Embed Size (px)
Citation preview

1
University of California
Student Mental Health and Study Abroad

2
Inés DeRomañaInés DeRomañaSafety, Security, and Health AffairsSafety, Security, and Health Affairs
University of California University of California Education Abroad Program Education Abroad Program
SystemwideSystemwide

3
Inés DeRomañaInés DeRomañaChairChair
NAFSANAFSAHealth and Safety SubcommitteeHealth and Safety Subcommittee

4
• Overview: National trends in college student mental health; scope of the problem
• Overview: Education abroad and mental health
• Good Practices: To respond effectively to students who are distressed
Objectives

5
Areas of Responsibility
• Safety
• Security
• Risk assessment
and management
• Crisis management (critical incident)
• Physical/Mental health policy
• EAP health clearance process; student health insurance
• Students with disabilities (policy)
• Student conduct (policy and management)
• Title IX Sexual Harassment Officer (students)

6
UCEAP Throughout the World4,500 students, 130 institutions, 109 cities, 35 countries

7
NAFSA
• Responsible Study Abroad:Responsible Study Abroad: Good Practices for Health & Safety, Interorganizational Task Force on Safety and Responsibility in Study Abroad
• Program Sponsors should:
• Develop and provide health and safety training for Develop and provide health and safety training for program directors and staff, including guidelines program directors and staff, including guidelines with respect to intervention and referral that take with respect to intervention and referral that take into account the nature and location of the study into account the nature and location of the study abroad programabroad program

8
The Forum on Education Abroad
• Standards of Good Practice for Short-Term Education Abroad Programs
• Health:Health:
The program leadership is aware of student The program leadership is aware of student health issues prior to departure and is well health issues prior to departure and is well prepared to handle student, faculty, and staff prepared to handle student, faculty, and staff health issues that may arisehealth issues that may arise

9

10

11
18 through 26 years old

12

13
14
Some Challenges
• Many different medical conditions (anxiety, mood, eating, depressive, bipolar disorders, etc.) Continuum of severity Different functional implications
• Mental illness and alcohol/drug addiction often occur together Youth depression and alcohol:
• Drinkers 2 times more likely to be depressed• Binge drinkers 4 times more likely*
* Hallforset al, 2004; Hall et al., 1999; Mann et al, 2006

15
Current Trends
• Anxiety/panic disorders
• Depression
• Eating disorders
• Suicidal tendencies
• Cutting (self injurious)
• Bipolar Disorder
• Asperger Syndrome

16
Current Trends
• More students with psychological issues
• Increasing frequency of occurrencefrequency of occurrence and degree of degree of debilitationdebilitation
• Arriving on campus with psychotropic medications
• Placing major strain on campus resources

17
DIAGNOSIS Average Age of Onset
Manic/Depression 18
Drugs & Alcohol 21
Schizophrenia 21
Depression 20-26
Borderline Personality Disorder 18-25
Anti-social Personality Disorder 18-25
Source: Dr. Reina Juarez, University of California, San Diego, Director of Psychological Counseling
Reality

18
Adding Complexity
• New evidence: Impulse control, planning and decision making are largely prefrontal cortex functions that are still maturing during adolescence*
• Lack of sleep 35% insomnia stress
*The Adolescent Brain: A Work in Progress. Daniel R.Weinberger, M.D., Brita Elvevåg, Ph.D., Jay N. Giedd, M.D. June 2005

19
Adding complexity
• Prescription medication abuse (non-medical purpose) or non-compliance Psycho stimulants (Ritalin®, Adderall®)
Opioid analgesics (Vicodin®, OxyContin®, Tylenol #3®) Buying/selling medication Self-medicating; non-prescribed
• Alcohol abuse/drug abuse 44% heavy drinkers*
*Harvard School of Public Health College Alcohol Study (CAS)

20
Adding complexity
• Failure to obtain needed help (resistance or lack of awareness) Waiting until problem becomes severe
• Resistant to seek help (moderate to severe symptoms) Notion of invincibility Fear
• Reluctance to continue treatment Time commitment Peer pressure

21
Adding complexity
• Millennials more stressed/more depressed
• Faculty/staff training Unfamiliar with policies Unfamiliar with distressed student behavior and
protocols Unfamiliar with confidentiality, notification, and
other legal issues• FERPA & HIPAA misunderstandings
Lack/limited knowledge• Observe and identify patterns of behavior

22
Study Abroad – Next Exit?
Helping distressed studentsHelping distressed students

23

24
Report from UC Study Center Director
• The single greatest problem I have seen in student well-being during the last year and a half is depression and anxiety
• Pre-departure orientation should warn students—all students—that study abroad, in addition to being exciting, is also stressful and may exacerbate existing mental health and substance abuse issues

25
Contributing elements(Anecdotal evidence)
• Separation
• Travel stress
• Culture shock
• Adjusting to local conditions
• Learning or using a learned foreign language to communicate
• Different housing
• Social pressure
New friends; host family
• Unforeseen events
• Family issues in the U.S.
• Financial hardship
• Different expectations
• Different academic environment/expectations

26
Common Issues Abroad
• Substance abuse
• Anger management
• Abruptly stopping medication, or medication not legal/locally available
• “magic cure”
• Hx of eating disorder
• hx of severe depression, anxiety, bipolar disorder
• hx of suicide attempt/ideation
• Students without any psychological illness experiencing symptoms for the first time abroad
• Cutting; self-injury

27
Good Practices

28
We are not Alone: A Team Approach in Responding to Student Mental Health Needs

29
Student in Distress
Faculty andStaff
Student’s Family
Education Abroad Office
PeersOther
Students’
Families
Community Systems Approach in Assisting Students in Distress
ResidentDirector
Spiritual
leaders
Roommates/ live-in Partners
Counseling Centers
Housing
Source: Dr. Reina Juarez,UCSD Director of Psychological Counseling

30
Why is Basic Mental Health Training Important?
• Increase awareness
• Increase confidence; be effective responders
• Reduce stigma
• Students in distress seek help (friend, family, faculty, staff)
• Others will not seek help, but will show warning signs
• Impact is on ALL students in programALL students in program

31
Who Should do the Training?
• Campus counseling center professionals Meet/consult/partner with campus/local counseling
center regularly Create partnerships to help manage problems
• Education abroad staff (culture shock, local resources, etc.)

32
Good Practices: Training Model
• Mental Health First Aid Train U.S. and on-site staff and faculty
• How to identify distress early assess risk of suicide or harm listen non-judgmentally and offer support reassure student; encourage self-help; other
support strategies (Family? Peers? Friends? Spiritual guide?)
• How/when to refer
• What to do if student is reluctant to seek help
• Notifying emergency contact

33
Good Practices
• Require and be familiar with accident/sickness insurance State parity law Covered number of outpatient visits. Adequate? Medical evacuation. Adequate?
• Require a pre-departure health clearance After acceptance; self-disclosure Respect confidentiality of medical records
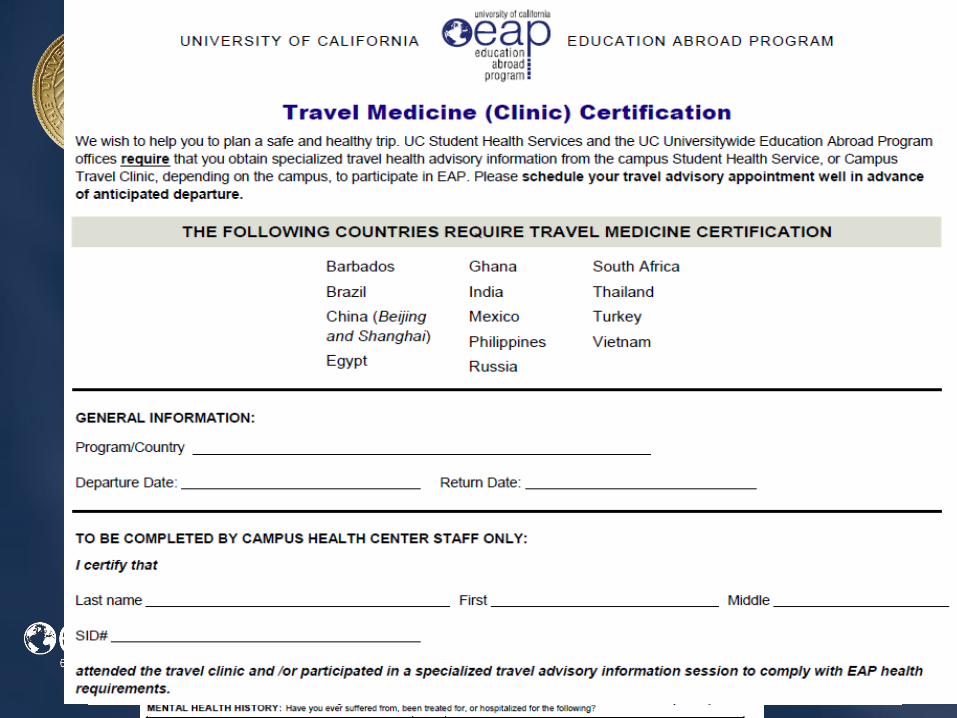
34
EAP Student Health Clearances

35
36

37
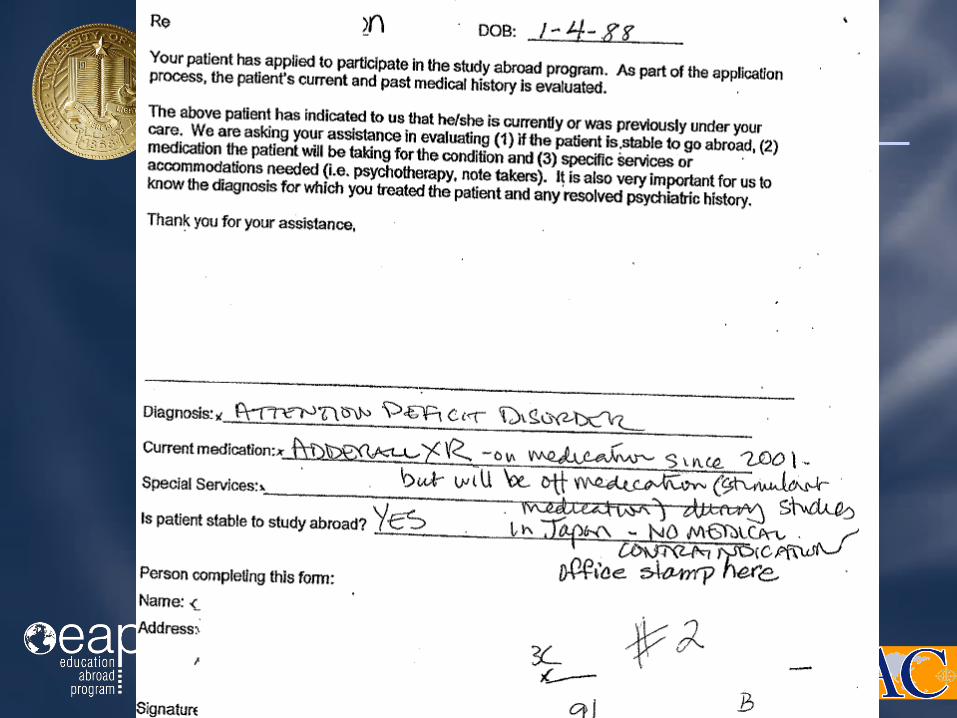
Good Practices
• Design policies to allow voluntary withdrawal for medical reasons Attorney and/or risk manager Focus on behavior: Use behavior contracts,
safety health plans, etc. Legal implications should never be the main
concern—student/faculty/staff safety
• Design policies to allow (or not) return to program Know if you can stipulate conditions

38

39
Good Practices
• During program planning, identify local resources (preferably bilingual)
• U.S. Embassy
• Insurance carrier (travel assistance)
• U.S. programs in area
• U.S. university counseling center
• Local area mental health clinics and hospitals
• Private mental health practitioners (English speaking; culturally sensitive)

40
Good Practices
• Educate (pre-departure/onsite orientations) students Signs and symptoms of mental illness Provide students with tools to recognize and
manage triggers and stressors
• Share information about availability of professional help abroad (confidentially) with all students
• Ensure all students know how to access these services (e.g. insurance, covered benefits) Ensure that students who need services receive
them

41
Good Practices
• Be aware of the attitudes toward mental disabilities in the local culture Include in pre-departure materials for students
• Know whether commonly prescribed medications in the U.S. are available Get list from the counseling center on campus Ask local contact or insurance carrier/travel
assistance plan

42
Good Practices
• Develop an emergency contact notification protocol Outline circumstances when contacts are notified Staff/faculty who can make such a notification
• Develop procedural “crisis or ‘what if’ checklists” Ensure
• appropriate action is taken• transparency of protocols• Staff/faculty have established guidelines

43
Conclusion

44
4 Simple Steps can Save Academic Careers and Lives
1. Learn to spot signs of distress early
2. Know how to offer support
3. Connect student to resources/refer
4. Know emergency procedures
Source: Dr. Jeffrey Prince, Director, Counseling and Psychological Services, UC Berkeley

45
What is MOST Helpful?
• Have a positive role
• Show concern
• You do not have to know everything; you just have to know resources to recommend

46
• The majority of students can participate successfully
Proper planning Self-awareness of potential stressors associated with
study abroad; dissemination of information Trained faculty/staff and students Adequate and required insurance Required health clearance
Be Proactive - Not Reactive

47
• The majority of students can participate successfully
Formalize protocols and structures Educate the study abroad community Who can tell what to whom? What happens after
this? Remove perceived and real barriers FERPA misperceptions HIPAA misperceptions
Be Proactive - Not Reactive

49
Resources





























