Embed Size (px)
Citation preview

11
Strategic Clinical Networks & Clinical Care Pathways: Creating & Managing
Quality in Alberta Health Services
CEO Forum Feb 6, 2013Montreal
Dr Tom Noseworthy

22
Alberta Health Services
• One health care delivery system for an entire Province• The ‘third way’ in Canada• Largest health care system in Canada- 3.7 million people• Budget $12B, 100,000 employees, 7500 doctors• Formed in 2008, 5 Zones added in 2010, Networks in 2012• Nine clinical networks launched to date• Up to six more planned• We aspire to being the best in Canada

33
How will the Provincial Clinical Mandate of AHS be Accomplished?
• Strategic Clinical Networks• Clinically-led change• Performance measurement, research & best
evidence drive practice• Clinical care pathways• Clinical variance management & peer review

44
Goals of Clinical Networks?
• Achieve the best outcomes• Practice the highest quality of clinical care• Seek the greatest value from resources used• Engage clinicians in all aspects of this work

55
Why Clinical Networks?
• Networks are positive ways for all partners along a broad continuum to be involved in planning & improving care & service delivery
• Networks have been shown to be an effective mechanism to ensure collaboration, joint decision-making and shared learning
• Networks are a proven model to promote the use/uptake of clinical experience, knowledge and evidence-based clinical pathways to reduce clinical variation & improve care

66
What are Strategic Clinical Networks (SCNs)?
• Collaborative clinical teams with a provincial strategic mandate to improve quality & outcomes
• Led by clinicians, driven by clinical needs, focused on outcomes & based on best evidence
• Comprised of an all-inclusive membership, with 25 core members (community & specialty clinicians, patients, policy-makers, researchers) & leadership (0.5 Senior Medical Director, 0.5 Strategy Vice-President & 0.3 Scientific Director)

77
How do SCNs Work?
• Broad mandate:– Specific populations: seniors, women's health, children– High impact: cardiovascular disease & stroke– High burden: diabetes, obesity & nutrition, amh
• Scope encompasses entire continuum of care– From population health & prevention to primary care to
acute care to chronic disease management to palliation
• Projects & activities aligned with AH & AHS, priority-setting integrated with & into organizational decision-making
• Resourced & supported to improve clinical outcomes

88
Planned Support & Resources for Each SCN
• Dedicated Business Intelligence Unit– Project management, clinical analytics, case costing, quality
improvement, pathway development, patient safety, knowledge management, health technology assessment
• Embedded research capability and expertise• Education & skills development for leaders• Funding including:
– Seed money for innovation, initiatives, and research
– Remuneration of core members
– Opportunities to retain savings that are realized

99
First Six SCNs (June 12/12)
• Addiction and Mental Health• Bone and Joint Health• Cancer Care• Cardiovascular Health and Stroke• Obesity, Diabetes and Nutrition• Seniors’ Health

1010
Next Six SCNs (Fiscal 2013)
• Population Health and Health Promotion• Primary Care & Chronic Disease Management• Maternal Health• Newborn, Child, and Youth Health• Neurological Disease, ENT, and Vision• Complex Medicine (GI, Kidney & Respiratory)

1111
Operational Clinical Networks
Similar to SCNs
i. Provincial, clinically led teams
ii. Similar infrastructure & resources
Differ from SCNs
i. Responsible across populations
ii. Operationally focused
iii. Social determinants/ EOL agenda not required in projects

1212
Three Operational Clinical Networks (Jan13)
• Critical Care• Emergency Services• Surgical Services

1313
Snapshot of all 12 SCN ( & 3 OCN Projects)** 9/15 new projects are ready to initiate by January 31, 2013
Obesity, Diabetes & Nutrition
SCN
Bone & JointSCN
Surgery OCN
Emergency OCN
Addiction & Mental Health
SCN
Cardiovascular Health and Stroke
SCN
Insulin Pump
criteria**
Rural Stroke Program**
Vascular Risk Reduction
C-CHANGE**
Enhancing recovery after
surgery**
ARTE-referral**
Fragility & Stability -
Hip Fracture Rx and
Prevention**
Inappropriate use of
antipsychotics**
Cancer SCN
Critical Care OCN
Seniors’ HealthSCN
Depression Pathway
Safe Surgery Checklist**
aCATS** TBDTBD
Hip & Knee 5 year Plan
Lung Cancer
Elder Friendly Care**
3 avoid risks for AHS
2 Mature Tier 1: in flight
4 with some external funding
1 aligned with IHHP concept 3 Placeholders for SCN/OCN Equity
4 equally high value

1414
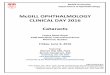
17.87
11.71
20.93
13.41
18.23
11.71
0
5
10
15
20
25
South Zone Calgary Zone Central Zone Edmonton Zone North Zone Best Large RHA/Zone (Calgary Zone, AB)
Risk
-Adj
uste
d Ra
te (p
er 1
00)
Source = CIHI CHRP
30-Day In-Hospital Mortality Following Stroke - 2010/11

1515
Project Scope:•Create standards and clear definition of rural stroke unit care•Implement early supported discharge (ESD) & enhanced stroke unit care in 5 small stroke centres•Implement enhancements to stroke unit care for 10 rural primary stroke centres
System Impact:• Acute care• Transition management
• Long term care
Project Financials:•Q4 (12/13): $ 141,964•13/14: $1,745,950• TOTAL Project: $2,873,594
Benefits to be Realized:Short term – Jan 31/ 13 – Mar 31 /14• ESD implemented in 5 small centres serving100 patients • 26% reduction in length of stay; 3 persons avoid nursing home care; 1 life savedLong term– 1- 3 year window • 214 new patients per year receive ESD and over 1000 new patients per year receiving full stroke unit services; 23 lives saved/year; 17 patients avoid nursing homes after stroke/year•Reduction in length of stay of over 20%
CV&S: Rural Stroke Action Plan