-
7/23/2019 10 Obstetric Haemorage
1/50
ntepartum Hemorrhage
International
Obstetrical Hemorrhage
Obstetrical Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
2/50
ntepartum Hemorrhage
International
Principles Prompt diagnosis
Recognize reserve and ability to compensate
Resuscitate vigorously Identify underlying cause
Treat underlying cause
Obstetrical Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
3/50
ntepartum Hemorrhage
International
Antepartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
4/50
ntepartum Hemorrhage
International
Objectives
Definitions and Incidence
Etiology and Risk Factors
Diagnosis
Management- maternal and fetal assessment
- appropriate resuscitation
- no vaginal exam prior to
determining placental location
Individual Causes
-
7/23/2019 10 Obstetric Haemorage
5/50
ntepartum Hemorrhage
International
Definition
vaginal bleeding between 20 weeks and delivery
Incidence
2% to 5% of all pregnancies
various causes of antepartum haemorrhage- abruptio placenta 40%
- 1% of pregnancies
- unclassified 35%
- placenta previa 20% - % of pregnancies
- lower genital tract lesion 5%- other
-
7/23/2019 10 Obstetric Haemorage
6/50
ntepartum Hemorrhage
International
Etiology of APH
Cervicalcontact bleeding (e.g. intercourse, pap, neoplasia,
examination)
inflammation (e.g. infection)
effacement and dilatation (e.g. labour, cervical
incompetence)
Placental
abruptio
previa
marginal sinus rupture
Vasa previa
Other - abnormal coagulation
-
7/23/2019 10 Obstetric Haemorage
7/50
ntepartum Hemorrhage
International
Diagnostic Procedures
History and physical - No digital pelvicexam
Ultrasound
definitive test for previa
less useful in abruptio
Electronic Fetal Monitoring
for fetal compromise and uterine tone
Speculum do ultrasound first if possible
No digital pelvic exam
-
7/23/2019 10 Obstetric Haemorage
8/50
-
7/23/2019 10 Obstetric Haemorage
9/50
ntepartum Hemorrhage
International
Hemodynamic Resuscitation
Risk Factors Tests (No vaginal exam)
Fetal / Maternal Assessment
Mother or fetus unstable Mother and fetus stable
Labs / Fetal Monitoring
U/S vaginal exam
Delivery
Vaginal Bleeding
Mother or fetus unstableExpectant
consider ongoing loss, etiology,
gestation
-
7/23/2019 10 Obstetric Haemorage
10/50
ntepartum Hemorrhage
International
Management - ABC s talk to and observe mother and
fetus
large bore IV access
crystalloid (N/S)
CBC and coagulation status
cross-match and type
get HELP!
-
7/23/2019 10 Obstetric Haemorage
11/50
ntepartum Hemorrhage
International
Hemodynamic Resuscitation
early aggressive resuscitation to protect fetus and
maternal organs from hypoperfusion and to prevent
DIC stabilize vital signs
large bore IV crystalloid infusion, plasma expanders
follow hemoglobin and coagulation status
oxygen consumption is up 20% in pregnancy
-
7/23/2019 10 Obstetric Haemorage
12/50
ntepartum Hemorrhage
International
Fetal Considerations lateral position increases cardiac output
up to
30%
consider amniocentesis for lung indices
external fetal and labor monitoring
Kleihauer-Betke if suspected abruption
post-trauma monitor at least 4 hours for evidenceof fetal
insult, abruptio, fetal maternal transfusion
-
7/23/2019 10 Obstetric Haemorage
13/50
ntepartum Hemorrhage
International
Abruptio Placenta - Definition
premature separation of normally implanted
placenta
Abruptio Placenta - Classification
Total - fetal death
Partial - fetus may tolerate up to 30-50%abruption
-
7/23/2019 10 Obstetric Haemorage
14/50
ntepartum Hemorrhage
International
Risk Factors for Abruption hypertension: gestational and
pre-
existing
abdominal trauma cocaine or crack abuse
previous abruption
overdistended uterus
multiple gestation, polyhydramnios
smoking, especially >1 pack/day
-
7/23/2019 10 Obstetric Haemorage
15/50
ntepartum Hemorrhage
International
Clinical Presentation of Abruption
vaginal bleeding usually painful, unremitting
presence of risk factor
hemodynamic status may not correlate withamount of vaginal blood
loss - concealed
abruptio
may be evidence of fetal compromise
uterus - tender, irritable, contracting or tetanic
ultrasound rules out previa and may show clot
-
7/23/2019 10 Obstetric Haemorage
16/50
ntepartum Hemorrhage
International
ABRUPTION
Live Fetus Dead Fetus
coagulopathy
Delivery
(watch for DIC)
Assess Maturity
Maturity Immaturity
Vaginal delivery or C/S Steroids plus expectancyTransfusion?
Transfer?
-
7/23/2019 10 Obstetric Haemorage
17/50
ntepartum Hemorrhage
International
Placenta Previa - Definition placenta covers or lies near the
cervix
Placenta Previa - Classification
total - entirely covers the os partial - partially covers the
os
marginal - close enough to the os to increase risk
of bleeding as cervical effacement and
dilatation occur
-
7/23/2019 10 Obstetric Haemorage
18/50
ntepartum Hemorrhage
International
Risk Factors for Previa previous placenta previa
previous caesarian section or uterine surgery
multiparity (5% in grand multiparous patients)
advanced maternal age
multiple gestation
smoking
-
7/23/2019 10 Obstetric Haemorage
19/50
ntepartum Hemorrhage
International
Clinical Presentation of Previa vaginal bleeding usually
painless (unless in labour)
maternal hemodynamic status corresponds to
amount of vaginal blood loss
well tolerated by fetus unless maternal instability
uterus - non-tender, not irritable, soft
may have abnormal lie
ultrasound shows previa
-
7/23/2019 10 Obstetric Haemorage
20/50
ntepartum Hemorrhage
International
PREVIA
Assess maturity
Maturity Immaturity
Delivery by C/S (consider accreta) Steroids plus expectancy
May try vaginal if marginal Transfusion? Transfer?
-
7/23/2019 10 Obstetric Haemorage
21/50
ntepartum Hemorrhage
International
Vasa Previa - Definition
blood vessels in the membranes run across the cerv requires a
vellamentous insertion or succenturiate
lobe
Complication
ex-sanguination following amniotomy or ROM
Diagnosis Apt test or Kleihauer test on vaginal blood
terminal fetal bradycardia initial tachycardia or
sinusoidal FH
Prognosis fetal mortality as high as 50-70%
-
7/23/2019 10 Obstetric Haemorage
22/50
ntepartum Hemorrhage
International
Conclusions
assess maternal status and stability
assess fetal well-being
resuscitate appropriately assess cause of bleeding - avoid
vaginal exam
expectant management if appropriate
deliver if indicated based on maternal or fetal
status
-
7/23/2019 10 Obstetric Haemorage
23/50
ntepartum Hemorrhage
International
Kleihauer-Betke
Indications
Measures fetal cells in maternal circulation
Used in assessing for Rh Sensitization
Maternal blood Rh negative
Large antepartum bleed
Mechanism
Blood Film stained with acid elution
Fetal Hgb more acid resistant
Fetal RBC darkly stained, Maternal RBC "ghosts"Technique
Count Fetal cells per 50 low power fields
Five cells per 50 (lpf) = 0.5 ml bleed
Interpretation
Calculate Maternal Blood Volume (ml) =
(Pre-pregnant weight in kg) x 70 ml/kg x (1.0 + (0.5 x weeks
gestation/36)) -
Estimated Blood loss (ml) at time of testCalculate Fetal Whole
Blood (ml) =
(Fetal Cell Count/Maternal Cell Count) x Maternal Blood
Volume
Rh Immune Globulin (RhoGAM) Dose
Give 300 ug per 30 ml fetal whole blood or 15 ml pRBC
http://www.fpnotebook.com/OB58.htmhttp://www.fpnotebook.com/HEM108.htmhttp://www.fpnotebook.com/HEM108.htmhttp://www.fpnotebook.com/OB125.htmhttp://www.fpnotebook.com/OB125.htmhttp://www.fpnotebook.com/HEM108.htmhttp://www.fpnotebook.com/OB58.htm
-
7/23/2019 10 Obstetric Haemorage
24/50
ntepartum Hemorrhage
International
Indications
Assess for Vasa Previa in Late Pregnancy Bleeding
Mechanism
Differentiates Fetal from Maternal Blood
Technique
Collect bloody vaginal fluid
Add a small amount of tap water (Hemolyzes blood)Centrifuge
sample
Add 5 cc pink supernatant to 1 cc Sodium Hydroxide 1%
Read in 2 minutes (may be difficult)
Pink sample indicates fetal Hemoglobin
Yellow-Brown sample indicates adult Hemoglobin
Modified Apt Test
http://www.fpnotebook.com/OB14.htmhttp://www.fpnotebook.com/OB11.htmhttp://www.fpnotebook.com/HEM79.htmhttp://www.fpnotebook.com/HEM79.htmhttp://www.fpnotebook.com/HEM79.htmhttp://www.fpnotebook.com/HEM79.htmhttp://www.fpnotebook.com/OB11.htmhttp://www.fpnotebook.com/OB14.htm
-
7/23/2019 10 Obstetric Haemorage
25/50
-
7/23/2019 10 Obstetric Haemorage
26/50
ntepartum Hemorrhage
International
Objectives Definition
Etiology
Risk Factors
Prevention
Management
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
27/50
ntepartum Hemorrhage
International
Traditional Definition blood loss of > 500 mL following
vaginal delivery
blood loss of > 1000 mL following cesarean
delivery
Functional Definition
any blood loss that has the potential to produce or
produces hemodynamic instability
Incidence
about 5% of all deliveries
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
28/50
ntepartum Hemorrhage
International
Etiology of Postpartum Hemorrhage
Tone - uterine atony
Tissue - retained tissue/clots
Trauma - laceration, rupture, inversion
Thrombin - coagulopathy
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
29/50
ntepartum Hemorrhage
International
Risk Factors for PPH - Antepartum
previous PPH or manual removal
placental abruption, especially if concealed
intrauterine fetal demise
placenta previa
gestational hypertension with proteinuria
overdistended uterus (e.g. twins, polyhydramnios)
pre-existing maternal bleeding disorder (e.g. ITP)
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
30/50
ntepartum Hemorrhage
International
Risk Factors for PPH - Intrapartum
operative delivery - cesarean or assisted vaginal
prolonged labour
rapid labour
induction or augmentation
chorioamnionitis
shoulder dystocia
internal podalic version and extraction of second tw
acquired coagulopathy (e.g. HELLP, DIC)
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
31/50
ntepartum Hemorrhage
International
Risk Factors for PPH - Postpartum lacerations or episiotomy
retained placenta/placental
abnormalities uterine rupture
uterine inversion
acquired coagulopathy (e.g. DIC)
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
32/50
ntepartum Hemorrhage
International
Prevention
be prepared
active management of the third stage
- prophylactic oxytocin with delivery or with
delivery of anterior shoulder
10 U IM or 5 U IV bolus
20 U/L N/S IV run rapidly
- early cord clamping and cutting- gentle cord traction with
suprapubic
countertraction
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
33/50
ntepartum Hemorrhage
International
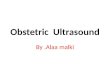
Active v.s Expectant Third Stage Management
Cochrane Library
Issue 1, 2000
PPH > 500 mL (n=4636)
PPH > 1000 mL (n=4636)
Maternal Hb < 91 (n=4256)
Blood transfusion (n=4829)
Therapeutic oxytocin (n=4829)
Nausea (n=3407)
Manual removal (n=4829)
0.1 1 10
Odds Ratio (95% Confidence Interval)
Outcome (subjects)
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
34/50
ntepartum Hemorrhage
International
Diagnosis - Is this a PPH?
consider risk factors
observe vaginal loss
express blood from vagina following C/S
REMEMBER
- blood loss is consistently underestimated
- ongoing trickling can lead to significant blood
loss
- blood loss is generally well tolerated to a point
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
35/50
ntepartum Hemorrhage
International
Diagnosis - What is the cause?
assess the fundus
inspect the lower genital tract
explore the uterus- retained placental fragments
- uterine rupture
- uterine inversion
assess coagulation
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
36/50
ntepartum Hemorrhage
International
A = airway
B = breathingC = circulation
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
37/50
ntepartum Hemorrhage
International
Management - ABCs
talk to and observe patient
large bore IV access ( 16
gauge)
crystalloid - lots!
CBC
cross-match and type get HELP!
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
38/50
ntepartum Hemorrhage
International
Management - Assess the fundus
simultaneous with ABC s
atony is the leading cause of PPH
if boggy bimanual massage
- rules out uterine inversion
- may feel lower tract injury
- evacuate clot from vagina and/or cervix
- may consider manual exploration at this
time
Postpartum Hemorrhage
P t t H h
-
7/23/2019 10 Obstetric Haemorage
39/50
ntepartum Hemorrhage
International
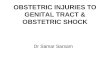
Management - Bimanual Massage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
40/50
P t t H h
-
7/23/2019 10 Obstetric Haemorage
41/50
ntepartum Hemorrhage
International
Management - Manual Exploration
if no response to bimanual massage and
oxytocin then proceed to exploration
manual exploration will:
- rule out uterine inversion
- palpate cervical injury
- remove retained placenta or clot from
uterus- rule out uterine rupture or dehiscence
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
42/50
ntepartum Hemorrhage
International
Replacement of Inverted Uterus
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
43/50
ntepartum Hemorrhage
International
Replacement of Inverted Uterus
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
44/50
ntepartum Hemorrhage
International
Management - Additional Uterotonics
ergotamine - caution in hypertension- 0.25 mg IM or 0.125 mg
IV
- maximum dose 1.25 mg
Hemabate (carboprost) - asthma is relative
contraindication- 15 methyl-prostaglandin F2
- 0.25 mg IM or intramyometrial
- Maximum dose 2 mg
Cytotec (misoprostil) - caution in asthma
- 400 mg pr or po
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
45/50
ntepartum Hemorrhage
International
Management - Bleeding with firm uterus
explore the lower genital tract
requirements - appropriate analgesia
- good exposure and lighting
appropriate surgical repair
- may temporize with packing
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
46/50
ntepartum Hemorrhage
International
Management - Continued uterine bleeding
possible coagulopathy - INR, PTT, TCT, fibrinogen
if coagulation is abnormal:
- correct with clotting factors, platelets
if coagulation is normal:
- prepare for O.R. (may consider embolization)
- rule out uterine rupture, inadequate incision repair
- consider uterine/hypogastric ligation, hysterectomy
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
47/50
ntepartum Hemorrhage
International
Management - ABC s
ENSURE that you are always
ahead with your resuscitation!!
consider need for Foley catheter, CVP, arterial line,
etc
consider need for more expert help
Postpartum Hemorrhage
Postpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
48/50
ntepartum Hemorrhage
International
Conclusions
be prepared
practice prevention
assess the loss
assess maternal status
resuscitate vigorously and
appropriately
diagnose the cause treat the cause
Postpartum Hemorrhage
ntepartum HemorrhagePostpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
49/50
International
Management - Evolution
Panic
PanicHysterectomy
Pitocin
Prostaglandins
Happiness
p g
ntepartum HemorrhagePostpartum Hemorrhage
-
7/23/2019 10 Obstetric Haemorage
50/50
International
Keep your bloody fingers offthe cervix!