Embed Size (px)
Citation preview

1
Where are all the adrenoceptors?
EYE
Mydriasis - contracts pupillary and radia dilator muscles (1)
HEART
SA Node - HR (1 > 2)
Atria - contractility and conduction velocity (1, 2)
AV Node - conduction velocity (1, 2)
His-Purkinje fibers - contractility and conduction velocity (1,2)
Ventricles - contractility, conduction velocity, (1, 2)

2
Where are all the adrenoceptors?
LUNG Bronchial Smooth Muscle - Relaxation, airway diameter (2)
Bronchiole glands - secretion (1); secretion (2)
URINARY Detrusor muscle - contractility, relaxation (2)
Bladder sphincter (trigone) - tone, closure (1)
GI GI tract (general) - tone and motility (gastric, intestinal) (1,2; () )
GI sphincters - tone, contraction (1)
GI secretions - secretions; 2 can secretions

3
Where are all the adrenoceptors?
BLOOD VESSELS
Skeletal Muscles - 1 = constriction; 2 = strong vasodilation
Skin and mucosa - 1,2 = constriction
Abdominal Cavity - 1,2 = constriction; = dilation in liver
Salivary glands - 1,2 = constriction
Renal - 1,2 = constriction
ReproductiveUTERUS
Contraction = 1 (pregnancy); 2 = relaxation (ritodrine)
Penis
Ejaculation =

4
Where are all the adrenoceptors?
• LIVER
Glucose (Gluconeogenesis) via 1,2
Glucose (Glycogenolysis) via 1,2
• PANCREAS
Insulin release via Beta cells (2)
• LIPOLYSIS
TG levels via 2,1,2
5
Sales of Supplements Containing Ephedrine Alkaloids (Ephedra) ProhibitedOn April 12, 2004, a final rule went into effect prohibiting the sale of dietary supplements containing ephedrine alkaloids (ephedra).
Ephedra, also called Ma huang, is a naturally occurring substance derived from plants. Its principal active ingredient is ephedrine, which when chemically synthesized is regulated as a drug.
In recent years ephedra products have been extensively promoted to aid weight loss, enhance sports performance, and increase energy.
But FDA has determined that ephedra presents an unreasonable risk of illness or injury. It has been linked to significant adverse health effects, including heart attack and stroke. From http://www.fda.gov

6
DIRECT-ACTING ADRENERGIC AGONISTSPhenylephrine*Direct-acting adrenergic agent that primarily binds to alpha receptors and favors alpha1.
*Not a catechol derivative
Physiological effects:Raises systolic and diastolic blood pressures byVasoconstriction (nasal decongestant, and in opthalmic solutions for mydriasis)

7
DIRECT-ACTING ADRENERGIC AGONISTSTerbutaline*Direct-acting adrenergic agent that primarily binds to beta2 receptors.
*Not a catechol derivative
Physiological effects:BronchodilatorReduce uterine contractions in premature labor

8
DIRECT-ACTING ADRENERGIC AGONISTSAlbuterol*Direct-acting adrenergic agent that primarily binds to beta2 receptors.
*Not a catechol derivative
Physiological effects:Bronchodilator
Widely used as an inhalant to relieve bronchospasm.

Compliments of Byron Yoburn, Ph.D. 9
AntagonistsOverview
• Basic pharmacology of alpha blockers• Basic pharmacology of ß blockers• Clinical uses• Discussion is focused on autonomic and
peripheral effects
You should know the profile of effects that occur from using alpha, ß and ß specific blockers

10
Adrenoreceptor Antagonists

11

12
Alpha Blockers• Reversible • Phentolamine, tolazoline, prazosin, labetolol*
(*=beta-blocking too)– duration of action is typically related to kinetics
– What would concentration-effect curve for an alpha agonist look like in the absence (A) or presence of increasing concentrations (B, C) of a reversible antagonist ?

13
Alpha Blockers• Irreversible/noncompetitive– Phenoxybenzamine
• binds covalently to alpha receptors– irreversible blockade of long duration (14-48hr)
– somewhat selective for alpha1
– duration of action is typically independent of kinetics
– the pharmacologic actions of phenoxybenzamine are primarily related to antagonism of alpha-receptor mediated-events.
– Most importantly, phenoxybenzamine attenuates catecholamine-induced vasoconstriction (pheochromocytoma).
– Low bioavailability/ side effects? Postural hypotension and tachycardia

14
Alpha Blockers
Pharmacologic effects• CV are of most interest
– arterial and venous tone are a function of alpha receptor activity, what does this mean for BP and vascular resistance?
– therefore, what is the effect of block? Why reflexive tachycardia?
– What will happen to the pressor response in the presence of an alpha antagonist? (prevent the pressor effects of usual doses of alpha agonists).

15
Alpha BlockersPharmacologic effects
– Other effects• nasal stuffiness• Miosis (alpha receptors which play a role in
mydriasis are blocked)• may be used in patients to decrease difficulty in
urination, reduces resistance to flow at the prostate and base of bladder (the bladder base, urethral sphincter and prostate contain alpha receptors that mediate contraction and therefore promote urinary continence when activated)

16
Alpha Blockers• Specific Agents
– prazosin, terazosin, doxazosin (competitive antagonists)• useful in hypertension• all tend to have rel selective alpha 1 effects
– tamsulosin (competitive antagonists)• used in prostatic hyperplasia• may have some selectivity for prostatic alpha 1 receptors
– Phentolamine (competitive antagonists)• mostly of experimental and historical interest• blocks alpha 1 and 2, complex effects• also blocks H1 and H2; and 5HT responses
– Phenoxybenzamine• irreversible; somewhat selective for alpha1• also has action at H1, AcH, and 5HT• used primarily for pheochromocytoma

17
Alpha BlockersClinical Uses
– Pheochromocytoma– Hypertensive emergency– Chronic Hypertension (typically alpha 1 blockers used)– Peripheral vascular disease (Raynaud’s)– Local vasoconstrictor excess (to reverse local vasoconstrictor effects of
administered drugs, e.g., NE); inadvertent infiltration of agonist into subcutaneous tissue during intended I.v. administration.
– Urinary obstruction: Benign prostatic hyperplasia.– Male sexual dysfunction (local injection, long-term consequences
unclear)
What is orthostatic hypotension? What might it have to do with alpha What is orthostatic hypotension? What might it have to do with alpha blockers??blockers??

18
Adrenoreceptor AntagonistsAdrenoreceptor Antagonists• Used for hypertension, arrhythmias, angina and infarction
• Antihypertensive action depends upon:
–Reduced cardiac output–CNS action, reduced sympathetic activity –Reduction of renin release (What’s this??)
• angiotensin produced through action of renin
• angiotensin is a potent pressor agent
Receptors:Receptors:
1 found in heart muscle
2 found in vasculature, bronchi; produces smooth muscle relaxation

19
Adrenoreceptor Adrenoreceptor AntagonistsAntagonists
Metoprolol is metabolizedby CYP IID6.
What might that mean?

20
ß Blockers
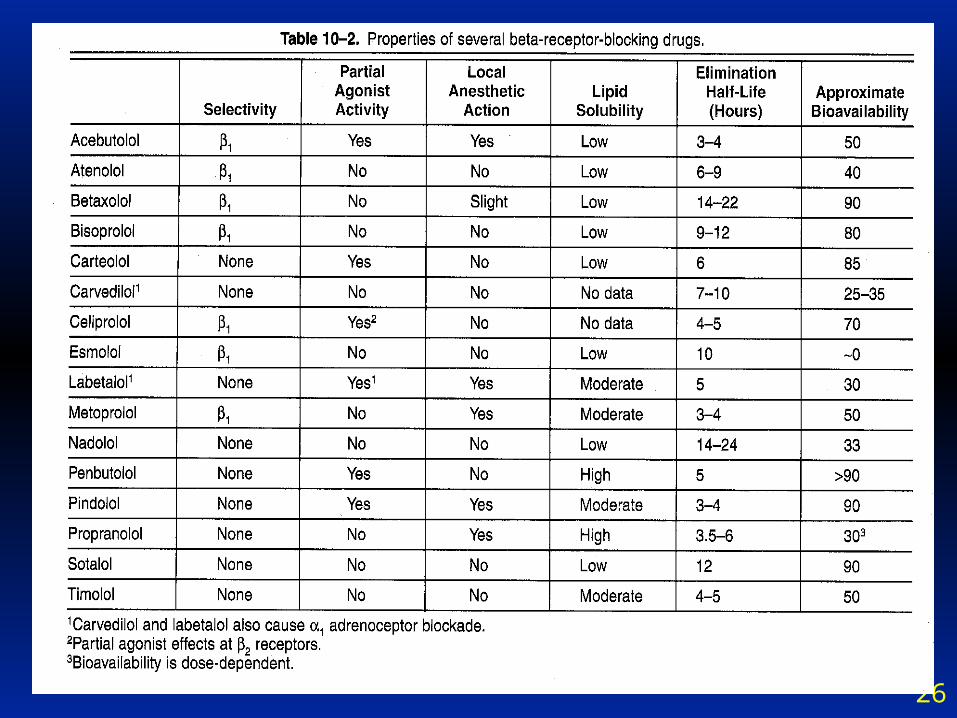
• Kinetics– typically well-absorbed– Bioavailablity varies (see Table 10-2)– typically well-distributed (Vd)– Interestingly clinical effect may extend beyond that
predicted from half-life (Lipid storage?)• Dynamics
– CV, Respiratory tract, eye, metabolic and endocrine• Clinical uses
– hypertension, ischemic heart disease, arrhythmias, glaucoma, hyperthyroidism, headache, anxiety, alcohol withdrawal, CHF

21
How does a Beta Blocker alter E action?
This is primarily alphaThis is primarily beta
Blood pressure is still elevatedby epinephrine because vasoconstriction is not blocked.

22
ß Blockers• Membrane stabilizing actions
– unrelated to ß effects– some ß blockers have Na+ channel blocking activity– This results in a “anesthetic-like” action
• effect on heart, neurons and skeletal muscle
– unlikely that this effect is important after systemic administration of these drugs, since the concentration in plasma usually achieved by these routes is too low for the anesthetic effects to be evident.
– This effect is probably not important for the CV actions of these drugs, but should be avoided if the drug is used locally in the eye-- local anasthesia of the cornea is undesirable.

23
Beta Blockers Improve Survival
Pederson, NEJM, 1985, 313:1055 in patients post MI

24
Drugs with Drugs with Adrenoreceptor AntagonistAdrenoreceptor AntagonistActionAction
• Propanolol**• Metoprolol• Nadolol• Atenolol• Carteolol• Betaxolol• Bisoprolol• Pindolol• Acebutolol• Penbutolol
• Labetolol• Carvedilol• Levobunonol• Celiprolol
** prototype
25
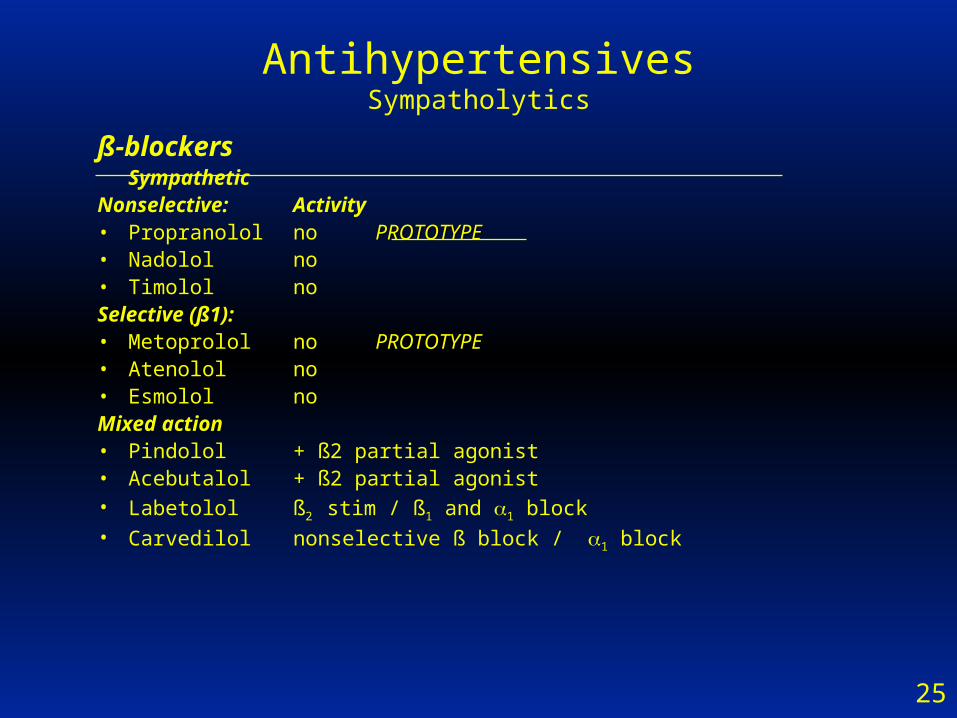
AntihypertensivesSympatholytics
ß-blockersSympathetic
Nonselective: Activity• Propranolol no PROTOTYPEPROTOTYPE• Nadolol no• Timolol noSelective (ß1):• Metoprolol no PROTOTYPEPROTOTYPE• Atenolol no• Esmolol noMixed action• Pindolol + ß2 partial agonist• Acebutalol + ß2 partial agonist• Labetolol ß2 stim / ß1 and 1 block• Carvedilol nonselective ß block / 1 block
26

27
ß Blocker Toxicity issues
• Rash, fever (minor;rare)• CNS effects:
– sedation, sleep disturbance, depression (may need to discontinue)• Effects in asthma patients
– beta receptor blockade may precipitate attacks, even in mild asthmatics
• CV issues– reduction in heart function (rate, contractility)– use cautiously in MI and CHF patients
• Discontinuation problems– requires dose tapering; may be due to upregulation of ß R

28
ß Blocker Therapeutics
• Arrhythmias– these drugs slow ventricular response rates in atrial flutter and
fibrillation• sotalol has additional antiarrhythmic effects involving ion channel blockade
• Ischemic Heart Disease– these drugs reduce the frequency of anginal episodes– these drugs may reduce the size of myocardial infarctions
• Hypertension– unclear– mechanism may include effects on the heart and blood vessels,
suppression of the renin-angiotensin system and quite possibly effects in the CNS.

29
ß Blocker Therapeutics
• Glaucoma
– topical administration (timolol lacks local anesthetic properties)
– inhibition of aqueous humor production mediated by beta-adrenergic receptors on the ciliary epithelium.
• Reduces secretory activity and intraocular pressure
• other beta blockers used to treat glaucoma– betaxolol, carteolol, levobunolol, metipranolol

30
ß Blocker Therapeutics
• Hyperthyroidism
– excessive catecholamine action is an important aspect of the pathophysiology of hyperthyroidism, especially in relation to the heart.
– Blockade of adrenergic receptors
– inhibition of the peripheral conversion of thyroxine to triiodothyronine??? Perhaps also contributing to anti-hyperthyroidism action
– propranolol has been used extensively in patients with thyroid storm (severe hyperthyroidism)

31
ß Blocker Therapeutics
• Neurologic diseases– several studies show a beneficial effect of propranolol in
reducing the frequency and intensity of migraine headache• other beta blockers with this action include:
– metoprolol
– atenolol
– timolol
– nadolol

32
ß Blocker Therapeutics
• Cirrhosis– beta receptor antagonists have been found to diminish
portal vein pressure in patients with cirrhosis.
– there is evidence that both propranolol and nadolol decrease the incidence of the first episode of bleeding from esophageal varices and decrease the mortality rate associated with bleeding in patients with cirrhosis.

33
ß Blocker: Propranolol
• Nonselective -antagonist• Therapeutic Effects
– Lowers blood pressure by decreasing cardiac output
– Diminish intraocular pressure in glaucoma (decreased aqueous humor secretion)
– Effective in reducing migrane episodes (may block catecholamine-induced vasodilation in the brain vasculature.

34
ß Blocker: Propranolol
• Therapeutic Effects (continued)– Angina pectoris (decreases the oxygen
requirements of heart muscle); does not allow for strenous exercise– tennis
– Myocardial infarction (propranolol has a protective effect on the myocardium– patients appear to be protected against a 2nd heart attack)
– Hyperthyroidism• Effective at blunting the widespread stimulation that
occurs in hypothyroidism

35
ß Blocker: Adverse Effects
• Adverse effects– Bronchoconstriction (beta2 is blocked;
contraindicated in patients with obstructive pulmonary disease).
– Arrhythmias (DRUG MUST BE TAPERED OFF GRADUALLY)
– Impaired sexual functioning in men (mechanism unclear)
– Altered metabolism (impaired glycogenolysis and decreased glucagon sectrion– fasting hypoglycemia)

36
ß Blocker: Adverse Effects
• Drug InteractionsInhibitors of propranolol metabolism
cimetidine (inhibitor of gastric acid secretion)furosemide (diuretic)
chlorpromazine (anti-schizophrenia)
Inducers of propranolol metabolismbarbituratesphenytoinrifampin





























