Embed Size (px)
Citation preview
8/4/2019 12 5 88 Claim Letter 5A
http://slidepdf.com/reader/full/12-5-88-claim-letter-5a 1/1
. . . __5#
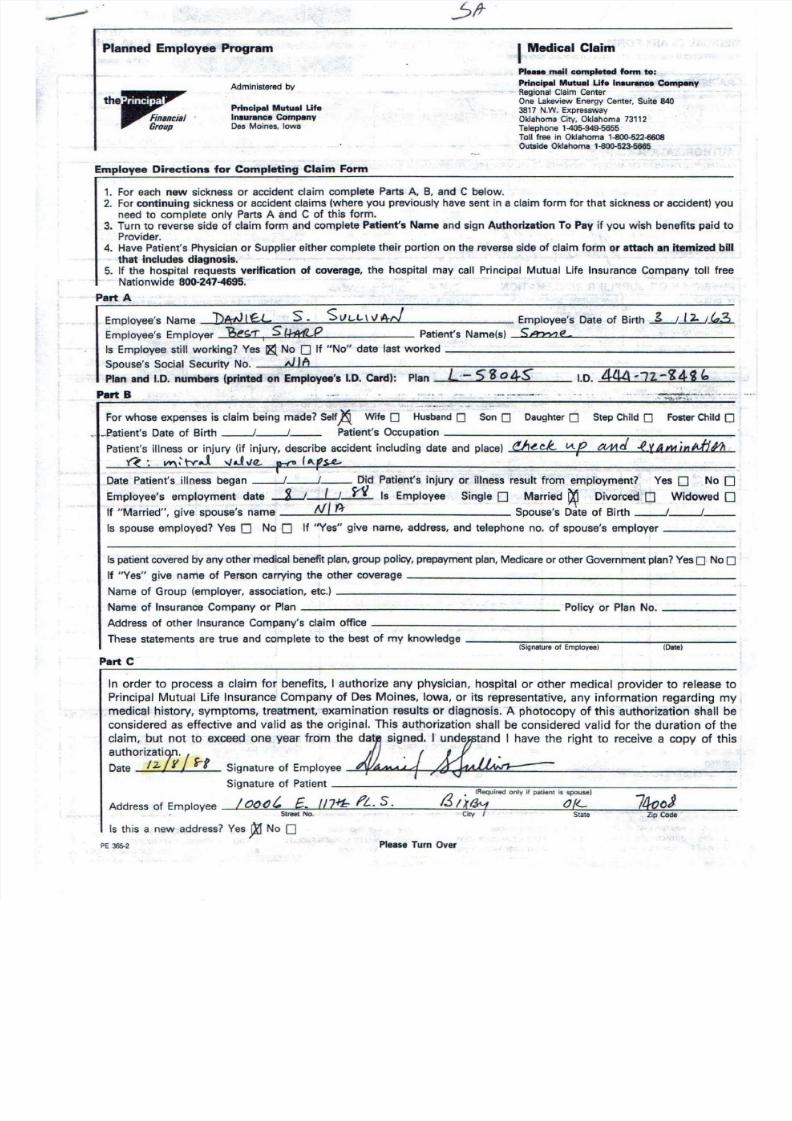
Planned Employee Program IMedical Claim
Pi.... man completed form to:
Principal Mutual Ute Inaurance' ComJHInyRegional Claim CenterOne Lakeview Energy Center. Suite B403817 N.W. ExpresswayOklahoma City. Oklahoma 73112Telephone 1 -405 · 949 · 56 55
Toll free in Oklahoma 1-1100·522·6608
Outside Oklahoma H30() '523-5665
Administered by
Principal Mutual UfeInaurance CompanyDes Moines. Iowa
Employee Directions for Completing Claim Form
1. For each new sickness or accident claim complete Parts A, B, and C below.2. For continuing sickness or accident claims (where you previously have sent in a claim form for that sickness or accident) youneed to complete only Parts A and C of this form.
3. Turn to reverse side of claim form and complete Patient's Name and sign Authorization To Pay if you wish benefits paid toProvider.
4. Have Patient's Physician or Supplier either complete their portion on the reverse side of claim form or attach an itemized bilthat includes diagnosis.
5. If the hospital requests verification of coverage, the hospital may call Principal Mutual Life Insurance Company toll freeNationwide 800-247-4695. '
Part A
Employee's Name Dt\fJ IfL S- S U , _ , _ \ \ ) 4,.) Employee's Date of Birth ~J.:b_;.k.3..Employee's Employer Be$([ I$1 - h 4 1 l . . P Patient's Name(s) _ S u : d ' J 7 7 ; J . . . . L . C J . . S , e _ ~ ~ _
Is Employee still working? Yes i & No 0If "No" date last worked _
Spouse~Social Securi~ N~_~~~ ~~-~~~~~---~~--~~-~~
Plan and 1.0. numbers (printed on Employee's 1.0. card): Plan L·-5S o4S" 1.0. 444 #72-~4i "Part B .','
, '" ~~>;;-7"~"" '- : ~
For whose expenses is ciaim being made?-self~ .Wife 0" H~;b~~~i~ Son0 Daughter0 StepChild0 FosterChild0
..•_Patient's Date of Birth__j__j__ Patient's Occupation ---; -:-_
Patient's illness or injury (if injury, describe accident including date and place) (!}'~ck til? t ' 1 M d .f~4minl1/l l1!v '< ~ " !'I ~ tv..J " ,J"e - p-r I"-S o L -
Date Patient's illness began__j__j __ Did Patient's injury or illness result from employment? Yes 0 No 0
Employee's employment date --i-J~ W Is Employee Single 0 Married ~ Divorced 0 Widowed 0
If "Married", give spouse's name A I / f . ) - - Spouse's Date of Birth__j~ __
Is spouse employed? Yes 0 No 0 If "Yes" give name, address, and telephone no. of spouse's employer _
Ispatientcovered by any other medical benefit plan, group policy, prepayment plan, Medicareor other Government plan?Yes0No0
If "Yes" give name of Person carrying the other coverage --:-, _
Name of Group (employer, association, etc.) _
Name of Insurance Company or Plan Policy or Plan No.
Address of other Insurance Company's claim office _
These statements are true and complete to the best of my knowledge -;;::-----:-_-;-;:---;-_-;-- =-:-:- _
(SignaturefEmployee) (Date)
Part C
In order to process a claim for benefits, I authorize any physician, hospital or other medical provider to release t
Principal Mutual Life Insurance Company of Des Moines, Iowa, or its representative, any information regarding m
medical history, symptoms, treatment,.examination results or diagnosis. A photocopy of this authorization shall b
considered as effective and valid asthe original. This authorization shall be considered valid for the duration of th
claim, but not to exceed one year from the datil signed. I undef7StandI have the right to receive a copy of thi
authorizati~.
Date 12 -JI rl Signature of Employee 4"I /4AML.<{ 7'4r.~ - - ' .
Signature of Patient-----------/?--.~IR~~~u~ire~d~O~nl~Y~if~p=ati~en=l7-is~S=~=u=~7)-------
Address of Employee IOO()G, £ _ 117.f1::.;!?t.s. I.;) /Xfk.1 O le 7400jStreeto. Cir;-f - State ZipCode
Is this a. new address? Yes f t 1 No 0PE 36 5- 2 Please Turn Over
















![2017 JMSC Civ.88 IN THE SUPREME COURT OF ......[2017] JMSC Civ.88 IN THE SUPREME COURT OF JUDICATURE OF JAMAICA CIVIL DIVISION CLAIM NO. CLAIM NO. 2011HCV02898 BETWEEN CAROLE REID](https://img.pdfslide.net/doc/110x75/5e6354bb1ebce66588307c73/2017-jmsc-civ88-in-the-supreme-court-of-2017-jmsc-civ88-in-the-supreme.jpg)