Embed Size (px)
Citation preview

1
Thyroid Associated Orbitopathy
10th Asia and Oceania Thyroid Association Congress
October 21-23, 2012
Yuji Hiromatsu, M.D., Ph.D. Division of Endocrinology and Metabolism, Department of Medicine,
Kurume University School of Medicine, Kurume, Japan

2
Thyroid Associated Orbitopathy
Yuji Hiromatsu, M.D., Ph.D. Division of Endocrinology and Metabolism, Department of Medicine,
Kurume University School of Medicine, Kurume, Japan
Pathogenesis Role of MRI Treatment
10th Asia and Oceania Thyroid Association Congress
October 21-23, 2012

外眼筋
脂肪組織
涙腺
外眼筋
上眼瞼挙筋
Proptosis
Lid retraction
Abnormal Secretion of Lacrimal fluid
Eyelid
Conj.
Cornea
Extra-ocularMuscle
Optic NerveRetina
Primary Secondary impairmentSiteMüller’s muscle
Lacrimal gland
Extraocular Muscle
Orbital connective tissue
上眼瞼挙筋Lev palpebrae sup

Geneticfactor
Enviromentalfactor
TRAb
Hyperthyroidism Graves’ ophthalmopathy Pretibial myxedema
Robert James Graves(1796~1853)
Graves’ disease Morbus Basedow
Carl von Basedow
Breakdown of immunological tolerance
(1799~1854)
80~90%
25~50%
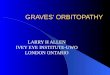
(Thyroid associated orbitopathy)

En
larg
em
en
t of
eye
mu
scle
s(
mm
2)
ー +0
200
400
600
800
1000
1200
1400
TNFαgene expression in eye muscle tissue
P < 0.05
0
500
1000
1500
2000
2500
Orb
ital fa
t volu
me
(mm
2)
P < 0.05
IL-4 IL-6 IL-10ー + + ー +
P < 0.05 P < 0.05
Cytokine gene expression in orbital fat tissue
ー
( Hiromatsu et al. : JCEM 85:1194, 2000 )
Increase of orbital fat tissueEnlargement of eye muscle

Expression of TSH-R mRNA in the orbitTSH-R
( 1.2kb )
TSH-R (296 bp)
RT-PCR
In situ hybridization
anti-sense sense (Hiromatsu et al. Thyroid 6: 553, 1996)

Gene Array StudiesGene Fold Function
PPAR-g 44.2 Signal transduction
Pro-platelet basic protein 32.9 Cell proliferaion
Collagen type 1a1 28.2 differentiation
Adiponectin 25.0 Metabolism
IL-6 23.9 Cell proliferation
Glycogenin 2 22.4 Glycogen biosynthesis
sFRP-1 18.5 Signal transduction
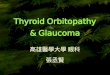
(Kumar et al.: JCEM 90:4730, 2005)sFRP-1 (secreted frizzled related protein-1)

(Kumar, S. et al. J Clin Endocrinol Metab 2005;90:4730-4735)
sFRP-1 (100 nM) induced adiponectin mRNA (A), leptin mRNA (B), and TSHr mRNA (C) expression
on orbital fibroblasts
sFRP-1 induces adipogenesis and expression of TSHR on orbital fibroblasts.
sFRP-1 (secreted frizzled related protein-1)

Peroxisome Proliferator-Activated Receptor-g in Thyroid Eye Disease: Contraindicaiton for Thiazolidinedion Use?
(Starkey et al: J Clin Endocrinol Metab 88: 55-59, 2003)
57 yr-old male, 8-yr history of type 2 DM
Pioglitazone 30mg/d for 3 months
6wk pre 3m on 3m stop Proptosis rt 19mm 21 20 lt 20 23 22Conj. Redness (-) mild (-)Lid swelling Mild Severe SevereDiplopia (-) Intermittent (-)CAS 6 2

Thiazolidinedione induced Graves’ ophthalmopathy
• Starkey K, Heufelder A, Baker G, Joba W, Evans M, Davies S, Ludgate M. : Peroxisome proliferator-activated receptor-gamma in thyroid eye disease: contraindication for thiazolidinedione use? J Clin Endocrinol Metab. 2003;88:55–9.
• Levin F, Kazim M, Smith TJ, Marcovici E. : Rosiglitazone-induced proptosis. Arch Ophthalmol. 2005;123:119–21.
• Dorkhan M, Lantz M, Frid A, Groop L, Hallengren B. : Treatment with a thiazolidinedione increases eye protrusion in a subgroup of patients with type 2 diabetes. Clin Endocrinol (Oxf). 2006;65:35–9.
• Lee S, et al. : Thiazolidinedione induced thyroid associated orbitopathy. BMC Ophthalmol. 2007; 7: 8.

CD34+OF CD34-OFIL-16
RANTES CXCL10
IGF-1R↑
IGF-1R Ab
Migration of T cells
T cellT cell
Macrophages
Adipogenesis
IL-6IL-8
CXCR4
TSHR↑
TSHR Ab
Glycosaminoglycansshort chainhyaluronan
long chainhyaluronan
proliferation
B cellactivation
TSHR Ab IGF-1R Ab
IL-1aIL-8
COX-2CXCL12
CytokineTh1, Th2
IL-1TNFaTGFb
IL-6TNFa
CD40CD40L
B7
TCR
HLA
Th1- : Leukoregulin,TNFα, IL-1β, INFβ, INFγ, IL-2, IL-12Th2- : IL-4, IL-5, IL-10Antibody
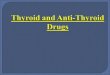
serumCD34+fibrocytes
Orbital fibroblasts
+
PPARgTGFbTNFa
_
IL-1bIFNgTGFbTNFa
+
Orbit
preadipocytes
TSHR Ab IGF-1R Ab

CD90 (Thy-1)+ orbital
fibroblasts may differentiate
into myofibroblasts, that
participate in the
development of fibrosis in
late stages of the disease.
Bahn R.S: N Engl J Med 2010; 362:726-738.
Myofibroblast
Thy-1+
OF
TGF-β
FibrosisFibrosisExtraocular muscle
enlargement
Extraocular muscle
enlargement
ExpandedAdiposetissues
ExpandedAdiposetissues
ElevatedTRAb
ElevatedTRAb

Relationships between anti-TSH receptor antibidies and GO
• TRAB ( 1st generation; TBII)• TRAb (2nd generation; hTRAb; TRAb-CT)• TRAb (3rd generation; M22)• TSAb• TSI [Mc4; chimeric TSH-R (amino acid residues
262-335 of human TSH-R replaced by rat LH-R) ]

Anti-TSH receptor Antibodies
TBII
TSAb
TSH-R antibodies TBII TSAb
GO (+) GO (ー) Normal 67% 85% 0%59% 83% 0%
(Hiromatsu et al., Thyroid 6: 553, 1996)
(Nishikawa et al., Acta Endocrinol 129: 213, 1993)
In GO patients there are significant correlation between TRAb and the enlargement of eye muscle.
At the first visit, there is no difference in the prevalence of TRAb between GO and GD without ophthalmopathy.
Enlargement of EM En
larg
em
en
t of
EM

Anti-TSH receptor antibody in GO
Mild GO Severe GO

The novel chimeric(Mc4) TSH-R (amino acid residues 262-335 of human TSH-R replaced by rat LH-R)

TSI level of GO was greater than that of Graves’ disease without ophthalmopathy.Majority of patients with GD had undergone antithyroid treatment and were rendered euthyroid at the time of blood sampling.
chimeric (Mc4) TSH-R (amino acid residues 262-335 of human TSH-R replaced by rat LH-R)
A novel thyroid stimulating immunoglobulin assay

Correlation of the thyroid stimulating lgs in GO with clinical disease activity.

Th2 thyroiditis
Shared antigens Between thyroid and orbit
Tg
Hyperthyroidism (Graves’ disease)
Breakdown of immune tolerance
Breakdown of immune tolerance
Genetic factors Genetic factors Enviromentalfactors
Enviromentalfactors
Th1, Th2cytokines
Anti-TSH receptor AbsAnti-TSH receptor Abs
Anti-EM Ab
Tg
adipogenesisTSH receptor ↑
sFRP-1, CYR61G2s
SDH1D
EM antigensG2s
1D
Calsequestrin
TSH receptor
Mild
SeveresmokingCTLA-4
CD40PTPN22
HLA TNFaICAM-1NFkB1FOXP3
IGF-1receptor↑
Greves’ ophthalmopathy
Collagen XIII
IGF-1R Ab
TSI
Infl
amm
atio
n /
fib
rosi
s

genotype Allele frequency
TT TC CC T C OR
n
28(45.2)
81(73.0)
29(46.7)
30(27.0)
5(8.1)
0(0)
85(68.5)
192(86.5)
39*(31.5)
30(13.5)
GO
GDw/ooph
62
111
TNF-α gene polymorphism (T-1031C) and GO
* P=0.0001
( Kamizono et al. Clin Endocrinol 2000; 52:759-764.)
2.9
(日本人)
The C allele frequency is higher in GO patients.

ICAM-1 gene polymorphism
class ⅢーⅥ
class 0-Ⅱ
AA
46
72
(%)
(49)
(36)
GA
36
99
(%)
(39)
(49)
GG
11
30
(%)
(12)
(15)
A (%)
128(69)
243(60)
G (%)
58(31)
159(40)
χ2=4.925 P=0.0852
χ2=3.825 P=0.0505
Allele frequencyGenotype frequency
class ⅢーⅥ
class 0-Ⅱ
AA
46
72
(%)
(49)
(36)
GA + GG (%)
47(51)
129(64)
χ2=4.643 P=0.0312
K469E (1405 A→G)
The AA genotype frequency is higher in severe GO .
OR
1.75
OR
1.44
ATA class

NFkB1 gene polymorphism( -94del ATTG )
Genotype frequency Allele frequency
Del (%) Hetero (%) Ins (%) Del (%) Ins (%)N
Ⅲ ~Ⅵ
0~Ⅱ 301 38(13%)
132(44%)
131(43%)
123 25(20%)
59(48%)39(32%)
109(44%)
137(56%)
208(35%)
394(65%)
χ2=6.853 P=0.0325OR 1.76
χ2=7.103 P=0.0077OR 1.51
The -94delATTG polymorphism of the NFkB1 gene is higher in severe GO.
ATA class

PPARγ ( Pro12Ala) gene polymorphism
Genotype Allele
CC (%) CG (%) GG (%) C (%) G (%)N
Ⅲ ~Ⅵ
0~Ⅱ 294 271(69%)
21(87%)2( 100 %)
123 120(31%)
3(13%) 0(0%) 243(30%)
3(11%)
563(70%)
25(89%)
Χ 2=4.439 P = 0.1087
Fisher’s exact probability testP = 0.0328OR 3.59
Patients with CC genotype frequently have severe ophthalmopathy.
ATA class
Χ 2=4.430 P = 0.0381OR 3.39

Summary (1) 1. TSH receptor is a primary autoantigen in GO.
Recent study suggests the presence of GO specific TRAb (Mc4)?
2. The increase of TSH receptor expression through adipogenesis is important in the pathogenesis of GO.
3. CD34+ fibroblasts, which are derived from peripheral blood and expand in the orbit, express TSH receptor in high level.

4. The increase of IGF-1 receptor expression in the orbital fibroblasts may also be important. Activation of IGF-1R leads secretion of IL-16 and RANTES on CD34-
fibroblasts, which enhance recruitment of activated T lymphocytes.
5. CD90 (Thy-1)+ orbital fibroblasts may differentiate into myofibroblasts that participate in the development of fibrosis in late stages of the disease.
6. Gene polymorphisms of the immunomodulator genes (such as TNFa, ICAM-1, NFkB, PPARg and FOXP3 etc) have been proposed as the susceptibility genes for GO.
7. The significance of the presence of anti-eye muscle antibodies, such as SDH, CASQ needs to be confirmed.

Thyroid Associated Orbitopathy
Pathogenesis Role of MRI Treatment

NOSPECS classification of eye changes of Graves’ disease (Thyroid 2:235, 1992)
Class Definition
0 No physical signs or symptoms
I Only signs, no symptoms (upper lid retraction, stare, and eyelid lag)
II Soft tissue involvement (symptoms and signs)
III Proptosis
IV Extraocular muscle involvement
V Corneal involvement
VI Sight loss (optic nerve involvement)

NOSPECS classification of eye changes of Graves’ disease (Thyroid 2:235, 1992)
Class Definition
0 No physical signs or symptoms
I Only signs, no symptoms (upper lid retraction, stare, and eyelid lag)
II Soft tissue involvement (symptoms and signs)
III Proptosis
IV Extraocular muscle involvement
V Corneal involvement
VI Sight loss (optic nerve involvement)
MRI 70%
50~75% of patients with
Graves’ disease do not have any signs or symptoms
of GO.

Occult Thyroid Eye DiseaseNo physical signs or symptoms
Enlargement of extra-occular muscles
Occult thyroid eye diseaseCase 1 Case 2

MRI
I Only signs, no symptoms (upper lid retraction, stare, and eyelid lag)
Total Mild Moderate severe
Lid retraction
1587(79.3) 792(39.6) 620(31.0) 175(8.7)
2000 eyes (%)Inoue et al.

Dalrymple sign (lid retraction)
Case 3 Case 4

von Graefe’s sign
R L R L
Case 5 Case 6

R LR L
Unilateral lid retraction
Case 7 Case 8

MRI
II Soft tissue involvement (symptoms and signs)
Total Mild Moderate severe
Lid swelling
1354(67.7) 958(47.9) 376(18.8) 20(1.0)
Conjunctiva 642(32.1) 451(22.6) 170(8.5) 21(1.0)
2000 eyes (%)Inoue et al.

Swelling of upper and lower eyelidCase 9

MRI
III Proptosis
Male 444 eyes
female 1556 eyes
Japanese
Untreated Graves’ disease Symptoms 24.2%
Hertel exophthalmometermild 39% total 57%
moderate 1 3% severe 5%
GO patients (4598 eyes) total 85% mild 39%
moderate 33% severe 13%
Proptosis alone 18.5% + lid lag 46.2% + lid swelling 19.0% + lid lag and lid swelling 16.3%

Proptosis
R) 13.0 mm L) 13.0 mm R) 17.0 mm L) 17.0 mm
R) 19.0 mm L) 19.0 mm R) 28.5 mm L) 30.5 mm

Proptosis 18mm~<21mm Proptosis ≥21mm
+ lid swelling
+ lid swelling+ lid retraction
Case 11 Case 13
Case 12 Case 14

MRI
IV Extraocular muscle involvement
Total Mild Moderate severe
Diplopia 447(22.3) 237(11.8) 74(3.7) 136(6.8)
2000 eyes (%)Inoue et al.

Diplopia
Restriction of motion in upward gazeVertical deviation of right eye
Enlargement of right inferior rectus muscle
Case 15

MRI
VI Sight loss (optic nerve involvement)
Total Mild Moderate severe
DON 168(8.4) 147(7.4) 13(0.6) 8(0.4)
2000 eyes (%)Inoue et al.
Papilledema Papillitis Optic disc atrophy

He complains orbital ache and decreased visual acuity.
Eyelid swellingEyelid eythema Conjunctival rednessProptosis
MRI: The enlargement of superior, inferior, medial and lateral rectus musclesmay compress optic nerve.
T2 immage:The increased T2 relaxation time indicates that GO is in active state.
Case 17

Summary (2)
MRI is • useful for the assessment of GO.• useful for planning of the management of GO.
We strongly recommend MRI for management of GO.

Thyroid Associated Orbitopathy
Pathogenesis Role of MRI Treatment

Mild Moderate to severe Sight-threatening (DON )
i.v. GCs (±OR)
prompt decompression
Still active
Iv GCs(±OR)
Rehabilitative surgery
Stable & inactive
Active
Rehabilitative surgery(if needed)
i.v. GCs (±OR)
Stable & inactive
Rehabilitative surgery (if needed)
Inactive
Local injection of GCs or Botulinum toxin
Ophtalmological examination, CAS, QOL
Local measuresWait and see
MRI
Poor response (2 weeks)
MRI
All patients with GO
NOSPECS Class 0 NOSPECS Class I~VI
Restore euthyroid (avoid hypothyroidism)Urge smoking withdrawal
Wait and see
Occult thyroid eye disease
Specialized center
MRI
Inflammation ofUpper eyelids
intractable
Immuno-suppressant ,Decompression
Inflammation of eye muscles
Stable &inactive
Progression
Treatment of Graves’ ophthalmopathy

Sight-threating GO (DTN)
MRI
i.v. Glucocorticoids
i.v. Glucocorticoids( orbital radiation)
Rehabilitative surgery
Still active
Poor response(2 weeks)
Prompt decompression
Stable and inactive
methylpredonisolone1g/d 3days 3 cycles
Pulse therapy
1w
Sight-threating GO (DON)Dysthyroid optic
neuropathy ( DON ) and/or
Corneal breakdown

Pulse therapy Before After
3 cycles

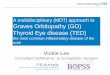
Transantral orbital decompression for Papilledema ( dysthyroid optic neuropathy)
pre
post
Papilledema
6 months after the surgery

Moderately to severe GO
MRI
i.v. Glucocorticoids( orbital radiation)
Rehabilitative surgery
Stable and inactive
active inactive

Severity
Activity
Immunosuppressive therapy
Severity
Activity
Immunosuppressive therapy
Outcome Outcome
Prediction of outcome of Immunosuppressive treatment
Rehabilitative therapy

Classical Pulse1g/d 3days 3 cycles
Irradiation2Gy 10 times
Prednisolone 20mg 15mg 10mg 5mg
Pulse therapyOral steroid
①
1w
Efficacy : 77 % ( Pulse + irradiation : 88 %) Side effects : peptic ulcer 、 glucose intolerance 、 osteoporosis
Efficacy : 59 % ( 44 % in 5 RCT )Side effects : exacerbation of inflammation 、 Cataract 、 Retinopathy, Tumorgenesis

Fatal liver failure• Acute liver damage occurred in 0.8%, and was lethal in 0.3% of
patients with GO underwent iv GC.• Direct toxic effect? Precipitation of virus-induced hepatitis? AIH?
ANAAIHNone 8Recovery439***
CMV3.2Recovery548
steatosisHBV15.7Recovery557
None17.1Recovery306
None15Recovery455
None17.1Death474
None7.1Death633
ANAsteatosisNone7.8 wkDeath562**
None4 wk after 5 cyclesDeath711*
Liver diseaseVirusTime of diagnosisOutcomeAgeCase
* Weissel et al. Thyroid 10: 521, 2000 ** Marino et al. Thyroid 14: 403, 2004*** Salvi et al. Thyroid 14: 631, 2004
The cumulative dose should be <8g methylprednisolone in one course of therapy. (EUGOGO)

Classical Pulse1g/d 3days 3 cycles
Irradiation2Gy 10 times
Prednisolone 20mg 15mg 10mg 5mg
Pulse therapyOral steroid
①
1w
Efficacy : 77 % ( Pulse + irradiation : 88 %) Side effects : peptic ulcer 、 glucose intolerance 、 osteoporosis
Efficacy : 59 % ( 44 % in 5 RCT )Side effects : exacerbation of inflammation 、 Cataract 、 Retinopathy, TumorgenesisMini-pulse
0.5g/d 3days 3 cycles
Irradiation2Gy 10 times
Prednisolone 20mg 15mg 10mg 5mg
Oral steroid
②1w

Liver dysfunction during and 1 year period after pulse therapy (4 centers, 480 cases)
020406080
100120140160180200220240260280300320340360380400420440460480500520540
前 (ALT) 高値 (ALT) 3(ALT) 6(ALT)
ALT
before 1 month 6months 12 months

NoLiver dysfunction ( ALT)
> 100 50 ~ 100 total
Methylprednisorone 1 g/d, 3 days, 3 courses
136
17cases
12.5 % 27cases
19.9 % 44cases
32.4 %
Methylprednisorone 0.5g/d, 3 days, 3 courses
97
3 3.1 % 17 17.5 % 20 20.6 %
Total 233 20 8.6 % 44 18.9 % 64 27.5 %Fisher’s exact probability testP=0.0115
c 2= 3.913 、 P=0.0479
Liver failure and steroid pulse therapy(4 centers )
Liver dysfunction (ALT>100) was more frequently found in patients with high dose of methylprednisolone (>9g) pulse therapy than in low dose (4.5g). -Dose dependency-
Out of 20 cases with increase of ALT>100, Two cases were HBcAb+, their ALT increased to 639 、 326. Four cases were were HCVAb positive, and their ALT elevated to 223,188,149,124. -Reactivation of hepatitis virus infection –
In 7 out of 11 cases, who were HCVAB positive before pulse therapy, the increase of ALT was observed.

HBV carrier and patietns with past history of HBV infection.
Check HBV-DNA.Avoid pulse therapy.
If ophthalmopathy needs pulse therapy, consult with hepatologists for the use of entecavir.
Check liver function and HBV-DNA every month during and 1 year-period after pulse therapy.

Treatment in inactive stage
Rehabilitative Surgery• Orbital Decompression • Eye Muscle Surgery• Eyelid Surgery

Pre 3 months after surgery
Proptosis
preRt 22mmLt 20mm
postRt 15mmLt 14mm
Rehabilitative Surgery Transantral Orbital Decompression
Case 19

6months afterbefore
Deep Lateral Orbital Decompression

6 months afterbefore
Rt 27mm Lt 28mm Rt 24mm Lt 24mm
Case 20

Rehabilitative Surgery
Eye Muscle Surgery
Removal of the cicatricial tissue of left inferior rectus muscle
Lt upward gaze impairment(enlargement of left inferior rectus muscle)
Case 21

Pre
Post
Rehabilitative SurgeryEyelid Surgery
Lengthening of Levator Muscle
Lenghening of Levator Muscle procedure by using polytetrafluoroethyrene as spacer.
Case 22

Mild GO
MRI
Rehabilitative surgery (if needed)
Stable and inactive
Local measures
active
Inflammation of EM and fat tissues
i.v. glucocorticoids(±orbital radiation
Stable and inactive
Local injection of triamcinolone acetonide and botulinum A toxin
Inflammation ofeyelid
progression
Wait and see

Triamcinolone acetonide injection
Rt ) lid swelling 、 lid lag 、 Graefe’s sign 2 months after the injection
Case 23

Botulinum toxin therapy
Full effect is evident after 2-3 days and persists for 4-6 weeks.
Indication: upper lid retraction
Case 24

Potential Therapeutic Targets in Graves’ ophthalmopathy
Target Current Agent TNF InfliximabTNF receptor EtanerceptIL-1 receptor AnakinraIL-6 receptor TocilizumabTGF-b LerdelimumabOxygen free radicals SeleniumCD20 RetuximabCD3 ChAglyCD3CD28 AbataceptCD154 IDEC-131PPAR-g Selective PPAR modulatorsSomatostatin receptor Octreotide-long acting release
SOM230 Thyrotropin receptor NIDDK/CEB-52
TSHR antagonist (Org-274179-0)

Anti-CD20 monoclonal Ab (rituximab)• Open study : 9 caces RTX 1000mg iv twice at 2wk interval• 20 cases IVGC methylprednisolone 500mg iv for 16 weeks
Salvi et al. Eur J Endocrinol 2007; 156:33-40
Rituximab (1000mg)
00
0

Anti-CD20 monoclonal Ab (rituximab)
Peripheral depletion of CD20+ cellsSalvi et al. Eur J Endocrinol 2007; 156:33-40
CD20
CD20
B cell
B cell

Anti-CD20 monoclonal Ab (rituximab)
RTX IVGC RTX v.s. IVGCCAS 4.7 1.8 4.1 2.0 better
TRAb 19.3 11.5 16.3 9.3 not significant not significant not significant
Proposis 22.4 20.9 22.6 22.1 not significant significantly decreased significantly decreased
Palpebra improve improve not significant
Side effecs 33 % 45 %Recurrence 0 % 10 %
Salvi et al. Eur J Endocrinol 2007; 156:33-40

Complete Inhibition of rhTSH-, Graves’ Disease IgG-, and M22-Induced cAMP Production in Differentiated Orbital Fibroblasts by a Low-Molecular-Weight TSHR Antagonist
Clementine J. J. van Zeijl, Chris J. van Koppen, Olga V. Surovtseva, et al.(J Clin Endocrinol Metab 97: E781–E785, 2012)
Clementine J. J. van Zeijl, Chris J. van Koppen, Olga V. Surovtseva, et al.(J Clin Endocrinol Metab 97: E781–E785, 2012)

Summary (3)
1. Liver dysfunction (ALT>100) was more frequently found in patients with high dose of methylprednisolone (>9g) pulse therapy than in low dose (4.5g).
2. Reactivation of viral hepatitis should be considered.

Conclusion
Significant progress has been made in our understanding of the immunogenetic mechanisms leading to GO. We hope that these findings may be translated into new therapies and prevention strategies in GO. All the patients with GO should benefit from these efforts in near future.

ご清聴ありがとうございました。
Thank you for your attention.