Embed Size (px)
Citation preview

1
Reading The Scene
August 2012 CE Condell Medical Center
EMS System
Site Code#107200E-1212
Prepared by: Sharon Hopkins, RN, BSN, EMT-P

2
ObjectivesUpon successful completion of this module,
the EMS provider will be able to:
• 1. Describe components of the scene assessment/size-up.
• 2. Describe benefits of the windshield survey.
• 3. Define the term mechanism of injury.• 4. Describe common mechanism of
injuries and potential injuries.• 5. Define nature of illness.

3
Objectives cont’d
• 6. Describe the index of suspicion.
• 7. Describe the 4 main impacts that occur in a motor vehicle collision (MVC).
• 8. Define the term general impression.
• 9. Describe the role of critical thinking or clinical judgment
• 10.Describe the components of the primary assessment.

4
Objectives cont’d
• 11. Given a scenario, determine a general impression
• 12. Given a scenario, determine key questions to ask
• 13. Given a scenario, determine the Region X SOP to follow
• 14. Given a scenario, demonstrate the primary survey.
• 15. Successfully complete the post quiz with a score of 80% or better.

5
Scene Assessment
• Completed for every call you go on
• Opportunity to gather information
• Starts with scene safety
• Is an on-going process and subject to change
• Utilize your senses– Sight, hearing, smell

6
Scene Size-up
• First part of any patient assessment process
• Always begins with evaluation of scene safety– This includes medical and trauma calls– Evaluated in an on-going manner
• Safety can be subject to change
• After a scene size-up, you will have more patient involvement

7
Scene Size-up
• Scene safety• Take Standard Precautions
– Minimally gloves on all calls
• What’s the mechanism of injury or nature of the illness?
• Determine number of patients– Is there a clue that something more is going on?– Is there a need to activate the multiple patient plan?
• Do you need additional help?

8
The “Windshield Survey”
• Implies the survey taken prior to exiting the ambulance– Is the scene safe?– Are there any hazards you perceive?– If trauma, what clues are there regarding the
mechanism of injury?– Will you need police for traffic or crowd
control?

9
Mechanism of Injury - MOI
• A force that produced an injury– A MVC at 45 mph
• Can have common/anticipated injuries to certain situations– i.e.: orthopedic injuries from falls– Allows prediction of injuries and complications
• i.e.: blow to the chest could cause a collapsed lung
• Some injuries will be assumed present based on the MOI until proven otherwise– Cervical spine injury if the patient is complaining of
neck pain after a fall from a height

10
Common MOI
• Twisting injuries tend to affect– Hip– Femur– Knee– Tibia/fibula– Ankle– Shoulder– Elbow– ulna,/radius– Wrist

11
Common MOI
• Forced bending or extension tend to affect– Elbow– Wrist– Fingers– Femur– Knee– Foot– Cervical spine

12
Common MOI
• Direct blows may affect– Clavicle – Scapula– Shoulder girdle– Humerus– Knee– Hip– Femur

13
Common MOI
• Indirect blows may affect– Pelvis– Hip– Femur– Knee– Tibia/fibula– Shoulder– Humerus– Elbow– Ulna/radius

14
Nature of Illness
• Information obtained from a medical patient to help determine the possible problem with the patient
• Information obtained from– The scene– The patient– The family members– Bystanders

15
Index of Suspicion
• Use your “sixth sense”
• Keep heightened suspicion and open mind
• Be cautious of jumping to a diagnosis
• Don’t be swayed by the patient’s opinion– “I’m not really hurt”– “It’s just a chest cold”
• Anticipate the worse and hope for the best

16
MVC
• With every one incident 3 collisions actually occur– A vehicle collision when the vehicle strikes an
object– The body collision when the body strikes the
interior of the vehicle– Organ collisions when the organs strike the
interior surfaces of the body

17
Reading the Scene
• The type of collision helps to predict the type of injuries most likely received by your patient
• Knowing your anatomy, you can predict what body parts have been injured
• You can then predict what signs and symptoms the patient is most likely to present
• You are already formulating your treatment plan based on your anticipation of the injuries

18
Traumatic Mechanism of Injuries
• Head-on collision• Rear-end collision• Side impact collision• Rollover collision• Rotational impact collision• Falls• Blunt trauma• Penetrating trauma

19
Reading the Scene
• Your patient may not be aware of how they were injured
• Gather clues as you approach the scene
• What kind of damage to the environment do you note?
• What marks on the body are giving clues?

20
General Impression
• Your impression of the patient’s condition– Based on your scene size-up with
mechanism of injury or nature of the illness (i.e.: the patient's chief complaint)
– Based on the patient’s appearance– Meant to evolve as you gather additional
data– Drives your decision on how to treat the
patient

21
Practice Forming Your General Impression
• Read the following 4 presentations
• Determine what you consider the patient’s general impression to be
• Determine which SOP(s) would be followed?

22
General Impression Presentation #1
A 60 y/o patient complains of burning chest pain for 2 hours with SOB
• They are pale, diaphoretic and anxious
• Your general impression?– Cardiac patient until proven otherwise
• SOP to follow?– Routine Medical Care; Acute Coronary
Syndrome

23
General Impression Presentation #2
• You respond to a school for a 6 y/o who fell off the jungle gym and is not acting right
• The patient has vomited several times
• Your general impression?– Head injury
• SOP to follow?– Routine Trauma Care, Pediatric; Nausea
Management

24
General Impression Presentation #3
• Your patient was stung by a bee while drinking from a can of soda
• The patient has hives and is anxious
• Your general impression?– Allergic reaction
• SOP to follow?– Allergic Reaction
• Will be able to determine specific level of reaction after further patient assessment

25
General Impression Presentation #4
• You are called to the scene for a mother in labor
• Upon arrival the patient states they want to push
• Your general impression?– OB delivery
• SOP to follow?– Emergency Childbirth

26
Critical Thinking or Clinical Judgment
• This is based on experience• The more experience you have the better
your critical thinking skills are and the better your clinical judgment– These are difficult skills to teach – These are honed with experience– These can be improved by learning lessons
from other calls
• This is the development of your “sixth sense”

27
Primary Assessment
• First step in any patient assessment process
• Purpose – to determine any life threats• Typical progression is A-B-C
– Perform C-A-B is the patient is apneic and pulseless following the AHA guidelines
• Complete the primary assessment without interruption EXCEPT for airway problem or uncontrolled hemorrhage

28
Primary Assessment
• Form a general impression
• Assess the mental status– Include cervical spinal immobilization
simultaneously if indicated
• Assess the airway
• Assess the breathing
• Assess the circulation
• Determine the transport priority

29
General Impression
• What is the patient’s chief complaint– “Read the scene” for a traumatic event to get
clues– Ask the patient what is wrong– Don’t rely only on the initial information from
dispatch

30
Control of the Cervical Spine
• Apply manual control/immobilization of the cervical spine if there is ANY suspicion of neck or spinal injury
• A more detailed assessment will follow• Maintain manual motion restriction until
the cervical spine has been cleared or until full motion restriction has been applied– Cervical collar, back board, head blocks
• Can be used in medical situations also

31
Determine the Mental Status
• Use the AVPU scale to determine the general mental status– A – the patient is awake
• They may be alert and oriented or confused
– V – the patient responds to verbal stimulation• Any slight movement is considered a response
– P – the patient responds to some tactile stimulation with some kind of response
• Watch for any small muscle movement including a twitch or moaning & groaning
– U – the patient is totally unresponsive without any response at all

32
Assess Airway
• Is the airway open?– Can the patient speak?– Do you hear any unusual noises?
• Is suction required?–Limit to <10 seconds if suction must be
used– Is there a need for any adjunct tools to be
used?

33
Assess Breathing
• Is the patient breathing?• Is there any evidence of distress?
– If yes, do you consider it mild, moderate, or severe?
• Does the patient meet criteria for supplemental oxygen?– Signs of respiratory distress?– When the pulse oximeter is applied, is it >94%?
• Is there evidence that the patient needs ventilation support (i.e.: BVM)?

34
Assess Circulation
• Were there any signs of major hemorrhage as you approached the scene?
• Does the patient have a pulse?– What is the general rate & quality?
• Do not spend time now yourself to actually count the heart rate!!!
• Is there any hemorrhage that needs to be controlled?

35
Determine Transport Priority
• How quickly do you need to initiate transport?– A stable patient allows for more
treatment/interventions at the scene– A potentially unstable patient indicates more
rapid transport with most interventions performed enroute
– An unstable patient requires most interventions to be started while enroute
• Perform only life-saving interventions at the scene

36
Practice “Reading the Scene” and Doing Your Job
Read the following scenariosDetermine your general impressionDetermine if there is any life threat
– Is it actual or highly likely?
What more information may be needed during assessment?
Determine which SOP(s) you will need to follow

37
Scenario #1
• Your “windshield survey” as you are approaching the scene:

38
Scenario #1
• You are called to the scene for a 25 y/o female with a seizure
• Upon arrival, the patient appears unresponsive– Lying on the ground– Audible gurgling, visible oral secretions– Responds to painful stimuli with moaning
• Your general impression?– Adult with seizure activity who is now post
ictal

39
Scenario #1- Critical Thinking
• What could cause seizures?– Epilepsy?– Diabetic – most likely hypoglycemia?– History of head injury?
• What is your priority of care?– Clear the airway
• Positioning – side-lying• Suction
– Consider need for cervical spine immobilization

40
Scenario #1 – Questions to Ask
• Does anyone know the history?
• Can witnesses describe the seizure?
• Was the patient helped to the ground or did they fall?

41
Scenario #1 - Interventions
• Protect the airway
• Consider c-spine control if needed
• Obtain a blood glucose level
• Perform a head to toe assessment looking for evidence of trauma
– Prior trauma that could cause seizures
– Trauma from the seizure event

42
Scenario #1 - Critical Thinking
• Which benzodiazepine is used to terminate active seizure activity per the Region X SOP’s?– Versed
• Which route is preferred initially and why?– IN – to avoid inadvertent needle sticks
• What is the dosage schedule for adults?– 2 mg IN/IVP/IO every 2 minutes titrated to 10mg– For peds: 0.1 mg/kg– For continued or recurring seizure, contact Medical
Control (to repeat same orders to additional 10 mg)

43
Scenario #1 – Critical Thinking• If your patient is having a long term active
seizure, how would you control/support the airway?– Positioning
• Side lying to drain oral secretions– Suctioning
• Limited to <10 seconds– BVM support
• Diaphragm in spasm so patient's ventilations ineffective and too hard to evaluate quality of respirations

44
Scenario #2 – Windshield Survey
• Your patient is in the car on the left

45
Scenario #2
• You respond to the scene of a MVC
• Your windshield survey shows major front end damage with airbag deployment
• The patient was unrestrained driver who is still in the car

46
Scenario #2 – Critical Thinking• What injuries are most likely with an
unrestrained driver in a front end collision?– Great potential for injuries to all parts of the
body– “Up and over” the steering wheel
• Head and neck from windshield impact• Chest and abdominal organs from impact with
steering wheel
– “Down and under” the steering wheel• Knee, leg, hip injuries from striking the dash

47
Scenario #2 – Questions to Ask
• What are the steps in the scene size-up?Take Standard PrecautionsIs the scene safe?Number of patients?What is the MOI?Do I need help or specialized equipment?
• When do you identify potential life threats?– By the time you get to the end of the primary
assessment

48
Scenario #2 - Interventions
• Immediate control of the c-spine• Provide airway & breathing assistance if
needed• Consider need for supplemental oxygen• Determine transport priority
– Guides decisions for interventions performed on scene versus enroute
• Determine transport destination– Level I or Level II trauma center?

49
Scenario #2 – Critical Thinking
• What are the evaluations performed for spinal clearance in the field?Evaluate the mechanism of injuryEvaluate the signs and symptomsEvaluate the reliability of the patient

50
Scenario #3
• You are called to the scene for an unconscious person
• Upon arrival, you recognize the patient– You are frequently called for hypoglycemia
• The patient is agitated, clammy, unable to follow commands
• The family is unable to get the patient to eat or drink anything

51
Scenario #3 – Critical Thinking
• What could be causing the signs and symptoms (be careful of tunnel vision)– Hypoglycemia (again on this patient!!!)– Head injury– Illicit drug use– Stroke– Heat stroke

52
Scenario #3 – Questions to Ask
• Is there anyone that can provide the history of events for today?
• Can we get a blood sugar level?– Blood sugar is 32
• Is there evidence of something other than hypoglycemia causing the altered level of consciousness?– What would be evidence of other reasons for
a change in mental status?

53
Scenario #3 - Interventions
• Establish IV access
• Administer 50% Dextrose 50 ml slow IVP
• Repeat blood sugar level at least once more and more as needed
• Watch for infiltration during administration of Dextrose

54
Scenario #3 – Critical Thinking
• What happens if Dextrose infiltrates?– It is very irritating to the vein and tissues and
may cause damage
• If you are unable to establish IV access, would you place an IO in this patient?– This patient most likely should be given
Glucagon IM and transported in the absence of IV access
• IO would be indicated if the glucose level was critical for this patient and causing seizure activity

55
Scenario #3 – Critical Thinking
• You establish IV access• You administer Dextrose• Can this patient sign a release?• Yes, if the blood sugar level is assessed
and documented to be over 60– Document instructions provided to the patient– Document who will be staying with the patient– Document the IV was discontinued and that
the catheter was intact

56
Scenario #4
• As you are approaching, this is what you see:

57
Scenario #4
• You are called to the scene for an older patient who fell and can’t get up
• You notice a fresh abrasion on their chin• The patient just requests help getting up
and does not want to be evaluated or transported– They say they are sorry to “bother you”– They don’t want to take up any more of your
time

58
Scenario #4 – Critical Thinking
• Why did the patient fall?– Consider a cardiac issue or stroke for any
patient with dizziness or syncope type complaints until proven otherwise
• What injuries could this patient have?– With a chin abrasion, consider hyperextension
of the neck• This patient very likely could have a
cervical spine injury even without neurological symptoms

59
Scenario #4 – Questions to Ask
• “What made you fall?” (VERY important to ask!!!)• What is the patient’s history?• Has the patient had other recent falls?• What medications is the patient taking?
– Anticoagulants increases the risk of internal bleeding
– Sleep aids may make the patient less alert– Beta blockers, calcium channel blockers, and
ACE inhibitors (used to control High B/P) could cause a drop in pulse rates resulting in dizziness

60
Scenario #4 - Interventions
• Try to convince the patient to allow for a physical assessment
• Try to talk the patient out of signing a release– Many elderly have frail bone structures and
are prone to fractures that may not be evident at the time of injury
– It is not unusual for the patient to self-transport to the ED a few days later and find they have a fracture or dislocation somewhere

61
Scenario #5
• As you approach the scene, you notice another adult is with the patient

62
Scenario #5
• You are called to the scene for an elderly patient who fell
• The patient has a GCS of 14– They are “pleasantly confused”– Answer most questions appropriately– Is cooperative
• Your evaluation finds a probable hip fracture

63
Scenario #5 – Critical Thinking• Why would this patient be confused?
– Dementia with advanced age – Influence of their prescribed medications– Taking non-prescribed medications– Head injury from the fall
• Epidural – usually see more rapid decline after a lucid period
• Subdural – usually develops signs and symptoms gradually over a period of time
– Elderly have shrunken brain tissue and more room to bleed before vital tissue is compromised

64
Scenario #5 – Questions to Ask
• Perform routine assessment of the patient– Patient fell so should receive a head-to-toe
assessment– Evaluate the level of consciousness and try to
compare to their norm– Perform a neurological exam

65
Scenario #5 – Critical Thinking
• What are the components of a field neurological exam?– Level of consciousness (i.e.: AVPU)– Speech– GCS – Pupillary response– Motor response– Sensory test
• Most important is to evaluate the responses over time watching for a change

66
Scenario #5• What are the components of the Cincinnati
Stroke Scale?Facial droopArm driftSpeech pattern
• How are they performed?Ask the pt to smile big to show all their teethAsk the pt to hold out their arms for 10 secondsAsk the pt to repeat a phrase

67
Scenario #5 - Interventions
• Provide care for the probable hip fracture– Immobilization provided by long back board
• Evaluate distal CMS before and after moving
• Evaluate for additional injuries due to the fall
• Obtain a blood glucose level
• Bring all medication containers to the hospital

68
Scenario #6
• As you approach, this is what you observe

69
Scenario #6
• EMS called to the scene for a patient with difficulty breathing
• Patient is extremely obese• Patient is anxious, pale, diaphoretic with obvious
labored breathing• Patient is partially reclined (ambulation is difficult
due to the obesity)• Patient is “less alert” than 1 hour ago per family• Monitor shows sinus tachycardia• SpO2 80%

70
Scenario #6 – Critical Thinking
• What would cause dyspnea in this patient?A respiratory issue?A cardiac issue?Their weight?
• What would cause a low O2 saturation?Poor oximetry probe site choicePulmonary hypoperfusion
• Pulmonary embolismPoor ventilation capacity due to size

71
Scenario #6 – Critical Thinking
• Pulmonary embolism - PE– A blood clot that lodges in a pulmonary artery– Blocks blood flow thru the vessel– Is life threatening – decreased pulmonary
blood flow could cause hypoxemia risk in sedentary people or immobility (i.e.:
recent surgery, long distance travel, long-bone fractures with casting, bedridden
risk in certain populations (i.e.: pregnancy due to venous pooling, atrial fib, sickle cell anemia, oral birth control pills especially if a smoker

72
Scenario #6 - PE
• Sources of PE– Blood clots – most common– Air embolism (i.e.: during external jugular stick)– Fat embolism (i.e.: from a long bone fracture)– Amniotic fluid embolism (i.e.: during OB
delivery)– Foreign body (i.e.: sheared IV catheter tip)
• Clots tend to form with stagnation of blood (i.e.: immobility)
• Clot blocks pulmonary blood flow

73
Scenario #6 – PE Signs & Symptoms
• Depends on size & location of obstruction• Usually have sudden onset severe unexplained dyspnea• Sometimes pleuritic chest pain• Unproductive cough (or hemoptysis if cough is
productive)• Labored breathing, tachypnea• Tachycardia; occasionally dropping B/P• Often clear breath sounds• Confusion/agitation with hypoxia• May find warm, swollen, painful lower extremity (a clot)• Key: low oxygen saturation!!!
– Does not improve even with supplemental oxygen

74
Scenario #6 – PE Management
• Establish and maintain airway• Assist ventilations if necessary• Supplemental oxygen at highest flow rate
possible• Carefully monitor vital signs and EKG rhythm
– Watch for cardiac arrest
• Rapid transport• Avoid lifting legs or knees to avoid dislodging
thrombi in lower extremities

75
Scenario #6 – Questions to Ask
• Patient’s history• Medications• Description of the dyspnea
– OPQRST evaluation
• Recent travel, surgeries, periods of immobilization
• Have high index of suspicion for pulmonary embolism especially if the SpO2 is low
– High mortality rates

76
Scenario #6 - Interventions
• High flow oxygen
• If IV established, minimal fluid for now (i.e.: TKO)
• Cardiac monitor
• Frequent reassessment of vital signs
• Rapid transport

77
Scenario #6 – Critical Thinking• How would you position an obese patient
for intubation?– Use towels to elevate the shoulders – notice
ear to sternal notch line-up on the right

78
Scenario #6 – Critical Thinking• Discussion point: What transport
modifications need to be made to move and then transport an extremely obese person?

79
Scenario #6
• Did you know?
• Where are you???• BMI rough calculation = weight (lbs) x 703 height (inches)2

80
Scenario #7
• This is what you see as you approach:

81
Scenario #7
• A 58 y/o male calls for abdominal pain, belching, nauseated, and weak
• Sudden onset while bowling
• Is pale, diaphoretic, anxious
• VS: 132/98; P 86; R 20; SpO2 98%

82
Scenario #7 – Critical Thinking
• What is your impression?– Abdominal pain?– Cardiac?– Indigestion?– The flu?
• Think: what’s the worst case scenario for a patient with “abdominal” pain?– An actual cardiac event until proven otherwise

83
Scenario #7 – Questions to Ask
• Assess the patient following the OPQRST format– Covers important assessment components
• The answers to questions may prompt further questioning– i.e.: “P” – What makes the pain worse?
- What makes the pain better?– What have you taken for the pain?

84
Scenario #7 - Interventions
• Routine Medical Care SOP
• Would you put the patient on a cardiac monitor?– Defend why not or why you would
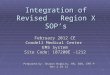
• EKG rhythm:
Normal sinus rhythm

85
Scenario #7 – Critical Thinking
• The patient’s rhythm is NSR
• What more could a 12 lead tell you?– Evidence of ST elevation and location– Location influences decisions of care by you:
• i.e.: NTG administration or not• Potential need for carefully monitored
fluid administration
Potential for heart blocks

86
Scenario #7 - Interventions
• Acute Coronary Syndrome SOP
• Critical thinking:– The patient states they took an antacid and
Tylenol
– Would you still administer ASA?• Yes, ASA has different actions than Tylenol
– Why is ASA important to give so early?• ASA blocks platelets from aggregating or
congregating at the site of the plaque rupture which would further block blood flow

87
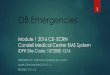
Scenario #7• Is there ST elevation?ST elevation I, aVL, V2 – V5

88
Scenario #7 – Critical Thinking
• Now what are your interventions?– Have IV access– Administer NTG after checking B/P and
screening for Viagra use – What is the dose of NTG?
• 0.4 mg SL; may be repeated every 5 minutes to max of 3
• Watch the blood pressure before & after administration
– Consider use of Morphine for pain– What is the dose of Morphine?
• 2 mg slow IVP every 2 minutes to max of 10 mg

89
Scenario #8
• As you approach, this is what you see:

90
Scenario #8
• You respond to the scene of a 4 y/o patient who has a peanut allergy and took a bite of dip with peanuts by mistake
• They are pale, clammy, anxious, itching, visible hives, increased respirations, and audible wheezing
• As you approaching, the parent is preparing the patient’s Epipen

91
Scenario #8 – Critical Thinking
• VS: B/P 88/50; P – 100; R - 26• What is your impression?
– Allergic reaction or anaphylaxis?– What is the difference?
• The blood pressure would be dropping in anaphylaxis due to the wide spread vasodilation response of the body
– Did you know?• The faster the reaction appears, usually the
more severe the reaction

92
Scenario #8 – Questions to Ask
• Determine the status of the airway– Laryngeal edema can occur so protecting the
airway is the first concern
• If the patient's Epipen is ready to be administered, would you allow that to be used or prepare your Epi dose?– It seems most prudent to use the quickest
available source of epinephrine

93
Scenario #8 - Interventions
• Which path of the Allergic reaction is followed on the Region X SOP’s?– Allergic reaction with airway involvement
• Why?– The patient is wheezing; B/P is adequate for a
4 y/o
• What drugs are indicated?– Epinephrine 1:1000 SQ, Benadryl, DuoNeb
(Albuterol mixed with Atrovent)

94
Scenario #8 – Critical Thinking
• What is the dose of the medications for this 4 year old who weighs 40 pounds?
• Epinephrine 1:1000 – 0.01 mg/kg SQ
0.18 ml (0.18 mg) SQ
• Benadryl 1 mg/kg slow IVP or IM
0.36 ml (18 mg)
• Albuterol 2.5 mg/3 ml mixed with Atrovent 0.5 mg/2.5 ml

95
Scenario #8 – Critical Thinking
• What benefit do these medications provide?– Epinephrine
• Bronchodilator to open the airways• Vasoconstrictor to prevent the blood vessels from
dilating causing a drop in cardiac output• Relatively short acting by often 1 dose is sufficient
– Benadryl• Antihistamine to stop the release of histamine that
is causing the reactions seen; last 4-6 hours– DuoNeb – Albuterol mixed with Atrovent
• Promotes bronchodilation

96
Bibliography
• Bledsoe, B., Porter, R., Cherry, R. Essentials of Paramedic Care 2nd edition Update. Brady. 2011.
• Limmer, D., O’Keefe, M. Emergency Care 12th Edition. Brady. 2012.
• Region X SOP’s IDPH Approved January 6, 2012
• Walraven, G., Basic Arrhythmias 7th Edition. Brady. 2011.