-
8/12/2019 10. Kuliah PEM sm I - 2014
1/57
-
8/12/2019 10. Kuliah PEM sm I - 2014
2/57
Malnutrition = imbalance between energyintake and energy
expenditure
Under nutrition:
Protein energy
malnutrition / PEM Micro-nutrient deficiency /
hidden hunger
Over nutrition:
obesity
7/1/14igustilanangsidiartha
2
-
8/12/2019 10. Kuliah PEM sm I - 2014
3/57
3
EXCESS NUTRITION(Energy, fat, cholesterol, carbohydrate, salt,
vitamins)
NORMAL NUTRITION
DEFICIENCYPRIMARY(Lack of food, poverty,
ignorance, refusal totake food, fad diet,alcoholism,drug
addiction,loneliness etc)
SECONDARY(Malabsorption,
defective metabolism,increased destruction,increased
excretion)
TISSUE DEPLETION
BIOCHEMICAL LESION
CLINICAL SIGNS
Blood and urinestudies: reducednutrient levels,abnormal
metabolites,enzyme changes)
(Robinson & Weigley, 1984)
Pathophysiology of malnutrition
7/1/14igustilanangsidiartha
-
8/12/2019 10. Kuliah PEM sm I - 2014
4/57
Classification of PEM
Based on the severity of deficiency:
Mild
Moderate .. no specific clinical sign Severe PEM:
Kwashiorkor
Marasmus
Marasmic-Kwashiorkor
!7/1/14igustilanangsidiartha
4
-
8/12/2019 10. Kuliah PEM sm I - 2014
5/57
Characteristics of
Kwashiorkor and MarasmusKwashiorkor
Age usually over 18 months
Lacks protein-rich foods and othernutrients
Relatively more often in tropicalcountries
wet malnutrition
Any edema means severemalnutrition, child is not fat
Swollen belly from fatty liver, edemaand/or parasites
Marasmus
Usually under 1 year old
Lacks energy-rich foods andother nutrients
Often in dry climate/disaster/war
dry malnutrition
Classified as severe malnutrition
May be swollen belly fromparasites or weak muscle
7/1/14igustilanangsidiartha
5
-
8/12/2019 10. Kuliah PEM sm I - 2014
6/57
Clinical manifestation of Kwashiorkor
Mental changes: irritable,apathies
Flag sign
Moon face
Liver enlargement (fatty liver)
Crazy pavement dermatosis
Potbelly (swollen abdomen)
Edema
7/1/14igustilanangsidiartha
6
-
8/12/2019 10. Kuliah PEM sm I - 2014
7/57
Clinical manifestation of Marasmus
Loss of subcutaneous fat and
muscle wasting
Old man face / monkey face
Piano ribs
Baggy pant
Hungry
7/1/14igustilanangsidiartha
7
-
8/12/2019 10. Kuliah PEM sm I - 2014
8/57
Edema in kwashiorkor
Pitting edema
Pathophysiology:
Low protein intake
hypoalbuminemialow
plasma oncotic pressure
fluids extravasations to
interstitial tissue
Edema most commonly
occurs in the feet
7/1/14igustilanangsidiartha
8
-
8/12/2019 10. Kuliah PEM sm I - 2014
9/57
-
8/12/2019 10. Kuliah PEM sm I - 2014
10/57
Diagnosis
Based on:
Clinical:
Anamnesis
Physical examination
Anthropometry
Laboratory
7/1/14igustilanangsidiartha
10
-
8/12/2019 10. Kuliah PEM sm I - 2014
11/57
Clinical
Anamnesis:
Dietary history
A detail dietary history mustbe taken
Quality and quantity of foodingested must be assessed
Medical history
Antenatal and perinatalhistory
Family history of atopic
Previous illness andhospitalization
Physical exam
Symptoms and signs ofkwashiorkor and marasmus
7/1/14igustilanangsidiartha
11
-
8/12/2019 10. Kuliah PEM sm I - 2014
12/57
Anthropometry
Commonly use: body weight and body height
Indicator:
Weight for age (W/A) Height for age (H/A)
Weight for height (W/H)
For adolescent (10-18 years) and adult:
Body mass index (BMI): weight (kg) / height (m) square Criteria
for severe malnutrition:
Adolescent: BMI for age less than 5thpercentile
Adult: BMI less than 16
7/1/14igustilanangsidiartha
12
-
8/12/2019 10. Kuliah PEM sm I - 2014
13/57
Criteria of diagnosis
Clinical Anthropometry Diagnosis
With edema W/H between -3SD
and -2SD
Kwashiorkor
With edema W/H < -3SD Marasmic-Kwashiorkor
Without edema W/H < -3SD Marasmus
7/1/14igustilanangsidiartha
13
-
8/12/2019 10. Kuliah PEM sm I - 2014
14/57
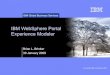
WHO growth standardchart
For example:
Boy, BW 7 kg,
H 75 cm
anthro < -3SD
Clinical sign
without
edema
Diagnosis
marasmus
7/1/14igustilanangsidiartha
14
-
8/12/2019 10. Kuliah PEM sm I - 2014
15/57
WHO growth standardtable
Boy, 7 kg
and 75 cm
Anthro < -
3SD
Clinical
sign with
edema
Diagnosis:marasmic-
kwashiork
or
7/1/14igustilanangsidiartha
15
-
8/12/2019 10. Kuliah PEM sm I - 2014
16/57
Laboratory
Blood analysis:
white blood cell, electrolytes, sugar,plasma protein
Urine analysis:
culture, ketone
Stool analysis:
for parasites
X-rayfor chest and heart
Tuberculintest for TB
7/1/14igustilanangsidiartha
16
-
8/12/2019 10. Kuliah PEM sm I - 2014
17/57
Management
general principles (ten steps)1. Treat/prevent hypoglycemia
2. Treat/prevent hypothermia
3. Treat/prevent dehydration
4. Correct electrolyte
imbalance
5. Treat/prevent infection
6. Correct micronutrient
deficiencies
7. Start cautious feeding
8. Achieve catch-up growth
9. Provide sensory stimulation
and emotional support
10. Prepare for follow-up after
recovery
7/1/14igustilanangsidiartha
17
-
8/12/2019 10. Kuliah PEM sm I - 2014
18/57
Initial treatment
Hypoglycemia
Blood glucose < 3 mmol/L or 5g/kg of body weight/d x 3
days
Most important determinant of recovery:
Amount of energy consumed: calories, protein,
micronutrients (K, Mg, I, Zn)
7/1/14igustilanangsidiartha
23
-
8/12/2019 10. Kuliah PEM sm I - 2014
24/57
Rehabilitation
Parental teaching
Correct feeding/food preparation practices
Stimulation, play, hygiene Treatment diarrhea, infections
When to seek medical care
Preparation for outpatient care
Reintegration into family & community
Prevent malnutrition recurrence
7/1/14igustilanangsidiartha
24
-
8/12/2019 10. Kuliah PEM sm I - 2014
25/57
-
8/12/2019 10. Kuliah PEM sm I - 2014
26/57
Criteria for outpatient care
Child
W/H reached -1SD
Eating appropriate amount of diet that mother can prepare at
home
Gaining weight at normal rate
Vitamin & mineral deficiency treated/corrected Infections
treated
Full immunizations
Mother
Able & willing to care for child
Knows proper food preparation Knows appropriate toys & play
for child
Knows home treatment fever, diarrhea, respiratory tract
infection
Health worker
Able to ensure follow up child & support for mother
7/1/14igustilanangsidiartha
26
-
8/12/2019 10. Kuliah PEM sm I - 2014
27/57
Follow up
Child usually remains stunted
Prevention of recurrence severe malnutrition
Follow up: 1,2,4 weeks, then 3 & 6 mos, then 2x/y
W/H no less than -1SD
Assess overall health, feeding, play
Immunizations, treatments, vitamin/minerals
Record progress
7/1/14igustilanangsidiartha
27
-
8/12/2019 10. Kuliah PEM sm I - 2014
28/57
Time frame for management
7/1/14igustilanangsidiartha
28
-
8/12/2019 10. Kuliah PEM sm I - 2014
29/57
Childhood Obesity
I Gusti Lanang SidiarthaSpesialis Anak Konsultan Nutrisi dan
Penyakit Metabolik
Bagian Ilmu Kesehatan Anak FK UNUD/RSUP Sanglah
-
8/12/2019 10. Kuliah PEM sm I - 2014
30/57
Definition
Childhood Obesity is a condition where excess body
fat negatively affects a childs health or wellbeing.
Obesity results from excessive caloric intake,decreased energy
expenditure and/or from a
combination of the two.
7/1/14igustilanangsidiartha
30
-
8/12/2019 10. Kuliah PEM sm I - 2014
31/57
Criteria for obesity based on BMI (WHO)
BMI (Body Mass Index) = Weight (kg) / Height (m)2
Underweight : < 18.5
Healthy weight : 18.524.9 Overweight (Grade I obesity) :
25.029.9
Obese (Grade II) : 30.039.9
Morbidly obese (Grade III) : 40 or above
Super obese (Grade IV) : > 50
for Adult
7/1/14igustilanangsidiartha
31
-
8/12/2019 10. Kuliah PEM sm I - 2014
32/57
forchildren and adolescence
Percentile of BMI-for-age and
gender
Underweight : < P-5
Healthy weight : P-5P-85
Overweight : P-85P-95
Obese : P-95P-97
Super obese : > P-97
7/1/14igustilanangsidiartha
32
-
8/12/2019 10. Kuliah PEM sm I - 2014
33/57
Classifications
Nutritional:
High
No mental retardation
No dismorphic
Normal bone age
Non-nutritional:
Endocrine: short
Hypothyroidism
Growth hormone deficiency
Genetic:
Prader-Willi
Turner
CNS conditions: hypothalamicdamage
Medications:
Glucocorticoids
Phenothiazine
Lithium, etc.
7/1/14igustilanangsidiartha
33
-
8/12/2019 10. Kuliah PEM sm I - 2014
34/57
Etiology
Heterogeneous and multifactorial
Environmental
Psychosocial
Genetic
7/1/14igustilanangsidiartha
34
-
8/12/2019 10. Kuliah PEM sm I - 2014
35/57
Genetics vs. Environment
Weight of adopted children correlate
better with biological parents
BMI of identical twins reared apart =together
Monozygotic twins more similar in fat
deposition and weight than dizygotic
twins.
7/1/14igustilanangsidiartha
35
-
8/12/2019 10. Kuliah PEM sm I - 2014
36/57
Environmental factors: Increased energy input
High caloric-density food
Supersized portions
Eating out
Working parents
Advertising
7/1/14igustilanangsidiartha
36
37
-
8/12/2019 10. Kuliah PEM sm I - 2014
37/57
Environmental factors: decreased energyexpenditure
TV: prevalence of obesity increases
2%/hour of viewing
Computers
Transportation
Inadequate safe areas for physical
activity
Sedentary lifestyle
7/1/14igustilanangsidiartha
37
38
-
8/12/2019 10. Kuliah PEM sm I - 2014
38/57
Complications
Diabetes type 2
Hypertension and heart
disease
Neurologic complications
Respiratory disease
Orthopedic condition
Psychosocial disorders
Hyperlipidemia
GI manifestations
Menstrual disorders
7/1/14igustilanangsidiartha
38
39
-
8/12/2019 10. Kuliah PEM sm I - 2014
39/57
Metabolic syndrome
Clustering of CV risk factors
related to insulin resistance
Including: Insulin resistance
Dyslipidemia
Hypertension
Obesity
7/1/14igustilanangsidiartha
39
40
-
8/12/2019 10. Kuliah PEM sm I - 2014
40/57
Obesity: respiratory diseases
Causes both restrictive and
obstructive disease
Sleep apnea 7-33%
Asthma ~ 30%
7/1/14igustilanangsidiartha
40
41
-
8/12/2019 10. Kuliah PEM sm I - 2014
41/57
Obesity: GI manifestations
Steatohepatitis
Fatty infiltration of the liver
Abnormal insulin metabolism
10% obese teens increased LFT
Can progress to fibrosis and cirrhosis
Gall bladder disease
Increased cholesterol excretion ~30% of gallstones in
children
7/1/14igustilanangsidiartha
41
42
-
8/12/2019 10. Kuliah PEM sm I - 2014
42/57
Obesity: orthopedic conditions
Genu varum/valgus deformities
Blount disease
Bowing of legs
Tibial torsion
50-80% obese
Slipped capital femoral epiphysis (SCFE)
Femoral epiphysis slips off of metaphysis
60% obese
Associated with hypothyroidism,
hypogonadism & GH deficiency
7/1/14igustilanangsidiartha
42
43
-
8/12/2019 10. Kuliah PEM sm I - 2014
43/57
Neurologic complications: Pseudotumor cerebri
Increased ICP
Vomiting, diplopia, blurred vision
30-80% obese
7/1/14igustilanangsidiartha
43
-
8/12/2019 10. Kuliah PEM sm I - 2014
44/57
45
-
8/12/2019 10. Kuliah PEM sm I - 2014
45/57
Obesity: psychological disorders
Difficult to quantitate
Stigmatization
Low self esteem
Depression
Discrimination
7/1/14igustilanangsidiartha
45
46
-
8/12/2019 10. Kuliah PEM sm I - 2014
46/57
Management
Prevention is the Key and prevention easier than cure
Team work
Individualized goal of weight loss; lifelong weight control
Components:
Education & motivation
Diet modification: decrease energy intake
Increased activity: increase energy expenditure
Parents are role models
Medicines & surgery
7/1/14igustilanangsidiartha
46
47
-
8/12/2019 10. Kuliah PEM sm I - 2014
47/57
Education
Need to educate family
Parents impose their lifestyle
+ family support improves weight loss
7/1/14igustilanangsidiartha
47
48
-
8/12/2019 10. Kuliah PEM sm I - 2014
48/57
Dietary therapy
Weight loss determined by # calories consumed
relative to expended
Healthy diet:
55% carbohydrates
30% fat
15% protein
Avoid fad diets
7/1/14igustilanangsidiartha
48
49
-
8/12/2019 10. Kuliah PEM sm I - 2014
49/57
Dietary therapy
Fat vs Carbs
Carb converted to fat 30% of energy consumed
Little energy used in absorbing fats
Glycemic Index
High carb diets
Leads to increased serum insulin
Promotes excessive food intake
7/1/14igustilanangsidiartha
49
50
-
8/12/2019 10. Kuliah PEM sm I - 2014
50/57
Physical activity
Physical activity essential for weight loss
Physical activity decreases 50% during adolescence
(girls > boys)
7/1/14igustilanangsidiartha
51
-
8/12/2019 10. Kuliah PEM sm I - 2014
51/57
Pharmacotherapy
Anti-obesity drugs not approved for pediatrics
None of drugs tested for:
Long term use Pediatric age groups
Drug options:
Appetite suppressants
Serotonin agonists
Inhibitors of fat absorption
Anti-hyperglycemic agents
7/1/14igustilanangsidiartha
-
8/12/2019 10. Kuliah PEM sm I - 2014
52/57
53
-
8/12/2019 10. Kuliah PEM sm I - 2014
53/57
Bariatric surgery or weight loss surgery
Works in three basic ways:
1. Restricting how much food
the stomach can hold at anytime
2. Preventing the digestive
system from absorbing all
the nutrition in the food
3. Combination of these two
ways
7/1/14igustilanangsidiartha
54
-
8/12/2019 10. Kuliah PEM sm I - 2014
54/57
Surgery indications
BMI greater than 40 (obese
class III)
BMI of 35-40 for people withheart disease, diabetes, high
cholesterol, or obstructive
sleep apnea
7/1/14igustilanangsidiartha
55
-
8/12/2019 10. Kuliah PEM sm I - 2014
55/57
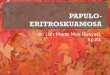
Types of weight loss surgery
Gastric banding and
gastroplasty (stomach
stapling): restrictive or
decrease the stomach sizefrom about six cups to one.
Gastric bypass (Roux-en-Y)
: reduces the size of the
stomach and prevent theabsorption of calories in the
small intestine.
7/1/14igustilanangsidiartha
56
-
8/12/2019 10. Kuliah PEM sm I - 2014
56/57
Risks of bariatric surgery
The risk of dying is less than 1%
Serious complications are rare
The risk including:
Vomiting from eating more than the stomach pouch canhold
The band disintegrating
Band and staples fall apart, reversing the procedure
Stomach contents leaking into the abdomen
Nutritional deficiencies and health problems: reducedabsorption
of vitamin B-12, iron, and calcium.
7/1/14igustilanangsidiartha
57
-
8/12/2019 10. Kuliah PEM sm I - 2014
57/57
Thanks for your attention
Any question ?