Embed Size (px)
DESCRIPTION
m,
Citation preview

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 1/20
.a >> Home TOC
Management of Developm ental
symmetrical Facial Growth
Birte Prahl Andersen an d Clara E. Fischer
Several aspects of the management of developmental asymmetrical facial
growth are addressed, The abnormality is further defined, Methods of
exam ination and assess ment of records are discussed, A complicating factor
has been the adoption of too many classification systems. With three-
dimensional imaging techniques computed tomog raph y scan and stereopho-
tography) great advancement has been made in efforts at describing the
range of variation, Hemifacial microsomia patients are best treated in
multidisciplinary centers by com pete nt specialists with t he necessary exper-
tise and skills, The procedure followed in the craniofacial center in Rotter-
dam is described and discussed in relation to current treatment strategies,
The success of the tre atm ent of the asymm etrical facial growth depends on
the original abnormality, on secondary abnormal development, and on
orthodontic and surgical intervention, International cooperation is necessary
to compile sufficient statistical data for a scientific evaluation of treatment
results and to improve the effectiveness and the efficiency of treatment,
Semin Orthod 1996;2:64-83.) Co p y r i g h t © 19 96 b y W B Sa u n d e r s Com p a n y
n u n d e r s t a n d i n g o f c r a n i o fa c i a l g ro wt h h a s
a lwa ys p o s e d p ro b l e m s , a n d d e v e l o p m e n t a l
a b n o rm a l i t i e s fu r t h e r c o m p l i c a t e s t h e u n d e r -
s t a n d i n g o f t h e s e g ro wt h p ro c e ss e s . T h e g ro wt h
p ro c e s s e s a r e n o t a s i m p l e c o o rd i n a t e d wh o l e ,
b u t r a t h e r i t s e e m s a s if m a n y c r a n i a l a n d f a c ia l
s t r u c t u re s i n t e r a c t a n d u n d e r g o d i f f e r e n t ia l
g ro wt h e i t h e r s y m m e t r i c a l ly o r a s y m m e t ri c a l ly .
T h e r e is n o d o u b t t h a t t h e c e ll s g e n o m e
c o n t a i n s s p e c i f i c i n s t ru c t i o n s t h a t d i c t a t e t h e
p a t t e r n o f g ro wt h, b u t c e l l s a r e a l s o r e s p o n s i v e t o
e p i g e n e t i c a n d e n v i ro n m e n t a l f a c t o r s . T h e p ro -
p o r t i o n o f g ro wt h t h a t is g e n e t i c a l l y d e t e rm i n e d
o r e n v i ro n m e n t a l l y c o n t ro l l e d i s n o t k n o wn , b u t
i t i s t h e i n t e rp l a y t h a t a c c o u n t s fo r n o rm a l
v a r ia t io n s a n d f o r a b n o r m a l d e v e l o p m e n t .
Ve ry f e w c ra ni o fa c i a l m a l fo rm a t i o n s c a n b e
p r e v e n t e d b a s e d o n k n o w l e d g e o f t h e i r e t i o lo g y
From the Academic Centre of Dentistry Amsterdam Department
of Orthodontics; and the Orthodontic Department University Hospi-
tal Rotterdam The Netherlands.
Address correspondence to B. Prahl-Andersen PhD DD S Aca-
demic Centre of Dentistry Amsterdam Department o f Orthodontics
Louwesweg 1 1066 EA Amsterdam The Netherlands.
Copyright © 1996 by W.B. Saunders Company
1073-8746/96/0202-000555. 00/0
o r p a t h o g e n e s i s . On t h e o t h e r h a n d , t h e i d en t if i -
c a t i o n o f c au s a l m e c h a n i s m s o f c r a n i o fa c ia l m a l-
fo rm a t i o n s m a y p l a y a ro l e in t h e fu t u re i n t h e
c l in i ca l m a n a g e m e n t o f m a l f o r m a t io n s .
W h e n c o n s i d e r i n g a s y m m e t r i e s a r i s i n g i n
c ra n i o fa c i a l d e v e l o p m e n t , t h e m o s t s i g n i f i c a n t
a s y m m e t r i c a l m a l fo rm a t i o n i s h e m i fa c i a l m i c ro -
s o m i a o r o t o m a n d i b u l a r d y so s to s is , a l so r e f e r r e d
t o a s t h e F i r s t a n d S e c o n d B ra n c h i a l Arc h S y n -
d r o m e . T h i s n o m e n c l a t u r e i n c l ud e s a n u m b e r o f
c o n d i t i o n s ; h o w e v e r , a l l s h o w a s y m m e t r i c a l
g r o w t h o f t h e m a n d i b l e . D u r i n g d e v e l o p m e n t it
c a n b e d i f f i c u l t t o d i s c r i m i n a t e b e t we e n e i t h e r
h y p e rp l a s i a o r h y p o p l a s i a o f o n e s i de o f t h e
m a n d i b l e . I t i s i m p o r t a n t t o c o n s i d e r t h e d i f f e r -
e n t i a l d i a gn o s i s o f h e m i fa c i a l m i c ro s o m i a f ro m
o t h e r f a c i al a s y m m e t r i c a l a b n o rm a l i t i e s , b e c a u s e
t h e t r e a t m e n t w i l l i n m o s t c a s e s , b e d i f f e r e n t .
Ap p ro p r i a t e e x a m i n a t i o n a n d o b s e rv a t i o n s h o u l d
a l l o w fo r t h e c o r r e c t d i a g n o s i s . T h e fo l l o wi n g
m o s t c o m m o n c o n d i t i o n s a r e il l u st r a te d : h e m i fa -
c ia l microsomia (F ig 1 ) , p lag iocephaly (F ig 2 ) ,
h y p e rp l a s i a o f o n e c o n d y l e (F ig 3 ), a n d P a r ry -
R o m b e rg s s y n d ro m e , p ro g re s s i ve h e m i fa c i a l a t -
ro p h y (F ig 4 ) .
I n o n e f o r m o r a n o t h e r a s y m m e tr i c al g r o w th
64 Seminar s in Orthodontics, Vol 2, No 2 June ), 1 996: pp 64 -83

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 2/20
i-,U'I~ ?.. >>
symmetrical Facial Growth
H o m e I T O C
6
SNA : 79 ° (83 ° )
' l/ J 9 -: -
Figure 1. (A) Illustrat ion of a patient with hemifacial microsomia. Note the asymmetrical position of the lower
jaw and the devia ted chin to the affected left side. (B) Profile view of this patient. Note the deformed ear on the
affected left side. (C) Profile headfilm o f the patient (1A and B). (D) Tracing of the profile headfilm of the
patient (1A-C). All measurements are smaller than normal measurements (shown in brackets).
of the mandi bular occurs in one of 3,000 births.
The etiology of hemifacial microsomia is un-
clear. A theory of mesodermal deficiency has
been suggested, as has a theory of a vascular
defect or circula tory deficiency. Poswillo 1 sug-
gested that the theory of a vascular defect was
plausible. The varying involvement of the differ-
ent structures suggests that the causal factor
varies in intensity and that it is active at several
periods during prenatal development. The
anomaly often extends beyond the mandible and
both primary and derived defects are observed
in the form o f deviation in the outer and middle
ear, affected malar region, orbit, frontal region,
maxilla, and many of the associated bony and
soft tissues, such as cleft palate. Th e g eneral ter m
craniofacial microsom ia has been propos ed by
Mun ro 2 to describe the severe forms. Th e final
clinical appearance of a patient who has not
undergone surgery with hemifacial microsomia
depends on the initial defect and the subsequent
secondary abnormal development.
M e t h o d s o f Ex a m in a t io n an d A s s e s s m e n t
of Records
To assure and improve quality care of chil dren
with asymmetrical facial developme nt, these chil-
dren are best treated in multidisciplinary cranio-
facial centers. In these centers a sufficient num-
ber of abnorm al children should be observed
and treated to ensure that competent specialists
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 3/20
: , t- J,. a >> Hom e I TO C
66
Prahl Andersen a nd F ischer
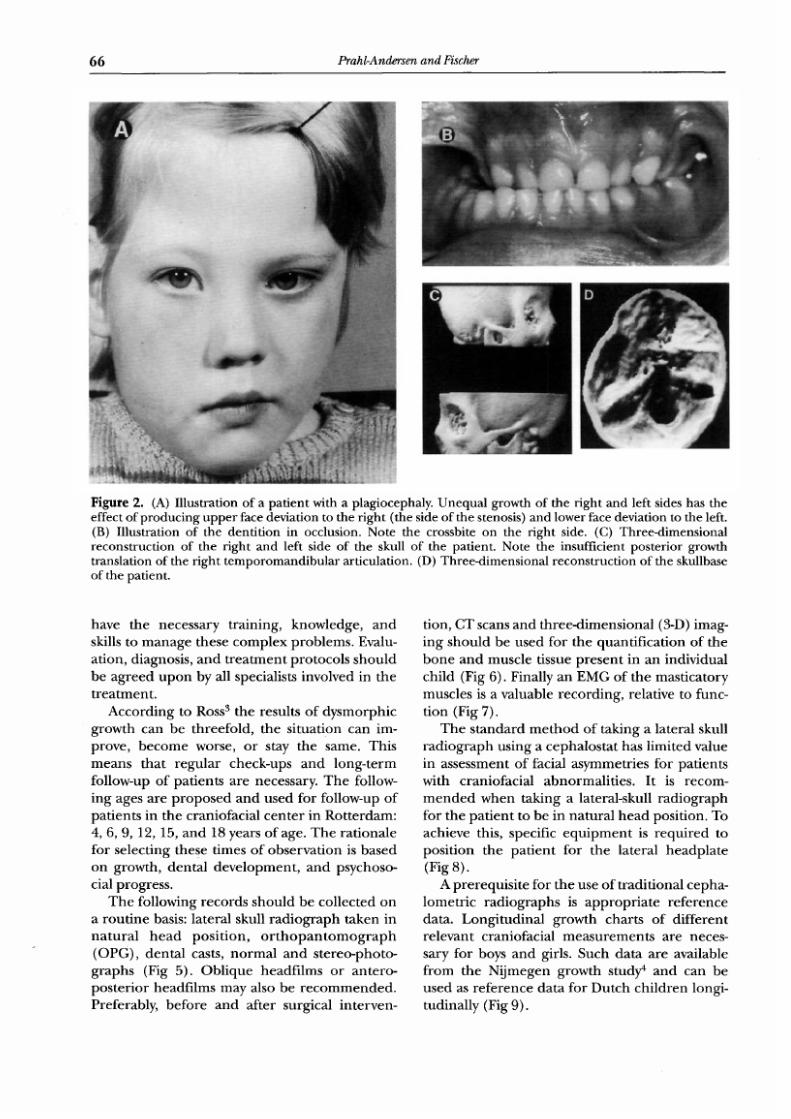
Figure 2. A) Illustration of a patien t with a plagiocephaly. Uneq ual g rowth of the right and left sides has the
effect of produc ing u pp er face deviation to the righ t the side of the stenosis) and low er face deviation to the left .
B) Illustration of the dentition in occlusion. Note the crossbite on the right side. C) Three-dim ensional
reconstruction of the right and left side of the skull of the patient. Note the insufficient posterior growth
transla t ion of the r ight tem porom andibu lar ar t icula tion. D) Three-dimensional recons truct ion of the skullbase
of the patient.
h a v e t h e n e c e s s a r y t r a i n i n g , k n o w l e d g e , a n d
s ki ll s t o m a n a g e t h e s e c o m p l e x p r o b l e m s . E v a l u-
a t i o n , d i a g n o s i s , a n d t r e a t m e n t p r o t o c o l s s h o u l d
be ag ree d u po n by a l l spec ial i s ts i nvolved in the
t r e a t m e n t .
A c c o r d i n g t o R o s s 3 t h e r e s u lt s o f d y s m o r p h i c
g r o w t h c a n b e t h r e e f o l d , t h e s i t u a t i o n c a n i m -
p r o v e , b e c o m e w o r s e , o r s t a y t h e s a m e . T h i s
m e a n s t h a t r e g u l a r c h e c k - u p s a n d l o n g - t e r m
fol low-up of pa t i en t s a re neces sa ry . Th e fo l low-
i n g a g e s a r e p r o p o s e d a n d u s e d f o r f o l l o w - u p o f
p a t i e n t s i n t h e c r a n i o f a c i a l c e n t e r i n R o t t e r d a m :
4 , 6, 9 , 12, 15 , and 18 yea rs o f age . The ra t ion a le
f o r s e l e c t in g t h e s e t i m e s o f o b s e r v a t i o n i s b a s e d
o n g r o w t h , d e n t a l d e v e l o p m e n t , a n d p s y c h o s o -
c i a l p rogres s .
T h e f o l l o w i n g r e c o r d s s h o u l d b e c o l l e c t e d o n
a rou t ine bas i s : l a t e ra l sku l l r ad iograph t aken in
n a t u r a l h e a d p o s i t i o n , o r t h o p a n t o m o g r a p h
O P G ) , d e n t a l c a s t s , n o r m a l a n d s t e r e o - p h o t o -
g r a p h s F i g 5 ) . O b l i q u e h e a d f i l m s o r a n t e r o -
p o s t e r i o r h e a d f il m s m a y a ls o b e r e c o m m e n d e d .
P r e f e r a b l y , b e f o r e a n d a f t e r s u r g i c a l i n t e r v e n -
t i o n, C T s c a n s a n d t h r e e - d i m e n s i o n a l 3 -D ) i m a g -
i n g s h o u l d b e u s e d f o r t h e q u a n t i f i c a t i o n o f t h e
b o n e a n d m u s c l e t i s s u e p r e s e n t i n a n i n d i v i d u a l
c h i l d F i g 6 ) . F i n al l y a n E M G o f t h e m a s t i c a t o r y
musc les i s a va luab le record ing , re l a t ive to func -
t ion Fig 7) .
T h e s t a n d a r d m e t h o d o f t a k i n g a l a t e ra l sk u ll
r a d i o g r a p h u s i n g a c e p h a l o s t a t h a s l i m i t e d v a lu e
i n a s s e s s m e n t o f f a c ia l a s y m m e t r i e s f o r p a t i e n t s
w i t h c r a n i o f a c i al a b n o r m a l i t i e s . I t is r e c o m -
m e n d e d w h e n t a k i n g a l a t e r a l - s k u l l r a d i o g r a p h
f o r t h e p a t i e n t t o b e i n n a t u r a l h e a d p o s i t i o n . T o
a c h i e v e t h is , s p ec i f ic e q u i p m e n t i s r e q u i r e d t o
p o s i t i o n t h e p a t i e n t f o r t h e l a t e r a l h e a d p l a t e
Fig 8) .
A p r e r e q u i s i t e f o r t h e u s e o f t r a d i t i o n a l c e p h a -
l o m e t r i c r a d i o g r a p h s is a p p r o p r i a t e r e f e r e n c e
d a t a . L o n g i t u d i n a l g r o w t h c h a r t s o f d i f f e r e n t
r e l e v a n t c r a n i o f a c i a l m e a s u r e m e n t s a r e n e c e s -
s a ry for boys and g i rl s . Such da ta a re ava i l ab le
f r o m t h e N i j m e g e n g r o w t h s t u d y 4 a n d c a n b e
u s e d a s r e f e r e n c e d a t a f o r D u t c h c h i l d r e n l o n g i-
tud ina l ly F ig 9) .
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 4/20
: d-'J~- ?:- >>
symmetrical Facial Growth
H o m e I T O C
67
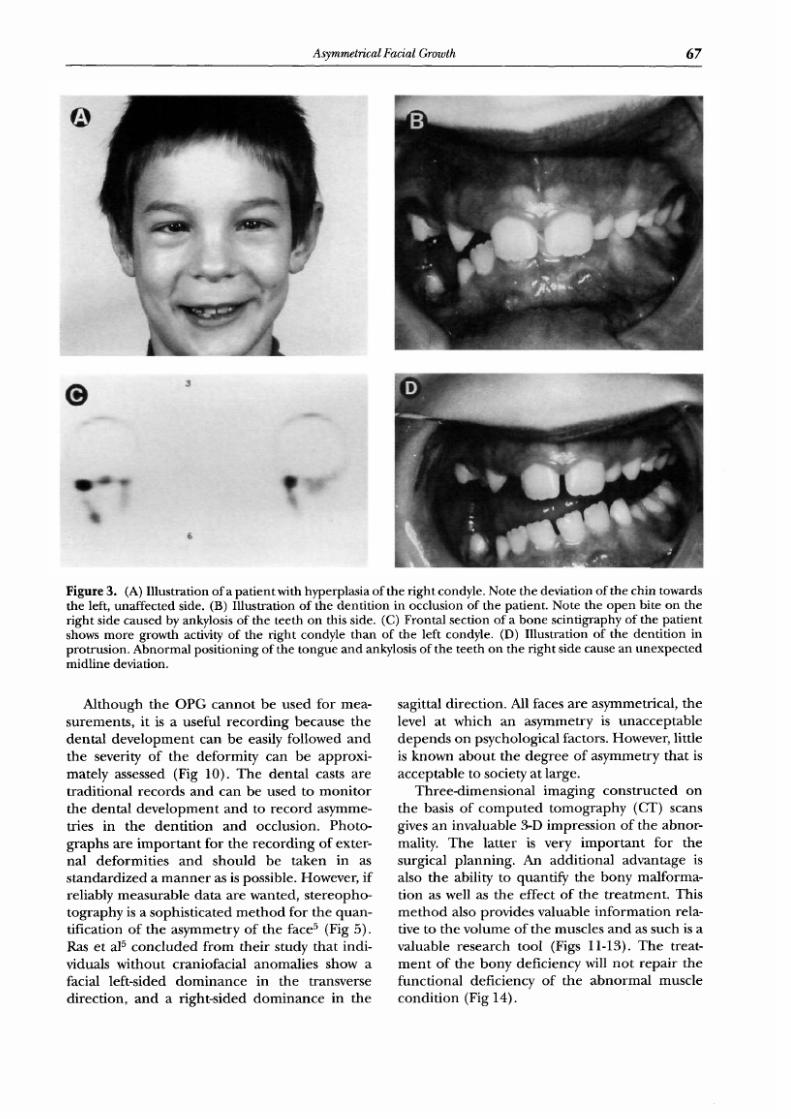
Figure 3. A) Illustration of a patient with hyperplasia of the right condyle. Note the deviation of the chin towards
the left, unaffected side. B) Illustration of the dentition in occlusion of the patient. Note the open bite on the
right side caused by ankylosis of the teeth on this side. C) Frontal section of a bone scintigraphy of the patient
shows more growth activity of the right condyle than of the left condyle. D) Illustration of the dentition in
protrusion. Abnormal positioning of the tongue and ankylosis of the teeth on the right side cause an unexpected
midline deviation.
Although the OPG cannot be used for mea-
surements, it is a useful recording because the
dental development can be easily followed and
the severity of the deformity can be approxi-
matel y assessed Fig 10). Th e den tal casts are
traditional records and can be used to monitor
the dental development and to record asymme-
tries in the dentition and occlusion. Photo-
graphs are important for the recording of exter-
nal deformities and should be taken in as
standar dized a man ner as is possible. However, if
reliably measurable data are wanted, stereopho-
tography is a sophisticated me tho d for the quan-
tification of the asymm etry of the face 5 Fig 5).
Ras et al 5 con clu ded fro m their study that indi-
viduals without craniofacial anomalies show a
facial left-sided dominance in the transverse
direction, and a right-sided dominance in the
sagittal direction. All faces are asymmetrical, the
level at which an asymmetry is unacceptable
depe nds on psychological factors. However, little
is known about the degree of asymmetry that is
acceptabl e to society at large.
Three-dimensional imaging constructed on
the basis of comp ute d tomogra phy CT) scans
gives an invaluable 3-D impression of the abnor-
mality. The latter is very important for the
surgical planning. An additional advantage is
also the ability to quantify the bony malforma-
tion as well as the effect of the treatment. This
method also provides valuable information rela-
tive to the volume of the muscles and as such is a
valuable research tool Figs 11-13). The treat-
ment of the bony deficiency will no t repair the
functional deficiency of the abnormal muscle
condi tion Fig 14).

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 5/20
: ¢J . ~ >> Ho me I TO C
8
Prahl Andersen and F ischer
The Range and Variation
Developmental asymmetry of the face is charac-
terized by varying degrees of underd evel opme nt
of the craniofacial structures. As mention ed, the
majo r deficiency effects the mandible. Several
classifications have been proposed in the litera-
ture: Pruzansky, 6 Har vol d et al, 7 David et al, s
Munr o, 2 and Vento et al. 9 Munr o 2 divided pa-
tients according to the skeletal deformity into 5
types, a purely surgical-anatomic classification.
Pruzansky6 had earlier i ntr oduc ed a 3-point scale
of severity of the m andi bula r deficiency (Fig 10).
It seems that most of these commonly used
classifications are approximate because a spec-
trum o f other abnormalities are not taken into
Figure 4. (A) Illustrat ion of a patient with the Parry-
Romberg s syndrome, progressive hemifacial atrophy
of the right side. Note the slight deviation of the chin
to the right, affected side. (B) Illustration of the
denti tion in occlusion. Premature loss of the lower
first deciduous molar on the right side causes an
unexpected midline deviation. (C and D) Three-
dimensional reconstruct ion of the r ight and left sides
of the skull of this patient with progressive hemifacial
atrophy. (E) Illustration of the denti tion of the patient
on slight mouth opening showing no deviation of the
lower jaw.
account. Other bony anatomical structures in-
volved can be the zygoma, zygomatic arch, orbit,
frontal bone, pterygoid processes of the sphe-
noid bone, mastoid and tympanic process of the
temporal bone and the maxilla. For the abnor-
mality of the ears a separate scale has also been
propos ed by Pruzansky. 6 Photog raphs are used
to record this abnormality (Fig 15).
Nonbony structures affected can be the facial
nerve (obvious when the child is smiling), the
mouth, eyes, facial muscles, muscles of mastica-
tion, tongue, and parotid gland (Fig 16). It is
considered that with the more sophisticated
met hod of CT scans and 3-D reconstructions, a
better measurement of the total bony deficiency

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 6/20
: ,U'J~- ?:- > >
symmetrical Facial Growth
H o m e I T O C
6 9
F i gur e 5 . A andB ) E x ampl e o f a pa i r o f s t e r eoph o t o -
g r aphs i nc l ud i ng t he r e f e r ence f r ames and po i n t s and
pr o j ec t i on o f a g ri d on t o t he f ace. C ) E qu i p men t f o r
s t e r eopho t ogr aphy cons i s t i ng o f t w o synchr on i zed
camer as f i xed on t o a f r ame w i t h a d i s tance o f 50 cm
be t w een t he camer as , and p os i t i oned conve r ge n t l y a t
an angle of 15 degrees . A f lash spot i s fas tened
be t w een t he camer as .
c a n b e o b t a i n e d . S t r u c t u r e s s u c h a s t h e p t e r y -
g o i d p r o c e s s a r e o f t e n a f f e c t e d t o g e t h e r w i t h a
h y p o p l a s t i c e x t e r n a l o r i n te r n a l p t e r y g o i d
mu sc l e , a0
I n r e v i e w i n g t h e s e r i e s o f p a t i e n t s w i t h h e m i f a -
c i al m i c r o s o m i a t r e a t e d i n t h e c r a n i o f a c i a l c e n -
t e r i n R o t t e r d a m n = 8 4 ) t h e a b s e n c e o f a n y
a p p a r e n t c o r r e l a t i o n b e t w e e n e x t e r n a l d e f o r m i -
t ie s, h y p o p la s t i c m u s c l e s a n d a c c o m p a n y i n g m a n -
d i b u l a r m a l f o r m a t i o n w a s s t r i k i n g . T h i s w a s a l s o
r e c o g n i z e d b y C o n v e r s e e t a l. n U n f o r t u n a t e l y
d a t a w a s n o t y e t a v a i l a b le a n d t h e r e f o r e a s tu d y
w a s u n d e r t a k e n t o o b t a i n d a t a . I n t hi s s t u d y t h e
v o l u m e a n d p o s i t i o n o f t h e i n v o l v e d m a s t i c a t o r y
m u s c l e s w e re m e a s u r e d i n p a t i e n t s w i th h e m i f a -
c i a l m i c r o s o m i a a n d i l l u s t r a t e d w i t h 3- D r e c o n -
s t r u c t e d C T s c a n s F i gs 1 1 -1 3 ). D i f f e r e n c e s b e -
t w e e n l e f t a n d r i g h t m a s t i c a t o r y m u s c l e s w e r e
i d e n t i f i e d a n d r e l a t e d t o t h e b o n y g r a d e o f
d e s t r u c t i o n . T h e r e a p p e a r e d t o b e n o l i n e a r
r e l a t i o n s h i p b e t w e e n t h e b o n y a n d t h e m u s c u l a r
u n d e r d e v e l o p m e n t . E v e n a m i n i m a l h y p o p l a s i a
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 7/20
A K in ; e > > Hom e I T O C
7
Prahl Andersen a nd F ischer
\4
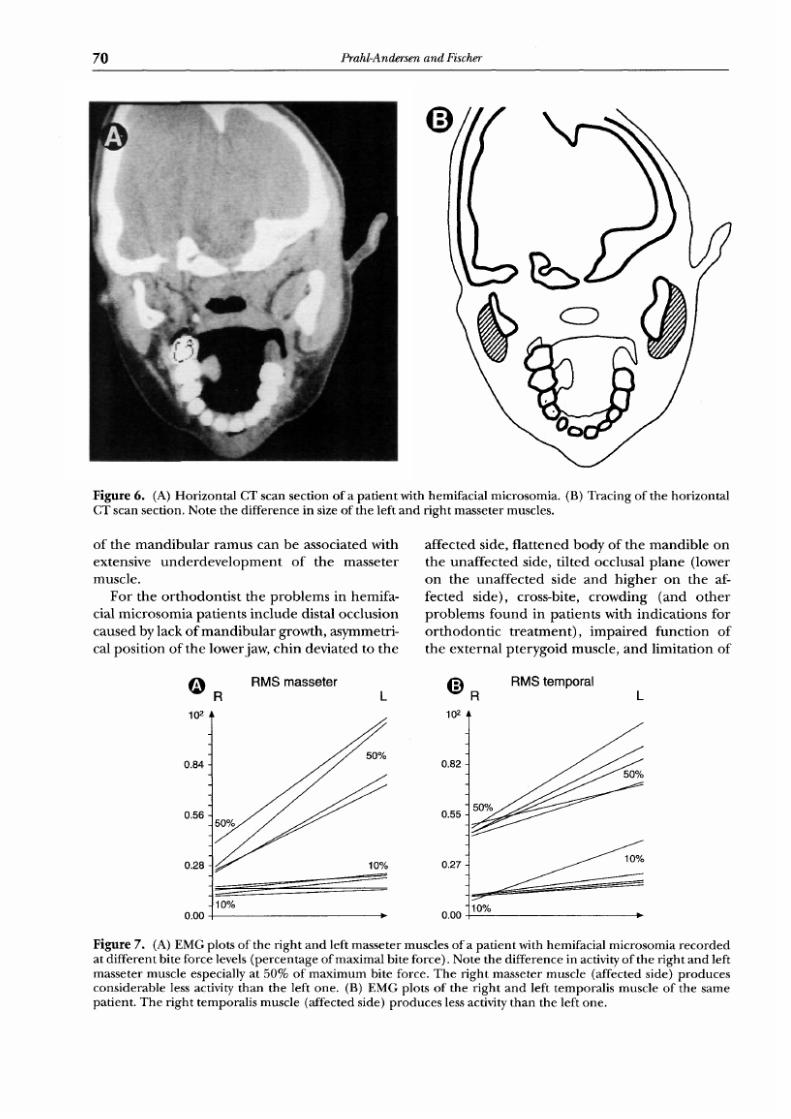
Figure 6. (A) Horizon tal CT scan section of a pat ient with hemifacial microsomia. (B) Tracing o f the horizontal
CT scan sect ion. N ote the difference in s ize of the left and r igh t masseter muscles.
o f t h e m a n d i b u l a r r a m u s c a n b e a s s o c i a te d w i th
e x te n si v e u n d e r d e v e l o p m e n t o f t he m a s s e t er
m u s c l e .
F o r t h e o r t h o d o n t i s t t h e p r o b l e m s i n h e m i f a -
c i a l m i c r o s o m i a p a t i e n t s i n c l u d e d i s t a l o c c l u s i o n
c a u s e d b y l ac k o f m a n d i b u l a r g r o w t h , a s y m m e t r i -
c a l p o s i t i o n o f t h e l o w e r j a w , c h i n d e v i a t e d t o t h e
a f f e c t e d s id e , f l a t t e n e d b o d y o f t h e m a n d i b l e o n
t h e u n a f f e c t e d s i d e , t i l t ed o c c l u s a l p l a n e ( l o w e r
o n t h e u n a f f e c t e d s i d e a n d h i g h e r o n t h e a f -
f e c t e d s i d e ) , c r o s s - b i t e , c r o w d i n g ( a n d o t h e r
p r o b l e m s f o u n d i n p a t i e n t s w i t h i n d i c a t i o n s f o r
o r t h o d o n t i c t r e a t m e n t ) , i m p a i r e d f u n c t i o n o f
t h e e x t e r n a l p t e r y g o i d m u s c l e , a n d l i m i t a t i o n o f
R M S m a s s e t e r
R L
10 2
0.84
0.56
0.28
0.00
50%
10
I1
R M S t e m p o r a l
~ a L
lO 2
0.82
0.55
0.27
0 00
50%
lO
Figure 7. (A) EMG plots of the r ight and left masseter muscles of a pat ient with hemifacia l microsomia rec orded
at different bi te force levels ( percentage of maximal bi te force) . Note the difference in activity of the r ight an d left
masseter muscle especia l ly a t 50 of max imum bite force . The r ig ht masseter muscle (affected s ide) prod uces
considerable less act ivi ty than the left one. (B) EM G plots of the r ight a nd left temporal is muscle o f the same
patient. Th e right temp oralis musc le (a ffected side) prod uce s less activity than the left one.
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 8/20
symmetrical Facial Growth
Home I TO C
7
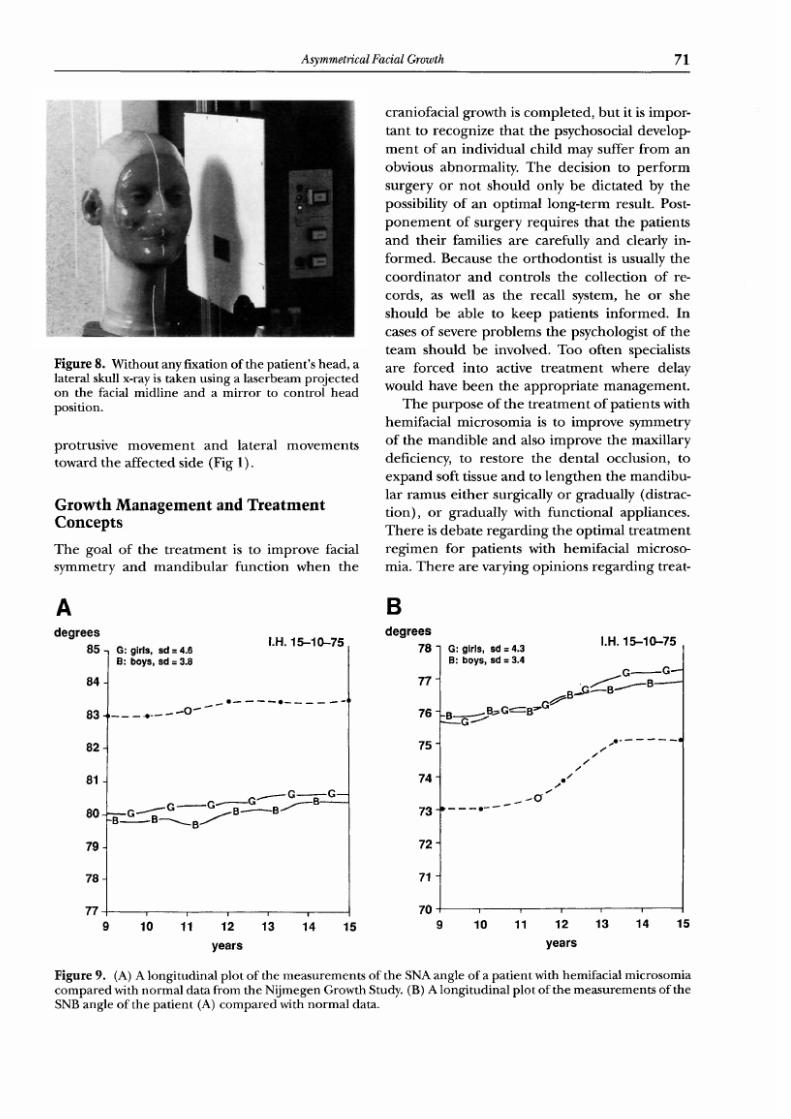
Figure 8. Without any f ixat ion of the pat ient s head, a
lateral skull x-ray is taken using a la serbeam projected
on the facia l midl ine and a mirror to control head
position.
p r o t r us i v e m o v e m e n t a n d l a te r al m o v e m e n t s
toward the a f fec t ed s ide (F ig 1) .
Growth Management and Treatment
oncepts
T h e g o a l o f t h e t r e a t m e n t i s t o i m p r o v e f a c i a l
s y m m e t r y a n d m a n d i b u l a r f u n c t i o n w h e n t h e
c r a n i o f a c ia l g r o w t h i s c o m p l e t e d , b u t i t i s i m p o r -
t a n t t o r e c o g n i z e t h a t t h e p s y c h o s o c i a l d e v e l o p -
m e n t o f a n i n d i v i d u a l c h i l d m a y s u ff e r f r o m a n
o b v i o u s a b n o r m a l i t y . T h e d e c i s i o n t o p e r f o r m
s u r g e r y o r n o t s h o u l d o n l y b e d i c t a t e d b y t h e
pos s ib i l it y o f an op t ima l long - t e r m resu l t . Pos t -
p o n e m e n t o f su r g e r y r e q u ir e s t h a t t h e p a t i e nt s
and the i r f am i l i e s a re ca re fu l ly and c l ea r ly in -
f o r m e d . B e c a u s e t h e o r t h o d o n t i s t i s u s u a ll y t h e
c o o r d i n a t o r a n d c o n t r o l s t h e c o l l e c t io n o f r e -
cords , a s we l l a s the reca l l sys t em, he or she
s h o u l d b e a b l e t o k e e p p a t i e n t s i n f o r m e d . I n
c a se s o f se v e r e p r o b l e m s t h e p s y c h o l o g i s t o f t h e
t e a m s h o u l d b e i n v o l v e d . T o o o f t e n s p e c i a l i s t s
a r e f o r c e d i n t o a c t i v e t r e a t m e n t w h e r e d e l a y
w o u l d h a ve b e e n t h e a p p r o p r i a t e m a n a g e m e n t .
T h e p u r p o s e o f th e t r e a t m e n t o f p at i e n ts w it h
h e m i f a c i a l m i c r o s o m i a i s t o i m p r o v e s y m m e t r y
o f t h e m a n d i b l e a n d a l so im p r o v e t h e m a x i l l a r y
de f i c i ency , t o re s to re the den ta l occ lus ion , t o
e x p a n d s o ft t is su e a n d t o l e n g t h e n t h e m a n d i b u -
l a r ramu s e i th e r surg ica l ly o r g radu a l ly (d i s t rac -
t i o n ) , o r g r a d u a l l y w i t h f u n c t i o n a l a p p l i a n c e s .
T h e r e is d e b a t e r e g a r d i n g t h e o p t i m a l t r e a t m e n t
r e g i m e n f o r p a t i e n t s w i t h h e m i f a c i a l m i c r o s o -
m i a . T h e r e a r e v a r y i n g o p i n i o n s r e g a r d i n g t r e a t -
d e g re e s
85
84
8 3 .
8 2 -
81
80
79
78
77
9
G: girls, sd = 4.6
B: boys, sd = 3.8
I .H. 15 10 75
G~ G ~ G~-'---'B--G - -
~ '- G -~ ._ .~ . . . B /~ e - - e /~
B
d e g re e s
7 8
7 7
76
75
7 4 '
7 3
7 2 -
71
70
I .H. 15 10 75
G: glr]s, sd = 4.3
B: bo ys, sd = 3.4
G G~
.B.~B~G...._B~G~ ~- ~B : --B~
~ o q
/o /
I
u ; u n I I ; I i ;
10 11 12 13 14 15 10 11 12 13 14
years years
5
Figure 9. (A) A longitudinal plot of the measu rem ents of the SNA angle of a patien t with hemifacial microso mia
comp ared with no rmal d ata from the N i jmegen Growth Study. (B) A longitudinal plot of the measu rements of the
SNB angle of the patie nt (A) com par ed with nor mal data.

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 9/20
: , t- J,. a >> Hom e I TO C
72
Prahl Andersen and Fischer
O M.B. 4.3 years
14 6 91
M.A. 10.11 years
6 7 84
M.K. 4.6 years
6 3 84
Figure 10. A) Ortho pantomogram showing a Pruzansky I affected mandible with only slight hypoplasia of the
left condyle. B) Tracing of the orthopant omogram with Pruzansky I affected mandible. C) Orthopanto mogram
showing a Pruzansky II affected mandible with severe hypoplasia of the condyle and mild hypoplasia of the ramns
at the left side. D) Tracing of the ortho pantomogr am C) with Pruzansky II affected mandible. E)
Orthopan tomogram showing a Pruzansky III affected mandible with severe hypoplasia of the ramus and absence
of the condyle and the coronoid process on the right side. F) Tracing of the orthopant omogr am E) with
Pruzansky III affected mandible.
ment strategies with varying claims regarding
optimal treatme nt results.
The controversy centers arou nd timing and
mo de of inte rven tion in relation to age, severity,
and psychosocial considerations. The lack of
agreement can only be reduced by intercenter
studies or even better with a mnlticenter ra ndom-
ized clinical trial. This means international coop-
eration is needed because no single center has a
sufficient pool, finance, or facilities to carr y out a
trial individually. This orphan abnormality needs
international funding to be able to solve the
probl em o f arriving at the optimal treatme nt
strategy.
The controversy seems to be conce ntrate d
aro und the question of timing of surgery and
whether or not it is possible to stimulate growth
of the affected mandible with functional appli-
ances. Bone-lengthening by gradual distraction
is the latest proposal which is still in the experi-
mental stage, but it could be an excellent method
of correcti ng asymmetries of the mandible Fig
17). Some clinicians claim success with this new
methodology, but if appropriat e evaluation of

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 10/20
/ ,V J,- ?:- >>
symmetrical Facial Growth
H o m e I T O C
7 3
F i gur e 11 . ( A ) P a t i en t w i t h a P r uzansky I a f f ec t ed man d i b l e ( r i gh t ) . ( B ) T hr ee - d i mens i o na l r econs t r uc t i on o f
t he sku l l o f the pa t i en t . ( C ) T h r ee - d i me ns i ona l r econ s t r uc t i on o f t he man d i b l e , t he m asse t e r musc l e s and t he
temp oral i s muscles , l a tera l r ight , and lef t view. Note s l ight hypo plas ia of these muscles on the r ight s ide .
( D ) T hr ee - d i mens i on a l r econs t r uc t i on o f t he mand i b l e , t he med i a l p t e r ygo i d musc l e s and t he l a t e r a l p t e r ygo i d
musc l es , an t e r i o r and pos t e r i o r v iew. N ot e s l i gh t hypop l a s i a o f t hese musc l e s on t he r i gh t s i de .
t h e m e t h o d o l o g y is n o t c a r r i e d o u t , i t w il l r e m a i n
e x p e r i m e n t a l a s d o s o m a n y o t h e r m e t h o d s o f
m a n a g e m e n t .
M u n r o z s t a te s t h a t t h e r u l e s h o u l d b e f i r s t
t h e b o n e , t h e n t h e s o ft t i s s u e . H e p r e f e r s e a r ly
i n t e r v e n t i o n a t 5 to 6 y e a r s o f a g e . H e f o u n d t h a t
u s i n g c o s t o c h o n d r a l g r a f t s r e s u l t e d i n le s s a s y m -
m e t r y a n d l e ss o c c l u s a l ti lt . I n s o m e c a s e s t h e r i b
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 11/20
: , t- J,. a >> Hom e I TO C
74
Prahl Andersen and Fischer
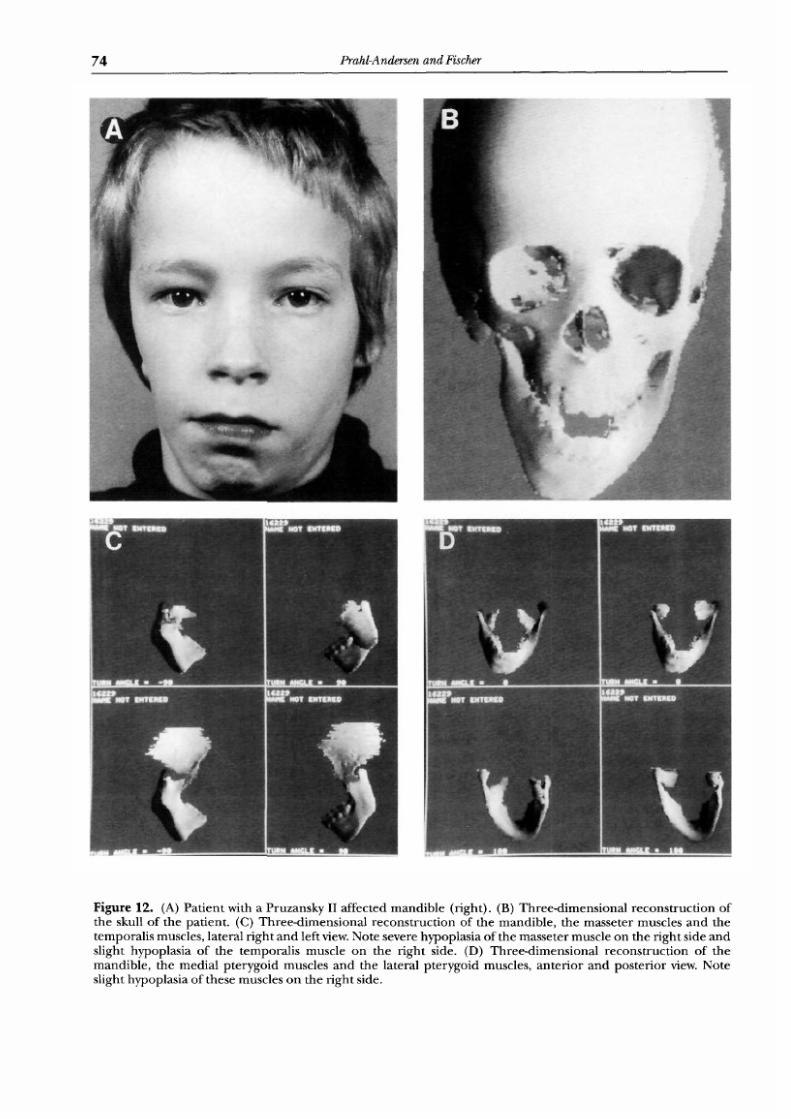
Figure 12. A) Patient with a Pruzansky II affected mandible right). B) Three-dimensional reconstructi on of
the skull of the patient. C) Three-dimensi onal reconstructi on of the mandible, the masseter muscles and the
temporalis muscles, lateral right and left view. Note severe hypoplasia of the massete r muscle on the right side and
slight hypoplasia of the temporalis muscle on the right side. D) Three-dime nsional reconstructi on of the
mandible, the medial pterygoid muscles and the lateral pterygoid muscles, anterior a nd posterior view. Note
slight hypoplasia of these muscles on the r ight side.
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 12/20
~,t- .t,. a >> Ho me I TO C
symmetrical Facial Growth
75
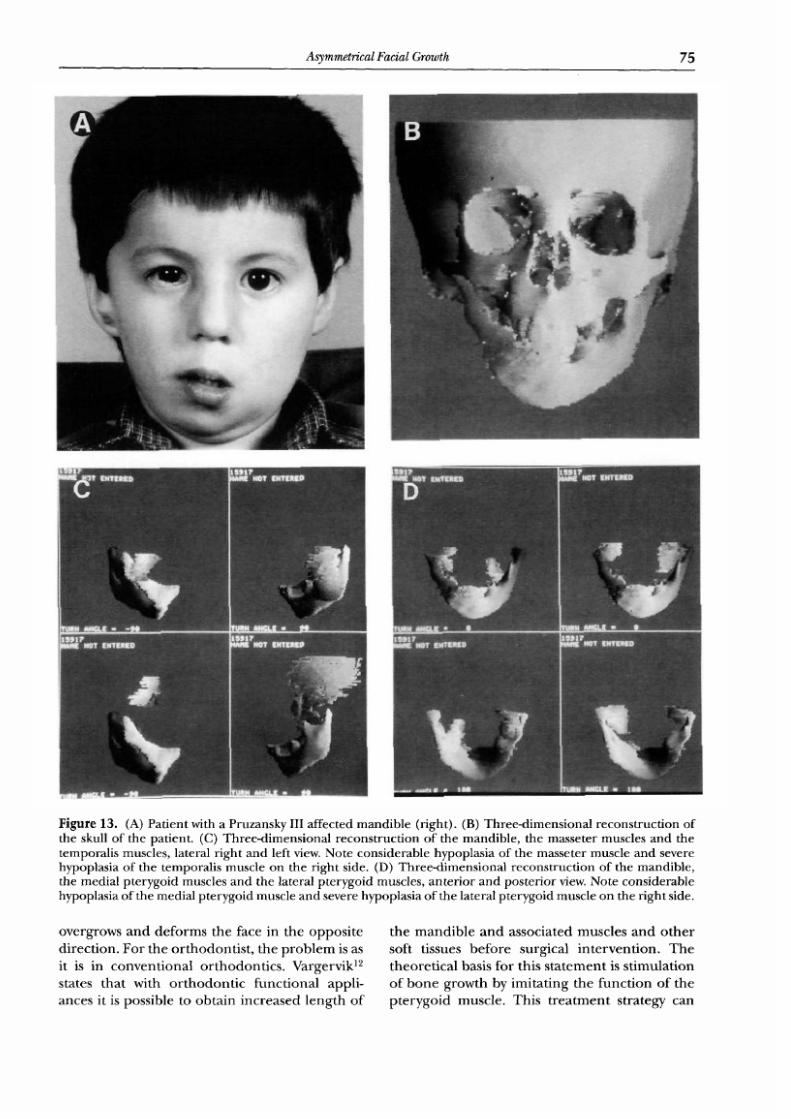
F i gur e 13 . A ) P a t i en t w i th a P r uzansky I I I a f f ec t ed mand i b l e r i gh t ) . B ) T hr ee - d i mens i o na l r econs t r uc t i on o f
t he sku l l o f t he pa t i en t . C ) T hr ee - d i men s i ona l r econs t r uc t i on o f t he mand i b l e , t he masse t e r musc l e s and t he
t empor a l i s musc l es , l a t e r a l f i gh t and l e f t v iew. N ot e cons i de r ab l e hypop l a s i a o f t he masse t e r musc l e a nd seve re
hypop l a s i a o f the t empor a l i s musc l e on t he f i gh t si de . D ) T hr ee - d i me ns i ona l r econs t r uc t i on o f the mand i b l e ,
t he med i a l p t e r ygo i d musc l e s and t he l a t e r a l p t e r ygo i d musc l e s , an t e r i o r and pos t e r i o r v iew. N ot e cons i de r ab l e
hypop l a s i a o f t he me d i a l p t e r ygo i d musc l e and seve re bypop l a s i a o f t he l a t e r a l p t e r ygo i d musc l e on t he r i gh t s i de .
o v e r g ro w s a n d d e f o r m s t h e f a ce i n th e o p p o s i t e
d i r e c t i o n . F o r t h e o r t h o d o n t i s t , t h e p r o b l e m i s a s
i t is i n c o n v e n t i o n a l o r t h o d o n t i c s . V a r g e r v i k 12
s t at e s t h a t w i t h o r t h o d o n t i c f u n c t i o n a l a p p l i -
a n c e s i t i s p o s s i b l e t o o b t a i n i n c r e a s e d l e n g t h o f
t h e m a n d i b l e a n d a s s o c i a te d m u s c l e s a n d o t h e r
s o f t t i ss u e s b e f o r e s u r g i c a l i n t e r v e n t i o n . T h e
t h e o r e t i c a l b a s i s f o r t h i s s t a t e m e n t i s s t i m u l a t i o n
o f b o n e g r o w t h b y i m i ta t i n g t h e f u n c t i o n o f t h e
p t e r y g o i d m u s c l e . T h i s t r e a t m e n t s t r a t eg y c an

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 13/20
; , t- . t ,. a >> Hom e I TO C
76
Prahl Andersen and Fischer
Figure 14. A) Illustration of a surgically treated hem ifacial micro somia patient. The bon y deficiency has been
recons tructed. B) Pat ient wi th open mou th af ter surgery. Note that t reatm ent of the bony deficiency has not
correc ted the fu nctional deficiency.
a l so b e a p p l i e d a f t e r s u r g i c a l r e p o s i t i o n i n g o f t h e
m a n d i b l e . T h e a d v a n t a g e o f th i s s t r a t eg y is t h a t
s u r g e r y c a n b e p o s t p o n e d u n t i l 8 t o 9 y e a r s o f
age . A t th i s age the d en t i t i on i s i n the t ran s i t iona l
p h a s e w it h e n o u g h p e r m a n e n t t e e t h f o r f i x at i o n
a n d s u r g e r y is p e r f o r m e d i n a d e v e l o p m e n t a l
s t ag e w i th m i n i m u m g r o w t h o f t h e m a n d i b l e F ig
18).
T h e t wo p re v i ou s l y m e n t i o n e d t r e a t m e n t p h i -
losoph ies have ye t t o be t e s t ed a s to which re su l t s
a r e u l t i m a t e l y o p t i m a l . I n s e v e r e c a s e s a s e c o n d
o p e r a t i o n i s o f t e n n e c e s s a r y , p r e f e r a b l y a f t e r
g r o w t h h a s c e a s e d .
I t c o u l d b e a s O s b o r n e 13 h a s s u g g e s t e d t h a t
s u r g e r y b e f o r e 6 y e a rs o f a g e g i v e s t h e m a x i l l a a
c h a n c e t o d e v e l o p a f t e r th e r e l e a s e o f t h e u p -
w a r d p r e s s u r e e x c e r t e d o n t h e a f f e c t e d s i d e b y
t h e h y p o p l a s t i c m a n d i b l e . H o w e v e r , i t h a s t o b e
d e m o n s t r a t e d t h a t th e m a n d i b l e d o e s e x e r t p r e s-
s u r e o n t h e m a x i l l a . T h e m a x i l l a m a y b e d e f i -
c i e n t f r o m b i r t h a n d b y c r e a t i n g a n o c c l u s al g a p
a t t h e a f f e c t e d s i de , o v e r - e r u p t i o n o f t h e t e e t h i n
t h e m a x i l l a m a y fo ll ow . T h e t r a n s i t io n a l p e r i o d
a f t e r th e e a r l y m i x e d d e n t i o n s t a g e i s p r e f e r r e d
b y m a n y s u r g e o n s f o r t h e f i rs t c o r r e c t i v e s u r g e r y
b e c a u s e t h e r e a r e e n o u g h p e r m a n e n t t e e t h f o r
i n t e r m a x i l l a r y f i x a t io n , l e ss c h a n c e o f d a m a g i n g
t o o t h b u d s , a n d t h e o p e r a t i o n i s p e r f o r m e d i n a
d e v e l o p m e n t a l s t a g e w i t h m i n i m a l g r o w t h o f t h e
m a n d i b l e .
T h e t r e a t m e n t m e t h o d f o l l o w ed in R o t t e r d a m
h a s b e e n i n s p i r e d b y t h e m e t h o d o f H a r v o l d e t
a l, 70 bw eg ese r , a4 and Gnoinsk i . 15 At 4 yea rs o f
a g e t h e p r e v i o u s l y d e s c r i b e d r e c o r d s o f t h e
p a t i e n t a r e c o l l e c t ed . I f c o o p e r a t i o n c a n b e
o b t a i n e d , t h e p o s i t i o n o f t h e m a n d i b l e i s n o r m a l -
i z ed , w i t h r e g a r d t o t h e m i d l i n e a n d t h e h o r i z o n -
t a l p o s i t i o n . W i t h t h e f u n c t i o n a l a p p l i a n c e t h e
mandib le i s kep t i n a s l igh t ly fo rward pos i t ion .
T h e p u r p o s e i s t o o b t a i n a m o r e s y m m e t r i c a l
musc le func t ion and the pos s ib i l it y , by ad jus t ing
the ac t iva tor on the a f fec t ed s ide , t o a l low for
p a ss i ve e r u p t i o n o f t h e m a x i l l a r y b u c c a l t e e t h . A t
the ag e of 9 yea rs a dec i s ion i s ma de e i the r to
o p e r a t e o r t o w a i t u n t i l t h e e n d o f t h e g r o w t h
p e r i o d . A t t h i s a g e m e a s u r e m e n t s a r e m a d e a t
th ree d i f fe ren t t imes , and usua l ly a l so a s e t o f CT
s c a n s a r e m a d e . O n t h e b a s is o f t h is i n f o r m a t i o n

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 14/20
: d-'J~- ?:- >>
symmetrical Facial Growth
H o m e I T O C
Figure 15. A) Ear abnormality, gradat ion I : s l ight hypoplas ia and bow led-form of oute r s t ructure of ear.
B) Gradat ion II : aplasia of external acoust ic tube and variable hypoplas ia of outer s t ructure . C) Grada t ion III :
dislocation o f ear-lobe, aplasia of oute r structu re, ear-lobe small, an d pl aced a nterior ly in most cases.
D) Gradat ion W: complete aplas ia of outer s t ruc ture and earlobe.
a n d d i s c u s s i o n s w i t h t h e p a t i e n t a n d t h e p a r e n t s
a n a g r e e d u p o n t r e a t m e n t g o a l is r e a c h e d .
I f s u r g e r y i s p l a n n e d , f i x e d o r t h o d o n t i c a p p li -
a n c e s a r e u s e d a s i n t e r m a x i l l a r y f i x a t i o n . A f t e r
s u r g e r y a n d t h e r e t e n t i o n p e r i o d t h e p a t ie n t s a r e
k e p t i n r e t e n t i o n w i t h a n a c t i v a t o r , a l l o w i n g f o r
f u r t h e r d e n t a l d e v e l o p m e n t . T h e d e f i n i t i v e o r t h -
o d o n t i c t r e a t m e n t is c a r r i e d o u t w it h f i x ed o r t h -
o d o n t i c a p p l i a n c e t h e r a p y a n d i f t h e s u r g e r y h a s
b e e n s u c c es s f u l, t h e r e t e n t i o n a p p l i a n c e m a y b e
a n a c t iv a t o r o r b o n d e d r e t a i n e r s F i gs 1 9 a n d 2 0 ) .
I n a f e w i n s t a n c e s t h e p a t i e n t s h a v e d e c l i n e d

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 15/20
At- .t~ e >> Ho me I TO C
8
Prahl Andersen and Fischer
Figure 16. Illustration of different anatomical abnormalities in patients with hemifacial microsomia. A) Aplasia
of the facial nerv e on the right side. g) Macrostomia on the left side. C) Abnorm al and small eye, the hypoplasia
of the muscles of masticati on on the right side. D) Small eye with epi bulb ar der moi d and hypoplasia of the
muscles of mastication and the man dible on the right side Goldenha r syndrome).
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 16/20
: - j - j , . ? .. >>
symmetrical Facial Growth
Home I TOC
9
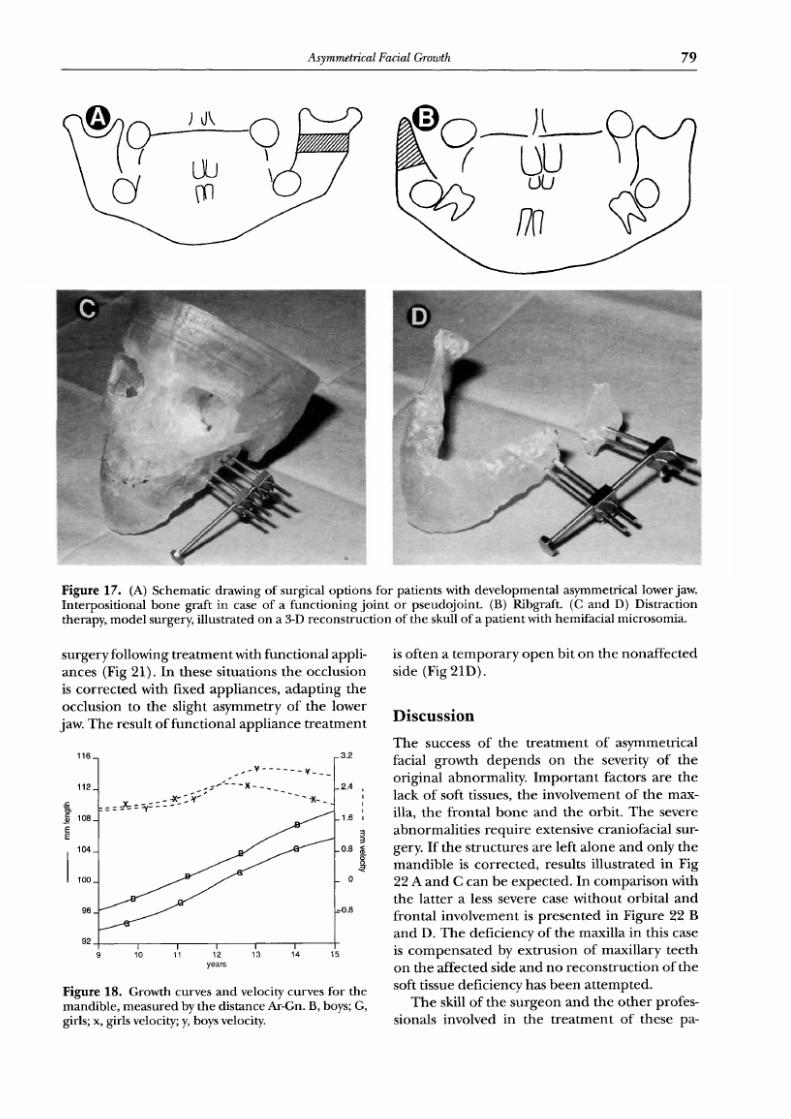
Figure 17. (A) Schematic drawing of surgical opt ions f or pat ients with developm ental asymmetrical lower jaw.
Interpos i t ional bo ne graft in case of a funct ion ing join t or pseudo joint . (B) Ribgraft. (C and D) Dis tract ion
therapy, mode l surgery, i llus tra ted o n a 3-D reconstruct ion of the skul l of a pat ient with hemifacia l microsomia.
s u r g e r y f o l l o w i n g t r e a t m e n t w i t h f u n c t i o n a l a p p l i -
a n c e s ( F i g 2 1 ) . I n t h e s e s i tu a t i o n s t h e o c c l u s i o n
i s c o r r e c t e d w i t h fi x e d a p p l i a n c e s , a d a p t i n g t h e
o c c l u s i o n t o t h e s l ig h t a s y m m e t r y o f t h e l o w e r
j aw . T h e r e s u l t o f f u n c t i o n a l a p p l i a n c e t r e a t m e n t
104_
I 100.
96.
92
116_ _3.2
< - -X - - . 2 .4
12
: = =__x===v: -'x ; ¥. - -~ - . ,,
} 1 8
0 8 ~
0
0 8
years
Figure
18. Growth curves and velocity curves for the
mand ible, mea sur ed by the distanc e Ar-Gn. B, boys; G,
girls; x, girls velocity; y, boys velocity.
is o f t e n a t e m p o r a r y o p e n b i t o n t h e n o n a f f e c t e d
s ide (F ig 21D ) .
i s cuss i on
T h e s u c ce s s o f t h e t r e a t m e n t o f as y m m e t r i c a l
f a c ia l g r o w t h d e p e n d s o n t h e s e v e ri t y o f t h e
o r i g i n a l a b n o r m a l i t y . I m p o r t a n t f a c t o r s a r e t h e
l a c k o f s o f t t i ss u es , t h e i n v o l v e m e n t o f t h e m a x -
i l l a , t h e f r o n t a l b o n e a n d t h e o r b i t . T h e s e v e r e
a b n o r m a l i t i e s r e q u i r e e x t e n s i v e c r a n i o f a c i a l s u r -
g e r y . I f t h e s t r u c t u r e s a r e l e f t a l o n e a n d o n l y t h e
m a n d i b l e i s c o r r e c t e d , r e s u l t s i l l u s t r a te d i n F i g
2 2 A a n d C c a n b e e x p e c t e d . I n c o m p a r i s o n w i t h
t h e l a t t e r a le s s s e v e r e c a s e w i t h o u t o r b i t a l a n d
f r o n t a l i n v o l v e m e n t i s p r e s e n t e d i n F i g u r e 2 2 B
a n d D . T h e d e f i c i e n c y o f t h e m a x i l l a i n t h i s c a se
is c o m p e n s a t e d b y e x t r u s i o n o f m a x i l l a r y t e e t h
o n t h e a f f e c t e d s id e a n d n o r e c o n s t r u c t i o n o f t h e
s o f t t i s s u e d e f i c i e n c y h a s b e e n a t t e m p t e d .
T h e s ki ll o f t h e s u r g e o n a n d t h e o t h e r p r o f e s-
s i o n a ls i n v o l v e d in t h e t r e a t m e n t o f t h e s e p a -
7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 17/20
: , l - 'J~£ ~-- >> H o m e I T O
~ ~
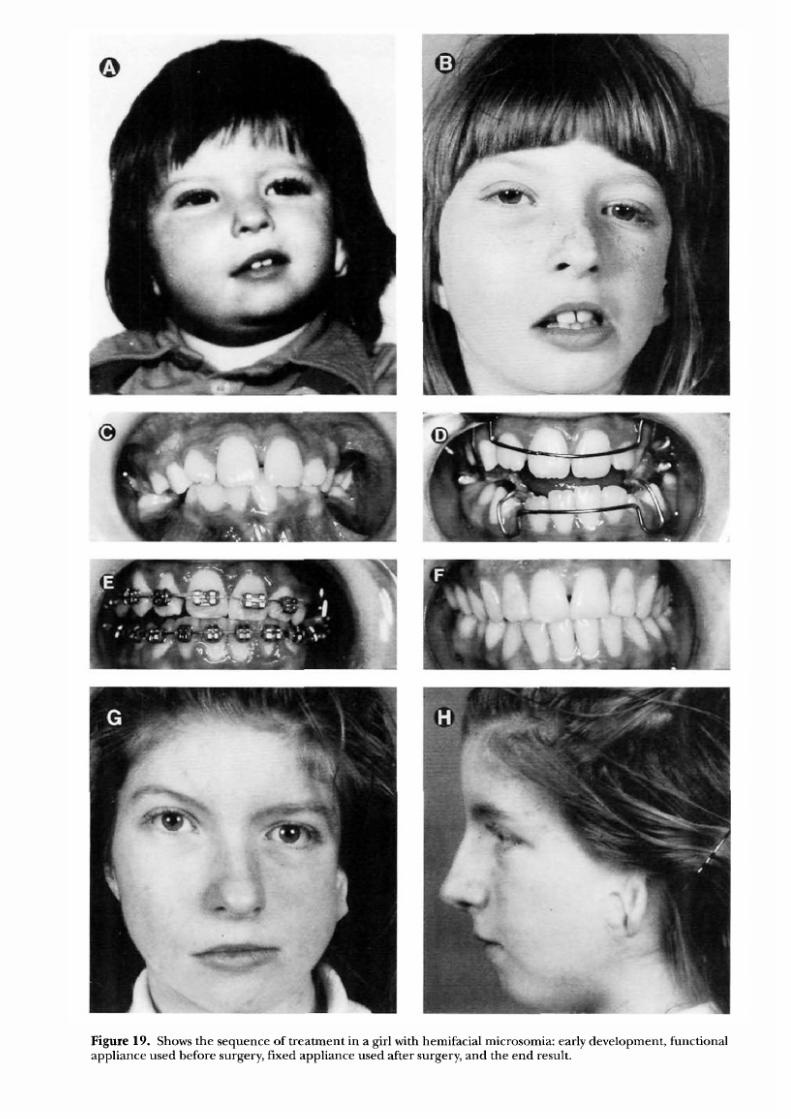
Figure 19 . Show s the seq uence o f t rea tm ent in a g i r l w i th hem i fac ia l m icrosom ia: ear ly deve lopm ent func t iona l
appl ian ce used before surgery f ixed appl ian ce used after surgery and the end result .

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 18/20
: , t- J,. a >> Hom e I TO C
F i g u r e 2 0 . A ) O P G o f t h e p a t i e n t s h o w n i n F i g 1 9 b e f o r e s u r g e r y . B ) O P G o f t h e p a t i e n t s h o w n i n F i g 1 9 a f t e r
surgery .
F i g u r e 2 1 . A ) I l lu s t r a t i o n o f a h e m i f a c i a l m i c r o s o m i a p a t i e n t w h o d e c l i n e d s u r g e r y , a t t h e a g e o f 4 y e a rs .
B ) P a t i e n t a t 6 y e a r s o f a g e . C ) P a t i e n t a t 9 y e a r s o f a g e a f t e r t r e a t m e n t w i t h a f u n c t i o n a l a p p l i a n c e . D )
D e n t i t i o n o f t h e p a t i e n t a t t h e a g e o f 9 y e a rs . N o t e t h e o p e n b i t e o n t h e n o n a f f e c t e d r i g h t s i d e as a r e s u l t o f t h e
t r e a t m e n t w i t h t h e f u n c t i o n a l a p p l i a n c e ,

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 19/20
: , t- J,. a >> Hom e I TO C
8
Prahl Ander sen and Fischer
Figure 22. A) A patient with hemifacial microsomia. Note the cant of the mout h a nd the involvement of the
orbital region. B) A patient with hemifacial microsomia. Note that the c ant of the mouth and the involvement of
the orbital region is less when compa red with the pat ient A). C) Illustrat ion of the tr eat ment result of the
pati ent A). Only the mandib le was correct ed an d the orbital involve ment was left alone. D) Illustrat ion of the
treatme nt result of the patient B). Only the mandi ble was affected and corrected.
t ients are of para moun t i mpor tance. This means
a sufficient caseload, expertise, and interest in
craniofacia l problems concen tra te d in a mul t id is -
ciplina ry team. An efficient appr oach to the
treatment of craniofacia l malformat ions , on an
int erna tio nal basis , is lacking. No consens us on
classif ication, for ex ample, hemifacial microso-
mia, has been reached. This makes discussions

7/17/2019 1-s2.0-S1073874696800454-main
http://slidepdf.com/reader/full/1-s20-s1073874696800454-main 20/20
At- .t~ e >> Ho me I TO C
symmetrical Facial Growth
8
on treatment indications and comparisons of
treatment results difficult. International coopera
tion is necessary to compile sufficient statistical
data for a scientific evaluation of treatment
results. This is the only way the quality of treat
ment results can be improved.
References
1. Poswillo D. Hemorrhage in development of the face.
Birth Defects 1975;11:61-81.
2. Munro IR. Treatment of craniofacial microsomia. Clin
Plast Surg 1987;14:177-186.
3. Ross RB. Lateral facial dysplasia first and seco nd bran-
chial arch syndrome, hemifacial microsomia). Birth
Defects 1975;11:51-59.
4. Prahl -Andersen B, Kowalski CJ, Heijdenda el P. A Mixed-
longitudinal Interdisciplinary Study of Growth an d Devel-
opment . NewYork: Academic Press, 1979.
5. Ras E Habets LLMH, v.Ginkel FC, et al. Facial left-f ight
dominance in cleft lip and palate: Three dimension
evaluation. Cleft Palate CraniofacJ 1994;31:461-465.
6. Pruzansky S. Not all dwarfed mandibl es are alike. Birth
Defects 1969;5:120-129.
7. Harvold EP, Vargervik K, Chierici G. Treatment of
Hemifac ial Microsomia. NewYork: Liss, 1983.
8. David DJ, Maha tumarat C, Coote r RD. Hemifac ial micro-
somia: A multisystem classification. Plast Reconstr Surg
1987;80:525-535.
9. Vento AR, LaBrie RA, Mulliken JB. The O.M.E.N.S.
classification of hemifacial microsomia. Cleft Palate J
1991;28:68-76.
10. Zonnevel d FW, Lobre gt S, v.d.Meulen JC, et al. Three-
dimens ional imagi ng in craniofacial surgery. World J
Surg 1989;13:328-342.
11. Converse JM, Coccaro PJ, Becker M, et al. On hemifacial
microsomia. The first and second branchial arch syn-
drome. Plast Reconstr Surg 1973;51:268-279.
12. Vargerv ik K, Ous ter hou t DK, Farias M. Factors affecti ng
long-t erm results in hemifacial microsomia. Cleft PalateJ
1986;23 Suppl 1:53-68.
13. Osbo rne R. The t reatme nt of Lhe unde rdeve loped ascend-
ing ramus. BrJ Plast Surg 1964;17:376.
14. Obwegeser HL. Correction o f the skeletal anomalies of
oto-mandibular dysostosis. J Maxillofac Surg 1974;2:
73-92.
15. Gnoinski W. The mor pholo gy of otom andib ular dysosto-
sis and its conse quen ces for therapy. Trans Eur Orth od
Soc 1974:77-84.





























