally. The
coronary extends from left to right across the middle of the
picture and is surrounded by epicardial fat. Increased
epicardial fat correlates with increasing total body fat. There
is
a lot of fat here, suggesting one risk factor for
atherosclerosis.
This coronary shows only mild atherosclerosis, with only an
occasional ellow-tan li id la ue and no narrowin .
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV017.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV170.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV017.html
-
7/29/2019 1. IHD
48/73
This is the left coronary artery from the aortic root on
the left. Extending across the middle of the picture tothe right
is the anterior descending branch. This
coronary shows severe atherosclerosis with extensive
calcification. At the far right, there is an area of
si nificant narrowin .
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV016.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV120.html
-
7/29/2019 1. IHD
49/73
This is coronary atherosclerosis with the
complication of hemorrhage into atheromatousplaque, seen here in
the center of the
photograph. Such hemorrhage acutely may
narrow the arterial lumen.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV017.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV108.html
-
7/29/2019 1. IHD
50/73
Cross sections of this anterior descending coronary artery
demonstrate marked atherosclerosis with narrowing. This is
most pronounced at the left in the more proximal portion ofthis
artery. In general, the worst atherosclerosis is proximal,
where arterial blood flow is more turbulent. More focal
lesions
mean that angioplasty or bypass can be more useful
rocedures.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV120.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV019.html
-
7/29/2019 1. IHD
51/73
The anterior surface of the heart
demonstrates an opened left anteriordescending coronary
artery.Within the
lumen of the coronary can be seen a dark
red recent coronary thrombosis. The dull
red color to the myocardium as seen below
the glistening epicardium to the lower right
of the thrombus is consistent with
underlying myocardial infarction.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV108.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV018.html
-
7/29/2019 1. IHD
52/73
There is pale white collagen within theinterstitium between
myocardial fibers. This
represents an area of remote infarction.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV126.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV026.html
-
7/29/2019 1. IHD
53/73
This is the left ventricular wall which has been
sectioned lengthwise to reveal a large recent
myocardial infarction. The center of the infarct
contains necrotic muscle that appears yellow-tan.
Surrounding this is a zone of red hyperemia.
Remainin viable m ocardium is reddish- brown.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV124.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV021.html
-
7/29/2019 1. IHD
54/73
The myocardium beneath the endocardialsurface at the top
demonstrates pale fibrosis with
collagenization following healing of a
subendocardial myocardial infarction.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV025.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV027.html
-
7/29/2019 1. IHD
55/73
The heart is opened to reveal the left ventricular free
wall on the right and the septum in the center. Therehas been a
remote myocardial infarction that
extensively involved the anterior left ventricular free
wall and septum. The white appearance of the
endocardial surface indicates the extensive scarrin .
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV026.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV118.html
-
7/29/2019 1. IHD
56/73
There has been a previous extensive
transmural myocardial infarction
involving the free wall of the left
ventricle. Note that the thickness ofthe myocardial wall is
normal
superiorly, but inferiorly is only a
thin fibrous wall. The infarction was
so extensive that, after healing, theventricular wall was
replaced by a
thin band of collagen, forming an
aneurysm. Such an aneurysm
represents non-contractile tissue that
reduces stroke volume and strains
the remaining myocardium. The
stasis of blood in the aneurysm
predisposes to mural thrombosis.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV027.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV143.html
-
7/29/2019 1. IHD
57/73
A cross section through the heart reveals a
ventricular aneurysm with a very thin wall at the
arrow. Note how the aneurysm bulges out. The
stasis in this aneurysm allows mural thrombus,
which is present here, to form within the
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV118.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV028.html
-
7/29/2019 1. IHD
58/73
This patient underwent coronary artery bypass grafting with
autogenous vein (saphenous vein) grafts. The largest of
these
runs down the center of the heart to anastomose with the
leftanterior descending artery distally. Another graft extends in
a
"Y" fashion just to the right of this to branches of the
circumflex artery. A white temporary pacing wire extends
from the mid left surface.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV143.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV158.html
-
7/29/2019 1. IHD
59/73
This cross section through the heart demonstrates the
left ventricle on the left. Extending from the anterior
portion and into the septum is a large recent
myocardial infarction. The center is tan with
surrounding hyperemia. The infarction is "transmural"
in that it extends through the full thickness of the wall.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV020.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV127.html
-
7/29/2019 1. IHD
60/73
The earliest change histologically seen with acute
myocardial infarction in the first day is contraction
band necrosis. The myocardial fibers are beginning tolose cross
striations and the nuclei are not clearly
visible in most of the cells seen here. Note the many
irregular darker pink wavy contraction bands
extendin across the fibers.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV021.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV022.html
-
7/29/2019 1. IHD
61/73
This high power microscopic view of the myocardium
demonstrates an infarction of about 1 to 2 days in duration.
The myocardial fibers have dark red contraction bands
extending across them. The myocardial cell nuclei have almostall
disappeared. There is beginning acute inflammation.
Clinically, such an acute myocardial infarction is marked by
changes in the electrocardiogram and by a rise in the MB
fraction of creatine kinase.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CV127.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV127.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV023.html
-
7/29/2019 1. IHD
62/73
In this microscopic view of a recent myocardialinfarction, there
is extensive hemorrhage along with
myocardial fiber necrosis with contraction bands and
loss of nuclei.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV022.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV024.html
-
7/29/2019 1. IHD
63/73
This myocardial infarction is about 3 to 4 days old.There is an
extensive acute inflammatory cell infiltrate
and the myocardial fibers are so necrotic that the
outlines of them are only barely visible.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV023.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV128.html
-
7/29/2019 1. IHD
64/73
This is an intermediate myocardial infarction of 1 to 2
weeks in age. Note that there are remaining normal
myocardial fibers at the top. Below these fibers are
many macrophages along with numerous capillaries
and little collagenization.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV024.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV125.html
-
7/29/2019 1. IHD
65/73
One complication of a transmural
myocardial infarction is rupture of
the myocardium. This is mostlikely to occur in the first
week
between 3 to 5 days following the
initial event, when the myocardium
is the softest. The white arrow
marks the point of rupture in this
anterior-inferior myocardial
infarction of the left ventricular free
wall and septum. Note the dark red
blood clot forming thehemopericardium. The
hemopericardium can lead to
tamponade.
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV128.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV126.html
-
7/29/2019 1. IHD
66/73
In cross section, the point of rupture of the
myocardium is shown with the arrow. In this case,there was a
previous myocardial infarction 3 weeks
before, and another myocardial infarction occurred,
rupturing through the already thin ventricular wall 3
http://www-medlib.med.utah.edu/WebPath/CVHTML/CVIDX.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV125.htmlhttp://www-medlib.med.utah.edu/WebPath/CVHTML/CV025.html
-
7/29/2019 1. IHD
67/73
Thank you
-
7/29/2019 1. IHD
68/73
-
7/29/2019 1. IHD
69/73
-
7/29/2019 1. IHD
70/73
-
7/29/2019 1. IHD
71/73
-
7/29/2019 1. IHD
72/73
-
7/29/2019 1. IHD
73/73



















![Ikebana[1]. Ihd Pps](https://img.pdfslide.net/doc/110x75/559105e21a28abbe6f8b4601/ikebana1-ihd-pps.jpg)